Embed Size (px)
Citation preview

Clinical Neurophysiology 119 (2008) 2437–2446
Contents lists available at ScienceDirect
Clinical Neurophysiology
journal homepage: www.elsevier .com/locate /c l inph
Independent component analysis of subdurally recorded occipital seizures
Anish Patel a, Faisal Alotaibi b, Warren T. Blume b, Seyed M. Mirsattari b,c,d,e,*
a Schulich School of Medicine and Dentistry, The University of Western Ontario, London, Ont., Canadab Department of Clinical Neurological Sciences, The University of Western Ontario, London, Ont., Canadac Department of Medical Biophysics, The University of Western Ontario, London, Ont., Canadad Department of Medical Imaging, The University of Western Ontario, London, Ont., Canadae Department of Psychology, The University of Western Ontario, London, Ont., Canada
a r t i c l e i n f o a b s t r a c t
Article history:Accepted 17 July 2008Available online 21 September 2008
Keywords:Occipital lobeEpilepsySeizuresEpileptogenic zoneElectroencephalogram (EEG)Independent component analysis (ICA)
1388-2457/$34.00 � 2008 Published by Elsevier Ireladoi:10.1016/j.clinph.2008.07.276
* Corresponding author. Address: Department of CThe University of Western Ontario, B10-108, 339 WinCanada N6A 5A5. Tel.: +1 519 663 3348; fax: +1 519
E-mail address: [email protected] (S.M. Mirsattari)
Objective: To study the components of occipital seizures using independent component analysis (ICA) ofsubdurally recorded electroencephalogram (EEG) data.Methods: Twenty-seven subdurally recorded occipital seizures from eight patients were studied. ICA wasperformed, and the resulting independent components (ICs) were compared with respect to their power,frequency, degree of spread within the epileptogenic zone, and propagation patterns. The ictal ICs werefurther subdivided into propagating and non-propagating types.Results: ICA provided information over and above that supplied by standard visual EEG analysis, confirm-ing that all the seizures originated in the occipital lobe, and affording additional knowledge regarding thenature of the seizure onset zone. Each seizure was composed of multiple ICs, some of which propagatedwhile others remained within the epileptogenic zone. There was no statistical difference between thepropagating and non-propagating ICs with respect to power or frequency. However, propagating ICsinvolved a significantly greater number of recording electrodes at their onset when compared to thenon-propagating ICs.Conclusions: The propagation likelihood of ICs in occipital seizures is independent of their power or fre-quency, but it is dependent on the volume of brain giving rise to that signal; ICs that are generated by agreater volume of brain within the epileptogenic zone are more likely to propagate.Significance: This study shows that ICA has the potential to be used to redefine the epileptogenic zone andguide the extent of cortisectomy for the treatment of patients with medically intractable occipital epilepsy.
� 2008 Published by Elsevier Ireland Ltd. on behalf of International Federation of ClinicalNeurophysiology.
1. Introduction
Occipital lobe seizures may present with an array of visual andnon-visual symptoms (Ludwig and Marsan, 1975; Blume et al.,1991; Salanova et al., 1992; Williamson et al., 1992; Blume andWiebe, 2000; Blume et al., 2005). Elementary visual phenomenasuch as sparks, stars, wheels, colors, lines, circles, shapes, shadows,and loss of vision result from the direct activation of primary visualcortex. Bilateral visual field involvement, complex visual symp-toms, motor, somatosensory, and experiential phenomena whichmay or may not be preceded by simple visual symptoms implicateseizure spread to other cortical and subcortical regions. Propaga-tion is more likely with ictal discharges of greater intensity, asshown by Collins and Caston (1979) when they varied the amount
nd Ltd. on behalf of International F
linical Neurological Sciences,dermere Road, London, Ont.,663 3440..
of the epileptogenic agent penicillin administered to rat occipitalcortex. Seizure spread may involve the ipsilateral or contralateralcerebral cortex and subcortical structures (Collins and Caston,1979). Rapid and variable propagation patterns even among differ-ent seizures from the same patient make occipital lobe epilepsy(OLE) hard to diagnose (Williamson et al., 1992).
Electroencephalography (EEG) records the extracellular electri-cal field potentials generated by a population of cortical neuronsand amplifies small changes in the voltage difference betweentwo input electrodes, displaying them continuously with greattemporal resolution (Hughes, 1982; Lothman, 1993). Scalp EEGhas poor spatial resolution; cortical gyri and sulci in the humanbrain make interpretations of EEG difficult such that scalp EEGmay not detect a deeply located epileptic focus involving themesial or inferior cortical surfaces (Gloor, 1985). In OLE, estimatesof the localizing accuracy of scalp EEG range from 17% to 68% (Leeet al., 2005) because topography of the occipital cortex mesially atthe banks of the calcarine fissure renders EEG detection of mesialoccipital spikes and seizure onset zone difficult. In one study,
ederation of Clinical Neurophysiology.

