Embed Size (px)
Citation preview

8334©
Saturday 21 May 1983
INCIDENCE AND PROGNOSTIC IMPORTANCE
OF JAUNDICE AFTER CARDIOPULMONARYBYPASS SURGERY
J. D. COLLINSR. FERNER
A. MURRAY†
M. F. BASSENDINEA. BLESOVSKY*D. T. PEARSON*
O. F. W. JAMES
Department of Medicine and Medical Physics†, and RegionalCardiothoracic Centre*, Freeman Hospital, Newcastle upon Tyne
Summary In a prospective study of 248 consecutivepatients undergoing cardiopulmonary
bypass surgery, early postoperative "post-pump" jaundice(PPJ) developed in 49 (20%). Development of PPJ wasstrongly associated with a bad outcome; 25% of jaundicedpatients and 1% of non-jaundiced patients died in the post-operative period. The jaundice was a conjugatedhyperbilirubinaemia, and was detectable in 48 out of 49patients by postoperative day 2. Hypotension, hypoxia, andhypothermia ("shocked liver") were not associated with thedevelopment of PPJ, nor was evidence of haemolysis or heart-failure. Although PPJ was significantly associated with
multiple valve replacement, higher transfusion requirements,and longer cardiopulmonary bypass time, it also occurred inpatients undergoing uncomplicated operations. It is
suggested that PPJ is caused by a defect in hepatic excretionof bilirubin.
Introduction
AFTER the widespread development of cardiopulmonarybypass surgery in the mid-1960s, it became apparent that
early postoperative jaundice (developing within two to threedays of surgery) occurred in a substantial number of cases,and retrospective studies showed an incidence of abouti0%.’ Retrospective studies suggested many possible riskfactors underlying the development of PPJ, which includedthe age of the patient,3 preoperative heart-failure,2,3hypoxia,4 bypass (perfusion) time, 3 blood-transfusion, 5-7hypothermia,8 haemolysis,2,9 sepsis,2,4 and shock.1,1O,11Despite improvements in preoperative ’management, in
surgical and anaesthetic techniques, and in postoperativecare, early "postpump" jaundice (PPJ) still occurs. Wetherefore decided to make a prospective study with thefollowing aims:
1. To determine the incidence of PPJ after modern cardio-pulmonary bypass surgery.
2. To determine the incidence of associated morbidity andmortality.
3. To analyse possible preoperative, peroperative, andpostoperative risk factors.
4. To describe the temporal course of biochemical changesassociated with PPJ.
Methods
Patients
248 patients over sixteen years old undergoing routine or
emergency cardiopulmonary bypass surgery in one centre wereconsecutively enrolled into the study.
Data Recorded
Preoperative.-Full blood-count, urea and electrolytes, aspartateaminotransferase (AST), bilirubin, alkaline phosphatase (AP), andHBsAg. Serum was stored at -80°C for further biochemical and
virological study. Preoperative right atrial pressure was recorded.Peroperative.-A record was made of operation type, bypass time,
oxygenator type, and flow rate and mode (pulsatile or non-pulsatile).Arterial oxygen tension (Pa02), oesophageal temperature, and meanarterial blood pressure (MAP) were measured continuously duringeach operation and minimum values for each were recorded. Plasmahaemoglobin, drugs, and anaesthetics used and amount of bloodtransfused were also recorded.
