Embed Size (px)
Citation preview

Increasing
Access toKidney
Transplantation
Image courtesy of Vic Kulihin

2
Objectives and Overview
• Review kidney transplantation and discuss the need to increase transplantation rates
• Compare transplantation of high-Kidney Donor Profile Index (KDPI) kidneys to remaining on dialysis and waiting for low-KDPI kidneys
• Discuss transplantation with underutilized sources of deceased donor (DD) kidneys
• Examine available strategies to increase the living donor (LD) kidney pool, including improving risk prediction and increasing access through kidney-paired donation (KPD)
• Discuss programs and resources designed to increase transplant knowledge and access through patient and caregiver education

The Growing Need for Kidney Transplantation

4
• Benefits of kidney transplantation over dialysis
Dialysis Transplant
Significantly lower mortality rates in most studies1
Significantly higher quality of life1
Improved outcomes regardless of recipient age or underlying comorbidities2
Kidney Transplantation Has Been Shown to Improve Patient Outcomes
1. Tonelli M, et al. Am J Transplant. 2011;11(10):2093-2109.
2. Gill JS, et al. Kidney Int. 2005;68(5):2345-2351.
3. Wolfe RA, et al. N Engl J Med. 1999;341(23):1725-1730.
Patients who receive a deceased donor kidney transplant are projected to
live an average of 10 years longer than those who remain on dialysis3

5
Despite Positive Trends, There Continues to Be a Gap Between Supply and Demand
• Kidney transplants rose in 2016 due to an increase in DD transplants, though
LD transplants have declined since 2004
• The number of candidates on the inactive waiting list decreased in 2016,
while the active list continues to be problematic
• By the end of 2016, 95,456 patients remained on the waiting list
OPTN/SRTR 2016 Annual Data Report. Rockville, MD: Department of Health and
Human Services, Health Resources and Services Administration; 2017.
DD, deceased donor; LD, living donor.
Hart A, et al. Am J Transplant. 2018;18(suppl 1):18-113.
Candidates on the Kidney
Transplant Waiting ListTotal Kidney Transplants
Year
Can
did
ate
s (
inth
ou
san
ds)
Year
Tra
nsp
lan
ts (
inth
ou
sa
nd
s)
All
DD
LD

6
Waiting List Times Remain Long and May Be Associated With Poor Outcomes
• More than 40% of adults listed in
2013 were still waiting for a transplant
3 years later (2016)
• In 2016, more than 20% of waiting list
candidates had been on dialysis for
at least 6 years
Hart A, et al. Am J Transplant. 2018;18(suppl 1):18-113.
3-Year Outcomes for Adults on the Waiting List
In 2016, more than 25% of adult patients were removed fromthe kidney transplant list due to death or deteriorating medical conditions,
reflecting the ongoing organ shortage
Months Postlisting
OPTN/SRTR 2016 Annual Data Report. Rockville, MD: Department of Health and
Human Services, Health Resources and Services Administration; 2017.
Pe
rce
nta
ge
Still waiting

7
Access toKidney Transplantation
• Strategies to increase transplantation rates may utilize both deceased and living donor kidneys
Growing living donor transplantation
Maggiore U, et al. Nephrol Dial Transplant. 2015;30(2):217-222.
Utilizing deceased donor kidneys

Deceased Donor TransplantationGrowing High-KDPI Transplantation Rates

9
• In the current KAS, KDPI replaced SCD/ECD terminology and provides increased precision in determining organ quality2
• KDPI is a measure of relative risk derived from the Kidney Donor Risk Index on a cumulativepercentage scale2
• KPDI is calculated using 10 donor criteria,2which are weighted differently
– Age
– Height
– Weight
– Ethnicity
– History of hypertension
– History of diabetes
– Cause of death
– Serum creatinine
– Hepatitis C virus (HCV) status
– Donation after circulatory death
Donor Kidneys Are Risk-Stratified Using KDPI1
ECD, expanded criteria donor; KAS, kidney allocation system; SCD, standard criteria donor.
1. Israni AK, et al. J Am Soc Nephrol. 2014;25(8):1842-1848.
2. OPTN. Guide to calculating and interpreting KDPI. 2012.
https://optn.transplant.hrsa.gov/media/1512/guide_to_calculating_interpreting_kdpi.pdf. Accessed January 24, 2018.
3. OPTN Membership and Professional Standards Committee. Transplant Program Performance Measures Review:
Outcome Measures Work Group Update. December 2015. https://www.transplantpro.org/wp-content/uploads/sites/3/MPSC-
Performance-Metrics-Project-Update_Dec-2015.pdf. Accessed January 24, 2018.
4. Stewart D et al. Am J Transplant. 2013;13(S5):123-124.
Graft Survival and Discard Rates by KDPI3,4
71.9%
71.1%
91.5%90.0% 89.0% 87.9% 86.6% 85.2% 83.7% 81.9%
78.9%76.3%
2-year graft survival
Discard rate(Post-KAS in DonorNet)
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
A lower KDPI is associated with better
posttransplant graft survival2
Kidney Donor Profile Index (KDPI)
Used with permission from Stewart D et al. Am J Transplant. 2013;13(S5):123-124.
© John Wiley and Sons.