2438 A. Patel et al. / Clinical Neurophysiology 119 (2008) 2437–2446
14% of OLE patients were found to have normal routine EEGs(Blume and Wiebe, 2000). A significant number (24–64%) of pa-tients with OLE may have unilateral, bilateral, or exclusively con-tralateral temporal lobe epileptiform potentials in their EEGs(Blume and Wiebe, 2000). Frontal lobe spread has also been re-ported (Williamson et al., 1992). Thus, patients with OLE couldpresent with apparent onset of their seizures in the frontal, parie-tal, or temporal lobes.
Approximately 30% of patients with focal epilepsy are resistantto medical therapy (Kwan and Brodie, 2000) and could benefitfrom surgical resection of the brain area responsible for the seizureactivity, i.e. the epileptogenic zone. The epileptogenic zone can bedefined as the area of cerebral cortex whose removal is required torender the patient seizure-free (Rosenow and Lüders, 2001). How-ever, there is currently no diagnostic test to accurately map out theextent of the epileptogenic zone. Failure to become seizure free fol-lowing epilepsy surgery is suggestive of a larger than expected epi-leptogenic zone in a given patient. On the other hand, if the patientbecomes seizure free after surgery it can be inferred that the epi-leptogenic zone was included in the resected cortex. Therefore,accurate mapping of the epileptogenic zone is needed in order toimprove the outcome of epilepsy surgery.
Treatment for OLE is complicated by varying manifestations ofthese seizures due to their variable propagation patterns (Aykut-Bingol et al., 1998). Such seizures may also involve the parietaland posterior temporal lobes, giving rise to the more inclusive des-ignation of posterior cortex seizures. In patients with medicallyintractable OLE who are surgical candidates, accurate localizationof seizure activity is required (Brekelmans et al., 1998). Thisrequires invasive EEG monitoring with depth electrodes, subdurallines, or grids. Although subdural EEG localization is superior tothat of scalp EEG, its accuracy depends on the extent of coverageand proximity to the epileptogenic zone. The reported accuracyof subdural EEG among patients with OLE ranges from 53% to74% (Weinand et al., 1995). One inherent limitation of EEG in pre-cise mapping of the epileptogenic zone is due to the obfuscationthat results from recording the summation of signals from a largepopulation of neurons.
Independent component analysis (ICA) is a mathematical algo-rithm that is able to extract a set of independent components (ICs)from a recorded mixture of signals, such that the ICs are an approx-imation of the source signals that gave rise to the original record-ing (Makeig et al., 1996; Brown et al., 2001; Stone, 2002). Giventhat an EEG recording consists of the combination of many neuralsignals, ICA of EEG data should be able to decompose the seizurerecording to yield a set of individual source signals which areresponsible for the underlying activity seen in the EEG. Indeed,ICA has already been applied to scalp EEG data to remove variousartifacts such as eye blinks, muscle potentials, and cardioballisticsignals (Iriarte et al., 2003), and also to differentiate and separateepileptiform spikes and lateralize seizure activity (Nam et al.,2002; Urrestarazu et al., 2006a). ICA application to invasive EEGrecordings is in its infancy; currently only one publication existsfor depth electrodes (Urrestarazu et al., 2006b) which showed thatICA was able to identify bilateral ictal activity at a time where stan-dard EEG interpretation of intracranial electrodes showed only uni-lateral activity.
To our knowledge, ICA has not been applied to subdurally re-corded EEG data, especially from the occipital lobe. Existing litera-ture on OLE has demonstrated the inability of standard EEGtechniques to adequately locate areas of epileptogenesis (Blumeet al., 2005), and given the complex and variable propagation pat-terns seen in occipital epilepsy patients, the need for other tech-niques to better localize the epileptogenic zone can beappreciated. The objective of this study is thus to apply ICA to sub-durally recorded occipital seizures in order to gain additional infor-
mation about the underlying generators of them and todemonstrate the usefulness of ICA as a supplementary tool in theanalysis of these seizures with respect to the composition of theepileptogenic zone and propagation patterns from the epilepticfocus.
2. Methods
2.1. Patient selection
We randomly chose 8 patients with OLE who underwent sub-dural electrode placement as inpatients in the Epilepsy MonitoringUnit (EMU) at London Health Sciences Centre (University Hospital,London, ON), between 2001 and 2007. The study was approved bythe Research Ethics Board of the University of Western Ontario.Age at seizure onset ranged from 5 to 16 years (mean =10.25 ± 3.32 years), with the age at the time of EMU admissionranging from 16 to 41 years (mean = 26 ± 9.35 years). Initial evalu-ation of all the patients included a clinical history, neurologicalexamination, neuropsychological evaluation, and anatomical mag-netic resonance imaging (MRI). Pertinent results from these inves-tigations, as well as other patient characteristics, are shown inTable 1.
