Embed Size (px)
Citation preview

American Journal of Medical Genetics 46:176-179 (1993)
Index Finger Hyperphalangy and Multiple Anomalies: Catel-Manzke Syndrome?
Golder N. Wilson, Teresa E. King, and Gail S. Brookshire Department of Pediatrics, University of Texas Southwestern Medical Center, Dallas
We describe a boy with short stature, develop- mental delay, unusual face, right iris colo- boma, malformed ears, micrognathia, and skeletal anomalies including hyperphalangy of the index fingers, bilateral fifth finger clinodactyly, short halluces, and scoliosis. In- ternal anomalies included asymmetric and di- lated cerebral ventricles and ventricular sep- tal defect. The neonatal history of small jaw with feeding and respiratory difficulties sug gested a Pierre Robin sequence, but there was no cleft palate. Two maternal uncles with sim- ilar anomalies had died at ages 13 months and 5 years, respectively. RFLP studies with the DNA probes DXS72 and FSC were consistent with but not diagnostic of X-linked recessive inheritance. The pattern of anomalies was compatible with a diagnosis of Catel-Manzke syndrome, but a novel dysostosis syndrome must also be considered. o 1993 Wiley-Lisa, Inc.
KEY WORDS: MCA/MR syndrome; Catel- Manzke syndrome; hyper- phalangy, Pierre Robin se- quence
INTRODUCTION The hyperphalangy producing “triphalangeal
thumb” is seen in many syndromes; however, clinodac- tyly of the index finger caused by extra phalanges is more unusual. The occurrence of index finger hyper- phalangy together with Pierre Robin sequence was rec- ognized by Catel in 1961 and then Manzke [1966] who reported on the same patient [Gorlin et al., 19903. Thir- teen males and 2 females with Catel-Manzke syndrome have now been described [Gorlin et al., 19901, and af- fected relatives have been reported in 4 families [Gewitz et al., 1978; Stevenson et al., 1980; Brude, 1984; Dignan
Received for publication July 6,1992; revision received Novem- ber 9, 1992.
Address reprint requests to Golder N. Wilson M.D., Ph.D., Divi- sion of Pediatric Genetics and Metabolism, University of Texas Southwestern Medical Center, 5323 Harry Hines, Dallas, TX 75235-9063.
0 1993 Wiley-Liss, Inc.
et al., 19861. Here we report on a boy with hyper- phalangy and micrognathia whose family history and DNA marker studies were consistent with X-linked in- heritance.
CLINICAL REPORT The propositus is a 2%-year-old boy referred because
of developmental delay and possible mucopolysac- charidosis. Birth weight was 3,200 g after a term gesta- tion to a gravida 3 para 1 18-year-old woman. She had taken Compazinem during months 2-3 of pregnancy, then switched to diphenhydramine hydrochloride for continued treatment of severe nausea. Decreased move- ment was noted in the last trimester. The nursery stay was extended to 10 days because of micrognathia with feeding and respiratory problems. A heart murmur was identified as a ventricular septa1 defect, and the patient had frequent upper respiratory infections during the first year. Motor delay was noted at 9 months, and devel- opment was approximately 50% of normal. Two mater- nal uncles were described as being very similar to the patient in their appearance and problems, but medical records could not be located. The oldest died at age 5 years and had a small jaw, “double palate,” neonatal feeding and respiratory problems, “pigeon chest,” and frequent infections. The cause of death was remembered as Bright’s disease. The youngest died at age 13 months because of a respiratory illness. He had a small jaw, but the grandmother does not remember curved index fingers in either child.
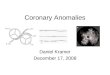
On physical examination, the propositus had a length of 85 cm (3rd centile), weight of 14.5 kg (90th centile), and an OFC of 53 cm (> 97th centile). He had arched eyebrows, small palpebral fissures (10th centile), right iris coloboma, shallow orbits, prominent nasal bridge, cupid’s bow upper lip, apparently low-placed and mal- formed ears, micrognathia, and a short neck (Fig. 1A). The index fingers were ulnarly deviated with hyper- phalangy (Fig. 1B); there was bilateral 5th finger clinodactyly and the fingers and toes appeared short and broad. The palate, genitalia, and abdominal organs were normal and there was scoliosis with a curve of about 15 degrees. The patient could not walk and said only a few words. CT scan (Fig. 1C) documented arrested hydrocephalus with asymmetric dilation of the ventri- cles. Karyotype (including fragile X testing), urine mu-

Hyperph.alangy and Multiple Anomalies 177
Fig. 1. Face (A), hand roentgenogram (B), and CT man (C) of the propositus.
copolysaccharide screen, and audiology evaluations were normal.
