Embed Size (px)
Citation preview

Personalized Medicine and Imaging
Incorporation of Next-Generation Sequencinginto Routine Clinical Care to Direct Treatment ofHead and Neck Squamous Cell CarcinomaNicole G. Chau1, Yvonne Y. Li1, Vickie Y. Jo2, Guilherme Rabinowits1, Jochen H. Lorch1,Roy B. Tishler3, Danielle N. Margalit3, Jonathan D. Schoenfeld3, Don J. Annino4,Laura A. Goguen4, Tom Thomas4, Hailey Becker1, Tyler Haddad1, Jeffrey F. Krane2,Neal I. Lindeman2, Geoffrey I. Shapiro1, Robert I. Haddad1, and Peter S. Hammerman1
Abstract
Purpose: The clinical impact of next-generation sequencing(NGS) in patients with head and neck squamous cell carcinoma(HNSCC) has not been described. We aimed to evaluate theclinical impact ofNGS in the routine care of patients withHNSCCand to correlate genomic alterations with clinical outcomes.
Experimental Design: Single-center study examining targetedNGS platform used to sequence tumor DNA obtained from 213HNSCC patients evaluated in outpatient head and neck oncologyclinic between August 2011 and December 2014. We correlatedtumor genomic profiling results with clinical outcomes.
Results: PI3K/RTK pathway activation occurred frequently[activating PIK3CAmutation or amplification (13%), PTEN inac-tivation (3%), RAS activation (6%), EGFR or ERBB2 activation(9%)]. Alterations in pathways affecting cell-cycle regulation[CCND1 amplification (9%), CDKN2A inactivation (17%),BRCA2 inactivation (2%)] and squamous differentiation
[NOTCH1 inactivation (8%) andEP300 inactivation (6%)] wereidentified. PIK3CA amplification (n¼ 43), not PIK3CAmutation,was associated with significantly poorer progression-free survival(P¼ 0.0006). Oncogenic RASmutations (n¼ 13) were associatedwith significantly poorer progression-free survival (P ¼ 0.0001)and lower overall survival (P ¼ 0.003). Eight patients withadvanced, treatment-refractory HNSCC enrolled on clinical trialsmatched to tumor profiling results, and 50% achieved a partialresponse.
Conclusions: Incorporation of NGS clinical assays into theroutine care of patients with HNSCC is feasible and may readilyfacilitate enrollment into clinical trials of targeted therapy with ahigher likelihood of success. Data can be utilized for discovery ofgenomic biomarkers of outcome. PIK3CA amplification and RASmutations were frequently identified and associated with poorerprognosis in this cohort.ClinCancer Res; 22(12); 2939–49.�2016AACR.
IntroductionHead and neck squamous cell carcinoma (HNSCC) is the sixth
most common cancer worldwide (1). Effective personalizedmed-icine approaches, including the evaluation of biomarker-driventargeted therapies, are lacking in this disease. Risk stratification
and treatment selection are largely determined by traditionalAmerican Joint Committee on Cancer (AJCC) staging parameters.The only molecular marker currently used routinely for riskstratification is the presence of high-risk human papilloma virus(primarily HPV-16) in oropharyngeal cancer, although its impactis tempered by smoking history (2). The sole FDA-approvedtargeted therapy in HNSCC is cetuximab, a monoclonal antibodyagainst the epidermal growth factor receptor, which is associatedwith a response rate of 10% to 15% in the recurrent or metastaticsetting (3), and for which there is no validated biomarker to guidepatient selection. Recent characterization of the genomic land-scape ofHNSCChas offered insight into underlying heterogeneityand discovery of potential new therapeutic targets (4–9). How-ever, these studies largely consisted of retrospective surgicalcohorts without long-term follow-up or data on response toconventional or investigational therapy. These studies have iden-tified frequent mutations of several genes including TP53,PIK3CA, CDKN2A, NOTCH1, and MLL2 among others as wellas copy-number alterations in EGFR, CCND1, PIK3CA, andFGFR1 (4–9). These genes, however, have yet to translate intoclinically useful prognostic or predictive biomarkers in HNSCC,although some such as TP53 mutations may be associated withpoor postoperative outcomes (10).
The application of next-generation sequencing (NGS) to theclinical setting has not been fully described in the care of patients
1Department of Medical Oncology, Dana-Farber Cancer Institute,Harvard Medical School, Boston, Massachusetts. 2Department ofPathology, Brigham andWomen's Hospital, Harvard Medical School,Boston, Massachusetts. 3Department of Radiation Oncology, Dana-Farber Cancer Institute/Brigham and Women's Hospital, HarvardMedical School, Boston, Massachusetts. 4Division of Otolaryngolo-gy, Brigham andWomen's Hospital, HarvardMedical School, Boston,Massachusetts.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
N.G. Chau and Y.Y. Li share first authorship.
R.I. Haddad and P.S. Hammerman share senior authorship.
CorrespondingAuthors:Peter S. Hammerman,Dana-Farber Cancer Institute andHarvard Medical School, 450 Brookline Avenue, Boston, MA 02215. Phone: 617-632-6335; Fax: 617-582-7880; E-mail: [email protected];and Robert I. Haddad, Phone: 617-632-3090; Fax: 617-632-4448; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-15-2314
�2016 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 2939
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314

with HNSCC, and the clinical significance of the most frequentlyrecurrent genomic alterations is largely unknown. The objective ofthis study was to examine the clinical utility of NGS in the routineclinical care of patients with HNSCC and correlate significantlymutated, deleted, and amplified genomic alterations with clinicaloutcomes. Here, we report our findings from NGS data generatedin a Clinical Laboratory Improvement Amendments (CLIA)-cer-tified clinical laboratory obtained from tumor specimens of 213HNSCC patients evaluated at our center. For the first time, wedemonstrate how incorporation of tumor genomic profiling intoroutine clinical care could readily facilitateHNSCCpatient enroll-ment into clinical trials of targeted therapy leading to objectiveresponses and offer insight into candidate prognostic biomarkers.
