Embed Size (px)
Citation preview

Indian Health Care
April 1986
NTIS order #PB86-206091

Recommended Citation:U.S. Congress, Office of Technology Assessment, Indian Health Care, OTA-H-290 (Wash-ington, DC: U.S. Government Printing Office, April 1986).
Library of Congress Catalog Card Number 86-600526
For sale by the Superintendent of DocumentsU.S. Government Printing Office, Washington, DC 20402

Foreword
American Indians and Alaska Natives have a unique historical and legal relation-ship with the Federal Government. Through treaties and statutes, the Federal Govern-ment acts as a trustee for Indian tribes. In this “government-to-government” relation-ship, Federal programs for Indians are administered principally by the Bureau of IndianAffairs in the Department of the Interior, except for medical and health-related serv-ices, which are provided through the Indian Health Service, a component of the PublicHealth Service in the Department of Health and Human Services.
The health of Indian people still lags behind the health status of the general U.S.population, and there are substantial differences in health status and causes of illnessamong the nearly 300 Indian tribes and more than 200 Alaska Native villages in theUnited States. Continuing concerns over the health of Indian people led the House Energyand Commerce Committee and its Subcommittee on Health and the Environment torequest that OTA examine the health status of Indians and the services and technol-ogies that are provided to them through Federal Indian health programs, The requestwas also supported by the Senate Select Committee on Indian Affairs and by the Chair-man and Vice-Chairman of OTA’s Congressional Board, one of whom was also actingin his capacity as Chairman of the House Committee on Interior and Insular Affairs.
An advisory panel, chaired by Rashi Fein, Professor of the Economics of Medi-cine, Harvard Medical School, provided guidance and assistance during the assessment.Also, four public meetings were held (in Portland, Oregon; Phoenix, Arizona; RapidCity, South Dakota; and Tulsa, Oklahoma) to provide tribes and their representativesthe opportunity to comment on assessment activities and to confirm the informationthat OTA had collected. Site visits to nearby reservations and health facilities were alsoconducted as part of these activities. A large number of individuals from Indian tribesand organizations, the Federal Government, academia, the private sector, and the pub-lic provided information and reviewed drafts of the report.
OTA gratefully acknowledges the contribution of each of these individuals, As withall OTA reports, the content of the assessment is the sole responsibility of OTA anddoes not necessarily constitute the consensus or endorsement of the advisory panel orthe Technology Assessment Board. Key staff responsible for the assessment wereLawrence Miike, Ellen M. Smith, Denise Dougherty, Ramona M. Montoya, and BradLarson.
?rd~AM “.
JOHN H. GIBBONSDirector
.,.///

Indian Health Care Advisory Panel
Rashi Fein, ChairDepartment of Social Medicine and Health Policy, Harvard Medical School
James A. CrouchBureau of Rural Health ServicesUtah Department of Health
Ada DeerSchool of Social Work and Office of Native
American ProgramsUniversity of Wisconsin, Madison
Ronald G. FaichDemographerThe Navajo TribeWindow Rock, AZ
Joel FrankUnited South and Eastern Tribes, Inc.Seminole TribeHollywood, FL
Forrest J. GerardWashington, DC
Ray GoettingNew Laguna, NM
Mario GutierrezCalifornia Rural Indian Health BoardSacramento, CA
Gerald HillVA Medical CenterSan Francisco, CA
Violet HillaireBellingham, WA
Joe Jacobs’Bureau of Health Care Delivery and
AssistancePublic Health ServiceU.S. Department of Health and Human
Services
Emery JohnsonRockville, MD
Patricia KingGeorgetown Law CenterWashington, DC
Irving LewisDepartment of Epidemiology and
Social MedicineAlbert Einstein College of Medicine
Ethel LundSoutheast Alaska Regional Health Corp.Juneau, AK
Clark MarquartIndian Health Management, Inc.Rosebud, SD
Robert OseasohnSchool of Public HealthUniversity of Texas, San Antonio
Norine SmithIndian Health Board, Inc.Minneapolis, MN
Father Ted ZuernBureau of Catholic Indian MissionsWashington, DC
‘Panel member until August 1985
NOTE: OTA appreciates and is grateful for the valuable assistance and thoughtful critiques provided by the advisory panelmembers. The panel does not, however, necessarily approve, disapprove, or endorse this report. OTA assumes fullresponsibility for the report and the accuracy of its contents.
iv

OTA Project Staff—Indian Health Care
Roger C. Herdman, Assistant Director, OTAHealth and Life Sciences Division
Clyde J. Behney, Health Program Manager
Lawrence Miike, Project Director
Ellen M. Smith, Analyst
Denise M. Dougherty, Analyst
Ramona M. Montoya, Research Analyst
Brad Larson, Research Assistant
Other Contributing Staff
Becky Berka, Research Assistant
Anne Guthrie, Research Analyst
Kerry Britten Kemp, Division Editor
Pamela J. Simerly, Research Assistant
Virginia Cwalina, Administrative Assistant
Carol A. Guntow, Secretary/Word Processor Specialist
Diann G. Hohenthaner, P.C. Specialist
Contractors
National Indian Health Board, Denver, CO
Steven Bjorge, Washington, DC
Paul Alexander, Alexander & Karshmer, Washington, DC
Henry Cole, S. Ken Yamashita, The Futures Group, Washington, DC

Contents
Chapter Page
l. Summary and Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
2. The Federal-Indian Relationship. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
3. Overview of the Current Indian Population . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
4. Health Status of American Indians . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
5. The Indian Health Service. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ......155
6. Selected Issues In Indian Health Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .......213
Appendix
A. American Indian and Alaska Native Population Estimates of the U.S. CensusBureau, Indian Health Service, Bureau of Indian Affairs, and Tribes . . . . . . .. ....259
B. Indian Health Status Data—Age-Specific and Age-Adjusted Death Rates andRatios to U.S. All Races Age-Adjusted Death Rates, by Leading Causes, BothSexes and Male/Female, All IHS Areas Combined and by Area, 1980-82........273
C. IHS Allocations by Area and Budget Category, With Service Population andUtilization Data, Fiscal Years 1972-85 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...345
D. Acknowledgments and Health Program Advisory Committee . .................350
E. Method of the Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...352
F. List of Acronyms and Glossary of Terms.... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ..360
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ....367

Chapter 1
Summary and Conclusions

—
Contents
PageIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3The Indian Population.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Eligibility for Federal Indian Health Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6The Federal-Indian Relationship . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Delivery of Health Services to Eligible Indians . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Federal Expenditures for Indian Health Care. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Health Status of Indians . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Major Issues in Federal Indian Health Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Eligibility and Entitlement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .....;.. 24Resource Allocation and Scope of Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Availability and Adequacy of Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Self-Determination and Tribal Assumption of Federal Indian Health Services . 33
Other Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Indian Demographics and Urban Indian Health Programs. . . . . . . . . . . . . . . . . . 36Congressional Control of Federal Indian Health Care Policies. . . . . . . . . . . . . . . 38Indian Health Service Management Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
List of TablesTable No. Pagel-1. Leading Causes of American Indian Deaths and Age-Adjusted Death Rates
for All IHS Areas (excluding California) (1980-82), Compared toAge-AdjustedDeathRates for U.S. All Races (1981). . . . . . . . . . . . . . . . . . . . . . . . . 21
l-2. Major Issues and Related Options. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Figure1-1.
1-2.1-3.1-4.1-5.1-6.1-7.1-8.1-9.
1-1o.1-11.
List of FiguresNo. PageFederally Recognized Indian Reservations and Alaska Native RegionalCorporations, 1985. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5IHS Estimated Service Population, Fiscal Years 1972-85 . . . . . . . . . . . . . . . . . 6Indian Health Service Population by Area . . . . . . . . . . . . . . . . . . . . . . . . . . ., 7Organization of the U.S. Department of Health and Human Services. . . . . 13IHS Allocations by Major Budget Category, Fiscal Year 1985... . . . . . . . . . 14Indian Health Service. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Indian Health Facilities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15IHS Total Allocations, Fiscal Years 1972-$5 . . . . . . . . . . . . . . . . . . . . . . . . . . . 18IHS Allocations Per Potential Beneficiary, 1972-85 . . . . . . . . . . . . . . . . . . . . . 18All Areas Crude Mortality Rates, All Causes, 1972-85 . . . . . . . . . . . . . . . . . . 20Age-Adjusted Death Rates: American Indians, 1980-8212 IHS Areas:Both Sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20

Chapter 1
Summary and Conclusions
INTRODUCTION
This report is an assessment of health care forAmerican Indians and Alaska Natives who areeligible for medical and health-related servicesfrom the Federal Government. The Federal agencythat is responsible for providing these services isthe Indian Health Service (IHS), a component ofthe Public Health Service (PHS) in the Depart-ment of Health and Human Services (DHHS).
The basic population that is eligible for serv-ices from IHS consists of “persons of Indian de-scent belonging to the Indian community servedby the local facilities and program. ” An individ-ual is eligible for IHS care “if he is regarded asan Indian by the community in which he lives asevidenced by such factors as tribal membership,enrollment, residence on tax-exempt land, owner-ship of restricted property, active participationin tribal affairs, or other relevant factors in keep-ing with general Bureau of Indian Affairs prac-tice in the jurisdiction” (42 CFR 36.12). EligibleIndians are not subject to an economic means testand may receive IHS services regardless of theirability to pay.
IHS estimates its service population by enumer-ating American Indians, Eskimos, and Aleuts liv-ing within the geographic boundaries of its serv-ice areas based on the most recent census, andadjusting those estimates for subsequent years byapplying birth and death statistics. Generally, IHSservice areas consist of counties that have the res-ervation of a federally recognized tribe within orcontiguous to their borders (exceptions to this gen-eral rule include designating the States of Alaska,Nevada, and Oklahoma as IHS service areas).(There are tribes that are State-recognized only,and other tribes that are not recognized by eitherFederal or State governments. ) Thus, even thougheligibility is not limited to Indians who are mem-bers of federally recognized tribes, in practice,Federal Indian health services are directed at In-dians because of their membership in (or affilia-tion with) tribes that are recognized by the Fed-
eral Government, and not because of the racialbackground of individual recipients.
This report was prepared at the request of theHouse Committee on Energy and Commerce andits Subcommittee on Health and the Environment,which have legislative and oversight jurisdictionover all Federal health programs funded throughgeneral revenues. The request was supported bythe Senate Select Committee on Indian Affairs andby the Chairman of the House Committee on In-terior and Insular Affairs, the committee with pri-mary jurisdiction over Indian affairs in the Houseof Representatives.
The principal issues identified by the request-ing committee were the health status of AmericanIndians and Alaska Natives (hereinafter collec-tively called “Indians”), the services provided toIndians in view of their health needs, the healthdelivery systems in which these services are pro-vided, and the growing problem of paying forhigh-cost care that cannot be provided in IHS fa-cilities and that must be purchased from otherproviders of medical care,
The rest of this chapter summarizes OTA’s find-ings and conclusions and provides options on ma-jor issues identified in this report.
Chapter 2 provides an overview of Federal-Indian relationships.
Chapter 3 provides information on the Indianpopulation.
Chapter 4 traces the changing health problemsof Indians, the current status of their health, re-gional differences in health status, and healthproblems of particular concern among Indians.
Chapter 5 describes the sources of Indian healthcare, with emphasis on the direct and contractcare programs conducted by IHS, and the IHS fa-cilities construction program.
3

4 • Indian Health Care—
Chapter 6 discusses in further detail some ofthe major issues identified in the previous chap-ters, including the effects of self-determination leg-islation on transfer of health services managementfrom IHS to tribal governments; efforts to achieve
THE INDIAN POPULATION
Information on the Indian population comesfrom three sources, the U.S. Bureau of the Census,the Bureau of Indian Affairs (BIA), and IHS. In1980, the census allowed individuals to choose theracial group with which they most identified, in-stead of relying on the observations of the censustakers as in the past. The census also distinguishedbetween Indians living inside “identified areas”and Indians living elsewhere. “Identified areas”are defined as reservations, tribal trust lands,Alaska Native villages, and historic areas of Okla-homa that consist of former reservations havinglegally established boundaries between 1900 and1907, excluding urban areas. BIA uses whateverinformation may be available for a reservationto estimate its service population and labor forceparticipation, primarily for the purpose of pro-viding information on employment and earningson Indian reservations. IHS bases its service pop-ulation estimates on data from the U.S. Census.
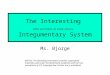
In 1980, the census identified 278 reservationsand 209 Alaska Native villages (figure 1-1), andcounted 1.4 million Indians, Eskimos, and Aleutsliving throughout the United States both on andoff reservations. The degree of Indian blood inthese self-identified Indians is not known. Manytribes have a tribal-specific blood quantum re-quirement (e.g., one-quarter) for membership;some tribes have a simple descendancy require-ment. The last relatively comprehensive surveyon “blood quantum” was reported by BIA for1950, when approximately 60.2 percent of all res-ervation Indians were full-blood, 26.7 percentwere half-blood, 9.5 percent were one-quarter,and 3.6 percent had less than one-quarter Indianblood quantum. IHS has no blood quantum re-quirement for its services, and any Indian whois considered an Indian by the Indian communityserved by the local IHS facility is eligible for IHSservices.
greater equity in the allocation of funds amongIHS service areas; the problem of high-cost casesin IHS’s contract care program; and data man-agement and use in IHS.
In 1980, 22 percent of the Indian populationlived in central cities, 32 percent lived in urbanareas outside central cities, and the remainderlived in nonmetropolitan areas. Thirty-seven per-cent actually lived inside identified Indian areasas defined by the census. The number of Indiansliving on reservations as enumerated in the 1980census ranged from 104,978 on the Navajo reser-vation to O on 21 reservations (these most likelywere small parcels of land, with tribal membersliving on nearby lands). Ten reservations ac-counted for 49 percent of all reservation residents.Four States had Indian populations in excess of100,000: California, Oklahoma, Arizona, andNew Mexico. The 10 Standard Metropolitan Sta-tistical Areas (SMSAs) with the largest numbersof Indians were, in descending order, Los Angeles-Long Beach, Tulsa, Oklahoma City, Phoenix, Al-buquerque, San Francisco-Oakland, Riverside-San Bernardino-Ontario, Seattle-Everett, Min-neapolis-St. Paul, and Tucson. (In the summaryof social and economic characteristics presentedbelow, it should be noted that national statisticson Indians are averages derived from wide re-gional variations. )
In 1979, the median income for families of allraces was $19,917, compared with median in-comes of $13,678 for American Indian, $13,829for Eskimo, and $20,313 for Aleut families. In1980, 27.5 percent of American Indians had in-comes that were below the poverty level, com-pared with 12.4 percent of the total U.S. popula-tion. Only Black persons had a higher percentage,with 29.9 percent having incomes below the pov-erty level. In 1980, 14 percent of all families inthe U.S. were headed by women, compared with23 percent of Indian families. The unemploymentrate for Indians was more than twice that of thetotal population.

mcoa)al
>.-Zzca.-QcIAI
Ch. 1—
Sum
mary and C
onclusions
(+’A.A
1-.=----+5”
“
/’ ●
Figure 1-1_ - Federally Recognized n ian Reservations and Alaska Regional Corporations, 985
" "' o~ ~c;:Jc:?QP.c:::.-.
SOURCE: Native American Science Education Association. 1986
• CJ'I

6 ● Indian Health Care
The median age for Indians in the 1980 Censuswas 22.9 years, compared with 30.0 years of agefor the general U.S. population. In 1980, 50 per-cent of the total population 25 years and olderhad completed 4 years of high school and somecollege, compared with 47 percent of Aleuts, 39percent of Eskimos, and 48 percent of American
Indians. The figures for persons over 25 years oldwho had completed 4 or more years of college,however, were quite different: 16 percent of thetotal population had completed at least 4 yearsof college, compared with 12 percent for Aleuts,5 percent for Eskimos, and 8 percent for Amer-ican Indians.
ELIGIBILITY FOR FEDERAL INDIAN HEALTH CARE
Although IHS services are not limited to reser-vation-based Indians, IHS clinical facilities havegenerally been placed on or near reservations, andmost IHS funds are appropriated for eligible In-dians who live on or near a reservation. One ofthe reasons that eligibility is not explicitly limitedto members of federally recognized tribes is thevariation across tribes in requirements for tribalmembership. Tribal rolls may be reopened onlyinfrequently, which would make it difficult forIndians not on the rolls to prove their eligibilityfor IHS services if tribal membership were the solecriterion. Another reason lies in the history ofreversals in Federal Indian policies, their effectson individual tribes and Indians, and the inequi-ties that would result if only members of tribesthat are presently federally recognized were eligi-ble for IHS services. Congress has therefore cho-sen not to restrict services to members of feder-ally recognized tribes.
In 1980, approximately 850,000 of the 1.4 mil-lion self-identified Indians in the census countresided in IHS areas. Figure 1-2 illustrates growthof the estimated IHS service population from 1972to 1985, and figure 1-3 presents the estimated 1986IHS service population of 987,017 in the 32 res-ervation States, grouped according to the 12 areaoffices of IHS. “Reservation States” are States con-taining the reservations of federally recognizedtribes and in which IHS services are provided.
Many tribes maintain rolls of their membersand dispute the IHS population estimates, whichare derived from census data. Besides the possi-bility of undercounting Indians in the census,many tribes count individuals as members with-out regard to their place of residence. Tribal rollsmay list full-fledged members and others who maybe enrolled but do not have the full privileges of
Figure 1-2.—IHS Estimated Service Population,Fiscal Years 1972-85
1r0.95
0.9 /’0.85
0.8
0.75
0.7
0.65
0.6
0.55
0.5 1 I I1972 1974 1976 1978 1980 1982 1984
Fiscal year
SOURCE U S Department of Health and Human Services, Indian Health Serv.Ice, Population Statistics Staff
members, such as voting rights or the right toshare in tribal benefits.
In order to augment the health services avail-able from IHS facilities, IHS purchases care fromnon-IHS providers through a contract care pro-gram. Currently, approximately 26 percent of theIHS clinical services budget is spent on servicesfrom non-IHS providers. Eligibility for contractcare is more restrictive than for IHS direct serv-ices. To be eligible for contract care, in additionto meeting the criteria for eligibility for IHS di-rect services, an individual must: 1) reside on areservation located within a contract health serv-ice delivery area (CHSDA) as designated by IHS;or 2) reside within a CHSDA and either be amember of the tribe or tribes located on that res-ervation or of the tribe or tribes for which the res-ervation was established, or maintain close eco-nomic and social ties with that tribe or tribes; or3) be an eligible student, transient, or Indian fos-ter child (42 CFR 36.23).

Ch. 1—Summary and Conclusions ● 7.— —-
Figure l-3.— Indian Health Service Population by AreaTotal Service Population, Fiscal Year 1986 Estimate: 987,017
California753306
SOURCE U S Department of Health and Human Services, Publ!c Health Service, Health Resources and Serwces Admlnlstratlon, Indian Health Service, PopulationStatlstlcs Staff
In most areas, the CHSDA consists of thecounty that includes all or part of a reservation,plus any county or counties that have a commonboundary with the reservation. Although Indianseligible for IHS direct services can live anywhere,only those Indians actually living in a designatedCHSDA are eligible for non-IHS care throughIHS’s contract care program. (It should be notedthat part of the growth in the eligible populationsummarized in figure 1-2 is the result of addingnew CHSDAs through legislated exceptions to thegeneral rule summarized above. )
IHS administers a small contract program forurban Indian health organizations, which gener-ally use IHS funds as core funds to attract andapply for funds from other public and private
sources directed at minority and economically dis-advantaged groups. Because of the use of theseother sources, urban Indian health programs usu-ally serve others besides their Indian clientele.Most urban programs provide a modest amountof direct clinical services, with their main empha-sis being to help clients gain access to other avail-able health and social services. The statutorydefinition of “Indians” to whom these urban pro-grams are directed is much more liberal than thedefinition for eligibility for IHS direct services:“urban Indians, ” for example, also include mem-bers of a tribe, band, or other organized groupterminated since 1940 and those recognized nowand in the future by the State in which they re-side (42 CFR 36.302 [h, u]).

8 • Indian Health Care
THE FEDERAL-INDIAN RELATIONSHIP
The fundamental relationship between Indiantribes and the U.S. Government was set forth inthe 1830s by the U.S. Supreme Court under ChiefJustice John Marshall. Indian tribes were describedas “domestic dependent nations, ” and their rela-tionship with the United States characterized asone that “resembles that of a ward to his guard-ian” (21,220). This view of the relationship origi-nated not from any one treaty or statute, but fromthe Supreme Court’s analysis of the relationshipof the tribes with the United States. It relied ona meshing of treaties, statutes, constitutional pro-visions, and international law and theory. The po-litical responsibility for dealing with Indian tribeswas constitutionally assigned to the Federal Gov-ernment, and the States were held to have no rolein Indian affairs. The Federal Government’sresponsibility is commonly known as its “trustresponsibility” for Indians.
The newly formed United States originallybased much of its relationship with Indians tribeson treaties, which are the exclusive responsibil-ity of the U.S. Senate. Since 1871, however, theUnited States has dealt with tribes by statuterather than by treaty, because the U.S. House ofRepresentatives also wanted to be involved in ne-gotiating agreements with Indian tribes.
In the 1880s, a number of statutes were passedto “civilize” Indians (the classic is the Dawes Act[24 Stats. 388 (1887)]). In this “allotment period,”each adult Indian on a reservation was assigneda specific amount of land (usually 160 acres), andsome relatively small amount of land was set asidefor tribal purposes (schools, cemeteries, and thelike). The remaining Indian lands were opened tonon-Indian settlement. Indian lands were to beheld in trust, as were the proceeds from the saleof “excess” lands, for a limited number of years.The theory was that during this trust period, in-dividual Indians would become farmers and leavetheir Indian ways. They were to be emancipatedfrom their tribes and become eligible for U.S.citizenship (Indians subsequently became U.S.citizens through the Citizenship Act of 1924 [8U.S. C. 1401(b)]). It was during the allotmentperiod that BIA became the dominant institutionalforce on Indian reservations (54).
The Indian Reorganization Act of 1934 (25U.S.C. 461, et seq. ) ended allotment, extended thetrust indefinitely, allowed tribes to form federallyrecognized tribal governments, and establishedeconomic development programs for tribes. Fol-lowing World War II, however, Federal Indianpolicy was again reversed. During this period,thousands of reservation Indians were forced toresettle in urban centers where they were to betrained and employed; major functions, respon-sibilities and jurisdiction over Indians were trans-ferred from the Federal Government to the States(18 U.S.C. 1162; 28 U.S.C. 1360); and the Fed-eral relationship with specific tribes was termi-nated, including ending services and distributingtribal assets to individual tribal members.
This “termination period” was replaced by thecurrent phase in Federal-Indian relationships,commonly known as Indian self-determination,following the Indian Self-Determination and Edu-cation and Assistance Act of 1975 (Public Law 93-638; 25 U.S. C. 450, et seq.). The 1975 law pro-vided for the transfer to tribes of functions thathad been previously performed for them by theFederal Government, including the provision ofhealth services (once assumed, tribes have the op-tion of returning these responsibilities to the Fed-eral Government). Furthermore, based on the In-dian Reorganization Act of 1934 and subsequentjudicial determinations, there is a preference forIndians for employment in IHS and BIA (42 CFR36.41-36.43; 25 CFR 5.1-5.3).
Services, including social and health services,were provided to Indian tribes from the very be-ginning of the United States as an independent na-tion. Congress routinely appropriated funds forthese purposes, though there was no specific stat-utory authority to do so until 1921. In that year,the Snyder Act (25 U.S. C. 13) was passed to avoida procedural objection to continuing to fund In-dian service programs without an authorizing stat-ute. The Snyder Act remains the basis for mostof the Indian health services provided by the Fed-eral Government. The pertinent language in re-gard to health care was simply “such moneys asCongress may from time to time appropriate, forbenefit, care, and assistance of the Indians through-

-.Ch. 1—Summary and Conclusions ● 9
—
%.
Photo credit: National Archives
Indian Health Service TB Sanitarium ward, circa 1900-1925.
out the United States . . . for the relief of distressand conservation of health . . . and for the em-ployment of . . . physicians” (25 U.S.C. 13).
While Congress has consistently provided fundsfor Indian service programs, the courts so far haveruled that these benefits are voluntarily providedby Congress and not mandated under the FederalGovernment’s trust responsibility for Indiantribes. Appropriated funds are “public moneys”and not treaty or tribal funds “belonging reallyto the Indians” (106). The trust responsibility forIndians does not in itself constitute a legal entitle-ment to Federal benefits. In the absence of atreaty, statute, executive order, or agreement thatprovides for such benefits, the trust responsibil-ity cannot be the basis for a claim against the Fed-eral Government (37, 79).
However, courts have relied on the trustresponsibility to liberally construe treaties and
statutes in favor of Indians (13). Moreover, theU.S. Supreme Court has ruled that special Indianprograms are not racial in nature but based ona unique political relationship between Indiantribes and the Federal Government (88).
The Federal Government’s obligation to dealfairly with Indian tribes when Snyder Act bene-fits are involved was addressed in 1974 in Mor-ton v. Ruiz (89), which determined that reason-able classifications and eligibility requirementscould be created in order to allocate limited funds.In Morton v. Ruiz, the Supreme Court found thatBIA had not complied with its own internal pro-cedures, nor had it published its general assistanceeligibility criteria in keeping with the rulemakingrequirements of the Administrative Procedure Act(5 U.S.C. 706). BIA had recognized the necessityof formally publishing its substantive policies andhad placed itself under the act’s procedures,

10 • Indian Health Care
The Administrative Procedure Act also containsthe standard used by the courts to review Fed-eral agency decisions and policies. Under the act,a Federal agency’s action is presumed to be validand must be confirmed if challenged in court aslong as it is not “arbitrary, capricious, or other-wise not in accordance with law” (5 U.S. C. 706[2][A]). An action is valid if all the relevant fac-tors were considered in its development and if anydiscernible rational basis existed for the agency’saction (22).
Courts will not address a larger issue if a morecircumscribed ruling is possible, however, so theconstitutional implications of Morton v. Ruizhave never been fully litigated. Because the Su-preme Court found that BIA had placed itself un-der the Administrative Procedure Act but had notfollowed the act’s procedures, the court did notaddress the issue of whether a stricter standardshould be applied.
Another standard for judicial review of agency
rulemaking is applicable to constitutional claimsunder the equal protection clause of the 14thamendment (25). There are two standards that arebased on the equal protection clause. One is a “ra-tional basis” test that is similar to, but not a sub-stitute for, the standard under the AdministrativeProcedure Act. A second, stricter constitutionaltest is applied when suspect classifications are in-volved, for example, ancestry (96); race (81);alienage (41); or fundamental constitutional rights,such as right of interstate travel (108), right to vote(14), or right of privacy with respect to abortion(105).
In the 1980 decision of Rincon Band MissionIndians v. Califano (104), a band of CaliforniaIndians sued for their fair share of IHS resources,claiming that their constitutional rights to equalprotection had been violated and that the SnyderAct was part of the Federal trust responsibility.The district court found that the plaintiffs’ equalprotection rights to due process under the fifthamendment had been violated. On appeal, theNinth Circuit did not find it necessary to addressthe constitutional argument, because it found thatIHS had breached its statutory responsibilities un-der the Snyder Act. The Ninth Circuit also didnot address the trust question because it was notnecessary to do so in reaching its decision. Thus,
IHS must at least meet the requirements of theAdministrative Procedure Act in administeringhealth services to Indians. Since the court deter-mined that IHS had not met the act’s standard,whether a constitutional standard is required hasnever been fully litigated.
In addition to the Federal Government’s respon-sibilities for and benefits conferred to Indiantribes, there are a number of Federal programsdirected at Indians as individuals and not neces-sarily as tribal members. Such Federal activitiesmay exist to augment tribally oriented programs,or Indians may be included within programs thatassist economically disadvantaged groups or haveother social policy objectives. Examples of Fed-eral activities to augment tribally oriented pro-grams include the health professions scholarshipprogram for Indian students (42 CFR 36.320-36.334) and grants for urban Indian health pro-grams (42 CFR 36.350-36.353), which are gener-ally used as core funds to help urban Indiansbecome eligible for and gain access to other gov-ernmental and private sources of services to theeconomically disadvantaged. An example of aprogram that is not directed specifically at Indiansbut that recognizes their needs is the NationalHealth Service Corps (NHSC). NHSC scholarshiprecipients must pay back their scholarships year-for-year by practicing in “health manpower short-age areas. ” In this program, the Indian popula-tion eligible for medical care from IHS is auto-matically designated as an underserved population(42 CFR Part 5, app. A).
Indians are U.S. citizens and are eligible formedical services provided to other U.S. citizens,including both Federal and State services. Throughregulations, IHS services are “residual” to thoseof other providers—i.e., other sources of care
(e.g., Medicaid, Medicare, private insurance) forwhich the Indian patient is eligible must be ex-hausted before IHS will pay for medical care. Fordirect IHS services, the residual payer role is dis-cretionary (42 CFR 36.12 [c]), and as a matter ofpolicy, IHS generally will provide services to apatient in IHS facilities regardless of other re-sources, but will seek reimbursement from thoseother sources for the care provided. For contractcare obtained from non-IHS providers, IHS’s re-sidual payer role is mandatory (42 CFR 36.23[f]),

—
and IHS will not authorize contract care paymentsuntil other resources have been exhausted or a de-termination has been made that the patient is noteligible for alternative sources of care.
One issue that has arisen in connection withIHS’s residual payer role is who is the primary,and who is the residual payer, when State or lo-cal governments also have a residual payer rule.This situation arose in litigation between IHS andRoosevelt County, Montana. The county had ar-gued that it was not discriminating against In-dians, but merely applying its alternate resourcepolicy across the board to all eligible citizens whohave double coverage, thereby meeting the “ra-tional basis” test for judicial review (79).
Amendments to the Indian Health Care Im-provement Act in 1984 contained a provision,commonly known as the “Montana amendment, ”that was designed to relieve several Montanacounties from providing and paying for medicalservices to indigent Indians and would have madeIHS financially responsible for medical care to in-digent Indians in Montana. This IHS responsibil-ity was to exist only where State or local indigenthealth services were funded from taxes from realproperty and the indigent Indian resided on In-dian property exempt from such taxation.
President Reagan vetoed the amendments be-cause of his objection to the “Montana amend-ment“ (and to a provision affecting the locationof IHS in DHHS ). There are two principal argu-ments that might prevail against the position thatState or local governments, instead of the IHS,can be the residual payer. First, Indians, as Statecitizens, are constitutionally entitled to State andlocal health benefits on the same basis as othercitizens under the equal protection clause of the14th amendment. The second argument is that theState or county cannot presume that Indians havea right or entitlement to IHS contract health serv-ices, and so cannot deny assistance on the groundsof double coverage. In fact, the Federal regula-tion on contract care expressly denies that sucha right exists. In such a conflict, the supremacyclause of the U.S. Constitution should resolve theissue in favor of the IHS regulation (79).
Ch. 1—Summary and Conclusions ● 1 1—.
In January 1986, the U.S. District Court for theDistrict of Montana, Great Falls Division, ruledthat the Federal Government, and not RooseveltCounty, was primarily responsible for the careof the Indian plaintiff (82). Though the court didnot find the trust doctrine, the Snyder Act, or theIndian Health Care Improvement Act as individu-ally entitling Indians to Federal health care, thecourt found that the two statutes, read in con-junction with the trust doctrine, placed the bur-den on IHS to assure reasonable health care foreligible members. The court, however, did not ad-dress the equal protection and supremacy clausearguments outlined above, and the decision is be-ing appealed (80).
A final observation is that radical changes inFederal policy toward Indians over the years haveintroduced a tremendous amount of complexityinto the Federal-Indian relationship, of which onlya fleeting glimpse can be presented in this assess-ment of Indian health care. Tribes may have con-tinued to exist as cultural, political, and socialentities, but they may have been officially “ter-minated” from recognition as tribes by the Fed-eral Government and therefore be ineligible forservices that the Government provides to recog-nized tribes and their members. Other tribes maybe federally recognized, but their reservation landsmay be only a miniscule portion of what theyonce had, so that most tribal members might notbe living on their official reservation but on landadjacent to or in the vicinity of the reservation.
Even tribes with large reservations have beenaffected by changing Federal policies. Most res-ervations contain sorer land that is owned by non-Indians, a legacy of the allotment period whenindividual Indians were given title to a portionof the reservation and sold it to non-Indians. Onsome reservations, “checkerboarding, ” the termgiven to the existence of a checkerboard patternof land ownership between Indians and non-Indians within reservation boundaries, is exten-sive, In addition, many reservations are in iso-lated rural areas, which have few economic op-portunities for tribal members who wish to remainon or close to their reservation. Finally, even

12 ● Indian Health Care— —
tribes with substantial natural resources or otherforms of capital assets often find it difficult tocommercialize those resources in ways that pro-vide employment for a significant number of their
DELlVERY OF HEALTH SERVICES
Federal responsibility for medical and health-related services was transferred in 1955 from BIAin the Department of the Interior to PHS in whatwas then the Department of Health, Education,and Welfare (42 U. S.C. 2004a). IHS is now lo-cated in the Health Resources and ServicesAdministration (HRSA), one of five administra-tive units that comprise the Public Health Serv-ice in the Department of Health and Human Serv-ices (figure 1-4).
Services that are available through IHS includeoutpatient and inpatient medical care, dental care,public health nursing and preventive care, andhealth examinations of special groups such asschool children (42 CFR 36.11). Within thesebroad categories are special initiatives in suchareas as alcoholism, diabetes, and mental health.However, the actual availability of particularservices depends on the area served. IHS regula-tions are very explicit on this point: “The Serv-ice does not provide the same health services ineach area served. The services provided to anyparticular Indian community will depend uponthe facilities and services available from sourcesother than the Service and the financial and per-sonnel resources made available to the Service”(42 CFR 36.ll[c]).
As previously described, direct care services areprovided through IHS at its clinics and hospitals,including IHS and some tribally constructed fa-cilities that are administered by tribes under theIndian Self-Determination and Education andAssistance Act of 1975 (Public Law 93-638; 25U.S. C. 450, et seq.); and through contract serv-ices purchased from non-IHS medical care pro-viders. Tribal administration most often involvesprimary care clinics and special programs such asalcoholism counseling and the community health
members. Thus, government programs are an im-portant source of employment, and IHS and BIAare major employers on many of the larger In-dian reservations.
TO ELIGIBLE INDIANS
representative program. Contracts with non-Indian providers usually involve specialty serv-ices and/or inpatient care not available throughIHS’s hospitals and clinics. In fiscal year 1985, outof a total appropriation of $807 million (exclud-ing the facilities construction program), the clin-ical services budget was $637 million (figure 1-5). The remainder was spent on preventive healthprograms and other activities such as urbanprojects, manpower training, and administrativecosts. Of the clinical services budget of $637 mil-lion, $164 million (26 percent) was spent on con-tract care, while $473 million (74 percent) wasspent on direct care. Approximately $141 million(30 percent) of the direct services budget wasadministered by tribal programs under self-de-termination contracts. Thus, of the $637 millionappropriated for clinical services in fiscal year1985, direct IHS operations accounted for 52 per-cent, tribally administered programs accountedfor 22 percent, and 26 percent was spent on con-tract care.
The organizational structure of IHS is depictedin figure 1-6. IHS facilities consist of 51 hospitals(6 are tribally administered), 124 health centers(over 50 tribally administered), and nearly 300health stations (over 200 tribally administered).A health center is a relatively comprehensive out-patient facility that is open at least 40 hours perweek, while a health station, which may be a mo-bile unit, is open fewer than 40 hours per weekand offers less complete ambulatory services. IHSalso maintains health locations, which generallyare outpatient delivery sites (but not IHS facil-ities) that are staffed periodically by traveling IHShealth personnel. The locations of IHS and triballyadministered hospitals and health centers aredepicted in figure 1-7.

Ch. 1—Summary and Conclusions ● 1 3
—
I
1
1 - _ . - - - - - - - .— - - -

14 ● Indian Health Care—
Figure 1-5.— IHS Allocations by Major BudgetCategory, Fiscal Year 1985
Preventive
Total IHS Allocations FY
Direct clinical care:$498 mil l ion- inc ludes ❑budget lines for hospi-tals and clinics; dental,mental health, alco-holism programs; main-tenance and repairs.
Preventive health serv-ices: $66 million —includes sanitation,public health nursing,health education, com-munity health represen-tatives, immunizations,
1985: $807 milllon
Contract care: $164 mil-Iion —services pur-chased from privateproviders,
Other: $79 million—in-cludes urban Indianhealth projects, healthmanpower, tribal man-agement, direct oper-ations.
SOURCE U S Department of Health and Human Servtces, Public Health Serv.Ice, Health Resources and Services Administration, Indian Health Serv.ice, Off Ice of Admtnlstration and Management, fiscal year 1985allocation includlng pay act funds, as of Sept 26, 1985 ($1 mllllon ofappropriation held In reserve)
In 1984, IHS also provided full or partial fund-ing for 37 urban Indian programs in 20 States.The urban programs’ emphasis is on increasingaccess to existing services funded by other publicand private sources for Indians living in urbanareas. Only 51 percent of the urban programs’ to-tal 1984 budget of $17.5 million was provided byIHS. Since some funding sources require theseprograms to serve certain populations that includenon-Indians, the only requirement that IHS im-poses on the urban programs is that the number
Figure 1.6.— Indian Health Service DHHS/PHS/HRSA
1 IW3 1~.-
1 ““”---m--’’-’--.,@--m--@\
R!l‘b—
Swlcsums
Mspltals *B mwCwlm Cltnlcs fibH9@h mdrsuhh
Cww mimaltacmlms
Kiil-... --.. . .-- 1. .
... -
n. Aberdeen● Alaska● Albuquerque● Bemidji P O. Billings● California P O. Nashville, P O. Navajo● Oklahoma● Phoenix● Portland. Tucson, P O
,I 1
Service units(79)
i
Hospitals Health othercenters clinics
WZFl. . .------:---
7. .
. . . . .
b
Indian & Alaskantribal
governments(500)
,I 1r-i Service units
(44)* h
H@@
SOURCE: U S Department of Health and Human Services, Publ[c Health Serv.Ice Health Resources and Serwces Administration, Indian Health Serwce/F/S Chart Ser/es Book, April 1985 (unpublished as charts 1.1.13, p 7)

Ch. 1—Summary and Conclusions ● 1 5-
● ✎
✞
\
● ● ●✎ ,4 :,, .0
4
4; ). :4 .
,.
● 3 ●. . . . .
- ; . a - - - -— . . .
r, , .
4
● .
0alal

16 • Indian Health Care—
of Indians served by each program be propor-tional to the amount of funds provided by IHS.
IHS hospitals are smaller than the average U.S.short-stay community hospital, with two-thirdsof IHS hospitals having 50 beds or less, comparedwith about 20 percent of all community hospi-tals in that size group. Thirteen of 45 IHS-operatedhospitals have 50 to 99 beds, and only 4 exceed100 beds: Anchorage, Phoenix, Tuba City, andGallup. Seven IHS hospitals have only 14 or 15beds. The average IHS hospital is over 35 yearsold. Of the hospitals operated by IHS, 18 werebuilt before 1940, 3 were built between 1940 and1954, and 26 have been built since the transferof Indian health services from BIA to IHS.
In general, an IHS hospital is likely to providea relatively wide range of health-related and so-cial support services, but few high-technologyservices. For example, only 13 of the 51 IHS andtribally administered hospitals offer staffed sur-gical services (5 of these are in Oklahoma), andan additional 7 hospitals offer modified or limitedsurgery (using part-time contract surgeons).
The fact that IHS hospitals are relatively limitedin the services they can provide is one reason thatthe contract care program has been under increas-ing budgetary pressures. Furthermore, IHS doesnot maintain hospitals in all its service areas. Inareas without IHS hospitals, inpatient services ofall types, as well as specialty services, must bepurchased from the private sector through thecontract care program. IHS maintains referralhospitals in Phoenix, Gallup, and Anchorage forIndians in those areas. These referral hospitals inturn have their own contract care budgets for fur-ther specialized services that they cannot provide.California and the Pacific Northwest, on the otherhand, have no IHS or tribal hospitals (there is ac-tually one hospital that is physically located inCalifornia to serve the Quechan tribe, which isadministered from the Yuma service unit out ofthe Phoenix area office) and must purchase all in-patient care with their contract care allocations.Except for the Mississippi Choctaw and NorthCarolina Cherokees, eastern Indians also are pro-vided inpatient services almost entirely throughcontract care.
As described earlier, IHS is by regulation a re-sidual provider. It will attempt to collect fromother sources of payment for care provided in IHSfacilities, and it will determine what other sourcesof financing are available before authorizing pay-ment for contract care (in addition to the previ-ously described eligibility criteria limiting contractcare to Indians living on or near reservations). Inpractice, other sources of payment are largely de-rived from Medicaid and Medicare, rather thanfrom private health insurance, because of the lowincome of many Indian people (especially thosewho are reservation-based) and their lack ofemployment-related health insurance benefits.
Photo credit: Indian Health Service
The 31-bed IHS hospital in Kotzebue, Alaska,constructed in 1961.
Photo credit: Indian Health Service
The 163-bed Phoenix Indian Medical Center, one ofthree referral hospitals in IHS.

Ch. l—Summary and Conclusions ● 1 7— - —
Even when patients have private insurance,companies routinely refuse to pay for services pro-vided in an IHS facility, because there is no obli-gation on the part of the insured Indian to pay.Through congressional amendments to the SocialSecurity Act, IHS facilities are eligible for reim-bursements from Medicare and Medicaid, withMedicaid payments to be made totally out of Fed-eral funds, and with the revenues to be used torestore or keep the facilities and their services incompliance with the conditions and requirementsof the Medicare and Medicaid programs. Indiansmay experience difficulties in maintaining theireligibility for Medicaid, however, if they are in
the “medically indigent” category of medical ben-eficiaries. Unlike “categorically needy” benefici-aries already enrolled in public assistance pro-grams who automatically qualify for Medicaid(e.g., Supplemental Security Income), the “med-ically indigent” must apply for and continue tomaintain their eligibility through county Medic-aid offices.
For those services that IHS (including triballyoperated programs) does purchase under contract,there are no uniform criteria for payment levelsamong IHS area offices. Physicians and otherhealth care providers (e.g., optometrists) are usu-ally paid on a fee-for-service basis; hospitalscharge their prevailing rates and often are paid100 percent of the amount billed. Individual serv-ice units within area offices may be able to nego-tiate lower payment rates, but this is the excep-tion and depends on such special factors as
long-standing relationships between the IHS serv-ice unit and outside providers, and on the avail-ability of a range of outside providers.
IHS has experimented only to a limited extentwith other methods of services delivery. In south-ern Arizona, the Pascua-Yaqui tribe’s outpatientand hospital services are provided through aprepaid arrangement with a health maintenanceorganization (HMO), financed through speciallyappropriated congressional funds. A similar dem-onstration is underway for the Suquamish tribein Washington State with Blue Cross/Blue Shield,but the demonstration is being conducted on a fee-for-service basis initially to develop informationon costs. In Oklahoma, the tribes served by thePawnee service unit have been provided with a“benefits package” in lieu of a replacement hos-pital. Under this arrangement, general outpatientcare is still provided through IHS clinics, but allother care is purchased from local providers atprevailing rates. The same limits (use of other re-sources first) are imposed on the Pawnee bene-fits package as are applied to IHS’s contract careprogram. The HMO option is not available in thePawnee service unit, because no HMOs exist there(or in many other IHS service areas). These ex-amples illustrate the extent to which availablealternate resources, and options in methods ofpaying for them, vary across the United States.As described earlier, similar variations in theavailability of direct IHS services exist across IHSareas.
FEDERAL EXPENDITURES FOR INDIAN HEALTH CARE
Federal expenditures for Indian health care areof two types: Federal programs targeted at spe-cific groups in the overall U.S. population forwhich individual Indians may qualify, and spe-cific appropriations for Indian health services. Theprincipal non-Indian health programs are Med-icaid and Medicare. Other Federal medical serviceprograms that serve some Indians include com-munity health centers and the Veterans Admin-istration’s (VA’s) medical care system, as well asmedically related social programs such as theWomen, Infants, and Children program. There is
also the National Health Service Corps (NHSC)program, which currently provides a large pro-portion of the physicians practicing in IHSthrough the payback requirement for NHSCscholarships (those physicians’ salaries are paidout of IHS funds).
Little information is systematically available onFederal, State, and private expenditures on In-dians. The best information is on Medicaid andMedicare, which are probably the largest non-Indian sources of expenditures, including State

18 Ž Indian Health Care—
and private health insurance sources. However,the information on Medicaid and Medicare islimited to reimbursement for services provided inIHS facilities. In the contract care program, theIndian beneficiary must first exhaust other sourcesof payment before the contract care program willauthorize care, but IHS does not keep track ofthe total costs of the care provided to Indian ben-eficiaries by non-IHS providers and only accountsfor IHS costs for contract care patients.
Figure 1-8 summarizes IHS appropriations from1972 to 1985 in actual and constant dollars. (Fa-cility construction funds are provided in separateappropriations and are not included in the figure.In 1985, the appropriations for facilities totaled$61.6 million, which was spent on new and re-placement hospitals, modernization and repair ofexisting hospitals, outpatient care facilities, grantsto community facilities, sanitation facilities, andpersonnel quarters, ) Adjusting for inflation, IHSallocations doubled between 1972 and 1985. How-ever, IHS’s estimated service population also dou-bled during this period (see figure 1-2), so thatallocations per estimated IHS beneficiary have re-mained essentially the same when adjusted for in-flation
900 “
800
700 -z.5 600—=~ 500m%: 4000
300
(figure 1-9).
Figure 1-8.—IHS Total Allocations,Fiscal Years 1972-85
—
Figure 1-9.—IHS Allocations Per Potential Beneficiary,
900
800
700
600
500
400
300
1972-85
1972 1974 1976 1978 1980 1982 1984
Fiscal year
— Actual dol lars
–– —–- 1972 dollarsSOURCES Allocations’ US DHHS, Indian Health Service, Resources Manage.
ment Branch Serwce Population U S DHHS, Indian Health Service,Population Statwtlcs Staff 1972 dollars obtained using OMB Feder.al non-defense deflators
In fiscal year 1984, IHS was reimbursed $12.7million from Medicare and $14.1 million fromMedicaid for services provided to eligible Indiansin IHS facilities. The Medicaid reimbursementsare somewhat surprising in view of the impres-sion OTA received during the course of thisassessment that many more Indians should beeligible for Medicaid than for Medicare. One ex-planation may be, as IHS officials have reported,that collections from Medicare for services pro-vided by IHS to Indians who also are Medicarebeneficiaries proceed relatively smoothly. IHS hasbeen reimbursed under Medicare’s prospectivehospital payment system since October 1983. Nor
#.- - - - - are contract care referrals a problem as long as- - - - - - # -the private provider is aware of the patient’s Medi-200 Lele=-”””,oo~
1972 1974 1976 1978 1980 1982 1984
Fiscal year
— A c t u a l d o l l a r s
–– -– - 1972 dollarsa
al glp dollars obtal ned using OM B Federal non-defense deflators
SOURCE U S Department of Health and Human Services, Publlc Health SerwIce, Health Resources and Services Administration, Indian Health Sew-Ice, Resources Management Branch
care eligibility and bills Medicare on behalf of thatpatient. Collections from State Medicaid pro-grams have been more difficult for both the IHSdirect and contract care programs, primarily be-cause of problems in ensuring that all Medicaid-eligible Indians are enrolled in the program. IHSmust deal with different and changing Medicaideligibility and coverage requirements in eachState; and State Medicaid programs, which areunder budgetary pressures of their own, have littleincentive to encourage Indian enrollment.

Ch. 1—Summary and Conclusions Ž 19
In the contract care program, some IHS areashave established their own manual or automatedsystems for identifying alternate resources. For ex-ample, in the Portland area (which has no IHShospitals), alternate resource utilization targetsbased on actual past collections have been estab-lished for each service unit and reviewed quar-terly. The targets, which reflect differences intribal population characteristics (especially age
HEALTH STATUS OF INDIANS
The overall health status of American Indianshas improved substantially since IHS assumedresponsibility for Indian health programs in 1955.The health of Indians is not yet comparable tothat of the general U.S. population (all races),however, and national IHS figures mask wide var-iations in overall mortality rates and cause-specificmortality rates among IHS service areas. More-over, analyses of the health status of AmericanIndians and the effectiveness of IHS efforts to im-prove it are limited by substantial data inadequa-cies. Therefore, all health status data should beinterpreted cautiously.
An overall improvement in Indian health is il-lustrated in figure 1-10, which shows a decline inthe crude mortality rate for 11 IHS service areas(California is not included because of seriousshortcomings in available data) for the decade be-tween 1972 and 1982. Comparisons with U.S. allraces data are not possible because of differencesbetween the age distinction of Indians and otherpopulations. Comparisons between IHS areasacross time should be made cautiously becauseof changes in populations and area boundaries.However, as also shown in figure 1-10, the de-cline was far from uniform across IHS areas: thePortland area appears to have experienced thegreatest decline, and the Billings area the least,In all IHS service areas, improvements in mor-tality rates for some conditions mask deteriora-tions due to other conditions. In Alaska, for ex-ample, reductions in death rates for suicide andinfant mortality were counterbalanced to someextent by increased deaths from heart and liverdisease. Improvement in Indian health is some-times inferred from the fact that heart disease in-
distributions) and the availability of other re-sources such as State Medicaid programs, rangefrom an expected 30 to 50 percent of contract carecharges that should be collected from non-IHSpayers. These estimates apply only to the serviceunits in the Portland area and are based on allalternate resources, not just Federal programs, butthey are likely to be largely dependent on Med-icaid programs.
stead of accidents has become the leading causeof death for Indians and from data that show thepattern of Indian illness to be shifting from in-fectious diseases toward chronic diseases. This ap-pears to indicate that Indians are living longer,but even heart disease is an affliction of youngerIndians, and the number of deaths from accidentsis almost as great as the number of deaths fromheart disease. Moreover, it is important to real-ize that differences between Indian and U.S. allraces mortality rates are primarily differences ofdegree; suicide and homicide were not among theleading causes of death for U.S. all races in theearly 1950s (155), but they are now (201).
Despite general improvement, much of the In-dian population residing in IHS service areas isin poor health relative to the rest of the UnitedStates. As shown in figure 1-11, in the 3-yearperiod centered in 1981 only one IHS service area,Oklahoma City, had an age-adjusted death ratethat was below that of the U.S. all races popula-tion (as explained above, information on the Cali-fornia service area is omitted because the data aretoo incomplete to support any conclusions).
Perhaps the most significant indicator of Indianhealth status is that Indians do not live as longas other U.S. populations. In the 3-year periodcentered in 1981, 37 percent of Indian deathsoccurred in Indians younger than age 45, com-pared with only 12 percent of U.S. all races deathsoccurring in that age group. Consistent with themortality experience, almost three-quarters of IHShospital patients in 1984 were under 45 years,compared with 48 percent of inpatients in U.S.short-stay, non-Federal hospitals being in that age

20 ● Indian Health Care
Figure 1-1O.—All Areas Crude Mortality RatesAll Causes, 1972-85
A1,3
12
11
1I
0.9 -838.2
0.8 -
0.7 -
06 -
“.-
1972-74 1975-77 1980-82
IHS Area Crude Mortality Rates All Causes, 1972-82
$ ‘3Fk 1.2 -m3
c: 1.1 -co 1 ~. . . . . . .76 ““-. . . . . . . . . .
. . . . . . . . . .3~ 0.9 ~ “-. .”-..... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
--WA- .-.- - - - . - . - , _- - - - - - : -.
k~ 0.6 -5u 0.5 , I-,-
1972-74 1975-77 1980-82
— A b e r d e e n — A l b u q u e r q u e . B i l l i n g s
—-. Alaska --- –- Bemidji
IHS Area Crude Mortality Rates All Causes, 1972.82
—.— .—. Navajo _ Phoenix ----------- Tucson
~ Oklahoma — P o r t l a n d ----- USET/Nashville
SOURCE Office of Technology Assessment, based on Indian Health Service data
Figure 1.11 .—Age-Adjusted Death Rates:American Indians, 1980.8212 IHS Areas: Both Sexes
(rates per 100,000 population in specified group)IHS total(excludingCalifornia)
U S all races
Aberdeen
Alaska
Albuquerque
Bemidj i
inma)a Bi l l ings
0’3I—
Cal i fornia
Nashvi l le
Navajo
Oklahoma City
Phoenix
Portland
Tucson
I 7783
5682
1,2613
9181
1,260.3
not available
765.4
6563
5306
918.2
7498
1,011 1
I 1 1 I 1 ) 1 J200 400 600 800 1,000 1,200 1 ,400
Age-adjusted mortality rateSOURCE: U S Department of Health and Human Services, Public Health Serv.
Ice, Health Resources and Services Admlnlstration, Indian Health Serv.ice, computer tape supplied to the Office of Technology Assessment,Washington, DC. 1985
group. These differences in age distribution areexplained primarily by the difference in causes ofillness and death.
For the 1980-82 period, the average age-ad-justed overall mortality rate for Indians residingin IHS service areas was 778.3 per 100,000, a rate1.4 times that of U.S. all races. For females, theage-adjusted mortality rate was 578.7, or 1.4 times0 ’

Ch. 1—Summary and Conclusions ● 2 1
that of all U.S. females; for males it was 998.8,1.3 times that of all U.S. males. These figures dif-fer markedly from those published by IHS, be-cause IHS averages all Indian deaths reported inall parts of each reservation State, whether or notIHS has service delivery responsibilities in thoseareas. In IHS’s view, it is necessary to publish datain this way to show changes since 1955, when IHStook responsibility for Indian health but at whichtime IHS had not yet been structured into serv-ice areas. For the 1980-82 period, IHS calculatedan average age-adjusted mortality rate for Indiansof 568.9, which was essentially the same as thatfor the U.S. all races population (191).
The leading causes of Indian deaths in 1980-82and their rates of occurrence compared to that ofU.S. all races are listed in table 1-1, using first-listed causes of death.
For U.S. all races, accidents were the fourthleading cause of death, For all IHS service areas,accidents were the second leading cause of death,and in seven IHS areas, accidents remained theleading cause of death. The accidental death ratefor Indians in all IHS areas was 3.4 times that of
the U.S. all races rate, and there was no IHS areathat did not have a mortality rate from accidentsat least 2.2 times greater than the U.S. rate.
On average, Indian mortality rates due to cardi-ovascular diseases and cancer were lower thanthose for the U.S. all races population. However,death rates from heart disease exceeded the ratefor the general U.S. population in four IHS areas:Aberdeen, Bemidji, Billings, and Nashville. Ineach of these four areas except Billings, heart dis-ease was the leading cause of death. Cerebrovas-cular disease also was a leading cause of deathin all IHS areas, and it exceeded substantially theU.S. all races rate in these same four areas plusAlaska. Similarly, the mortality rate due to alltypes of cancer, which was the third leading causeof death in IHS’s service population, exceeded therate for the U.S. all races population in five IHSareas. Some IHS areas have experienced high mor-tality rates for particular types of cancers, suchas for cancers of the digestive system in the Aber-deen and Alaska areas.
Diabetes mellitus was the seventh leading causeof death in the IHS service population. DuringOTA field work for this assessment, medical
Table 1-1.— Leading Causes of American Indian Deaths and Age-Adjusted Death Rates for All IHS Areas(excluding California) (1980-82), Compared to Age-Adjusted Death Rates for U.S. All Races (1981)
American Indian U.S. all races RatioIHS Number Age-adjusted Age-adjusted American Indiancodea R a n kb Cause name of deaths rate c rate to U.S. all races
ALL310790150620430510260830820740640730540090030
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
All causes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diseases of the heart . . . . . . . . . . . . . . . . . . . . . . .Accidents/adverse effects . . . . . . . . . . . . . . . . . . .Malignant neoplasms . . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis . . . . . . . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Pneumonia/influenza. . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Perinatal conditions . . . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . . . . . . .Septicemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . , . . . . . . . . . . . .
15,3213,0582,9461,713
801664580470458447331229205177122
772,910
778.3166.7136.398.448.133.826.627.821.219.49.8
12.46.59.66.54.2
144.4
568.2195.039.8
131.611.438.112.39.8
10.411.5
9.24.55.8
16.32.90.6
67.5
1.40.93.40.74.20.92.22.82.01,71.12.81.10.62.27.02.1
aco~parable to ICD-9 Codes, available from IHSbRanked by number of deaths
cNote that age and sex distributions are for reservation States and may or may not reflect age and sex dlst ri butlon I n I HS areas
SOURCES U.S. All Races: U S Department of Health and Human Servtces, Public Health Service, National Center for Health Statistics, “Advance Report, Final Mortal!.ty Stat! stlcs, 1981 ,“ Month/y V//a/ Stat/sties l?eporf 33(3) Supp , DHHS Pub No (PHS) 84-1120 (Hyatt swlle, M D PHS, June 22, 1984); Indians in IHS areas:U S Department of Health and Human Services, Publlc Health Service, Health Resources and Serwces Admlnlstratlon, Indian Health Service, computertape supplied to the Office of Technology Assessment, 1985.

professionals in several IHS areas cited the rap-idly increasing incidence of diabetes as a seriousconcern. Despite a 10-percent decline between1972 and 1982 in crude death rates from diabetes,the age-adjusted mortality rates for Indians ex-ceeded the U.S. all races rate in every IHS areabut Alaska, where diabetes was not among the15 leading causes of death. The overall diabetesdeath rate for Indians in IHS service areas was2.8 times the U.S. all races rate; and in the Aber-deen IHS area, it was 5.2 times the U.S. rate. Kid-ney failure was one of the common sequelae ofdiabetes, and deaths in the IHS population dueto renal failure exceeded the U.S. all races rateby a ratio of 2.8.
Pneumonia and influenza remain commoncauses of death among Indians. In the 3-yearperiod centered in 1981, the category combiningpneumonia and influenza was the sixth leadingcause of death among Indians, as it was for U.S.all races. For Indians, however, the 1980-82 raterepresented almost a 50-percent decline in deathsfrom pneumonia and influenza since 1972-74; yetit still was nearly twice the mortality rate for U.S.all races. In the Aberdeen area, the pneumoniaand influenza mortality rate was almost four timesthe U.S. rate in 1980-82. On the other hand,Indian death rates due to chronic pulmonary dis-eases (the 13th leading cause of death) were be-low the U.S. all races rate, even when age-ad-justed, for all IHS areas combined and in allindividual IHS areas but two.
While suicide and homicide were the 10th and11th leading causes of death for U.S. all races,they were the 9th and 8th leading causes, respec-tively, among Indians residing in IHS serviceareas. The 1980-82 crude death rate due to sui-cide among Indians exceeded the U.S. all racesrate by a ratio of 1.7. There was only one IHSservice area (Oklahoma City) for which the age-adjusted suicide mortality rate was lower than thatfor U.S. all races. Furthermore, suicide tends toclaim the lives of younger Indians: the Indian age-specific death rates for suicide exceeded those ofthe U.S. population for all age groups up to age44, and in the 15 to 24 year age group, the Indiandeath rate was 3.2 times greater than the U.S. rate.
The homicide mortality rate among Indians ineach of the IHS service areas was greater than the
U.S. all races homicide mortality rate. On aver-age, an Indian residing in an IHS service area was
6.3 times as likely to die as a result of homicidethan was a member of the general U.S. popu-l a t i o n . 3 . 0
Infant deaths have declined since 1972 in theU.S. population at large and among Indians. Inthe 3-year period centered in 1981, however, in-fant mortality rates in the IHS service populationexceeded the rate for U.S. all races in all but twoof the IHS service areas (excluding California).The overall IHS infant mortality rate of 13.3deaths per 1,000 live births in 1980-82 was 1.1times the U.S. all races rate. When infant deathsare analyzed in more detail, it is the first year oflife rather than the period immediately followingdelivery that is most dangerous for Indian infants.The IHS neonatal death rate (deaths occurring inthe first month of life) was lower than that forU.S. all races (Indian neonatal death rates ex-ceeded the U.S. rate in only two IHS areas), butdeath rates among Indian infants in the post-neonatal period (from 1 to 12 months of age) ex-ceeded the U.S. rate in all IHS areas but one.
Alcohol abuse is implicated in Indian deathsand illnesses from many causes, including acci-dents, suicide, homicide, diabetes, congenitalanomalies in infants, pneumonia, heart disease,and cancer. A high prevalence of alcohol abusecan be inferred from the extremely high rates ofdeath due to liver disease and cirrhosis of the liverin almost all IHS areas. In 1980-82, there were801 deaths in which liver disease or cirrhosis waslisted as the underlying (chief) cause. This repre-sented an age-adjusted death rate among Indiansof 48.1 per 100,000, which was 4.2 times the U.S.all races rate. In one IHS area, the death rate fromliver disease and cirrhosis was 10 times the U.S.rate, and there was no IHS area in which the In-dian rate was below the U.S. rate.
Mortality rates, of course, are not ideal indi-cators of a population’s health status. A numberof important health problems can be describedonly from epidemiologic surveys or patient caredata. Used cautiously, IHS inpatient and out-patient utilization statistics may be applied to sup-plement an evaluation of Indian health status. Forexample, patient care utilization data indicate thatotitis media is a severe problem among Indian

Ch. 1—Summary and Conclusions ● 2 3
●
A community health nurse examining Indian
Photo credit: Indian Health Service
children at home.
children. In 1984, otitis media accounted for 5.7percent of all outpatient encounters for males inthe IHS system, and 3.7 percent of the encoun-ters for females. In the same year, the rate of hos-pitalization for otitis media in IHS and contractcare hospitals was 18.0 per 10,000 population,compared with a rate of 12.8 per 10,000 in U.S.short-stay, non-Federal hospitals. This hospitali-zation rate reached 63.9 per 10,000 in Alaska.
There is considerable variability among IHSservice areas and between IHS service populationand U.S. all races rates in the relation betweenhospitalization and mortality rates. This is dueonly in part to the younger age distribution ofAmerican Indians and missing data and may in-dicate lack of access to services. Using U.S. short-stay, non-Federal hospitals as a benchmark, IHShospitalization rates (in both direct and contractcare hospitals but excluding two tribally run hos-pitals) generally were inconsistent with mortal-ity rates for accidents and violence, circulatory
system diseases, malignant neoplasms, alcohol-related conditions, diabetes, congenital anoma-lies, and conditions arising in the perinatal period.For all of these conditions except the last, aver-age IHS hospitalization rates were low relative tocause-specific Indian mortality rates, althoughthere were substantial variations among IHS serv-ice areas.
The example of the Portland IHS area may pro-vide a partial explanation for the apparent lackof relationship between causes of death among In-dians and cause-specific hospitalization rates. Inthe Portland area, IHS operates no hospitals andmust purchase all inpatient care through the con-tract care program, which has been used in re-cent years to purchase only emergency and ur-gent care because of limited funds. The numberof hospital discharges for the Portland IHS serv-ice population in 1984 was almost identical to thenumber in 1979, despite a 41-percent increase inthe service population size. As a result, Portland

24 • Indian Health Care
area hospital discharge rates for most diagnosticcategories were well below what might have beenexpected based on the mortality data. Limited IHShealth services may have similar effects in reduc-ing IHS hospitalization rates in the Bemidji, Nash-ville, and California service areas.
Hospitalizations for mental disorders have beendeclining in the IHS system more rapidly than inall U.S. short-stay, non-Federal hospitals, andmental health problems are not among the 15leading reasons for IHS outpatient visits. One ex-planation for this finding is that many mentalhealth and alcoholism treatment programs aretribally operated under self-determination con-tracts, and thus may not be included in IHS datareporting systems. However, mental health serv-ices are regarded by Indians and IHS area officestaff as relatively unavailable in most IHS areas;alcohol treatment and prevention programs arealso conceded to be inadequate to meet the needfor them.
There is very little information on the healthstatus of Indians living in urban areas, despite thefact that they constitute about 54 percent of thetotal Indian population. IHS does not collectmuch cause-specific patient care information fromurban programs, nor does it analyze or publishvital statistics and population characteristics forurban Indians except when those data are included
with national level data on the reservation Statesor included in service area data (some urban pro-grams are located in IHS service areas).
Vital statistics for Indians residing in StandardMetropolitan Statistical Areas (SMSAs) were pro-vided to OTA as part of the 1980-82 mortalitydata set. Thus, OTA was able to generate somedeath rate information on Indians living in urbanareas. Because of the lack of age-specific Indianpopulation data for urban areas, however, OTAwas not able to generate age-adjusted rates. Mor-tality rates for Indians in urban areas thereforemay be compared only with the crude death ratesfor other Indian populations, or with crude deathrates of the total population of particular urbanareas; they should not be compared with U.S. allraces age-adjusted rates, the standard of compar-ison generally used in this report.
On average, Indians in urban areas have essen-tially the same pattern of causes of death that isfound in IHS service areas. The leading causes ofdeath for Indians in urban areas were: 1) diseasesof the heart; 2) accidents, particularly motor ve-hicle accidents; 3) cancer; 4) liver disease and cir-rhosis; 5) cerebrovascular diseases; 6) homicide;7) diabetes mellitus; 8) suicide; 9) pneumonia andinfluenza; and 10) conditions arising in the peri-natal period.
MAJOR ISSUES IN FEDERAL INDIAN HEALTH POLCIYEligibility and Entitlement
Federal-Indian relationships historically devel-oped between the Federal Government and indi-vidual tribes or groups of tribes. Current relation-ships are based primarily on this cumulativeexperience and not on any relationship betweenthe Federal Government and some type of “UnitedNations” of all tribes. Thus, there is tremendousvariability in eligibility, ranging from tribes withland-based reservations, to tribes that have re-tained close social and cultural ties among itsmembers but who no longer have a significantland base, to Indians who may or may not bemembers of a tribe but who retain access to Fed-
eral benefits because they are descendants of pre-vious beneficiaries.
To be eligible for IHS direct services, a personneed only be of Indian descent and be regardedas an Indian by the community in which he livesas evidenced by factors in keeping with generalBIA practices. To be eligible for services not avail-able within IHS’s direct care system and whichtherefore must be purchased through contractcare, there are the additional requirements thatthe potential patient: 1) actually reside “on ornear” a federally recognized tribe’s reservation,which has been generally defined in the regula-tions as consisting of the county (ies) containing

or adjacent to the reservation (contract healthservices delivery areas, or CHSDAs); and 2) bea member of the tribe served or be recognized bythe tribe as having close economic and social tieswith it. Thus, the current IHS system is keyed toreservation-based Indians, but any Indian is eligi-ble at least for IHS direct services. There are, ofcourse, practical constraints in taking advantageof the IHS system, such as the physical locationof IHS facilities and limits on available resources,which may mean a long wait for elective car-e.
Currently, individual Indians need not regis-ter with IHS prior to seeking care. IHS estimatesits service population through the use of censusdata for counties meeting the CHSDA criteria,that is, for the same geographic areas in whichIndians must live to qualify for contract care.(This situation is not unlike the VA medical caresystem, in which all veterans are potentially eli-gible for VA care. Veterans must show proof oftheir eligibility when seeking care, as do Indiansfor IHS care, and there is no preregistration re-quirement in either system. The VA, however-,does have a priority system that favors veteranswith service-connected disabilities, indigent vet-erans, and veterans over 65 years of age. )
Toward the end of 1985, IHS was consideringthree changes in its eligibility policies: 1 ) using aregistration system started in January 1984 to ob-tain more accurate accounting of IHS’s servicepopulation instead of relying on census-basedpopulation estimates; 2) combining eligibility cri-teria for direct arid contract care so that a poten-tial IHS patient must reside in defined geographi-cal areas; and 3) imposing a minimum Indianblood quantum requirement of one-quarter formembers of federally recognized tribes and one-half for other Indians. According to IHS, com-bining eligibility for direct and contract carewould make IHS a single rather than a dual sys-tem of care. A minimum blood quantum require-ment is being considered because the presentdescendancy provision means that the eligiblepopulation is and will continue to grow muchmore rapidly than IHS appropriations. Limita-tions on eligibility are being proposed by IHS toengage Congress and the tribes in debate on theissue of budget pressures, which must be ad-
Ch. 1—Summary and Conclusions ● 2 5—
dressed either by increasing funds, cutting serv-ices, or limiting eligibility (51,99).
The registration system is a reasonable step indetermining who among the self-identified Indiansin the U.S. Census are not only eligible for IHSservices but also may reasonably be expected tomake use of such services. The registration sys-tem should also contribute to resource allocationdecisionmaking (discussed in the next section),which, as one of its basic parameters, requires anaccurate count of the Indian population that IHSserves. However, use of the registration systemas a factor in determining an IHS service area’sbudget would have negative effects in areas thathave not yet reached many members of the eligi-ble population, as might be the case for- recentlyrecognized tribes. These effects will be greater ifthe registration system is directed only at thosepatients who are actually treated, instead of ad-vertising and promoting the need to register withIHS regardless of any immediate need for medi-cal care. Thus, if the purpose of registration is toobtain a better account of IHS’s actual and po-tential user population, and not another meansof restricting eligibility, it would be reasonablefor IHS to implement its registration system overa few years and to take active steps to registereligible Indians. After this initial enrollmentperiod, IHS could then operate like a typicalhealth insurance plan. For example, IHS couldlimit services to enrollees, with open enrollmentperiods every year and provisions for emergencycare for patients who would have been eligiblefor services had they been enrolled.
Combining eligibility for direct and contractcare may not have a large impact on IHS’s presentclientele. IHS already estimates its service popu-lation to be Indians living in essentially the samegeographic areas that determine who is eligiblefor contract care. Currently, eligibility for con-tract care is further limited to tribal members andother Indians who are officially recognized by thetribe as having close economic and social ties withit. Indians not living in the specified geographicareas would be adversely affected by this pro-posal, but Indians living in these geographic areasand not members of the tribe(s) served by the lo-cal IHS facility would no longer have to prove

26 Ž Indian Health Care—
that they have close economic and social ties withthe tribe(s).
A minimum blood quantum requirement foreligibility would be extremely controversial, notonly because of the racial overtones if the Fed-eral Government rather than a tribe imposes it,but also because it would be seen as an encroach-ment on the authority of tribal governments. Rep-resentative of this view is the statement of onetribal chairman that “blood quantum eligibilityfor IHS patient care should be set by individualtribes as to correlate with tribal standards fortribal enrollment” (6).
In sum, IHS is proposing to restrict eligibilityby defining where Indians can live and still beeligible for IHS services, and by establishing aminimum Indian blood quantum requirement ofone-quarter for members of federally recognizedtribes and one-half for other Indians. Alternativesto this approach include:
Option 1: IHS or Congress could develop a pri-ority system for access to IHS services.
Rather than excluding whole categories of cur-rently eligible Indians, IHS or Congress could de-velop a priority system similar to the one that ex-ists in the VA medical system. For example, theIHS proposal could be modified by giving priorityin descending order to: 1) tribal members who liveon or near the reservation; 2) members of the In-dian community who have close economic andsocial ties to the tribe; and 3) all other currentlyeligible Indians.
Option 2: IHS or Congress could use bloodquantum criteria to supplement rather than re-strict eligibility criteria based on tribal mem-bership.
One such approach could be to specify that In-dians eligible for IHS services would consist ofmembers of federally recognized tribes withouta blood quantum requirement, plus descendantsof members of federally recognized tribes whowere at least one-quarter Indian blood. The lat-ter category may grow in importance as tribalmembers increasingly marry outside their tribes,because their descendants may be ineligible formembership in any specific tribe if they do nothave the minimum tribal-specific blood quantum
required for tribal membership, even if their cle-gree of total Indian blood remains high.
An unresolved issue in this option is the varia-tion among tribes in the use of blood quantumto determine membership. Many tribes have aminimum tribal-specific blood quantum require-ment for membership, the most common beingone-quarter or more, but there are many tribesthat only require members to be descended froma member. (There are variations even in descend-ancy requirements, e.g., membership only throughmaternal lineage. ) While tribes and Indian peo-ple in general are understandably very sensitiveto the issue of blood quantum, this promises tobe an increasingly divisive issue in the future astribes with only descendancy requirements growmuch more rapidly than tribes with some type ofblood quantum requirement.
Of course, the IHS initiative to limit servicesto persons with at least one-quarter Indian bloodis directed at this issue, but as already noted, itclashes with tribal political authority. A partialsolution may be found by examining what mem-bership means for tribes that have descendancyrather than blood quantum requirements. Sometribes have several categories of membership, withthe lesser categories not eligible for all rights oftribal citizenship (e.g., voting or receiving occa-sional per capita payments from tribal enter-prises). These special membership categories mayhave been established so that the larger tribal com-munity could receive Federal services from BIAand IHS. Thus, “membership” for the purposesof IHS eligibility could be defined as includingonly those members of a tribe who have the rightto participate in all political and economic activ-ities of the tribe. By linking eligibility for IHS serv-ices only to those members who have the powerto determine who controls the tribal government,there should be a built-in incentive for tribes tobe conservative in their membership criteria. Thismay even be the case for tribes with only descen-dancy as a requirement for full membership.These tribes are aware of the increasing difficul-ties in both tribal governance and preservationof their resources because of their descendancyprovisions, and may feel compelled to move inthe future toward more conservative criteria fortribal membership.

Ch. 1—Summary and Conclusions . 27
Option 3: If eligibility criteria are made morerestrictive, Congress could make IHS services lessa residual source of care and more an entitlementprogram.
The proposed IHS restrictions on eligibility arebased on limiting services to members of feder-ally recognized tribes and other Indians who liveon or near reservations. Thus, there would be acloser link between Federal health benefits and thegovernment-to-government relationship betweenthe Federal Government and Indian tribes. If thisis the direction that Federal policy follows, thenit is reasonable to argue that health care shouldbecome an explicit part of the trust responsibil-ity. The legal relationship between the FederalGovernment and Indian tribes, in which there arepresently no trust rights for Indian health care,is no impediment. Congress has the power to de-cide whether or not health services should be partof the Federal trust responsibility. All the courtshave said is that it is Congress’s option to pro-vide health services to Indians as a discretionaryor guaranteed benefit.
The current position of IHS is that it is a resid-ual payer to other resources available to its serv-ice population. Congress could change this situ-ation and establish a trust fund similar to that forMedicare, thereby providing an entitlement healthcare program for Indians. Alternatively, Congresscould continue with yearly appropriations butestablish a more comprehensive services packagefor eligible Indians, such as those long availableto military personnel and their dependents, andto veterans. The Defense Department and the VApurchase services that are not available in theirown medical care systems from the non-Federalsector for their members and dependents (10U.S. C. 1071-1090; 38 U.S. C. 601-654). The mili-tary and VA contract health programs are muchmore generous than IHS’s contract care program.They provide a wider range of benefits and willapprove contract care when it is difficult to reacha military or VA facility, in addition to purchas-ing care not available in these facilities. In con-trast, eligibility for IHS’s contract care programis limited to Indians living in the general vicinityof Indian reservations and expressly excludes In-dians who do not live nearby. Thus, Federal pro-grams for special populations already exist that
can serve as models for providing vested or morereliable and comprehensive sources of care thanare currently provided to Indians,
This approach could be used to help supportspecific policies. For example, one policy mightbe to limit IHS services to tribal members but topreserve tribal sovereignty by not dictating to thetribes who among their members would be enti-tled to services (the IHS proposal would limit eligi-bility to tribal members who had a minimum de-gree of Indian blood of one-quarter). If eligibleIndians had to use specified non-IHS providerswhen IHS direct services were not available, suchas an HMO, tribal members who live far awayfrom the reservation would have difficulty inmaking use of services, but IHS would not haveto dictate to the tribes who among their memberswould be IHS-eligible. In contrast, a Medicare-type insurance policy could be used anywhere.The availability of services through HMO-typeorganizations obviously varies tremendously andmay not be available in many parts of the coun-try where IHS provides services, but it could beIHS policy to seek out and encourage these typesof organizations.
Resource Allocation andScope of Services
IHS has traditionally allocated its appropria-tions among its 12 service areas through a “his-torical” or “program continuity” budget approach.Thus, each area could expect to receive its recur-ring base budget from the previous year, plus anincrease in mandatory cost categories (e. g., per-sonnel cost-of-living and relocation expenses, sup-ply cost increases) equal to the percentage increasein those categories awarded to the overall IHSprogram. This method of allocating resources waschallenged in the 1970s in the Rincon decision (de-scribed above). The court criticized the histori-cal budgeting approach, found that IHS was ob-ligated to provide health services to Indians inCalifornia that were comparable to those offeredIndians elsewhere in the United States, and de-termined that IHS was obligated to allocate itslimited resources equitably by the consistent ap-plication of reasonable distributive standards.
52-81’15 o - 86 - 2

IHS proposed using an equity fund to be allo-cated by a needs-based formula as its means ofachieving comparability among the tribes. For fis-cal years 1981 to 1984, the congressional appropri-ations committees earmarked about 1.3 percentof the total IHS health services appropriations an-nually for an Equity Health Care Fund, or about$7 to $9 million per year. Indians in Californiareceived about 35 percent of this amount. Al-though Congress did not earmark equity fundsin fiscal year 1985 appropriations, IHS set aside$5 million of its appropriations, as it has a con-tinuing obligation to reduce these funding dis-parities.
For fiscal year 1986 appropriations, IHS plannedto apply an equity-based formula to any fundingincreases (including mandatory budget categoryincreases) over the 1985 area base budgets. Inaddition, the population figures for each area wereto be based on the patient registration system (be-gun in January 1984) rather than on the census-based estimated eligible service population.
The effects of the equity funds are cumulative.Equity awards become part of the recurring basebudget and thus are guaranteed in future yearsas long as overall IHS allocations continue tocover the increase. These equity awards can havea significant impact on upgrading services, par-ticularly among small tribes, where the increasecan represent significant additions to their previ-ous budgets. New equity funds, however, con-tinue to represent less than 2 percent of the totalIHS services budget and do not play a major rolein the overall IHS budget allocation process,which continues to be driven by the historicalfunding approach.
The larger issue of a more equitable distribu-tion of the overall IHS clinical services budget hasbeen a topic of discussion for years, and tribesthroughout the United States increasingly havepressed for a resolution of the matter. For exam-ple, the Navajo Tribal Council passed a formalresolution in response to this OTA assessment,calling for “the consistent application of reason-able distributive standards, ” through the use of“a set of economically and epidemiologically-based formulae” which take into account “the con-tinually changing health conditions of the vari-
ous tribes, shifts in the geographic distribution ofeligible Indian beneficiaries, and regional differ-ences in the availability of alternative health caredelivery systems” (120). The Northwest PortlandArea Indian Health Board made suggestions alongsimilar lines, identifying the key points in resourceallocation as including population, the benefitspackage provided, the alternative resources avail-able, and cost differentials between IHS areas (95).
There are major impediments to the develop-ment of a redistribution formula for the total IHSclinical services budget that would be generallyaccepted by most parties. These impediments in-clude: 1) lack of agreement on what constitutesthe eligible population; 2) differences in the de-gree and type of services currently available inIHS service areas; and 3) questions on the valid-ity of the data that would be used in applying areallocation formula.
IHS uses estimates of its eligible population thatare based on the most recent census data, adjustedby birth and death statistics. Under a historicalbudgeting system, the accurateness of these esti-mates was not crucial, since the budgets wouldnot have been adjusted for per capita differencesin funding between IHS areas. The patient regis-tration system initiated in January 1984 will pro-vide more reliable information on eligible and po-tential users for resource allocation purposes, butif it is applied before adequate efforts have beenmade to seek out and register eligible Indians, itcould reward areas with high use or successful en-rollment efforts while penalizing areas with unmetneed. Several areas already are operating undersevere budget restrictions, especially in the con-tract care program. Present patterns of use inthose areas do not reflect need, and the expresseddemand for services is also likely to be artificiallylow because of these restraints.
In addition, there is the larger underlying ques-tion of who is (or ought to be) an Indian for thepurpose of eligibility for IHS services. This con-troversy includes the descendancy versus bloodquantum requirements discussed in the previoussection, and the status of Indians in terms of Fed-eral recognition. The descendancy issue surfacesmost often when the Oklahoma area is discussed,because of the common belief among Indians else-

Ch. 1—Summary and Conclusions ● 2 9
where that many of the users of IHS services inOklahoma may be descended from Indians butare only nominally Indians. The Federal recog-nition issue is most applicable to the Californiaarea, where tribes have a bewildering mixture ofdifferent types of recognized and unrecognizedstatus, largely because of past government pol-icies. The California area, then, would also be im-mersed in controversy over the number of Indianswho are eligible for IHS services.
The scope of services available in IHS areas isnot uniform. Thus, before funds are redistributed,there has to be agreement on how these differ-ences should be factored into any redistributionformula. One criterion for redistributing resourcesthat has been suggested and examined by IHS isthe availability of alternate resources. In fact, themethod that IHS has developed to distribute itsequity funds subtracts these alternate resourcesin calculating area funding needs. This policypenalizes areas that make the most efficient useof their IHS funds and provides built-in incentivesnot to be too aggressive in third-party collections.On the other hand, this policy could have the ef-fect of shifting more funds to areas heavily de-pendent on contract care. In the contract care pro-gram, efforts are made to have other resourcespay first before contract care funds are author-ized. Since the contract care program does not ac-tually collect money from these other sources,areas heavily dependent on contract care wouldnot have these payments subtracted from theirbudgets.
There are serious deficiencies in most of thehealth data on Indians, including data on theirhealth status and their use of IHS and contractcare services. This has been a problem for OTAthroughout this assessment, and much of the datawe have provided has had to be qualified in termsof its completeness and accuracy. Nevertheless,OTA has provided its best estimates of such in-dicators, because much of this information is notreadily accessible. It is hoped that the informa-tion provided in this report will serve as a com-mon starting point for negotiations among Indiantribes, Congress, and IHS on equitable methodsof resource allocation.
Option 4: Continue with the modest, incre-mental approach to resource redistribution thatIHS has implemented.
An equity fund, whether provided through ear-marked congressional appropriations or througha set-aside by IHS of a small portion of its ap-propriations, is the least controversial method toimplement, but it has only a modest impact. Pastand current redistribution decisions have been ap-plied only to increases in IHS appropriations. Thisimpact could become more substantial if budgetreductions, instead of increases, are made by Con-gress as part of its overall efforts to reduce theFederal budget deficit, and if IHS became moreassertive in decreasing some area budgets insteadof trying to minimize the impact of the realloca-tion process.
At the end of 1985, IHS area directors hadagreed to reserve any funding increases over thelevel of the 1985 base budgets, including manda-tory budget category increases, for special distri-bution by an equity-based formula. In the firstyear of this potential distribution, however, noarea would receive less than its 1985 funding (214).Thus, while the principle of the equity approachhas been accepted by IHS area directors, it re-mains to be seen if it will be accepted and imple-mented if additional funds are not available and,instead, budget reductions must be made.
Congress could make this incremental approachmandatory either through earmarking of part ofthe annual appropriations, or through legislationspecifying the percent of IHS appropriations thatshould be subject to reallocation.
Option 5: Accelerate the rate of reallocatingfunds among IHS areas.
The general approach taken by IHS could beimplemented on an expanding basis, with theproportion of reallocated IHS funds increasingfrom one year to the next. This approach couldalso be implemented either through earmarked ap-propriations or through legislation. However,such a move would be much more controversialthan the present, modest reallocation, and greaterdiscussion and consensus on the criteria for redis-

30 ● Indian Health Care
tribution would be needed by the tribes and IHSarea offices.
Option 6: Work toward a common minimumservices package for all IHS areas.
A different approach that is not entirely di-rected at gaining funding equity among IHS serv-ice areas would be to focus on the services thatare available to the individual Indian beneficiary.A principal objective in equity funding is to ensurethat eligible Indians everywhere have access tocare that is appropriate to their needs. But equityin the sense of relative need may prove to be anelusive concept, considering the complicated fac-tors that have been identified as essential partsof the formula, and the necessity of having toconvert these complicated factors into monetaryamounts.
Equity can also be viewed in terms of access:if eligible Indians in all IHS service areas gener-ally have access to the same types of services,much of the dissatisfaction over the present allo-cation of resources might be muted. A commonservices package would have to include both di-rect and contract care services for two reasons:1) to neutralize the present disparity between IHSareas in the mix of direct and contract care serv-ices available, and 2) to ensure that eligible In-dians in all areas have access to the same rangeof services. A common services package is prob-ably best accomplished by limiting access to non-IHS providers. For example, instead of paying forcare from any non-IHS provider, services couldbe limited to designated non-IHS providers on aprepaid basis, such as HMOs where available.
Availability and Adequacyof Resources
IHS provides ambulatory and hospital care andpurchases services not available at IHS facilities.In some areas, only ambulatory care is provideddirectly, either through IHS or tribally adminis-tered clinics. There are also a few demonstrationprograms in purchasing all care from outsideproviders, such as the Pascua-Yaqui HMO men-tioned earlier. Those demonstration programs re-flect the variability around the United States inthe availability of alternative methods of provid-
ing and financing health services, and also indi-cate the basic changes that are occurring in theUnited States’ health delivery systems.
Approximately 26 percent of the IHS clinicalservices budget is spent on contract care. Despitethe policy that alternative resources must be usedfirst, many IHS areas have had to limit the useof contract care to emergency and urgent cases.Furthermore, a few high-cost cases can quicklydeplete a service unit’s contract care budget, andseveral area offices have set aside a portion of theircontract care dollars in a contingency fund forsuch events. In the 1984 Indian Health Care Im-provement Amendments that were vetoed byPresident Reagan, Congress had addressed thisproblem by establishing a $12 million revolvingfund for high-cost contract care cases (the “Cat-astrophic Health Emergency Fund”) that wouldpay for contract care cases once a threshold ofbetween $10,000 to $20,000 had been exceeded.The adequacy of this proposed fund was exam-ined by OTA in detail, and the results of our anal-ysis are summarized later in this section.
Several factors suggest that IHS will become in-creasingly reliant on the contract care program.The present IHS and tribal network of hospitalsand clinics is limited in the types of services it canprovide, and budgetary limits increasingly restrictnew facilities construction, the replacement of oldand inadequate facilities, and needed maintenanceand repair of existing facilities. Diagnostic andtherapeutic equipment purchases are limited, fur-ther reducing service capabilities. This limitationis due to the overall Federal budget situation andin part to the practical limitations of deliveringcomprehensive and specialty services to manywidely dispersed, small populations.
Perhaps the most critical factor that in the nearfuture may orient IHS away from direct care togreatly increased contracting is the growing prob-lem of how to recruit and retain adequate medi-cal staff. IHS depends on the PHS CommissionedCorps and on the service payback obligations ofNHSC trainees for many of its physicians, nurses,and other medical and administrative staff. TheCommissioned Corps is not a growing resource.The NHSC program is being eliminated, and thelast trainees will be available to IHS in 1990. If

Ch. 1—Summary and Conclusions ● 3 1
IHS staff positions cannot be filled, IHS will haveto turn to the services of private providers, wherethey exist, under the contract care program.
High-Cost Cases in theContract Care Program
“Catastrophic health costs” usually refers to thedevastating financial effects that extremely costlyand long-term illnesses can have on individualswho may have no insurance or who may be in-adequately insured. Catastrophic costs most oftenare defined in terms of out-of-pocket costs to in-dividuals that exceed a certain percentage of in-dividual or family income, or as total costs percase in the range of $20,000 to $25,000 and above.In the IHS contract care program, the costs of cat-astrophic illnesses not covered by other payers areborne by IHS, not by individual Indians (althoughthere may be cases that are disputed between IHSand another payer as to whom is the responsibleparty, leaving the individual Indian caught be-tween the two). The discussion of catastrophiccosts in the IHS contract care program, therefore,has revolved around the idea of a limit for indi-vidual service unit obligations to be set somewherebetween $10,000 and $20,000 per case, with costsover this threshold to be covered by a specialrevolving fund. This fund, as explained above,would have been set at $12 million.
The data that OTA was able to obtain on thetypes, incidence, and costs of these cases wereincomplete and poorly identified, Thus, it was notpossible to determine from the available datawhether what is called a problem of catastrophiccare is in fact a problem of excessive incidenceof catastrophic conditions in the Indian popula-tion, or whether it is more properly described asa budget management problem. Nor was it pos-sible to consider alternative financing arrange-ments for these cases because of the lack of actu-arially reliable data and the relatively smallnumber of cases identified (i. e., small in terms ofbasic insurance principles on risk-spreading).Nevertheless, the data were sufficient to reach thefollowing conclusions,
Based on the 1983 high-cost case experience inIHS, if the threshold was set at $10,000 per case,at least $5.5 million of the $12 million fund would
have been needed to cover IHS contract hospitalexpenditures alone. Areas with higher averagecosts per case, such as Alaska, could expect themost relief. Some areas, such as California andperhaps Bemidji, would not benefit from the spe-cial fund, because they presently cannot affordto spend up to the threshold figure to qualify forthe fund.
If the threshold was set at $15,000 per case, totaloutlays would have been a minimum of $3 mil-lion, and 2 of the 10 (of 12) IHS areas in the 1983data set would not benefit at all. A $20,000 thresh-old per case would require outlays of about $1.2million and assist only 4 of 10 areas. Includingestimated nonhospital costs (physicians’ fees, labwork, etc. ) of from 16 to 30 percent of the hospi-tal costs, the $12 million fund still would havebeen adequate in 1983 whether the threshold wasset at $10,000, $15,000, or $20,000.
Problems in identifying high-cost case recordsto make up the data sets used in this analysis sug-gest that undercounting of cases may be consid-erable. Furthermore, the effects of health cost in-flation could be substantial. For example, the 1983data set included 524 cases, and there were origi-nally 390 cases identified for 1984, When the 1984billing file was searched again in October 1985,746 high-cost case records were found. Since thedata set identified any cases that cost the contractcare program $10,000 or more, it might be ex-pected that the number of cases would increasesignificantly from year to year from cost infla-tion alone. Thus, there is justifiable concernwhether a $12 million fund would be adequatefor very long.
Conclusion.—A high-cost care fund to spreadthe financial burden of high-cost contract carecases among all IHS service areas is a reasonableapproach, whether those funds are derived fromadditional, earmarked appropriations or set asidefrom overall contract care funds. However, thefund would not assist IHS service areas that arenot able to pay for contract care up to the thresh-old (between $10,000 and $20,000 per case) be-fore the fund becomes available. If the high-costcare fund is financed by setting aside a portionof contract care funds instead of from additionalappropriations, IHS service areas that would not

benefit from the fund could be exempted fromhaving a portion of their contract care allocationsredirected to the high-cost fund. For those serv-ice areas that would benefit from the high-costfund, different thresholds to trigger eligibility forfunds could be considered, since a commonthreshold would clearly favor a few areas overothers. Finally, high-cost cases seem to be a budgetmanagement problem in the contract care pro-gram rather than a problem of excessive occur-rences of catastrophic conditions. The possibil-ity of incurring high-cost cases has led several IHSservice areas to set aside a portion of their con-tract care funds. This practice can lead to severerationing of contract care early in the fiscal year,followed by accelerated spending at the end of theyear if the expected high-cost cases did not materi-alize. One method to alleviate this situation is togive IHS the authority to carry over a portion ofits contract care appropriations into the next fiscalyear (see option 8 below).
Options To Improve the Cost-Effectivenessof the Contract Care Program
Given expected rates of increase in generalhealth care costs relative to likely IHS budget in-creases, even the most efficient management tech-niques will not be able to overcome the problemsof inadequate funding and a growing service pop-ulation in the IHS contract care program. How-ever, the following options could help to mitigatesome of the financial problems.
Option 7: Negotiate payment rates with con-tract care providers instead of paying 200 percentof billed charges, and impose a rate structure onIHS contractors, such as use of Medicare DRG(diagnosis-related groups) rates.
IHS could negotiate more aggressively, wher-ever possible, to obtain better prices for the serv-ices it purchases. Instead of paying full billedcharges, which many service units do, bargain-ing for reduced fees and encouraging competitionamong contract providers could be undertakenby several service units acting in concert or bythe area office. Use of Medicare DRG rates couldgenerate substantial savings for the hospital in-patient care portion of the contract care program.
IHS intends to issue a general notice sometimein 1986 that will state that IHS will not use pri-vate providers (except in emergencies) unless theprovider has a contract with IHS. IHS will notsign a contract with a provider unless it agreesto accept payment at no more than the “Medicare-allowable” rate, whether that rate be based onDRGs for inpatient care or on “reasonable andcustomary” charges for physician services. Thispolicy would be applied to the 1,300 to 1,400standing contracts that IHS currently maintains(78). Whether IHS will be successful in imposingthese changes on private providers may dependon the existence of competition among those pro-viders for IHS patients, because at least someproviders can be expected to refuse to participatein the contract care program if these paymentchanges are made.
Option 8: Authorize IHS service units to carryover a percent of contract funds from one fiscalyear to the next.
Although some tribally operated contract careprograms may exercise this option, service unitcontract care programs managed by IHS are notallowed to carry over funds, which further limitsthe ability to manage the program. Services maybe restricted too severely early in the fiscal yearin order to conserve funds, then virtually anyservice request may be authorized at the end ofthe year, including previously deferred services,to close out the budget. Congress could author-ize IHS to carry over a certain percent of the an-nual allocation, perhaps 5 or 10 percent, to easethis problem.
Option 9: Provide greater IHS headquartersand area office support to service unit contractcare programs in dealing with alternative re-sources, both public (especially State Medicaidprograms) and private.
In order to utilize alternative resources most ef-fectively, the contract care program must be ableto respond to changes in the general health careenvironment that will affect services to IHS ben-eficiaries. Changes in State Medicaid programscan have significant impacts on IHS contract careprograms. For example, in the State of Washing-ton, a health services program for the medically

indigent that included a large number of Indianswas discontinued for about 6 months in 1985. ThePortland area office estimated that if the programwas not reinstated (it was reinstated in October1985, but its future was uncertain), additionalcosts to the Portland IHS contract care programwould have totaled at least $2 million per year.In Arizona, recent implementation of a Medicaidprogram has brought about a major realignmentof IHS, county, and State health programs avail-able to Indians. Thus, IHS contract care programsmust keep current about changes in State Medicaidprograms and assist all eligible Indians in enroll-ing and maintaining eligibility in those programs.
Option 10: Explore possibilities of developinglong-term relationships with community facilitiesand of providing more services to non-Indians.
For IHS, discount rates might be possible ifcommunity facilities were assured a certainamount of referrals. If services were provided tonon-Indians with the approval of the tribe(s), theextra revenues might make it possible for the pro-gram to provide a wider range of services thanwould be available if only Indians were served.(Some tribal and IHS programs already serve non-Indians with the consent of the affected tribes. )This would be consistent with the policy of self-determination, with the extra revenues used to im-prove services delivery. Congress already author-izes IHS to serve non-Indians in specific locations(e.g., Alaska), and the vetoed 1984 Indian HealthCare Amendments would have provided this au-thority throughout IHS service areas, subject tothe consent of the specific tribes affected.
Self-Determination and TribalAssumption of Federal Indian HealthServices
Under the Indian Self-Determination and Edu-cation Assistance Act of 1975 (Public Law 93-638,commonly known as the “638” law or program;see 25 U. S.C. 450, et seq. ), tribes have the op-tion of taking over the administration of programsmanaged by BIA and IHS. For tribes that havebeen provided direct IHS services, self-determi-nation programs have often involved limited
Ch, 1—Summary and Conclusions Ž 33
activities instead of the entire range of medicaland health-related services. Indians that have mostrecently been added to the IHS service popula-tion (through restoration of their Federal status),such as in California and especially the EasternUnited States, however, have received health serv-ices primarily through self-determination con-tracts. Under these contracts, tribes or their rep-resentatives, instead of IHS, operate outpatientclinics and purchase specialty and inpatient serv-ices through contract care.
The Self-Determination Act modifies the stand-ard cost-reimbursement or fixed-cost contract.Federal procedures for procurement contracts re-quire an “arms length” relationship between theFederal Government and the contractor. The gov-ernment may unilaterally order changes in thescope of the contract and may terminate the con-tract at its convenience, while the contractor maynot. Federal labor laws and equal opportunityprovisions also apply to the contractor. On theother hand, in self-determination contracts, IHSand BIA are directed to assist tribes in develop-ing contracts and to enter into all proposed con-tracts unless there are compelling reasons not todo so. All changes require the consent of the con-tractor. While the government may reassumemanagement of the contract only for specified rea-sons, the contractor may terminate the contractand return management to IHS (retrocession) on120 days’ notice. Employees of tribal contractorsare not subject to some Federal labor laws, andIndian preference in employment and training su-persedes equal opportunity rules. Tribal contrac-tors also enjoy exemption from bonding require-ments and may carry over unspent contract fundsto the following year.
The limited involvement in self-determinationactivities by tribes that have been accustomed toreceive direct IHS services may be due to any ofa number of factors. First, their lack of experi-ence in administering health care programs hasmotivated many tribes to start slowly with limitedresponsibilities. Second, the common perceptionof tribes seeking to administer more of their ownprograms is that IHS will not fund their activi-ties at the same level that IHS itself had to oper-ate the programs, so tribes are reluctant to assumeresponsibility for a marginally funded program

34 ● Indian Health Care
or one with declining resources. This disagreementon funding levels is most often focused on the levelof administrative or indirect costs. Tribes pointto IHS administrative positions that they believeshould be abolished and the funds made availableto them. IHS maintains that these positions areneeded to monitor the self-determination contractsand to insure that IHS can resume administrationof the programs if the tribes decide to return them,because the act allows tribes to retrocede thesewith 120 days’ notice. Third, many IHS serviceunits serve multiple tribes, and the unanimousconsent of all tribes within the service unit mustbe obtained before a takeover will be approvedby IHS. Fourth, given the history of Federal-Indian relationships, some Indians suspect that thetransfer of program administration from IHS maybe another “termination” policy in disguise. Fifth,when tribes have contested IHS’s self-determina-tion policies, it has not been clear what they cancontest and what procedures they must follow toappeal negative IHS rulings. Finally, Federal em-ployees generally receive higher salaries and morefringe benefits than can be provided by the tribes,so there sometimes is resistance against conver-sion from IHS to tribal management even by In-dian employees. These differences, as well as costsfor such items as malpractice insurance that IHSneed not account for in its budget but for whichtribally administered programs are responsible,have been cited as additional evidence that thetribes are not being offered the same level of re-sources as has been available to IHS.
A central issue that underlies many of the par-ticular difficulties that have arisen in IHS’s im-plementation of the Self-Determination Act is theapparent difference of opinion between the Fed-eral Government and the tribes as to the intentof the law. While the Federal Government seemsto view self-determination primarily as a contract-ing program, the tribes point out that the law dis-tinguishes 638 contracts from other Federal con-tracts and suggest that the intent of the law is tosupport tribes in taking over and managing theirown services.
Tribes believe that leadership commitment inIHS has not been strong enough, with little posi-tive guidance provided to the area offices, towhich responsibility for self-determination con-
tract administration has been delegated. The areaoffices vary in their enthusiasm for such contractsand in the specific policies and procedures theyapply in contract development, approval, andmonitoring. As a consequence, there are unevenefforts to provide tribes with technical assistanceto apply for these contracts, to negotiate con-tracts, and to manage these programs. Problemstribes claim to have experienced in applying forthese contracts include: 1) lack of encouragementand adequate technical assistance from area of-fice staff; 2) lack of cost data from area offices;3) difficulties in some areas in securing and hold-ing project support from 100 percent of the af-fected tribes (a particular problem in Alaska, withits many small native villages; and tribes canswitch their affiliation from one health consor-tium to another, as sometimes happens in Cali-fornia); and 4) apparent inconsistencies in areadecisions to approve or disapprove a proposal.
The contracts that are signed between IHS andthe tribes in the self-determination program varyfrom area to area in terms of the flexibility theypermit the tribes. Contracts in some areas specifyexactly what services will be provided, to whom,and in what manner. In other areas, comprehen-sive service delivery contracts allow more roomfor tribal adjustments. The voucher reimburse-ment system that is used by IHS, as opposed tothe BIA letter of credit approach, is the target ofmany complaints concerning delays and arbitrarydecisionmaking by area staff.
The appropriate instrument to execute the le-gal and financial relationship between IHS andthe tribes is a subject of disagreement. Contract-ing has been the predominant means, and grantshave been used sparingly to support developmentof tribal capabilities in preparation for contractmanagement. A new option known as a cooper-ative agreement is under consideration by IHS,but whether it would change the essential rela-tionship is unclear.
Although some area offices seem to fear thatthe tribes will expand and redirect services con-trary to the contract terms, the tribes cite man-agement difficulties that require innovative solu-tions and argue that flexibility is justified.Conflicts such as these aggravate other disincen-tives, such as the greatly increased administrative

Ch. 1—Summary and Conclusions ● 3 5
responsibilities of tribal governments and theiremployees (including full responsibility for col-lecting applicable third-party reimbursements),the need to develop or expand personnel manage-ment and fringe benefits programs, and additionalFederal reporting requirements. Self-determina-tion contracts give tribes greater control over theselection of health program employees and includethe option of maintaining or releasing staff whowere Federal employees; but they also place onthe tribe the burden of recruiting and retaininghealth professionals in locales that often are iso-lated, both physically and professionally.
Option 11: Clarify the intent and purpose ofthe Self-Determination Act.
It is the opinion of PHS that an IHS self-deter-mination contract project is legally an extensionof IHS itself. IHS is responsible for administer-ing these contracts on behalf of its parent agency,HRSA, according to applicable Federal contract-ing and procurement policies as modified by theSelf-Determination Act. Tribal contractors mustbe monitored to ensure that they adhere to theterms of their contracts. This interpretation allowslittle flexibility to the contractor to modify thescope of services it has agreed to deliver or to rede-fine its service population.
The purpose of the self-determination programas tribes see it is not contracting per se, which hasbeen an option for many years under “Buy In-dian” contracts, but self-determination. Tribescontend, with reason, that self-determination con-tracts are not supposed to be administered exactlyas other Federal contracts.
A variety of conflicts has developed over the10 years of IHS implementation of the Indian Self-Determination Act. Rather than attempting to re-solve each specific complaint, it would be morereasonable to work to clarify and reaffirm the in-tent of the law. The technical aspects of theadministrative and financial relationship betweenIHS and its tribal contractors are the subject ofa study by the General Accounting Office (GAO)that will be available sometime in 1986. The studyinvolves extensive field data collection, includinginterviews of tribal and IHS headquarters and areaoffice officials. The GAO study will generate spe-cific recommendations for improving the self-
determination contracting process. An evaluationof BIA’s implementation of the Self-DeterminationAct was completed in the summer of 1984 andidentified problems similar to those uncovered inOTA’s analysis of IHS’s implementation of thelaw (118).
Option 12: Develop a cost-accounting methodthat addresses the question of comparable fund-ing when tribes take over services previouslyadministered by IHS.
The adequacy of funding for self-determinationcontracts is perhaps the issue most frequently de-bated between the tribes and IHS. Aside from theproblem of the adequacy of IHS’s overall budget,there are disputes over the appropriate level offunding that should be provided to tribal contrac-tors. The law states that tribes should receiveresources equivalent to what IHS spends on a par-ticular package of services, but there is disagree-ment over what that amount should be, oftenfocusing on the issue of compensation for indirectcosts. What usually is meant by indirect costs isthe administrative and support costs that are pro-vided to IHS in its function as part of the Federalbureaucracy but all of which are not reflected inIHS’s clinical services budget. These costs, whichnevertheless become part of the tribal contractor’sresponsibilities, include employee fringe benefitspackages; malpractice and other insurance cov-erage; costs of leasing facilities; technical staff foraccounting, procurement, and data management;and other functions.
There appears to be disagreement about howindirect costs are determined , and no researchhas been done in IHS to determine a reasonablerange of indirect costs. Early tribal contractorswere awarded indirect costs in addition to theservice delivery contract, but this additional fund-ing is no longer available. Tribes therefore believethat they are being asked to absorb these costs,which cut into their direct care awards.
Option 13: Revise the retrocession provision sothat a year’s notice, instead of the present 120days, must be given before a tribe can return themanagement program to IHS.
Another factor is the belief of tribes that astribal contract activity increases, IHS area office

36 ● Indian Health Care—
staff should be reduced so that more funds can a stable area office staff. Extending the notifica-be devoted to direct care and tribal programs. IHS tion period for retrocession would ease this situ-argues that monitoring of tribal contractors re- ation somewhat.quires area office staff, and that the provision al-lowing tribes to retrocede a contract with only
The issues and their related options are sum-
120 days’ notice also necessitates maintenance ofmarized in table 1-2.
OTHER ISSUES
Several other issues that have or may have sig-nificant effects on the Federal-Indian relationshipand the provision of health services to Indians de-serve explicit recognition in this summary. Theseissues are: 1) Indian demographics and urban In-dian health programs, 2) congressional control ofFederal Indian health care policies, and 3) man-agement issues concerning IHS.
Indian Demographics and UrbanIndian Health Programs
One of the more difficult issues in providinghealth care to Indians is the basic question of whoshould be eligible for services. Yet, IHS must de-velop uniform standards for eligibility, which attimes has led Congress to legislate exceptions tothese regulations.
The issue of who is an “Indian” for the purposeof Federal health care benefits will be an increas-ingly difficult one as time passes. Even land-based,reservation Indians will not be immune to thesechanges. Marriage to non-Indians and migrationaway from the reservation to seek better employ-ment opportunities will require tribes to make in-creasingly difficult decisions on who is a mem-ber of their tribe. Even for Indians who marryother Indians, their prospects for marrying an In-dian from the same tribe are diminishing, and itis not improbable that a large number of non-tribal member Indians will result who will havemore Indian blood than the average tribal mem-ber. Already, some tribes have had to reduce theirtribal-specific blood quantum requirements formembership.
In the 1980 census, almost two-thirds of the 1.4million persons identifying themselves as Indianslived off reservations, tribal trust lands, or other
Indian lands. Of the 1.4 million Indians, 54 per-cent lived in metropolitan areas, and 59 percentwere included in IHS’s estimated service popula-tion. About 10 percent of Indians were living onor near reservations that were in or contiguousto metropolitan areas, and these Indians wereserved by IHS or tribal facilities.
However, IHS-supported programs for urbanIndians have always been viewed as a separateactivity from IHS’s reservation-oriented directservices system. In 1972, IHS began to fund ur-ban programs through its community develop-ment branch under the general authority of theSnyder Act. Appropriations were subsequentlyderived from the Indian Health Care ImprovementAct of 1976, which authorized urban Indian orga-nizations to contract with IHS to operate healthcenters and to increase accessibility of Indians topublic assistance programs. There were 37 pro-grams in 20 States in 1984.
A major distinction from IHS’s direct servicesprogram is the urban programs’ emphasis on in-creasing access to existing services funded by otherpublic and private sources, instead of IHS’s pro-viding and paying for those services directly.Thus, IHS funds have provided an average of 51percent of total urban Indian health programfunds. Most of the programs offer a variety ofsocial services and are “human service organiza-tions. ” Thirty-two percent of the reported urbanprogram encounters in fiscal year 1984 were med-ical; 10 percent were dental; 27 percent werehealth-related (health education, nutrition, men-tal health, optometry, and substance abuse pro-grams); and 31 percent represented other commu-nity service contacts.
Urban Indian health programs serve both In-dians and non-Indians. IHS regulations do not

Eligibility and entitlement
Current situation:Persons of Indian descent, no blood quan-tum requirement. For services purchased byIHS from non-IHS providers, additional re-quirement that the individual must live onor near a federally recognized Indian reser-vat ion.
IHS proposed change:Eligible persons would have to be eithermembers of federally recognized tribes andhave at least one-quarter Indian blood, orother Indians of at least one-half Indianblood. In addition, eligible Indians must liveon or near a federalIy recognized Indian res-ervation.
OTA options:#1: IHS or Congress could develop a priority
system for access to IHS services.#2: IHS or Congress could use blood quan-
tum criteria to supplement rather thanrestrict eligibility criteria based on tribalmembership.
#3: If eligibility criteria are made more re-strictive, Congress could make IHS serv-ices less a residual source of care andmore an entitlement program.
SOURCE Off Ice of Technology Assessment
Table 1-2.—Major Issues and Related Options
Resource allocation andscope of services Availability and adequacy of resources Self-determination—
IHS does not provide the same healthservices In each of Its service areas, andservice area budgets are determined ona “historical” or “program continuity”basis.
“Equity fund” of from $5 to $9 millionper year (less than 2 percent of IHS’s to-tal clinical services budget) allocated ona needs-based formula to most-deficientservice units; equity awards becomepart of future base budgets.
Equity fund approach would be appliedto any future increases in appropri-ations
#4: Continue with the modest, incre-mental approach to resource redis-tribution that IHS has implemented.
#5: Accelerate the rate of reallocatingfunds among IHS service areas.
#6: Work toward a common m i n i m u mservices package for all IHS serviceareas.
Minimal negotiations by IHS contract careprograms with non-lHS providers on ratesof payment
Will initiate negotiations with IHS’s contrac-tors to accept payment at no more than theMedicare-allowable rate.
#7: Negotiate payment rates with contractcare providers instead of paying 100percent of billed charges, and imposea rate structure on IHS contractors,such as use of Medicare DRG (diagno-sis-related groups) rates.
#8: Authorize IHS service units to carryover a percent of contract funds fromone fiscal year to the next.
#9: Provide greater IHS headquarters andarea office support to service unit con-tract care programs in dealing with al-ternative resources, both public (espe-cially State Medicaid programs) andprivate.
#10: Explore the possibilities of developinglong-term relationships with commu-nity facilities and of providing moreservices to non-lndians.
Federal Government emphasizes its fis-cal responsibilities for funds administeredunder 638 contracts. Indian tribes empha-size self-determination objectives and ex-ceptions to Federal contracting rules.
Major issue involves level of funding fortribes to provide the same level of servicespreviously provided under IHS management,and to cover Indirect costs such as liabilityinsurance.
New tribal contractors would be provided in-direct costs up to 14 percent; source offunds not yet determined.
#11: Clarify the intent and purpose of theSelf-Determination Act.
#12: Develop a cost-accounting method thataddresses the question of comparablefunding when tribes take over servicespreviously administered by IHS.
#13: Revise the retrocession provision sothat a year’s notice, instead of the pres-ent 120 days, must be given before atribe can return program managementto IHS.
—

38 • Indian Health Care
prohibit its urban programs from serving non-Indians, and funding from other Federal sourcesoften requires urban Indian programs to serve cer-tain populations that include non-Indians. Hence,the only requirement that IHS has required is thatthe number of Indians served by each programbe proportional to the amount of money providedby IHS.
Support by IHS for urban Indian programs hasraised conflicts in the Indian community, and theAdministration has consistently tried to end fund-ing of these programs, claiming that alternativeresources are adequate for urban Indians. The Na-tional Tribal Chairmen’s Association, for exam-ple, supported efforts to assist Indians in Indiancommunities and urban areas but felt that non-tribal organizations, such as the nonprofit corpo-rations that operate urban Indian programs,should coordinate the services they provide forIndians with tribal governments and elected In-dian officials (93). Leaders of several urban In-dian organizations, on the other hand, point outthat in some urban centers, there are as many as40 tribal governments nearby, and representationof tribes on urban Indian program governingboards might include over 80 different tribes. Ur-ban Indian organizations also feel that the Fed-eral Government must provide health care andsocial services to Indians regardless of their cho-sen residence (4). As for the claim that alterna-tive resources are adequate, the Administrationhas never documented that claim. Moreover, IHSfunds serve as core funding that enables the ur-ban programs to seek out and qualify for othersources of care. Considering the modest funds thathave been appropriated for these programs, pastgovernment policies (e.g., allotment and termina-tion) that broke up tribes and encouraged Indiansto leave the reservation, and the use of IHS fundsto help urban Indians qualify and gain access toother resources, these activities appear to be a log-ical and appropriate response that is not at crosspurposes with IHS’s reservation-oriented directcare system.
Congressional Control of FederalIndian Health Care Policies
The Snyder Act of 1921 remains the basic au-thorizing legislation for Indian social services pro-
grams, including health services. Other statutesthat have been relevant to the provision of healthservices to Indians are: 1) the Johnson O’MalleyAct of 1934, which authorized contracts betweenthe Federal Government and State and local gov-ernments to provide health care and other socialservices to Indians; 2) the Transfer Act of 1954,which transferred health care functions from theDepartment of the Interior’s Bureau of Indian Af-fairs to the Public Health Service in the precur-sor to the current Department of Health and Hu-man Services; 3) The Indian Health Facilities Actof 1957, which authorized IHS to contribute tothe construction costs of community hospitals ifthat was a more effective alternative to direct con-struction of facilities for Indians; 4) the IndianSanitation Facilities and Services Act of 1959, au-thorizing IHS to provide sanitation facilities to In-dians; 5) the Indian Self-Determination and Edu-cation Assistance Act of 1975, which authorizedBIA and IHS to turn over responsibilities for In-dian programs to the tribes; and 6) the IndianHealth Care Improvement Act of 1976 (reauthor-ized in 1980, passed again by Congress in 1984with additional provisions but vetoed by thePresident, and extended through fiscal year 1986by continuing resolution of Congress [H.R. Res.465]).
These statutes provide the basis for Federal In-dian health care, but the Snyder Act and the In-dian Health Care Improvement Act have been theprincipal statutes authorizing health services toIndians. Without reauthorization of the IndianHealth Care Improvement Act, congressional in-fluence over Indian health care policies maydiminish with only the general language of theSnyder Act as the statutory basis for definingwhat health care the Federal Government will pro-vide to Indians. This impact can be expected toextend to the judicial system’s role in resolvingIndian health care issues, because much of thecourts’ role is in interpreting the congressional in-tent behind a statute. If explicit congressionaldirectives on the kinds of programs the FederalGovernment should be conducting are lacking,the Administration will have much more discre-tion in determining what health benefits it willprovide,
Congressional direction on Federal Indianhealth care will be especially crucial in the Fed-

Ch. 1—Summary and Conclusions ● 3 9
eral budget climate of the next 5 to 10 years. Un-like the previous three decades, where attentionwas primarily directed at adding new initiatives,hard choices will most likely have to be madeamong Indian health care programs, either interms of discontinuing some activities outright,or in determining which activities should be cutback more severely than others.
Indian Health ServiceManagement Issues
It has not been the purpose of this OTA assess-ment to evaluate IHS management practices andinformation systems. In fact, when managementissues arose during the course of this assessment,OTA suggested that GAO was the proper agencyto be involved, a suggestion that in part led tothe concurrent study by GAO on managementpractices in the self-determination contract pro-gram. Nevertheless, after a year’s experience inworking with a variety of IHS offices and staff(primarily at or through IHS headquarters) to ob-tain data, some general observations about IHS’sdata systems can be made.
First, however, it would be helpful to identifyat least two other management issues facing IHS.These issues involve: 1) where in the Departmentof Health and Human Services IHS should be lo-cated, and 2) growing personnel problems in IHS.
The location of IHS in DHHS was an issue thatwas addressed by Congress in the vetoed 1984amendments to the Indian Health Care Improve-ment Act. In fact, the provision in the amend-ments elevating IHS to a higher level within PHSwas one of the reasons the President vetoed thebill. Within the Department of the Interior, BIAis a separate agency solely concerned with Indianaffairs. IHS, whose responsibilities were trans-ferred to PHS from BIA in the mid-1950s, is cur-rently part of HRSA, one of five Federal agen-cies that comprise PHS (the other four are theNational Institutes of Health; the Centers for Dis-ease Control; the Food and Drug Administration;and the Alcohol, Drug Abuse, and Mental HealthAdministration). IHS represents the bulk ofHRSA’s direct health care activities and approxi-mately 35 percent of the total HRSA budget, andis the largest Federal health care system after those
of the Department of Defense and the VeteransAdministration. Thus, in terms of access to higherlevels within PHS and DHHS and accountabilityto organizations at lower levels (i.e., HRSA),IHS’s position is not comparable to the positionenjoyed by BIA in the Department of the Interior.The attempted elevation of IHS through the ve-toed amendments was based on the premise thatIHS would have greater access to higher levelswithin DHHS, and that there would also be lessduplication and clearer requirements for the pa-perwork that accompanies program administra-tion and receipt of IHS funds.
Indians are given preference in employmentwith BIA and IHS. This preference given to In-dians is in contrast to the relative preference givento veterans for Federal employment by the “point”system. Indian preference applies to all BIA andIHS positions, whether for initial hiring, reinstate-ment, transfer, reassignment, promotion, or anyother personnel action intended to fill a vacancy(42 CFR 36.42). This preference is also applied totribally administered programs, although in a lessstrict manner, with the regulations stating thattribes may hire non-Indians “after giving full con-sideration to Indians” (42 CFR 36.221).
The positive and negative effects of Indianpreference have never been formally assessed, butone consequence is that non-Indian BIA and IHSemployees have limited opportunities for ad-vancement, and this limitation is increasing. Nec-essary recruitment of highly qualified non-Indianswill become increasingly difficult, and few willcontemplate more than temporary employmentbecause their career opportunities will be severelylimited.
For the Indian BIA or IHS employee, a grow-ing issue may well be that of conflicting roles—as a representative of the Federal Government inits relationship with Indians and as an advocatefor increasing Federal benefits for Indians. For ex-ample, IHS is presently viewed by its parent orga-nization (PHS in DHHS) as an advocate for itsclients.
A different personnel issue concerns the im-pending end of a very important source of phy-sicians and other health professionals from theNHSC scholarship program, which has given IHSfirst priority when the time comes for these profes-

40 Ž Indian Health C a r e
sionals to repay their obligation through servicein health manpower shortage areas. As mentionedpreviously, after 1990, IHS cannot expect newrecruits from this source. Furthermore, the PHSCommissioned Corps will have a difficult time instaffing IHS, as that program also is not as at-tractive to professionals now that there is no mil-itary draft (service in the Corps was equivalentto active duty in the military). The Indian HealthCare Improvement Act established scholarshipprograms for Indian health professionals, but thatactivity, although important in developing an In-dian health professional cadre, cannot be expectedto substantially replace NHSC and CommissionedCorps anytime in the near future. Thus, a seri-ous problem for maintaining IHS direct servicesis staff shortages, and innovative approaches mustbe explored to address this problem.
Turning finally to IHS’s data systems, O T Afound an array of uncoordinated service-specificdata systems that have developed over the yearsin response to particular information needs. Thedelegation of most management responsibilitiesto IHS area offices has contributed to a lack ofincentives to establish complete and consistent in-formation for all 12 IHS areas. The difficultiesOTA had with evaluating the high-cost contractcare cases illustrate this problem.
Another major impediment to the generationof complete and consistent IHS data is the exemp-tion of self-determination contract programs andurban Indian health projects from IHS data re-porting requirements. Tribal participation in ex-isting IHS data systems is voluntary, and mosttribal contractors do not operate within IHS sys-tems. The lack of clinical, utilization, and man-agement data due to nonparticipation in IHS data
systems is a serious problem and will becomeworse as more services are transferred to tribalmanagement, unless an IHS policy of November1985 requiring participation in essential data sys-tems is enforced. Lack of data was a particularlydifficult obstacle in OTA’s attempts to comparefunding, utilization, and health status among In-dians in the 12 IHS areas (particularly those heav-ily dependent on self-determination contracts).
It is likely that much more information couldbe derived from existing IHS data systems thancurrently is being sought and provided. A greatamount of data is being collected by IHS, butthere is no overall framework or purpose guid-ing that data collection and its use. An assessmentand coordination of existing data systems couldbe undertaken as an interim solution while plan-ning for implementation of a more rational andcost-effective system takes place. Such planningnow is underway, and IHS budget proposals forfiscal year 1987 include earmarked funds for IHSdata system implementation. In IHS, however,where resources for services delivery are seen aschronically inadequate, any funds spent on datasystems are likely to be viewed as better spent ondirect services. This attitude certainly would bemore pronounced among tribal contractors, whoalready view their budgets as inadequate for di-rect services.
Agreement by all parties concerned on the va-lidity and comprehensiveness of data on the In-dian population, their health status, and on theavailability and use of services among the 12 IHSservice areas, is a necessary precondition to thekinds of negotiations that will be taking place be-tween Indian tribes, Congress, and the Adminis-tration in the coming years.

Chapter 2
The Federal= lndian Relationship

Contents
Overview . . . . . . . . . . . . . . .Eligibility for Federal Services . . . . . .
Federally Recognized Tribes . . . . . .Eligibility of Indian Individuals for
. . . . . . .
. . . . . . .. . . . . . ,. . , . . . ,
. . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . .Is the Indian HealthConclusions . . . . . . .
Service. . . . . . .
a Primary or Residual Health Care Provider?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Page● ✎ ✎ ✎ ✎
✎ ✎ ✎ ✎ ✎
✎ ✎ ✎ ✎ ✎
✎ ✎ ✎ ✎ ✎
✎ ✎ ✎ ✎ ✎
✎ ✎ ✎ ✎ ✎
434646485253

Chapter 2
The Federal= lndian Relationship
HISTORICAL OVERVIEW
Most colonial powers followed some variationof the “doctrine of discovery” and “aboriginal ti-tle” in their land dealings with Indians. Europeansconsidered Indian political-tribal units as holdingsomething akin to “use rights” over their tradi-tional territories, with the ability to transfer validtitle to the arriving nations. Under the “doctrineof discovery, ” the nation with the first contactcould acquire title from individual Indian tribes.Individual settlers had no rights to acquire landfrom Indians and could only acquire land throughtheir sovereign.
This land acquisition system was a critical partof the relationship that eventually was establishedbetween the United States and the Indian tribes.Tribes and their members were treated as sepa-rate and legally different from other people in-habiting the continent. Great Britain and, later,the United States, assumed the obligation to pro-tect the tribes. (For example, the Royal Procla-mation of 1763 acknowledged tribal rights to pro-tection of their lands, borders, and the removalof non-Indians. ) In addition to practices maintain-ing tribal separatism, the Federal Governmentsought to “civilize” Indians, which included Euro-pean forms of education and farming, and conver-sion to Christianity. Thus, non-Indian govern-ments gradually assumed responsibilities thatwent beyond overseeing only the physical assetsof the tribes.
The policies that the United States would adopttoward Indian tribes and their members were care-fully considered by the Founding Fathers. GeorgeWashington was of the view that the United Statesneeded to protect Indians from the “avarice” ofnon-Indians and observed that it also was goodpolicy to be on friendly terms with the Indians(103). This viewpoint was codified in the North-west Ordinance and the Indian Trade and Inter-course Act of 1790 and was reflected in the seriesof treaties that the United States entered into withthe tribes following the Revolutionary War.
Treaties became a major basis for the legal rela-tionship of the newly formed United States withthe Indian tribes, including the obligation of theFederal Government to provide services. Havinga treaty that specified some form of health carewas, however, not a prerequisite for a tribe to re-ceive health services. By the mid-19th century,appropriations for Indian health care had becomeroutine. About half of the approximately 70 In-dian agencies had a doctor on its staff (217). In-dian agents, the local representatives of the Fed-eral Government, were judicially determined tohave inherent or discretionary authority to pro-vide medical services to tribes under their con-trol (125).
Treaties were the exclusive responsibility y of theSenate, but by 1871, the treaty-making period hadended as the House of Representatives sought in-creased involvement in the agreements with In-dian tribes. Thereafter, both the House and theSenate would deal with the tribes by statute ratherthan by treaty (23,210). It is important to notethat at the time treaty-making ended, the Stateswere almost entirely excluded from any involve-ment in Indian affairs, and Indian tribes func-tioned as political units in their relationships withthe government of the United States. Moreover,almost no attention was paid to individual Indiansby the United States; they were the responsibil-ity of their tribes. Indians were not citizens of theUnited States and as individuals had almost norights within the legal system of the United States.
The allotment period began a decade after theend of treaty-making, with the Federal relation-ship with Indians shifting from that of a govern-ment dealing with another government to a newstratagem that was anti-tribal government. Allot-ment essentially broke up tribally held commu-nal lands. (Although there were a number of al-lotment acts, the classic is the Dawes Act [24 Stat.388 (1887) ].) Although many tribes existed in de-
43

44 ● Indian Health Care
plorable conditions, they existed on lands wantedby settlers, miners, and other economic interests.
Assimilation, often referred to as “civilization”of individual Indians, became the dominant thrustof the Federal allotment policy (35,102). Eachadult was assigned a specific amount of land (usu-ally 160 acres), and some relatively small amountof land was set aside for tribal purposes (schools,cemeteries, and the like). The “excess lands” re-maining were opened to non-Indian settlement.Indian land was to be held in trust, as were theproceeds from the sale of “excess lands, ” for alimited period of years. The theory was that dur-ing this trust period individual Indians would be-come farmers and leave their Indian ways. Theywere to be emancipated from their tribes and be-come eligible for U.S. citizenship.
During the allotment period, the Bureau of In-dian Affairs (BIA) became the dominant institu-tional force on Indian reservations (54). The bu-reau, along with missionaries, were to civilize theIndians. Along with the expansion of social serv-ices to the tribes, the bureau actively suppressedtraditional modes of tribal governance, Indian lan-guages, and Indian religious and cultural prac-tices, Thus, education, medical services, law en-forcement, and all components of governmentbecame an aggressive part of the Federal defini-tion of its trustee role to “civilize” Indians.
The first Indian hospital was built in Pennsyl-vania, where there were no reservations, in con-nection with the Carlisle Indian Boarding School.Carlisle was the prototype boarding school whereIndian children who had been removed from theirreservations were to be “civilized” in the absenceof tribal influences. By the turn of the century,a total of five hospitals had been constructed toserve Indians. None of the five had a specific au-thorization or appropriation from Congress (217).Health services were seen as a natural and neces-sary part of the “civilizing” function that the Na-tion had adopted.
By the early 1900s Congress began to passdisease-specific legislation. In 1906, Congress be-
gan the effort against tuberculosis among Indians(34 Stat. 325, 328 [1906]). In 1909, programsagainst trachoma were begun (35 Stat. 269, 271[1909]).
The 1920s provided several events of signifi-cance to Indians. They became citizens of theUnited States through the Citizenship Act of 1924(8 U.S.C. section 1401 b). The Snyder Act, the ma-jor basis for Federal health and social services forIndians, was enacted in 1921 (25 U.S. C. section13), and the congressionally commissioned MeriamReport of 1928 was influential in changing thecourse of Federal-tribal relations.
The Snyder Act of 1921 was passed to provideauthorizing legislation for appropriations thatCongress had been providing for some time, butwithout specific statutory authority. The entireact (except for a 1976 amendment making post-secondary Indian schools eligible for participationin the Higher Education Act of 1965) reads as fol-lows (25 U.S.C. section 13):
The Bureau of Indian Affairs, under the su-pervision of the Secretary of the Interior, shalldirect, supervise, and expend such moneys asCongress may from time to time appropriate, forthe benefit, care, and assistance of the Indiansthroughout the United States for the followingpurposes:
General support and civilization, includingeducation.
For relief of distress and conservation of health.For industrial assistance and advancement and
general administration of Indian property.For extension, improvement, operation, and
maintenance of existing Indian irrigationsystems and for development of watersupplies.
For the enlargement, extension, improvement,and repair of the buildings and grounds ofexisting plants and projects.
For the employment of inspectors, supervisors,superintendents, clerks, field matrons,farmers, physicians, Indian police, Indianjudges, and other employees.
For the suppression of traffic in intoxicating liq-uor and deleterious drugs.