MATERIALS AND METHODS Transformed lymphocyte cultures were prepared from
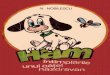
the relatives indicated in Figure 2 and DNA was extrac- ted as described (Macias et al., 1992). DNA linkage studies employed the probes DXS72 (Xq2l-Hind I11 polymorphism) and F8C (Xq28-BcZ I polymorphism). Southern analysis and probe labeling were as described (Macias et al., 1992).
RESULTS AND DISCUSSION RFLP studies with the markers DXS72 and F8C are
shown in Figure 2. The DXS72 polymorphic alleles de- tected in the propositus, his normal brother, the mother, her normal brother, and the maternal grandmother are those expected if the propositus and his maternal uncles have the same disorder determined by a gene on the X chromosome. The F8C alleles were not informative. The limited family size does not support a more detailed linkage study, but segregation with an Xq21 locus sug-

178 Wilson et al.
1
DXS 72
TABLE I. Manifestations of the F’ropositus and Reported Patients with Catel-Manzke Syndrome*
Literature Propositus General + - Male sex 13/15
Prenatal growth delay 2/10 Developmental delay 3/11 + Postnatal growth delay 8/12 + Unusual head shape 2/15 + Shallow orbits 2/15 + Malformed ears 5/15 + Clefthigh palate 13/14 + Micrognathia 13/14 + Short neck 4/10 + Hyperphalangy 2nd digit 15/15 -k Clinodactyly digits 5 5/15 + Single palmar creases 6/15 - Short fingerdtoes 418 + Talipes equinovarus 2/15 -
Vertebrallrib anomalies 2/15 + Pectus excavatum 3/15 - Joint laxity/dislocation 3/15 + Cardiac defects 6/15 +
Craniofacial
9
Limbs
Other
*Data from index cases of Manzke [19661, Famworth and Pacik [1971], Holthusen [19721, Gorlin et al. 119751, Silengo 119771, Gewitz et al. [1978], Stevenson et al. [19801, Sundaram et al. U9821, Klug et al. [1983], Brude [19841, Dignan et al. [19861, Thompson [I9861 and Skin-
2 ner et al. [19891.
F8C
1
2
Fig. 2. Abbreviated pedigree and Southern blots employing X chro- mosome markers DXS72 (allele 1 = 7.2 kb, allele 2 = 0.7 kb) and F8C (allele 1 = 1.2 kb, allele 2 = 0.88 kb).
gests this region as a target for the future. Against the hypothesis of X-linkage are the propositae of Klug et al. [1983] and of Dignan et al. 119863; the latter patient had an affected sister. The more extensive family of Steven- son et al. [1980] includes a case of male to male trans- mission if their historical diagnoses were correct. Gorlin et al. [19901 argue against X-linkage of Catel-Manzke syndrome, and there is probably heterogeneity unless non-random lyonization or X-linked dominant inheri- tance is invoked for affected females. Neither the mother of the propositus, the maternal grandmother, nor the mother’s sister had skeletal manifestations or past med- ical histories which were suggestive of partial expres- sion.
In Table I, manifestations of the propositus are com- pared to those of 15 propositi with Catel-Manzke syn- drome [Gorlin et al., 19901. Parental ages for these index
cases averaged 28.0 years for mothers (7 cases) and 26.3 years for fathers (6 cases). Growth delay, “globular” head shape, “prominent eyes” due to shallow orbits, mal- formed ears, palatal anomaly, micrognathia, short neck, 2nd digit hyperphalangy and 5th finger clinodactyly are among the abnormalities shared by literature cases and the propositus. His facial appearance is also quite simi- lar to that of the patient reported by Gorlin et al. 119751. The propositus and 6 literature cases have had cardiac septa1 defects that were accompanied by over-riding aorta, aortic coarctation, and dextrocardia in 3 cases. A stillborn sister of the proposita of Dignan et al. 119863 had transposition of the great vessels. Skeletal mani- festations of the syndrome include joint laxity (3 cases including 1 with severe knee dislocation), talipes equi- novarus (2 cases), pectus carinatum or excavatum (2 cases), and vertebral anomalies (2 cases plus scoliosis in the propositus). Miscellaneous anomalies have included cryptorchidism, bilateral inguinal hernias, and vitiligo [Skinner et al., 19891, umbilical hernia [Gorlin, 19751, facial paresis [Manzke, 19661, and digital camptodac- tyly [Stevenson, 1980; Skinner et al., 19891.