Materials and MethodsPatient selection and data collection
Patients withHNSCCwho received outpatient care in theHeadand Neck Oncology Program at the Dana-Farber Cancer Institutebetween August 2011 and December 2014 and consented toan Institutional Review Board (IRB)–approved, institute-wideresearch protocol that aimed to assess feasibility and utility ofgenomic profiling and potential targetable alterations in cancerpatients were identified. Data analysis of tumor specimens andabstractionof pertinent clinical data frompatient chart reviewwasconducted in accordance with an IRB-approved protocol. Alltumor specimens underwent secondary histopathologic reviewby a dedicated pathologist for confirmation of the diagnosis andidentificationof optimal areas of the section for isolationof tumorDNA. Human papillomavirus (HPV) status was determined byp16 immunohistochemistry and classified as negative (weak orno staining) or positive (strong and diffuse). Progression-freesurvival (PFS) was measured as the time from initial diagnosis of
HNSCC until the time of first disease relapse, progression ordeath, or until last contact if noneof these events occurred.Overallsurvival (OS) was defined as the time from diagnosis until thetime of death or until last contact.
Genetic analysisAll sequencing assays were performed in a CLIA-certified
laboratory within the Center for Advanced Molecular Diagnos-tics Laboratory of the Brigham and Women's Hospital. DNAwas isolated from 5 to 10.5 mM FFPE slides containing at least20% tumor nuclei using routine extraction methods as previ-ously described (11, 12) and analyzed by massively parallelsequencing using a solution-phase Agilent SureSelect hybridcapture kit and an Illumina HiSeq 2500 sequencer. MuTect andGATK were used to detect single-nucleotide variants (SNV) andindels, and VisCap was used to detect copy-number variations(CNV).
Samples were initially sequenced utilizing the first-genera-tion platform, Oncomap, a multiplex mass spectrometry–basedplatform capable of detecting 471 loci from 41 cancer geneswhich was instituted in August 2011 (12). In August 2013,Oncomap was replaced by a second-generation platform,Oncopanel, a multiplexed targeted assay which surveys exonicDNA sequences of 275 cancer genes to identify somatic muta-tions and CNVs, in addition to 91 introns from 30 genes todetect rearrangements (11). Alterations are tiered based onclinical significance, and results are communicated in a reportto the treating physician with a turnaround time on the order ofweeks.
Variant callingAlterations were classified into five tiers using the following
guidelines by an expert panel at our institution. Tier 1 designationwas used for alterations with published evidence confirmingclinical utility in HNSCC in predicting response to FDA-approvedtherapy, prognosis, diagnosis, or increased inherited risk of can-cer. Tier 2 classification applied to alterations with clinical utilityin selection of an investigational therapy in clinical trials forHNSCC, or proven association of response to treatment with anFDA-approved therapy in a different type of cancer. Tier 3 encom-passed alterations of uncertain clinical significance but withassociation with treatment response in preclinical HNSCC stud-ies, or selection of an investigational therapy for a different cancertype. Tier 4 was used for novel alterations or those that have notbeen studied in cancer. Tier 5 described alterations that have noclinical utility.
Copy-number changes were detected as per previouslydescribed methods (11): amplifications were defined as meansequence coverage >3-fold greater than reference normal, anddeletions were defined as mean sequence coverage >3-fold lowerthan the reference normal.
Statistical methodsStatistical analyses to test for correlation between genomic and
clinical features were performed using standard R packages. Weused the Fisher exact test for discrete variables, the log-rank test forcontinuous variables, and the Bonferroni method of multipletesting correction. Median follow-up time was calculated using areverse Kaplan–Meier estimate. Mutual exclusivity significancewas calculated using the muex R package.
Translational Relevance
Precision medicine approaches for patients with head andneck squamous cell carcinoma (HNSCC) are lacking. Unlikemany other cancer types, no validated biomarkers exist topredict response to targeted therapies in HNSCC, and notargeted therapies have been approved by the Food and DrugAdministration for HNSCC since 2006. Several large genomicsurveys of HNSCC have been published; however, the lack ofclinical annotation of the studied samples has limited theability to determine the clinical significance of genomic var-iants. Here, we report for the first time, the incorporation oftargeted NGS in the routine clinical care of 213 individualswith HNSCC, and correlate genomic alterations with clinicaloutcomes. For the first time, we identified that PIK3CA ampli-fication and RAS mutations were associated with inferioroutcome, suggesting candidate biomarkers for prognosticvalidation and biomarker-driven clinical trials. We demon-strate examples of personalized approaches in advancedHNSCC patients in which genomic information was used toselect clinical trials of targeted therapy resulting in a higherlikelihood of response. Our findings suggest the incorporationof molecular analyses into the clinical care of patients withHNSCC may enable biomarker discovery efforts and enhanceenrollment of biomarker-driven clinical trials.
Chau et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2940
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314

ResultsClinical characteristics of the cohort
Our cohort consisted of 158 males and 55 females, with amedian age of 59 years at diagnosis of HNSCC (Table 1). Primarytumor siteswere predominantly of the oropharynx (n¼ 97, 46%),and oral cavity (n¼ 60, 28%). Most patients (n¼ 123, 58%) had
stage IVA disease at diagnosis. Forty-eight percent of patients hadp16-positive tumors, and the vast majority of oropharynx cancercases (89%) were p16-positive. The majority of patients (52%)had a smoking history of 10 pack years ormore, whereas only onethird had never smoked. Heavy smoking history was associatedwith larynx cancer (P ¼ 0.002) and age over 55 years old (P ¼0.002). Tumor DNA was sequenced from 213 patients withavailable HNSCC tumor specimens, which were obtained fromthe primary tumor (n ¼ 155), neck lymph node (n ¼ 15), locor-egional recurrence (n ¼ 35), or distant metastasis (n ¼ 12).Of the 213 specimens tested, 97 were tested by Oncomap, and116 were tested by Oncopanel. A total of 140 specimens had atleast one genomic alteration and 73 tested negative [negative ratewashigher forOncomap(66/97¼68%)comparedwithOncopanel(7/116¼6%)].