10
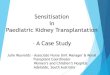
About Half of Recovered High-KDPI Kidneys Are Discarded1
• In 2017, 1,652 kidneys with a KDPI 86%-100% were discarded2
• The willingness to accept an ECD or high-KDPI kidney has continued to decrease since 20141
Rates of Kidneys Recovered for Transplant and Not Transplanted1
Percentage of Patients Willing to Accept ECD or KDPI >85% Kidney1
1. Hart A, et al. Am J Transplant. 2018;18(suppl 1):18-113.2. Organ Procurement and Transplantation Network. US Department of Health and Human Services.
https://optn.transplant.hrsa.gov/data/view-data-reports/national-data/. Accessed January 30, 2018.
3. Massie AB, et al. Am J Transplant. 2014;14(10):2310-2316.
High-KDPI score alone should rarely disqualify a
potential donor kidney from consideration3
Year
Pe
rce
nta
ge
Year
OPTN/SRTR 2016 Annual Data Report. Rockville, MD: Department of Health and
Human Services, Health Resources and Services Administration; 2017.P
erc
en
tag
e

11
High-KDPI Kidneys Offered a Survival Advantage Compared With Remaining on the Waiting List
KT, kidney transplant.
Massie AB, et al. Am J Transplant. 2014;14(10):2310-2316.
0 1 2 3 4
Years Since High-KDPI KT
5
3
2.5
2
1.5
1
.8
.6
.4
Cu
mu
lati
ve M
ort
ality
Rati
o (
log
scale
)
Worse survival with high-KDPI KT
Equal survival
Better survival with high-KDPI KT
KDPI=91-100
KDPI=81-90
KDPI=71-80
• A retrospective study examined outcomes associated with accepting a
>70 KDPI kidney vs remaining on the waiting list for a ≤70 KDPI kidney
• Patients who received a transplant with a >70 KDPI kidney had a 6-month
period of higher mortality risk followed by an extended period of lower
mortality risk compared with those who waited for a lower-KDPI kidney and
remained on dialysis (n=50,708)
Relative Survival
High-KDPI KT vs Waiting for a Lower-KDPI Kidney
Used with permission from Massie
AB, et al. Am J Transplant.
2014;14(10):2310-2316. © 2014
John Wiley and Sons.

12
The Benefit of High-KDPI Kidneys Depends on Patient Characteristics
Massie AB, et al. Am J Transplant. 2014;14(10):2310-2316.
• The highest-risk kidneys were a benefit for patients older than 50 years at centers with waiting times of ≥33 months
Decision Tree for Acceptance of High-KDPI Organ Offers
KDPI 91-100
Age >50
years?
Centerwait
Centerwait
time ≥33 months?
time ≥33months?
Diabetic?
No
No
No
No
Yes
Yes
Yes
Yes
High-KDPI kidneys may offer a benefit to appropriate patients
Harm Equipoise Benefit
Used with permission from Massie AB, et al. Am J Transplant. 2014;14(10):2310-2316. © 2014 John Wiley and Sons.