Postoperative.-We recorded minimum arterial oxygen tension,(mMAP) and right atrial pressure daily. We also kept a record of theuse of intra-aortic balloon pump, inotropic agents, and all drugs.Surgery was performed on day 0. Postoperative estimations ofserum bilirubin, AST, and AP were made on day 2 and on alternatedays thereafter until death or discharge. AST was also measuredwith creatine phosphokinase (CK) on days 0 and 1, serum alanineaminotransferase (ALT) was measured on days 2, 4, and 6. At eachsampling time serum was saved and stored at -80°C. Blood film,reticulocyte count, plasma haemoglobin and haptoglobin levels,and urinary haemosiderin and urobilinogen were examined todetect haemolysis. PPJ was defined as a bilirubin level >50 mol/1(equivalent to 3 mg/dl) within the first postoperative week.Conjugation of bilirubin was estimated 12 in serum in which totalbilirubin was >50 mol/1, and in all these patients serological viralstudies were performed to exclude infection with hepatitis A (HAVIgG+IgM), hepatitis B (HBsAg and HBcAb), cytomegalovirus(IgG and IgM), Epstein-Barr virus (IgG and IgM), herpes virus, andLeptospira. In the event of death, a post-mortem liver biopsyspecimen was obtained immediately if possible. We performedbacteriological culture of urine, sputum, blood, wound aspirate, andcentral catheter tips in every patient, and where appropriate ofpleural fluid or renal dialysate.Other observations.-In all PPJ patients abdominal ultrasound
examination of the extrahepatic biliary tree or post-mortem

1120
examination of the biliary tree was carried out. AP was typed in serawhere postoperative values exceeded 200 IU/1. A retrospectiveanalysis of the non-fasting concentration of the primary bile acid,cholic acid (cholylglycine), was undertaken on stored sera (RIAAbbott Laboratories Ltd). We measured preoperative and
postoperative concentrations on the day of maximum increase inbilirubin in all PPJ patients. These results were compared withresults from sera of 32 randomly selected non-PPJ patients.
Data AnalysisData were stored on a PDP11 computer so that the following
factors which may have been implicated in the pathogenesis of PPJcould be examined prospectively:
1. High preoperative alcohol consumption was assessed byquestionnaire; each patient was given a score of 0 (no alcohol), 1 (lessthan 40 g/day), 2 (40-80 g/day), or 3 (more than 80 g/day).
2. Preoperative hepatocellular damage, as reflected by raisedpreoperative serum AST.
3. Peroperative hypotension, measured by minimum meanarterial blood pressure (mMAP). A score to reflect both the level andduration of hypotension was devised: 1 =mMAP above 50 mmHgthroughout the operation (recognised as a minimum desirable
perfusion pressure). 2 = mMAP below 50 mmHg for less than 5 min.3=mMAP below 50 mmHg for longer than 5 min. Thus the higherthe score the greater the degree of peroperative hypotension.
4. Peroperative hypoxia was assessed by measuring minimumarterial oxygen saturation (in kPa).
5. Prolonged cardiopulmonary bypass time. The length of cardio-pulmonary bypass was recorded in minutes.
It was also possible to analyse the following factors which mighthave been associated with the pathogenesis of PPJ:Preoperative.-Age, serum bilirubin and alkaline phosphatase,
and right atrial pressure (as an indication of degree of right heart-failure).Peroperative.-Minimum oesophageal temperature, total blood
transfused, type of operation.Postoperattve.-Haemolysis, evidence of viral or bacteriological
infection. The use of anaesthetic agents and all drugs given before,during, and after every operative procedure was also analysed inrelation to PPJ.The results obtained in the PPJ and non-PPJ patients were
analysed by Student’s t and X2 tests.
Results
Incidence of Jaundice
Jaundice was found in 49 of 248 patients (20%). It
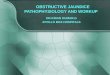
developed in the early postoperative phase; 48 out of 49 caseswere identified by day 2. It was usually short-lived; serumbilirubin was below 50 pmol/I in 26/41 patients surviving onday 8 (figs 1 and 2).
Mortality16 patients died. 2 died during operation and their data
were excluded from subsequent postoperative analysis. 12PPJ patients died (2507o mortality in the PPJ group), but only2 of 197 (1 %) non-PPJ patients died (p<0 00 I). ,
Possible Causative Factors
Preoperative estimated alcohol consumption, preoperativeAST, peroperative mMAP, or peroperative minimum Pa02were similar in the two groups. There was a significantdifference in mean bypass time between the PPJ group (102min) and the non-PPJ patients (89 - 5 min) (table I). Both meanpreoperative serum bilirubin and alkaline phosphatase weresignificantly higher in the 49 patients in whom PPJdeveloped than in the 197 in whom it did not (table n). Meanpreoperative right atrial pressure was greater in the PPJ
Fig I-Liver function tests after operation in 49 jaundiced patients.