For the whole cohort, median PFS was 15 months (0.5–86months), and median OS was 20 months (0.5–96 months).Three-year PFS and OS were 68% and 69%, respectively. Medi-an follow-up was 20.4 months. Clinical factors, such as age,gender, alcohol, smoking, and primary site, were not signifi-cantly correlated with OS and PFS. As expected, patients withp16-positive oropharynx cancers (n ¼ 86) had better outcomescompared with their p16-negative counterparts (n ¼ 8), andthis was evident for PFS and OS despite the low number of p16-negative cases [3-year PFS 79% vs. 53% (P ¼ 0.13), 3-year OS61% vs. 42% (P ¼ 0.06)].
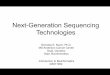
Overview of SNVs and CNVs: Molecular profiling identifiesfrequent mutations (SNVs) in TP53, NOTCH1, MLL2, PIK3CA,and CDKN2A, and frequent CNVs in CCND1, CDKN2A/B,and EGFR
We first identified mutations that were sequenced in bothOncomap and Oncopanel. A genomic overview of the mostfrequent somatic mutations of interest (Supplementary TableS1A) in all Oncomap and Oncopanel cases with at least onemutation (n ¼ 140) is shown in Fig. 1A according to anatomicsite, p16 status, and smoking status. Twenty patients hadcanonical PIK3CA mutations (E542K, E545K, H1047R), 15patients had CDKN2A mutations (13 nonsense, 2 missense),13 patients had TP53 mutations (1 nonsense, 12 missense), 5patients hadHRASmutations (5 missense), 4 patients had JAK3mutations, 2 patients had AKT1 mutations, 2 patients hadFGFR3 mutations, 2 patients had MET mutations, 2 patientshad NRAS mutations, 2 patients had PTEN mutations, and 2patients had RB1 mutations. The observed variants were largelyconsistent with previously profiled nonclinical cohorts (4–6).
A more comprehensive mutational analysis utilizing the sec-ond-generationplatform,Oncopanel, revealedTP53was themostcommon mutational event and was identified in 42 patients,followed by NOTCH1 mutations (n ¼ 24), MLL2 mutations(n ¼ 20), PIK3CA mutations (n ¼ 16), and CDKN2A mutations(n ¼ 16; Fig. 1B). As expected, TP53 mutations were morefrequently observed in HPV-negative patients than in HPV-pos-itive patients (4) and were enriched in heavy smokers.
A genomic overview of high-level CNVs identified by Onco-panel is depicted in Fig. 1C and ordered according to loci. Copy-number analysis of the Oncopanel cohort identified focal regionsof amplification in PIK3CA, SOX2, BCL6, EGFR, CDK6, MYC,JAK2, CCND1, ERBB, GATA6, and SRC. Focal regions of deletionwere found in CDKN2A, CDKN2B, NOTCH1, STK11, TCF3, andSRC. Genes most frequently affected by high-level gain or
Table 1. Characteristics of 213 patients with HNSCC
Characteristic N
Age, median (range) in years 59 (22–88)SexMale 158Female 55
Primary siteOral cavity 60Oropharynx 97Larynx 24Hypopharynx 6Nasopharynx 7Paranasal sinus 5Unknown primary 14
Tumor stageT1-2 145T3-4 54Unknown (Tx) 14
Nodal stageN0 64N1 27N2 111N3 8Unknown (Nx) 3
AJCC stageI 20II 29III 29IVA 123IVB 6IVC 5Unknown 1
Tobacco exposureNever smoked 70�10 pack-years 31>10 pack-years 110Unknown 2
P16 expression across all tumorsPositive 103Negative 34Unknown 76
P16 expression in oropharyngeal primary tumorPositive 86Negative 8Unknown 3
TreatmentUpfront surgery 91Definitive radiation 9Definitive chemoradiation 71Sequential therapy 31Palliative systemic therapy 2Unknown 9
Type of first treatment failureLocoregional disease 58Distant metastases 18Both 8
AssayOncomap positive 31Oncomap no variants identified 66Oncopanel positive 109Oncopanel no variants identified 7
Clinical Next-Generation Sequencing in Head and Neck Cancer
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2941
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314

Figure 1.Mutational spectrum of HNSCC tumors detected by clinical NGS sequencing and copy-number alterations. A, specific mutations of interest detectedacross the HNSCC cohort (n ¼ 213), identifying PIK3CA, CDKN2A, TP53, and HRAS as the most recurrently mutated genes. Samples with at least onedetected alteration are shown (n ¼ 140), stratified by sequencing platform, tumor anatomic site, p16 expression, and smoking level. B, Oncopanel mutationsdetected across the HNSCC cohort (n¼ 116), showing the most recurrently mutated genes in samples with at least one detected alteration (n¼ 109). (Continued onthe following page.)
Chau et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2942
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314

homozygous loss were CCND1 gain (n ¼ 10), CDKN2A/B loss(n ¼ 8), and EGFR gain (n ¼ 8).
Clinical correlation:Oncogenic driver events andPI3Kpathwayalterations and pan-RAS alterations are associated with patientoutcomes
Weperformed an exploratory analysis in theOncoPanel cohortand correlated gene aberrations (SNVs and CNVs) with clinicalfactors (age, primary site, tumor–node–metastasis stage, AJCCstage, tobacco exposure, p16 status, treatment, and type of firsttreatment failure; Table 1) and outcomes including OS and PFS.The total number of SNVs (upper quartile was �8 and lowerquartile was �3 across the cohort) or CNVs (upper quartile was�45 and lower quartile was �1) did not stratify PFS or OS(Supplementary Fig. S1). There was a trend for higher numberof SNVs (greater than the median number of 5 SNVs) to beassociated with heavy smoking history (P¼ 0.001), andCDKN2Amutations to be associatedwith nonoropharynx sites (P¼ 0.002).Amplifications of IKZF1 and MCL1 were associated with lowerPFS (P ¼ 0.000002 and P ¼ 0.0002, respectively; SupplementaryFigs. S2 and S3). Genomic events associated with poorer OS werePIK3CA amplification (P¼ 0.004; Supplementary Fig. S4),NRAS
mutation or CNV gain (P ¼ 0.0016; Supplementary Fig. S5), andGATA4 amplification (P ¼ 0.003; Supplementary Fig. S6). How-ever, we note that aside from PIK3CA, the other genes hadrelatively few events in the cohort, which may lead to inaccurateestimates of survival curves.