13
High-Risk Kidneys Did Not Negatively Affect Program Reports
0.5
1.0
2.0
Ad
jus
ted
HR
Transplantation of High-KDPI Kidneys Did Not
Affect the HR for a Program’s Graft Survival1
0
HR, hazard ratio.
*P value reflects test for change in volume between centers with and without low-performance evaluations.
1. Snyder JJ, et al. Am J Transplant. 2016;16(9):2646-2653.
2. Schold JD, et al. Am J Transplant. 2013;13(1):67-75.
There is no evidence that changing volume will improve center performance. Centers should
ensure that high-risk patients have access to transplant despite low-performance concerns2
0.00 0.05 0.10 0.15 0.20 0.25 0.30 0.35
Proportion of Each Program’s Recipients
Receiving a High-Risk Donor KidneyOPTN/SRTR 2014 Annual Data Report: Kidney. Rockville, MD: Department of Health
and Human Services, Health Resources and Services Administration; 2014.Used with permission from Snyder JJ, et al. Am J Transplant. 2016;30(9):1066-1073.
© 2016 John Wiley and Sons.
Ave
rag
e C
en
ter
Ch
an
ge
in
Tra
nsp
lan
tV
olu
me
-20
-15
-10
0
10
15
5
LD
Transplants
P=0.01*
ECD
Transplants
P=0.001*
-5 -3.7
-14.7
SCD
Transplants
P=0.02*
+10.3
+3.9
-4.7-3.1
Centers without low-performance
evaluations
Centers with low-performance
evaluations
Low-Performance Flags Lead to
Reductions in Transplant Volume2

Deceased Donor TransplantationIncreasing Access to Underutilized Donor Sources

15
U.S. Public Health Service Guideline for Infectious Risk Kidneys
• PHS categorizes some donors as atincreased risk for disease transmission (IRD)1,2
• The PHS guidelines include risk of HIV, HBV, and HCV2
The Percentage of Donor Kidneys Classified as IRD Is Rising1
– 12.3% of kidneys (2/1/2013-7/1/2013)
– 19.5% of kidneys (2/1/2014-7/1/2014)
• The exact reasons for these increases are unknown but may be related to the opioid epidemic3
HBV, hepatitis B virus; PHS, U.S. Public Health Service.
*Within the preceding 12 months.
1. Kucirka LM, et al. Am J Transplant. 2015;15(12):3215-3223.
2. Seem DL, et al. Public Health Rep. 2013;128(4):247-343.3. OPTN. Public comment proposal. Guidance on explaining risk related to use of U.S. PHS increased risk donor organs
when considering organ offers. https://optn.transplant.hrsa.gov/media/2116/guidance_increased_risk_organ_offers_
20170327.pdf. Accessed January 28, 2018.
Risk Factors Associated With IRD2,*
• Sex with a person known or suspected to have HIV, HBV, or HCV infection
• Men who have had sex with men (MSM)
• Sex with a man with a history of MSM behavior
• Sex in exchange for money or drugs
• Sex with a person who has had sex in exchange for money or drugs
• Sex with a person who has injected drugs byintravenous, intramuscular, or subcutaneousroute for nonmedical reasons
• Use of injected drugs by intravenous, intramuscular, or subcutaneous route for nonmedical reasons
• Lockup, jail, prison, or a juvenile correctional facility for more than 72 consecutive hours
• Diagnosis with, or treatment for, syphilis, gonorrhea, chlamydia, or genital ulcers

16
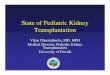
Opioid Epidemic:Impact on Kidney Transplant
• Opioids were involved in42,249 deaths in 2016, and opioid overdose deaths were 5 times higher in 2016 than in 19991
• PHS guidelines classify organs from individuals who use opioid for nonmedical reasons as at increased risk for infection with HIV, HBV,and HCV2
• However, the risk of HIV or HCV transmission from a NAT-negative donor organ from an injection drug user is <1%3,4
NAT, nucleic acid testing.1. Centers for Disease Control and Prevention. Drug overdose death data.
https://www.cdc.gov/drugoverdose/data/statedeaths.html. Accessed January 28, 2018.
2.Seem DL, et al. Public Health Rep. 2013;128(4):247-343.
3. Kucirka LM, et al. Am J Transplant. 2011;11(6):1176-1187.
4. Kucirka LM, et al. Am J Transplant. 2011;11(6):1188-1200.5.Durand CM, et al. Ann Intern Med. 2018;168(10):702-711. 6.
Pullen LC. Am J Transplant. 2017;17(9):2231-2232.
Number of Kidneys Transplanted From
Death by Overdose Donors5
The risks of using donor kidneys from opioid users should be consideredalong with the benefits for appropriate patients6
Nu
mb
er
of
Kid
ne
yTra
nsp
lan
ts
2000 2002 2004 2006 2008 2010 2012 2014 2016
Year Transplanted
0
300
600
900
1200
1500
1800
From Annals of Internal Medicine, Durand CM, et al. 168(10), 702-777.© 2018 American College of Physicians. All Rights Reserved.
Reprinted with the permission of American College of Physicians, Inc.