Ch. 2—The Federal-Indian Relationship ● 4 5
For the purchase of horse-drawn and motor-propelled passenger-carrying vehicles forofficial use.
And for general and incidental expenses in con-nection with the administration of Indianaffairs.
Utilizing the Meriam Commission’s report, theNew Deal proposed extensive legislation for thelong-term renewal of tribal governments. Assimi-lation was still an underlying, ultimate goal, butit was to be achieved by Indians operating throughtheir own systems.
A number of legislative proposals were enactedinto law by Congress in the 1930s. The Indian Re-organization Act of 1934 (25 U.S. C. sections 461,et seq. ) ended allotment, extended the trust in-definitely, established federally chartered corpo-rations for tribes to reorganize into, and estab-lished economic development programs for tribes,The Johnson O’Malley Act of 1934 (25 U,S.C. sec-tions 452, et seq. ) authorized the Federal Govern-ment to contract with agencies, including Stateagencies, to provide services (including medicalservices) to Indians. The Johnson O’Malley Actdid two things of major consequence: it providedfor expanded health services to Indians and estab-lished the first real mechanism for State involve-ment with Indian health care.
Following World War II, Federal-Indian pol-icy again changed course, reversing the policiesof the New Deal toward what was eventually con-demned as “termination. ” Termination had sev-eral components: 1) the induced resettlement ofthousands of reservation Indians into urbancenters where they were to be trained and em-ployed; 2) the transfer of major functions, respon-sibilities and jurisdiction over Indians to Statesfrom the Federal Government (18 U.S. C. section1162; 28 U.S. C, section 1360); and 3) terminationof the Federal relationship with specific tribes, in-cluding ending services and distributing tribal as-sets to individual tribal members.
Indian hospitals were closed, and there was in-creased emphasis on transferring service respon-sibilities to the States. California, for example,requested that the Federal Government cease pro-
viding health care to Indians residing in that State.In part, the terminationist thrust was responsiblefor the transfer of the responsibility for Indianhealth care away from BIA in the Department ofthe Interior to the Public Health Service in whatwas then the Department of Health, Education,and Welfare (42 U.S. C. sections 2001, et seq.).
The termination period was in turn replaced bythe current phase of Federal-Indian relationships,commonly known as Indian Self-Determination.But termination had created profound changes inthe demographics and definitions of Indians. Hun-dreds of thousands of Indians who were membersof recognized tribes no longer resided on reser-vations or even near reservations. Thousands ofother Indians had been declared to have been ter-minated by acts of Congress and no longer werefederally recognized Indians.
The modern self-determination era began atroughly the same time as the major expansion ofFederal programs and services that characterizedthe “Great Society. ” This recent self-determinationera has been characterized by a general revitali-zation of tribal governments and a large increasein Indian-related litigation. Two statutes havebeen of special importance. The Indian Self-Determination and Education and Assistance Actof 1975 (25 U.S. C. sections 450, et seq. ) providedfor the transfer to tribes of functions that werepreviously performed by the Federal Government,including the provision of health services. Theother statute, the Indian Health Care Improve-ment Act of 1976 (25 U.S.C. sections 1601, etseq.), was the only Federal statute to clearly re-flect Congress’ view on health care for Indians andwas, in effect, a clarification of the Federal respon-sibilities recognized by the Snyder Act. The ln-dian Health Care Improvement Act states that (25U.S.C. section 1602):
The Congress hereby declares that it is the pol-icy of this Nation, in fulfillment of its specialresponsibilities and legal obligation to the Amer-ican Indian people, to meet the national goal ofproviding the highest possible health status to In-dians and to provide existing Indian health serv-ices with all resources necessary to effect thatpolicy.

46 • Indian Health Care—
ELIGIBILITY FOR FEDERAL SERVICES
Federally Recognized Tribes
Membership in a federally recognized tribe isthe single most common standard for determin-ing eligibility for Federal services. Therefore, thequestions of what is a tribe, and for what pur-poses, need to be addressed.
Tribes were defined early in the Nation’s judi-cial history in Worcester v. Georgia (220), andalthough modified by many cases, the definitionremains applicable:
Indian tribes are “distinct, independent polit-ical communities possessing and exercising thepower of self government . . .“
The tribe, whether denoted as a band, nation,rancheria, Pueblo, community, or native village,is the only self-governing political unit that rep-resents Indians within the Federal-Indian relation-ship. Conceptually, whatever rights exist for in-dividual Indians in the Federal-Indian relationshipare derived from tribal membership.
The seeming purity of the concept, however,has been muddled by the pendulum swings in Fed-eral laws and policies toward Indians. The al-lotment period left a legacy of vested rights inindividual Indians with respect to part of the res-ervation lands. The 1934 Indian ReorganizationAct created additional definitions of Indians in itsattempt to assist tribes. Still later, termination cre-ated a situation in which persons who racially andculturally had remained Indian no longer had apolitical entity (the tribe) representing them thathad any legal/political relationship with theUnited States. As a result, these Indian individ-uals for the most part lost their rights to servicesprovided to Indians. Relocation created a situa-tion in which Indians who retained their tribalmembership might no longer be located near thenetwork of reservation-based services that hadbeen created. Finally, the explosion of social serv-ice and poverty-oriented programs in the 1960sand 1970s sometimes included tribes and some-times did not. Some of these programs extendedeligibility to Indian individuals who did not qual-ify for Federal services that were directed attribally affiliated Indians.
With the exception of non-Indians appointedto represent Indians in some trustee capacity, theentity that represented Indians was whatevergoverning body the particular band, tribe, or con-federacy of Indians set for itself. In dealing withthe Federal Government, however, competing oreven bogus entities became an issue in determin-ing who spoke for particular groups of Indians.During the treaty period, unscrupulous negotia-tors on the part of the United States would some-times choose or bribe individual Indians to serveas “official” representatives for the tribe involvedin the treaty. The treaty that was so negotiatedwas allowed to stand, even though the individ-uals involved often did not in fact represent thetribe in question. Whomever the United Stateschose to deal with became the official tribe in theeyes of the U.S. legal system. This outcome is notdissimilar to those in international relations,where the United States or other governmentsmay deny formal recognition to a government ifthey prefer to recognize a different or prior gov-ernment. (For example, for more than 20 yearsthe United States recognized the Nationalist Chi-nese Government of Taiwan, but not the People’sRepublic of China, as representing “China.”) Suchmatters are viewed by the courts as political ques-tions and generally are not held to be reviewable.Currently, there still are tribes with governingbodies that have been recognized by the UnitedStates but which have other, often-times tradi-tional, governing bodies in existence.
Individual bands and tribes that were placedon a single reservation have also been consoli-dated into new political units corresponding tothe larger reservation community, such as theConfederated Tribes of the Colville Reservationor the Three Affiliated Tribes of the Fort BertholdIndian Reservation. Generally, the treaty, stat-ute, executive order, and/or constitution of thetribe or tribes involved will delineate who is theresponsible governing body, and that documentor documents will be controlling in determiningwho is the official tribal government. Thesemergers or consolidations of preexisting tribes orbands, however, have not always been success-ful. There are situations that have completely

Ch. 2—The Federal-Indian Relationship ● 4 7
paralyzed reservation communities and preventedany entity from effectively serving as a tribal gov-ernment. Such situations may require congres-sional adjustment of the affected reservation.
Once a tribe has been recognized as a tribe bythe United States, it does not lose its status un-less the United States terminates the political rela-tionship. Although it is not always clear howsome tribes became federally recognized andothers did not, Federal recognition of a tribe isthe key ingredient for access to most Federal serv-ices that are provided on the basis of the Federal-Indian relationship. Early statutes rarely provideddefinitions of Indians or tribes and simply referredto either a particular tribe or to Indians generally.It was quite clear to everyone involved in thoseearlier days who the tribes were and who was anIndian.
Most of the modern statutes that provide serv-ices to Indians as part of the Federal-Indian rela-tionship follow a fairly standard definition of anIndian tribe, The Indian Health Care Improve-ment Act contains the following definition (25U.S.C. section 1603d):
“Indian tribe” means any tribe, band, nation,or other organized group or community, includ-ing any Alaskan Native Village or group or re-gional or village corporation as defined or estab-lished pursuant to the Alaska Native ClaimsSettlement Act (85 Stat. 688) [43 U.S.C. sec. 1601et seq.], which is recognized as eligible for thespecial programs and services provided by theUnited States to Indians because of their statusas Indians.
Given this somewhat circular definition of anIndian tribe as one recognized by the United Statesas an Indian tribe, the issue is: Who are the rec-ognized tribes? Where either a statute, treaty, orhistorical relationship clearly has linked the UnitedStates with the governing body of a tribe, thattribe is usually a recognized tribe for the purposesof the Federal-Indian relationship. For the rest ofthe groups of Indians, the issue is more com-plicated.
One case that addressed this issue was UnitedStates v. Washington (126), in which the courtfound that neither Congress nor the executivebranch has prescribed any standardized definition
for either the term “Indian” or “Indian tribe” interms of the special Federal relationship with In-dians (126). The case involved a determinationof which descendants of groups that were partiesto the various western Washington fishing trea-ties were tribes for the purpose of sharing in thetreaty rights. The Federal District Court Judgestated in his conclusion (126):
In determining whether a group of personshave maintained Indian tribal relations and atribal structure sufficient to constitute them asan Indian tribe having a continuing special po-litical relationship with the United States, the ex-tent to which the group’s members are personsof Indian ancestry who live or were brought upin an Indian society or community, the extentand nature of the members’ participation in tribalaffairs, the extent to which the group exercisespolitical control over a specific territory, the his-torical continuity of the foregoing factors and theextent of express acknowledgment of such po-litical status by those Federal authorities togetherwith the power and the duty to prescribe oradminister the special political relationships be-tween the United States and Indians are all rele-vant factors to be considered.
The judge found on the basis of this reasoning thatnone of the Indian groups petitioning to intervenein United States v. Washington (126) were Indiantribes. They were Indian descendants or groupsthat had participated in the treaties, but they werenot tribes, and their members, although raciallyIndian, were not Indians with respect to the Fed-eral-Indian relationship. To the extent that theseindividuals were eligible for any Federal services,specific statutory authorization would need to befound.
Contemporaneous with the decision in UnitedStates v. Washington, in 1978 the Department ofthe Interior issued in final form its first formalmechanism for determining whether a group wasan Indian tribe for the purpose of the Federal-Indian relationship (25 CFR 54). (Congress, ofcourse, did not give up its authority to recognizespecific tribes by statute; e.g., the Maine ClaimsSettlement Act [25 U.S.C. sections 1721, et seq. ].)These regulations created what is known as theFederal Acknowledgment Process and set out thecriteria that petitioning groups would have to

48 ● Indian Health Care
meet to receive Federal recognition. In generalterms, petitioners would have to show that theIndian group (141):
had been identified as Indian from historictimes to the present on a substantially con-tinuous basis;had occupied a specific geographic area orcommunity distinct from other populationsin the area, and its members are descendantsof an Indian tribe that historically inhabiteda specific area;had maintained tribal political authority overits members as an autonomous entity through-out history;had governing procedures pertaining tomembership;had a membership role that was historicallytraceable to the historical entity definedabove;had no members who were primarily of anyother tribe; andhad not been legislatively terminated.
criteria have not been easy to meet, and theAcknowledgment Process has not resulted in thespeedy determination of which Indian groupsshould be recognized as tribes.
In addition to federally recognized tribes andgroups that have not been recognized, there aretribes that have been terminated. Termination wasa legal process where by statute, the United Statessevered its ties with particular tribes. Termina-tion is now a discredited Federal policy, but, aswith all Federal Indian policies of the last two cen-turies, the negative effects linger. Many termi-nated tribes remain terminated; their members arenot “Indians” for the purpose of Federal programs.Several tribes, however, have been statutorilyrestored by Federal legislation to their previousstatus as federally recognized tribes (e. g., theMenominee Tribe of Wisconsin). In addition tothose few tribes that have been statutorily re-stored, the termination of many of the Califor-nia tribes and rancherias has been held to be defec-tive by the Federal courts, and these tribes retaintheir service rights.
There are also a host of Indian organizations—formal, informal, statutorily created, statutorilyacknowledged, or creatures of tribal government
—that are not tribes. Membership in any suchorganization is not the same as membership in afederally recognized tribe, and no generic rightsare conferred by membership. To the extent thata role is provided for any particular organization,that role is specific and, unlike tribes, no inher-ent governmental power is inferred. For example,the statute on Indian education (25 U.S. C. sec-tion 2019) defines both agency school boards andIndian organizations and delineates the specificfunctions each will assume in the BIA educationsystem. In the health area, the Indian Health CareImprovement Act acknowledged urban Indianhealth programs (they were begun under the gen-eral authority of the Snyder Act) and authorizedfunds for them. Urban Indian organizations oper-ating these programs are recognized as having dis-tinct and specific roles in the delivery of healthcare to Indian people in urban settings (25 U.S. C.sections 1651-1658).
Eligibility of Indian Individuals forFederal Services
For most of the years that the Federal Govern-ment has been providing services to Indians, thequestion of who was an Indian was not particu-larly significant. Such questions most frequentlyarose in determining whether a particular individ-ual or class of individuals had been emancipatedfrom their tribal ways, or whether a particularindividual or class of individuals was subject toFederal criminal statutes that asserted Federaljurisdiction over Indians for some offenses.
Who was an Indian for the provision of healthservices was definitely not a significant issue. Fre-quently, appropriations language was so vaguethat it was BIA that determined who received ben-efits. The Federal bureaucracy that had developedto provide services to Indians became accustomedto determining the nature and scope of servicesthat the tribes were to receive.
Historically, during the period when tribes weredistinct and separate, who was an Indian was nota particularly difficult factual or legal question.Congress in the Snyder Act did not see any needto define “Indian” because at the time of the act(1921), services were only provided to those In-

Ch. 2—The Federal-Indian Relationship ● 4 9
dian tribes that were recognized as having a po-litical relationship with the United States.
Today r however, several hundred years ofshifting law and policy have generated differentcategories. For example there are, among othercategories, terminated, nonrecognized, and urbanIndians. The post-1960 statutes that authorizeservices pursuant to the Federal-Indian relation-ship do not really address the issue of who is anIndian because of the somewhat circular defini-tion described above,
Generally speaking, the political definition of“Indian” is the province of each Indian tribe. Thispower of tribes to define their membership hasbeen repeatedly recognized by Federal courts(20,28,98). Each tribe may use its own criteria,but for the most part, tribes have required somelevel of Indian blood of the particular tribe formembership. With the exception of a number oftribes without blood quantum requirements, mosttribes have at least a one-eighth blood quantumrequirement (129). Without specific Federal leg-islation that overrides or controls the membershipdetermination, the courts defer to the tribes (75).This is true even under the Indian Civil Rights Actof 1968 (25 U. S.C. sections 1301-1303), whichstates that no Indian tribe shall “deny any per-son within its jurisdiction the equal protection ofthe laws or deprive any person of liberty or prop-erty without due process of law . . .“ The courtswould not interfere in a case where only the chil-dren of male tribal members were eligible for tribalmembership in mixed marriage situations, andheld that such matters were within the authorityof the tribe to determine (74).
Congress, however, can and does expand ornarrow the definition of “Indian. ” Thus, it is im-portant to examine the specific purposes for whichthe definition of Indian is being used in given cir-cumstances.
Statutes that define who is an Indian may havebroad implications. A prime example is a statutethat either acknowledges the Federal-Indian rela-tionship with a tribe, or terminates that relation-ship. Other statutes that are part of the Federal-Indian relationship are more limited in their scope.For example, the definition that Congress used forNative Alaskans concerning the importation of
reindeer (25 U.S. C. section 500), although ap-propriate for this purpose, should have no par-ticular implications for the delivery of healthservices. Moreover, rolls established for the dis-tribution of monetary judgments awarded in casesof ancient Indian claims may include persons whoare not eligible for tribal membership accordingto the criteria that the tribe currently has in place.
There are also a host of Federal statutes thatprovide services to Indians and that contain vary-ing definitions of Indians and/or Indian tribes.Many of these statutes are not premised on theFederal-Indian relationship, and the services pro-vided to Indians are usually part of a larger pro-gram of which Indians are but one beneficiaryclass.
The Snyder Act contains no express statutorylanguage on who shall be eligible for IndianHealth Service (IHS) services other than “Indiansthroughout the United States. ” In the absence ofclear congressional direction, the question be-comes to what degree agencies can restrict or alterthe definition of who is an Indian.
The leading case in the area of agency discre-tion is the 1974 decision of Morton v. Ruiz (89).Ruiz, a member of a federally recognized tribe,had close ties with his reservation but lived offthe reservation in a nearby Indian community lo-cated on the former aboriginal lands of his tribe.He was denied benefits from a BIA programknown as General Assistance. The denial wasbased solely on the fact that he did not live onthe reservation. BIA’s authority to provide generalassistance to Indians is the Snyder Act, which doesnot contain any express limitations with respectto reservation residency. The Supreme Court,however, did not consider Morton v. Ruiz as acase where the statutory language was clear andcontrolling. Such an analysis by the Court wouldhave struck down any agency construction of thestatute that had the effect of narrowing the stat-utorily designated group of beneficiaries. Instead,the Supreme Court viewed the Snyder Act as anenabling act under which an agency would be al-lowed significant discretion in determining thescope of programs.
The Government urged in Morton v. Ruiz thatunder a previous ruling giving great discretion to

50 ● Indian Health Care
administrative agencies (42), agencies should beallowed great latitude in implementing their gov-erning statutes. The Government also assertedthat the limitation of services to reservation resi-dents was required, given the limited appropria-tions that Congress had provided for the program,and that Congress by not overturning the regu-lations had ratified the agency’s actions over thecourse of the years.
The Supreme Court found that Ruiz was an in-dividual within the class of intended beneficiaries,and in effect struck down the reservation-onlyservice criteria. Its decision seems to be basedmore on the lack of consistency between BIA’sown policy and its representations to Congressthan on any other factor. In reaching its conclu-sions, however, the Court did set out a fairly per-missive standard for agency decisionmaking (89):
(I)t does not necessarily follow that the Secre-tary is without power to create reasonable clas-sifications and eligibility requirements in orderto allocate the limited funds available . . . (I)fthere were only enough funds appropriated toprovide meaningfully for 10,000 needy Indianbeneficiaries and the entire class of eligible ben-eficiaries numbered 20,000, it would be incum-bent upon the BIA to develop an eligibility stand-ard . . . The power of an administrative agencyto administer a congressionally created andfunded program necessarily requires the formu-lation of policy and the making of rules to fillany gap left implicitly or explicitly by Congress.
Morton v. Ruiz is therefore extremely relevant tothe issue of who is an Indian for the delivery ofhealth care services because of the latitude it givesto agencies to determine eligibility.
Shortly after the Morton v. Ruiz decision, IHSattempted to limit the eligibility of Indians for con-tract care to Indians living on or near reservations.Since IHS chose to codify its policy by fiat, itsinitial attempt was struck down (65) for failureto follow the publication and notice requirementsof the Administrative Procedure Act (APA) (5U.S. C. section 601e). However, similar regula-tions were subsequently published under APAthat contained the same contract care restrictions.These regulations, which have not been chal-lenged on a substantive basis, are currently oper-ational.
Therefore, adequate notification and opportu-nity to comment must take place before a regu-lation implementing a statute is formalized. How-ever, under APA, the Federal agency’s action ispresumed to be valid and must be confirmed ifits actions were not “arbitrary, capricious, orotherwise not in accordance with law” (5 U.S. C.section 706[2][A]). The action is valid if all therelevant factors were considered, and any discern-ible rational basis existed for the agency’s actions(22).
Another standard for judicial review of agencyrulemaking is applicable to constitutional claimsunder the equal protection clause of the 14thamendment. Under this standard, a “rational ba-sis” must exist for the agency’s actions (25). Thisstandard is similar to, but not a substitute for,the statutory standard set out in APA. A stricterstandard is applicable when suspect classifications(e.g., ancestry [96], race [81], alienage [41]) orfundamental constitutional rights (e.g., right ofinterstate travel [108], right to vote [14], right ofprivacy with respect to abortion [105]) are in-volved.
In the 1980 case of Rincon Band of Mission In-dians v. Califano (104), a band of California In-dians sued for their fair share of IHS resources.They argued that, in examining IHS’s method ofallocation, the stricter constitutional standard ofreviewing IHS’s conduct be applied. IHS, on theother hand, argued that a “rational basis” test beused, claiming that no constitutional rights wereinvolved.
The district court found that IHS’s allocationsystem had no rational basis, thereby violatingCalifornia Indians’ right to equal protection of thelaws as guaranteed by the due process clause ofthe fifth amendment. Because it found that theallocation system had no rational basis, the courtdid not find it necessary to decide whether the“strict scrutiny” standard was appropriate.
On appeal, the ninth circuit affirmed the dis-trict court’s decision, but on the basis that IHShad breached its statutory responsibilities to theCalifornia Indians, so it did not find it necessaryto address the constitutional question. Thus, atleast the minimum requirements of APA must be

Ch. 2—The Federal-Indian Relationship ● 5 1
met, with the application of a higher constitu-tional standard yet to be fully adjudicated.
The California Indians had also contended thatthe Snyder Act and the Indian Health Care Im-provement Act of 1976 created a trust obligationbetween the United States and Indians, and thatIHS had breached its fiduciary duty as trustee byfailing to provide California Indians with a levelof health services comparable to that provided In-dians elsewhere in the United States. The ninthcircuit indicated that it would not make such afinding, but stated that it did not have to rule onthe applicability of the trust responsibility to thetwo statutes to make its decision,
Turning next to the degree of Indian blood anindividual must have in order to be eligible forFederal benefits, the issue of a blood quantum re-quirement beyond the level that a tribe sets foritself is a conceptually difficult one, because theFederal-Indian relationship is based on political,not racial, factors. Moreover, blood quantum asa standard for providing services comes factuallyclose to a suspect racial classification under con-stitutional law.
Congress, in its attempt to revitalize the tribes,provided in the Indian Reorganization Act (25U.S. C. section 45) for preference in employmentfor Indian persons in the Federal Indian Service.(Earlier statutes also contained preference provi-sions. ) The act set out a several-part definitionof eligibility (25 U.S. C. section 45):
All persons of Indian descent who are mem-bers of any recognized tribe now under Federaljurisdiction, and all persons who are descendantsof such members who were on June 1, 1934,residing within the present boundaries of any In-dian reservation, and shall further include allother persons of one-half or more Indian blood.
The clear language of the statute created three cat-egories. However, for over 40 years, BIA tookthe third category, one-half or more Indian blood,and used it as an overlay governing the other cat-egories. Thus, to qualify for Indian preference,one had to be a half-blood member or a half-blooddescendant of a member. The action of BIA wasoutside the plain language of the law, and the half-blood requirement was finally dropped follow-ing a legal challenge (213).
While IHS considers its eligible population tobe persons of Indian descent (42 CFR 36.12), someof the programs provided by BIA under the au-thority of the Snyder Act require that individualIndians be a member of a federally recognizedtribe or have one-fourth degree or more Indianblood to receive services (25 CFR section 20.l[n]).However, unlike the Indian Employment Prefer-ence legislation, which contained a statutory def-inition of who was eligible that BIA had clearlyviolated, there is no express statutory languagein the Snyder Act other than “Indians through-out the United States. ” Under these circumstances,therefore, the rational basis test of Morton v. Ruiz(89) is probably operable.
Finally, there is the question of whether AlaskaNatives stand in any different position than In-dians generally with respect to the Federal provi-sion of health services. The issue comes up be-cause of the unique land claims settlement andcorporate structure created by the Alaska NativeClaims Settlement Act (ANCSA) (43 U.S. C. sec-tions 1601, et seq.). Under ANCSA a complex sys-tem of corporations has been set up to hold andinvest both the land and monetary aspects of thesettlement, Alaskan native people received stockin these corporations. Undeveloped lands were toremain nontaxable until the year 1991, the yearthat Native-held stock would also become freelytransferable. These provisions resemble aspectsof the Federal trust relationship with respect tothe physical assets of tribes in the “lower 48”States. ANCSA, however, is a land claims settle-ment and not legislation that defines or limits inany way the preexisting special trust relationshipthat Alaska Natives have with the United States.
ANCSA by its own terms provides that it is forthe extinguishment of land claims and shaIl notbe deemed to substitute for any governmental pro-grams otherwise available (43 U.S. C. section1626a). Most commentators agree that ANCSAneither created a new trust relationship nor ter-minated the preexisting trust relationship betweenthe United States and Alaska Natives. (ANSCA,however, did provide a definition of Alaskan Na-tives that has been adopted in other Federalstatutes. )

52 Ž Indian Health Care
IS THE INDIAN HEALTH SERVICE A PRIMARY OR RESIDUALHEALTH CARE PROVIDER?
Indians are U.S. citizens and also are eligiblefor services provided to other U.S. citizens, in-cluding both Federal and State services. Throughregulations, IHS services are residual to othersources; i.e., other governmental and privatesources of care for which the Indian patient is eligi-ble must be exhausted before IHS is obligated topay for medical care. The residual payer role ofIHS is discretionary for direct IHS services (42CFR 36.12 [c]); and as a matter of policy, IHS gen-erally will provide services to a patient in IHS fa-cilities regardless of other resources, but will seekreimbursement from these other sources for thecare provided. In contrast, IHS’s residual payerrole is mandatory for contract care obtained fromnon-IHS providers (42 CFR 36.23 [f]); and IHS willnot authorize contract care until other resourceshave been exhausted or a determination has beenmade that the patient is not eligible for alterna-tive sources of care.
One issue that has arisen from this “residualpayer” situation is the question of who is the pri-mary, and who is the residual payer, when Stateor local governments also have a residual payerrule. This situation arose in litigation between IHSand Roosevelt County, Montana, with the countyarguing that it was not discriminating against In-dians, but merely applying its alternate resourcepolicy across the board to all eligible citizens whohave double coverage, thereby meeting the “ra-tional basis” test for judicial review (79).
The vetoed Indian Health Care ImprovementAct Amendments of 1984 provided for a “Dem-onstration Program Regarding Eligibility of Cer-tain Indians for Medical and Health Services”(section 204[a]). The provision, commonly knownas the “Montana amendment, ” was designed torelieve what several Montana counties saw astheir financial burden in providing and paying formedical services to indigent Indians. The amend-ment was converted into a Montana-only dem-onstration project in the House-Senate conferenceand would have made IHS financially responsi-ble for medical care to indigent Indians in Mon-tana. This responsibility was to exist only whereState or local indigent health services were funded
from taxes on real property and the indigent In-dian resided on Indian property exempt from suchtaxation. Senator Melcher of Montana analogizedhis amendment to the type of services that BIAprovides to Indians for education or general assis-tance. The conference report on the bill stated thatthe provision would not preclude an Indian fromreceiving State or county-provided health careservices or financial assistance for health care serv-ices that are provided to all State citizens; nor thatit would preclude an otherwise eligible Indianfrom participating in Medicaid, even where thosebenefits were paid for in part by State or localfunds derived from revenues raised from real es-tate property taxes (133).
President Reagan disagreed with such an ap-proach and vetoed the legislation. Two conceptsunderlie the President’s veto. The first is that theamendment would allow States to deny servicesto Indians, an act that would be unconstitutionalunder the equal protection clause of the 14thamendment. Indians, as State citizens, are con-stitutionally entitled to State and local health ben-efits on the same basis as other citizens. The otherconcept is that, under IHS’s contract care eligi-bility standards, the Federal Government canplace its provision of services to Indians in a sec-ondar y or residual position. The State or countycannot presume that Indians have a right or en-titlement to IHS contract care services so that itcan deny assistance on the grounds of double cov-erage. In fact, the Federal regulations on contractcare expressly deny that such a right exists. In sucha conflict, the supremacy clause of the Constitu-tion would resolve the issue in favor of the IHSregulation (79).
In January 1986, in McNabb v. Heckler, et al.(82), the United States District court for theDistrict of Montana, Great Falls Division, ruledthat the Federal Government, and not RooseveltCounty, was primarily responsible for the careof the Indian plaintiff. Though the court did notfind the trust doctrine, the Snyder Act, or the In-dian Health Care Improvement Act as individu-ally entitling Indians to Federal health care, thecourt found that the two statutes, read in con-

Ch. 2—The Federal-lndian Relationship ● 5 3
junction with the trust doctrine, placed the bur- The better avenue for resolution of disputesden on IHS to assure reasonable health care for of the type presented here rests with the legisla-eligible members. The court, however, did not ad- tive branch. This court can only interpret thedress the equal protection and supremacy clause limited legislative enactments and statements of
arguments outlined above, and the decision is be- congressional intent available to it. Congress
ing appealed (80). Furthermore, the court invited could quickly resolve a question which this court
Congress to address the issue by stating that:has wrestled with for many months (82).
CONCLUSIONS
Federal law and policy have evolved througha complex mixture of practice, court decisions,and congressional legislative and appropriationsactivities. Periodic shifts, including complete re-versals, in Federal-Indian policy have created un-clear responsibilities as well as various categoriesof Indians. Several generalizations are, however,relatively clear. Indian affairs is predominantlya Federal and not a State responsibility. The oper-ative relationship is between the Federal Govern-ment and the tribal government. On the Federalside, the power is constitutionally assigned toCongress; however, until recently very few of thehealth-related statutes have contained specificcongressional directives on how they should beimplemented. This situation has long favoreddecisionmaking and policy development by theadministrators of Indian programs. For most ofthe history of Federal-Indian relationships, thepower of administrators was not able to be legallychallenged by dependent Indian tribes. Only inthe last several decades has litigation begun to de-fine the perimeters of agency power.
The trustee role adopted by the Federal Gov-ernment has its origins in more than the UnitedStates being the technical legal owner of Indianland. Among other roles, the Federal Governmentwas to protect tribes against non-Indians (States)and to provide necessary services. The operativedocuments for determining the scope of the Fed-eral responsibility in any given situation are thetreaties and statutes. In situations where the stat-utes or treaties are unclear, the courts have de-veloped special rules of interpretation-rules thatgive the most favorable interpretation or construc-tion to the Indian parties.
With the exception of specific congressionaldirectives, whatever rights exist for individual In-
dians in the Federal-Indian relationship are de-rived from membership in a federally recognizedtribe, even though it is not always clear how sometribes became federally recognized and others didnot. Federal recognition is the key ingredient foraccess to most Federal services that are providedon the basis of the Federal-Indian relationship. Al-though Congress has the power to determine whois eligible for benefits, it expresses that power in-frequently and has usually deferred that determi-nation to the executive branch.
As noted, for the most part rights within theFederal-Indian relationship derive from an indi-vidual Indian’s membership in a federally recog-nized tribe. The definition of that membership isa tribal prerogative. Although Congress routinelyuses the tribal membership definition, it can addadditional definitions, or use specific definitionsof Indian eligibility for specific programs. Courtswill defer to these congressional determinationsas long as they have the overall purpose of fur-thering the Federal-Indian relationship. It is impor-tant to distinguish, however, whether Congressis or is not acting pursuant to the Federal-Indianrelationship. There are many Federal statutes thatmay provide services to individuals who are de-fined as Indian for the purposes of the particularstatute but who are not Indians for purposes ofthe Federal-Indian relationship.
In addition to the issue of what definition Con-gress is adopting for the provision of services, isthe issue of agency discretion to modify, expand,or limit the congressional definition. Where Con-gress has provided no definition, what is the scopeof agency discretion to create service eligibilitycriteria that in effect define Indians for that par-ticular service? To date, litigation has addressedthese questions in only a limited fashion. Mor-

54 ● Indian Health Care
ton v. Ruiz (89) is probably the leading case. Itevaluated the agency determination of serviceeligibility by determining if the agency action hadany “rational basis. ”
Reid Chambers, formerly the Associate Solici-tor for Indian Affairs at the Department of theInterior, in his classic 1975 article on the trustresponsibility (18), came to the conclusion thatit is unlikely that the judiciary would, in the ab-sence of a specific treaty, agreement, or statute,find the social services provided by the FederalGovernment to be a trust obligation to Indians.An exception is perhaps provided, he reasoned,where the denial of services is so extreme that aright somewhat analogous to “the right of treat-ment” developed in prisoners’ rights cases mayarise.
Several factors existing at the time of the Cham-bers article invariably led to such conclusions. Nocase had held that the trust responsibility requiredthat social services be provided. The one case inpoint at the time was the 1970 decision in GilaRiver Pima Maricopa Indian Community v.United States (37), which held that the UnitedStates had no legally enforceable duty in the ab-sence of a specific provision in a treaty, statute,or other legally controlling document. In additionto cases that directly consider the scope of the trustobligation, another factor was the plenary powerdoctrine. Pursuant to the plenary power doctrine,the courts defer to congressional judgments in In-dian affairs; this deferral had permitted Congressto unilaterally alter, modify, or eliminate the Fed-eral Government’s obligations to Indians.
The judiciary had been clinging to the narrowrole that had been defined for it in the 1903 clas-sic case on congressional plenary power, LoneWolf v. Hitchcock (66a). Lone Wolf had stoodfor the proposition that Congress has extraordi-nary power in Indian affairs and that the judici-ary, while it will interpret the actions of Congress,will only rarely scrutinize on a constitutional ba-sis the exercise of the power of Congress. In LoneWolf, the Kiowas and Comanches had by treatywith the United States provided for a specificmechanism to control the sale of Indian lands.Congress subsequently enacted a statute contain-ing a process different from that in the treaty. The
tribes sued to have the land sales set aside forviolating the treaty. Allegations of fraud were alsomade by the tribes. The Supreme Court refusedto look behind the action of Congress in passingthe statute, but, fortunately for the complainingtribes, also held that the statute had abrogatedthe treaty.
The Lone Wolf doctrine has been somewhatmodified in recent years (127). The two modify-ing cases are Delaware Tribal Business Commit-tee v. Weeks (28a), where the Supreme Courtreached the merits of a due process challenge, andUnited States v. Sioux Nation (125a), where theSupreme Court indicated that it would determinein what capacity the United States was acting,rather than following the conclusive presumptionin Lone Wolf of congressional good faith. Weeksrequires that congressional efforts to affect its trustobligation to Indian tribes must be rationally tiedto its “unique (trust) obligation. ” Sioux Nationfound the United States to be exercising the tradi-tional function of a trustee and therefore held theUnited States to the usual standards of a tradi-tional trustee. These modifications, which involvethe utilization of constitutional standards analo-gous to those standards used in equal protection/due process analyses, have potential implicationsfor any definition of the Federal Government’shealth obligation to Indians. For if Congress is tobe held to any constitutional standard of fairnessthat ties the scope of its responsibilities to the pur-pose of its obligation—e.g., to benefit Indians—then the executive branch must be held to at leastas stringent a standard in determining the scopeof its authority.
There has been only one case, White v. Cali-fano (212), that considered directly the FederalGovernment’s obligation to provide health serv-ices. White v. Califano, like most cases, has aunique factual and jurisdictional setting, in whichthe court answered a relatively narrow question.An indigent Indian residing on the Pine Ridge Res-ervation in South Dakota was held to be incompe-tent by the Pine Ridge Tribal Court. The tribalcourt then entered an order seeking to have the“incompetent Indian” committed to a South Da-kota State mental institution. South Dakota re-fused to accept the patient, arguing that under

Ch. 2—The Federal-lndian Relationship ● 5 5
applicable Federal law, it lacked jurisdiction overher and could not take custody. South Dakotaalso asserted that an “incompetent” Indian wasthe responsibility of the Federal Government. TheUnited States had also refused to provide anyservices to the patient. Her guardians sued theUnited States and South Dakota to provide serv-ices. Interestingly, the U.S. Government viewedthe case as primarily one of a State violating the“civil rights” of an individual Indian, and the casewas in large part the responsibility of the CivilRights Division of the Department of Justice. TheJustice Department used the same conceptual ar-gument on dual entitlement contained in the Presi-dent’s veto message on the Indian Health Care Im-provement Act amendments.
White v. Califimo does not settle the issue ofprimary versus secondary responsibility, since theeighth circuit sustained South Dakota’s assertionthat it lacked jurisdiction over incompetent In-dians and as such could not provide custodialservices. The court rejected the argument that theUnited States had no duty to provide facilities formental health and found that instead the UnitedStates had the duty to provide care under its trustresponsibility and, specifically, that it was pur-suant to the Indian Health Care Improvement Act.
White v. Califano has been criticized by at leastone Indian commentator, Pine Ridge Tribal JudgeMario Gonzalez (40). Judge Gonzalez does not ac-cept the analysis that begins with Indians beingState citizens; he argues that even though Indiansbecame U.S. citizens in 1924, it is not necessaryfor them to be State citizens to enjoy constitu-tional protections. He argues that under the fullfaith and credit clause of the constitution, SouthDakota should have accepted the tribal court de-cree and provided services. He also notes thatSouth Dakota mental health services were in anyevent 68 percent federally funded. The attemptof the Federal Government to evade its responsi-
bilities also was severely criticized by JudgeGonzalez.
If White v. Califano is followed, an eligible In-dian who has no other alternative probably wouldnot be denied health services by the Federal Gov-ernment. Any award of damages under presentlaw would seem to require specific statutory au-thorization. However, where breaches are prov-able, equitable relief should be available againstthe appropriate Federal agency and its officials.
White v. Califano was also cited by the judgein the 1986 McNabb v. Heckler, et al. (82) deci-sion discussed above, where an alternative sourceof payment, Roosevelt County, was available.The judge stated that:
. . . the court believes that the real importanceof White lies in its extended discussion of the(F)ederal Government’s trust responsibility to In-dians. Further, this court believes that the trustanalysis employed in White was equally respon-sible for the result reached therein, to be ac-corded equal footing with the court’s conclusionthat local governments had no authority to in-voluntarily commit mentally ill Indian persons(82).
Whatever difficulties the legal profession mayhave in defining the perimeters of the trust obli-gation, it is within Congress’ powers to definethose perimeters, and Indian people have consist-ently maintained that health care is part of thetrust obligation of the United States. Accordingto a report in the mid-1970s by the American In-dian Policy Review Commission (130):
Indian people are unanimous and consistentin their own view of the scope of the trust respon-sibility. Invariably they perceive the concept tosymbolize the honor and good faith, which his-torically the United States has always professedin its dealings with the Indian tribes. Indian peo-ple have not drawn sharp legal distinctions be-tween services and custody of physical assets intheir understanding of the applications of thetrust relationship.

Chapter 3
Overview of the CurrentIndian Population

Contents
PageIntroduction . . . . . . . . . . . . . . . . . . . . . . . .. ...,,. 59Sources of Estimates of the Size of the
Indian Population . . . . . . . . . . . . . . . . . . . . . . 59U.S. Bureau of the Census Estimates.. . . . . . . 60Indian Health Service Estimates . . . . . . . . . . . . 61Bureau of Indian Affairs Estimates. . . ...... 61Implications of Varying Estimates . . . . . . . . . . 63
Characteristics of the American Indian,Eskimo, and Aleut Populations . . . . . . . . . . . 64
Four Projections of the Effects of Intermarriageon the Number of Indian Descendants . . . . 74
Scenario I . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77Scenario . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77Scenario III . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79Scenario IV. ..,...... . . . . . . . . . . . . . . . . . . . . 80Summary and Conclusions . . . . . . . . . . . . . . . . 81
List of TablesTable No. Page3-1. Indian Population in the United States,
Decennial Censure numerations and BIAEstimates, Selected Years 1890-1980....,.. 59
3-2. American Indian Population LivingOn and Off Reservations or IdentifiedTribal Trust Lands, by State, 1980 . . . . . . . 62
3-3. 32 Reservation States as of 1985 . . . . . . . . . 633-4. American Indians, Eskimos, and
Aleuts, by State, Urban/Rural Residence,and Sex, 1980. . . . . . . . . . . . . . . . . . . . . . . . . . 66
3-5. Settlement Patterns of Indians in 114SMSAs With l,000 or More AmericanIndians, Eskimos, and Aleuts . . . . . . . . . . . . 74
3-6. American Indian and Alaska NativePopulation for 32 Reservation States,by 5-Year Age Group and Sex, 1980Census Data.... . . . . . . . . . . . . . . . . . . . . . . . 76
3-7. Age-Specific Fertility Rates for AmericanIndians and Alaska Natives by Age ofMother, Reservation States, 1980-82 . . . . . . 76
3-8. Number of American Indians and AlaskaNatives in 28 Reservation States, Livingat Beginning of Age Interval of 100,000Born Alive, 1979-81 . . . . . . . . . ● . . . . . . . . . . 77
3-9. Age-Focused Population ProjectionSummary, All Indians and IndianDescendants, Selected Years, 1980-2080 . . . 78
List of FiguresFigure No. Page
3-1. Facsimiles of Race and AncestryQuestions: 1980 U.S. Census..........,. 60
3-2. Distribution of the American Indian,Eskimo, and Aleut Population, 1980 . . . . . 63
Figure No. Page3-3
3-4*
3-5,
3-6.
3-7,
3-8.
3-9.3-10.
3-11.
3-12.
3-13.
3-14.
3-15.
3-16.
3-17.
3-18.
3-19.
3-20.
3-21.
3-22*
Ten Reservations With Highest Number of Indians, 1980 ......., . . . + . . . . . . . . . . . 65Urban and Rural Residence forAmerican Indian, Eskimo, and AleutPopulations, 1980 . . . . . . . . . . . . . . . . . . . . . 65Ten SMSAS With the Highest Numbersof American Indians, Eskimos, andAleuts, 1980 . . . . . . . . . . . . . . . . . . . . . . . . . . 65Distribution of the Eskimo andAleut population, 1980.... . . . . . . . . . . . . . 65Percent of Total U.S. American IndianPopulation, by Region of Residence:1970 and 1980 . . . . . . . . . . . . . +.. . . . . . . . . 67Ten States With the LargestAmerican Indian, Eskimo, and Aleutpopulation, 1980 . . . . . . . . . . . . . . . . . . . . . . 67Median Family Money Income in 1979 . . . 68Poverty Rates of Persons,1970 and 1980 . . . . . . . . . . . . . . . . . . . . . . . . 68Families Maintained by Women,1970 and 1980 . . . . . . . . . . . . . . . . . . . . . . . . 69Unemployment Rates for AmericanIndians, Eskimos, and Aleuts,1970 and 1980 . . . . . . . . . . . . . . . . . . . . . . . . 69Occupation of Employed AmericanIndians, Eskimos, and Aleuts, 1980 . . . . . . 70Educational Attainment of Persons 25Years Old and Over, United StatesAll Races and Indian Population: 1980 . . . 71Percent of Occupied HousingUnits Lacking Complete PlumbingFacilities, 1980 . . . . . . . . . . . . . . . . . . . . . . . . 72Year Householder Moved IntoOwner-Occupied Housing Unit. . . . . . . . . . 73Year Householder Moved IntoRenter-Occupied Housing Unit . . . . . . . . . . 74Distribution of Reservation Residents,by Quantum of Indian Blood for SelectedBureau of Indian Affairs AdministrativeAreas, United States, 1950 . . . . . . . . . . . . . . 75OTA Population Projection Scenario I:No Outmarriage.. . . . . . . . . . . . . . . . . . . . . . 77OTA Population Projection Distributionof Indian Population by Blood QuantumScenario II: Outmarriage-53%,Both Sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80OTA Population Projection Distributionof Indian Population by Blood QuantumScenario III: Outmarriage-53%, BasePopulation Mix, Both Sexes . . . . . . . . . . . . 80OTA Population Projection Distributionof lndian Populatioin by Blood QuantumScenario IV: Outmarriage-40%, Basepopulation, Both Sexes. . . . . . . . . . . . . . . . . 81

Chapter 3
Overview of the CurrentIndian Population
INTRODUCTION
The number of American Indians, Eskimos, andAleuts identified by the U.S. Bureau of the Censusand Bureau of Indian Affairs (BIA) is far fewerthan the number, perhaps 10 million, who arethought to have been living in North America atthe time of its discovery by the Europeans. West-ward expansion (85), contact with disease, wars,and other scourges reduced the number of Indiansby 90 percent within a century after Columbusarrived (71). Little recovery has been made byIndians in the United States in rebuilding thepopulation as shown by records kept by govern-ment agencies. In 1890, there were approximately274,000 Indians, Eskimos, and Aleuts in this coun-try. Fifty years later, in 1940 the population hadgrown by almost 34 percent to 366,000 (see table3-l). In the 1980 Census of Population, whichused improved techniques for counting people,1.4 million Indians, Eskimos, and Aleuts were self-identified—almost quadrupling the 1940 count.The blood quantum of these self-identified In-dians, however, is not known. While most Indiantribes have a minimum blood quantum require-ment for membership, the Bureau of the Census’definition of race does not denote any clear-cutscientific definition of biological stock. In the 1980census, 6.7 million persons identified their ances-try as American Indian and 51,000 persons iden-tified themselves as being of Aleut or Eskimo an-cestry (these figures include persons who reportedsingle and multiple ancestry groups) (150). (Raceand ancestry are separate characteristics; personsreporting a particular (or multiple) ancestry maybe of any race. )
Table 3-1 .—Indian Population in the United States,Decennial Census Enumerations and BIA Estimates,
Selected Years 1890.1980
U.S. Census Alaska BIAYear enumeration Natives estimate
1890 . . . . . . 248,253 25,354 248,3001900 . . . . . . 237,196 29,536 270,5001910 . . . . . . 265,683 25,331 305,0001920 . . . . . . 244,437 26,558 336,3001930 ., . . . . 332,397 29,983 340,5001940 . . . . . . 333,969 32,458 360,5001950 . . . . . . 343,410 35,047 421,6001960 . . . . . . 551 ,669’ — 344,951 b
1970 . . . . . . 827,268’ — 477,458C
1980 . . . . . . 1,423,043a — 734,895 d
alncludes Eskimos and Aleuts, they are In a separate column prior to 1%0 asAlaska was granted statehood in 1959
bFrom B}A, “lndlan population, April 1, 1960, ” JUIY 1%1CFrorn the B[A repoti, “[rlcllarl Population On and Near Reservations, ” March 1970‘From the BIA report, “Indian Service Population and Labor Force Estimates,
December 1981 ,“ January 1982BIA figures represent local resident service population.
SOURCES Except where noted U S Department of Health, Education, and Wel.fare, Public Health Service, “Health Services for American Indians, ”Washington, DC, Feb. 11, 1957, verified by the U S Census Bureauon Nov 11, 1985, and U S Bureau of the Census, PC80-S1.13, 1984
This chapter explains the U.S. Bureau of theCensus compilation of statistics on Indians, Fed-eral agencies’ use of Indian data, a demographicreview of the Indian population, and 100-yearprojections of the future Indian population. In thischapter, the term “Indians” includes American In-dians, Eskimos, and Aleuts except when referringto population characteristics gathered in the 1970census, which pertain only to American Indians.“Reservation Indians” includes American Indians,Eskimos, and Aleuts living on identified Amer-ican Indian reservations or identified historic areasof Oklahoma (excluding urbanized areas).
SOURCES OF ESTIMATES OF THE SIZE OF THE INDIAN POPULATION
There are at least as many definitions of who agencies, the U.S. Bureau of the Census, actuallyis an Indian as there are Federal agencies whose counts all the people in this country every 10constituencies include Indians. Since one of these years, it is agreed that this agency’s count of the
59

60 ● Indian Health Care —
number of Indians is generally the most reliablemeasure. Even so, tribes and Federal, State, andlocal agencies have serious disagreements over theaccuracy of the census count. In large measure,such disagreements reflect concerns about fund-ing. Because funding for major Federal and Stateprograms—including revenue sharing, commu-nity development block grants, home energy assis-tance, and various social programs—is keyedlargely to population, and administering agenciesuse census figures to define service populations,differences in population estimates can be critical.
One reason that varying estimates of the sizeof the Indian population are controversial is thatFederal agencies and individual tribes use differ-ent definitions of “Indian. ” Many differences inthe operational definitions of “Indian” can be re-solved only through changes in authorizing leg-islation in which definitions are set forth. Changesin authorizing legislation would arouse significantdisputes and bring out many opposing views. Be-cause the economic and philosophic stakes are sohigh, it is not likely that laws will be revised toachieve a consistent definition of “Indian” that canbe applied universally.
U.S. Bureau of the Census Estimates
In 1980, for the first time, the Bureau of theCensus relied on self-identification, which allowedindividuals themselves to choose the racial groupwith which they most identified. In the 1970census, race had been determined “on the basisof observation by enumerators in rural areas ofthe country, including most reservations” (148).
Two questionnaires were used in the 1980census; a “short form” with questions asked ofall housing units/households, and a “long form”with additional questions. Both forms includedthe question regarding race from which the Bu-reau of the Census tabulated the Indian popula-tion. The long form, which was administeredrandomly to 80 percent of all housing units/households, included a separate question on an-cestry (see figure 3-l).
For respondents who left the race questionblank on the 1980 census questionnaire, the re-ported race of other members of the householdwas used. Additionally, if race was not reported
Figure 3-1 .—Facsimiles of Race and AncestryQuestions a: 1980 U.S. Census
ASKED OF ALL HOUSEHOLDS
4. Is this person— W h i t e Asian IndianBlack or Negro Hawaiian
Fill one circle Japanese GuamanianChinese SamoanFilipino EskimoKorean AleutVietnamese Other—SpecifyIndian (Amer. ) below
II I Print tr ibe .— I
ASKED OF SAMPLE HOUSEHOLDS
r14. What is this person’s ancestry? /f uncertain about how toreport ancestry, see instructions guide,
aAncest~ and race are separate characteristics perSOnS repOrtlng d Partlcu Iarancestry may be of any race
SOURCE U S Department of Commerce, Bureau of the Census, 1980 Censusof the United States Leaflet showing the content of the two que:j.tlonnaires used In the Census of population and housing
for any member of the household, the race of ahouseholder in a previously processed householdwas assigned by computer. Persons who did notcheck one of the specific race categories but wrotein the name of an American Indian tribe, “Cana-dian Indian, ” “French-American Indian, ” or“Spanish-American Indian” were counted asAmerican Indians, Responses to the ancestry ques-tion on the 1980 questionnaires yielded a signifi-cant number of persons who regarded themselvesto be ethnically Indian. Like race, ancestry wasascertained by self-identification, so responsesreflected the ethnic group with which individualsidentified regardless of the number of generationsremoved from their ancestor(s).
It is widely held that both the 1970 and 1980censuses undercounted the population of Amer-ican Indians, Eskimos, and Aleuts for many agegroups; and the count was particularly poor insome geographic areas. Critical discussions of theIndian undercount in the 1980 census and whetherthe American Indian, Eskimo, and Aleut countis accurate generally fall into two categories: 1)

— —
that intercensal measures of population changeare unreliable, and 2) that the enumeration tech-niques used by the Bureau in the census are in-adequate. According to the census, the AmericanIndian population grew by 72 percent between1970 and 1980. If one assumes that the 1970 countwas accurate, however, the natural increase (i. e.,the effect of American Indian births and deaths)yields a number that is lower than the 1980 count.The same inconsistency occurred between 1960and 1970 (97).
One intercensal measure adjusts for the natu-ral increase in population using-data from the Na-tional Center for Health Statistics (NCHS). Short-comings inherent in this method are that Indianbirths and deaths are undercounted. States do notrecord paternal race if a birth has occurred outof wedlock. Therefore, children born out of wed-lock to an Indian father and non-Indian motherwill not be included in the count of Indian birthsunless an Indian father has acknowledged pater-nity. Indian deaths are underreported in manyStates, most notably in California, in part becauseof the difficulty in distinguishing Indians from in-dividuals of other races and ethnic heritages suchas Hispanics.
In addition to counting Indians, the census alsodistinguishes between Indians living inside “iden-tified areas” and Indians living elsewhere. Anidentified area includes reservations, tribal trustlands, Alaska Native villages, and historic areasof Oklahoma (which consist of the former reser-vations having legally established boundaries be-tween 1900 and 1907, excluding urbanized areas).The boundaries of identified areas used in thecensus are those established by treaty, statute, ex-ecutive order, or court order for federally andState-recognized tribes. In 1970, 115 reservationswere identified. In 1980, 278 reservations and 209Alaska Native villages were identified. Table 3-2shows the American Indian population living onand off reservations or identified tribal trust landsby State, and figure 3-2 shows the total distribu-tion for 1980.
Indian Health Service Estimates
A second source of population estimates fre-quently cited is that of the Indian Health Service(IHS), which computes its service population
Ch. 3—Overview of the Current Indian Population ● 6 1— — —.—-—-.—
based on figures from the 1980 census as reportedby county. The IHS service population consistsof American Indians, Eskimos, and Aleuts (whoidentified themselves as such in the 1980 census)living within the geographic areas that definewhere IHS has responsibilities. These geographicareas are counties within reservation States hav-ing the reservation of a federally recognized tribewithin or contiguous to its borders. This conceptof geographic proximity is referred to as “on ornear” a federally recognized reservation. A “res-ervation State” is a State in which IHS has respon-sibilities; not all States in the United States areconsidered “reservation States. ” The reservationmust be federally recognized (there are tribes withland holdings that have State recognition only).The 32 reservation States as of 1985 are listed intable 3-3, Local administrative units within IHSarea offices are known as service units. For at-tributing population to specific service units whenservice units cross county lines, estimates aremade by field administrators as to the number ofindividuals within each county to include in theservice unit. These proportions, which are fromthe 1980 census, are applied to all subsequent esti-mates, IHS adjusts its population estimates an-nually for the natural increase only, using themost recently available data on Indian births anddeaths from NCHS, As previously noted, theseIndian births and deaths are undercounted byStates. In some States the undercount may be sig-nificant. Except where noted, the Office of Tech-nology Assessment (OTA) has used IHS’s 1985estimates of its service population throughout thisreport,
Bureau of Indian Affairs Estimates
A third population estimate, from BIA, iden-tifies local resident population, but as in the caseof the IHS service population does not necessarilyrefer to tribal membership. According to BIA’sOffice of Financial Management, local BIA agen-cies estimate population figures and labor forceparticipation using “whatever information maybe available for the reservation. Accuracy variesfrom place to place; it is relatively high at small,isolated locations where everyone’s activity iscommon knowledge” (208). “Data for the NavajoArea, the State of Oklahoma (Anadarko andMuskogee Areas), and the State of Alaska are

62 ● Indian Health Care
Table 3-2.—American Indian Population Living On and Off Reservations or Identified Tribal Trust Lands,by State, 1980
Number Percent
American On On trust Off reservationStates All races
west:Alaska . . . . . . . . . . . . . . . . . 401,851
On O n t r u s t --reservation lands
4.30/o
o f f r e s e r v a t i o nor trust landsIndian reservation lands or trust lands
21,86942,234a
152,498198,275
17,7342,655
10,41857,59813,306
107,33826,59119,15858,1867,057
942
113,7639,2651,966
—4,771
24,0434,400
61,8763,0726,868
16,4404,159
————
1,30330—
210—
2,7564,8444,749
728—
859118
—
——
492715
1,6079,901
—2,846
11,287—
28,4689,361
271,235
1——
6,734———
20,927 95.7 %— —
Arizona . . . . . . . . . . . . . . . . 2,718,215 74.6California . . . . . . . . . . . . . . 23,667,902 4,7Colorado. . . . . . . . . . . . . 2,889,964 11.1Hawaii . . . . . . . . . . . . . . . 964,691Idaho . . . . . . . . . . . . . . . . . .
—943,935 45.8
Montana . . . . . . . . . . . . 786,690 63,9Nevada . . . . . . . . . . . . . . 800,493 33.1New Mexico . . . . . . . . . . . . 1,302,894 57.6Oregon . . . . . . . . . . . . . . . . 2,633,105 11.6Utah. . . . . . . . . . . . . . . . . . . 1,461,037 35.8Washington . . . . . . . . . . 4,132,156 28.3Wyoming . . . . . . . . . . . . 469,557 58.9
South:Alabama . . . . . . . . . . . . . . . 3,893,888Arkansas. . . . . . . . . . . . . .
—2,286,435
Delaware. . . . . . . . . . . . .—
594,338District of Columbia. . . . .
—638,333
Florida ., . . ... . . .—
9,746,324 6.8Georgia. . . . . . . . . . . . . . . . 5,463,105 0.4Kentucky . . . . . . . . . . . . . . 3,660,777Louisiana . . . . . . . . . . . .
—4,205,900 1.8
Maryland, . . . . . . . . . . . . . . 4,216,975Mississippi. . . . . . . . . . . . .
—2,520,638 45.0
North Carolina . . . . . . . . . 5,881,766 7,5Oklahoma . . . . . . . . . . . . 3,025,290 2,8South Carolina . . . . . . . . . 3,121,820 12.9Tennessee . . . . . . . . . . . . 4,591,120Texas . . . . . . . . . . . . . . . 14,229,191
—2.2
Virginia . . . . . . . . . . . . . 5,346,818 1.3West Virginia. . ..., . . . . 1,949,644 —
MidwestIllinois . . . . . . . . . . . . . . . . . 11,426,518 —Indiana . . . . . . . . . . . . . . . . 5,490,224Iowa . . . . . . . . . . . . . . .
—2,913,808 9,2
Kansas . . . . . . . . . . . . . . . 2,363,679 4.7Michigan, . . . . . . . . . . . . . . 9,262,078 4.0Minnesota . . . . . . . . . . 4,075,970 28.4Missouri ..., . . . . . . . . . 4,916,686Nebraska . . . . . . . . . . . . .
—1,569,825 31.1
North Dakota . . . . . . . . . . 652,717 56.1Ohio . . . . . . . . . . . . . . 10,797,630South Dakota . . . . . . . . . . .
—690,768 63.3
Wisconsin . . . . . . . . . . . . . 4,705,767 31.9
NortheastConnecticut . . . . . . . . . 3,107,576 0.6Maine . . . . . . . . . . . . . . . 1,124,660 30.4Massachusetts . . . . . . . . 5,737,037New Hampshire. . . . . . .
—920,610
New Jersey . . . . . . . . . . . .—
7,364,823New York . . . . . . . . . . . . . . 17,558,072
—17,3
Pennsylvania . . . . . . . . . . . 11,863,895Rhode Island . . . . . . . . .
—947,154
Vermont ., . . . . . . . . .—
511,456 —
Total United States .. ..226,545,805 1,366,676 339,836 30,265 996,575 24.90/a 2,2% 72,90/aaE~kimos ~nd Aleuts residing in Alaska. An additional 14,133 Eskimos and Aleuts Ilve outside of Alaska and are not Included in this table
SOURCE, U.S. Bureau of the Census, PC80-S1.13, 1984.
46577
38,270188,93315,7682,6555,644
13,5448,567
23,90623,50712,27342,4362,898
0 . 3 %——
25.195.388,9
100,054.236.064.422.388.464.171.241.1
——
31
33921,556
1217
310
——
2,520.1
0.10.5
—
7,5029,3641,307
99619,1347,4423,518
11,9697,8236,131
64,536169,292
5,6655,013
39,7409,2111,555
7,5029,3641,307
99617,8317,4123,518
11,5747,8232,965
59,692164,543
4,9375,013
38,8819,0931,555
100.0100,0100.0100.093.299.6
100,096.7
100.048.492.597,287.1
100.097.898.7
100.0
——
———————
————
185 1.5—
6.7410————
——— —
——— —
15,8467,6825,369
15,25639,73434,83112,1299,145
20,12011,98544,94829,320
15,8467,6824,877
14,54137,94424,71212,1296,2997,080
11,98511,82319,880
100.0100.090.895.395.570.9
100.068.935,2
100.026.367.8
— ———
———
0.50.6
183218
——
1,753—
4,65779
8,7
10.40.3
4,4314,0577,4831,2978,176
38,9679,1792,872
968
4,4042,8227,4821,2978,176
32,2339,1792,872
968
99.469.6
100.0100.0100,082,7
100.0100.0100.0
— ———
——— —
————
——
——
——

—
Ch. 3—Overview of the Current Indian Population ● 6 3
Figure 3-2.— Distribution of the American Indian,Eskimo, and Aleut Population, 1980
(inside and outside identified areas and villages)
Remainder of U S (63°/0)
[ /I
-Tribal trust lands (2.10%)
Historic areas of OK (8.2%)(excluding urbanized areas)
Native villages (2.8%)
YReservations (23.9%)
SOURCE U S Bureau of the Census, PC80-S1.13, 1984
Table 3-3.–32 Reservation States as of 1985
AlabamaAlaskaArizonaCaliforniaColoradoConnecticutFloridaIdaholowaKansasLouisiana
MaineMichiganMinnesotaMississippiMontanaNebraskaNevadaNew MexicoNew YorkNorth CarolinaNorth Dakota
OklahomaOregonPennsylvaniaRhode IslandSouth DakotaTexasUtahWashingtonWisconsinWyoming
SOURCE U S Department of Health and Human Serv!ces, Public Health SerwIce, Health Resources and Serwces Adminlstratlon, Ind!an Health Sew-Ice, Charf Series Book, 1985
considered the least accurate and the most diffi-cult to estimate because of the large populationscattered over large geographic areas” (208). Theprimary purpose of BIA’s population publicationis for the information it contains on employmentand earnings on Indian reservations.
Appendix A summarizes 1980 U.S. census, IHS,and BIA estimates of the Indian population orga-nized by IHS area, along with tribal estimateswhen available. The fourth column of appendixA has been included to show tribal versions ofpopulation that OTA received from some tribesor from enrollment figures provided by BIA.Apparent discrepancies exist between what sometribes may claim their population to be and what
the Bureau of the Census and BIA report. IHSdoes not compute service population by tribe buthas provided OTA with a list of tribes served byeach of its service units.
Implications of Varying Estimates
The discrepancies in population size are at-tributed largely to the varying definitions of “In-dian” that are used by each of these sources. Suchdefinitions are included in regulations governingBIA, IHS, and other governmental programs serv-ing Indians. Moreover, many tribes maintain rollsseparately from those kept by BIA and its localagencies,
A major difference between tribal rolls andcensus or BIA estimates is that many tribes countindividuals without regard to their residence. Thetribal rolls list full-fledged members, and may in-clude others who are enrolled but do not have thefull privileges of members such as voting rightsor rights to share in tribal benefits such as occa-sional per capita payments. The 1980 census sup-plementary survey of Indians living on reserva-tions found that 87 percent were enrolled in theirtribe (152). According to Vine Deloria, a contem-porary Indian social theorist, the passage of theIndian Reorganization Act and the Oklahoma In-dian Welfare Act in 1934 and 1936 made certainFederal services available to tribal members thathad not been available in previous decades, andtribes may have developed special categories oftribal membership to enable more individuals tobecome eligible for some of these Federal services(29).
One of the reasons that IHS regulations extendeligibility to nonmembers of tribes is in recogni-tion of the variations across tribes in the require-ments for tribal membership. Tribal rolls may beclosed and reopened infrequently, a situation thatwould make it difficult for Indians who are noton their tribal rolls to prove their eligibility ifmembership were the sole criterion for servicesfrom IHS. Tribal edict or personal choice (for po-litical reasons, some individuals choose not to bemembers of their tribes) keep many Indians frombecoming members of their tribes. Though tribalmembership requirements are not uniform across

64 ● Indian Health Care
the United States and in some cases may not seemfair to the individuals concerned, when chal-lenged, courts have consistently upheld the sover-eign right of tribes to determine their own rulesgoverning membership.
Having an accurate estimate of the number ofIndians, especially those living within or in closeproximity to reservations, is necessary for plan-ning of services delivery, allocating resources toprovide services, and eventually for detectingwhether the services provided have had any im-pact. The size of a given population being served
is generally a good indicator of the expected de-mand for the services being offered, but withinthe IHS system, demand for health care variesconsiderably by area and is not necessarily relatedto its estimated population size (see ch. 5). IHSpreviously estimated its service population with-out regard to actual users of its services, but a pa-tient registration system instituted in January 1984now accounts for current users of IHS services andshould improve IHS’s use of population data forplanning purposes.
CHARACTERISTICS OF THE AMERICAN INDIAN,ESKIMO, AND ALEUT POPULATIONS
The most important point to be made about theIndian population in the United States is that eachIndian tribe has its own unique culture, history,geography, and demography. No single variableor socioeconomic indicator encompasses the di-verse characteristics of Indians and Alaska Na-tives in this country.
The characteristics presented here, which aredrawn from census reports, are based on a sam-ple and are therefore subject to errors. Thesedescriptive statistics are also limited by the factthat they are national aggregates. National meas-ures of the Indian population and the U.S. allraces population may not accurately describe lo-cal conditions nor reflect changing situations,since they are collected at one point in time. (Fora more complete discussion of the sources of sta-tistical error in census data, see the “Accuracy ofData” appendix in any of the Bureau of the Cen-sus’ subject reports. )
Characteristics cited in this section are for In-dians throughout the United States except wherecertain subpopulations are specified. “ReservationIndians, ” for example, include Indians on identi-fied reservations and in historic areas of Okla-homa (excluding urbanized areas).
The size of the Indian population living on res-ervations in 1980 ranged from 104,978 on theNavajo reservation to O on 21 reservations. ThePine Ridge Reservation of the Oglala Sioux had11,946 Indian persons. The Blackfeet, Montana;
Fort Apache, Gila River, Hopi, Papago, and SanCarlos reservations of Arizona; Rosebud, SouthDakota, and Zuni, New Mexico each had morethan 5,500 Indian residents, or 14.8 percent of allreservation Indians when combined. The 10 mostpopulous reservations had 49 percent of all res-ervation Indians (see figure 3-3).
The Indian population is residing in urban areasmore than ever before. As of 1980, 22 percent ofthe Indian, Eskimo, and Aleut population livedin central cities, 32 percent lived in urbanizedareas outside central cities, and the remaining 46percent chose nonmetropolitan residences (see fig-ure 3-4). In 1970, 19.9 percent of American In-dians lived in central cities, 25 percent in otherurban areas, and 55.1 percent in rural areas. The10 Standard Metropolitan Statistical Areas (SMSAs)having the largest number of Indians, Eskimos,and Aleuts in 1980 (in descending order) were LosAngeles-Long Beach, Tulsa, Oklahoma City,Phoenix, Albuquerque, San Francisco-Oakland,Riverside-San Bernardino-Ontario, Seattle-Everett,Minneapolis-St. Paul, and Tucson (see figure 3-5). Each of these cities has an urban Indian healthprogram with IHS funding, though their level ofservices may vary. Table 3-4 shows the distribu-tion of Indians by urban or rural residence andsex as well as the total number of persons of allraces for each State. The Eskimo and Aleut pop-ulation has begun a similar shift away from theirtraditional homelands, though the majority, 74percent, of all Eskimos and Aleuts still lived inAlaska in 1980 (see figure 3-6).

Ch. 3—Overview of the Current Indian Population ● 6 5—.——
Figure 3.3.–Ten
.
Reservations With Highest Number Figure 3-5.—Ten SMSAs With the Highest Numbersof American Indians, Eskimos, and Aleuts, 1980of Indians, 1980 -
Navajo, AZ-NM-UT Los Angeles-Long Beach
48,120
Tulsa
38,489
Oklahoma City
I pine Ridge, SD
I I 11,946
PhoenixI Papago, AZ
Fort Apache, AZ
16,660San Francisco-Oakland
Riverside-San Bernardlno-Ontario
Seattle-Everett
16,596
Minneapolis-St, Paul
15,950
Tucson
14,928
I Rosebud. SD
I 15,688
I I I 1 1 Jo 10,000 20,000 30000 40000 50000 60,000SOURCE U S Bureau of the Census PC80.1 BI 19830 4,000 8,000 12,000 16,000 20,000
SOURCE U S Bureau of the Census PC80SI 13 1984
Figure 3.4. —Urban and Rural Residence for AmericanIndian, Eskimo, and Aleut Populations, 1980 Figure 3-6.— Distribution of the Eskimo and Aleut
Population, 1980American Indian,
● ● “*.Eskimo, and Aleut 22
* ,,+
32 ;0 q 46%54 % b .
● t. .
. .
U S all races74% 30
.-. 4
.“. 4
In Alaska
34,144/
8,090
] Outside Alaska
6,115L I 1 1 1 1 I J
80 60 40 20 0 20 40 60 80Percent
o 10000 20,000 30,000 40,000Urban residence Rural residence
Eskimo Aleut
SOURCE U S Bureau of the Census, PC80.SI 13 1984

66 • Indian Health Care
Table 3-4.—American Indians, Eskimos, and Aleuts, by State, Urban/Rural Residence, and Sex, 1980
American Indians, Eskimos, and Aleuts
Us., Urban Rural Total urban and rural
States all races Male Female Male Female Male Female Both sexes
Alabama . . . . . . . . . . . . . . .Alaska. . . . . . . . . . . . . . . . .Arizona ., . . . . . . . . . . . . . .Arkansas . . . . . . . . . . . . . .California . . . . . . . . . . . . . .Colorado. . . . . . . . . . . . . . .Connecticut . . . . . . . . . . . .Delaware . . . . . . . . . . . . . .District of Columbia. . . . .Florida . . . . . . . . . . . . . . . .Georgia . . . . . . . . . . . . . . . .Hawaii . . . . . . . . . . . . . . . . .Idaho . . . . . . . . . . . . . . . . . .Illinois . . . . . . . . . . . . . . . . .Indiana . . . . . . . . . . . . . . . .lowa . . . . . . . . . . . . . . . . . .Kansas . . . . . . . . . . . . . . . .Kentucky . . . . . . . . . . . . . .Louisiana . . . . . . . . . . . . . .Maine . . . . . . . . . . . . . . . . .Maryland . . . . . . . . . . . . . .Massachusetts . . . . . . . . .Michigan . . . . . . . . . . . . . .Minnesota . . . . . . . . . . . . .Mississippi . . . . . . . . . . . .Missouri . . . . . . . . . . . . . . .Montana . . . . . . . . . . . . . . .Nebraska . . . . . . . . . . . . . .Nevada . . . . . . . . . . . . . . . .New Hampshire . . . . . . . .New Jersey . . . . . . . . . . . .New Mexico. ......, . . . .New York . . . . . . . . . . . . . .North Carolina . . . . . . . . . .North Dakota . . . . . . . . . . .Ohio . . . . . . . . . . . . . . . . . .Oklahoma . . . . . . . . . . . . . .Oregon . . . . . . . . . . . . . . . .Pennsylvania . . . . . . . . . . .Rhode Island . . . . . . . . . . .South Carolina . . . . . . . . .South Dakota . . . . . . . . . . .Tennessee . . . . . . . . . . . . .Texas . . . . . . . . . . . . . . . . .Utah . . . . . . . . . . . . . . . . . .Vermont . . . . . . . . . . . . . . .Virginia . . . . . . . . . . . . . . . .Washington . . . . . . . . . . . .West Virginia . . . . . . . . . . .Wisconsin . . . . . . . . . . . . .Wyoming . . . . . . . . . . . . . .
3,893,888401,851
2,718,2152,286,435
23,667,9022,889,9643,107,576
594,338638,333
9,746,3245,463,105
964,691943,935
11,426,5185,490,2242,913,8082,363,6793,660,7774,205,900
124,6604,216,9755,737,0379,262,0784,075,9702,520,6384,916,686
786,6901,569,825
800,493920,610
7,364,8231,302,894
17,558,0725,881,766
652,71710,797,6303,025,2902,633,105
11,863,895947,154
3,121,820690,768
4,591,12014,229,191
1,461,037511,456
5,346,8184,132,1561,949,6444,705,767
469,557
1,6749,211
23,0692,117
80,3236,6711,826
225479
7,2432,5301,3111,6836,9852,7021,9115,4601,2593,125
7173,3142,993
12,5539,883
7323,9574,6402,3013,959
3653,389
14,69912,854
7,1612,0144,623
40,4507,8633,3981,1161,2565,5821,545
16,6555,014
1423,615
17,129273
6.716
1,65410,39325,127
2,27683,8556,4401,889
243552
7,0432,1621,0461,7637,0812,7712,0125,430
9722,943
7363,3433,090
13,04810,563
6783,9875,1702,4594,131
3343,536
16,73214,7387,1752,1294,804
43,6198,0993,6501,2581,1186,2341,495
15,7505,372
1953,055
17,804282
7,0211,038
2,14923,33151,328
2,49219,1152,556
413416
—2,6061,548
1933,5211,1111,210
7732,251
6553,0861,317
681800
7,2697,3382,3052,209
13,8082,2172,645
344748
36,3286,323
24,9097,9401,442
42,3995,7071,288
2491,690
16,3981,0723,9864,371
3291,405
13,074505
7,8752,470
2,09721,16853,221
2,52618,076
2,401399423
—2,3411,376
1963,5441,1061,142
7452,211
7052,9001,287
672853
7,1807,2322,4312,168
13,6522,2102,554
295695
38,3545,667
25,4078,0601,361
42,9815,6451,129
2491,671
16,734983
3,6844,486
3021,366
12,797532
7.887
3,823 3,75132,54274,3974,609
99,4389,2272,239
641479
9,8494,0781,5045,2048,0963,9122,6847,7111,9146,2112,0343,9953,793
19,82217,2213,0376,166
18,4484,5186,604
7094,137
51,02719,17732,070
9,9546,065
82,84913,5704,6861,3652,946
21,9802,617
20,6419,385
4715,020
30,203778
14,5913,522
31,56178,3484,802
101,9318,8412,288
666552
9,3843,5381,2425,3078,1873,9132,7577,6411,6775,8432,0234,0153,943
20,22817,7953,1096,155
18,8224,6696,685
6294,231
55,08620,40532,58210,1896,165
86,60013,7444,7791,5072,789
22,9682,478
19,4349,858
4974,421
30,601814
14,9083,556
7,57464,103
152,7459,411
201,36918,0684,5271,3071,031
19,2337,6162,746
10,51116,2837,8255,441
15,3523,591
12,0544,0578,0107,736
40,05035,0166,146
12,32137,270
9,18713,289
1,3388,368
106,11339,58264,65220,14312,230
169,44927,314
9,4652,8725,735
44,9485,095
40,07519,243
9689,441
60,8041,592
29,4991,052 2,518 7,078
Total United States . . . 225,545,805 361,764 378,295 340,195 339,619 701,959 717,914 1,419,873SOURCE: US. Bureau of the Census, PC80-1-B1, 1983,

Ch. 3—Overview of the Current Indian Population
Changes in the regional distribution of Indiansfrom 1970 to 1980 were apparently minute. In theMidwest, the Indian population declined by 1 per-cent, and in the South, it increased by 2 percentbetween the 1970 and 1980 censuses. The regionwith the most (49 percent) Indians is the West.The South had 27 percent of the Indians in the1980 census, the Midwest had 18 percent, and theNortheast had 6 percent (figure 3-7). (For a listof States by region, see table 3-2, above. )
Four States dominate the list of 10 States withthe largest number of Indians (figure 3-8). Indianpopulation growth between 1970 and 1980 washighest in the State of California, which grew by118 percent to 201,489—more than doubling itsIndian population in 10 years. The Indian popu-lation in California is concentrated in urban areas(81 percent). Oklahoma had the second largest in-crease, from 98,468 in 1970 to 169,459 in 1980.
Figure 3-7.— Percent of Total U.S. American IndianPopulation, by Region of Residencea: 1970 and 1980
60
50
40
30
20
10
0
49 49
2527
—West South Midwest Northeast
American Indian population only, excluding Eskimos and Aleuts
a For a list of states by region, see table 3-2.
SOURCE U S Bureau of the Census, PC(2)-1 F, 1973 and PC80-S1-13, 1984
● 6 7
Figure 3-8.—Ten States With the Largest AmericanIndian, Eskimo, and Aleut Population, 1980
California I 201,489
North Carollna 84,652
Alaska 64,103
Washington 80,604
South Dakota 44,988
Texas 40,440
Michigan 40,070
I 1 I t t 1
0 50.000 100,000 150,000 200,000 250,000
SOURCE U S Bureau of the Census, PC80-S1-13, 1984
Two other States, Arizona and New Mexico, hadmore than 100,000 Indians in 1980, with 152,745and 107,481, respectively.
Median income (for American Indian families)in 1979 was $13,678, the figure was $13,829 (forEskimo families), and $20,313 for Aleut families.Indian families living on reservations had medianincomes in 1979 of $9,924. The corresponding fig-ure for U.S. families of all races was $19,917 (seefigure 3-9). (Median income is the amount atwhich half the people are below and half abovethe quoted figure. )
The difference in poverty rates (the percentageof the population whose income falls below thepoverty level) between American Indians and thetotal population provides another example of theextent to which the U.S. all races population isbetter off than the Indian population. In 1980, thepoverty rate for American Indian persons was27.5, 28.8 for Eskimos, and 19.5 for Aleuts; whencombined, poverty occurs at more than twice therate of 12.4 for the U.S. all races population,

68 ● Indian Health Care
Figure 3-9.— Median Family Money Income in 1979
25,000
20,000
15,000
(n%=2
10,000
5,000
American Eskimo Aleut U. S., ReservationIndian
I I
I American Indian, Eskimo, or Aleut
all races Indians
U. S., all races
❑ Reservation Indians
SOURCE U S Bureau of the Census, PC80-1-C1, 1983 and PC80-21D, part 1, 1985
These are believed to be decreases in the povertyrates compared to 1970. Only one racial grouphad a higher poverty rate; 29.9 percent of all blackpersons reported incomes in 1979 that were be-low the poverty level. Poverty among Indians onreservations is significantly higher, with 44.8 per-cent of persons who had income in 1979 belowthe poverty level (see figure 3-10). (Data on pov-erty status are derived from responses to theCensus Bureau’s questions on income level in1979. Poverty thresholds are based on income,size of household, age of householder, and thepercentage of income that families spend on food.The number of individuals below the poverty levelis the sum of related and unrelated persons in fam-ilies with incomes below the poverty level. )
Figure 3-10.— Poverty Rates of Persons, 1970 and 1980
50
45
40
35
30
al%
$ Z5$)
2
20
15
10
5
0
(percent below poverty level)
44.8
38.3
—
728.
—
9.
—
13.7
American American Eskimo Aleut Reservation U. S., all racesIndian Indian Indians
1970 ~ 1 9 6 0 — { 1970 1980
❑ American Indian, Eskimo, or Aleut
❑ Reservation Indians
U. S., all races
SOURCE US Bureau of the Census, PC(2).1 F, 1973, PC80.1.C1, 1983, andPC80.2-1 D, part 1, 1985
The number of families maintained by women,which may be related to changes in poverty sta-tus, rose between 1970 and 1980 in the UnitedStates and among Indians. In 1980, for the U.S.all races population, 14 percent of all families weremaintained by women, whereas 22.7 percent ofAmerican Indian families, 21.3 percent of Eskimofamilies, 17,4 percent of Aleut families, and 25.8percent of reservation families were maintainedby women (see figure 3-11).
Unemployment rates, another indicator of rela-tive economic well-being, show that unemploy -

Ch. 3—Overview of the Current Indian Population Ž 69
Figure 3-12.—Unemployment Rates for AmericanIndians, Eskimos, and Aleuts, 1970 and 1980
Figure 3-11.— Families Maintained by Women,1970 and 1980 (percent of families)
3 0
27.8
258—
—
25
18
227
—
2 1 3
20185
1 7 4
—
1 4 8
—
14
3.0
11
10
65
Lll
445
0American American Eskimo Aleut Reservation U S all races
Indian Indian Indians
1970 ~ 1980 —————i 1970 1980
— — — —— —American American Eskimo Aleut Reservation U S , all races
Indian Indian Indians
1970 ~ 1980 ~ 1970 1980
American Indian, Eskimo, or Aleut
Reservation Indians
American Indian, Eskimo, or Aleut
Reservation Indians
U S , all races U S , all races
SOURCE U S Bureau of the Census, PC(2).1 F, 1973 PC80.1-C1, 1983 andPC80.2.1 D, part 1, 1985
For over 507,000 Indians 16 years old and overwho were employed in 1980, jobs held werelargely in the technical, sales, and administrativesupport occupations (24.2 percent), followedclosely by jobs as operators, fabricators, andlaborers (23 percent), and then by service occu-pations (18 percent). Three occupational catego-ries with the highest numbers of Indians includedfood service, cleaning, and building service work-ers; administrative support occupations, especiallysecretaries and typists; and professional special-ties with highest representation in the job cate-gory including teachers, librarians, and coun-selors. These top three categories included 39.6
SOURCE U S Bureau of the Census PC(2). I F 1973 PC801 -Cl, 1983 andPC80 21 D, part 1 1985
ment rates for Indians were more than twice theU.S. all races rates of 4.4 and 6.5 percent in 1970and 1980, respectively (see figure 3-12). In 1980,13 percent of American Indians, 18.5 percent ofEskimos, and 14.8 percent of Aleuts were unem-ployed. On reservations, unemployment in 1980was 27.8 percent of the labor force—more thanfour times higher than the U.S. all races rate. (Un-employment figures include civilians 16 years oldand over who were neither “at work” nor “witha job but not at work, ” who were looking forwork during the last 4 weeks and were availableto accept a job, and who were waiting to be calledback to a job from which they had been laid off. )

70 ● Indian Health Care
Figure 3-13.-Occupation of Employed AmericanIndians, Eskimos, and Aleuts, 1980
(percent of employed persons 16 years and over)
Precision production,
F
15
craft, and repair13
Farming, forestry, and 4
fishing3
18Service occupations
13
I 1 1 I 1 I I 10 5 10 15 20 25 30 35
Percent
[American Indians, Eskimos,
and Aleuts
U.S. aft races
SOURCE U S Bureau of the Census, PC80.1-C1, 1983
percent of all Indian workers age 16 and over in1980. The remaining workers were moderatelywell represented in other occupations (see figure3-13).
One difference in employment patterns by sexamong Indians is that a slightly higher percent-age of female workers than male workers heldmanagerial or professional jobs, although in 1980there were only 854 Indian women out of a totalof 5,804 Indian engineers and natural scientists.There were only 150 Indian women and 713 In-dian men in health-diagnosing occupations.
Further, a substantially higher percentage of In-dian women than men were employed in sales,technical, administrative support, and service oc-cupations. A similar edge was held by Indian men
over women in the precision production, craft,repair, machine, fabricating, and labor occupa-tions. These gross comparisons are based on onlysix major occupational categories that were de-lineated by the U.S. Bureau of the Census to rep-resent as closely as possible the structure of theAmerican economy in 1980. Clearly, the occupa-tional categories are oversimplified here. It is alsoimportant to note that reporting and coding er-rors have been known to be particularly prob-lematic with individual, self-reported occupations,including those collected by the census.
Many people assume that Federal, State, andlocal governments (including tribal governments)are the major employers of Indians. This percep-tion is most likely due to the relatively high visi-bility of Indians employed in the public sector,especially those employed by BIA and IHS. Ac-tually, American Indian, Eskimo, and Aleutworkers in 1980 were predominantly employedin private sector jobs. Sixty-six percent of Indianworkers 16 years of age and over worked in theprivate sector, another 5 percent were self-em-ployed, and a marginal number were unpaid fam-ily workers. Government workers comprised 29percent of the total with 11 percent, 6 percent,and 12 percent employed in Federal, State, andlocal government jobs, respectively.
Educational attainment includes within eachcategory of the highest grade of school completed:1) the number of persons who reported the indi-cated grade as the highest grade attended and thatthey had finished it; 2) those who attended butdid not complete the next higher grade; and 3)persons still attending the next higher grade.Largely because of government and tribal scholar-ship or financial aid programs, American Indianswere receiving more education beyond highschool between 1970 and 1980. In 1980, 16 per-cent of the U.S. all races population over 25 yearshad completed 4 or more years of college; the per-centages for Aleuts, Eskimos, and American In-dians were 12, 5, and 8 percent, respectively. Bycomparison, the number of persons completing4 years of high school and some college werecloser across each of these four groups; 50 per-cent of the U.S. all races population, 47 percentof Aleuts, 39 percent of Eskimos, and 48 percentof American Indians 25 years old and over had

Ch. 3—Overview of the Current Indian Population ● 7 1
Figure 3-14.— Educational Attainment of Persons 25Years Old and Over, United States All Races and
Indian Populationa: 198070
60
50
40Ealokn.
30
20
10
0American Eskimo Aleut United States,
Indian All races
Four years of high Four or more yearsof college
aThe two categories combl ned (figure at top of each column) represent the per-cents of the population groups that have, at a minimum, graduated from highschool
SOURCE U S Bureau of the Census, PC80-1-C1, 1983
high school diplomas or the equivalent plus somecollege background (see figure 3-14). In 1980, 43.2percent, or roughly three out of every seven res-ervation Indians 25 years old and over, were highschool graduates.
Median age in 1980 was 23.4 for American In-dians, 21.3 for Eskimos, 24,5 for Aleuts, and 19.7for reservation Indians, compared to 30.0 for theU.S. all races population.
One would expect that educational attainmentrates would increase as the Indian populationages, and this might indeed be the overall effectnationally; but recently published data for reser-vation Indians suggest that educational opportu-nities are not as widely pursued by reservationIndians as they are among Indians living off res-
ervations. The Bureau of the Census reports that27.1 percent of reservation Indians 16 to 19 yearsold were not enrolled in a regular school and werenot high school graduates in 1980. These persons,in all likelihood, were drop-outs. If individualswere enrolled in trade or business schools, companytraining, or were receiving schooling through atutor, they were counted as being enrolled onlyif the course credits they would obtain were trans-ferable to a regular elementary school, highschool, or college. So this indicator, which in-cludes only “regular schooling, ” might overstateeducational deficiencies slightly. Nevertheless,only 2.6 percent of reservation Indians 20 to 34years old, an age group spanning 15 years, wereenrolled in school.
Unpublished findings based on an analysis ofthe Bureau of the Census’ 1980 public-use micro-sample data set indicate that for certain Indians25 years and older living on or near a reserva-tion, the probability of completing 4 or moreyears of postsecondary education was the lowestthat it had been for 50 years. In the 25 to 30 and61 to 65 year age groups, Indian men and womenwho had finished high school had less than a 10percent chance of ever completing 4 or more yearsof college. The highest probabilities of complet-ing postsecondary education and perhaps the besteducational opportunities were found among In-dian men in three age groups comprising thosewho were 41 to 55 years of age in 1980. This isprobably due to GI bill educational benefits, sincethe same phenomenon does not exist among In-dian women (114).
A recent study of over 9,500 Indian studentsat the University of New Mexico (UNM) foundan alarmingly high propensity for failure to com-plete postsecondary education programs. An In-dian student at UNM completing an undergradu-ate degree in 4 years and a master’s degree in 2years is a rare exception. Tentative findings showthat the median number of years it has takenUNM’s Indian students to complete an associatedegree is 8 if a student attended UNM on a part-time basis. A small minority of students, around1 percent of the total included in the study, re-quired a median number of 5 years to completea bachelor’s degree if they undertook 13 or morecredit hours per semester (53). While these find-

72 Ž Indian Health Care
ings perhaps should not be generalized to all In-dian students enrolled in universities, research ofthis type may aid in explaining why Indian stu-dents have greater difficulty completing degreeprograms than their non-Indian counterparts.Budgets of many Indian scholarship programs, in-cluding those of private foundations, have beencut back in recent years, and restrictions on thenumber of semesters for which support can be ex-tended create financial barriers that many Indianstudents cannot overcome. While national leveldata on Indian educational attainment appearpositive, closer examination over time by agegroup, sex, and residence indicate serious deficien-cies in educational opportunities for Indians. In-terrupted, nontraditional educational careers seemto prevail, and therefore the economic returns re-sulting from higher education are probably notthe same for Indians as those experienced by thegeneral U.S. population.
The lack of complete plumbing facilities for ex-clusive use was no longer a problem of majorproportion in 1980 in the United States as a whole.On the other hand, American Indian, Eskimo, andAleut housing units on average were about 20years behind the U.S. all races average in this re-spect. The last time housing units in the UnitedStates had experienced plumbing deficiencies thatwere roughly equal to the 1980 average for In-dian housing units was in 1960. Worse yet, in1980, more than 50 percent of all Eskimo hous-ing units lacked plumbing for exclusive use—78.9percent of these households had no plumbing fa-cilities at all (see figure 3-15). Among over 81,000Indian housing units on reservations, 24.1 percentwere without complete plumbing for exclusive usein 1980.
Settlement patterns of Indians in SMSAs showthat urban Indians are a highly mobile group.According to the 1980 census, approximately 52million housing units in the United States wereowner-occupied, and 29 million were occupied byrenters. In other words, 64 percent of all U.S.housing units were occupied by owners them-selves. Each percentage point represents more thanhalf a million (517,964) housing units for theUnited States as a whole. Of the 60 million U.S.housing units within SMSAs, 37 million werelived in by owners and 23 million by renters.
—
Figure 3-15.—Percent of Occupied Housing UnitsLacking Complete Plumbing Facilities, 1980
9.8
n
50.8
24.1
14.0
American Eskimo Aleut Reservation U. S.,Indian Indians all races
American Indian, Eskimo, or Aleut
n Reservation Indians
US,, all races
SOURCE U S Bureau of the Census, HC80-1-A1, 1983, and PC80-2.1 D, part 1,1985.
Thus, 61 percent of U.S. householders in SMSAswere in owner-occupied housing. In rural areas,an even higher percentage of U.S. housing units,80 percent, were occupied by owners,
According to the 1980 census, trends in homeownership were similar in rural and urban areas.Fifty-six percent of the 52 million owner-occupiedhousing units in the United States had been movedinto since 1970; 21 percent were established be-tween 1960 and 1969, 12.8 percent between 1950and 1959, and only 9.7 percent in 1949 or earlier.

In SMSAs, 56 percent of all householders hadmoved into owner-occupied housing since 1970;22.1 percent had done so between 1960 and 1969,13.4 percent between 1950 and 1959, and 8.5 per-cent in 1949 or earlier. In rural areas, 60 percenthad moved into owner-occupied housing unitssince 1970; 20 percent had done so between 1960and 1969, 10 percent between 1950 and 1959, and11 percent in 1949 or earlier.
In 114 SMSAs where the combined AmericanIndian, Eskimo, and Aleut population was greaterthan or equal to 1,000, the 1980 census identified99,998 Indian householders in owner-occupiedhousing units. Sixty-eight percent of these house-holds—the vast majority–had been establishedsince 1970; 19 percent between 1960 and 1969, and13 percent in 1959 or earlier (contrasted with theU.S. a]] races average of 22.5 percent) (see figure3-16). Each percentage point in SMSAs with 1,000or more Indians, Eskimos, and Aleuts represents997 housing units with an Indian householder.
Among 117,201 Indian householders in renter-occupied housing units in the same 114 SMSAs,54 percent (representing 63,501 renter-occupiedhousing units) had just moved into these unitswithin the 15-month period prior to the censusdate. Thirty-one percent had moved into theirrented units between 1975 and 1978, 8.8 percentbetween 1970 and 1974, and 6.6 percent in 1969or earlier (see figure 3-17). For every five Indianrenters living in SMSAs, roughly two had movedone or more times within the same metropolitanarea, and another two had lived in the same placeduring the 5 years prior to the 1980 census.
On an individual level, mobility among urbanIndians is pronounced. For persons 5 years andolder, the Bureau of the Census ascertained resi-dence in 1975. There were 620,502 Indian personswho were at least 5 years old living in the top 114SMSAs in 1980. Between 1975 and 1980, 58.8 per-cent of these individuals had lived in a differenthouse in the United States, 39.6 percent lived inthe same house, and 1.6 percent lived abroad. Ofthe 58.8 percent (or 364,834 individuals) who livedin a different house in the United States, 136,229had moved in from outside of their current SMSA;of these, 86,753 had lived in a different SMSA,and 49,476 had moved in from nonmetropolitansettings. In 1975, 121,528 or one-third of those
Ch. 3—Overview of the Current Indian Population Ž 73
Figure 3-16.— Year Householder MovedInto Owner-Occupied Housing Unit
100
80
60
cal~
If
40
20
0U.S. Inside
SMSAs
1979 toMarch 1980
1970 to 1960 to1974 1969
Rural Top IndianSMSAsN = 114
1975 to1978
1959 orearlier
SOURCE U S Bureau of the Census, HC80 1 Al, 1983, and State reports onSMSAS tabulated by OTA
living in a different house in the United Stateslived in the central city of their current SMSA.Thus, of the 620,502 Indian persons 5 years andolder living in the top 114 SMSAs in 1980, theoverwhelming majority (90.4 percent) had beenmetropolitan dwellers for at least 5 years; 8 per-cent were new metropolitan dwellers; and 1.6 per-cent moved to a metropolitan area after havinglived outside of the United States (see table 3-5).
A point that should be made here is that notall Indians living off reservations and other des-ignated areas are urban Indians. According to theCensus Bureau, 63 percent of the Indian, Eskimo,and Aleut population in 1980 lived outside iden-

74 ● Indian Health Care
I
100
80
60
40
20
0
Figure 3-17.— Year Householder MovedInto Renter-Occupied Housing Unit
U.S.
I
InsideSMSAs
Rural
1979 to 1975 to 1970 toMarch 1980 1978 1974
Top IndianSMSAsN = 114
❑1969 orearlier
SOURCE: US Bureau of the Census, HC80-I-AI, 1983, and State reports onSMSAS tabulated by OTA
tified Indian areas (reservations, tribal trust lands,Alaska Native villages, and historic areas of Okla-homa excluding urbanized areas). Only 54 per-cent of the Indian, Eskimo, and Aleut population(compared to 74 percent of the U.S. all races pop-ulation) in 1980, however, lived in metropolitanareas (146). In other words, some nonreservationIndians lived in nonmetropolitan areas. A sepa-rate but closely related point is that some reser-vation Indians are urban Indians. A number ofIndian reservations are located in metropolitanareas inside SMSAs because of increasing growthof urban land areas nationally, and roughly 10percent of IHS’s estimated service population forits reservation-oriented direct care system residesn metropolitan areas.
Table 3-5.—Settlement Patterns of Indians in114 SMSAs With 1,000 or More American
Indians, Eskimos, and Aleuts
Number Percent
Residence in 1975:Persons 5 years old and over . . . . . . . . . 620,5021. Living in the same house . . . . . . . . . . 245,727 39.6°/02. Living in a different house
in the U.S. . . . . . . . . . . . . . . . . . . . . . 364,834 58.8Central city of this SMSA . . . . . . . . . . 121,528Remainder of this SMSA . . . . . . . . . . . 107,077Outside of this SMSA . . . . . . . . . . . . . 136,229
Different SMSA . . . . . . . . . . . . . . . . . 86,7533. Abroad . . . . . . . . . . . . . . . . . . . . . . . . . . 9,941 1.6SOURCE: U.S. Bureau of the Census, State reports on SMSAS tabulated by OTA.
FOUR PROJECTIONS OF THE EFFECT OF INTERMARRIAGEON THE NUMBER OF INDIAN DESCENDANTS
The U.S. Bureau of the Census reported in 1985that both American Indian women and men weremarrying non-Indians at rates exceeding 50 per-cent (149). In 1980, 119,448 out of 258,154 mar-ried American Indian, Eskimo, and Aleut coupleswere married within the same racial group; 130,256Indian individuals were married to either whites,blacks, Filipinos, Japanese, or Chinese; and 8,450Indians were married to individuals of other races.A married couple in the census is a husband andwife enumerated as members of the same house-hold and includes persons in formal as well ascommon-law marriages. Fourteen categories ofrace were used to determine whether husbands
and wives were of the same or different race. From1970 to 1980, the rate of marriage to non-Indiansincreased by almost 20 percentage points. In 1970,the rate was already quite high: 35.6 percent ofmarried Indian women were married to white hus-bands, and 33.4 percent of married Indian menwere married to white wives (97).
Births resulting from unions of Indians and non-Indians, whether consensual or within marriage,will greatly increase the number of persons claim-ing to be of Indian descent and will decrease theblood quantum of the “average” Indian in the longrun. Especially with respect to health care pro-

Ch. 3—Overview of the Current Indian Population . 75
vialed by IHS, the implications of this projectedgrowth for tribes in determining who is an Indianand for services provided on the basis of Indiandescendancy, are that growth must be accommo-dated by increasing services or by eventually re-stricting services to fewer individuals.
Figure 3-18 shows an estimated distribution ofreservation residents by Indian blood quantumfor 1950. This information, which had been col-lected in part to provide justification for the ter-mination and assimilation policies of the 1950s,is no longer available from BIA but may be avail-able on an individual tribal basis. BIA headquar-ters has no interest in maintaining such records,
Figure 3-18.— Distribution of Reservation Residents,by Quantum of Indian Blood for Selected Bureau of
Indian Affairs Administrative Areas,a
United States, 1950Adminlstratlve
area
Window Rock
Albuquerque
Phoenix
Portland
Aberdeen
Billings
Minneapolis
Sacramento
Fullblood
Quantum of Indian blood
1 / 2 b u t 1/4 but Less Non-
not full not 1/2 than 1/4 Indian
aThose for which data on blood quafltum were reported
SOURCE U S Department of Health, Educat!on, and Welfare, Surgeon Generalof the Publ[c Health Serv!ce, Hea/fh Serwces for fhe Arner/carr Ind(an(Washington, DC U S Department of Health, Education, and Welfare,Feb 11, 1957), p 14
because a one-fourth blood Indian is treated thesame as a full-blooded Indian for eligibility pur-poses, and certification for services takes place atthe agency (field) level (15).
A special version of an age-cohort, demo-graphic projection model specifying populationsfor each of nine different blood quantum group-ings was developed under an OTA contract. Themodel was applied under four sets of assumptionsto estimate the distribution of Indians by bloodquantum in the 32 reservation States for variousyears up to 100 years into the future (221).
Indians were tracked according to blood quan-tum in order to estimate the composition of theIHS service population for these years. The basicassumptions were that fertility rates, mortalityrates, and survival rates would remain constantfrom the base year of the projection, 1980, andthat they are the same for all nine blood quan-tum groupings. The model permits one to changeany of the basic assumptions. Such a change couldbe, for example, to assume that Indian mortalityrates would reach the current level of the U.S. allraces population by the year 2000. Throughoutall four scenarios, the fertility, mortality, and sur-vival rates are assumed to be the same.
To show the range of future possibilities in thecomposition of the Indian population, OTA cre-ated four different scenarios, varying the outmar-riage rates and distribution of the base popula-tion into blood quantum groups. In Scenario I,all Indians are assumed to be full-blooded in thebase year, and all unions are presumed to be withother Indians; hence, all offspring would also befull-blooded Indians. In Scenario II, the assump-tion again is that in the base year all Indians arefull-blooded, but the 53 percent outmarriage ratereported by the Bureau of the Census is used toassign probabilities that births resulting from In-dian/non-Indian unions will fall into specificblood quantum groups. The use of “marriage rate”and “outmarriage rate” is meant to represent“unions-potential for births, ” not actual marri-ages. Marriage and outmarriage “rates” are usedto determine potential populations of females towhich the fertility rates will be applied to calcu-late births, In Scenario III, an approximation ofthe 1950 blood quantum information is used; i.e.,

76 ● Indian Health Care
that 60.2 percent of all Indians are full-blooded,26.7 percent are half, 9.5 percent are one-fourthand 3.6 percent are less than one-fourth. Thesefigures have been adjusted by including an ap-proximated blood quantum distribution for Okla-homa area Indians. The Oklahoma area, whichcomprised 21 percent of the BIA population in1950, was assumed to have a blood quantumdistribution equal to that of Indians in theSacramento area. A constant outmarriage rate of53 percent was applied across all blood quantumgroups. Scenario IV is almost identical to Scenario111, except that the rate at which births result fromIndian and non-Indian unions is lowered to 40 per-cent. The rate has been adjusted downward totake into consideration births resulting from In-dian unions occurring consensually that may notbe reflected in the census data on marriage. Theinformation generated by the latter three projec-tions are used to examine variations in the futuresize of the Indian population at certain bloodquantum thresholds.
All of the data for OTA’s population projec-tions were made available by the IHS ProgramStatistics Branch and the U.S. Bureau of theCensus. Insofar as the projection model yields re-sults in actual numbers, OTA advises that theybe used cautiously. The data on which OTA’s pro-jections are based are presented below along witha description of the four scenarios outlined above.Results for 1985 and each 20-year period after thebase year through 2080 are printed in a summarytable at the end of this section. Twenty-yearperiods are used to approximate one generation,though in many areas, a generation in the Indianpopulation may be less than 20 years.
The distribution of the Indian population in the32 reservation States by age and sex is shown intable 3-6. (Note that the population in table 3-6,1.3 million, is for 32 States, compared to 1.4 mil-lion in all 50 States. ) Given the age-specific dis-tribution of fertility shown in table 3-7, one is ableto calculate that the total fertility rate is 2.92 (i. e.,the number of live births per woman of childbear-ing age were she to progressively follow through-out her life the birth pattern of each age group).Births to women in age groups less than 15 yearsold are not included; there were 413 live birthsto Indian women under 15 living in reservation
Table 3.6.—American Indian and Alaska NativePopulation for 32 Reservation States, by 5-Year
Age Group and Sex, 1980 Census Data
Age Total Male Female
<5 . . . . . . . . . 139,529 70,783 68,7465 to 9 . . . . . . . 136,361 68,859 67,502
10 to 14 .., . . . 144,882 73,496 71,38615 to 19 . . . . . . 156,749 79,005 77,74420 to 24 . . . . . . 134,769 67,184 67,58525 to 29 . . . . . . 112,519 55,193 57,32630 to 34 . . . . . . 95,949 46,810 49,13935 to 39, . . . . . 75,169 36,591 38,57840 to 44 . . . . . . 61,983 30,009 31,97445 to 49 . . . . . . 52,134 24,986 27,14850 to 54 . . . . . . 46,307 22,308 23,99955 to 59 . . . . . . 40,313 19,170 21,14360 to 64 . . . . . . 30,711 14,463 16,24865 to 69 ..., . . 25,817 11,748 14,06970 to 74 . . . . . . 18,076 8,062 10,01475 to 79 .., . . . 12,476 5,587 6,88980 to 84 . . . . . . 6,367 2,619 3,748>85 . . . . . . . . 5,339 2,126 3,213
Total . . . . . . . 1,295,450 638,999 656,451SOURCE U S Department of Health and Human Services, Publ!c Health %w.
!ce, Health Resources and Serwces Administration, Indian Health Serv.Ice, Population Statlsttcs Staff, September 1985, (O062K)/p 15
Table 3-7.—Age-Specific Fertility Rates for AmericanIndians and Alaska Natives by Age of Mother,
Reservation States, 1980-82
Age of Live Female Age-specific –
mother births population fertility rate15 to 19 . . . . . . 23,746 231,195 0 . 5 1 3 5 –
20 to 24 . . . . . . 39,764 199,239 0.998025 to 29 . . . . . . 25,672 168,981 0.759530 to 34 . . . . . . 12,170 144,327 0.421535 to 39 . . . . . . 4,062 113,089 0.179540 to 44 . . . . . . 834 93,873 0.044545 to 49 . . . . . . 41 79,705 0.0025SOURCE U S. Department of Health and Human Services, Publlc Health Se;.
ice Serwce, Health Resources and Services Adml ntstration, I ndlanHealth Service, Vital Events Staff, Apr 2, 1985 (262K}
States from 1980 to 1982. Survival rates for malesand females are computed as the proportion ofindividuals in each age group at one point in timewho survive into the next age group and timeperiod. Survival rates for the Indian populationare included in table 3-8. Information to calcu-late survival rates is available in “life tables” com-puted from vital statistics. For example, the In-dian male survival rate in the 15 to 19 age groupequals 97,518 divided by 97,792 or 0.99, whichindicates that 99 percent of the males aged 10 to14 can be expected to survive to the next agegroup, 15 to 19. (Numerical results by selected

Table 3-8.—Number of American Indians andAlaska Natives in 28 Reservation States,
Living at Beginning of Age Interval of100,000 Born Alive, 1979-81
A g e g roup ‘- Males Females
<5 . “. . . . . . : .:- 98,478 98,7055 to 9 ... , . . . . . . . . . . . 98,037 98,326
10 to 14 ., . . ... . . . 97,792 98,15915 to 19 ..., ... , ... . . 97,518 98,02220 to 24 ... . . . . . . . . 96,274 97,60525 to 29 . . ... . . 94,152 96,96630 to 34 . . ... . . ... 92,053 96,17035 to 39 . . . . . . . . . . . . . . 90,061 95,22740 to 44 . . . . . . . . . . . . . . 87,597 94,05045 to 49 . . . . . . . . . . . . . . 84,519 92,34550 to 54 . . . . . . . . . . . . . . 80,971 90,24555 to 59 . . . . . . . . . . . . . . 76,614 87,47360 to 64 . . . . . . . . . . . . . . 70,853 84,35565 to 69 . . . . . . . . . . . . . . 63,546 79,59970 to 74 . . . . . . . . . . . . . . 54,922 73,0437 5 t o 7 9 . . , . . . , . . , . . 45,531 65,52580 to 84 . . . . . . . . . . . 35,924 57,266>85 . . . . . 26,748 45,589SOURCE US Deparfmentof Health and Human Services, Publlc Heal;h Serv.
Ice Service, Health Resources and Services Admlnlstratlon, IndianHealth Servtce, Indian Health Serwce, Vital Events Staff, “AmericanIndian and Alaska Native Life Expectancy 19791981; June 1984
age group, sex, and total population are presentedlater in table 3-9 for all four projections.)
Ch. 3—Overview of the Current Indian Population . 77—
tions of females to which thebe applied to calculate births
Scenario II
We assume again that all
fertility rates will(see figure 3-19).
Indians are full-blooded in the base year but use an outmarriagerate of 53 percent as reported by the Bureau ofthe Census for 1980 to assign offspring to one ofnine blood quantum groups. For example, thechild of two full-blooded Indians remains in thesame blood quantum group as his or her parents;the child born of a mother who is one-quarter In-dian and a father who is one-half is assigned tothe three-eighths group. Assignment of offspringto specific blood quantum groups works cor-respondingly for succeeding generations. Underthe assumptions of Scenario II, doubling occursmore quickly than in Scenario I, in roughly twogenerations, shortly after the year 2000. Over the
Figure 3.19.—OTA Population ProjectionScenaro 1: No Outmarriage
5,000,000
Scenario I4,500,000
As a lower bound, assuming a 100 percentblood quantum (all Indians are full-blooded) inthe base year and presuming that all births resultfrom unions of Indians with Indians, the 1980 In-dian population of 1.3 million doubles in about45 years and grows to roughly 4.6 million Indiansin 2080. The unrealistic aspects of this scenarioare that all Indians in 1980 were not full-blooded,and the effect of out-unions is not captured. Sub-sequent scenarios use assumptions that comeprogressively closer to representing existing fac-tors likely to influence Indian population growth.One factor is the rate of births resulting from thepairing of Indians and non-Indians which, whenthey have children, have considerable potentialto increase the number of Indian descendants.Another factor that we try to account for is thedilution of Indian blood quantum on average thatnaturally occurs with intermarriage. Recall thatthe use of “marriage rate” and “outmarriage rate”or “out-union” rate is meant to represent “unions-potential for births, ” not actual marriages. These“rates” are used to determine potential popuIa-
4,000,000
3,500,000
3,000,000c0.-% 2,500,0003c12
2,000,000
1,500,000 tn
n I I I
1980 1985 2000 2020 2040 2060 2080Year
M a l e Female
SOURCE Off Ice of Technology Assessment

78 ● Indian Health Care
Table 3-9.—Age-Focused Population Projection SummaryAll Indians and Indian Descendants, Selected Years, 1980.2080
Projection year—1980 1985 2000 2020 2040 2060 2080
Scenario 1:Females:
<5 . . . . . . . . . . . . . . . . . . . . . . 68,746 88,219 96,872 128,134 156,038 192,632 242,15315 to 49 ..., . . . . . . . . . . . . . . . 349,494 386,945 471,487 573,843 729,875 913,817 1,134,337>60 . . . . . . . . . . . . . . . . . . . . . . 54,181 63,248 90,591 162,259 216,461 275,675 344,537
Total females . . . . . . . . . . . . – 656,451 722,136 927,549 1,213,497 1,527,602 1,901,854 2,375,910Males:
<5 . . . . . . . . . . . . . . . . . . . . . . . 70,783 91,819 100,826 133,364 162,407 200,495 252,03715 to 49 . . . . . . . . . . . . . . . . . . . 339,778 376,180 459,897 570,454 726,685 909,324 1,129,211>60 . . . . . . . . . . . . . . . . . . . . . . 44,605 48,332 58,589 98,319 127,190 168,897 210,712
Total males. . . . . . . . . . . . . . 638,999 697,196 880,879 1,139,494 1,429,027 1,785,740 2,230,092Both sexes:
<5 . . . . . . . . . . . . . . . . . . . . . . . 139,529 180,038 197,698 261,498 318,445 393,127 494,19015 to 49 ..., . . . . . . . . . . . . . . . 689,272 763,125 931,384 1,144,297 1,456,560 1,823,141 2,263,548>60 . . . . . . . . . . . . . . . . . . . . . . 98,786 111,580 149,180 260,578 343,651 444,572 555,249
Total both sexes . . . . . . . . . – 1,295,450 1,419,332 1,808,428 2,352,991 2,956,629 3,687,594 4,606,002
Scenario ii:Females:
<5 . . . . . . . . . . . . . . . . . . . . . . . 68,746 134,975 148,214 294,353 494,497 812,098 1,325,20115 to 49 ..., . . . . . . . . . . . . . . . 349,494 386,945 516,788 831,448 1,462,830 2,522,578 4,259,294>60 . . . . . . . . . . . . . . . . . . . . . . 54,181 63,248 90,591 162,259 216,461 398,248 689,583
Total females . . . . . . . . . . . . 656,451 768,892 1,126,293 1,890,643 3,158,066 5,358,944 9,054,242Males:
<5 . . . . . . . . . . . . . . . . . . . . . . . 70,783 140,484 154,263 306,367 514,680 845,245 1,379,29315 to 49 . . . . . . . . . . . . . . . . . . . 339,778 376,180 506,762 832,157 1,466,109 2,524,929 4,264,264>60 . . . . . . . . . . . . . . . . . . . . . . 44,605 48,332 58,589 98,319 127,190 249,578 435,220
Total males. . . . . . . . . . . . . . 638,999 745,861 1,087,193 1,837,183 3,085,888 5,247,613 8,861,834Both sexes:
<5 . . . . . . . . . . . . . . . . . . . . . . . 139,529 275,459 302,477 600,720 1,009,177 1,657,343 2,704,49415 to 49 . . . . . . . . . . . . . . . . . . . 689,272 763,125 1,023,550 1,663,605 2,928,939 5,047,507 8,523,558>60 . . . . . . . . . . . . . . . . . . . . . . 98,786 111,580 149,180 260,578 343,651 647,826 1,124,803
Total both sexes . . . . . . . . . 1,295,450 1,514,753 2,213,466 3,727,826 6,243,954 10,606,557 17,916,076
Percent one-half or more . . . . . . 100.0 100.0 100.0 81.2 56.9 32.9 15.7Percent one-fourth or more . . . . 100.0 100.0 100,0 100.0 92.3 75.7 55.2
Scenario Ill:Females:
<5 . . . . . . . . . . . . . . . . . . . . . . . 68,746 134,973 148,216 287,217 464,419 715,609 1,076,40815 to 49, . . . . . . . . . . . . . . . . . . 349,494 386,946 516,790 830,222 1,437,144 2,404,500 3,847,954>60 . . . . . . . . . . . . . . . . . . . . . . 54,181 63,330 90,637 162,259 216,461 398,251 677,794
Total females . . . . . . . . . . . . 656,451 768,974 1,126,342 1,872,653 3,068,394 5,025,108 7,991 ,378Males:
<5 . . . . . . . . . . . . . . . . . . . . . . . 70,783 140,485 154,264 298,941 483,374 744,817 1,120,34415 to 49 . . . . . . . . . . . . . . . . . . . 339,778 376,181 506,764 830,887 1,439,816 2,405,154 3,847,892>60 . . . . . . . . . . . . . . . . . . . . . . 44,605 48,333 58,588 98,318 127,192 249,579 427,029
Total males. . . . . . . . . . . . . . 638,999 745,860 1,087,175 1,818,491 2,993,081 4,904,347 7,775,828Both sexes:
<5 . . . . . . . . . . . . . . . . . . . . . . . 139,529 275,458 302,479 586,157 947,793 1,460,425 2,196,75315 to 49. . . . . . . . . . . . . . . . . . . 689,272 763,126 1,023,552 1,661,114 2,876,962 4,809,655 7,695,846>60 . . . . . . . . . . . . . . . . . . . . . . 98,786 111,659 148,227 260,577 343,653 647,827 1,104,823
Total both sexes . . . . . . . . . 1,295,450 1,514,834 2,213,517 3,691,144 6,061,475 9,929,455 15,767,206
Percent one-half or more . . . . . . 86.9 83.8 77.8 57.4 36.1 18.8 8.2Percent one-fourth or more . . . . 96.4 95.3 93.4 87.4 76.0 58.8 41.1

. — — . —
Ch. 3—Overview of the Current Indian Population ●
Table 3-9.—Age-Focused Population Projection SummaryAll Indians and Indian Descendants, Selected Years, 1980-2080—Continued
79
Projection year
1980 1985 2000 2020 2040 2060 2080
Scenario IV:Females:
<5 . . . . . . . . . 68,746 123,506 135,621 242,350 370,028 550,613 822,20515 to 49. , . . . . . . . . . . . . . . . . 349,494 386,947 505,678 766,331 1,242,909 1,961,008 3,001,000>60 . . . . . . . . . . . . . . . . . . . . 54,181 63,329 90,637 162,259 216,463 368,184 586,391
Total females . . . ... , . . . . . 656,451 757,506 1,077,594 1,696,233 2,628,134 4,083,941 6,260,685Males:
<5 , . . . . . . . . . . . . . . . . . 70,783 128,546 141,555 252,242 385,130 573,088 855,76515 to 49. , . . . . . . . . . . . . . . . . . 339,778 376,180 495,269 765,970 1,243,648 1,959,546 2,998,853>60 . . . . . . . . . . . . . . . . . . 44,605 48,332 58,589 98,318 127,191 229,788 367,260
Total males. . . . . . . . . . . . . 638,999 733,923 1,036,574 1,636,630 2,544,988 3,960,277 6,060,519Both sexes:
<5 . . . . . . . . . . . . . . . . . 139,529 252,054 276,777 494,593 755,158 1,123,701 1,677,92015 to 49 . . . . . . . . . . . . . . . . . . 689,272 763,126 1,000,947 1,532,303 2,486,556 3,920,556 5,999,857>60 . . . . . . . . . . . . 98,786 111,661 149,227 260,577 343,653 597,974 953,651
Total both sexes . . . . . . . . . 1,295,450 1,491,429 2,114,168 3,332,863 5,173,122 8,044,218 12,321,204
Percent one-half or more . . . . . . 86.9 84.6Percent one-fourth or more . . . . 96.4 95.7SOURCE Off Ice of Technology Assessment
next several generations, the one-fourth and lessthan one-fourth blood groups increase in num-bers, becoming the majority of the Indian popu-lation in the generation between 2040 and 2060.In 2060, 4.1 percent of Indians are projected tobe full-blooded; the blood quantum of 33 percentwould be one-half or more. Then by 2080, lessthan 1 percent of the projected Indian populationof 17.9 million would be comprised of survivingfull-blooded Indians compared with a majorityof descendants whose Indian blood quantum issignificantly diminished. In this scenario, the In-dian blood quantum of only 16 percent of the to-tal Indian population in 2080 would be one-halfor more. Fifty-five percent would be at least one-fourth, and 45 percent of the total would be lessthan one-fourth (see figure 3-20).
Scenario Ill
The third scenario assumes a distribution of In-dians in the 1980 base year into blood groups re-flecting the findings of the 1950 BIA data with anapproximated value for Oklahoma. The total In-dian population of all age groups are distributedsuch that 60.2 percent are assumed to be full-blooded, 26.7 percent are one-half, 9.5 percentare one-fourth, and 3.6 percent are less than one-fourth. For each blood group the outmarriage
80.1 64.7 46,6 29.1 15.694.2 90.5 83.2 71,5 57,6
rates to non-Indians is the same as in Scenario II;we have assumed that the marriage rates, or rather“union” rates which produce children, betweenIndians in different blood groups are determinedby the proportions of Indians of marriageable agein each group.
For about two generations, population growthacross the four blood quantum groups remainssomewhat constant except that in the category offull-blooded Indians, the contribution of inmar-riage and reproduction rates is not high enoughto keep up with the number being born in lowerblood quantum categories. The number of full-blooded Indians declines from 60.2 percent in thebase year to 34 percent in 2000, 16 percent in 2020,6 percent in 2040, to just under 1.5 percent in2060, and decreases to three-tenths of 1 percentin 2080. The proportion of persons who are atleast one-half Indian grows from 1980 for aboutthree generations and then begins dropping off bythe fourth generation. Growth in the lower bloodquantum groups increases at a fairly steady ratefrom the base year and grows quite rapidly threegenerations into the future. Having started out in1980 with 13.1 percent of the Indian populationbeing one-fourth or less Indian, by 2040, the In-dian blood quantum of the majority of the Indianpopulation, 53 percent, would be one-fourth orless, a transition taking approximately 60 years

80 ● Indian Health Care
Figure 3-20.—OTA Population Projection Distributionof Indian Population by Blood Quantum Scenario II:
Outmarriage = 53%, Both Sexes
100
90
80
70
60
Falo 50;a
40
30
20
10
0
Full blood
—
—
—
I
I —
I
—1980 1985 2000 2020 2040 2060 2080
Year
u Half, but not full
❑ One-fourth, butnot one-half ❑ Less than one-fourth
SOURCE Office of Technology Assessment
from the base year. At that point, surviving in-dividuals born into either the full- or one-halfblood quantum group between 1980 and 1985would be between 60 and 65 years old, well be-yond the end of their childbearing years (see fig-ure 3-21).
In terms of the total Indian population, includ-ing persons in all nine blood quantum groups, abase population of 1.3 million individuals in 1980is projected to grow by 71 percent in 20 years andto double by the year 2005 under the assumptionsof Scenario III. The much larger population of2020, some 3.7 million persons, is projected tohave grown 67 percent in the 20 years since 2000.Another generation later, the number of Indiansis projected to increase 64.2 percent to just over6 million. Under the assumptions of Scenario 111,
Figure 3-21 .—OTA Population Projection Distributionof Indian Population by Blood Quantum Scenario Ill:Outmarriage-53%, Base Population Mix, Both Sexes
100
90
80
70
60
gv 50;n
40
30
20
10
0
n
Full blood
I
—
I
I — —1980 1985 2000 2020 2040 2060 2080
Year
Half, but not full
One-fourth, butnot one-half
Less than one-fourth
SOURCE Office of Technology Assessment
the Indian population is projected to be 4.7 timeshigher in 2040 than in the base year. By 2060, theIndian population is projected to grow to 9.9 mil-lion and reaches 15.8 million by 2080, more thana twelvefold increase from the base year.
Scenario IV
This scenario attempts to account for births thatoccur to Indians out of wedlock that might nothave been reflected in the census data on mar-riage. For example, reports from the States of NewMexico and South Dakota show births to unmar-ried Indian women to be 47 and 62 percent, re-spectively, of all Indian births in those States(115,116). The proportion of these births that arefrom Indian versus non-Indian fathers is not

Ch. 3—Overview of the Current Indian Population ● 8 1
known. In South Dakota, birth data are based onthe race of the mother, and no attempt is madeto determine the race of the child based on thefather’s race. Likewise, in New Mexico birth cer-tificates of infants born to single mothers by lawcontain no information about the father withoutacknowledgment of paternity. Therefore, datafrom which an estimate could be drawn of thenumbers of children born out of wedlock to In-dian and non-Indian fathers are not available.
The only assumption changed in Scenario IVfrom the assumptions of Scenario 111 is the out-marriage rate, which is lowered to 40 percent.Again, the base population in 1980 is distributedby Indian blood quantum with 60.2 percent of allmales and females assumed to be full-blooded,26.7 percent are one-half, 9.5 percent are one-fourth, and 3.6 percent are less than one-fourth.By 1985, given a 40 percent rate of unions betweenIndians of all blood quantum groups and non-Indians, the difference in the distribution of thepopulation as compared with Scenario III is mi-nor, and the total Indian population is projectedto be only 1.5 percent lower. For approximatelythree generations, the percentage of individualsin the full and one-half blood quantum groups areslightly higher in Scenario IV compared with Sce-nario III. By the end of the next two 20-yearperiods, 2060 and 2080, the percentages of indi-viduals in the full- and one-half blood quantumgroups are about twice as high as in Scenario 111.This indicates that over time, a lower outmarri-age rate has a considerable positive effect on thenumber of Indians with higher degrees of Indianblood. At the 2060 turning point, under ScenarioIV there are close to 2.3 million persons in the twolowest blood quantum groups, whereas ScenarioIII includes roughly 4.1 million persons in thesame two groups. The total Indian population in2060 is projected to be 8 million under ScenarioIV and 9.9 million under Scenario III. Under Sce-nario IV, by 2080 the total number of Indians isprojected to have grown to 12,3 million, with 58percent being of one-fourth or more Indian bloodquantum (see figure 3-22), Scenarios III and IVdemonstrate sensitivity to the size of the outmar-riage rate. There would be more individuals inhigher Indian blood quantum groups given lowerrates of outmarriage.
Figure 3-22.—OTA Population Projection Distributionof Indian Population by Blood Quantum Scenario IV:Outmarriage-40%, Base Population Mix, Both Sexes
100
90
80
70
60
&o 50&a
40
30
20
10
0
Full blood
——
—
— — I —
—
—
m —
—
—
—
-1980 1985 2000 2020 2040 2060 2080
Year
Half, but not full
❑ One-fourth, butnot one-half Less than one-fourth
SOURCE Office of Technology Assessment
As shown in table 3-9, the numerical differencesbetween Scenarios 111 and IV are relatively mi-nor for the first two generations following the baseyear. The projected population under Scenario IIIis 15 percent higher in 2040, 19 percent higher in2060, and 22 percent higher in 2080. Under theassumptions of Scenario IV, the Indian popula-tion is projected to grow by a factor of 9.5 fromthe base year to 12.3 million in 100 years.
Summary and Conclusions
A summary of the four population projectionsappears in table 3-9, which is organized by se-lected age groups (less than 5 years; 15 to 49; 60years and over), sex, and total population for each

of the projection years, and includes the percent-ages of the total Indian population that are one-half or more and one-fourth or more Indianblood. What is most evident in table 3-9 and thepreceding presentation of Scenarios I through IVis that even between 1980 and 2000, the projectedpopulation growth is quite large, ranging from 40to 71 percent. The projections of Indian popula-tion that are farthest into the future are so largenumerically that they should be interpreted withcaution.
An important point that should be kept in mindwhen referring to these population projections isthat several of the scenarios use assumed distri-butions of blood quantum in the base year. Theuse of blood quantum by Indian tribes as one ofthe bases for determining tribal membership anduse of blood quantum to determine eligibility forFederal services are ridden with controversy.Many tribal members are emphatically against theFederal Government’s use of a blood quantumstandard; and the opposing Government view isthat if tribes use blood quantum, then it shouldbe acceptable for the Federal Government to useit in determining eligibility. Indians are the onlygroup of people in this country who use bloodquantum to define their members.
The potential effects of imposing a blood quan-tum eligibility rule on current users of IHS serv-
ices are serious. There will be many individualsituations in which a nationally applied definitionof “Indian” for eligibility purposes will mean abso-lute termination of health care benefits. A com-plicated situation, illustrated by OTA’s popula-tion projections, is that there is a growing numberof Indian descendants of mixed Indian parentagewho may not have enough Indian blood of anyparticular tribe to qualify for membership. IHS’sproposed rule to extend eligibility to nontribalmembers who are at least one-half Indian is a par-tial solution.
One can easily think of individual situationswhere descendants would be unable to meet astricter eligibility standard while still maintain-ing strong tribal affiliations. Moreover, eligibil-ity for services to individuals would have to becut off summarily at some point. Hypothetically,under the proposed rule, a baby born in an IHSfacility and requiring expensive intensive care,who was three-eighths Indian and not eligible formembership in his or her tribe, could be liable forthe cost of his or her care. Situations such as thesecould occur on a potentially large scale. Provi-sions would have to be made to ensure that indi-viduals caught in transition from relatively broadto comparatively strict eligibility rules would notbe denied treatment if an eligibility standard basedon blood quantum were to be implemented.