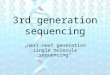
Patients with tumors harboring previously reported markers ofPI3K pathway activation that were tested in theOncoPanel cohort(Tier 1/2mutations in PIK3CA, PIK3C2B, PIK3R1, PIK3CA ampli-fication or PTEN loss) appeared to have poorer outcomes andlower PFS (P ¼ 0.19; Fig. 2A). Specifically, patients with PIK3CA-amplified tumors (40 patients had CNV gain, 3 patients had highgain) had significantly worse PFS (P¼ 0.0006; Fig. 2B) and worseOS (P ¼ 0.004; Supplementary Fig. S4). In contrast, PIK3CAmutations alone were not associated with PFS (SupplementaryFig. S7; P ¼ 0.79). The reason for this correlation with outcomewith PIKC3A amplifications but not mutations is unclear, and noother obvious confounding clinical variable, including p16 status,was associatedwithPIK3CAmutation to explain thisfinding (datanot shown). PI3K pathway mutation or copy-number alterationwas not significantly associated with OS (P ¼ 0.17).
RAS alterations were also associated with poorer survival out-comes. Notably, patients with tumors harboring previously
Figure 1.(Continued. ) C, Oncopanel copy-number alterations detected across the HNSCC cohort (n ¼ 109) for samples with at least one detected copy-number event(n ¼ 94). Genes with at least two high-level events (high gain or homozygous loss) are shown, arranged by loci.
Clinical Next-Generation Sequencing in Head and Neck Cancer
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2943
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314

reported activating RAS mutations [Tier 1/2 mutations for HRAS(n ¼ 10), NRAS (n ¼ 2), and KRAS (n ¼ 1)] appeared to have asignificantly poorer PFS (P¼ 0.0001; Fig. 2C) and lower OS (P¼0.003; Fig. 2D). RAS and PIK3CA events tended to be mutuallyexclusive.
Pathway overview and potential genotype-driven targetedtherapies for HNSCC
Themost frequent and clinically significant somatic alterationsthat we identified belong to key oncogenic pathways affecting cellsignaling, cell-cycle regulation, or squamous differentiation, andfor which potentially relevant targeted agents are in clinical
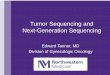
development. We utilized previously described functional anno-tations of somatic alterations of squamous cell carcinomas toclassify mutations and copy-number alterations in this cohort(6, 9). Notably, activation of the PI3K/RTK pathway occurredfrequently as evidenced by recurrent activating PIK3CAmutationor amplification (13%), PTEN inactivatingmutation or loss (3%),RAS activation (6%), and EGFR or ERBB2 activating mutation orhigh amplification (9%; Fig. 3A). Cell-cycle deregulation viatumor suppressor loss-of-function occurred frequently via TP53inactivating mutations (30%) or via retinoblastoma tumorsuppressor pathway inactivation [CDKN2A deletion or mutation(17%), CCND1 amplification (9%)] or BRCA2 inactivation
Figure 2.PIK3CA and RAS alterations are associated with survival in HNSCC patients. Kaplan–Meier estimates of PFS and OS. A, patients with PIK3-family (PIK3CA,PIK3C2B, PIK3CR1) or PTEN Tier 1/2 mutation had poorer PFS across the Oncopanel cohort (n ¼ 109, 15 with PI3K/PTEN mutations). B, patients with any PIK3CAcopy-number amplification events significantly associated with poorer PFS in the Oncopanel cohort (n ¼ 109, 43 with PIK3CA amplification). Patients withTier 1/2 activating RASmutations associatedwith both poorer PFS in C andpoorer OS inD across the entire cohort (n¼ 213), 10HRAS-, 2NRAS-, and 1 KRAS-mutatedpatients.
Chau et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2944
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314

EGFR1%
KRAS NRAS HRAS1% 5%
AKTBRAF
NF2
Prolifera�on, survival
7% 3%
3%
PTEN2%
MTOR STK11
2%2% 3%
3%
4%
NF12% 1%
JAK2 JAK35%
ERBB22% 4%
High-level amplifica�on orTier1/2 ac�va�ng muta�on
Homozygous loss orinac�va�ng muta�on
Tier3/Tier4 muta�onof unknown effect
CNV High gainCNV GainCNV LossCNV Homozygous loss
Missense SNVNonsense/frameshi� SNVInser�on/dele�onOther SNV (splice site, etc)
S*IO
Tier1/2Oncomap+OncopanelA
B
muta�on frequency (if in Oncomap)
1% 9% 13%
PIK3CA PIK3R1 4% 3%
3% 3%
1%
MET3%3%3%
2%
1%
1% 2%
2%
3%
1% 3% 2%
1%
CDKN2A3%
TP536%
ATM ATRX7% 5%
BRCA1 BRCA23% 2% 4%
Apoptosis
CNV High gainCNV GainCNV LossCNV Homozygous loss
Missense SNVNonsense/frameshi� SNVInser�on/dele�onOther SNV (splice site, etc)
S*IO
CCND1
G1–STransi�on
9% 23%
9% 17%
30%
High-level amplifica�on orTier1/2 ac�va�ng muta�on
Homozygous loss orinac�va�ng muta�on
Tier3/Tier4 muta�onof unknown effect
Tier1/2Oncomap+Oncopanelmuta�on frequency (if in Oncomap)
Figure 3.Recurrently altered pathways in HNSCC based on integrated analysis of genomic alterations. A–C, key affected signaling pathways in the HNSCC cohort.Pathway genes with recurrent alterations detected in Oncopanel are classified as activating (high-level amplification or Tier 1/2 activating mutationcolored red), inactivating (homozygous loss or truncatingmutation colored blue), or potentially cancer associated (Tier 3/4mutation colored white). The frequencyof Tier 1/2 mutations across the entire cohort (Oncomap and Oncopanel) is shown in gray if different from Oncopanel alone. For each pathway, integratedheatmaps show the detailed alteration pattern of each gene, with shades of red and green representing copy-number events and black text representingmutations.Note that each heatmap is sorted independently across the samples, to best illustrate the pattern of mutations, such as mutual exclusivity or concurrence.A, PI3K/RTK. B, cell cycle. (Continued on the following page.)