Scalp EEG based on the extended 10–20 International Systemof electrode placement (Jasper, 1958) plus two mandibularnotch electrodes (M1,M2) was first used to identify and confirmthat these patients had seizures originating in the occipital lobe.In all the cases, scalp EEG in combination with clinical andimaging results were not sufficient to accurately localize theepileptic focus. Therefore, all these patients required invasivesubdural EEG monitoring. The number of electrodes and theirplacement varied for each patient. In some cases, the subduralEEG recording was able to provide more specific localizationof the seizure focus, while in other cases, the epileptogenic zoneremained ill-defined. Multiple seizures were recorded from eachpatient; of these, approximately 2–5 were analyzed from eachpatient, resulting in a total of 27 seizures for consideration inthis study.
For those patients who underwent resective surgery, post-oper-ative outcome was defined by the Engel classification: Class I refersto those patients who become post-operatively free of disablingseizures; class II refers to patients who subsequently have rare epi-sodes of disabling seizures; class III describes patients who experi-ence some degree of worthwhile improvement; class IV refers tothose patients who experience no worthwhile improvement intheir seizures (Engel et al., 1993). The term ‘‘seizure onset zone”was used to refer to the potential epileptogenic zone because notall the patients underwent surgery and not all those who had sur-gery became seizure free. The seizure onset zone refers to the areaof the cortex from which the clinical seizures were generated(Rosenow and Lüders, 2001).
2.2. Data analysis
Patients were monitored using XLTEK equipment (Oakville,ON), recording 128-channels of subdural EEG at sampling rates ofeither 250 or 500 Hz. The subdural wire lines were embedded insilicon and consisted of 8 to 12 EEG recording contacts made ofplatinum (Ad-Tech Medical Instrument Corp., Racine, WI). EachEEG contact measured 2.5 mm in diameter and was surroundedby a ring made of the same material that measured 4 mm in diam-eter. The center of EEG contacts in the subdural lines was 1 cmapart from each other.
Using the computer software platform MATLAB (Mathworks,Natick, MA), an in-house program was created and used to loadthe subdural EEG data from each seizure into memory and

Table 1Clinical profile of the patients (n = 8)
Pt Age at seizureonset (years)
Age at subduralrecording (years)
Seizuretypes
Etiology ofseizures
Epileptogenic zonelocalization by scalpEEG
Epileptogenic zonelocalization by subduralEEG
MRI findings Visual fields(Goldmannperimetry)
AEDs
1 10 16 SFSCPSGTCS
Cryptogenic L occipital L mesial occipital belowthe calcarine sulcus
Normal Full OXC*PHT*CBZ*CLB*VPA*LTG*LEVPRM
2 12 37 CPSGTCS
Trauma,stroke
R posterior lateraloccipital
R mesial inferioroccipital–temporal
R inferior–posterioroccipital–parietalinfarct
L inferiorhomonymousquadrantopia
CBZ*PB*PHT
3 8 21 CPSGTCS
Cryptogenic R temporal R mesial inferior occipital Normal Full LEV*PHT*CLB*VPA*TPM*CBZLTGCNZ
4 8 22 SFSCPSGTCS
Cryptogenic Bioccipital Bilateral mesial occipital,R mesial temporal
Normal Full CBZ*LTG*CLB*PHTOXC
5 11 41 CPSGTCS
Corticaldysplasia
R inferior occipital R inferior and convexityoccipital
R inferior occipitalcortical dysplasia
Full PHT*PB*TPM*CBZ*OXC
6 12 18 CPSGTCS
Cavernoushemangioma
R hemisphere R occipital R occipital cavernoushemangioma
Full CLB*LTG*TPM*GBP*VPA*CBZLEV
7 16 21 SFSCPS
Corticaldysplasia
L posterior temporal L anterior inferioroccipital
L occipital–temporalcortical dysplasia
R superiorquadrantopia
CBZ*PHTCLB
8 5 32 SFSCPS
Trauma,stroke
R hemisphere R occipital–parietal R hemisphericencephalomalacia
L homonymoushemianopsia
PHT*CBZ*VPA*OXC*LEVTPM
Pt, patient; SFS, simple focal seizure; CPS, complex partial seizure; GTCS, generalized tonic–clonic seizure; EEG, electroencephalography; L, left; R, right; MRI, magneticresonance imaging; AEDs, anti-epileptic drugs; CBZ, carbamazepine; CLB, clobazam; CNZ, clonazepam; GBP, gabapentin; LTG, lamotrigine; LEV, levetiracetam; OXC,oxcarbazepine; PB, phenobarbital; PHT, phenytoin; PRM, primidone; TPM, topiramate; VPA, valproic acid; *, previously prescribed but not currently used.