17
Transplantation of Infectious Risk Kidneys
• Discard rates of IRD kidneys were higher than their non-IRD counterparts, despite potential benefit in some patient populations1,2
• 5 years after declining an IRD kidney offer2
– 39.5% of patients had died or had been removed from the waiting list
– 31% of patients had received a non-IRD DD kidney transplant
• Patients declined an IRD kidney with a median KDPI of 21 and accepted a non-IRD kidney with a median KDPI of 522
1. Chow EK, et al. Am J Transplant. 2013;13(5):1227-1234.
2. Bowring MG, et al. Am J Transplant. 2018;18(3):617-624.
Years PostdecisionUsed with permission from Bowring MG, et al. Am J Transplant. 2018; 18(3):617-624.
© John Wiley and Sons.
Patient Mortality Among Those WhoAccepted
vs Declined the IRD Kidney Offer2
Education on the risks and benefits can help increase utilization of IRD
kidneys in appropriate patients2
P<0.001
Cu
mu
lati
ve M
ort
ality
,%

18
A Prediction Model for IRD Kidneys
Base-case estimate – mortality risk (if seroconverted) increased by 4.12% HIV, 3.42% HCV per year.
Worst-case estimate – mortality risk (if seroconverted) equivalent to immediate (100% chance) death.
Chow EK, et al. Am J Transplant. 2013;13(5):1227-1234.
100
70
55
40
25
48 60
Perc
en
tag
eA
live 85
93%92%90%
100
70
55
40
25
48 60
• A Markov decision process model was designed to predict survival associated with accepting an IRD kidney vs declining an IRD kidney and remaining on dialysis based on patient characteristics
• A functional implementation of this model can be found at http://transplantmodels.com/ird
Predicted Survival After Accepting or Declining IRD Kidneys
40F, 3 Months Until Non-IRD Transplant 65F, Diabetic, 60 Months to Non-IRD Transplant
Perc
en
tag
eA
live
Accept IRD (base-case)
Accept IRD (worst-case)
Decline IRD
0 12 24 36
85
69%67%
33%
Accept IRD (base-case)
Accept IRD (worst-case)
Decline IRD
0 12 24 36
Months Since IRD Accept/Decline Decision Months Since IRD Accept/Decline Decision
Used with permission from Chow EK, et al. Am J Transplant. 2013;13(5):1227-1234. © 2013 by John Wiley and Sons.

19
Direct-Acting Antivirals Have Changed the Utilization of HCV+ Kidneys
D+, donor positive; DAAs, direct-acting antiviral agents; FW, follow-up week; POD, postoperative day;
R-, recipient negative; TW, treatment week.
*A cure was defined as a sustained virologic response 12 weeks after the end of treatment.
1. Kamar N, et al. Am J Transplant. 2016;16(5):1474-1479.
2. Lin MV, et al. PLoS One. 2016;11(7):e0158431. doi: 10.1371/journal.pone.0158431.
3. Goldberg DS, et al. N Engl J Med. 2017;376(24):2394-2395.
4. Durand CM, et al. Ann Intern Med. 2018;168(8):533-540.
• The development of DAAs and thesubsequent reduction of interferon-based regimens have resulted in awell-tolerated and efficacious treatment for HCV1,2
• The open-label, single-center THINKER trial found that transplant of HCV+ kidneys into HCV- recipients, followed by the use of DAAs, provided excellent allograft function with a cure of HCV infection3,*
• Durand et al also showed that pretransplant and posttransplant HCV treatment was safe and prevented chronic HCV infection in HCV D+/R-kidney transplant4
HCV RNA Was Not Detected in HCV
D+/R- Kidney Transplant Recipients
After Treatment4
HC
V R
NA
, lo
g1
0IU
/mL
1
2
3
4
5
Time Point
From Annals of Internal Medicine, Durand CM, et al. 168(8), 533-540.© 2018 American College of Physicians. All Rights Reserved.
Reprinted with the permission of American College of Physicians, Inc.