Chapter 4
Health Status ofAmerican Indians
Contents
Page
Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85Sources and Limitations of Data . . . . . . . . . . . . . . . . . . . . . . . 85
Overview of Health Status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89Age Distribution of Deaths . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90Rates and Causes of Death . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90Illness and Use of Services . ...........................104Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .108
Area-Specific Findings. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .111Aberdeen Area . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ....111Alaska Area.... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. ...116Albuquerque Area . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...121Bemidji Area . . . . . . . . . . ..............................123Billings Area . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. ....126California Program . . . . . . . . . . . . . . . . . . ................130Nashville Program . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .131Navajo Area . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ... ...133Oklahoma City Area . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .136Phoenix Area... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...139Portland Area... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ..142Tucson Area . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .......147
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ......151
List of TablesTable No. Page
4-1.
4-2.
4-3.
4-4.
4-5.
Estimated Total U.S. Indian Population and IHSService and Nonservice Population, by State 1980 . . . . 86Estimated Indian and Alaska Service Population byArea, 1980-90 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87Estimated Indian and Alaska Service Population byArea, 1970-80, Including Revised 1971-79 Estimates . . . 88Age-Specific and Age-Adjusted Mortality Rates ofIndians in IHS Areas, 1980-82, U.S. All Races, Whiteand All Other Races, 1981 . . . . . . . . . . . . . . . . . . . . . . . . . 91Age-Adjusted Death Rates for U.S. All Races 1981,Indians in Reservation States, and Indians in IHSService Areas 1980-82, in Order by Rate.. . . . . . . . . . . . 92
TabIe No. Page4-6. American Indian Deaths and Age-Adjusted Death
Rates All IHS Areas for 15 Leading Causes 1980-82Compared to Age-Adjusted Death Rates for U.S. AllRaces 1981 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
4-7. 15 Leading Causes of Death and Age-Adjusted DeathRates Ranked for U.S. All Races 1981 and IHS Areas1980-82 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94
4-8. Leading Causes of Indian Deaths 1951-53 and U.S. AllRaces 1952 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
4-9. Crude Death Rates for 3 Year Periods Centered in1973, 1976, and 1981 for Indians IHS Areas, 15Leading Causes of Death . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
4-10. Mortality Rates From Diseases of the Heart by Age:Indians inn IHS Areas 1980-82 and U.S. AllRaces 1981 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
4-11. Mortality Due to Accidents by Age Indians in IHSAreas 1980-82 and U.S. All Races 1981 . . . . . . . . . . . . . . 97
4-12. Mortality Rates for Pneumonia by Age U.S. All Racesand Indians in lHS Areas 1980-82 and U.S. AllRaces 1981 . . . . . . . . ............................,..100
4-13. Suicides and Suicide Rates by Age Indians in IHSAreas 1980-82 and U.S. All Rates 1981 , .............102
4-14. Hospital Discharge Rates for Leading Causes: IndianHealth Service Direct and Contract General Hospitalsand U.S. Short-Stay Non-Federal Hospitals ... ... ....1os
4-15. Age Distribution of Inpatient Discharges IHS ServiceAreas 1984 and U.S. All Races 1984 Compared to AgeDistribution in the Population and Age-SpecificMortality Rates.. .. ..................,............106
“4-16. Estimated Hospital Discharge Rates, U.S. Non-FederalShort-Stay Hospitals, Calendar Year 1984 and IHSHospitals Federally 1984 in Order by U.S. HospitalDischarge Rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .107
4-17. Number of Outpatient Clinical Impressions, Males andFemales: Indian Health Service Facilities, FY 1984.....108
4-18. Number of Outpatient Clinical Impressions by LeadingDiagnostic Categories Indian Health Service Facilities:11 IHS Areas, FY 1984 . ...........................108

Table No. Page
4-19. Age Distribution of Outpatient Care IHS ServiceAreas 1984 and U.S. All Races 1981 Compared to AgeDistribution in the Population and Age-SpecificMortality Rates. . . . . . . . . . . . . . . . . . . . . . . . . . . ........109
4-20. Percent Distribution of Outpatient Visits by PatientAge Group and Area: Indian Health Service Facilities,FY 1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...109
4-21. Dental Services Required in 12 IHS Areas. . ..........1104-22. Changes in Crude Death Rates, 1972432: IHS
Aberdeen Area . . . . . . . . . . . . . . . . . . . . . . .............1114-23.15 Leading Causes of Deaths and Age-Adjusted Death
Rates for Aberdeen IHS Area Indians 1980-82 andU.S. All Races 1981 . . . . . . . . . . . . . . . . . ..............112
4-24. Heart Disease Mortality by Age IHS Aberdeen AreaIndians 1980-82 and U.S. All Races 1981 . ...........113
4-25. Suicide Mortality by Age IHS Aberdeen Area Indians1980-82 and U.S. All Races 1981 . ......,...........113
4-26.15 Most Frequent Outpatient Diagnoses: AberdeenArea, FY 1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 114
4-27. Infant Deaths and Death Rates IHS Aberdeen Area,1980-82 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ........116
4-28.15 Leading Causes of Deaths and Age-Adjusted DeathRates for Alaska IHS Area Indians 1980-82 and U.S.All Races 1981 . . . . . . . . . . . . . . . . . . . . . .............,117
4-29. Changes in Crude Death Rates, 1972-82: IHS AlaskaArea . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. ..118
4-30.15 Most Frequent Outpatient Diagnoses: Alaska Area,FY 1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .119
4-31. Infant Deaths and Death Rates IHS Alaska Area,1980-82 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ........120
4-32.15 Leading Causes of Deaths and Age-Adjusted DeathRates for Albuquerque IHS Area Indians 1980-82 andU.S. All Races 1981 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .122
4-33. Changes in Crude Death Rates, 1972-82: IHSAlbuquerque Area . . . . . . . . . . . . . . . . . . . . . ..........123
4-34. Changes in Crude Death Rates, 1972-82: IHS BemidjiArea . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. ..124
4-35.15 Leading Causes of Deaths and Age-Adjusted DeathRates for Bemidji IHS Area Indians 1980-82 and U.S.All Races 1981 . . . . . . . . . . . . . . . . . . . . .. .............125
4-36.15 Most Frequent Outpatient Diagnoses: Bemidji Area,FY 1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .126
4-37. 15 Leading Causes of Deaths and Age-Adjusted DeathRates for Billings IHS Area Indians 1980-82 and U.S.All Races 1981 . ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .127
4-38. Changes in Crude Death Rates, 1972-82: IHS BillingsArea . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .........128
4-39. 15 Most Frequent Outpatient Diagnoses: Billings Area,FY 1984 . . . . . . . . . . . . . . . . . . . .., ...................129
4-40. 15 Leading Causes of Deaths and Age-Adjusted DeathRates for Nashville IHS Area Indians 1980-82 and U.S.All Races 1981 . . . . . . . . . . . . . . . . . . . .........,......132
4-41. Estimated Deaths and Age-Adjusted Death Rates forIndians in the Nashville Program, by Service Unit1980-82 . . . . .,....! . . . . . . . . . . . . . . . . ..?,.... . . . . . . . 133
4-42. 15 Most Frequent Outpatient Diagnoses: NashvilleArea, FY 1984.... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .134
4-43. Changes in Crude Death Rates, 1972-82: IHSNavajo Area . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ...135
4-44. 15 Leading Causes of Deaths and Age-Adjusted DeathRates for Navajo IHS Area Indians 1980-82 and U.S.All Races 1981 . . . . . . . . . . . . . . . . . . .. ...............136
4-45. 15 Most Frequent Outpatient Diagnoses: Navajo Area,FY 1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 3 7
4-46. 15 Leading Causes of Deaths and Age-Adjusted DeathRates for Oklahoma IHS Area Indians 1980-82 andU.S. All Races 1981 . ..............................138
4-47, Changes in Crude Death Rates, 1972-82: IHSOklahoma Area . . . . . . . . . . . . . . . . . . . . . .............139
Table No. Page
4-48. 15 Most Frequent Outpatient Diagnoses: OklahomaArea, FY 1984 . . . . . . . . . . . . . .. .....................140
4-49. Changes in Crude Death Rates, 1972-82: IHSPhoenix Area. . . , . . . . . . . . . . . . . . . . . . . . . . , . . . , . . . . . .141
4-50. 15 Leading Causes of Deaths and Age-Adjusted DeathRates for Phoenix IHS Area Indians 1980-82 and U.S.All Races 1981 . . . . . . . . . . . . . . . . . . . ................142
4-51. 15 Most Frequent Outpatient Diagnoses: PhoenixArea, FY 1984. . . . . . . . ............................143
4-52. Changes in Crude Death Rates, 1972-82: IHSPortland Area.. . . . . . . . . . . . . . . . . . . ................144
4-53. 15 Leading Causes of Deaths and Age-Adjusted DeathRates for Portland IHS Area Indians 1980-82 and U.S.All Races 1981 . . . . . . . . . . . . . . . . . . . ......,.........145
4-54. 15 Most Frequent Outpatient Diagnoses: PortlandArea, FY 1984 . . . . ..........................,.....146
4-55. Infant Deaths and Death Rates IHS Portland Area,1980-82 . . . . . . . . . . . . . . . . . . . . . . . . . . . . , .............147
4-56. Changes in Crude Death Rates, 1972-82: IHSTucson Area . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. ...148
4-57. 15 Leading Causes of Deaths and Age-Adjusted DeathRates for Tucson IHS Area Indians 1980-82 and U.S.All Races 1981 . . . . . . . . . . . . . . . . . . . ............,...149
4-58. 15 Most Frequent Outpatient Diagnoses: Tucson Area,FY 1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ....150
4-59. infant Deaths and Death Rates IHS Tucson Area,1980-82 . . . . . . . . . . . . . . . . . . . . . . . . . . . . .............,151
List of FiguresFigure No. Page
4-1. Percent Distribution Deaths by Age Indians 1980-82and U.S. All Races 1981 . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
4-2. Population by Age, Indians in Reservation States andU.S. All Races 1980 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91
4-3. Age-Specific Mortality Rates Ratio of Indians in IHSService Areas 1980-82 to U.S. All Races 1981 . . . . . . . . 91
4-4. Age-Adjusted Death Rates for Diseases of the HeartAmerican Indians in 11 IHS Areas 1980-82,. . . . . . . . . . 96
4-5. Age-Adjusted Death Rates for Accidents andAdverse Conditions, American Indians in 11 IHSAreas 1980-82 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
4-6. Age-Adjusted Death Rates for Malignant Neoplasms,American Indians in 11 IHS Areas 1980-82. . . . . . . . . . . 97
4-7. Age-Adjusted Death Rates for Liver Disease andCirrhosis, American Indians inn IHS Areas 1980-82 . 98
4-8. Age-Adjusted Death Rates for CerebrovascularDisease, American Indians inn IHS Areas 1980-82. . . 98
4-9. Age-Adjusted Death Rates for Pneumonia, AmericanIndians in 11 IHS Areas 1980-82 . . . . . . . . . . . . . . . . . . . . 99
4-10. Age-Adjusted Death Rates for Diabetes Mellitus,American Indians in 11 IHS Areas 1980-82. . ..,......100
4-11. Age-Adjusted Death Rates for Homicide, AmericanIndians in 11 IHS Areas 1980-82 . . . . . . ., ....,.......101
4-12. Age-Adjusted Death Rates for Homicide, AmericanIndians Male and Female, in 11 IHS Areas 1980-82 ...101
4-13. Age-Adjusted Death Rates for Renal Failure AmericanIndians Both Sexes, in 11 IHS Areas 1980-82 . ........103
4-14. Age-Adjusted Death Rates for Chronic PulmonaryDiseases American Indians Both Sexes, in 11 IHSAreas 1980-82 . . . . . . . . . . . . .. ...............,,.....103
4-15. Infant Mortality Rates: American Indians in IHS Areas1980-82 and U.S, All Races, 1981...,...............104
4-16. Hospitalizations for Mental Disorders IHS Direct andContract Hospitals and U.S. Non-Federal Short-StayHospitals 1973-1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .110

—
Chapter 4
Health Status of American Indians
INTRODUCTION
Information on the health status of AmericanIndians is presented in this chapter. The focus ison health problems of Indians in areas served bythe Indian Health Service (IHS), and not on In-dians in urban or other nonservice areas. Thehealth status of all Indians in IHS areas is pre-sented, followed by analyses of health conditionsin each of the 12 IHS service areas. Mortality ratesare the primary source of health status informa-tion, but patient care data from IHS and othersources are also used to provide information onmorbidity (illness) and access to health services.
Sources and Limitations of Data
Sources
Except where otherwise indicated, the data usedin this chapter were obtained from IHS, the Na-tional Center for Health Statistics (NCHS), andthe U.S. Bureau of the Census.
Population Data. —As discussed in chapter 3,the Indian Health Service obtains Indian popula-tion statistics from the U.S. Census, which is con-ducted every 10 years. Using these data, IHSprojects its estimated Indian population for thecoming decade. Then, every year between cen-suses, IHS reestimates the Indian population byusing Indian birth and death data obtained an-nually from the National Center for Health Sta-tistics. IHS provided OTA with population esti-mates using NCHS birth and death data throughcalendar year 1982; these population estimateswere used to calculate mortality (death) and healthcare utilization rates.
Mortality (Death) and Morbidity (Illness andInjury) Data.—A computer tape with informa-tion about Indian deaths during the period 1980-82 was provided by IHS to OTA; OTA’s analy-sis of this information is explained in appendix D.
Information concerning morbidity (illness andinjury) was derived from two IHS data sources:1) the Inpatient Care System (IPC), which con-
tains IHS direct care and contract care generalhospital discharge data; and 2) the AmbulatoryPatient Care System (APC), which contains in-formation on the number of outpatient visits atIHS facilities by various patient characteristics(age, sex, diagnosis, community of residence,etc. ). IHS provided OTA with computer tapespertaining to its IPC and APC systems; its inter-nal documents and outpatient care on hospital uti-lization by area (166,176); and printouts of the15 leading diagnoses for outpatient visits by res-ervation State, county, IHS area, and IHS serv-ice unit.
Limitations
These data sets and resulting analyses have sev-eral limitations that affect the validity of the in-formation on Indian health status presented in thischapter.
Population Estimates.—While the data col-lected by the U.S. Bureau of the Census andNCHS have limitations generally (e.g., see ch, 3for limitations of the census data), data concern-ing Indians are believed to be particularly prob-lematic, especially in areas of the country whereIndians have integrated into other populations.In addition, there are limitations to IHS’s calcu-lation of its service population. The service pop-ulation is determined by counting those AmericanIndians, Eskimos, and Aleuts (as identified in thecensus) who reside in the geographic areas, de-fined by county, in which IHS has responsibili-ties (“on or near” reservations and in contracthealth service delivery areas [CHSDAs]). Figure1-7 in chapter 1 shows the location of IHS facil-ities; in general, the eligible population is esti-mated from census counts of Indians residing incounties surrounding these facilities. IHS estimatesthat about 60 percent of the Indian population waseligible for services in 1984 (see tables 4-1 and 4-2), but the people IHS counts as eligible may ormay not use IHS services or even be eligible forsuch services. Thus, IHS does not have a firm idea
85

86 ● Indian Health Care
Table 4-1 .–Estimated Total U.S. Indian Population and IHS Service and Nonservice Population, by State 1980
Estimated Reservation States
total Indian Total IHSpopulation Indian service Nonservice
State 1980 Census data population population populationAlabama . . . . . . . . . . . . . . . .Alaska . . . . . . . . . . . . . . . . . .Arizona . . . . . . . . . . . . . . . . .Arkansas . . . . . . . . . . . . . . . .California . . . . . . . . . . . . . . .Colorado , . . . . . . . . . . . . . . .Connecticut . . . . . . . . . . . . .Delaware . . . . . . . . . . . . . . . .District of Columbia . . . . . .Florida. . . . . . . . . . . . . . . . . .Georgia . . . . . . . . . . . . . . . . .Hawaii . . . . . . . . . . . . . . . . . .Idaho ... , . . . . . . . . . . . . . . .Illinois . . . . . . . . . . . . . . . . . .Indiana ., . . . . . . . . . . . . . . .lowa. ., . . . . . . . . . . . . . . . . .Kansas . . . . . . . . . . . . . . . . .Kentucky . . . . . . . . . . . . . . . .Louisiana . . . . . . . . . . . . . . .Maine . . . . . . . . . . . . . . . . . .Maryland . . . . . . . . . . . . . . . .Massachusetts. . . . . . . . . . .Michigan . . . . . . . . . . . . . . . .Minnesota. . . . . . . . . . . . . . .Mississippi . . . . . . . . . . . . . .Missouri . . . . . . . . . . . . . . . .Montana . . . . . . . . . . . . . . . .Nebraska . . . . . . . . . . . . . . . .Nevada . . . . . . . . . . . . . . . . .New Hampshire . . . . . . . . . .New Jersey . . . . . . . . . . . . . .New Mexico . . . . . . . . . . . . .New York . . . . . . . . . . . . . . .North Carolina . . . . . . . . . . .North Dakota . . . . . . . . . . . .Ohio . . . . . . . . . . . . . . . . . . . .Oklahoma . . . . . . . . . . . . . . .Oregon . . . . . . . . . . . . . . . . .Pennsylvania . . . . . . . . . . . .Rhode Island . . . . . . . . . . . .South Carolina . . . . . . . . . . .South Dakota . . . . . . . . . . . .Tennessee . . . . . . . . . . . . . .Texas . . . . . . . . . . . . . . . . . . .Utah . . . . . . . . . . . . . . . . . . . .Vermont . . . . . . . . . . . . . . . .Virginia . . . . . . . . . . . . . . . . .Washington . . . . . . . . . . . . .West Virginia . . . . . . . . . . . .Wisconsin . . . . . . . . . . . . . . .Wyoming . . . . . . . . . . . . . . . .
All States . . . . . . . . . . . . .
7,72471,329
169,8699,937
216,07020,2064,7281,3771,034
20,0957,9224,000
11,45317,6578,3156,083
16,6883,790
13,0954,5158,5568,428
42,45339,4026,729
12,94841,69510,34014,674
1,4329,165
116,15040,87669,57522,97613,513
186,26829,60910,0403,1706,089
50,1395,372
41,97021,468
1,0159,760
66,4231,642
32,1488,256
1,548,168
7,72471,329
169,869
216,07020,206
4,728
20,095
11,453
6,08316,688
13,0954,515
42,45339,4026,729
41,69510,34014,674
116,15040,87669,57522,976
186,26829,60910,0403,170
50,139
41,97021,468
66,423
32,1488,256
1,416,216
2,69671,329
169,869
73,2622,989
830
5,956
7,598
2,0523,261
1,1643,004
8,94419,0744,563
34,6394,347
14,674
113,56910,2666,045
18,554
186,26828,039
721,226
45,854
76310,229
61,217
18,9825,467
936,802
5,028
142,80817,2173,898
14,139
3,855
4,03113,427
11,9311,511
33,50920,328
2,166
7,0565,993
2,58130,61063,530
4,422
1,5709,9681,944
4,285
41,20711,239
5,206
13,1662,789
479,414
NonreservationState
9,937
1,3771,034
7,9224,000
17,6578,315
3,790
8,5568,428
12,948
1,4329,165
13,513
6,089
5,372
1,0159,760
1,642
131,952SOURCE: US. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, lndian Health Service, Program Statls-
t!cs Branch, Population Statistics Staff, tnternal document, Rockville, MD, Feb 20, 1985

Ch. 4—Health Status of American Indians Ž 87
Table 4-2.— Estimated Indian and Alaska Service Population by Area, 1980-90a
Area 1980 1981 1982 1983 1984 1985 1986 1987 1988 1989 1990
Aberdeen . ., . . . . . .Alaska. ., . . . . . . . .Albuquerque ., ., .,Bemidji . . . . . . . . . .Billings . . . . . . . . . . . . . . . . . . . .California . . . . ., . .Nashville . . . . . . . . . . .Navajo, . . . ,., ....,., . . . . .Oklahoma City, . . . . . . . .Phoenix . . . . . . . . . , , , . . . .Portland ..., . . . . . . .Tucson . . ., . .
All areas, . . . . . . . . . . ,...,
63,25364,04746,61042,68635,70865,75726,731
145,162172,63674,02075,76916,230
828,609
64,99065,74347,69543,66436,73567,04827,181
149,208176,52776,30977,38516,590
849,075
66,80567,52148,82544,71137,81368,46028,136
153,360180,66478,20679,08616,980
870,567
68,68869,38349,99745,82138,93569,98930,644
157,627185,81180,20387,88117,400
902,399
70,64871,32951,21147,00040,10671,64235,822
162,005190,45182,30996,42717,852
936,802
72,67973,35152,47148,24541,32673,41436,413
166,493195,34684,51698,99618,332
961,582
74,78175,46153,77149,55042,59475,30637,025
171,097200,488
86,826101,275
18,843987,017
76,96177,64755,11750,92943,90677,30937,663
175,809205,87189,244
103,63719,386
1,013,479
79,22079,91756,50652,36345,27279,43938,332
180,635211,510
91,755106,082
19,9581,040,989
81,54182,26757,93653,88146,68281,68739,021
185,571217,402
94,378108,610
20,5611,069,537
83,94484,70259,41255,45348,14284,04839,736
190,621223,536
97,104111,21121,194
1,099,103aEstlmates were based on dataon US Census counfsfor 1980 and lndianbirths and deaths through calendar year 1982 Prior and subsequent estimates for 1980-1990
are based on Indian birth and death data as available to IHS from NCHS.
SOURCEUS Department of Health and Human Sewices, Public Health Setvice, Health Resources and Services Adm!nistratlon, lndian Health Servtce, Program Statls-tlcs Branch, Population Statistics Staff, internal document, Rockville, MD, Feb 1, 1985.
of how many Indians are in its potential servicepopulation.
These limitations affect conclusions abouthealth status, because the estimate of the servicepopulation is used as the denominator in calcu-lating mortality and morbidity rates, If a popu-lation is undercounted while deaths in that pop-ulation are counted accurately, the health of thepopulation will appear to be worse than it actu-ally is. Conversely, if the population is countedaccurately, but the number of deaths is under-counted, the health of the population will appearto be better than it really is. The latter situationapplies to information on Indians in California,where IHS estimates that the eligible service pop-ulation was approximately 73,000 in 1984. How-ever, NCHS data contained information on only471 Indian deaths in that population in those 3years, resulting in a mortality rate of less than 300per 100,000 population, a rate lower than that ofthe wealthiest communities in the United States.
Other limitations of the population estimatesprovided by IHS occurs because of the way IHScalculates the age and sex characteristics of itsservice populations. These are based on censuscounts for reservation States, not the countieswithin the States covered by IHS service areas(193). These may or may not differ. The effect,however, is that age and sex distributions for en-tire reservation States are used to calculate age-and sex-specific mortality and morbidity rates forservice areas, introducing unknown error.
In addition, IHS does not currently adjust forchanges in the age and sex distribution of its in-
tercensus estimates (191). Rather, age and sex dis-tributions from the most recent census are appliedto population estimates for intercensus years. Ifthe estimated age and sex distribution in a par-ticular area changed significantly in the years af-ter the census, health indicator rates for that areathat were supposedly age-adjusted or sex-specificwould not be accurate. However, OTA’s analy-sis is based on data from 1980 to 1982, so the er-rors introduced by using the 1980 census age andsex distributions are minimal. (At the time thisreport was being published, IHS was consideringrevising its population forecasting techniques toprovide more precise age and sex distributionestimates. )
Depending on the extent of discrepancies be-tween population counts and estimates, IHS mayalso recalculate estimates for previous decades.The IHS service population enumerated in 1980was approximately 13 percent higher than thatestimated by IHS for 1979, which was projectedfrom the 1970 census. The 1980 census was prob-ably more reliable with respect to Indian data thanthe 1970 census (see ch. 3). After the 1980 census,IHS recalculated its population estimates for 1971to 1979 in order to show a more gradual transi-tion to the population enumerated during the 1980census (see table 4-3). OTA took account of therevised population estimates to calculate deathand hospital discharge rates for periods prior to1980.
Mortality Data.—A great deal of the discussionin this chapter relies on mortality information asan index of health status, but the source of such

88 Ž Indian Health Care
Table 4-3.—Estimated Indian and Alaska Service Population by Area, 1970 -80,a
Including Revised 1971-79 Estimates
Area 1970 1971 1972 1973 1974 1975 1976 1977 1978 1979 1980
Aberdeen area . . . . . . . . . . . . 44,290 45,870 47,443 49,020 50,595 52,814 54,385 55,968 57,546 61,607 63,253Alaska, . . . . . . ... ... 50,654 51,916 53,179 54,440 55,700 57,198 58,454 59,710 60,964 62,223 64,047Albuquerque . . . . . . . . . . . 33,109 34,573 36,035 37,496 38,960 40,426 41,886 43,350 44,811 45,360 46,610Bemidji . . . . . . . . . . . . . 21,674 23,050 24,423 25,799 27,165 32,457 34,115 35,780 37,444 39,963 42,686Billings . . . . . . . . . . . . . . . 27,127 27,859 28,589 29,274 30,951 31,734 32,496 33,262 34,024 34,932 35,708California b . . . . . . . . . . . . . . — — 57,803 61,324 65,757Nashville . . . . . . . . . . . . . . . . . . 8,539 8,824 9,559 – – – – –9,866 11,947 12,314 12,672 13,037 22,729 25,910 26,731Navajo. ....,.. . . . . . . . 91,553 96,476 101,396 106,317 111,237 116,161 121,078 126,000 130,919 138,531 145,162Oklahoma City.. . . . . . . . . . 98,976 106,416 113,548 120,691 128,000 135,168 142,290 149,444 156,587 165,448 172,636Phoenix ., ..., ,.., . . . . . . 49,241 51,652 54,057 56,467 58,875 61,296 63,695 66,108 68,649 71,565 74,020Portland . . . . . . . . . . . . . . . . . . . 25,081 26,803 28,528 30,248 31,974 34,908 36,586 38,367 40,140 68,041 75,769Tucson ..., . . . . . . ..., . . . 9,752 10,401 11,047 11,696 12,343 12,992 13,639 14,287 14,935 15,582 16,230
All areas . . . ..., . . . . . . . . 459,996 483,840 507,804 531,314 557,747 587,468 611,296 635,313 726,551 790,486 828,609aEstimates are based on u,s. census counts for 1970 and 1980, and NCHS information on Indian births and deaths, 1970.80bDld not become IHS service area untd 1978
SOURCE US. Departmentof Health and Human Services, Pubhc Health Service, Health Resources and Services Administration, Indian Health Service, Pro~ram Statls.tics Branch, Population Statistics Staff, Internal document, Rockwlle,
data has several limitations, only some of whichare specific to data about Indians. The most im-portant Indian-specific limitation is that in manyareas Indians may be identified as belonging toa non-Indian ethnic group. As mentioned above,this is highly likely in California, where many In-dians have Hispanic surnames; it also maybe truefor nonreservation Indians everywhere (e.g.,Oklahoma, urban areas). Another limitation isthat the mortality tapes that NCHS provides toIHS contain information only about the under-lying (chief) cause of death, and not on other con-tributing causes of death. This is a problem in in-vestigating the contribution of illnesses such asalcoholism and drug abuse to mortality rates.
Perhaps the most serious limitation of usingmortality data is that such information may notidentify the actual causes of death. For example,using the autopsy as a measure of accuracy of thedeath certificate in a Connecticut sample, Kircherand his colleagues found major disagreement onthe major ICD-9 (International Classification ofDiseases, 9th Edition) classifications (e.g., diseasesof the heart) for causes of death in 29 percent ofdeaths, and disagreement on the specific cause inanother 26 percent of deaths (63). Circulatory dis-orders, ill-defined conditions, and respiratory dis-eases were the most overdiagnosed; specific trau-matic conditions (suicide, homicide, or accident)and gastrointestinal disorders were the most un-derdiagnosed. Similar findings have been reportedin other studies (199).
MD, Feb. 1, 1985
Patient Care Information.—In both IHS’s andNCHS’s hospital discharge and ambulatory pa-tient care information systems, data are collectedfor each hospital discharge and for each outpatientvisit (encounter), not for each patient. Therefore,a number of hospital discharge records and, morelikely, outpatient visit records, could be for a sin-gle patient. Medical records are, of course, keptfor all patients in each facility they visit, but theserecords are not linked in an electronically acces-sible data system.
Comparisons of the prevalence and incidenceof illnesses between IHS and U.S. all races popu-lations are difficult to make because of differencesbetween IHS’s data system and those of the Na-tional Center for Health Statistics. For outpatientinformation, NCHS collects data from office-based physicians (200). The IHS health care sys-tem relies heavily on nonphysicians (see ch. 4),so comparisons between IHS and U.S. all racesoutpatient care are not exact. Further, IHS usesa different outpatient diagnostic coding systemand aggregates data from this system in a non-standard way (168). Also current IHS reportingsystems exclude diagnostic data from several im-portant sources of health services delivery. Theseinclude contract outpatient providers, most trib-ally managed facilities, and urban providers. Sys-tematic data on the prevalence of mental healthproblems and the utilization of mental health serv-ices are lacking for both Indians and U.S. all racespopulations.

Some difficulties also arise from IHS’s use ofthe concept “clinical impression. ” Clinical impres-sion refers to the diagnosis first suspected by theexamining physician at the initial visit; it may notbe the final diagnosis. This has several implica-tions for morbidity analyses based on APC data.For example, IHS had used APC records to de-rive incidence of diseases considered “notifiable”b y the U.S. Centers for Disease Control (e.g.,measles, syphilis) and other communicable dis-eases recognized as important sources of morbid-ity in Indian communities (e. g., otitis media).These data made it appear as if Indians weresuffering from notifiable and communicable dis-eases at a much greater rate than the U.S. all racespopulation, when in fact such incidence rates in-cluded mistaken, perhaps overcautious, diagno-ses. For example, a validity check of a count ofseveral hundred clinical impressions of measlesturned up only one actual case. For this reason,IHS no longer publishes such information, al-though it can still be obtained from APC records(58).
Comparisons With IHS Publications.— For cer-tain statistical calculations (e. g., mortality ratesreported in the Chart Series Book published in1984 and 1985) the IHS uses census counts of thetotal American Indian and Alaska Native popu-lation residing in all reservation States, and thetotal number of Indian deaths in those States, tocalculate national Indian death rates. In thesecases, the nonservice population (those who donot reside in the geographic areas in which IHShas responsibilities), are included in IHS’s calcu-lations. IHS uses this method in order to be ableto compare current Indian health status with In-
OVERVIEW OF HEALTH STATUS
Overall Indian health status relative to thehealth of “U.S. all races” combined can be pre-sented in several ways: the age distribution ofdeaths, differing causes of death, and differingpatterns of health care utilization. In this sectionthese health indicators are averaged for Indiansin all IHS service areas, and comparisons acrossIHS services areas are made. Then, the health sta-
Ch. 4—Health Status of American Indians ●
——-89
dian health status in 1955 (26), when IHS becameresponsible for providing Indian health care butIHS service areas as they are now known had notbeen organized. However, the number of reser-vation States and the Indian population base haschanged considerably since 1955, so even thesecomparisons should be made extremely cautiously.At the time this report was being prepared, IHSwas conducting a congressionally requested studyof health parity which will include reports onIndian mortality in individual IHS service areas,including age-adjusted mortality rates. OTA’sanalysis has generally focused on IHS’s servicepopulation. Consequently, OTA’s rates may dif-fer from some of IHS’s published rates. Thesedifferences are identified in the following analy-ses. In the 3-year period centered in 1981, therewere an estimated 15,321 deaths among IHS’sservice population, and another 4,408 deaths inthe nonservice population.
Comparisons Over Time. –A report publishedin 1979 included mortality rates for IHS areas forthe 3-year periods centered in 1973 and 1976 (157),but these were not adjusted for age and so werenot comparable to rates for the U.S. all races.They are used in OTA’s analysis to make roughestimates of changes in health status over the dec-ade for which data on IHS areas are available.These estimates should be interpreted cautiouslybecause of changes over time in a number of otherfactors: the IHS population base (as a result of,for example, “termination” and subsequent re-recognition of tribes as federally recognized);changes in census methods; and changes in IHSservice area boundaries.
tus of Indians in each IHS area is analyzed. Theseanalyses indicate that while there has been steadyimprovement, in almost every IHS area and onalmost every health indicator, Indian health re-mains poorer than that of the U.S. population ingeneral. Further, there appear to be significantdifferences in health care utilization, which maybe indicators of unmet need.

90 ● Indian Health Care
Age Distribution of Deaths
Perhaps the most significant indicator of Indianhealth status is that Indians do not live as longas other U.S. populations. In the early 1950s, 56percent of Indian deaths occurred in individualsyounger than age 45 (155). By 1982, that had onlyimproved to 37 percent of Indian deaths occur-ring to those younger than 45, compared withonly 12 percent of U.S. all races deaths occurringin that age group (see figure 4-1 ). Indians’ higherbirth rate (see ch. 3) contributes to a younger pop-ulation (see figure 4-2) and thus more deathsamong younger Indians. However, the moreproblematic health status of younger Indians isreflected by the fact that Indian mortality rate(deaths relative to population) exceed the rates forthe U.S. all races in every age group below age75; the difference is especially pronounced in theyears 1.5 through 44 (see table 4-4 and figure 4-3).
In the 3-year period centered in 1981, 345,430years of potential life were lost by Indians whodied before their 65th birthdays. Per 100,000 pop-ulation, the Indian rate of potential years of lifelost was approximately two times that of the U.S.all races rate.
Rates and Causes of Death
In 1980 to 1982, the average age-adjusted mor-tality rate for all IHS service areas excluding Cali-
fornia was 778.3 per 100,000, a rate 1.4 times thatof U.S. all races. Rates ranged from 1,261.3 inAberdeen to 530.6 in the Oklahoma City area.(Existing data on the health status of Indians inCalifornia is too incomplete to use, so death ratesattributed to this group are not included. ) Thesefigures differ markedly from those published bythe Indian Health Service in 1985, because, as dis-cussed above, IHS typically averages all reportedIndian deaths in all parts of all reservation States,whether the IHS has service delivery responsibil-ities throughout the State or not. For the 1980-82period, IHS’s method resulted in an average age-adjusted overall mortality rate for Indians of568.9, essentially equal to that of the U.S. all races(see table 4-s).
Leading Causes of Death
In the 3-year period centered in 1981, the 15leading causes of death for Indians in IHS areaswere heart disease, accidents, cancer, liver diseaseand cirrhosis, cerebrovascular disease, pneumo-nia, diabetes, suicide, homicide, conditions orig-inating in the perinatal period (the period rightaround birth), nephritis, nephrotic syndrome andnephrosis, congenital anomalies (birth defects),chronic pulmonary diseases, septicemia, and tu-berculosis (see table 4-6). While there are substan-tial differences among IHS areas in mortality andhealth care utilization rates, the pattern of disease
Figure 4-1.— Percent Distribution Deaths by Age Indians 1980-82 and U.S. All Races 1981
Under 5
5 to 24
: 25 to 44
45 to 64
6 5 +
130/oI 80/0
130/o110/0
160/0180/0
2 1 %I 25 ”/o
670/0
1 I 1 1 1 1 1 1 1 1 1 1 I 1 Jo 10 20 30 40 50 60 70
Percent d is t r ibut ion
- I n d i a n s 1 9 8 0 - 8 2 1—1 U.S. all races 1981
SOURCE US Department of Health and Human Serwces, Public Health Service, Health Resource and Services Adminlstratlon, Indian Health Service, Program Statis.tics Btanch, “Chart Series Book, ” Rockville, MD, April 1985

—
Figure 4.2.— Population by Age, Indians in ReservationStatesa and U.S. All Races 1980
~--,/8 “~. . e -
6 - U.S. all races
4
2
0 1 1 I 1 1 I 1 I 1 1 I 1 I 1 L-1<5 10 20 30 40 50 60 70 80-85 +
1 1 1 1 1 [ 1 1Age 14 24 34 44 54 64 74 84
alJ~ed by IHS t. Infer age distribution of Indians In IHS service areas
SOURCE U S Department of Health and Human Services, Publ!c Health Sew-Ice, Health Resources and Sew!ces Admln!stratton Indian Health Sew.Ice, Program Statlstlcs Branch, “Chart Series Book “ Rockvllle, MD,ADrll 1985
and death is essentially consistent across IHS areas(see table 4-7). (For the number of deaths, age-specific and age-adjusted mortality rates, and ra-tios to U.S. all races rates for 72 selected causesof death in all areas excluding California, see app.B.) As shown in tables 4-8 and 4-9, the leadingcauses of death among Indians have changedsomewhat over the past 30 years. Since 1951 therehas been significant improvement in infectious dis-eases only-to have the so-called “social” or be-havioral causes of mortality (accidents, suicide,homicide) become prominent.
Ch. 4—Health Status of American Indians • 91
Figure 4-3.—Age-Specific Mortality RatesRatio of Indians in IHS Service Areas 1980-82 to
U.S. All Races 1981
Under 1
1-4
5-14
15-24
25-34
al 35-44
z45-54
55-64
65-74
75-84
85+
1.5
2.2
1.5
2,7
3.0
2.5
1.7
1.3
11
0.9
0.9
0 1 2 3
RatioSOURCE U S Department of Health and Human SewIce, Ind!an Health SewIce,
Off Ice of Admlnlstratlon and Management, 1985
Diseases of the heart have been the leadingcause of death for U.S. all races for some time.They are now the leading cause of death for In-dians in IHS service areas, although there are still
Table 4-4.—Age-Specific and Age-Adjusted Mortality Rates of Indians in IHS Areas (excluding California), 1980-82,U.S. All Races, White and All Other Races, 1981 (rate per 100,000 population)
IHS service area Indians1980-82
Number of Mortality United States-1981 mortality rates Ratio of ratesAge deaths a rate
<1 . . . . . . . . . . . 1,021 1,834.81 to 4 . . . . . . . . . . 249 129.55 to 14. . . . . . . . . 228 43.1
15 to 24. . . . . . . . . 1,522 285.525 to 34 . . . . . . . . . 1,459 397.135 to 44 .., . . . . . 1,312 555.445 to 54 ........, 1,625 950.555 to 64 . . . . . . . . . 2,082 1,694.865 to 74 . . . . . . . . . 2,422 3,081.575 to 84. . . . . . . . . 2,097 6,097.0>85 . . . . . . . . . . . 1,310 13,325.2
Age-adjusted rate . . . . . . . . . . . . 778.3
All races White All other Indians to U.S. all races
1,207.360.229.4
107.1132.1221.3573.5
1,322.12,922.36,429.9
15,379.7568.2
1,062.054.328.0
104.6116.2192.5524.9
1,255.72,855.96,423.4
15,628.0544.6
1,786,587.335.6
120.0226.2508.2921.0
1,890.83,531.96,478.6
12,547.9732.6
1.52.21.52.73.02.51.71,31.10.90.91.4
.
NOTE Excludes 14 deaths for which age at death was unknown
SOURCES Indian data: U S Department of Health and Human Services, Publ!c Health Service, Health Resources and SewIces Administration, Indian Health Sewice,computer tape supplled to the Office of Technology Assessment, Washington, DC, 1985 U.S. data: U.S Department of Health and Human Sew!ces, PublicHealth Sewice, National Center for Health Statistics, “Advance Report— Final Mortality Statlst!cs, 1981 ,“ ?#onth/y V/ta/ Statistics Report 33(3) supp , June22, 1984

Table 4-5.—Age-Adjusted Death Rates for U.S.All Races 1981, Indians in Reservation States, andIndians in IHS Service Areas (excluding California)1980-82, in Order by Rate (rate per 100,000 population)
Age-adjustedmortality rate
U.S. all races 1981 . . . . . . . . . . . . . . . . . . . . .IHS published rate—lndians in 28
reservation States. . . . . . . . . . . . . . . . . . . .IHS areas—total . . . . . . . . . . . . . . . . . . . . . . .Aberdeen . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Billings. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tucson . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Bemidji . . . . . . . . . . . . . . . . . . . . , . . . . . . . . . .Phoenix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Alaska . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Nashville . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Portland . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Albuquerque . . . . . . . . . . . . . . . . . . . . . . . . . .Navajo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Oklahoma City . . . . . . . . . . . . . . . . . . . . . . . .
568.2
568.9778.3
1,261.31,260.31,011.1
943.5918.2918,1765.4749.8703.1656.3530.6
SOURCESU.S. atlraces:U.S. Department of Health and Human Services, PublicHealth Service, National Center for Health Statistics, “Advance Reportof Final Mortality Statistics, 1981,” Monthly Vita/Statistics Report33(3)supp. June 22, 1984. IHSpubiished data: U.S. DepartmentofHealth and Human Services, Public Health Service, Health Resourcesand Services Administration, Indian Health Service l Indian Hea/thService Chart Series Book Apri/ 1985 (Rockville, MD IHS, 1985)Indians in iHS areas: U.S. Department of Health and Human Services,Public Health Service, Heaith Resources and Services Administration,Indian Health Service, computer tape supplied to the Office ofTechnology Assessment, Washington, DC, 1985.
almost as many deaths from accidents. On aver-age, the Indian death rate from diseases of theheart is slightly lower than the rate for U.S. allraces combined (and for U.S. whites). However,as shown in table 4-10, relative to U.S. all races,mortality from heart disease is greater amongyounger Indians than among younger people ofother U.S. populations, and there is considerablevariation among IHS areas in mortality due toheart disease. The death rate from heart diseaseis considerably lower than the U.S. all races ratein most areas, but the heart disease death rate ex-ceeds that of U.S. all races in four IHS areas:Aberdeen, Bemidji, Billings, and Nashville (seefigure 4-4). The reasons for these differences areunclear; heart disease is a matter of increasing con-cern to providers of Indian health care in all IHSareas (111).
The accident mortality rate for Indians in IHSservice areas is on average 3.4 times the U.S. allraces rate. In seven IHS areas, accidents are stillthe leading cause of death, and there was no IHSarea that did not have a mortality rate from ac-cidents at least 2.2 times the U.S. all races rate
(figure 4-5). In general, accidents and other ex-ternal causes are the leading cause of death amongU.S. youth (92); among Indians, the accidentaldeath toll among the young is far worse thanamong other U.S. populations (table 4-11). Theexcess Indian risk of death from accidents hasmany causes, but those related to motor vehiclespredominate. Long distances between destina-tions, poor roads, overcrowded and unsafe ve-hicles, and driving under the influence of alco-hol are among the major causes of motor vehicledeaths among Indians.
Cancer (malignant neoplasms) is the third lead-ing cause of death among the IHS’s service pop-ulation, having accounted for 1,713, or 11.2 per-cent, of Indian deaths in 1980 to 1982. Althoughon average the cancer mortality rate among In-dians is lower than that of U.S. all races, thereis considerable variability among IHS areas, andthe Indian cancer mortality rate exceeds that ofU.S. all races in five IHS areas: Aberdeen, Alaska,Bemidji, Billings, and Nashville (figure 4-6), Sub-stantial cancer death rates for particular organ sys-tems in specific IHS areas, such as mortality fromcancer of the digestive system in both the Aber-deen and Alaska areas, are masked by aggregat-ing cancer rates. The tendency of American In-dians to have higher than average death rates fromcancer was noted tentatively in the journal of theNational Cancer Institute (NCI), but the smallnumbers of Indians in NCI’s epidemiologic sur-vey kept them from being able to demonstrate sta-tistically significant differences from other pop-ulations (223).
Alcohol abuse is implicated in Indian death andillnesses from many causes; e.g., accidents, sui-cide, homicide, diabetes, congenital anomalies ininfants, pneumonia, heart disease, and cancer. Ithas also been implicated in 50 percent of adultcrime on Indian reservations (204,205,206,207).The prevalence of alcohol abuse can be inferredfrom the extremely high liver disease and cirrho-sis death rates in almost all IHS areas. In 1980 to1982, there were 801 deaths which listed liver dis-ease and cirrhosis as the underlying (chief) cause,for an age-adjusted death rate of 48.1 per 100,000,exceeding the U.S. all races rate by 4.2 times. Inone area the ratio to U.S. all races was almost10:1, and there was no IHS area in which the In-

Ch. 4—Health Status of American Indians ● 9 3
Table 4-6.—American Indian Deaths and Age-Adjusted Death Rates All IHS Areas (excluding California) for15 Leading Causes 1980-82 Compared to Age-Adjusted Death Rates for U.S. All Races 1981
American Indian U.S. all races RatioIHS Number Age-adjusted Age-adjusted American Indiancodea Rank b Cause name of deaths - rate c rate to U.S. all races
Both sexes combined:310 1.790 2.150 3.620 4.430 5.510 6.260 7,830 8.820 9.740 10.640 11.730 12.540 13.090 14.030 15,
ALL . .
Female?310 1.150 2.790 3.620 4.430 5.260 6.510 7.740 8.640 9.830 10.730 11.820 12.090 13.540 14.480 15.
ALL ., .
Male: c
790310150620820510830430260740540640730840090
ALL
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
. . .
Diseases of the heart . . . . . . . . . . . . . . . . . . 3,058Accidents/adverse effects. . . . . . . . . . . . . . . 2,946Malignant neoplasms. . . . . . . . . . . . . . . . . . 1,713Liver disease/cirrhosis ., ... . . . . . . . . . 801Cerebrovascular diseases . . . . . . . . . . . . . . 664Pneumonia/influenza . . . . . . ... ... . . 580Diabetes mellitus . . . . ... . . . . . . . . . . . . 470Homicide . . . . . . . . . . . . . . . . . . . . . . . . . 458Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 447Conditions arising in perinatal period . . . . 331Nephritis, et al. . . . . . . . . . . . . . . . . . . . . . . . . 229Congenital anomalies . . . . . . . . . . . . . . . . . . 205Chronic pulmonary diseases . . . . . . . . . . . . 177Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . 122Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . 77All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3,043All causes . . . . . . . . . . . . . . . . . . . . . .......15,321
Diseases of the heart ., ... ... ... . . . .Malignant neoplasm.. . . . . . . . . . . . . . .Accidents/adverse effects. . . . . . . . . . . . . . .Liver disease/cirrhosis . . . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period ,...Nephritis, et al.. . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Congenial anomalies . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . .Atherosclerosis. . . . . . . . . . . . . . . . . . . . .All others. . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . ..., . . . . . . . . . . . . . . . . .
1,23482778135133426124112712512510266655443
1,2585,994
Accidents/adverse effects . . . . . . . . . . . . . . . 2,165Diseases of the heart . . . . . . . . . . . . . . . . . . 1,824Malignant neoplasms. . . . . . . . . . . . . . . . . . . 886Liver disease/cirrhosis . . . . . . . . . . . . . . . . . . 450Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 381Pneumonia/influenza . . . . . . . ..., ..., . . . 339Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . 333Cerebrovascular diseases. . . . . . . . . . . . . . . 330Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . 209Conditions arising in perinatal period . . . . 204Chronic pulmonary diseases . . . . . . . . . . . . 123Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . 104Congenital anomalies . . . . . . . . . . . . . . . . . . 103All other external causes . . . . . . . . . . . . . . . 97Septicemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,722All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9,327
166.7136.398.448.133.826.627.821.219.49.8
12.46.59.66.54.2
151.0778.3
121,589.469.040.131.328.821.0
7.512,811.76.55.46.55.63.5
118.1578.7
207.8219.0109.157.034.033.231.137.026.712.014.212.06.5
10.06.5
182.7998.8
%omparabletolCD-9 codes, available from IHS
195.039.8
131.611.438.112.3
9.810.411.59.24.55.8
16.32.90.6
69.0568.2
135.1108.620.4
7.435.4
9.69.28.23.64,35.55.72.49,54,6
50.9420.4
60.2271.2163,7
16.018.016.616.741.710.010.326.2
5.66.12.23.4
85.4753.3
0.93.40.74,20.92.22.82.01.71.12.81.10.62.27.02.21.4
0.90.83.45.40.93.02.30.93.62.71.21.02.70.60.82.31.4
3.50.80.73.61.92.01.90.92.71.20.52.11.14.51.92.11.3
b Ra nk ed by number of deathsCNote that age and sex distributions are CalCulatecj for reservation States and may or may not reflect age and sex distribution in IHS areas.
SOURCES U.S. allracea:US Department of Health and Human Services, Publlc Health Service, National Centerfor Health Statistics, “AdvanceReporl, Final MortalityStatistics, 1981,’’ &fonth/y Vita/ Sfaf/sf/cs Reporl 33(3) suPP, June22, 1984, Indiansin IHS areas: US. Department of Health and Human Services PubllcHealth Serwce, Health Resources and Services Admlnistratlon, Indian Health Service, computer tape supplied to the Office of Technology Assessment,Washington, DC, 1985

Table 4-7.— Fifteen Leading Causes of Death and Age-Adjusted Death Ratesa Rankedb for U.S. All Races 1981 and IHS Areas 1980.82, . - - - -(rate per 100,000 population)
All IHS areas(excluding
u s California)(rank)
Cause (rate)
Diseases or the heart
Malignant Neoplasms
Cerebrovascular disease
Accidents/adverse conditions
Chronic pulmonary disease
Pneumonia/influenza
Diabetes Mellitus
Liver disease/cwrhosis
Atherosclerosis
Suicide
Homicide and legal Intervention
Conditions arising inperinatal period
Nephritis et al
Congenital anomalies
Septicemia
Tuberculosis
All others
All causes
11950
2131 6
3381
4398
5163
6123
798
811 4
95210
11 511
104
9’;13
4514
5815
29–d
06—
638—
5682
(rank)(rate)
11667
39 8 5
5
3 3 82
136313
9 66
2 6 67
2 7 84
48. 1d
——
9195
821 2
9.811
12412
6 514
6.515
4 2
1508—
7783
Aberdeen(rank)(rate)
12890
31542
7499
21823
12167
5481
104 4 6
4
98.9–d—8
3746
452
9179
11234
1364–d—14
9 4
2379—
1,261 3
Alaska Albuquerque(rank) (rank)(rate) (rate)
21651
31382
4457
12105
10142
5354
–d—
9271
153.9
8214
6255
7153
139011
68–d—12
101—
1899
9181
2
8013
8208
2361
1244–d—
7235
6359
4470
1436
5293
9154
124 8
11151
107813
95—
—201 1
—7031
Bemidji Billings(rank) (rank)(rate) (rate)—1
32803
15044
5362
13079
20.46
2677
3075
36311
11 28
18110
11. 9
1262
159913
5714
85——
952—
9435
22826
3156.8
6446
12361
11276
83 5 3
93 8 4
41122
– d—
73 3 4
53 6 4
10123
12142
154 513
4 9– d——
2210—
1,2603—aEj.oth SexeS Combined Rates and rank may differ subs(antlallv bv sex see text See aOD B for deaths and @3S for 72 CausesbRanked by number Of deaths In Order 10 & consistent with NCHS methods Order by ‘age-adlusted mortatlly rates may be differentCvalld rates not available see text for fuller explanationdNot among 15 Ieadlr!g causes Of death
California( rank)
1
3
4—
2—
10
9—
7—
5—
13
8—
6
12—
11
—
—
14
—
—
.
Nashville(rank)(rate)
1 -2249
21260
4522
3909
–d—
6259
5399
7308
–d
9174
8225
10138
1254–d
5213
42–d——
1063
7654
Navajo(rank)(rate)
—.. —2
7733
766
617.1
11657
154 6
4286
11141
521 4
– d—
9123
7150
125 2
10131
115 213
5 0– d—
1951
6563
Oklahoma(rank)(rate)
11464
28 5 7
42 9 7
36 6 9
11
7 37
1 3 75
2 6 96
2 5 415
3 212
6 98
126
99 210
7 78
8 414
4 4
7 6 2
5306
Phoenix Portland Tucson(rank) (rank) (rank)(rate) (rate) (rate)
21778
4760
93 4 2
11500
14
8 35
4 1 37
4543
873– d—
8282
6355
9 ’ ;10
21613
4 713
8 3– d
—
1899
9182
21703
4739
53 9 8
11256
11126
8220
7247
371 7
– d—
621 1
10172
911 9
1211 8
127.714
6 0– d
—
1335—
7498
2171 6
471 9
1026.7
11438
– d—
73 3 0
654.2
3
8 1 3– d
54 2 2
92 3 8
– d—
122 3 6
14
6 38
2 7 613
159—
2892—
1. 011. 1
!SOURCES U.S. all races: Department of Health and Human Services, Publlc Health Service, National Center for Health Statlstlcs, Monthly V/fa/ Stat/st/cs Report 33(3) supp June 22 1984, IHS Areas: U S Depart-
ment of Health and Human Serwces, Publlc Health Serwce, Health Resources and Services Admlnistratlon, Indian Health Service, computer tape supplled to the Off Ice of Technology Assessment,Washington, DC, 1985

Table 4-8.—Leading Causes of Indian Deaths 1951-53and U.S. All Races 1952
Percent ofCause all causes
Ch. 4—Health Status of American Indians • 95
Table 4.9.—Crude Death Rates for 3 Year PeriodsCentered in 1973, 1976, and 1981 for Indians in
11 IHS Areas,a 15 Leading Causes of Death(rate per 100,000 population, not adjusted for age)
Indians 1951 -52.&Heart diseases . . . . . . . . . . . . . ... . . . . . . . 14.2Accidents . . . . . . . . . . . . . . . . . . . . . . . . . . 14.1Influenza and pneumonia . . . . . . . . . . . . . . . . . . 10.5Tuberculosis, all forms . . . . . . . . . . . . ... . . 8.1Certain diseases of early infancy ... . . ... 7.1Malignant neoplasms . . . . . . . . . . . . . . . . . ... , 5.9Gastritis, duodenitis, enteritis, and colitis . . . 5.9Vascular lesions affecting
central nervous system . . . . . . . . . . . . 4.3Congenital malformations . . . . . . . . . . . . . . . . 1.6Homicide and legal execution . . . . . . . . . . . . 1.6
All races 1952:Heart diseases . . . . . . . . . . . . . . . . . . . . . . . . . . 37,1Malignant neoplasms . . . . . . . . . . . . . . . . . . . . 14,9Vascular lesions affecting central
nervous system. . . . . . . . . . . . . . . 11.1Accidents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6.4Certain diseases of early infancy . . . . . . . . . . . 4.3Influenza and pneumonia . . . . . ... . . . . . . . . 3.1General arteriosclerosis . . . . . . . . . . . . . . . . . . . 2.1Diabetes mellitus. . . . . . . . . . . . ... ... . . . . . 1.7Tuberculosis, all forms . . . . . . . . . . . . . . . . . 1.6Congenital malformations . . . . . . . . . . . . . . . . 1.3aBaSed on rnortallty data for populaton of 460,0C0 Indians in 23 reservation States
SOURCE U S Department of Health, Educat!on, and Welfare, Hea/fh Serv/cesfor ,4rner(can /nd/ans (Washington, DC U S DHEW, 1957)
dian rate was below the U.S. all races rate (seefigure 4-7). Despite a long-standing recognitionthat alcohol abuse is the major health problemof American Indians (156), there is still no agree-ment on either the causes or treatment for thisproblem among Indians (66,72).
Cerebrovascular diseases (diseases of the cir-culatory system affecting the brain) are the fifthleading cause of death among IHS area Indianson average. Like the death rate from diseases ofthe heart, the mortality rate from cerebrovascu-lar disease is on average lower among Indians thanamong U.S. all races. It substantially exceeds theU.S. all races rate in the same IHS service areasas for heart disease (Aberdeen, Bemidji, Billings,Nashville), plus Alaska (see figure 4-8).
In the 1950s pneumonia and influenza com-bined were the third leading cause of Indiandeaths; in the 3-year period centered in 1981,pneumonia and influenza had declined to the sixthleading cause of Indian death. However, the age-adjusted rate of 26.6 Indian deaths per 100,000population compares unfavorably to the U.S. allraces rate for 1981 of 12.2. Pneumonia is largely
IHS 1972-74 1975-77 1980-82code Cause rate rate
790
800810310150620430
510260830820740
640730
9030
480
Accidents/adverseconditions . . . . . . . . . . 186.1Motor vehicles. . . . . . . 104.2All other accidents . . . . 82.0
Diseases of the heart. . . . 141.8Malignant neoplasms . . . . 70.6Liver disease/cirrhosis . 46.2Cerebrovascular
disease . . . . . . . . . . . . . . 42.5Pneumonia/influenza . . . . 43.0Diabetes mellitus . . . . . . . 22.2Homicide . . . . . . . . . . . . . 22.6Suicide . . . . . . . . . . . . . . . . 22.0Conditions arising in
perinatal period . . . . . . . 22.8Nephritis, et al . . . . . . . . . 6.2Congenital anomalies . . . 10.0Septicemia . . . . . . . . . . . . . 5.7Tuberculosis . . . . . . . . . . 8.9Atherosclerosis . . . . . . . . . 7.3All other causes . . . . . . . . 180.3All causes . . . . . . . . . . . . . 838.2
158.691.167.5
126.667.844.3
35.835.919.921.323.7
21.25.39.96.17.07.0
154.7745.1
rate
125.571.154.4
130.373.034.2
28.324.720.019.519.0
14.19.88.75.23.33.2
134.0652.8All
aEXcludeS califofflla which did not become an IHS Service area Until 1978
SOURCES 1972.74 and 1975-77 deaths: U S Department of Health, Education,and Welfare, Public Health Service, Health Services Admlnlstration,Indian Health Serwce, Selected Vita/ Statisf/cs for /rrd/an f+ealfh Sew-ice Areas and Service Units, 1972 to 1977, DH EW Pub No (HSA)79-1005 (Rockville, MD HSA, 1979) 1972.74 and 1975.77 population:U S Department of Health and Human Serwces, Public Health Serv.Ice, Heatth Resources and Serwces Administration, Indian HealthService, Program Statistics Branch, Population Statistics Staff, In.ternal document, Rockwlle, MD, Feb 1, 1985 1980-82 data: U SDepartment of Health and Human Services, Publlc Health Service,Health Resources and Services Administration, Ind!an Health Serv.Ice, computer tape provided to the Office of Technology Assessment,Washington, DC, 1985
Table 4.10.—Mortality Rates From Diseases of theHeart by Age: Indians in 11 IHS Areas 1980-82
and U.S. All Races 1981 (rate per 100,000 population)
Indians in IHS areas U.S. Ratio IHS(excluding California) all races to Us.
Age group 1980-82 1981 all races
0 to 4 . . . . 14.5 106.1 0.15 to 14 . . . 0.9 0.9 1.0
15 to 24 . . . 5.3 2.6 2.025 to 34 . . . 15.2 8.4 1.835 to 44 . . . 55.9 43.2 1.345 to 54 . . . 172.6 177.7 1.055 to 64 . . . 454.2 481.5 0.965 to 74 . . . 1,024.2 1,175.8 0.975 to 84 . . . 2,064.3 2,850.3 0.7>85. . . . . . . 4,363.8 7,459.0 0.6SOURCES Indian data:U S. Department of Health and Human Services, Pub)ic
Health Service, Health Resources and Serwces Administration, Indi.an Health Serwcel computer tape supplled to the Office of Technol-ogy Assessment, Washington, DC, 1985 U.S. all racea data: U SDepartment of Health and Human Services, Publlc Health Service,National Center for Health Statistics, “Advance Report of Final Mor.tality Statlstlcs, 1981 ,“ Monthly V/ta/ Stat/stfcs Report 33(3) supp ,June 22, 1984

Figure 4-4.—Age-Adjusted Death Rates for Diseasesof the Heart, American Indians in 11 IHS Areas
(excluding California) 1980-82
U S. all races
IHS total excludingCalifornia
A b e r d e e n
195.0
166.7
Alaska
Albuquerque
Bemidji
Billings
Nashville
165.1
80.1
289.0
328.0
A
282.6
4
224.8
&
Navajo
L
77.3
Oklahoma City 146.4
Phoenix 177.8
Portland 170.3
Tucson 171.6
1 1 1 1 I i 1 1
50 100 150 200 250 300 350 400
Age-adjusted mortality rate (per 100,000 population)
SOURCE U.S Department of Health and Human Services, Publlc Health Serwice, Health Resources and Services Administration, Indian Health Sew.Ice, computer tape supplied to the Off Ice of Technology Assessment,Washington, DC, 1985
Figure 4-5.—Age.Adjusted Death Rates for Accidentsand Adverse Conditions, American Indians in
11 IHS Areas (excluding California) 1980-82
U S all races
IHS total excludingCalifornia
Alaska
39.8
136.3
182.3
210.5
Albuquerque 124.4
Bemidji 130.7
Billings 236.1
Nashville 90.9
Navajo
Oklahoma City
Phoenix
Portland
Tucson
165.7
66,9
149,9
125.6
4
dt 1 1 1 1 1 1 I 1
30 60 90 120 150 180 210 240
Age-adjusted mortality rate (per 100,000 population)
SOURCE U S Department of Health and Human Services, Public Health Serv.ice, Health Resources and Services Administration, Indian Health Serv.Ice, computer tape supplied to the Office of Technology Assessment,Washington, DC, 1985.

Table 4-11 .—Mortality Due to Accidents by AgeIndians in IHS Areas (excluding California) 1980-82and U.S. All Races 1981 (rate per 100,000 population)
Ratio IHS areaIHS area Us . Indians to U.S.
Age group Indians all races all races
<1 . . . . . . . . . . . . . . . 27.0 27.3 1.01 to 4 ., . . . . . . . . . . 88.0 23.6 3.75 to 14 . . . . . . . . . . . 26.1 14,2 1.8
15 to 24 . . . . . . . . . . . 164.2 56.0 2.925 to 34 . . . . . . . . . . . 182,0 45.1 4.035 to 44 . . . . . . . . . . 159.2 35.7 4.545 to 54 . . . . . . . . . . . 159.7 37.7 4.255 to 64 . . . . . . . . . . . 170,1 40.4 4.265 to 74 . . . . . . . . . . . 170.5 54.3 3.175 to 84 . . . . . . . . . . . 209.3 108.2 1.9>85. . . . . . . . . . . . . . . 356.0 273.3 1.3Age-adjusted rate ., . 136.2 39.8 3.4SOURCES Indian data:U.S Department of Health and Human Serv!ces, Publtc
Health Service, Health Resources and Servtces Administration, lndl-an Health Service, computer tape supplied to the Office of Technol-ogy Assessment, Washington, DC, 1985 U.S. all races data: U.SDepartment of Health and Human Serwces, Publ!c Health Serwce,National Center for Health Statistics, “Advance Report of Final Mor.taltty Statistics, 1981 ,“ Monthly V(fa/ Stafisfics r?epor? 33(3) supp ,June 22, 1984
responsible for the high Indian death rate in thiscategory. In the 3-year period centered in 1981,all IHS areas had pneumonia mortality rateshigher than the U.S. all races rate (see figure 4-9). The pneumonia mortality rate for Indians ex-ceeded the U.S. all races rate in all age groups,but particularly among the very young and thosebetween 25 and 55 (table 4-12), This widespreadproblem with pneumonia mortality indicates thata variety of causes may be responsible (e.g., in-adequate access to care (see below), alcohol abuse(loo)).
Diabetes mellitus is the seventh leading causeof death among the IHS service population andhas been identified as a growing problem. Despitea drop in crude death rates from diabetes between1972 and 1982, the age-adjusted death rate in IHSareas exceeds that of U.S. all races in every areabut Alaska, where diabetes is not even among the15 leading causes of death (see figure 4-10), Theoverall diabetes death rate in IHS areas exceededthe U.S. all races rate by 2.8 times, exceeding itby 5.2 times in the Aberdeen area.
Ch. 4—Health Status of American Indians ● 9 7
Figure 4-6.—Age-Adjusted Death Rates for MalignantNeoplasms (Cancer), American Indians in 11 IHS Areas
(excluding California) 1980-82
U S all races
IHS total excludingCalifornia
Aberdeen
131.6
98.4
Alaska
Albuquerque
138,2
8 2 0
Bemidji 150.4
Billings
Nashville
Navajo
Oklahoma City
Phoenix
Portland
Tucson
\
76.6
85.7
76.0
4
73.9
%
71,9
I ●
126,0
1 1 1 1 1 1 1 1 I
20 40 60 80 100 120 140 160
Age-adjusted mortality rate (per 100,000 population)
SOURCE U S Department of Health and Human Services, Public Health Serv.Ice, Health Resources and Services Administration, Indian Health SewIce, computer tape supplled to the Office of Technology Assessment,Washington, DC, 1985

98 ● Indian Health Care
Figure 4-7.—Age-Adjusted Death Rates for LiverDisease and Cirrhosis, American Indians in11 IHS Areas (excluding California) 1980.82
U S all races
IHS total excludingCalifornia
Aberdeen
Alaska
Albuquerque
Bemidji
Billings
(ua)z
Nashville
Navajo
Oklahoma City
Phoenix
Portland
Tucson
1 11.4
98.8
Figure 4-8.—Age-Adjusted Death Rates forCerebrovascular Disease, American Indians
in 11 IHS Areas (excluding California) 1980-82
U S all races
IHS total excludingCalifornia
Aberdeen
27.1 Alaska
36.3
1 30.8
I 112.2
J
21.4
25,4
87.3
81.3
1 I 1 1 J20 40 60 80 100 120
Age-adjusted mortality rate (per 100,000 population)
SOURCE U S Department of Health and Human Services, Public Health Serv-ice, Health Resources and Services Administration, Indian Health Serv.ice, computer tape supplied to the Office of Technology Assessment,Washington, DC, 1985
Albuquerque
Billings
38.1
33.8
49.9
45.7
23.6
53,6
44.6
Navajo 17,1
Oklahoma City 29.7
Portland 39.8
Tucson 26.7
I 1 I I I I I
10 20 30 40 50 60
Age-adjusted mortality rate (per 100,000 population)
SOURCE’ U.S Department of Health and Human Services, Public Health Serv-ice, Health Resources and Serwces Administration, Indian Health Serv-ice, computer tape supplied to the Office of Technology Assessment,Washington, DC, 1985

Ch. 4—Health Status of American Indians ● 9 9
123
26.6
Figure 4-9.—Age-Adjusted Death Rates forPneumonia, American Indians in 11 IHS Areas
(excluding California) 1980-82
U.S. all races
IHS total excludingCalifornia
Aberdeen
Alaska
Albuquerque
Bemidji
Billings
Nashville
Navajo
Oklahoma City
Phoenix
Portland
Tucson
3 5 4
2 3 , 5
2 6 7
3 5 3
2 5 . 9
2 8 6
.
137
2 2 . 0
3 3 . 0
1 1 I 1 1 I
10 2 0 3 0 4 0 5 0
Age-adjusted mortality rate (per 100,000 population)
SOURCE U S Department of Health and Human Services, Public Health Servtee, Health Resources and Serwces Admlnlstratlon, Indian Health Sew-Ice, computer tape supplied to the Office of Technology AssessmentWashington, DC 1985
While homicide and suicide are the 11th and10th leading causes of death for U.S. all races,on average they are the 8th and 9th leading causesof death, respectively, among IHS service area In-dians. There was no IHS area with a homicidemortality rate less than that of U.S. all races (fig-ure 4-11), and there was no Indian age group witha homicide mortality rate less than that of U.S.all races. (The rate for blacks, which is the high-est of all U.S. populations, exceeds that for In-dians, at a ratio of 2:1 for males, ) On average theIndian homicide rate in IHS areas was twice thatfor U.S. all races, with ratios as high as 6.3:1among Aberdeen area females (see figure 4-12).
Although the crude death rate from Indian sui-cide has apparently declined since the 3-yearperiod centered in 1973, the age-adjusted rate stillexceeded the U.S. all races rate by a ratio of 1.7:1.Suicide tends to claim the lives of young Indians;as shown in table 4-13, the Indian age-specificdeath rates for suicide exceeded those of U.S. allraces for all age groups up to age 44, with a 3.2:1ratio in the 15 to 24 age group. Hypotheses aboutthe causes of suicide vary. Despair and low self--esteem resulting from lack of social and economicopportunities and persistent poverty (109), tribalnorms operating against achievement and successand against interference in another’s personal life(11), acculturation pressures associated with eco-nomic development (110), and other factors havebeen posited as causes of self-inflicted injury inIndians.
Death rates in IHS service areas from condi-tions originating in the perinatal period (the periodimmediately around the time of birth) have de-clined since 1972, but they are still the 10th lead-ing cause of death among Indians, compared tobeing the 12th leading cause of death for U.S. allraces. The importance of these causes, and con-genital anomalies, another leading cause of infantdeath, to Indian infant mortality in general is dis-cussed below under “Infant mortality. ”

100 ● Indian Health Care
Table 4-12.—Mortality Rates for Pneumonia by AgeU.S. All Races and Indians in IHS Areas (excluding
California) 1980-82 and U.S. All Races 1981(rate per 100,000 population)
Ratio IHS areaIHS area U.S. Indians to U.S.
Age group Indians all races all races
<1 ............................... 71.9 22.2 3.21 to 4 . . . . . . . . . . . . 6.7 1.7 3.95 to 14 . . . . . . . . . . . 1.5 0.4 3.7
15 to 24 . . . . . . . . . . . 1.9 0.7 2.725 to 34 . . . . . . . . . . 5.0 1.4 3.635 to 44 . . . . . . . . . . . 9.7 3.2 3.045 to 54 . . . . . . . . . . . 22.2 7.2 3.155 to 64 . . . . . . . . . . . 37.4 17.7 2.165 to 74 . . . . . . . . . . . 96.7 50.0 1.975 to 84 . . . . . . . . . . . 383.8 197.6 1.9>85 . . . . . . . . . . . . . . . 1,566.6 787.6 2.0Age-adjusted rate . . . 25.6 13.9 1.8SOURCES Indian data:U S Department of Health and Human Services, Public
Health Service, Health Resources and Services Adminlstratlon, Indl.an Health Service, computer tape supplied to the Off Ice of Technol.ogy Assessment, Washington, DC, 1985 U.S. all racas data: U S.Department of Health and Human Services, Public Health Service,National Center for Health Statistics, “Advance Report of F!nal Mor.taltty Statwtics, 1981, ” Monthly Vftal Statistics Report 33(3) ”supp ,June 22, 1984
As discussed above, diabetes is perceived to bea growing problem among Indians in almost allareas. Kidney failure is a common sequelae of di-abetes, and IHS area Indian deaths from renal fail-ure exceeded the U.S. all races rate by 2.8 (figure4-13). The larger category of kidney problems(nephritis, nephrotic syndrome, and nephrosis)was the 11th leading cause of death for Indiansin IHS areas in 1980 to 1982, showing an appar-ent 50 percent rise since the 3-year period centeredin 1973.
Deaths due to chronic pulmonary diseases, the13th leading cause of death among IHS servicearea Indians, were below the U.S. all races rateon average, although they exceeded the U.S. allraces rate in three IHS areas: Aberdeen, Bemidjiand Billings (figure 4-14).
Mortality from septicemia (systemic infection)was the 14th leading cause of death among In-dians, accounting for 122 deaths. Overall this ratewas more than twice that of the U.S. all races rate;small numbers in individual areas make compar-isons difficult.
Figure 4-10.—Age-Adjusted Death Rates for DiabetesMellitus, American Indians in 11 IHS Areas
(excluding California) 1980.82
U S all races
IHS total excludingCalifornia
Aberdeen
Alaska
Albuquerque
Bemidji
Billings
Navajo
Oklahoma City
Phoenix
10.4
21.2
45.2
25.5
15.4
11,9
36.4
22.5
15.0
12.5
35.5
PortlandI I 17,2
Tucson 23.8
1 I 1 1 I10 20 30 40 50
Age-adjusted mortality rate (per 100,000 population)
SOURCE U S Department of Health and Human Serwces, Public Health Sewice, Health Resources and Serwces Administration, Indtan Health Sew-Ice, computer tape supplied to the Office of Technology Assessment,Washington, DC, 1985

Ch. 4—Health Status of American Indians ● 101—
Figure 4“11. —Age-Adjusted Death Rates forHomicide, American Indians in 11 IHS Areas
(excluding California) 1980.82
Figure 4-12.—Age-Adjusted Death Rates for Homicide,American Indians Male and Female, in 11 IHS Areas
(excluding California) 1980-82
P 9.8U S all races
IHS total excludingCalifornia
Aberdeen
4,3
117
U S al! races
IHS total excludingCalifornia 2 7 . 8
182
4.9
7.5
16.2
Alaska
Albuquerque
44.6
-
2.7
.
3 5 9
3 0 7
3 8 4
39.9
AberdeenBemidji
Billings
AlaskaNashville 13.1
Navajo 57
Oklahoma City 7.4
Phoenix 18.3
Portland 138
Albuquerque
Tucson 57
mal<
U S all races 16.7
IHS total excludingCalifornia 3 1 1
Billings
NashvilleAberdeen [ 6 4 . 9
Alaska I 3 2 . 4
P 144NavajoAlbuquerque 270
Bemidji 1 6 5
2 6 9
1
4 5 , 4
A
Oklahoma City
Nashville
Phoenix
Portland I 2 4 7
Tucson 4 3 8
1 1 I 1 1 I 110 20 30 40 50 60 70
Tucson I 5 4 . 2
I 1 1 1 1 1 1
10 20 30 40 50 60
Age-adjusted mortality rate (per 100,000 population)
SOURCE U S Department of Health and Human Services Publlc Health Serv.Ice, Health Resources and Services Adminlstrat!on, Indian Health Sew.Ice computer tape supplled to the Of f!ce of Technology Assessment,Washington DC 1985
Age-adjusted mortality rate (per 100,000 population)
SOURCE U S Department of Health and Human Services, Publ!c Health Serv.Ice Health Resources and Services Adminlstratlon, Indian Health Serv.Ice, computer tape supplied to the Office of Technology Assessment,Washington, DC, 1985

102 ● Indian Health Care
Table 4-13.—Suicides and Suicide Rates by Age Indians in IHS Areas1980-82 and U.S. All Rates 1981 (rate per 100,000 population)
IHS U.S. all races Ratio IHS serviceAge group Number Rate rate areas to U.S. all
0 to 4 . . . . . . . . . . . . . . . —5 to 14 . . . . . . . . . . . . . . 4
15 to 24 .., . . . . . . . . . . . 21825 to 34 . . . . . . . . . . . . . . 13635 to 44 . . . . . . . . . . . . . . 5745 to 54 . . . . . . . . . . . . . . 2555 to 64 . . . . . . . . . . . . . . 1265 to 74 . . . . . . . . . . . . . . 775 to 84 . . . . . . . . . . . . . . 1>85 . . . . . . . . . . . . . . . . . —
—0.78
39.237.323.714.08.98.92.9—
—0.5
12.316.315.916.116.416.218.617.7
—1.53.22.31.50.90.50.50.2—
SOURCES” Indian data:U S Department of Health and Human Services, Public Health Serwce, Health Resources and SerwcesAdministration, Indian Health Serwce, computer tape suppl!ed to the Office of Technology Assessment, Washing-ton, DC, 1985. U.S. all racas data: U S, Department of Health and Human Servtces, Public Health Service, NationalCenter for Health Statistics, “Advance ReDOrt of Final Mortality Stattstlcs, 198t ,“ Morrth/v Vital Statistics Ffmort33(3) supp , June 22, 1984
The declining incidence of tuberculosis is amongthe most notable improvements in Indian health.In the early 1950s tuberculosis was the fourth lead-ing cause of death among Indians across theUnited States, accounting for 8.1 percent of In-dian deaths. In the 3-year period centered in 1981,tuberculosis was the 15th leading cause of Indiandeaths, accounting for 0.5 percent of deaths. Theage distribution of most deaths from tuberculo-sis also identifies it as a declining problem amongIndians. A total of 77 Indians were identified ashaving died of tuberculosis in the 3-year periodcentered in 1981; almost 90 percent of them wereage 45 or above.
Infant Mortality
In the early 1950s, what were then called “dis-eases of early infancy” (now called certain con-ditions arising in the perinatal period) were thefifth leading cause of death among Indians andother U.S. populations alike, although these dis-eases accounted for a greater proportion of In-dian deaths (7.1 percent) than U.S. all races deaths(4.3 percent). Congenital malformations (nowcalled congenital anomalies) were the 9th leadingcause of death among Indians in the early 1950S,and the 10th among U.S. all races. Since the early1950S, infant mortality has declined significantlyamong all U.S. populations, but, reflecting theIHS emphasis on maternal and child health, at agreater rate among Indians (188,191). However,as with most other causes of death, infant mor-tality rates still exceed that of U.S. all races on
average, a situation due primarily to the persist-ence of high mortality rates among postneonates(i.e., infants between 28 days and 1 year). Deathrates of Indian postneonates exceeded that of U.S.all races in all areas but Oklahoma City (figure4-15). Most of these deaths were attributed to sud-den infant death syndrome, the cause of whichis unknown, but which in general has been re-ported to occur among low birth weight infantsborn to young mothers who smoke (185). OTAwas not able to investigate fully those relation-ships from available data. About one-quarter ofIndian infants are born to females 19 or younger,compared to a rate of about 1.5 percent of birthsto U.S. all races teenage females (175a,191). Onaverage, the percent of low birth weight infantsamong Indians (6.1 percent in 1980 to 1 9 8 2(175a,191) is about equal to the percent for U.S.all races (6.3 percent in 1981), but this figure isconsidered high among industrialized nations,Most of these low birth weight infants are bornto older Indian women, unlike the U.S. all racesexperience, in which a higher proportion of lowbirth weight infants are born to teenagers.
On average the death rate among Indian neo-nates (from O to 27 days old) was lower than thatof U.S. all races; only two areas (Aberdeen andAlaska) exceeded the U.S. all races rate (figure4-15),
Indians in Urban Areas
There is very little information on the healthstatus of urban Indians, despite the fact that they

Figure 4-1 3.—Age-Adjusted Death Rates for RenalFailure American Indians Both Sexes, in 11 IHS Areas
(excluding California) 1980-82
U S all races
IHS total excludingCalifornia
Aberdeen
Alaska
Albuquerque
Bemidji
Billings
Nashville
Navajo
3.8
+
107
20.9
7.8
124
,
8 7
12.8
3.9
i
11.7
Oklahoma City
P
6,4
Phoenix I 18,2
Portland
P
9.9
TucsonI I
2 1 . 0
Jt 1 1 I 1 1 1 1
3 6 9 12 15 18 21
Age-adjusted mortality rate (per 100,000 population)
SOURCE U S Department of Health and Human Services, Public Health Serv.Ice, Health Resources and Services Admlnlstratlon, Indian Health Sew-Ice, computer tape supplled to the Off Ice of Technology AssessmentWashington, DC 1985
Ch. 4—Health Status of American Indians Ž 103
Figure 4-14.—Age-Adjusted Death Rates for ChronicPulmonary Diseases American Indians Both Sexes,
in 11 IHS Areas (excluding California) 1980-82
U S all races
IHS total excluding CA
Aberdeen
Alaska
Albuquerque
Bemidji
16.3
9.6
16.7
7
14.2
4
+2.1
20.4
Nashville
P
4.7
NavajoP 4 .5
Oklahoma City P 7 .3
Phoenix P 8 .3
Portland
F
12,6
Tucson 7 .9
1 1 1 1 1 I J5 10 15 20 25 30
Age-adjusted mortality rate (per 100,000 population)
SOURCE U S Department of Health and Human Serwces, Publlc Health Serv.ice, Health Resources and Serwces Administration, Indian Health Serv.ice, computer tape supplied to the Off Ice of Technology Assessment,Washington, DC, 1985.

104 ● Indian Health Care
Figure 4-15.—lnfant Mortality Rates: American Indiansin IHS Areas 1980-82 and U.S. All Races, 1981
Area
Bemidji 11.3
Billings 14.0
Nashville 14.9
Navajo 12.8
Phoenix 12.3
Portland 16.9
Tucson 1 9 . 5
U S all races j8.0
IHS total
e
5.8
Aberdeen 10.2
Alaska 8.6
Albuquerque 4.6
Navajo
E
4.2
Oklahoma City 5.1
Phoenix 5.3
Portland 7.2
Tucson
U S all races
IHS total
E
7.4
Aberdeen 11.5
Alaska 8.7
Oklahoma City
Phoenix
Portland
Tucson
7.1
17.4
8.4
18.6
3 . 8
7 .0
I 9.7
13 .5I 1 1 1 i 1 13 6 9 12 15 18 21
Mortality rate(rates per 1,000 live births)
SOURCES: Indian data: U S Department of Health and Human Serwces, PublicHealth Service, Heaith Resource and Services Admln!stration, lndi-an Health Service, Computer tape supplied to the OTA, 1985. U.S. AllRaces data: U.S Department of Health and Human Serwces, PublicHealth Service, Health Resource and Services Administration, Indl.an Health Service, Chart Series, 1985
are estimated to constitute about 50 percent of thetotal Indian population. IHS does not collect diag-nostic patient care information from urban pro-grams, and does not analyze or publish vital sta-tistics or population characteristics for urbanIndians except when these data are included withnational level data on the reservation States.
Vital statistics information on Indians residingin Standard Metropolitan Statistical Areas (SMSAs)was provided to OTA as part of 1980 to 1982mortality information. Thus, OTA was able togenerate some death rate information on urbanIndians. However, because of the lack of age-specific population information, OTA was notable to generate age-adjusted rates; therefore theurban rates may only be comparable to cruderates for other Indians or to crude rates of par-ticular urban areas; they are not comparable toU.S. all races age-adjusted rates, the standard ofcomparison generally used in this report. On aver-age, however, Indians in SMSAs show essentiallythe same pattern of causes of death that is shownin IHS service areas. The leading causes of deathwere: 1) diseases of the heart; 2) accidents andadverse effects; particularly motor vehicle acci-dents; 3) cancer; 4) liver disease and cirrhosis; 5)cerebrovascular diseases; 6) homicide; 7) diabetesmellitus; 8) suicide; 9) pneumonia and influenza;and 10) conditions arising in the perinatal period.The existence of these and other problems simi-lar to those of reservation Indians is supportedby findings of studies by IHS (170), urban pro-grams (5), and others (211),
Illness and Use of Services
There have been no large-scale epidemiologi-cal studies of overall Indian health. Therefore,conclusions about the prevalence and incidenceof illness in IHS areas are subject to limitationsof data on outpatient and inpatient care. Thesedata must be used cautiously because they maybe a more accurate reflection of the availabilityof services than the incidence and prevalence ofillness. OTA found substantial differences be-tween the use of medical services in IHS areas andwhat might be expected based on other sourcesof information, particularly patterns of mortality.

-
Use of Hospital Care andPatterns of Mortality
Given the poor health status reflected in Indianmortality statistics, it is striking that the overall1984 hospital discharge rate in IHS areas (1,210per 10,000 population) was lower than that inU.S. non-Federal short-stay hospitals (1,585 dis-charges per 10,000 population) (see table 4-14).In general, using data from U.S. non-Federalshort-stay hospitals as a benchmark, IHS totalhospitalization rates (excluding two tribally runhospitals) were lower than would be expectedfrom mortality rates for accidents and violence,circulatory system diseases, malignant neoplasms,alcohol-related conditions, diabetes, and congen-ital anomalies. While Indian death rates from ac-cidents, suicide, homicide, and other externalcauses substantially exceeded U.S. mortality ratesin the 3-year period centered in 1981, the IHS hos-pitalization rates for injuries and poisonings in1981 only slightly exceeded the U.S. rates.
Part of the reason for low hospitalization ratesfor certain diagnoses can be explained by the rela-tive youth of the Indian population. For exam-
Ch. 4—Health Status of American Indians Ž 105
pie, diseases of the circulatory system are the lead-ing cause of hospitalization in U.S. non-Federalshort-stay hospitals, but are the eighth leadingcause of hospitalization in IHS direct and contractgeneral hospitals (hospitals to which IHS service-eligible patients are sent when care is not avail-able in IHS-run facilities). This can be partiallyexplained by the fact that individuals age 65 andover account for 11.3 percent of the U.S. all racespopulation and 60 percent of discharges for cir-culatory system diseases in U.S. non-Federalshort-stay hospitals (203). In IHS hospitals, In-dians 65 and over account for 5.3 percent of theIHS service population and 41 percent of such dis-charges.
But the relative youth of the Indian populationcannot explain all the variation among health sta-tus indicators; the disparity between services pro-vided and need is also apparent from a compari-son of health care utilization and mortality ratesby age. As shown in table 4-15, the ratio of IHSto U.S. non-Federal short-stay hospital inpatientdischarges is lower than the ratio of Indian to U.S.all races mortality rates in all age groups 16 andabove. Thus, there is a discrepancy between
Table 4-14.—Hospital Discharge Rates for Leading Causes: Indian Health ServiceDirect and Contract General Hospitals and U.S. Short-Stay Non-Federal Hospitals
(rates per 10,000 population)
Calendar year 1984Fiscal year 1984 U.S. all races in
Indian and U.S. short-stayDiagnost ic category Alaska nat ive a Non-Federal hospitals
Compl icat ions of pregnancy, chi ldbir th,and puerperium, . . . . . . . . . . . . . . . . . 282 149
Normal deliveries . . ... . . . . . . . . . . . . . . 65 67In ju r i es and po i son ings . . . . . . . . . . . . . . 151 148Respiratory system diseases . . . . . . ... . . . . 114 143Digestive system diseases. . . . . . . . . . . . . . 112 184Genitourinary system diseases . . . . . . . . . . . . . 65 133Supplementary conditions . . . . . . . . . . . . . . . . 64 117Circulatory system diseases . . . . . . . . . . . . . . . 63 239Mental disorders . . . . . . . . ... ... ... . . . 57 72Symptoms, signs, and ill-defined
conditions . . . . . . . . . . . . . . . . . . . . . . . . . , . . 57 22Nervous system and sense organs
diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 71All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 130 240
All categories . . . . . . . . . . . . . . . . . . . . . . . . . . 1,210 1,585alncludes only those persons seen at IHS hospitals or paid for by IHS at contract hospttals, does nOt Include trlba) hospitalworkloads or hospltallzat~ons not paid for by IHS
SOURCES IHS data: U S Department of Health and Human Services, Publlc Health Service, Health Resources and ServicesAdminlstratlon, Indian Health Serwce, Patient Care Statistics Staff, Internal document, Rockvllle, MD Feb 11 1985U.S. data: U S Department of Health and Human Services, Publlc Health Service, National Center for Health Statls-ttcs, “1984 Summary Nat{onal Hospital Discharge Survey, Advance Data from V/fa/ and Health Staf/st/cs, No 112DHHS Pub No (PHS) 85-1250 (Hyattsvllle, MD PHS, Sept 27, 1985), and unpublished data.

106 ● Indian Health Care
Table 4-15.—Age Distribution of Inpatient Discharges IHS Service Areas 1984 and U.S. All Races 1984Compared to Age Distribution in the Population and Age-Specific Mortality Rates
Percent distribution of inpatientdischarges (by age group) Percent in age groupa
Ratio age-specificIHS U.S. Ratio Ratio mortality rate
11 areas all races Indians to Us . Indians to Indians b to U.S.Age group 1984 1984 U.S. all races Indians c all races U.S. all races all racesd
All ages . . . . . . . . . . . 100.0% 100.0% 100.00/0 100.00/0<15 . . . . . . . . . . . . . . . 19.4 8.6 2.3 32.5 22.7 1.4 1.515 to 44 . . . . . . . . . . . 54.0 39.1 1.4 49.2 46.5 1.1 3.645 to 64 . . . . . . . . . . . 15.8 22.1 0.7 13.1 19.7 0.7 1.2>65 . . . . . . . . . . . . . . . 10.9 30.2 0.4 5.3 11.3 0.5 0.9%s of 1980 U S CenSUSbThree year period centered In 1981clndians ,n ~esemation states, Separate calculations are not made for service area Indians.
‘Calendar year 1981
SOURCES IHS Inpatient data: U.S Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Indian HealthService, Office of Planning, Evaluation and Legislation, Program Statistics Branch, Patient Care Statistics Staff, “Utilization of Indian Health Service andContract Hospitals, Fiscal Year 1984, ” internal document, Rockwlle, MD, no date. U.S. all racea lnpatiant data: U S. Department of Health and Human Serv.Ices, Public Health Serwce, National Center for Health Statistics, “1984 Summary: National Hospital Discharge Survey, ” Advance Data from Vital arrd Hea/thStafisflcs, No. 112, DHHS Pub. No (PHS) 831250 (Hyattsville, MD: PHS, Sept. 27, 1985). Age group data: U S. Department of Health and Human Services,Public Health Service, Health Resources and Services Administration, Indian Health Service, Office of Planning, Evaluation and Legislation, Program Statis-tics Branch, Indian Hea/fh Serwce Chart Series Book APrI/ 1985 (Rockville, MD IHS, 1985).
apparent need and the use of health care. Incon-sistencies can more accurately be traced to vari-ations in services available to Indians. The Port-land area, for example, has no IHS hospitals andmust purchase hospital care through the contractcare program, and contract care has been limitedin the past years to emergency and urgent cases.In the Portland area, the number of hospital dis-charges in 1984 (176 discharges) was almost iden-tical to the number in 1979 (166 discharges),despite a 50-percent increase in the service popu-lation. As a result, the Portland area hospital dis-charge rate for most of the diagnostic categorieswas below what would have been expected frommortality data. The Bemidji and Nashville pro-gram areas also follow this pattern. The consid-erable variation in hospital discharge rates bycause among IHS areas is shown in table 4-16.
Outpatient Care
Data generated from IHS outpatient clinics canserve as a general guide to Indian health prob-lems, subject to limitations discussed earlier. Lead-ing diagnostic indicators are consistent with med-ical literature, reports from Indians, and otherdata (e.g., birth rates). Otitis media is a commonreason for seeking outpatient care, as is diabetes,injuries, and well child and prenatal care (see ta-bles 4-17 and 4-18). As discussed above, compar-isons with U.S. all races figures are difficult tomake because of differences between IHS’s and
NCHS’s coding procedures. Other ailments affect-ing Indians in individual areas are discussed be-low. While Indians’ use of outpatient services ishigh, it does not appear to be as great as the needwhen compared with mortality rates by age (ta-bles 4-19 and 4-20).
Dental Needs
An IHS survey of its dental patients in 1983 to1984 found that differences between Indian andU.S. all races dental health were “staggering”(47,160,176). For example, 81 percent of IHS’s 5to 19 year old dental patients had caries (cavities)compared to 63 percent of 5 to 17 year olds ina national survey. Based on its patient experience,IHS’s dental program estimates that 60 percent ofIHS’s service population require an average of11.8 “units” of dental care (e.g., examination,periodontal care, extraction) each, In 1984, thisamounted to a total of 6,632,558 units of care re-quired, but only about 30 percent of these unitswere able to be provided by IHS direct and con-tract dental staff leaving a 70 percent deficiency(180). OTA’s calculations for individual areas in-dicate a range of deficiencies, to as high as an 80percent unmet need for dental services in the Tuc-son service area (table 4-21),
Mental Health Needs
Utilization of mental health (and alcoholism)care is perhaps most dissonant with the estimated

I
Comwrdcqmmeqm. .
U2-mo-mlocn=rmoac c l Lncm u - ! cDLn. c-u.
P.r-o-ulwmucne r - .Cvm Ln=rm=t--tmomm7 m u - J . r-r--cu.r-cu-0-)0. -
CDocncu mwmcucur-lncc
::~:mgg:mmmmLn c u .
mm - . .
C o - r - o.mmmmr.mmm
-cDma P.Jmr. m-mwcx- ? . c u r - .cocnwmlo= l - mmm-. N.
OOOOCn OOP- macOO
r.-rcocd mr-mlo. .r. .::mm CnmcurQ - * m
Cvcw. -
ocoo-raoom-t~a
r. 0 L’T m T 0 7 0 C.7 a cc m-y m w - r r Lc r (0 0. -mm - --
-.-m cuulm. mr-mcnmccLncnr-m- mcflmcnmmm-Omam -rr?r-)-mocc
.- m a r .= 7 Cncnmarum
CUOOOJO
- ? Cnoul=rlnmcu -
OOCU C - 3 0 3
cur - - m!n -c-’dm.
=tC-3c--)=r -
.m=Tm -C u m
Cocurs)qr.
.nCO m - mUJ-=rm.
—
ea . - m-rmmln -.m
CXJUJOCDO
cnm~mt.
Oo m o oU3r--ar.- T r - 0 .r-
rnOm--rwr-r)omc9u)cw -
C D . F-C-3YJ.CumrwcvO r - -
0m
c-d
r-
0-
-r
m
Cu
(7
0
0Ln
r’.
r .ru - -. --
mcnmC.JmoC-Drum.
0 0 0CD*Uu - l - .
Ch.
wz
ma
0
;
b
m
c-?LC
0b
mml
LCm
am
0w
mCx
0r.
0
4—Health Status of American Indians • 107
F - w
-mm
NW
- r -* I
=$
WLc
mr-Cnco
r--
mma0
mm
OccI
-mm
mm- [T
L.>w
Icum
auC9m
-r-
v>
L>u. .

108 • Indian Health Care
Table 4-17.—Number of Outpatient Clinical Impressions, Males and Females:Indian Health Service Facilities, Fiscal Year 1984
Male
Number ofclinical
Condition i repressions
Upper respiratory infection, common cold . . .Acute otitis media . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus. . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . .Laceration, open wound . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . .Refractive error . . . . . . . . . . . . . . . . . . . . . . . . . .
97,99163,69761,20358,36557,89242,43736,62932,562
Female
Number ofclinical
Condition impressions
Prenatal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155,270Upper respiratory infection, common cold . . . 134,881Diabetes mellitus. . . . . . . . . . . . . . . . . . . . . . . . . 102,268Hypertensive disease . . . . . . . . . . . . . . . . . . . . . 75,277Acute otitis media . . . . . . . . . . . . . . . . . . . . . . . . 63,661Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . 58,790Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . 55,721Refractive error . . . . . . . . . . . . . . . . . . . . . . . . . . 51,962
SOURCE U S Department of Health and Human Servlces~ Publlc Health Service, Health Resources and Serwces Adminlstratlon, Indian Health Service, Patient C;eStatistics Staff, Internal document, Rockvdle, MD, Feb 15, 1985
Table 4-18.—Number of Outpatient ClinicalImpressions by Leading Diagnostic Categories
Indian Health Service Facilities:11 IHS Areas, Fiscal Year 1984
Number ofclinical Percent
Diagnostic category impressions of totalSupplementary classification. . . . . . 756,960 20.6Respiratory system diseases. . . . . . . 473,983 12.9Nervous system and sense organ
diseases . . . . . . . . . . . . . . . . . . . . . 457)282 12.4Injuries and poisonings . . . . . . . . . . . 245,526 6.7Diseases of skin and subcutaneous
tissue . . . . . . . . . . . . . . . . . . . . . . . . . 215,625 5.9Pregnancy, childbirth, and
puerperium . . . . . . . . . . . . . . . . . . . . 207,734 5.7Endocrine, nutritional, and
metabolic disorders. . . . . . . . . . . . 202,037 5.5Circulatory system diseases . . . . . . . 199,044 5.4Symptoms and ill-defined
conditions . . . . . . . . . . . . . . . . . . . . . 174,923 4.8Musculoskeletal system diseases . . 172,424 4.7All other . . . . . . . . . . . . . . . . . . . . . . . . 567,951 15.5
Total, all categories . . . . . . . . . . . . 3,673,489 100.0aThis category includes well child care, hospital and medical/surgical followup,
physical examinations, tests (lab and X-ray), socio-economic and environmentalproblems, and “all other” clinical impressions
SOURCE: U S Department of Health and Human Services, Public Health Serwce,Health Resources and Services Administration, Ind!an Health Service,Patient Care Statlst!cs Staff, internal document, Rockville, MD, Feb13, 1985.
need for such services in the Indian population.The need for these services can be inferred fromthe high poverty and unemployment rates dis-cussed in chapter 3, the high mortality rates frompreventable or “social” (101) causes and the widelyheld view that mental health problems are epi-demic among both reservation and urban Indians(121,124,211). Many problems of American In-
dians are related to continuing social and emo-tional stresses: alcohol abuse, accidents, suicide,homicide, teenage pregnancy, and child abuse andneglect (34). Even as social and emotional distur-bances are resulting in higher death rates amongIndians, the high death rate itself leads to addi-tional mental health problems of grief (110). De-spite this need, hospitalizations for mental dis-orders have been declining in the IHS system morerapidly than they have in U.S. non-Federal short-stay hospitals (see figure 4-16), and outpatient en-counters for mental health problems were notamong the leading reasons for IHS outpatientvisits in 1984. Mental health services are gener-ally regarded as relatively unavailable in IHSareas, and alcohol treatment and prevention pro-grams are conceded to not meet the need for themamong the IHS areas (19,76).
Summary
In summary, a global view across IHS areas in-dicates that although there have been substantialimprovements, the health status of Indians con-tinues to lag behind that of U.S. all races popu-lations taken together. Considerable improvementhas been achieved in neonatal health and reduc-ing deaths from accidents, infectious diseases, andtuberculosis. The health of older infants andyoung children, and death from external causes(accidents, homicide, suicide), alcoholism, pneu-monia, and diabetes, remain significant problems.Health status in individual IHS areas is discussedin the following section.

Ch. 4—Health Status of American Indians Ž 109
Table 4-19.—Age Distribution of Outpatient Care IHS Service Areas 1984 and U.S. All Races 1981Compared to Age Distribution in the Population and Age-Specific Mortality Rates
Percent distribution of outpatient visits-.
(by age group) Percent in age groupa
Ratio age-specificIHS U s . Ratio Rat io mortality rate
11 areas all races Indians to Us . Indians to Indians b to U.S.Age group 1984 1981 U.S. all races Indians c all races U.S. all races all racesd
All ages. . . . . . . . . 1OO.OO/O 100,00/’0 100.00/0 100.0 ”/0<15 . . . . . . . . . . . 31.2 18.3 1.7 32.5 22.7 1.4 1.515 to 24. ....., . . 18.3 13.5 1.4 22,5 18,7 1.2 2.725 to 44. . . . . . . . . 25.4 26.6 1.0 26.7 27.8 1.0 4,645 to 64 . . . . . . . . . 16.4 23.3 0.7 13.1 19.7 0.7 1.2>65 . . . . . . . . . . 8.4 18.4 0.5 5.3 11.3 0.5 0.9Unknown. . . . . . . . 0.3 – — — — — —
—aAs of 1980 U.S. CensusbThree year period centered In 1981clndlans , n rese~atlon States, separate calculat Ions are not made for service area I ndl ans‘Calendar year 1981
SOURCES. IHS outpatient data: U S Department of Health and Human Services, Publlc Health Serwce, National Center for Health Statlstfcs, “1981 Summary NationalAmbulatory Medtcal Care Survey, ” Advance Data from Vita/ and Hea/th Stat/st/cs, No 88 (Hyattsv{lle, MD PHS, Mar 16, 1983) U.S. all races outpatient data:U S Department of Health and Human Servlms, Publlc Health Service, Health Resources and Services Admlnlstratlon, Indian Health Service, Office of Plannlng, Evaluation and Legwlatlon, Program Statlstlcs Branch, Summary ot Leading Causes for Outpatient VIsIts, /rid/an F/ea/tb Serwce Fac//it/es F/sea/ Year1984 (Rockvllle, MD IHS, no date)
Table 4-20.—Percent Distribution of Outpatient Visits by Patient Age Group and Area:Indian Health Service Facilities, Fiscal Year 1984
Total Age groups
Area Number Percent <1 1 to 15 15 to 24 25 to 44 45 to 64 >65
Aberdeen . . . . . . . . . . . 410,354 100.0 6.1 27.2a 17,4 24.5b 16.8 8.0Alaska . . . . . . . . . . . . . . 323,097 100.0 7.0 20.3b 19,5a 29.8a 15.5b 7.0b
Albuquerque. . . . . . . . . 302,817 100.0 7.2 24.4 17.9 26.2a 15.0b 8.9Bemidji . . . . . . . . . . . . . 112,356 100,0 4.8b 23.6 15.4b 24,7 20.9a 10.7a
Billings . . . . . . . . . . ....... . . 332,379 100.0 6.2 24.1 18.9 25.8 16.1 7.8Nashville . . . . . . . . . . . . 73,059 100.0 5.6b 27.7a 16.3 24.2b 16.7 9.4a
Navajo . . . . . . . . . . . . . . 698,150 100,0 8.7a 26.2a 19.1a 25,1 14.0b 6.7b
Oklahoma . . . . . . . . . . . 661,217 100.0 5.6b 22.6b 18.8 22.9b 18.2a 11 .8a
Phoenix . . . . . . . . . . . . . 445,770 100.0 8.4a 23.1 19.1a 25,9 16.4 6.7b
Portland . . . . . . . . . . . . 235,924 100.0 6.2 24.8 15.6b 25.7 18.1 9.4a
Tucson . . . . . . . . . . . . . 78,366 100.0 8.7a 22.6b 15.0b 26.5a 19.0a 8.0Total . . . . . . . . . . . . . 3,673,489 100.0 7,0 24.2 18.3 25.4 16.4 8.4
“Are’ W!th one of highest three percentages wlthln age 9rou Pb Area with one of the lowest three percentages wlthln a9e 9rou P
SOURCE U S Department of Health and Human Services, Public Health Service, Health Resources and Services Adm!nlstratlon Indian Health Service Office of Plann I n g, Evaluation, and Leglslatlon, Program Stat! stlcs Branch Summary of Lead(ng Causes for Oufpaf/enf VIs Ifs, /nd(an Health Serv/ce Fac///eses F~sca/ Year1984 (Rockvtlle, M D IHS, no date)

110 • Indian Health Care
Table 4-21 .—Dental Services Required in 12 IHS Areas
Services providedb
Number of Percent requiredServices Tribe services required but not
Area Population required a IHS Contract (638) Total but not providedc providedAberdeen . . . . . . ... . . . . 70,648 500,188 104,490 17,706 25,555 147,751 352,437 70%Alaska ... . . . . . . . . . . . 71,329 505,009 103,249 23,481 67,093 193,823 311,186 62Albuquerque . . . . . . . 51,211 362,574 114,402 34,512 1,410 150,324 212,250 59Bemidji. . . . . . . . . . . . . . . . 47,000 332,760 55,921 29,970 43,778 129,669 203,091 61Billings. ., ... . . . . . . . 40,106 283,951 135,068 8,770 – 143,838 140,113 49California . . . . . . . . . . . . . 71,642 507,226 6,563 119,108 125,671 381,555 75Nashville ... ... . . 35,822 253,620 33,843 12,956 42,380 89,179 164,441 65Navajo . . . . . . . . . . . . . . . 162,005 1,146,995 295,296 39,071 – 334,367 812,628 71Oklahoma . . . . . . . . . . . 190,451 1,348,393 267,704 42,597 11,874 322,175 1,026,218 76Phoenix . . . . . . . . . . . . . 82,309 582,748 136,430 8,769 2,327 149,853 432,895 74Portland .... . . . . . . . . 96,427 682,703 89,448 50,075 15,477 155,000 527,703 77Tucson, ...., . . . . . . . . . 17,852 126,392 12,748 2,520 – 15,268 111,124 88
Area total. . . . . . . . . . . . . . 936,802 6,832,559 1,348,599 276,990 329,002 1,954,918 4,675,641 7 0 %
aEqual tO 11 8 Units required x 60 percent of service ~pulation (IHS, “Findings from an Oral Health Surveyof Native Americans,” internal document, Rockville, M~,Jan 31, 1985)b Do es not inciude se~ices provided in urban programs, some of which may have been provided to IHS se~ice area PopulationcEqual to total services provided subtracted from services required.
SOURCE U.S Department of Health and Human Services, Publlc Health Service, Health Resources and Services Administration, Indian Health Service, Dental ServtcesBranch, tnternal documents, Rockvllle, MD, var!ous dates, 1985
Figure 4-16.— Hospitalizations for Mental DisordersIHS Direct and Contract Hospitals and U.S.Non-Federal Short-Stay Hospitals 1973-1984
1972 1974
Year
aMissing data
SOURCES” 1973.1983 IHS and 1974-1980 and 1882-83 U.S. data: IHS, Patient Statis-tics Branch, Hospital discharge rates, internal documents, January15, 1974 -Feb. 6, 19W; 1984 IHS data: US Department of Health andHuman Services, Public Health Service, Health Resources and Serv-ices Administration, Office of Planning, Evaluation and Legislation,Program Statistics Branch, Patient Care Statistics Staff, Utilizationof /ndiarr Hea/fh Service and Corrtracf f+ospifa/s, Fisca/ Year 1984,internal document, Rockville, MD no date. 1981 U.S. data: US. Depart-ment of Health and Human Services, Public Health Service, Nat Ion.al Center for Health Statistics, “Utilization of Short-Stay HospitalsUnited States, 1981 Annual Summary, ” V~tal and Health Statistics,Series 13, No. 72 DHHS Publication No (PHS) 83-1733 (Hyattsville,MD Public Health Service, August 1983). 1984 U.S. data: U.S Depart-ment of Health and Human Services, Public Health Service, Nation-al Center for Health Statistics, 1984 Summary: iVationa/ HospitalDiscfrarge Survey, Advance Data from Vital and Health S(at/sties, No112, DHHS Publication No (PHS) 85.1250 (Hyattsville, MD: PHS, Sept27, 1985)

AREA-SPECIFIC FINDINGS
Aberdeen Area
Aberdeen is the seventh most populous of theIHS areas, with IHS estimating that the servicepopulation was 70,648 persons in 1984. Aberdeenincludes the four reservation States of NorthDakota, South Dakota, Nebraska, and Iowa, al-though most Indians in the Aberdeen area residein North or South Dakota, States with great ex-tremes of temperature, rough terrain, and few nat-ural resources. Harsh living conditions and limitedsocioeconomic opportunities in the Aberdeen areacontribute to the poor health of Indians.
Although death rates have declined in the Aber-deen area in the past decade, and the pattern ofcauses has changed somewhat (see table 4-22),Aberdeen continues to have the highest mortal-ity rate of IHS areas. The age-adjusted mortalityrate in Aberdeen for the 3-year period centeredin 1981 (1,261.3 per 100,000 population) exceededthat of the U.S. all races population by more than200 percent. The rate for females was 2.3 timesthat of U.S. all races females, and for males, 2.1times that of U.S. all races males. Current hospi-talization rates for Aberdeen (2,199.4 per 10,000
C/T, 4—Health Status of American Indians ● 111
IHS eligible population (195)) also exceed thoseof U.S. all races (203), although there are diag-nostic categories for which hospitalization ratesare lower for the Aberdeen population.
For all but one of the 15 leading causes of death(malignant neoplasms among males), mortalityrates were higher in the Aberdeen area than theywere for the U.S. all races population (table 4-23). The 15 leading causes of death among Aber-deen females were diseases of the heart, malig-nant neoplasms, accidents, liver disease, cerebro-vascular disease, diabetes, pneumonia, homicide,conditions arising in the perinatal period, nephritisand other diseases of the urinary tract, suicide,congenital anomalies, tuberculosis, septicemia,and “all other external causes. ” Among Aberdeenmales, diseases of the heart were the leading causeof death, followed by accidents, malignant neo-plasms, liver disease, suicide, homicide, pneumo-nia, conditions arising in the perinatal period,cerebrovascular disease, diabetes, “all other ex-ternal causes, ” chronic pulmonary diseases, ne-phritis and other diseases of the urinary tract,congenital anomalies, and other diseases of thearteries, arterioles, and capillaries. Thus, what are
Table 4.22.–Changes in Crude Death Rates, 1972.82:IHS Aberdeen Area (rates per 100,000 population)
PercentIHS 1972-74 1975-77 1980-82 changeCode Cause rate rate rate 1972-82
790 Accidents/adverse effects . . . . . . . . . 252.3 231.7 158.4 –37.2800 Motor vehicle . . . . . . . . . . . . . . . . . . 134.0 135.4 101.5 –24.2810 All other accidents . . . . . . . . . . . . . 118.3 96.2 56.9 –51 .9310 Diseases of the heart . . . . . . . . . . . . . 218.9 211.4 192,8 – 11.9150 Malignant neoplasms . . . . . . . . . . . . . 96.5 80.3 99.0 2.5620 Liver disease/cirrhosis . . . . . . . . . . . 67,3 71.1 61.0 –9.3510 Pneumonia/influenza. . . . . . . . . . . . . . 64.6 55.2 39,0 – 39.7740 Conditions arising in
perinatal period . . . . . . . . . . . . . . . . . . 50.3 47.8 31.8 – 36.8430 Cerebrovascular disease . . . . . . . . . . 42.8 41.0 36.4 – 15.0260 Diabetes mellitus . . . . . . . . . . . . . . . . 32.6 31.8 28.7 – 11,9830 Homicide . . . . . . . . . . . . . . . . . . . . . . . 27.8 36.1 37.4 34.6820 Suicide . . . . . . . . . . . . . . . . . . . . . . . . . 23.1 28.1 32.8 42.0
All other causes . . . . . . . . . . . . . . . . . 247.8 275.5 174.6 – 29.5ALL All causes . . . . . . . . . . . . . . . . . . . . . . 1,124.0 1,110.0 945.9 – 15.8SOURCES 1972.74 and 1975-77 deaths: U S Department of Health, Education and Welfare, Publlc Health Service, Health Serwces
Admlnlstratlon, Indian Health Service, Se/ecfed V/fa/ Sfat/st/cs for /rrdfan Health Serwce Areas and Serwce Un~fs,1972 to 1977, DHEW Pub No (H SA).79-1 005 (Rockwlle, MD HSA, 1979). 1972.74 and 1975-68 population: U S Depart.ment of Health and Human Sew!ces, Publlc Health Service, Health Resources and Services Administration, IndianHealth Serwce, Program Statistics Branch, Internal documents, Rockville, MD, 1985 1980-82 data: U S Departmentof Health and Human Services, Publlc Health Serwce, Health Resources and Services Administration, Indian HealthService, computer tape supplied to the Office of Technology Assessment, Washington, DC, 1985

112 • Indian Health Care —
Table 4-23.—Fifteen Leading Causes of Deaths and Age-Adjusted Death Rates forAberdeen IHS Area Indians 1980-82 and U.S. All Races 1981
—
IHS Number Age-adjusted mortality rateRatio of Aberdeen
area Indians tocode Rank Cause name of deaths Indians U.S. all races U.S. all races —Females:310 1.150 2.790 3.620 4.430 5.260 6.510 7.830 8.740 9.640 10.820 11.730 12.030 13.090 14.840 15.
ALL . . . .
Males:310 1.790 2.150 3.620 4.820 5.830 6.510 7.740 8.430 9.260 10.840 11.540 12.670 13.730 14.490 15.
ALL . . . .
Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . . .Accidents/adverse effects. . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . .Cerebrovascular disease . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Pneumonidinfluenza . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Perinatal conditions . . . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . .Suicide ., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other external causes . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Ail causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Accidents/adverse effects . . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .Cerebrovascular disease . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .All other external causes . . . . . . . . . . . . . . . . . . .Chronic pulmonary disease . . . . . . . . . . . . . . . . .Renal failure, etc. . . . . . . . . . . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .Other artery diseases . . . . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
136100975639322922201710
9776
160747
240212
936354514742322420181012
9171
1.098
181.5149.3108.086.348.947.933.427.111.225.511.55.6
10.08.55.7
193.8954.2
414.7263.4159.8113.465.064.965.324.852.341.429.629.917.0
7.114.8
249.61,613.0
135.1108.620.4
35.49.69.24.38.23.65.75.50.42.40.9
63.7420.4
271.260.2
163.716.018.016.716.610.341.710.02.2
26.24.96.18.5
81.0753.3
1.31.45.3
11.71.45.03.66.31.47.12.01.0
25.13.56.33.02,3
1.54.41.07.13.63.93.92.41.34.1
13.41.13.51.21.73.12.1
SOURCES U.S. allraces: US. Department of Health and Human Resources, Publ!c Health Service, National CenterforHealth Statistics, “AdvanceReport, Final Morfal~tyStatlstics, 1981,’’ &forrthly Vifa/Statisf/cs r?eport 33(3) supp., June 22, 1984; Indiansin IHSareas:U.S Departmentof Health and Human Services, Publ{cHealth Service, Health Resources and Services Administration, Indtan Health Service, computer tape supplled to the Office of Technology Assessment,Washington, DC, 1985
widely believed to be preventable causes of mor- older Indians. The Aberdeen Indian death ratetality predominate among both male and female from heart disease begins to exceed that of U.S.Indians in Aberdeen. all races for the 15 to 24 year age bracket, and
exceeds the U.S. rate for all subsequent age groupsAlthough deaths from diseases of the heart and (table4-24) Cerebrovascular disease is also a lead-
the circulatory system are generally lower among ing cause of death among Aberdeen Indians, oc-Indians than among other U.S, populations, they curring at 1.4 times the U.S. all races rate for fe-are slightly higher among Aberdeen area Indians males, and 1.3 times the U.S. all races rate forof both sexes than among the U.S. all races pop- males, The Aberdeen area hospitalization rate forulation, despite a 12-percent decline in the Aber- circulatory system diseases, however, is substan-deen death rate from heart disease since the 1972 tially lower than that in U.S. non-Federal short-to 1973 period. When deaths from both sexes are stay hospitals. The low hospitalization rate can-combined, diseases of the heart are the leading not be explained fully by the relatively young In-cause of death among Aberdeen area Indians. In dian population, because younger Aberdeen areaAberdeen, diseases of the heart are not limited to Indians have a high heart disease death rate. One-

Ch. 4—Health Status of American Indians ● 113.
Table 4-24.— Heart Disease Mortality by AgeIHS Aberdeen Area Indians 1980-82 and
U.S. All Races 1981 (rate per 100,000 population)
Mortality rate – Ratio Aberdeen– IHS Aberdeen Us . area Indians to
Age group area Indians all races U.S. all races
0 to 4 . . . . . . . 7,2 106. 1 0.15 to 14 . . . . . . — 0.9 —
15 to 24 . . . . . 11.5 2.6 4.425 to 34 ...., 18.4 8.4 2.235 to 44. , . . 143,4 43,2 3.345 to 54 . . . . . . 358.1 177.7 2.055 to 64 . . . . . . 846.4 481.5 1.865 to 74 . . . . . . 1,692.4 1,175,8 1.475 to 84 .., . 2,955.1 2,850.3 1.0>85 . . . . . . . . 7,265.0 7,459.0 1.0SOURCES Indian data: U S Department of Health and Human Services, Public
Health Service, Health Resources and Services Admlnlstratlon, Indl.an Health Service, computer tape supplied to the Off Ice of Technology Assessment Washington, DC 1985 U.S. all races data: U SDepartment of Health and Human Services Public Health ServiceNational Center for Health Statlstlcs, Advance Report of Final Mor.tahty Statlstlcs 1981 , Mofrfhly V/ta/ Statistics Report 33(3) suppJune 22 1984
third of female deaths and one-half of male deathsfrom heart disease in Aberdeen area Indians arecaused by acute myocardial infarction, indicat-ing that medical care is often not obtained in timeto save the victim.
Although the Aberdeen area death rate fromaccidents has declined almost 40 percent since theearly 1970s, accidents, particularly motor vehi-cle accidents, remain the leading cause of deathfor Aberdeen males. Furthermore, the death ratefrom accidents for female Indians in Aberdeen farexceeds that of U.S. all races females, and Aber-deen, with Alaska, has the second highest (afterthe Billings area) accidental death rate for femalesof all IHS areas. Deaths from causes other thanmotor vehicle accidents account for most of thedecline in mortality since the early 1970s.
Aberdeen has the second highest rate of suicideamong IHS areas for both males and females. Fur-thermore, the Aberdeen suicide rate increased 42percent in the decade for which data are avail-able. Age-specific information is not available forearlier periods, but as shown in table 4-25, com-pared to other U.S. populations in 1980 to 1982,suicide in Aberdeen was a problem of youngerIndians. As in the United States generally, therewere more suicides among men (160). Althoughthe Aberdeen female rate was much lower thanthat for Aberdeen males, it was still double thatof U.S. all races and U.S. white females (201).
Age
Table 4.25.—Suicide Mortality by AgeIHS Aberdeen Area Indians 1980.82 and U.S.All Races 1981 (rate per 100,000 population)
Mortality rate Ratio AberdeenIHS Aberdeen Us. area Indians to
Group area Indians all races U.S. all races
0 to 4, . . . . . — — —5 to 14 . . . . . . 2.0 0.5 4.0
15 to 24. , . . . 59.6 12.3 4.825 to 34 . . . . . . 80.9 16.3 5.035 to 44 . . . , 53,8 15.9 3.445 to 54, ... . 53.8 16.1 3.355 to 64 .., . . 22,0 16.4 1,365 to 74 . . . . . . – 16.2 —75 to 84 . . . . . . — 18,6 —>85 . . . . . — 17,7 —
SOURCES Indian data:U S Dep;tment of Health and Human Se;!ces Publ;cHealth Service Health Resources and Services Admln!strahon, Indlan Health Service, computer tape supplled to the Off Ice of Technology Assessment, Washington, DC 1985 U.S. ail races data: U SDepartment of Health and Human Services Publ!c Health ServiceNational Center for Health Statistics, “Advance Report of Final Mortallty Statistics 1 9 8 1 Monthly V(ta/ Sfalwf/cs Reporf 33(3) suppJune 22 1984
In addition to having substantial numbers ofdeaths due to accidents and suicides, the Aber-deen area had the highest rate of deaths by homi-cide of all IHS areas for both males and females.In 1980 to 1982, deaths by homicide among Aber-deen men exceeded that of U.S. all races men bya ratio of 3.9; for women the comparable ratiowas even greater, 6,3. As it has for suicide, thehomicide rate increased by one-third between1972 and 1982.
Deaths due to “ail other external causes” (e.g.,substance abuse, injury by firearms) were alsohigh in the Aberdeen area, particularly for males.These were the 11th leading cause of death inAberdeen, compared to being the 15th leadingcause of death for both sexes for all IHS areas.
Violence contributes substantially to illness andinjury as well. Injuries and poisonings were thesecond leading reason for hospitalization in theAberdeen area. At a rate of 297.0 per 10,000 pop-ulation, it was almost twice that of patients of allraces in U.S. non-Federal short-stay hospitals. Theserious nature of many of the injuries in Aber-deen is reflected in the greater proportion of pa-tients sent outside of the IHS direct system forcontract care: in 1984, 17.6 percent of inpatienttreatment for injuries and poisonings was handledby Aberdeen contract general hospitals, comparedto 15.1 percent for all IHS areas (201). Further-

774 ● Indian Health Care
more, almost 8 percent of outpatient visits bymales (12,816 visits) in fiscal year 1984 were forlacerations and open wounds; dislocations, sprainsand strains; and superficial injuries and contusions(table 4-26).
Cancer is the third leading cause of death in theAberdeen area. (As for the general U.S. popula-tion, the cancer mortality rate for Indians in theAberdeen area remained about level during the1972-82 period. ) Cancer mortality in Aberdeenarea Indians differs somewhat by sex, For Indianwomen the mortality rate from all malignant neo-plasms exceeded the rate for U.S. all races femalesby a ratio of 1.4. While the overall cancer death
rate for Indian men in Aberdeen (159.8 per 100,000population) exceeded that of other IHS areas onaverage (98.5 per 100,000 population), it wasslightly below the rate for U.S. all races m e n
(163.7). However, the age-adjusted rate for Aber-deen males exceeded that of U.S. all races men
for cancers of the digestive system (1.8 ratio).Aberdeen cancer deaths also differ from those ofU.S. all races in that rates were generally higherin both the youngest age group (O to 4 years) andthe age groups after 34 years of age, although age-specific differences varied somewhat by cause.
The rate of hospital discharges for malignantneoplasms among Aberdeen Indians was about
Table 4-26.–Fifteen Most Frequent Outpatient Diagnoses:a Aberdeen Area, Fiscal Year 1984
Percent ofNumber of total visits
Rank Code Clinical impressions visits by sex —Female:
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.Male:
1.2.3.4.5.6.
7.8.9.
10.11.12.13.14.15.
300080819480250283818301812400510823575821827
300819250080283818730301821702731812575820510
ALL
Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Prenatal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well-child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pharyngitis and tonsillitis (non-strep) . . . . . . . . . . . . . . . . . . . . . . . . . .Other ill-defined, undiagnosed diseases . . . . . . . . . . . . . . . . . . . . . . . .Urinary tract infection. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Eczema, urticaria or skin allergy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tests only (laboratory and X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other muskuloskeletal, connective tissue disease . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well-child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Laceration, open wound . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pharyngitis and tonsillitis (non-strep) . . . . . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Dislocations, sprains, and strains . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Superficial injury or contusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other ill-defined, undiagnosed diseases . . . . . . . . . . . . . . . . . . . . . . . .Other musculoskeletal, connective tissue diseases . . . . . . . . . . . . . .Hospital medical/surgical followup . . . . . . . . . . . . . . . . . . . . . . . . . . . .Eczema, urticaria, or skin allergy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
All other causes, both sexes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
17,85515,99213,77012,4478,1627,8426,4726,1025,2254,8114,7154,6694,2254,0534,915
12,2908,9747,8427,7366,7616,3635,6304,2764,1613,7603,4263,1712,9932,9512,837
205,928410,354
7.36.65.65.13.33.22.72,52.12.01.91.91.71.71.9
7.65.64.94.84.24.03.52.72.62.32.12.01.91.81.8
100.0aTh e IHS refers t. these as ctinical impressions, because they are recorded before a clinical diagnosis is completed, therefore, they may not be valid.
SOURCES: 15 Ieadlng clinical lmpr8s8ions: US. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, lndi.an Health Service, “Special Report on 15 Leading Causes of Outpatient Care By Area and Service Unit, State and County, ” internal document, Albuquerque,NM, 1985. Aberdean total: U.S Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, IndianHealth Service, Office of Planning, Evaluation and Legislation, Program Statistics Branch, Summary of Leading Causes for Outpatient Visits, Indian F/ea/thSendce Faci/if/es, Fiscal Year 1984 (Rockville, MD: IHS, no date).

.
one-third that of U.S. all races in non-Federalshort-stay hospitals (see table 4-19). Cancer wasalso not among the 15 leading reasons for Aber-deen outpatient visits. These findings again indi-cate that medical care for cancer is relatively de-ficient.
The extent of the diabetes problem in Aberdeenis difficult to deduce from available mortality andmorbidity information. Although it is still abovethe national rate, the diabetes death rate in Aber-deen has declined over time and has decreased inimportance as a leading cause of death. Diabeteswas the 10th leading cause of death in 1980 to1982, compared to its being the 8th leading causeof deaths in 1972 to 1974 and the 9th leading causein 1975 to 1977. However, the diabetes death ratesin Aberdeen still exceeded the U.S. all races ratefor females by 5:1 and for males by 4:1, althoughthe absolute number of deaths attributed to dia-betes in Aberdeen was small. However, the deathrate from renal failure increased, exceeding theU.S. all races rates by 7.9 for females and 3.5 formales. A continuing problem with diabetes andits effects is reflected in the rate of health care uti-lization for diabetes. Hospital discharge rates inAberdeen for diabetes was 60 per 10,000 popula-tion in 1984, compared to 25.3 per 10,000 popu-lation for U.S. all races. Diabetes was also a lead-ing cause of outpatient visits for both male andfemale Aberdeen Indians, accounting for 4.8 per-cent (7,736) of male visits (fourth leading cause)and 6.6 percent (15,992) of female visits in 1984(second leading cause). Based on the high ratesof care for diabetes, it seems unusual that visionproblems were not among the 15 leading causesof outpatient visits.
Pneumonia and upper respiratory system dis-eases were also significant problems in Aberdeen,with Aberdeen Indians dying and being hospi-talized at rates more than three times that of U.S.all races populations with pneumonia. Chronicpulmonary disease was a less likely cause of death,but upper respiratory infections including thecommon cold, pharyngitis and tonsillitis, andacute otitis media predominated as causes of out-patient visits. Hospitalizations for otitis mediawere common in the Aberdeen area, which hadthe second highest rate of IHS areas, and exceeded
Ch. 4—Health Status of American Indians • 115
the rate for U.S. non-Federal short-stay hospitalsby more than 2:1.
In 1980 to 1982, Aberdeen’s neonatal death rateexceeded that of U.S. all races by a ratio of 1.3.The postneonatal death rate for Aberdeen Indianswas 11.4 per 1,000 live births, compared to 3.9for U.S. all races, a ratio of 2.9. The leading causeof neonatal deaths was prematurity and/or lowbirth weight, and the leading cause of death forAberdeen postneonates was sudden infant deathsyndrome, which occurred at a rate 1.8 times thatof U.S. all races in 1981 (table 4-27).
The contribution of alcohol use to most causesof mortality and morbidity in the Aberdeen areacannot be quantified. However, chronic liver dis-ease and cirrhosis, which is related to alcoholabuse, ranked fourth as a cause of death amongAberdeen Indians in 1980 to 1982, as it has sinceat least 1972. Aberdeen deaths from liver diseaseand cirrhosis were 8.7 times the U.S. all races ratefor both sexes (11.7 for females and 7.1 times formales), although Aberdeen was not the highestof all IHS areas, Correspondingly, the Aberdeenarea had a slightly higher rate of hospitalizationsfor alcoholic liver disease (5.9) than did IHS areasas a whole (4.4). Hospitalization for alcohol de-pendence syndrome in Aberdeen was 6.1 timesthe rate of U.S. non-Federal short-stay hospitals,which was the highest among IHS areas, but thiswas influenced by the fact that Aberdeen has oneof only two psychiatric wards in the IHS system.(Aberdeen has 9 psychiatric beds and the IHS hos-pital in Gallup has 13. )
Aberdeen patient care statistics also indicatehigh rates of health care utilization for chronicinfectious diseases and conditions. Hospitaliza-tions for infectious and parasitic diseases werecommon among Aberdeen Indians relative to U.S.all races populations, as were outpatient visits forthe skin diseases eczema and urticaria, urinarytract infections among women, and musculoskele-tal and connective tissue disorders.
In summary, for almost all diseases and causesof death, Indians in the Aberdeen area were inpoor health compared to other U.S. populationsand to other Indians.