A. Patel et al. / Clinical Neurophysiology 119 (2008) 2437–2446 2439
analyzed it. The seizure dataset was divided into multiples of 10 sepochs for all the analyses as described below. Initial processinginvolved band-pass filtering the data between 1 and 70 Hz in orderto remove artifact contamination and other non-biological signals;this is the same filter setting that is usually used for visual inter-pretation of EEG data at our centre. Therefore, these filter settingsmade comparison of ICA to the visual analysis of the same datamore meaningful. Principal component analysis (PCA) was per-formed on the data to determine the distribution of informationwithin. The Infomax ICA algorithm (Bell and Sejnowski, 1995)was then implemented on the EEG data, which yielded a set ofindependent components representing the source signals. The ex-tended version of the Infomax algorithm was used in order to accu-rately identify and remove sub-Gaussian artifact signals from thedata, such as 60 Hz line noise (Jung et al., 1998). In each case, thenumber of ICs extracted represented 90% of the variance, as deter-mined by the PCA breakdown, within the original EEG data for thatseizure. Input of different epoch lengths into the ICA algorithm didnot yield any identifiable difference in output, and for this reason
all subsequent analyses were performed on one concatenatedepoch representing the entire seizure length.
Validity of the output from ICA was confirmed by regeneratingthe original EEG from the ICA output using a reverse mixing pro-cess. Visualization of the EEG recording as well as of the ICA com-ponents was helpful in correlating the sources to those signals seenin the EEG seizure data. Analysis of the source signals was then car-ried out; the power spectrum and frequency spectrum of each ICwas calculated via a fast Fourier transform (FFT) algorithm. Thenumber of electrodes involved by each IC at the onset of the ictalsignal as well as throughout the duration of the seizure was alsocatalogued. Manipulation of the numerical output from ICA, incombination with 3-D electrode locations from CT–MRI superim-position images generated by Atamai software (London, ON), al-lowed further localization of the IC signals as well as a depictionof their routes of propagation.
Results from all 27 seizures were categorized by the type ofevent as delineated by the ILAE (1981) classification: simple focalseizure (SFS), complex partial seizure (CPS), or generalized

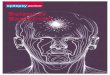
Fig. 1. Comparison of ICA to visual EEG interpretation. (A) Subdural EEG recording of a seizure in a 16-year-old female patient with diagnosed occipital epilepsy. Seizureactivity can be seen to begin at approximately 10 s in electrode 135. (B) independent component analysis (ICA) of the same seizure EEG data. Seizure activity can beappreciated in independent component (IC) 4, beginning at approximately 10 s, with similar morphology as that seen in electrode 135 on the EEG. (C) Subsequent analysis ofIC 4 confirms that this signal is primarily responsible for the seizure activity seen in electrode 135.
2440 A. Patel et al. / Clinical Neurophysiology 119 (2008) 2437–2446

A. Patel et al. / Clinical Neurophysiology 119 (2008) 2437–2446 2441
tonic–clonic seizure (GTCS). Seizures were classified based on theirculminant clinical presentation; for example, seizures that startedas SFS or CPS but later became secondarily generalized weregrouped as GTCS. ICs that moved to electrodes other than those in-volved at their onset were classified as ‘‘propagating”, whereasthose ICs that remained only at their source electrode throughoutthe duration of the seizure were classified as ‘‘non-propagating”.
3. Results
ICA of the subdural EEG recordings revealed the underlyingsource signals responsible for the seizure activity in all the 8patients studied. In addition to confirming the occipital origin ofthe seizure activity as demonstrated by standard visual EEG inter-pretation (Fig. 1), ICA was able to provide additional informationregarding the locations and propagation patterns of the source sig-nals underlying the seizure activity. Some of these ICs spread tolocations distant to their onset electrode, while others remainedstationary throughout the time course of the seizure. The numberof ICs responsible for the seizure onset varied between patients,and even within different seizures from the same patient. Thecharacteristics of the various components responsible for each sei-zure also varied greatly; their power, frequency, localization, andpropagation patterns were different from one component to thenext. Nevertheless, some trends did emerge from the data; resultsfrom all 27 seizures were categorized into 9 SFS, 11 CPS, and 7GTCS, and are described below. Surgery was offered to all the 8patients; 5 individuals declined surgical intervention because ofthe visual loss that would likely have resulted from an occipitalcortex resection, while 3 patients accepted and underwent occipi-tal lobe surgery (Table 2).
3.1. Simple focal seizures (SFS)
The group of SFS was characterized exclusively by the experi-ence of visual auras by the patients during the seizure events.The duration of these seizures ranged from 59 to 611 s(mean = 220 ± 165 s). The number of ICs responsible for the seizureonset varied from 4 to 11 per seizure (mean = 7 ± 3 signals). Over-all, there were 61 source signals identified; 44/61 (72%) of thesewere found to spread from the region of onset to other areas overthe duration of the seizure, while 17/61 (28%) did not spread andstayed confined to the region of origin throughout the seizure.There was no significant difference between the average totalpower of the propagating ICs, 56.840 arbitrary units (AU), andthe non-propagating ICs, 52.890 AU; p = 0.580. The differencebetween the average root mean square (RMS) power of the propa-gating ICs and the non-propagating ICs was not found to be signif-icant (0.814 vs. 0.809 AU; p = 0.195). There was no significant
Table 2Surgical outcomes of the patients (n = 8)
Pt Type of surgery Post-operative outcome (Engelclassification)
1 L mesial infracalcarine occipitalcortisectomy
Class IV
2 Declined –3 R infracalcarine occipital
cortisectomyClass IV
4 Declined –5 Declined –6 Declined –7 Declined –8 R occipital lobectomy Class II
Pt, patient; L, left; R, right.