20
Increasing Access to HIV+Kidneys
• Patients with HIV have similar graft failure rates to patients without HIV1
• Transplant between HIV+ recipient/donor pairs has been conducted in South Africa but was not allowed in the United States prior to 20131,2
• The HOPE Act was passed in 2013 and allowed HIV+ kidneys to be transplanted into HIV+ patients2
• The first HIV+ to HIV+ transplant in the United States took place in 20163
• As of November 2017, 22 transplant centers were approved to perform HIV+ to HIV+ transplants4
1. Muller E, et al. N Engl J Med. 2015;372(7):613-620.
2. Boyarsky BJ, et al. Ann Surg. 2016;263(3):430-433.
3. Cohn M. Johns Hopkins performs first transplants between donors, recipients infected with HIV.
The Baltimore Sun. March 30, 2016.
http://www.baltimoresun.com/health/bs-hs-hiv-transplant-20160329-story.html. Accessed January 25, 2018.
4. Doby BL, et al. Curr Opin Organ Transplant. 2018;23(2):271-278.
Patients with HIV can be organ donors or receive a transplant3

Living Donor TransplantationExpanding Donation by Improving Risk Prediction

22 <insert Sanofi Genzyme logo>
Living Donation Has Lifetime Implications
• Every year in the United States, approximately 6,000 healthy adults accept the risks of donor nephrectomy to help improve the lives of others1
• Donating a kidney is a decision with lifetime implications for the living donor2
• Transplant programs should support donor candidates throughout the decision-making process and have a responsibility to ensure that donors are aware of all the potential risks1,2
• In 2017, KDIGO published clinical practice guidelines on the evaluation and care of living kidney donors and provided recommendations to assist medical professionals who evaluate living donor candidates2
KDIGO, Kidney Disease: Improving Global Outcomes.
1. Muzaale AD, et al. JAMA. 2014;311(6):579-586.
2. Lentine KL, et al. Transplantation. 2017;101(8S suppl 1):S1-S109.

23
Risk of Developing ESRD in Living Donors
• The most direct effect of living kidney donation is the long-term risk of developing ESRD1
• Analysis of national registry data revealed that estimated risk of ESRD in living donors varied according to donor characteristics2:
ESRD, end-stage renal disease.
1.Lentine KL, et al. Transplantation. 2017;101(8S suppl 1):S1-S109.2.Massie AB, et al. J Am Soc Nephrol. 2017;28(9):2749-2755.
3. Muzaale AD, et al. JAMA. 2014;311(6):579-586.
ESRD per 10,000 P Value
Living donors 90 REF
Unscreened nondonors 326 <0.001
Healthy nondonors 14 <0.001
Overall, the magnitude of the absolute risk increase of ESRD in living donors was small3
– Biologically related to recipient
– High BMI
– Male
– Black
Estimated Risk of Developing ESRD by Age 803
Living donors are at higher risk of
ESRD than similarly healthy
non-donors but still have a much
lower risk than the general
population3

24
Tool to Help Evaluate Risk of ESRD
• Together KDIGO and CKD-Prognosis Consortium developed an online risk tool to help evaluate, counsel, and accept living kidney donor candidates1,2
• The risk of developing ESRD is influenced by a combination of demographic and health characteristics1
• The model can be found at www.transplantmodels.com/esrdrisk2
Projections of the Incidence of ESRD in the US According to
Age, Race, and Sex for the Base-Case Scenario2
15-Year Projected Incidence of ESRD* Lifetime Projected Incidence of ESRD
From N Engl J Med. Grams ME, et al. 374, 411-421 © 2016 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
BMI, body mass index; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate.*The base-case scenario for the 15-year projected risk is the following: an age-specific eGFR (114, 106, 98, 90, 82, 74, and 66 mL per minute per 1.73 m2 for an age of
20, 30, 40, 50, 60, 70, and 80 years, respectively), systolic blood pressure of 120 mm Hg, a urinary albumin-to-creatinine ratio
of 4, a BMI of 26, and no diabetes mellitus or use of antihypertensive medication.1. Lentine KL, et al. Transplantation. 2017;101(8S suppl 1):S1-S109.
2. Grams ME, et al. N Engl J Med. 2016;374(5):411-421.
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0.0
Inc
ide
nc
e,%
Black men
Black women
White men
White women
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0.0
Inc
ide
nc
e,%
20 30 40 50 60 70 80 20 30 40 50 60 70 80
Age, years Age, years
Black men
Black women
White men
White women

