Embed Size (px)
Citation preview

Br Heart J 1992;67:266-8
CASE REPORTS
Incessant atrial tachycardia accelerated bypregnancy
J Colin Doig, Janet M McComb, Douglas S Reid
AbstractA 24 year old patient presented withincessant atrial tachycardia during thecourse of a twin pregnancy. Medicaltreatment slowed the ventricular res-ponse without restoring sinus rhythm.During labour the tachycardia spontan-eously reverted to sinus rhythm. Sub-sequently the same arrhythmia wasdocumented with a slower ventricularresponse than during pregnancy.
RegionalCardiothoracicCentre, FreemanHospital, Newcastleupon TyneJ C DoigJ M McCombD S ReidCorrespondence toDr J Colin Doig, UniversityDepartment of Cardiology,Regional CardiothoracicCentre, Freeman Hospital,Newcastle upon Tyne,NE7 7DN.
Case reportAt 21 weeks' gestation of a twin pregnancy a 24year old patient was transferred for man-
agement of incessant supraventriculartachycardia because of concerns about theeffect on placental function. There was a threemonth history of palpitation and chest discom-fort, dizziness, and exertional dyspnoea thathad begun eight weeks into the pregnancy.
There was no history of viral illness and she hadbeen otherwise healthy with no previous his-tory of palpitation. At admission the heart ratewas 200 beats/min and systolic blood pressure
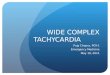
was 90 mm Hg. Her electrocardiogram showeda narrow QRS complex tachycardia withupright P waves in the inferior limb leads andVI, with a frontal P wave axis of + 900 (fig IA).The PR interval was 140 ms. Occasionally non-conducted P waves of identical configurationand timing were seen during the tachycardia(fig 1B). The rate of the arrhythmia showedconsiderable diurnal variability ranging from135 to 210 beats/min. Isolated ventricularextrasystoles did not reset the tachycardia.There was QRS alternans at ventricular ratesfaster than 190 beats/min. Haematologicalstudies, urea and electrolytes, and liver func-tion tests were normal. A free thyroxine plasmaconcentration of 164 nmol/l (normal range60-140) and thyroid stimulating hormone con-
centration of 1-4 IU/I (normal range 0 15-3-2)were consistent with pregnancy. Transthoracicechocardiography and chest x ray were normal.Fetal echocardiography showed normal heartsand rates.The arrhythmia did not respond to carotid
sinus massage, Valsalva manoeuvres or
intravenous verapamil. Digoxin was used with-out benefit and cardioversion did not restore
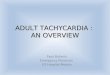
sinus rhythm or affect the ventricular responserate. Metoprolol and digoxin in combinationslowed the ventricular rate to 185 beats/minbut the diurnal fluctuation in PP and RRintervals continued. Flecainide was thereforeintroduced in place of metoprolol and digoxin.This slowed the atrial rate to 115 beats/min andallowed transient episodes of sinus rhythm at75 beats/min to appear with a frontal P waveaxis of + 10°. The PR interval was 200 ms withno evidence of pre-excitation (fig 2). This wasconsidered a satisfactory interim result and thepatient was discharged on oral flecainide100 mg three times daily. During the nextmonth the QRS duration increased from 80 msto 100 ms and the heart rate was never consis-tently below 130 beats/min on Holter monitor-ing. Because of this inadequate rate control,flecainide was stopped and amiodarone wasintroduced at a dose of 800 mg a day for oneweek and maintained at 400 mg daily. Thisslowed the heart rate to 110 beats/min. On thistreatment, she felt better, but was considerablyrestricted in her exercise capacity by palpita-tion, fatigue, and dyspnoea. There was noclinical evidence of heart failure or com-promised fetal development.At 31 weeks' gestation two healthy infants
were delivered vaginally by forceps. Sinusrhythm returned spontaneously and the moth-er's heart rate fell below 100 beats/min duringthe first stage of labour. After delivery shereported that palpitation had ceased and sheremained in sinus rhythm when seen in out-patients two weeks after hospital discharge.Amiodarone was stopped at this time and herelectrocardiogram was similar to that in fig 2.The diagnosis was therefore assumed to bepregnancy related atrial tachycardia and thiswas supported by the prominent left atrialcomponent to the P wave in sinus rhythm. Shewas re-referred, however, six months afterdelivery with non-cardiac symptoms at whichtime an electrocardiogram showed return ofatrial tachycardia with a ventricular rate of 1 15beats/min. She was on no antiarrhythmic treat-
ment.