Clinical Next-Generation Sequencing in Head and Neck Cancer
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2945
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314

(2%; Fig. 3B). Squamous differentiation pathway deregulationwas often observed via significant homozygous loss or inactivat-ing mutations in NOTCH1 (8%), NOTCH2 (3%), EP300 (6%),and FBXW7 (3%; Fig. 3C). Together, these findings confirm thesufficient frequency of targetable alterations inHNSCC to supportthe development of biomarker-driven clinical trials for HNSCCpatients.
Examples of NGS profiling of tumors leading to clinical trialenrollment
In this cohort, 8 patients with recurrent or metastaticHNSCC enrolled on clinical trials utilizing agents prospective-ly matched to their tumor profiling results (SupplementaryTable S1B). Of these, 4 patients achieved partial response, 1patient had stable disease, and 3 patients had progressivedisease as their best response. Specifically, a 56-year-oldfemale presenting with widely metastatic HPV-positiveHNSCC harboring a PIK3CA mutation (p.E545K) enrolled ona clinical trial of an oral PI3K/mTOR inhibitor and achieveddramatic symptomatic clinical benefit within days of startingtherapy and a significant partial response on first assessmentscans (71% tumor shrinkage; Fig. 4A). Another patient withHPV-negative oral cavity squamous cell carcinoma (SCC) whoprogressed after surgery and chemoradiation and developedpainful locoregional recurrence and lung metastases refractoryto multiple lines of palliative systemic therapy, includingcetuximab, was found to have high copy-number gain in EGFRin her tumor. She enrolled on a clinical trial of an EGFRinhibitor and PI3K/mTOR inhibitor resulting in complete re-solution of pain and also significant partial response (47%tumor shrinkage) on first assessment scans which was main-tained for 8 months (Fig. 4B). A 55-year-old male patient withrecurrent HPV-positive oropharynx SCC was found to have atumor harboring an AKT1 (p.E17K) mutation and enrolled on
a clinical trial of a PI3K/mTOR inhibitor and also achieved asustained partial response. Another 52-year-old female withEGFR-amplified recurrent and metastatic oral cavity SCC wastreated with a novel EGFR inhibitor and achieved a radio-graphic partial response (39% shrinkage) at initial treatmentassessment with symptom improvement.
In contrast, 12 patients with recurrent or metastatic HNSCCwere enrolled on clinical trials of novel therapies unmatched totheir tumor profiling results. The best response was stabledisease for 4 patients and progressive disease for 8 patients(Supplementary Table S1B). In addition, there were 6 patientsfor whom tumor profiling results were used to match therapyon a clinical trial; however, the patients either declined enroll-ment or were deemed ineligible. Of these 6 patients, 1 patientachieved stable disease as best response on further chemother-apy and then died within 5 months, whereas the remaining 5patients had progressive disease (4 died within 4 months and 1died within 6 months). Taken together, 50% of patients onmatched therapy experienced a partial response, whereas nopartial responses were observed in patients who receivedunmatched therapy on clinical protocols at our institutionfrom late 2011 through 2014.
DiscussionThis study represents the first comprehensive characterization
of the use of NGS in the routine clinical care of HNSCC patients,including the identification of candidate biomarkers for furtherprognostic validation, and examples of the application of NGSresults to personalize therapy. While the molecular landscape ofHNSCC has been described in several cohorts (4–7), the clinicalsignificance of genomic alterations in HNSCC is underreportedand is a major impediment to the realization of personalizedmedicine in HNSCC. Initial research efforts to genomically
NOTCH1 NOTCH28% 3%
Squamous differen�a�on
14% 4%
FBXW73% 3%
EP3006% 7%
CNV High gainCNV GainCNV LossCNV Homozygous loss
Missense SNVNonsense/frameshi� SNVInser�on/dele�onOther SNV (splice site, etc)
S*IO
TP536%23% 30%High level amplifica�on or
Tier1/2 ac�va�ng muta�on
Homozygous loss orinac�va�ng muta�on
Tier3/Tier4 muta�onof unknown effect
Oncomap+Oncopanel Tier1/2C
muta�on frequency (if in Oncomap)
Figure 3.(Continued. ) C, squamous differentiation.
Chau et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2946
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314

characterizeHNSCC include three large studies employingwhole-exome and whole-genome sequencing of fresh-frozen primaryHNSCC tumors (4–6). TheCancerGenomeAtlas study reflects thelargest cohort to date (comprised of 279 cases), and is biasedtoward a surgically resected oral cavity or laryngeal squamous cellcarcinoma population (only 15% were HPV-positive; 6). Tocharacterize HPV-positive tumors, a University of Chicago cohortof 120 locally advanced HNSCCs (43% were HPV-positive) wasexamined utilizing a targeted approach evaluating 617 selectedcancer-associated genes in the frozen primary tumors and did notinclude gene-rearrangement data (9). Recently, 252 clinicalHNSCC FFPE samples were evaluated in aggregate utilizing theFoundationMedicineNGSplatform(13). The genomic profiles inthis Foundation Medicine cohort (33% were HPV-positive) werecomparablewithprior reports obtained fromTheCancerGenomeAtlas (TCGA) and University of Chicago; however, treatment andsurvival data were limited. In our study, the most commongenomic alterations were identified at frequencies in concordancewith prior reports (4–6), confirming that the genomic landscapeobtained from clinical HNSCC FFPE specimens appears consis-tent with research-derived frozen specimens.