25
The Living Kidney Donor Profile IndexAllows for Comparison of DD and LD Kidneys
• The Living Kidney Donor Profile Index (LKDPI) allows for comparison of all available kidneys and can help ensure that candidates receive the kidney that will provide the greatest benefit
• Donor factors that affect living donor transplant outcomes, which are weighted differently, include
– Age (among donors aged >50 years)
– Body mass index
– Race
– History of cigarette use
– Systolic blood pressure
– ABO incompatibility with recipient
– HLA-B mismatches with recipient
– HLA-DR mismatches with recipient
HLA, human leukocyte antigen.
Massie AB, et al. Am J Transplant. 2016;16(7):2077-2084.
Distribution of LKDPI and KDPI
-40 -20 0
20
15
10
5
0
LD KDPI
DD KDPI
20 40 60 80 100
KDPI
Dis
trib
uti
on
,%
Used with permission from Massie AB, et al. Am J Transplant. 2016;16(7):2077-2084.
© 2016 John Wiley and Sons.

26
Kidneys From Older Living Donors May Benefit Appropriate Patients
• An analysis of SRTR data evaluated outcomes of patients who underwent transplant with living donor kidneys from donors aged≥70 years
• Rates of graft loss were higher than those observed with younger living donors but were not significantly different from outcomes with deceased donors aged 50 to 59 years
• Appropriately selecteddonor-recipient pairs may benefit from transplantation of kidneys from living donors of advanced age
DD50, kidneys from deceased donors aged 50 to 59 years; LD50, kidneys from living donors aged 50 to 59 years;
LD70, kidneys from living donors aged ≥70 years; SRTR, Scientific Registry of Transplant Recipients.
Berger JC, et al. Clin J Am Soc Nephrol. 2011;6(12):2887-2893.
Incidence of Graft Failure
Recipients of LD70 (n=219)
Recipients of DD50 (n=21,195) P=0.5
Recipients of LD50 (n=16,051) P=0.037
50
40
30
20
10
0
0 1 2 3 4 5 6 7 8 9 10
Years After Transplantation
Cu
mu
lati
ve I
nc
ide
nc
e o
f G
raft
Fa
ilu
re,
%
Used with permission from Berger JC, et al.
Clin J Am Soc Nephrol. 2011;6(12):2887-2893.
© 2011 John Wiley and Sons

Living Donor TransplantationIncreasing Access Through Kidney Paired Donation (KPD)

28
KPD Programs Increased the Rate of Living Donation
• KPD programs have been predicted to increase the use of LD kidneys in the United States1
• A study of 34,843 LDKTs found that KPD transplants increased from 1.5% of LDKTs in 2006 to 9.9% of LDKTs in 20112
• A survey of potential living donors found that 64% were very willing to participate in paired donation3
– Significantly more than listexchanges or nondirecteddonation (P<0.001)
LDKT, living donor kidney transplant.
1. Segev DL, et al. JAMA. 2005;293(15):1883-1890.
2. Massie AB, et al. Am J Transplant. 2013;13(5):1317-1322.
3. Waterman AD, et al. Am J Transplant. 2006;6(7):1631-1638.
If all transplant centers perform KPD at the
same rates as very high-performing centers,
an estimated additional 1099 LDKTs will occur
each year2
KPD Utilization, 2006-20112
100
200
300
400
500
600 10
8
6
4
2
Perc
en
tag
e
Nu
mb
er
Number of KPD
per year
Percentage of all
LDKT that are KPD
2006 2007 2008 2009 2010 2011Used with permission from Massie AB, et al.
Year Am J Transplant. 2013; 13(5):1317-1322.
© John Wiley and Sons.