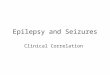
difference between the average peak frequencies of the propagat-ing ICs and the non-propagating ICs (2.705 vs. 4.647 Hz;p = 0.135). A significantly greater number of electrodes were foundto be involved at the onset for propagating ICs versus non-propa-gating ICs (1.591 vs. 1.235 electrodes; p = 0.063). The routes ofspread of the propagating ICs and location of the non-propagatingICs are illustrated on CT–MRI superimposition images (Fig. 2).
3.2. Complex partial seizures (CPS)
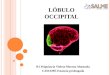
The duration of the CPS ranged from 64 to 278 s(mean = 173 ± 79 s). The number of ICs identified as being respon-sible for the onset of each seizure ranged from 2 to 11 components(mean = 6 ± 3 signals). Forty-five of the 62 (73%) ICs identifiedspread to other cortical areas, and only 17/62 (27%) did not spread.There was no significant difference between the average totalpower of the propagating ICs and the non-propagating ICs(41.044 vs. 41.249 AU; p = 0.973). The difference between the aver-age RMS power of the propagating ICs and that of the non-propa-gating ICs did not reach statistical significance (0.813 vs. 0.814 AU;p = 0.827). There was no significant difference between the peakfrequencies of ICs which propagated and non-propagating ICs(3.911 vs. 3.706 Hz; p = 0.807). A greater number of electrodeswere found to be occupied at the onset of the propagating ICs ver-sus the non-propagating ICs; this difference was statistically signif-icant (1.756 vs. 1.235 electrodes; p = 0.006). The path of spread ofthe propagating ICs and location of the non-propagating ICs are de-picted on CT–MRI illustrations (Fig. 3).
3.3. Generalized tonic–clonic seizures (GTCS)
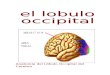
The duration of the GTCS varied from 112 to 243 s(mean = 157 ± 46 s). The number of ICs determined to be at theroot of each seizure ranged from 2 to 12 signals (mean = 7 ± 3 com-ponents). Twenty-nine of the 46 (63%) source signals spread toother areas, whereas 17/46 (37%) of the components stayed at theirarea of onset. There was no significant difference between theaverage total power for propagating ICs and non-propagating ICs(46.219 vs. 42.036 AU; p = 0.365). The difference between the aver-age RMS power of the spreading components was not found to besignificantly different from the average RMS power of the non-spreading ICs (0.820 vs. 0.816 AU; p = 0.467). There was no signif-icant difference between the peak frequency of the propagating ICsand the non-propagating ICs (8.655 vs. 6.941 Hz; p = 0.183). Thepropagating ICs did not involve a significantly different numberof electrodes at their onset versus the non-propagating ICs in theGTCS category (1.552 vs. 1.647 electrodes; p = 0.749). The courseof spread for the propagating ICs and location of the non-propagat-ing ICs are mapped out on CT–MRI superimposition images (Fig. 4).
Overall analyses of the data from all types of seizures suggestthat ICs which propagate have different characteristics than thosewhich do not propagate. All signals were analyzed with respect totheir total power, RMS power, peak frequency, and onset electrodevolumes; these results are presented below and summarized inTable 3.
3.4. Total power
In each of the SFS, CPS, and GTCS categories, there was no signif-icant difference found between the total powers of propagating ICsand the non-propagating ICs (SFS – 56.840 vs. 52.980 AU, CPS –41.044 vs. 41.249 AU, GTCS – 46.219 vs. 42.036 AU; p = 0.580,0.973, 0.365). The cumulative results from the propagating andnon-propagating ICs of all 27 seizures showed no significant differ-ence with respect to the total powers, either (48.206 vs. 45.422 AU;p = 0.429).

2442 A. Patel et al. / Clinical Neurophysiology 119 (2008) 2437–2446
3.5. RMS power
The difference between the RMS powers of propagating ICs andnon-propagating ICs in each of the seizure groups (SFS – 0.814 vs.
Fig. 2. Location of onset and routes of propagation for independent
0.809 AU, CPS – 0.813 vs. 0.814 AU, GTCS – 0.820 vs. 0.816 AU) wasnot found to be significantly different in any of these groupings(p = 0.195, 0.827, 0.467). Results from the RMS powers of propagat-ing ICs and non-propagating ICs were also analyzed regardless of
components (ICs) of simple focal seizures (SFS) for each patient.

Fig. 3. Location of onset and routes of propagation for independent components (ICs) underlying complex partial seizures (CPS) for each patient.
A. Patel et al. / Clinical Neurophysiology 119 (2008) 2437–2446 2443
the type of seizure; no statistically significant difference was found(0.815 vs. 0.813 AU; p = 0.490).