Catel-Manzke syndrome has been lethal in at least 3 cases besides the potentially affected maternal uncles of the propositus. Two sibs were stillborn [Gewitz et al., 1978; Dignan et al., 19861 and another died of respira- tory distress and aspiration at age 3 months [Brude, 19841. These 3 sibs and the 3-generation pedigree of Stevenson et al. [19801 with 3 potentially affected rela- tives provide strong evidence for a genetic cause of Catel-Manzke syndrome. The presumptive gene(s) may be quite interesting since Stevenson [19911 has proposed

Hyperphalangy and Multiple Anomalies 179
Gewitz M, Dinwiddie T, Yuille T, Hill E, Carter CO (1978): Cleft palate and accessory metacarpal of index finger syndrome: Possible famil- ial occurrence. J Med Genet 15:162-164.
Gorlin FLJ, Cervenka J, Moller K, Horrobin M, Witkop CJ J r (1975): A Selected Miscellany. In Bergsma D (ed): “Malformation Syn- dromes.” New York Alan R. Liss, Inc., for the National Foundation, March of Dimes, BDOAS XI(2):39-50.
Gorlin FLJ, Cohen MM Jr, Levin LS (1990): “Syndromes ofthe Head and Neck.” (3rd ed.) New York: Oxford University Press, pp 746-747.
Klug MS, Ketchum LD, Lipsey J H (1983): Symmetric hyperphalang- ism of the index finger in the palatodigital syndrome: A case report. J Hand Surg 8:599-603.
Lewis EB (1992): Clusters of master control genes regulate the develop- ment of higher organisms. JAMA 267:1524-1531.
Macias VR, Day DW, King TE, Wilson GN (1992): Clasped-thumb mental retardation (MASA) syndrome: Confirmation of linkage to Xq28. Am J Med Genet 43:408-414.
Manzke VH (1966): Symmetrische Hyperphalangie des zweiten Fingers durch ein akzessorisches Metacarpale. Fortschr Rontgenstr 105:425-52’7.
Skinner SA, Flannery DB, Stevenson RE (1989): Catel-Manzke syn- drome. Roc Greenwood Genet Center 860-63.
Stevenson RE (1991): Commentary at David W. Smith Workshop. Stevenson RE, Taylor HA Jr, Burton OM, Hearn HB 111 (1980): A
digitopalatal syndrome with associated anomalies of the heart, face, and skeleton. J Med Genet 17:238-242.
Sundaram V, Taysi K, Hartmann AF Jr, Shackelford GD, Keating J P (1982): Hyperphalangy and clinodactyly of the index finger with Pierre Robin anomaly: Catel-Manzke syndrome. A case report and review of the literature. Clin Genet 21:407-410.
Thompson EM, Winter RM, Williams MJH (1986): A male infant with Catel-Manzhe syndrome and dislocatable knees. J Med Genet 23:271-274
hyperphalangy as a segmentation anomaly worthy of consideration as a homeotic mutation. This perspective is supported by the expression of homeotic genes in limb buds and the similarity of triphalangeal thumb to the antero-posterior segment transformations which occur in Drosophila [Lewis, 19921. Teratogenic factors should also be considered since first trimester exposures to Syn- throid@ [Skinner et al., 19891, Amitriptyline hydro- chloride [Stevenson et al., 19801, and Compazine” (pro- positus) have been documented in affected pregnancies. In addition, Thompson et al. [19861 suggest that an affected child of a hyperphenylalaninemic mother had coincidental Catel-Manzke syndrome rather than ter- atogenic effects of phenylalanine.
ACKNOWLEDGMENTS We appreciate Dr. Robert J. Gorlin’s mention of hyper-
phalangy in Catel-Manzke syndrome after reviewing this case. Portions of the work were supported by a grant to G.N.W. from the Biological Humanics Foundation, Dallas, TX.
REFERENCES Brude E (1984): Pierre Robin sequence and hyperphalangy: A genetic
entity. Eur J Pediatr 142:222-223. Dignan PStJ, Martin LW, Zenni EJ Jr (1986): Pierre Robin anomaly
with an accessory metacarpal of the index fingers. Clin Genet 29:168-173.
Farnsworth PB, Pacik F” (1971): Glossoptotic hypoxia and micro- gnathia: The Pierre Robin syndrome reviewed. Clin Pediatr 10600-606.