29
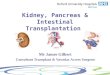
Approaches to KPD Vary Widely
NDD, non-directed donor; NEAD, nonsimultaneous extended altruistic donor.1. Wallis CB, et al. Nephrol Dial Transplant. 2011;26(7):2091-2099.
2. Glorie K, et al. Transpl Int. 2014;27(4):333-343.
3. Ferrari P, et al. Nephrol Dial Transplant. 2015;30(8):1276-1285.
4. Gentry SE, et al. Am J Kidney Dis. 2011;57(1):144-51.
Domino-Paired Donation Using Compatible Pairs
Donor 1
Donor 2
Recipient 1
Recipient 2(hard to match)
x
CompatibleR1
R2
R3
D1
D2
D3
NEAD Chain – Closed Chain
NDD
Waiting list
Time passes
x
Altruistic
donor
Donor 1
Donor 1
Donor 2
Recipient 1
Recipient 2x
Schematic Representations of Paired Donor Kidney Exchanges1-4
2-Way Exchange 3-Way Exchange
Donor 1
Donor 2
Recipient 1 (hard to match)
Recipient 2
Recipient 3Donor 3
x
D4R4
Donor 2 Recipient 2
Recipient 1
x
Waiting list

30
Potential Advantages of Using Compatible Pairs
28.2
64.5
37.4
75.480
70
60
50
40
30
20
10
0
Perc
en
tag
e o
f
Pati
en
tsM
atc
he
d
Single-center program
National KPD registry
• Simulated donors and recipients were used to investigate the impact of including ABO-compatible pairs* in KPD1
• Donors who were ABO-incompatible or crossmatch-incompatible with their intended recipients were included in this analysis1
• Including compatible pairs was predicted to double the match rate of KPD programs1
Percentage of Simulated Donor/Recipient
Pairs Who Find KPD Matches1
*Desensitization is not required for compatible pairs.2
1. Gentry SE, et al. Am J Transplant. 2007;7(10):2361-2370.2. UW Medicine. Desensitization. http://www.uwmedicine.org/health-library/Pages/desensitization.aspx.
Accessed January 24, 2018.
Incompatible Pairs Including Compatible Pairs
Used with permission from Gentry SE et al. Am J Transplant. 2007;17(10):2361-2370.
© 2007 John Wiley and Sons.

31
KPD Can Be Utilized at All Transplant CentersMulticenter KPD - Kidney Paired Donation Pilot Program
• The Organ Procurement and Transplantation Network, or OPTN, has developed the Kidney Paired Donation Pilot Program, a national exchange program to facilitate multicenter KPD1
• Centers in 40 states and the District of Columbia participate2
• Any candidate on the national organ transplant waiting list can join and will remain on the deceased donor waiting list1
Single-Center KPD - Methodist Specialty and Transplant Hospital
• In the first 3 years of implementation3
– Performed 134 total KPD transplants (114 with incompatible pairs, 17 with compatible pairs)
– 36% of KPDs were 2-way exchanges, 36% were 3-way exchanges, and 28% were chain transplants
– In the third year, KPD accounted for 35% of LDKTs
1. United Network for Organ Sharing. OPTN Paired Kidney Exchange Pilot Program.
https://www.unos.org/wp-content/uploads/unos/Living_Donation_KidneyPaired.pdf. Published 2015. Accessed January 24, 2018.2. United Network for Organ Sharing. Transplant centers participating in the OPTN Kidney Paired Donation Pilot
Program (KPDPP) as of December 31, 2017.
https://www.unos.org/wp-content/uploads/unos/OPTNKPDPPCentersByState.pdf?e4f722. Accessed January 24, 2018.
3. Bingaman AW, et al. Am J Transplant. 2012;12(8):2125-2132.

Increasing Transplantation Through Education

33
UNOS Kidney Transplant Learning Center
• An online national clearinghouse of public educational resources for people living with ESRD, those awaiting a kidney transplant, and potential living donors
• Resources were developed by national leaders in transplant education
• The learning center contains information on
– Kidney disease and treatment
– Dialysis
– Transplant from a deceased donor
– Transplant from a living donor
– Finding a living donor
– Being a living donor
UNOS. About the kidney transplant learning center.
https://transplantliving.org/kidney/about-the-kidney-transplant-learning-center/. Accessed January 26, 2018.
One-of-a-kind resource that is easy to
understand, navigate, and use
https://transplantliving.org/kidney/

34
Explore Transplant
• Explore Transplant is a nonprofit organization established to educate patients and caregivers on transplant and living donation1
• My Transplant Coach is an interactive decision aid for patients with kidney failure that is part of the Explore Transplant educational program2
– A recent pilot study found that MyTransplant Coach significantly increased transplant knowledge (P<0.001)3
• Explore Transplant and Explore Living Donation education materials are available in English and Spanish and help kidney patients and their caregivers make informed choices about treatment1
1. Explore Transplant and Living Donation. http://exploretransplant.org. Accessed January 26, 2018.
2. Explore Transplant and Living Donation. https://mytransplantcoach.org/#/. Accessed January 26, 2018.
3. Axelrod DA, et al. Clin Transplant. 2017;31(5). doi: 10.1111/ctr.12944.
https://mytransplantcoach.org/#/