Results are given as median ±34°lo range equivalent to the range of :tlSDfo!normally distributed data.
-
group than in the non-PPJ patients. Minimum peroperativfoesophageal temperature was slightly greater in the PPJ tharthe non-PPJ group. Mean blood transfusion requirement 01
patients in whom PPJ subsequently developed was almosttwice as great as that in the patients in whom it did notdevelop (10-1 ±7-5 5 units, 4±3 1 versus 5.3:t3’5 5 units,2’1±1’4 1). Table III shows the incidence of PPJ and themortality associated with the various operations performed,There was no evidence of significant postoperative
haemolysis in any PPJ patient; haemolysis was found in Ipatient whose maximum postoperative bilirubin was 22
mol/1. There were 7 cases of postoperative septicaemia (4PPJ patients, 3 non-PPJ patients). The pattern of post.operative liver function tests was similar in both jaundiced
TABLE I-ANALYSIS OF 5 PROSPECTIVELY SELECTED RISK FACTORS

1121
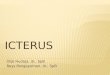
Fig 2-Liver function tests after operation in 197 non-jaundicedpatients.Bihrubm rose to between 17 and 49 mot/1 on day 2 in 140 patients.
and non-jaundiced patients. In both groups bilirubin rosepostoperatively and had almost invariably reached a
maximum by day 2. In all PPJ patients more than 75% ofbilirubin was conjugated. In a further 140 patientspostoperative bilirubin was raised without overt jaundiceoccurring. ,
Aspartate aminotransferase invariably rose on the day ofoperation, was markedly raised on day 2, and then fell rapidlytowards normal and did not markedly increase after day 6,except when there was good evidence for myocardialinfarction or when reoperation was necessary. That thispattern of enzyme release reflected cardiac muscle damage issupported by the changes seen in ALT and CK (figs 1 and 2).Serum alkaline phosphatase typically fell in both PPJ andnon-PPJ patients immediately after operation, thereafter
rising commonly to levels of about 150 IU/1 (normal <92IU/1) around postoperative day 10 (figs 1 and 2). In 39 patientsalkaline phosphatase exceeded 200 IU/1 (14 PPJ, 25 non-PPJpatients); in 2 instances it exceeded 850 IU/1. Serum alkaline
TABLE II-ANALYSIS OF OTHER POSSIBLE RISK FACTORS
I I
’Catheter data on 36/49 PPJ and 96/197 non-PPJ patients
TABLE III-INCIDENCE OF JAUNDICE AND DEATH ASSOCIATED WITHTYPE OF OPERATION RANKED IN FREQUENCY OF ASSOCIATED PPJ
TV=tricuspid valve. MV=mitral valve. AV=aortic valve. CA=coronaryartery. NS =not significant.
phosphatase generally began to fall after day 10, but at 6months 34 patients (12 PPJ, 22 non-PPJ) still had abnormallyraised concentrations. This was almost exclusively the resultof increases in the hepatic isoenzyme. Ultrasoundexamination of the biliary tree in patients with persistentlyhigh postoperative alkaline phosphatase concentrationsshowed no evidence of large bileduct obstruction.A liver specimen was obtained immediately post mortem in
7 PPJ patients. No evidence of cholestasis, massive liver-cellnecrosis, or underlying chronic liver disease was found. Somemild changes of chronic venous congestion were seen withdilatation of efferent venules and sinusoids and evidence ofmild centrilobular necrosis. A mild inflammatory cellinfiltrate with expansion of portal tracts was also noted insome instances. All but 2 of the 49 patients in whom PPJdeveloped had positive preoperative hepatitis A IgG, andonly 1 showed evidence of previous hepatitis-B infection(HBcAb-positive), while all patients showed evidence ofprevious exposure to cytomegalovirus (IgG), EB virus (IgG),and herpes virus. There was no evidence in any PPJ patient tosuggest reactivation of previous viral infection or evidence ofnew primary infection within the first postoperative month.