DiscussionPregnancy is frequently associated with sinustachycardia and increased ectopic activity has
266
on June 29, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.67.3.266 on 1 M
arch 1992. Dow
nloaded from

Incessant atrial tachycardia accelerated by pregnancy
..4!::
'~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~...!..Fc
I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~....5... S a.~~~~~~~~~~~~~~ IK
-e:;-:~~~~~~~ ~ ~~ ~~~~~~~~~~~~~~~~~~.._.I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ O'
Figure I (A) Electrocardiogram showing narrow QRS tachycardia. (B) Rhythmstrip showing non-conducted P waves of identical configuration and timing duringtachycardia.
been noted both in the atrium and the ventriclethroughout pregnancy.'2 Paroxysmalsupraventricular tachycardia has been seen'and usually occurs in a patient with a history ofsupraventricular arrhythmias before preg-
nancy or in a patient with pre-existingrheumatic heart disease.5 Such arrhythmiasusually occur in the third trimester6 but thetrue incidence is unknown.7 Persistent atrial
Figure 2 Electrocardiogram after return to sinus rhythm.
267
tachycardia such as was present in this patientis uncommon and has rarely been reportedduring pregnancy.89 It has not previously beenseen reverting to sinus rhythm during labour.An automatic atrial tachycardia more typicallyoccurs in childhoodl'01 or complicating heartdisease'2 or metabolic upset including digitalistoxicity.'3 In this case, recurrence of the sametachycardia some months later suggests thatthe patient had a potential for atrial tachycardiaunrelated to pregnancy, but which first presen-ted at an accelerated rate during pregnancy.The mechanism of the tachycardia in this
patient was probably enhanced sympatheticreactivity of an ectopic atrial focus. Thisaccords with the increased plasma cate-cholamine concentrations and the increasedadrenergic receptor sensitivity during preg-nancy.4 " Increased atrial stretch due to plasmavolume enlargement might also be implicated.The possible influence of the high concentra-tions of oestrogen and progesterone in preg-nancy is unknown. An enhanced response toprostaglandins has been reported in preg-nancy, '5 and in susceptible patients this couldperhaps induce an atrial tachycardia.Thyrotoxicosis could also facilitate' atrialarrhythmias; but there was no clinical orbiochemical evidence of thyroid overactivity.Why the arrhythmia stopped during labour isnot clear.
Because the persistent atrial tachycardiamight have caused congestive cardiac failure inour patient'6'8 or have affected placental func-tion and subsequent fetal development'9 wetried to reduce the ventricular rate responsewhen sinus rhythm could not be restored. Themanagement of such arrhythmias in pregnancyis difficult. Verapamil, digoxin, or cardio-selective f blockade are appropriate andusually well tolerated.202' Flecainide seems tobe safe and cardioversion is not contrain-dicated.' Amiodarone is regarded as an agentof last resort because of concerns about neon-atal goitre and its presence in breast milk.2324An alternative treatment is to insert a tem-porary pacing electrode to terminate the arr-hythmia or convert it to atrial fibrillation.Though appropriate radiation protection couldbe used, pacing was not thought likely to besuccessful in our patient and we thought thatatrial fibrillation might further compromiseplacental function.This rare case highlights the risk that
inpatients with the potential for atrial tachycar-dia the condition can be precipitated andaccelerated by pregnancy. The arrhythmia waspersistent and led to unrealised concerns aboutplacental function but it reverted to sinusrhythm early during labour. Treatment of a
persistent tachycardia in pregnancy may bepotentially toxic to the mother or fetus or both.Despite a twin pregnancy and incessantsupraventricular tachycardia our patientdelivered two healthy infants.
1 Mendelson CL. Disorders of the heartbeat during preg-nancy. Am J Obstet Gynec 1956;72:1268-301.
2 Sullivan JM, Ramanathan KB. Management of medicalproblems in pregnancy-severe cardiac disease. N Engl JMed 1985;313:304-9.
on June 29, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.67.3.266 on 1 M
arch 1992. Dow
nloaded from

Doig, McComb, Reid
3 Oakley GDG. Pregnancy and heart disease. In: Julian DG,Camm AJ, Fox KM, Hall RJC, Poole-Wilson PA, eds.Diseases of the heart. London: Balliere Tindall, 1989:1363-71.
