Embed Size (px)
Citation preview

PROCEEDINGS
100 Vol. 8, No. 4 n March 2008
INCIDENCE, PREVALENCE, AND PATHOPHYSIOLOGY OF ACNE*—
Anthony J. Mancini, MD, FAAP†
ABSTRACT
Acne is the most common dermatologic condi-tion encountered in clinical practice, affectingnearly all adolescents and young adults to somedegree. The pathophysiology of acne is complex.Increased sebum production by sebaceous glandsand abnormal desquamation of hair folliclesoccur in response to increasing androgen levelswith the onset of puberty. Obstruction of folliclescauses follicular distention, which is often accom-panied by the proliferation of the bacteriaPropionibacterium acnes and the activation of aninflammatory response. Although the diagnosis ofacne is usually straightforward, some conditionsare occasionally confused with acne, includingperiorificial dermatitis, keratosis pilaris, angiofi-bromas, bacterial folliculitis, and demodex folli-culitis. In addition to physical discomfort, acne isassociated with considerable psychological dis-tress, limitation of activities, and increased risk ofdepression and suicide. The relationship betweenacne and diet is controversial. Some studies havedemonstrated that diets that are high in minimallyprocessed plant or animal foods or low in highlyprocessed carbohydrates are associated withlower rates of acne, although other studies have
failed to demonstrate important differences in dietbetween subjects with and without acne. Recentresearch suggests that some dairy products mayincrease acne risk during adolescence. (Adv Stud Med. 2008;8(4):100-105)
Acne vulgaris is the most common skincondition that is treated by physicians,accounting for more than 14 millionoffice visits per year. Acne typicallyappears for the first time during early
adolescence, and is present to some degree in approxi-mately 85% of individuals between the ages of 15 and17 years.1 The first acne lesions often appear before theemergence of secondary sexual characteristics, and areone of the earliest signs of impending puberty. Acnepresents several significant challenges, including a com-plex etiology, concerns about antibiotic resistance, andthe potential for scarring. The effects of acne are notlimited to the skin—acne lesions among adolescentsand young adults generally occur at a time of height-ened emotional sensitivity, and may contribute to sig-nificant psychological distress, depression, and evenincreased risk of suicide.
ACNE PATHOPHYSIOLOGY AND CLINICAL PRESENTATION
The pathophysiology of acne is a multifactorialprocess that begins with the obstruction of the piloseba-
*Based on proceedings from a satellite symposium heldduring the American Academy of Pediatrics Annual Meetingon October 28, 2007, in San Francisco, California.
†Head, Division of Pediatric Dermatology, Children’sMemorial Hospital, Associate Professor of Pediatrics andDermatology, Northwestern University’s Feinberg School ofMedicine, Chicago, Illinois.
Address correspondence to: Anthony J. Mancini, MD,FAAP, Head, Division of Pediatric Dermatology, Children’sMemorial Hospital, Box 107, 2300 Children’s Plaza,Chicago, IL 60614. E-mail: [email protected].