Serum Bile-acids
Preoperative serum concentrations of cholylglycine wereraised (> 150 jjg/dl) in 5 out of 49 PPJ patients and 1 out of 32non-PPJ patients. Postoperative concentrations were normalin all patients without PPJ, whilst they were raised in 24 PPJpatients; the highest concentration was 1300 g/dl.
Discussion
This prospective study has shown that despitedemonstrable improvements in all aspects of operative andperioperative care in the past 15 years PPJ is, if anything,more common than the figures suggested by the retrospectivesurveys of the late 1960s; 1,2 it occurred after 20% ofcardiothoracic bypass operations.98% of cases of PPJ were detected by postoperative day 2,
and 25% of patients with PPJ died. Thus a single serumbilirubin measurement on postoperative day 2 will identifythose patients at high risk in the ensuing postoperativeperiod. We wished to examine as many factors as possible todetermine the pathogenesis of PPJ. However, these were sonumerous that formal prospective analysis was limited to the

1122
5 factors regarded as being of greatest importance before thestudy was started. High preoperative alcohol consumptiondid not predispose to the postoperative development ofjaundice, nor was there a significant difference between meanpreoperative AST in the PPJ and non-PPJ patients, althoughPPJ did develop in 4 out of 7 patients with preoperative AST>40 IU/1. Analysis of the degree of per operative hypotensionand hypoxia has enabled us to refute the previously suggestedhypotheses that either, or both, of these factors were
important in the development of PPJ. Although there was asignificant difference between the mean time of cardio-
pulmonary bypass in the two groups of patients, the meandifference of around 10 min is a small fraction of an averagebypass time of 90 min. There was a wide scatter of bypasstimes within each group, leading to considerable overlapbetween them. Although mean preoperative serum bilirubinand alkaline phosphatase were slightly higher in the PPJgroup there was again enormous overlap in results betweenPPJ and non-PPJ patients, and in an individual patientpreoperative serum estimation had no predictive value.
Preoperative right atrial pressure (RAP) was significantlyhigher in the group who developed PPJ, suggesting thatpreoperative right heart-failure may predispose to PPJ. ButPPJ did not develop in all patients with severe right heart-failure, while others who became profoundly jaundicedpostoperatively had had normal preoperative RAP and noevidence of right heart-failure. There was no direct relationbetween preoperative RAP and preoperative liver functiontests.
Although Lockey et al. suggested that the degree ofhypothermia induced during the operation was related toPPJ, our data did not support this. Mean oesophagealtemperature of patients in whom PPJ developed was higherthan that in the non-PPJ patients.
There was a clear difference between the blood-transfusion
requirements of the two groups of patients, but transfusion ofa large volume of blood was not inevitably followed by PPJ. 2patients in whom PPJ did not subsequently develop hadreceived 23 and 29 units of whole blood, while 10 patients inwhom PPJ did develop had received 5 or fewer units of blood.There is a clear relation between type of operation, bypasstime, and volume of blood transfused, with multiple valvesurgery requiring more time and far more blood than
coronary bypass graft procedures. Lockey et al. 2 suggestedthat jaundice was more common after mitral-valve surgery,but we could not confirm this, the incidence of PPJ in patientsafter mitral-valve surgery alone being no different from thatin the group as a whole (table III). PPJ occurred less oftenafter coronary-artery surgery than after the other operations.The present study has shown that the more major theprocedure the more likely the development of PPJ, but westress that this still offers no specific clue to the cause orcauses of PPJ and PPJ may occur after very straightforwardprocedures.Although PPJ occurred far more frequently after multiple-
valve surgery, particularly surgery involving the tricuspidvalve, than after other operations, once PPJ had developedthe subsequent mortality risk was the same irrespective of thepreceding operation. Thus, whereas PPJ developed in 82% ofpatients undergoing multiple-valve operations involving thetricuspid valve, and developed in only 8% of those
undergoing coronary-artery bypass surgery alone, in bothinstances about a quarter of the patients in whom PPJdeveloped died. No non-PPJ patients died after either type ofoperation. Both Lockey et a1.2 and Schalm and Weber9
proposed that haemolysis contributed to PPJ. We have foundno evidence to support this. More than 75% of the bilirubin is
conjugated,. and there is associated bilirubinuria.