116 ● Indian Health Care
Table 4-27.—infant Deaths and Death Rates IHS Aberdeen Area, 1980.82
IHS Deaths Rates (per 1,000 live births)
c o d ea C a u s e Total Neonates Postneonates Total Neonates Postneonates
010040120130140150
170180200220230240380
580590600610650680ALL
Intestinal infection . . . . . . . . . . . 1Septicemia . . . . . . . . . . . . . . . . . . 2Blood diseases . . . . . . . . . . . . . . 1Meningitis . . . . . . . . . . . . . . . . . . . 2Other nervous diseases . . . . . . . 1Acute upper respiratoryinfection . . . . . . . . . . . . . . . . . . . . 2Pneumonia/influenza . . . . . . . . . . 8
Pneumonia . . . . . . . . . . . . . . . . 8Other respiratory diseases . . . . . 2Gastritis, etc. . . . . . . . . . . . . . . . . 1Other digestive . . . . . . . . . . . . . . 3Congenital anomalies . . . . . . . . . 17Conditions arising inperinatal period . . . . . . . . . . . . . . 62Symptoms/signs/other . . . . . . . . 47
SIBS. . . . . . . . . . . . . . . . . . . . . . 39Symptoms/signs/other . . . . . . 8
Accidents/adverse effects . . . . . 6Homicide . . . . . . . . . . . . . . . . . . . 1All other causes . . . . . . . . . . . . . 6All . . . . . . . . . . . . . . . . . . . . . . . . . 162
—————
——————
10
605411
——
76
12121
2882137
24235
7516
86
0.10.30.10.30.1
0.31.11.10.30.10.42.3
8.36.35.21.10.30.10.8
21.7
—————
——————1.3
8.00.70.50.10.1——
10.2
0.10.30.10.30.1
0.31.11.10.30.10.40.9
0.35.64.70.90.10.10.8
11.5alHs ~~de, equivalence to ICD-9 Recode 61 for infant deaths available from IHS
—
SOURCE U.S Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Indian Health Service, computer tapesuppl!ed to the Office of Technology Assessment, Washington, DC, 1985
Alaska Area
Eskimos, Aleuts, and Indians in the entire Stateof Alaska are served by the Alaska area, a popu-lation estimated to be 71,329 in 1984.
Alaska shows many of the same mortality pat-terns as do other Indian areas, particularly thosein the Central and North Central Western con-tinental States, but it is unusual in several aspects;notably, accidents, liver disease, cancers of thedigestive system, and diabetes. Morbidity data aredifficult to interpret, because information is notcollected from one tribally administered hospitaland a number of tribally administered healthcenters.
The Alaska overall crude mortality rate de-creased an estimated 8.1 percent from 1972 to1982. In 1980 to 1982 the age-adjusted mortalityrate in Alaska exceeded that of U.S. all races by1.6 (see table 4-28).
As for almost all IHS areas, the most commoncause of death in Alaska was accidents. Alaskadiffers from most other IHS areas, however, inthat accidents were the leading cause of death forfemales as well as males, and many of the deaths
caused by accidents were not caused by motor ve-hicles. Accidents were responsible for 17 percentof female deaths in 1980 to 1982, at a rate 4.8times that of U.S. all races females, and for almosta third of male deaths (299 of 957), at a rate 5.3times that of U.S. all races males, While Alaska’smortality rate from accidents declined between1972 and 1982 (see table 4-29), most of the changehas been in the motor vehicle rate, and the over-all decline has not been as great as it has for mostother IHS areas.
As they are in almost all IHS areas, Alaskadeath rates from other forms of “social” mortal-ity were higher than U.S. all races rates. Alaskais an interesting area to watch because of signifi-cant social and economic changes in the last sev-eral years. The mortality rate from homicides hasfluctuated since 1972, resulting in a total increaseof 19.4 percent compared to a U.S. average in-crease of 4 percent (142,143). By contrast, therehas been an average decline for all IHS areas of16.8 percent. The Alaska crude mortality ratefrom suicide declined between 1972 to 1982, asdid that of IHS areas on average, while the U.S.crude rate remained stable (142,143). In 1980 to1982, the age-adjusted homicide and suicide rates

—- —
Ch. 4—Health Status of American Indians ● 117
Table 4-28.—Fifteen Leading Causes of Deaths and Age-Adjusted Death Rates for Alaska IHS Area Indians 1980-82and U.S. All Races 1981
Ratio of AlaskaIHS Number Age-adjusted mortality rate area Indians tocodea Rank Cause name of deaths Indians U.S. all races U.S. all racesFemales:790 1.310 2.150 3.430 4.510 5.620 6.830 7.740 8.840 9.030 10.640 11.730 12.820 13.540 14.090 15.
ALL ...
Males:
790 1.310 2.150 3.430 4.820 5.830 6.510 7.740 8.840 9.620 10.540 11.730 12.030 13.140 14.260 15.
ALL . . . .
Accidents/adverse effects. . . . . . . . . . . . . . . . . . .Diseases of the heart . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period ., . . . . . .All other external causes . . . . . . . . . . . . . . . . . . .Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . .Congenital anomalies ., . . . . . . . . . . . . . . . . . . .Suicide ... , . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Accidents/adverse effects. . . . . . . . . . . . . . . .Diseases of the heart . . . . . . . . . . . . . . . . . .Malifnant neoplasms . . . . . . . . . . . . . . . . . . . . . . .Cerebrovascular disease. . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .All other external causes . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . .Chronic pulmonary disease . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . .Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other infectious/parasitic diseases . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . .All others. ..., . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
88826726262016149888875
116508
299145115373433322927171411
544
151957
97.7122.299,938.333,228.518.210.1
7,612.812.75.87,5
11.27,0
149.1661.8
319.6206.9175.152,434.832.437.620,329.525.816,6
7.77.36.65.3
212.01,164.4
20.4135.1108.635.4
9.27.44.38.20.90.43.65.55.79.52.4
63.8420.4
60.2271.2163,741.718.016.716.610.32.2
16.026.2
6.11.01.7
10.091.6
753.3
4,80.90.91.13.63.94.21.28.5
32.03.51.11.31.22.9
55.81.6
5.30.81.11.31.91.92.32.0
13.41.60.61.37.33.90.5
44.21.5
aEqulvalence to ICD-9 Codes avallabel frOm IHS
SOURCES” U.S. all races: US. Department of Fiealth and Human Resources, Publlc Health Service, National CenterforHealth Statlstlcs. ’’Advance Report, Final Mortall-tyStatisttcs, 1981,’’ Month/y V/tal Statistics Ffeporf 33(3) supp, June 22, 1984, 1nd~ansln IHSareas:US Deparfrnent of Health and Humar?Servlces, PubhcHealth Service, Health Resources and Services Administration, Indian Health Service, computer tape supplied to the Office of Technology Assessment,Washington, DC, 1985
for Alaska males were both 1.9 times that of U.S. IHS average of 151 per 10,000 population. Theall races males, making suicide and homicide the high rate of accidents and injuries among Alaskafifth and sixth leading causes of death for Alaska males also can be inferred from outpatient statis-area males. tics. In fiscal year 1984, diagnoses related to
It is unusual for the rate of hospitalizations inviolence (laceration, open wound; dislocations,sprains, and strains; fracture of an extremity) ac-
an IHS area to exceed the rate for U.S. non-Federal short-stay hospitals (see discussion of
counted for 7.4 percent, and 3 of the 15 leadingcauses, of male outpatient visits (see table 4-30).
other areas), but in fiscal year 1984 Alaska Na-tives were hospitalized for injuries and poisonings Heart disease was the second leading cause ofat a rate of 240 per 10,000 population, well above death in Alaska, but it did not exceed the U.S.the U.S. all races average of 148.1 (203), and the all races rate for either male or female Alaska Na-

118 ● Indian Health Care
Table 4-29.—Changes in Crude Death Rates, 1972-82:IHS Alaska Area (rate per 100,000 population)
PercentIHS 1972-74 1975-77 1980-82 changeCode Cause rate rate rate 1972-82790 Accidents/adverse effects . . . . . . . . . 231.6 220.6 196,1 –8.2800 Motor vehicle accidents . . . . . . . . . 30.6 45.6 26.4 – 13.9810 All other accidents . . . . . . . . . . . . . 183.0 175.0 169.8 –7.2310 Diseases of the heart . . . . . . . . . . . . . 100.4 95.8 115.1 14.6150 Malignant neoplasm . . . . . . . . . . . . . . 91.2 87.8 92.2 1.1430 Cerebrovascular disease . . . . . . . . . . 39.1 29.0 31.9 – 18.3510 Pneumonia/influenza. . . . . . . . . . . . . . 38.5 34.7 29.4 –23.6280 Diabetes mellitus . . . . . . . . . . . . . . . . 2.0740 Conditions arising in
perinatal period . . . . . . . . . . . . . . . . 33.0 26.8 21.8 –34.0820 Suicide . . . . . . . . . . . . . . . . . . . . . . . . . 30.0 43.9 21.3 –29.0830 Homicide . . . . . . . . . . . . . . . . . . . . . . . 20.8 26.2 24.8 19.4620 Liver disease/cirrhosis . . . . . . . . . . . . 16,5 27.3 18.8 13.6730 Congenital anomalies . . . . . . . . . . . . . 11.0 10.8 9.6 – 12.5
All other causes . . . . . . . . . . . . . . . . . 194.9 187.4 179.5 – 7.9ALL All causes . . . . . . . . . . . . . . . . . . . . . . . 807.6 790.3 742.5 –8.1SOURCES 1972-74 and 1975-77 deaths: U.S Department of Health, Education and Welfare, Publlc Health Service, Health Ser’wces
Administration, Indian Health Service, Selected Vita/ Statistics for /rrdian Health Sewice Areas and Sewice Units,1972 to 1977, DHEW Pub. No. (HSA)-79-1OO5 (Rockville, MD” tiSA, 1979). 1972.74 and 1975-88 population: U S.Department of Health and Human Services, Public Health Service, Health Resources and Services Administration,Indian Health Service, Program Statistics Branch, internal documents, Rockville, MD, 1985. 1980-82 data: U.SDepartment of Health and Human Services, Public Health Service, Health Resources and Services Administration,Indian Health Service, computer tape supplied to the Office of Technology Assessment, Washington, DC, 1985.
tives. However, mortality from heart disease hasincreased since 1972, from a crude rate of 100.4per 100,000 population to 115.1 in the 1980 to1982 period, so it is a disease of increasing con-cern to Alaska Natives. The increased concernwith heart disease and continuing concern withcerebrovascular disease are reflected in an increasein hospitalizations for circulatory system diseases,from 3.5 percent of all diagnoses in 1979 to 4.4percent in 1984 (excluding Norton Sound), but the1984 rate (74.7 per 10,000 population in 1984, ex-cluding the Norton Sound service unit populationfrom the denominator) was still far below the U.S.all races rate of 238.6 per 10,000 population.
Malignant neoplasms (cancers) were the thirdleading cause of death for Alaska Native malesand females (67 females and 115 males in the 3-year period, 1980-82). Occurring at a rate aboutequal to that of U.S. all races males and females.The exception was cancers of the digestive sys-tem, for which the rate was about twice that ofthe U.S. all races rate, probably as a consequenceof an epidemic of hepatitis resulting in hepatocel-lular cancer (1,160). A greater proportion ofAlaska hospitalizations was accounted for bymalignant neoplasms than in the IHS system onaverage (2.6 percent of discharges in Alaska v.
1.5 percent of discharges on average (195)), al-
though the rate per 10,000 population for Alaska(44.1) was almost half that of U.S. non-Federalshort-stay hospitals (203).
Respiratory system diseases are a significantproblem for Alaska Natives. Pneumonia con-tinues to be a leading cause of death for both maleand female Alaska Natives, exceeding the U.S. allraces rate by more than 2:1. The Alaska Nativedeath rate from pneumonia and influenza did notdecline as much as it did for Indians in other IHSservice areas (a 23.6-percent decline in Alaska v.a 42.6-percent decline on average). In 1984 up-per respiratory infections accounted for 8.7 per-cent of outpatient visits among males and 3.6 per-cent among females. Otitis media alone accountedfor another 8.8 percent of male, and 5.4 percentof female, outpatient visits, making it the lead-ing cause of outpatient visits for males, and thethird leading cause of outpatient visits for females.Alaska’s hospitalization rate for otitis media wasfive times the rate of U.S. non-Federal short-stayhospitals.
Alaska’s high infant mortality rate of 17.3deaths per 1,000 live births was due primarily tohigh postneonatal mortality. As in all other IHS

Ch. 4—Health Status of American Indians • 119
Rank
Female:1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.Male:
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
Table 4.30.—Fifteen Most Frequent Outpatient Diagnoses: Alaska Area, Fiscal Year 1984
IHSCode
480251820300819283301823450210821400818810827
251820300730818821283301310702819823701810827
A L L
Clinical impressions
Prenatal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Chronic otitis media with or without mastoiditis . . . . . . . . . . . . . . . .Hospital medical/surgical followup . . . . . . . . . . . . . . . . . . . . . . . . . . . .Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pharyngitis and tonsillitis (nonstrep) . . . . . . . . . . . . . . . . . . . . . . . . . . .Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Infection of female genitalia (excluding VD) . . . . . . . . . . . . . . . . . . . .Refractive error . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Urinary tract infection. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other symptoms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Chronic otitis media with or without mastoiditis . . . . . . . . . . . . . . . .Hospital medical/surgical followup . . . . . . . . . . . . . . . . . . . . . . . . . . . .Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Laceration or open wound. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pharyngitis and tonsillitis (nonstrep) . . . . . . . . . . . . . . . . . . . . . . . . . . .All other respiratory diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Dislocations, sprains, and strains . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Fracture of extremtiy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other symptoms.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Percent ofNumber of total visits
visits by sex
16,62610,2357,5396,6975,5904,5104,1054,0943,8393,6183,5073,4733,3695,037
10,507
10,2155,0524,9183,9623,5162,8712,7562,6452,5432,4802,3702,3152,2553,4806,467
172,506323,097
8.85.44.03.63.02.42.22.22.01.91.91.81.82.75.6
8.84.34.23.43.02.52.42.32.22.12.02.01.93.08.8
All other causes, both sexes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
alHS refers to the as clinical impressions because they are recorded before a clinical diagnsis is completed, therefore, they may not be valid diagnoses100.0
SOURCES 151eadlngclinical impresaions:US Department of Health and Human Services, Public Health Service, Health Resourcesand Services Administration, lndi-an Health Sewlce, “Special Reporfon 15 Leading Causes of Outpatient Care By Areaand Service Unit, State and County, “ internal document, Albuquerque,NM, 1985.Alaskatotal US Department of Health and Human Services, Pubhc Health Service, Health Resources and Semices Administration, Indian HealthService, Offlceof Planning, Evaluation and Legislation, Program Statistics Branch, Surnrnary ofLeading Cawes forOutpatient Visits, /rrdiarr Hea/th ServiceFactifties, F/sea/ Year 1984 (Rockville, MD IHS, no date)
areas, sudden infant death syndrome contributedmost to the postneonatal death rate, but pneumo-nia was also a leading cause of death for Alaskainfants, particularly postneonates (see table 4-31).Some Alaska area hospitalizations for causes re-lated to infant mortality have declined in the re-cent past, but they were still high relative to ratesfor U.S. all races. In 1979, the Alaska dischargerate for congenital anomalies was 18 per l0,000population. In 1984 it was 15.2 per 10,000 popu-lation, compared to a U.S. non-Federal short-stayhospital discharge rate of 13.5. For conditions aris-ing in the perinatal period, the 1979 hospital dis-charge rate in Alaska was 14.1 per l0,000 popu-lation; in 1984 the Alaska rate (excluding Norton
Sound) was a striking 38.2, 5.4 times the U.S. allraces rate of 7.1, although this high hospitaliza-tion rate was at least partially due to a need tohospitalize because of hazardous weather, road,and flight conditions. (The overall rate of hos-vitalizations and the average length of stay arehigher for Alaska IHS direct and contract facil-ities than for both the IHS and the U.S. average. )Alaska ranks second among IHS areas in the num-ber of visits for prenatal care.
The Alaska area is unusual in that it has a verylow diabetes mortality rate, only four Indians(males) having died from this disease in the 1980-82 period. Similarly, diabetes was not among the

120 ● Indian Health Care
Table 4.-31.— Infant Deaths and Death Rates IHS Alaska Area, 1980-82
IHS Deaths Rates (per 1,000 Iive births)c o d ea C a u s e Total Neonates Postneonates Total Neonates Postneonates040 Septicemia 1 — 1 0.1 0.1050 Viral diseases.. . . . . . . . . . . . . . .
—1 — 1 0.1 0.1
130 Meningitis . . . . . . . . . . . . . . . . . . . 3—
— 3 0.4 0.4140 Other nervous diseases . . . . . . . 4
—— 4 0.6 0.6
160 Bronchitis . . . . . . . . . . . . . . . . . . .—
— 1 0.1 0.1170 Pneumonia/influenza, . . . . . . . . .
—1 1 7 1.2 0.1 1.0
180 Pneumonia . . . . . . . . . . . . . . . . 8 1 7240
0.1 1.0Congenital anomalies . . . . . . . . . 17 13 4 2.5 1.9
3800.6
Conditions arising inperinatal period . . . . . . . . . . . . . . 42 42 — 6.1 6.1
580 Symptoms/signs/other . . . . . . . . 29—
1 28 4.2 0.1590
4.1SIBS. . . . . . . . . . . . . . . . . . . . . . 26 1 25 3.8 0.1 3.6
600 Symptoms/signs/other . . . . . . 3 — 3 0.4 0.4610 Accidents . . . . . . . . . . . . . . . . . . .
—4 — 4 0.6
650— 0.6
Homicide . . . . . . . . . . . . . . . . . . . 2 — 2 0.3 0.3680 All other causes . . . . . . . . . . . . . 7
—
ALL1.0 0.3 0.7
All . . . . . . . . . . . . . . . . . . . . . . . . . 119 59 60 17.3 8.6 8.7aIHS code, equivalence to ICD-9 recode 61 for infant deaths available from IHS.SOURCE U.S. De~rtment of Health and Human Services, Public Health service, Health Resources and Services Admlnlstratlon, Indian Health Serwice, computer tape
supplied to the Office of Technology Assessment, Washlngto~ DC, 1985
15 leading reasons for outpatient encounters in1984. However, the increase in hospitalizationsfor diabetes from 5.9 per 10,000 population in1979 (166) to approximately 9.2 per 10,000 in 1984(excluding two tribally administered hospitals)may mean that diabetes is increasing as a prob-lem, although this rate was still much lower thanthe IHS 1984 average hospitalization rate of 26.2.
Alcohol abuse is viewed as a problem in Alaskaas elsewhere among Indian populations (64), butthe death rate from liver disease and cirrhosis wassurprisingly low, particularly among males. Com-placency about the issue of alcohol use and abuseis not in order, however, as the death rate fromliver disease and cirrhosis may be rising. Therewas an overall increase of 13.6 percent in deathsfrom liver disease and cirrhosis between 1972 and1982, compared to a decline for IHS on averageof 29.7 percent and a decline for U.S. all racesof 20 percent (142,143,202).
Consistent with the lower death rate from liverdisease and cirrhosis, the hospitalization rate foralcoholic liver disease in Alaska (1.9 per 10,000population in 1984) was only slightly higher thanthat for U.S. short-stay non-Federal hospitals(1.6), and much lower than that of IHS hospitalson average (4.4 excluding all tribally administeredhospitals), Comparisons among rates for alcohol-related conditions that are treated as mental dis-
orders are less clear. In 1984, 55 Alaska Nativeswere hospitalized for alcoholic psychoses, whichresulted in a rate (8.9 per 10,000 population) fourtimes that of U.S. short-stay non-Federal hospi-tals, but less than the average IHS rate of 10.1per 10,000 population. On the other hand, 1984hospitalization rates for both alcohol-dependencesyndrome and nondependent alcohol abuse werehigher in Alaska than among either the U.S. allraces or IHS population on average.
Hospitalizations for mental disorders werehigher in Alaska (635 hospitalizations, includingBristol Bay, for a rate of 96.7 per 10,000 popula-tion) than in U.S. short-stay non-Federal hospi-tals (1.7 million hospital discharges, for a rate of72.1 per 10,000 population).
In summary, the health status of Alaska Na-tives is both like and unlike other IHS areas. Basedon mortality data, there have been substantial im-provements since 1972 in cerebrovascular disease,pneumonia, suicide, and infant mortality, al-though death rates from these causes still exceededthose of the U.S. all races population. In the sameperiod, Alaska Native death rates from heart dis-ease, liver disease and cirrhosis, and homicide in-creased, while death rates from these causes de-clined throughout IHS on average. In particular,accidents, especially those not involving motorvehicles, pose a special problem for Alaska Na-

Ch. 4—Health Status of American Indians Ž 121
tives, and deaths caused by accidents have notdeclined as much in Alaska as throughout IHS onaverage. Further, patient care data indicate thatchronic otitis media is a severe problem amongAlaska Natives, a problem undoubtedly contrib-uted to by reduced access to medical care as a re-sult of geographic isolation.
Albuquerque Area
The Albuquerque area serves about 40 percentof the Indian population in New Mexico and avery small percent of the Indian population inColorado, for an estimated total service popula-tion of 51,329 Indians.
The Albuquerque area overall mortality ratefor the 3-year period centered in 1981 was not oneof the highest of the IHS areas, but mortality ratesfor both males and females nevertheless exceededthe U.S. all races rate. Among males, the 10 lead-ing causes of death were accidents and adverseeffects, heart disease, malignant neoplasms, sui-cide, liver disease and cirrhosis, pneumonia andinfluenza, cerebrovascular disease, homicide,nephritis, and, diabetes mellitus. For females, the10 leading causes were accidents, heart disease,malignant neoplasms, diabetes mellitus, liverdisease and cirrhosis, cerebrovascular disease,pneumonia and influenza, congenital anomalies,atherosclerosis, and suicide. The age-adjusteddeath rates and ratio to the U.S. all races areshown in table 4-32, but these figures should beinterpreted cautiously because of small absolutenumbers.
The Albuquerque death rate from accidents,particularly motor vehicle accidents, exceededthat of U.S. all races populations by 3.2 for bothmales and females, and was the leading cause ofdeath for both sexes. Death from other violence-related causes also exceeded that of the U.S. allraces population: the female suicide rate by 1.2,the male suicide rate by 3, and the male homi-cide rate by 1.6. As shown in table 4-33, substan-tial progress has been made in reducing the deathrate from accidents and homicide, but the suicidedeath rate changed very little between 1972 and1982. That this pattern of mortality may be con-tinuing can be gathered from observing that in-juries and poisonings were the second leading
cause of hospital discharges in Albuquerque in1984. However, the 1984 rate of hospitalizationsfor these external causes (161.5 per 10,000 popu-lation) was only slightly greater than the rates forboth U.S. short-stay non-Federal hospitals (148.1)and IHS hospitals (151.0). Between 1979 and 1984,the Albuquerque rate of hospitalizations for in-juries and poisonings declined slightly, but not asmuch as the U.S. all races rate.
As a further indication of the prevalence of vio-lence and injury in Albuquerque, lacerations andopen wounds were responsible for 3.2 percent ofmale outpatient visits to IHS facilities, makingthem the 10th leading cause of male visits. Hos-pitalizations for mental disorders were also un-usually high in Albuquerque, although this wasundoubtedly due in part to the availability of 13psychiatric beds in the Gallup (New Mexico) serv-ice unit.
In general, death rates for cancer and cardiovas-cular diseases were lower among Albuquerque In-dians than among the U.S. all races population,with the two exceptions of Albuquerque malemortality rates from genital cancer and intra-cerebral hemorrhage. Crude mortality rates forboth diseases of the heart and malignant neoplasmsdeclined between 1972 and 1982, the decline incancer mortality being an exception to the pat-terns for the U.S. and IHS on average. As werethe IHS rates on average, Albuquerque hospitali-zation rates in 1984 were substantially lower thancomparable rates for U.S. all races for circulatorysystem diseases and malignant neoplasms.
The diabetes death rate was apparently not ashigh in Albuquerque as it was in other IHS areas,but the problem may be getting worse. The crudedeath rate from diabetes increased 26.6 percentbetween 1972 and 1982, although small numbersmay make comparisons unreliable. Albuquerque’shospital discharge rate for diabetes in 1984 (30.9per 10,000 population) exceeded that of IHS di-rect and contract hospitals on average (26.2), andof U.S. short-stay non-Federal hospitals (25.3).Further, diabetes accounted for 4.6 percent ofmale outpatient visits and 4.9 percent of femaleoutpatient visits in Albuquerque in 1984, a sub-stantial proportion of all outpatient encounters.

122 ● Indian Health Care
Table 4-32.—Fifteen Leading Causes of Deaths and Age-Adjusted Death Rates for Albuquerque IHS AreaIndians 1980-82 and U.S. All Races 1981
IHS
Ratio of
Number Age-adjusted mortality rateAlbuquerque area
Indians to
ALL . . . .
Males:790310150820620510430830640260740730840090270
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
. . . .
Accidents/adverse effects. . . . . . . . . . . . . . . . . .Diseases of the heart . . . . . . . . . . . . . . . . . . . . .,Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . .,Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .Atherosclerosis. . . . . . . . . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .All other infectious/parasitic diseases . . . . . . . .Other arterial diseases . . . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Accidents/adverse effects . . . . . . . . . . . . . . . . . . .Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Malignant neoplasm . . . . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenzaCerebrovascular diseases . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .All other external conditions . . . . . . . . . . . . . . . .Septicemia. .,..... . . . . . . . . . . . . . . . . . . . . . . . .Nutrition deficiencies . . . . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes ., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4332301917
8885544322
66256
109494436261917161110
86542
137494
65.757.663.944.735.315,717.0
8.47.76.89.54.92.63.43.4
121.2467.8
189,9104.8100.453.660.329.530.627.025.926.1
7.07.4
12.59.01.8
273.8959.6
U.S. all races U.S. all racescodea Rank Cause name of deaths Indians.
Females:790 1.310 2.150 3.260 4.620 5.430 6.510 7.730 8.480820 9.10.090 11.830 12.740 13.140 14.490 15.
20.4135.1108.6
9.67.4
35.49.25.54.65.72.44.38.21.33.0
59.7420.4
AllaEquivalence to ICD-9 codes available from the Indian Health Service.
SOURCESU.S.all racea:U,S Department of Health and Human Services, Public Health Service, National Center for Health Statktics, ”Advance Report, Final MortalityStatistics, 1981,’’ Month/y Vita/ Statistics Reporf 33(3)supp., June 22, 1984; Indianain IHSareaa: U.S. Departmentof Health and Human Services, Publ!cHealth Service, Health Resources and Serwces Administration, Indian Health Service, computer tape supplied tothe Officeof Technology Assessment,Washington, DC, 1985.
60.2271.2163.7
18.016.016.641.716.7
5.610.010.3
6.12.23,40.5
111,1753.3
3.20.40.64.74.80.41.81.51.71.23.91.10.32.61.12.01.1
3.20.40.63.03.81.80.71.64.62.60.71.25.72.63.62.51.3
As in other IHS areas, postneonatal mortalityin Albuquerque remains a significant health prob-lem. In the 3-year period 1980-82, the total Albu-querque area infant mortality rate (9.7 per l,000live births), and the rate for neonates (4.6), wereboth lower than the rates for U.S. all races (11.9and 8.0). The postneonatal rate of 5.l was, how-ever, l.3 times that of the U.S. all races rate (3.9),and was accounted for mostly by sudden infantdeath syndrome (SIDS) (7 of the 38 infant deathsin 1980 to 1982). As throughout IHS, Indians inAlbuquerque suffer from severe problems relatedto alcohol abuse. The relatively high infant death
rate from congenital anomalies and the high mor-bidity and mortality rates from accidents, suicide,and diabetes are all consistent with an alcoholismproblem in Albuquerque that is illustrated moredirectly by liver disease and cirrhosis death ratesand hospitalizations for alcoholic liver disease, al-coholic psychoses, and other alcohol-related men-tal disorders. Most dramatic were the liver dis-ease and cirrhosis death and hospitalization rates.In 1980 to 1982 Albuquerque mortality rates foralcoholic liver disease exceeded U.S. all races ratesby 4.8 for females and 3.8 for males. Comparedto a hospitalization rate for alcoholic liver disease

Ch. 4—Health Status of American Indians ● 123
Table 4-33.—Changes in Crude Death Rates, 1972-82:IHS Albuquerque Area (rate per 100,000 population)
PercentIHS 1972-74 1975-77 1980-82 changeCode Cause rate rate rate 1972-82
790800810310620150430830510520820260740
630
Accidents/adverse effects . . . . . . . . . 166.2Motor vehicle accidents . . . . . . . . . 119.1Ail other accidents . . . . . . . . . . . . . 47.1
Diseases of the heart . . . . . . . . . . . . . 78.2Liver disease/cirrhosis . . . . . . . . . . . . 66.6Malignant neoplasms . . . . . . . . . . . . . 61.3Cerebrovascular disease . . . . . . . . . . 35.5Homicide . . . . . . . . . . . . . . . . . . . . . . . 28.4Pneumonia/influenza. . . . . . . . . . . . . . 27.5
Pneumonia . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . 26.6Diabetes mellitus . . . . . . . . . . . . . . . . 16.0Conditions arising in
perinatal period . . . . . . . . . . . . . . . . 13.3All other causes . . . . . . . . . . . . . . . . . 249.2
140.096.343.758.050.153.324.615.125.4
31.016,7
17.5236.7
106.265.740.556.630.051.717.514.018.918.928.720.3
7.7172.4
– 36.1– 44.9– 14.0– 27.6– 54.9– 15.7– 50.8–50.8–31 .4
7.726.6
–42.2–30.8
ALL All causes . . . . . . . . . . . . . . . . . . . . . . . 769.8 668.4 524.0 –31 .9SOURCES” 1972.74 and 1975-77 doatha: U.S. Department of Health, Education and Welfare, Public Health Sewce, Health Services
Administration, Indian Health Service, Selected Vital Statistics for /rrdiarr Health Service Areas and Serwce Un~ts1972 to 1977, DHEW Pub No (HSA)-79-1OO5 (Rockville, MD: HSA, 1979) 1972.74 and 1975-66 population: U S.Department of Health and Human Services, Public Health Service, Health Resources and Services Admin!stratlon,Indian Health Service, Program Statistics Branch, internal documents, Rockville, MD, 1985 1960.62 data: U SDepartment of Health and Human Services, Public Health Service, Health Resources and Services Admlnistratlon.Indian Health Service, computer tape supplied to the Office of Technology Assessment, Washington, DC, 1985
for U.S. all races of 1.6 per 10,000 population andan overall IHS rate of 4.4, the Albuquerque rateof 7.0 per 10,000 population was striking. Hos-pitalization rates for alcoholic psychoses, alcoholdependence syndrome, and nondependent alco-hol abuse also exceeded U.S. and IHS rates onaverage.
Bemidji Area
In 1984, the Bemidji area served an estimated47,000 Indians in the reservation States of Min-nesota, Wisconsin, and Michigan. The small IHSservice population and the relative lack of IHSfacilities in the Bemidji area make the analysis ofhealth status in Bemidji difficult. However, de-spite improvement over time, the health of Be-midji Indians apparently remains poor. In the 3-year period centered in 1973, the crude mortal-ity rate for Bemidj i was 879.9 per 100,000 popu-lation. In the 3-year period centered in 1981, itwas 707.3, a 19.6-percent decline (table 4-34).Most of the decline was due to reductions in mor-tality from accidents, pneumonia and influenza,diabetes mellitus, cerebrovascular disease, andhomicide, although declines in diseases of theheart and atherosclerosis contributed to overall
improvement as well. However, there has beenno improvement in the cancer mortality rate, anddeaths from suicide and chronic liver disease andcirrhosis have increased. In the 3-year period cen-tered in 1981, overall mortality of Bemidji Indiansexceeded that of U.S. all races by 1.7.
The Bemidji area crude death rate from heartdisease declined only 3.2 percent between 1972to 1974. In 1980 to 1982, the age-adjusted deathrate from diseases of the heart exceeded that ofU.S. all races by 1.5 for males and almost 2 forfemales (table 4-35). Bemidji females had theworst, and Bemidji males the second worst, over-all mortality rate from heart disease of all Indiansin IHS service areas (see figure 4-14). Bemidji isunusual in that diseases of the heart rather thanaccidents are the leading cause of death amongIndian males, and cerebrovascular disease ratherthan liver disease is the fourth leading cause ofdeath among Indian males and females. IHS out-patient, but not inpatient, information indicatesa severe problem with cardiovascular disease (seetable 4-36). Hypertension, which is implicated inischemic heart disease and cerebrovascular dis-ease (100), accounted for 6.7 percent of male visitsand 4.8 percent of female visits in 1984, makingthese the second and third reasons for outpatient
52-805 0 - 86 - 5

124 ● Indian Health Care
Table 4-34.–Changes in Crude Death Rates, 1972-82:IHS Bemidji Area (rate per 100,000 population)
PercentIHS 1972-74 1975-77 1980-82 changeCode Cause rate rate rate 1972-82
310790800810150430510260620830820480
ALL
Diseases of the heart . . . . . . . . . . . . .Accidents/adverse effects . . . . . . . . .
Motor vehicle accidents . . . . . . . . .All other accidents . . . . . . . . . . . . .
Malignant neoplasms . . . . . . . . . . . . .Cerebrovascular disease . . . . . . . . . .Pneumonia/influenza. . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . .Liver disease/cirrhosis . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . .Atherosclerosis . . . . . . . . . . . . . . . . . .All other causes . . . . . . . . . . . . . . . . .
All causes . . . . . . . . . . . . . . . . . . . . . . .
232.5175.7104.671.096.969.760.736.120.618.014.211.6
143.9
879.9
218.8121.158.662.581.074.229.333.238.123.424.410.7
141.0
795.2
225.1120.673.347.398.439.720.619.123.711.519.18,4
121.1
707.3
–3.2–31 .4–30.0–33.4
1.6–43.1–66.1–47.1
14.8– 36.4
34.4– 27.7– 15.8– 19.6
SOURCES 1972.74 and 1975-77 deaths: US. Department of Health, Education and Welfare, Public Health Service, Health ServicesAdministration, Indian Health Service, Selected Vita/ Statisf/cs for /ndian /-/ea/th Service Areas and Sewice Units,1972 to 1977, DHEW Pub. No. (HSA)-79-1OO5 (Rockville, MD: HSA, 1979). 1972-74 and 1975-86 population: U.SDepartment of Health and Human Services, Public Health Service, Health Resources and Services Administration,lndlan Health Service, Program Statistics Branch, internal documents, Rockville, MD, 1985. 1980-82 data: U.SDepartment of Health and Human Services, Public Health Service, Health Resources and Services Administration,lndlan Health Service, computer tape supplied to the Office of Technology Assessment, Washington, DC, 1985
visits respectively (see table 4-35). Only the Okla-homa City area (see below) had a higher percent-age of IHS direct care encounters for hypertensivedisease. However, the Bemidji area hospitaliza-tion rate of 54 per 10,000 population for circula-tory system diseases was far lower than the U.S.short-stay hospital rate of 238.6 per 10,000 pop-ulation, and was among the lowest of IHS areas(see table 4-19).
In the 3-year period centered in 1981, the age-adjusted cancer mortality rate of Bemidji femalesexceeded the U.S. all races female rate. The higherdeath rates for females were primarily from malig-nant neoplasms of the digestive and respiratorysystems. The only cancer site for which Bemidjimales had a greater death rate than U.S. all racesmales was the urinary tract. As have U.S. rateson the whole, the cancer death rate in Bemidji re-mained essentially unchanged between 1972 to1974 and 1980 to 1982. Bemidji hospitalizationrates for neoplasms have been surprisingly low,and average lengths of stay shorter than that inU.S. hospitals. The hospital discharge rate formalignant neoplasms in Bemidji was 10.7 per10,000 population in 1979 (166), and 10.8 per10,000 population in 1984. Comparable rates inU.S. non-Federal short-stay hospitals were 80.8and 87.8 per 10,000 population. No cancer related
diagnoses are among the leading causes of out-patient visits in Bemidji. (The low Bemidji ratescould mean that fewer Indians than should be aretreated for cancer, that coding for either or boththe underlying cause of death and the first-listeddiagnosis for hospital discharge are listed incor-rectly, or that Indians are receiving treatment forcancer in non-IHS facilities. )
As in most IHS areas, in the 3-year period cen-tered in 1981, accidents were the second leadingcause of death among Bemidji males, and the thirdleading cause of death among Bemidji females, ex-ceeding the U.S. all races rates by more than threetimes for both males and females. Deaths fromviolent causes other than accidents appear to berelatively less of a problem in Bemidji than inother IHS areas, the exception being male suicides,of which there were 22 in 1980 to 1982, a rate 1.7times that of U.S. all races. Compared to otherIHS areas, Bemidji was notable in that suicide wasnot among the 15 leading causes of death for In-dian females in 1980 to 1982. Despite high acci-dent and injury mortality rates, Bemidji’s 1984hospitalization rate per 10,000 population for in-juries and poisonings (63.0) was markedly lessthan that of U.S. non-Federal short-stay hospi-tals (148.1). However, injury-related diagnoses(lacerations and open wounds; superficial inju-

Ch. 4—Health Status of American Indians ● 125
Table 4-35.—Fifteen Leading Causes of Deaths and Age-Adjusted Death Rates for Bemidji IHS Area Indians 1980-82and U.S. All Races 1981
Ratio of BemidjiIHS Number Age-adjusted mortality rate area Indians tocodea Rank Cause name of deaths Indians
310150790430620260510480090540830640610630730
ALL
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
. . .
Males:310 1.790 2.150 3.4.430820 5:510 6.620 7.540 8.260 9.830 10.740 11.730 12.640 13.480 14.490 15.
ALL . . .
Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Malignant neoplasms. ... . . . . . . . . . . . . . . . . . .Accidents/adverse effects. . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis, . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Atherosclerosis. . . . . . . . . . . . . . . . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hernia/intestinal obstruction . . . . . . . . . . . . . . . .Cholelithiasis/gallbladder . . . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Disease of the heart . . . . . . . . . . . . . . . . . . . . . .Accidents/adverse effects. . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . .
bCere rovascular diseases . . . . . . . . . . . . . . . . . . .Suicide ., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . .Atherosclerosis. . . . . . . . . . . . . . . . . . . . . . . . . . . .Other arterial diseases . . . . . . . . . . . . . . . . . . . . .All others. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
125664621161511
76554333
45381
170112633122161513101097544
55546
262.5148.3
74.936.636634.823.113.010.4
9.37.58.94.86.13.4
82.3762.5
402.2189.7153.2
73.530.630.635.433.026.216.510.2
7.910.8
9.410.3
102.61,142.1
a Equivalence to ICD-9 code available from the Indian Health Service.
U.S. all races U.S. all races
135.1 1.9108.6 1.420.4 3.735.4 1.0
7.4 4.99.6 3.69.2 2,54.6 2.82.4 4.39.5 1.04.3 1.73.6 2.51.3 3.70.7 8.85.5 0.6
62.8 1.3420.4 1.8
271.260.2
163.741.718.016.616.026.210.016.710.3
6.15.66.08.5
76.5753.3
1.53.20.91.81.71.82.21.32.61.01.01.31.91.61.21.31.5
SOURCES U.S. allraces:US Department of Health and Human Servicespubhc Health Service, National Center for Health Statistics “Advance Report, F!nal MortalityStatlstlcs 1981:’ Monthly V/fa/Statfsf/cs F?eport33(3)supp , June22, 1984, Indians in IHS areas: US Department of Health and Human Services, PublicHealth Service, Health Resources and Serv!ces Administration. Indian Health Service, computer tape supplied to [he Office of Technology Assessment,Washington. DC, 1985
ries and contusions; dislocations, sprains, and in 1984. As in almost all IHS areas, otitis mediastrains) were among the 15 leading causes of out- accounted for a high proportion of ambulatorypatient visits for Bemidji males in 1984, account- care. Although there were few deaths from dia-ing for 6.7 percent of male visits. betes in 1980 to 1982 in Bemidji, it was a leading
cause of outpatient visits in 1984, accounting forOther ailments of special note in Bemidji are 6.8 and 7.2 percent of visits among females and
reflected in morbidity but not mortality data: skin males, respectively. Bemidji’s hospitalization ratediseases, vision problems, disorders of the mus- for diabetes (97 discharges 20.6 per 10,000 popu-culoskeletal system, and for females, urinary tract lation in 1984) was lower than that of U.S. short-infections. Skin diseases constituted 2 of the 15 stay non-Federal hospitals (25.3) in 1984, but itleading causes of male outpatient visits, and 1 of was high relative to hospitalization rates for otherthe 15 leading causes of female outpatient visits diseases.

126 Ž Indian Health Care
Table 4-36.–Fifteen Most Frequent Outpatient Diagnoses:a Bemidji Area, Fiscal Year 1984
Percent ofIHS Number of total visits
Rank Code Clinical impressions visits by sexFemale:
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
Male:1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
080819300283250480575823210818812400510301827
080283250300819818730575210731702520355510827
ALL
Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Prenatal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other muskuloskeletal and connective tissue disease . . . . . . . . . . . .Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Refractive error . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other iii-defined, undiagnosed diseases . . . . . . . . . . . . . . . . . . . . . . . .Urinary tract infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Eczema, urticaria, orskin allergy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pharyngitis and tonsillitis (nonstrep) . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Laceration, open wound . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other muskuloskeletal and connective tissue disease . . . . . . . . . . . .Refractive error . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Superficial injury or contusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Dislocations, sprains, and strains . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other diseases of skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diseases of teeth and gums . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Eczema, urticaria, or skin allergy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
All other causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4,2764,1233,6683,0202,7762,6511,7941,4821,4731,3621,2191,1051,1031,0931,143
3,4813,2373,1642,6382,3961,4871,4191,3931,116
939884836833824836
54,585112.356
6.86.55.84.84.44.22.82.32.32.21.91.71.71.71.8
7.26.76.65.55.03.12.92.92.32.01.81.71,71.71.7
All causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . , 100.0alHS ~efer~ t. these as ~linical impre~~ion~, be~a”~e they are recorded before a clinical diagnosis is completed; therefore, they may nOt be valid diagnoses
SOURCES” 151eadlngclinlcal impraaaiona:U.S. Department of Health and Human Services, Public Health Service, Health Resources and Sewices Administration, lndl-an HeaHh Service, “SpecialReport on 15 Leading Causesof Outpatient Care ByAreaand Service Unit, State and County, “ internal document, Albuquerque,
NM11985. BamidJitotak US. Departmentof Health and Human Services, Public Health Service, Health Resources and Sewices Administration, Indian HealthService, Officeof Planning, Evaluation and Legislation, Program Statistics Branch, Summawof Leading Causes for Outpatier?t Visifs, /ndiarr HeaHhServiceFaci/itles, Fkca/ Year 19#(Rockville, MD: IHS, no date)
Billings Area
IHS estimates that its Billings area serves ap-proximately 40,000 Indians residing in Montanaand Wyoming.
The Billings service population is equal to 4.3percent of the estimated IHS service population.However, in the 1980-82 period, Billings had 6.8percent of IHS deaths. As in most other IHS areas,poor socioeconomic conditions in Billings corre-late with poor health. The Billings area has shownonly a 7-percent decline in overall mortality sincethe early 1970s, from a crude rate of l,015.6 to943.3 deaths per 100,000 population. The com-
bined age-adjusted mortality rate for the Billingsarea in the 1980-82 period was l,260, 1.3 deathsper l00,000 service population, a rate more thantwice that of U.S. all races.
The leading causes of death among Indian malesin 1980 to 1982 were accidents, heart disease,cancers, liver disease and cirrhosis, suicide, homi-cide, and cerebrovascular disease (see table 4-37).These causes accounted for 74 percent of alldeaths. For females, the leading causes of deathin 1980 to 1982 were heart disease, accidents, ma-lignant neoplasms, liver disease and cirrhosis, di-abetes mellitus, conditions originating in theperinatal period, cerebrovascular disease, pneu-

Ch. 4—Health Status of American Indians • 127
Table 4-37.–Fifteen Leading Causes of Deaths and Age-Adjusted Death Rates for Billings IHS Area Indians 1980.82and U.S. All Races 1981
Ratio of BillingsIHS Number Age-adjusted mortality rate area Indians tocodea Rank Cause name of deaths Indians U.S. all races US. all races
Females:310 1.790 2.150 3.620 4.260 5.740 6.430510 7.8.830 9.540 10.640 11.630 12.730 13.090 14.140 15.
ALL . . . .
Males:790 1.310 2.150 3.620 4.820 5.830 6.430 7.510 8.540 9.260 10.090 11.740 12.140 13.640 14.030 15.
ALL . . . .
Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Accidents/adverse effects, . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . .Cholelithiasis/gallbladder . . . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other infectious/parasitic diseases . . . . . . . .All others ... . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Accidents/adverse effects. . . . . . . . . . . . . . . . . . .Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. ., . . . ... , . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Cerebrovascular diseases. . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary disease . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .All other infectious/parasitic diseases . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . .Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
88635940181514149874433
75424
168119
51402929201511
977554
97616
229.6122.4159.6109.050.416.732.630.116.223.616.68.94.49.16.9
161.0997.1
354.5340.3153.6114.861.657.457.841.231.925.520.9
7.912.311.612.5
235.61,539.4
135,120.4
108.67.49.68.2
35.49.24.39.53.60.75.52.41.3
59.2420.4
60.2271.2163.7
16.018.016.741.716.626.210.0
3.410.3
1.75.61.0
91.0753.3
1.76.01.5
14.75.22.00.93.33,82.54.6
12.80.83.85.32.72.4
5.91.30.97.23.43.41.42.51.22.66.20.87.22.1
12.52.62.0
aEquivalence to ICD-9 code available from the Indian Health SefvlCe
alHS refers t. these as cllnlcal ImpressIons, because they are recorded before a clinical diagnosis IS completed, therefore, they maY nOt be valld diagnoses
SOURCES U.S. allracea:US Department of Health and Human Services, Public Health Service, National Center for Health Statistics, “AdvanceR eport.F inal MortahtyStatistics, 1981,” Morrth/y V/ta/Stat/st/cs Report 33(3) supp , June22, 1984, Indians In IHS areaa: US Department of Health and Human Serv!ces, PublicHealth Service, Health Resources and Serwces Administration, Ind!an Heatth Serwce, computer tape supplted to the Office of Technology Assessment,Washington, DC, 1985
monia and influenza, and homicide. These causes males, for whom the mortality rate was almostaccounted for 75 percent of all deaths (see table six times that of U.S. all races males. This ratio4-13), Deaths from other causes are too small from also applied to females, although in 1980 to 1982which to draw solid inferences, but severe health accidents were not the leading cause of death forproblems are suggested in the finding that the rates females. While suicide and homicide were the 10thof almost all major causes of Indian deaths in Bill- and 11th causes of death for U.S. all races popu-ings exceeded that of U.S. all races. lations in 1981, they were the 5th and 6th lead-
ing causes of death among Billings males, eachThe Billings area crude death rate from acci- having claimed 29 lives in the 3-year period cen-
dents of all types declined an estimated 11 per- tered in 1981. The age of suicides in 1980 to 1981cent between 1972 and 1982 (table 4-38), but ac- was different from both U.S. all races and othercidents remained the leading cause of death among IHS areas. The greatest single number of Billings

128 ● Indian Health Care
Table 4.38.–Changes in Crude Death Rates, 1972-82:IHS Billings Area (rate per 100,000 population)
PercentIHS 1972-74 1975-77 1980-82 changeCode Cause rate rate rate 1972-82790 Accidents/adverse effects . . . . . . . . . 236.4 214.3 209.5 – 11.4310 Diseases of the heart . . . . . . . . . . . . . 190.2 185.6 187.7 – 1.3150 Malignant neoplasms . . . . . . . . . . . . . 84.4 80.0 99.8 18.2620 Liver disease/cirrhosis . . . . . . . . . . . . 69.8 66.6 72.6 4.0510 Pneumonia/influenza. . . . . . . . . . . . . . 55.1 32.8 26.3 –52.3430 Cerebrovascular disease . . . . . . . . . . 36.0 29.7 30.8 – 14.3740 Conditions arising in
perinatal period , . . . . . . . . . . . . . . . 32.6 28.7 20.0 –38.8820 Suicide . . . . . . . . . . . . . . . . . . . . . . . . . 29.2 20.5 29.0 –0.6820 Homicide . . . . . . . . . . . . . . . . . . . . . . . 23.6 25.6 34.5 46.1730 Congenital anomalies . . . . . . . . . . . . . 14.6 7.3 – 50.3
All other causes . . . . . . . . . . . . . . . . . 243.7 219.8 225.8 – 7.1ALL All causes . . . . . . . . . . . . . . . . . . . . . . . 1,015.6 903.6 943.3 – 7.1SOURCES: 1972.74 nnd 197$77 deatha: US. Department of Health, Education and Welfare, Public Health Service, Health Services
Administration, Indian Health Service, Selected Vita/ Sfaf/sf/cs for /nd/arr )-lea/th Ser-v/ce Areas and Serv/ce un/@,1972 to 1977, DHEW Pub. No. (HSA)-79-1OO5 (Rockvllle, MD: HSA, 1979). 1972-74 and 1975-86 population: U.S.Department of Health and Human Services, Publlc Health Service, Health Resources and Services Administration,Indian Health Service, Program Statistics Branch, internal documents, Rockviile, MD, 1985. 1980-82 data: US.Department of Health and Human Services, Public Health Service, Health Resources and Services Administration,Indian Health Service, computer tape supplied to the Office of Technology Assessment, Washington, DC, 1985
area suicides occurred in the 15 to 24 age group,while this age group was among the lowest forU.S. all races in 1981.
Hospitalizations and outpatient visits reflect theimpact of accidents and other violence. Hospitali-zations for injuries and poisonings occurred at arate almost twice that for all IHS direct and con-tract hospitals and U.S. non-Federal short-stayhospitals. Lacerations and open wounds accountedfor 2.7 percent of male outpatient visits, and dis-locations, sprains, and strains accounted foranother 2 percent (see table 4-39).
Deaths from diseases of the heart have remainedrelatively stable, from a crude rate of 190.2 per100,000 population (169 deaths) in 1972 to 1974,to 185.6 (181 deaths) in 1975 to 1977, and to 187.7(207 deaths) in 1980 to 1982, a decrease of only2.4 percent. Based on data for 1980 to 1982, Bill-ings area males are 1.25 times as likely as U.S.all races males to die from diseases of the heart,particularly acute myocardial infarction, makingheart disease the second leading cause of maledeaths. The ratio is worse for females, who are1.7 times as likely as their U.S. all races counter-parts to die of heart disease. The 88 heart diseasedeaths in 1980 to 1982 accounted for 21 percentof Billings area female deaths. Cerebrovascularmortality was also the seventh leading cause ofdeath for males and females, although absolute
numbers were small. Consistent with the high rateof cardiovascular mortality, hospitalizations fordiseases of the circulatory system occurred at arate twice that of IHS areas on average, thougha little less than that of U.S. non-Federal short-stay hospitals.
Malignant neoplasms were the third leadingcause of death in 1980 to 1982. In the decade be-tween 1972 and 1982, the cancer mortality rateincreased from a crude rate of 84.4 per 100,000population to 99.8 per 100,000, an 18-percent in-crease, although absolute numbers are small andchanges should be interpreted cautiously. In the3-year period centered in 1981, 51 males and 59females died of cancer. As in Aberdeen and Be-midji, age-adjusted cancer death rates exceededthe U.S. all races rate by 1.5 for women, but didnot exceed the U.S. rate for men. Cancer of therespiratory system was the leading cause of can-cer deaths in both sexes. Data indicating that 1984hospitalizations for cancer occurred at twice therate of IHS hospitals in all areas indicate that can-cer continues to be a problem in Billings relativeto other IHS areas.
Unlike the experience in other IHS areas, theBillings diabetes crude death rate increased from16.4 per 100,000 population to 24.5 per 100,000population in the 8-year period from 1975 to 1982.Small numbers indicate that inferences should be

Ch. 4—Health Status of American Indians ● 129
Table 4.39.–Fifteen Most Frequent Outpatient Diagnoses:a Billings Area, Fiscal Year 1984
IHSRank Code.Female:
1.2.3.4.5.6.7.8.9.
10.11,12.13.14.15.
Male:1.2.3.4.5.6.7.8.9.
10.11.12,13.14.15.
480300819080251823820821812818301810400283827
251300821812819820818080730823301810283702827
Clinical impressionsNumber of
visits
Prenatal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Chronic otitis media with/without mastoiditis . . . . . . . . . . . . . . . . . . .Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hospital medical/surgical followup . . . . . . . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other ill-defined, undiagnosed diseases . . . . . . . . . . . . . . . . . . ... . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pharyngitis and tonsillitis (nonstrep) . . . . . . . . . . . . . . . . . . . . . . . . .All other symptoms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Urinary tract infection. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Another . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Chronic otitis media with/without mastoiditis . . . . . . . . . . . . . . . . . . .Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other ill-defined, undiagnosed diseases . . . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hospital medical/surgical followup . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Laceration, open wound . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pharyngitis and tonsillitis (nonstrep) . . . . . . . . . . . . . . . . . . . . . . . . . . .All other symptoms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Dislocations, sprains, and strains . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ALLAll other causes, both sexes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11,0378,9606,6636,4756,3426,1925,0684,7044,2034,1653,9403,9323,1812,886
38,362
6,8946,3855,2244,8014,7144,1544,0874,0633,5463,2022,7762,6722,5792,513
25,320
133,339332,379
Percent oftotal visits
by sex—
5.64.63.43.33.23.22.62,42.12.12.02.01.61.5
19,6
5.24.83.93.63.53.13.13.02.72.42.12.01.91.9
18.9
100.0alHS refers to these as cl!n!cal Impressions, because they are recorded before a clinical diagnosis IS completed, therefore, they may not be valld diagnoses
SOURCES 151aadlngcllnical impressiona:US Department of Health and Human Se~ices, Publlc Health Service, Health Resources and Services Admlnlstrat!on, lnd!an Health Service, “Special Reporf on 15 Leading Causesof Outpatient Care By Areaand Service Unit, State and County.” internal documenf, AlbuquerqueNM, 1985 Billlngs totalUS Department of Health and Human Services, Public Health Service, Health Resources and Services Admlnlstratlon, Indian HealthServ{ce Offlceof Planning, Evaluation and Leglslatlon, Program Stat!sttcs Branch SwmnaryofLeadmg Causes forOutpatlent Vw/fs, /rid/an Hea/fh Serv/ceFacd/fres, F/sea/ Year l%?4(Rockvtlle, MD IHS, no date)
made cautiously, but the growing significance ofthe diabetes problem is also reflected in the Bill-ings hospitalization rate. The 217 hospital dis-charges for diabetes in 1984 (195) equaled a rateof 54.1 discharges per 10,000 population, morethan twice the diabetes discharge rate for U.S.short-stay non-Federal hospitals (see table 4-19),although, as is typical, the proportion of hospitali-zations was lower than the proportion of deaths.Outpatient encounters for diabetes were, how-ever, relatively low in Billings (about 3 percentof visits compared to an IHS average of 4.4), anddespite the high rate of hospitalization for dia-betes, refractive disorders were not among the top15 clinical impressions.
Both neonatal and postneonatal infant mortal-ity were higher in 1980 to 1982 than for U.S. allraces, but not as high as the infant death rates forseveral other IHS areas (see figure 4-16). The sin-gle largest cause of infant deaths in Billings, asin most other IHS areas, was sudden infant deathsyndrome (175a).
Billings is no different from other areas in thatalcohol abuse has been implicated in almost allthe leading causes of death. High death rates fromliver disease and cirrhosis, the fourth leading causeof death, confirm the alcoholism problem. In 1980to 1982 the male death rate from liver disease andcirrhosis was more than 7 times that of U.S. all

130 ● Indian Health Care
races males, and the female death rate was morethan 14 times that of U.S. all races females. Asanother indicator of the alcohol abuse problem,the hospitalization rate for Billings Indians foralcohol-related conditions was substantially greaterthan that of both IHS and U.S. non-Federal short-stay hospitals.
Both otitis media and urinary tract infectionswere among the leading causes of outpatient visits.In 1984, 6,894 (5.2 percent) of male outpatientvisits, and 6,342 (3.2 percent) of female outpatientvisits to Billings area IHS facilities were for chronicotitis media, making the condition the secondleading cause of outpatient visits for males andthe third for females. Billings had the third high-est rate of hospitalizations for otitis media of IHSareas, at a rate more than twice that of U.S. non-Federal short-stay hospitals.
Mental disorders accounted for a higher pro-portion of hospitalizations in Billings than in otherIHS areas. In Billings, 474 discharges for mentaldisorders were made in direct and contract hos-pitals in 1984, for a rate of 118.1 per 10,000 serv-ice population. The U.S. short-stay non-Federalhospital rate for 1984 was considerably lower,72.1 (203), Two-thirds of Billings inpatient visitswere for disorders related to alcohol abuse. Men-tal disorders, however, were not among the 15leading reasons for outpatient visits in Billings,although one or more categories of mental dis-orders were among the leading reasons for out-patient encounters in several of the Billings serv-ice units (175),
California Program
The California program covers an estimated73,262 of California’s 216,070 Indians.
While data pertaining to the health status of allother IHS programs and areas have their limita-tions, information about Indians in California ispractically nonexistent. This state of affairs ex-ists for several reasons, the primary one being theloss of reservation lands as a consequence ofchanging and diverse Federal policies applied toCalifornia Indians. The California population isa great ethnic mix, with a great number of His-panics and individuals who are part Hispanic, and
Indians from countries other than the UnitedStates, making identification of “Indians” diffi-cult. Thus, Indians may be harder to recognizeas Indians for vital statistics purposes (births anddeaths), although they may be likely to identifythemselves as such for U.S. Census purposes. Asa consequence, natality and mortality statisticsare said to be seriously underreported. Althoughno one knows how extensive the undercountingis, it is clear that 471 deaths in 3 years for theservice population of nearly 70,000 people and1,056 Indian deaths among the estimated 216,000Indians in the entire State of California is veryunlikely. Those numbers of deaths would reflectmortality rates of 278.74 and 201.7, half that ofthe U.S. all races rate and even lower than thedeath rates of some of the wealthiest counties inthe country. Douglas County (Colorado) for ex-ample, the seventh wealthiest county with a me-dian family income of $30,154 in 1979, had anage-adjusted death rate of 362.4 per 100,000 pop-ulation in 1981. The 1980 age-adjusted death ratesfor Montgomery County (Maryland), the sixthwealthiest county in the Nation, was 460.7 per100,000 population. The lack of valid mortalitydata might be remedied by the availability of pa-tient care statistics, but there are no IHS directcare facilities in California, and IHS-funded fa-cilities administered by Indian organizations areneither required to report on reasons for treat-ment, nor provided the equipment to do so effi-ciently and compatibly with IHS patient care sys-tems (43).
However, while actual mortality rates appearedinvalid to California Indian health care adminis-trators, officials and tribal members contacted byOTA agreed that, based on their experience, therank order of causes reflected in the mortality sta-tistics was probably correct. In fact, the rank or-der is comparable to that of causes of death forIndians in other IHS areas. The leading causes ofdeath among California Indians in 1980 to 1982were estimated to be, in descending order, dis-eases of the heart; accidents; malignant neoplasms;cerebrovascular disease; chronic liver disease andcirrhosis; homicide; diabetes mellitus; suicide;pneumonia; chronic pulmonary disease; nephri-tis, nephrotic syndrome, and nephrosis; certainconditions originating in the perinatal period;

Ch. 4—Health Status of American Indians ● 131
atherosclerosis; tuberculosis; and other diseasesof arteries, arterioles, and capillaries. These dataindicate that Indians in California experiencemuch the same health problems as Indians in otherparts of the country.
Nashville Program
It is difficult to write of the Nashville programin the same sense that other IHS programs andareas are discussed. Indian areas in the Nashvilleprogram are widely dispersed. Currently, the areaserves an estimated 36,000 Indians in nine reser-vation States: Alabama, Mississippi, Louisiana,Florida, North Carolina, Pennsylvania, NewYork, Connecticut, and Maine (see figure 1-3 inch. 1). However, unlike most other IHS areas, thereservation States included in the Nashville pro-gram contain more Indians who are not eligiblefor IHS service than they contain IHS service-eligible Indians (table 4-l). (The Nashville pro-gram office is located in Tennessee, which is nota reservation State, although it has an estimated5,372 Indian residents).
There is little demographic, social, housing, andeconomic information about Indians served by theNashville program. Many of the reservations areso small that the census will not release informa-tion on their social, economic, and housing char-acteristics in order to maintain confidentiality.The socioeconomic information that is availablevaries considerably across reservations. Based ondata released by the U.S. Census Bureau, for ex-ample, the percent of Nashville area reservationIndians aged 25 and over who were high schoolgraduates ranges from 69.4 percent among theShinnecocks, a reservation of only 261 individ-uals in New York State, to 30.1 percent on theIndian Township Reservation in Maine, a reser-vation estimated to have only 384 Indians (146).Median family income ranged from $26,250 ona reservation in Connecticut to $6,250 on a res-ervation in Maine, and the percent of Indianhomes lacking plumbing ranged from O to 39.6percent (145). Bureau of Indian Affairs reportsemployment data for only six of the reservationStates in the Nashville area. In these States, from28 (Mississippi) to 60 percent (New York) of thelabor force was estimated to be able to work butunemployed in January 1985 (209).
In the 1980-82 period, 557 Indian residents ofIHS service areas in the Nashville area died, foran overall age-adjusted mortality rate of 765.4 per100,000 population, a rate 1.3 times the U.S. allraces rate (1.4 for females and 1.3 for males; seetable 4-40). Because of the dispersion of Nashvillearea Indians, it is possible that the death rate isunderstated. In addition, as shown in table 4-41,in most service units the number of deaths thatwas reported was too small from which firm con-clusions could be drawn. The largest service units,which contained the largest numbers of deaths,were the Seneca, the Cherokee, and the Choctaw;and the service units with the worst Indian to U.S.all races ratios were the Choctaw, the Seneca, andthe St. Regis Mohawk, although all service unitsbut the Seminole had age-adjusted mortality ratesexceeding the U.S. all races average.
The leading cause of death was diseases of theheart, with the mortality rate exceeding that ofU.S. all races by 1.3 for females, and 1.1 formales. The leading cause of death among maleswas accidents. In 1980 to 1982 Indian males diedfrom accidents at an average rate 2.7 times thatof U.S. all races in 1981. For females, on the otherhand, accidents were the fifth leading cause ofdeath. Suicide and homicide were the fifth andsixth causes of death among Nashville males, ex-ceeding the rate for U.S. all races males by 1.7and 1.9 times, respectively. As shown in table 4-43, the number of females who died from thesetwo violent causes in 1980 to 1982 was too smallfor valid conclusions to be drawn.
On average, male deaths from cancer occurredat a rate lower than that of U.S. all races, exceptfor cancer of the digestive system, which occurredat 1.2 times the U.S. rate for both sexes. The cir-cumstances of the Nashville program make dis-cussion of the absolute numbers of other deathsinappropriate. It is also difficult to draw conclu-sions about health status from patient care datafor the Nashville area, because there are only twoIHS-supported hospitals (one of them triballyoperated) and only 11 health centers/stations infour States to serve the Indian population, which,as noted, is dispersed over nine States. Thus, onewould expect that many Indians, even if IHSservice-eligible, obtain health care from otherproviders. The patient care data that are avail-able, primarily from tribally administered facil-

132 ● Indian Health Care
Table 4-40.— Fifteen Leading Causes of Deaths and Age-Adjusted Death Rates for Nashville IHS Area Indians1980.82 and U.S. All Races 1981
Ratio of NashvilleIHS Number Age-adjusted mortality rate area Indians tocodea Rank Cause name of deaths Indians U.S. all races U.S. all racesFemales:310 1.150 2.430 3.260 4.790 5.510 6.620 7.830 8.640 9.730 10.740 11.820 12.090 13.250 14.270 15.
ALL . . . .
Males:310 1.790 2.150 3.430 4.260 5.820 6.830 7.620 8.510 9.740 10.840 11.090 12.250 13.490 14.540 15.
ALL . . . .
Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Accidents/adverse effects. . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Benign neoplasms, other . . . . . . . . . . . . . . . . . . .Nutritional deficiencies . . . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Accidents/adverse effects . . . . . . . . . . . . . . . . . . .Malignant neoplasm.. ..,.. . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .All other external conditions . . . . . . . . . . . . . . . .Septicemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Benign neoplasms, other . . . . . . . . . . . . . . . . . . .Other arterial diseases . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6641191312
9753332111
37223
89624319141414121110
32222
35334
173.7116,846.434.226.422.521.313.1
7.16.46.44.22.82.52.5
96.2582.5
285.0159.0138.960.946.730.431.441.129.421.0
6.05.75.25.37.1
92.5965.6
135.1108.635.4
9.620.4
9.27.44.33.65.58.25.72.41.70.4
62.9420.4
271.260.2
163.741.710.018.016.716.016.610.3
2.23.42.18.5
26.286.5
753.3
1.31.11.33.61.32.42.93.02.01.20.80.71.21.56.31.51.4
1.12.60.81.54.71.71.92.61.82.02.71.72.50.60.31.11.3
aEquivalence to ICD-9 code available from the Indian Health Sewice.
SOURCESU .S.allr aces: US, Departmentof Health and Human Services, Public Health Service, National Centerfor Health Statistics, ’’Advance Report, Final MortahtyStatistics, 1981,’’ Monthly Vital Statistics Reporl 33(3)supp., June 22, 1984, lndianalnlHS areas: U.S. Departmentof Health and Human Services, PubhcHealth Service, Health Resources and Sewices Administration, Indian Health Sewice, computer tape supplied to the Office of Technology Assessment,Washington, DC, 1985,
ities, were summarized earlier and show that over- Hospitalization rates in the Nashville area inall hospital discharges from Nashville facilities 1979 (166) were much higher than they were inoccur at a rate far lower than from other IHS and 1984, which may reflect the decreasing pool ofU.S. short-stay non-Federal hospitals. The only contract care funds (see ch. 6) and the increasingexceptions are the categories ’’supplementary clas- population base. Nashville is similar to other IHSsification” (for Nashville, this is primarily after- areas in that “complications of pregnancy, ” in-care in IHS hospitals following discharge form eluding normal deliveries, is the first cause of hos-contract hospitals) at a rate of 82.4 per 10,000 pitalization.population, compared to an average IHS rate of64 per 10,000 population and an average U.S. rate Nashville was also unusual in that outpatientof 19.4 per 10,000 population; and “symptoms, visits for diseases of the teeth and gums weresigns and ill-defined conditions” (Nashville rate among the leading causes of visits for both malesof 56.1, IHS rate of 57, and U.S. short-stay hos- and females, and gastroenteritis and diarrhea werepital rate of 22 per 10,000 population). among the leading causes of visits for males (ta-

Ch. 4—Health Status of American Indians ● 133
Table 4-41 .—Estimated Deaths and Age-Adjusted Death Rates for Indians in the Nashville Program,by Service Unit, 1980-82
Both sexes
Age-adjusted - - - - - -
Service unit Deaths death ratea
Cherokee . . . . . . . . . .
Chitimacha . . . . . . . .
Choctaw ... . . . . . .
Coushatta . . . . . . . . .
Miccosukee . . . . . . .
Narragansett b . . . . . .Passamaquoddy . . . .
Penobscot ., . . . . . .
Pequot b . . . . . . . . .Poarch Creeksc . . . . .Seminole . . . . . . . . .
Seneca . . . . . . . . . . . .
St. Regis Mohawk .
Tunica Biloxid . . . . . .All . . . . . . . . . . . . . . . .
122
5
108
5
14
NA28
21
NANA28
170
55
NA557
805.6
428,3
865.5
1,379.7
276.4
NA813.6
636.9
NANA
488.7
876.0
846.6
NA765.4
Ratio to U.S. 1980 serviceall races rate population Leading causes
1.4 5,604
NA
1.5
NA
NA
NA1,4
1.1
NANA0.9
1.5
1.5
NA1.3
388
4,155
1,352
[821]b
[4,612]C
2,139
7,258
2,526
[484]d
35,822
Male:Female:
Male:Female:Male:
Female:
MaleFemale:Male:Female:
Male:
Female:
Male:Female:
Male:Female:Male:
Female:
Male:Female:
Male:
Female:
aRate per 10o,ooo Popdatto”bBecame a ~ewlce Unit ,n 1983, ~opulat{on ~ho~n ,~ estimate for 1983 Deaths In 1980.82 not availableC B ecame a ~ewlce Unit ,n 1984 ~opulatlon shown is estimate for 1984 Deaths In 1980.82 not availabledgecame a sewlce Unit ,n 1982, population shown is estimate for 1982 Deaths In 1980.82 not available
Heart disease, cancer, accidentsHeart disease, cancer, diabetesmellitusHeart diseaseDiabetes mellitusAccidents, heart disease, homicide,suicideCancer, heart disease,cerebrovascular diseaseHeart diseaseHeart diseaseAccidents, suicideHeart disease
Cancer, heart disease,cerebrovascular diseaseHeart disease, cerebrovasculardisease, homicideHeart disease, cancer, accidentsCancer, heart disease, pneumonia/influenza
Cancer, accidentsCancer, heart diseaseHeart disease, accidents, cancer,cerebrovascular diseaseHeart disease, cancer, diabetes,cerebrovascuIar diseaseHeart disease, cancerHeart disease, cancer,cerebrovascular disease
Heart disease, accidents, cancer,cerebrovascular disease, diabetesHeart disease, cancer,cerebrovascular, diabetes, accidents
SOURCES Indian deaths: U S Department of Health and Human Services, Public Health Service. Health Resources and Services Admln!stration, Indian Health Service,computer tape supplied to the Off Ice of Technology Assessment. Washington, DC, 1985 Population: U S Department of Health and Human Serwces, PublicHealth Serwlce, Health Resources and Services Admlnistratlon, Indian Health Service, Off Ice of Plannlng, Evaluation and Legislation. Population StatisticsStaff, “Estimated Indian and Alaska Natwe Service Population by Area and Service Unit, ” Internal document, Rockville, MD, Feb 1, 1985
ble 4-42). The Choctaw and Cherokee service Utah. The service population in the Navajo areaunits account for most of the visits for gastroente- was estimated to be 162,005 in 1984.ritis. The St. Regis Mohawk service unit stood In some respects the health status in the Navajoout, because skin diseases were among the lead-ing cause of visits for both males and females, and
area is better than that of the U.S. all races pop-ulation. Between 1972 and 1982, the Navajo area
vitamin deficiencies and neuroses are among theleading causes of visits for females (175).
experienced a 31.2 percent decline in the crudedeath rate (see table 4-43), although the death
Navajo Area rates from cancer and congenital anomalies rosein the same period. Of the 15 leading causes of
The Navajo area serves the Navajo reservation death in 1980 to 1982, mortality rates were bet-located in the States of Arizona, New Mexico, and ter on average than those of U.S. all races for dis-

134 ● Indian Health Care—
Table 4.42.—Fifteen Most Frequent Outpatient Diagnoses:a Nashville Area, Fiscal Year 1984
Percent o f –
IHS Number of total visitsRank Code Clinical impressions visits by sex.Female:
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
300819080480283250818575823305355808450301827
819283080250818575730305731821355014702827
ALL
Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Prenatal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis medis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other muskuloskeletal and connective tissue diseases.. . . . . . . . . .Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Respiratory allergy, asthma, and hay fever . . . . . . . . . . . . . . . . . . . . . .Diseases of teeth and gums . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Headache . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Infection of female genitalia (excluding VD) . . . . . . . . . . . . . . . . . . . .Pharyngitis and tonsillitis (nonstrep) . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other musculoskeletal and connective tissue disease. . . . . . . . . . . .Laceration, open wound . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Respiratory allergy, asthma, and hay fever . . . . . . . . . . . . . . . . . . . . . .Superficial injury, contusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diseases of teeth and gums . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Gastroenteritis, diarrhea, etc. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Dislocations, sprains, and strains . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
All other causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4,3282,8342,0201,7311,3591,3031,1241,055
919836836788728707
2,483
2,9901,6741,3571,1721,1361,009
868805719698687604591548
1,630
33,52073,059
10.06.64.74.13.23.12.62.52.22.02.01.81.71.75.8
10.25.74.64.03.93.43.02.72.42.42.32.12.01.95.5
100.0alHS ~efer~ t. these as clinical impre~~ion~, be~a”~e theY are recorded before a clinical diagnosis is completed; therefore, they may nOt be valid diagnoses
SOURCES” 151eadingcllnicai impresalona:U,S. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Indi.an Heaith Service, “SpecialReport on 15 Leading Causesof Outpatient Care By Areaand Service Unit, State and County,” internal document, Albuquerque,NM, 1985. Nashville totaL U.S. Department of Health and Human Services, Publlc Health Service, Health Resources and Services Administration, IndianHealth Service, Office of Planning, Evaluation and Legislation, Program Statistics Branch, Surrrrnary ofLeadirrg Causes forOutpatient Visits, /rrdian Hea/thService Faci/it/es, fiscal Year 1984 (Rockville, MD: IHS, no date)
eases of the heart (although it was the secondleading cause of death among Navajo), cancer,cerebrovascular disease, chronic and obstructivepulmonary disease, and neonatal mortality. How-ever, for the remaining leading causes of death,and for several other causes, Navajo mortality ex-ceeded that of U.S. all races in the 3-year periodcentered in 1981 (table 4-44).
The death rate from accidents, the leading causeof deaths in Navajo Indians of both sexes, ex-ceeded that of U.S. all races by 4 times, 4.5 timesfor males, and 3.5 times for females. Navajo maleswere 1.3 times as likely as U.S. all races malesto die from suicide, and l.5 times as likely to dieby homicide. Consistent with the high rate of
death by violence, the Navajo hospitalization ratefor injuries and poisonings was relatively high asIHS areas go (142.8 per 100,000 population; seetable 4-19), but the excess mortality among Navajoswould seem to warrant an even higher hospitali-zation rate. Outpatient encounters in Navajo rein-force the impression that social causes of morbid-ity and mortality are prevalent. The categories oflacerations and open wounds, superficial injuryor contusion, and fracture of the extremities ac-counted for 8.2 percent of male outpatient visitsin 1984 (see table 4-45).
The Navajo female death rate for diabetes alsoexceeded that of U.S. all races females, and thehigh female death rate from chronic renal failure

Ch. 4—Health Status of American Indians ● 135
Table 4-43.—Changes in Crude Death Rates, 1972-82:IHS Navajo Area (rate per 100,000 population)
PercentIHS 1972-74 1975-77 1980-82 changeCode Cause rate rate rate 1972-82
790800810310510150620740
430830820
All
Accidents/adverse effects . . . . . . . . .Motor vehicle accidents . . . . . . . .All other accidents . . . . . . . . . . . . .
Diseases of the heart . . . . . . . . . . . . .Pneumonia/influenza. . . . . . . . . . . . . .Malignant neoplasms . . . . . . . . . . . . .Liver disease/cirrhosis . . . . . . . . . . . .Conditions arising in
perinatal period . . . . . . . . . . . . . . . .Cerebrovascular disease . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . .Enteritis, other diarrheal disease . . .All other causes . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . .
241.7153.088.768.043.542.026.6
25.323.522.219.711.9
259.7784.1
196.8130.466.352.541.844.022.8
18.917.617.821.4
215.8648.6
155.190.253.858.726.851.614.1
8.913.913.211.8
185.1539.2
– 35,8–41 .0– 39.3– 13.6– 38.4
22.8–47.1
–64.7–41 .1– 40.2– 39.9
– 28.6–31 .2
SOURCES 1972-74 and 1975-77 deatha: U S Department of Health, Education and Welfare, Public Health Serwce, Health SerwcesAdministration, Ind!an Health Setvlce, Selected Vita) Statistics for /rtd/an /-/ea/th Sewice Areas and semlce Un(ts,1972 to 1977, DHEW Pub. No (HSA).79-1OO5 (Rockville, MD HSA, 1979) 1972.74 and 1975-66 population: U SDepartment of Health and Human SewIces, Pubilc Health Service, Health Resources and Sew!ces Admlnistratlon,Ind!an Health Service, Program Statistics Branch, internal documents, Rockvllle, MD, 1985 1960.82 data: U SDepartment of Health and Human Services, Public Health Service, Health Resources and Services Administration,Indian Health Service, computer tape supplied to the Office of Technology Assessment, Washington, DC, 1985
(22 deaths in the 1980-82 period, four times greaterthan the U.S. all races female rate) may be relatedto excess morbidity from diabetes. The Navajomale death rates from diabetes and renal failurealso exceeded the U.S. all races male rates, butnot by as much. It is interesting, then, that the1984 hospitalization rate for diabetes was 16.5 per10,000 population, a rate substantially below thatof U.S. all races (25.3) and the IHS on average(26.2).
Among IHS areas, the Navajo have a fairly lowinfant mortality rate (12.8 in 1980 to 1982), al-though it still exceeded that of U.S. all races (11.9in 1981). The postneonatal rate in Navajo (8.6),however, was more than twice that of U.S. allraces. Unlike most other areas, SIDS was not thesingle most significant cause of death amongNavajo postneonates. Eight Navajo infants diedof congenital anomalies of the heart, eight frommeningitis, and eight from SIDS in 1980 to 1982(175a).
Deaths from liver disease and cirrhosis were thefifth leading cause of death among the Navajo,although the death rate from this cause, 21.4 per100,000 population, was fairly low among IHSareas (an average of 48.1 per 100,000 IHS serv-ice population, compared to 11.4 for U.S. all
races), Navajo hospitalizations for alcoholic liverdisease (2.8 per 10,000 population in 1984) werelow relative to most other IHS areas (4.4), buthigher than those of U.S. all races. Hospitaliza-tions for mental disorders, including alcoholdependence syndrome, were extremely low inNavajo (a discharge rate of 38.3 per 10,000 pop-ulation) compared to the U.S. rate (72 per 10,000population), and even compared to the IHS aver-age rate (57 per 10,000 population). In addition,infant deaths from congenital anomalies may bedue to fetal alcohol syndrome, the prevention ofwhich has been the focus of a special effort amongIndians (77). Pneumonia mortality and morbid-ity may also be related to alcohol abuse (100);among the Navajo, pneumonia is the fourth lead-ing cause of death for both males and females.
In addition to disorders that lead eventually todeath, the Navajo had a high prevalence of otitismedia, upper respiratory infections, strep throat,and musculoskeletal and connective tissue dis-orders.
Thus, the Navajo area can be characterized asone whose health status has improved substan-tially in recent years and that has lower mortal-ity rates for some of the leading causes of deathin the general U.S. population—cancer, heart and

136 • Indian Health Care—
Table 4-44.—Fifteen Leading Causes of Deaths and Age-Adjusted Death Rates for Navajo IHS Area Indians 1980-82and U.S. All Races 1981
IHSRatio of Navajo
Number Age-adjusted mortality rate area Indians tocodea Rank Cause name of deaths Indians U.S. all races U.S. all races .Females:790 1.150 2.310 3.510 4.620 5.430 6.730 7.640 8.260 9.740 10.830 11.090 12.270 13.630 14.030 15.
ALL . . . .
Males:790 1.310 2.150 3.510 4.820 5.830 6.430 7.620 8.730 9.740 10.670 11.840 12.260 13.140 14.540 15.
ALL ., . .
Accidents/adverse effects. . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . . .Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes meilitus . . . . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Nutritional deficiencies . . . . . . . . . . . . . . . . . . . . .Cholelithiasis/gallbladder disease . . . . . . . . . . . .Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Accidents/adverse effects. . . . . . . . . . . . . . . . . . .Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . ....,., . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .Renal failure, et al . . . . . . . . . . . . . . . . . . . . . . . . .All other external causes . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .All other infectious/parasitic diseases . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
149132108503231282423131210876
267900
49615599704947313130271719181111
4031,514
71.385.662,723.920.516.6
7.913.215.33.55.75.93.34.03.7
143.8486.9
271.193.365.834.223,725.617.522.2
8.96.9
10.911.313.25.37.0
328.2845.1
20.4108.6135.1
9.27.4
35.45.53.69.68.24.32.40.40.70.4
69.2420.4
60.2271.2163.7
1 .61 .016.741.716.0
6.110.34.92.2
10.01.7
26.287.8
753.3
3.50.80.52.62.80.51.43.71.60.41.32.58.25.79.32.11.2
4.50.30.42.11.31.50.41.41.50.72.25.11.33.10.33.71.1
aEquivalence to ICD-9 code available from the Indian Health Service
SOURCES U.S.allraces:US Department of Health and Human Services, Public Health Service, National Center for Health Statistics, “Advancer eport,Finai MortatityStatistics, 1981:’ Month/y Vita/Statistics Ffepor733(3)supp., June22, 1984, Indianain IHS areaa: US Department of Health and Human Services, PublicHealth Ser(ice, Health Resources and Services Administration, Indian Health Service, computer tape suppiled to the Officeof Technology Assessment,Washington, DC, 1985
other cardiovascular disease, and chronic pulmo- population to be 190,451 in 1984. It further esti-nary disease. But it is an IHS area with one of mated that 49.6 percent of the Indian populationthe highest rates of death due to accidents, and of the State of OkIahoma, and 70.8 percent of thegreater than U.S. all races rates of death due to Indian population of the State of Kansas live inpneumonia and influenza, diabetes, and infectious urban areas.diseases. The high rate of death from accidents Oklahoma Indians appear to have relativelywas not accompanied by higher hospitalization favorable health statistics, although deaths amongrates for injuries. Indians may be underreported because Oklahoma
Indians are well-integrated into the general pop-
Oklahoma City Area ulation of Oklahoma. Higher rates of employment(209) may mean that Oklahoma Indians are more
The Oklahoma City area covers the State of likely to have sources of health care other thanOklahoma and a small part of the State of Kansas. those of IHS, which would also tend to under-IHS estimated the Oklahoma City area service state morbidity indicators taken from IHS patient

Ch. 4—Health Status of American Indians ● 137
Table 4-45.— Fifteen Most Frequent Outpatient Diagnoses:a Navajo Area, Fiscal Year 1984
IHSRank Code
Female:1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
Male:1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15,
— —
480300819250821080818210301823400575283022827
300250818730283821819575080301751022701210827
A L L
Clinical impressions
Prenatal care ., . . . . . . . ... , . . . . . . . . . . . . . . . . ... , . . . . . . . . . .Upper respiratory infections, common cold . . . . . . . . ... ... . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media. . . . . . . . . . . . . . . . . . ... . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . ..., . . . . . . . . . . . . . . . . . . . . .Diabetes meilitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care. . . . . . . . . ..., . . . . . . . . . . . . . . . . . . . . ..., . . . . . .Refractive error . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pharyngitis, tonsillitis, (nonstrep) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Urinary tract infection. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other muskuloskeletal, connective tissue diseases . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Strep throat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Upper respiratory infections, common cold . . . . . . . . . . . . . . . . . . . . .Acute otitis media. ,. ....., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care... . . . . . . . . . . . ..., . . . . . . . . . . . . . . . . . . . . . . . . . .Lacerations, open wounds . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ..., . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other muskuloskeletal, connective tissue diseases . . . . . . . . . . . . . .Diabetes mellitus . . . ..., . . . . . . . . . . . . . . . . . . . . . . . ..., ...,Pharyngitis, tonsillitis (nonstrep) . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Superficial injury, contusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Strep throat . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Fracture of extremity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Refractive error . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . ..., ..., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
All other causes, both sexes. ., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Number ofvisits
37,60833,59619,70219,54012,72811,67311,6298,8698,6448,5868,5288,4278,2677,951
13,082
24,88419,79111,85210,2988,4008,1077,5416,9986,9555,9625,9155,7885,5755,3128,427
337,515698,150
Percent oftotal visits
by sex
9.38.34.94.83.22.92.92.22.12.12.12.12.02,03.2
9.47.54.53.93.23.12.82.62.62.22.22.22.12.03.2
100.0alHS refers to these as cllnlcal ImpressIons, because they are recorded before a clinical diagnosis is completed; therefore, they may not be valid diagnoses
SOURCES 151eading cllnlcal impressions: US Department of Health and Human Services, Public Health Serv!ce, Health Resources and Services Admlnistratlon, lndi-an Health Servfce, “SpecialReporton 15 Leading Causes of Outpat!en! Care By Areaand Service Unit, State and County,” internal document, Albuquerque,NM 1985 Navaiototal:US Deoarfment of Health and Human Services. Public Health Service. Health Resources and Servtces Admlnfstration. lndlan HealthService, Off!ce ~f Planning, Evaluation and Legislation, Program Statlst!cs Branch, Surnmaryof Leadfrrg Causes forOufpat/ent Vis~ts, lndianf-lealth Serv(ceFac//lf~es, Fisca/ Year 1984 (Rockville, MD IHS, no date)
care data. Furthermore, the high population ofIndians living in urban areas tends to make morealternate sources of health care available, al-though as a practical matter access to health careeven in urban areas depends largely on socioeco-nomic status.
In the 1980-82 period, 2,873 Indians in theOklahoma City area were reported to have died,for an average age-adjusted mortality rate of 530.6per 100,000 population (table 4-46), a rate lessthan that of U.S. all races for 1981 (568.2). 0kla-homa Indians had lower death rates than the U.S.all races population for diseases of the heart,cerebrovascular disease, cancer, suicide, and in-
fant mortality, and had age-adjusted death ratesequal to that of the general population for con-ditions arising in the perinatal period and, unusualfor IHS areas, in the postneonatal period, Thecrude death rate declined 13 percent in the 1972to 1982 decade. Although the crude death ratefrom cancer increased unestimated 8.7 percent(see table 4-47), a rise in cancer rates incompati-ble with increasing life expectancy. However,Oklahoma Indians had other death rates and ra-ties resembling those of Indians in other IHSareas. Accidents were the third leading cause ofdeath at a rate of 66.9 for both sexes, a rate l.7times that of U.S. all races. Diabetes was the fifthleading cause of death, with a rate of 26.9 for both

138 • Indian Health Care
Table 4-46.—Fifteen Leading Causes of Deaths and Age-Adjusted Death Rates forOklahoma IHS Area Indians 1980.82 and U.S. All Races 1981
Ratio of OklahomaIHS Number Age-adjusted mortality rate area Indians tocodea Rank Cause name of deaths Indians US. all races U.S. all racesFemales:310 1.150 2.430 3.790 4.260 5.620 6.510 7.740 8.640 9.730 10.830 11.480 12.540 13.090 14.490 15.
ALL . . . .
Males:310 1.790 2.150 3.430 4.620 5.260 6.510 7.830 8.740 9.820 10.540 11.640 12.090 13.730 14.480 15.
ALL ., . .
Diseases of the heart . . . . . . . . . . . . . . . . . . . . . . 335Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . ., 211Cerebrovascular diseases . . . . . . . . . . . . . . . . . . . 109Accidents/adverse effects. . . . . . . . . . . . . . . . . . . 93Diabetes melitus . . . . . . . . . . . . . . . . . . . . . . . . . . 73Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . . 46Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . . 36Conditions arising inperinatal period . . . . . . . . 28Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Congenital anomalies . . . . . . . . . . . . . . . . . . . . . . 18Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Atherosclerosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Chronic pulmonary diseases . . . . . . . . . . . . . . . . 11Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Other arterial diseases . . . . . . . . . . . . . . . . . . . . . 8All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 175All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,209
Diseases of the heart . . . . . . . . . . . . . . . . . . . . . . 494Accidents/adverse effects . . . . . . . . . . . . . . . . . . . 251Malignant neoplasms . . . . . . . . . . . . . . . . . . . . . . . 239Cerebrovascular diseases . . . . . . . . . . . . . . . . . . . 73Liver disease/cirrhosis.. . . . . . . . . . . . . . . . . . . . . 69Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . 59Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . . 51Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Conditions arising in perinatal period . . . . . . . . 32Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Chronic pulmonary diseases . . . . . . . . . . . . . . . . 28Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Septicemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Congenital anomalies . . . . . . . . . . . . . . . . . . . . . . 11Atherosclerosis. . . . . . . . . . . . . . . . . . . . . . . . . . . . 9All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 239All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,664
96.572.830.034.527.019.19.98.88.16.07.43.53.72.72.7
60.6393.3
208.8101.2102.329.332.327.018.817.9
9.712.211.8
7.36.53.53.0
101.4693.0
135.1108.635.420.4
9.67.49.28.23.65.54.34.69.52.43.0
53.6420.4
271.260.2
163.741.716.010.016.616.710.318.026.2
5.63.46.16.0
81.6753.3
0.70.70.81.72.82.61.11.12.31.11.70.80.41.10.91.10.9
0.81.70.60.72.02.71.11.10.90.70.51,31.90.60.51.20.9
aEquivalenc. t. ICD.g code available from the Indian Health Sewice.
SOURCES: U.S.all racea:U.S. Department of Health and Human Services, Public Health Service, National CenterforHealth Statistics, “Advance Report, Final MortalityStatistics, 1981,’’ Month/y Vl!a/ Statistics Repor’f 33(3)supp. June 22, 1984; lndlanainlHSaraaa: U.S. Departmentof Health and Human Services, PublicHealth Service, Health Resources and Services Administration, Indian Health Service, computer tape supplied to the Office of Technology Assessment,Washington, DC, 1985.
sexes, equal to 2.7 times the U.S. all races rate. In addition to problems of interpretation causedLiver disease and cirrhosis was the sixth leading by the presence of alternative health care sources,cause of death, with a rate of 25.4, 2.2 times the hospitalization rates for Oklahoma Indians arerate of U.S. all races. Pneumonia and influenza, difficult to interpret because IHS does not collectthe seventh leading cause of death, had a rate of diagnostic data on the tribally administered hos-13.7, a ratio of l.0 for females and 1.1 for males pital in the Claremore service unit. For this re-compared to the U.S. population. Homicide was port, hospitalization rates were derived by exclud-the eighth leading cause of death at a rate of 12.6 ing only the Claremore service unit populationfor both sexes, equal to a ratio of l.7 for females, from the population denominator, which mayand l.0 for males when compared to the U.S. pop- tend to overstate hospital discharge rates. Never-ulation. The crude death rate for motor vehicle theless, some hospital discharge rates are whataccidents increased by almost 13 percent between might be expected, or even lower than expected,1972 and 1982. given the pattern of mortality. Thus, for exam-

. — —
Ch. 4—Health Status of American Indians ● 139
Table 4-47.—Changes in Crude Death Rates, 1972-82:IHS Oklahoma Area (rate per 100,000 population)
PercentIHS 1972-74 1975-77 1980-82 changeCode Cause rate rate rate 1972-82
310150790800810430260620510830740
820
ALL
Diseases of the heart . . . . . . . . . . . . .Malignant neoplasms . . . . . . . . . . . . .Accidents/adverse effects . . . . . . . . .
Motor vehicle accidents . . . . . . . . .All other accidents . . . . . . . . . . . . .
Cerebrovascular disease . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . .Liver disease/cirrhosis . . . . . . . . . . . .Pneumonia/influenza. . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in
perinatal period . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . .All other causes . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . .
186.678.171.240.031.149.927.024.222.915.1
9.68.5
130.2623.3
164.981.066.040.925.045.623.834.424.812.1
13.37.0
119.0651.9
156.584.964.945.119.834.424.921.716.411.5
11.36.6
109.2542.3
– 16.18.7
– 8.812.8
– 36.3–31 .2
– 7.7– 10.3– 28.3– 23.8
17.8–22.2– 16.1– 13.0
SOURCES 1972.74 and 1975-77 deaths: U S Department of Health, Education and Welfare, Public Health Service, Health SerwcesAdministration, Indian Health Service, Selected Vita/ Statisffcs for Indian Health Service Areas and Service Units,1972 to 1977, DH EW Pub No (HSA).79-1OO5 (Rockville, MD” HSA, 1979). 1972.74 and 1975.66 population: U SDepartment of Health and Human Services, Public Health Service, Health Resources and Services Administration,lndlan Health Service, Program Statistics Branch, internal documents, Rockville, MD, 1985 1960-62 data: U.SDepartment of Health and Human Services, Publlc Health Service, Health Resources and Services Administration,Indian Health SewIce, computer tape supplied to the Off Ice of Technology Assessment, Washington, DC, 1985
pie, the hospitalization rate for injuries andpoisonings (74.6 per 10,000 service population)seems low relative to the area’s death rates for ac-cidents and homicide. The same can be said forhospitalizations for diabetes; even though theOklahoma death rate exceeded that of U.S. allraces, the area’s hospitalization rate for diabetes(23.5 per 10,000 population, excluding Claremore)is about the same as that of U.S. all races.
Hospitalizations for conditions arising in theperinatal period (14.7 per 10,000 population in1984) were higher than expected—more than twicethe rate for U.S. short-stay non-Federal hospitals(7.1)–given that the infant mortality rate in theOklahoma area was lower than that of U.S. allraces in the 1980-82 period. The Oklahoma 1979hospitalization rate for conditions arising in theperinatal period (5.7) was closer to what mighthave been expected in 1980 to 1982, as was the1979 hospitalization rate for pregnancies withcomplications (36 percent of hospitalizations forpregnancies (166)).
Outpatient visits in Oklahoma are similar tothat for the general U.S. population (i. e., highproportions of visits for hypertension, upper res-piratory infections, prenatal care, well child care),except for higher percentages of care for refrac-
tive disorders and diabetes relative to the U.S. allraces population (table 4-48) (200).
Phoenix Area
The Phoenix area served an estimated 82,309Indians in 1984, primarily in Arizona. Indians inNevada and Utah are also included in the Phoe-nix service area.
As shown in table 4-49, the mortality rate inthe Phoenix area has declined almost 20 percentsince the 3-year period centered in 1972 to 1974,although changes in Phoenix area health statusare difficult to interpret. The boundaries of theservice area have changed since the early 1970swhen the Phoenix area included small service unitsin Idaho, Oregon, and California (157). Oneshould be cautious in drawing conclusions fromhospitalization data as well, because the Phoenixarea is the site of the Phoenix Indian Medical Cen-ter, a teaching and referral hospital of IHS.
In 1980 to 1982 the Phoenix area age-adjustedmortality rate was 918.2 for all causes, 1.6 timesthe U.S. all races rate (see table 4-so). The leasi-ing cause of the 1,711 deaths in the area in 1980to 1982 was accidents, which occurred at a rate3.8 times the U.S. all races rate for males and 3.9

140 ● Indian Health Care—
Table 4-48.–Fifteen Most Frequent Outpatient Diagnoses:a Oklahoma Area, Fiscal Year 1984
Percent of —
IHS Number of total visitsRank Code Clinical impressions visits by sex
Female:1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
Male:1.2.3.4.5.6.
7.8.9.
10.11.12.13.14.15.
480819283080210300818823250821400461575301827
283300819080210818250305823575520301355821827
ALL
Prenatal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Refractive error . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Urinary tract infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other gynecologic problems . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other musculoskeletal, connective tissue diseases . . . . . . . . . . . . . .Pharyngitis and tonsillitis (nonstrep) . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Refractive error . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Respiratory allergy, asthma, and hay fever . . . . . . . . . . . . . . . . . . . . . .Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other musculoskelatal, connective tissue disease . . . . . . . . . . . . . . .Other diseases of the skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pharyngitis and tonsillitis (nonstrep) . . . . . . . . . . . . . . . . . . . . . . . . . . .Diseases of teeth, gums . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
All other causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31,19928,93626,67622,38519,20617,51811,28110,92610,0659,7127,6186,8126,0145,847
37,199
18,15313,19112,84812,34112,32811,12010,3105,2925,0784,4814,0914,0334,0063,579
19,818
269,179661,217
7.67.06.55.44.74.22.72.62.42.41.81.71.51.49.0
7.75.65.55.25.24.74.42.32.21.91.71.71.71.58.4
100.0alHS ~efer~ t. these as clinical ,mpre~~lon~, becau~e they are recorded before acllnical diagnosis is completed; therefore, they may not be valid diagnoses,
SOURCES151 eadlngcllnical lmpreaalona: U.S. Department of Health and Human Sewices, Public Health Service, Health Resources and Sewices Administration, lndi-an Health Service, “SpecialReport on 15 Leading Causes ofOutpatient Care By Areaand Service Unit, State and County,” internal document, Albuquerque,NM, 1985. Oklahoma totaLU S. Departmentof Health and Human Services, Public Health Service, Health Resources and Sewices Administration, IndianHealth Semice, Office of Planning, Evaluation and Legislation, Program Statistics Branch, Surnrnaryof L.eadirrg Causes forOutpatierrt Visits, /rrdian Hea/thService Faci/ifies, Fiscal Year 1984 (Rockvflle, MD: IHS, no date)
times the U.S. all races rate for females. Deaths Outpatient information confirms the prevalencefrom other forms of violence also ranked high in of violent injury among Phoenix area Indians. To-the Phoenix area. Suicide was the sixth leading gether, lacerations and open wounds; disloca-cause of death for males, at a rate 2.6 times that tions, sprains and strains; superficial injuries andof U.S. all races males, and the male death rate contusions; and fractures of the extremities ac-as a result of homicide was 3.2 times that of U.S. counted for 9.6 percent of male outpatient visitsall races males. Although the 1984 Phoenix area in 1984 (see table 4-51).hospitalization rate for injuries and poisoningswas almost double that of U.S. short-stay non- Diseases of the heart were the second leadingFederal hospitals (table 4-19), the ratio between cause of death for Phoenix area Indians in 1980Phoenix and U.S. hospital discharges was still to 1982, and cerebrovascular disease the ninth.lower than the ratio of combined mortality rates The U.S. all races population had higher rates offor deaths by external cause (3,3, the average of death from these cardiovascular diseases, andthe ratios for accidents, suicide, homicide, and all from malignant neoplasms, which were the thirdother external causes). leading cause of death for Phoenix area females

Ch. 4—Health Status of American Indians • 141
Table 4-49.–Changes in Crude Death Rates, 1972-82:IHS Phoenix Area (rates per 100,000 population)
PercentIHS 1972-74 1975-77 1980-82 changeCode Cause rate rate rate 1972-82
790800810310620510150820830740
480030
ALL
Accidents/adverse effects . . . . . . . . .Motor vehicle accidents . . . . . . . . .All other accidents . . . . . . . . . . . . .
Diseases of the heart . . . . . . . . . . . . .Liver disease/cirrhosis . . . . . . . . . . . .Pneumonia/influenza. . . . . . . . . . . . . .Malignant neoplasms . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in
perinatal period . . . . . . . . . . . . . .Atherosclerosis . . . . . . . . . . . . . . . . . .Tuberculosis. . . . . . . . . . . . . . . . . . . . .All other causes ., . . . . . . . . . . . . . . .All causes. . . . . . . . . . . . . . . . . . . . . . .
210.7129.281.499.783.856.051.332.426.5
17.116.510.6
306.2910.8
175.8104.171.697.867.549.754.932.431,9
21.4
284.4815.8
136.580.556.0
130.065.636.353.830.234.1
12.72.63.1
243.8748.7
– 35.2– 37.7–31 .2
30.4–21 .7– 35.1
4.9– 6.828,8
– 25.8– 84.2– 70.1– 20.4– 17.8
alnclude~ atherosclerosis and tuberculosis, rates unknown
SOURCES 1972.74 and 1975-77 deaths: U S Department of Health, Educat!on and Welfare, Publlc Health Sewice, Health SerwcesAdministration, Indian Health Service, Selected V/ta/ Stafist/cs for Irrdi.?rr /-/ea/fh Service Areas and Service Ur?Its,1972 to 1977, DHEW Pub No (HSA)-79.1OO5 (Rockville, MD HSA, 1979). 1972.74 and 1975-66 population: U SDepartment of Health and Human Services, Public Health Service, Health Resources and Services Administration,Indian Health Service, Program Statistics Branch, Internal documents, Rockville, MD, 1985 1980-82 data: U SDepartment of Health and Human Services, Public Health Service, Health Resources and Services Admlnlstratlon,Indian Health Service, computer tape supplied to the Off Ice of Technology Assessment, Washington, DC, 1985
and the fourth for Phoenix area males. The com-paratively low rate of hospitalization in the Phoe-nix area for circulatory system diseases is some-what consistent with these cardiovascular deathrates, if a bit low compared to U.S. all races rates.Phoenix area hospitalization rates for cancer (16.9per 10,000 population) were also well below theU.S. average in 1984 (87.8 per 10,000 population).
Despite a decline in the mortality rate from di-abetes mellitus between 1975 to 1977 and 1980 to1982, the disease was responsible for the deathsof 28 Phoenix area males and 44 females in the1980-82 period, making diabetes the seventh lead-ing cause of death. Deaths from renal failure andhospitalizations and outpatient encounters for dia-betes were also indications of the incidence andseventy of diabetes in the Phoenix area. Renal fail-ure accounted for 30 deaths in 1980 to 1982, equalto 3.7 times the U.S. all races male death rate,and 5.9 times the U.S. all races female death rate.The Phoenix death rate from kidney disorders(nephritis, et al.) was one of the highest in the IHSsystem in 1980 to 1982 (see table 4-7). Hospitali-zation rates for diabetes in Phoenix (49.4 per10,000 population) were almost double the U.S.all races and IHS al] areas average rates in 1984,In 1984, diabetes was the leading cause of out-
patient visits among Phoenix area women and thesecond leading cause of outpatient visits amongPhoenix area men, accounting for 19,514 femalevisits and 10,806 male visits, resulting in a rateof 3,683.6 visits per 10,000 population. (ThePhoenix area is the site of a long-term epidemio-logical study of diabetes among the Pima Indians. )
The death rate from pneumonia was also mark-edly high in the Phoenix area, 3.3 times the U.S.all races rate for males (50 Phoenix area deaths)and 3.7 times the U.S. all races rate for females(33 Phoenix area deaths). Consistent with the rela-tively high rate of deaths from pneumonia, up-per respiratory infections were a leading cause ofoutpatient visits in 1984 (table 4-51). Hospitali-zation rates for respiratory system disease (200. Iper 10,000 population in 1984) substantially ex-ceeded the U.S. short-stay non-Federal hospitalrate.
The death rate from liver disease and cirrhosiswas particularly high in Phoenix. Ninety-six malesand 54 females died from liver disease and cir-rhosis in 1980 to 1982, at rates 7.3 and 8.2 timesthe U.S. all races rate, making this the third lead-ing cause of death in the area. The Phoenix hos-pitalization rate for alcoholic liver disease was

142 ● Indian Health Care
Table 4-50.—Fifteen Leading Causes of Deaths and Age-Adjusted Death Rates for Phoenix IHS Area Indians 1980-82and U.S. All Races 1981
Ratio of PhoenixIHS Number Age-adjusted mortality rate area Indians tocodea Rank Cause name of deaths Indians U.S. all races U.S. all races
Females:310 1.790 2.150 3.620 4.260 5.510 6.430 7.830 8.640 9.740 10.820 11.730 12.090 13.480 14.490 15.
ALL . . . .
Males:790 1.310 2.620 3.150 4.830 5.820 6.510 7.430 8.260 9.640 10.740 11.090 12.540 13.730 14.840 15.
ALL . . . .
Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Accidents/adverse effects. . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Atherosclerosis. . . . . . . . . . . . . . . . . . . . . . . . . . . .Other arterial disease . . . . . . . . . . . . . . . . . . . . . .All others. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Accidents/adverse effects . . . . . . . . . . . . . . . . . . .Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Malignant neoplasm.. . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .Septicemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .All other external causes . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1208758544433272017151412
655
128645
225117966558555035281814
9988
2711,066
133.078.966.460.552.331.729.218.320.710.010.79.55.73.85.7
126.5662.9
227,2229.4116.9
87.153.546.252.640.037.522.5
9.411.310.85.86.8
244.61,201.6
135.120.4
108.67.49.69.2
35.44.33.68.25.75.52.44.63.0
57.4420.4
60.2271.2
16.0163.7
16.718.016.641.710.0
5.610.33.4
26.26.12.2
85.4753.3
1.03.90 . 68.25.43.50.84.25.71.21.91.72.40.81.92.21.6
3.80.87,30.53.22.63.21.03.84.00.93.30.41.03.12.91.6
aEquivalence t. ICD.9 code available from the Indian Health Sewice
SOURCESU.S. aIlraces: U.S. Department of Health and Human Services, Public Health Service, National Center for Health Statistics, “Advancer eport,F inal MortalityStatistics, 1981,’’ Morrtfrly Vifal Sfafistics Repoti 33(3)supp., June 22, 1984; Indianshr IHS areas: U.S. Departmentof Health and Human Services, PubllcHealth Service, Health Resources and Services Administration, Indian Health Service, computer tape suppliedto the Office of Technology Assessment,Washington, DC, 1985
more than 12 times the rate in U.S. short-stay non- areas. On all of the 10 leading causes of death inFederal hospitals, and Phoenix area hospitalize- the 3-year period centered in 1973, there had beention rates for alcohol-related mental disorders also at least a 37-percent decline in the crude mortal-exceeded the rates in U.S. short-stay non-Federal ity rate by 1980 to 1982, including diseases of thehospitals. heart, malignant neoplasms, and suicide, which
sometimes rose or showed no improvement in
Portland Area other IHS areas (see table 4-52). However, thechanging composition of the Portland service area
Judging from changes in crude mortality rates, (179,166) should be taken into account when com-the Portland area, which in 1984 served 96,427 paring mortality rates over time. The populationIndians in the reservation States of Washington, of the Portland area increased by almost 300 per-Oregon, and Idaho, has experienced the most dra- cent in the decade between 1972 and 1982 (see ta-matic improvement in health status of the IHS ble 4-3 and 4-4). The mortality rate (adjusted for

Ch. 4—Health Status of American Indians ● 143—
Table 4-51.— Fifteen Most Frequent Outpatient Diagnoses:a Phoenix Area, Fiscal Year 1984
Percent ofIHS Number of total visits
Rank Code Clinical impressions visits by sex
Female:1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.Male:
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
080480300819250283818210305823400575821014827
300080250818730283819821305702210731575701014
ALL
Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Prenatal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Refractive error . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Respiratory allergy, asthma and hay fever . . . . . . . . . . . . . . . . . . . . . .Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Urinary tract infection. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other muskuloskeletal, connective tissue diseases . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Gastroenteritis, diarrhea, etc., no other symptoms. . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Laceration, open wound. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease ., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Respiratory allergy, asthma, and hay fever. . . . . . . . . . . . . . . . . . . . . .Dislocations, sprains, and strains . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Refractive error . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Superficial injury, contusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other muskuloskeletal, connective tissue diseases . . . . . . . . . . . . . .Fracture of extremity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Gastroenteritis, diarrhea, etc., no other symptoms . . . . . . . . . . . . . . .
All other causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19,51417,52114,28911,93210,5088,4098,2597,0506,3486,1695,9064,9084,2884,1955,974
10,80610,56610,4198,0227,1077,0816,4264,3234,2933,8543,7273,6983,6563,5953,538
219,389445,770
7.56.75.54.64.03.23.22.72.42.42.31.91.61.62.3
6.36.26.14.74.14.13.72.52.52.22.22.22.12.12.1
100.0afHS ~efer~ t. these as clinical ,mpre~~lon~, because they are recorded before a clinical diagnosis is completed, therefore, they may flOt be valid diagnoses
SOURCES 151eading clinical impressions: U.S Department of Health and Human SewIces, Pubhc Health Service, HealthResources and Services Administration, lndi-an Health Servfce “Special Reporton 15 Leading Causes of Outpatient Care By Area and Sewlce Unit, State and County, “ internal document, Albuquerque,NM,1985 Phoenix total:US Department of Health and Human Services, Public Heaith Serv!ce, Health Resources and Services Administration, lndlan HealthSerwice, Off!ceof Planning, Evaluation and Leglslat!on, Program Statistics Branch, Surnrnary of Leading Causes for Outpatient Visits, /ndiarr Hea/th SerwceFaclhties, Fisca/ Year 1984 (Rockvflle MD IHS, no date)
age) in the Portland area in 1980 to 1982 remained mortality rate exceeded the U.S. all races femalesignificantly above that of U.S. all races: 749.8 rate by almost 9 times.per 100,000 population compared to the U.S. allraces rate for 1981 of 568.2, for a ratio of l.3 (1.4for females and l.2 for males; table 4-53).
As in most other IHS areas, the leading causesof death among Portland males were from acci-dents, particularly motorvehicle accidents. Liverdisease, suicide, and homicide death rates also ex-ceeded the U.S. all races rates for males. Althoughdeaths from diseases of the heart took more fe-male lives than did the social causes, the accidentmortality rate for females still was 3.7 times theU.S. all races female rate, and the liver disease
Because of the way medical care is provided inthe Portland area, hospitalization and outpatientdata are almost impossible to use as indicators ofmorbidity and mortality. Portland has no directcare hospital, so all inpatient care must be pur-chased through contract care, which has been se-verely restricted in recent years (see ch. 6). Thus,although Portland experienced a high death ratefrom violent causes in 1980 to 1981, the hospitaldischarge rate for injuries and poisonings wasalmost the lowest of the IHS areas in 1984. In1979, the number of discharges for injuries and

144 ● Indian Health Care
Table 4-52.—Changes in Crude Death Rates, 1972.82:IHS Portland Area (rates per 100,000 population)
PercentIHS 1972-74 1975-77 1980-82 changeCode Cause rate rate rate 1972-82 a
790
810310620150430510820740
830260
ALL
Accidents/adverse effects . . . . . . . . . 254.5Motor vehicle accidents . . . . . . . . . 152.0All other accidents . . . . . . . . . . . . . 102.4
Diseases of the heart . . . . . . . . . . . . . 219.2Liver disease/cirrhosis . . . . . . . . . . . . 121.2Malignant neoplasms . . . . . . . . . . . . . 79.3Cerebrovascular diseases . . . . . . . . . 73.8Pneumonia/influenza. . . . . . . . . . . . . . 59.5Suicide . . . . . . . . . . . . . . . . . . . . . . . . . 39.6Conditions arising in
perinatal period . . . . . . . . . . . . . . . . 35.2Homicide . . . . . . . . . . . . . . . . . . . . . . . 34.1Diabetes meilitus . . . . . . . . . . . . . . . . 29.7All other causes . . . . . . . . . . . . . . . . . 268.2All causes . . . . . . . . . . . . . . . . . . . . . . . 1,214.3
163.8104.6
59.1155.678.261.835.440.932.7
25.416,312.7
170.0792.8
117.671.546.1
116.750.849.528.416.822.0
15.515.516.8
137.3586.9
–53.8–53.0–55.0–46.8–58.1–37.6–61 .5–71 .8–44.5
– 56.0– 54.5–43.5–48.8–51 .7
aMay be invalid due to changes in population covered,
SOURCES: 1972.74 and 1975-77 deaths: US, Department of Health, Education and Welfare, Public Health Service, Health ServicesAdministration, Indian Health Service, Selected Wtal Stat/sfics for /rid/an Hea/th Service Areas and Servke Units,1972 to 1977, DHEW Pub. No, (HSA)-79-1CXJ5 (Rockville, MD: HSA, 1979). 1972.74 and 1975-66 population: US.Department of Health and Human Services, Public Health Service, Health Resources and Services Administration,Indian Health Service, Program Statistics Branch, internal documents, Rockville, MD, 1985 1980-82 data: U SDepartment of Health and Human Services, Public Health Service, Health Resources and Services Administration,Indian Health Service, computer tape supplied to the Office of Technology Assessment, Washington, DC, 1985
poisonings (166 discharges) was greater than in1984, even though the Portland area populationwas 27 percent lower in 1979 than in 1984. Thissituation is characteristic of the Portland area ingeneral: the total number of hospital dischargeswas 4,210 in 1979 and 4,222 in 1984, which, whenadjusted for the rise in population, was a substan-tial decline. The 1984 proportion of outpatientvisits for trauma was more consistent with Port-land’s mortality rate from those causes relativeto other IHS areas: of the 15 leading reasons foroutpatient visits among males, lacerations andopen wounds accounted for 1.9 percent; and dis-locations, sprains, and strains accounted foranother 1.8 percent (see table 4-54).
Although more males than females in the Port-land area died from diabetes in 1980 to 1982, thefemale death rate from renal failure was consider-ably worse than the male death rate. It is alsonoteworthy that refractive error was not amongthe leading causes of outpatient visits for eithermales or females, reportedly an effect of the limi-tation on contract care expenditures.
Although cardiovascular diseases and malig-nant neoplasms were leading causes of death forPortland area males and females, deaths fromthese causes did not exceed the U.S. all races rates.
As was typical of IHS areas, however, hyperten-sive disease was one of the five leading causes ofoutpatient visits for males and females in the Port-land area.
The infant mortality rate in 1980 to 1982 was16,9 per 1,000 live births, compared to the 1981U.S. all races rate of 11.9. Causes of mortalityvaried, although for neonates, a large portion wasattributable to respiratory distress (see table 4-55).The Portland 1980 to 1982 mortality rate forSIDS, the leading cause of death among post-neonates, was the worst of the IHS areas (see fig-ure 4-16). It is noteworthy that outpatient visitsfor prenatal care, usually one of the five leadingreasons for female encounters (194), was the 15thleading reason in Portland, accounting for 2,400visits, or 1.7 percent. However, many pregnan-cies in the Portland area are apparently referredout of the IHS system because obstetricians arenot available. IHS records show that in 1984 anadditional 576 visits for prenatal care were madeto non-IHS facilities, but not all non-IHS visitsare coded and recorded for diagnosis, so it is im-possible to estimate the amount of prenatal caregiven in the Portland area.
The high infant mortality rate may be relatedto a high rate of alcohol abuse among Portland

Ch. 4—Health Status of American Indians . 145
Table 4-53.—Fifteen Leading Causes of Deaths and Age-Adjusted Death Rates forPortland IHS Area Indians 1980.82 and U.S. All Races 1981
IHSRatio of Portland
Number Age-adjusted mortality rate area Indians toc o d ea Rank Cause name of deaths Indians
Females:310 1.790 2.150 3.620 4.430 5.510 6.260 7.640 8.830 9.740 10.820 11.540 12.090 13.730 14.420 15.
ALL . . .
Diseases of the heart . . . . . . . . . . . . . . . . . .Accidents/adverse effects, . . ... . . . . . . . . . .Malignant neoplasm. . . . . . . . . . . . . . . . . . . . . .,Liver disease/cirrhosis . . . . . , . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al ., . . . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . ... , . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . ... . . . . . . . . . .Cogenital anomalies . . . . . . . . . . . . . . . . . . . . . .Hypertension with or without renal disease .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Males:790 1.310 2.620 3.150 4.820 5.430 6.260 7.740 8.830 9.510 10.540 11.730 12.840 13.640 14.090 15.
ALL ...,.. .aEqu!val~nce t. ICD.9 code available from the Indian Health service.
Accidents/adverse effects. . . . . . . . . . . . . . . . . . .Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .All other external causes . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . .Septicemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . ...,
113845655342015141412
87664
102550
18915863594332242422191310
754
141813
129.776.167.664.539.120.617.816.513.88.06.17.77.04.04.4
105.7588.6
176.2215.5
79.280.736.441.231.715.820.523.618.37.58.46.54.9
154.8921.2
U.S. all races U.S. all races
135.120,4
108.67.4
35.49.29.63.64.38.25.79.52,45.51.7
53.8420.4
60.2271,2
16.0163.7
18.041.710.010.316,716.626.2
6.12.25,63.4
85.4753.3
1.03.70.68.71.12.21.94.63.21.01.10.82.90.72.62.01.4
2.90.85.00.52.01.03.21.51.21.40.71.23.81.21.41.81.2
SOURCES U.S. allraces:US Department of Health and liuman Services, Publlc Health Service, National Center for Health Statistics, “AdvanceReport, F!nal MortahtyStat!stlcs, 1981 “ Monthly V/tal Sfat{stics Report 33(3) supp , June 22, 1984, Indians in IHS areaa: US. Departmentof Health and Human Services, PubllcHealth Serv!ce, Health Resources and Serwces Administration, Indian Health Serv!ce, computer tape suppl!ed to the Office of Technology Assessment,Washington, DC, 1985
area females, a hypothesis which is supported byanecdotal reports to OTA of alcohol abuse in thePortland area, and by vital statistics data indicat-ing that the 1980 to 1982 Portland area femaledeath rate from liver disease and cirrhosis was 8.7times the U.S, all races rate for females. The liverdisease and cirrhosis rate was also markedly highamong Portland males. Liver disease and cirrho-sis was the third leading cause of death amongPortland area males, accounting for 63 deaths in1980 to 1982, a rate 5 times that of U.S. all racesmales. Another indication of the prevalence of al-cohol abuse in the Portland area was the hospi-
tal discharge rate of 1.3 per 10,000 population foralcoholic liver disease, which was comparable tothe rate in U.S. short-stay non-Federal hospitalsof 1.6 despite the overall decline in hospitaliza-tions in Portland. However, hospital dischargerates for alcohol dependence syndrome and alco-holic psychoses were lower in Portland than inU.S. short-stay non-Federal hospitals and havedeclined markedly from 1979 (166). No mentaldisorders of any kind, including those related toalcohol abuse, were among the 15 leading causesof outpatient visits in 1984, although they wereamong the leading causes of visits in several serv-

146 • Indian Health Care
Table 4-54.— Fifteen Most Frequent Outpatient Diagnoses:a Portland Area, Fiscal Year 1984
Percent ofIHS Number of total visits
Rank Code Clinical impressions visits by sex.Female:1.2.3.4.5.6.
7.8.9.
10.11.12.13.14.15.
1.2.3.4.5.6.7.8.9.
10.11.12.13.14,15.
300819080283250823818305575510812821550480827
300819250283818080823821305575730510702812827
ALL
Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Respiratory allergy, asthma, and hay fever . . . . . . . . . . . . . . . . . . . . . .Other musculoskeletal, connective tissue disease . . . . . . . . . . . . . . .Eczema, urticaria, or skin allergy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other ill-defined, undiagnosed disease. . . . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Rheumatoid arthritis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Prenatal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Acute otitis media . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tests only (lab, X-ray) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Respiratory allergy, asthma, and hay fever . . . . . . . . . . . . . . . . . . . . . .Other musculoskeletal, connective tissue diseases . . . . . . . . . . . . . . .Laceration, open wound . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Eczema, urticaria, or skin allergy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Dislocations, sprains, and strains . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other ill-defined, undiagnosed diseases . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
All other causes, both sexes. ..,.... . . . . . . . . . . . . . . . . . . . . . . . . .All causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
13,2329,7575,9785,4924,9744,5924,0663,8112,9522,8142,7152,6802,6662,4004,025
9,2665,3494,8124,5123,8393,6172,5172,3132,3101,8971,7131,6321,5981,5912,776
114,028235.924
9.57.04.33.93.63.32.92.72.12.02.01.91.91.72.9
10.25.95.35.04.24.02.82.52.52.11.91.81.81.83.1
100.0afHS ~efer~ t. these as ~linical impre~~ions, be~ause they are recorded before a clinical diagnosis iS completed; therefore, they may not be valid diagnoses.
SOURCES: 151eadlrrg clinical lmpresalons: US. Department of Health and Human Services, Public Health Service, Health Resources and Sendces Administration, lndi-an Health Service, “SpecialReport on 15 Leading Causesof Outpatient Care ByAreaand Service Unit, State and County,” internal document, Albuquerque,NM, 1985, Portland lotak U.S. Department of Health and Human Sewlces, Pubiic Health Service, Health Resources and Services Administration, Indian HealthService, Officeof Planning, Evaluation and Legislation, Program Statistics Branch, SurnrnaryofLeadirrg Causes forOufpatierrt Vlslfs, /ndian Hea/thSemlceFacl/ifies, Fkxa/ Year 1984 (Rockville, MD” IHS, no date)
ice units. These figures do not, however, include eases. Thus, it seems particularly inconsistent forthe facilities which are funded under Self-Deter- the hospital discharge rate for diseases of the mus-mination legislation and by Portland area Indian culoskeletal system to be 18.6 per 10,000 popu-tribes (76). lation, far lower than the U.S. short-stay non-
Certain other problems that do not appear asunderlying causes of death have been noted asparticular problems in the Portland area. Besidesthe usual high number of outpatient encountersfor otitis media and diabetes, rheumatoid arthri-disappears to be unusually prevalent in Portlandarea females. In 1984, this autoimmune diseaseaccounted for 2,666, or 1.9 percent, of femalevisits in the Portland area on average. Another2,952 female and l,897 male visits were attributedto other musculoskeletal and connective tissue dis-
Federal hospital average and the average in otherIHS areas. Skin diseases, including eczema andurticaria, were also among the leading causes ofoutpatient visits in the Portland area, making itall the more surprising that the area had the lowesthospital discharge rate (8.7 per 10,000 population)for such diseases in 1984, declining from a rateof 14.3 in 1979.
In summary, Portland area Indians suffer frommuch the same diseases and risk factors for ill-ness and injury that Indians in other IHS areas

.——
Ch. 4—Health Status of American Indians • 147
Table 4-55.—infant Deaths and Death Rates IHS Portland Area, 1980-82
IHS Deaths Rates (per 1,000 live births)
c o d ea C a u s e Total Neonates Postneonates Total Neonates Postneonates
010040130150160170200240380
500580590600610680ALL
Intestinal infection . . . . . . . . . . .Septicemia . . . . . . . . . . . . . . . . . .Meningitis. . . . . . . . . . . . . . . . . . .Acute URI . . . . . . . . . . . . . . . . . . .Bronchitis , . . . . . . . . . . . . . . . . . .Pneumonia/influenza. . . . . . . . . .Other respiratory diseases. . . . .Congenital anomalies . . . . . . . . .Conditions arising in
perinatal period . . . . . . . . . . . .Respiratory distress . . . . . . . . . .Symptoms/signs/other . . . . . . . .
SIDS . . . . . . . . . . . . . . . . . . . . . .Symptoms/signs/other . . . . . .
Accidents/adverse effects . . . . .All other causes . . . . . . . . . . . . .All . . . . . . . . . . . . . . . . . . . . . . . . .
1111111
14
36114443
112
104
—
——
3611————1
46
11111115
——
4443
111
58
0.2 —0!2 —0.2 —0.2 —0.2 —0.2 —0.2 —2.2 1.4
5.6 5.61.7 1.76.9 —6.7 —0.2 —0.2 —0.3 0.2
16.9b 7.2
0.20.20.20.20.20.20.20.8
——6.96.70.20.20.29.7b
alHS code, equivalence to ICD-9 Recode 61 for infant deaths available from IHS.bwi~l not totat due to rounding error
SOURCE. U.S. Department of Health and Human Services, Public Health Service, Health Resources and Services Admln!strat!on, Indian Health Serwce, computer tapesupplied to the Office of Technology Assessment, Washington, DC, 1985
do. Accidents, diabetes, and liver disease can besaid to be epidemic among Portland area Indians,and in 1980 to 1982 the postneonatal mortalityrate was the highest of IHS areas. In addition,Portland area Indians appear to suffer dispropor-tionately from skin diseases and rheumatoid ar-thritis. Health status data indicate that restrictionson contract care funds may be affecting the avail-ability of health services to Portland area Indians.
Tucson Area
The IHS Tucson area is located in South Cen-tral Arizona. It is the smallest of the IHS areas,with a service population estimated to be 17,852in 1984.
As in all IHS areas, the crude death rate in Tuc-son declined in the decade between 1972 and 1982,although not as much as in IHS areas in total (seetable 4-56). In the 3-year period centered in 1973,Tucson had the fourth highest death rate of theIHS areas; in 1980 to 1982 it had the third high-est. The poor health status of Tucson Indians isalso apparent from an estimated age-adjustedmortality rate of 1011.1 per 100,000 populationin the 3-year period centered in 1981, a rate 1.8times the U.S. all races rate.
Accidents remained the leading cause of deathin Tucson in 1980 to 1982 (see table 4-57), despite
a 27-percent decline in the death rate from acci-dents since 1972 to 1974. Forty-two Tucson malesdied as a result of accidents in 1980 to 1982, a rate3.7 times that of U.S. all races males. Though thenumber of Tucson females killed in accidents (19deaths) was lower, accidents were the second lead-ing cause of death for females, and their rate ofdeath from accidents was 3.6 times the rate forU.S. all races females. Other forms of violentdeath were also prevalent in Tucson, particularlyamong males. Suicide was the fifth leading causeof death for males, and homicide, the eighth. In-juries and poisonings were the second leadingcause of hospitalization in Tucson in both 1979and 1984, although neither the 1979 or 1984 dis-charge rates for injuries and poisonings exceededeither the IHS or the U.S. all races averages. Asfor many other IHS areas, lacerations and openwounds, and superficial injuries and contusionswere among the 15 leading causes of male out-patient visits in Tucson, accounting for a total of5 percent of male visits (see table 4-58).
Heart disease was the leading cause of deathfor Tucson females, and Tucson is unusual in thatthe 1980 to 1982 mortality rate from heart dis-ease for females exceeded that of U.S. all racesfemales (by a ratio of 1.3).
The 1980 to 1982 infant mortality rate in Tuc-son was the second highest of IHS areas and 1.6

148 ● Indian Health Care
Table 4-56.—Changes in Crude Death Rates, 1972-82:IHS Tucson Area (rates per 100,000 population)
PercentIHS 1972-74 1975-77 1980-82 changeCode Cause rate rate rate 1972-82790 Accidents/adverse effects . . . . . . . . . 168.1 166.1 122.5 –27.1800 Motor vehicle accidents . . . . . . . . . 114.0 124.6 90.4 –20.7810 All other accidents . . . . . . . . . . . . . 54.1 41.5 32.1 –40.6620 Liver disease/cirrhosis . . . . . . . . . . . . 82.6 80.6 52.2 –36.8310 Diseases of the heart . . . . . . . . . . . . . 71.2 83.0 114.5 60.8150 Malignant neoplasms . . . . . . . . . . . . . 62.7 70.8 44.2 –29.5510 Pneumonia/influenza. . . . . . . . . . . . . . 54.1 31.7 28.1 –48.0260 Diabetes mellitus . . . . . . . . . . . . . . . . 42.7 19.5 36.1 – 15.4030 Tuberculosis. . . . . . . . . . . . . . . . . . . . . 37.0 10.0 –72.9430 Cerebrovascular diseases . . . . . . . . . 31.3 24.4 18.1 –42.3830 Homicide . . . . . . . . . . . . . . . . . . . . . . . 31.3 19.5 20.1 – 35.8820 Suicide . . . . . . . . . . . . . . . . . . . . . . . . . 22,8 26.8 38.2 67.3
All other causes . . . . . . . . . . . . . . . . . 315.7 318.3 271.0 – 14.1ALL All causes . . . . . . . . . . . . . . . . . . . . . . . 920.5 840.7a 755.0 – 18.0alncludes tuberculosis; rate unknown.
SOURCES’ 1972.74 and 1975-77 deaths: U.S Department of Health, Education and Welfare, Public Health Service, Health ServicesAdministration, Indian Health Service, Selected Wtal Stafistms for lrr~larr Health Service Areas and Service Units,1972 to 1977, DHEW Pub. No. (HSA)-79-1OO5 (Rockville, MD: HSA, 1979). 1972-74 and 197548 population: U S.Department of Health and Human Services, Public Health Service, Health Resources and Services Administration,Indian Health Service, Program Statistics Branch, Internal documents, Rockville, MD, 1985. 1980-82 data: U SDepartment of Health and Human Services, Public Health Service, Health Resources and Services Administration,Indian Health Service, computer tape supplied to the Office of Technology Assessment, Washington, DC, 1985
times that of the U.S. all races rate. As for almostall other IHS areas, the neonatal mortality ratein Tucson (6.1 per 1,000 live births) was lowerthan that of U.S. all races (8.0), but Tucson’s post-neonatal mortality rate was 3.5 times that of U.S.all races and the highest of all IHS areas. Unfor-tunately, the cause or causes of this high mortal-ity rate cannot be specified; the two largest cate-gories of postneonatal death being SIDS (sixdeaths) and other “symptoms, signs and ill-definedconditions” (four postneonatal and one neonataldeath; table 4-59).
Although the absolute numbers were small, asfor most other causes of death, liver disease andcirrhosis caused death in Tucson females at a rate5.5 times (8 deaths) the U.S. all races females rate,and Tucson males had a death rate 8.3 times (18deaths) the U.S. all races male rate. The Tucsonhospital discharge rate for alcoholic liver disease(9.0 per 10,000 population) was also higher thanthe comparable rate in U.S. short-stay non-Federalhospitals (1.6). The Tucson hospital dischargerates for alcohol-related mental disorders relativeto that of U.S. short-stay non-Federal hospitalsvaried and are difficult to interpret. There werehigher rates of hospital discharges for both non-dependent alcohol abuse and alcoholic psychosesin Tucson than in U.S. short-stay non-Federal hos-
pitals, but a lower rate in Tucson for alcohol de-pendence syndrome (9.5 per 10,000 populationfor alcohol dependence syndrome compared toa rate of 16.7 for U.S. short-stay non-Federal hos-pitals). These statistics do not include data fromthe Papago tribe’s alcohol program (funded un-der Public Law 93-638), which includes outpatientand residential treatment components (76). TheTucson discharge rate for mental disorders (38,1per 10,000 population) was about half that of U.S.short-stay non-Federal hospitals (72.0), which isnot surprising because there are no IHS psychiatricbeds in the Tucson area. No mental disorders, in-cluding those for alcohol abuse, were among the15 leading causes of outpatient visits in Tucson.
It is notable that in 1984 the Tucson hospitaldischarge rate for diabetes (53.2) was twice thatof both the IHS on average and U.S. short-staynon-Federal hospitals. The Tucson rate in 1979was 17.4 per 10,000 population, indicating per-haps that diabetes is a growing problem. Diabeteswas also the leading cause of outpatient visits forfemales (8.0 percent of female visits) and the sec-ond leading cause of outpatient visits for males(6.9 percent of male visits). Changes in the crudedeath rate from diabetes (shown in table 4-30) arehard to interpret; apparently, low absolute num-bers result in substantial variation year-by-year.