PROCEEDINGS
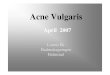
ceous unit, which consists of the hair follicle, hair shaft,and sebaceous gland.2 Acne lesions are therefore concen-trated in areas of greatest sebaceous gland density, includ-ing the face, neck, chest, upper arms, and back.3 Usuallybeginning at approximately 8 to 9 years of age, increasedproduction of adrenal androgens stimulates the secretionof sebum—a waxy substance containing a mixture ofwax and sterol esters, triglycerides, cholesterol, andpotentially inflammation-inducing free fatty acids—bythe sebaceous glands.1,4 Sebum secretion is accompaniedby increased production of squamous cells lining the fol-licle, increased adhesion of follicular epithelial cells toone another, and abnormal keratinization of the follicleinner surface. The accumulation of sebum, epithelialcells, and keratin obstructs the follicle, causing the for-mation of a keratin plug and follicle swelling, resulting inthe formation of a microscopic lesion (the microcome-done) below the skin surface (Figure 1). The micro-comedone is the earliest acne lesion, and is common toinflammatory and noninflammatory acne.2
Enlargement of the keratin plug and continuedswelling of the follicle result in the formation of a visiblecomedone, which is the basic acne lesion. A comedonemay have a widely dilated opening to the skin surface (anopen comedone or blackhead), or an opening that is onlymicroscopic (a closed comedone or whitehead).Although the dark coloration of the blackhead is believedby many patients to be caused by dirt, it actually reflectsthe oxidation of compacted epithelial cells and sebaceouslipid.1 Inflammatory acne occurs when the follicles
become colonized by Propionibacterium acnes, a gram-positive anaerobe that is part of the normal skin flora.2
The proliferation of P acnes stimulates the infiltration ofimmune cells (eg, CD4 T lymphocytes and neutrophils),which disrupt the follicular wall and cause the dispersalof lipids, cellular components, and bacteria into the sur-rounding dermis. Cytokines, peptides, and other inflam-matory mediators released during this process stimulatea localized inflammatory response, resulting in papuleformation. A more intense inflammatory response resultsin the formation of pustules, which are often accompa-nied by overlying comedonal acne. Larger inflammatorylesions may result in the formation of cysts. Nodules aredeeper lesions that often involve more than 1 follicle andare associated with a high likelihood of scarring.1
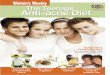
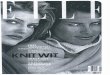
Typical clinical presentations of acne are depicted inFigures 2 and 3. Comedonal acne is shown in Figure 2,including open and closed comedones on the patient’schin. Inflammatory acne is illustrated in Figure 3. Asdescribed in more detail later in this monograph, postin-flammatory dyspigmentation or hyperpigmentationoften occur following acne healing, especially in patientsof color. Finally, scarring is a common complication ofacne that may be prevented by early treatment.5
The diagnosis of acne is usually straightforward,although some conditions may occasionally be con-fused with acne. Periorificial dermatitis is a commonacneiform disorder in children and young adults that isgenerally thought to represent a pediatric form of acnerosacea. Previously referred to as perioral dermatitis,
Johns Hopkins Advanced Studies in Medicine n 101
Figure 1.Types of Acne Lesions
Reprinted with permission from http://www.niams.nih.gov/Health_Info/Acne.

PROCEEDINGS
this condition is characterized by papules and pustules,typically without comedones, that are usually distrib-uted near the eyes, nose, and mouth.6,7 Keratosis pilaris,a common disorder in pediatric dermatology practice,is characterized by hyperkeratotic papules associatedwith hair follicles, typically involving the cheeks, outerarms, and dorsal thighs.8 This condition is especiallylikely to be confused with acne when it is inflammato-ry. Keratosis pilaris is very difficult to treat, and shouldbe regarded as a skin type rather than a disorder.Angiofibromas (formerly referred to as adenomasebaceum) are encountered in the setting of tuberoussclerosis, an autosomal dominant multiple hamartomasyndrome.9 These papules may resemble acne, but aretypically translucent (resembling molloscum), arelocated in the midfacial region, generally appear earlierthan acne (typically at approximately 4–6 years of age),and are not accompanied by comedones. Bacterial fol-liculitis may cause erythematous papules and pustulesthat are rarely mistaken for acne. These lesions typical-ly involve the buttocks and posterior thighs of diaper-wearing children, although they may also appear inother locations. Other forms of folliculitis are some-times confused with acne. For example, pityrosporumis often associated with truncal papules in immunosup-pressed patients.10,11 This disorder may be distinguishedfrom acne by the absence of facial lesions and by a pos-itive potassium hydroxide (KOH) test result.
Demodex folliculitis is also sometimes encounteredin individuals with immunosuppression, presenting as apersistent acne-like eruption on the face that does notrespond to acne therapy. The presence of demodexmites may be confirmed by a skin surface biopsy.Treatment with topical permethrin or sulfa-basedantibiotics is usually effective for these patients.12 Finally,milia is unlikely to be confused with acne, although thecharacteristic white papules on a background of nonin-flamed skin may resemble closed comedones. Theselesions tend to occur sporadically during childhood,especially at sites of abrasional trauma, presenting asclusters of white papules with a total absence of inflam-mation. They may rarely be syndrome associated.