Furthermore, peroperative plasma haemoglobinconcentrations were no higher in the PPJ patients than in thenon-PPJ patients, and postoperative investigations for
haemolysis were negative in every instance in the PPJ group.The suggestion of Kantrowitz4 that septicaemia might beanimportant risk factor has also not been borne out; only 7patients (4 in the PPJ group) had septicaemia. Advances inviral serology have now enabled us to exclude the possibilitythat infection with, or reactivation of, a virus or virusesknown to be associated with clinical hepatitis is responsiblefor PPJ.PPJ was believed to occur because the liver, "shocked" by
hypotension, hypoxia, or hypothermia or chronicallycongested by right heart-failure, could not handle thebilirubin load presented after massive transfusion.
Peroperative and postoperative mMAP, Pa02 or temperatureand post-mortem histology did not show any evidence of such"shock". 13-15
The clinical course and the fact that serum bilirubin was
predominantly conjugated, suggest that PPJ is similar to
postoperative jaundice in 12 cases which followed severalnon-cardiac operations reported by Schmid;" but these
patients all showed features of intrahepatic cholestasis notseen in the present group. The postoperative increase inserum conjugated cholic acid in 24 of 49 patients may supportthe concept that a failure of canalicularbilirubin excretionis ISthe important abnormality.Thousands of gaseous microemboli between 10 and 40 m
are returned from the pump to the patient duringcardiopulmonary bypass.16 In addition platelet aggregatesand debris from the bypass tubing may contribute to theseemboli, and the plasticiser used to coat the tubing may actasatoxin. Chronic changes in hepatic histology have beenrecognised in association with intrahepatic accumulation ofsilicone particles from tubing after long term haemodialysis."These factors may be related to PPJ.Whatever the mechanism for this specific functional
derangement of the liver cell, we regard PPJ as a specificcondition associated with bypass procedures analogous to thechange in cerebrospinal fluid adenylate kinase activity andintellectual impairment after bypass procedures. Thecomplex metabolic effects of cardiopulmonary bypassrequire further investigation.We thank all our consultant colleagues in cardiology, cardiothoracicsurgery,
and anaesthesia for their active co-operation, Miss D. LenaghanandMrsA.Asch, and the nursing and secretarial staff. We also thank colleagues in thehistology, microbiology, and chemical pathology departments at FreemapHospital and virology department, Newcastle General Hospital for the
assembly of the data.
Correspondence should be addressed to 0. F. W. J., Department ofMedicine, Freeman Hospital, Newcastle upon Tyne NE7 7DN.
REFERENCES
1. Sanderson RG, Ellison JH, Benson JA, Starr A. Jaundice following open heart surgery.Ann Surg 1967; 165: 217-24.
2. Lockey E, McIntyre N, Ross DN, Brokes E, Sturridge MF. Early jaundice after open-heart surgery. Thorax 1967; 22: 165-69.