—
Ch. 4—Health Status of American Indians ● 149
Table 4-57.—Fifteen Leading Causes of Deaths and Age-Adjusted Death Rates for Tucson IHS Area Indians 1980.82and U.S. All Races 1981
Ratio of TucsonIHS Number Age-adjusted mortality rate area Indians tocodea Rank Cause name of deaths Indians U.S. all races U.S. all racesFemales:310 1.790 2.260 3.090 4.620 5.150 6.430 7,510 8.420820 l::140 11.640 12.730 13.740 14,840 15.
ALL . . . .
Males:790 1.310 2.620 3.150 4.820 5.260 6.510 7.830 8.030 9.640 10.420 11,430 12.090 13.540 14.730 15.
ALL . . . .
Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Accidents/adverse effects. . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Septicemia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . . .Cerebrovascular diseases . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Hypertension with or without renal disease . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other infectious/parasitic diseases . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .Conditions arising in perinatal period . . . . . . . .All other external causes . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Accidents/adverse effects. . . . . . . . . . . . . . . . . . .Diseases of the heart . . . . . . . . . . . . . . . . . . . . . .Liver disease/cirrhosis. . . . . . . . . . . . . . . . . . . . .Malignant neoplasms. . . . . . . . . . . . . . . . . . . . . . .Suicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . .Pneumonia/influenza . . . . . . . . . . . . . . . . . . . . . . .Homicide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Nephritis, et al . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hypertension with or without renal disease . . .Cerebrovascular disease . . . . . . . . . . . . . . . . . . . .Septicemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Chronic pulmonary diseases . . . . . . . . . . . . . . . .Congenital anomalies . . . . . . . . . . . . . . . . . . . . . .All others . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2919
9887654433322
39151
42281815159994433222
60225
173.674.253.945.940,742.538.320.220.915.219.319.37.55.07.6
197.1781.2
222.5169.9132.2106.2
73.255.545.043.826.328.024.012.1
7.59.95.0
311.71.272.8
135.120.4
9.62.47.4
108.635.4
9.21.75.71.33.65.58.20.9
65.1420.4
60.2271.2
16.0163.7
18.010.016.616.7
1.05.62.2
41.73.4
26.26.1
94.7753.3
1.33.65.6
19.15.50.41.12.2
12.32.7
14.95.41.40.68.53.01.9
3.70.68.30.64.15.62.72.6
26.35.0
10.90.32.20.40.83.31.7
aEqulvalence to ICD-9 code available from the Indian Health Sewlce
SOURCES U.S. all races: US. Department of Health and Human Services, Public Health Service, National Centerfor Health Statistics, “Advancer eport,F inal MortalityStatfst!cs, 1981,’’ A40rrflrly Vifa/ Sfatist/cs Report 3<3)”supp, June 22, 1984, Indiansin iHSareas:US Department of Health and Human Services, PublicHealth Service, Health Resources and Services Administration, Indian Health Service, computer tape supplied to the Office of Technology Assessment,Washington, DC, 1985
In the 1980-82 period, relatively few (only six) In- fections accounted for a substantial portion of out-dian residents in Tucson died of renal failure, patient visits by females, and hypertensive dis-another common sequelae of diabetes, but this is ease also seemed to be common in both sexes. Thenot surprising if the problem is emerging only rela- Tucson area did seem to be unusual in having rela-tively recently, as suggested by the hospital dis- tively large numbers of outpatient visits for skincharge data. diseases, including bacterial infection, fungal dis-
eases, and “other diseases of the skin, ” amount-There are other health problems in Tucson that ing to 6.2 percent of male, and 4.7 percent of fe-
are not evident from mortality data. As shown male visits. These skin diseases were not amongin table 4-32, otitis media accounted for 4.8 per- the leading causes of visits to physicians’ officescent of outpatient visits among males, and 3,0 per- in the last survey of ambulatory medical care incent among females, although this rate was not the United States (200). Hospital discharge ratesunusually high for IHS areas. Urinary tract in- fer skin diseases in Tucson (31.4 per 10,000 pop-

150 ● Indian Health Care
Table 4-58.—Fifteen Most Frequent Outpatient Diagnoses:a Tucson Area, Fiscal Year 1984
Percent ofIHS Number of total visits
Rank Code Clinical impressions visits by sex.Female:
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
080480300251283823520820486504400818810819827
300080251283820818520730731810821014501504827
ALL
Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Prenatal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Chronic otitis media with or without mastoiditis . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Tests only (lab, X-ray) , . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other diseases of skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hospital medical/surgical followup . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other complications of pregnancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Fungal diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Urinary tract infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other symptoms.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other preventive health services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Another . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Upper respiratory infection, common cold . . . . . . . . . . . . . . . . . . . . . .Diabetes mellitus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Chronic otitis media with or without mastoiditis . . . . . . . . . . . . . . . .Hypertensive disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Hospital medical/surgical followup . . . . . . . . . . . . . . . . . . . . . . . . . . . .Well child care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Other diseases of skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Laceration, open wound . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Superficial injury, contusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other symptoms.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Physical examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Gastroenteritis, diarrhea, etc., no other symptoms. . . . . . . . . . . . . . .Other bacterial infections of skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Fungal diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
All other causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .All causes, both sexes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3,8893,7262,6531,4721,4221,4121,3631,339
940921913909905837
4,637
2,0822,0261,4081,2831,100
922776762700683597583532530
2,42934,61578,366
8.07.75.53.02.92.92.82.81.91.91.91.91.91.79.6
7.16.94.84.43.73.12.62.62.42.32.02.01.81.88.2
100.0alHS ~efer~ t. these ~~ ~linic.l impre~~ion~, because they are recorded before a clinical diagnosis IS completed; therefore, they may not be valid diagnoses,
SOURCES: 1510adlngctlnlcal impresaiona: U.S. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, lndi-an HealthServlce, “SpecialReport on 15 Leading Causes of Outpatient Care By Area and Service Unit, State and County,” internal document, Albuquerque,NM, 1985. TucsontotakUS. Department of Health and Human Services, Pubiic Health Service, Health flesourcesand Services Administration, Indian HealthService, Officeof Planning, Evaluation and Legislation, Program Statistics Branch, Surrwrrary ofLead/ng Causes for Outpatient Visits, /ndiarr Hea/th Serv/ceFacflltles, Fisca/ Year 19&?4(Rockviile, MD: IHS, no date)
ulation) were higher than the U.S. races and IHSaverage rates, although other IHS areas experi-enced even higher rates.
Although gastrointestinal infections are nolonger a leading cause of death among Indians,gastroenteritis and/or diarrhea were among theleading causes of outpatient visits among Tucsonmales, and the hospital discharge rate for infec-tious and parasitic diseases was the second high-est of IHS areas, second only to the Phoenix area.Skin and other infectious diseases are due at least
In summary, the health status of Indians in theTucson area is in many respects similar to thatof Indians elsewhere in the United States, althoughthere are certain problems such as gastroenteri-tis, skin diseases, and other infectious diseases thatpatient care and mortality data indicate are moreprevalent among Indians in the Tucson area thanelsewhere. With the small population, and result-ing small absolute number of deaths, interpreta-tions about change and relative importance aresometimes difficult to make.
in part to the lack of indoor plumbing (145).

Ch. 4—Health Status of American Indians
Table 4-59.—infant Deaths and Death Rates IHS Tucson Area, 1980-82
● 151
IHS Deaths Rates (per 1,000 live births)
codea Cause Total Neonates Postneonates Total Neonates Postneonates
040 Septicemia . . . . . . . . . . . . . . . . . . 1 — 1 0.7 — 0.7130 Meningitis. . . . . . . . . . . . . . . . . . 1 — 1 0.7 — 0.7170 Pneumonia/influenza. ... . . 2 2 — 1.3 1.3 —180 Pneumonia . . . . . . . . . . . . . . . . 2 2 — 1.3 1.3220 Gastritis, etc. . . . . . . . . . . . . . . . . 2
—— 2 1.3 1.3
230 Other digestive . . . . . . . . . . . . . .—
1 — 1 0.7 0.7240 Congenital anomalies . . . . . . . . . 5
—4 1 3.4 2.7 0.7
380 Conditions arising inperinatal period . . . . . . . . . . 4 2 2 2.7 1.3 1,3
580 Symptoms/signs/other . . . . . . . . 11 1 10 7,4 0.7 6.7590 SIDS . . . . . . . . . . . . . . . . . . . . ., 6 — 6 4.0 — 4.0600 Symptoms/signs/other . . . . . . 5 1 4 3.4 0.7 2.7640 Accidents . . . . . . . . . . . . . . . . . . . 1 — 1 0.7 — 0.7680 All other causes . . . . . . . . . . . . . 1 — 1 0.7 — 0.7ALL All . . . . . . . . . . . . . . . . . . . . . . . . . 29 9 20 19.5 6.1 13.3alHs code, equivalence to ICD.g Recode 61 for Infant deaths available frOrn IHsSOURCE U S. Department of Health and Human Services, Public Health Service, Health Resources and Services Adm!n!stratlon, Indian Health Serv!ce, computer tape
supplied to the Off Ice of Technology Assessment, Washington, DC, 1985
CONCLUSION
In conclusion, the health of American Indianson average has improved on many measures overthe past 15 years, but in almost every IHS serv-ice area and on almost every measure it is still farbehind that of the U.S. all races population. Thereis considerable variation among IHS areas, butthe available mortality data indicate that Indiansin almost all IHS service areas are at considerablerisk for death by accident, suicide, homicide, andother external or “social” causes. In addition, theysuffer disproportionately from alcoholism, dia-
betes, and pneumonia. Infant mortality has de-clined, but Indian infants continue to be at greaterrisk for death than infants of all other U.S. racescombined, particularly in the postneonatal period.Comprehensive data about illness in Indians aredifficult to obtain because of IHS’s position thatit is not the sole provider of health care to Indians,but for the most part available data support theconclusions drawn from mortality data and in-dicates the existence of additional problems.

Contents
Chapter 5
The Indian Health Service
PageIntroduction . . . . . . . . . . . . . . . . . . . . . ..........155The IHS Direct Care Program . ..............156
Eligibility for Direct Care Services . .........156Funding for Direct Care Services . ..........157IHS Staff ing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 158Delivery of Direct Care Services . ..........168Conclusions . . . . . . ........................173
The IHS Contract Care Program . ............175Eligibility and Funding for Contract Care ...175Funding and Utilization of Contract Care
by IHS Area..... . . . . . . . . . . . . . . . . . . . . ..177Operation of the Contract Care Program. ...182Issues Related to the U-IS Contract Care
Program . . . . . . . . .......................185
Page
Conclusions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .190Urban Indian Health Projects . ...............193
Funding for Urban Indian HealthInitiatives . . . . . . . .......................194
Services Provided by Urban Indian Healthp r o j e c t s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 9 8
Conclusions . . . . . . ......................,.199The IHS Health Facilities Construction
Program. . . , . . . . . . . . . . . . . . . 4 . . . . . . . . . . . 200Priority System for the Construction of
Health Facilities . . . . . . . . . . . . . . . . . . . . 200Methods for Assessing Need for New
and Replacement Facilities . . . . . . . . . . . . ...204

5-1.
5-2.
5-3.
5-4.
5-5.
5-6.
s-7.
5-8.
5-9.
5-10.
5-11,
5-12
5-13
5-14
5-15.
IHS Staff by Function and Area,Fiscal Year 1984 . . . . . . . . . . . . . . . . .......162IHS Indian and Non-lndian Employees byProfession and Area, Fiscal Year 1984 ...163IHS Weal and Dental Officers inRelation to Eligible Service Populationby Area, Fiscal Year 1984..............164IHS Area Comparison of IHS DirectCare Workload by Clinical Units, Fiscalyear 1984 . . . . . . . . . . . . . . . . . . . . .......,165IHS Indian and Non-Indian CommissionedCorps Officers by Clinical andNonclinical Function, Fiscal Year 1984...166Number of Admissions and UtilizationRate for IHS, Contract, and Tribal Self-Determination Hospitals, Fiscal Years1955-84 . . . . . . . . . . . . . . . . . . . . ..........170Average Daily Patient Load in IHS,Contract, and Tribal Self-DeterminationHospitals, Fiscal Years 1955-84..........171IHS and Tribally Operated Self-Determination (638) Facilities by IHSArea, With Fiscal Year 1984 Utilization ..172Numbers of Outpatient Visits to IHS,Contract, and Tribal Facilities, Actual forFiscal Years 1955-84 and Estimates for1985-86 . . . . . . . . . . . . . . . . . . . . .. ........174Estimated IHS Contract Care Obligationsby Type of Expenditure, With Utilizationand Unit Costs, Fiscal Years 1983-86.....178Ten Leading Causes of Hospitalization forGeneral Medical and Surgical Patients,IHS and Contract General Hospitals,Fiscal Year 1984 . . . . . . . . . . . . . . . . .. ....,178IHS Contract Care Program Obligationsby Area, Total and Per Capita,Fiscal Year 1984. . . . . . . . . . . . . . . . . . . . . .179Numbers of Admissions, Hospital Days,and Average Lengths of Stay in IHS,Contract General, and Tribal SeIf-Determination Hospitals, FiscalYear 1984 . . . . . . . . . . . . . . . . . . . . ,.......180IHS Contract Care Program, Utilizationand Costs for Inpatient and OutpatientCare, by Area, Fiscal Year 1984.........181
5-19..
$-20.
5-21.
5-22.
5-23.
of Reported Revenues in Dollars, bySource and by Program ...............,196IHS-Funded Urban Indian HealthPrograms, Fiacal Year 1984: Distributionof Costs in Dollars by Programcomponent ● . * . . * . * . . . . ” . . . . . . . . . . . * * . 197Distribution of the American Indian,Eskimo, and Aleut Population AmongSMSAs, 1980 .......,..... ● . . . ● . . . ,198Nonmedical, Nondental Services Offeredby IHS-Supported Urban Indian HealthPrograms: Fiscal Year 1984...,......,..199Indian Health Facilities, History ofAppropriations by Activity, Fiscal Years1956-85 . . . . . . . . . . . . . . + + .. ............201
List of FiguresFigure No. Page5-1. IHS Annual Allocations, Fiscal Years “
592.
5-3.
5-4.
5-5.
5-6.
5-7.
5-8.
5-9.
5-1o.
1972-85 . . . . . . . . . . . . . . . . . . . . . .........158IHS Allocations by Category, Fiscal Years1981-85 ..+ . . . . . . . . . . . . . . . . . . . . . . . . . . 159IHS Allocations by Area and BudgetCategory, Fiscal Years 1981 and 1985....160Occupancy Rates in All U.S. CommunityHospitals, U.S. Nonmetropolitan Hospitals,and IHS Hospitals, Fiscal Years 1970-85 ..168Average Length of Stay in All U.S.Community Hospitals, U.S. Nonmetro-politan Hospitals, and IHS Hospitals,Fiscal Years 1970-85 .. .................169Number of Admissions to IHS andContract and Tribal Hospitals, FiscalYears 1970-$5 . . . . . . . . . . . . . . ...........169Average Daily Patient Load in IHS,Contract, and Tribal Hospitals, FiscalYears 1970-85 . . . . . . . . . . . . . . . . . . . ......170Numbers of Outpatient Visits to IHS,Contract, and Tribal Facilities, FiscalYears 1970-85 . . . . . . . . . . . . . . . . . . . . . ’ . . . .173Ten Leading Causes of Hospitalization inIHS and Contract General Hospitals,Fiscal Year 1984 ..., .. ...+. . ..........,179IHS Facilities Construction Process FromAssessment of Need to CongressionalAppropriation. . . . . . . . . . . . . . . . . . . . . .. ..202

— . .
Chapter 5
The Indian Health Service
INTRODUCTION
The primary source of health care services de-livered to most American Indians is the IndianHealth Service (IHS) of the Public Health Serv-ice (PHS), U.S. Department of Health and Hu-man Services (DHHS). The involvement of otherFederal, State, and local public health programsand private providers is significantly less, and infact the extent to which Indians depend on theseother sources of care is not precisely known.
Federal responsibility for the provision of healthcare to American Indians and Alaska Natives un-der the Snyder Act of 1921 (25 U.S. C. 13) wasconveyed from the Bureau of Indian Affairs (BIA)in the Department of the Interior to the Depart-ment of Health, Education, and Welfare (nowDHHS) by the Transfer Act of August 5, 1954 (42U.S. C. 2001 et seq.). Under that law, IHS cameinto being on July 1, 1955. The early focus of IHSwas on elimination of the infectious diseases thatwere widespread in the Indian population and onchronic care for the large numbers of Indianssuffering from tuberculosis, IHS achieved markedsuccess in both of those areas.
The present mission of IHS, articulated mostclearly in the Indian Health Care ImprovementAct of 1976 (Public Law 94-437), is to raise thehealth status of American Indians and Alaska Na-tives to the highest possible level. IHS defines itsservice delivery responsibilities to include a com-prehensive range of inpatient and ambulatorymedical services, dental care, mental health andalcoholism services, preventive health (immuniz-ations and environmental services such as sani-tation and water safety), health education, andIndian health manpower development programs.For Indians who live in isolated rural areas on ornear reservations, a broad definition of IHS re-sponsibilities is justified, because the infrastruc-ture of roads, utilities, and public services thatsupport health care delivery to non-Indian ruralresidents often is lacking on Indian reservations.IHS also includes a health facilities constructioncomponent that focuses its activities on provid-
ing hospitals, clinics, and facility staff livingquarters for reservation-based IHS services. IHS-funded programs for Indians who live in urbanareas, on the other hand, do not directly providehospital care; but they do offer a range of ambu-latory medical, dental, mental health, social sup-port, and referral services.
IHS provides comprehensive health and health-related services to approximately 960,000 eligi-ble Indians (1985) who live on or near reserva-tions at no cost to the individual Indian, regard-less of other health insurance coverage or abilityto pay. Both the comprehensiveness of the serv-ices IHS provides and the absence of premiumsand user charges for these services set Indiansapart from the general population in terms of theirhealth care delivery expectations and problems.Thus, it is difficult to directly compare health serv-ices systems for Indians and the U.S. population.Non-Indians do not enjoy the preventive andhealth-related services available to Indians, andas a rule, they cannot receive such services freeof charge. But with private health insurance, non-Indians have easier access to more technologicallyadvanced medical services than are available toIndians dependent solely on IHS.
Although in principle IHS services are compre-hensive and readily available at no user cost, infact they are limited by IHS budget constraintsand by the uneven distribution of services amongIHS areas that has developed over the years. IHSfacilities, for example, are not equally availableand accessible to eligible populations in all partsof the country; and facilities construction plansare not necessarily related to local service popu-lation size or utilization patterns. The servicesoffered by many of the smaller IHS hospitals maybe less specialized than those found in the typi-cal small rural community hospital. When no IHSfacility is accessible or when specific services arenot available from IHS facilities, Indian patientsmay require referral to private providers underthe IHS contract care program; but contract care
155
52-805 0 - 86 - 6

156 ● Indian Health Care
budgets sometimes have been so limited thatneeded referrals cannot be made. Thus, while theymay not be directly affected by ability to pay, In-dians may face serious obstacles in obtaininghealth care services through IHS.
IHS provides inpatient and ambulatory medi-cal, dental, and mental health services eitherdirectly through its network of IHS-owned hos-pitals, health centers, and clinics, or indirectly,by purchasing services that are not available fromIHS facilities through contracts with private pro-viders. Another factor in the IHS delivery systemsince the Indian Self-Determination and Educa-tion Assistance Act of 1975 (Public Law 93-638)has been the operation of health facilities and serv-ice programs by Indian tribes. Direct care facil-ities, contract care programs, facilities construc-tion, and special programs such as communityhealth representatives, mental health and drugabuse, and health education initiatives may beadministered by tribes under self-determinationor 638 contracts. Most of these services, like IHS’sown services, are reservation based; they are au-
THE IHS DIRECT CARE PROGRAM
Although the IHS direct care program also pro-vides preventive health, dental, mental health,and alcoholism services, this discussion of the pro-gram focuses on hospital-based and ambulatorymedical services, since they are by far the mostimportant components of IHS services delivery.IHS direct care services to Indians living on ornear reservations are delivered by Federal staff inIHS-owned and operated facilities, or by employ-ees of tribal self-determination (638) contractorsin IHS-owned, tribally operated facilities. As dis-cussed in chapter 6, the 638 contract program im-plements the 1975 Indian Self-Determination andEducation Assistance Act (Public Law 93-638).Hospitals and clinics operated under the self-determination program are considered part of theIHS direct care system, as opposed to the supple-mental services that are obtained through the IHScontract care program; but tribes also may oper-ate their own contract care programs under 638contracts. Utilization data for tribally operated
thorized and funded under the general authorityof the Snyder Act; and they are provided to IHS-eligible Indians at no cost to the individual.
The urban Indian health projects, which arespecifically authorized and funded under the In-dian Health Care Improvement Act, operate sep-arately from the reservation-based IHS system.Urban projects may receive funds from non-IHSsources, are likely to treat non-Indians, and mayrequest payment from Indians and non-Indiansalike based on a sliding fee scale. Although ur-ban projects may not be operated by tribes un-der the self-determination program, they are sim-ilar to tribally operated programs in that they aremore active than IHS programs in treating andbilling non-Indians and in coordinating their ef-forts with other non-IHS health delivery programs.
The IHS direct care program, the IHS contracthealth services or contract care program, urbanIndian health projects, and the IHS facilities con-struction program are described in this chapter.
programs are incomplete because of differencesin reporting systems.
Eligibility for Direct Care Services
Eligibility for direct services in IHS and triballyoperated facilities is defined in Federal regulations(42 CFR 36 subpart B). The regulations state thatmedically indicated services will be provided “topersons of Indian descent belonging to the Indiancommunity served by the local facilities and pro-gram. ” An individual maybe considered eligiblefor IHS care “if he is regarded as an Indian bythe community in which he lives as evidenced bysuch factors as tribal membership, enrollment,residence on tax-exempt land, ownership of re-stricted property, active participation in tribal af-fairs, or other relevant factors in keeping with gen-eral Bureau of Indian Affairs practices in thejurisdiction” (42 CFR 36.12). Non-Indian womenpregnant with an eligible Indian’s child may re-

Ch. 5—The Indian Health Service ● 157.
ceive obstetrical care, and services to prevent thespread of infectious diseases may be provided toIndian and non-Indian members of the community.
These regulations allow broad interpretation ofeligibility for IHS direct care, with notable vari-ations among IHS areas. (Eligibility for contractcare services is more restrictive because of the re-quired residence “on or near” a reservation, ) TheFederal Government limits its responsibility forhealth services to Indians, however, by stating inregulations that IHS does not provide the sameservices in all areas and that service availabilitydepends on the capabilities of local IHS and otherproviders and on the “financial and personnel re-sources” of IHS. If funds, facilities, or personnelare insufficient to meet demand, IHS may set pri-orities for care on the basis of relative medicalneed and access to other services (42 CFR 36.11(c)).
Differences by IHS area between the numbersof Indians who are eligible for IHS direct careservices and those who actually use them are un-known at this time. A patient enrollment systemwas instituted throughout IHS beginning in Jan-uary 1984, and when this system is fully imple-mented, user populations will be defined more ac-curately. In the meantime, analyses of IHS serviceutilization rates and trends among the areas andcomparisons with general U.S. rates should beviewed with caution, because the comparabilityof the denominator populations is not known. Theuneven availability of IHS direct care facilities alsohas a significant, though unquantifiable, effect onservices utilization.
Funding for Direct Care Services
IHS funding for direct care services comes fromthe basic Snyder Act appropriation. Most of theadditional funding appropriated for the IndianHealth Care Improvement Act, authorized in fis-cal years 1985 and 1986 by continuing resolution,is directed to particular programs such as man-power training, the community health represent-atives program, and urban Indian projects. Thatfunding amounted to $129 million in fiscal year1984, or 15 percent of the total IHS appropria-
tion (135). Growth in overall IHS allocations, in-cluding Indian Health Care Improvement Actfunding but not including IHS facility construc-tion funds, is illustrated in figure 5-1 (for alloca-tions by budget category and area for fiscal years1972-85, refer to app. C). In actual dollars, IHSallocations increased from $157 million in fiscalyear 1972 to $807 million in 1985, During thattime, the IHS eligible service population doubled,more as a result of adding new population groups,such as the California Indians, than of natural in-crease. Consequently, annual allocations per IHSbeneficiary have remained essentially the samesince 1972 when adjusted for inflation (see ch. 1,figures 1-8 and 1-9).
Direct clinical services delivery has always beenthe major component of the IHS budget, averag-ing over 60 percent of total funding in recent years(see figure 5-2). Budgets for contract care serv-ices, preventive health programs, and other serv-ices (urban projects, manpower training, admin-istration) are much smaller. Figure 5-3 illustratesthe relative importance of these major budgetcomponents by IHS area and compares area fund-ing levels for fiscal years 1981 and 1985.
Within the IHS direct care budget (excludingcontract care), line items for hospital and clinicoperations, facility maintenance and repairs, den-tal care, mental health, and alcoholism programsare specified (the reimbursements category refersnot to Medicare and Medicaid collections, but topayments from other Federal agencies for the useof IHS facilities and services). Table 5-1 presentsthe breakdown of fiscal year 1985 direct healthallocations by IHS area into these categories. Theoperation of IHS hospitals and clinics always hasconsumed the bulk of the direct services budget,representing 84 percent of the overall IHS directdelivery allocation in 1985. Hospitals and clinicsfunding ranged from a low of 67 percent of thetotal in the Portland IHS area to a high of 88 per-cent in Alaska. Dental care and alcohol programseach accounted for about 5 percent of the directcare budget (although funding for alcohol pro-grams ranged from 2 percent in Alaska to nearly19 percent in Portland in 1985), with lesseramounts allocated to mental health and facilitymaintenance and repair.

158 ● Indian Health Care
Figure 5-1.— IHS Annual Allocations, Fiscal Years 1972-85
900
800
700
600
400
300
200
100
0
.
F- I I - - I I I I
—
—
—
—
—
1972 1973 1974 1975 1976 1977 1978 1979 1980 1981 1982 1983 1984 1985
Fiscal year
SOURCE U S Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Indian Health Service, Officeof Administration and Management, 1985
IHS Staffing
Personnel represents the largest single cost com-ponent in the IHS hospitals and clinics operatingbudget. Fiscal year 1984 IHS staff by area and bytype of staff are shown in table 5-2. These figuresinclude staff of IHS-operated direct care facilitiesand IHS employees assigned to tribally operated638 contract programs under the terms of the In-tergovernmental Personnel Act; but staff hireddirectly by the tribes are not included. Altogether,there were 10,342 permanent, full-time positions,nearly half of which were classified as adminis-trative and support staff. The two categories ofnurses in table 5-2 (including facility-based R.N. sand L. P.N.s, public health nurses, and nursing as-
sistants) made up the largest group of healthproviders, accounting for nearly 27 percent of allpositions. The 645 medical officers (excluding 44who served primarily as administrators) made up6.2 percent of total positions. Personnel datamaintained at IHS headquarters do not identifymedical officers by specialty; however, they dodistinguish between medical officers in clinicalpractice and those engaged primarily in nonclin-ical work (171).
In 1984, the Navajo, Oklahoma, Phoenix, andAlaska areas had the largest numbers of IHS staff,a combined 62 percent of total IHS positions. TheIHS system included 83 physician assistants, whowere used most widely in the Navajo area. Thelargest numbers of medical officers in clinical prac-

Ch. 5—The Indian Health Service ● 159
Figure 5-2.—IHS Allocations by Category,Fiscal Years 1981-85
900 r
: 300a t
200
100
01 1 I 1 I
1981 1982 1983 1984 1985Fiscal year
–. — - —“ Total allocation
Direct clinical services
~ Contract care
- - - - - - O t h e r
— P r e v e n t i v e h e a l t h
SOURCE. U.S. Department of Health and Human Services, Public Health Serv-ice, Health Resources and Services Administration, Indian Health Serv-ice, Office of Administration and Management, 1985
tice were in the Navajo, Phoenix, Alaska, andOklahoma areas (see table 5-2). This observationsuggests that a wider and more advanced rangeof services is available in those areas. It also re-flects the location of IHS’s three referral medicalcenters in Anchorage, Gallup, and Phoenix, andof seven hospitals in the Oklahoma IHS area.
Indian preference in employment applies to ini-tial appointments, reappointment, reinstatement,transfer, reassignment, promotion, or any otherpersonnel action intended to fill a vacancy in IHS(42 CFR 36.42 (a)), BIA, or in tribal programsoperated under self-determination (638) contracts.Preference in employment is extended to: 1) mem-bers of federally recognized tribes; 2) descendantsof such members who were residing within thepresent boundaries of any Indian reservation onJune 1, 1934; 3) persons of Indian descent whoare of one-half or more Indian blood of tribes in-digenous to the United States; 4) Eskimos andother aboriginal people of Alaska; and 5) certaindescendants of the Osage tribe (42 CFR 36,41).Table 5-3 shows the fiscal year 1984 breakdownof Indian and non-Indian IHS employees by pro-
fession for each area. In 1984, 59.3 percent of theIHS work force was Indian, compared with 1970,when Indians comprised 52.2 percent of the totalIHS work force (171). There were 23 Indian med-ical officers and 9 Indian dental officers servingin IHS in 1984; but 6 of the medical officers and1 dental officer were working in nonclinical ca-pacities. In fiscal year 1983, nearly 60 percent ofthe staff in urban Indian health projects wereIndian.
IHS estimates its unmet need for health profes-sionals relative to workloads in terms of unfilledpositions, using an application of the resource re-quirement methodology (described in ch. 6). In1985, unfilled staff positions in IHS facilities andtribally operated health programs were estimatedto exceed 1,500 health professionals, including 166surgeons (among other types of physicians) and697 nurses (137).
Table 5-4 shows numbers of IHS medical anddental officers, by area, and ratios per 1,000 esti-mated eligible service population in 1984. Thephysician-to-population ratio for IHS as a wholewas 0.7 physicians per 1,000 population. Thehighest ratios were in the Alaska (1.4 per 1,000)and Phoenix areas (1.3 per 1,000), followed byAlbuquerque, Billings, Navajo, and Tucson (rang-ing from 1.0 to 0.8 physicians per 1,000 servicepopulation). The dentist-to-population ratio forIHS as a whole was 0.3 dentists per 1,000 popu-lation.
For the U.S. population as a whole, there were1.65 active, non-Federal, patient care physicians(1980) and 0.46 dentists (1979) per 1,000 persons(202). Within the United States, the supply of phy-sicians and, to a lesser extent, dentists differs frommetropolitan to nonmetropolitan areas. In 1980,the United States had 1.91 physicians per 1,000population in metropolitan areas and 0.84 per1,000 in nonmetropolitan areas. In 1979, dentistsin the United States numbered 0.5 per 1,000 pop-ulation in metropolitan areas versus 0.31 per 1,000in nonmetropolitan areas. IHS average ratios of0.7 physicians and 0.3 dentists per 1,000 eligibleservice population are closer to U.S. ratios fornonmetropolitan areas, which more nearly ap-proximate IHS delivery locations, than to U.S.ratios for metropolitan areas.

160 ●
Indian H
ealth C
are
ucm
(Suo!ll!lu) S
JellOp Ien]av
Figure 5·3.,-IHS Allocations by Area a d Budget Category, Fiscal Years 1981 and 1985
120
110
100
90
80
Ul c 70 .Q
I en
~ 60 "0 "0
«i :::l
U 50 <
40
30
20
10
o 1981 1985 1981 1985 1981 1985 1981 1985 1981 1985 1981 1£185 1981 1985 1981 1985 1981 1985 1981 198!; 1981 1985 1981 1985
Aberdeen Albuquerque Alaska Bemidji Billin~ls Calilornia Navajo Oklahoma Phoenix Portland Tucson Nashville
_ Direct clinical services D Contract care D Preventive health II Other
SOURCE: U.S. Department of Health and Human Services. Public Health Service. Health Resources and Services Administration. Indian Health Service. Office of Administration and Management, 1985

Ch. 5—The Indian Health Service • 161
69
‘ml
00mm-00-3”-3
t9
000a“-04r-
ta
5m“0
w“m
t9
000-
8mm“
W
.
00mm-W-$N“w
@
00
0“cmcma3-
t9 *
00
E$mr=-
000-a-1Inac7-1=
*
00O*mrCD
- -
W3
00=+-UI0mm-C9
49
000h-Zm-
e
—
(uv z
uz
t9t9#3t9b9 t9@49e969t9e3
69
00co-
b0m-m
i+
cw
;
%<
t9
00u-la)”0
N-Cn
b9
2m(uz
m
00Inw-CNCN
.xw
m.—c8.-75L)
*
00
g
o-N
4s9
al=.-
ZCA
2’

162 ● Indian Health Care—
Table 5-2.—IHS Staff by Function and Area, Fiscal Year 1984
Clinical
Medical a Dental a Physician Other Allied Administrative/ TotalArea officers officers assistants Nurses b nursing c health support staff d
Aberdeen . . . . . . . . . . 25 20 10 161 81 179 439 9 1 5 –
Alaska. . . . . . . . . . . . . 98 35 8 269 76 114 660 1,260Albuquerque . . . . . . . 52 20 12 157 66 181 430 918Bemidji . . . . . . . . . . . . 18 13 0 50 12 53 124 270Billings . . . . . . . . . . . . 40 17 1 77 32 125 324 616California . . . . . . . . . . 1 0 0 0 0 4 56 61Nashville . . . . . . . . . . 9 3 1 38 18 36 84 189Navajo . . . . . . . . . . . . 145 42 25 393 245 341 842 2,033Oklahoma . . . . . . . . . . 94 44 9 319 128 327 684 1,605Phoenix . . . . . . . . . . . 110 23 11 317 170 164 751 1,546Portland . . . . . . . . . . . 25 17 3 40 7 92 204 388Tucson . . . . . . . . . . . . 14 3 3 26 17 22 69 154Headquarters . . . . . . . 14 3 0 12 15 28 315 387
IHS total . . . . . . . . . 645 240 83 1,859 867 1,666 4,982 10,342 -
aourlng fi~Cal ~ear lg84, an addlt~on~ 44 f’nedlcal officers and 29 rjental Officers served in nonclinical capacities. They have been excluded from these clinical categories—
and included In the administrative/support categorybNur~e~ working In hospitals and clinics.cf+ur~es ~Orklng In other settings, e.g., community health and public health nursesdTotal IHS staff in this labie includes full. time, permanent IHS employees working in IHS faciiit[es and programs, and IHS employees assigned to tribal 638 COntraCt
programs under Intergovernmental Personnel Act provisions. Staff of 638 contract programs hired directly by the tribes (both former Federal and non-Federal) arenot included.
SOURCE Adapted by the Office of Technology Assessment from U S. Department of Health and Human Services, Publlc Health Service, Health Resources and SerwcesAdministration, Indian Health Service, “Annual Report to Congress on the Indian CIVII Service Retirement Act, Publlc Law 96. t 35, Fiscal Year 19&, ” table Xll
Tables 5-2 and 5-4 should be interpreted care-fully, because the number of IHS physicians inan area is dependent on the degree to which IHSand tribally operated direct services are available.For example, the numbers and rates of healthprofessionals in California do not accurately re-flect the situation there, because California deliv-ers care entirely through tribal 638 contractors.Some employees of these tribal 638 contractorsare not included in table 5-4 because they are di-rect tribal employees rather than IHS assigneesthrough the Intergovernmental Personnel Act,This data limitation probably affects the Bemidjiand Nashville areas as well, where there is a sub-stantial amount of self-determination contracting.The Portland IHS area appears to be low in staff-ing, because nearly half of its clinical servicesbudget is spent for contract care provided by pri-vate physicians and dentists. When these areas areexcluded, the Aberdeen area stands out with alower than average physician-to-population ratio.
Another means of comparing IHS staffingamong the areas is to attempt to standardize forworkload. Variations of this approach have beenused in recent years by several IHS area directors(e.g., in the Aberdeen and Navajo areas) to ex-amine and compare direct care workloads. The
workload measure is the number of “clinicalunits, ” with each unit representing 1 hospital day.Outpatient visits are converted to clinical unitsby equating six outpatient visits to 1 hospital day(120). Table 5-5 presents such an analysis for fis-cal year 1984. This table distinguishes clinical carestaff from administrative staff.
What is evident in table 5-5 is that the distri-bution of IHS clinical staff among the areas is notnecessarily related either to direct care workload,as approximated by the clinical units measure, orto the size of the service population. The num-ber of clinical units delivered per clinical staff po-sition in the Aberdeen area, for example, is about63 percent higher than the number in the Albu-querque area. This finding, conditional as it is,tends to confirm reports from the field that inareas such as Aberdeen, the problems of attract-ing medical staff to extremely isolated rural areasare complicated by the demands of unusuallyheavy workloads.
An important source of medical and healthprofessional staff for IHS is the PHS Commis-sioned Corps. Eighty-one percent of IHS’s medi-cal officers and 99 percent of its dental officersin clinical practice are members of the PHS Com-

Table 5-3.—IHS Indian and Non-Indian Employees by Profession and Area, Fiscal
Aberdeen
Profession I n d i a n N o n - I n d i a n—
Medical officers. ... ... , 2 26
Dental of fibers . . . . . . . . . . . 2 19
Physician assistants . . . . . . 8 2
Nurses . . . . . . . . . . . . . . . . . . 51 114
Other nursing . . . . . . . . . . . . 78 3
Clinical support . . . . . . . . . . 85 99
Administrative support . . . . 356 70. — — —
Area total . . . . . . . . . . . . . . 582 333
Navajo
Profession I n d i a n N o n - I n d i a n
Medical of fibers . . . . . . . . . . 4Dental of fibers . . . . . . . . . . . 1P h y s i c i a n a s s i s t a n t s . , 2 5Nurses . . . . . . . . . . . . . . . . . . 116Other nursing . . . . . . . . . . . . 240Clinical support . . . . . . . . . . 230Administrative support . . . 727
Area total ., . ...........1.343-
Alaska A l b u q u e r q u e—
I n d i a n N o n - I n d i a n I n d i a n N o n - l n d i a n
o05
184440
409
516
10336
3252
3277
241
744
Oklahoma
I n d i a n N o n - I n d i a n
145 844 1
0 9281 106
5 125123 181
92 600-690 - 1,030
8945
0217
315665
575
1 541 23
10 258 10564 290 102
361 45
585 333
Phoenix
Indian Non-Indian
1 1172 249 2
89 237763 7108 66556 165
928 618
—Bemidji b Billings
Indian Non-Indian Indian Non-lndian
o 18 2 ’38 –
o 14 0 180 0 1 0
11 40 26 529 3 32 0
15 40 62 6483 37 288 33
118 152 411 205
Year 1984a
C a l i f o r n i ab Nashville b ‘
Indian Non-lndian Indian Non-lndian—o 2 0 11 —
o0000
33
33
2 00 11 80 184 15
19 60
28 102
40
320
2317
87
Port land T u c s o n Headquarters IHS total—Indian Non-Indian Indian Non-Indian Indian Non-Indian Indian Non-lndian
1 27 1 15 3 21 23 6662 16 0 3 0 12 9 2601 2 3 0 0 0 72 11
16 24 6 20 9 6 514 1,3815 2 17 0 13 2 808 59
41 57 10 12 9 24 886 847144 50 58 9 149 139 3,824 982
‘ 210 178 95 5 9 183 204 6.136 4.206 a~~e 44 ~ed,Cal ~fflcers and 29 dental ~ffl~ers ~ewlng )n admlnlstrat,”e capacl~les are !ncluded with cllnl~al officers In this table AS noted In table 5-2, ~HS employees Of tribal 638 COntraCt programs assigned
—.
under the Intergovernmental Personnel Act are Included With other I H S staff In the total 6,136 Indian and 4,206 non-1 ndlan employees Staff hired dl rectly by tribal 638 programs (former Federal and nonfederal)are not Included
bstafflng may be Iow ,n Bemld]l, Callfornla, and Nashville because tribal dtrect employees of self -determination (638 contract) Pro9rams are not Included
SOURCE Adapted by the Off Ice of Technology Assessment from U S Department of Health and Human Services Publlc Health Service, Health Resources and Serwces Admlnlstratlon, Indian Health Service“Annual Report to Congress on the lndlan CIV!I Serwce Retirement Act, Publlc Law 96-135, F]scal Year 1984 table Xll

164 ● Indian Health Care
Table 5-4.—IHS Medical and Dental Officers in Relation to Eligible Service Population by Area, Fiscal Year 1984a
IHS Service population ratios –
eligible service Clinical Physicians D e n t i s t s –
Area population (1984) Medical officers Dental officers per 1,000 per 1,000
Aberdeen . . . . . . . . . . . . . 70,648 25 20 0.4 0.3Alaska . . . . . . . . . . . . . . . 71,329 98 35 1.4 0.5Albuquerque . . . . . . . . . . 51,211 52 20 1.0 0.4Bemidji b. . . . . . . . . . . . . . 47,000 18 13 0.4 0.3Billings . . . . . . . . . . . . . . 40,106 40 17 1.0 0.4California b . . . . . . . . . . . . 71,642 1 0 0.0 0.0Nashville b . . . . . . . . . . . . 35,822 9 3 0.3 0.1Navajo . . . . . . . . . . . . . . . 162,005 145 42 0.9 0.3Oklahoma . . . . . . . . . . . . 190,451 94 44 0.5 0.2Phoenix . . . . . . . . . . . . . . 82,309 110 23 1.3 0.3Portland c . . . . . . . . . . . . . 96,427 25 17 0.3 0.2Tucson . . . . . . . . . . . . . . . 17,852 14 3 0.8 0.2Headquarters . . . . . . . . . 0 14 3 — —
IHS total . . . . . . . . . . . 936,802 645 240 0.7 0.3 -
aTb~ 44 ~edi~~l ~fflC~rs and 29 dent~l ~ffiCer~ ~~rvl”~ i“ “~”cllnlcal capacities during fiscal year 19W have been excluded from these calculations. AS In tables 5.2
and 5.3, IHS employees of Ir!bal 638 contract programs assigned under the Intergovernmental Personnel Act are !ncluded with IHS full-time, permanent staff. Staffhired directly by tribal 638 programs (former Federal and nonfederal) are not !ncluded
b Numbers of staff may be Iow ,n these areas, because direct trtbal employees of self-determination (638 contract) programs are not included Consequently service
population rat~os !n these areas may be lowc I HS staffl ng ,s IOW In the Portland area because there are no I HS hospitals there, and nearly half of the budget Is sPent On contract care
SOURCES U S Department of Health and Human Services, Publlc Health Service, Health Resources and Services Administration, Indian Health Service” service POPU.Iatlon est!mates are from the Population Statistics Staff, medical and dental officers In clinical practice are from the Of ftce of Indian Resources Llalson(unpublished data), 1985
missioned Corps (216). One of the most persua-sive arguments in support of the Transfer Act of1954 had to do with the recruitment of physicians,because at that time the BIA health program washeavily dependent on PHS for medical staff. ThePHS Commissioned Corps offered better careeropportunities than were available through BIA,including a commission that satisfied the militaryservice obligation (with the end of the draft, thisincentive ceased to exist).
Table 5-6 lists the number of PHS Commis-sioned Corps personnel serving in IHS in fiscalyear 1984, by area, broken down by Indian andnon-Indian officers and by clinical and nonclini-cal function. The 2,063 Commissioned Corpsofficers represented nearly 20 percent of total IHSstaff. Only 7.2 percent of those positions, how-ever, were filled by Indian members of the Corps.
The National Health Service Corps (NHSC)scholarship program, which now is being phasedout, has been another important source of phy-sicians for IHS. As of September 30, 1984, NHSCscholarships had been awarded to a total of 13,559individuals. During fiscal year 1984, 1,303 NHSCrecipients (including 1,131 physicians) began tofulfill their service obligations (164). Of these1,303 NHSC scholarship recipients, 185 accepted
placements in IHS: 155 physicians (in an IHS clin-ical care physician force of about 650), 22 nurses,and 8 dentists (196). In addition to working di-rectly for IHS, NHSC providers have been em-ployed in tribally operated 638 health programs;and in fiscal year 1983, nine urban Indian healthprojects received 18 NHSC assignees, represent-ing almost 14 percent of the urban projects’ totalmedical and dental staff (183). Nearly all physi-cians who enter IHS with NHSC scholarship pay-back obligations, however, leave after their obli-gation is fulfilled. Only about 5 percent stay atleast 1 additional year (38).
The IHS health manpower scholarship pro-grams, which are authorized by Title I of the In-dian Health Care Improvement Act, have severalspecial features designed to recruit and train newhealth professionals and to provide continuingeducation for IHS physicians, dentists, and otherhealth providers. Scholarships authorized by sec-tion 103 of Title I provide support to Indian stu-dents who require additional education to com-pensate for deficiencies in their prior academictraining in order to qualify for enrollment in ahealth professions school. Section 104 scholar-ships, which carry a service payback obligation,are awarded to students pursuing degrees in a va-riety of health professions. Non-Indians are eligi-

Ii
Table 5-5.—IHS Area Comparison of IHS Direct Care Workload by Clinical Units, Fiscal Year 1984a
( i ) (ii) (iii)Hospital days
(v) (vi) (vii) (viii) (ix)
Cl in ic Hospital - Cl inical units1984 service outpat ient outpatient A d u l t s Clinical Total C l in i ca l C l in i ca l un i t s per clinical
Area population visits visits and peals. Newborns units staff staff per staff staff
Aberdeen . . . . . . . . 70,648 116,660 29<,104- 44,612 -2,654 115,893 915” 476 127 243Alaska . . . . . . . . . . 71,329 64,508 197,872 68,084 4,348 116,162 1,260 600 92 194Albuquerque. . . . . 51,211 108,754 162,900 27,467 1,485 74,228 918 488 81 152Bemidji . . . . . . . . . 47,000 47,037 62,349 5,380 242 23,853 270 146 88 163Billings . . . . . . . . . 40,106 169,519 100,866 11,819 800 57,683 616 292 94 198California . . . . . . . 71,642 86,440b NA NA NA o 61 5Nashville. . . . . . . .
—35,822
—4,563 56,338 6,329 199 16,678 189 105 88 159
Navajo . . . . . . . . . . 162,005 111,305 462,894 88,813 9,881 194,394 2,033 1,191 96 163Oklahoma . . . . . . . 190,451 254,337 312,036 49,653 7,830 151,879 1,605 921 95 165Phoenix . . . . . . . . . 82,309 94,510 295,289 80,439 3,436 148,842 1,546 795 96 187Portland . . . . . . . . 96,427 212,547 NA NA NA 35,425 388 184 91 193Tucson . . . . . . . . . 17,852 22,388 36,616 7,315 184 17,333 154 85 113 204Headquarters . . . . 0 NA NA NA NA o 387 72 — —
IHS total . . . . . . 936,802 1,206,128 1,982,264 389,911 3 1 , 0 5 9 952,369 10,342 5,360 92 178aUtl I tzatlon f!gu res I n this table represent IHS dl rect care workloads Outpatient visits to trl bal Iy operated factl !tles and urban projects, and utl I Izatlon data for the contract care program are not Included I n
.—
this table Columns (I) through (Iv) Include IHS facll!tles Only. column (v) assumes 6 outpatient vIsIts equal 1 hosp!tal day, and columns (VI) and (VII) Include Federal employees asstgned to tribal 638 contractprograms through the Intergovernmental Personnel Act. but not staff h!red directly by the tribal 638 contractors
bprovlsional data from California Program Off Ice Workload Statlstlcal Summary, calendar year 1984
SOURCES u S Department of Health and Human Serwces. publlc Health Service Health Resources and Servtces Admlnlstratlon Indian Health Service Service Population estimates from the Population Statls-tlcs Staff, outpatient vlslts and hospital days from the Patient Care Statlstlcs Staff. total staff and cllnlcal staff from the Off Ice of Indian Resources Llalson (unpubhshed data). 1985
II
ii
II

166 ● Indian Health Care
Table 5-6.—IHS Indian and Non-Indian Commissioned Corps Officers byClinical and Nonclinical Function, Fiscal Year 1984a
Indian Non-Indian Corps PercentArea Clinical Nonclinical Total Clinical Nonclinical Total total by area
Aberdeen . . . . . . . . . . . . . 11 2 13 102 29 131 144 7.0 ”/0Alaska . . . . . . . . . . . . . . . 5 0 5 215 44 259 264 12.8Albuquerque . . . . . . . . . . 10 4 14 137 30 167 181 8.8Bemidji . . . . . . . . . . . . . . 4 0 4 78 16 94 98 4.8Billings . . . . . . . . . . . . . . 7 1 8 91 11 102 110 5.3California. . . . . . . . . . . . . 1 0 1 5 18 23 24 1.2Nashville . . . . . . . . . . . . . 0 0 0 39 9 48 48 2.3Navajo . . . . . . . . . . . . . . . 23 1 24 272 58 330 354 17.2Oklahoma . . . . . . . . . . . . 30 3 33 229 37 266 299 14.5Phoenix . . . . . . . . . . . . . . 27 1 28 257 43 300 328 15.9Portland . . . . . . . . . . . . . . 10 1 11 84 16 100 111 5.4Tucson . . . . . . . . . . . . . . . 1 1 2 26 3 29 31 1.5Headquarters . . . . . . . . . 1 5 6 37 28 65 71 3.4
IHS total . . . . . . . . . . . 130 19 149 1,572 342 1,914 2,063 100.0”/0–aNO! i“~lud~d in !fli~ !abl~ are direct employees Of tribal self-determination 638 programs These exclusions affect some areas (e.g., Bernld~i, cdifOrn@ and N=hV@more than others.SOURCE U.S. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Indian Health Service, Indian Resources
Liaison, computer printouts dated 01/1 7/85 and 9/30/85.
ble for scholarships authorized by section 104,although preference is extended to Indian ap-plicants.
To determine the staffing categories for whichscholarships will be awarded under its health man-power programs, IHS uses the resource require-ment methodology, combined with informationon current vacancies, attrition, and turnover. Forthe academic and fiscal year 1986, for example,section 103 scholarships were awarded in nurs-ing and accounting and, for juniors and seniors,in premedicine and predentistry. Section 104scholarships were awarded to students in medi-cine, nursing, accounting, master of public healthprograms, health records, pharmacy, engineering,nutrition/dietetics, sanitary science, and medicaltechnology. From 1979 through the beginning offiscal year 1986,2,004 students had received IHShealth scholarship program support (24).
IHS scholarship programs have had a dropoutrate approaching 40 percent, but are credited withthe graduation of 600 health professionals since1979 (unfortunately, information is not availableto specify graduates by profession). Approxi-mately 80 percent of the 600 who have graduatedcontinue to work for IHS (24). Thus, as a train-ing and recruitment mechanism, the Indian healthmanpower scholarship programs hold promise.At present operating levels, however, it is notlikely that the programs can support enough phy-
sicians to meet the expected loss of NHSC physi-cians. In addition, the scholarship programs areauthorized and funded under the Indian HealthCare Improvement Act, the reauthorization forwhich was vetoed in 1984 and had not beenreenacted by the end of 1985; but the programsstill operate under continuing resolution funding.
Although the retention of health care person-nel, including NHSC assignees, traditionally hasbeen viewed as a problem for IHS, the tribes alsohave a responsibility to take an active role in ad-dressing it. Better retention of NHSC scholars af-ter their obligations are completed could signifi-cantly enhance the stability of IHS medical staffin all areas. For the tribes, a more stable medicalstaff would improve the quality and range of serv-ices provided. It would be helpful if PHS Com-missioned Corps officers were available for relo-cation within the system as needed, but there arelimits to what can be done in the way of volun-tary relocations. Remedying apparent staffingdeficiencies in certain IHS areas would requireacceptance by IHS and the tribes of a method ofallocation that is driven more by relative need ordemand than by historical funding patterns. Al-though a major redistribution of IHS health caredelivery staff may not be easy to implement, theranges in direct care physician- and dentist-to-population ratios and in clinical unit workloadrates among IHS areas suggest that further workon this subject is in order.

Ch. 5—The Indian Health Service ● 167
Policies governing NHSC placements requirethat scholarship recipients repay their service obli-gations in designated health manpower shortageareas. These areas are designated by PHS on thebasis of detailed sets of criteria involving geog-raphy, population characteristics, the availabil-ity of facilities, and other factors. Indian andAlaska Native groups are automatically desig-nated as having primary care manpower short-ages if they are groups of members of federallyrecognized tribes as defined in section 4 (d) of theIndian Health Care Improvement Act. If the In-dian groups fit section 4 (c) of the act, the def-inition applicable to Indians who may not bereservation-based members of federally recog-nized tribes but who meet other criteria of beingIndian, they may be designated if they meet othermanpower shortage criteria applicable to non-Indian populations (42 CFR Part 5 app. A), Inother words, all IHS service units are eligible forNHSC assignments, and IHS receives priority con-sideration in those assignments (60). Private prac-tice options in medically underserved areas alsoare acceptable for NHSC paybacks and may pro-vide some services to Indians.
In the absence of the NHSC, IHS will have torely more heavily on the PHS CommissionedCorps and on its own scholarship programs to en-sure a future supply of professionals, especiallyphysicians, who are willing to work on reserva-tions, A recent study of the U.S. medical schoolclass of 1975 found that minority physicians ofthat class now provide more care to patients oftheir own racial or ethnic groups and to Medic-aid patients than do their nonminority counter-parts (59).
Problems of training and retaining health pro-fessionals will become critical for IHS over thenext 5 years as the NHSC program is phased out.Although IHS has received preferential consider-ation with respect to the assignment of NHSCscholars in the past, that special relationship isnot expected to continue beyond 1986. NHSC hasplaced 1,083 scholars who will begin repayingtheir service obligations in July 1986. Of this num-ber, IHS requested 142 physicians and its requestwas met. Fifty-six of the IHS assignees, almost 40percent, had elected to work in the IHS system;the remaining 86 were assigned to IHS without
having indicated such a preference. While NHSCis no longer trying to project the distribution ofplacements beyond the 1986 cycle, its scholarshipbranch currently estimates that the followingnumbers of scholars (a few are not physicians) willbe available in future years, from which IHS hasno guaranteed assignments: 886 scholars in 1987;413 in 1988; 76 in 1989; and 4 in 1990 (52). Thesefigures may be slightly overestimated, subject toreduction for scholars choosing to buy out theirobligation and for deaths.
The need to develop strategies for the replace-ment of NHSC medical personnel in the IHS sys-tem is an imminent problem. NHSC has begunto recruit unobligated physicians and other healthprofessionals for career positions. Its goal is toestablish and maintain permanent practices inareas having health manpower shortages. Al-though the success of such an approach wouldhave been limited in recent years by a lack of in-dividuals willing to practice in rural areas, con-ditions are changing. Economic factors such as aprojected oversupply of physicians, along witha slight decrease in the average annual earningsamong physicians and changes in health care de-livery systems (e.g., greater enrollment in healthmaintenance organizations, which require fewerphysicians), may mean that more physicians willbe available and willing to work in rural areas.The Federal Government could encourage thispossibility by strategies such as NHSC as a ca-reer or by offering financial incentives to individ-uals in exchange for agreements to work in under-served areas.
One difficulty with Federal intervention intomedical manpower distribution is that commit-ments from health professionals are generallyshort term. In addition, the public may not be sup-portive of education subsidies in a field where sup-ply now exceeds anticipated needs in many partsof the country. Bills have been pending in bothHouses of Congress to extend the life of NHSCfor 3 years: the Senate bill (S. 1285) would allow450 new scholarships, and the House bill (H.R.2234) would authorize 1,176 new scholarshipsover 3 years. Neither of these bills would makea significant contribution toward replacing IHS’sprojected loss of physicians, unless a large propor-tion of the new scholarships was targeted for pay-back in IHS.

168 ● Indian Health Care
Another option that is more directly withinIHS’s control would be to increase the number ofIHS health manpower training scholarships avail-able to persons for undergraduate degrees in pre-medicine, accompanied by a strengthened com-mitment to students in medical school throughincreased scholarship support. This option couldbe designed to include scholarships for otherhealth professionals and might include non-In-dians as well as Indians. Indian medical studentsalso might be assisted through the activities ofprofessional organizations such as the Associa-tion of Native American Medical Students and itsparent organization, the Association of AmericanIndian Physicians.
The recruitment of physicians to replace NHSCassignees from outside the Federal sector is anotherpossibility. The potential of such an approach hasnot yet been examined, but large-scale directhiring of medical personnel would have to beweighed carefully against the feasibility and costsof expanded contracting for needed staff andservices.
Delivery of Direct Care Services
IHS direct care services are delivered throughan organizational structure of area and programoffices and service units. The eight area officesand four smaller program offices (Tucson, Be-midji, Nashville, and California) serve definedgeographic areas of varying sizes and service pop-ulations. Area and program office staffs allocateannual budgets among their several service units,which are the basic health care delivery units. Asof October 1984, there were 123 service units, ofwhich 44 were operated by the tribes under self-determination (638) contracts (191). Direct careservices are delivered (or monitored, in the caseof 638 contract services), and contract care refer-rals are authorized at the service unit level. Likethe areas, the service units are responsible forvarying budget allocations, eligible populations,and numbers of facilities.
The types of facilities in the IHS direct care de-livery system include hospitals, health centers,health stations, health locations, and school healthcenters. The 51 IHS and tribally operated hospi-tals (discussed in greater detail below) vary greatlyin size and service capabilities: for example, only
13 of them offer staffed surgery services. Most ofthe hospitals have active outpatient departmentsand often are the location for outpatient dental,mental health, and alcoholism services. Healthcenters are relatively comprehensive outpatientfacilities that are open at least 40 hours per week.Health stations, which include some mobile units,are open fewer than 40 hours per week and offerless complete ambulatory services. Health loca-tions are generally outpatient delivery sites (butnot IHS facilities) that are staffed periodically bytraveling health personnel.
Figures 5-4 and 5-5 illustrate recent trends inhospital occupancy rates and average length ofstay for all IHS hospitals, U.S. community hos-pitals, and U.S. nonmetropolitan community hos-pitals. IHS hospitals are smaller than the averageU.S. community hospital; two-thirds of IHS hos-pitals (compared with about one-fifth of all U.S.community hospitals) have fewer than 50 beds.IHS hospital occupancy rates, in the range of 50to 55 percent, have been consistently lower than
Figure 5-4.—Occupancy Rates in All U.S. CommunityHospitals, U.S. Nonmetropolitan Hospitals,
and IHS Hospitals, Fiscal Years 1970.85
A l l I H S h o s p i t a l s
U.S. nonmetropol i tan hospi ta ls
‘----- All U.S. community hospitals
SOURCES: For all U.S. short.stoy community hospitals and U.S. nonmetro@itan corn.munity hoapitala: AHA /+ospita/ Statistics, editions for 1971 through1984 IHS hospitala: U.S Department of Health and Human Services,Public Health Service, Health Resources and Sewices Adm(nlstra.tlon, Indian Health Service, “Inpatient and Outpatient Summary Datafor Ind!an Health Serwce Hospitals by Area and Facility, ” fiscal years1970-85.

Ch. 5—The Indian Health Service ● 169
Figure 5-5.–Average Length of Stay in All U.S.Community Hospitals, U.S. Nonmetropolitan
Hospitals, and IHS Hospitals, Fiscal Years 1970-85
9 t -
8.5
5.5
K
.— ------ - --- ---
1 1 1 I I I t I 1 1 I I I J.1972 1974 1976 1978 1980 1982 1984
Fiscal year
A l l I H S h o s p i t a l s
U S nonmetropolitan hospitals
-–––-– A l l U S communi ty hosp i ta ls
SOURCES For all U.S. shOrt.st8y community hospitals and U.S. nonmetropolitan corn.munity hospitals: AHA l-losp~tal S/at/s t/es, edltlons for 1971 through1984 IHS hospitals: U S Department of Health and Human SerwcesPubllc Health Service Health Resources and Services Admln!stratlon Indian Health Service ‘Inpatient and Outpatient Summary Datafor Indian Health Serwce Hosp!tals by Area and Faclllty ‘ fiscal years197085
the average 75 percent occupancy for all U.S.community hospitals. U.S. nonmetropolitan com-munity hospitals, which are closer to IHS hospi-tals in size and range of services, have experiencedoccupancy rates of 65 to 70 percent (3).
Average lengths of stay (figure 5-5) in IHS hos-pitals have fallen from well above to below theaverage stays in all U.S. community and U.S.nonmetropolitan hospitals. While inpatient staysheld relatively stable until 1983 at just below 8days per stay in all U.S. community hospitals andbetween 7 and 7.5 days in nonmetropolitan hos-pitals (3), the average length of stay in IHS hos-pitals has declined steadily from a high of nearly9 days per stay in 1970 to 4.9 days in 1984. It islikely that the lower average length of stay in IHShospitals relates to the comparatively limitedrange of inpatient services many of these facilitiesoffer (patients requiring specialized care usuallyare referred to private hospitals under contractcare), but how much is explained by this factoris not known.
Figure 5-6.- Number of Admissions to IHS andContract and Tribal Hospitals, Fiscal Years 1970-85
1970 1975 1980 1985
Fiscal yearSOURCE U S Department of Health and Human Services, Publ!c Health Serv.
ice, Health Resources and Serwces Adml nlstrat Ion, Indian Health ServIce, Chart Ser/es Book, Rockvllle, MD, April 1985
Total numbers of admissions to IHS hospitalspeaked in 1978 at about 112,000 (including IHSand tribally operated hospitals, and contract careinpatient referrals) and have declined since thattime to about 103,000 admissions in 1984 (see fig-ure 5-6 and table 5-7). Contract care admissionsdeclined more sharply than admissions to IHS di-rect care and tribally operated hospitals, whichsuggests the effects of limited contract care budg-ets. The combination of declining admissions andaverage lengths of stay explains the low anddeclining occupancy rates of IHS hospitals. Giventhe substantial increase in IHS’s estimated eligi-ble service population since 1970, however, otherfactors such as limited access to facilities, a limitedrange of services, and differences between IHS’sestimated service population and its actual userpopulation may contribute to declining hospitalutilization. The overall hospital utilization ratedecreased from 206 admissions per 1,000 IHS pop-ulation in 1970 to 125 per 1,000 in 1984 (table 5-7). This compares with a current hospital utiliza-tion rate for the U.S. general population of about159 discharges per 1,000 in 1982 (202). Figure 5-7 and table 5-8 show that the average number ofpatients receiving inpatient care (the average dailypatient load) in IHS direct, IHS contract, andtribally operated hospitals combined has declinedsince 1980.
The discussion that follows will focus on healthfacilities and programs at the IHS area office level,including those operated by tribes under 638 self-determination contracts. (Detailed listings of fa-

170 ● Indian Health Care
Table 5-7.—Number of Admissions and Utilization Rate for IHS, Contract, andTribal Self. Determination Hospitals, Fiscal Years 1955-84
Total utilization Total IHS and Indian Health Service
Fiscal year ratea tribal admissions Total IHS Contract b Tribal
1984 . . . . . . . . . . . . . . . . . 124.6 102,843 99,849 77,522 22,327 2,9941983 . . . . . . . . . . . . . . . . . 130.1 104,806 102,961 78,027 24,934 1,8451982 . . . . . . . . . . . . . . . . . 132.7 104,418 102,343 77,070 25,273 2,0751981 . . . . . . . . . . . . . . . . . 142.3 109,353 107,087 81,387 25,700 2,2661980 . . . . . . . . . . . . . . . . . 144.3 108,242 106,992 77,798 29,194 1,2501979 . . . . . . . . . . . . . . . . . 157.8 107,269 106,329 75,174 31,155 9401978 . . . . . . . . . . . . . . . . . 179.0 112,203 112,203 77,567 34,6361977 . . . . . . . . . . . . . . . . . 181.5 110,025 110,025 78,424 31,6011976 . . . . . . . . . . . . . . . . . 197.9 106,461 106,461 76,382 30,0791975 . . . . . . . . . . . . . . . . . 212.2 105,735 105,735 74,594 31,1411974 . . . . . . . . . . . . . . . . . 218.2 103,853 103,853 73,402 30,4511973 . . . . . . . . . . . . . . . . . 213,5 102,350 102,350 75,245 27,1051972 . . . . . . . . . . . . . . . . . 218.2 102,472 102,472 76,054 26,4181971 . . . . . . . . . . . . . . . . . 206.6 94,945 94,945 70,729 24,2161970 . . . . . . . . . . . . . . . . . 205.7 92,710 92,710 67,877 24,8331965 . . . . . . . . . . . . . . . . . 226.1 91,744 91,744 67,744 24,0001960 . . . . . . . . . . . . . . . . . 201.9 76,754 76,754 56,874 19,880
1955 . . . . . . . . . . . . . . . . . 150.2 50,143 50,143 42,762 7,381aNUrnber Of admissions per 1,000 IHS estimated eligible service population.bfqumberof discharges used as estimate for numberof admissions.
SOURCE: U.S. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Indian Health Service, /HSCharfSer./es Book, April 1985 Data published astable5.5, from the following IHS documents: IHS Monthlv ReDort of lnDatient Services: Annual ReDof131 for contracthospitals; and area submissions for tribal hospitals.
Figure 5.7.—Average Daily Patient Load in IHS,Contract, and Tribal Hospitals, Fiscal Years 1970.85
2,500 Contract and tribal
2,000
a 1500a,E
z 1,000
500
0 1
1970 1975 1980 1985
Fiscal year
SOURCE U S. Department of Health and Human Services, Public Health Serv.ice, Health Resources and Services Administration, Indian Health Serv-ice, Charl Series Bookr Rockville, MD, April 19S5
cilities by type, with utilization data, by serviceunit and associated tribe, State, and IHS area areavailable from the Office of Technology Assess-ment (OTA). )
Table 5-9 summarizes the numbers of health fa-cilities by IHS area and type, with utilization data,in fiscal year 1984. Two areas, Portland and Cali-fornia, have no IHS hospitals and hence no di-rect inpatient care. The small (18,000 service pop-
,. -, -r
ulation) Tucson program office has one 40-bedhospital, the Nashville area has one IHS and onetribally operated hospital, and there are two IHShospitals in the Bemidji area (both in Minnesota).The Phoenix and Aberdeen areas are served bynine hospitals each, all operated by IHS. Thereare five IHS and two tribally operated hospitalsin Alaska (as of January 1986, a third IHS hospi-tal converted to tribal control). The three IHS hos-pitals that are considered major medical referralcenters, even though they do not offer all tertiaryservices, are located in Anchorage, Phoenix, andGallup. Excluding California and Portland, whichhave no hospitals, inpatient beds per 1,000 IHSestimated eligible service population ranged fromless than 1 bed per 1,000 in Bemidji (an area thatis heavily dependent on contract care) to a highof 5.4 in Alaska (1984 beds and populations). TheIHS average was about 2.4 beds per 1,000 (1984,combining IHS and 638 hospital beds). In 1982,there were 4.4 community short-stay hospital bedsper 1,000 U.S. population, ranging from 3.3 per1,000 in the Pacific region to a high of 5.9 per1,000 in the West North Central region (includ-ing the Dakotas and Minnesota) (202).

—
Ch. 5—The Indian Health Service ● 171
Table 5-8.—Average Daily Patient Load (ADPL) in IHS, Contract, and TribalSelf-Determination Hospitals, Fiscal Years 1955-84
Indian Health Service
Fiscal year Grand total ADPL Total IHS Contract Tribal
1984 . . . . . . . . . . . . 1,392 1,353 1,072 281 391983 . . . . . . . . . . . . 1,477 1,449 1,119 330 281982 . . . . . . . . . . . . 1,488 1,460 1,121 339 281981 . . . . . . . . . . . . 1,575 1,550 1,194 356 251980 . . . . . . . . . . . . 1,594 1,576 1,178 398 18
1979 . . . . . . . . . . . . 1,586 1,569 1,192 377 171978 . . . . . . . . . . . . 1,723 1,256 4671977 . . . . . . . . . . . . 1,710 1,302 4081976 . . . . . . . . . . . . 1,736 1,299 4371975 . . . . . . . . . . . . 1,768 1,330 438
1974 . . . . . . . . . . . . 1,840 1,376 4641973 . . . . . . . . . . . . 2,013 1,499 5141972 . . . . . . . . . . . . 2,172 1,626 5461971 . . . . . . . . . . . . 2,177 1,627 5501970 . . . . . . . . . . . . 2,353 1,729 624
1965 . . . . . . . . . . . . 3,127 2,244 883
1960 . . . . . . . . . . . . 3,142 2,232 910
1955 . . . . . . . . . . . . 3,711 2,531 1,180SOURCE” US Department of Health and Human services, Public Health serviCf3, Health Resources andSemiceSAdrnifliStra.
tion, lndian Health ServlCe, lllSChwtSeries Book, April 1965 Data publlshedas table 56, frornthf3 follow!flg IHSdocuments” IHS Monthly Report of Inpat!ent Services, Annual Report 31 for contract hosD!tals, and area submlssions for tribal hospitals.
IHS hospitals differ from the typical U.S. com-munity hospital in that IHS hospitals are older,smaller in bed size, and more limited in the rangeof inpatient services they offer. The average IHShospital is more than 35 years old. Of the 47 hos-pitals operated by IHS, 18 were built before 1940,3 were built between 1940 and 1954, and 26 havebeen built since responsibility for Indian healthwas transferred to the Department of Health, Edu-cation, and Welfare (now DHHS) in 1955 (135).
In 1984, the IHS system consisted of 47 hospi-tals operated by IHS plus 4 hospitals operated bytribes: the hospitals at Dillingham and Nome,Alaska; the Creek Nation hospital in Oklahoma;and the Choctaw hospital in Mississippi. As ofFebruary 1986, two more IHS hospitals had con-verted to tribal operation, the Mt. Edgecumbehospital in Southeast Alaska and the OklahomaChoctaw hospital at Talihina. As of January 1985,40 of the 47 IHS-operated hospitals were accred-ited by the Joint Commission on Accreditation ofHospitals (JCAH); the remaining 7 were not ac-credited (191). All four of the tribally operatedhospitals had JCAH accreditation. JCAH accred-itation represents a minimum level of adequacyin a hospital’s physical facility, equipment, and
staffing. Many IHS hospitals have correctedJCAH deficiencies since 1976, when only 23 of 51hospitals were accredited. In 1984, 38 of the 47IHS-operated hospitals met national fire andsafety standards, and all hospitals are certified toreceive Medicare and Medicaid reimbursements.
Most IHS hospitals are small, and many aremore isolated geographically than the averageU.S. community hospital even in nonmetropoli-tan areas. In 1982, the average U.S. hospital had174 beds. Only 20 percent of all U.S. hospitalshad 50 beds or fewer (representing about 4 per-cent of total beds). Two-thirds of the hospitalsoperated by IHS are in that size category (3).Twelve of the 47 IHS-operated hospitals havefrom 50 to 99 beds, and only 4 exceed 100 beds:Anchorage, Phoenix, Tuba City, and Gallup. FiveIHS hospitals have only 14 or 15 beds (60).
Differences between IHS and U.S. communityhospitals also are apparent in the scope of serv-ices they offer. In general, an IHS hospital is likelyto provide a relatively wide range of health-relatedand social support services (e.g., social work, out-patient psychiatric and alcoholism services, familyplanning) and fewer high-technology services. Anespecially noticeable difference is in the availabil-

172 ● Indian Health Care
Table 5-9.—IHS and Tribally Operated Self-Determination (638) Facilities by IHS Area,With Fiscal Year 1984 Utilization
Hospitals Health centers Health stationsc
— —
70,648
71,329
51,211
47,000
40,106
71,642
35,822
162,005
190,451
82,309
96,427
17,852
9—
52
5—
2—
3—
——
11
6—
61
9—
——
1—
323—
34343a
209—
41—
86—
——
3535a
400—
29139a
369—
——
40—
Admissions visits Number visits b Number visits b
1984 IHS service Outpatient Outpatient OutpatientIHS area population Number Beds a
Aberdeen . . . . . .IHS . . . . . . . . .638 . . . . . . . . .
Alaska. . . . . . . . .IHS . . . . . . . . .638 . . . . . . . . .
Albuquerque . . .IHS . . . . . . . . .638 . . . . . . . . .
Bemidji . . . . . . . .IHS . . . . . . . . .638 . . . . . . . . .
Billings . . . . . . . .IHS . . . . . . . . .638 . . . . . . . . .
California . . . . . .IHS . . . . . . . . .638 . . . . . . . . .
Nashville . . . . . .IHS . . . . . . . . .638 . . . . . . . . .
Navajo . . . . . . . .IHS . . . . . . . . .638 . . . . . . . . .
Oklahoma. . . . . .IHS . . . . . . . . .638 . . . . . . . . .
Phoenix . . . . . . .IHS . . . . . . . . .638 . . . . . . . . .
Portland . . . . . . .IHS . . . . . . . . .638 . . . . . . . . .
Tucson . . . . . . . .IHS . . . . . . . . .638 . . . . . . . . .
Totals . . . . . . . 936,802IHS . . . . . . . 47 2,137 77,316 1,976,962 71 975,689638 . . . . . . . 4 117a 2,994 50,151 53 714,961b
aFOrtriballyOperated Self.deterrnination (638) hospitals, numbersof beds are reported from the 1984AHA Guicfe(1983 survey data), because that information was notreported by IHS, Numbers of admissions and outpatient visits, however, are from the same 1984 IHS sources as for IHS hospitals,
bout patient visits t. tribally operated health stations and to Alaska’s 172 village clinics, not avatlable separately, are included in numbers of VlsitS to 638 health centerScNumbers of health stations include Indian school health centers and the 172 village clinics in Alaska Health Iocatlons are not Included.
SOURCE U S. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Indian Health Service, Office of Plan-nlng, Evaluation, and Legislation, Program Statistics Branch, 1985
10,725—
9,8801,483
5,629—
1,597—
3,472—
——
1,103693
18,638—
11,586818
13,401—
——
1,285—
295,104—
197,87226,369
162,900—
62,349—
100,866—
——
51,03618,798
462,894—
312,0364,984
295,289—
——
36,616—
42
53
81
27
9—
—17
—10
91
176
32
124
2—
42,99828,612
64,497257,866
75,65213,620
33,478110,742
157,211—
—121,306
—76,142
105,7893,144
240,87059,558
31,18611,321
202,55532,650
21,453—
202
—172
121
711
3—
—10
14
13—
4—
11—
49
1—
73,662—
——
33,102—
13,559—
18,690—
——
4,563—
59,402—
13,467—
63,324—
9,992—
935—
76C 290,696209C —b
ity of surgical services. Of the 51 IHS and triballyoperated hospitals, only 13 offer staffed surgeryservices (5 of these 13 are in Oklahoma), and anadditional 4 hospitals deliver modified or limitedsurgery using part-time contract surgeons, for ex-ample, rather than staff surgeons. Difficulties inrecruiting and retaining medical staff limit thetypes of services available at many IHS hospitals,and surgeons are particularly difficult to recruit,in part because there are no NHSC scholarshipsfor surgeons.
The IHS major medical centers at Anchorage,Phoenix, and Gallup do not provide some of thesophisticated services that would be expected atmany university teaching hospitals. The follow-ing are among the services not provided in anyIHS hospital, according to the 1983 AmericanHospital Association Annual Survey of Hospitals:cardiac intensive care unit, open heart surgery,cardiac catheterization, X-ray radiation therapyand other megavoltage and radio-isotope thera-peutic services, organ transplantation, burn care,

Ch. 5—The Indian Health Service ● 173
and neonatal intensive care. Only nine IHS hos-pitals have a separate mixed intensive care unit,four operate premature nurseries, and three pro-vide hospital-based renal dialysis (Tuba City,Sells, and Mississippi Choctaw). On the otherhand, 32 of 51 IHS and tribally operated hospi-tals have obstetrical services and 42 offer dentalservices. Although outpatient psychiatric and al-coholism services are widespread, there is onlyone inpatient alcoholism service and there are fiveinpatient psychiatric units (2). In part because IHSdirect inpatient services are relatively limited evenwhere hospitals are accessible, the IHS contractcare program (see discussion below) has been un-der increasing budgetary pressures in recent yearsto fill these service gaps.
In contrast to a declining trend in inpatient uti-lization, total ambulatory visits provided by IHShospitals and direct care clinics, contract carereferrals, and tribal facilities have more than dou-bled since 1970 (see figure 5-8 and table 5-10).About half of the total visits were delivered byIHS hospital outpatient departments, The num-ber of ambulatory care visits provided by IHS di-rect care hospitals and clinics only has increasedby nearly 80 percent since 1970, while contractcare visits have declined by 24 percent since 1980and visits to tribally operated facilities increasedby 36 percent in that same period.
There were 1,786,920 ambulatory visits in 1970for a total service population of 460,000, or about3.9 visits per person. In 1984, 4,231,772 visits wereprovided (down slightly from totals for 1981 and1982) for 936,802 eligible beneficiaries, a rate of
Figure 5-8.— Numbers of Outpatient Visits to IHS,Contract, and Tribal Facilities, Fiscal Years 1970-85
5 r
IHS contractTotal
\> T r i b a l f a c i l i t i e s -
1- \4 . I H S f i e l d c l i n i c s
1970 1975 1980 1985Fiscal year
SOURCE U S Department of Health and Human Services, Public Health Serv.!ce, Health Resources and Services Admlnlstratlon, Indian Health ServIce Chart Series Book, Rockvl I Ie, MD, Aprtl 1985
4.5 visits per person. In 1981, when the annualrate of IHS outpatient visits was 5.0 per person,all Americans made an average of 4.6 visits to hos-pital outpatient departments, clinics, group prac-tices, and physicians’ offices (202). Therefore, onthe basis of utilization rates alone, it cannot beargued that IHS beneficiaries do not have ade-quate access to ambulatory services. On the otherhand, however, national data indicate that higherrates of outpatient visits are to be expected amongpopulations like those of IHS that are atypicallyyoung (under 6 years of age) or old (45 yearsand older), nonwhite, and in low family incomegroups.
The distribution of ambulatory care facilitiesamong IHS areas and their approximate utiliza-tion in 1984 are shown in table 5-9 (referred toearlier). Utilization is approximate because not allof the tribally operated 638 facilities report to IHSdata systems, and 638 clinics provide a substan-tial amount of health care in some areas. All ofthe ambulatory care facilities in California, forexample, which are the only direct services pro-vided by IHS, are 638 facilities. In the Nashvillearea, all clinics except one health station are trib-ally operated. When health stations and locationsare excluded because of their small size and vari-able operating schedules, a comparison of healthcenter availability among IHS areas reveals thatthe heaviest concentrations of facilities are inOklahoma, California, and Portland.
Conclusions
IHS defines its responsibility for the health ofAmerican Indians to include many services thatare beyond the scope of basic inpatient and am-bulatory medical care. This broad definition seemsappropriate to meet the special health needs andservice delivery problems of isolated reservation-based Indian populations. As is discussed later inthis chapter, however, IHS does not extend thisbroad definition to the health care needs of In-dians living in urban areas. The IHS’s traditionalfocus, derived from the long history of BIA in-volvement in Indian health, has been to serve res-ervation Indians. That role has been challengedin recent years by advocates of urban Indians.How to balance its response to the conflicting de-mands of these two groups, within current budg-

174 ● Indian Health Care
Table 5-10.—Numbers of Outpatient Visits to IHS, Contract, and Tribal Facilities,Actual for Fiscal Years 1955.84 and Estimates for 1985.86
Fiscal year
1986 (est.) . . . .1985 (est.) . . . .
1984 . . . . . . . . .1983 . . . . . . . . .1982 . . . . . . . . .1981 . . . . . . . . .1980 . . . . . . . . .
1979 . . . . . . . . .1978 . . . . . . . . .1977 . . . . . . . . .1976 . . . . . . . . .1975 . . . . . . . . .
1974 . . . . . . . . .1973 . . . . . . . . .1972 . . . . . . . . .1971 . . . . . . . . .1970 . . . . . . . . .
1965 . . . . . . . . .
1960 . . . . . . . . .
1955 . . . . . . . . .
Indian Health Service
Grand total
4,200,0004,210,000
4,231,7724,190,7214,266,7764,284,1984,058,568
3,880,850
Total Hospitals
3,200,000 2,010,0003,200,000 1,990,000
3,248,660 1,982,2643,252,701 1,955,4623,334,365 1,973,6883,319,479 1,934,5903,194,935 1,795,607
3,083,350 1,710,6863,124,716 1,783,6422,980,850 1,715,1142,751,546 1,593,1302,501,050 1,465,816
2,361,654 1,366,5642,329,160 1,330,6602,235,881 1,275,7262,195,236 1,202,0271,786,920 1,068,820
1,325,400 757,700
989,500 585,100
455,000 355,000
Health centers(including schools) Other
950,000970,000
1,019,7641,049,8431,109,9601,155,2941,120,737
1,059,6901,009,960
910,356871,796778,411
240,000240,000246,632247,396250,708229,595278,592312,974331,114335,380286,620256,823
719,700 275,390712,282 286,218603,443 356,712572,869 420,340459,713 258,386
567,700
404,400100,000
Contract
200,000210,000
218,000a
236,690236,706266,577b
275,000 ab
275,000 ab
Tribal
800,000800,000765,112701,330695,705698,142588,633522,500a
aEstlmate,bcomparable contract care data not available prior to fiscal year 1981.
SOURCE: U.S. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Indian Health Service, //-/S Chati SeriesBook, April 19S5. Data published as table 5.11
etary constraints, is a problem that IHS must be-gin to address. According to the 1980 U.S. census,54 percent of the 1.4 million individuals who iden-tified themselves as Indian lived in metropolitanareas. Most urban Indians now are excluded fromIHS estimated service populations; but a gradualstrengthening of urban Indian claims for IHS serv-ices may be anticipated if urban Indian popula-tions continue to grow.
Whether in an urban or a reservation setting,however, the delivery of health services to Amer-ican Indians cannot be accomplished by the samemeans used to provide health care to the generalU.S. population. The socioeconomic, cultural,and geographic isolation of many Indians, and thedominating presence of the Federal Governmentthrough IHS and BIA, create circumstances thatnecessitate special approaches to health care de-livery. Independent of problems relating to IHSfunding levels, the expressed demand for healthservices and the availability of IHS facilities varyso much from one IHS area to another that nosingle benefits package or delivery strategy islikely to be successful in all areas. In some areas,
few health services other than those provided byIHS are readily available and accessible to Indianpopulations. Even in areas where non-IHS “alter-nate resources” (other public and private healthcare providers) are available, some Indians whohave private insurance may prefer to use IHS di-rect services because they feel they are entitled tothem, they want to avoid the deductibles andcopayments associated with private insurance, orthey feel more comfortable with IHS than withprivate providers.
This section of chapter 5 has presented a de-scription of the IHS direct care program centeredon the most important component of that pro-gram, the medical services provided by IHS andtribally operated hospitals and clinics. It may beconcluded that the volume and scope of IHS hos-pital and clinic services vary considerably amongthe areas, apparently without consistent basis.The inventory of services provided directly byIHS and by tribal 638 facilities reveals a systemthat has evolved in an unplanned manner in re-sponse to changing BIA and IHS policies forhealth care delivery, variable and incompletely

Ch. 5—The Indian Health Service ● 175
documented local needs and demands, and thelimits of available funding as appropriated byCongress. Clearly, IHS does not deliver the samepackage of health services in each of its areas. Thismay not necessarily be bad, because it is likelythat health problems also differ among the areas.However, it appears that there have been no sys-tematic attempts to match the services that aredelivered to area-specific health problems andservice needs. Both among and within the 12 areasof the decentralized IHS system, a more rationalapproach to needs assessment and services plan-ning could result in more cost-effective decision-making about appropriate types and volumes ofhealth services.
IHS staffing, which represents the major costcomponent of hospital and clinic services, hasbeen described. It maybe concluded that in keep-ing with the uneven availability of IHS facilitiesand services, IHS staffing distributions by areaand service unit also could be more closely ad-justed to eligible or user population size and ac-tual utilization trends. This might require new
placement policies and the relocation of PHSCommissioned Corps and NHSC staff to areas ofgreatest need. Future sources of IHS medical staff-ing will have to be rethought in general, however,because the NHSC program is being discontinuedand the Commissioned Corps is not an activelyexpanding resource.
Shortages of particular types of clinical staffmay limit the range of services provided in a givenservice unit and, consequently, affect the extentto which the service unit must rely on contracthealth services. This problem will be aggravatedin the future unless medical officers can be re-cruited from other sources to fill positions vacatedby NHSC assignees. The Indian health manpowerscholarship program, although small, is one pos-sible solution to this staffing problem. It wouldbe costly to recruit IHS physicians from the pri-vate sector by offering competitive salaries, butso would be an increasing dependence on contractservices purchased from the private sector to sup-plement diminishing IHS direct care capabilities.
THE IHS CONTRACT CARE PROGRAM
The purpose of the IHS contract health serv-ices or contract care program is to supplement theservices provided by IHS direct care hospitals andclinics. Since 1981, the contract care program hasrepresented about 20 percent of total annual IHSallocations and 25 percent of the IHS clinical serv-ices budget. This program provides for the pur-chase of medical services for IHS beneficiariesfrom non-IHS providers. The purchase of outsideservices is essential to the overall IHS health caredelivery system because many IHS hospitals andclinics do not have the staff and equipment nec-essary to offer a full range of services, particu-larly specialty services, and because not all eligi-ble Indians live within a reasonable travel distanceof IHS facilities.
Contract services have long been part of the In-dian health system. Authority for BIA to enterinto health services contracts for Indians wasestablished by the Johnson O’Malley Act of 1934and transferred with IHS to the Department ofHealth, Education, and Welfare (now DHHS) in
1955. The present IHS contract care program pur-chases hospital medical-surgical services and am-bulatory care, including outpatient physician care,laboratory, X-ray, pharmacy, limited dental care,and patient and escort travel. The services are de-livered under approximately 1,300 ongoing con-tracts, mostly with private physicians, and by spe-cial purchase orders for other authorized services.Contract care programs in some IHS service unitsare operated by the tribes under 638 self-deter-mination contracts. The types and amounts ofcontract services purchased vary from one areaand service unit to another depending on medi-cal need and the capabilities of local IHS andtribally operated facilities.
Eligibility and Funding forContract Care
Contract care funding is appropriated annuallyas a separate category within the IHS clinical serv-ices budget. The contract care allocation grew

176 ● Indian Health Care
from over $109 million in fiscal year 1980 to $158million for 1984. Approximately $164 million wasallocated to purchase contract health services infiscal year 1985. Figure 5-1 (in “The IHS DirectCare Program” section, above) illustrates trendsin the total IHS budget since 1972; growth in con-tract care funding since 1981 is shown in figure5-2 (for detailed budget data over the years, re-fer to app. C).
Eligibility requirements for contract care aremore restrictive than those applied to IHS directcare. It is possible for a patient being treated inan IHS hospital, and requiring services that hos-pital cannot provide, to be denied referral for theservices because of ineligibility for the contractcare program (although how frequently this sit-uation occurs cannot be documented). In orderto qualify for contract care, an individual mustbe eligible for direct care. IHS direct care maybeprovided “to persons of Indian descent belong-ing to the Indian community served by the localfacilities and program” (42 CFR 36.12 (a)), whichmay be determined by tribal membership, resi-dence on tax-exempt land, participation in tribalaffairs, or other factors consistent with BIA pol-icies. An individual must meet an additionalresidency requirement to qualify for contract care:that is, he or she must (168):
reside on a reservation located within a con-tract health service delivery area (CHSDA)as designated by IHS; orreside within a CHSDA, and either “be amember of the tribe or tribes located on thatreservation or of the tribe or tribes for whichthe reservation was established, or maintainclose economic and social ties with that tribeor tribes”; orbe an eligible student, transient, or Indianfoster child.
A CHSDA is defined as “a county which in-cludes all or part of a reservation, and any countyor counties which have a common boundary withthe reservation” (42 CFR 36.22 (a) (6)). This “onor near” a reservation residency requirement wasformally applied to the contract care program by1978 regulations in response to the 1976 lawsuit,Lewis v. Weinberger, which required a definitionof the term.
Congress has legislated and IHS has developedregulatory exceptions to the general rule thatCHSDAs consist of counties containing and/oradjoining a reservation. The entire States ofAlaska, Nevada, and Oklahoma are specially des-ignated CHSDAs, as are groups of counties in theStates of Michigan, Wisconsin, and Minnesota (42CFR 36.22 (a)). Arizona was provisionally des-ignated a CHSDA, for 1982 through 1984, but itdid not operate as one because the Arizona tribeswould not agree to expanded eligibility for con-tract services without additional funding, and nosuch appropriation was made (60). The IndianHealth Care Amendments of 1985 (H.R. 1426 andS. 277, not enacted by the end of 1985) proposedan extension of the Arizona CHSDA designationwith authorization for additional funding.
In California, all IHS services are triballyadministered and all services that cannot be pro-vided by the outpatient clinics themselves (e.g.,specialty care, hospitalization, laboratory, radi-ology, and optometry services) must be providedthrough contract care. Eligibility requirements forcontract care in California have been under dis-pute since contract health service regulations firstwere published. According to the executive direc-tor of the California Rural Indian Health Board,one of the organizations established in 1970 to re-turn IHS resources and services to California (44):
. . . (Sixteen) local health projects service unitswere created throughout rural California asCRIHB (California Rural Indian Health Board)subcontractors. By and large, these service unitsencompassed more than one county and wereconstituted without reference to the number orlocation of Indian tribes in those service units.In practice, with the acknowledgment of the IHS,it was these multi-county service units that havebeen viewed as “CHSDA’s” for provisions ofcontract health services to eligible residents ofthe service units for fifteen years.
According to IHS (60):
After the issuance of CHS (Contract HealthServices) regulations, services were continued inCalifornia (and in a number of other places) toeligible Indians who did not meet the new CHSregulations. Such services were continued on thebasis of direction contained in congressional ap-propriation action rather than the CHS regu-lations.

Ch. 5— The Indian Health Service . 177
A provision of the vetoed 1984 reauthorizationof the Indian Health Care Improvement Act andof the 1985 amendments would have resolved theeligibility issue in California by designating theentire State, excluding nine heavily urbanizedcounties, as a CHSDA. Pending enactment of theamendments or possible revision of the eligibil-ity regulations, the California projects are con-tinuing to serve their usual populations (32).
The 1976 American Indian Policy Review Com-mission recommended that all IHS services, in-cluding direct and contract, be made available onthe basis of tribal membership rather than resi-dence (128). More recently, the 1983 ContractHealth Services Task Force supported combinedeligibility for IHS direct and contract services,with eligible persons being of Indian blood, be-ing members of federally recognized tribes, liv-ing in clearly defined IHS service areas (e. g.,CHSDAs), and being formally enrolled for serv-ices. The task force considered defining eligibil-ity based on Indian blood quantum, but rejectedthat approach primarily because of the lack ofreliable data to document blood quantum (181).
Funding and Utilization of ContractCare by IHS Area
The amount of contract care funding, contractcare in relation to direct care dollars, and the typesand amounts of services purchased under contractcare all vary among IHS areas, Although infor-mation to document the extent of these variationsis not as detailed as might be wished, availabledata are presented here. Note that incomplete andsometimes inconsistent reporting from contractcare programs administered by tribes under self-determination (638) contracts affects these datatables.
Table 5-11 shows provisional budget obliga-tions, or commitments, by general category ofcontract care expenditure for fiscal years 1983 and1984, with estimated obligations for 1985 and1986. Obligations for hospital services representabout half of total contract care expenditures. Thecontract care medical priority system (describedlater) tends to authorize acute inpatient servicesrather than less urgent outpatient care, and there
have been substantial increases in the average costper hospital day since 1983. Recent reductions incontract care hospital average daily patient load—from about 312 inpatients per day in fiscal year1983 to an estimated 282 inpatients per day in1985 and 273 inpatients per day in 1986—are theresult of increased per diem costs and slowinggrowth in contract care program funding, Declin-ing numbers of contract care ambulatory visits,patient and escort trips, and dental services alsoare projected as unit costs increase more rapidlythan overall budget allocations (162,163).
Table 5-12 and figure 5-9 present 10 leadingcauses of hospitalization for patients in IHS hos-pitals and in contract general hospitals, fiscal year1984 (the four hospitals operated by tribes underself-determination contracts are not included). Al-though the differences are not striking, admissionsto contract care hospitals showed higher propor-tions of injuries, poisonings, and diseases of thedigestive and circulatory systems. IHS direct carehospitals provided relatively more care for com-plications of pregnancy and childbirth (the lead-ing cause of all admissions) and mental disorders.
Table 5-13 shows a breakdown of fiscal year1984 contract care obligations by IHS area, withcontract care as a percent of total clinical serv-ices funding, service population estimates, and percapita contract care funding. Although contractcare represents about 25 percent of the IHS clini-cal services budget, there are wide variations inthe extent to which the areas rely on contract care,ranging from only 19 percent of the clinical serv-ices budget in Alaska to a high of nearly 50 per-cent in the Portland area.
In the Nashville area, where about one-thirdof the inpatient days and two-thirds of the am-bulatory visits are delivered by tribal 638 pro-grams, 25 percent of the clinical services budgetis obligated to contract care. In California, how-ever, where all IHS services (mainly ambulatorycare) are provided under self-determination con-tracts, only 3 percent of the clinical care budget($525,000) is obligated specifically to the contractcare program. The California figures are not com-parable to those for other areas because of the wayin which contract care funds have been accountedto direct or contract care budget categories. Most

178 ● Indian Health Care
Table 5.11 .—Estimated IHS Contract Care Obligations by Type of Expenditure,With Utilization and Unit Costs, Fiscal Years 1983-86a
Fiscal year 1983 Fiscal year 1984 Fiscal year 1985 Fiscal year 1986Type of expenditure (provisional) (provisional) (estimate) (estimate)
HospitalizationCost per day. . . . . . . . . . . . . . . . . . . $ 644 $ 719 $ 792 $ 872Average daily patient load 312 299 282 273Dollars . . . . . . . . . . . . . . . . . . . . . . . . $ 73,544,000 $ 78,703,000 $81,708,000 $86,773,000
Ambulatory careCost per visit . . . . . . . . . . . . . . . . . . $ 109 $ 116 $ 124Visits . . . . . . . . . . . . . . . . . . . . . . . . . 273,082 266,000 265,000Dollars . . . . . . . . . . . . . . . . . . . . . . . . $29,988,000 $29,766,000 $30,902,000 $32,818,000
Patient and escort travelCost per one-way trip . . . . . . . . . . . $ 136 $ 164 $ 197Number of trips . . . . . . . . . . . . . . . . 38,044 33,000 29,000Dollars . . . . . . . . . . . . . . . . . . . . . . . . $ 3,937,000 $ 5,174,000 $ 5,372,000 $ 5,705,000
Dental servicesCost per patient. . . . . . . . . . . . . . . . $ 186 $ 207 $ 220Number of patients . . . . . . . . . . . . . 39,420 38,000 37,000Dollars . . . . . . . . . . . . . . . . . . . . . . . . $ 6,597,000 $ 7,338,000 $ 7,656,000 $ 8,130,000
OtherDollars . . . . . . . . . . . . . . . . . . . . . . . . $30,840,000 $36,929,000 $38,318,000 $32,440,000
Total IHS contractcare obligations . . . . . . . . . . . . . . $144,906,000 $157,910,000 $163,956,000 $165,866,000
(provisional) (provisional) (estimate) (estimate)aTh~~~ IHs ~OntraCt ~-re ~bll~~ti~”~ a~~ ~~~~~”t~d to ~h~w the relative importance and costs of the five major contract care expenditure categories. Contract care
programs managed by the tribes as self-determination (638) programs are not included. Because the figures are taken from briefing books prepared by IHS for itsannual appropriations hearings, fiscal years 1985 and 1966 are proposed rather than actual appropriations, and figures for fiscal years 1983 and 1964 are provisional,
SOURCE: U S. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Indian Health Service, “AppropriationsBriefing Books,” fiscal years 1985 and 1966
Table 5-12.—Ten Leading Causes of Hospitalization for General Medical and Surgical Patients,IHS and Contract General Hospitals, Fiscal Year 1984a
Number of discharges Percent distributionDiagnostic category Combined IHS Contract Combined IHS Contract —
All categories . . . . . . . . . . . . . . . . . . . . . . . . . . . . 99,816 77,561 22,255 100.0 100.0 100.0Complications of pregnancy, childbirth,
and puerperium. . . . . . . . . . . . . . . . . . . . . . . . . 23,248 18,642 4,606 23.3 24.0 20.7Injuries and poisonings . . . . . . . . . . . . . . . . . . . 12,432 9,070 3,362 12.4 11.7 15.1Respiratory system diseases. . . . . . . . . . . . . . . 9,413 7,181 2,232 9.4 9.3 10.0Digestive system diseases. . . . . . . . . . . . . . . . . 9,243 6,769 2,474 9.3 8.7 11.1Genitourinary system diseases . . . . . . . . . . . . . 5,397 4,091 1,306 5.4 5.3 5.9Supplementary conditions . . . . . . . . . . . . . . . . . 5,253 5,045 208 5.3 6.5 0.9Circulatory system diseases . . . . . . . . . . . . . . . 5,172 3,537 1,635 5.2 4.6 7.3Mental disorders . . . . . . . . . . . . . . . . . . . . . . . . . 4,720 3,873 847 4.7 5.0 3.8Symptoms and ill-defined conditions. . . . . . . . 4,699 3,738 961 4.7 4.8 4.3Nervous system and sense organs . . . . . . . . . 4,108 3,108 1,000 4.1 4.0 4.5All other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16,131 12,507 3,624 16.2 16.1 16.3 —aHOspitalizatiOns in tribal self-determination (638) hospitals are not included in this table
SOURCE: US. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Indian Health Service, /HS Ctrarl SeriesBook, April 1965. Data published as table 5,7, from IHS Annual Reports 2C and 31.

Ch. 5—The Indian Health Service ● 179
Figure 5.9.—Ten Leading Causes of Hospitalizationin IHS and Contract General Hospitals,
Fiscal Year 1984a
Diseases of genitourinary system hospitals~ I. . .—
Supplementary conditionsContract
Diseases of circulatory system general JMental disorders hospitals
Symptoms and ill-defined conditionsDiseases of nervous system
and sense organs - 1 1 I 10 5 10 15 20Percent of total discharges
aH~~Pltall~atl~n~ ,” tribal 638 hospi ta ls are not included In these fig UrtlS
SOURCE U S Department of Health and Human Services, Public Health Serv.ice, Health Resources and Serwces Administration, Indian Health Serv.ice, Chart Series Book, Rockvllle, MD, April 1985.
self-determination funding is accounted in directcare budgets, although it may be used to purchasesome services under contract. The $525,000 inCalifornia represents the contract care programsof only two tribes and does not include contractcare that may have been purchased by other 638projects (43,58).
Other IHS areas besides Portland in which theproportion of contract care funding is high areBillings, Aberdeen, and Tucson (note that all threeof these areas have higher per capita contract careobligations than the Portland area, and Billingshas a contract care budget equivalent to Portland’sto service a population half the size). IHS areasthat have relatively comprehensive direct care ca-pabilities, such as Alaska, Phoenix, Navajo, andOklahoma, have lower proportions of contractcare funding in their total clinical services budgets.Per capita contract funding among the areasranges from $86 in Oklahoma to $473 in Billings,with an average per capita obligation of $182 (ex-cluding California).
Table 5-14 presents fiscal year 1984 utilizationdata on inpatient care delivered by IHS direct carehospitals, IHS contract care hospitals, triballyoperated (638) hospitals, and tribally operatedcontract care programs. Numbers of admissions,inpatient days, and average lengths of stay maybe compared among the areas in these deliverysettings. Average lengths of stay by type of hos-pital varied little around the combined averageof about 5 days per stay. The tribally operatedhospitals had shorter average stays, but that wasin only four hospitals. Combined average lengths
Table 5-13.—IHS Contract Care Program Obligations by Area, Total and Per Capita, Fiscal Year 1984a
Contract care Contract careprogram obligations as percent of IHS estimated Contract care dollars
Area fiscal year 1984 clinical services service population 1984 per capita
Aberdeen . . . . . . . . . . . $20,029,000 33.40/0 70,648 $283.50Alaska . . . . . . . . . . . . . . 19,296,000 18.5 71,329 270.52Albuquerque. . . . . . . . . 10,694,000 24.7 51,211 208.82Bemidji . . . . . . . . . . . . . 8,980,000 28.9 47,000 191.06Billings . . . . . . . . . . . . . 18,976,000 44.6 40,106 473.15California . . . . . . . . . . . 525,000 2.5 71,642 7.33Nashville . . . . . . . . . . . . 6,712,000 25.6 35,822 187.37Navajo . . . . . . . . . . . . . . 19,074,000 21.1 162,005 117.74Oklahoma . . . . . . . . . . . 16,478,000 20.5 190,451 86.52Phoenix . . . . . . . . . . . . . 14,284,000 20.2 82,309 173.54Portland . . . . . . . . . . . . 18,549,000 48.6 96,427 192.36Tucson . . . . . . . . . . . . . 4,330,000 33.9 17,852 242.55
All areas . . . . . . . . . . $157,927,000 24.5% 936,802 $168.58All areas excluding
California . . . . . . . . . $157,402,000 24.40/o 865,160 $181.93aAll IHs SeWiCeS in California are deliVer@ “la tribal Self.detemllnation (638) contracts, MOSt 638 funding is accounted i n direct Care budgets, although it fllay be usedto purchase some services under contract. This may explaln the small contract care budget in California, which represents specific contract care obligations for onlytwo projects. The Bemidji and Nashville areas also have substantial tribal 638 health delivery programs. Figures for Alaska are somewhat low due to delayed data reporting.
SOURCE US Department of Health and Human Services, Public Health Serwce, Health Resources and Services Administration, Indian Health Service, Office of Ad-ministration and Management, Resources Management Branch, 1985

180 ● Indian Health Care
-i C9w
Igllllgl:lll
. . . . . .
I. . . . . . . .. . . . . . . . . . . .. . . . .. . . . . . . .. . . . . . . . .
a).. . . . . . . ..3..... . . . .

. — —
Ch. 5—The Indian Health Service . 181
of stay by area ranged from a low of 3.9 days inBemidji (on a low volume of admissions) to a highof 6.3 days in Alaska. In the Billings area, morethan half of the inpatient admissions were to non-IHS contract general hospitals. In the Nashvillearea, more patients were admitted to communityhospitals under tribally operated contract careprograms than to the one tribal hospital, the IHSdirect care hospital, or to community hospitalsby IHS-operated contract care programs. Wellover half of the inpatient admissions in the Aber-deen, Alaska, Albuquerque, Navajo, Oklahoma,Phoenix, and Tucson areas were to IHS direct carehospitals. Because there are no IHS or triballyoperated hospitals in the Portland or Californiaareas, in Portland all inpatient care was providedthrough the contract care program; and in Cali-fornia, the few admissions that were reportedwere authorized by tribally operated contract careprograms.
Additional information on fiscal year 1984 ex-penditures for inpatient care and outpatient visitsin the 12 IHS area contract care programs is pre-sented in table 5-15. Total combined 1984 in-patient and outpatient expenditures in table 5-15,approximately $94 million, represent only part ofthe overall 1984 contract care budget allocationof $158 million (table 5-13). Excluded from table5-15 are disbursements for patient and escort
travel (about $5 million), dental services ($7 mil-lion), and other types of contracts ($37 million).Incomplete cost data reporting may account forthe remainder of the difference. Note also thatdata in table 5-15 cannot be compared directlywith those in table 5-14 because they come fromdifferent IHS source reports. The average costs(disbursements) per “full-pay equivalent” inpatientday and outpatient visit in table 5-15 are artifi-cial figures that combine proportions of days andvisits paid in full by IHS with those partially paidby IHS and partially paid by other sources. Thesefigures are used by the IHS contract care programfor budget planning purposes only. A compari-son of actual inpatient days by area in table 5-14with full-pay equivalent days in table 5-15 sug-gests that 638 contract care programs may havebeen included in Alaska but excluded from Be-midji and Nashville data. Most other inpatientday figures are reasonably close, except in thePortland area. Data reporting appears to be in-complete for California.
Actual contract care disbursements per full-payequivalent inpatient day varied substantiallyamong IHS areas. The lowest cost, $535 per in-patient day in the Bemidji area, was only 60 per-cent of the $902 average cost per day paid inAlaska. Albuquerque, Nashville, and Tucson alsohad high costs per contract care inpatient day. A
Table 5-15 .—IHS Contract Care Program, Utilization and Costs for Inpatient and Outpatient Care,by Area, Fiscal Year 1984
Inpatient care - Outpatient careTotal - Cost per full- Full-pay Total Cost per full- Full-pay —
Area disbursements pay day equivalent days disbursements pay visit equivalent visitsAberdeen ., . . . . $13,325,540 - $598 22,284 $ 2,935,501 $124 23,673Alaska . . . . . . . . . . 6,295,317 902 6,979 2,552,971 145 17,607Albuquerque ., . . . . . 4,943,063 843 5,864 1,833,540 173 10,598Bemidji . . . 1,576,977 535 2,948 1,187,296 103 11,527Billings . . . . . . . . . 13,232,389 698 18,958 3,044,936 91 33,461California. . . . . . . . . NA NA NA NA NA NANashville . . . . . . . . . . 918,836 813 1,130 202,604 137 1,479Navajo ., ... 5,572,359 799 6,974 3,022,670 57 53,029Oklahoma . . . . . . . . . . . . 7,333,354 780 9,402 2,128,747 134 15,886Phoenix . . . . . . . . 6,948,429 802 8,664 1,985,347 154 12,892Portland . . . . . . . . . . . 7,876,537 717 10,985 4,844,191 143 33,875Tucson . . . . . . . . . . . . . 1,583,336 867 1,826 203,320 142 1,432
IHS total . . . . . . . . . $69,606,628 $722 96,014 $23,953,263 $111 215,459aTOtal disbursements are comb! ned full pay by IHS contract care Program, Partial PaY, and unknown PaY “Full. pay equivalent” days and vIs Its are artificial figures
developed for comparability with the total disbursement figures Outpatient vlslt expenditures Include physlclan, X.ray, laboratory, emergency room, drugs, prostheses,and other expenses, but no patient and escort travel Data from tn bal (638) cent ract care programs are not Included { n this table, which accounts for the lack of ! nforma-tlon from California
SOURCE U S Department of Health and Human Services, Public Health Service, Health Resources and Services Admln!strat!on Indian Health Service Program Stat Is.tics Branch, October 1985

182 ● Indian Health Care
number of factors may contribute to such differ-ences, including the charges prevailing amonglocal private sector providers, a service unit’s abil-ity to negotiate reasonable charges, and the rela-tive severity of the cases for which contract carewas authorized. Average costs for full-pay equiva-lent contract care outpatient visits also were vari-able. They appear to be high in table 5-15 becauseall expenditures associated with the outpatientvisits, such as physician fees, X-ray, laboratory,emergency room, drugs, and prostheses were in-cluded.
Service-specific contract care program cost dataare available from a so-called “piggyback” datasystem that has been added onto the Health Re-sources and Services Administration (HRSA)accounting system. By grouping contract care ex-penditures by cost center code, the system cangenerate utilization and cost data by service andIHS area. The piggyback data system is the sourceof table 5-16, which shows a breakdown of fiscalyear 1984 area contract care disbursements, com-bining full and partial pay, by percent of total areafunds devoted to each cost center. The five maincost centers are: patient and escort travel; dentalcare; inpatient care; outpatient visits; and an“other” category that includes payments for nurs-ing home care, the Pascua-Yaqui prepaid plan inthe Tucson area, and use of other medical special-ists. The category “contracts to support directservices” includes ongoing contracts for medicalprofessionals and services delivered in IHS facil-ities (in some areas, a good deal of dental careis provided under such contracts). The final cat-egory includes incomplete data on contract careexpenditures by tribes under self-determinationcontracts (58).
The amount of contract care reported to beadministered by tribes varies widely among theareas and distorts the proportions of total dis-bursements that are attributed to each of the ma-jor cost centers. This is because available datawere not adequate to distribute 638 expendituresamong those cost centers. In the Nashville area,87 percent of total contract care disbursementswere administered by the tribes, and in Califor-nia, the figure was 82 percent; but the averagethroughout IHS was only 19 percent of contractcare funds. The Billings and Phoenix areas indi-
cated that no contract care funds were disbursedby 638 programs. The Navajo area reported thatit managed 22 percent of its contract care alloca-tion via 638 contract, but IHS headquarters statedthat the Navajo have only one 638 contract forabout $200,000 and it is not for contract care(216). Because of data questions such as these, lit-tle can be concluded from table 5-16 except forIHS as a whole, where inpatient services repre-sent more than half of all contract care expendi-tures. The Aberdeen, Alaska, and Albuquerqueareas are roughly comparable to overall IHSproportions in the five main cost centers; Phoe-nix and Oklahoma are close; but the other areasare difficult to interpret.
Operation of the Contract CareProgram
The contract care program may purchase med-ical services when no IHS direct care facility isavailable, when the direct care facility is not ca-pable of delivering the emergency or specialty carerequired, when the workload of the direct carefacility exceeds its capacity, or when IHS fund-ing is necessary to supplement alternate resources(e.g., Medicare) to ensure care for eligible Indians.Contract care may be delivered to individuals whoare physically present in an IHS facility but, mostfrequently, the services are provided in non-IHSpublic or private facilities (168).
Since 1972, rates of increase in the IHS contractcare budget have been less than those experiencedin general health care costs (119), while the IHSservice population has nearly doubled from 507,804in 1972 to an estimated 961,582 in 1985. As a re-sult, it has become increasingly difficult to meetthe growing demand for contract care withinavailable funding limits: it is not uncommon fora service unit to expend its entire contract careallocation well before the end of the fiscal year.
The IHS contract care program has appliedvarious means in attempting to manage its limitedannual resources. In addition to the required resi-dence in a CHSDA, contract care authorizationsare governed by a medical needs priority systemthat in some areas restricts care to emergency andlife-threatening conditions (priority one) and de-nies referral for less urgent services due to lack

Table 5-16.—IHS Contract Care Program, Major Cost Centers as Percent of Total
IHSCost centers total Aberdeen Alaska Alberdeen Bemidji Billings California
Disbursements,a by Area, Fiscal Year 1984—
N a s h v i l l e N a v a j o O k l a h o m a P h o e n i x P o r t l a n d T u c s o n—.1, Patient and escort travel . . . . . . . . 3.1 %
—
3.1 % 3 . 4 % 1 . 8 % 0.6% 2.5% — 9.80/0 1.1 “/0 4.80/0 1 .50/02. Dental care . . . . . . . . . . . . . . . . . . . .
— 0 . 7 %
4.1 1.8 4.2 6.0 4.1 2.2 0.3 0.2 ”/0 2.4 8.4 2.0 9.3 2.03. Inpatient care . . . . . . . . . . . . . . . . . 46.8 66.2 37.2 53.1 20.5 73.4 9.8 31.8 51.3 58.74. Outpatient care . . . . . . . . . . . . . . . . 16.1
— 42.5 37.614.3 15.1 19.4 15.5 16.9 2.4 2.2 17.3 14.9 16.6 26.3 4.4
5. Other contract care . . . . . . . . . . . . . 4.7 4.0 3.9 2.2 0.7 1.0 15.6 5.3 0.1 13.4 1.26. Contracts to support
— 52.5
direct services . . . . . . . 5.8 4.9 4.0 14.7 0.6 4.0 0.6 11.6 9.9 4.57.638 contract care (incomplete) . . . 19.4
— 3.8 0.25.7 32.2 2.8 58.0 – 81.7 87.2 21.8 14.3 — 15.4 2,6
IHS total contract care . . . . . . . . . . 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 1 OO.OO/O 100.0”/0 100.0 ”/0 100.0 ”/0 100.0 ”/0af3a~ed on total contract care program disbursements: full pay, partial pay, and unknown pay. There are substantial variations i n how areas may rePOfl contract PaYments by cost center, especially Ime 6,contracts to support direct serwces, and line 7, tribal 638 contract care Note also that data reported for 638 contract care are Incomplete
SOURCE” U.S Department of Health and Human Services, Public Health Service, Health Resources and Services Administration, Indian Health Serwce, Program Statistics Branch, September 1985

784 ● Indian Health Care
of funds. By regulation, the IHS contract care pro-gram may only pay charges that are not coveredby Medicare, Medicaid, or any other third-partypayers (42 CFR 36.23 (f)). Because there is no dol-lar cap on the amount that maybe authorized foran individual contract care referral, and becausethere are no absolute constraints on the types ofservices that may be authorized, available fund-ing is the major limiting factor.
The contract care headquarters office is respon-sible for overall program management. It estab-lishes general administrative policies and stand-ards of performance, develops long-term programplans and objectives, provides staff assistance toarea offices, and administers funds to the areasto meet expenditures through the IHS financialmanagement branch. The program’s managementphilosophy is “to delegate to the greatest degreepossible, within the limits of available funds, au-thority for the operation of the Contract HealthServices Program to the Area Director and theService Unit Director” (168).
The area offices are responsible for administer-ing contract care services in accordance with head-quarters policies and procedures. The area officesallocate funds among the service units and, in co-operation with them, negotiate annual providercontracts. It is the area offices that “establish med-ical priorities for the care of eligible Indian peo-ple that will most effectively meet their needswithin the funds available” (168). Service unit di-rectors and physicians determine on a case-by-casebasis whether a specific request for contract caremay be authorized within the area’s contracthealth services priority guidelines and the limitsof available funding. All requests must be actedupon, with written denials and maintenance ofappeals files as appropriate, Service unit staffprocess patient referrals and payment authoriza-tions, while area office staff provide invoice ver-ification and claims processing services. Day-to-day operations of the contract care program fol-low
1.
the general steps outlined below (168):
Contracting for Services. Contracts are ne-gotiated annually by the service units andarea offices to cover services performed ona routine basis by private hospitals, clinics,laboratories, physicians, and other providers.
2.
3.
When emergency or one-time services are au-thorized from a provider that is not an estab-lished contractor, individual purchase ordersare used.
Authorization for Contract Care. For eachcontract provider utilized by an eligible In-dian, a purchase order must be issued by theservice unit director or a member of the med-ical staff. In emergencies, such authorizationmust be sought within 72 hours of admis-sion; in nonemergency cases, authorizationmust be secured in advance. Service unit staffgenerally set up the approved appointmentsand prepare a formal authorization sheet,with identification of other sources of pay-ment for which the patient may be eligible.
The authorization form includes an esti-mated cost for the service. Because contractcare is a budget-limited program, authorizedestimated costs become obligated and reducethe available contract care funds balance forthe service unit. Accurate estimates are crit-ical, and it is important that actual disburse-ments be compared against the obligatedestimates on a timely basis so that excessobligations may be deobligated to permitexpenditure of those funds for additionalservices.
Contract care authorizations for students,transients, and other eligible persons awayfrom their home service delivery areas arethe responsibility of the home service unit.
Provider Invoices. Upon performance of theservices, the provider completes the author-ization form, indicates the charges, andreturns it to the service unit as an invoice.Actual charges are compared with the esti-mated obligation and adjustments made ac-cordingly, taking into account applicablethird-party resources. Documentation of theprovider’s attempts to obtain other paymentshould be verified locally. (IHS headquar-ters maintain no records of the verificationof alternate resources. At the service unitlevel, each contract care authorization formindicates full pay by IHS or partial pay, andthe amount paid by IHS, but the other pay-ers usually are not identified. ) Approved in-voices are forwarded to the area office for

audit review, entry into the area data sys-tem, and check processing for payment.
IHS area and service unit staff are responsiblefor the day-to-day management of the contractcare program. Because of differences in the avail-ability of IHS facilities, levels of contract carefunding, and the extent to which an area relieson contract care to supplement its direct deliv-ery system, administration of the contract careprogram is not standard among the areas. Sev-eral areas have developed their own explicit pro-gram management policies and guidelines.
The particular services that may be authorizedunder contract health services priority guidelinesvary among the areas. Decisions on what serv-ices will be purchased are made on a case-by-casebasis in each service unit. A service that mightbe approved early in the quarter, when funds wereavailable, might be denied when funds were run-ning out or exhausted. When a service unit’s con-tract care budget is depleted before the end of thefiscal year, it may apply to the area office for assis-tance; but it is not assured of getting any addi-tional funding. When a patient’s life is threatened,emergency contract care must be provided by anearby private hospital that has no guarantee ofbeing paid in a timely manner. Such bad debtscan be a severe financial hardship on small ruralhospitals, and can strain relations between IHSand those hospitals.
Issues Related to the IHS ContractCare Program
The Adequacy of Contract Care Funding andthe Rationing of Care
The scope of services offered by many IHS hos-pitals is relatively limited compared with U.S.community hospitals in general; and because IHScannot economically employ specialized medicalstaff in all service units (assuming such specialistscould be recruited and retained), specialty serv-ices often must be obtained through the contractcare program. The majority of the small IHS hos-pitals do not provide surgery, and they lack so-phisticated diagnostic and therapeutic equipmentas well as the specialized staff to operate it. Thesefactors contribute to a demand for contract healthservices that is likely to increase and to put greater
Ch. 5—The Indian Health Service ● 185
pressures on area contract care budgets, especiallyif those budgets experience little or no growth.The volumes of contract services purchased in re-cent years have shown a level or declining trendbecause general health care cost inflation has in-creased service charges more rapidly than the IHScontract care budget has grown, Under these cir-cumstances, how should IHS balance its direct andcontract care services to achieve maximum cost-effectiveness? It may be more expensive to pur-chase services through contract care than for IHSto provide them directly, where IHS is capableof doing so; but direct care delivery requires cap-ital and staffing investments that cannot be justi-fied in many isolated IHS areas.
When the demand for contract services exceedsavailable funding, IHS contract care programs inthe areas and service units must ration servicesin order to operate within fixed annual budgets.The means by which services are rationed includeapplication of the contract care eligibility require-ments, authorization of services according to themedical priority system (which may differ fromone IHS area to another), and the required firstuse of alternate resources.
Medical urgency determinations are made bya physician or by the service unit director withinthe guidelines of the area’s contract health serv-ices priority system. That system defines some,but not all, of the medical conditions that are con-sidered emergencies and that should receive firstpriority for contract care referral. Urgent non-emergency services and elective procedures maybe provided if sufficient funds are available, butif not, they may be deferred or not provided at all.
Because this medical priority system tends torefer out the more specialized and expensive in-patient cases, the contract care budget graduallyis becoming a high-cost care fund and its origi-nal purpose of supplementing the full range of IHSdirect care services is being lost. (The effects ofespecially high-cost cases on the contract care pro-gram are discussed inch. 6.) When no IHS directcare facilities are available, patients may face longwaits for elective and urgent care that must beobtained under contract. Serious medical condi-tions may be aggravated during the wait, andsome patients may fail to seek and obtain neededservices altogether. Although in recent years some

186 ● Indian Health Care
of the areas have maintained lists of deferred con-tract care needs, whether or not patients receivethe deferred services depends on the state of thearea’s contract care budget at the end of the fis-cal year.
IHS’s methods for allocating and administer-ing contract care resources over the years haveresulted in inevitable inequities among IHS areas,service units, and individual beneficiaries. Boththe 1976 American Indian Policy Review Com-mission and the Grace Commission cited inequi-ties in the range of health services available toeligible Indians, based on residence. The 1976commission concluded that the contract care pro-gram contributed to the maldistribution of re-sources because the extent to which the areas de-pended on contract funding for overall clinicalservices delivery varied so much (128).
Contract care funds purchase services to sup-plement those available from the IHS direct caresystem of hospitals and clinics. In areas with rela-tively comprehensive direct care resources, thisprinciple may work reasonably well even undercurrent funding constraints because direct serv-ice capabilities are there to back up the contractcare program and provide some of the servicesthat cannot be purchased because of a lack of con-tract care funds. A patient with an urgent but notlife-threatening condition (such as the need for gallbladder surgery) might not receive the needed carein an area authorizing only priority one (emer-gency and life-threatening) contract services; butcare might be authorized in another area wherefunding was less restricted. Or, the patient couldtravel to the nearest IHS hospital and receive serv-ices that were denied under contract care, if thehospital did not have an extensive waiting list forthe service. In the Portland and California areas,however, this is not an option because there areno IHS hospitals.
Another aspect of the overall funding problemis a perceived vulnerability of the contract careprogram to budget cuts, relative to the more dif-ficult task, politically, of closing existing IHS fa-cilities and laying off staff to reduce the direct carebudget. Areas dependent on contract care believethat they already receive fewer services than di-rect care areas, and they fear they are at greaterrisk of absorbing service cutbacks due to reduced
contract care funding. Again, Portland is an ex-ample of an IHS area where contract care budgetcuts could have serious effects, because nearly halfof the clinical services funding in that area is forcontract care.
Neither the California nor the Portland IHSarea receives compensatory contract care fund-ing to offset the absence of direct care capabil-ities. It is difficult to dispute the contention oftribes in those areas that they are not receivingtheir fair share of total IHS resources in compar-ison with IHS direct care areas like Navajo, Okla-homa, Albuquerque, and others. The idea thatsome adjustment should be made in contract carerelative to direct care funding, or that a clinicalservices resource allocation formula should be de-veloped to reflect combined direct and contractcare needs, has been proposed but not imple-mented (182). This would be one way to worktoward a more comparable services packageamong IHS areas.
The Use of Alternate Resources
By regulation, the IHS contract care programis designated as the residual payer, or payer oflast resort, for eligible Indians who have accessto other sources of reimbursement or health caredelivery (42 CFR 36.23 (f)). The identification ofthese so-called alternate resources and aggressiveefforts to collect appropriate reimbursements fromthem are vital to the contract care program, inwhich funds are so limited. Chapter 3 of the IHSIndian Health Manual defines alternate resources(third-party payers and providers) as “those re-sources, including IHS facilities, that are avail-able and accessible to an individual. Alternateresources would include but not be limited to,Medicare, Medicaid, vocational rehabilitation,Veterans Administration, crippled children, pri-vate insurance, and State programs” (168).
In the contract care program, the use of alter-nate resources is mandatory: that is, an individ-ual is required to apply for an alternate resourceif there is a reasonable chance that he or she maybe eligible for coverage, and IHS disbursementsare authorized only for charges not covered byother payers. The numbers of IHS beneficiarieseligible for and/or enrolled in Medicare, Medic-aid, and other third-party payers, however, are

not known with accuracy. There is no IHS datasystem that maintains records of eligibility foralternate resources, although the patient registra-tion system that has been implemented since Jan-uary 1984 may help to fill this gap in the future.Each individual who presents himself for treat-ment at an IHS facility (or who seeks a contractcare referral through the facility) now must reg-ister for services and be screened for eligibility forthird-party resources.
Some IHS areas have set up their own manualor automated systems for identifying alternate re-sources. In the Portland area, for example, thecontract care program is monitored closely by thearea office. Since 1983, alternate resource utili-zation targets based on actual collections experi-ence have been established for each service unitand reviewed quarterly. The targets, which reflectdifferences in tribal population characteristics(especially age distributions) and the availabilityof other resources such as State Medicaid pro-grams, range from an expected 30 to 50 percentof contract care charges that should be collectedfrom non-IHS payers (46).
Data from the U.S. Census Bureau’s 1980 sup-plementary survey of American Indians, Eskimos,and Aleuts provide the only national estimates ofother sources of payment for health services.However, those data refer only to Indians resid-ing on reservations and in historic areas of Okla-homa (336,000 out of a 1980 total self-identifiedIndian population of 1.4 million and an IHS esti-mated eligible service population of 829,000) andcannot be generalized with confidence to other In-dian populations. Data from the census surveysuggested that about 85 percent of the reservation-based Indians had received some type of healthservice during 1979, Eighty percent of those serv-ice users reported that their usual place of treat-ment was an IHS facility; for 11 percent, the de-livery site was a private physician’s or dentist’soffice; and for 5 percent, it was a tribal clinic orhospital. Eighty-four percent of service users re-ported that their recent services had been paid forby IHS (including IHS contract care and tribal 638health programs), nearly 5 percent of the serviceswere paid by private insurance, 5 percent by therecipient or recipient’s family, and 3 percent byMedicare or Medicaid (147).
Ch. 5—The Indian Health Service ● 187
It is surprising that only 3 percent of the Indianservice users reported their care had been paid forby Medicare or Medicaid, especially in view ofother census data showing that of Indians 15 yearsof age and older, 7.3 percent reported receivingbenefits from Medicare or Medicaid, an additional12 percent reported social security benefits, and6.6 percent received BIA general assistance. It ispossible that when an IHS facility is the first pointof contact, it is assumed that IHS pays for thecare, although this may not be the case if IHS cancollect reimbursement from Medicare, Medicaid,and other payers (147).
IHS pursues two approaches in its efforts tomake full use of alternate resources. First, serv-ices may be provided in IHS facilities to Indianswho are eligible both for IHS care and for Medi-care, Medicaid, private insurance, or other cov-erage. In such cases, IHS seeks reimbursementsfrom those other sources before absorbing thecosts in its direct care budget, In a second situa-tion that affects the contract care program, anIHS-eligible Indian also having other sources ofpayment may be referred for care to a non-IHSprovider. IHS then must verify that all otherapplicable sources have paid their shares beforethe IHS contract care program can pay the re-mainder of the bills. If the individual has no othersource of payment, IHS is responsible for the fullcharges.
IHS officials report that collections from Medi-care for services provided in IHS facilities to In-dians who also are Medicare beneficiaries proceedrelatively smoothly. IHS has been reimbursed un-der the Medicare prospective payment diagnosis-related group (DRG) system since October 1983.Likewise, Medicare payments associated with con-tract care referrals are not a problem as long asthe private provider is aware of the patient’s Medi-care eligibility and bills Medicare on behalf of thatpatient. IHS direct and contract care programshave found it more difficult to collect from StateMedicaid programs, however, primarily becauseof problems in ensuring that all Medicaid-eligibleIndians are enrolled. IHS must deal with differ-ent and changing Medicaid eligibility and coveragerequirements in each State, and State Medicaidprograms, which are under budgetary pressuresof their own, have little incentive to encourageIndian enrollment (70).