3.6. Peak frequency
In the seizure subcategories of SFS, CPS, GTCS, the peak in thefrequency spectrum for the propagating ICs was not significantlydifferent when compared to that of the non-propagating ICs (SFS– 2.705 vs. 4.647 Hz, CPS – 3.911 vs. 3.706 Hz, GTCS – 8.655 vs.6.941 Hz; p = 0.135, 0.807, 0.183). Overall analysis of the frequencypeaks regardless of seizure type did not show a significant differ-ence between propagating ICs and non-propagating ICs (4.627 vs.5.098 Hz; p = 0.490).
3.7. Onset electrode volume
The number of electrodes involved at the onset of each compo-nent was significantly greater for propagating ICs versus non-prop-agating ICs for the SFS and CPS groups (SFS – 1.591 vs. 1.235electrodes, CPS – 1.756 vs. 1.235 electrodes; p = 0.063, 0.006).
The GTCS group did not show any significant trend in this domain;the propagating ICs involved 1.552 electrodes while the non-prop-agating ICs involved 1.647 electrodes (p = 0.749). The cumulativepropagating ICs from all 27 seizures studied showed statisticallysignificantly greater electrode involvement at their onset versusnon-propagating ICs (1.644 vs. 1.373 electrodes; p = 0.041). Theseanalyses regarding the extent of electrode involvement at signalonset are illustrated in Fig. 5.
4. Discussion
Using ICA, all the subdurally recorded occipital seizures in thisstudy could be decomposed into their underlying ICs. The validityof these ICs was verified by using a reversed ICA algorithm toreproduce the original EEG from all the generated ICs. For all 8 pa-tients, ICA confirmed and improved upon the visual interpretationof the respective EEG recordings with regard to the seizure onsetzone within the occipital lobe. A novel aspect of this ICA studywas that most seizures contained propagating and non-propagat-ing ictal ICs, a concept which could help to better define the seizure

Fig. 4. Location of onset and routes of propagation for independent components (ICs) at the root of generalized tonic–clonic seizures (GTCS) for each patient.
2444 A. Patel et al. / Clinical Neurophysiology 119 (2008) 2437–2446
onset zone with closer approximation of the potential epilepto-genic zone so that more accurate prognosis for surgical outcomecan be made. Moreover, every IC displayed different propertieswith respect to signal power, frequency spectrum, onset electrodevolume, and propagation pattern.
Categorization of the 27 seizures analyzed in this study into SFS,CPS, and GTCS groups revealed several trends for propagating ver-sus non-propagating ICs throughout the duration of each seizure.No significant differences were found between propagating andnon-propagating ICs, with respect to their total power or RMSpower, in any of the three seizure groups. Although higher fre-quency signals have been reported to be responsible for seizure ini-tiation and propagation (Traub et al., 2001), such a trend was notfound in this study. The frequency spectrums of the propagating
Table 3Summary details of independent component (IC) characteristics within each seizure categ
Type of seizure Average total power (AU)
Propagating ICs Non-propagating ICs P
SFS 56.840 ± 21.993 52.980 ± 24.925 0.CPS 41.044 ± 24.398 41.249 ± 20.030 0.GTCS 46.219 ± 20.717 42.036 ± 10.165 0.All seizures 48.206 ± 23.518 45.422 ± 19.735 0.
Peak frequency (Hz)
Propagating ICs Non-propagating ICs P
SFS 2.705 ± 1.875 4.647 ± 4.987 0.CPS 3.911 ± 2.770 3.706 ± 2.974 0.GTCS 8.655 ± 4.886 6.941 ± 3.631 0.All seizures 4.627 ± 3.937 5.098 ± 4.110 0.
SFS, simple focal seizure; CPS, complex partial seizure; GTCS, secondarily generalized tocomponents.
ICs were not significantly different from the non-propagating ICsfor different seizure types and all the seizures grouped together.It would thus appear that attributes other than power or frequencyare important in determining the propagating properties of ICs in agiven seizure, regardless of the seizure type.
One characteristic that did predict the propagating capability ofan ictal IC was the volume of brain from which it was originated. Itwas found that propagating ICs arose from a greater number ofelectrodes, and thus a larger volume of the brain, than non-propa-gating ICs. This difference was statistically significant among theSFS, CPS, and all seizures when grouped together (p = 0.063,0.006, 0.041). This observation could not be confirmed amongthe GTCS (p = 0.749), likely due to a smaller sample size, i.e. 7 GTCSvs. 11 SFS and 9 CPS. Nonetheless, the data suggest that those ictal
ory
Average RMS power (AU)
value Propagating ICs Non-propagating ICs P value
580 0.814 ± 0.0186 0.809 ± 0.0132 0.195973 0.813 ± 0.0206 0.814 ± 0.0225 0.827365 0.820 ± 0.0150 0.816 ± 0.0179 0.467429 0.815 ± 0.0186 0.813 ± 0.0181 0.490
Onset volume (electrodes)
value Propagating ICs Non-propagating ICs P value
135 1.591 ± 0.844 1.235 ± 0.562 0.063807 1.756 ± 0.981 1.235 ± 0.437 0.006183 1.552 ± 0.910 1.647 ± 0.996 0.749490 1.644 ± 0.911 1.373 ± 0.720 0.041
nic–clonic seizure; AU, arbitrary units; RMS, root mean squared; ICs, independent

A. Patel et al. / Clinical Neurophysiology 119 (2008) 2437–2446 2445
ICs which are generated by larger areas of the brain are more likelyto spread to the other areas of the brain and act as better reflec-
Fig. 5. Comparison of the extent of electrode involvement at seizure onset for propagatinsignificantly greater number of electrodes were found to be occupied at the onset of ICsseizures grouped together.