We utilized more complete outcome data to identify candidategenomic alterations for further prognostic validation based onour exploratory analysiswith clinical correlations.PIK3CAwas themost frequently altered oncogene in our cohort (13% amplifiedor mutated) and was enriched in HPV-positive oropharynx can-
cers, consistent with prior reports (6, 8, 9, 13–16). For the firsttime, we found that PIK3CA amplification was associated withsignificantly decreased PFS, whereas PIK3CA mutation was notassociated with survival outcomes. Prior smaller studies wereunable to identify a significant correlation between PI3K pathwayactivation and survival outcomes (9, 15, 17) and did not distin-guish the relative contribution of various mechanisms of activa-tion of the PI3K pathway (e.g.,PIK3CAmutation vs. amplificationvs. PTEN loss; 15). One study identified that PIK3CA amplifica-tion in 32% of 115 surgical HNSCC cases was associated withearlier relapse in a subset of patients without lymph node metas-tases (n ¼ 59, P ¼ 0.026; 17). Another study reported PIK3CAmutationswere potentially correlatedwith poorer prognosis in anHPV-negative subset of locally advanced HNSCC (n ¼ 69; 9).PIK3CA overexpression (not mutation) has been associatedwith shorter OS in other cancers (18). Preclinical studieshave demonstrated that patient-derived PIK3CA mutantHNSCC tumorgrafts are sensitive to PI3K/mTOR inhibitors(8), and PI3K pathway inhibition may sensitize cancer cells toradiation (19). Clinical trials of a PI3K inhibitor in combinationwith chemoradiation (NCT02113878) or chemotherapy alone(NCT01816984) are underway. In our cohort, 2 patients withPIK3CAmutant tumors received a PI3K/mTOR inhibitor on studyand one achieved partial response while another had progressivedisease as best response. For the purpose of clinical trials enroll-ment, clinically restricting testing to PIK3CA hotspot mutations is
Figure 4.Examples of NGS profiling leading toenrollment on clinical trials of matchedtargeted therapy resulting in objectiveresponses in HNSCC patients. A, 56-year-old female with metastatic HPV-positive HNSCC harboring a PIK3CAmutation (p.E545K) matched to PI3K/mTOR inhibitor on trial achieved asignificant partial response on firstassessment PET/CT scans (71% tumorshrinkage) accompanied by reductionin SUVmax from 9.6 to 2.7 in bilateralhilar and left axillary nodes. B, anotherpatient with recurrent and metastaticHPV-negative HNSCC harboring highcopy-number gain in EGFR treated on aclinical trial of an EGFR inhibitor andPI3K/mTOR inhibitor resulting in partialresponse on first assessment CT neckscans (47% tumor shrinkage).
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2947
Clinical Next-Generation Sequencing in Head and Neck Cancer
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314

a feasibly attractive option (14, 20); however, our findings suggestthat PIK3CA amplification may also bear clinical significance.Taken together, our data support further evaluation of PIK3CAamplification as a potential negative prognostic indicator inHNSCC, independent of HPV status, and preclinical and clinicalinvestigation of biomarker-driven studies in patients with PI3Kpathway–activated tumors is warranted.
RAS mutations [Tier 1/2 mutations for HRAS (n ¼ 10), NRAS(n¼ 2), and KRAS (n¼ 1)] were also associated with significantlypoorer survival in our cohort. This has not been previouslydescribed in HNSCC. In contrast to our findings, in the TCGAdataset, patients with HRAS mutant oral cavity tumors and fewcopy-number alterations hadbetter PFS.HRASmutations occur in5% to 10% of HNSCC (4, 5 ,21) and are enriched in tobacco-related SCCup to frequencies as high as 35% (22).RASmutationsmay also predict lack of response to EGFR inhibitors in HNSCC(23, 24). Preclinical studies suggest that PIK3CA and RAS muta-tions may predict intrinsic resistance to cetuximab, whichmay beprevented by concomitant administration of cetuximab and PI3Kand/ormTOR inhibitors inHNSCCpatients (23). Taken together,RAS mutations warrant further prognostic evaluation in largercohorts, and biomarker-driven clinical trials in RAS mutantHNSCCpatients arewarranted. RAS-directed therapies inHNSCCare lacking (25); however, an HRAS biomarker–driven trial iscurrently open to HNSCC patients (NCT02383927). We alsoconfirmed the presence of other targetable alterations, includingErB2 and EGFR amplification, FGFR3 mutations, CCND1 ampli-fication, and CDKN2A mutations. Early clinical development ofnovel HER2 and EGFR inhibitors, FGFR inhibitors, CDK inhibi-tors, and p53 modulators are all under way, and may be open toHNSCC patients who undergo appropriate genotyping studies. Inthe closely related disease, lung squamous cell carcinoma, geno-mic stratification for clinical trials is increasingly being adopted asevidenced by the recently initiated Lung-MAP study (26).
Notably, our study illustrates how the application of NGSresults may be used to guide selection of targeted therapy foradvanced HNSCC patients on clinical trials. In our cohort, 8patients with advanced disease enrolled on clinical trials oftargeted agents matched to their NGS results. Given that 84patients had recurrent disease (26of these hadmetastatic disease),it is possible that NGSmay be used to direct clinical trial selectionin approximately 10% to 31% of advanced cases. Patientsmatched to therapy appeared to have a higher objective responserate than patients unmatched to therapy in our cohort; however,these results need to be interpreted with caution as many patientscould not bematched to therapy because no targetable alterationswere identified, and many genomic alterations in HNSCC are notreadily "druggable." In our cohort, approximately half of thepatients were tested with the Oncomap panel (n ¼ 97), and halfwere tested with the Oncopanel platform (n ¼ 116). However, acomparison of the Oncomap and OncoPanel platforms clearlydemonstrates a higher negative result rate for the older version,Oncomap (68% vs. 6%), and also differences in mutation rates
between the two tests, suggesting that the detection of actionablealterations may be improved with newer, more comprehensiveNGS panels which are becoming increasingly available. To date,the development of targeted therapies in HNSCC is fraught withnegative clinical trials which have largely tested targeted agents inunselected patient populations (27–31). Our findings wouldsuggest that a greater likelihood of success may be achieved withthe incorporation of genomic stratification into clinical trialsevaluating targeted agents in HNSCC, and such approaches areconsistent with national initiatives, such as NCI-MATCH (32).