188 ● Indian Health Care
Non-IHS private hospitals and physicians thattreat IHS contract care patients should bill pri-vate third-party insurers, in addition to Medicareand Medicaid, before submitting bills for any re-mainder to IHS. Service unit contract care staffare responsible for verifying that all other appro-priate payments have been made before author-izing contract care disbursements. IHS collectionsfrom private payers for services delivered in IHSfacilities pose other problems: because individualIndians are not billed and are not legally liablefor the costs of their medical care, their privateinsurers likewise cannot be held liable. Thus IHSusually is not able to collect reimbursements forsuch care from an Indian’s private insurance com-pany. In spite of these difficulties, IHS has beendirected to continue to pursue all possible third-party reimbursements (60).
The fiscal year 1985 IHS appropriations brief-ing book cited unidentified preliminary data in-dicating that “less than 2 percent of the Indianpopulation have private insurance” (162). Evenin view of high unemployment among Indians andother factors, this figure seems quite low. OneFederal official familiar with the program esti-mates that at least 5 to 10 percent of Indians haveprivate insurance, because Indian employees ofthe Federal Government alone would account formore than 2 percent (83). IHS states that a studyis underway to generate better data on thisquestion.
Reimbursements from Medicare, Medicaid, andprivate payers are used primarily to upgrade hos-pital and clinic facilities or equipment and to hiretemporary staff. The amounts of reimbursementscollected vary among IHS areas. Those that aremost dependent on contract care may of neces-sity be more active in third-party collections thanIHS areas where pressures on contract care fundsare not so great. Some areas express fears thatthird-party collections will be used to offset theirregular budget allocations. Furthermore, aggres-sive third-party collections are discouraged if thefunds are not available to the service unit wherethey were collected. Title IV of the Indian HealthCare Improvement Act provided that third-partycollections would be held in a special DHHS levelfund for redistribution as needed to upgrade fa-cilities and services, but some areas and service
units complained that they received less than theyhad collected. The 1985 amendments proposedthat each service unit be able to use at least 50percent of the amount it collected, but that legis-lation had not been enacted by the end of 1985.At the least, clarification of whether third-partycollections will be treated as offset or supplemen-tal funds for budget allocation purposes could en-courage greater collection efforts.
In order to utilize alternate resources most ef-fectively, the IHS contract care program must beable to respond to changes in the general healthcare delivery environment that will affect its ben-eficiaries. Changes in State Medicaid programscan have significant effects on IHS contract careprograms. In the State of Washington, for exam-ple, a health program for the medically indigentthat served a large number of Indians was discon-tinued for about 6 months in 1985. The Portlandarea IHS office estimated that if the program werenot reinstated (it was reinstated in October 1985,but its future still was uncertain), additional coststo the IHS contract care program would total atleast $2 million per year (107). Indians in the Stateof California have relied on the relatively gener-ous MediCal system for a large volume of serv-ices, especially hospital services, that CaliforniaIHS contract care programs often cannot afford.Recent implementation of a Medicaid program inthe State of Arizona, the Arizona Health CareCost Containment System, has brought about amajor realignment of IHS, county, and State healthprograms available to Indians.
IHS contract care programs must keep currentof changes in State Medicaid programs in orderto encourage all eligible Indians to enroll andmaintain eligibility in those programs. In Min-nesota, the Medicaid program recently requiredthat all Medicaid beneficiaries be treated in State-qualified health maintenance organizations. Howthis new requirement will affect services deliveryto Medicaid-enrolled Minnesota Indians is not yetknown. The Minneapolis urban Indian healthproject, for example, which serves both Indiansand non-Indians who are covered by Medicaid,is not a health maintenance organization, but inorder to continue serving its Medicaid-eligibleclients, it joined a network of qualified healthmaintenance organizations.

The question of whether IHS and tribally oper-ated facilities should treat and bill non-Indiansraises other issues involving appropriate relationsbetween IHS and the alternate resources, Indianhealth facilities serve non-Indians in Alaska,where IHS facilities are the only health servicesavailable in some areas. Some tribal 638 healthprograms in California serve non-Indians, as dosome urban Indian projects. The practice is notprohibited by IHS, as long as there are assurancesthat Federal funds destined for Indians are notspent to care for non-Indians. In some IHS facil-ities, Indian users do not want their facility to treatnon-Indians.
Management Efficiency in theContract Care Program
The use of contract care and private resourcesrepresents a growing portion of IHS clinical serv-ices delivery, and, as a number of recent studieshave pointed out, there are questions as to whetherIHS management techniques have kept pace withprogram growth. Under current budget constraints,it is of critical concern that IHS’s purchase of con-tract services be as cost-effective as possible.Questions have been raised about program man-agement policies that allow the payment of IHScontract care funds to private providers on termsthat are not always advantageous to IHS and thatultimately may reduce the volume of contractservices purchased.
Management of the IHS contract care programhas been reviewed by the American Indian Pol-icy Review Commission’s task force on Indianhealth, 1976 (128); a General Accounting Office(GAO) study of contract care claims processing,1982 (132a); the Grace Commission’s private sec-tor survey on cost control, 1982 (119); the IHSDirector’s Contract Health Services Task Force,1983 (181); and a Macro Systems study of fiscalintermediary costs, 1984 (69).
Among potential problems in the IHS contractcare program identified by these studies were thefollowing: 1) IHS pays 100 percent of chargesbilled instead of the 80 percent of customary feesusually covered by private insurers; 2) the con-tract care program does not reimburse its vendorsat Medicare DRG rates, although it receives its
Ch, 5—The Indian Health Service ● 189. .
reimbursements from Medicare based on DRGs;3) in some areas there is a lack of aggressive com-petitive bidding for IHS contracts and of force-ful negotiations for reduced charges; 4) IHS proc-esses its own contract care claims instead of usinga fiscal intermediary or billing agency at poten-tially lower cost; and 5) procurement policies andcost accountability in IHS area offices and serv-ice units, where the contract care program isadministered, could be improved with more ex-perienced staff and computer capabilities.
There seems to be agreement that IHS shouldnegotiate more aggressively, where it can, to ob-tain better prices for the services it purchases. In-stead of paying 100 percent of billed charges, thecontract care program could bargain for reducedfees and encourage competition among contractproviders wherever possible. In some geographicareas, IHS does not represent a sufficient shareof the health services market to negotiate effec-tively for reduced rates; elsewhere, the lack ofalternate providers may eliminate the effects ofcompetition; but these limitations do not existeverywhere.
The GAO study recommended that IHS con-tract providers be reimbursed at Medicare ratesrather than at 100 percent of the amount billed,as has been IHS practice (132a). This recommen-dation was supported by the Director’s Task Forceon Contract Health Services and by the GraceCommission report, both of which called for auniform, standardized IHS rate structure basedon Medicare and the use of Medicare intermedi-aries for claims processing. Use of a Medicare-based rate structure, such as DRG rates, wouldgenerate substantial savings for the IHS contractcare program. One way to implement Medicarerates in IHS would be to make acceptance of thoserates for IHS patients a condition of Medicare pro-gram participation. This approach would requirelegislation and is not under active consideration.Another approach that IHS was considering at theend of 1985 was the issuance of a “general notice, ”which is provided for under Federal contractingprocedures and would not require formal rule-making. The notice to prospective contractorswould state that IHS would refer patients onlyto private providers with which it had contracts,and that it would enter into such contracts only

190 • Indian Health Care
if the contractor agreed to accept payment at nomore than Medicare-allowable rates. IHS stillwould be the last or residual payer, but if IHSwere the only payer, it would pay 100 percentrather than the usual 80 percent of the Medicare-allowable rate. Emergency services provided bynoncontract sources would be paid at full billedcharges. IHS officials have stated that the prob-lem of obtaining more favorable contract carerates is not so much one of authority as of inade-quate leverage, and it is hoped that the termsspecified in the proposed general notice may im-prove IHS’s position in negotiating with contrac-tors (78).
The use of fiscal intermediaries and carriers forIHS contract care claims processing also has beenrecommended. In addition to reducing the costsof claims processing by taking advantage of ex-isting automated systems, it was suggested thatexperienced fiscal intermediary staff could per-form the essential steps of identifying and verify-ing third-party resources for each claim. Moreefficient invoice processing could reduce dupli-cate payments and other errors. GAO, the GraceCommission, and the contract health services taskforce all supported this recommendation, and IHSwas directed to explore its potential costs and sav-ings. An analysis completed in March 1984 sug-gested that IHS could process claims more effi-ciently and at lower cost by retaining the functionin-house (69). IHS officials also have pointed outthat legislation would be necessary to permit IHSto delegate its responsibility for determining eligi-bility for services to an outside party such as afiscal intermediary (78).
The Grace Commission in 1982 noted varia-tions in claims processing policies and proceduresamong IHS areas and service units. Third-partyresources usually were identified, but verificationof provider invoices relative to claims filed wasinconsistent. Too many people were involved inthe largely manual claims processing system, andthere was a general lack of uniformity in proce-dures and of adequate controls throughout thesystem. One processing problem was the failureto deobligate on a timely basis unused funds setaside in service unit contract care budgets for au-thorized services. Excessive withholding of ob-ligated reserves reduced the funds available for
new referrals. In addition, more than one studymentioned a variety of deficiencies in contract careprogram procurement policies (119).
Conclusions
The contract care program is an essential com-ponent of IHS clinical services delivery becauseit purchases services that IHS facilities and staffcannot provide directly. Contract care now rep-resents about 20 percent of the total IHS budgetand 25 percent of the clinical services budget na-tionally, although those figures vary considera-bly among IHS areas.
Contract care allocations among the areas aredetermined by the same program continuity budg-et methods that are applied to IHS direct serv-ices: that is, each area’s share of the annual ap-propriation is approximately the same from yearto year. Contract care funding does not reflectneed, in terms of what cannot be provided by IHSdirect facilities, or demand, as expressed by ac-tual requests for contract service authorizations.Although it has been suggested that contract carefunding might be adjusted to compensate areasthat have relatively limited direct care facilitiesand that a combined direct/contract care resourceallocation formula might incorporate such a com-pensation factor, there has been no action on suchproposals. Because the types and amounts of IHSdirect services vary considerably among the areasand because contract care programs supplementthe services that IHS facilities provide directly,the mix of services covered by contract care like-wise is different in each IHS area. The private re-sources that are available as potential contractorsin a given area also affect the contract servicespackage.
In recent years, increases in annual contractcare appropriations have been less than rates ofgeneral health cost inflation. As a result, the pres-sures of funding constraints are mounting, andthe IHS contract care program currently is ration-ing services in several ways: 1) contract care eligi-bility criteria are more restrictive than criteria forIHS direct services; 2) services maybe authorizedonly according to each area’s medical needs pri-ority system; and 3) all other payers must betapped before IHS can pay the remainder of a bill

(the residual payer principle). The primary ration-ing force behind these policies is the limitation ofannual area and service unit contract care budgets,the effects of which are felt more severely in someareas than in others.
Funding levels, management policies, and con-tract care utilization patterns vary substantiallyamong IHS areas, aggravating inequities in re-source allocations and in the services available toeligible Indian residents in the 12 areas. Manage-ment of the contract care program, includingbudget management and the necessary rationingof services, is implemented at the service unit andIHS area levels within general guidelines from IHSheadquarters. The contract care program is par-ticularly difficult to manage at the immediate serv-ice unit level, where budgets have the least flexi-bility, the incidence rates of particular diseases andconditions are most variable, referral decisionsmust be made on a case-by-case basis, and unex-pectedly high-cost contract referrals can severelydislocate budget management plans. The level ofservice unit staff expertise and the quality of sup-porting data systems also affect program admin-istration. In addition, the IHS contract care pro-gram does not permit the carryover of funds fromone fiscal year to the next (although tribal 638contract care programs do have that option),which further limits the ability to manage theprogram effectively. Instead, services may be re-stricted too severely early in the fiscal year in or-der to conserve funds, and then at the end of theyear virtually any service request may be author-ized, including previously deferred services, toclose out the budget. Provision to carry over acertain percent of the annual allocation, perhaps5 or 10 percent, could ease this problem.
Some IHS area offices have established formal,centralized contract care program managementpolicies, including systems to monitor perform-ance in all service units. In some areas, such ef-forts are supported by large, labor-intensive man-ual data systems, although automated systemsclearly are needed (for example, the Portland IHSarea manages its contract care program, whichrepresents half of its total clinical services budgetor nearly $19 million, with manual systems). Pro-cedures to ensure that all applicable paymentshave been made by alternate resources (third-
Ch. 5—The Indian Health Service ● 191
party payers), a critical part of contract caremanagement, also vary depending on area officeleadership, staff capabilities and, perhaps, the im-portance of contract services in the areawide de-livery system. The mandatory use of alternate re-sources may require substantial efforts by serviceunit staff to encourage all eligible Indians to en-roll in Medicaid and other programs, and thento verify and process claims applicable to thoseprograms. Greater assistance from area office staffcould relieve the service units of some of the bur-den of dealing with many outside providers.
It is not likely that IHS’s annual appropriationswill increase substantially in the immediate future.Growth in the contract care appropriation since1980 has averaged about 10 percent per year (al-though there have been wide variations in budgetgrowth from year to year, as shown in app. C),which is somewhat below average annual infla-tion in general health care costs. Over the sameperiod, while numbers of IHS direct care inpatientadmissions and outpatient visits remained rela-tively constant or increased slightly, inpatient ad-missions and outpatient medical visits authorizedby the contract care program each declined by ap-proximately 6 to 7 percent per year (191). Theaverage number of patients being treated daily inIHS direct care hospitals has declined only slightlysince 1980, from 1,178 to 1,072 inpatients per day(a decline of 9 percent); but the average dailycensus of contract care patients has declined from398 in 1980 to 281 in 1984, or by nearly 30 per-cent (191).
That inpatient utilization has declined substan-tially while the overall contract care appropria-tion has continued to grow (even if at rates be-low general health inflation) raises questionsabout increases in inpatient per diem charges tothe contract care program, by area, comparedwith such increases in other groups of U.S. com-munity hospitals. In spite of the effects of gener-ally declining average lengths of stay, when theseutilization trends are viewed against the back-ground of a 16-percent growth in the IHS eligi-ble service population since 1980, they suggestthat budgetary restraints are limiting the servicesdelivered by IHS and, in particular, by the IHScontract care program. This conclusion is sup-ported by reports from the field that contract care

192 ● Indian Health Care—
programs have been forced by budget limitationsto authorize services primarily for medical emer-gencies and life-threatening conditions, while nec-essary but less urgent services are deferred or de-nied. Declining utilization of the contract careprogram appears to reflect funding limitations,rather than any actual decline in the need or de-mand for contract services (although demand,too, may decline if there is little likelihood of ob-taining care).
In spite of recently declining utilization, sev-eral factors suggest that in the future, IHS of ne-cessity may become increasingly reliant on thecontract care program. The present IHS networkof direct care hospitals and clinics is limited in thetypes of services it can provide, and budgetarylimits increasingly restrict new facility construc-tion, the replacement of old and inadequate fa-cilities, and needed maintenance and repair forexisting facilities. Diagnostic and therapeuticequipment purchases are limited, further reduc-ing service delivery capabilities. As the older IHShospitals and clinics deteriorate, it is not likelythat they will either be maintained or replaced ashas been the practice in the past. This situationis due to the overall budget situation and, in part,to the practical limitations of delivering compre-hensive and specialty services to many widely dis-persed small population groups. It may in fact bemore cost-effective for IHS to discontinue the pro-vision of extensive inpatient services in its ownfacilities, to contract for more of its inpatient care,and to concentrate IHS direct delivery on out-patient clinic facilities and services.
A critical factor that may orient IHS towardincreased contracting in the near future is thegrowing problem of how to recruit and retain ade-quate medical staff. IHS depends for physicians,nurses, and other medical and administrative staffon the PHS Commissioned Corps, which is nota growing resource, and on the service paybackobligations of NHSC trainees. The NHSC pro-gram is being eliminated, and the last few NHSCscholars will be assigned to IHS in 1990. It is notclear how IHS anticipates meeting this loss ofprofessional staff. If IHS direct care staff positionscannot be filled, there would appear to be littlealternative but to turn to the services of privateproviders, where they exist, under the contractcare program.
If IHS is going to continue to provide a com-prehensive range of health services to AmericanIndians, it seems likely that it will have to relyincreasingly on the contract care program. Thismay be especially true for inpatient services, ex-cept in areas so isolated that no private resourcesare available for contracting. As a result, the con-tract care program may claim an increasing shareof the IHS clinical services budget and may com-pete more intensely with direct care hospitals andclinics for funding. At current low rates of utili-zation in most IHS hospitals, averaging onlyabout 50 percent occupancy, their continued ex-istence will be hard to justify except where noalternative facilities exist.
Whether greater reliance on contract care willincrease or decrease the overall costs of health caredelivery for Indians cannot be determined at thistime. Much will depend on IHS’s ability to man-age contract care efficiently. Current administra-tive systems, levels of staff expertise, data systemssupport, and headquarters guidance and techni-cal assistance devoted to contract care might notbe adequate to manage a greatly expanded pro-gram. Because of the decentralized IHS structure,headquarters has not taken the initiative in help-ing areas and service units to resolve their con-tract care management problems.
Management policies that could maximize thepurchase of contract care services (some of thesetechniques would be difficult to implement on thesmall scale of the service unit) have been notedearlier in this section: payments to private con-tractors at rates more comparable to those paidby other buyers, i.e., 80 percent of Medicare-allowable or Medicare DRG rates, rather thanpayments of 100 percent of billed charges; en-couragement of competition among providers andmore aggressive negotiations for reasonable or dis-count service charges, where possible; automatedsystems to track and monitor contract care obli-gations and claims processing; and IHS area orheadquarters support in resolving the legal andoperational problems of dealing with many dif-ferent alternate resources, both public (especiallyState Medicaid programs) and private. Authori-zation to carry over funds from one fiscal yearto another has been mentioned as a possible meansof assisting contract care program managers touse their limited resources more effectively. The

planning and management difficulties inherent inuncertain annual appropriation levels cannot beavoided entirely in the present system, but moreserious efforts at assessing health services needsand planning services, and particularly in the co-ordination of services available through the di-rect and contract programs, could contribute tomore cost-effective services delivery.
At the same time, however, given expectedrates of increase in general health care costs rela-tive to likely IHS budget increases, even the mostefficient management techniques may not beenough to overcome the problems of inadequatefunding and a growing service population. Cur-rent methods of rationing limited contract carefunds create inequities in the services that maybe provided to individual beneficiaries living in
different IHS areas and service units. Beyond theseequity problems, the central policy and manage-ment question involves identifying and imple-menting the most cost-effective balance of IHS di-rect and contract services, and the appropriate mixof direct and contract services will be different ineach IHS area because of differences in availabledirect and alternate resources.
As IHS contract care budgets are increasinglystressed, IHS will have to become more aggres-sive and efficient in collecting applicable third-party reimbursements for services provided to
Ch. 5—The Indian Health Service ● 193. . —— — — — .
eligible Indians both in IHS facilities and by pri-vate providers under contract, Increased collec-tions will tend to shift the costs of health care forIndians to State, county, and local programs, in-creasing existing conflicts over which level ofgovernment is ultimately responsible for Indianhealth.
The IHS contract care program relates to a widerange of other public and private health providers.Changes in the general health care delivery envi-ronment affect IHS contract care, and IHS shouldmonitor such changes to anticipate how its con-tract care program can best respond to them.Changes in eligibility criteria and in the range ofservices covered by State Medicaid programs,which have been implemented in a number ofStates recently to slow the growth in Medicaidexpenditures, can have immediate and substan-tial effects on local IHS contract care programs.The non-Indian health care delivery system in theUnited States is under increasing financial stress,and future limitations in other public health pro-grams and in private provider obligations forcharity care may reduce the extent to which alter-nate resources are available to relieve pressureswithin the IHS contract care program. AlthoughIHS cannot prevent such changes, it should be pre-pared to respond to them.
URBAN INDIAN HEALTH PROJECTS
According to the 1980 U.S. census, almost two-thirds of all Indians lived off reservations, tribaltrust lands, or other Indian lands. Of all identi-fied American Indians, Eskimos, and Aleuts in1980, 24 percent lived on reservations, 8 percentin historic areas of Oklahoma (excluding urbanizedareas), 3 percent lived in Alaska Native villages,2 percent on tribal trust lands, and 63 percent livedin the remainder of the United States (148). Partof the growth in off-reservation residency can beattributed to past Federal policies such as allot-ment and termination (see ch, 2) in addition tothe changing nature of reservations and the eco-nomic developments surrounding them. Incen-
tives for Indians to move and stay away from theirhomelands exist, for example, if traditional formsof subsistence are diminished because the carry-ing capacity of reservation lands has approachedan upper limit or because of the loss of fishingor hunting resources; if there is little or no chanceof earning a living wage or maintaining gainfulemployment; if the educational system is viewedas inferior; or if the social climate is unacceptableor dangerous. With an unemployment rate of 27.8percent on all reservations in 1979 (152), it is notsurprising that more and more Indians are choos-ing to reside off of reservations, where opportu-nities to work are greater.

194 ● Indian Health Care
Funding for Urban Indian HealthInitiatives
In the early 1970s, the Federal Government be-came increasingly interested in programs to as-sist urban Indians. President Nixon’s special mes-sage to Congress on Indian Affairs stated: “BIA’sresponsibility does not extend to Indians whohave left the reservation, but this point is not al-ways clearly understood. As a result of this mis-conception, Indians living in urban areas haveoften lost out on the opportunity to participatein other programs designed for disadvantagedgroups” (94). The Office of Economic Opportu-nity was directed to lead an effort by four Fed-eral departments and agencies to alleviate theproblems faced by urban Indians, for example,by supporting existing Indian centers in major cit-ies as links between urban Indians and variousgovernment programs.
In 1972, IHS began to fund urban programsthrough its community development branch un-der the general authority of the Snyder Act. Sincethen, 42 different projects have received financialsupport from IHS. The Indian Health Care Im-provement Act of 1976 explicitly authorized ur-ban Indian organizations to contract with IHS tooperate health centers and to increase Indian ac-cess to public assistance programs. In 1984, therewere 37 urban programs in 20 States funded by
Table 5-17.—lHS-Supported Urban Indian
IHS (see table 5-17). Staffing for the urban pro-grams is shown in table 5-18.
Urban health projects are distinguished fromIHS’s reservation-based clinics by their emphasison increasing access to existing services fundedby other public and private sources rather thanproviding or paying for services directly. Theaverage number of funding sources for the 37 ur-ban programs was 5.3 in fiscal year 1984. Twourban programs, both well established, had morethan 10 sources of support each. At the other endof the spectrum, five programs relied solely onIHS for funding. Fifty-one percent of total urbanprogram funding was provided by IHS. Forty-sixpercent of the remainder came from other Fed-eral sources including the Community HealthCenters program, Maternal and Child Health, theAdministration for Native Americans, Women In-fants and Children, and Medicare. Although onlyfour programs received funds from the Commu-nity Health Centers program, this $1.6 millioncomprised 9.1 percent of total funding. State Med-icaid programs represented 3 percent of urbanprogram revenues (184).
Out-of-pocket and private insurance collectionsand private grants have been important sourcesof income to the urban programs, although in fis-cal year 1984, only 5.6 percent of total funds wereobtained from patient collections and 4.4 percent
Health Programs, by State, Fiscal Year 1984
State Location State Location1, Arizona . . . . . . . . . . . . . . . . . . . . Phoenix 20. Great Falls2. Tucson 21. Helena3. California . . . . . . . . . . . . . . . . . . Bakersfield 22, Miles City4. Compton 23. Missoula5. Fresno 24. Nebraska . . . . . . . . . . . . . . . . . . Omaha6. Sacramento 25. New Mexico. . . . . . . . . . . . . . . Albuquerque7. San Diego 26. Nevada . . . . . . . . . . . . . . . . . . . Reno8. San Francisco/Oakland 27. New York . . . . . . . . . . . . . . . . . . New York9. San Jose 28. Oklahoma. . . . ... . . . . . . . . . . Tulsa
10. Santa Barbara 29, Oklahoma City11. Colorado. . . . . . . . . . . . . . . . . . . Denver 30. Oregon . . . . . . . . . . . . . . . . . . Portland12. Illinois. . . . . . . . . . . . . . . . . . . . Chicago 31. South Dakota. . . . . . . . . . . . . . . Pierre13. Kansas . . . . . . . . . . . . . . . . . . . . Wichita 32. Texas . . . . . . . . . . . . . . . . . . . . . Dallas14. Massachusetts . . . . . . . . . . . . . Boston 33. Utah . . . . . . . . . . . . . . . . . . . . . . Salt Lake City15. Michigan . . . . . . . . . . . . . . . . . . Detroit 34. Washington . . . . . . . . . . . . . . . . Seattle16. Minnesota . . . . . . . . . . . . . . . . . Minneapolis 35. Spokane17. Montana . . . . . . . . . . . . . . . . . . . Anaconda 36. Wisconsin . . . . . . . . . . . . . . . . .Green Bay18. Billings 37. Milwaukee19. ButteSOURCE U S Department of Health and Human Services, Public Health Service, Health Resources and Serv!ces Administrallon, Indian Health Service, “Major Health
Facilities for Indians and Alaska Natives, ” I!sting urban Indian health programs by State, 1984.

Ch. 5—The Indian Health Service ● 195
Table 5-18.—Urban Indian Health Program StaffProfile, Full-Time Equivalents, Fiscal Year 1983
Medical Other Total IndianProgram or dental staff staff (percent)
All programs . . . . . 112.5 479.2 591.6. . ,Albuquerque, NM . . . 0.5Anaconda, MT . . . . . . —Bakersfield, CA . . . . . 0.5Billings, MT . . . . . . . . 0.4Boston, MA . . . . . . . . 0.7Butte, MT . . . . . . . . . . —Chicago, IL . . . . . . . . 0.2Compton, CA. . . . . . . 9.8Dallas, TX. . . . . . . . . . 4.9Denver, CO . . . . . . . . 1.4Detroit, Ml . . . . . . . . . 0.6Fresno, CA. . . . . . . . . 3.5Great Falls, MT . . . . . 3.0Green Bay, WI . . . . . . —Helena, MT . . . . . . . . 1.7Miles City, MT. . . . . . —Milwaukee, WI . . . . . . 11.0Minneapolis, MN . . . 5.3Missoula, MT. . . . . . . —New York, NY . . . . . . 1.0Oklahoma City, OK. . 5.4Phoenix, AZ . . . . . . . . —Pierre, SD. . . . . . . . . . 4.5Portland, OR . . . . . . . 3.7Reno, NV . . . . . . . . . . 1.0Sacramento, CA . . . . 5.0Salt Lake City, UT . 2.1San Diego, CA. . . . . . 3.5San Francisco, CA . . 8.6San Jose, CA. . . . . . . 2.6Santa Barbara, CA . . 4.0Seattle, WA . . . . . . . . 14.2Spokane, WA. . . . . . . 4.2Tucson, AZ . . . . . . . . 2.0Tulsa, OK . . . . . . . . . . 5.1Wichita, KS . . . . . . . . 2.0
8.01.07.83.0
14.11.04.8
29.521.8
7.09.39.81.59.10.82.0
48.060.6
2.68.09.87.03.5
12.95.3
19.07.57.0
28.08.28.1
64.011.62.2
24.610.8
8.51.08.33.4
14.81.05.0
39.326.7
8.49.9
13.34.59.12.52.0
59.065.9
2.69.0
15.27.08.0
16.66.3
24.09.6
10.536.610.812.178.215.84.2
29.712.8
59.3 ”/0
11.8100.060.288.281.1
100,080.031.073.073.885.951.177.8
100.040.0
100.038.158.6
100.088.965.878.662.565,131.766.755.257.165.627.824.870.155,152.468.753.1 0/0
SOURCE’ U S Department of Health and Human Services, Public Health Serv-ice, Health Resources and Services Admirrtstration, Indian Health Serv-ice, Division of Health Systems Development, Urban /nd/arr Hea/fhProgram Eva/uaf ion Project, Fisca/ Year 1983 (Tucson, AZ IHS, Febru-ary 1984), table 5
from private grants. An average 17 percent of In-dian clients across all programs had some formof private health insurance, but the extent of cov-erage and ability to meet deductible and copay-ment requirements is not known (138). Twenty,or 55 percent, of all urban programs request someform of payment from their clients (184). The pro-grams do not require payment for services, how-ever, and sliding fee scales are used to determinethe amount requested of clients. A complete ac-count of funding sources and allocation of costs
for the urban programs is provided in tables5-19 and 5-20.
In order to receive IHS support for an urbanIndian health project, an organization must sub-mit an application. Criteria that IHS applies tomake funding determinations on the urban pro-grams include attention to cultural barriers, con-ditions discriminating against Indians, inabilityto pay for health care, lack of facilities provid-ing free care to indigent persons, lack of State orlocal health programs, technical barriers createdby State and local health agencies, availability oftransportation to health care services, and dis-tance between Indian residences and the nearesthealth care facility (42 CFR 36.351). Funding forspecific programs has taken into consideration theextent of unmet health needs in the urban com-munity, as determined by the incidence and prev-alence of disease, life expectancy, infant mortal-ity, dental needs, housing conditions, familyincome, and employment status. There have beenno new urban Indian health projects establishedin the past few years. Projects that have been inexistence longer and have had time to strengthentheir organizations tend to receive a greaterproportion of IHS’s allocation for urban Indianhealth projects.
Two other important factors in determiningfunding priorities are the Indian population in ur-ban centers and whether the city has an existingurban Indian health program. With respect topopulation, there are five levels of priority, withgreatest preference given to cities with more than9,000 Indians and lowest preference given to lo-calities with fewer than 1,000 Indians (42 CFR36.351). The 1980 census identified 114 out of 318Standard Metropolitan Statistical Areas (SMSAs)as having more than 1,000 American Indians, Es-kimos, and Aleuts (see table 5-21). Two of thefour largest urban Indian health programs sup-ported by IHS are located in SMSAs that rankedeighth and ninth on the list of SMSAs with thelargest numbers of Indians; however, 7 of the 37’projects funded in fiscal year 1984 served Indiansin communities that had fewer than 1,000 Indianinhabitants in the 1980 census, and 3 programswere located in cities with an IHS hospital or clinicin close proximity.

Table 5-19.—IHS. Funded Urban Indian Health Programs, Fiscal Year 1984:Distribution of Reported Revenues in Dollars, by Source and by Program
—CHC Other IHS IHS
ProgramOther 3d Patient
Total Sec 330 MCH Title X WlC Federal Title V other Medicare Medicare party collections State County City Other
$508.967 $144.671 $774,2862.91% O 83% 4.42%
— — —— — —— — —— — —— 1880 –— — —— — 19539
165761 – –— 4,625— 13,000 25,880
25000 –— — 15501— — —
30,500 – 21 801— — —— — —— 60,575
57654 2 7 5 2 4 1 2 7 2 4 513,000 – 37008
— 60,000 –— 11,250
— — —— — —— — —— — 8,268
35319 – 25,935— — 17497— — 5,554
68500 – 9,500— — —— — 10,000
135031 17267 264,026— — 29,460
3202 – 769— 34,604
— — 45,249
All programs $17517,838 $1595143 $294,233 $108.502 $645979$1234015 $7,928,531 .$929,533 $97,154 $590478 $546,390 $980,502 $1 139,454Percent by source
Albuquerque NMAnaconda, MTBakersfield, CABillings, MTBoston, MAButte MTChicago, ILCompton, CADallas, TXDenver, CODetroit, MlFresno, CAGreat Falls, MTGreen Bay, WIHelena, MTMiles City, MTMilwaukee, WIMinneapolis, MNMissoula, MTNew York, NYOklahoma City, OKPhoenix, AZPierre, SDPortland ORReno, NVSacramento, CASalt Lake City, UTSan Diego, CASan Francisco, CASan Jose, CASanta Barbara, CASeattle, WASpokane, WATucson, AZTulsa, OKWichita, KS
100 .0%
111,51930.429
14069077,012
34901437,543
179,7711,5394101 121,760
222,027231856494,556101 49418336492,229
1099092,1387131,432,838
129,798316,000517,600165297197,528394,222158,436514,889201,620407,801
1 087,898469,338326190
2,263,198317,262156,099924.942375586
9.11%——
—
—
———
———
864,414328451
———
12,586——
—
——————
389,692—
1 68%——————————
11,90650,000
————
43459————————
——
188868———————
O 62% 3 69% 7 . 0 4 %—
—
3738
10.603—
—642675
——————
68,780246737
—20,00017000
——————17————
126,665——
97800—.
45.26%
98,49930,429
118,2167701296,57437543
137,992548,676357,226183,147193,000175,436101 494129,00064,62041,129
389232588899
59,790119000463,000133,226165,500276,200150168122419146727231,061352,680187662176785
1,093,254173716134,369332,894241,956
5.31% o 55% 3 37% 6 50%————
22257——
183194———
99565—
206319547
——
10875—
9000015,057
—11 478
——
208775—
108579116,874128,00172,665
9,534—
1 012—
39,978
3 12% 5 60%
13.020 —— —
——
18.736—
— — —— — — —
217700—— — —
13319192000
—6.197
—24,390
—
10044481
2,274— —106,002 56,699
— 92844
—287078
—
—— — — —50300 1.500
21 553
— —— 88.020 —— —
—— — —1.869
72962—
3604—
91000292190
—
2589— ——— — — —
251400— 72146 31688 15.100—— — —
— — — —30000— — —
64315,081
—390
—370
—26890
—
26257787
34.29916,56317,828
260000—
44,87744,66911,16912,93527.06111.837
— —— 14,301 2,689 —
5339— — — —15,991
—11 544
1,39928085
97,88911 23043,29215541
9335,987
15,193
— 39.660 18000 36584— —
—
—4449 72149
70612,889
—— 18711
3805——
—91 47653.286
—
21,43147,481
36,904
—2500 —
— 10,63315336535640
—341 700 12964
4,2552,201
—1 772
—————
—678
—19,601—. —— — —.—
Revenue Sources CHC = Federal Commumty Health Center MCH = Federal Maternal and Chdd Health TKle X= Federal Family Planning WIC = Federal Women lnfarws and Children Title V = IHS UrDan Indian Funding
SOURCE U S Department of Health and Human Serwces Pubhc Health Serwce Health Resources and Serwces Admmlslfallon Inolan Health Serwce Diwslon of Health Systems Development Urban /rrdMn Hea/fh F7qecr Eva/ua(~on Reporl Fma/ Year7984 (Tucson AZ IHS June 1985I table I

Table 5-20.—lHS-Funded Urban Indian Health Programs, Fiscal Year 1984: Distribution of Costs in Dollars by Program Component
Program Total Medical
All programs $16567293 $3724830
Lab and PharmacyX-ray (medical Dental
$451940 $342139 $2167395
Community FacilityHealtheducation
$796.3724.81%
5.827
7020348
4.1098544384,572
303723500
—5273
94287130976
1 678—
2522
4931-.
90003008
100216
223290
Mentalhealth
SubstanceabuseNutrition Optometry
$2166751. 31%
Other service ‘ Administration related
$628232 $1.293.840 $3.548.400 $1022693$6021453. 63%
10.020
——
—
763311.160
—
840
6 6 2 6 82604
6996
186039
654
—14301
23500
—16325
91 476
4843123250
—
33.950
5 5 9 1 0 0 93 . 5 7 %
$1 .181 .6237 13%
200——
433 183
—
3 7 4 6 6
3 3 0 7 8
8751 5 0 0 0 0
11 478
5 1 5 3 4 3—
Percent of costs
A lbuquerque NMAnaconda MTBakersfield CABillings MTBoston MABut te MTChicago ILCompton CADallas TXDenver CODetroit MlFresno CAGreat Falls MTGreen Bay WIHelena MTMiles City MTMi lwaukee WIMinneapo l is MNMissoula MTNew York NYOklahoma City OKPhoenix AZPierre SDPortland ORReno NVSacramento CASalt Lake City UTSan Diego CASan Francisco CASan Jose CASanta Barbara CASeattle WASpokane, WATucson, AZTulsa OKWich i ta KS
100.00%
1 1 0 0 5 82 6 9 7 1
1 2 9 9 7 67 7 0 1 2
3 6 4 9 0 23 8 3 2 3
1 5 3 8 3 41 539410
7 7 8 4 9 5211 .7941 7 9 3 4 94 9 4 5 5 6101 4941 6 7 3 6 41 1 8 9 3 7
41 .1292 0 4 2 7 2 41 345261
6 7 7 3 74 1 8 0 0 04 5 4 5 4 1165 ,2972 3 8 5 2 7378 ,6001 5 0 1 6 83 4 7 5 7 61 3 6 0 2 9355 ,355
1 ,081 ,898187 ,7423 0 2 2 5 0
2 4 8 8 0 5 04 6 6 1 0 12 3 1 4 1 3801 1663 7 5 2 5 4
2 2 . 4 8 %
3 0 8 3 0—
21 9761 6 8 0 01 2 0 3 0
2 4 0 121 .524
3 8 0 4 2 18 7 8 3 61 4 7 0 320 .932
1 2 0 7 0 24 2 8 5 2
—
4 5 3 2 8—
3 4 3 3 3 42 6 2 9 0 2
11 80724 .300
122 ,417111 6371 0 4 8 0 6139 ,275
4 2 0 9 485 ,0342 7 5 6 8
1 2 4 3 7 4497 ,742
6 1 6 3 7—
4 7 6 8 4 41 1 9 5 0 81 2 9 7 6 5156 ,522
6 4 9 2 9
2.07% 13.08%
—1 370
25.168239401104847
90783867
70832—
709
175792258789
2583—
90096
6950312 196
124554202980
8035199188317779
87351
8993573342
3.79%
1.5001 6582318
—135 505
796
13689
246522273
4462
338248
—I 7000
19422
4800
3,536
172672570514501
900
7 81%
1 45040.3351563329481
2292267066564
195,08164.3323823861 309
968160036
902531 41648023
115625749
10390018023
8749160002812924,437
—357827070015.6194225257998
129013075218721
21 42%
5890621.25351.071%29498
148 1462428873408
151 045182847
71 80753.052
105765268765992320282
755344803022286641.27118600
118,06939,35950,41963,00042349
1242366632670645
137,0005890560360
4462359785750298
169988136867
6.17%
1.0072610
14276b 840
—28956221
25281920452655924954146563892
1432715,000
2160180765104383
400710200057382
22,20745000
4 794280893600
900026298
4420321.08297.70619454
1 768—
1 184
4.123734
4.97111.142
910
7 0 5 7
217’
1 5001 8 9 6 5
310—
—32720 —
1 656—
75270
1 0 4 0 6
—6 175
6084
8051868503
1 312—
22,929—
2357423,825
51493,324
—3641
—
3955 1 823
1 1 9 2 1 51 2141 9952 2 0 0
2 3 1 0 3—
5 0 0 021.000
3 3 0 01 2 9 5 3
—
28473180003
806—
1 2 2 9 447,000
—5214
360002700
—8841027342
286624.155
6010
—18.000 1 0 0 0 0
8004450
1760224530335885
—
881812463—
1982025000
— —
8618S O U R C E U S I)er)arlrnenf of Health and Human Serv)ces Publlc Heallh Serwce Health Resources and Sewlces Admln[stratlon Jndlan Hedl!h S~r#lce Olvlslon of Health Systems Development Urodfl ~ndk?n /led//h Pro/cc/ Evahalm @x?r/ &icJ/ Veal/
1984 (Tucson AZ IHS June ~ q85 I table 2

198 • Indian Health Care
Services Provided by Urban IndianHealth Projects
In the summer of 1985, OTA conducted a shortmail survey of the existing urban Indian healthprojects to supplement information available fromtwo evaluations performed by IHS. These evalu-ations, covering fiscal years 1983 and 1984, weredesigned to assess the progress of urban Indianhealth projects from their inception in 1972 totheir current status as a program authorized bythe Indian Health Care Improvement Act,
The OTA Survey found that most of the ur-ban projects or “human service organizations”funded by IHS offer a wide range of social serv-ices that are organized to alleviate individual orfamily problems or to fulfill basic human needs(48). Thirty-two percent of the patient encoun-ters reported by the urban programs in fiscal year1984 were medical; 10 percent were dental; 27 per-cent were health-related (health education, nutri-tion, mental health, optometry, and substanceabuse programs); and 31 percent represented othercommunity service contacts (184).
Table 5-22 outlines 10 broad categories of non-medical, nondental services provided by the ur-ban programs. The health education category in-cludes activities such as health fairs, diabeticcontrol sessions, prenatal classes for mothers, ahealthy babies perinatal project, instruction in firstaid, management of chronic medical problems,and literature on disease and trauma prevention.The jobs and training category includes employ-ment and training services, economic assistanceto Indian businesses, classes for the illiterate, aJob Training Partnership Act program, an Indian
Table 5.21 .—Distribution of the American Indian,Eskimo, and Aleut Population Among SMSAs, 1980
Numbers of American Indians, Numbers PercentEskimos, and Aleuts in SMSAs of SMSAs of total
> 9,000 . . . . . . . . . . . . . . . . . . . . . . 20 6.30/o4,500 to 8,999 . . . . . . . . . . . . . . . . . 15 4.73,000 to 4,499 . . . . . . . . . . . . . . . . . 16 5.01,000 to 2,999 . . . . . . . . . . . . . . . . . 63 19.8< 1,000 . . . . . . . . . . . . . . . . . . . . . . 204 64.2
Total population . . . . . . . . . . . . . 318 100.0%0SOURCE: U.S. Department of Commerce, Bureau of the Censusl 1980 Census
of Population: Characteristics of the Population, General PopulationCharacterlstks, U.S. Summary (Washington, DC: U.S. Department ofCommerce, December 1963), PC60-1-B1, table 69.
leadership program, and training programs foremployees. The nutrition category, which is fundedmostly from non-IHS sources, encompasses theWomen, Infants and Children program (one ofthe major services provided to non-Indian clients),Federal food commodity distribution, and severalemergency food banks. Outreach includes homehealth care similar to the community health rep-resentatives program, referral, transportation, andliaison with governmental agencies and the public.
The social services category, which includes abroad range of services, is similar to what sometribal health departments provide to complementthe medical care delivered directly by IHS. Ex-amples of the social services provided by someurban programs include: paralegal counseling andadvocacy; housing counseling, including food andlodging for the homeless; limited financial assis-tance, ranging from prescriptions and partialpayment of emergency health care to fuel billassistance; offender/ex-offender rehabilitation; apatient representative program; a senior center;a recreation center; and clothing. In some cases,these social services are part of mental healthactivities staffed with professional counselorsoffering help to all age groups.
The urban Indian health programs serve Indiansand non-Indians. IHS regulations do not prohibitthe programs from serving non-Indians, and othersources of Federal funds often require urban In-dian centers to serve certain populations that in-clude non-Indians. Hence, the only requirementthat IHS imposes is that the number of Indiansserved by each program be proportional to theamount of money provided by IHS.
In fiscal year 1984, close to 60 percent of theusers of the urban programs were Indian. In halfof the programs, Indians represented 90 percentor more of the clientele; and four of these pro-grams served Indians only (184). Verification ofeligibility for IHS-funded urban Indian activitiesconsists primarily of presentation of a certificateof degree of Indian blood issued by a tribe or BIA,a tribal membership card, or certifying affidavitssigned by three eligible Indians (138).
Most. of the urban Indian programs could notsurvive on IHS funding alone and would be in-efficient if they served only Indians. Because they

—
Ch. 5—The Indian Health Service . 199
Table 5-22.— Nonmedical, Nondental Services Offered by IHS-Supported Urban Indian Health Programs:Fiscal Year 1984
Small programs Medium programs Large programs Total(N= 10) (N= 10) (N =7) (N =27)
Type of service Number Percent a Number Percent a Number Percent a NumberHealth education . . . . . . . . . 9 360/o 14 560/o 2 8% 25Family planning . . . . . . . . . . 1 25 1 25 2 50 4Jobs and training . . . . . . . . 3 50 0 0 3 50 6Nutrition . . . . . . . . . . . . . . . . 5 21 8 33 11 46 24Formal outreach . . . . . . . . . 12 55 8 36 2 9 22Social services. . . . . . . . . . . 22 48 14 30 10 22 46Alcohol and drug ... , . . . . . 1 17 2 33 3 50 6Counseling . . . . . . . . . . . . . . 3 38 2 25 3 37 8Children and youth . . . . . . . 2 33 3 50 1 17 6Family support. . . . . . . . . 3 25 4 33 5 42 12ap~rC~ntag~~ ~hOWn are percent of row totals The number of services may exceed the sample size since some programs offered more than one unique service within
a given category
SOURCE U S Congress, Off Ice of Technology Assessment, “Survey of Urban Indian Health Program s,” 1985
were established to provide medical and socialservices to a group of clients who are largely eligi-ble for public health care, a few of the programshave competed successfully for a place within theirlocal health delivery and social services network.For example, the Urban Indian Health Board, Inc.,in the San Francisco Bay Area contracts withAlameda County to provide care to medically in-digent non-Indian adults in its Oakland clinic. InJune 1985, the State of Minnesota decided to serveits Medicaid population through health mainte-nance organizations. The Indian Health Board ofMinneapolis, an urban Indian clinic that served945 Medicaid-eligible clients in 1984, became qual-ified as part of the health maintenance organiza-tion delivery network (113).
Conclusions
Urban Indian health programs are importantbecause of the demographic changes that havetaken place in the Indian population, In the 1980U.S. census, 50 percent of the 1.4 million personswho identified themselves as Indians lived in met-ropolitan areas. Approximately 829,000, or 59percent, of the 1.4 million Indians were includedin IHS’s estimated service population living on ornear a federally recognized reservation. Thus,about 10 percent of Indians identified in the 1980census were living on or near reservations thatwere in or contiguous to metropolitan areas.However, IHS-supported programs for urban In-dians have always been viewed and treated as sep-arate from IHS’s reservation-based service system.
Health care services are provided to Indiansbased on political relationships between theUnited States and tribal governments. When serv-ices are extended to Indians on the basis of race,as might be the view of urban program servicessince tribal governments are not involved in them,one of the basic premises of the trust relationshipis undermined. An essential feature of IHS serv-ices for Indians is that individual recipients of careare affiliated with political entities, Indian tribes,that have established claims to such care. WhenIndians leave their reservations and the jurisdic-tion of their tribes, they lose whatever degree oftribal affiliation is associated with residence onan Indian reservation. One group, the NationalTribal Chairmen’s Association, once viewed asthe major opponent of programs for urban In-dians, has held that urban Indians relinquish theirright to health care from IHS by leaving tribaljurisdiction. In congressional hearings of March1985 (93), the executive director of the NationalTribal Chairmen’s Association retracted the orga-nization’s opposition to IHS funding for urban In-dian health projects. Members of the NationalTribal Chairmen’s Association still feel, however,that non-tribal organizations, such as the non-profit corporations that operate urban Indian pro-grams, should coordinate the services they pro-vide for Indians with tribal governments andelected Indian officials. But coordination of serv-
ices between urban Indian health projects and areatribes is a formidable task. In some urban centers,there are as many as 40 tribal governments nearby,and representation by tribes on governing boardsmight include over 80 different tribes (4).

200 ● Indian Health Care
Urban Indian health programs, lacking tribalgovernment legitimacy, may always be subject toopposition from tribal groups. The disagreementbetween some tribal leaders and proponents of theurban programs is as much over having to sharefunding as over points of law. Leaders of severalurban Indian organizations feel strongly that theFederal Government is responsible for providinghealth care and social services to Indians regard-less of their chosen residence (4,57). The fact thaturban Indian health projects have been fundedsince 1976 by appropriations under the IndianHealth Care Improvement Act, and have been
operating under continuing resolution appropri-ations in fiscal years 1985 and 1986 in the absenceof reauthorization of that act, indicates that theirfuture is uncertain. The Administration’s IHSbudget proposals in recent years and for fiscal year1987 have eliminated funding for urban Indianhealth projects. The negative effects of the Fed-eral budget deficit on overall IHS funding suggestthat priority is likely to be given to maintainingreservation-based direct and contract care deliv-ery programs, rather than to maintaining or ex-panding urban Indian programs.
THE IHS HEALTH FACILITIES CONSTRUCTION PROGRAM
The IHS health facilities program providesfunds for the construction of hospitals, healthcenters, health stations, sanitation facilities, andpersonnel quarters for eligible staff at these facil-ities. Since 1970, the program has built 14 hospi-tals, 20 health centers, and about 700 units of per-sonnel quarters. The program also provides fundsfor the major modernization and repair of exist-ing facilities. In 1960, a program to provide sani-tation facilities and systems for Indian homes andcommunities began. This responsibility is sharedby IHS with the Department of Housing and Ur-ban Development (HUD) and BIA through itshousing improvement program.
Funding for the IHS facilities construction pro-gram is appropriated by Congress separately fromthe IHS health services delivery budget. In fiscalyear 1985, $61.6 million was appropriated for fa-cilities construction, compared with $807 millionfor services delivery and program management(see app. C). Appropriations for facilities con-struction by type, 1956 through 1985, are sum-marized in table 5-23.
As of October 1984, within IHS’s direct andtribally operated system, there were 51 Indianhospitals; 124 health centers; 285 smaller healthstations, Alaska village clinics, and school healthcenters; 489 treatment locations (not fixed facil-ities); and 1 extended care facility (191). With thecompletion of sanitation facilities provided by the1984 appropriations, over 144,000 American In-dian and Alaska Native homes will have received
water supply and/or sewage disposal systems(177). It is estimated, however, that about 22,000existing homes have not yet received first serviceand that the unmet need for sanitation facilitiesis approximately $520 million (60). The IHS fa-cilities construction program, its operation, andplanning methodologies are described below.
Priority System for the Constructionof Health Facilities
IHS has developed a priority system for theconstruction of clinical facilities (167). A commit-tee that may include members from PHS, HRSA,IHS headquarters, and IHS area offices applies thispriority system. The first priority list under thissystem was compiled in 1980; application of thesystem is described below and illustrated in fig-ure 5-10.
Application of the priority system results inthree groups: Group A consists of those projectspreviously proposed to Congress for which fundswere not appropriated (these projects are placedat the top of the priority list); Group B includesthe top 10 new inpatient and ambulatory careprojects respectively (5 each); and all otherprojects comprise Group C.
Phase I of the priority ranking system dividesGroups B and C by assigning numerical valuesto workloads at the facility, demand for healthcare in the area, ability of the current facility to

::“G.—(u=.—.—.—
l%%(/3”
Ch. 5—The Indian Health Service ● 201
Oooomoo ooooooo ooooooo oooooooooooo0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 00. 0-0.0-0 0- 0.0-0-0-0 .0-0-0 0. 0-0 0.0.0.0-0.0.0.0-0-0.0.0. 0-0.=$ WI o N m-ml o h C9 * CD - r= m-m m N-m m m o m o u- l m -r b o 0 CN m~$E~z%%z?g”mN””””a”aamom*”a”m”mC L . - t - m - l n - t - y c n r ’ cc-=r-o-cq--mm.-h. *-O.I-.*U7-mm-mm-s-m---r-mbm*momomm@**mmmmmme@omom-m-Oobmmhhbo-mmssm-mrrr-
7
t9
0 0 0 0 0 0 0 0 0 gcg0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 gg0-000-00-0.0 0- ,0.0-, 0 0 0 0 0 0 0 0 0 0 0 0O-o-omohcc.omo.o- 0.0.0.0- , 0-0.
%eg%$$s%%o::o+++”o”o’”o”ooo”ossk-30JooxrhNoool---=t-onmcocqo-al ~ -. F ~.~.m~.=-fqo.~~ 00KIN-3 CDc-’l
-.=Ln -m r N*N- .N
6 9 -
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0g.g-g-g-g.g.goooooooooooooooooooo-o”o-o.o-o-omomoeo-o.o-o-oeo-o-o~o-o-o%o-Oocoooooocove.mmoomb=tacoohooooooooOommwsqqqmsmhemmommmmmmoomo !00!lqoocc-hcNcc)-co (moRlnmr-bm*hcn cq=J-FxN.m.cQmohomu-hNqe-m-aw-o-oe-m-rm-o-am-m”mm’mommqsemmaolTtmlnlnlnnlN7m-=tc9moJ.?-l-r-
0 0 0~ 0 0 0s 000 000 000000 ~,0,0 ,000,0000 0 0 0 00 0 0 ~-o 0-0 0 - . - O - O ~ - q - o - o o 0 0 :- :-:-0 :-0 o 0(w C90m U-loln
%co- U71-fx m-co NONO ~I-mm
i#
88888gEsg 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 00 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0O-omo-o-o”o.omo Ov , o-o-o-o~o-o o-b CNobcl)omo.=t-o. 0.0.ao*ooocno-ooooolnolnbm-r==”b-m-cL5u--o-m-mlnoooa)oqooomu)m c9LnOJ-tul=tm.*FmJr=r=m4b*c90cDomam-olm-a-~-rm CDCC-N -u--)coTt--a)bNmohnlLr-obobcum m-mm
. .v 04 VT- l-ml-
-“
ucm

Figure 5-10.—IHS Facilities Construction Process From Assessment of Need to Congressional Appropriation
SOURCE: Adapted by the Office of Technology Assessment from Information provided by U.S. Depadment of Health and Human Services. Public Health Service, Health Resources and Services Administrat-ion, Indian Health Service, Program Planning Branch, 1985.

Ch. 5—The Indian Health Service . 203
meet demand, accessibility of alternative sourcesof care, and facilities evaluations conductedwithin the past 3 years by DHHS regional offices.Phase II verifies Group B scores and further ranksthe projects on each list. The final priority con-struction list, then, is headed by Group A projectsand followed by the top five Group B projects foreach type of facility (inpatient and ambulatorycare).
After a project has been approved by the pri-ority system committee for inclusion on the pri-ority list, the proposed facility then undergoes amore complete evaluation and a program infor-mation document (PID) is developed. The PID,which defines the scope of the project, is preparedby IHS headquarters or the area office in conjunc-tion with the affected tribes. It contains informa-tion about existing health care delivery patternsand conditions, availability and accessibility ofalternate resources, existing and projected work-loads, populations to be served, existing programdeficiencies, staffing conditions and requirements,alternative construction sites and the conditionof those sites, and the amount and type of con-tract health care. The PID is used to define thesize and location of the proposed facility and itsequipment (78). Staffing requirements for a pro-posed facility are determined by IHS’s resourcerequirement methodology, based on the projectedsize of the service population and projected work-loads (60).
In 1984, PID development became more stand-ardized with introduction of the “Facility Plan-ning Forecasting Guidelines” (190). This documentis essentially a procedures manual that containsthe relevant information outlined above and in-structions for calculating the workload rates andprojections.
The methods used in projecting workloads as-sume that future utilization patterns will reflectcurrent utilization, adjusted to the size of the esti-mated future service population. For example, a3-year base period actual utilization rate is usedto correct for aberrations in any single year, andadjustments are made to compensate for unmetneed in the base utilization rate. Such adjustmentsare made only if documentation, such as lists ofdeferred cases, can be provided.
There are differences of opinion concerningboth current population figures and assumed ratesof growth. IHS derives its population figures fromU.S. Census Bureau data, but there are concernsabout the accuracy of these numbers in many In-dian areas. IHS projections are adjusted to the lo-cal level for Indian births and deaths but do nottake into account migration, i.e., Indians mov-ing out of or into the service area. Until recently,IHS used the population figure for the middle yearof the 3-year base period (a statistically accept-able method) to calculate a facility’s utilizationrate. At the request of PHS, however, the last yearof the 3-year period now is used. This yields alower utilization rate than would result if the mid-year population were used, assuming growth inpopulation and utilization.
Workloads are projected 8 years into the fu-ture, which represents the estimated length of timefrom PID development to completion of a newlyconstructed facility. Workload projections arebased on an analysis of the following currentworkloads: 1) the direct workload of the subjectIHS facility generated by people residing withinand outside the subject service area; 2) directworkload at nearby IHS facilities generated bypeople residing within the subject service area; and3) a portion of contract care cases generated bypeople residing within the service area that couldbe handled in the new facility based on plannedservices (190). If data on contract health cases areinadequate and a detailed analysis cannot be per-formed, it is assumed that no more than 25 per-cent of the contract care workload will be pro-vided in the new facility. This is a recent revisionin IHS planning standards. Prior to publicationof the forecasting guidelines, a default value of50 percent of contract care was used.
The completed PID is submitted to PHS throughHRSA. Unanimous approval of the PID by IHS,HRSA, PHS, and DHHS is the next essential steptoward actual construction. As of late 1985, theguidelines for facilities planning described abovehad been adopted only by IHS, not by HRSA,PHS, or DHHS. Most PIDs developed since IHSadopted the guidelines in 1984 have not yet beenthoroughly reviewed by HRSA, PHS, or DHHSbecause of a backlog of projects, and therefore

204 • Indian Health Care
these agencies have not had an opportunity to as-sess how well the process works. HRSA, PHS,and DHHS are not required to apply a particularmethodology in making their facilities construc-tion decisions.
Methods for Assessing Need for Newand Replacement Facilities
Bed Size and Surgical Services
Prior to the mid-1970s, IHS based its decisionsregarding the size of new or replacement hospi-tals on one of four hospital bed planning meth-odologies. In 1977, however, in response to a re-port by GAO, Congress imposed a moratoriumon IHS’s hospital construction until its acute carebed need methodology was revised (131).
IHS began using its revised system, the “Meth-odology for Determining Future IHS Acute CareHospital Bed Needs, “ in 1980. Inpatient servicesare divided into general acute care and obstetrics.The average daily patient load over the 3 mostrecent years forms the base period workload rate.This figure is adjusted for eligible individuals whoreceived care elsewhere because of limitations inthe services available from their existing IHS fa-cilities, and for documented cases where care wasprovided at the patient’s own expense. This ad-justment reflects the assumption that an ade-quately staffed replacement hospital would be ex-pected to provide directly some of the care beingreferred out to other hospitals. The expected uti-lization rates are applied to a population estimateprojected 8 years into the future from the baseyear. Projected average daily patient loads are ad-justed to cover daily census fluctuations by esti-mating the number of beds that would be neededif the number of general acute care patients ex-ceeded bed capacity no more than 10 percent ofthe time, and if obstetrical patients exceeded bedcapacity no more than 5 percent of the time.
The results of these calculations are comparedwith those of two other standards: 1) generalhealth planning guidelines recommending 3.7 bedsper 1,000 population; and 2) an average facilityoccupancy rate of 80 percent, which representsreasonably efficient operation in short-stay hos-pitals (although nationally, hospital occupancy
has averaged around 75 percent in recent years).If both of these methods generate a need for fewerbeds than the forecasting guidelines calculation,the larger of these two alternatives is selected asthe final estimate of needed hospital beds. Other-wise, the calculated value is used as the finalestimate.
In estimating future needs for surgical services,the most recent 3-year surgical caseload is aver-aged and projected 8 years into the future, ad-justed for simple population growth. Under IHScriteria for establishing an inpatient surgical serv-ice, a workload of 1,200 to 1,300 surgical casesper year is accepted as firm evidence of need fora surgical service. The minimum workload nec-essary for consideration of a surgical service is 600to 900 cases per year. These rates were derivedfrom IHS’s resource requirement methodology,which requires need for a minimum of three sur-geons to establish a surgical service. The 1,200case level reflects 400 cases per surgeon per year,and the 600 to 900 figure reflects 200 to 300 casesper surgeon. (OTA applied these planning criteriato a particular facility construction case at the re-quest of the U.S. Congress, Senate and House Ap-propriations Committees. The results of that anal-ysis may be found in“Replacing the Rosebud1985 (140). )
Staff Quarters
the OTA Staff Memo,Sioux Hospital, ” August
In addition to establishing the size of the facil-ity and its scope of services, the PID developmentand approval process provides the basis for de-termining the number of personnel quarters neededto house facility staff. Although IHS attempts tocoordinate funding requests for staff quarters withthe facility construction schedule, such requestsfrequently have been disallowed or omitted fromfinal budget plans at higher levels in DHHS. Asa result, construction of personnel quarters maynot begin until after completion of the facility,leaving new facility staff without adequate oracceptable housing. When staff cannot be housed,expected levels of services cannot be provided(78).
Staff quarters are provided for new facilitiesand for facilities where there is a housing short-

Ch 5—The lndian Health Service . 205
age or where the units are substandard. The num-ber of units for newly constructed facilities is esti-mated from PID information on optimal staffingrequirements for the proposed facility. In addi-tion, the Public Health Service Quarters Manage-
ment Handbook aids in determining need for staffquarters by setting down the rules governingwhich staff qualify for quarters. The housing needdetermination is further adjusted by local hous-ing availability, whether this local housing meetsHUD standards, and the experiences of other IHSfacilities regarding the numbers of eligible employ-ees who live on or off the reservation. The deter-mination of the need for personnel quarters forexisting IHS facilities is similar to that describedabove, except that it is based on current author-ized staffing instead of projected staffing.
The House Committee on Appropriations re-quested that a priority system for the funding andconstruction of personnel quarters be in place bySeptember 1985. At the end of 1985, IHS was de-veloping such a priority system (62,78).
Medical Equipment
The PID summarizes relevant information con-cerning the equipment needs of the new facility.Funds for equipment generally are provided in thefacility construction appropriation, but the equip-ment list is subject to additional approval. Eacharea office submits a list to IHS headquarters forverification and approval. Replacement equip-ment for an existing facility is considered in themaintenance and repair budget and undergoes aseparate approval process, described later.
Site Selection
Selection and approval of the construction sitetakes place while the PID is under development.Site selection occurs in two phases. In phase 1,the tribe, by tribal resolution, provides severalsites for the proposed new construction. Each ofthe sites is evaluated by IHS as to size, terrain,availability of utilities and access, and ease of con-struction. After the surveys of proposed construc-tion sites have been completed, the sites areranked in order of preference. If the planned fa-cility is approved, an in-depth analysis of the firstchoice construction site is done, including soil bor-ings and the estimates of costs of site development(78).
When site selection is approved, the project costis estimated. This was the responsibility of DHHS’SOffice of Facilities Engineering until 1982, whena new cost estimating system was adopted andIHS began to prepare estimates on a case-by-casebasis; but either IHS or the Office of FacilitiesEngineering may prepare cost estimates for pro-posed projects. This budgeting system relies on:1) modifying hospital or health center gross squarefoot values for changes in costs over time andlocation; 2) addition of special program costs tothe base budget; and 3) monitoring costs throughthe design and construction phases to keep themwithin the established budget. Hospital and healthcenter costs are categorized into five major com-ponents (78):
1.
2.
3.
4.
5.
Inflation allowance: the estimated buildingcost is inflated to the expected mid-point inthe construction schedule.Base building: a gross square foot value thatincludes structural, architectural, electrical,and mechanical systems costs (solar and ma-terials handling systems are excluded).Site work: the site work value is obtainedby using the gross square foot value or, whensite information is available, by pricing ma-jor site work items based on anticipatedquantities.Fixed equipment: gross square foot valuesfor fixed equipment are used.Special program systems; solar systems, ma-terials handling, and lawn sprinkler systemsmust be estimated and added if they are partof the proposed facility.
Project cost estimates are reviewed by IHS,HRSA, and PHS to arrive at the estimate that willbe included in the budget request to Congress.There have been and continue to be differencesin the cost estimates supported by the three levelsof DHHS, in particular relative to the use ofphased funding and to PHS’s allowances for cer-tain types of equipment, which IHS views as in-sufficient. IHS must, however, comply with PHSpolicies in these matters (78).
Finally, IHS prepares a budget proposal thatmust be approved by HRSA, PHS, DHHS, andthe Office of Management and Budget (OMB). Ifa project is not included in the IHS facility pro-gram’s budget request or if it is not submitted toCongress, the project can be submitted for reeval-

206 • Indian Health Care—
uation during the next application of the prioritysystem. However, if a project is proposed for con-gressional appropriation and is not funded, it isplaced automatically in Group B of the facilityconstruction priority list. If funds are appropri-ated for a project by Congress, DHHS apportionsthe funds to IHS and steps toward actual construc-tion begin.
Facility construction projects on the priority listare funded in phases by direct congressional lineappropriations. Congress usually appropriatesfunds for design and planning in 1 fiscal year,phase I construction the following year, and thenphase II construction including equipment coststo complete the facility. Funds for each subsequentphase generally are not appropriated until thepreceding phase has been completed or is near-ing completion. Consequently, in any particularset of annual appropriations, it may appear thatthe priority list system is not being followed, whenin fact it is.
Facility Maintenance, Modernization,and Repairs
Funds for the maintenance and repair of IHSfacilities, modernization projects (including thebacklog of essential maintenance and repair proj-ects, known as BEMAR), and energy conserva-tion retrofit projects are specified in separate linesof the IHS health facilities appropriation.
Maintenance and Repair
Although these services are not within the pur-view of the facilities program proper, a briefdescription is provided. Each area office is allo-cated a specific amount for maintenance and re-pair based on an IHS-modified version of whatis called the “University of Oklahoma methodol-ogy. ” Approximately 60 percent of these fundsare spent for day-to-day maintenance items, e.g.,in-house maintenance and repair projects and con-tractual services (boilers, elevators, generators,etc.). The remaining 40 percent are used for spe-cial maintenance and repair and BEMAR projects,the priority of which is the responsibility of eacharea office. Those special projects not fundedwithin the maintenance and repair projects budgetcan be requested by the area office as a special
maintenance and repair project under BEMAR(funding for which is discussed below). The fundsalso may be used to replace or upgrade equip-ment, e.g., boilers, heating and air-conditioningequipment, and air handlers in IHS facilities. The1985 allocation for maintenance and repair proj-ects was $8.6 million and the 1986 budget was ex-pected to increase to around $8.7 million.
Additional funding for certain maintenance andrepair projects can be provided from Medicareand Medicaid collections, which are generated bybilling those programs for services provided totheir Indian beneficiaries in IHS facilities. Suchcollections must be used to correct deficienciescited by JCAH and to meet Medicare conditionsof participation, e.g., staffing levels (by hiringtemporary personnel) and life-safety code defi-ciencies. Each facility prepares an annual plan forcorrection of deficiencies and submits it to IHSheadquarters. The plans are approved and/ormodified and returned to the area office. As a mat-ter of policy, which would have been mandatedby the vetoed 1984 amendments to the IndianHealth Care Improvement Act, the Medicare andMedicaid reimbursements collected in an IHS areashould be available for use in that area. The areaoffice has discretion in further distributing fundsto the facilities in its jurisdiction, based on an ap-proved annual plan. In fiscal year 1984, nearly$27 million was collected from all IHS areas. Atone point, there was an estimated unobligated bal-ance of $10 million in Medicare and Medicaid col-lections from 1984. According to IHS headquar-ters, such balances result from the fact thatcollection cycles may require up to 2 years to com-plete, from billing the intermediary, to receivingthe funds at IHS and making final decisions re-garding their distribution (122).
Modernization and Repair
The health facilities program is responsible forthe modernization and repair of the facilities itbuilds. This includes providing construction fundsfor current projects and those on the BEMAR list,as well as funds needed for energy conservationretrofit projects.
As of June 1984, there was an estimated back-log of $98 million in IHS modernization and re-pair projects (174). This included $65 million for

Ch. 5—The Indian Health Service ● 207
BEMAR projects. The other projects resulted fromdeficiencies in such areas as fire, life, and safetycodes; environmental quality; requirements toprovide access for handicapped individuals; andenergy management and installed equipment (e.g.,boilers). Backlog project information derives fromarea office totals of the annual facilities deficiencysurvey. The survey supports an automated datasystem, updated annually, which maintains an in-ventory and condition evaluation of IHS prop-erty, estimated facility repair costs, and life ex-pectancies of all real and installed equipment.Every fifth year, data are collected for the “deeplook” facility deficiency survey. Approval ofBEMAR projects is based on this information.
Area offices are responsible for ranking theirBEMAR projects in order of priority, and a pri-ority list combining all 12 area lists is assembledat IHS headquarters. This list is based on a scor-ing system that assigns points for deficienciesinvolving life-support systems, life-safety regula-tions, facility accreditation, and emergency re-pairs. IHS may or may not further revise its pri-ority list depending on the total BEMAR budget.For example, IHS’s initial BEMAR budget requestfor 1985 amounted to $20 million; PHS reducedthis request to $8 million, a cut that required IHSto develop a new priority list. The budget wascut again to $2.1 million to accommodate theOMB allowance, leaving funds for only six newprojects. The projects that ultimately were fundedwere chosen from IHS priority lists in keepingwith a policy decision to favor inpatient facilities.Similarly, the five projects to be funded in fiscalyear 1986 from a budget of $2.45 million wereselected because of a subjective, though informed,decision to favor emergency repairs (27).
In order to better ensure the equitable alloca-tion of funds and to reduce the number of projectson the current BEMAR list, IHS has formed a re-pair and improvement project prioritization com-mittee comprised of representatives from eacharea office. The objective of this committee is toeliminate the estimated $98 million backlog(BEMAR) in 5 years beginning in 1987.
According to congressional mandate in theEnergy Policy and Conservation Act of 1975(Public Law 94-163), as modified by Presidential
order*, by 1985 all existing Federal facilities mustreduce their energy usage by 20 percent from thebase period, October 1974 to September 1975. Allnew Federal facilities must use 45 percent lessenergy than existing facilities did during the baseperiod. In 1982, IHS was appropriated $192,000to conduct energy conservation retrofit studies.As a result of these studies, IHS compiled a listof 27 projects complete with project descriptionsand estimated costs. IHS’s preliminary budget re-quest for fiscal year 1986 included these projectsestimated to cost $4.6 million. To date, however,none of the projects has been included in the OMBallowance.
Sanitation Facilities
The Indian Sanitation Facilities Act of 1959(Public Law 86-121) provided for the supply ofwater and waste disposal facilities to AmericanIndian homes, lands, and communities. Environ-mental health funds for IHS are split between theIHS sanitation budget (in the preventive healthservices allocation) and the IHS facilities construc-tion appropriation.
Funding in the preventive health services allo-cation is primarily service-oriented, providing per-sonnel, such as sanitarians, environmental healthtechnicians, injury control specialists, sanitaryengineers, and engineering technicians who pro-vide the technical services necessary to constructand maintain sanitation facilities. The IHS envi-ronmental health program funded 428 staff posi-tions in fiscal year 1985, when the allocation was$20.2 million.
The IHS facilities construction program, on theother hand, funds the construction of sanitationfacilities. For the first 15 years of the sanitationfacilities program, the main thrust was to serveexisting homes; but congressional appropriationschanged the bias toward providing facilities fornew homes, usually sponsored by either HUD,BIA’s housing improvement program, or by in-dividual tribes. The relationship between the threeFederal agencies—IHS, HUD, and BIA—wasestablished in a 1976 agreement. In 1982, this
‘Executive Order 12003, Energy Policy and Conservation, FR Doc77-21414, July 20, 1977.

208 ● Indian Health Care
agreement was modified at the suggestion of OMBso that HUD-sponsored Indian housing projectswould receive HUD funds for sanitation facilities.In 1986, for example, IHS anticipates that approx-imately $24 million in funding authority will berequired from HUD to provide sanitation facil-ities for the 2,500 HUD-sponsored housing unitsexpected to be allocated.
In general, BIA’s housing improvement projectsreceive first IHS funding priority. In fiscal year1986, IHS’s preliminary budget request providedfor $8 million for the construction of facilities for1,000 BIA project homes. The remaining fundswould be allocated to other new Indian housingprojects on the basis of greatest need and “firstcome, first serve. ” IHS, in its fiscal year 1986 pre-liminary budget request, anticipated the need foran additional $15 million to fund sanitation fa-cility construction for 1,900 tribally sponsoredhousing projects.
The need for sanitation facility construction forexisting homes has been estimated at $520 mil-lion for over 22,000 existing homes that havenever received first service sanitation facilities(60). This information is based on the sanitationfacilities’ unmet needs data system, which collectsdata annually. For fiscal year 1986, IHS requested$29 million to provide services for 3,800 existinghomes. The DHHS allowance for 1986 providedconstruction funds for 300 BIA project homes (at$2.3 million) and 350 tribally sponsored homes(at $2.7 million). Funds for existing homes werenot provided.
Conclusions
The IHS facilities construction program hasbeen active since 1970 in building 14 hospitals,20 health centers, and 700 units of staff quarters.It also has completed facility modernizations andrepairs, as well as sanitation projects in coopera-tion with HUD and BIA, Since 1980, a relativelydetailed system for setting priorities among facilityconstruction proposals has been applied to de-velop the annual priority lists that are submittedto Congress for appropriations.
IHS facility planning guidelines specify criteriaand standards to determine facility size and rangeof services. It should be noted, however, that
planning for individual facilities does not repre-sent health system planning based on an assess-ment of health problems, service needs, and uti-lization patterns throughout IHS area or overallservice populations. The service delivery and fa-cilities construction components of IHS, fundedthrough two separate appropriations, have neverbeen closely integrated. For this reason, questionshave been raised as to whether IHS facilities havebeen located where they can serve the largest num-bers of eligible Indians in the most cost-effectiveway. Tribes have been very active in promotingtheir own facility construction projects, becausethey have found that new facilities bring withthem increased staffing and other resources (staff-ing that is considerably more generous than levelsassigned to existing facilities), and thus are an ef-fective means of securing funding increases be-yond what would be expected under the IHS pro-gram continuity budget approach.
The Administration has called for eliminationof the IHS facilities construction program, includ-ing the sanitation facilities component, in itsbudget proposals for fiscal years 1985, 1986, and1987. In spite of this clear Administration direc-tion, Congress has continued to fund some proj-ects such as the replacement hospitals at Rosebud,South Dakota, and Kanakanak, Alaska. Butwhether Congress will continue to find IHS fa-cility construction requests compelling, in viewof the severely constrained budget climate, can-not be predicted.
If IHS’s mission is to raise Indian health to thehighest possible level, given present budget con-straints, any funds that Congress may appropri-ate for facilities construction and maintenancewould be better spent if facilities planning werecoordinated with planning to meet present andprojected health service needs. The loss of NHSCphysicians and the potential for serious medicalstaffing shortages in the 1990s also indicate a needto reevaluate IHS facility construction plans.
Needs-based services planning might result ina rethinking of the IHS facilities construction pro-gram. For example, resources might be directedtoward construction and renovation of ambula-tory care facilities, rather than hospitals, in areaswhere inpatient care could be purchased at rea-sonable prices from private providers. Or, rather

Ch. 5—The Indian Health Service ● 209
than commit large amounts of money to new fa-cility construction, lesser amounts might fund sub-stantial improvements in existing facilities by com-pleting needed renovations and repairs, providingstaff quarters where required, and purchasing es-sential medical equipment. With limited prospectsof budget growth for the immediate future and- —a likely shortage of physicians, IHS might choose
facilities rather than undertake new construction.Finally, because there is general agreement amongpublic health professionals that safe water andadequate sanitation are essential to maintaininghealth, IHS could request funds to continue itssanitation projects, which will not be undertakenby any other Federal, State, or local agency, in-stead of constructing new hospitals and clinics.
to support and maintain its existing network of

Chapter 6
Selected Issues InIndian Health Care

Contents
PageIntroduction . . . . . . . . . . . . . . . . . . . . . ......213Self-Determination and Tribal Assumption
of Health Services Management .. ....215Introduction . . . . . . . . . . . . . . . . ... ... ..215IHS Implementation of the Self-
Determination Program and theResponse of Indian Tribes ... ... ... ..2l6
Issues Related to Contracting Under theSelf-Determination Act .. .. ... ... ....22l
C o n c l u s i o n s . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 6Resource Allocation in IDS . . . . . . . . . . ....229
I n t r o d u c t i o n . . . . . . . . . . . . . . . . . . . . . . . . . 2 2 9IHS Resource Management in the
1 9 7 0 s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 3 2The IHS Equity Health Care Fund. .....233Resource Allocation in the 1980s . . . . . ..235C o n c l u s i o n s . . . . . . . . . . . . . . . . . . . . . . . . . 2 3 7
The Problem of High-Cost Cases in theIHS Contract Care Program . ........238
I n t r o d u c t i o n . . . . . . . . . . . . . . . . . . . . . . . . 2 3 8Data on IHS High-Cost Cases . ........240Managing High-Cost Cases in the IHS
Contract Care program . ............249C o n c l u s i o n s . . . . . . . . . . . . . . . . . . . . . . . . . 2 5 0
IHS Data Management Issues . . . . . . . . . . ..251
List of TablesTable No. Page6-I. IHS Tribal Health Contract and
Grant Obligations, Fiscal Years1 9 7 5 - 8 4 . . . . . . . . . . . . . . . . . . . . . . . . . , 2 1 7
6-2. IHS Tribal Health Contract andGrant Obligations by TribalActivity, Fiscal Year 1984 ...........218
6-3. IHS 638 Contract Activity by Area,Number, and Dollar Amount ofContract Awards, Fiscal Years1979-85 . . . . . . . . . . . . . . . . . ... ... ..219
Table No. Page6-4.
6-5.
6-6.
6-7.
6-8.
6-9.
6-1o
6-11.
6-12.
6-13.
IHS Budget Allocations by AreaWith Estimated Per CapitaAllocations, Fiscal Year 1985 . ......230IHS Equity Health Care FundAppropriations, Fiscal Years 1981-84,and IHS Special Fund, Fiscal Year1985 . . . . . . . . . . . . . ................234IHS Ranking of Tribal Groups byDeficiency Level for Equity HealthCare Fund Distribution, 1980-85 ....235High-Cost Cases in the IHS ContractCare Program, by Area, Fiscal Year1982 . . . . . . . . . . . . . ................242High-Cost Cases in the IHS ContractCare Program, by Area, Fiscal Year1983 . . . . . . . . . . . . . ................243High-Cost Cases in the IHS ContractCare Program, by Area, Fiscal Year1984 . . . . . . . . . . . . . . . . . . . . . . . . . . . . .243High-Cost Cases in the IHS ContractCare Program, by Cause: All Cases,Fiscal Years 1982, 1983, and 1984 ...244High-Cost Cases in the IHS ContractCare Program by Cause and Area,Fiscal Year 1983. . . . . . . . . . .. .......246Hospitalization Costs to CatastrophicFund at Various Thresholds,Fiscal Year 1983 Data. .. ... ... ... ..248Estimated Total Costs to the lHSCatastrophic Fund at DifferentThresholds, Based on Fiscal Year1983 Experience . . . . . . . . . . . . . . . . . . .249
List of FiguresFigure No. Page6-1.
6-2.
IHS Tribal Health Contract and GrantObligations, Fiscal Years 197744.....217IHS Tribal Health Contract and GrantObligations by Tribal Activity,Fiscal Year 1984.. . . . . . . . . . . . . . . . . . .218

Chapter 6
Selected Issues In Indian Health Care
INTRODUCTION
This chapter presents more detailed discussionsof several issues that have been raised earlier inthis report on Indian health care. The issues wereselected because of their evident importance to In-dian groups in all parts of the country, as ex-pressed in discussions at the Office of Technol-ogy Assessment (OTA) regional meetings, andbecause of their interest to congressional commit-tees in view of possible legislative action. The is-sues that have been selected for special analysisare: Indian Health Service (IHS) implementationof the Indian Self-Determination and EducationAssistance Act of 1975 (Public Law 93-638); meth-ods of resource allocation in IHS; the effects ofhigh-cost cases in the IHS contract care program;and problems of data management in IHS.
From the time of its initiation 10 years ago, theIHS self-determination program (or 638 contractprogram, as it is known) has had a dual purpose—both to deliver health services under the admin-istration of Indian tribal governments, and tostrengthen the tribal governments themselves.the disagreements that have arisen between IHSand the Indian tribes during the program’s imple-mentation. The issues most often raised revolvearound the adequacy of funding for tribally oper-ated IHS programs, IHS contract administrationpolicies (which vary somewhat among IHS areas),and striking a reasonable balance between II-IScontrol and tribal flexibility in program implemen-tation.
Although there have been many frustrations forthe tribes and for IHS, there have been no pro-posals to abandon the self-determination pro-gram. Enthusiasm for self-determination has var-ied among the tribes, but 20 to 30 percent of theIHS clinical services budget now is administeredby tribes under 638 contracts. The adequacy ofIHS funding for self-determination health pro-grams is the major concern. In view of currentand expected future constraints on all Federalspending, including appropriations for IHS, thefunding issue is likely to remain critical. Tribes
may decide not to undertake 638 contracts dueto reasonable fears of the financial risks involved.Because Congress may consider amending theSelf-Determination Act, this assessment reportsviews on the program gathered from discussionswith IHS headquarters, IHS area office staff, andIndian tribal governments and health program ad-ministrators around the country. The IHS self-determination program also was identified forspecial study by the General Accounting Office(GAO), which is due to issue its report in 1986.
IHS’s methods of allocating funds among its 12service areas are a subject of general complaint:whether an area receives a large or small shareof IHS resources, it is likely to be dissatisfied. IHSallocates its annual appropriations by a “histori-cal” or “program continuity” budgeting approach,which means that existing facilities and servicesare supported at their previous year’s level plusa share of budget increases. Contrary to the un-derstanding of many tribes, the resource require-ment methodology that figures in IHS’s equityfund distribution does not play a role in overallbudget allocations. To date, the IHS allocationprocess has not incorporated factors such as pop-ulation size, health status and health service needs,relative geographic isolation, or the availabilityof other IHS or non-IHS services. It is not likelythat IHS now could generate the data necessaryto take all of these factors into account.
The results of IHS’s program continuity budgetapproach can be documented in the unplanned,uneven distribution of funding (on a per capitabasis), facilities and services, and staffing through-out the system. While some IHS areas are rela-tively well-served by IHS direct and contract careprograms, other areas lack certain types of directcare services and are forced by inadequate fund-ing to ration contract care referrals. Areas lack-ing IHS direct services are not compensated withadditional contract care funding. IHS’s ownmethod of identifying tribes with the greatest re-source deficiencies, in order to distribute a court-
213

214 ● Indian Health Care
ordered equity fund, provides ample evidence thateligible Indians in different parts of the countrydo not have equal access to IHS services. Theequity fund distributions since 1981, which havebeen applied to less than 2 percent of IHS ap-propriations each year, have had little impact onIHS area base budgets, Although work has beenunderway recently to develop a resource alloca-tion formula similar to the equity approach thatreflects relative resource needs, the extent to whichsuch a formula will be applied will be a politicaland administrative decision. IHS, which to datehas been unable to apply a systematic approachto the cost-effective and equitable distribution ofprogram increases, may in the near future be facedwith the more difficult task of distributing budgetreductions.
The congressional request for this assessmentspecifically asked for an analysis of the effects ofhigh-cost cases on the IHS contract care program.For several years, there has been consensus amongtribes, IHS, and Congress that the provision ofcontract care, which is intended to supplementservices available from the IHS direct care sys-tem, is being seriously disrupted by the very highcosts of a few emergency cases. Because of limitedfunding, IHS contract care programs operate un-der various rationing techniques, including eligi-bility requirements more restrictive than for di-rect care, a medical priority system that authorizescare for emergency and life-threatening conditionsat the expense of less urgent services, and the re-quired first use of non-IHS alternate providers andpayers. The need to ration contract care servicesindicates that contract care funding is not ade-quate to meet expressed demand. It is not surpris-ing, then, that a few high-cost cases can havesevere negative effects on already constrainedbudgets. Some IHS areas have established area-level high-cost case contingency funds to helpservice units manage their contract care programs.
When Congress addressed the problem of IHShigh-cost cases in the 1984 Indian Health Improve-ment Act (vetoed in October 1984), it found thatavailable information did not indicate whether theproposed $12 million catastrophic health emer-gency fund would be adequate to relieve the sit-uation. For this reason, OTA made particularefforts to develop information on the subject;
however, the inability to obtain reliable, consist-ent data remained an obstacle to the analysis. Ex-isting IHS data systems did not provide neededdata items (e.g., complete costs of services in di-rect and contract care programs); and a specialIHS data collection effort was informal and in-complete. Data on the causes of high-cost caseswere not adequate to determine if IHS experiencesan unusually high incidence of such conditions.The IHS population at risk for high-cost casescould not be defined with sufficient detail to meritconsideration of options such as private rein-surance.
It was concluded, therefore, that the problemcould be addressed as a budget management prob-lem. The proposed revolving fund would be a rea-sonable way to provide temporary budget relief,although it would not benefit all IHS areas equallyunless the threshold were adjusted to reflect rela-tive costs among the areas. Work with availableIHS cost data suggested that the $12 million con-tingency fund would have been adequate to coverhigh-cost cases in 1983, but given medical cost in-flation, it probably would not be adequate now.
The last issue in this chapter deals with the qual-ity and availability of usable patient care and pro-gram management data in the IHS system. OTAdid not attempt to perform a management evalu-ation of IHS in general or of its data systems inparticular. In working with a wide range of IHSoffices and staff over the course of the assessment,however, some general observations about datasystems became apparent. First, IHS operates alarge number of uncoordinated data systems thatare not uniform among IHS areas, and which,therefore, cannot be easily aggregated to providenational program data. The systems depend ona mix of automated and manual support systems,which add to the problems of incompatibility.Second, data from most 638 contract programshave not been included in IHS data systems. Thus,many tables in this report include footnotes in-dicating the absence of data from 638 contractors.Although IHS issued a memorandum late in 1985to require minimum data reporting from 638 pro-grams, the effects of this policy change are notyet apparent. Third, cost data are particularly dif-ficult to obtain from existing IHS data systems,There are systems that monitor IHS disbursements

Ch. 6—Selected Issues In Indian Health Care . 215
for contract care, but these costs cannot be com- apparent. For several years, IHS has been plan-pared with costs of delivering the same services ning a new, comprehensive Resource and Patientin IHS direct care facilities, so decisions about Management System that may or may not resolvewhether a service would be provided more cost- some of these data problems; but it will requireeffectively by IHS or under contract cannot be national program leadership, funding, and timemade. for this new system to become a reality.
In many aspects of IHS operations, the inade-quacy of program management information is
SELF-DETERMINATION AND TRIBAL ASSUMPTION OFHEALTH SERVICES MANAGEMENT
Introduction
The Indian Self-Determination and EducationAssistance Act of 1975 (Public Law 93-638) of-fered Indian tribes the opportunity to assumemanagement of programs operated for their ben-efit by the Bureau of Indian Affairs (BIA) in theU.S. Department of the Interior and by IHS inthe U.S. Department of Health and Human Serv-ices (DHHS).
The Self-Determination Act (also known as the638 law) has been implemented separately by BIAand IHS according to their own policies and reg-ulations. IHS, BIA, and Indian tribes now havehad 10 years’ experience with self-determination.In IHS, self-determination is primarily a contractprogram, with decentralized administration throughthe 12 IHS area offices. There is no self-deter-mination program office at IHS headquarters, al-though there is an office that coordinates liaisonbetween IHS and tribal self-determination con-tractors. Officially, IHS has taken a neutral stancein encouraging or discouraging tribes from enter-ing into self-determination contracts. The IHS po-sition is that tribes exercise their rights under self-determination either by deciding or declining toassume management of health service programs(42 CFR Subpart 1, 36.201-36.202).
The responses of Indian tribes and tribal orga-nizations to the opportunities of self-determina-tion or 638 contracting have varied. While someIndian groups have worked enthusiastically totake over management of major components oftheir health care systems, other groups have beenreluctant to participate, perhaps because they are
satisfied to let IHS manage their services or be-cause they fear self-determination will lead to ter-mination of the Federal responsibility for Indianhealth. Differences in the numbers and types of638 contracts managed by tribes in the 12 IHSareas, described later in this section, illustrate thevariability of tribal responses. Given this lack ofunanimous support for 638 contracting among In-dian tribes, IHS has preferred not to become astrong advocate of self-determination.
Self-determination has been the subject of con-siderable interest during its 10-year history. It wasa major topic of discussion at the four regionalmeetings conducted by OTA to obtain tribal in-put to this study. Many tribal representatives ex-pressed immediate concerns and frustrations withthe 638 contract application process and with IHSmonitoring of contracts. In spite of these difficul-ties, however, there was no apparent desire toeliminate the program; on the contrary, therewere many suggestions on how self-determinationcould be made more attractive to tribes. GAO iscompleting a study of the IHS 638 contract proc-ess, based on detailed case studies in several IHSareas, which should be available in spring 1986.Congress may address some of the problems asso-ciated with self-determination contracting in fu-ture amendments to the law.
This section presents OTA’s findings on the IHSself-determination program based on interviews,comments, and materials obtained during the re-gional meetings and related visits with tribes,tribal 638 contractors, and IHS headquarters andarea staff. Following a background discussion ofIHS implementation activities and a survey of

216 ● Indian Health Care
tribal contracts by IHS area, the discussion willfocus on issues related to self-determination con-tracts with IHS.
IHS policies and regulations for implementingits self-determination program are an issue inthemselves. The law specifies that self-determi-nation contracts should be administered differ-ently from Federal procurement contracts, becausea 638 contract represents a transfer of funds andmanagement responsibility, not a purchase ofservices from an outside provider. Rather than theusual arm’s-length relationship between the Gov-ernment and the contractor, self-determination re-quires IHS to work with prospective tribal con-tractors in developing their applications and toprovide technical assistance as necessary. Self-determination contracting requires unique policiesand modified contract regulations, which may ex-plain some of the difficulties experienced both bytribal contractors and by IHS area staff. Also, be-cause of IHS’s decentralized administration of theprogram, variations have developed in how differ-ent IHS area offices implement and monitor 638contracts.
Complaints about particular problems with 638contract development and administration, whichmay be unavoidable to some extent, reflect largerissues of project control between IHS and tribalcontractors. IHS contends that 638 contractedactivities are extensions of IHS itself, and there-fore IHS should retain responsibility and control.Tribes argue that they are assuming both respon-sibilities and financial risks and therefore shouldbe allowed more flexibility in managing 638 ac-tivities.
IHS and Indian tribes agree that the major ob-stacle to increased self-determination contractingis inadequate funding. The Self-Determination Actstates that a tribal contractor should receive fund-ing equivalent to what IHS itself spent on pro-viding the services in question. IHS’s estimate ofthis amount (referred to as the “Secretarial levelof funding”), however, does not always satisfytribal contractors, who argue that they have legiti-mate operating costs that are not included in theIHS estimate. “Indirect costs” is the term mostoften heard in this debate, and malpractice insur-ance costs are the most frequently cited example.
When the Self-Determination Act became lawin 1975, it was anticipated that tribes would beable to operate service programs more efficientlythan IHS, and therefore be able to expand serv-ices or to cover additional operating costs suchas liability insurance. Some of the first 638 con-tracts received additional indirect or adminis-trative overhead costs, and IHS sometimes hasprovided additional support when funding wasavailable; but in recent years, there have been noIHS appropriations for the indirect costs associ-ated with 638 contracts. Many tribal contractorsbelieve that the total contract award, which IHScontends covers both direct and administrativecosts (IHS’s total cost of service delivery), is in-adequate and, in effect, forces the contractor toreduce services in order to cover essential admin-istrative costs.
Another issue concerns IHS area office staff astribal contractors assume responsibility for moreIHS services. When a tribe contracts to operatean IHS facility or service unit, it may simply trans-fer most of the IHS staff to tribal employment.Some tribal contractors believe, however, that astheir own management capabilities grow, IHSarea office staff should be reduced and part of thesavings in personnel costs earmarked for 638 con-tract administrative expenses and additional serv-ices. IHS responds that area office staff must bemaintained because developing and monitoring638 contracts require as much or more effort thanwas needed when IHS delivered services directly.Another reason cited by IHS is that tribes mayturn back their self-determination contracts to IHSwith 120 days’ notice (retrocession), and IHS mustbe prepared to resume program management. Thefuture of the IHS self-determination program willdepend to a large extent on how these issues areresolved.
IHS Implementation of the Self-Determination Program and theResponse of Indian Tribes
IHS Program Implementation
The Self-Determination Act and the regulationsthat govern its implementation in IHS state thatgrants or contracts maybe awarded to tribes and

—..— Ch. 6—Selected Issues In lndian Health Care . 217
—
tribal organizations “to carry out any or all of thefunctions, authorities, and responsibilities of theSecretary of Health and Human Services underthe Act of August 5, 1954” (the Transfer Act, asamended) (42 CFR Subpart I 36.201). The use ofcooperative agreements, which are similar togrants, was authorized in 1984 by an amendmentto the law; but no cooperative ‘agreements hadbeen used in IHS as of the end of 1985,
IHS programs implemented pursuant to the1976 Indian Health Care Improvement Act, suchas the Indian health manpower scholarship pro-grams and urban Indian health projects, are notsubject to self-determination contracting becausethey were not among the functions conveyed toDHHS by the Transfer Act. Furthermore, it is theIHS position that the administration and supportresponsibilities of IHS headquarters and areaoffices usually are not contractible, because suchfunctions are difficult to associate with specifictribes (60).
Although IHS regulations provide that tribesmay administer the same types of health programseither by grant or by contract, the grant compo-nent of the IHS self-determination program hasnever been very large. Grants may be awardedto tribes to administer health services, subject toannual renewal. One-year grants are also avail-able to develop tribal management capabilitiessuch as personnel and accounting systems, for fea-sibility studies to help tribes determine whetheror not they should contract a service, and fortribal health planning activities (42 CFR 36 Sub-part G). IHS 638 grants have not exceeded 10 per-cent of annual combined tribal health contract(including Buy Indian contracts) and grant ex-penditures (see table 6-1 and figure 6-l). In fiscalyear 1984, grants for the self-determination pro-gram represented only $16.5 million, or 8.5 per-cent, of the total $194 million obligation.
Contracts have been the predominant meansof transferring IHS health programs to tribal man-agement. In some IHS areas, such as Nashvilleand California, tribal organizations contracted todeliver health services well before the Self-Deter-mination Act became law. Some contracts thatpredated self-determination, such as those exe-cuted under the Buy Indian Act of 1910, havesince been converted to 638 contracts. Most tribes
Table 6-1 .—IHS Tribal Health Contract and GrantObligations, Fiscal Years 1975-84a
(millions of dollars)
Fiscal year Total Contracts Grants
1984 . . . . . . . . . . . . . . $194.0 $177.5 $16.51983 . . . . . . . . . . . . . 157.7 143.1 14.61982 . . . . . . . . . . . . . 141.1 126.5 14.61981 . . . . . . . ., . . . . 142.8 130.7 12.11980 . . . . . . . . . . . . 121.91979 , , . . ., . . 74.01978 ., . . . . . . . . . . . 70,11977 ., . . . . . . 57.91976 . . . . . . . . . . . . 32.61975 . . ., . . . . . . . . . 17.4aR~p~~t ~Om ~lete ~~ of Feb I I gas Contracts In c l ud e both 638 and BU Y Indian
contracts Grant obligations are shown separately for the first time In 1981
SOURCE U S Department of Health and Human Serv!ces, Publlc Health Sew-Ice, Health Resources and Serwces Adminlstrat!on, Indian Health Serv.ice, Chart Ser/es Book April 1985, publtshed as table 52 From TRAISContracts Data Base, Management Systems Development Branch IHS
Figure 6-l.— IHS Tribal Health Contract andGrant Obligations, Fiscal Years 1977-84a
1977
Fiscal year
afleport complete as of Feb 1, 1985 Contracts include both 638 and Buy Indiancontracts Grant obligations are shown separately for the first time In 1981
SOURCE U S Department of Health and Human Servtces Publlc Health Serv.Ice, Health Resources and Serwces Adminlstratlon, Indian Health Sew-ice, Chart Ser/es Bookr April 1985, publ!shed as f!gu re 52, from TRAISContracts Data Base, Management Systems Development Branch
seem to prefer contracts to grants, possibly be-cause they are familiar with the long-standing BuyIndian contract program. In addition, grants maybe perceived as reflecting the relationship of a su-perior entity, in this case the Federal Governmentthrough IHS, to a lesser one, the Indian tribe;whereas a contractual relationship is often seenas an agreement between equally responsible par-ties and more appropriate to a government-to-government transaction (87).
As noted earlier, the intent of the Self-Deter-mination Act is for IHS to facilitate 638 contract-ing. The law directs the Federal Government to

218 ● Indian Health Care
assist tribal governments in developing necessarymanagement capabilities; to provide technicalassistance to tribes in preparing contract pro-posals; and to enter into all contracts that are pro-posed unless specific conditions for denial can bedocumented (e.g., that services would not be pro-vided in a satisfactory manner, or that trust re-sources would not be adequately protected) (42U.S. C. 2001). A tribal 638 contractor with causemay return a project to IHS management with 120days’ notice. IHS, on the other hand, may not re-scind a 638 contract without first working withthe tribe to correct deficiencies and allowing fortribal appeals, except where there is an immedi-ate threat to life or safety (42 CFR 36.231-36.234).
Table 6-1 shows that tribal health contract andgrant activities increased from $17.4 million in fis-cal year 1975 to $142.8 million in 1981 and $194million in 1984 (tables 6-1 and 6-2 combine obli-gations for IHS self-determination and Buy Indiancontracts). In fiscal year 1984, total IHS obliga-tions to tribes for 638 contracts, Buy Indian con-tracts, and 638 grants ($194 million) amountedto 30 percent of the IHS clinical services budgetof $645.5 million. As shown in table 6-2 and fig-ure 6-2, the primary use of 638 and Buy Indiancontract funds in fiscal year 1984 was health serv-ices delivery ($111.4 million, or about 63 percentof total contract obligations of $177.5 million).
Table 6-2.—IHS Tribal Health Contract and GrantObligations by Tribal Activity, Fiscal Year 1984a
Tribal activity
Contract and grant total ... ... ... ... ... .. .$193,953,186
Contracts total . . . . . . . . . . . . . . . . . . . . . . . . . . 177,479,579
Health department management . . . . . . . . 5,472,660Health services delivery . . . . . . . . . . . . . . . . 111,352,779Training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2,984,009Other contracts . . . . . . . . . . . . . . . . . . . . . . . 40,895,626b
Indirect costs . . . . . . . . . . . . . . . . . . . . . . . . . 16,774,505C
GrantsProjects. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16,455,589d
aRepo~ complete as Of Feb 1, 1985, Contracts include both 638 and BUY Ind!ancontracts.
bother contracts includes $36,538,512 that has been reported but not assignedto a specific tribal activity as defined in this table
clndirect costs are shown separately and are not included In each tribal contractactivity
dThe grants total includes scholarships, applied training and development, andstudy grants
SOURCE U S Department of Health and Human Serwces, Public Health Serv.Ice, Health Resources and Services Admlnlstration, Indian Health Serv.ice, Clrarf Series Book, April 1985, published as table 5.3, from TRAISContracts Data Base, Management Systems Development Branch, IHS,and PHS Grants Data System.
Figure 6-2.— IHS Tribal Health Contract and GrantObligations by Tribal Activity, Fiscal Year 1984a
services contracts costs (all department -
delivery activities) c managementaRepOrf complete as of Feb. 1, ISMM. Contracts include both 638 and BUY Indian
contracts.bother contracts includes $36,538,512 which has been reported but not assigned
to a specific tribal activity as defined in this figure.clndirect costs are shown separately and are not included in each tribal contract
activity.dThe grants total includes scholarships, applied trainin9 and development, and
study grants.
SOURCE: U.S. Department of Health and Human Services, Public Health Serv-ice, Health Resources and Services Administration, Indian Health Serv.ice, C~arf Series Book, April 1985, published as figure 5-3, from TRAISContracts Data Base, Management Systems Development Branch, IHSand PHS Grants Data System
Indirect costs amounted to 9.5 percent of totalcontract awards.
Table 6-3 presents data for self-determinationcontracts only, by IHS area, obtained from IHSby special request. These data indicate that 638contracts represented about 85 percent ($152.4million) of the $177.5 million in 1984 IHS con-tract obligations, while Buy Indian contracts rep-resented 15 percent (215).
The data in table 6-3 also suggest that in fiscalyear 1985, Indian tribes administered more than$141 million under 638 contracts. The 1985 IHSclinical services budget (excluding funds for IHSheadquarters operations in Rockville and dataprocessing in Albuquerque) was $637 million, Ofthis amount, $164 million (26 percent) was spenton IHS contract care and $473 million (74 per-cent) was spent on IHS direct services. There aresome inconsistencies among IHS areas in how 638contract funds are accounted to direct care or con-tract care budget components. However, if the$141 million in 638 contracts (excluding Buy In-dian contracts and 638 grants) was associated pri-marily with tribal management of direct carerather than contract care services, it would rep-resent 30 percent of the direct care budget and 22

Ch. 6—Selected Issues In Indian Health Care ● 219—
Table 6-3.—IHS 638 Contract Activity by Area, Number, and Dollar Amount of Contract Awards,Fiscal Years 1979.85a
Fiscal year
Areas 1979 1980 1981 1982 1983 1984 1985
Aberdeen . . . . . . . . . . . . . $ 1,897,5751
Alaska. . . . . . . . . . . . . . . . . 10,959,83912
Albuquerque . . . . . . . . . . . 1,083,8188
Bemidji . . . . . . . . . . . . . . . . 988,50112
Billings . . . . . . . . . . . . . . . . —
California . . . . . . . . . . . . . . 232,1105
Nashville . . . . . . . . . . . . . . 2,949,13116
Navajo . . . . . . . . . . . . . . . . —
Oklahoma. . . . . . . . . . . . . . 2,215,89921
Phoenix . . . . . . . . . . . . . . . 1,908,71610
Portland . . . . . . . . . . . . . . . 411,841
Tucson . . . . . . . . . . . . . . . . 967,51?10
3522,654,392
2,562,05721
11,729,11987
672,0723
6,539,69626
14,659,01623——
4,383,35124
5,218,66137
8,707,34174
1,937,12211
$ 2,708,968 $ 6,680,295 $ 11,048,649 $ 12,153,028 $ 13,284,084 $ 13,038,422
5,875,00322
2,292,58216
9,452,36451
469,6602
1,371,5379
6,306,96315—
3,267,57819
3,204,99424
6,904,59857
1,762,16311
3920,913,797
351,919,462
1417,557,043
972,681,906
167,645,647
2612,753,153
1530,995
18,803,967
394,767,554
419,513,176
711,619,297
13
7229,859,667
312,715,689
2019,353,373
964,063,432
2516,893,751
3614,840,895
2065,168
18,124,916
476,789,882
589,697,788
981,794,369
6
4338,703,156
222,763,060
2121,729,906
864,057,974
2514,561,825
3920,235,864
19101,771
113,316,233
468,611,486
6112,646,744
852,402,507
9
4026,341,939
192,252,020
2017,310,251
524,916,113
2320,784,286
2420,212,334
16280,148
112,882,942
576,923,748
5213,740,282
752,394,639
5
IHS total . . . . . . . . . . . . . $23,614,947 $43,616,410 $85,743,122 $99,254,646 $126,351,958 $152,414,610 $141,077,124104 234 374 407 510 457 384
aThe “umber~ of contracts are total ~~ntract~ a c t i v e durln~ the fl~~al Year, ~~mbined new and renewal c e n t racts Dollar a m o u n t s a r e totai aWarcIs i ncludl ng f u n d ! ng
modif!cat!ons and !ndlrect costs
SOURCE U S Department of Health and Human Services, Public Health Serwce, Health Resources and Serwces Admlnistratlon, Indian Health Service, TRAIS datasystem, as reported from Albuquerque Data Center to IHS Off Ice of Tribal Activities, Division of Indian Resource Liaison, summary sheets received 11/12/85
percent of the total $637 million IHS clinical serv-ices budget.
In spite of contract regulations and proceduresthat have been modified in favor of tribes, com-ments from tribal organizations and IHS staffaround the country suggest that some tribes be-lieve the risks and problems of self-determinationcontracts outweigh the advantages. Some of theseproblems are discussed later in this section.
Tribally Operated Health Programs
The numbers and types of health programs ad-ministered by the tribes under self-determinationvary substantially among IHS areas. The num-bers of 638 contracts by area, with dollar awards,have been summarized in table 6-3. (Detailed listsof 638 contracts active as of March 1985 have beentabulated from IHS sources and displayed bytribe, service unit, State, and IHS area office; theseare available from OTA. )
Some of the more traditional reservation-basedtribes in areas with well-established, comprehen-sive IHS direct care programs (especially, hospi-tals and clinics) have not been active in 638 con-tracting. The Navajo tribe is an example. This isthe largest single tribe served by IHS, with an esti-mated IHS service population of 166,493 in 1985.Although the Navajo tribal government has con-siderable administrative expertise, 638 contract-ing plays virtually no role in health care deliveryfor the Navajo. The tribe manages only one IHS638 contract for the community health nursingprogram. In the Albuquerque area, only 2 of 22health clinics are tribally operated, and the other638 contracts are for specific programs such ascommunity health representatives, alcoholism,otitis media, speech and hearing problems, andmental health. This pattern applies in general tothe Aberdeen, Billings, Phoenix, and Tucson IHSareas (with the exception of the Pascua-Yaquiprepaid plan in the Tucson area).
52-805 0 - 86 - 8

220 ● Indian Health Care
The Oklahoma City IHS area differs somewhatfrom IHS areas identified above, but it is closerto them than to other areas more active in 638contracting. There is an extensive IHS direct caresystem in Oklahoma, and the entire State is des-ignated a contract health services delivery area.There are seven Indian hospitals in the OklahomaIHS area, five operated by IHS and two, the CreekNation hospital at Okemah and the OklahomaChoctaw hospital at Talihina (as of January 1985),operated under 638 contracts. Oklahoma area IHShospitals are larger, newer, and offer a widerrange of inpatient services (including surgery) thanthe typical IHS hospital. The health clinics in theOklahoma City IHS area are predominantly IHSoperated. Many of the Oklahoma tribes manage638 contracts, but most are relatively small con-tracts for specific services.
In contrast to the IHS areas just mentioned, inwhich 638 contracting is relatively unimportantto the overall Indian health care system, are theIHS areas of Alaska, California, Bemidji, andNashville. Each of these areas has a relatively re-cent and unique relationship with IHS.
The approximately 73,000 Alaska Natives areserved by seven hospitals of varying sizes and ca-pabilities, including the IHS medical center at An-chorage. The hospitals at Nome (Norton Sound),Dillingham or Kanakanak (Bristol Bay), and Mt.Edgecumbe (Southeast Alaska, as of January1986) are tribally operated. In addition, theAlaska Native Health Corporations contract un-der 638 to operate substantial components of theIHS system. In fiscal year 1984, the native cor-porations managed about $39 million (38 percent)
of the area’s total clinical services budget of nearly$102 million (see table 6-3 and app. C). Two en-tire service units and a number of facilities (in-cluding 3 of 8 health centers and all 173 villageclinics) are administered by Alaska Natives. De-spite requirements of the 638 contract applicationprocess that pose particular problems in Alaska(discussed below), Alaska Native Health Corpo-rations seem determined to take over managementof their health service systems.
In the California, Bemidji, and Nashville IHSareas, many Indian groups live in small, scatteredbands and rancherias. Tribes in these areas gen-erally do not have reservations and may, at best,
have limited tribal trust land bases. A relativelylarge number of these tribes have had their Fed-eral recognition reinstated only recently. In theseareas, tribally operated 638 programs are an im-portant part of the IHS system.
The California area has no IHS direct care fa-cilities (the Yuma IHS hospital is physically lo-cated in California, but it is administered by thePhoenix area office). IHS services are providedentirely through 638 contracts with the many Cali-fornia tribes, which are grouped into 20 projectsequivalent to service units. The bulk of 638 fund-ing in California goes to tribally operated clinicsand health stations that deliver ambulatory healthservices.
The Bemidji area has two IHS direct care hos-pitals. Half of the area’s health clinics are triballyoperated, and nearly every tribe administers atleast one 638 contract for a specific service suchas community health representatives or substanceabuse. Some tribes also administer comprehen-sive health delivery and sanitation 638 contracts.
IHS historically has not had a major presencein the Eastern United States. The Nashville pro-gram office was separated from the OklahomaCity area office in 1971 and now serves 16 smalltribes dispersed throughout the eastern one-thirdof the country. Several of these tribes have re-gained Federal recognition since 1980. Because oflimited IHS staff and the geographic dispersionof tribes in the Nashville area, most IHS servicesare delivered through comprehensive 638 con-tracts. The contracts range in scope from thetribally operated Choctaw hospital in Philadel-phia, Mississippi, to limited health referralservices.
The Portland IHS area is similar to the Cali-fornia, Bemidji, and Nashville areas in that it ischaracterized (with a few exceptions) by relativelysmall tribes with limited land bases. Several tribesin the Portland area have regained Federal rec-ognition recently. There are no hospitals in thePortland area operated either by IHS or by tribes.Four of 16 health centers and 13 of 21 health sta-tions in the Portland area are tribally operated.Unlike tribes in the California, Bemidji, and Nash-ville areas, Portland area tribes are less likely toadminister comprehensive health service 638 con-tracts. Most of the 638 contracts are for specific

Ch. 6—Selected Issues In Indian Health Care ● 221— —.
health services such as community health nurs-ing, community health representatives, and sub-stance abuse. The two tribes that contract under638 to administer their own contract care pro-grams do so in compliance with Portland area of-fice guidelines.
It is c]ear from reviewing 638 contract activi-ties in the 12 IHS areas that responses to the self-determination program have varied among tribesaround the country. Differences are apparent bothin the amounts (number of contracts, doIlarawards) and in the types of health services thatare contracted by the tribes, Questions might beraised over how many of the 638 contracts rep-resent actual takeovers of health program man-agement and how many are essentially transfersof administrative responsibility. Some of the prob-lems and issues involved in 638 contracting thatmay affect a tribe’s decision to contract or not tocontract are discussed below.
Issues Related to Contracting Underthe Self= Determination Act
A central issue in this analysis concerns IHS’simplementation of the Indian Self-DeterminationAct in relation to the intent of the law as passedby Congress. Congress sought to support tribalgovernments and to encourage more active par-ticipation by Indian tribes and tribal organizationsin the delivery of IHS services. Although Con-gress and many American Indian groups view self-determination as an opportunity for Indian tribesto exercise greater influence over services providedto them, IHS appears to focus primarily on thecontract administration aspects of the self-deter-mination program. These different approachesmay account for some of the difficulties that havearisen between IHS and Indian groups in carry-ing out the provisions of the self-determinationlegislation.
The following discussion deals with issues re-lated to self-determination as implemented byIHS. The specific areas of discussion include IHSimplementation policies and procedures at IHSheadquarters and area office levels; the adequacyof funding for 638 contracts; and tribal experi-ences in administering 638 contracts.
IHS Policies and Procedures for Implementing638 Contracts
In the view of some participants, IHS has notshown a clear commitment to achieving Indianself-determination. Perhaps the reason that IHShas not been aggressive in implementing the pro-gram is because some tribes continue to suspectthat self-determination may be a means of reduc-ing Federal responsibility for Indian health. IHSself-determination regulations include the follow-ing statement (42 CFR Subpart I 36.201 (a)(4)):
It is the policy of the Secretary to continuallyencourage Indian tribes to become increasinglyknowledgeable about Indian Health Service pro-grams and the opportunities Indian tribes haveregarding them; however, it is the policy of theIndian Health Service to leave to Indian tribesthe initiative in making requests for contracts andto regard self-determination as including the de-cision of an Indian tribe not to request contracts.
IHS has been criticized by some Indian organiza-tions for not moving as quickly as it might haveto support tribal interests in 638 contracting. Un-certainties about IHS headquarters’ policies andthe delegation of administrative responsibility tothe area offices have resulted in variations amongIHS areas, both in 638 contract application pro-cedures and in monitoring contracts awarded tothe tribes.
The 638 Contract Application Process in IHS.—The Self-Determination Act directs IHS to pro-vide technical assistance to tribes in developing638 contract proposals and to approve all suchproposals unless specific grounds for denial canbe documented.
Resolutions of support for a 638 contract pro-posal must be obtained by the prospective con-tractor from all affected tribes (42 CFR SubpartI, 36.206). This requirement may not be a con-cern in areas where a health program serves onlyone tribe, but in areas such as Alaska, wheremany native villages are served under a singleAlaska Native Health Corporation, obtainingresolutions of support from 100 percent of thevillages can be an obstacle. In some instances,Alaska villages have bargained for other unrelatedbenefits by withholding their support for a 638contract proposal (67). A similar situation exists

222 Ž Indian Health Care
in California, where Indian bands are affiliatedwith health consortiums that deliver servicesthrough 638 contracts. A tribe may change its af-filiation apparently at any time, and such changesdisrupt program administration and fundingthroughout the area (9).
Another significant problem in developing a 638contract application, according to tribal organi-zations, is the reluctance or inability of IHS areaoffices to provide adequate cost data on existingIHS operations. Cost data are essential to thetribes in order to develop their financial manage-ment plans for a project; however, IHS does notmaintain an internal cost-accounting system andso cannot provide data in the detail that wouldbe expected by a private organization develop-ing a management contract for a hospital or clinic.When IHS has not been able to identify the costsassociated with a project to the satisfaction of thepotential tribal contractor, disputes have resulted.As will be discussed in relation to 638 funding is-sues, a tribe is entitled to the same level of fund-ing that IHS would have committed to providethe service directly.
IHS Monitoring of Self-Determination Con-tracts.—Once a tribe signs a 638 contract to man-age a particular health service, IHS responsibili-ties for that service shift from direct delivery toprogram monitoring and contract administration.The staffing levels of IHS area offices have notdeclined as direct delivery functions have beentransferred to the tribes because, according toIHS, 638 contracts require substantial monitor-ing. In addition, regulations provide that tribesmay return a contract to IHS responsibility with120 days’ notice. Tribal contractors, on the otherhand, argue that unnecessary personnel in IHSarea offices absorb funds that should be madeavailable for 638 contracts.
The suggestion that 638 contract administra-tion creates special demands on IHS staff is plau-sible, given the differences between 638 contract-ing requirements and other Federal contractingrequirements. In the case of Federal fixed-cost orcost-reimbursement contracts, an arm’s lengthrelationship between the Government and thecontractor is required. The Government may or-der changes in contract scope unilaterally and mayterminate the contract at its convenience, while
the contractor may not. Federal labor laws andequal opportunity provisions also apply to thecontractor. In the case of self-determination con-tracts, however, these requirements are modified:IHS is directed to assist tribes in developing 638contracts; all changes in a 638 contract requirethe consent of the contractor; the Governmentmay reassume management of a 638 contract onlyfor specified reasons, but the contractor may turnback a 638 contract with 120 days’ notice; em-ployees of tribal 638 contractors are not subjectto certain Federal labor laws; and Indian prefer-ence in employment and training supersedes equalopportunity rules. In addition, tribal 638 contrac-tors enjoy exemption from bonding requirements(42 CFR Subpart I, 36.223) and may carry overunspent contract funds to the following year (42CFR Subpart I, 36.236) (187).
IHS regulations for 638 grant and contract ad-ministration were published in November 1975(42 CFR 36 Subparts H and I). Since 1981, IHSheadquarters has provided additional guidance onspecific points in the form of Indian self-deter-mination memoranda. Nonetheless, variationsamong IHS areas appear to be common when itcomes to the application of 638 contracting pol-icies and procedures. IHS decisionmaking on 638applications and contract management questionssometimes is viewed by tribal contractors as arbi-trary and capricious; and tribes have complainedthat the appeals process is not adequate (68).
In some IHS areas, such as Nashville and Cali-fornia, many of the 638 contracts are written forambulatory clinic management and comprehen-sive health service programs. In such cases, it maybe desirable to allow tribal contractors as muchflexibility as possible to operate their programswithin the terms of their contracts. That is the ex-plicit policy of the Nashville IHS area, where IHSstaff also believe there should be routine contractaudits for effective financial monitoring and ac-curate indirect cost determinations (84). In thePortland area, by contrast, individual 638 con-tracts are strictly defined and monitored by IHSarea office personnel from their initiation. IHSstaff in some area offices believe tribes occasion-ally seek to expand services beyond the scope oftheir 638 contracts. For example, contractors mayincur unauthorized costs by hiring additional staff

Ch. 6—Selected Issues In Indian Health Care ● 223
whose services may not be directly related to thecontract (84).
Health Facilities Construction Under 638 Con-tracts.—IHS regulations implementing Public Law93-638 permit tribal construction of health facil-ities under grants or contracts (42 CFR 36 Sub-parts H and I), but facilities construction has notbeen a major component of the 638 program. Per-haps five or six 638 construction grants wereawarded for staff quarters and one clinic before1982 (16), when the Public Health Service (PHS)decided to allow facilities construction by contractonly. This was because construction under a grantmight be interpreted as conferring facility owner-ship (60). The first clinic constructed under a 638contract was built by the Menominee tribe, andbetween 5 and 10 IHS clinics now have been con-structed by tribal contractors. The first hospitalconstructed under a 638 contract was at Red Lake,Minnesota. At the end of 1985, two hospitals werein the planning and construction stages as 638projects: one in Kanakanak (Dillingham), Alaska,and one in Rosebud, South Dakota (16).
The limited amount of facilities constructionthat has been authorized under the self-determi-nation program reflects the opposition of PHS andthe Health Resources and Services Administration(HRSA), the agencies in which IHS operates, toany construction of new Indian health facilities.Concerns have been expressed in HRSA about in-adequate monitoring of 638 facilities constructionand about the difficulties that may arise if a tribalcontractor does not adhere to contract terms re-
garding facility size and service capabilities (117).Finally, tribes may collect a contract managementfee for overseeing 638 construction subcontrac-tors, which is seen by Federal administrators asunearned profit.
The Cost-Reimbursement Contract in the 638Process.—Much of the dissatisfaction that isvoiced by tribal 638 contractors about IHS areaoffice contract administration centers on the con-tract format itself and inconsistencies in the inter-pretation of Federal contracting regulations. Manytribes regard the voucher reimbursement systemthat IHS applies in 638 contract management asunnecessarily time-consuming, inflexible, and re-strictive. The question then arises whether thecost-reimbursement contract is the most suitable
means of transferring responsibility for servicesdelivery from the Federal Government to Indiantribes.
Another type of instrument—the cooperativeagreement—was introduced by the Federal Grantsand Cooperative Agreement Act of 1977 (PublicLaw 95-224). Public Law 95-224 did not apply spe-cifically to the Indian self-determination process,but a technical amendment to Public Law 93-638in 1984 provided that cooperative agreementscould be used, if mutually acceptable to IHS andthe tribes. Tribes in some areas, particularly inthe Southwest, are interested in cooperative agree-ments as a more flexible alternative to standardcontracting. IHS and HRSA officials point out,however, that cooperative agreements are likegrants in that they allow the Government (not thetribes) more discretion than is permitted in a con-tract to modify the products, timeframes, andfunding levels of the project (87). It appears thatthe more discretionary cooperative agreements area sensitive subject, because they may be viewedby some tribes as another step toward termina-tion. A few years ago, BIA proposed to convertits 638 contracts to cooperative agreements, butso many tribes opposed the change that it wasabandoned. Contracts, for all their difficulties, arepreferred by many tribes because they are legallybinding agreements between parties of relativelyequal stature (in the case of 638 contracts, betweenthe Federal Government and tribal governments).IHS has considered the use of cooperative agree-ments but has not as yet adopted a formal policyon the subject, and it is unlikely that any coop-erative agreements will be used by IHS in fiscalyear 1986 (87).
Another instrument that is authorized underseparate legislation (Public Law 86-121), thememorandum of agreement, is unique to IHSenvironmental health and sanitation projects.Memoranda of agreement usually specify theterms of cooperation between IHS and a tribe ortribes in completing sanitation projects. IHS’s gen-eral counsel has ruled that memoranda of agree-ment projects are exempt from the Federal Davis-Bacon union wage scale requirement, and this isan important consideration because tribes oftencannot pay union scale.