35
Live Donor Champions Can Assist Patients by Serving as Advocates
• Live donor champions (LDCs) are family members or friends who serve as patient advocates and can help identify suitable livingdonors
• Results of LDC training
– Trained LDCs became more comfortable initiating conversations aboutlive kidney donation
– Significantly more potential donors contacted the transplant center
– Significantly higher rates ofliving donor transplantationwere reported
LDCParticipants
(n=15)
Matched
Controls
(n=15) P Value
Donor inquiries 25 0 <0.001
Outcomes
Live donor
transplantation4 0 <0.001
Live donor
evaluation
pending3 0 Not reported
Deceased donor
transplantation4 5 Not reported
Deaths 0 0 Not reported
Wait-listed 4 10 Not reported
Garonzik-Wang JM, et al. Transplantation. 2012;93(11):1147-1150.
Used with permission from Garonzik-Wang JM, et al. Transplantation, 93, 11; 1147-1150. © 2012.

36 <insert Sanofi Genzyme logo>
Increasing Donation Rates Through Social Media
• On May 1, 2012, Facebook® began allowing their users to select an organ donor status1
– A 21.1-fold increase over the baseline daily registration rate was observed on the first day of the Facebook initiative
• A Facebook app was also developed that allows transplant candidates to share their need for a donor with their Facebook friends2
• Transplant candidates who used the Facebook app were more likely to have a potential donor come forward than matched controls (P<0.001)2
app, application.1. Cameron AM, et al. Am J Transplant. 2013;13(8):2059-2065.
2. Kumar K, et al. Am J Transplant. 2016;16(12):3548-3553.
Time to First Donor Referral2
0
0
Control
Facebook app
Perc
en
tag
e
10
20
2 4 6 8Follow-up Time, months
10
P<0.001
150
53
144
49
142
46
139
46
138
40
Number at riskControl 154
Facebook app 54
Used with permission from Kumar K, et al. Am J Transplant. 2016;16(12):3548-3553.
© 2016 John Wiley and Sons.

37
Using House Calls to Educate on Living Donor Transplantation
• Racial/ethnic disparities exist in living donor transplant rates, mostly affecting black patients with ESRD
• Educational interventions developed to address these disparities have been evaluated
• Patients were randomized to receive 1 of 3 educational interventions
– House call – held in a patient’s home, included invited guests (n=54)
– Group based – held at a transplant center, included invited guests (n=49)
– Individual counseling – 1-on-1 counseling between a patient and a health care provider at a transplant center (n=49)
65
39
27
0
20
40
60
80
100
House Calls Group Based Individual Counseling
Perc
en
tag
e o
fE
valu
ati
on
s P<0.001
House Call Patients Were the Most
Likely to Have Donor Evaluations
Educating a patient’s social network
may increase the likelihood of
identifying potential living donors
Rodrigue JR, et al. Transplantation. 2014;98(9):979-986.

38
Conclusions
• Kidney transplantation provides a well-established benefit to patients with ESRD
• Strategies to improve access to kidney transplantation will allow as many patients as possible to receive this beneficial treatment
• Early transplantation with underutilized deceased donor kidneys may provide survival benefits over waiting for a lower-KDPI kidney and does not affect program reports
• Living donation is associated with improved patient outcomes; risk prediction tools and KPD may improve utilization of living donor kidneys
• Educational programs for caregivers, patients, and family members may be used to better understand the transplant process, make informed treatment decisions, and identify potential living donors

38
Conclusions
• Kidney transplantation provides a well-established benefit to patients with ESRD
• Strategies to improve access to kidney transplantation will allow as many patients as possible to receive this beneficial treatment
• Early transplantation with underutilized deceased donor kidneys may provide survival benefits over waiting for a lower-KDPI kidney and does not affect program reports
• Living donation is associated with improved patient outcomes; risk prediction tools and KPD may improve utilization of living donor kidneys
• Educational programs for caregivers, patients, and family members may be used to better understand the transplant process, make informed treatment decisions, and identify potential living donors