In summary, we demonstrate that it is feasible to incorporateNGS into the routine clinical care of patients withHNSCC. For thefirst time, we identify an association of PIK3CA amplification andRAS mutations with poorer survival outcomes. This warrantsfurther evaluation and validation in larger cohorts, but lendssupport for the pursuit of further preclinical evaluation andbiomarker-driven clinical trials in HNSCC patients. We demon-strate examples of personalizedmedicine approaches in advancedHNSCC patients by using genomic profiling results to guideselection of targeted therapy on clinical trials leading to objectiveresponses. Our experience suggests the potential value of incor-porating NGS into the clinical care of patients with HNSCC tobetter define genomic markers associated with outcome and toenhance accrual to biomarker-driven trials.
Disclosure of Potential Conflicts of InterestR.I. Haddad is a consultant/advisory board member for Bristol-Myers
Squibb, Celgene, Eisai, Merck, and Pfizer. No potential conflicts of interestwere disclosed by the other authors.
Authors' ContributionsConception and design: N.G. Chau, V.Y. Jo, L.A. Goguen, N.I. Lindeman, R.I.Haddad, P.S. HammermanDevelopmentofmethodology:N.G.Chau, Y.Y. Li, L.A.Goguen,N.I. Lindeman,P.S. HammermanAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): N.G. Chau, Y.Y. Li, V.Y. Jo, J.H. Lorch, R.B. Tishler,D.N.Margalit, J.D. Schoenfeld, D.J. Annino, L.A. Goguen, T. Thomas, H. Becker,T. Haddad, J.F. Krane, N.I. LindemanAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis):N.G. Chau, Y.Y. Li, V.Y. Jo, J.H. Lorch, D.N. Margalit,T. Thomas, N.I. Lindeman, G.I. Shapiro, P.S. HammermanWriting, review, and/or revision of themanuscript:N.G. Chau, Y.Y. Li, V.Y. Jo,G. Rabinowits, J.H. Lorch, R.B. Tishler, D.N. Margalit, J.D. Schoenfeld,D.J. Annino, L.A. Goguen, T. Thomas, J.F. Krane, N.I. Lindeman, G.I. Shapiro,R.I. Haddad, P.S. HammermanAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): N.G. Chau, L.A. Goguen, H. Becker, T. Haddad,N.I. Lindeman, R.I. Haddad, P.S. HammermanStudy supervision: N.G. Chau, L.A. Goguen, R.I. Haddad, P.S. Hammerman
AcknowledgmentsThe authors would like to acknowledge all of the patients and their families.
Received September 24, 2015; revised December 23, 2015; accepted Decem-ber 30, 2015; published OnlineFirst January 13, 2016.
References1. Ferlay J, Soerjomatarm I, ErvikM,DikshitM, Eser S,Mathers C, et al. Cancer
incidence and mortality worldwide: IARCCancerBase No. 11 [Internet].2012 v1.0. Available from: http://globocan.iarc.fr. September 4, 2015.
2. Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-Tan PF, et al.Human papillomavirus and survival of patients with oropharyngeal can-cer. N Engl J Med 2010;363:24–35.
3. Vermorken JB, Trigo J, Hitt R, Koralewski P, Diaz-Rubio E, Rolland F, et al.Open-label, uncontrolled, multicenter phase II study to evaluate theefficacy and toxicity of cetuximab as a single agent in patientswith recurrentand/or metastatic squamous cell carcinoma of the head and neck whofailed to respond to platinum-based therapy. J Clin Oncol 2007;25:2171–7.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2948
Chau et al.
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314

4. Agrawal N, Frederick MJ, Pickering CR, Bettegowda C, Chang K, Li RJ, et al.Exome sequencing of head and neck squamous cell carcinoma revealsinactivating mutations in NOTCH1. Science 2011;333:1154–7.
5. Stransky N, Egloff AM, Tward AD, Kostic AD, Cibulskis K, Sivachenko A,et al. Themutational landscape of head andneck squamous cell carcinoma.Science 2011;333:1157–60.
6. Cancer GenomeAtlasN. Comprehensive genomic characterization of headand neck squamous cell carcinomas. Nature 2015;517:576–82.
7. Pickering CR, Zhang J, Yoo SY, Bengtsson L, Moorthy S, Neskey DM, et al.Integrative genomic characterization of oral squamous cell carcinomaidentifies frequent somatic drivers. Cancer Discov 2013;3:770–81.
8. Lui VW,HedbergML, LiH, Vangara BS, Pendleton K, Zeng Y, et al. Frequentmutation of the PI3K pathway in head and neck cancer defines predictivebiomarkers. Cancer Discov 2013;3:761–9.
9. Seiwert TY, Zuo Z, Keck MK, Khattri A, Pedamallu CS, Stricker T, et al.Integrative and comparative genomic analysis of HPV-positive and HPV-negative head and neck squamous cell carcinomas. Clin Cancer Res2015;21:632–41.
10. Poeta ML, Manola J, Goldwasser MA, Forastiere A, Benoit N, Califano JA,et al. TP53mutations and survival in squamous-cell carcinoma of the headand neck. N Engl J Med 2007;357:2552–61.
11. Wagle N, Berger MF, Davis MJ, Blumenstiel B, Defelice M, Pochanard P,et al. High-throughput detection of actionable genomic alterations inclinical tumor samples by targeted, massively parallel sequencing. CancerDiscov 2012;2:82–93.
12. MacConaill LE, Campbell CD, Kehoe SM, Bass AJ, Hatton C, Niu L, et al.Profiling critical cancer gene mutations in clinical tumor samples. PLoSOne 2009;4:e7887.
13. Chung CH, Guthrie VB, Masica DL, Tokheim C, Kang H, Richmon J,et al. Genomic alterations in head and neck squamous cell carcinomadetermined by cancer gene-targeted sequencing. Ann Oncol 2015;26:1216–23.
14. Nichols AC, Palma DA, ChowW, Tan S, Rajakumar C, Rizzo G, et al. Highfrequency of activating PIK3CA mutations in human papillomavirus-positive oropharyngeal cancer. JAMA Otolaryngol Head Neck Surg 2013;139:617–22.