The emotional impact of acne is often very difficultfor patients to tolerate. Adolescents are in a period oflife that is characterized by pronounced emotionalvolatility, and they are often especially sensitive to theeffects of acne or other conditions that adversely affecttheir physical appearance. As a result, acne often caus-es significant anxiety, depression, frustration, and
102 Vol. 8, No. 4 n March 2008
Figure 2. Comedonal Acne
Images courtesy of Anthony J. Mancini, MD, FAAP.
Figure 3. Inflammatory Acne
Images courtesy of Anthony J. Mancini, MD, FAAP.

PROCEEDINGS
anger.13 Approximately 7% of patients with acneexhibit depression or suicidal ideation.14 Impairmentsin functional ability have been observed in several set-tings, including socializing with friends, dating, partic-ipating in sports, and academic attainment.Individuals with moderate-to-severe acne are also atincreased risk of unemployment.15 In addition to theemotional difficulties associated with acne in adoles-cent patients, these individuals also tend to expectimprovement very quickly, and they are often impa-tient with and poorly adherent to acne therapy.Education about the time required for acne therapy towork is especially important for these patients, accom-panied by regular follow-up visits with positive rein-forcement whenever possible. As described in thearticle by Dr Hebert, acne therapy typically employs acombination of treatments to reduce acne lesions andavoid antibiotic resistance.
THE RELATIONSHIP BETWEEN ACNE AND DIET
There are several common misconceptions about thecauses or treatment of acne. Many people think that acneis caused by dirt, and that intensive scrubbing of the skincan cure acne. However, vigorous scrubbing or abrasivecleansers do not improve acne, and may actually worsenit by traumatizing the skin and exacerbating inflamma-tion.16 The relationship between acne and diet is contro-versial. Acne is often attributed to several dietary causes,including chocolate, soda, sweets, or fried foods,although many acne experts have argued that diet is nota significant contributor to acne.
A relationship between acne and glycemic load wasinitially suggested by the observation that the prevalenceof acne is relatively low in some nonwesternized societies,and that acne becomes more common when previouslyisolated societies adopt westernized diets.17 In particular,researchers have noted that acne is nearly absent inregions where the diet consists primarily of minimallyprocessed plant or animal foods and very low amounts ofwestern-style high-carbohydrate foods that yield veryhigh glycemic loads when ingested. For example,Cordain et al examined the prevalence of acne in 2 non-westernized populations—Kitavan islanders of NewGuinea and the Ache hunter-gatherers of Paraguay.18 InNew Guinea, dermatologic examination revealed nocases of acne among a total of 1200 subjects, including300 subjects between the ages of 15 and 25 years. Of 115subjects in Paraguay, no cases of acne were identified over
a follow-up period of more than 2 years. It has been sug-gested that increasing glycemic load modulates acne riskby altering serum insulin concentration and the produc-tion of insulin-like growth factor-1 (IGF-1), a mitogenthat may stimulate follicle growth.
Test subjects from New Guinea have been shownto exhibit low serum insulin concentrations and highinsulin sensitivity, in contrast to hyperinsulinemia andinsulin resistance that are more commonly encoun-tered in association with westernized high-carbohy-drate diets.19 Diet-related hyperinsulinemia may alsocontribute to acne by stimulating androgen produc-tion.20 Smith et al recently conducted a randomizedstudy to evaluate the effect of a low–glycemic-load dieton acne in male subjects between 15 and 25 years ofage.20 A total of 43 subjects were randomly assigned to1 of 2 dietary treatment groups for 12 weeks. Subjectsin 1 group consumed a low–glycemic-index diet con-sisting of 25% energy from protein, 30% from fats,and 45% from carbohydrates with low glycemic indexvalues. Subjects in the control group consumed a diet
Johns Hopkins Advanced Studies in Medicine n 103
EVIDENCE-BASED PRACTICE RECOMMENDATION
I. Practice Recommendation: The pathogenesis ofacne is multifactorial and includes hormonal, microbi-ological, and immunological mechanisms.Combination therapy should be used to target as manypathogenic factors as possible. Topical antibioticsalone may increase the risk of antibiotic resistance.Patients who require topical antibiotic therapy shouldbe treated with benzoyl peroxide in combination witherythromycin or clindamycin.