Fig. 6. Outcomes for those patients who underwent surgery (n = 3). In the cases of patientthe epileptogenic zone, as determined by ICA, and for this reason their post-operative oanalysis did include the ICA-determined epileptogenic zone, and thus this patient fared
tions of the epileptogenic zones, regardless of other characteristicssuch as component power or frequency.
g independent components (ICs) versus non-propagating ICs for each seizure type. Athat propagated when compared to ICs that did not propagate, in SFS, CPS, and all
s 1 and 3, surgical resection based on standard visual EEG analysis did not include allutcome was poor (Engel IV). In the case of patient 8, resection based on visual EEGmuch better post-operatively (Engel II).

2446 A. Patel et al. / Clinical Neurophysiology 119 (2008) 2437–2446
The need for more accurate localization of the epileptogeniczone can be appreciated when considering patients who undergoresective surgery but experience minimal improvement in theirseizure outcomes (Engel classification III–IV); this was the casewith patients 1 and 3 in this study. Fig. 6 demonstrates the utilityof ICA in more accurately localizing the epileptogenic zone. In thecase of patient 3, localization of seizure activity based on standardvisual EEG interpretation led to surgical removal of the infracalcar-ine occipital cortex. However, her post-operative course was com-plicated by recurrent seizure events with no improvement insymptomology (Engel IV). ICA showed that the epileptogenic zonein her occipital region extended both above and below the calca-rine fissure. A repeat surgical intervention which removed supra-calcarine cortex resulted in an improvement in her seizureoutcome (Engel II). In the case of patient 8, the initial surgicalresection removed all the regions of cortex that were determinedto involve epileptogenesis as determined by ICA. Consequently,this patient experienced a considerable improvement in her post-operative outcome with respect to seizures (Engel II). This studytherefore shows that the application of ICA to such patients’ sei-zure data may be one method by which additional informationcan be gained about the areas of cerebral cortex required for thegeneration of clinical seizures.
The application of ICA to subdural grids and depth electrodes, aswell as higher sampling rates of the acquired EEG data, will bevaluable for future studies involving ICA and epileptogenic zones.Additional knowledge regarding the volume of neural tissue re-quired to give rise to propagating and non-propagating ICs couldhelp to establish a physiological connection between the specificneuronal populations underlying the statistical signals from ICA.As the goal of resective epileptic surgery is the complete removalof the epileptogenic region(s) of the brain with maximal preserva-tion of eloquent cortex, additional information regarding thethreshold volume of neural tissue required to produce propagatingictal ICs may allow removal of the epileptogenic zone with greateraccuracy that would achieve the best post-operative outcome.
Difficulties encountered in this study were primarily a conse-quence of the novelty of this analytic technique in subdurally re-corded seizures. Implementation of ICA is cumbersome; manydifferent algorithms exist, with each having a different set ofvariables influencing how well the analysis operates. An addi-tional source of complication in this study was the heterogeneityof the patient population, which may have suppressed some ofthe trends present in the data. Many of the patients in this studyhad different etiologies for their respective OLEs, and in particu-lar, different structural lesions in their brains that could have ledto a lack of agreement in the data analysis. For example, cortico-cortical and cortico-subcortical connections may have been al-tered in patients who experienced neurological insults early inlife, while patients with cryptogenic OLE may have had intactpathways. These differences in patient characteristics may haveprevented the emergence of consistent patterns of propagationacross groups.
This study shows that ICA is a useful supplementary tool in theanalysis of subdurally recorded occipital seizures with respect tothe determination of the epileptogenic zone and propagation pat-terns. Despite the complexity of OLE and the limited accuracy ofthe current state of visual analysis in subdural EEG display, ICAof occipital seizures resulted in clinically relevant information thatcould not otherwise be obtained. The application of this informa-tion from ICA, in combination with the diagnostic output from sub-dural EEG, may be used to improve the surgical outcome ofpatients with medically intractable epilepsy.
Acknowledgement
A.P. was funded by the Summer Research Training Program(SRTP) at the Schulich School of Medicine and Dentistry in the Uni-versity of Western Ontario.
References
Aykut-Bingol C, Bronen RA, Kim JH, Spencer DD, Spencer SS. Surgical outcome inoccipital lobe epilepsy: implications for pathophysiology. Ann Neurol1998;44:60–9.