3. Robinson JS, Cole FR, Gibson P, Simpson JA. Jaundice following cardiopulmonarybypass. Thorax 1967; 22: 232-37.
4. Kantrowitz PA. Postoperative hyperbilirubinaemia simulating obstructive jaundice. NEngl J Med 1967; 276: 591-98
5 Geller W, Tagnon HJ Liver dysfunction following abdominal operations. Arch IntMed 1950; 86: 908-16.
6. Caroli J, Paraf A, Champeau J, Desvigner M. Les icteres de la gastrectomie. Arch MalAppar Dig 1950; 39: 1057-85

1123
7 Pichlmayer I, Stitch W. Der bilirubinoatatische Iktèrus—eine neue Ikterusform beimZusammentreften von Operation, Narkose und Bluttransfusion. Klin Wschr 1962;40: 665-67.
8. Kingsley DPE. Hepatic damage following profound hypothermia and extracorporealcirculation in man Thorax 1966; 21: 91-98.
9 Schalm L, Weber AP. Jaundice with conjugated bilirubin in hyperhaemolysis. ActaMed Scand 1964; 176: 549-53
10 Nunes G, Blairdell W, Margaretten W. Mechanism of hepatic dysfunction followingshock and trauma. Arch Surg 1970; 100: 546-56.
11 Mundth ED, Keller AR, Austen WG. Progressive hepatic and renal failure associatedwith low cardiac output following open heart surgery. J Thorac Cardiovasc Surgery1967, 53: 275-84
12. Michaelsson M, Nosslin B, Sjolin S. Plasma bilirubin determination in the newborninfant. Paediatrics 1965; 35: 925-31.
13. Babior BM, Davidson CS. Postoperative massive liver cell necrosis. N Engl J Med1967; 276: 645-52.
14. Schmid M, Heffi ML, Gattiker R, Kistler HJ. Benign postoperative intrahepaticcholestasis. N Engl J Med 1965; 272: 545-50.
15. Sevitt S. Hepatic jaundice after blood transfusion in injured and burned subjects. Br JSurg 1958; 46: 68-74.
16. Pearson DT, Carter RF, Hanmo MB, Waterhouse PS. Gaseous microemboli duringopen heart surgery. In: Longmore DB, ed Towards safer cardiac surgery.Lancaster: MTP, 1981: 325-35.
17. Lashapand T, Osman EM, Morley AR, Ward MK, Kerr DNS. Accumulation ofsilicone elastomer in regular dialysis. Abstract, p. 85. XIXth Congress of EuropeanDialysis and Transplant Association, 1982.
18. Aberg T, Ronquist G, Tyden H, Ahlund P, Bergstrom K. Release of adenylate kinaseinto cerebrospinal fluid during open-heart surgery and its relation to postoperativeintellectual function. Lancet 1982; i: 1139-42
RANDOMISED, CONTROLLED TRIAL OF THECOMPARATIVE EFFICACY, AUDITORYTOXICITY, AND NEPHROTOXICITY OFTOBRAMYCIN AND NETILMICIN
A. MARTIN LERNER
LAWRENCE A. CONEWINFRIED JANSEN
MILAGROS P. REYESDONALD C. BLAIRGRACE E. WRIGHT
RICHARD R. LORBER
Department of Medicine, Wayne State University School ofMedicine, Detroit, Michigan, Department of Medicine, Eisenhower
Medical Center, Rancho Mirage, California; Department ofMedicine, Upstate Medical Center, Syracuse, New York; Office of
the Physician-in-Chief, Fritz Hintermayr Geriatric Hospital,Nuremberg, W. Germany; Research Division of Schering
Corporation, Bloomfield, New Jersey; and the CollaborativeCentres*
Summary 254 patients with serious gram-negativebacillary infections were enrolled into a
multicentre, randomised, blind clinical trial and treated withtobramycin-ticarcillin or netilmicin-ticarcillin. The two
treatment groups were similar as to sex, age, and weight. Themean daily dose of netilmicin (237 mg) was higher than that oftobramycin (211 mg), p<0·01, but the mean duration of
therapy was longer with tobramycin (9·4 days versus 8·7
days), p<0·01. The netilmicin cohort also had more serious
underlying diseases, p<0·028. Clinical (tobramycin, 93%and netilmicin, 91%) and bacteriological responses
(tobramycin, 87% and netilmicin, 89%) were similar. 84tobramycin and 73 netilmicin patients had serial audiograms.Eighth nerve deficits developed in 10 (12%) tobramycin andtwo (3%) netilmicin patients, p=0·037. Drug-related renaldysfunction developed in 5 (4%) of 114 tobramycin patientswhose renal function was monitored and in 1 (1%) of 116netilmicin patients, p=0·12.