Name of AAFP-Approved Source: American Academyof Dermatology: Guidelines of Care for Acne VulgarisManagement.
Specific Web Site of Supporting Evidence fromApproved Source: http://www.aad.org/pm/science/_docs/ClinicalResearch_Acne%20Vulgaris.pdf.
Strength of Evidence: A group of experts in the man-agement of acne, convened by the American Academy ofDermatology, reviewed the clinical evidence supportingvarious acne management strategies. The authors identi-fied several reports demonstrating that combinations ofbenzoyl peroxide and a topical antibiotic reduce or elim-inate antibiotic resistance, and that combination therapyis more effective than either individual treatment alone.

PROCEEDINGS
high in carbohydrate-dense foods similar to their base-line diets. After 12 weeks, subjects in thelow–glycemic-index diet group exhibited a greaterreduction from baseline than the control subjects forboth inflammatory lesion counts and total lesioncounts (Figure 4). The dietary intervention was alsoassociated with reduced circulating insulin andimproved insulin resistance,20 in addition to reductionin the free androgen index and an increase in IGF-
binding protein.20 However, other studies have foundno significant differences in several metabolic factorsbetween individuals with or without acne vulgaris,including serum glucose, insulin, glycemic index, orself-reported dietary glycemic load.17
The relationship between acne and the consumptionof dairy products and other foods was examined usingdata from the Nurses’ Health Study II, a long-term,ongoing prospective study that is examining associationsamong several lifestyle factors and illnesses amongwomen who were between the ages of 25 and 42 yearswhen the study began in 1989.21 These investigators ret-rospectively evaluated data from 2 questionnaires thatwere provided by more than 47 000 women. One ques-tionnaire asked the participants about their diet duringtheir high school years, and the second questionnaireasked the subjects whether they had a lifetime history ofphysician-diagnosed acne. A history of physician-diag-nosed acne was significantly associated with self-reportedhigh-school milk intake, but only among women whohad regularly consumed skim milk.
Acne was also significantly associated with more fre-quent consumption of several other dairy products,including instant breakfast drink, sherbet, creamcheese, and cottage cheese. Physician-diagnosed acnewas not significantly associated with patient-reportedintake of other foods that have been associated with
104 Vol. 8, No. 4 n March 2008
Figure 4. Effects of a Low–Glycemic-Load Dieton Acne Vulgaris
Mean (±SEM) percentage changes from baseline in inflammatory acnelesion counts and in total acne lesion counts in the low–glycemic-loadgroup (solid line; n = 23) and the control group (dashed line; n = 20) ateach visit. Repeated-measures analysis of variance was performed by incor-porating the absolute data (log transformed) from each follow-up visit, withbaseline counts as the covariate.
EVIDENCE-BASED PRACTICE RECOMMENDATION
II. Practice Recommendation: Routine dietary modi-fication or the avoidance of particular foods are not rec-ommended for patients with acne.
Name of AAFP-Approved Source: American Academyof Dermatology: Guidelines of Care for Acne VulgarisManagement.
Specific Web Site of Supporting Evidence fromApproved Source: http://www.aad.org/pm/science/_docs/ClinicalResearch_Acne%20Vulgaris.pdf.
Strength of Evidence: The American Academy ofDermatology expert panel noted that few studies havedirectly compared the effects of different dietary modi-fications with one another, and that some studies havefailed to demonstrate associations between acne andparticular dietary factors. The panel therefore conclud-ed that restriction of foods or food classes is not recom-mended for patients with acne.Reprinted with permission from Smith et al. J Am Acad Dermatol.
2007;57:247-256.20

PROCEEDINGS
acne, including chocolate, soda, pizza, and french fries.The authors noted that milk contains numerous pro-teins that might potentially influence acne risk, includ-ing estrogens, progesterone, androgens and androgenprecursors, IGF-1, and others. They also hypothesizedthat differences in processing between whole milk andskim milk might affect acne risk by altering thebioavailability of some of the hormonal components ofmilk. For example, they noted that whole milk containsmore estrogen than skim milk, and that estrogens mayexert a protective effect against acne. Although theseresults provide some evidence for an associationbetween acne and the consumption of dairy productsduring adolescence, a significant limitation of thisstudy was that it relied entirely on participants’ retro-spective recall of diet and acne diagnosis.