Bell AJ, Sejnowski TJ. An information-maximization approach to blind separationand blind deconvolution. Neural Comput 1995;7:1129–59.
Blume WT, Whiting SE, Girvin JP. Epilepsy surgery in the posterior cortex. AnnNeurol 1991;29:638–45.
Blume WT, Wiebe S. Occipital lobe epilepsies. Adv Neurol 2000;84:173–87.Blume WT, Wiebe S, Tapsell LM. Occipital epilepsy: lateral versus mesial. Brain
2005;128:1209–25.Brekelmans GJF, van Emde Boas W, Velis DN, Lopes da Silva FH, van Rijen PC, van
Veelen CWM. Comparison of combined versus subdural or intracerebralelectrodes alone in presurgical focus localization. Epilepsia1998;39:1290–301.
Brown GD, Yamada S, Sejnowski TJ. Independent component analysis at the neuralcocktail party. Trends Neurosci 2001;24:54–63.
Collins RC, Caston TV. Functional anatomy of occipital lobe seizures: anexperimental study in rats. Neurology 1979;29:705–16.
Engel J, Van Ness PC, Rasmussen TB, Ojemann LM. Outcome with respect toepileptic seizures. In: Engel J, editor. Surgical treatment of the epilepsies. NewYork: Raven Press; 1993.
Gloor P. Neuronal generators and the problem of localization inelectroencephalography: application of volume conduction theory toelectroencephalography. J Clin Neurophysiol 1985;2:327–54.
Hughes JR. EEG in clinical practice. Massachusetts: Butterworth publishers; 1982.ILAE. Proposal for revised clinical and electroencephalographic classification of
epileptic seizures. From the commission on classification and terminology ofthe international league against epilepsy. Epilepsia 1981;22:489–501.
Iriarte J, Urrestarazu E, Valencia M, Alegre M, Malanda A, Viteri C, et al. Independentcomponent analysis as a tool to eliminate artifacts in EEG: a quantitative study.J Clin Neurophysiol 2003;20:249–57.
Jasper HH. The ten-twenty electrode system of the International Federation.Electroencephal Clin Neurophysiol 1958;10:371–5.
Jung T-P, Humphries C, Lee TW, Makeig S, McKeown MJ, Iragui V, et al. Extended ICAremoves artifacts from electroencephalographic recordings. Adv Neural InfProcess Syst 1998;10:894–900.
Kwan P, Brodie MJ. Early identification of refractory epilepsy. New Engl J Med2000;342:314–9.
Lee SK, Lee SY, Kim DW, Lee DS, Chung CK. Occipital lobe epilepsy: clinicalcharacteristics, surgical outcome, and role of diagnostic modalities. Epilepsia2005;46:688–95.
Lothman EW. The neurobiology of epileptiform discharges. Am J EEG Technol1993;33:93–112.
Ludwig BI, Marsan CA. Clinical ictal patterns in epileptic patients with occipitalelectroencephalographic foci. Neurology 1975;25:463–71.
Makeig S, Bell AJ, Jung TP, Sejnowski TJ. Independent component analysis ofelectroencephalographic data. Adv Neural Info Process Syst 1996;8:145–51.
Nam H, Yim TG, Han SK, Oh JB, Lee SK. Independent component analysis of ictal EEGin medial temporal lobe epilepsy. Epilepsia 2002;43:160–4.
Rosenow F, Lüders H. Presurgical evaluation of epilepsy. Brain 2001;124:1683–700.Salanova V, Andermann F, Olivier A, Rasmussen T, Quesney LF. Occipital lobe
epilepsy: electroclinical manifestations, electrocorticography, corticalstimulation, and outcome in 42 patients treated between 1930 and 1991:surgery of occipital lobe epilepsy. Brain 1992;115:1655–80.
Stone JV. Independent component analysis: an introduction. Trends Cogn Sci2002;6:59–64.
Traub RD, Whittington MA, Buhl EH, LeBeau FEN, Bibbig A, Boyd S, et al. A possiblerole for gap junctions in generation of very fast EEG oscillations preceding theonset of, and perhaps initiating, seizures. Epilepsia 2001;42:153–70.
Urrestarazu E, Iriarte J, Artieda J, Alegre M, Valencia M, Viteri C. Independentcomponent analysis separates spikes of different origin in the EEG. J ClinNeurophysiol 2006a;23:72–8.
Urrestarazu E, LeVan P, Gotman J. Independent component analysis identifies ictalbitemporal activity in intracranial recordings at the time of unilateraldischarges. J Clin Neurophysiol 2006b;117:549–61.
Weinand ME, El-Saadany WF, Labiner DM, Talwar D, Ahern G. Subdural stripelectrode monitoring and surgical decision making in refractory epilepsy:validity and prognostic value of noninvasive localizing data. J Epilepsy1995;8:131–8.
Williamson PD, Thalani VM, Darcey TM, Spencer DD, Spencer SS, Mattson RH.Occipital lobe epilepsy: clinical characteristics, seizure spread patterns, andresults of surgery. Ann Neurol 1992;31:3–13.