224 ● Indian Health Care— — — —
The Adequacy of Funding for 638 Contracts
Currently, there are significant financial disin-centives to 638 contracting: many tribes believethat funding levels set by IHS for 638 contractsare inadequate. Some tribes argue that the costdata on which IHS determines its contract awardsmay be inadequate or incorrect; and tribal con-tractors may not feel confident in judging the ade-quacy of a proposed 638 contract amount, be-cause they cannot obtain sufficiently detailed andreliable cost accounting data from IHS, In addi-tion, 638 contracts are for a fixed amount, andtribal contractors are responsible for actual costsin excess of that amount.
The larger and more comprehensive the healthservice activities managed by 638 contract, thegreater the financial risks to tribal contractors.This situation may explain in part why relativelyfew comprehensive contracts have been negoti-ated and why the majority of tribes prefer to man-age small, limited-service contracts. Specific serv-ice programs also may be more attractive to tribalcontractors because they require less-specializedmanagement expertise, frequently are add-ens toexisting IHS services, and offer employment op-portunities at relatively low financial risk to thetribe.
The financial risk factor is especially acute intribally operated contract care programs, whereunpredictably high-cost cases can make budgetsdifficult to control. The catastrophic health emer-gency fund proposed in recent legislation wouldinclude 638 contract care programs in its cover-age. At present, however, tribes that manage theirown contract health services under 638 contractsmust follow area office regulations in order toqualify for the area’s catastrophic care contin-gency fund, if available (as in Alaska, Portland,and the Oklahoma City IHS areas); make specialprovision for the catastrophic coverage part of the638 contract; aggressively collect third-party pay-ments to supplement IHS funding; or deny con-tract care authorizations for costly emergencyservices.
The most frequently voiced tribal complaintabout funding has to do with administrative orindirect costs. This issue often is raised when thecosts to a tribal 638 contractor of providing a par-
ticular health program exceed the costs attributedto that program by IHS. A number of factors areinvolved in this problem. Tribal 638 contractorsmay have legitimate costs that are not requiredof IHS at the area or service unit level. For ex-ample, central IHS support services (e.g., legaland accounting resources, budget development,procurement and contract administration, special-ized technical assistance, data collection and proc-essing, and facilities planning) are not likely tobe charged to local service programs. Managersof 638 programs may have to purchase theseneeded services from the private sector at addi-tional cost. IHS cannot authorize contractors topurchase facilities if no funds have been appro-priated specifically for that purpose; hence con-tractors may be obliged to lease facility space athigher cost.
Medical malpractice insurance is frequentlycited by the tribes and by IHS as a significantproblem for 638 contractors. Medical profes-sionals employed by the Federal Government arecovered by the Federal Tort Claims Act; but pro-grams operated by the tribes need separate mal-practice insurance for their medical professionals,because Indian tribes have sovereign immunityagainst suit (60). Tribal contractors also have dif-ficulty matching the fringe benefits available toFederal employees, such as life and health insur-ance and retirement plans, because of the cost ofpurchasing those benefits in the private sector.
Although Public Law 93-638 does not specifythat tribal contractors should receive direct andindirect costs, IHS self-determination regulationsdo address the issue. The basic guideline regard-ing 638 contract funding levels is expressed as the“Secretarial level of funding” (25 U.S.C. 450j), andthe IHS regulation states: “The tribal organiza-tion shall be entitled to be funded for direct andindirect costs at a level which is not less thanwould have been provided if the IHS had oper-ated the program or portion thereof during thecontract period” (42 CFR 36.235). Allowable in-direct costs are defined in Federal contract gen-eral provisions, but different interpretations canresult from variations in accounting systems anddefinitions.
No research has been done in IHS to identifythe actual range of 638 contract indirect costs or

to determine what would be reasonable. Althoughsome of the earlier 638 contractors received in-direct costs from IHS through additional appro-priations (as is still the case for BIA 638 contracts),such funding has been reduced or eliminated.Tribes object to the inequities that have resultedfrom this change. As a result, tribal contractorsbelieve they now are expected to cover indirectcosts out of their direct service funds, thus reduc-ing the level of services they can provide, whichis contrary to the intent of the Self-DeterminationAct (134).
A recent example of a dispute involving indirectcosts was the disagreement between IHS and theSoutheast Alaska Regional Health Board over theboard’s proposal to manage the Mt. Edgecumbehospital. The disagreement, which was the firstcase ever to reach the IHS declination appealsboard (in April 1985), centered on the amount ofthe contract award. The board argued that as a638 contractor, it should receive all IHS costs at-tributable to the hospital, including the share ofAlaska area office functions (e.g., claims process-ing and accounting), that supported hospital oper-ations. The native group sent an accountant tothe IHS area office to review records and estimateadministrative costs associated with the Mt. Edge-cumbe hospital. When the area office stated it didnot have adequate funds to cover the amount re-quested by the native group and it would not en-ter into a 638 contract, the board appealed thatdecision. Despite questions raised by the AlaskaNatives about the declination appeals process it-self, the appeal was denied (68). Following nego-tiations between IHS and the Southeast AlaskaRegional Health Board over the course of 1985,an agreement was reached on the contract fund-ing level and the Mt. Edgecumbe hospital andservice unit were transferred to board control inJanuary 1986 (33).
Tribal Administration of 638 Contracts
Tribes have widely different attitudes about 638contracting. Many tribes in the Alaska, Califor-nia, Bemidji, and Nashville IHS areas are en-thusiastic about self-determination. In other areas,such as Aberdeen, fears of termination of the Fed-eral responsibility for Indian health persist. Othertribes may recognize no compelling reasons to
Ch. 6—Selected Issues In Indian Health Care ● 225— ——
change, particularly in view of the financial risksof 638 contracting.
In addition to the financial difficulties of 638contracting, administrative considerations maydiscourage tribal participation. Managing a healthprogram or facility, especially in the first yearsof a 638 contract, may impose unexpected de-mands on tribal employees. In addition to respon-sibilities for developing and administering person-nel functions and employee benefits plans, tribalgovernment and contract staff are likely to findnew Federal reporting requirements associatedwith the contract.
The responsibility for collecting third-partyreimbursements transfers from IHS to tribal staffwith a 638 contract. Depending on the efficiencyof previous IHS collection systems and the natureof relations with the payers, this transition maybe more or less difficult. Delays in collectionsquickly have an adverse effect on cash flow and,consequently, on a project’s ability to deliverservices.
The third-party reimbursement situation is fur-ther complicated in California, where 638 pro-grams traditionally have served significant num-bers of unaffiliated Indians and unknown numbersof non-Indians. California 638 contractors re-cently have undergone extensive audits to deter-mine whether Federal funds have been expendedon services for non-Indians (43). IHS’s opinion isthat a 638 contract is an extension of IHS itself,and this relationship requires a separation of fund-ing and services to Indians and non-Indians, evenin areas such as California where the distinctionsare not always clear.
When a 638 contract includes operation of anIHS facility, tribal contractors maybe justifiablyconcerned about the physical condition of the fa-cility and the prospects for securing IHS funds formajor renovations or facility replacement, if nec-essary. Because it was not clear whether triballyoperated facilities would be eligible for renova-tion and replacement under the same priority sys-tem that applies to IHS direct care facilities, theSenate version of the 1985 Indian Health Care Im-provement Act provided for inclusion of 638 con-tract facilities in the IHS facilities constructionprogram.

226 ● Indian Health Care— —
One of the most difficult management problemsconfronting a 638 contractor is project staffing.Many IHS delivery sites are so isolated that staffrecruitment and retention are difficult regardlessof available funding, and the programs may de-pend on PHS Commissioned Corps and NationalHealth Service Corps placements to fill medicalpositions. When such programs transfer to tribalcontrol under 638 contracts, the tribes may chooseto hire Federal employees already at the site. Ifthis is not successful, however, tribal contractorsmay have difficulty recruiting private healthprofessionals. Some tribes also may find it diffi-cult to retain Federal or private employees dueto an inability to match Federal salaries and fringebenefits, the uncertainties of tribal politics, orother reasons.
Tribal 638 contractors have several staffing op-tions when they assume operation of an IHShealth facility, service unit, or service program.At the time of the initial 638 transfer (and at thattime only), tribal contractors may acquire IHSemployees under special Intergovernmental Per-sonnel Act (IPA) agreements. Under the condi-tions of these special IPAs, staff members remainFederal IHS employees, retain Federal benefits,and answer to both a Federal and a tribal super-visor. These IPAs have no time limit and can beextended indefinitely at the agreement of the tribe,the employee, and IHS. Special IPAs are the mostfrequently used means of staffing 638 contractprograms. (For example, the transfer of 180 IHSemployees from the Mt. Edgecumbe hospital andservice unit to tribal control was accomplishedwith special IPAs. ) After the initial 638 takeover,tribes may obtain the services of Federal employ-ees under regular, 2-year time-limited IPAs (re-newable for a total of 6 years). Tribes may ter-minate IPA employees at any time. In anotheroption that effectively is the same as an IPA, PHSCommissioned Corps may be assigned to 638 con-tractors under memoranda of agreement (33).
A second important means of staffing 638 fa-cilities and programs is by tribal direct hiring offormer Federal employees. The employee must re-sign from his Federal position before being hiredby the tribal contractor but may retain his Fed-eral benefits if the tribe agrees. In most cases,direct-hire employees switch to tribal government
benefit plans. (The 638 transfer of the IHS hos-pital at Talihina, Oklahoma, to the OklahomaChoctaw tribe in January 1985 primarily involvedthe direct hire of former Federal staff. ) Tribes mayalso direct hire non-Federal outside staff (33).
Tribal control of 638 project staff has its ad-vantages. Federal employees may be retainedselectively, and tribes may terminate IPA anddirect-hire employees at any time. Tribes may hirenew staff from the Indian community, thus pro-viding needed jobs (this can be an important con-sideration for both economic and political rea-sons). Local Indians who are IHS employees,however, may not always be eager to transferfrom Federal to tribal government control becauseof reduced job security and fringe benefits.
IHS regulations require that contracts awardedunder the Self-Determination Act incorporate aclause requiring Indian preference in employmentand training (42 CFR 36.221). This clause, how-ever, is less restrictive than the Indian preferencerequirement for IHS employees, because it per-mits 638 contractors to hire non-Indians after giv-ing full consideration to Indian applicants (42 CFR36.41). Most tribes prefer not to be bound by In-dian preference in employment and training.
Conclusions
Tribal governments and IHS both acknowledgefrustrations with the self-determination program,but there have been no suggestions that it be aban-doned. Some tribes think IHS should providestronger leadership to achieve the goals of self-determination, together with clear policy guidanceto the area offices in their application of contract-ing and procurement regulations to the specialneeds of 638 projects. Applying Federal regula-tions too strictly can create administrative andreporting problems for tribes as they attempt tomanage their service delivery programs. Seriouscash flow problems can result from the inevita-ble delays of the IHS voucher reimbursement sys-tem, Some tribes that now manage 638 contractscomplain of inadequate technical assistance, lackof expertise, and inconsistent, uninformed deci-sionmaking at the area office level. IHS area staff,on the other hand, reply that they are requiredto spend a great deal of time educating tribal staff,

Ch. 6—Selected Issues In Indian Health Care ● 227
who may change frequently, in the policies andprocedures of 638 contract management. The in-depth study by GAO of IHS 638 contract admin-istration, which will be reported in 1986, shouldprovide current, detailed information for the ob-jective evaluation of many of these issues.
The level of funding necessary to support tribal638 health programs, discussed above, has beendebated since the act became law. With IHSbudgets now stable or undergoing reductions,funding for 638 contracts may become an increas-ingly serious problem. The most frequently de-bated complaint about IHS self-determinationfunding is that it does not adequately compen-sate tribes for necessary indirect or administra-tive costs.
Many of the specific points at issue between In-dian tribes and IHS are tests of a question cen-tral to the self-determination program: Who is incontrol of a 638 project? opinions naturally dif-fer, depending on the viewer’s perspective. IHSimplementation of self-determination tends to fo-cus on contract administration responsibilities,while tribes look to 638 contracts as a means tomore effective self-government.
IHS regulations state clearly that the self-deter-mination law is not intended to alter existing eligi-bility criteria for IHS services. IHS 638 contractprojects are considered extensions of IHS itself.If 638 contract projects are extensions of IHS, thenIHS is responsible for administering the contractson behalf of its parent agency, HRSA, accordingto Federal contracting and procurement policiesspecially adapted for the program. Tribal contrac-tors are monitored by IHS to ensure that they ad-here to the terms of their contracts, an approachthat limits the flexibility of 638 contractors tomodify the scope of services they have agreed todeliver or to redefine their service populations.IHS monitors and processes 638 contract finan-cial records through its area offices, which havethe primary role in the procurement and account-ing aspects of contract management under theoverall supervision of the HRSA financial man-agement office.
If 638 programs are extensions of IHS, it alsofollows that they should be included with direct
care services in all IHS data systems. At the endof 1985, most 638 programs were not included inIHS data systems. Many tribal contractors, giventhe option of using IHS data collection forms andprocessing systems or their own noncompatiblesystems, chose to use their own systems. Some638 contracts specifically included data reportingrequirements compatible with IHS systems, butarea office staff found they lacked effective meansof enforcing the requirements. As a result, IHSclinical services data are incomplete, because 638contract data are not captured for all programs.
IHS staff in the Nashville area have stated thatdespite special efforts over the period of a yearor more, they were unable to get IHS headquar-ters to include records from their 638 contractorsin the contract care “piggyback” data system (84).IHS headquarters staff ascribe that particularproblem to incompatible codes in the automateddata records obtained from the tribes. As moreIndian health services are provided under 638 con-tracts, this loss of clinical and management datawill become an increasingly serious problem un-less, as announced in a memorandum from theIHS Acting Director in fall 1985, comparable datareporting is required as a condition of funding for638 contracts (50).
One consequence of administering Public Law93-638 as a contract program and 638 contractsas extensions of IHS has been the retention of IHSheadquarters and area office staff at virtually un-changed levels. The fact that IHS staffing has notdeclined as tribal 638 management responsibili-ties have increased is an issue with some tribeswho believe, rightly or wrongly, that IHS staffduplicate tribal contract managers at the expenseof additional funding that could be devoted to pa-tient care. Maintenance of IHS staffing levels maybe justified to some extent, however, by the 638program provision that allows a tribe to returnor retrocede a contract with only 120 days’ no-tice. IHS argues that staff must be retained in caseof such retrocessions and because of the admin-istrative functions associated with monitoring 638contracts. The retrocession provision could be re-vised so that a longer notice would be required,allowing for a more orderly transition and nec-essary staffing adjustments.

228 ● Indian Health Care
Many tribal governments are interested in self-determination as a means of gaining greater con-trol over their own health services. The purposeof the program as they see it is not contractingper se (which has been an option since 1910 un-der the Buy Indian Act), but self-determination.Because the law and regulations state that tribal638 contractors are entitled to the level of fund-ing committed by IHS to the contracted services,a view has developed that each tribe has the rightto a certain portion of the area budget and shouldbe able to spend it as it sees fit.
From the point of view of self-determination,the 638 contracting process could be made sim-pler and more flexible than it is at present. Tribescontend, with reason, that self-determination con-tracts are not supposed to be administered exactlyas other Federal contracts, Contract negotiationand monitoring procedures have been modified,and could be modified further by IHS and HRSAthrough regulations and Indian self-determinationmemoranda, to make the procedures more suit-able to implementation of “a meaningful Indianself-determination policy which will permit an or-derly transition from Federal domination of pro-grams for and services to Indians to effective andmeaningful participation by the Indian people inthe planning, conduct, and administration ofthose programs and services” (42 CFR 36.201 (2)).
If tribal governments are to assume responsi-bility for program management, the tribes argue,they should have adequate authority and flexi-bility to succeed. Because 638 contract funds arerelatively limited and may not cover all programadministrative costs, tribal contractors believethey need greater flexibility to manage the pro-grams effectively. If the contractors had more flex-ibility in program financial management (and per-haps some limitation of financial risk), they mightbe more likely to take over comprehensive healthdelivery programs instead of following the pat-tern seen in many areas, the management of mul-tiple, small, limited 638 contracts. For some 638projects, financial survival may depend on aggres-sive third-party payer collections and the abilityto serve and bill all local users. In such cases, theissue of serving non-Indians is not one of properuse of IHS funds, but of the right of tribes to pro-vide services to whomever they choose to aug-
A variety of conflicts has developed over the10 years of IHS implementation of the Indian Self-Determination Act. Rather than attempting to re-solve each specific complaint, it would seem morereasonable for Congress, the Administration, andIndian tribes to work to clarify and reaffirm theintent of the law. If the intent is to promote Indianself-determination, defined as active, meaningfulIndian participation in their health services sys-tems, then the IHS contracting process should bemodified further to serve that purpose, and ef-forts should be made to achieve greater con-sistency among IHS areas.
Another basic issue regarding the self-determi-nation process remains to be considered: Whatwould be the effects of Indian self-determinationcarried to an ultimately successful conclusion?What if most tribes were to contract to managetheir entire service units? For one thing, integra-tion of IHS-operated and tribally operated serv-ices would be a greater problem than it is today.What would happen to IHS headquarters and areaoffice staff if 638 contracts were to increase fromthe current 20 to 30 percent of IHS clinical serv-ices to 50 percent or more? The status of Federalemployees then would be a major concern.
The overall costs of greatly expanded tribalmanagement of the Indian health care systemshould be considered. Each tribal contractor mayfind it necessary to duplicate at greater cost cer-tain support functions that are now provided byIHS. To minimize costs, some support functionsmight be separated from direct care delivery andprovided to tribal 638 contractors by special area-level organizations, like the present area offices,at lower costs than each contractor would payindividually, Areawide buyers groups could beorganized to obtain discounts on supplies. Area-wide 638 employee benefits packages and mal-practice insurance plans could contribute to morecost-effective operations. Third-party collectionsand technical support also might be better pro-vided at an area level. IHS area office staff couldassume some of these roles. Areawide service staffwould not have to be tribal employees, but tribalcontractors should have a role in directing the sup-port services.
The administrative problems of Indian self-determination that have been experienced by IHS
ment health program revenues. and the tribes can be reduced by continued co-

Ch. 6—Selected Issues In Indian Health Care ● 229. —
operative efforts. Actions such as those briefly de-scribed above are implementation and manage-ment alternatives. Another management actionwould be to assume more responsibility for ad-ministering ongoing (renewal) self-determinationcontract programs directly from IHS headquar-ters, leaving area office staffs more time to pro-vide technical assistance in 638 contract proposal
RESOURCE ALLOCATION IN IHS
Introduction
Most Indian tribes and all IHS area offices haveopinions about the methods and results of IHS’sapproach to resource allocation: none of the areasis satisfied that it is receiving adequate resources.In part, this view reflects dissatisfaction with theoverall level of IHS appropriations. In addition,however, there is a general belief that IHS is notallocating resources among its areas as equitablyand cost-effectively as it could. These issues ofequity, a rational basis for resource allocation,and the most cost-effective use of IHS’s limitedresources were debated at all of OTA’s regionalmeetings.
The present distribution of IHS facilities, man-power, and programs among the 12 IHS areas isnot the result of health systems planning. Instead,it has evolved over many years in response to con-gressional appropriations and directives and theadministrative decisions of Federal agencies, espe-cially BIA and IHS. Historically, Federal healthservices for Indians have been concentrated on thelarge, reservation-based Indian populations in theAmerican West, and some of the smaller groupsand tribes lacking Federal recognition have beenneglected. IHS regulations state that it is not ob-ligated to provide the same range and level ofservices in all IHS areas (42 CFR 36.11 (c)), be-cause IHS is not a Federal entitlement program.The courts have determined, however, that if re-sources are not adequate to meet all needs, IHSis responsible for allocating available resourcesamong its eligible population groups on a rationalbasis.
In order to support the existing network of fa-cilities and programs, IHS allocates its annual ap-
development and the implementation of new 638contract projects. These and other actions couldbe considered more productively within a clari-fied policy framework that reflects a consensusof tribal organizations, IHS administrators, andCongress about the intent and objectives of theSelf-Determination Act.
propriations on the basis of “historical” or “pro-gram continuity” budgeting: that is, each area canexpect to receive its base budget from the previ-ous year, plus a share of funding increases equalto the percent increase in the IHS budget. Excep-tions to this general allocation rule are made whenCongress earmarks special program funds for cer-tain areas, or when an area secures new IHS fa-cilities that bring with them increased levels ofstaffing and support resources. The lack of co-ordination between the IHS facilities constructionprogram and IHS clinical services reduces the cost-effectiveness of the overall system.
Resource allocations from IHS headquarters toits area offices are not based on the size of theservice population, the relative health status andparticular service needs of the population, the his-torical demand for services in the area, or theavailability of alternate, non-IHS resources. Con-trary to the perceptions of many tribes, the an-nual resource requirements methodology (RRM)application process, which estimates resourceneeds by service unit and area based on work-load history and population projections, does notenter into the allocation formula except to distrib-ute a small annual equity fund. Although IHSareas agree that the current resource allocationsystem is not satisfactory, they have not reachedconsensus on how the allocation formula shouldbe revised.
The uneven, unplanned distribution of re-sources among the 12 IHS areas can be docu-mented in a number of ways. Although tribes donot generally support a per capita approach toresource allocation, recognizing that the costs ofhealth care and the mix of IHS direct, contract,and non-IHS alternate resources vary substan-

230 ● Indian Health Care
tially from one area to another, any analysis ofper capita budget allocations results in a widerange of figures. The area populations applied inper capita calculations are subject to particulardebate, because IHS uses estimates derived fromthe 1980 U.S. census which, it is argued, over-counts the Indian population in some areas andundercounts in others. Variations among the areasin determining who is eligible for IHS services alsoaffect estimates of the base populations.
Table 6-4 shows that based either on the IHScensus-based area service populations or on esti-mated user populations derived from other sources,per capita dollar resources are unevenly distrib-uted among IHS areas. IHS service populationestimates yield 1985 per capita allocations rang-ing from $497 in the Portland IHS area to $1,633in the Alaska area. Four areas (California, Port-land, Oklahoma, and Navajo) received per cap-ita allocations below the IHS average, and Bemidjiand Nashville were not far above average. Esti-mated IHS user population figures, on the otherhand, resulted in a range of from $552 per capitain the Navajo area to the high in Alaska. Areasbelow the IHS average per capita allocation wereOklahoma, Navajo, Portland, and Bemidji. Okla-
homa area per capita allocations were low, inpart, because the entire State is a contract healthservice delivery area, and therefore all Indian resi-dents are IHS-eligible and potential users, whetherthey rely on the IHS system or not. Areas thatare dependent on IHS contract care also rankedrelatively low in per capita funding. It is appar-ent, however, that the accuracy of the service pop-ulation figures is the critical factor in equitableper capita resource allocations.
Because the largest portion of the IHS budgetis dedicated to clinical services delivered by di-rect care hospitals and clinics, resource allocationsby area follow closely the distribution of IHS andtribally operated health facilities. Figure 1-7 inchapter 1, the map locating IHS and tribal hos-pitals and clinics, illustrates that facilities are notequally available and accessible to Indians in allIHS areas. Descriptions of the location and rangeof services offered by IHS direct care, contractcare, and urban Indian health programs in chap-ter 5 also support the conclusion that the presentdistribution does not offer equal access to com-parable types of services. The California and Port-land IHS areas have no IHS hospitals at all, andonly two of the widely scattered tribes in the
Table 6-4. -IHS Budget Allocations by Area With Estimated Per Capita Allocations, Fiscal Year 1985
1985 IHS service population 1985 IHS user population
Fiscal year 1985 Population Per capita Population Per capitaIHS area allocation estimate a allocation estimate b allocationAberdeen . . . . . . . . . . . . . . . . . . $ 74,270,100 72,679 $1,021.89 72,679a $1,021.89Alaska. . . . . . . . . . . . . . . . . . . . . 119,792,600 73,351 1,633.14 73,351 a 1,633.14Albuquerque . . . . . . . . . . . . . . . 53,365,300 52,471 1,017.04 51 ,363’ 1,038.98Bemidji . . . . . . . . . . . . . . . . . . . . 39,332,100 48,245 815.26 44,337C 887.12Billings . . . . . . . . . . . . . . . . . . . . 51,495,000 41,326 1,246.07 38,470C d 1,338.58California . . . . . . . . . . . . . . . . . . 31,243,300 73,414 425.58 26,640e 1,172.80Nashville . . . . . . . . . . . . . . . . . . 32,421,600 36,413 890.39 28,696 f 1,129.83Navajo. . . . . . . . . . . . . . . . . . . . . 106,834,600 166,493 641.68 166,493 a 641.68Oklahoma. . . . . . . . . . . . . . . . . . 98,540,400 195,346 504.44 178,456C 552.18Phoenix . . . . . . . . . . . . . . . . . . . 88,369,600 84,516 1,045.60 79,502C 1,111.54Portland . . . . . . . . . . . . . . . . . . . 49,198,500 98,996 496.97 62,380 f 788.69Tucson . . . . . . . . . . . . . . . . . . . . 17,796,000 18,332 970.76 1 5,959cg 1,115.11
IHS area totals . . . . . . . . . . . $762,659,100 h 961,582 $ 793.13 838,326 $ 909.74alHs ‘ensus.based eligible SeWlce population estimates, 1985. When estimated user population counts from other sources exceeded census-based est~rnates, IHSOffice of Program Statistics elected to use the census-based estimates (fourth column).
bFi~cal year 1985 population estimates &VelOp@ by It-is Office of Program Statistics, recommended for Use in fiscal Year 1968 allocation.cEstimate modified by special computer routine to remove duplicates from ambulatory Patient care records.d B as ed on contract workload dataeBased on special count of users from individual California tribal Prolects.fBased on IHS area office user count data.g{ncludes enrollment in Pascua.yaqui health maintenance organization.hThis sum of IHS area allocations in fiscal year lg85 (final as of 9/26/85) exciudes funding for IHS headquaflers functions in Rockviile, MD, and Albuquerque, NM,
SOURCE U S Congress, Office of Technology Assessment, based on data from U S Department of Health and Human Services, Public Health Service, Health Resourcesand Services Administration, Indian Health Service, Office of Program Statistics, Resources Management and Program Statistics Branches, 1965

Ch. 6—Selected Issues In Indian Health Care ● 231
Nashville area have access to IHS or tribal hos-pitals. In these areas, IHS-eligible Indians mustrely primarily on their contract care programs forinpatient services, but limited contract care budg-ets often force rationing of contract referrals toemergency and life-threatening conditions only.In contrast, areas that have IHS hospitals andclinics also have contract care budgets to supple-ment their direct services. The present approachto resource allocation does not provide a com-parable package of services in all areas, nor doesit compensate IHS areas that are dependent oncontract care for their lack of IHS direct services(although a combined allocation was recommendedby the Director’s Contract Health Services TaskForce in 1983, as discussed below).
A comparison of IHS staff assignments relativeto inpatient and ambulatory care workloadsamong the 12 areas also was described in chap-ter 5 (see table 5-5). While the average through-out IHS in fiscal year 1984 was 178 clinical work-load units per clinical staff position, that measureranged from a low of 152 workload units per po-sition in the Albuquerque IHS area to a high of243 units per position in Aberdeen. Such dispar-ities in the workloads carried by IHS staff in dif-ferent areas support complaints from some areas(Aberdeen, for example) that staffing shortagesnot only limit the range and volume of servicesthat can be delivered, but unusually heavy work-loads also discourage the recruitment of additionalstaff.
Perhaps the most detailed and systematic docu-mentation of the uneven distribution of IHS re-sources is generated by the IHS’s equity fund al-location formula. As will be described later in thissection, IHS allocates an annual equity or specialfund by a method that incorporates RRM criteriato determine resource requirements, available re-sources, and unmet resource needs at the serviceunit and tribal levels. This formula allows tribesto be ranked by resource deficiency levels in fivegroups, from level I (O to 20 percent deficiency)to level V (80 to 100 percent deficiency). Follow-ing distribution of the 1985 special fund, 46 of 266tribes ranked in level I, 99 in level II, 101 in levelIII, and 20 in level IV. There were no tribes inlevel V, the group with 80 to 100 percent resourcedeficiencies. This means that by IHS’s own assess-
ment, 121 tribes, or 45 percent of all tribes, wereat least 40 percent deficient in their estimated re-source needs. The equity formula thus providesevidence of differences in resource availabilityamong IHS areas, and among service units andtribes within IHS areas, which is another aspectof the debate about equity in resource allocation.
Decentralization has been an explicit manage-ment philosophy in IHS for many years. Withinbudget categories and other constraints placed onthe funds by Congress, IHS allocates its annualappropriations only to the IHS area office leveland permits the areas to redistribute funds amongtheir service units by their own methods. Therehave been complaints about the rationale for area-to-service-unit allocations, coming most oftenfrom smaller and recently reinstated tribes thatbelieve they are not able to compete effectivelyfor resources against larger, well-establishedtribes.
Individual service units and tribes generally donot relate directly to IHS headquarters in thebudget allocation process, but some tribes main-tain direct political relationships with Congressand individual members of Congress. In terms ofhealth care, tribal political efforts most often havefocused on securing earmarked funding for spe-cial initiatives and demonstration projects (e. g.,hepatitis-B vaccinations in Alaska or diabetestreatment programs) and for health facilities con-struction and renovation projects. Facilities proj-ects are selected and funded by Congress underprocedures separate from those applicable to IHShealth service resource allocations. Nonetheless,new facilities and the expanded staff and operat-ing budgets associated with them are major fac-tors in the overall resource allocation picture.
The limitations of reliable IHS program plan-ning and management information pose problemsin many aspects of IHS operations, including re-source allocations. Sophisticated allocation for-mulas cannot be applied without adequate data,nor can the actual extent and impact of resourceinequities be convincingly defined. Data are avail-able, however, that could improve resource al-
location decisions, given the political consensusto use them. Serious efforts have been underwayto improve IHS resource allocation methods since

232 ● Indian Health Care
1980, and especially since summer 1985. These ef-forts, which are described below, have culminatedin a new allocation formula that is proposed forapplication to a portion of the fiscal year 1986appropriation. Following a brief description of thedevelopment of the RRM criteria and their rolesince 1981 in distributing the court-ordered an-nual equity funds, this section will review recentactivities in IHS resource allocation and considerfactors that might usefully be incorporated in anyallocation formula.
IHS Resource Managementin the 1970s
Overall appropriations in the 1970s reflectedsteady growth, and IHS headquarters allocatedthose funds by budget category to the area officesin keeping with the historical or program conti-nuity budget approach. Each area office could ex-pect to receive its recurring base budget from theprevious year, plus an increase in built-in man-datory cost categories (e.g., staff cost of living,relocation expenses, and supply cost increases)equal to the percentage increase in those catego-ries awarded to the overall IHS program.
A process of rationalizing IHS resource man-agement methods was initiated in 1972 with orga-nization of the resource allocation criteria (RAC)workgroup. RAC development was undertakenin an environment of general interest in healthplanning methods, with encouragement from theOffice of Management and Budget and the Of-fice of the Secretary, U.S. Department of Health,Education, and Welfare. RAC standards were notintended to guide the distribution of available re-sources among competing IHS areas and serviceprograms, but were developed as part of a plan-ning algorithm to quantify the resources required(primarily staffing) to provide a specific volumeand mix of services. Modified versions of theoriginal RAC criteria (now known as RRM) stillare used in the annual IHS budget developmentprocess, in the distribution of equity funds, andin planning the staffing requirements for new fa-cilities and services.
The RAC committee worked from 1972 to 1975to develop sets of service-specific criteria thatdefined workload measurements and associated
staffing requirements. The RAC committee wasmade up of IHS headquarters and area office staff,representatives of the IHS Office of Research andDevelopment, and consultants such as health pro-viders and industrial engineers. The analyticalsteps followed by the committee and its techni-cal working groups included: 1) definition of IHSclinical service functional areas; 2) review of pub-lished criteria and standards; 3) determination ofappropriate tasks within each IHS service func-tion; 4) determination of unit times by function;5) definition of a productive person-year, by typeof staff; 6) construction of staffing tables; and 7)submission of proposed or revised criteria to ex-pert panels and the RAC committee for final ap-proval (218).
The original RAC criteria sets defined functionsand tasks for inpatient services such as medicalcare, nursing, laboratory, X-ray, and facilitymaintenance, to name 5 of the 14 inpatient carecomponents; and for ambulatory medical care,dental care, optometry, audiology, and supportservices (169). In developing its criteria and stand-ards, the RAC committee drew on the literature,academia, and professional associations for ex-isting manpower criteria, and on industrial engi-neering techniques including time-and-motionstudies. Field work specific to the IHS system wasdone only for ambulatory care services. Estimatesof the times and frequencies of performing definedtasks, by type of service and provider, were in-corporated into mathematical models to gener-ate staffing tables that displayed numbers of staffrequired for each workload level (218).
RAC criteria sets, most of which were detailedto the level of available and required annual serv-ice minutes, by type of service and provider, de-liberately reflected the staffing levels needed toprovide health services under ideal circumstances.Although this was a logical planning approach,the decision to base RAC on ideal service deliv-ery conditions has resulted in a large gap betweenrequired resources, as estimated by RAC criteria,and the resources actually available to IHS. Thus,it has produced the awkward deficiency level ap-proach to assessing relative health resource needsamong the service units.
Some RAC criteria sets have been updated forchanges in technology and delivery patterns, but

. —
Ch. 6—Selected Issues In Indian Health Care ● 233
they are not all updated on a routine basis. In the1983 edition of the RAC reference manual, mostof the inpatient care criteria dated from 1977 to1979, while ambulatory services reflected 1980 to1983 revisions (169). A quick review of all re-source allocation criteria sets was completed insummer 1984 by an in-house group known as the“interim fix” committee. That committee reducedstaffing requirements overall by 17 percent, in-corporated support costs, and changed the meas-ure of resource requirements from staff positionsto dollars (214). Another review of the criteria setsin fall 1985 established limits to the range of var-iation in the workload factors (214).
Late in the 1970s, RAC became known as theresource requirement methodology, or RRM. Asthen described, the purpose of the RAC/RRM sys-tem was “to provide the Indian Health Servicewith a comprehensive, systematic, and consist-ent process for determining resource requirements,primarily manpower, as well as a process for dis-tributing nonearmarked program increases (po-sitions and funds) to the Area/Program Offices”(169).
In the annual IHS budget application process,service unit and area office staff follow detailedinstructions in the RAC/RRM manual to projectservice unit workload and resource requirementsfor each functional program. In a process knownas demand forecasting, the previous year’s work-load (utilization) figures and IHS census-basedpopulation estimates are applied to determine thenumbers of staff, by type, that would be neededto deliver the expected volume of each type ofservice. Numbers of required staff then are con-verted to personnel costs using an average costper position from IHS headquarters, support costsassociated with each service are calculated, andthese combined costs represent total resource re-quirements for each service unit. For a new facil-ity or service that has no workload history, utili-zation experience from similar IHS facilities isapplied to the estimated new service population.Results of the RRM application process by serv-ice unit are aggregated to the area office level andthen incorporated by IHS headquarters into theoverall IHS budget proposal. Therefore, the RAC/RRM criteria do play a role in developing theannual IHS budget request, but neither DHHS nor
Congress is obligated to provide the level of re-sources needed according to the RRM application.
The IHS Equity Health Care Fund
IHS’s methods of allocating resources amongits area offices, service units, and tribes were thetarget of legal challenges in the late 1970s. Onecase, Rincon Band of Mission Indians v. Califano(104), resulted in a court order directing IHS totake steps to reduce the disparities in fundingamong tribes. The Rincon case was a class actionsuit filed in May 1974 by certain groups of Cali-fornia Indians who claimed that IHS had illegallydenied them health care services comparable tothose provided to other American Indians. Theplaintiffs documented that from 1968 through1978, IHS had allocated only 2 percent of its an-nual appropriations to California Indians who,according to the 1970 census, represented over 10percent of the IHS service population (132). (Seech. 2 of this assessment for a more detailed dis-cussion of Rincon and related decisions. )
Both the U.S. District Court for the NorthernDistrict of California and the U.S. Court of Ap-peals for the ninth circuit ruled for the plaintiffs.The Court of Appeals criticized the long-standingIHS practice of basing annual resource allocationson the previous year’s budget. The courts foundthat IHS had not established that its funding de-cisions affecting California Indians were made ona rational basis, and ruled that IHS was “obligatedto adopt a program for providing health servicesto Indians in California which is comparable tothose offered Indians elsewhere in the UnitedStates” (132). Neither court specified how IHS wasto implement this directive, but both cited Mor--ton v. Ruiz (89), a case involving BIA, as prece-dent for invalidating IHS’s program continuityfunding approach. The Ruiz decision, in brief,stated that if an agency did not have adequateresources to serve all eligible beneficiaries, theagency was obligated to allocate those limited re-sources equitably by the consistent application ofreasonable distributive standards.
In response to the court order, IHS proposedto allocate an equity fund by a needs-based for-mula as its means of achieving comparabilityamong tribes in health care funding. For fiscal year

234 ● Indian Health Care
1981, the House and Senate Appropriations Com-mittees earmarked $7,856,000 of the $594 millionIHS health services appropriation, or 1.3 percent,as an equity health care fund (note that $594 mil-lion was the initial appropriation, prior to a sup-plementary appropriation for personnel cost in-creases that brought the final fiscal year 1981appropriation to $613 million). Questions aboutthe application and effects of the IHS equity fundmechanism were raised soon after its initiationwhen GAO analyzed the fiscal year 1981 equitydistribution. Fifty-one tribes that ranked in levelV (80 to 100 percent resource deficiency) in Feb-ruary 1980 received 1981 equity funds, and onlytwo tribes remained in level V in November 1981.GAO concluded, however, that because of weak-nesses in the allocation methodology, the tribesthat received 1981 equity funds may not have beenthose with the greatest relative health servicesneeds (132).
Although equity funds totaling $32,362,000were earmarked for fiscal years 1981 through1984, their shares of the overall IHS budgets wereless than 2 percent per year, as illustrated in ta-ble 6-5 (135). The effects of equity funds on serv-ice unit budgets are cumulative, however, becauseequity awards become part of the recurring basebudget and thus are assured in future years. TheCalifornia Indians received $11,134,000 (34.4 per-cent) of the 4-year equity funds. Congress did notearmark equity funds in fiscal year 1985, but IHS,still under court order to reduce funding dispari-ties, set aside a special fund of $5 million for anequity distribution (78).
The equity fund allocation methodology at-tempts to determine unmet resource needs by tribe(not by service unit, although the method appliesequally well to service units), on a systematic, uni-form basis. The methodology: 1) estimates re-source requirements for all “tribal and non-tribalentities” (except urban Indian groups) using IHSpopulation estimates, utilization experience, andRRM criteria sets; 2) determines the health re-sources available to each tribe, including IHS andother Federal, State, local, and private resources;3) divides unmet need (the difference between re-source requirements and available resources, ex-pressed in dollars) for each tribe by its estimatedresource requirement to define a percentage defi-ciency; and 4) ranks all tribes in five levels of re-source deficiency, from level I (zero to 20 percentdeficiency) to level V (80 to 100 percent defi-ciency). Available equity funds then are awardedto tribes with the greatest levels of deficiency (17).A newly recognized tribe could be 100 percent re-source deficient, if it had not previously receivedIHS funds; and in fact the equity fund has beenan important source of initial funding for newlyrecognized tribes.
The resources available to a tribe are definedas its recurring base budget from the previous year(including previous year equity funds), plus otheravailable non-IHS health resources. IHS officialsbelieve that data on Medicare and Medicaid re-sources are reasonably reliable, but other sourcesincluding State, local, and private providers andinsurers are not well-reported (17,214). Tribes areasked to self-report these other resources, but
Table 6-5.—IHS Equity Health Care Fund Appropriations, Fiscal Years 1981-84,and IHS Special Fund, Fiscal Year 1985°
Fiscal year1981 1982 1983 1984 1985a
Appropriation. . . . . . . . . . . . . . . $7,856,000 $7,636,000 $7,000,000 $9,870,000 $5,000,000
Percent of total IHSappropriations . . . . . . . . . . . . 1 .13%0 1 .13 ”/0 0.9% 1.19% 0.60/0
%ngress did not appropriate an equity fund in fiscal year 1985. Instead, IHS set aside a $.5 million special fund from its hospitalsand cllnics budget that was distributed by the equity formula.
SOURCES: For flacal yeara 1981-84: Data from the Indian Health Service published in U.S. Congress, House of Representa-tives, Committee on Energy and Commerce, staff report for the Subcommittee on Health and the Environment,“lndian Health Care: an Overview of the Federal Government’s Role,” committee print 98-Y, U.S. Government Print-ing Office, Washington, DC, April 1984. For fiscal year 1985: U S. Department of Health and Human Services, Pub-lic Health Service, Health Resources and Services Administration, Indian Health Service, 1985,

clearly it is not advantageous for them to do soand thus reduce their estimated unmet resourceneeds.
After distribution of the 1985 special equityfund, 46 of 266 tribes had resource deficienciesof 20 percent or less (level I); 99 were in level II;101 in level III; and 20 tribes ranked in level IVwith resource deficiencies exceeding 60 but lessthan 80 percent (see table 6-6). There were notribes with resource deficiencies exceeding 80 per-cent (level V) (189). It is interesting to note thataccording to IHS’s equity methodology, the Rose-bud Sioux service unit in South Dakota, whichfrequently is cited as an example of poor qualityIndian health care, now ranks among the 46 best-served tribes with a resource deficiency of lessthan 20 percent. Peculiarities such as this raisequestions about the validity of the equity formulaand its supporting data. Nonetheless, the specialequity fund was the only portion of the fiscal year1985 IHS allocation that was distributed on a basisother than program continuity.
Resource Allocation in the 1980s
From October 1982 through publication of itsreport in February 1983, a special interagency IHSDirector’s Task Force on Contract Health Serv-ices analyzed a number of problems affecting IHSoperations. Among its recommendations, the taskforce suggested that improvements be made in IHSresource allocation methods (181).
The task force concurred with judicial directivesthat IHS should develop and apply rational, equi-table methods of allocating its appropriated re-
Ch. 6—Selected Issues In Indian Health Care . 235
sources. Furthermore, it concluded that a formulashould be developed to combine direct and con-tract care resource needs, and it should be basedon enrolled user populations rather than IHS eligi-ble service population estimates (181). The taskforce observed that IHS’s long-standing practiceof allocating funds on the basis of program con-tinuity, combined with the earmarking of fundsin congressional appropriations, had contributedto substantial inequities in the funding of healthservices among IHS service areas and tribes.
The contract health services task force urgedthat a new set of allocation formulas be devel-oped to take into account a defined service pop-ulation, reasonable estimates of third-party re-sources, the unique geographic, economic, andhealth status characteristics of the areas, and in-centives for good management. A model resourceallocation formula was proposed that defined anarea’s annual need for clinical services funding byits actual user population, multiplied by user percapita costs of hospital and ambulatory care serv-ices, respectively, minus estimated third-partyreimbursements. Individual IHS area dollar re-quirements then would be divided by the com-bined requirements of all areas and the resultingpercentage multiplied by the congressional ap-propriation for IHS clinical services. The taskforce recommended that IHS areas use this sameapproach to determine service unit allocations(181).
Although these specific recommendations of thecontract health services task force were notadopted, they provided the starting point forwork during the summer of 1983 by another in-
Table 6-6.—IHS Ranking of Tribal Groups by Deficiency Level for Equity Health Care Fund Distribution, 1980-85
Number of tribes
Deficiency As of As of As of As ofPercent deficiency level February 1980 November 1981 April 1984 March 1985
<20 . . . . . . . . . . . . . . I 1 10 36 4621 to 40 . . . . . . . . . . . . . II 15 30 60 9941 to 60 . . . . . . . . . . . . . . Ill 88 95 156 10161 to 80 . . . . . . . . . . . . . . IV 93 107 0 2081 to 100 . . . . . . . . . . . . . v 51 2 0 0
IHS total . . . . . . . . . . . 248’ 244’ 252a 266a
aT~t’1~ “aV frOm year t. year because of newly recognized tribes and c hang!ng tribal health conso~lums
SOURCES U S. Congress, General Accounting Office, “Indian Health Serwce Not Yet Dlstrlbutmg Funds Equitably Among Tribes,”’ publication GAO/H RD-82-54 (Washing.ton, DC U.S Government Pnntlng Office, July 2, 1982); and tribal rankings for 1984 and 1985 from U S Department of Health and Human Services, PublicHealth Service, Health Resources and Serwces Admlntstrat!on, Indian Health Service, Program Planning Branch, 1985

236 ● Indian Health Care
house group, the Resource Allocation Method-ology (RAM) Task Force (182). The objective ofthe RAM approach was “to promote cost-effec-tiveness and quality of existing IHS services andto promote equal access to equivalent health careto all eligible Indians” (182). The RAM task forcedefined equity as “relative equal access of the serv-ice population to equivalent health care services, ”and recognized both the need for continuity inserving current user populations and the need toaddress limited access to IHS services in someareas. A two-part approach to allocating IHS re-sources was proposed: resources to maintain ex-isting services (the bulk of the funding) would con-tinue to be allocated primarily on a historicalfunding basis; but a portion of the resourceswould be distributed to selected areas to compen-sate for their lack of access.
To determine appropriate resource compensa-tion for underserved areas, utilization rates forinpatient and ambulatory care (combining IHS di-rect services and contract care programs) wouldbe calculated for each area and compared withutilization rates for IHS as a whole (rates basedon summed area figures). If an area’s utilizationrates were lower than the IHS average, the differ-ence would figure into a formula to generate ad-ditional resource requirements. The RAM taskforce did not fully develop this part of its ap-proach because of data limitations, but it assumedthat below-average utilization reflected a lack ofaccess to services and was a proxy for unmet need(182). Some of the task force’s proposals were pi-lot tested by IHS headquarters staff from Novem-ber 1983 through January 1984 with verified areaworkload and cost data. IHS concluded that theapproach that incorporated RRM criteria to de-termine existing service requirements, which wassimilar to the equity distribution formula, wassound.
In fiscal year 1984, IHS received program in-creases of nearly $42 million in budget categoriesfor hospitals and clinics, contract health services,and support to tribally operated services. Allo-cation of the hospitals and clinics program in-crease of $9.5 million reflected a measure of un-met need based on RRM, but it was the only oneof the three special allocations that incorporatedRRM. Of the $27,4 million increase for contract
care, $9.4 million was withheld and allocated ad-ministratively to cover priority I emergency care.The remaining $18 million was allocated amongIHS areas by a method that incorporated actualrates of cost inflation experienced in each area.There were substantial variations in those rates,as area offices appear to have little control overincreases in charges by non-IHS contract careproviders. A total of $5 million in additional fund-ing was available in 1984 to support tribally oper-ated 638 health programs. It was allocated by aninflation-based model, in which the same Officeof Management and Budget inflation rate was ap-plied to all IHS areas, with the result that all areasreceived the same percentage increase (7.6 percent)over fiscal year 1983 funding (222).
Combining the allocations of fiscal year 1984increases in hospitals and clinics, contract care,and tribal support, the Aberdeen IHS area re-ceived the largest percentage increase (about 26percent above its 1983 recurring base budget), al-though its overall budget was relatively small.Tucson received a 15-percent increase on a smallbudget, and the Bemidji, Navajo, and PortlandIHS areas received increases of about 10 percenteach. California received the smallest increase,6.7 percent.
This discussion of recent modifications in IHSresource allocation methods illustrates that whenadditional funds have been available, as they werein fiscal year 1984, efforts have been made to dis-tribute at least part of the increases to achieve amore equitable balance in funding and serviceavailability among the areas. It is not surprising,however, that there remains a great reluctance toredistribute area recurring base budgets. Therewere virtually no additional moneys in fiscal year1985, and the methods tested in 1984 were notused again. The fiscal year 1985 distribution fol-lowed the program continuity allocation processof supporting recurring base budgets, with a spe-cial fund of $5 million withheld for an equity for-mula distribution. In addition, a small reserve ofabout $2 million was distributed from headquar-ters to meet emergencies during the year (214).
Allocation of the fiscal year 1986 IHS appropri-ation had not been completed by the end of Feb-ruary 1986, due to uncertainties about final 1986funding levels and proposed modifications to the

Ch. 6—Selected Issues In Indian Health Care . 237.——
resource allocation process. IHS was appropriated$818 million for health services and nearly $47million for facilities construction under the fiscalyear 1986 continuing resolution (91). The Gramm-Rudman legislation (Public Law 99-177), effectiveMarch 1, 1986, reduced IHS appropriations by1 percent in service delivery categories and 4.3percent in administrative functions, resulting inlosses of $10,4 million to health services and $0.4million to facilities construction budgets. Stillpending in March 1986 were recisions proposedby the Office of Management and Budget amount-ing to an additional $32 million cut in IHS serv-ices and $44 million in facilities construction (91).Because Congress would have to adopt the Of-fice of Management and Budget recisions in or-der for them to take effect, it is thought that theywill fail; but the issue remained unresolved inMarch 1986.
Since fall 1985, an IHS workgroup known asthe Operations Analysis Project has been consid-ering possible modifications to the IHS resourceallocation process. The work of this group re-sulted in a detailed draft proposal to the IHS Di-rector early in 1986. RRM criteria sets (modifiedby screens, or limits in the range of acceptableworkload values) will be applied at the service unitlevel and aggregated to area offices, allowing theareas to be ranked by levels of deficiency and ad-ditional funds to be distributed to compensate themost deficient areas (214). The basic approachwould be similar to the equity fund formula: useof RRM criteria sets, actual utilization data, andenrolled (not census-based) population figures toidentify area resource requirements; quantifica-tion of IHS and non-IHS available resources; esti-mation of a health status indicator, years ofproductive life lost, based on mortality rates, byarea; and comparison of resource requirementsagainst available resources, adjusting for healthstatus and resource deficiencies, to generate a fi-nal allocation formula by IHS area.
The IHS Director must determine what amountof funding will be subject to the new allocationformula, what amount of non-IHS resources (col-lections from Medicare, Medicaid, and otherthird-party resources) should be offset against to-tal resource needs, and how two new weightingfactors–the area percentage of the IHS weighted
resource deficiency, and the area percentage ofIHS total years of productive life lost—should fig-ure in the formula (214), The IHS Director con-sulted on these questions with the area directorsin meetings held in late fall 1985 and March 1986.The IHS area directors have agreed that any fund-ing increases over fiscal year 1985 base budgetlevels (including mandatory budget categories)will be distributed by a special RRM-based, eq-uity type formula; but no area will receive lessthan its 1985 funding (the areas simply will re-ceive varying amounts of the additional funds).Furthermore, area population figures will be basedon the patient registration system, rather than onIHS census-based estimates of the eligible servicepopulations. The resource allocation formula thatultimately will be applied, however, will be de-cided when the final level of fiscal year 1986 fund-ing is known.
Conclusions
IHS traditionally has distributed its annual ap-propriations among its areas by budget category,according to each area’s share of the budget fromthe previous year. Thus, there has been incre-mental funding growth to support existing pro-grams and facilities. The RAC/RRM system, de-veloped in the 1970s to rationalize planning forstaffing needs, has been used since 1981 in thecourt-ordered distribution of IHS equity funds.The RRM criteria, however, do not play a majorrole in the overall IHS budget allocation process,which continues to be driven by the historical orprogram continuity funding approach. Even ifRRM criteria were incorporated in IHS allocationmethods, distributions based on RRM criteria,workloads, and population estimates would notfactor in relative health status, health needs, spe-cial geographic problems, availability of alternateresources, or other measures that could providefor more rational and cost-effective decisionmak-ing. When health care needs do not result in serv-ice utilization, as may be the case in areas whereIHS and other services are not readily availableand accessible, those needs usually are not takeninto account at all.
Although the equity fund distribution appearsto follow a straightforward approach incorporat-

238 ● Indian Health Care
ing the RRM criteria, the formula is vulnerableto problems of data quality and validity, com-pleteness of reporting, and the apportionment ofpopulation estimates. The need to make assump-tions about data sources and processes in orderto apply the methodology can result in unpredict-able and unintended outcomes. IHS has respondedto criticisms such as these with efforts to improvesupporting data systems and to increase con-sistency in application of the equity formula. After5 years of equity fund distribution, some tribes(especially newly recognized tribes) have bene-fited; but because the equity formula has been ap-plied to less than 2 percent of the overall IHSbudget each year, the approach has not producedsignificant changes in area budget shares. A reso-lution by the Navajo nation (120) and commentsfrom the Northwest Portland Indian Health Board(95) and other groups indicate that the IHS eq-uity approach so far has been an unsatisfactorymeans of attempting to equalize resources andservices among tribes.
Recent IHS efforts to refine a resource alloca-tion formula, like the equity formula, that couldbe applied to redistribute a portion of IHS arearecurring base budgets (as well as to budget in-creases or reductions) are encouraging. Given thepractical and political arguments against a sud-den, substantial redistribution of IHS resources,greater equity in overall resource distributionscould be achieved gradually by the allocation ofdesignated funds by a needs-based formula. Con-gress has earmarked IHS funds for equity distri-bution in the past and could continue to do so,pacing the redistribution by the amount of ear-marked funds. Likewise, appropriations could beearmarked for development of the needed IHS pa-tient care and program management informationsystem. Congress has expressed support for theconcept of comparable service packages in all IHS
areas, an approach that is supported by a num-ber of tribal organizations as well.
There are reasons to expect that equity and cost-effectiveness in IHS resource allocation will con-tinue to be important issues for the program, andin fact may become more critical in the near fu-ture. In the past, IHS was able to allocate budgetincreases from year to year; but in the future, itmay be required to manage stable or reducedoverall appropriations (how the proposed 1986resource allocation formula might be applied tobudget reductions, instead of increases, is understudy in IHS). Although Gramm-Rudman reduc-tions in the fiscal year 1986 IHS budget werelimited to 4.3 percent of administrative and 1 per-cent of service costs, future applications of thatlaw would have serious cumulative effects.
In many IHS areas, limited funding alreadyforces rationing of services in the IHS contractcare program, and overall budget constraints willincrease pressures to ration those services. At thesame time, if adequate funding is not availableto maintain IHS facilities and equipment, thosefacilities will deteriorate and the capacity to de-liver services directly could decline and forcegreater reliance on contract care purchases, IHSalready experiences shortages of qualified medi-cal staff, and when the National Health ServiceCorps is phased out (the last assignees will beavailable in 1990), those shortages could becomecritical. Finally, IHS is planning to publish newrules governing eligibility for IHS services, whichcould result in a realignment of IHS area servicepopulations. All of these factors will focus greaterattention on the cost-effectiveness of IHS resourceallocation decisionmaking, especially if IHS is ina position to distribute budget losses rather thangains, and will intensify the debate about the data,allocation criteria, and formulas that should beused.
THE PROBLEM OF HIGH-COST CASES IN THEIHS CONTRACT CARE PROGRAMIntroduction
ties some service units experience in purchasingThe IHS contract care program and its man- only the most urgently needed services with their
agement at the service unit and area office levels limited contract funds, it is not surprising that onewere discussed in chapter 5. Given the difficul- or more extremely costly cases could absorb a

Ch. 6—Selected Issues In Indian Health Care . 239
large part of a service unit’s contract care budget.Not only is it difficult for service units to coverthe costs of these so-called “catastrophic cases, ”but because most of the high-cost cases involvelife-threatening conditions that take precedenceover less urgent care, the entire contract care de-livery system may be disrupted. In areas that donot have IHS direct care hospitals to fall back onfor basic inpatient services, the budget effects ofhigh-cost cases can result in the deferral or denialof substantial amounts of contract care.
The problem of catastrophic costs in the IHScontract care program should not be confusedwith the subjects of catastrophic illness and cata-strophic health insurance as they generally are un-derstood in the field of health research. Cata-strophic costs usually refer to the devastatingfinancial effects that extremely costly and long-term illnesses can have on individuals who mayhave no insurance or who may be inadequatelyinsured. In the IHS contract care program, thecosts of catastrophic illnesses not covered by otherpayers are borne by IHS, not by individual In-dians (although there may be cases that are dis-puted between IHS and another payer as to whichis the responsible party, leaving the individual In-dian caught between the two). Catastrophic costsmost often are defined in terms of out-of-pocketcosts to individuals exceeding a certain percent-age of individual or family income, or as totalcosts per case in the range of $20,000 to $25,000and up. In IHS, on the other hand, the discus-sion of catastrophic costs has revolved around theidea of setting a threshold for individual serviceunit obligations somewhere between $10,000 and$20,000 per case.
The negative effects of high-cost cases on con-tract care program management have been felt forseveral years, and some IHS areas have takensteps to assist their service units in dealing withthe problem. The most frequently used mecha-nism is an areawide contingency fund that is with-held from the area’s annual contract care alloca-tion and made available to service units for caseswhose costs exceed a predetermined threshold.This approach currently is applied in the Alaskaand Portland IHS areas. Other areas have ex-pressed interest in setting an upper limit on theirobligation to pay for individual high-cost cases
(a cap was imposed in the Oklahoma City IHSarea until recently), but this approach has beendetermined to be illegal by the IHS general coun-sel (60).
Congress addressed the problem of high-costcases in the Indian Health Care Amendments of1984 (vetoed by President Reagan). A provisionearmarking the sum of $12 million for a cata-strophic health emergency fund was reintroducedin 1985 versions of the amendments. The fundwould be used to meet “the extraordinary medi-cal costs associated with the treatment of victimsof disasters or catastrophic illness falling withinthe responsibility of the Service” (133).
The proposed catastrophic fund would not beapportioned among the IHS areas and serviceunits, but would be administered by IHS head-quarters. The legislation provided that cata-strophic conditions would be defined solely interms of cost, not cause, by a threshold to beestablished between $10,000 and $20,000 per case,and all IHS costs above the threshold would beapplicable to the catastrophic fund. The fund wasseen primarily as a means of providing temporarybudget relief to area and service unit contract careprograms and to the contract care programs oper-ated by tribes under the Self-Determination Act(60).
Although the catastrophic fund was not citedas a reason for the President’s veto of the 1984Indian Health Care Amendments, Administrationofficials in testimony on the 1985 amendmentsstated their opposition to it. The Administrationposition was that separate authorization was notnecessary, because IHS already can shift resourceswithin its system to cover the costs of unusuallyexpensive contract care cases (136).
During congressional review of the 1984 IndianHealth Care Amendments, it was found that nei-ther the number of high-cost cases in the IHS serv-ice population, nor the costs, nor the causes ofthose cases could be documented. In response toquestions from Congress, IHS estimated that therewere about 400 cases in fiscal year 1983 for whichcosts of at least $25,000 per case were incurredby the IHS contract care program. The total costof those 400 cases to IHS was estimated at $15million. The amount of high-cost care for eligi-

240 ● Indian Health Care
ble Indians that was funded at least in part bythird-party payers, including Medicare, Medic-aid, and private insurance, could not be deter-mined. IHS suggested that trauma (especially fromautomobile accidents) accounted for a large num-ber of the cases, and that end-stage renal diseaseand neonatal intensive care represented cata-strophic costs when patients did not have third-party coverage (172). Because of this lack of in-formation to describe the IHS high-cost care prob-lem, OTA was specifically requested to addressthe matter.
Data on high-cost cases that have been obtainedfrom the IHS contract care program are incom-plete and poorly identified. Data items are not al-ways uniform in records from different areas, anddescriptive diagnoses have been reported by per-sons unskilled in extracting information frommedical records. It is not known if all cases meet-ing the selection criteria (an IHS obligation of$10,000 or more per case) were reported to head-quarters. Costs per case are incomplete becausemost area offices were able to provide hospitalcosts only. Thus, it is not possible to determinefrom available data whether what is called a prob-lem of catastrophic care is in fact a problem ofexcessive incidence of catastrophic conditions inthe Indian population, or whether it is more prop-erly described as a budget management problem.Lacking documentation of unusually high inci-dence rates, and because IHS itself defines cata-strophic cases strictly in terms of costs, it seemsmost useful for the present analysis to address thesituation as a budget management problem withinthe IHS contract care program.
Data on IHS High-Cost Cases
Special IHS Data Collection Activities
In the fall of 1984, possibly in anticipation ofpassage of the Indian Health Care Amendmentsand the consequent charge to IHS to implementthe catastrophic health emergency fund, staff ofthe IHS headquarters contract care program be-gan an informal data collection effort to identifyhigh-cost cases. This effort followed the steps out-lined below (86):
1. IHS headquarters searched the automatedcontract care billing files, known as the
2.
3,
4.
5.
“piggyback” data system, for all bills inwhich the IHS obligation for hospital chargeswas $10,000 or more (associated physicianfees, laboratory, pharmacy, operating room,and other charges were not included if billedseparately from hospital charges). This ini-tial search was performed during late Oc-tober and early November 1984 on the fileof processed fiscal year 1984 contract carebills. Inpatient stays for high-cost cases oftenexceed 45 days; thus it is likely that an un-known number of 1984 cases was missedbecause bills had not yet been filed andprocessed.Headquarters listed the bills by area, sent thelists to the IHS area offices, and requestedthat contract care authorization forms (HealthServices Administration forms 43 for in-patient care or 64 for other than inpatientor dental care) be pulled for each of the bills,photocopied, and returned to headquarters.No attempt was made at headquarters, thearea offices, or service units to aggregate allbills associated with the same patient andepisode of care (except, it has been reported,in the Phoenix and Alaska areas). This isanother factor that may contribute to an un-dercounting of cases costing the IHS $10,000or more.The IHS areas filled the headquarters requestas best they could given their different man-ual and automated contract care record sys-tems. As a result, there is variability in thedata items that each area could provide. Theservice units were involved in pulling thecontract care authorization forms for eachlisted bill.When the contract care authorization formswere received at headquarters, they werechecked against the lists of requested formsand edited informally; but there is no rec-ord of what followup activities, if any, werecarried out. Bills were excluded if they rep-resented payment for a block of services toa group of patients (a standing, negotiatedservice contract); for example, laboratoryservices for all service unit contract care pa-tients for the year.Individual high-cost case billing records thenwere entered into a personal computer sys-tem with a LOTUS program. The data items

Ch. 6—Selected Issues In Indian Health Care ● 241
6.
usually included IHS area; service unit; insome cases, the name of the private provider;a document identification number, if avail-able; one selected noncoded, nonstandard-ized description of the diagnosis or cause ofthe hospitalization; a description of oneselected procedure; the amount paid by IHSon the hospital bill; the amount paid by analternate payer, if available; and a total ofIHS and alternate payer expenditures. In-patient days per case were added in subse-quent requests for fiscal year 1982 and 1983records.The preliminary data set for fiscal year 1984consisted of 331 cases. IHS decided that inorder to support further analyses, additionalrecords were required. Following the sameprocedures outlined above, headquarters re-quested contract care authorization forms forhigh-cost cases in fiscal years 1982 and 1983.These records were received and entered inthe personal computer system beginning inApril 1985.
OTA staff performed preliminary analyses onthe 331 cases for fiscal year 1984 (the number ofcases grew to 390 by the time of the final OTAanalysis described later in this section). In responseto the interests of congressional committees andOTA’s Indian health advisory panel, OTA beganto work closely with IHS contract care programstaff to design a more complete and formal studyof high-cost cases. Negotiations regarding thisstudy went on from April through June 1985, andresulted in a methodology prepared by IHS thatwould manipulate automated data files to gener-ate information on the numbers, causes, and to-tal costs of the high-cost cases. During the sum-mer, however, it became apparent that althoughthe extensive reprogramming that would be re-quired for the study was feasible, it could not bedone by the IHS data center in Albuquerque. Theproject was referred to the PHS computer centerin Rockville for cost estimates. In September, dis-cussions with IHS staff made it clear that the workwould not be completed in time for inclusion inthe OTA study (45). At that time, OTA again be-gan to explore use of the high-cost case data col-lected by the IHS contract care program for fis-cal years 1982, 1983, and 1984, described above.
It should be understood that the informationpresented here is rough, but it is the best that wasavailable to describe high-cost cases in the IHScontract care program. Unfortunately, many ofCongress’ specific questions about total costs percase, the role of third-party payers, accurate anddetailed causes of these costly hospitalizations,and patient demographics cannot be answered onthe basis of the information at hand. Answers toquestions such as these are necessary before meth-ods of financing and insuring IHS high-cost casescan be seriously considered.
Analysis of the IHS High-Cost Case Data Set
The data presented here are the product of workwith the IHS file of 1,295 high-cost cases from fis-cal years 1982, 1983, and 1984 (123). Problemswith these data already have been noted: for ex-ample, there is no way to verify that all cases areincluded, and in fact there is evidence that some1984 cases were missed because the billing file wassearched so soon after the close of the fiscal year.A second search of the 1984 contract care billingfile in October 1985 generated 746 records of IHShospitalization disbursements exceeding $10,000(122). This more recent run of 746 records couldnot be closely compared with the 390 cases finallyidentified for 1984 by the IHS special data col-lection effort, but it represents a substantial in-crease over the number of cases included in thepresent analysis.
The reported costs in these cases are IHS dis-bursements for hospital care only. They do notrepresent total costs per case. Fiscal year 1984 dataon 37 catastrophic cases from the Portland IHSarea, if applicable to all areas, suggest that hos-pital costs alone make up about 84 percent of to-tal IHS expenditures for high-cost hospitalizations(198). The number of high-cost cases involvingIHS-eligible Indians whose bills were paid entirelyby a third-party payer cannot be identified by anyIHS data system; and if other payers left a resid-ual liability to IHS of less than $10,000, the casewould not have been selected for IHS special datacollection.
The relative completeness and accuracy of datareporting from IHS areas are not known, but thereare obvious gaps in the data. The California, Be-

242 ● Indian Health Care
midji, and Nashville IHS areas reported very fewcases, probably because much of the care in thoseareas is delivered by the tribes under self-deter-mination (Public Law 93-638) contracts, and datafrom 638 programs usually are not included in thecontract care “piggyback” data system that wasused for IHS case selection (58). Those same IHSareas also are particularly active in collecting fromthird-party payers, which may have reduced thenumber of cases that cost IHS more than $10,000.Finally, service units such as some of those in Cali-fornia (e.g., Toiyabe) may rarely if ever author-ize inpatient referrals, because of budget limita-tions, and by not incurring bills of $10,000 o rmore would not appear in the IHS special dataset. In Oklahoma, high-cost cases are under-reported because the contract care program in re-cent years attempted to impose a cap of $3,000per case, thereby reducing demands on the con-tract care budget.
The tables that follow present numbers of high-cost cases in the IHS data file for fiscal years 1982,1983, and 1984, respectively, by IHS area. Thecases are described with total costs for the area,average costs per case and, for fiscal years 1982and 1983, average inpatient days per case andaverage cost per inpatient day (Alaska did not re-port inpatient days, and so is excluded from thelast two items).
A total of $7.9 million was spent on hospitalcare for 381 cases identified in fiscal year 1982 (ta-ble 6-7). The average cost per case was $20,752,and the average inpatient stay was 30 days at $684per day. The highest average cost per case wasin Alaska, at $24,272, but the Phoenix area alsowas high at $23,934. IHS area office sources inPhoenix report that they attempted to match allcontract care bills associated with individual epi-sodes of care, possibly including more than onehospitalization per patient. All cases with cumu-lative IHS disbursements exceeding $10,000 perpatient per year were reported for Phoenix, whichmay explain in part the large number of cases fromthat area and their high average costs (61). Nocases at all were reported for 1982 from the Be-midji, Nashville, Oklahoma, California, or Tuc-son IHS areas. Because of the obvious differencesamong the areas in their responses to the IHSheadquarters data request, comparisons amongIHS areas should not be overemphasized.
Fiscal year 1983 (table 6-8) is the most completeannual data set in this analysis. IHS disbursementsfor high-cost hospitalizations totaled $10.8 mil-lion. There were 524 cases reported from all IHSareas except California and Tucson (although Be-midji, Nashville, and Oklahoma reported fewcases). The average cost per case was slightlylower than in 1982, at $20,549, and was associ-
Table 6-7.—High-Cost Cases in the IHS Contract Care Program, by Area, Fiscal Year 1982a
Number of Total Average Average inpatient Average cost/Area cases cost cost/case days/case inpatient dayAberdeen . . . . . . . . . . . . . . . 46 $ 831,629 $18,079 43 $423 –
Alaska b . . . . . . . . . . . . . . . . . 37 898,048 24,272Albuquerque. . . . . . . . . . . . . 24
— —401,015 16,709 28 591
Bemidji c . . . . . . . . . . . . . . . . — — —Billings . . . . . . . . . . . . . . . . . 50
— —1,072,103 21,442 29 733
California c. . . . . . . . . . . . . . . — — —Nashville c . . . . . . . . . . . . . . . —
— —— —
Navajo . . . . . . . . . . . . . . . . . . 74—
1,301,984 17,594 26 6 &Oklahoma c . . . . . . . . . . . . . . – — — —Phoenix . . . . . . . . . . . . . . . . .
—114 2,728,461 23,934 27 894
Portland . . . . . . . . . . . . . . . . 36 673,419 18,706 33 560Tucson c. . . . . . . . . . . . . . . . . — — — — —
IHS all areas. . . . . . . . . . . 381 $7,906,659 $20,752 30 $684aAverages have been computed by area. Cases without Inpatient days have been excluded from average inpatient day and average cost/day calculations.blnpatient days not available for Alaska.CN o data reported fr~ Bemidji, Nashville, Oklahoma, California, and Tucson.
SOURCE: U.S Congress, Office of Technology Assessment, with data from U.S. Department of Health and Human Services, Public Health Service, Health Resourcesand Servicas Administration, Indian Health Service, contract care program special data collection, fall 1984-spring 19S5,

Ch. 6—Selected Issues In Indian Health Care ● 243
Table 6-8.—High-Cost Cases in the IHS Contract Care Program, by Area, Fiscal Year 1983a
Number of Total Average Average inpatient Average cost/Area cases cost cost/case days/case inpatient day
Aberdeen . . . . . . . . . . . . . . . 74 $ 1,291,481 $17,452 35 $504Alaska b . . . . . . . . . . . . . . . . . 94 2,859,738 30,423 — —Albuquerque. . . . . . . . . . . . . 34 682,911 20,086 28 722Bemidji b . . . . . . . . . . . . . . . . 2 22,485 11,243 — —Billings . . . . . . . . . . . . . . . . . 89 1,750,740 19,671 26 758California c. . . . . . . . . . . . . . . — — — — —Nashville . . . . . . . . . . . . . . . . 2 58,782 29,391 42 700Navajo . . . . . . . . . . . . . . . . . . 76 1,653,086 21,751 22 987Oklahoma . . . . . . . . . . . . . . . 9 107,271 11,919 18 679Phoenix . . . . . . . . . . . . . . . . . 93 1,422,039 15,291 17 893Portland . . . . . . . . . . . . . . . . 51 918,985 18,019 36 507Tucson C . . . . . . . . . . . . . . . . . — — — — —
IHS all areas. . . . . . . . . . . 524 $10,767,518 $20,549 21 $707aAV~~~~~~ ha”~ b~~” ~Orn~ut~d by area cases without inpatient days have been excluded frOM average lnPtlent day and average costfday calculationsblnpatlent days not available for Bemidji and Alaskacf.Jo data repofled from California or Tucson.
S O U R C E ’ U.S Congress, Office of Technology Assessment, with data from U S. Department of Health and Human Serv!ces, Public Health Service, Health Resourcesand Serwces Administration, Indian Health Service, contract care program special data collection, fall 1984.spring 1985
ated with an average stay of 21 days for all areasexcept Alaska, compared with 30 days in 1982.The average cost per day was $707 in 1983, upfrom $684 in 1982. The range in average costs percase was wider than in 1982: excluding averagecosts in Bemidji, Nashville, and Oklahoma be-cause of incomplete reporting, the range was from$15,291 in the Portland area to $30,423 per casein Alaska.
Inpatient days were not reported by any of theareas in fiscal year 1984, and this is the year inwhich the greatest amount of case underreport-ing is suspected. Total hospital disbursementsassociated with the 390 cases were $8.5 million,well below the 1983 amount. Again, the smallnumbers of cases reported from Bemidji (nocases), Nashville, Oklahoma, California, andTucson distort data for those IHS areas. Table 6-9 shows that in 1984 the average cost per case wasnearly $22,000, ranging from about $15,000 percase in the underreported areas of Oklahoma,Nashville, and California to a high of $37,852 percase in Alaska. (Note that 1984 costs for Alaskaare somewhat higher than for other areas becausetotal expenditures, including hospital and somephysician charges, were reported instead of hos-pital costs alone. If the average cost per case inAlaska is reduced by the approximately 16 per-cent nonhospital costs found in Portland, theaverage cost per case would be about $32,000which, when deflated by 25 percent for the higher
Table 6-9.—High-Cost Cases in the IHS ContractCare Program, by Area, Fiscal Year 1984
Number of Total AverageArea cases cost cost/case a
Aberdeen . . . . . . . 56Alaska b . . . . . . . . . 69Albuquerque. . . . . 13Bemidji c . . . . . . . . —Billings . . . . . . . . . 85California d . . . . . . 1Nashville d . . . . . . . 4Navajo . . . . . . . . . . 66Oklahoma d . . . . . . 16Phoenix . . . . . . . . . 44Portland . . . . . . . . 29Tucson d . . . . . . . . 7
$ 903,8352,611,785
232,853—
1,766,29215,23258,640
1,169,000206,257764,571703,595113,494
$16,14037,85217,912
—20,78015,23214,66017,71212,89117,37724,26216,213
IHS ail areas . . 390 $8,545,554 $21,912aAVer”geS have been computed by area~For the rj9 cases from Alaska, reported costs include hospitalization and phy-
sician fees, In other areas, costs are for hospitalization onlyC NO data repofled f rom Bernidiidcalifornia, f.JaStlVille, C)klahoma, and Tucson retorting maY be incOrnPlete.SOURCE U S Congress, Office of Technology Assessment, with data from U S
Department of Health and Human Services, Publ!c Health Service,Health Resources and Services Administration, Ind!an Health Service,contract care program special data collection, fall 1984.spring 1985
costs of living in Alaska to $27,000, is closer tothe IHS average. )
Causes of the IHS High-Cost Cases
All IHS high-cost case records for fiscal years1982, 1983, and 1984 were combined for the dis-tribution of cases by cause presented in table 6-10. Nineteen individual cause categories are sub-totaled in seven groups: complications of preg-nancy, childbirth, and puerperium; infections;

244 ● Indian Health Care
Table 6-10.—High-Cost Cases in the IHS Contract Care Program, by Cause:All Cases, Fiscal Years 1982, 1983, and 1984a
Fiscal years 1982-83Fiscal years 1982-84 Average
Number Percent of Total Average Cases with inpatient Average cost/Causes of cases all cases costs cost/case inpatient days days/case inpatient dayComplications of pregnancy,childbirth, and puerperium . . . . . . 228 17,6 $ 6 , 7 4 9 , 1 0 6 $29,601 119 36 $ 694
1. Prematurity . ... . . . . . 167 12,9 5,489,332 32,870 76 39 6962. Congenital anomalies . . . . . . . . 25 1,9 539,102 21,564 21 37 6213. Neonatal complications
associated with delivery . . . . . 23 1.8 548,590 23,852 14 27 8404. Maternal complications . . . . . . . 13 1,0 172,082 13,237 8 21 662
Infections. ... ... ... . . . . . . . 141 10.9 2,704,798 19,183 82 27 666
5. Respiratory . . . . . . . . . . . . . . 59 4,6 1,214,978 20,593 31 27 7676. Other . . . . . . . . . . . . . . . . . . . . 82 6.3 1,489,820 18,169 51 27 605
Trauma . . . . . . . . . . . . . . . . . . . . . . . 307 23.7 6,093,984 19,850 182 29 623
7. Motor vehicle . . . . . . . . . . . . . . . 548. Violence . . . . . . . . . . . . . . . . . . . . 369. Other trauma. . . . . . . . . . . . . . . 174
10. Burns ... . . . . . . . . . . . . . . . . . 3811. Poisonings. ., ... ... . 5Malignancies (12.). . . . 64
Cardiovascular . . . . . . . . . . . . . . . 176
4.22.8
13.42.90.44.9
991,153695,830
3,322,7931,009,709
74,4991,412,204
18,35519,32919,09726,57114,90022,066
3421
10915
332
282331292329
703756587594569662
13.6 3,169,621 18,009 106 16 1,087
13. Heart . . . . . . . . . . . . . . . . . . . . . 138 10.7 2,517,485 18,243 83 14 1,25714. Vascular system (emboli,
aneurysms; including strokes) 38 2.9 652,136 17,161 23 24 719Digestive system (exceptinfections, malignancies) (15.) . . . 125 9.7 2,176,447 17,412 75 22 750
Other . . . . . . . . . . . . . . ... . . . . . . 254 19.6 4,913,571 19,345 164 30 638
16. Diabetes. . . . . . . . . . . ... . 14 1.1 234,618 16,758 11 24 74117. End-stage renal disease . . . . . . 24 1.9 389,854 16,244 19 21 826
18. Alcoholism . . . . . . . . . . . . . . . . . 4 0.3 96,645 24,161 3 32 86819. All others . . . . . . . . . . . . . . . . . . . 212 16.4 4,192,454 19,776 131 32 609
All causes . . . . . . . . . . . . . . . . . . 1,295 100.0 $27,219,731 $21,019 760 28 $ 695aAverages computed by cause and group of causes.SOURCE : u S. Congress, Office of Technology Assessment, with data from U.S. Depatiment of Health and Human Semices, Public Health Service, Health Resources
and Setices Administration, Indian Health Service, contract care Program special data collection, fall 1984-spring 1985.
trauma; malignancies; cardiovascular conditions;digestive system (other than infections and malig-nancies); and other. As noted above, the incon-sistent and incomplete nature of available diag-nosis and procedure descriptions made coding bycause difficult. The information is sufficiently im-portant, however, to consider even within theselimitations.
The distribution of cases by cause in the IHSdata set tends to confirm anecdotal reports aboutthe major causes of high-cost cases. As expected,trauma (23.7 percent of all 1,295 cases) andpremature infants (12.9 percent) were among theleading causes. (Trauma descriptions often wereinsufficient to sort as either motor vehicle acci-dents or violence, but it is believed that many ofthe “other trauma” cases are in fact attributableto those specific causes. ) Cardiovascular condi-tions, which included heart attacks and open heartsurgery, accounted for 13.6 percent of all cases;
infections also ranked relatively high, at 10.9 per-cent. Hospitalizations associated primarily withthe treatment of malignancies, diabetes, end-stagerenal disease, and alcoholism did not stand outas significant causes of high-cost care. In the caseof renal patients, great efforts are made at theservice unit and IHS area levels to ensure that In-dian patients are enrolled in the Medicare pro-gram, if eligible, so that IHS will not be liable forthis costly care (averaging at least $25,000 per di-alysis patient per year). For Indians who do notqualify for Medicare coverage, Medicaid pro-grams in most States pay for renal dialysis andtransplantation.
In addition to the number and percent of allcases in each cause category, table 6-10 presentsthe total and average costs associated with thecases by cause. These figures include data fromall 1,295 cases over 3 years. The total IHS expend-iture was $27.2 million, or close to $10 million

Ch. 6—Selected Issues In Indian— -
Health Care • 245
per year, and the average cost per case over the3-year period was $21,000. Average costs per casevaried by cause from a low of $13,000 to $14,000per case for poisonings and maternal complica-tions of pregnancy and childbirth, to a high ofnearly $33,000 per case for the care of prematureinfants. These average costs relate to averagelengths of stay by cause. Note, however, that be-cause inpatient days were not reported for 1984cases, the columns presenting average inpatientdays per case and average cost per inpatient dayby cause reflect only the 760 cases having thatdata item from 1982 and 1983 (Alaska excluded).Therefore, average days multiplied by averagecosts per day will not equal the column based on3 years’ data, average cost per case. The longestaverage stay by cause was 39 days for prematureinfants; infants with congenital anomalies also hadlonger than average stays, 37 days. The averagelength of stay for all 1982 and 1983 cases was 28days. Maternal complications, heart conditions,some trauma, digestive system problems, dia-betes, and end-stage renal disease were associatedwith shorter than average lengths of stay. Aver-age costs per inpatient day, by cause, variedaround $695 per day.
Because of differences in databases, it is diffi-cult to compare the distribution of IHS high-costcontract care cases, by cause, with all IHS hos-pitalizations, by cause, or with other IHS healthstatus indicators. For example, the OTA healthstatus analysis presented in chapter 4 found that6.1 percent of all Indian live births in all IHS areas(1980-82) were low birth weight infants. For U.S.women of all races (1981), 6.8 percent of all birthswere low birth weight infants (191). In 1981, theinfant mortality rate among Indians (13.3 per1,000 live births) exceeded that for the U.S. allraces, 11.9 per 1,000 live births, but was lowerthan the infant mortality rate of 17,8 per 1,000for nonwhite Americans (see ch. 4) (191). On thebasis of these figures, it is not possible to assertthat high-cost care for low birth weight infantsis a substantially greater or lesser problem in IHSthan in the general population.
As shown in chapter 4, the leading causes ofdeath in Indians residing in IHS service areas (age-adjusted mortality rates) are heart disease (166,7deaths per 100,000) and accidents (136.3 deaths
per 100,000). For accidents, chrome liver diseaseand cirrhosis, diabetes mellitus, pneumonia andinfluenza, homicide, suicide, and tuberculosis,age-adjusted mortality rates for American Indiansexceed rates in the general population. Compli-cations of pregnancy, childbirth and puerperium,and injuries and poisonings are the two leadingcategories of hospitalization for all IHS generalmedical and surgical patients, direct and contractcare combined (191). This is not inconsistent withthe pattern of high-cost hospitalizations, but be-cause of differences in coding, more detailed com-parisons are not useful.
Table 6-11 presents the 524 high-cost cases iden-tified for fiscal year 1983 distributed by the num-ber and percent of cases in each IHS area, by causecategory. Too much should not be made of thesedata because of the small numbers of cases re-ported by several areas, and because differencesin contract care authorization policies among theareas (which relate to funding levels and the avail-ability of direct care services) may affect the dis-tributions by cause more than actual incidenceof the conditions. No data were available in fis-cal year 1983 from California or Tucson, and thesmall numbers of cases included from the Bemidji,Nashville, and Oklahoma IHS areas make thosedistributions unrepresentative. The number anddistribution of high-cost cases from Albuquerquealso seems atypical. Some of the variations prob-ably are due to different medical coding habits,because “other” diagnoses categories ranged from6.4 percent of the cases in Alaska to 32.4 percentin the Albuquerque area, while 16.4 percent ofall cases were so coded throughout IHS.
Given these caveats, however, extreme varia-tions from the overall IHS distribution by causein individual IHS areas might indicate a need forfurther investigation. For example, in the Alaskaarea there appears to be a very high proportionof high-cost contract care cases due to complica-tions of pregnancy and premature births, 37.2 per-cent of the cases, compared with 20.6 percent ofthe 1983 high-cost cases throughout IHS. One ex-planation for this high rate might be the limitedobstetrical and neonatal care capabilities of Alaskabush hospitals and the high cost of transportingpatients to the Anchorage Indian medical center.Inquiry to the Alaska area office revealed that al-

246 ● Indian Health Care
Table 6-11 .—High-Cost Cases in the IHS Contract
IHS total Aberdeen Alaska Albuquerque
Causes Number Percent Number Percent Number Percent Number Percent
Complications of pregnancy, childbirth,and puerperium . . . . . . . . . . . . . . . . . . . . . . . 108 20.6 16 21.6 35 37.2 2 5.9
1. Prematurity . . . . . . . . . . . . . . . . . . . . . . . . 78 14.9 9 12.2 30 31.9 1 2.92.Congenital anomalies . . . . . . . . . . . . . . . 13 2.5 5 6.8 1 1.1 1 2.93. Neonatal complications associated
with delivery . . . . . . . . . . . . . . . . . . . . . . . 11 2.1 2 2.7 4 4.3 0 0.04. Maternal complications . . . . . . . . . . . . . 6 1.1 0 0.0 0 0.0 0 0.0
Infections . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59 11.3 14 18.9 9 9.6 2 5.9
5. Respiratory . . . . . . . . . . . . . . . . . . . . . . . . 26 5.0 5 6.8 6 6.4 1 2.96. Other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33 6.3 9 12.2 3 3.2 1 2.9
Trauma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 131 25.0 17 23.0 21 22.3 10 29.4
7. Motor vehicle . . . . . . . . . . . . . . . . . . . . . . 20 3.8 2 2.7 2 2.1 4 11.88. Violence . . . . . . . . . . . . . . . . . . . . . . . . . . . 14 2.7 2 2.7 2 2.1 2.99.0ther trauma . . . . . . . . . . . . . . . . . . . . . . . 78 14.9 9 12.2 10 10.6 5 14.7
10.Burns . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 3.4 4 5,4 7 7.4 0 0.011.Poisonings . . . . . . . . . . . . . . . . . . . . . . . . 1 0.2 0 0.0 0 0.0 0 0.0Malignancies . . . . . . . . . . . . . . . . . . . . . 30 5.7 2 2.7 10 10.6 3 8.8
Cardiovascular . . . . . . . . . . . . . . . . . . . . . . . . 63 12.0 7 9.5 7 7.4 4 11.8
13.Heart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46 8.8 1 1.4 6 6.4 3 8.814.Vascular system (emboli, aneurysms;
including strokes) . . . . . . . . . . . . . . . . . . 17 3.2 6 8.1 1 1.1 1 2.9Digestive system (except infections,malignancies) . . . . . . . . . . . . . . . . . . . . . 47 9.0 5 6.8 6 6.4 2 5.9
Other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86 16.4 13 17.6 6 6.4 11 32.4
16.Diabetes . . . . . . . . . . . . . . . . . . . . . . . . . . 2 0.4 0 0.0 0 0.0 0 0.017.End-stage renal disease . . . . . . . . . . . . . 11 2.1 1 1.4 0 0.0 3 8.818.Alcoholism . . . . . . . . . . . . . . . . . . . . . . . . 1 0.2 0 0.0 0 0.0 1 2.919. All others . . . . . . . . . . . . . . . . . . . . . . . . . . 72 13.7 12 16.2 6 6.4 7 20.6
All causes . . . . . . . . . . . . . . . . . . . . . . . 524 100.0 74 100.0 94 100.0 34 100.0a percen ts are calculated on columns to show distributionof cases by cause within the areas.bThere wereno data from California and Tucson.cData from Bemldjj, Nashville, and Oklahoma maY be incomplete.
SOURCE: U.S. Congress,Office of TechnologyAssessment, with datafrom U.S.Departmentof Health and HumanServices, Public Health Service, Health Resourcesand Services Administration, Indian Health Service, contract care program special data collection, fall 1984-spring 1985.
though field hospital limitations and consequenttransportation costs were a factor, the main rea-son that premature infants standout as high-costcases in the contract care program is that the An-chorage IHS hospital is capable of providingnearly all specialty services directly, includingtrauma care and a level II premature nursery, butneonatal cases requiring the most intensive carein a level III nursery (usually long-term ventila-tor patients) must be referred out under contractcare (112).
High-cost contract care cases due to infectionswere above the IHS average in the Aberdeen area;trauma referrals were somewhat high in Albu-querque; and in Billings, cardiovascular and diges-
tive system high-cost cases exceeded proportionsfound throughout IHS. In the Navajo area, com-plications of pregnancy, premature births, andtrauma were more frequently the causes of high-cost cases than in IHS generally. In Phoenix andPortland, on the other hand, high-cost referralsdue to complications of pregnancy and prematu-rity were well below IHS averages. These are thetypes of variations that would be worth explor-ing in a more complete and accurate data set.
Would a $12 Million Catastrophic Fund BeAdequate?
The Indian Health Care Amendments proposedin 1984 and 1985 would have provided for a cat-

Ch. 6—Selected Issues In Indian Health Care ● 247
Care Program by Cause and Area, Fiscal Year 1983a b
Bemidji c Billings Nashville c Navajo Oklahoma c Phoenix Port land
Number Percent Number Percent Number Percent Number Percent Number Percent Number Percent Number Percent
o 0.0 16 18.0 1 50.0 19 25.0 0 0.0 15 16.1 4 7.8
0 0.0 10 11.2 1 50.0 14 18.4 0 0.0 9 9.7 4 7.80 0.0 3 3.4 0 0.0 2 2.6 0 0.0 1 1.1 0 0.0
0 0.0 0 0.0 0 0.0 3 3.9 0 0.0 2 2.2 0 0.00 0.0 3 3.4 0 0.0 0 0.0 0 0.0 3 3.2 0 0.00 0.0 7 7.9 0 0.0 8 10.5 0 0.0 9 9.7 10 19.6000
0,00.00.0
25
20
000000
0.00.00.00.00.00.0
04
16003
2.25.6
22.5
0.04.5
18.00.00.03.4
000
0.00.00.0
44
2 3
000000
0.00.00.00.00.00.0
60
12503
5.35.3
30.3
7.90.0
15.86.60.03.9
0 0.00 0.03 33.3
0 0.00 0.02 22.21 11.10 0.00 0.0
5 5.44 4.3
24 25.8
3 3.23 3,2
18 19.40 0.00 0.05 5.4
37
13
5.913.725.5
326114
5.93.9
11.82.02.07.8
0 0,0 16 18.0 1 50.0 11 14.5 1 11.1 12 12.9 4 7.80 0.0 12 13.5 1 50.0 8 10.5 1 11.1 11 11.8 3 5.9
0 0.0 4 4.5 0 0.0 3 3.9 0 0.0 1 1.1 1 2.0
0 0.0 12 13.5 0 0.0 6 7.9 4 44.4 4 4.3 8 15.7
2 100.0 15 16.9 0 0.0 6 7.9 1 11.1 24 25.8 8 15.7
0 0.0 1 1.1 0 0.0 0 0.0 0 0.0 1 1.1 0 0.00 0.0 0 0.0 0 0.0 2 2.6 0 0.0 5 5.4 0 0.00 0.0 0 0.0 0 0.0 0 0.0 0 0.0 0 0.0 0 0.02 100.0 14 15.7 0 0.0 4 5.3 1 11.1 18 19.4 8 15.7
2 100,0 89 100.0 2 100.0 76 100.0 9 100.0 93 100.0 51 100.0—
astrophic health emergency fund of $12 millionto absorb costs to IHS service unit contract careprograms exceeding a threshold of between $10,000and $20,000 per case. The service unit would beresponsible for IHS expenditures up to the thresh-old amount, and then could turn to the nationalfund for the remainder of the bill. Table 6-12shows what the costs to such a catastrophic fundmight be, by IHS area, given fiscal 1983 high-costcase experience with hospital disbursements onlyand thresholds set at $10,000, $15,000, and$20,000. The effects of these thresholds were cal-culated separately for each IHS area, because withtheir different average costs per case, the areasmight expect varying levels of relief from the cat-astrophic fund. It may be noted that IHS areas
that now cannot afford to purchase much in-patient contract care, such as California and per-haps Bemidji, would not benefit from the specialfund because they cannot afford to spend up tothe threshold figure to qualify for catastrophicfund relief.
Based on 1983 high-cost case experience, if thethreshold were set at $10,000 per case, the cata-strophic fund would be tapped for at least $5.5million to cover IHS contract hospital expendi-tures alone. Areas with higher average costs percase, such as Alaska, could expect the most re-lief. If the threshold were set at $15,000, total out-lays would be $3 million, minimum, and 2 of 10IHS areas in the 1983 data set would not benefit

248 ● Indian Health Care
Table 6-12.—Hospitalization Costs to Catastrophic Fund at Various Thresholds, Fiscal Year 1983 Data.- —
Costs to fund if threshold at:a
Number Total Threshold Threshold ThresholdArea of cases cost $10,000 $15,000 $20,000
Aberdeen . . . . . . . . . . . . . . . . 74 - $ 1 , 2 9 1 , 4 8 1 $ 551,481 $ 181,481 $ –Alaska. . . . . . . . . . . . . . . . . . . . . 94 2,859,738 1,919,738 1,449,738 979,738Albuquerque . . . . . . . . . . . . . . . 34 682,911 342,911 172,911 2,911Bemidji b . . . . . . . . . . . . . . . . . . . 2 22,485 2,485Billings . . . . . . . ... , . . . . . . . .
— —89 1,750,740 860,740 415,740
California c . . . . . . . . . . . . . . . . . —
—— —
Nashville b. . . . . . . . . . . . . . . . . .— —
2 58,782 38,782 28,782 18,782Navajo. . . . . . . . . . . . . . . . . . . . . 76 1,653,086 893,086 513,086 133,086Oklahoma b . . . . . . . . . . . . . . . . . 9 107,271 17,271Phoenix . . . . . . . . . . . . . . . . . . .
— —93 1,422,039 492,039 27,039
Portland . . . . . . . . . . . . . . . . . . .—
51 918,985 408,985 153,985Tucson c . . . . . . . . . . . . . . . . . . . —
—— — — —
IHS all areas . . . . . . . . . . . . . 524 $10,767,518 $5,527,518 $2,942,762 $ 1 , 1 3 4 , 5 1 7 –
%oststo the catastrophic fund by area precalculated by multiplying the threshold amount by the number of cases and subtracting that result from the total costof the cases in 1983
bflepo~ing from Bemjdj~ Nashville, and Oklahoma maY be incomplete.Cf.Jo data were reportecI for Cal!fornla Or Tucson
SOURCE: U.S Congress, Office of Technology Assessment, with data from U.S Department of Health and Human Services, Public Health Service, Health Resourcesand Services Adminlstratlom, Indtan Health Service, contract care program special data collection, fall 19i34.spring 1985
at all. A $20,000 threshold would reduce demandson the catastrophic fund to about $1.2 million andassist only 4 of 10 areas.
The figures in table 6-12 represent IHS disburse-ments for hospital charges only, but in practicethe catastrophic fund would cover all chargesabove the threshold. It is useful, therefore, to at-tempt to estimate the amounts of additional, non-hospital costs that would be covered by the fund.IHS data on which to base such estimates arelimited. The Portland IHS area was able to pro-vide expenditures for its recent high-cost casesbroken down by billing cost center. Data for 37cases paid out of the 1984 Portland area cata-strophic contingency fund showed hospital chargesto be 84 percent of total disbursements. Physicianservices associated with inpatient care but billedseparately represented 14 percent, and all othercharges to the contract care program for out-patient physician services, outpatient X-rays,drugs, supplies, and soon amounted to 2 percentof the total (198). Physician services at 14 per-cent of total hospital-related costs per case seemlow, especially in view of data from nationalhealth expenditure studies that show physicianfees at about 22 percent both of all health expend-itures and of all expenditures related to inpatientcare (36). The difference may result from howphysician services are billed: it is likely that the
services of some hospital staff physicians are in-cluded in hospital bills to the IHS contract careprogram (58).
Portland IHS officials have estimated physiciancosts associated with hospitalizations in the area’soverall contract care program to be as high as 30percent (107). IHS headquarters program statis-tics staff report that for the IHS contract care pro-gram in fiscal year 1984, physician fees repre-sented about 25 percent of total contract hospitalexpenditures per case; and that proportion appliedto the Portland area as well (58). Table 6-13 sum-marizes the effects of these estimates of additionalnonhospital charges on the potential costs to anIHS catastrophic fund at thresholds of $10,000,$15,000, and $20,000.
It is important to note that the base figures usedin table 6-13 are taken from table 6-12, whichpresents the effects of three cost-per-case thresh-olds on numbers of IHS high-cost cases identifiedin 1983, in 1983 dollars. For a number of reasons,the 1983 data set may not include all high-costcontract cases; and it is known that only contracthospital disbursements are reflected in the costfigures. Even with these reservations, and withthe inclusion of estimated nonhospital costs rang-ing from 16 to 30 percent, according to the cal-culations in table 6-13 it appears that in 1983 a

—
Ch. 6—Selected Issues In Indian Health Care ● 249
Table 6-1 3.—Estimated Total Costs to the IHS Catastrophic Fund at Different Thresholds,Based on Fiscal Year 1983 Experience
Number of fiscal year 1983 cases for which IHS hospital expenditures per case exceeded $10,000: 524 cases
Total IHS hospital expenditures for the 524 cases in fiscal year 1983: $10,767,518
Estimated costs to fiscal year 1983 catastrophic fundEstimated total IHS disbursements for 524 cases, for 524 cases with threshold set at:
adding physician inpatient charges $10,000 $15,000 $20,000at 16°/0 of totala = $12,818,473 - $7,578,473 - $ 4 , 9 5 8 , 4 7 3 — $2,338,473at 22°/0 of totalb = $13,804,510 $8,564,510 $5,944,510 $3,324,510at 30°/0 of totalc = $15,382,168 $10,142,168 $7,522,168 $4,902,168aportland area ijata for 37 cases paid from 1984 cata.strophlc contingency fund 16 percent of total IHS disbursements for those cases were for other than hospital
charges, e g , phystclan services to inpatients billed separately, and outpatient chargesbR M G,bson and D R Waldo, Nat,onal Health Expenditures, 1981, ’ Hea/th Care F(nan~(ng ~evfe~ 4(1) 1.35, septernber 198P phystctan fees represent approximately
22 percent of all expenditures related to inpatient carecportland area IHS Officials estimate physician fees associated with inpatient services in the area’s total contract care Pr09ram at a maximum ~ Percent This ‘Igh
est I mate is supported by I HS headquarters Program Statistics Branch staff physician fees represent about 25 percent of total contract hospital expenditures percase throughout I HS and In the Portland area
SOURCE U S Congress, Office of Technology Assessment, w!th data from U S Department of Health and Human Services, Publlc Health Servtce, Health Resourcesand Services Adminlstrat~on, Indian Health Serwce, contract care program special data collection, fall 1984-spring 1985, and assumptions cited In notes, above
$12 million catastrophic fund probably wouldhave been adequate to meet expected demands onit, whether the threshold was set at $10,000,$15,000, or $20,000.
In a high-cost contingency fund that could be-come available no earlier than fiscal year 1986,however, the effects of 3 years’ health cost infla-tion could be substantial. A threshold of $10,000per case would include more of the total IHS con-tract care cases in 1986 than in 1983, based onincreases in billed charges alone. With contracthospital charges inflated at private sector rates,a fund of $12 million would not go as far in 1986as in 1983. Problems in identifying high-cost caserecords to make up the data sets for this analysissuggest that undercounting of cases may be con-siderable. There were 524 cases identified for fis-cal year 1983 and, originally, 390 cases for 1984.When the 1984 billing file was searched again inOctober 1985, however, 746 high-cost case rec-ords were found. Such uncertainties about thenumbers of high-cost cases that may be expectedannually justify concerns for the adequacy of a$12 million fund. Finally, in most IHS areas (ex-cepting perhaps Alaska and Portland), high-costcases in tribally operated 638 contract care pro-grams have not been included in IHS contract careprogram data systems. If the catastrophic fundis implemented as proposed, 638 contract careprograms would be eligible to use it along withIHS-administered contract care programs. No in-formation is available at present to estimate thenumbers of additional cases that could draw on
the high-cost case contingency fund from 638 con-tract care programs.
Managing High-Cost Cases inthe IHS Contract Care Program
Although high-cost cases are known to havenegative effects on the delivery of contract carein most IHS areas, at present there is no head-quarters policy or program designed to help easethis problem. A headquarters level contingencyfund similar to programs operating in the Alaskaand Portland IHS areas apparently has been con-sidered, but has not been implemented becauseof fears that it would be politically unworkable.IHS maybe relying on the proposed catastrophichealth emergency fund to relieve pressures on itscontract care budgets. Reauthorization of the In-dian Health Care Improvement Act would be nec-essary, however, and there still would be difficul-ties in establishing a system to administer sucha program.
In the meantime, headquarters has developedno special policies or guidelines for the areas andservice units, but has delegated responsibility forhigh-cost case management to those field offices.Headquarters becomes involved only if there isan extraordinarily expensive case, such as a childrequiring liver transplantation for biliary atresiaor an accident with multiple burn victims. Head-quarters then may attempt to reprogram funds toassist in paying for such cases. Like other Federalhealth programs, IHS does not authorize payment

250 ● Indian Health Care
for treatments judged to be experimental, i.e.,liver transplants for other than biliary atresia,heart transplants, pancreas transplants, and otheremerging procedures.
IHS area offices of necessity have tried to dealwith the effects of high-cost cases, and they haveapproached the problem in a number of ways.Perhaps the most effective is the areawide cata-strophic contingency fund approach. The Alaskaarea office has been withholding a contingencyfund for many years, and 638 programs partici-pate in the fund on the same terms as IHS-oper-ated contract care programs. A fund of between$2 and $3 million was withheld in fiscal year 1985.The threshold was raised from $5,000 per case to$15,000 per case in mid-1984. Alaska works ag-gressively to collect from third-party payers asanother means of reducing its contract care ex-penditures (8).
The same management approach is applied inthe Portland IHS area, where there are no IHSdirect care hospitals and all inpatient services notcovered by other payers must be purchased bythe contract care program, A labor-intensive man-ual system of monitoring costly cases has beendeveloped there, and as noted earlier, disburse-ment reporting by cost center is maintained. Thereis general agreement among Portland area tribesthat the fund has improved the situation, but pres-sures on contract care budgets still are extreme.Also, the contingency fund has the disadvantagethat if too much is put aside for high-cost casesthat do not occur, then a substantial amount ofmoney has been withheld from service unit con-tract care programs, and needed services mayhave been denied or deferred to stay within theservice unit’s allocation. If the catastrophic de-mand is less than expected, the Portland areaspends contingency funds remaining at the endof the year on lists of deferred contract care cases.
The Oklahoma City IHS area removed its con-tract care cap of $3,000 per case in April 1985 andinstituted a catastrophic fund. The area has setaside 5.3 percent of its contract care allocation,or $600,000 in fiscal year 1985, to be availableto its service units (excluding the Pawnee BenefitPackage Program and 638 contract care pro-grams). Written guidelines specify a threshold of
$15,000 total costs per case, which raises the ques-tion of whether all service units would want toparticipate because of the requirement to spendup to the $15,000 threshold (197).
Contract care program policies for managinghigh-cost cases have not been studied in detail inall IHS areas. It has been reported that serviceunits in areas without contingency funds attemptto manage their programs by monitoring expend-itures closely against their quarterly budget allo-cations. Other factors that affect service unit costsfor catastrophic care include the extent to whichalternate resources (third-party payers) are avail-able and pursued. Areas with IHS hospitals canreduce their expenditures in high-cost cases byproviding care in IHS facilities before and afterreferral to contract providers. This is not an op-tion in all areas, however, and the capabilities ofavailable IHS hospitals affect the usefulness of thisapproach.
Conclusions
The question is, how can the IHS contract careprogram best manage and pay for high-cost carefor its service population? If the problem is pri-marily one of budget management, the feasibil-ity of implementing programs such as the contin-gency funds in the Alaska and Portland IHS areasmight be considered for all IHS areas. Private re-insurance is not a realistic option at this time be-cause IHS lacks adequate data to describe theextent of the problem: data on patient demo-graphics, numbers of high-cost cases, and causesare inadequate or nonexistent. The population atrisk and the numbers of high-cost cases even atthe national level may be too small for privatereinsurance; and most insurance plans are de-signed to protect individual patients from exces-sive costs of care, not public program budgets.Information to describe the contributions of otherthird-party payers in IHS contract care is com-pletely inadequate, and this certainly would af-fect any plans for reinsuring the program pri-vately.
The most feasible interim approach to easingthe problem of high-cost cases in the IHS contractcare program may well be something along the

—
Ch. 6—Selected Issues In Indian Health Care ● 251
lines of the proposed revolving fund. It would rec-ognize the immediate problem, budget effects, andwould seek to deal with it within the program’sexisting budget framework through uniform na-tional administrative policies. Such a fund wouldprovide some relief to contract care budgets andto Indians requiring contract care in some IHSareas. In other areas, however, contract care fund-ing already is inadequate to permit the area tospend up to the $10,000 to $20,000 threshold inorder to take advantage of the contingency fund.This problem might be overcome by adjusting thethreshold to reflect differences in costs of careamong IHS areas.
Finally, it is not realistic to expect high-costcases to be managed effectively in health deliv-ery systems as small as many IHS service units.Some service units have eligible populations un-der 10,000 and contract care budgets of severalhundred thousand dollars to pay for a year’s serv-ices. The IHS policy of decentralizing responsi-
IHS DATA MANAGEMENT ISSUES
It has not been the purpose of this OTA assess-ment to conduct a complete and systematic evalu-ation of IHS management practices and informationsystems. Nonetheless, after a year’s experience inworking with a variety of IHS offices and staff(primarily at or through IHS headquarters) to ob-tain data for the Indian health services analysis,some general observations about IHS data sys-tems may be made.
IHS depends on an array of uncoordinatedservice-specific data systems that has developedover the years in response to particular informa-tion needs. None of the IHS data systems has beendesigned specifically to provide consistent, relia-ble information for national program manage-ment and reporting requirements. IHS’s delega-tion of many management responsibilities to itsarea offices has contributed to a lack of incentivesto establish uniform national data systems, a sit-uation that continues to exist in 1985. Althoughthere has been recent recognition in IHS of theneed for national data, and planning efforts tomeet those needs are underway, the efforts arenot near to producing results.
bility for health care delivery to the service unitlevel, including management of contract services,is contradictory to the principle of sharing the riskfor exceptionally costly cases.
There may be some question as to whether allIHS area offices have large enough contract carebudgets to effectively manage high-cost cases.Some areas are attempting to make budget ad-justments among their service units for these un-expected costs, with some success; but this is be-ing done at the expense of funding for the overallcontract care program. An additional fund forhigh-cost cases would assist some of these areas.If an acceptable formula could be developed forallocating an IHS high-cost contingency fundamong the areas, it might be worth consideringwhether the fund would be administered more ef-fectively at the IHS area office level than at head-quarters, because the area offices are most famil-iar with their contract providers and with themanagement problems involved.
One example of how IHS data systems are notdesigned to respond to national policy and man-agement questions relates to the proposed $12 mil-lion catastrophic health emergency fund (see thepreceding section of this chapter on high-costcases). In considering reauthorization of the In-dian Health Care Improvement Act in 1984,which included the catastrophic fund, congres-sional committees requested data to describe theproblem of high-cost cases in the IHS contract careprogram. IHS responded with an estimate of 400cases annually costing $25,000 or more, anecdotalreporting of the causes, and no actual case countsby area or total. There was an ad hoc attempt atdata collection late in 1984, followed by devel-opment of a detailed plan to manipulate existingIHS data files, which was not implemented. Byfall 1985, OTA had obtained three different listsof fiscal year 1984 cases that reportedly had costIHS $10,000 or more, generated from various IHSdata systems and ranging in number from 390 tonearly 750 cases. Over a year after the initial con-gressional request,duce reliable basiccost cases.
IHS still was unable to pro-descriptive data on its high-
52-805 0 - 86 – 9

252 ● Indian Health Care
Many existing IHS data systems do not gener-ate complete and consistent information for all12 IHS areas. Some of the systems are automated,some are not; some systems are automated in cer-tain IHS areas but not in others. Little effort hasbeen made in the automated systems to use hard-ware and software that are compatible among theareas, and this has created unnecessary compli-cations and expenses in attempting to aggregatedata from the different area systems. Service-specific IHS cost data are virtually nonexistent be-cause facilities and programs operate within an-nual budgets, but are not otherwise required toaccount for or report detailed annual operatingcosts .
The Patient Care Information System (PCIS)is an example of the lack of consistency amongIHS area data systems. The PCIS, which is per-haps the most ambitious automated data systemto be developed in IHS, has been implemented inonly 3 of 12 areas (Tucson, Alaska, and Billings),reportedly because of its high implementation andoperating costs. An outside consultant’s evalua-tion of the system in 1984 found that the total costof operating PCIS in three areas was about $2,4million per year, or $3.00 per encounter, in com-parison with $0.80 per encounter for data report-ing to the Ambulatory Patient Care system thatexists in other IHS areas (55), The consultants alsofound substantial differences in PCIS operatingprocedures among the three areas, including useof a different basic encounter form in Billings, andsignificant delays in Alaska and Billings betweenpatient encounter and data availability comparedwith on-line data retrieval and flexible report gen-eration capabilities in Tucson, the area where thesystem first was developed and implemented in1975. Two points may be made in this example:first, an expensive automated patient data systemwas implemented without consistency in only 3of 12 IHS areas; and second, the system was notdeveloped by IHS headquarters to meet nationalprogram management needs, but by one of theareas (Tucson) to meet its own particular researchinterests.
Even in IHS data systems that are used to mon-itor and report on the national program (in theIHS Chart Series Book, for example, or in annualbudget justification documents), IHS headquar-
ters does not take an active role in defining datareporting procedures, ensuring consistency amongthe areas, and validating the completeness andaccuracy of data reporting. Beyond the minimalcomputer edits that are run on some incomingrecords, it is IHS headquarters policy to acceptdata as reported by the areas. In the IHS contractcare “piggyback” data system that maintains ex-penditures by cost center and object class, forexample, flexibility is allowed to the areas inaccounting the costs of services delivered undercontract, but in an IHS facility, as either a directcare or contract care program cost.
Another major impediment to the generationof complete and consistent IHS data is the exemp-tion of self-determination (638) contract programsfrom IHS data reporting requirements. Tribal 638contractors may voluntarily elect to participatein existing IHS data systems, using IHS data col-lection forms. Such participation has not been re-quired, however, and most 638 contractors do notoperate within IHS data systems. This loss of clin-ical, utilization, and management data due to thenonparticipation of 638 contractors is a seriousproblem now and will become more serious asmore services are transferred to tribal manage-ment, as is the expressed intent of the Adminis-tration and Congress. IHS recognized the need tocorrect this problem and issued a memorandumin November 1985 requiring uniform reporting forinpatient services, ambulatory medical services,and contract health services with standard IHSrecord formats from all new and renewal 638 con-tracts, effective immediately (50).
Currently, 20 to 30 percent of the total IHS clin-ical services budget is administered by the tribesunder 638 contracts. Many tables in this reportthat present IHS data are noted to be incompletebecause of the absence of data from 638 contrac-tors. Interpretation of some data sets is furthercomplicated by the fact that IHS area reportinggaps due to 638 contracting vary in their impor-tance, because the level of 638 contracting by areavaries considerably. Data for the California area,where most IHS services are delivered under 638contracts, are particularly affected by this non-reporting problem. The Nashville and Bemidji IHSareas, also active in 638 contracting, are also af-fected. In providing data on all 12 areas, IHS gen-

Ch. 6—Selected Issues In Indian Health Care Ž 253
erally does not attempt to correct or adjust fordata gaps such as these.
OTA staff had difficulty obtaining data fromIHS headquarters to describe the 638 programeven in simple terms (e.g., numbers of active con-tracts and dollar amounts, by area). The admin-istration of 638 contracts is viewed entirely as anarea office responsibility, and therefore the col-lection, maintenance, and analysis of data to mon-itor 638 contract performance are area office func-tions. Information reported in the IHS ChartSeries Book is for total IHS only, not by area; andit is not clearly indicated that in some tables “tribalcontracting” includes both 638 and Buy Indiancontracts (191). IHS sources have expressed res-ervations about the Tribal Resource and Assis-tance Information System data used in some ChartSeries Book tables, because contracts are not al-ways removed from the file when they expire, re-sulting in overstatement both of numbers of con-tracts and of dollar amounts (details of these dataproblems were described earlier in this chapter)(216). In late 1985, the lack of basic informationon the scope of the 638 contract program led IHSto conduct a survey of all tribes to collect accurateinformation on active contracts, dollar amounts,638 project staffing, and other matters. The re-sults of that survey were not available to thisstudy, but an interim report on the project waspublished in February 1986 (186).
IHS data systems are especially weak when itcomes to data on the costs of providing specifichealth services through different IHS programsand facilities to different population groups. Be-cause IHS must pay private providers for serv-ices authorized to IHS-eligible Indians under thecontract care program, reasonably accurate dataon those expenditures (not costs) by cost centerand object class are maintained in the IHS con-tract care “piggyback” data system (part of theHRSA-PHS financial accounting system) (58). Butcost accounting data relative to services deliveredby IHS direct care facilities are not requested ormaintained either by IHS area offices or by head-quarters. As a result, IHS is unable to determinein any detail how much it costs to provide a par-ticular package of services in a given area.
This lack of information to describe the costsof IHS direct services is an obstacle to 638 con-
tracting, because it leaves open to dispute theamount of contract funding that should be trans-ferred to tribal control. The lack of cost informa-tion also makes it difficult for IHS to compare thecosts of directly providing a service with the costsof buying it from the private sector under con-tract, thus undermining the ability of programmanagers to make cost-effective decisions aboutservices delivery.
IHS is not required by law or regulation to pro-vide a uniform package of health services to eligi-ble Indians throughout the country. Therefore,it has not been necessary to collect data nation-ally that could be used for national or area-specifichealth services planning. IHS headquarters andarea offices do not plan services delivery on thebasis of epidemiologic or socioeconomic data foreligible or user patient populations. Data systemssuch as the PCIS are designed for clinical man-agement purposes; but they are not implementedthroughout IHS, and the data they generate arenot applied to services planning or administration.Data supporting the RRM system relate man-power needs to service-specific workloads. Al-though this type of service planning goes intopreparations for new or replacement facilities con-struction, RRM-based estimates of resource needsdo not affect budget allocations among the areasexcept in the small equity fund distributions. Tosome degree, IHS services are delivered in re-sponse to expressed demand (historical utilizationpatterns); but this is not the result of planningbased on a population’s defined health problemsand needs.
It is likely that much more information couldbe derived from existing IHS data systems thancurrently is being sought and used. It appears thata great amount of data is being collected by IHSand its areas, but there is no overall frameworkor purpose guiding that data collection. The IHSOffice of Program Statistics, for example, pro-duces a variety of reports that could be useful toprogram management; but while the informationmay figure in the annual budget justification orin new facility plans, it is not applied systemati-cally for program management purposes.
An assessment and coordination of existing datasystems could be undertaken as an interim solu-tion, while plans are made for implementation of

254 ● Indian Health Care
a more rational and cost-effective national sys-tem. Where resources for services delivery are seenas chronically inadequate, however, as in IHS,any funds spent on data systems are likely to beviewed as better spent on direct services. Whenit comes to the data collection and reporting thatmust take place in the service units and IHS areaoffices, where staff may feel overworked already,resistance to additional demands and lack of timemay undermine complete and accurate data re-porting. Attitudes and work priorities such asthese might be modified by intensive managementefforts to define and demonstrate the usefulnessof the information.
In times of stable or declining IHS budgets,pressures to spend every available dollar on di-rect service delivery will be great. The payoff forbetter management data will have to be found inincreased program efficiency and effectiveness:getting more services for the same dollars by bettermanagement. This might require staff expertisenot widely available in IHS (and which might beparticularly limited in future supply under Indianpreference in hiring regulations as IHS Indianmanpower development funds are reduced).
IHS has acknowledged its data systems prob-lems and is working toward improvements. Since1980, IHS headquarters has taken a greater inter-est in data systems for management purposes bycreating a high-level staff position for manage-ment information systems and appointing two adhoc data system advisory committees. In springof 1982, a new in-house group at IHS began todefine and investigate the issues involved in a datasystems master plan (this was the Service UnitAutomation Task Group). In February 1983, adocument titled “Planning for an InformationManagement System” was produced. Althoughthat document was judged too abstract to serveas an implementation plan, it recommended thatIHS work with General Services Administrationconsultants to develop the implementation plan,and that recommendation culminated in an inter-agency agreement with the General Services Ad-ministration in June 1983. The IHS liaison groupdesignated to work with the General ServicesAdministration, the IHS Information SystemsStrategic Planning Task Force, produced a firstiteration of the 5-year strategic information plan
for implementation beginning in fiscal year 1984.The task force’s review of existing IHS data sys-tems and its approach to information managementwas quite critical. It found (49):
IHS data systems were large and unwieldy,tended to collect large volumes of data with greatredundancy and without clear purpose, were ex-pensive, and most important, only partially suc-ceeded to produce information that was usefulin the field for patient care and program man-agement, or in headquarters for policy decisionsand response to concerns of higher levels of theFederal Government.
The task force proposed a plan to guide futureadministration of information systems in IHS.Data systems should be able to evolve to meetchanging needs; information activities should re-late clearly to IHS objectives; the plan should pro-mote coordination and control of existing and newsystems; and the system should be a distributeddata processing framework to promote local con-trol. Implementation of such a system would re-quire strong top management support and clarifi-cation of relations and responsibilities betweenarea offices and headquarters.
Late in 1985, work continued in IHS to developdetailed specifications for the outputs, hardware,and software needs of the new strategic informa-tion system, known as the Resource and PatientManagement System (219). Funding for systemdevelopment and operation is not assured, but theAdministration’s fiscal year 1987 IHS budget pro-posal includes $2,5 million for data system sup-port (178).
In summary, as budgets become more con-strained there will be pressures within IHS to di-rect all available funds to direct patient services,rather than to functions viewed as peripheral andsupportive, such as data systems. The balancingof these conflicting demands will not be easy. Inview of the uncertain outcome of these conflictsand of the continuing inability of IHS data sys-tems to respond to clinical and program manage-ment information needs, much more could bedone to improve and coordinate existing data sys-tems to generate usable information for the in-terim. In spite of the clear need for improved IHSdata capabilities, it may be overly optimistic toexpect adequate funding for development and im-

Ch. 6—Selected Issues In Indian Health Care ● 255
plementation of a new, state-of-the-art manage- mated costs of implementing a new, comprehen-ment information system. The question might be sive data system? It is likely that money could beasked, however, at what cost are so many par- saved by careful integration of existing systems,tially redundant data systems being maintained, and that would seem to be a realistic goal for theand how would those costs compare with the esti- immediate future.

Appendixes

Appendix A
Americanthe U.S.
Aberdeen Area
IndianCensusIndian
and Alaska Native Population Estimates ofBureau, Indian Health Service, Bureau ofAffairs, and Tribes
A.1980 1980 IHS 1980 BIA
State of Iowa:1. Sac and Fox (non-SU) -- 658 -- --
a. Sac and Fox of the Mississippi 492 -- 695 9751
State of Nebraska:1. Omaha-Winnebago SU -- 3,849 -- --
a. Omaha Tribe of Nebraska 1,275 -- 1,469 3,0001
b. Winnebago of Nebraska 1,140 -- 1,143 2,0451
State of North Dakota:1. Fort Berthold SU
a. Three Affiliated Tribes3,037
--2,640-- --
3,194 6,0552
2. Fort Totten SUa. Devil’s Lake Sioux
2,681--
--2,261
-- --2,916 2,1871
3. Fort Yates SUa. Standing Rock Sioux
5,528--
--4,800
-- --7,958 6,7891
4. Turtle Mountain SU (Belcourt)a. Trenton-Williston (West ND)b. Trenton-Williston (MT)c. Turtle Mountain Chippewa
7,744------
--. -. -
4,021
-- --1,214 --
363 --8,656 21,0071
State of South Dakota:1. Cheyenne River SU (Eagle Butte Hosp.) --
a. Cheyenne River Sioux 1,5294,801
--- - --
4,449 8,5001
3,3602. Pierre SU --a. Crow Creek Sioux 1,474b. Lower Brule Sioux 850
-- --2,091 2,700
988 1,405----
14,5323. Pine Ridge SU --a. Oglala Sioux 11,946
--
--13,417 18,000 5
-- 12,753 1--
4. Rapid City SU --a. Rapid City Health Board --
3,637--
-- ---- --
5. Rosebud SU --a. Rosebud Sioux 5,688
7,455--
-- --9,484 15,0332
259

260 ● Indian Health Care
Aberdeen Area1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Service POP, Resident POp. Tribal6. Sisseton-Wahpeton SU -- 3,664 --
a. Sisseton-Wahpeton Sioux 2,700 -- 4,054 6,1401
b. Flandreau Santee Sioux 158 -- 413 5761
7. Yankton SU -- 2,307 -- --a. Santee Sioux of Nebraska 420 -- 434 2,0001b. Yankton Sioux 1,688 .- 2,531 3,6001
ABERDEENAREA TOTAL 43,082 63,253 65,469 112,765
B. Alaska Area1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Service POD. Resident POD. Tribal
State of Alaska*:1. Anchorage SU
a. Aleutian-Pribilof Is. Assn.b. Cook Inlet Native Assn.c. Copper River Native Assn.d. Kanaitze Indian Communitye. Northern Pacific Rimf. Kodiak Area Native Assn.
1 7 , 5 4 4 --1,889
10,324--
--------------
----
----
----
----
----
------
----
----
------------
----
2,477
9819
--2. Annette Island SU
a. Metlakatla-.
942--
976
3. Barrow SUa. N. Slope Borough H.C.
2,600--
----
----
4. Bristol Bay SUa. Bristol Bay H.C.
3,688--
----
--4,003
5. Interior SUa. Tanana Chiefs
6,759--
----
--6,514
6. Kotzebue SUa. Mauneluk (Maniilaq)
4,547--
----
--4,426
7. Mt. Edgecumbe SUa. Ketchikan Indian Corp.b. SE Alaska Reg. H.C.
9,782----
------
------
8. Norton Sound SUa. Norton Sound H.C.
5,174--
----
----
9. Yukon-Kuskokwim Delta SUa. Yukon-Kuskokwim H.C.
13,953--
-.-.
----
ALASKAAREA TOTAL 942 64,047 30,609 --
* Census data include Indians on reservations only of which Alaska has only one.