15. Chiosea SI, Grandis JR, Lui VW, Diergaarde B, Maxwell JH, Ferris RL, et al.PIK3CA, HRAS and PTEN in human papillomavirus positive oropharyn-geal squamous cell carcinoma. BMC Cancer 2013;13:602.
16. Lechner M, Frampton GM, Fenton T, Feber A, Palmer G, Jay A, et al.Targeted next-generation sequencing of head and neck squamous cellcarcinoma identifies novel genetic alterations in HPVþ and HPV- tumors.Genome Med 2013;5:49.
17. Suda T, Hama T, Kondo S, Yuza Y, Yoshikawa M, Urashima M, et al. Copynumber amplification of the PIK3CA gene is associated with poor prog-nosis in non-lymph node metastatic head and neck squamous cell carci-noma. BMC Cancer 2012;12:416.
18. Bellmunt J, Werner L, Leow JJ, Mullane SA, Fay AP, Riester M, et al.Somatic copy number abnormalities and mutations in PI3K/AKT/mTOR pathway have prognostic significance for overall survival inplatinum treated locally advanced or metastatic urothelial tumors. PLoSOne 2015;10:e0124711.
19. Abazeed ME, Adams DJ, Hurov KE, Tamayo P, Creighton CJ, Sonkin D,et al. Integrative radiogenomic profiling of squamous cell lung cancer.Cancer Res 2013;73:6289–98.
20. Theurer JA, StechoW, Yoo J, Kwan K, Wehrli B, Harry V, et al. Feasibility oftargeting PIK3CA mutations in head and neck squamous cell carcinoma.Pathol Oncol Res 2016;22:35–40.
21. Cancer Genome Atlas Research N. Comprehensive genomic characteriza-tion of squamous cell lung cancers. Nature 2012;489:519–25.
22. SaranathD,Chang SE, Bhoite LT, Panchal RG, Kerr IB,Mehta AR, et al. Highfrequency mutation in codons 12 and 61 of H-ras oncogene in chewingtobacco-related human oral carcinoma in India. Br J Cancer 1991;63:573–8.
23. Wang Z, Martin D, Molinolo AA, Patel V, Iglesias-Bartolome R, Degese MS,et al. mTOR co-targeting in cetuximab resistance in head and neck cancersharboring PIK3CA and RAS mutations. J Natl Cancer Inst 2014;106.
24. Hah JH, Zhao M, Pickering CR, Frederick MJ, Andrews GA, Jasser SA, et al.HRAS mutations and resistance to the epidermal growth factor receptortyrosine kinase inhibitor erlotinib in head and neck squamous cell carci-noma cells. Head Neck 2014;36:1547–54.
25. Mazumdar T, Sen B, Wang Y, Peng S, Nicholas C, Glisson BS, et al. Drug-induced RAF dimerization is independent of RASmutation status and doesnot lead to universal MEK dependence for cell survival in head and neckcancers. Anticancer Drugs 2015;26:835–42.
26. Herbst RS, Gandara DR, Hirsch FR, Redman MW, LeBlanc M, Mack PC,et al. Lung master protocol (Lung-MAP)-a biomarker-driven protocol foraccelerating development of therapies for squamous cell lung cancer:SWOG S1400. Clin Cancer Res 2015;21:1514–24.
27. Ang KK, Zhang Q, Rosenthal DI, Nguyen-Tan PF, Sherman EJ, Weber RS,et al. Randomized phase III trial of concurrent accelerated radiation pluscisplatin with or without cetuximab for stage III to IV head and neckcarcinoma: RTOG 0522. J Clin Oncol 2014;32:2940–50.
28. Machiels JP, Haddad RI, Fayette J, Licitra LF, TaharaM, Vermorken JB, et al.Afatinib versus methotrexate as second-line treatment in patients withrecurrent or metastatic squamous-cell carcinoma of the head and neckprogressing on or after platinum-based therapy (LUX-Head & Neck 1): anopen-label, randomised phase 3 trial. Lancet Oncol 2015;16:583–94.
29. Machiels JP, Subramanian S, RuzsaA,RepassyG, Lifirenko I, FlygareA, et al.Zalutumumab plus best supportive care versus best supportive care alonein patients with recurrent or metastatic squamous-cell carcinoma of thehead and neck after failure of platinum-based chemotherapy: an open-label, randomised phase 3 trial. Lancet Oncol 2011;12:333–43.
30. Vermorken JB, Stohlmacher-Williams J, Davidenko I, Licitra L, Winquist E,Villanueva C, et al. Cisplatin and fluorouracil with or without panitumu-mab in patients with recurrent or metastatic squamous-cell carcinoma ofthe head and neck (SPECTRUM): an open-label phase 3 randomised trial.Lancet Oncol 2013;14:697–710.
31. Cohen EE, Kane MA, List MA, Brockstein BE, Mehrotra B, Huo D, et al.Phase II trial of gefitinib 250 mg daily in patients with recurrent and/ormetastatic squamous cell carcinoma of the head and neck. Clin Cancer Res2005;11:8418–24.
32. Mullard A. NCI-MATCH trial pushes cancer umbrella trial paradigm. NatRev Drug Discov 2015;14:513–5.
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2949
Clinical Next-Generation Sequencing in Head and Neck Cancer
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314

2016;22:2939-2949. Published OnlineFirst January 13, 2016.Clin Cancer Res Nicole G. Chau, Yvonne Y. Li, Vickie Y. Jo, et al. CarcinomaCare to Direct Treatment of Head and Neck Squamous Cell Incorporation of Next-Generation Sequencing into Routine Clinical
Updated version
10.1158/1078-0432.CCR-15-2314doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2016/01/13/1078-0432.CCR-15-2314.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/22/12/2939.full#ref-list-1
This article cites 30 articles, 11 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/22/12/2939.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/22/12/2939To request permission to re-use all or part of this article, use this link
on December 28, 2020. © 2016 American Association for Cancer Research.clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2314