Introduction
GENTAMICIN, introduced in 1969, helped greatly in thetreatment of serious infections caused by gram-negativebacilli, including Pseudomonas aeruginosa, against whichstreptomycin (the earliest available aminocyclitol antibiotic)had been ineffective. Although it caused renal dysfunction in8-37% of treated patients and auditory toxicity in 2-10%,gentamicin was used extensively.2-4In 1975 tobramycin, an aminoglycoside approximately
equal in activity to gentamicin, was introduced, and in 1980 a
*Canada: M. G. Bergeron, V. Haldane, and J. H. Thornley; West Germany: F.D. Daschner; USA: C. D. Ericsson, R. R. Martin, D. Mildvan, J. Mills, E.Quinn, and M. J. Raff, and Mexico: P. Leal Del Rosal.
well-executed prospective, blind, controlled trial showed thatit was less nephrotoxic than, but as ototoxic as, gentamicin.2Amikacin, an aminoglycoside whose gram-negative spectrumincluded organisms resistant to both gentamicin and
tobramycin was made available in 1976, but animal studiessuggested that it was more ototoxic than either gentamicin ortobramycin.5 5The synthesis of netilmicin ( (I-N-ethylsisomicin, a 9
dehydrogenated gentamicin Cia) was announced in 1975.6 Invitro and animal studies showed that netilmicin extended theantibacterial spectrum of gentamicin and tobramycin to
isolates resistant to these two agents, and it was less toxic tothe eighth cranial nerve and kidneys than was
tobramycin.7-10 The present report is a prospective,controlled, blind, randomised, international trial, in which15 university medical centres assessed the relative efficacyand toxicity of tobramycin and netilmicin in patients withserious gram-negative bacillary infections.
Patients and Methods
Study PlanPatients aged 18 years old admitted to one of the participating
centres from September, 1980, to March, 1982, with serious gram-negative bacillary infections and who had serum creatinines 2.4mg/dl were included in this study. The protocol was approved bythe human research committee of each institution and informedconsent was obtained from each patient. Patients were allocated toone of two treatment regimens-tobramycin plus ticarcillin ornetilmicin plus ticarcillin-by a computer-generated random code.Patients excluded were those on dialysis for renal failure; pregnantwomen; others who had received an aminoglycoside antibiotic in thepreceding 14 days; those who had hypersensitivity reactions to anyof the study medications; or those who had meningitis,osteomyelitis, or endocarditis. Patients were initially given 3
mg/kg/day of tobramycin, or 4 mg/kg/day of netilmicin in threedivided doses, and dosage was subsequently adjusted according toserum antibiotic and creatinine values, the maximum permissiblefor tobramycin being 5 mg/kg/day and that for netilmicin 6.5
mg/kg/day. Each patient also received ticarcillin, 3 g intravenouslyevery 4 h. No other antibiotic was given.Cultures of blood, urine, sputum, pleural fluid, and exudate(s)
were taken before, during, and after therapy. Haematopoietic,hepatic, and renal functions were assayed before treatment and atleast every third day during treatment, as well as at completion ofthe course. When clinically possible, baseline, mid-course, and post-treatment audiograms were done. Peak (Cmax, 1 h after intravenousinfusion of drug) and trough (Cmin, just before the next dose) serumaminoglycoside levels were taken periodically during therapy.Patients who remained on either of the two treatment regimens forat least 72 h were evaluated for safety.
MicrobiologyInitial isolates were susceptible to both tobramycin and
netilmicin. Gram-negative bacilli grown in Mueller-Hinton broth