4 Kay J, Priano LL. Paroxysmal atrial tachycardia duringpregnancy. Anesthesiol Rev 1987;14:8-15.
5 Szekely P, Snaith L. Heart disease and pregnancy. Edin-burgh: Churchill Livingstone, 1974:90-101.
6 Perloff JK. Pregnancy and cardiovascular disease. In:Braunwald E, ed. Heart disease. 3rd ed. Philadelphia: WBSaunders, 1988:1848-69.
7 Metcalfe J, McAnulty JH, Ueland K. Burwell and Metcalfe'sHeart disease and pregnancy. 2nd ed. Boston: Little,Brown, 1986:307-35.
8 Proclemer A, Feruglio GA. Tachicardia "sinusale"idiopatica permanente in gravidanza. G Ital Cardiol1988;18:333-8.
9 Hubbard WN, Jenkins BAG, Ward DE. Persistant atrialtachycardia in pregnancy. BMJ 1983;287:327.
10 Olsson SB, Blomstrom P, Sabel KG, William-Olsson G.Incessant ectopic atrial tachycardia: successful surgicaltreatment with regression of dilated cardiomyopathypicture. Am J Cardiol 1984;53:1465-6.
11 Keane JF, Plauth WH, Nadas AS. Chronic ectopic tachycar-dia ofinfancy and childhood. AmHeart J 1972;84:748-57.
12 Haines DE, DiMarco JP. Sustained intraatrial reentranttachycardia: clinical, electrocardiographic and electro-physiologic characteristics and long-term follow up. JAmColl Cardiol 1990;15:1345-54.
13 Camm AJ. The recognition and management of tachyarr-hythinias. In: Julian DG, Camm AJ, Fox KM, Hall RJC,Poole-Wilson PA, eds. Diseases of the heart. London:Balliere Tindall, 1989:509-83.
14 Symonds EM. Pregnancy Hypertension. In: Julian DG,
Camm AJ, Fox KM, Hall RJC, Poole-Wilson PA, eds.Diseases of the heart. London: Balliere Tindall, 1989:1372-83.
15 Broughton Pipkin F, Morrison R, O'Brien PM. The effect ofprostaglandin El upon the pressor and hormonal responseto exogenous angiotensin II in human pregnancy. Clin Sci1987;72:351-7.
16 Vitale P, de Stefano R, Vitale N, Pisacane C. Disfunzionemiocardia conseguente a tachicardia sopraventricolare. GItal Cardiol 1989;19:928-32.
17 Antonelli Incalzi R, Gemma A, Frustaci A, Rossi E,Carbonin PU. Low atrial tachycardia as primary cause ofthe heart failure complicating congestive cardiomyopathy.Acta Cardiol 1989;44:335-9.
18 Cruz FES, Cheriex EC, Smeets JLRM, et al. Reversibilityof tachycardia-induced cardiomyopathy after cure ofincessant supraventricular tachycardia. J Am Coll Cardiol1990;16:739-44.
19 Homans DC. Peripartum cardiomyopathy. N Engl J Med1985;312: 1432-7.
20 Metcalfe J, McAnulty JH, Ueland K. Burwell and Metcalfe'sHeart disease and pregnancy. 2nd ed. Boston: Little,Brown, 1986:367-89.
21 Kendall MJ. Impact of beta 1 selectively and intrinsicsympathomimetic activity on potential unwanted non-cardiovascular effects of beta blockers. Am J Cardiol1987;59:44F-7F.
22 Schroeder JS, Harrison DC. Repeated cardioversion duringpregnancy. Am J Cardiol 1971;27:445-9.
23 Foster CJ, Love HG. Amiodarone in pregnancy. Case reportand review ofthe literature. Int J Cardiol 1988;20:307-16.
24 McKenna WJ, Harris L, Rowland E, Whitelaw A, Storey G,Holt D. Amiodarone therapy during pregnancy. Am JCardiol 1983;51:1231-3.
268
on June 29, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.67.3.266 on 1 M
arch 1992. Dow
nloaded from