CONCLUSIONS
Acne is a common disorder that is associated withconsiderable patient distress, anger, and depression.The pathophysiology of acne involves a series of com-plex interactions between hormones, alterations tokeratinization of the sebaceous glands, and bacterialinfection. For the past 2 decades, most acne specialistshave argued that there is no clear association betweenacne and foods, such as chocolate or other sweets.Some newer studies have suggested that acne may infact be linked to diet, although the benefits of dietarymodification to reduce the incidence or severity ofacne are not well established at present.
REFERENCES
1. Krowchuk DP. Managing adolescent acne: a guide for pedi-atricians. Pediatr Rev. 2005;26:250-261.
2. Zaenglein AL, Thiboutot DM. Expert committee recommendationsfor acne management. Pediatrics. 2006;118:1188-1199.
3. Feldman S, Careccia RE, Barham KL, Hancox J. Diagnosis andtreatment of acne. Am Fam Physician. 2004;69:2123-2130.
4. Cotterill JA, Cunliffe WJ, Williamson B, Bulusu L. Furtherobservations on the pathogenesis of acne. BMJ.1972;3:444-446.
5. Layton AM. Optimal management of acne to prevent scarringand psychological sequelae. Am J Clin Dermatol.2001;2:135-141.
6. Nguyen V, Eichenfield LF. Periorificial dermatitis in childrenand adolescents. J Am Acad Dermatol. 2006;55:781-785.
7. Laude TA, Salvemini JN. Perioral dermatitis in children. Semin Cutan Med Surg. 1999;18:206-209.
8. Alai NN. Keratosis pilaris. Available at: http://www.emedicine.com/derm/topic211.htm.Accessed November 25, 2007.
9. Hurst JS, Wilcoski S. Recognizing an index case of tuberoussclerosis. Am Fam Physician. 2000;61:703-708, 710.
10. Faergemann J. Pityrosporum yeasts—what’s new? Mycoses.1997;40(suppl 1):29-32.
11. Elmets CA. Management of common superficial fungal infec-tions in patients with AIDS. J Am Acad Dermatol.1994;31:S60-S63.
12. Karincaoglu Y, Bayram N, Aycan O, Esrefoglu M. The clini-cal importance of demodex folliculorum presenting with non-specific facial signs and symptoms. J Dermatol.2004;31:618-626.
13. Fried RG, Wechsler A. Psychological problems in the acnepatient. Dermatol Ther. 2006;19:237-240.
14. Fried RG, Gupta MA, Gupta AK. Depression and skin dis-ease. Dermatol Clin. 2005;23:657-664.
15. Cunliffe WJ. Acne and unemployment. Br J Dermatol.1986;115:386.
16. Leyden JJ. Therapy for acne vulgaris. N Engl J Med.1997;336:1156-1162.
17. Kaymak Y, Adisen E, Ilter N, et al. Dietary glycemic indexand glucose, insulin, insulin-like growth factor-I, insulin-likegrowth factor binding protein 3, and leptin levels in patientswith acne. J Am Acad Dermatol. 2007;57:819-823.
18.Cordain L, Lindeberg S, Hurtado M, et al. Acne vulgaris: adisease of Western civilization. Arch Dermatol.2002;138:1584-1590.
19. Lindeberg S, Eliasson M, Lindahl B, Ahrén B. Low seruminsulin in traditional Pacific Islanders—the Kitava Study.Metabolism. 1999;48:1216-1219.
20. Smith RN, Mann NJ, Braue A, et al. The effect of a high-pro-tein, low glycemic-load diet versus a conventional, highglycemic-load diet on biochemical parameters associatedwith acne vulgaris: a randomized, investigator-masked, con-trolled trial. J Am Acad Dermatol. 2007;57:247-256.
21.Adebamowo CA, Spiegelman D, Berkey CS, et al. Milk con-sumption and acne in adolescent girls. Dermatol Online J.2006;12:1.
Johns Hopkins Advanced Studies in Medicine n 105