App. A —American Indian and Alaska Native Population Estimates of the U.S. Census Bureau, IHS, BIA, and Tribes ● 261
c . Albuquerque Area1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Service Pop. Resident POD, Tribal
State of New Mexico:1. Acoma-Canoncito-Laguna SU
a. Acoma Pueblob. Canoncito Navajoc. Laguna Pueblo
2. Albuquerque SUa. Alamo Navajob. Albuquerque Service Areac. Isleta Pueblod. Jemez Puebloe. Sandia Pueblof. Santa Ana Pueblog. Zia Pueblo
3, Mescalero SUa. Mescalero Apache
4. Santa Fe SU
::c.
d.e.
Cochiti PuebloJicarilla ApacheEight Northern Pueblos:Nambe PuebloPicuris PuebloPojoaque PuebloSan Ildefonso PuebloSan Juan PuebloSanta Clara PuebloTaos PuebloTesuque PuebloSan Felipe PuebloSanto Domingo Pueblo
--2,268
9693,564
--1,062
--2,2891,504
227407524
--1,922
--613
1,715.-
18812594
488851
1,8391,034
2361,7892,139
5. Southern Colorado SU --a, Southern Ute 855b. Ute Mountain Ute 1,111
6. Zuni-Ramah SU --a. Zuni Pueblo 5,988b. Ramah Navajo 1,163
6,705
15,358
2,223--
14,730
2,8519
----
7,594----
--2,940
--6,406
------
3,1101,889
295501584
--2,415
--910
2,269--
37017778
4301,8422,3271,860
2992,0723,332
--1,0961,528
--6,999
--
--3,5861
--6,4061
------
3,2241
2,2271
3161
5261
6501
--2,4651
--9541
2,3081
--4381
2451241
5201
1,8061
1,3741
1,9511
3121
2,1511
2,8901
--1,0961
1,5281
--6,9991
1,6961
ALBUQUERQUEAREA TOTAL 34,964 46,610 43,729 45,792

262 ● Indian Health Care
D. Bemidji Program Office1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Service POp. Resident POD, Tribal
State of Michigan:1. Eastern Michigan SU -- 6,986 - - - -
a. Bay Mills Chippewa 283 -- 466 8031
b. Grand Traverse Ottawa Chippewa -- -- 834 1,1651
c. Saginaw Chippewa -- .- 7801
d. Sault Ste. Marie Chippewa o -- 2,246 10,0001
2. Western Michigan SU -- 1,383 -- --a. Keweenaw Bay Chippewa -- -- 893 2,0891
b. Michigan Potawatomi (Hannahville) 206 -- -- 3751
State of Minnesota:1. Greater Leech Lake SU
a. Greater Leech Lake Chippewa4,124
----
2,759--
4,034--
5,4931
2. Headwaters SUa. Fond du Lac Chippewab. Grand Portage Chippewac. Mine Lac Chippewad. Nett Lake Chippewa (Bois Forte)
5,180--514187293392
--1,431
310897940
2,5413
7243
1,93731,6373
3. Minnesota River SUa. Lower Siouxb. Prairie Island Siouxc. Shakopee-Mdewakanton Siouxd. Upper Sioux
729--65807751
--20911898
127
--2681
2121
1021
1271
--------
4. Red Lake SUa. Red Lake Chippewa
3,297--
--2,823
.-4,399
--6,0271
5. White Earth SUa. White Earth Chippewa
3,547-.
--2,550
--3,948
----
State of Wisconsin:1. Central Wisconsin SU
a. Menomineeb, Oneidac. Stockbridge-Munseed. Wisconsin Winnebago
11,393--2,3771,821
582349
--3,3843,384
9481,718
--6,1821
7,5621
1,1061
3,1741
--------
2, N.W. Wisconsin SUa. Bad River Chippewab. Lac Courte Oreilles Chippewac. Red Cliff Chippewad. St. Croix Chippewa
4,165.-699
1,145589392
--1,3161,8111,3491,041
--2,8171
8071
2,1371
4443
--------

App. A —American Indian and Alaska Native Population Estimates of the U.S. Census Bureau, IHS, BIA, and Tribes ● 263
Bemidji Program Office1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Service Pop. Resident POp. Tribal
3. Nicolet SU -- 1,882 -- --
a. Lac du Flambeau Chippewa 1,092 -- 1,485 1,5901b. Sokoagan Chippewa 95 -. -- 7691
c. Wisconsin Potawatomi 220 -- -- 6031
AREA TOTAL 19,641 42,686 37,386 61,471
E. Billings Area1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Service Pop. Resident POD. Tribal
S t a t e of M o n t a n a :
1. Blackfeet SUa. Blackfeet
5,537--
--5,525
--6,632
--12,0331
--6,7011
--6,0311
--4,0001
--7,0971
--4,889 1
--2,9001
2. Crow SUa. Crow
6,876--
--3,953
--4,969
3. Flathead SUa. Confederate Salish & Kootenai
5,465--
--3,771
--3,300
4. Ft. Belknap SUa. Gros Ventre & Assiniboine
2,582--1,870
--2,097
5. Ft. Peck SUa. Assiniboine & Sioux
4,931 --5,095
--4,273
3,262--
6. Northern Cheyenne SUa. Northern Cheyenne
..-3,101
--3,110
7. Rocky Boy’s SUa. Chippewa-Cree
2,509--
--1,549
--1,897
State of Wyoming:1. Wind River SU -- 4,546 -- --
a. Arapahoe-Shoshone 4,159 -- 5,705 5,6951
BILLINGSAREA TOTAL 28,201 35,708 32,805 49,346

264 ● Indjan Health Care
F. California Program Office 1980 1980 IHS 1980 BIA
IHS Project and Trib e Census Service Pop. Resident POD, Tribal
State of California:1. Auburn IHP
a. Shingle Springs Ra.b. Northern Sierra
2. Central Valley IHPa. Big Sandyb. Cold Springs Ra.c. Table Mountaind. Santa Rosa Ra.
3. Clear Lake IHP (Lake County)a. Middletown Ra.b. Robinson Ra.c. Sulphur Bank Ra.d. Upper Lake
4. Hupa Health Assoc.a. Hoopa Valley Re. (Yurok)
5. Indian Health Council &Southern Indian Health Council
a. Barona Ra.b. Campo Re.c. Capitan Grande Re.d. Cuyapaipe Re.e. Inaja-Cosmit Re.f. Jamul Indian Villageg. La Jolla Re.h. La Posta Re.i. Los Coyotes Re.j. Manzanita Re.k. Mesa Grande Re.1. Pala Re.m. Pauma & Yuiman. Rincon Re.o. San Pasqual Re.p. Santa Ysabel Re.q. Sycuan Re.r, Viejas Ra.
6. Karok Tribal HPa. Karok Tribe
7. Consolidated Tribal HP(Mendocino)
a. Coyote Valley Ra.b. Hopland Ra.c. Laytonville Ra. (Cahto Tribe)d. Manchester/Pt. Arenae. Sherwood Valley Ra.
--0
--
--63--
117
.-39--
115--
.-1,913
22286020
. .141
145130
43386
29713318148142
.---
--
010
1057717
2,423--.-
4,421---..-.-
806---..---
2,020-.
--.-.--.--.----..----------.-----.--
1,485--
1,815
----.-----
---.--
-.129209
76271
. -6268-.
133
- -1,816
301205-.241062
22114
1614028
45593
26134788970
183
----
--
21612517788
173
751--
--.-563603
2091
--353--.-
1093
--3,8001
3501
781--61131
621
4201
151
1311
501
2861
4751
911
5001
2781
2171
551
1831
.-2,0003
. .
-.12516832321
2311

App. A—American Indian and Alaska Native Population Estimates of the U.S. Census Bureau, IHS, 81A, and Tribes ● 265
California Program Office1980 1980 IHS 1980 BIA
IHS Project and Tribe Census Service POD, Resident POD, Tribal
8. Modoc IHPa. Alturas Ra.b. Cedamille Ra.c. Likely Ra.d. Lookout Ra.e. X-L Ranch Re,
Pit River
9. Northern Valley IHPa. Berry Creek Ra.b. Enterprise Ra.c. Colusad. Cachil DeHe Ra.e. Cortina Ra.f. Grindstone Creek Ra.g. Sutterh. Tehemai. Rumsey Ra.
10. Pi-Ma-Pa IH Consortiuma. Susanville Ra,b. Ft. Bidwell Re.c. Montgomery Creek Ra.d. Roaring Creek Ra.
11. Riverside-San Bernardinoa. Agua Caliente Re.b. Augustine Re. (Cahuilla Mission)c. Cabazon Re.d. Cahuilla Re.e. Morongo Re.f. Pechanga Re.g. Ramona Re.
Santa Rosa Re. (Cahuilla Mission)i. Soboba Re.j. Torres-Martinez Re.k. San Manuel Re.1. Twenty-nine Palms Re.
12. Round Valley IHPa. Round Valley Re.
13. Santa Ynez IHPa. Santa Ynez Re.
14. Shasta-Trinity IHPBig Bend Ra.
15. Sonoma County IHPa. Dry Creek Ra.b, Stewarts Pt. Ra.
--760
1224--
--0
16--172
72----11
--82931
24
-.6508
29313117
012
23011240
--528
--120
--8
. .4172
238---.--------
6,649------------------
1,000--------
17,292-.--.----------.---.-.--
560--
134--
2,825--
3,480- -- -
--1016--1154-.
--1541844--81
173----47
--3501621936
------22
148743428
3100457818818
--709
--200
--106
--126204
--211
151
0133
311
3,000 1
--2001
651
261
--871
871
----491
--1751
1991
193
363
--2181
0381
1681
7181
2151
--461
3901
2151
401
131
--2,3001
--1891
--243
--1273
--

266 ● Indian Health Care
C a l i f o r n i a Program Office1980 1980 IHS 1980 BIA
IHS Project and Tribe Census Service Pop. Resident POD. Tribal
16. Toiyabe IHPa. Big Pine Ra.b. Bishop Ra.c. Death Valleyd. Ft. Independence Re.e. Lone Pine Ra.f. Benton Paiute Re.g. Bridgeport Paiute Colony
17. Tule River IHPa. Tule River Re.
18. Tuolumne Rural IHPa. Jackson Ra.b. Sheep Ranch Ra.c, Tuolumne Ra.
19. United IHPa. Resighini Ra.b. Big Lagoon Ra.c. Table Bluffd. Trinidad Ra.
.-269784
. -31
1721247
.-424
--15
273
-.188
--47
1,943--.--.-.-.----
2,557- -
1,611----.-
4,946----.---
--419
1,006
932042581
-.549
--19--
276
--104
77067
--4411
1,1001
1991
6511821
1013
70
--5491
-.30311
1021
--171
-.883
1251
CALIFORNIAAREA TOTAL 8,133 65,757 14,435 22,104
G. Nashville Program1980 1980 IHS 1980 BIA
IHS Planning Areas and Tribe Census Servi e POD.c Resident P D.o Tribal
1 .2.3.4.5.6.7.8.9.
10.11.12.13.14.15,16.
Cherokee, NCChitimacha, LA
Choctaw, MSCoushatta, LAMaliseets, MEMashantucket Pequot, CTMiccosukee, FLNarragansett, RIPassamaquoddy (Indian Twnshp), ME8
Passamaquoddy (Pleasant Point), MEPenobscot, MEPoarch Band of Indians, ALSeminole, FLSeneca, NYSt. Regis, NYTunica-Biloxi, LA
4,844185
2,75618.--.
213--
333504398------
1,7637
5,604388
4,155234--.-
1,729--
1,346-.
1,352--
2,1397,2582,526
--
5,664 5,9717278 325
4,914 4,487272 326239 299
- - - -457 320 1
- - 1,150367 476691 698
1,029 1,297- - 1,425
1,424 1,8275,418 5,3002,799 3,250
- - 115
NASHVILLEAREA TOTAL 11,021 26,731 23,552 27,266

App. A—American Indian and Alaska Native Population Estimates of the U.S. Census Bureau, IHS, BIA, and Tribes ● 267
H. Navajo Area1980 1980 IHS 1980 BIA
S Service Unit and Tribe Census Service Pop. Res ident POD. Tribal
States of Arizona, New Mexico,Colorado, and Utah:
Navajo Tribe:1. Chinle SU2. Crownpoint SU3. Ft. Defiance SU4. Gallup SU5. Kayenta SU6. Shiprock SU7. Tuba City SU8. Winslow SU
104,978 145,16220,39811,31720,51621,58911,96131,82217,07310,486
165,0003
NAVAJOAREA TOTAL 104,978 145,162 -. 165,000
I . Oklahoma City Areat1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Servi ce Pop. Resident Pop. Tribal
State of Oklahoma:1, Ada SU
a. Chickasawb. Seminole
2. Claremore SUa. Eastern Shawneeb. MiamiC. Modocd. Ottawae. Peoriaf. Quapawg. Seneca-Cayugah. Wyandotte
3. Clinton SUa. Cheyenne Arapaho Tribes
4. Haskell SUa. Haskell Indian School & Hlth Ctr
5. Kansas (Holton) SUa. Iowa of Kansas & Nebraskab. Kickapoo of Kansasc. Prairie Band of Potowatomid. Sac & Fox of Missouri
6. Lawton SUa. Apacheb. Caddoc. Comanche
18,311----
53,655--.-.-----------
5,960--
---.
3,172-..----.
13,996--. .--
8,5073,719
--335350150336355
1,193670440
--. .
--. .
--280598
1,30236
.-517
1,2153,597
11,4804
3,142 4
--1,40031,9003
20031,9893
2,0503
2,9003
3,10032,4003
--7,6771
----
--2,1181
1,1981
3,2891
2431
--833 1
2 , 0 3 11
7,4131

268 ● Indian Health Care
Oklahoma City Area1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Service Pop. Resident POD. Tr ibal
d. Delaware-Westerne. Ft. Sill Apachef. Kiowag. Wichita
7. Pawnee SUa. Pawnee
b. Kawc. Tonkawad. Osagee. Otoe-Missourif. Ponca
8. Shawnee SUa. Absentee Shawneeb. Citizens Band of Potawatomic. Iowa of Oklahomad. Kickapoo of Eagle Pass (Texas)e. Kickapoo of Oklahomaf. Sac & Fox of Oklahoma
9. Tahlequah SUa. Cherokee Nation of Oklahomab. Creek
10. Talihina SUa. Choctaw
--------
-----.---.
4,749----
.---.-. .-----.
--.---
-.--
.-----.-
11,406
------------
23,616------.-----
26,101----
16,419-.
52270
4,005610
--2,066
--617
1,2655,6121,1652,065
--1,3656,354
203--
7151,352
--42,99237,679
--19,660
9551
2721
7,9481
9961
--2,5005
2,2491
7811
1821
10,00031,4501
2,0221
.-1,9711
11,07112861
--1,5281
2,1451
-.43,5124
18,8674
--28,0221
OKLAHOMA CITYAREA TOTAL 4,749 172,636 151,917 192,120
J. Phoenix Area1980 1980 IHS 1980 BIA
IHS Service Unit and Tr ibe Census Service Pop. Resident Pop. Tribal
State of Arizona:1. Colorado River SU -- 4,306 -- --
a. Chemehuevi 23 .- 124 316 6
b. Colorado River 1,965 .- 2,084 2,3006
c. Ft. Mojave 127 -. 537 6401
d. Havasupai 267 -- 475 4751
e. Hualapai 809 -- 1,017 1,1336
2. Ft. Yuma SU -- 2,242 -- --a, Cocopah 349 -. 835 4756
b. Quechan (Ft. Yuma 1,105 -- 1,500 1,8751
c. Riverside School -- -. -- --

App. A —American Indian and Alaska Native Population Estimates of the U.S. Census Bureau, IHS, B/A, and Tribes ● 269
Phoenix Area1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Service POD. Resident POD, Tribal
3. Keams Canyon SUa. Hopib. Kiabab/Paiute
--6,591
93
4,129 8,439
2296,66711391
----
4526
8,3101
4,10953,31311501
9511
--4231
8,3101
--8,5001
--7,7001
----
22,2594. Phoenix SUa. Campe Vereb. Ft. McDowellc. Gila Bendd. Gila River (pop. split
with Sacaton SU)*e. Payson Apachef. Salt River
--173345--.-
-.516383760
9,592
----.--.
66-.2,624
--66----.-
--.-----------
3,364--.-g. Yavapai-Prescott
Yavapai-Apacheh. Phoenix Indian Schooli. Phoenix Service Area
. .----
5. Sacaton SUa. Ak Chinb. Gila River (pop. split
with Phoenix SU)*
8,996----
7,067
--433
9,592----
6. San Carlos SUa. San Carlos Apache
7,186--
--5,872
.-5,967
7. Whiteriver SUa. White Mountain Apache
7,903--
.-6,880
--8,010
State of Nevada:1. Owyhee SU .- 2,358 .- --
::c .d.e.f.
::i.
Battle MountainDuck Valley (Shoshone-Paiute)Duck WaterElkoElyGoshuteRuby ValleySouth ForkTe-Moak
-.932103
-------------.---.
196 1751
-- 1,2001139 1501
468 3956
234 1601
211 2001
--67
105-- -- --
123 119 1
- - 500 1
--91
2. Schurz SUa, Fallen Colonyb. Ft. McDermittc. Las Vegasd. Lovelock Paiutee. Moapa Paiutef. Pyramid Lakeg. Reno Sparksh. Summit Lake
--30446310611718272045115
11,586 -- -.677 1,2001
653 5291
123 1051
163 1631
216 3801
776 1,1201
603 5071
-- 661
--------.-------

270 ● Indian Health Care
Phoenix Area1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Servi ce Pop . Resident Pop. Tribal
i. Walker Riverj . Washoe
CarsonDresslervilleWoodfords
k. Winnemucca1. Yeringtonm. Yomba
4714
21312712635
10557
980 1,1001
544 1,8001
-- 1291
-- 1531
-- 2501
81 301
342 3631
114 951
State of Utah:1. Uintah & Ouray SU -- 3,055 -- . .
a. Uintah & Ouray Ute 2,050 -- 1,890 1,7201
b. Paiutes of Utah 186 -. 312 5431
(Southern Paiute)c. Skull Valley 13 -- 72 611
PHOENIXAREA TOTAL 41,399 74,020 62,840 69,451
K. Portland Area1980 1980 IHS 1980 BIA
IHS Service Unit and Tr ibe Census Service P o p . Residen t POD. Tribal
State of Idaho:1. Fort Hall SU -- 3,685 -- 3,1001
a. Shoshone-Bannock 2,542 -. 3,820 --
2. N. Idaho SU -- 7,538 -- --a. Coeur d’Alene 538 .- 822 1,200 1
b. Kootenai 40 .- 115 651c. Nez Perce 1,463 -- 2,020 2,5601
State of Oregon:1. Umatilla SU
a. Umatilla Tribe
2. Warm Springs SUa. Burns Paiuteb. Warm Springs
3. Western Oregon SUa. Chemawab. Cow Creek Umpquac. Grande Ronded. Siletze. Coos-Umpqua-Siuslaw
--908
-.160
2,004
1,670.-
4,052
7,268
--1,500
.-194
2,412
.-671
--
--1,3421
2051
2,4001
-..-
70031,1001,5501
8003

App. A—American lndian and Alaska Native Population Estimates of the U.S. Census Bureau, IHSJ BIA, and Tribes Ž 271
Portland Area1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Servi ce Pop. Resident POP, Tribal
State of Washington:1. Colville SU
a. Colville Tribe2, Neah Bay SU
a. Jamestownb. Lower Elwhac. Makahd. Quileute
3. NW Washington SUa. Lummib. Nooksackc. Swinomishd. Upper Skagit
4. Puget Sound SU
;:c .d.e.f.
::
::
MuckleshootNisquallyPuyallupPort Gamble
.-3,500
----47803273
--1,259
0414
0
--37542
856(Clallam) 266
Sauk Suiattle oSkokomish 305Squaxin Island 35Stillaguamish --Suquamish (Port Madison) 148Tulalip 768
5. Wellpinit SUa. Spokane (inc. Kalispel
until FY 83)b. Kalispel
6. Taholah SUa. Chehalisb. Hohc. Quinaultd. Shoalwater Bay
7. Yakima SUa. Yakima Tribe
1,050
98
.-20046
94328
.-4,983
5,175
2,113--
--
4,390.-------
27,251
1,831
--
3,090.------.
7,706--
--6,090
--323
1,191927327
--2,290
694648376
--2,2271,2575,660
446255
1,008926464
1,784855
1,921
205
--72161
2,01362
--8,502
--6,2401
--15034031
1,7893
5461
--1,2251
4251
4951
2151
-.4081
1751
1,2001
4791
2201
5011
2901
1531
5831
9501
1,9381
1851
--3771
1011
1,8001
1011
--6,7751
PORTLANDAREA TOTAL 24,094 75,769 52,787 42,746

272 ● Indian Health Care
L. Tucson Program Office1980 1980 IHS 1980 BIA
IHS Service Unit and Tribe Census Service POD . Resident Pop. Tribal
State of Arizona:1. Sells SU .- 15,109 .- --
Papago Tribe 6,959 . 10,610 16,5301
2, Total Contract SU -- 1,121 -- .-Pascua-Yaqui 551 . . 616 7,0001
TUCSONAREA TOTAL 7,510 16,230 11,226 23,530
ALL IHSAREAS TOTAL 328,714 828,609 526,755 811,591
1980 Census figures include American Indians living on reservations only.
12345678
9
Enrolled population as of 12/811978 payment rollsBIA estimate considered ‘rough”1906 Final RollReported at an OTA regional meeting, 1985Tribal MembershipEstimated service unit populationIHS service population figure combines Indian Townshipgroups of the Passamaquoddy.IHS service population, 1981
SOURCES: U.S. Bureau of the Census, PC80-S1-13, 1984; U.
and Pleasant Point
S. Department of Healthand Human Services, Public Health Service, Health Resources and ServicesAdministration, Indian Health Service, Population Statistics Staff; Bureau ofIndian Affairs, cal Estimate s of R e s i d e n t Status. December 1981, Jan. 1982; and approximate enrollment figuresfrom an unpublished BIA document, 1981.

.
Ap
pen
dix B
W5IiVI
m
e+
273
IBS COOE-
ALL
310 350
360 390
370 380 410 320 330 400
340 790
800
810 150 170
180 220
200 190 210 240
230
160 620 430 470 440
450 460
510
520
530 260
CAUSEb
ALL CAUSES
DISEASE OF HEART · . ISCHMC HR.T DIS
· ... ACUT KYO INF · ... OLD MI, OTHER
· ... OTH ACUT IHD · ... ANGINA PECTO
· .ALL OTB HR.T OS · . RHEUM FEVER · . HYPRTNS HR.T OS · .OTB ENDOCRD OS
· . HYPRTNS+RENAL ACCIDENTS / ADVERS
· .HOTOR VEBICLE · . ALL OTB ACCDNT MALIG NEOPLASMS .. MAL NEO-DIGEST
.. MAL NEO-RESPIR · . MAL NEO-OTHER
· .MAL NEO-GENITL · . MAL NEO-BREAST
· . MAL NEO-URINAR · OTB NEOP L YMPB
· . LEUKEMIA · .MAL NEOPLS-LIP
LIVER DIS/CIRRHS CEREBROVASC OS
· . ALL OTB CBV OS
· . INTRCRB HMRHG · . CERBRL THROMB
· CEREBRL EMBOL PNEUMONIA/ INFLNZ · . PNEUMONIA
· INFLUENZA DIABETES MELLITU
DEATHS, AGE-SPECIFIC AND AGE-ADJUSTED DEATB RATES AND RATIO TO US. ALL RACES AGE-ADJUSTED DEATH RATES
72 SELECTED CAUSES 11 IBS AREAS, 1980 - 82
BY LEADING CAUSES, BY BOTH SEXES AND MALE/FEMALE
ALL AREAS (EXCLUDING CALIFORNIA) BO SEXES
CRUDE
...MrL ER ULA AGE- RATIO TO
TOTAL ALL 0-4 5-14 15-24 25-34
DEATBS AGES YEARS YEARS YEARS YEARS
15321
3058 1956 1212
692 49
3 932
60
55 44
11 2946 1669 1277
1713 548
343 262
215 90
80 79
62 34
801 664
473 113
76 2
580 556
24 470
652.8
130.3 83.3
51.6 29.5
2.1 0.1
39.7 2.6
2.3 1.9 0.5
125.5 71.1 54.4
73. a 23.3 14.6 11. 2
9.2 3.8
3.4 3.4
2.6 1.4
34.1
28.3 20.2 4.8
3.2 0.1
24.7 23.7
1.0 20. a
471.3
14.5 0.4
0.4
13.7 0.4
63.5
25.6 37.9
2.6
0.4 0.7
0.4 0.4 0.7
0.4 1.5
0.7
0.7
19. 18.
0.4 0.4
43.1
0.9
0.8 0.2
285.:)
5.3 0.4 0.4
3. a 1.5
0.4
397.1 15.2 6.3
3.3 2.8
0.3
5.8 1.9
0.3 0.8
26.1 164.2 181.9
11.3114.3107.9 14.7 49.9 74.0
1.9 5.6 10.5 0.6 2.2
0.2 0.3 0.8 1.9 3.3
0.9 1.4 0.3
1.4 0.2 0.3
1.1 1.9 1.4
1.7 34.8 0.8 3.6
0.2 1.9 0.4 1.1
0.2 0.3 0.3
1.5 2.1 5.0 1.5 1.9 5.0
0.2 0.2 3.9
35-44 45-54 55-64 65-74 75-84 85 YEARS ADJUST U.S. ALL-RACES YEARS YEARS YEARS YEARS YEARS AND OVER RATE AGE-ADJUSTED RATES
555.4 55.9
28.8 19.5 8.9 0.4
22.4 3. a 0.8
0.8
159.2 87.6 71.5
37.3 10.2
3.4 6.8
6.8 4.2
0.8 1.7
2.5 a 8
95.2 10.6
7.2 3.4
9.7 9.7
8. a
950.5 1694.8 172.6 454.2
114.6 311.8 80.1 210.8 31.0 89.5 3.5 11.4
48.6 115.6 4.7 12.2
2.3 8.1 1.8 6.5
0.6 159.7 80.7
79. a 129.9
42.7
26.3 14.6
14.6 15.8
7. a 4.1
2.3 2.3
128.1 26.3
12.9 11.7
1.8
23.4 22.2
1.2 31. 6
170 .1
81. 4 88.7
302.8 91.2 84.7 31.7
29.3 22.0
17.9 10.6
8.1 7.3
109.1 72 45 21. 2 5.7
38.3 37.4
0.8 107.5
3081. 5 6097. a 13325.2 1024.2 2064.3 4363.7
736.7 1334.5 2481.9 492.4 773.4 1047.7 225.2 535.0 1383.4
19.1 23.3 30.5 2.9 20.3
245.6 610.6 1749.6 12.7 8.7 19.1 61.1 20.3 8.9 34.9 71.2 1.3 14.5 40.7
170.5 209.3 356. a 72.5 81.4 71.2 98.0127.9284.8
606.9 1023.4 1190.1 198.5 369.3 457.7
143.8 162.8 142.4 95.4 177.4 183.1
64.9 159.9 223.8 20.4 11 . 6 50.9 29.3 32.0 40.7 36.9 49.4 61.0
7.6 29.1 30.5 10.2 32.0 82.7 55.2 30.5
171.8 575.7 1536.0
122.1 441.9 1241.0 26.7 58.1 101.7 22.9 72.7 193.3
2.9 100.5 407.0 1647.8
96.7 383.8 1566 5
3.8 23.3 81.4 178.1 258 8 203.4
778.3 166.7
109.3 69.8 36.6 2.8 0.1
48.1 3.4
3.1 2.3
0.5 136.3
75.6 60.7
98.4
31. 5 20.7 14.5
11.9 5.6 4.7 4.5
3.1 2. a
48.1 33.8 23.5 6.4
3.7 0.1
26.6 25.6
1.1 27.8
1."
0.9 0.8 0.9 0.6
2.2 1.1
1.2 1.5
0.5 1.1 0.6 3.4
3.5 3.4
0.7 1.0 0.6 0.9 0.9 0.4
0.9 0.7
0.6 0.7
4.2 0.9
0.9
1.1 0.6 0.5
2.2 2.2
1.8 2.8
a Equivalence to ICD-9 codes available from IHS.
Cause ranked in order by number of deaths for leading causes
SOURCES: Indian data: U. S. Department of Health and Human Services, Publ ic Health Service, Health Resources and Services Administration, Indian Health Service, computer tape suppl ied to the Office of Technology Assessment, Washington, DC, 1985. U. S. data: U. S. Department of Health and Human Services, Public Health Service, National Center for Health Statistics, "Advance Report-Final Mortality Statistics, 1981," Monthly Vital Statistics Report 33(3) :supp., June 22, 1984.

274 ● Indian Health Care
L-J. . . .
0+
m
4“””
m
A“””
u. . . . . . . . .
0
* N N. . . . . . . . . . . . . . . . . . .
0 0 0...
-4
‘4

Ap
p.
B—
Ind
ian
H
ea
lth
Sta
tus
Da
ta
● 2
75
IHS CODE a
ALL 310
350 360 390 370 380 410 320 330 400 340 150 170 220 200 180 190 240 230 210 160 790 800 810 620 430 470 440 450 460 260 510 520 530 740 760 750 640
CAUSEb
ALL CAUSES DISEASE OF HEART · . ISCHHC HRT DIS · ... ACUT KYO INF · ... OLD HI, OTHER · ... OTH ACUT IHD · ... ANGINA PECTO · . ALL OTH HRT DS · . RHEUM FEVER · . HYPRTNS HRT DS · .OTH ENDOCRD DS · . HYPRTNS+RENAL HALIG NEOPLASMS · .HAL NEO-DIGEST · . HAL NEO-OTHER · . HAL NEO-GENITL .. HAL NEO-RESPIR .. HAL NEO-BREAST · . OTH NEOP LYMPH · . LEUKEMIA .. HAL NEO-URINAR .. HAL NEOPLS-LIP ACCIDENTS/ ADVERS · . MOTOR VEHICLE · . ALL OTH ACCDNT LIVER DIS/CIRRHS CEREBROVASC DS · . ALL OTH CBV DS · . INTRCRB HHRBG · . CERBRL THROHB · . CEREBRL EHBOL DIABETES HELLITU PNEUMONIA! INFLNZ · .PNEUMONIA .. INFLUENZA PERINATAL CONDIT · .OTH COND PERIN · . BIRTH TRAUMA
NEPHRITIS. ET AL
DEATHS, AGE-SPECIFIC AND AGE-ADJUSTED DEATH RATES AND RATIO TO US. ALL RACES AGE-ADJUSTED DEATH RATES, 72 SELECTED CAUSES
11 IRS AREAS, 1980-82 BY LLWINt; CAUSES. BY BOTH SEXES AND HALE/FEMALE
ALL AREAS (EXCLUDING CALIFORNIA FEMALE
CRUDE ....MIL RA
TOTAL ALL 0-4 5-14 15-24 25-34 35-44 DEATHS AGES YEARS YEARS YEARS YEARS YEARS
5994 503.4 loll!. II 3D.:.! 142.2 229.9 357.1 1234 103.6 14.3 1.1 5.6 9.2 23.8
731 61.4 0.8 3.8 7.4 421 35.4 1.6 6.6 293 24.6 0.8 1.6 0.8
15 1.3 0.5
408 35 28 23
827 255 145 130 102
90 37 30
25 13
781 510 271 351 334 251
49 33
1 261 241 228
13 127
88 39
125
0.2 34.3 2.9 2.4 1.9 0.8
69.5 21. 4
12.2 10.9 8.6 7.6 3.1 2.5 2.1 1.1
65.6 42.8 22.8 29.5 28.1 21.1
4.1 2.8 0.1
21.9 20.2 19.1 1.1
10.7 7.4 3.3
10.5
12.8 0.8
3.8
1.5
0.8 0.8 0.8
54.9 24.8 30.1 0.8 0.8
0.8
19.5 19.5
95.5 66.2 29.3 1.5
0.8 0.4
1.9
0.8
1.1
18.7 9.6 9.2
0.8 0.8
3.4 1.5
0.7
5.6 0.7 1.1 1.1
2.6
79.7 67.0 12.7 1.9 0.4 0.4
1.1 1.1
1.5
3.2 1.6 0.5
9.2 1.1 3.8 2.7
0.5
0.5 0.5
92.1 66.2 25.8 29.1 4.8 2.7 1.6
0.5 2.2 2.2 2.2
1.6
12.3 3.3
0.8
42.7 11.5
4.1 12.3 2.5 8.2 1.6 1.6 0.8
73.1 47.6 25.5 76.4 13.1
9.9 3.3
4.9 6.6 6.6
6.6
ER ULA AGE- RATIO TO 45-54 55-64 65-74 75-84 85 YEARS ADJUST U. S. ALL-RACES YEARS YEARS YEARS YEARS AND OVER RATE AGE-ADJUSTED RATES
688.8 1252.4 2410.8 5072.9 11773.8 578.6 1.4 95.2 286.7 748.1 1718.7 3964.5 121.5 0.9 48.2 165.8 511.2 1062.5 2426.5 72.6 0.8 33.6 114.7 328.3 567.7 974.0 43.6 0.9 14.6 43.4 175.9 468.7 1401.2 27.3 0.6
7.7 7.0 20.8 34.2 1.5 1.9
35.8 93.0 5.6 15.5 2.2 6.2 2.2 6.2 1.1
133.3 277.4 32.5 75.9 17.9 37.2 23.5 37.2 13.4 54.2 30.2 41.8 6.7 6.2 3.4 9.3 3.4 10.8 2.2 4.6
81.8 69.7 45.9 41.8 35.8 27.9
107.5 86.8 24.6 58.9 12.3 37.2 11.2 15.5 1.1 6.2
28.0 116.2 16.8 24.8 14.6 23.2 2.2 1.5
14 .6 38.7
5.2 17.1 0.2 1.5 206.4 510.4 1384.1 11.7 10.4 14.1 67.7 34.2
4.7 41. 7 68.4 26.0 51.3
501.9 833.31042.4 182.9 322.9 324.7 98.5171.9188.0 53.9135.4222.1 77.4 72.9 85.4 37.5 20.8 85.4 30.5 36.5 68.4 2.3 20.8 34.2
11.7 26.0 34.2 7.0 26.0
75.0119.8222.1 30.5 46.9 34.2 44.6 72.9 188.0 77.4 67.7
147.7 468.7 1606.3 119.6 364.6 1315.8 18.8 36.5 102.5
9. 4 67 . 7 188. 0
190.0 291. 239.2 82.1 343 1127.8 77.4 317.7 1076.6 4.7 26.0 51.3
65.7 130.2 290.5
39.4 3.8 2.9 2.2 0.8
89.4 27.5 15.2 13.8 11. 5 10.5 3.9 2.8 2.7 1.4
69.0 44.5 24.5 40.1 31. 3 23.0 5.2 2.9 0.1
28.8 21. 0 19.8 1.3 7.5 5.2 2.3
12.8
1.3
1.4 0.6 1.4 1.1 0.8 1.1 1.1 1.0
0.6 0.5 0.7 0.7 0.9 1.0 3.4 3.9 2.7 5.4 0.9 1.0
0.9 0.5 0.4 3. a 2.3 2.3 2.1 0.9 0.9 1.0 3.6
a Equivalence to ICD-9 codes available from IHS. b Cause ranked in order by number of deaths for leading

276 ● Indian Health Care
,+
.
m,.
.-i *U
i“ “ 0 0u
. . . . . . . .0
.‘e
-4gc1
mm. . . . .C-4
I/l
3

App. B—Indian Health Status Data • 277
.Y
Om,-iinoo-mml. . . . . .
.I-! Nm m-a m.
,+ml..,e4d
WI
i’
. .
.,
m- -z00 0
m 1-. .d a 0
0 -. . . .
L,

278 • Indian Health Care
u
0
u-l20 ~
AU-i,+,-4
v *oum. . . . . . . .
*“i
. .
a. .0
. .
.
r- O h m. . . . . . .m e)u”ui
l.-l.-la.-4
*. . . . . . .0
* Uau. . . . . . . .
0 0 0 0
* -1. . . . . . . .
0 a
In l-1. . . . . . . . .
-ur.

App. B—Indian Health Status Data ● 279
.+
0 0. .
4A0
u’
N.
C O . 8 0 1 ( - 4*. . . . . .
r-

280 ● Indian Health Care
,.
.+ .+ ,-4
,+ AU m.+ !%
“i.-4
. .0
. . . . . .e
m m *. . . ..
. .
m
“t-i
,.
. .
. . .
. . . . . . . . . .
. . . . . . . . . . . . . . . . . . .
,+. . . . . .G
. . . . . . . . . . . . . . . . . .
m. . . . . . . . .
.+r-
r+. . . . . ...+

App. B—Indian Health Status Data ● 281
m
NL-4
ulNhn-?dm . ( - +.+-l-a
Od4
0 0
.r-0
u-l.
m .... .0!u
Dw*O
*U)smoMU *D

282 ● Indian Health Care
N OJN. . . . . .
.8m s 2
N
“uF1
N
“ *l-l
.-l
“4 “,+
,4.4
“4 “Ui “k++
. . . . . .
*“.-i
.+
*‘A
.-l
et-.?. . . . .. . . . . .
0 0 0 m. . . ,
“Wb,-1 Uie+ln
. . . . . .
N*. . . . . .
m mA
. . . . . . . . .
04. . . . . .
m. . . . . .
,-!. . . . . .
--e-l. . . . . .

App. B—Indian Health Status Data . 283
l-de .-4.+
,-4
.+
00 ammo 0
,.
m
“<
.
. .
.
ma.1-
.,
,.
i“”.-l
m
‘h”
.
,..
m. . .h
mN -
0 0 0 0. . . .v u’ -7 v“
.
,.
.-l
.0t-l(/I
5
52-805 0 - 86 - 10

284 Ž Indian Health Care
.-4
0mN
mmw
. . .
m. . . . .r-
*,..u’
. . . . .
-. . . . .“bm
m
‘u+m
*. .Amm
*. . .m0!
0!
-’”1.
. . .
.
. . .
. . .
. . .
. . .
* w. . . . .
*. .l-lm
,.
. .
@“i.+
.,
. .
. .
0,.mN
k-l
NW. . . . . .au,+
0. . . . .e
m me-l, +. . . . . . .

App. B—Indian Health Status Data Ž 285
. .
,+
. . . .
. . . ..8. . . . . . .* -7U
admeom o-s. . .
r. ,-4 .+ r+

286Ž Indian Health Care
. .
. .
1+
. .
. .
. .
..
. .
. .
.
In. . . . . . . . . . .i
. .
. .
. .
..
. .
. .
.
. .
. .
. .
Deaths. Age-Specific and Age-adjusted Death Rates. Alaska Both Sexes (cont'd)
AGti-SPECllIC DMIB RAIn n~ER 120 000 fglULAII2!!l AGE- RATIO TO TOTAL ALL 0-4 5-1/1 15-24 25-34 35-44 45-54 55-64 65-74 75-84 85 YEARS ADJUST u. s. ALL-RACES
COD CAUSE DEATHS AGES YEARS YEARS YEARS YEARS YEARS YEARS YEARS YEARS YEARS AIID OVER RATE AGE-ADJUSTED RATES
730 CONGD AlI<»tALIES 19 9.6 79.8 2.1 6.8 1.2 030 TUBERCULOSIS 13 6.6 20.5 6.7 31.3 33.1 133.3 10.1 16.8 040 · . TB-RESPIRATORY 11 5.6 15.4 31. 3 33.1 133.3 8.6 17.1 050 .. OTHER T 2 1.0 5.1 6.7 1.5 15.0 640 NEPBlUTIS. ET AL 12 6.1 2.1 5.1 20.9 49.7 222.1 9.0 2.0 670 · . RElfAL FAIL, ETC 10 5.1 5.1 10.4 49.7 222.1 7.8 2.1 660 .• CBR.I GLMlt/NEPH 2 1.0 2.1 10.4 1.2 2.5 140 ALL OTB IIfF/PIJU. 3.5 8.9 6.7 31. 3 16.6 4.8 3.2 480 ATHER.OSCLEROSIS 3.5 88.8 862.1 3.9 0.8 590 ULCER - ST<»f, DUOD 3.5 6.7 31. 3 16.6 88.8 5.6 3.3 090 SEPTICEKIA 6 3.0 4.4 5.1 6.7 33.1 44.4 4.2 1.5 680 K.IDrmY IIfFECTIOR 6 3.0 2.1 13.4 10.4 16.6 44.4 4.4 8.8 260 DIABETES HELLITU 2.0 2.1 16.6 88.8 2.7 0.3 290 MDIIfCITIS 2.0 13.3 5.1 1.8 3.6 630 CHOLELI GALLBLDll_ 2.0 20.9 44.4 172.4 2.9 4.2 250 BElIIGN NEO, OTHER. 1.5 44.4 344.8 1.7 0.9 610 HERNIAl IIfTST .OBS 1.5 133.3 2.3 1.8 120 VIRAL HEPATITIS 2 1.0 3.3 6.7 1.3 4.4 420 · . HYPllTNS+ 1- RlfL 2 1.0 2.1 6.7 1.2 0.6 080 MDIlIGOCOCCL IIfF 0.5 10.4 0.8 4.2 270 NUTlUTIOR DEFICS 0.5 172.4 0.5 1.0 280 ANEMIAS 0.5 10.4 0.8 0.9 490 OTHER. AllTERY DIS 0.5 16.6 0.8 0.2 700 PUGMAltCY CCK'LI 0.5 3.3 0.5 5.3 720 · .OTH PUG CQ4PL 0.5 3.3 0.5 5.3 770 SYMP/SICI/ILL-DP 65 32.9 128.6 4.3 22.8 !.S.4 6.7 31. 3 99.3 177.7 1551.7 32.4 3.3 840 ALL OTB EXTRlfL C 36 18.2 4.4 32.0 39.0 10.2 26.9 10.4 16.6 18.7 12.5 780 ALL OTHER. DISUS 151 76.5 44.3 4.5 23.5 61.8 82.0 147.7 261.0 380.8 710.8 1206.9 102.4 3.0

App. B—Indian Health Status Data ● 287
,4,-! .
,, . . . .e l-l f--lnm -v. . . . . . . . . . . . . . . . . . . . . . . . .
+m m. . . . . .u-lo 0-0 m.+ (-l m
mm. . . . . . . .mmmm
mm m,. .,..mm c.)m.-! m
t-i++ ,-lbur. h. . . . . . . . . . .
r.r.. .
; “A.-4,+
W
iik
!
Uu.0 0+.+
4
mwwmr+. . . ..+.-+ ?40;lnmme4m
. . .
. . .
,.,
. .
,,.
. . . .aN
l-l
-’”’.-4
. . . . .
*.. .,.,..u
. . . . . . . . .
woo W. . . . .

580560090480680140590250290080120420610630700720770840780
6155533221111111
269
64
6.21.05.15.15.13.13.12.12.11.01.01.01.01.01.01.0
26.89.3
65.9
9.2 .
18.3 .
1 8 . 3
146.6 .9 . 2
27.5 4.6
4.3
4.325.917.3
6.5
6.56.5
13.113.139.2
10.4
62.3
13.7
13.7
13.713.7
13.7
150.4
21.1
21.1
21.1
21.1
21.1
21.1
316.9
33.3
33.3
33.3
33.3
66.6
366.5
350.3
87.6175.187.6
87.6
87.6
87.6
437.8
1027.4
684.9
684.9
684.9
9.5 1.61.7 0.97.0 2.96.6 1.47.2 12.13.0 2.34.9 4.12.3 1.31.4 3.61.7 8.31.1 3.61.6 0.91.6 1.21.7 2.41.1 3.61 1 5.4
23.3 3.37.6 8.5
91.7 3.2

App. B—Indian Health Status Data ● 289
oak
.ici&UI V - 3mom.-Id
0 0.,.
z~
m mu-u N
4 “ “$+. - + - . - 4 . 3 *UT r.o!(mr+ 4
,-4
c+
m“r .
. . . . .-?OemQm
(- 4(-4 N,., . . . . .u “a u
.?4(’4 Wm-Tu. . . . .U* ;Umrn
mm
-S(NN,..
CQ*;
. . . . . . . . . . . . . . . . .
u!
4“’””””””’””
muXoHW
*XI

290 ● Indian Health Care
.-l
. . . . . . . . . .
. .
0+
“4m
. .
0 00 0. . .0 0mm
0 0 0 0. . . . . .0 0 0 0tjJlnam
0. .“ 0m
. . .
‘a
‘0 “el
0.+. . . .01- 2NO I
“0 “ “0m m1+
. .
. .
*“ 0N
m @ -. . . .. . . ... ,+00*NO
e+
N. . . . . .m
N. . . .m4
,.. . .
d. .0d
. .
. .
,.
*
‘m
,+
mN.+. . . . . . . . .0 0 0me4,-1
. . . . . . . . .
. . . .
. . . .
. . . .
*. . . . . . .*. . . . . . . . . . . . . .
m
4“””””””””m
-N,. ...,,. . . .

App. B—Indian Health Status Data ● 291
. . . . .
.-4
m **. . . . . . .
u l-r.1+
u r.l-‘+
- l o w - i. . . .
“f.1**l-l
m Ulw. . . . . . . . . . . . . .
“i mm mm 0 u-tt.-lv m
mo mmm. . . . . . . .twm *UIW
m
mm. . . . . . . .
N-.+
. . . .
... ,
. . .
0. . .
A’”””. .
. .
. . . . . . . .
. . . . . . . .
id

292 ● Indian Health Care
Oom k-1. . . . . . . . . .
0 0. . .hr..+ .-l
. .
.,
. .
. .
*“&
. .
. .
. .
. .
. .
*OI
“;4
. . .
. . .
. . . .
0, . .,.
:
N, . .,.,
z
. . . . . .
. . . . . .
. . . . .
. . . . . .
. . . . .
u-l mm
“4 “ ‘riam com. ..4.
.-l. . . . . .
mC-4N
u
“h”1-NA
0
“m!2
m
“ 0l-lu
0 ?+O .-4. . . . . . . . .
i- Wm,i$+ m.+e4
Aei
C-4 n-lNl-. . . . . . . .
d C+I .-4-7.-! -Am
*. .1.
. .
.
. .
. .
N
um l-1. . . . . .-N.-i
.- 4.+.+
c91fl c-4. . . . . .
m--lNm
molul. . . . . .
ON-7N.-i
0. . . . . .*A
mm. . . . . .

——— .
App. B—Indian Health Status Data Ž 293—
. ..
r.
im
. .
N
m.
,.
,.
.-l
0 0 0 0 0 0 0 0 0 0 0 0a 0 0 0 0 00,. . . .
i CiUld!-ii ‘,-lC4 * O NNIWN
0
.+m m w. .
mli &r+,+ ,-4
mmm. . . . . .m.;.+,++
,.
,,.
,.
ml-.. . . .r.m.-i
r . 0
4 “iN
elm. . . . . . . . . . .
r .2,+
., ...,,
. . . .
. .
. . . . . . . . . ,..
. .
0,4.
. . . .
.nww
3
*lng❑ oI-(V

660670030040250270420540580590610770840780
11111111111
192
34
1.41.41.41.41.41.41.41.41.41.41.4
25.82.7
46.2
54.8 5.9
21.9 .
8.7 “13.85.6 8.7 .11.2 34.6 41.5
21.0 .48.2
21.0 .31.9
21.0 .
95.7
105.0 191.3 144.6
122.1 .122.1 .
358.4
358.4358.4
122.1 .488.4 1433.7
732.6 1075.3
RATIO TOU.S. ALL-RACESME-ADJUSTED RATES
2.4 4.82.4 0.82.2 5.52.2 7.41.2 0.72.4 6.02.5 1.51.2 0.11.2 0.22.4 2.02.2 1.7
29.8 4.22.5 2.7
66.3 2.3

App. B—Indian Health Status Data ● 295
. . . . . . . . . . . . . . . . . . . . . . . .
w. .mN.-l
m.
u. .mW
mmmmm m f-. . . . . . . . . . . .
m. . . .mN
0 0. . . . . . . . . . . .
-W!+ .-4
. . . .
(-4 NN. . . . . . . . .
m mm
*OIU* .-i C-4 c-d
uirn&w-l
. . . .
0. . . . . . . . . . . .
SD
0 ! 0 0 0 00 0. . . . . . . . . . . .
0
‘i
,.
. . . .
0. . . . . . . . . . . .
.0. . . . . . . . . . . . . . . . .
m. . . . . . . . . . . .
0. . . . . . . . . . .
.-i
nC4u-l
3

0
“w
. .
,,
. .
. . .
. . .
W,.. .
0,.. .
i+
,.. .
,..
,.. .
,.. .
. .
WI.
z
.-IV,.. .
co~
+
0 0
l-i ‘Gvi-l
lwm.

App. B—Indian Health Status Data ● 297
m Omm mm. . . . . . . . .
.+ ml. wl *Av **.+ Am,+
euriw m. . . . . . . . . . . . . .
m f - r -. . . . . . .vm~
04 * m. . .
t-m m ‘iv .-(
mu -Y. .
+: ‘mmN
e . . . . .u’*
-*,-IN C-4. . . . . . . . . . .
w
t+”””. . . . . . .
m a r . d ,-4. . .*ma< . .;
I.-la-.+
.-4A. . . . . . .
r.l-
.+. . . . . . .*

U-I
W-4
. . .mm m, . .
“A- WIWIN N
Olw m. . . . . .*.-4NW! :
ma. . . . . . . . .
mQN*
C-J
WCnmm m. . . . . . . . . . . . .
Inlnu-lln *d-l- l-i m
mow-l mm a. . . . . . . . . . .b-!-!: .+0 a
F-Id .4
f-b b b I -. . . . . . . . . .
0 0 0 0 0.++ .-l !++
I--(.4. . . . .
‘0 0 C4-Am
. . . . . .
e. . . . .
mN
. . . . . . . . . . . . . .
- r -. . .Ins “ “ “ “
m. . . . .4
. . . . . .
. . . . . .
. . . . . . . . . . . . . .

App. B—lndian Health Status Data Ž 299
Ou-1. . . . ..+i$:
d ,+.-i W-l
“; “m”&*’ “Nr4.+
: C4Nd
m
G’””v
m. .hm
,.
. .
. . . . . . . . . .Q.+mm$nar. r .e4m4~~ummAI-l ,+
C--)- *O IL-I
’ 0 0 “ 0 0 0ml. -) -for)
,+ .+,+-Indml-l al-1. . . . . . . .-l!-4a 0 0 0n-1!-4fomuY .-l.+(-4
.+
02000 mo
&c.il.ii “ii04 -8(-4 w+(-4
0 0 0
“t-i; “ “i*U N
0 0,., .d.-4(NC+
m .+Uuu
muu.i ‘ ‘m - l .+,+
*m*um. . . . . .
‘Ul ( o v u mmr4drl N
urn. . . . . . . .
‘*UI.-( (-+
.,
.*. . . .m
. . . .
. . .
. . .
u
m
. .
*i
l-l. .
-?Ci ” ” ”
r+mu,..*U); “mum
-Y*. . . . . .m m
loco r.r.. . . . . .0 0 ****
. . . . . .,
,.
. .
u
‘i ‘ “ ‘mvv
“N.i.i “ “+.. .,..,
m
!!
aw(0
3

300 ● Indian Health Care—
,..
. . .
. . . .
0 0 0. . .,-4 . 4 :cNt+N
4.*.+
. .
1-
;
. .
0
A“u
1-
‘Ui
,,
m.
. . . . . .
u-l.+. . .*& “,+Ndw
. . . .
. . . .
. . .
. . . .
. . . .
. . . .
. . . .
m I-mmr.l. . . . . .
In. .
i0u
. .
. .
m. .0m
dt-i.+
,.. .
1-, . .
G
,.. .
0,.. .mu

App. B—Indian Health Status Data ● 301
.+
.+0 0. . . .*N NUN N
0 0 0400 d
44 iii ‘*”NC+ mNN -z
0 0. . .
m i’.-l,+
d,.,0!--l
0. . . . .
0(--,
0. . . . .
r.C-4
.
-Y Ooooo r4dd. . , . ,0 0 0 0 0 0 “000-7u-lu m.+!- -T f.f.u N,+
0 0 0 0. . . . . .0 0 0 0$064 (-4 A
.,,
a. .f.m
r. lmf.-
Ii “ “u(-iim U.+m
c1. . . . . . . .
a...
. .
w!. . ..,.

302 ● Indian Health Care
* *. . . . . . . . . . . . . . . . . .N0*
~*
+ .-4
. . .
. . .
0 0
“ 0 0e4e4
. . .
. . .
. . . . . .
. . . . . .
. . . . . .
mm. . . . . .
0. . . . . .NN
. . . . .
. . . . .
. . . . .
. . . . .
m m r -. . . . . . .lni.luim.+tnA

App. B—Indian Health Status Data ● 303
. . . .
.-4
e
‘Ii
1-. .
:
.
. .
. . . .
. . . . . . . ,.. .
ON I-U-I. . .***& . .
g::e.1
. . . . . . . . .
.,. .al. .
A“”””. . . . .
0
‘i “ “ “++
0 0 0. . . . . . . . . . moo. . . . . . . .. . . . . . .r- r.r-

304 ● Indian Health Care
. . .
. . . . .
*W
Mli‘a.-l
. .
m
&
. .
. .
. . . .
. . . .
0. . . .
.#
. . . .
0
*“””
mo. . . .*o
1-
0 m. . . . . . . . . .
* +
0
‘*
. .. . . . . . . . . .
0 0 0 0. . . . . . .‘u; !-*
,4. -4 m
0
‘; “mo
. . . .

App. B—Indian Health Status Data ● 305
** O!. +M4 Nwtiri Nr. *e e4r+eie4 Nm. . . . . . . . . . . . . . . . . . . . . . . . .
l-+m. . . . .
F1l.!-40,+ (-I
Ollnln mi“””m
mwm
.iC-4
. . . . .r’. wmcot.mmm
Om r- t-4-8.-(. . . .
U* *a-1 .+m .-l. . . . . . . .
.+.+ (0,-4
,+* am
;; “4;OJI. In.+
-m
U1.imd
.,.
b
i’m
N
s
i-m“CN
0,.,u,+
f.im
-s
z
,...., ...,iil-+
.,
1+.,
,..
...ho 0. . . . . . .mu *cod .+m
*(-4 0 0.,, ,.
.Y.n
nwIA
3

670660630730090140820030050130250270480500590610770840780
6144333111111111
132
49
10.81.87.27.25.45.45.41.81.81.81.81.81.81.81.81.8
23.43.6
88.1
14.0 .
56.2 .
14.0 :
14.0 .126.4 .
14.0 7.9
15.8
7.97.9
7.97.9
7.9
15.8
11.4 18.318.3
11.4 18.3
11.4 18.379.8 183.5
38.9
26.1 77.8
38.9
208.9 233.5
61.6 133.2
123.2 .
61.6 133.2
61.6 .61.6 .
61.6 .
246.3 798.9
14.02.68.94.49.16.95.93.03.01.51.5
452.5 1.5452.5 1.5
1.13.11.1
905.0 17.54.4
1810.0 119.1
4,55.1
12.80.83.85.31.07.5
30.1
0.93.70.3
11.12.60.92.54.94.2

App. B—Indian Health Status Data Ž 307
,+. . . . .G’N
U-I f-m. .(ornm” “mlr?a
m. . . . . ...
. . . . . .
0! m. . . . . .b r.
. . . . . . .
. . . . . . .
. . . . . . . . . . . .

670030730040050480490420500590610120250270630680770840780
5 9.14 7.34 7.33 5.51 1.83 5.53 5.52 3.72 3.72 3.72 3.71 1.81 1.81 1.81 1.81 1.8
16 29.31 1.8
57 104.3
13.9
55.8
27.9
13.9
139.4
27.9 23.2 39.5
11.9
11.9
59.7
19.4
155.0
28.1
28.1
28.128.128.1
28.1
393.1
39.3
39.3
39.339.3
39.3
117.9
275.2
67.167.1
67.1
67.1
67.1
67.167.167.167.167.167.1
402.7
161.0161.0
161.0
161.0
161.0
636.9
636.9
483.1 2547.8
11.612.54.59.23.29.28.56.62.36.64.71.13.23.23.23.2
28.33.2
147.6
2.412.50.7
11.532.21.51.03.0
11.32.93.62.81.56.44.06.42.21.53.5

App. B—Indian Health Status Data ● 309—
,-4
. . .
mmr. m mmr-f.. . . . .
au-. . . .mmmmm,+d
-O Olnwl. . . . . . .m.+ .+00r.r+ N$-+r.
Irllrl n - 1. . .
0 0 0.+,+.+
*O*. . . .400. - l - i ? - !
mumo+ o.+ 0mmm.+m,+m .+
0. .
r.
0 0. .r.r.
mmooo. . . . .
m.,
‘i”u
0 0. .-f.
e. . .
In
. .
,,. W. .
.+,+
*r.
&wmrA
,.,
.,
. . . .
.,.
.,.
.
. . .
. . . NN
C-7i.+.+

310 ● Indian Health Care
m m
;! “ “ “ “ “ “ “
em. . . . . . . . . .40em.-l
. .
. .
. .
0
“c
. .
. .
,.. ,
. . . .
. . . .
. . . .
. . . .
. . . .
. . . .
CN. . . . .ml.-l
(NW. . . . . .

App. B—Indian Health Status Data Ž 311
0. . . .
$.N.- 4-4. . . . . . .0 0 0r4um-,+(U
.+. . . . . .0
z
. . . . .I-4
Hu loo 0 I n d o u - l u - i n - l o u-l b-l. . . . . .mmWN
. . . . . .
u!. . . . . .
. .
(n w r -. . . . .
0 0(UN
. ..-l
. . . . . . . . . . .
. . . . . .
. . . . . .
. . . . . .
. .
Ml ’am. . . . . . . . .Centi*UN
m. . .. . . . . . . . . . .
. . . . . .
:
. . . .0 0. . . . . . . . .V)lnNti
. . . . .
40 0 0 0 ,+,-t,-. . . . . . . . . . . . . . . . . . . . . .
w0

270290490540570770840780
1111171
26
2 . 42.4 27.02 . 42.4 .2.4 .
16.9 54.12.4 .
62.8 54.1
2 5 . 011.4
12.5 11.4
56.756.756.7
170.0
20.7 85.5 146.9 566.6
140.1 . 2.5 6.32.1 5.32.8 0.92.8 0.32.8 2.5
16.8 2.42.1 2.3
420.2 469.5 69.6 2.5

App. B—Indian Health Status Data ● 313
.,.
-Y-Y
m -Y-7U. . . . . .m vu-lu br. h
-7
uf-
a
4-3.+
. . .
0
u“.
.
. . .
.+
C-J. . . . . .
.+*
w r 4 -. . ..+. +0mu!m
m -am,, .,..
.-l .NOOm Nmel
,+
t-l. . . . .
:
0 0. .u “vr+.+
0. . .
G’”U-1
. . . . . . .
. . . . . .
. . .
0. .(-i’””d
.

730550580020030040480590640670770840780
2 4.91 2.51 2.51 2.51 2.51 2.51 2.51 2.51 2.51 2.59 22.13 7.4
19 46.7
22.2 .74.474.4
25.9 .
30.6 .74.474.4
129.6 . 21.3 . 42.6 74.43 3 . 3
77.7 12.0 22.2 14.0 85.4 61.2 42.6 223.2
189.4 .189.4 .
628.9
628.9
189.4 628.9
RATIO TOUs. ALL-RACESAGE-ADJUSTED RATES
4.0 0.73.6 2.43.6 0.22.1 21.03.1 3.13.1 3.91.5 0.33.7 1.63.6 0.63.6 0.7
22.0 1.76.0 2.7
52.6 1.2

App. B—Indian Health Status Data ● 315
m !--ld
m - t - - 4 mr4=-?Q4mmwa. , . , . , . , . , . ,
Owmd.
m,+. rn$-1. r.
. . ..-+ f.-l*”&Nv< ‘iam me w-! .+.
-T
m
Udr.1
m
?-i
m
0 ’mm. .No
m.
.
mmm. .
000 “
,..
52 –80 5 0 – El ~, – 11

316 ● Indian Health Care
1-
&“”m
m
“4m.
L-4 emca m m. . . . . . . .
.-4 u-l?-?+ +“ “i(- !.+
WI*O
y.+
I.l N
,..
.,.
-?U
c-ii
,.,
mm
“ 0 0
. .
,-
=$
A’-Y
A
,.
0.’+. . . . .,.
. . . .
1.
,+ “i

App. B—Indian Health Status Data ● 317—
00 a
mm t-.0.0 m-s. r.
mm m
r.. r.00 n. . w
r.. r..
mmmmm.
ma m
am “cc. . .
.+ Lr)”-owl
mi
0
m
0 0
m .
mm
.Ae-, r.r-
.mr-
m
.
.C-lr.

090270630030040050140290250540820580570490280700720420480590610770840780
3.4 .
1.81.8
44.8 3.7 9.21.8
65.4 . 9.2
3.0
11.8
23.6
4.5
4.5
4.54.5
27.19.0
40.6
6.36.3
6.3
12.56.36.36.3
6.3
62.7
81.5
19.49.7
9.79.7
154.819.477.4
4 4 . 4
14.8
14.814.8
14.8
14.8
310.8
192.6
71.936.0
107.971.971.9
107.971.936.036.0
36.036.0
36.036.0
827.336.0
395.7
187.6562.9187.693.893.8
93.8
93.8
93.8187.6
93.8
21S7.6
1782.4
5.9 2.53.3 8.24.0 5.73.7 9.3
2.4 7.91.4 13.52.7 2.12.1 5.3
2.8 1.72.4 0.31.7 0.31.8 0.30.7 0.61.7 0.60.6 0.81.0 3.21.0 4.80.7 0.40.3 0.10.7 0.50.7 0.5
68.3 9.63.7 4.2
54.4 1.9

—
Ap
p.
B—
Ind
ian
H
ea
lth
Sta
tus
Da
ta
● 3
19
IHS
CODEa
ALL 790 800
810 310
410 350
360 390
320 330 400 340
150 170
220 200
180 240 230 210 160 510
520 530
820 830 430 620
470 440
450 730
740 760
750 640
670 660
CAUSE b
ALL CAUSES
ACCIDENTS / ADVERS · MOTOR VEHICLE
· ALL OTH ACCDNT DISEASE OF HEART
.ALL OTa HRT OS · . ISCHMC HRT DIS
. ACUT MYO INF
. OLD MI, OTHER
· RHEUM FEVER
· HYPRTNS HRT OS .OTB ENDOCRD OS · aYPRTNS+RENAL
MALIG NEOPLASMS .. MAL NEO-DIGEST
· MAL NEO-OTHER .. MAL NEO-GENITL
.. MAL NEO-RESPIR · . OTB NEOP L"iMPB
· . LEUKEMIA .MAL NEO-URINAR
· .MAL NEOPLS-LIP PNEUMONIA{ INFLNZ
. PNEUMONIA
· INFLUENZA SUICIDE HOMICIDE
CEREBROVASC OS LIVER DIS/CIRRHS
.ALL OTB CBV OS
· INTRCRB HMRHG · CERBRL THROMB
CONGEN ANOMALIES
PERINATAL CONDIT .OTH COND PERIN
· BIRTH TRAUMA
NEPHRITIS, ET AL
RENAL FAIL, ETC · CHRN GLMR/NEPB
DEATHS, AGE-SPECIFIC AND AGE-ADJUSTED DEATH RATES AND RATIO TO US. ALL RACES AGE-ADJUSTED DEATH RATES, 72 SELECTED CAUSES
11 IHS AREAS, 1980-82
BY LEADING CAUSES, BY BorH SEXES AND MAL EMAL
CRUDE
RATE TOTAL ALL 0-4
DEATHS AGES YEARS
1514 697 6 502.9
496 228.5 75 . 3 298 137.3 37.6 198 91 . 2 37 . 6 155 71.4 37.6
78 359 37.6 65 29.9
37 17 28 12
1
99 46 14 12
11
70
68 2
49 47
31 31
22 7
2 30 27 15
12 20 17
1 1.8 1 4 0.5
45.6 21. 2 6.5 5.5 5.1 2.8 2.3 1.8 0.5
32.3
31. 3 0.9
22.6 21. 7
14.3 14.3
10.1 3.2
0.9 13.8 12.4
6.9
5.5 9.2 7.8 1.4
23.9
20.5 3.4
3.4
3 85 85 5 44.5
41.1
NAVAJO
5-14 15-24 25-34
YEARS YEARS YEARS
60.7 494.0 670.3
31. 307.8 349.4 12. 223.5 222
18.4 84.3 127 1.8 5.9 12.7
1.8 2.0 6.4
1.8
1.8
3.7
3.7
1.8
3.9 3.2
9.8
2.0 3.9
2.
2
2.0
2.0
43. 39
3.9
2.
2.
3.2
6.4
3.2
3.2
15
15
57.2 25.4
22.2
6.
9.5 6.4 3.2
MALE
ULA AGE- RATIO TO 35-44 45-54 55-64 65-74 75-84 85 YEARS ADJUST U. S. ALL-RACES
YEARS YEARS YEARS YEARS YEARS AND OVER RATE AGE-ADJUSTED RATES
727.7 973 1476.2 2725.9 5628.815238.1 845.1 1.1 335.1 372 326.8 446.1 463.1 634.9 271.1 4.5 199.0 205. 124.0 214.8 178.1 105.8 156.8 4.8
136.1 167 202 8 231.3 285.0 529.1 114.3 4 2 26.2 91.2 191.6 578.2 1282.5 3280.4 93.3 0.3
20.9 38.0 33 8 165.2 676.9 2328.0 39.6 0.7 5.2 53.2 146.5 396.5 463.1 740.7 47.5 0.2
5.2 30.4 90.2 214.8 249.4 423.3 27.2 0.2
26.2 5.2
5.2 5.2
10.5
20.9 52.4
62.8
20. 20.
22.8 56. 181. 7 213.8 317.5 20.3 0.2 11. 2.1 1.2
142.5 16.5 105.8
105.8 91.2 135.2 429.5 783.8 1481.5 38.0 90.2 181. 7 498.8 740.7 7.6 99.1 106.9 211.6 7. 6 66.1 35.6 423.3
30.4 11.3 33.0 106.9 33.0 105.8
16.5 7.6 33.8
22.8
22.8
30.4 30.4
30.4
7.6
7.6
35.6 67.6 148.7 427.52645.5 67 6 148.7 427.5 2539.7
105.8
33.8 16.5
56.3 49 498.8 846.6 45. 16 106.9 22 33.0 427.5 634.9 33.8 16.5 71.3 105 8
105.8 105.8
33.8 33.8
49.6 106.9 211.6
33.0 106.9 211.6 16
2.3
1.6 0.3
65.8 31. 3
8.8 6.4 8.6 3.4
2.9 3.7
0.6 34.2
33.7 0.5
23.7 25.6
17.5 22.2
11.9 5.0
0.5 8.9 6.9 3.6 3.3
13 .1
10.9 2.2
0.4 0.6 0.3 0.4 0.8 0.4 0.4 0.1 0.4 0.4 0.5 0.1 2.1
2.1 0.9
1.3 1.5 0.4 1.4
0.4 0.8 0.1
1.5 0.7 0.5
1.0 2.3
2.2 3.7
a Equivalence to ICD-9 codes available from IHS. b Cause ranked in order by number of deaths for leading caUSeS

260140540580550570560030090420630040050290270080480490120250500610770840780
1811116221888871743331111
16519
179
8.35.15.12.80.90.90.53.73.73.73.73.20.53.21.81.41.41.40.50.50.50.5
76.08.8
82.5
6.83.4
3.4
13.7
20.5
10.3
3.4
3.4
51.33.4
75.3
1.8
12.9
5.5
45.17.8
27.4
3.23.2
3.2
50.819.185.8
5.25.2
5.2
5.2
36.610.5
115.2
22.815.27.6
7.6
7.6
7.6
7.6
7.6
106.415.2
106.4
45.1
45.133.8
11.3
11.322.556.333.811.3
11.3
169.011.3
180.3
99.1
16.5
16.5
16.5
16.5
16.516.5
462.649.6
297.&
317.535.6 317.535.6 317.535.6 211.6
105.8
106.9 317.5
35.6 .106.9 211.671.3 317.535.6 .3 5 . 61 0 6 . 9
211.6
3 5 . 6819.4 1693.1
641.3 2645.5
13.25.37.03.91.21.20.84.34.36.85.03.80.62.22.50.81.32.60.30.70.30.6
94.011.3
100.3
1.33.10.30.20.81.20.14.31.33.16.34.75.83.25.14.20.20.30.70.3l.40.47.25.12.4

App. B—Indian Health Status Data Ž 321
.
u
f.N
mm.
(-I-.*(-I.-l
m
A“”’m
. .A
m
0
N
. - i ” ” ’m
w m. . . . . . .i i
.,. .,
m. . .
.-4
-4
clm:moWV en

322 ● Indian Health Care
m 0 0. . . . . . .u mm
0 0: +,-4
...
U2 u
‘i ‘Q.-4
m,.
A’”l-w
w+ “0.+W
.
w-ll-,., .Wlri
W*. . . .mw
C’4,+
G. . .,,,u
m m. . , . , .
l-l .+
ma. . . .+
wmuwm.,.+,-i iit.i
u
,..
m
i“
m
0 “ ’
. . .
. . . . .
@. . . . .0
. . . . . .
m,.0“””
Vmo!. . . . . .Uob
. m: “ “ 0 0 0 0
m m.,
0“mo,, . . . .., ...,
0 0 - 8
m m. . . . . .
.-l ,-4

App. B—Indian Health Status Data Ž 323
.n-l. .m
.-4
U-I .--l-m m. ,.u ‘; “N ;“’” N C +;-” “w”u-a A
am
& “i
m m r.1.. . . .
A “A “ “m;
0 0 mchm O!ma-rf.. . . . . . . . . . . . . . . . . . . . . . . . . .

324 ● Indian Health Care
m. . . . . .
:
. . . .
. . . .
0!. . . . . .
.+. . . . . . . .
. .

Status Data Ž 325 . .,App.. B-—Indian Health—.
4
OJ.nou? r i m
Inlnom ”l.0 m r. r4 *“mf. vmdm
V I . .?4 ..- -Yme4c-’Jb
mor. r.,-l-Yti C-4
r40J.Y-Y r. I.r..,.+.i
w In,. ..,.
Ill u-ld
C-l U-l ml.?
z,+ .
-Y
Am
r. r. (w C41nwe+mmr+m

326 Ž Indian Health Care
N. . . . . .AN
+. . . . . .m
r-co. . . .;*Vlin .+-l
$++m U-1 u-in-1 Iii. -l,+ lnvl
,-4
m. . . . . .
m
m. . . .
u
. . . .
. . . .
. . .
. . .
f-
;“
,.. .
. . .
. . . .
. . . .
**,.CQli
. . . .
hl-. . . .
+.+
1.. .
.-4
. .
N-.4. . .
U-l?+rn. . .
03. . . . .
-1mr4,.. .. . . . . . . . . .
,-4
-u!. . .
r- r-ti. . . . . .
f- . . .“A
40!,., .,co1- :
** I-I*,+
. . . .mmN
m m.-!,+
i

App. B—Indian Health Status Data ● 327
. .
. ..
w
ii
ii . .
. .
. .
.,
m. ,(+’”’
r.m
i ‘A
w!+,.G “t-i
4 ,-4,+. . . . . .u i “t-i “ “
00+ Nlw. . . . . . .A&i “ ‘-i “u “
00. .. . . .

328 ● Indian Health Care
.
.
N
vim
r.. .v,-+
w-l ml-l .-mm. . . . . . . . .
A
,.
. .
*
‘4
.,
. .
m
‘i
.-4
0 0. . .mu
000 0. . . , . ,-saw *
0 am
u’ ‘m “Iim
. . ..-!
.
m. . .
,+
mm,.,.-l :“
m. . ..+
03-0,., .,.mm;N
,+. . . .C-4
N. . . . . . .i
. . . . .
NW mm,., .,.,-7-s i “W+
U)*
F-IN m,.mi “.4
. . . .

App. B—Indian Health Status Data ● 329
omr. m m m 0 0 Omamo
mac+
wo<
*O.+ d ,-(CO mm
0 0. .
r.r-, .
r..WI
-a
0N
am. +
.Vlm,+!-(m
u-la
OL‘a.
m
ir.
C- 4,+
mum
O*. . .
urn*u
-UN. .
r.r.. . . .m,--)c--, m
m-l. .
InN
,-4

4905405805502900301402506100500406306804207708&0780
5541k333321221
15b
83
4.34.33.40.93.42.62.62.62.61.70.91.71.70.9
12.93.4
71.4
16.9 .
8.4
8.4 .
5 0 . 6
50.6 8.3
3.83.8
11.5
5.1
5.1
10.210.240.8
7.7
7.7
7.7
99.8
10.8
10.832.3
10.8
10.810.8
129.4
15.7
15.7
15.7
15.7
31.4
26.953.926.926.9
26.9
26.926.9
26.9
26.9
26.9
404.2
191.9 .1 9 1 . 9
188.0
188.0
64.0 188.0
188.064.0 188.0
575.8 2443.6
AGE-ADJUSTRATE
5.76.14.81.33.23.63.73.22.82.31.31.82.00.6
12.03.6
83.8
RATIO TOU.S. ALL-FACESAGE-ADJUSTED RATES
1.90.60.82.28.09.12.91.92.1
23.14.42.53.30.41.74.03.0

App. B—Indian Health Status Data . 331
IwrJ. .+rJ. ..
I n Ooor)owuvm mmoco c o -. . . . . . . . .
.,+
co. . .;“
r-l .
-J- m“” “’
(-1 nlr-lm (-l. . . . .,..
wo<
*m%❑ oHu

332 ● Indian Health Care—
Un-1.+
0 0. . . .N;*O*.-4d.
. . .
,+Q“1-
. , .
*,..
1-.+
,..
. .
u. .
c-l
4m
.8. . .1-rl
a). .A,+
. .
.
*,..b.
,..
m
G“
. .
m
1+
. .
,.
,-4
*. . . . .V-I
u
&
,.
e. . . .
W-I
m. . .
A“ .,. ,
,+.., .,. .,. . . . .m
m. . . . .
1-*
l-l m. . . . . . .

App. B—Indian Health Status Data ● 333
!+ 4,+.4 +(-4 U? C-4-NQ3 u mm v. . . . . . . . . . . . . . . . . . . . . . . . . . .
4, +.-4
U*mm
-d
m
A“”u
.
.,. . .., ,., .
.+. .u
.-i

334 ● Indian Health Care
. . . . . . .
.-I I-If-l .-l. . . . . .(wlNe4 ir--b m
dul. . . . .
-8-U. .
??
!+. .1.‘-4
WW. . . . .C9m
., ...., . . . . .
mm. . ..-I(T
,-4
. . . . . . . ., .,,
0. . . . . . .l-i
. . . . . .., .
wV
.5w-l
0+. . . .
N*’ “ “w
l-l. . . . . ,-4 +.4 m+.+. . . . . . . .u
.cu
2

App. B—Indian Health Status Data ● 335
m
b bbl--4tN0.?4Nd
mm U-lm. .
,-11-lmm. . . .muumI-*.
Q.e mem
. . . . . . . . . .
au-a v “6N
.+m m. . . . . . .
.el m*.+
m. . , .A
0
i“’”. . . 0 0 0
.m-”v
. . . . . . . . . .
.-I* v.dai m’C-4u
0.+0!. .mr4imu+
daa.., .. ..,,,
dooOu-lm,+
., .,.,.,,,

336 ● Indian Health C a r e
*. . . . .mm.-l
Iii.
*e
. . .
. . .
. . .,. m+. . . .*.-I,+In
.+
me+
4 “AC-+-4
e4eJe4. . . . .
,-4 .+4. + , + . - l
. . .‘a*.+
**. . .r- l-l
In
m<. . .vm
u
m. . .e-l
. . .
,..
,..
.
. . .
*. . .m
. . . .
.., .
. . . .
*“0 “m
,-4

App. B—Indian Health Status Data ● 337
r.0r4NN
Od o d d
m am-ma. . . .u.dmmuo.+m r.
,.1.(wm
-mu-mm-am. . . . . .
O**
C.;**V)OI
.
-Y
.+w
*
0,+
,.
w-l. .m
L%”m
da. . . . . .
,-lmmri
u (--4 -NW. . ,-7
0.
m. . .
m
m u-l.
m Ar.
.-l. .
m
tin

338 ● Indian Health Care
0. . . . . . .
C-4 L-i. . . . .N 4m m
. . .r-Q0!+
e+ WC-4. . . . . . . . . .
c+ mmm Com
we+“$i ‘m
o0.+
m moa4“””” “ci~e-l
m. . . . . .Nm
WI 0 0
L “AA “ “ “ “‘+ mm
U-lul In. . . . . . . .++ -1,-4.+ ,-4
moo!. . . ..+ *!-+.+-7m
. . . .
Com. .r-b
. .
.
. .
m;’
. . . . . . . .
. . . . .
m. . . . . . . . . . . . . . .
m.o“ 0 “ 0+-#N
,4
O.i. . . . .
n-
i

App. B—Indian Health Status Data Ž 339
.+,.
-s
4’*.4
m.+.+ Olmmmm !+ . - (Ulr+fl$+ .+ .-4 N
02
,, ,...+ ,4’+
w
ii
i
.1..,. . .<0.
w-l. . . .
4N
a,.
G
.,
.
.
.
. . . .
f.-. . . .m m
*A. . . . . . . .Cob
m
04(--4. . . . . . .,., . . . .m m
. . . . . . . . . . .mr.
WumoHW

340 ● Indian Health Care
m. . . . .m0*
.+ .-l
0 “~r.
4,. . . ,
u-lu
a. .mw
. .
,., ,.
,., ,.
. . . . .
A
mm *
Wd. , . m:-Y.-l
U-lm. . .+0NW-l
.-l
,+++Vv”i.-l,-twl
(-4. . . .m

App.
B—
Indian H
ealth S
tatus D
ata ●
34
1.
0r-’
d
,..
t.:Nr..
d.
mm
r..m00
.,r.<.-.
.a“
$-).
.-?m
mS+mm
Bwm3m
DEATHS, AGE-SPECIFIC AND AGE-ADJUSTED DEATH RATES AND RATIO TO U. S. ALL RACES AGE-ADJUSTED DEATH RATES,
IHS CODE'·
ALL
310 410
350 390 360 320 330 790 800 810 260 090
620 150
170 220 200 210 230 430 440 470
450 510 520 420
820 140
640 670
730 740
760 010
030 04 Q
490 540
CAUSEb
ALL CAUSES
DISEASE OF HEART · ALL OTB HRT DS · ISCBHC HRT DIS
. OLD HI, OTHER
.ACUT MYO INF
· . RHEUM FEVER
· BYPRTNS HRT DS ACCIDENTS/ ADVERS · .MOTOR VEHICLE · . ALL OrB ACCDNT DIABETES MELLITU SEPTICEMIA
LIVER DIS/CIRRBS MALIG NEOPLASMS
· MAL NEO-DIGEST · .MAL NEO-OTHER
· MAL NEO-GENITL .MAL NEO-URINAR
. LEUKEMIA CEREBROVASC DS
· INTRCRB BMRBG · ALL OTB CBV DS
· CERBRL THROHB PNEUMONIA/INFLNZ
. PNEUMONIA BYPRTNS+/- RNL
SUICIDE ALL OTB INF /PARA NEPHRITIS, ET AL
· RENAL FAIL, ETC CONGEN ANOMALIES PERINATAL CONDIT
.OTB COND PERIN SHIGELL/AMEBIASI TUBERCULOS I S
· TB-RESPIRATORY OTHER ARTERY DIS CHRON PULMON DIS
TOTAL
DEATHS
151
29 15 12
19 14
5
.. Equival~nce to 1CD-9 codes available from IHS.
CRUDE
....&ill... ALL
AGES
591.1
113.5 58.7
47.0 27.4 19 6
3.9 3.9
74.4
54.8 19.6
35.2 31. 3 31.3 27.4
7.8 7.8
3.9 3 9 3.9
23.5
11 7 7.8
3.
19. 19.6 15 7
15 7 11 7
11 7 11 7 11.7
7.8
7 8 3 Q
3 Q
3 'I
3 9
3 9
b Cause rank~d in order by 111..unber of death., for eading caU!5f"s.
72 SELECTED CAUSES 11 IHS AREAS, 1980-82
BY LEADING CAUSES, BY BOTB SEXES AND MALE/FEMALE
TUCSON FEMALE
AGE-SPECIFIC DEATB RATES (PER 100, 000 POPULATION) AGE- RATIO TO
0-4 5-14 15-24 25-34 35-44 45-54 55-64 65-74 75-84 85 YEARS ADJUST U.S. ALL-RACES
\'EARS YEARS YEARS YEARS YEARS YEARS YEARS \'EARS YEARS AND OVER RATE AGE-ADJUSTED RATES
534.1
31.4 31. 4
94.3
3l.4
62.8
3l. 4
3l. 4
94.3 62.8
62.8
65.6
65.6 65.6
36.3
5l. 1
51. 1
17.0 17.0
17.
34 1
299 7
81 7
81 7
8 7
54.5
243.0 969.3 1752.9 4672.9 6441. 7518.8 40 161.6 166. 2002. 1840 751.9 40 53 9 83. 934. 1227.0
53.9 83.5 934.6 613.5 751.9 534.0 613.5 751.9
53.9 83.5 400. 133
53.9 215.4 306.7 751.9
161.6 53.9 306 7 751.9
166.9 267.0 1533.7 53.9 83.5 400.5 613.5 751.9
161.6 306.7 333.9 267.0 83.5 133.5 83.5 133.5
83.5 83.5
250.4 267.0 306.7
250.4 267. a
306.7
53.9 133.5 1503.8 53 133.5 1503.8
40.5 53. 133.5 751.9
53.9 166.9 53. 83 5 133.5 53. 83.5 133 5
83.5 133.5 133 5
751.9
306.7
781.2
173.6 88
72. 39.7 32.4 6.5
6.2 74.2 55 19
53 45
40.7 42 5 13.1 13.1 6.6 6.6 3.1
38.3
19 13.
5 20
20.2 20.
15 19.3
19 3 19.3
7.5 5.0
5. a 6.6
6.5 6.5
2.5
5.5
1.9
1.3 2.9
0.8 0.9
0.6 2.4
1.2 3.6 4.9 2.1 5.6
19.1
5.5 0.4
0.5 0.9
0.5 2.2 0.8 1.1 3.6 0.6 0.9 2.2
2.3 12.3
2.7 14.9
1.4 0.6
0.9
16.3 21.8
0.8 0.6

Deaths, Age-Specific and Age-, ~ I\)
• :;-
AGE-SPECIFIC DEATH RATES {PER 0,000 PO~!:!.!a\n2!!1 ~ TOTAL ALL 0-4 5-14 15-24 25-34 35-44 45 4 55-64 65-74 :;:, CODE CAUSE DEATHS AGES YEARS YEARS YEARS YEARS YEARS YE .s YEARS YEARS ::r:
(f) Cb
580 .. OTH CHRN PUU«> 3.9 S 3.9
~ 3.9
610 HERRIAI IMTST .OBS 680 ltIDNEY INFECTION 830 HOMICIDE 3.9 40.5 ~ 770 SYHP!SIGH!ILL-Df 10 39.1 94.3 53.9 840 ALL OTH EXl'RJ(L C 2 7.8 17.0 27.2 780 ALL OTHER DISEAS 22 86.1 125.7 54.5 121.5 107.7

App. B—Indian Health Status Data ● 343
.-l
,.
.,
.
-mmmm.,. m
. . .
,..do
0 “;muN
0000. . . .(-4Nmmmmmu
N-s
& “mNb-1
.,.
. . . .
,..
-aPi”*d
. . .
,,,,-.:
nww
5

Deaths. Age-Speci£ic and Age-adjusted Death Rates. Tucson Male (cont' d
• AGE-SPECIFIC DEATH RATES ~P!! 100 000 POPULATIOIf~ AGE- RATIO TO
TOTAL ALL 0-4 5-14 15-24 25-34 35-44 45-54 55-64 65-74 15-84 85 YEARS ADJUS1 U.S. ALL-RACES CODE CAUSE DEATHS AGES YEARS YEARS YE.AlI.S YEARS YEARS YEARS YE.AlI.S YEARS YEARS AND OVER RATE AGE-ADJUSTED RATE~
150 .. BIRTH TRAUMA 8.2 62.3 5.0 I.! 140 ALL OTH IlIF I p AltA 4.1 91.9 8.0 4. ,
280 ANEMIAS 4.1 141.5 1.1 1.1 290 MENINGITIS 4.1 31.1 2.5 3.E 490 OTHER ARTERY DIS 4.1 141.5 1.1 O.~
590 ULCEll-STOH. DUOD 10 .1 65.8 1.9 3. J
690 PROSTATE HYPERPL 1 4.1 900.9 2.2 5.1 780 ALL OTHER DISEAS 27 111.3 62.3 16.2 35.6 58.4 184.1 191.5 489.7 295.0 909.1 2702.7 148.5 3. ! 840 ALL OTH EXl'RNL C 4.1 97. 9 8.0 3. t 770 SYMP I SIGN I ILL-OF 24 99.0 2"9.1 29.2 46.0 65.8 195.9 590.0 1818.2 900.9 115.4 8.l

. .
Appendix C
INS Allocations by Area and Budget Category, with Service Populationand Util ization Data, Fiscal Years 1 9 7 2 - 8 5
IHS Allocations by Area and Budget Category, with Service Population Data, Fiscal Year 1 9 8 5a
Service C l i n i c a lArea P o p u l a t i o n S e r v i c e s. . . . . . . . . . . ....--. . . . . . . . ------- ------- . . . .
Aberdeen 72,679 S61,025,600Alaska 73,351 101,786,500Albuquerque 52,471 44,003,900Bemidj i 48,245 32,103,900B i l l i n g s 41,326 42,449,200C a l i f o r n i a 73,414 24,760,500Headquarters East o 22,887,200Headquarters West o 2,561,100Nashvi l le (USET) 36,413 27,823,000Navajo 166,493 92,392,800Oklahoma 195,346 83,591,100Phoenix 84,516 73,859,000Port land 98,996 39,305,400Tucson 18,332 13,559,700
C o n t r a c tC a r e b
. . . . . . . . . . . . . .
$22,008,00019,677,00011,246,0009,304,000
18,990,100534,000
00
6 , 9 3 3 , 0 0 019,242,00017,349,90014,618,00019,547,0004,507,000
PreventiveHealth Other
. . . . . . . . . . . . . . . . . . . . . . . . .
S7,151,600 % , 0 9 2 , 9 0 010,352,100 7,654,0004 , 1 1 0 , 0 0 0 < ’ 5 , 2 5 1 , 4 0 03,578,500 3 , 6 4 9 , 7 0 04,386,300 4,659,5001,923,900 4,558,900
107,500 14,929,700528,000 3 , 4 7 5 , 3 0 0
2,168,100 2 , 4 3 0 , 5 0 09,902,900 4 , 5 3 8 , 9 0 08,032,100 6 , 9 1 7 , 2 0 07,402,700 7,107,9004,321,300 5,571,8001,757,000 2,479,300
TOTAL FY 85. . . . . . . . . . . . . . .
$74,270,100119,792,600
53,365,30039,332,10051,495,00031,243,30037,924,400
6,564,40032,421,600
106,834,60098,540,40088,369,60049,198,50017,796,000
Total FY 1985: 9 6 1 , 5 8 2 S 6 6 2 , 1 0 8 , 9 O O $ 1 6 3 , 9 5 6 , 0 0 0 S 6 5 , 7 2 2 , 0 0 0 $ 7 9 , 3 1 7 , 0 0 0 $807,147,900
a Fiscal year 1985 allocations include 1985 supplemental p a y a c t a p p r o p r i a t i o n s ; f i g u r e sf i n a l a s o f 9 / 2 6 / 8 5 .
b C o n t r a c t c a r e a l l o c a t i o n s a r e i n c l u d e d i n t h e c l i n i c a l s e r v i c e s a l l o c a t i o n s f o r f i s c a l y e a r s 1 9 8 1 - 8 5 .
IHS Allocations by Area and Budget Category, w i th Serv ice Popu la t ion and Ut i l i za t ion O a t a , F i s c a l Y e a r 1 9 8 4
S e r v i c eArea P o p u l a t i o n. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aberdeen 70,648Alaska 71,329Albuquerque 51,211Bemidj i 47,000B i l l i n g s 40,106C a l i f o r n i a 71,642Headquar ters East oHeadquarters West oNashvi l le (USET) 35,822Navajo 162,005Oklahoma 190,451Phoenix 82,309P o r t l a n d 96,427Tucson 17,852
C l i n i c a lS e r v i c e s
. . . . . ------ . . . .
$59,951,000104,469,40043,349,00031,082,40042,590,00021,390,50021,228,700
2,906,80026,209,60090,383,90080,237,40070,816,80038,140,70012,756,000
ContractCare b
----- . . . . . . ---
S20,029,00019,296,00010,694,0008,980,000
18,976,000525,000
00
6,712,00019,074,00016,478,00014,284,00018,549,0004,330,000
P r e v e n t i v eH e a l t h
- - - - - - - - - - -
$7,104,1007,719,4004,098,4003,455,6004,404,6001,861,500
111,700502,000
2,074,0009,155,1007,919,6007,098,1004,299,3001,792,600
Other---- . . . . . -----
$6,063,9007,755,7005,325,6003,506,2004,676,7004,247,400
14,742,0003,510,5003 , 0 8 8 , 1 0 04,569,1006,685,7006,524,1005,380,9002,416,200
TOTAL FY 84....- . . . . . . .
$73,119,000119,944,500
52,773,00038,044,20051,671,30027,499,40036,082,400
6,919,30031,371,700
104,108,10094,842,70084,439,00047,820,90016,964,800
O u t p a t i e n tD i s c h a r g e s V i s i t s. . . . . . . . . . . . . . . . . . . . .
1 0 , 7 3 1 4 1 1 , 7 6 49 , 8 9 5 2 6 2 , 3 8 05 , 6 3 2 2 7 1 , 6 5 41 , 5 8 9 1 0 9 , 3 8 63 , 4 5 9 2 7 6 , 7 6 7
. .
. .
.- .1 , 3 1 9 6 0 , 9 0 1
1 8 , 6 4 7 6 2 8 , 0 8 51 1 , 6 0 6 5 6 6 , 3 7 31 3 , 4 1 9 3 8 9 , 7 9 9
2 1 2 , 5 4 71 , 2 7 8 5 9 , 0 0 4
Total FY 1984: 936,802 $645,512,200 $157,927,000 $61,596,000 $78,492,1OO $785,600,300 7 7 , 5 7 5 3 , 2 4 8 , 6 6 0
b C o n t r a c t c a r e a l l o c a t i o n s a r e i n c l u d e d i n t h e c l i n i c a l s e r v i c e s a l l o c a t i o n s f o r f i s c a l y e a r s 1 9 8 1 - 8 5 .
IHS Allocations by Area and Budget Category, wi th Serv ice Popula t ion and Ut i l i za t ion Data , F isca l Year 1983
S e r v i c e C l i n i c a l Contract P r e v e n t i v e O u t p a t i e n tArea P o p u l a t i o n Services Care b Health Other TOTAL FY 83 D i s c h a r g e s V i s i t s. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ..-.--
Aberdeen 68,688 $53,863,200 $17,171,000Alaska 69,383 93,129,300 17,644,000Albuquerque 49,997 39,961,700 9,406,000Bemidj i 45,821 27,389,600 7,927,000B i l l i n g s 38,935 38,049,600 16,686,000C a l i f o r n i a 69,989 19,074,000 475,000Headquar ters East o 16,957,500 50,000Headquarters West o 2,429,200 0Nashvil le (USET) 30,6454 22,957,000 6,054,000Navajo 157,627 76,543,200 16,185,000Oklahoma 185,811 67,286,400 13,971,000Phoenix 80,203 64,390,300 12,862,000P o r t l a n d 87,881 34,402,200 17,039,000Tucson 17,400 12,656,600 4,352,000
Total FY 1983: 902,399 $569,089,800 $139,822,000
b c o n t r a c t c a r e a l l o c a t i o n s a r e i n c l u d e d i n t h e c l i n i c a l
$ 6 , 1 2 2 , 6 0 0 $ 5 , 4 6 9 , 6 0 06,310,400 7,459,0003,836,800 4,756,0003,127,200 2,836,2003,999,900 4,142,4001,434,300 3,187,400
2 2 2 , 5 0 0 1 3 , 3 4 4 , 9 0 0460,000 2,537,600
1,732,100 2,151,4007,597,200 4,180,7006 , 9 2 0 , 0 0 0 5,594,5006,713,700 5,967,0003,530,900 4,456,1001,538,500 2,253,200
$53,546,100 $68,336,000
s e r v i c e s a l l o c a t i o n s f o r
% 5 , 4 5 5 , 4 0 0106,898,70048,554,50033,353,00046,191,90023,695,70030,524,900
5,426,80026,840,50088,321,10079,800,90077,071,00042,389,20016,448,300
$690,971,900
1 0 , 9 6 99 , 5 5 05 , 1 9 01 , 7 3 23 , 5 6 4
. .2,201
18,66712,17012,881
1,200
78,124
f lscal years 1 9 8 1 - 8 5 ,
411,928259,227273,681106,135268,768
. .
83,857586,752593,131402,717206,028
6 0 , 4 7 7
3 , 2 5 2 , 7 0 1
345

346 Ž Indian Health Care
IHS Al locations by Area and Budget Category, wi th Serv ice Populat ion and Ut i l i zat ion Data, F i scal Year 1982
Service C l i n i c a l Contract Preventive OutpatientArea Populat ion Services Care b Health Other TOTAL FY 82 Discharges V i s i t s. . . . . . . . . . . . . . . . . ------ ------ . . . . . . ------ ------ ----- . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aberdeen 66,805 $47,020,800 $13,781,000 $6,103,8OO $6,224,300 $59,348,900 10,642 386,227Alaska 67,521 83,595,500 12,325,000 5,950,200 6 , 8 1 1 , 3 0 0 96,357,000 8 , 9 7 3 265,720Albuquerque 48,825 3 38266,400 8,229,000 4,079,000 4,471,600 41,817,000 4 , 8 7 7 276,761Bemidji 44,711 24,502,900 3,967,000 2,978,400 2,847,600 30,328,900 1,962 103,584B i l l i n g s 37,813 33,818,300 14,973,000 4,009,100 4,134,200 41,961,600 3 , 8 9 9 261,723C a l i f o r n i a 68,460 16,099,800Headquarters East o 16,789,000Headquarters West o 2,499,800Nashvi l le (USET) 28,136 17,986,700Navajo 153,360 65,413,400Oklahoma 180,664 59,542,100Phoenix 78,206 61,478,400Port land 79,086 31,028,800Tucson 16,980 10,983,000Regions o 21,400
Total FY 1982: 870,567 $ 5 0 4 , 0 4 6 , 3 0 0 $ 1
377,00000
2,854,0001,255,0000,721,0002,572,0005,177,0004,196,000
0
1,327,800218,000480,000
2,072,0008,375,1007,940,5006,553,4003,356,1001,619,600
0
2,898,90013,154,1003,007,6001,882,0004,108,1005,831,4005,599,3005,194,1002,370,700
0
20,326,50030,161,100
5,987,40021,940,70077,896,60073,314,00073,631,10039,579,00014,973,300
21,400
2,0358,3282,7852,403
1,248
75,833644,806646,136419,450194,686
59,439
0,427,000 $55,063,000 $68,535,200 $627,644,500 77,152 3,334,365
b Cont ract care a l locat ions are inc luded in the c l in ica l serv ices a l locat ions for f i scal years 1981-85.
IHS Allocations by Area and Budget Category, wi th Serv ice Populat ion and Ut i l i zat ion Data, F i scal Year 1981
Service C l i n i c a l Contract Preventive OutpatientArea Populat ion Services Care b Health Other TOTAL FY 81 Discharges V i s i t s. . . . . . . . . . . . . ------ . . . . . . . ------ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aberdeen 64,990 $44,491,400 $12,953,700 $ 6 , 9 9 4 , 9 0 0 $ 5 , 0 0 9 , 7 0 0 $56,496,000 11,636 383,486Alaska 65,743 83,796,100 11,267,000 6 , 5 6 8 , 6 0 0 6 , 8 4 2 , 2 0 0 97,206,900 10,274Albuquerque 47,695 32,892,000
203,3598,474,300 4,661,700 4,722,600 42,276,300 5,135 262,596
Bemidji 43,664 23,157,800 3,941,000 3,315,400 2,869,800 29,343,000 1,811 98,724B i l l i n g s 36,735 32,446,500 14,461,000 4,489,200 4,016,400 40,952,100 3,722 270,781C a l i f o r n i a 67,048 14,616,700 241,000 1,484,600 3,909,600 20,010,900Headquarters East 0 17,476,500
. .3,000,000 1 6 1 , 0 0 0 1 2 , 9 2 8 , 2 0 0 30,565,700
Headquarters West
. .
0 2,979,000 467,100 2,632,500 6 , 0 7 8 , 6 0 0Nashvi l le (USET) 27,181 18,797,100
. -3 ,205 ,00 ; 2,459,800 2,190,200 23,447,100 2,160 89,026
Navajo 149,208 61,322,800 10,779,700 9 , 4 0 2 , 3 0 0 4 , 1 5 9 , 6 0 0 74,884,700 18,311 632,505Oklahoma 176,527 55,175,700 9,164,000 8,684,900 6,081,300 69,941,900 13,414 620,097Phoenix 76,309 55,769,800 12,228,200 7,148,400 6,503,800 69,422,000 14,033 425,113Port land 77,385 27,673,400 14,255,000 3,772,800 5,131,300 36,577,500 188,411Tucson
. .
16,590 10,293,200 3,682,100 2,046,800 3,701,400 16,041,400 1,149 52,964
Total FY 1981: 849,075 $480,888,000 $107,652,000 $ 6 1 , 6 5 7 , 5 0 0 $ 7 0 , 6 9 8 , 6 0 0 $ 6 1 3 , 2 4 4 , 1 0 0 81,645 3,227,06
b Cont ract care a l locat ions are inc luded in the c l in ical serv ices a l locat ions fo r f i scal years 1981-85.
IHS Allocations by Area and Budget Category, with Service Population and Util ization Data, Fiscal Year 1980
Service D i r e c t IndirectArea Populat ion Pt . Care Pt . Care. . . . . . ------- ------- ----- . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aberdeen 63,253 $13,210,600 $11,993,800Alaska 6 4 , 0 4 7 32,580,000 12,890,500Albuquerque 46,610 10,662,500 7,934,000Bemidji 42,686 2,298,700 4,892,000B i l l i n g s 35,708 5,137,200 14,031,400C a l i f o r n i a 65,757 4,534,000 925,000Headquarters East o 13,164,700 2,700,000Headquarters West o 1,048,200 0Nashvi l le (USET) 26,731 3,168,900 6,221,200Navajo 145,162 26,616,400 12,642,700Oklahoma 172,636 16,193,300 7,433,000Phoenix 74,020 20,341,700 11,976,200Port land 75,769 1,020,000 13,478,000Tucson 16,230 5,231,000 2,088,000
Total FY 1980: 8 2 8 , 6 0 9 $ 1 5 5 , 2 0 7 , 2 0 0 $109,205,800
P r e v . H l t h / OutpatientAmb. Care Other TOTAL FY 80 D i s c h a r g e s V i s i t s
. . . . . . . . . . . . . . . . . ------ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . -----
S 2 3 , 2 2 1 , 3 0 0 $ 4 , 0 9 5 , 9 0 0 $52,521,600 11,614 374,66835,955,700 6,186,600 87,612,800 10,646 271,91416,974,700 3,764,500 39,335,700 4,344 249,67115,231,500 1,715,000 24,137,200 1,555 92,82816,034,200 3,112,400 38,315,200 3,843 249,0226,478,200 668,800 12,606,000 . . . .
2 , 4 0 5 , 7 0 0 1 0 , 5 1 2 , 8 0 0 28,783,200 . - . .2,525,000 2,035,900 5,609,100 . . . .7,692,500 1,583,000 18,665,600 2,112 87,472
30,373,800 2,671,500 72,304,400 18,270 651,29031,970,700 4,275,700 59,872,700 11,060 569,47627,169,100 4 , 4 6 9 , 1 0 0 63,956,100 13,348 416,04915,803,700 2,461,500 32,763,200 . . 176,1506,046,000 1,169,100 14,534,100 1,063 56,396
$237,882,1OO $48,721,800 $551,016,900 77,855 3,194,936

App. C—IHS Allocations by Area and Budget Category, With Service Population and Utilization Data, FY 1972-85 ● 347
IHS Allocations by Area and Budget Category, with Service Population and Utilization Data, Fiscal Year 1979
S e r v i c e D i r e c t I n d i r e c t P r e v . H l t h . / Out patientArea P o p u l a t i o n Pt. Care Pt. Care Amb. Care Other TOTAL FY 79 Discharges V is i ts
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aberdeen 6 1 , 6 0 7 $12,221,300 $10,627,000 $23,309,300 $1,685,300 $47,842,900 10,958 371,766Alaska 62,223 30,020,000 11,303,500 34,605,900 2,477,400 78,406,800 9,921 245,227A b u q u e r q u e 45,360 9,476,400 7,253,400 16,249,800 1,%55,900 34,715,500 4 , 0 4 9 229,545B e m i d j i 39,-
B i l l i n g s 34C a l i f o r n i a 61H e a d q u a r t e r s E a s tH e a d q u a r t e r s W e s tN a s h v i l l e ( U S E T ) 25N a v a j o 138Oklahoma 165P h o e n i x 71
963 2,367,500 4,269,000 15,231,600 o 21.868,100 1,483 82,836932324
00
910531448565
5,327,4004,292,800
18,293,8001,385,8002,775,900
24,542,80013,827,60018,224,300
11,826,200691,000
2,400,00075,000
5,113,60011,347,8006,789,200
10,454,900
16,255,400 1,463,5005,596,800 01,676,100 4,199,0001,861,900 1,605,3008,799,900 0
29,841,400 985,30030,583,300 1,799,70026.304,400 1,864,700
34,872,500 3 , 9 2 9 230,71310,580,600 . . - -26,568,900 . . . -
4 ,928,000 . . . .16,689,400 2,086 85,03766,717,300 18,482 686,74252,999,800 10,744 525,35656,848,300 12,469 403,014
P o r t l a n d 68,041 1,207,900 11,117,300 15,682,200 7 7 7 , 7 0 0 28,785,100 -- 170,832Tucson 15,582 5,279,200 1,586,100 7,223,600 0 14,088,900 1,137 52,282
Total FY 1979: 790,486 $149,242,700 $ 9 4 , 8 5 4 , 0 0 0 $ 2 3 3 , 2 2 1 , 6 0 0 $ 1 8 , 5 9 3 , 8 0 0 $495,912,100 7 5 , 2 5 8 3 , 0 8 3 , 3 5 0
IHS Al locat ions by Area and Budget Category , wi th Serv ice Popula t ion and Ut i l i za t ion Data , F isca l Year 1978
S e r v i c eArea P o p u l a t i o n. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aberdeen 57,546Alaska 60,964Albuquerque 44,811Bemidj i 37,444B i l l i n g s 34,024C a l i f o r n i a c 57,803Headquar ters East oNashvi l le (USET) 22,729Navajo 130,919Oklahoma 156,587Phoenix 68,649P o r t l a n d 40,140Tucson 1 4 , 9 3 5
D i r e c tPt . Care
----- . . . . . . --
$11,300,90027,127,000
9,686,2001,872,2004,638,1003,783,800
16,739,8002,468,300
20,873,50012,616,30014,252,900
879,6004,261,000
I n d i r e c tPt . Care----- . . . . . .
$9,948,30010,799,900
6,395,0003,887,200
11,826,600229,000
1,753,0003,644,800
11,471,5006,156,700
11,314,0009,974,0001,442,000
Total FY 1978: 726,551 $130,499,600 $88,842,000
P r e v . H l t h . /Amb. Care Other
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
$20,371,600 $1,670,00032,287,700 2,514,10015,481,800 3,158,20010,362,900 013,957,700 1,363,6004,302,200 01,270,600 4,342,1007,055,500 0
26,662,700 920,30028,106,300 1,746,80022,908,100 1,819,40013,307,400 752,6006,752,500 0
$202,827,000 $18,287,1OO
c C a l i f o r n i a o f f i c i a l l y a d d e d a s a n I H S s e r v i c e a r e a .
IHS Al locat ions by Area and Budget Category , wi th Serv ice Populat ion and Ut i l
S e r v i c e D i r e c t I n d i r e c t P r e v . H l t h . /Area P o p u l a t i o n Pt. Care Pt. Care Amb. Care. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ------ . . . . . . ------ ---- . - . - . . - . . . -
Aberdeen 55.968 $10,192,300 $7,541,700 $ 1 6 . 4 8 3 , 2 0 0 $ 1 ,
O u t p a t i e n tTOTAL FY 78 Discharges V is i ts
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
$43,290,800 12,429 382,00372,728,700 10,119 305,59534,721,200 3,894 215,99916,122,300 1,663 83,45131,786,000 3 , 5 6 9 238,389
8 , 3 1 5 , 0 0 0 . .
24,105,500 . - . .
13,168,600 2 , 2 7 9 88,61159,928,000 19,032 722,18548,626,100 10,755 472,31650,294,400 12,782 403,98224,913,600 . . 159,80412,455,500 1,090 52,381
$440,455,700 7 7 , 6 1 2 3 , 1 2 4 , 7 1 6
izat ion Data, F isca l Year 1977
O u t p a t i e n tOther TOTAL FY 77 Discharges V is i ts------ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
521,300 $35,738.500 13,161 383.300AlaskaAlbuquerqueBemidj iB i l l i n g sC a l i f o r n i a d
Headquar ters EastNashvi l le (USET)NavajoOklahomaPhoen ix d
P o r t l a n dTucsonRegions
59,71043,35035,78033,262
00
13,037126,000149,444
66,10838,36714,287
0
23,193,8006,294,8001,600,4003,762,600
11,00012,531,5002,250,200
18,670,80010,584,50013,075,500
821,3003,543,000
63,900
7,127,1005,117,3003,258,0007,850,100
01,190,0001,826,3008,100,3005,047,3007,519,0007,933,900
712,0000
26,907,50011,044,700
7,253,70011,593,400
01,977,7005,882,800
22,189,60021,036,70020,650,00010,374,9005,637,800
0
2,346,0002,668,300
01,271,800
04,046,000
01,007,1001,639,8001,680,500
684,20000
59,574,40025,125,10012,112,10024,477,900
11,00019,745,2009 , 9 5 9 , 3 0 0
49,967,80038,308,30042,925,00019,814,3009,892,800
63,900
Tota l FY 1977: 635,313 $106,595,600 $63,223,000 $161,032,000 $16,865,000 $347,715,600
10,2343,4421,6313,504
. .
2,05219,29710,32213,800
- -
1,078.
78,521
285,340205,426
78,244238,229
. .
86,187648,682432,219404,484147,32651,413
. .
2,960,850
d P h o e n i x s e r v i c e a r e a a l l o c a t i o n s i n c l u d e l i m i t e d f u n d i n g f o r t h e C a l i f o r n i a F i e l d O f f i c e .

348 ● Indian Health Care
IHS Allocations by Area and Budget Category, with Service Population and Util ization Data, Fiscal Year 1976
Service D i r e c t I n d i r e c t P r e v . H l t h / Outpat ientArea Populat ion Pt . Care Pt . Care Amb. Care Other TOTAL FY 76 D ischarges V is i t s. . . . . . . . . . . . . . . . . .-..-. . . . . . . --- . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ------- ------ ------ . . . . . . . . . . . . . . . . . . . . . . . . .
Aberdeen 56,385 S9,528,500 $6,224,800 S12,845,000 $1,305,100 $29,903,400 12,850 346,223Alaska 58,454 20,843,200 6,385,000 19,865,750 2,116,800 49,210,750 9 , 5 6 6 268,409Albuquerque 4 1 , 8 8 6 5 , 2 4 8 , 7 0 0 4 , 5 2 7 , 0 0 0 7,967,800 2,198,200 19,941,700 3 , 2 3 5 185,698Bemidji 34,115 1,427,600 2,903,000 4,481,400 0 8 , 8 1 2 , 0 0 0 1,650 68,369B i l l i n g s 32,496 3,178,300 6,713,000 8,646,600 1,148,200 19,686,100 3,111 221,618Headquarters East o 10,962,600 1,500,500 1,774,200 3,998,000 18,235,300 -- . .
Nashvi l le (USET) 12,672 1,804,500 1,672,000 3,410,100 0 6 , 8 8 6 , 6 0 0 1,928 74,568Navajo 121,078 17,707,200 6,545,000 18,656,600 804,900 43,713,700 19,242 627,669Oklahoma 142,290 8,757,000 4,436,000 14,480,800 1,450,900 29,124,700 9 , 9 7 0 406,678Phoenix 63,695 11,175,100 6,479,700 15,975,000 1,546,000 35,175,800 13,602 368,676Port land 3 6 , 5 8 6 630,000 6,886,000 8,090,150 619,900 16,226,050 -- 135,695Tucson 13,639 3,108,200 638,000 4,463,600 0 8 , 2 0 9 , 8 0 0 1,042 47,943Regions 0 25,600 0 0 0 25,600 -- . .
Total FY 1976: 611,296 $ 9 4 , 3 9 6 , 5 0 0 $ 5 4 , 9 1 0 , 0 0 0 $ 1 2 0 , 6 5 7 , 0 0 0 $ 1 5 , 1 8 8 , 0 0 0 $285,151,500 7 6 , 1 9 6 2 , 7 5 1 , 5 4 6
IHS Allocations by Area and Budget Category, wi th Serv ice Populat ion and Ut i l i zat ion Data, F i scal Year 1975
ServiceArea Populat ion----- . . . . . . ------ ---- . . . . . . . . . .
Aberdeen 52,814Alaska 57,198Albuquerque 40,426Bemidji 3 2 , 4 5 7B i l l i n g s 31,734Headquarters East oNashvi l le (USET) 12,314Navajo 116,161Oklahoma 135,168Phoenix 61,296Port land 3 4 , 9 0 8Tucson 12,992Regions o
D i r e c tPt . Care
. . . . . . . . . . . . . -.
$11,705,20023,257,000
5,974,8001,523,7004 , 4 1 9 , 7 0 09 , 6 0 8 , 8 0 02,056,800
17,879,90010,438,60015,026,900
501,1003,245,800
40,300
I n d i r e c tPt . Care
. . . . . . . . . . . .
$5,269,0005,518,0003,755,0002,529,0005,542,000
415,0001,414,0005,095,0004,173,0005,558,0006,065,000
580,0000
F ie ld Heal th. . . . . . . . . . . . . . . .
$7,856,70010,429,400
5,608,4002,480,3005,905,9001,470,6001,742,400
10,564,6008,918,0008,080,4005,499,6002,972,700
0
Other. . . . . . . . . . . . .
$1,224,9002,005,6002,039,800
1,087,8003,617,300
0765,700
1,411,3001,454,700
569,20000
TOTAL FY 75. . . . . . . . . . . .
$26,055,80041,210,00017,378,0006 , 5 3 3 , 0 0 0
16,955,40015,111,700
5,213,20034,305,20024,940,90030,120,00012,634,9006 , 7 9 8 , 5 0 0
40,300
Outpat ientD i s c h a r g e s V i s i t s
. . . . . . . . . . . . . . . . . . . --
12,900 310,7009,705 264,4023 , 4 6 9 162,2971,530 56,6563 , 0 2 8 202,806
. .
1,864 70,81218,083 513,5999 , 8 4 8 364,933
13,216 340,407127,195
924 23,944. . . .
Total FY 1975: 587,468 $105,678,6OO $45,913,000 $71,529,000 $ 1 4 , 1 7 6 , 3 0 0 $ 2 3 7 , 2 9 6 , 9 0 0 7 4 , 5 6 7 2 , 4 3 7 , 7 5 1
IHS Allocations by Area and Budget Category, with Service Population and Util ization Data, Fiscal Year 1974
ServiceArea Populat ion. . . . . . . . . . . . . . . . . . . . . . . . ------
Aberdeen 50,595Alaska 55,700Albuquerque 38,960Bemidji 27,165B i l l i n g s 30,951Headquarters East oNashvi l le (USET) 11,947Navajo 111,237Oklahoma 128,000Phoenix 58,875Port land 31,974Tucson 12,343Regions o
D i r e c tPt . Care
. . . . . . . . . . . . . .
$9,967,99120,974,900
4,183,8001,184,8003 , 5 1 9 , 2 0 05,286,0001,569,000
16,530,7009 , 2 0 4 , 6 0 0
13,315,500306,000
2,902,30054,200
I n d i r e c tPt . Care
. . . . . . . . . . . --
$4,748,0005,052,0003,074,0002,168,0004,976,500
437,0001,085,0004,505,0003,863,9005,143,0005,107,600
493,0000
F ie ld Heal th. . . . . . . . . . . . .
$6,797,8508,106,6004,700,1001,952,1004,975,0001,287,0001,329,9009,200,5506,560,8007,111,6004,674,3002,032,100
18,300
Other. . . . . . . . . . . . . . . .
$1,180,9001,950,0001,975,600
01,045,4003,503,000
0719,700
1,331,4001,382,000
562,00000
TOTAL FY 7 4... . . . . . .
$22,694,74136,083,50013,933,500
5,304,90014,516,10010,513,0003 , 9 8 3 , 9 0 0
30,955,95020,960,70026,952,10010,649,9005,427,400
72,500
Outpat ientD i s c h a r g e s V i s i t s
----- ------ . . . . . . . . . .
11,933 302,44210,486 246,8963 , 5 8 0 151,3311,537 54,8392,871 198,150
. . . .1,620 67,259
18,124 513,5999 , 3 5 9 328,196
12,805 341,377. . 117,603
1,098 39,962. . . .
Total FY 1974: 5 5 7 , 7 4 7 $ 8 8 , 9 9 8 , 9 9 1 $ 4 0 , 6 5 3 , 0 0 0 $58,746,200 $13,650,000 $202,048,191 7 3 , 4 1 3 2 , 3 6 1 , 6 5 4

App. C—IHS Allocations by Area and Budget Category, With Service Population and Utilization Data, FY 1972-85 Ž 349
IHS Allocations by Area and Budget Category, with Service Population and Utilization Data, F i seal Year 1973
S e r v i c eArea P o p u l a t i o n. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aberdeen 49,020Alaska 54,440Albuquerque 37,496Bemidj i 25,799B i l l i n g s 29,274Headquar ters East oNashvi l le (USET) 9 , 8 6 6Navajo 106,317Oklahoma 120,691Phoenix 56,467P o r t l a n d 30,248Tucson 11,696Regions o
D i r e c t IndirectPt. Care Pt. Care
. . . . . . . . . . . . . . . . . . . . . . . . . .
$8,661,700 $3,932,90019,757,700 3,796,9003,893,700 2,337,4001,061,973 1,677,7002,939,000 4,333,8005,390,700 413,0001,355,600 896,000
13,929,200 3,638,1007,970,200 3,058,300
11,771,400 4,461,700233,200 4,028,800
2,595,300 426,00025,500 0
O u t p a t i e n tF i e l d H e a l t h Other TOTAL FY 73 Discharges V is i ts
... . . . . . . . . . . . . . . . . . . ------ ------ ------ ------ . . . . . . . . . . . . . . .
$5,722,400 $1,100,800 $19,417,800 13,844 315,5337,838,500 1,818,900 33,212,000 10,733 223,9543,852,400 1,842,600 11,926,100 3,435 149,0591,488,900 0 4,228,573 1,690 56,7224,384,100 974,200 12,631,100 3,.247 210,7811,577,700 3,251,000 10,632,400 . . .
1,200,900 0 3,452,500 1,572 60,7108,313,300 647,300 26,527,900 18,407 500,7705,268,100 1,236,800 17,533,400 9 , 4 0 2 318,6146,081,100 1,293,000 23,607,200 11,855 325,3053,823,100 514,600 8,599,700 131,1141,979,600 0 5,000,900 1,321 36,598
9,000 0 34,500 . . .
Total FY 1973: 5 3 1 , 3 1 4 $ 7 9 , 5 8 5 , 1 7 3 $33,000,600 $ 5 1 , 5 3 9 , 1 0 0 $ 1 2 , 6 7 9 , 2 0 0 $176,804,073 7 5 , 5 0 6 2 , 3 2 9 , 1 6 0
IHS Al locat ions by Area and Budget Category , w i th Serv ice Popula t ion and Ut i l i za t ion Data , F isca l Year 1972
S e r v i c e D i r e c tArea P o p u l a t i o n Pt. Care. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aberdeen 47,443 $7,783,100Alaska 53,179 18,485,600Albuquerque 36,035 3,652,400Bemidj i 24,423 982,700B i l l i n g s 28,589 2,901,000Headquar ters East o 3,237,200Nashv i l le ( U S E T ) 9 , 5 5 9 1,239,600Navajo 101,396 13,103,992Oklahoma 113,548 7,468,400Phoenix 54,057 11,067,100Port land 28,528 263,800Tucson 11,047 2,352,000
I n d i r e c tPt . Care
. . . . . . . . . . . . .
$3,452,7003,269,1002,251,4001,402,1003,719,300
387,000822,000
3,122,1002,858,4004,149,1003,728,800
384,000
F i e l dHealth
. . . . . . . . . . . . . .
$4,795,1976,242,7003,166,6001,215,0003,811,0001,362,303
723,6007,467,2004,317,3005,059,8003,283,7001,438,600
Other TOTAL FY 72. . . . . . . . . . . . . . . . . . . . . . . . . .
$1,052,900 $17,083,8971,722,000 29,719,4001,724,800 10,795,200
0 3,599,800911,300 11,342,600
2,843,600 7,830,1030 2,785,200
586,800 24,280,0921,156,600 15,800,7001,228,200 21,504,200
481,400 7,757,7000 4,174,600
O u t p a t i e n tD i s c h a r g e s V i s i t s----- . . . . . . . . . . . . . . .
12,786 306,41211,410 202,8493 , 7 0 0 140,8531,980 53,9863 , 3 1 0 194,278
. . . .
1,663 56,51118,160 508,0899 , 4 9 6 311,115
12,144 323,935104,117
1,525 33,736
Tota l FY 1972: 507,804 $72,536,892 $ 2 9 , 5 4 6 , 0 0 0 $ 4 2 , 8 8 3 , 0 0 0 $ 1 1 , 7 0 7 , 6 0 0 $156,673,492 7 6 , 1 7 4 2 , 2 3 5 , 8 8 1
SOURCE: U.S. Congress, Off ice of Technology Assessment ; based on docunents from U.S. Department of Healthand Human Services, Public Health Service, Health Resources and Services Administration, IndianHealth Service, Program Statistics Branch (population and util ization data) and Resources ManagementBranch (budget allocations), Rockville, MO, 1985.

Appendix D
Acknowledgments andHealth Program Advisory Committee
ACKNOWLEDGMENTSThis report depended heavily on the participation and experience of many people throughout the United
States. The staff would like to especially acknowledge the following people for their valuable assistance.Individuals who provided information from Indian Health Service sources included Thomas Berry, Anthony
D’Angelo, Mary Elrod, Michael Gomez, Aaron Handler, Stephen Kaufman, Russell Mason, Richard McCloskey,Thomas Seidl, Craig Vanderwagen, and Cliff Wiggins. Other individuals who provided information and assis-tance included Jake Whitecrow, John O’Connor, and Scott Cull of the National Indian Health Board; SheilaWeinmann of the N.W. Portland Area Indian Health Board; Edna Paisano of the U.S. Bureau of the Census;and Linda Mellgren and Laurie Young of the U.S. Department of Health and Human Services, The staff wouldalso like to acknowledge the contribution of the participants in the four regional meetings held in Portland, Oregon;Phoenix, Arizona; Rapid City, South Dakota; and Tulsa, Oklahoma.
HEALTH PROGRAM ADVISORY COMMITTEE
Sidney S. Lee, ChairPresident, Milbank Memorial Fund
H. David BantaProject DirectorSTG Project on Future Health TechnologyThe Netherlands
Rashi FeinProfessorDepartment of Social Medicine and Health PolicyHarvard Medical School
Harvey FinebergDeanSchool of Public HealthHarvard University
Patricia KingProfessorGeorgetown Law Center
Joyce C. LashofDeanSchool of Public HealthUniversity of California, Berkeley
Alexander LeafProfessor of MedicineHarvard Medical SchoolMassachusetts General Hospital
Frederick MostellerProfessor and ChairDepartment of Health Policy and ManagementSchool of Public HealthHarvard University
Norton NelsonProfessorDepartment of Environmental MedicineNew York University Medical School
Robert OseasohnAssociate DeanSchool of Public HealthUniversity of Texas
Nora PioreSenior Fellow and Advisor to the PresidentUnited Hospital Fund of New York
Dorothy RiceRegents LecturerDepartment of Social and Behavioral SciencesSchool of NursingUniversity of California, San Francisco
Richard RiegelmanAssociate ProfessorGeorge Washington University
School of Medicine
350

Walter RobbVice President
App. D—Acknowledgments and Health Program Advisory Committee Ž 351—
Frank E. Samuel, Jr.& General Manager President
Medical Systems Operations Health Industry Manufacturers’ AssociationGeneral ElectricMilwaukee, WI
Rosemary StevensProfessor
Frederick C. Robbins Department of History and Sociology of ScienceUniversity Professor University of PennsylvaniaDepartment of Epidemiology and BiostatisticsSchool of MedicineCase Western Reserve UniversityCleveland, OH

Appendix E
Method of the Study
The purpose of this assessment of Indian health carewas to evaluate: 1) the health status of American In-dians and Alaska Natives who are provided health carethrough the Federal Indian Health Service (IHS), 2) thehealth services provided to them in view of their healthneeds, and 3) the health delivery systems in whichthese services are provided. Also identified as a morespecific issue to be evaluated was the growing prob-lem of paying for high-cost care that cannot be pro-vided in IHS facilities and that must be purchased fromnon-IHS providers. (Letters from Congress requestingand supporting the assessment follow this narrative. )
The assessment began on October 1984. Projectactivities included: selection of an advisory panel; twoadvisory panel meetings and other extensive reviews;four regional meetings with tribal representatives; sitevisits to Indian reservations and IHS service units;meetings and consultations with IHS personnel; anal-ysis of Indian social and economic characteristics,health services, and health status; and responding toa special request in addition to the overall assessment.
The advisory panel for this assessment of Indianhealth care consisted of 19 members from Indian tribalgovernments and private and tribal health programsfor Indians, policy analysts of Indian issues, and rep-resentatives of State governments, public health, med-ical economics, pubIic policy/health care administra-tion, sociology, and law. Rashi Fein, professor of theeconomics of medicine at Harvard Medical School,chaired the panel.
The first panel meeting was held on January 29-30,1985. OTA project staff identified the sources of avail-able information and presented a preliminary analy-sis of these sources to the panel. The panel discussedthe overall, study plan and provided advice on the fo-cus of the study, Information for this assessment wasobtained primarily from unpublished documents (moreso than for usual OTA assessments), interviews, re-gional meetings, and site visits.
OTA project staff was also assisted by several con-tractors in preparing this assessment. In May-July1985, four regional meetings were held by OTA inconjunction with the National Indian Health Board(NIHB), an organization that represents the tribes onhealth issues. The meetings were publicized in NIHB’snewsletter, and a common agenda was used at the fourmeetings, which were held in Portland, Oregon; Phoe-nix, Arizona; Rapid City, South Dakota; and Tulsa,
Oklahoma (the meeting agenda is described below).Several advisory panel members participated in meet-ings in their localities. The objectives of these meet-ings were to provide tribes and OTA staff with the op-portunity to communicate directly with each other,and to confirm or correct the area-specific health sta-tus, socioeconomic, and health services informationOTA had sent in advance of these meetings. In con-junction with the regional meetings, OTA project staffvisited many reservations to gain a sense of the diver-sity and special concerns of the tribes.
Projections of the future Indian population were de-veloped under OTA guidance by Henry Cole and S.Ken Yamashita of the Futures Group; computer anal-ysis of data sources on Indian health status was pro-vided by Steven Bjorge of Washington, D. C,; and PaulAlexander of the law firm of Alexander & Karshmerprovided a legal analysis of the Federal-Indian rela-tionship, (The method used in the Indian health sta-tus data analysis is described below. )
The advisory panel met again on October 28-29,1985, to review a draft of the final report, Based onthat meeting, the summary chapter was rewritten andagain submitted to the panel for their review. The draftfinal report was sent for review to nearly 200 organi-zations and individuals. The OTA project director alsoattended the annual meeting of the National IndianHealth Board in Albuquerque, New Mexico, in No-vember 11-14, 1985, at which time the draft report wasdiscussed in an open forum, with several advisorypanel members participating in the discussion. The fi-nal report was submitted to OTA’s Technology Assess-ment Board on January 17, 1986.
During the course of this assessment, the House andSenate Appropriations Subcommittees for the Depart-ment of the Interior and related agencies requested thatOTA conduct an analysis of the number of beds andwhether a surgical suite should be included in thereplacement hospital planned for the Rosebud Siouxin South Dakota. The request was made in June 1985because of a dispute between the Rosebud tribe andthe Public Health Service on the size and services ofthe replacement hospital. The analysis was completedand delivered on August 1, 1985, in the form of anOTA staff memorandum. OTA’s conclusions werethat, using PHS’s own criteria, a 30- to 35-bed insteadof a 25-bed hospital was warranted, but that a surgi-cal suite was not.
352

App. E—Method of the Study ● 353
Purpose of the Regional Meetings
The regional meetings and site visits were held: B.1) to give IHS’s client population the opportu- C.nity to comment on the information OTA was D.gathering at the national level and on whetherthis information reflected the local situation; and E.2) to provide OTA with information and opin-ions on local health issues, problems, and pri- F.orities. The meetings covered the followingareas:I. Characteristics of Indian peoples
A. Tribal membership: eligibility, trends, G.general demographics
B. Health status and special health problems11. Delivery of health care
A. Direct IHS services
self-determination (638) fundsContract careOther sources of funding (Medicare, Med-icaid, private, etc.)Equity funding-criteria, application, imp-a c tHigh-cost (“catastrophic”) contract care—impact on contract care funds, types ofcases, trends, relationship to presence orabsence of relevant IHS direct care servicesHealth-related services: community healthrepresentatives, sanitation, housing, nu-trition, other environmental services.
Health Statistics Information
IHS provided OTA with three data files on mag-netic tape of the records of all American Indian andAlaska Native deaths during the years 1980,19$1,and 1982, as compiled by the National Center forHealth Statistics (NCHS). In all cases, death ratescomputed by OTA represent the centered-averageof the 1980-82 period.
There was a slight discrepancy between the num-ber of records on the tape and the number of deathsas described in IHS publications. There were 20,200death records on the tape supplied by IHS, whileIHS publications list 20,210 deaths for this 3-yearperiod. This was assumed to be a minor discrepancyand was not pursued further. IHS uses a matchingprogram based on State, county, and communityof residence to assign death records to an IHS serv-ice area. OTA excluded death records without anassigned IHS area. The number of death records as-signed to all IHS areas during the 3-year period was15,792.
These deaths were stratified into age-specific, sex-specific, and IHS-area-specific totals. Rates werecalculated for each of the 72 selected causes of deaththat are used by NCHS in monitoring the health ofthe U.S. population. Age-specific, age-adjusted andcause-specific Indian death rates were computed: 1)for each of the 12 IHS service areas, and 2) for allareas, excluding California.
In California, especially in urban areas wheremost Indians in California live, health officials re-ported that Indian death statistics are not reliable
and are probably too low because of reporting defi-ciencies. Examination of the calculated death ratesshowed that rates in California were indeed improb-ably low, casting doubt on the reliability of thereporting system on Indians in California. (For ex-ample, calculations of California Indian death ratesresult in rates less than half the U.S. all races rate,as well as being far below death rates for peopleresiding in some of the wealthiest counties in theUnited States.)
OTA also made preliminary computations ofdeaths by reservation States, by service units, andby Standard Metropolitan Statistical Areas (SMSA)as a surrogate for urban areas. Analyses by reser-vation State were not pursued because of Congress’request that OTA concentrate on health status inIHS service areas. Analyses by service unit andSMSA were not pursued because in most cases thepopulations and numbers of death were too smallfor meaningful analysis.
IHS service area populations that were used asthe denominators for calculating death rates werecomputed in the following way. IHS used the 1980census to determine population totals in IHS serv-ice areas. For succeeding years, IHS projects Indianpopulation growth using actual birth and death datasupplied by NCHS. OTA used these population es-timates for each of the IHS areas, totaled for the3-year period, 1980-$2.
In order to arrive at age- and sex-stratified pop-ulation totals for each of the IHS areas, tables sup-

354 ● Indian Health Care
plied by IHS were also used. These tables were de-rived from the 1980 census and list the percent ofpopulation in each we and sex bracket for each ofthe 32 reservation States. These tables were usedas a “best estimate” of the actual age and sex distri-bution in the various IHS areas because the majorityof the Indian population in most reservation Statesactually live in or near IHS service areas, but theiruse may introduce some error.
Using these sex-stratified and age-specific deathrates, age-adjusted death rates were computed,using the 1940 Standard Million Population andstandard methodology. Each death rate was muli-plied by its appropriate percentage of the standardmillion (based on sex and age), then these rates weresummed to obtain the weighted averages that rep-resent age-adjusted death rates for each of theselected causes in each of the IHS service areas. Age-adjusted death rates for the U.S. all races popula-tion were obtained from NCHS mortality reportsand used to compute the ratio of Indian to U.S. allraces death rates.
OTA also obtained published and unpublisheddata on the use of IHS health care services from IHS
and used this information to analyze morbidity (ill-ness and injury), needs for health care services, andaccess relative to that of the general population. In-formation concerning morbidity (illness) was de-rived from two IHS data sources: 1) the InpatientCare System (IPC), which contains IHS direct careand contract care general hospital discharge data;and 2) the Ambulatory Patient Care System (APC),which contains information on the number of out-patient visits at IHS facilities by various patientcharacteristics (age, sex, diagnosis, community ofresidence, etc.). IHS provided OTA with computertapes pertaining to its IPC and APC systems, itspublications on hospital utilization by area (IHS,1978, 1979, 1985), and printouts of the 15 leadingdiagnoses for outpatient visits by reservation State,county, IHS area, and IHS service unit. NCHS pub-lications and unpublished data were the primarysources of information on U.S. ail races health careutilization.
The limitations of ail data sources on health sta-tus are discussed in chapter 4.

App. E–Method of the Study ● 3 5 5
Dear Dr. Gibbons:
The Committee on Energy and Commerce has oversight andl eg i s l a t i ve j u r i sd i c t i on ove r a l l Fede ra l hea l th p r o g r a m s f u n d e dthrough general revenues, including those relat ing to the d i s c h a r g e o fthe Federal trust responsibility to the Native American population.In cons ider ing the rev i s ion and ex tens ion o f the Indian Hea l th CareImprovement Act, P.L. 9 4 - 4 3 7 , i t h a s b e c o m e a p p a r e n t to us t h a t a ni n - d e p t h s tudy o f some o f the i s sues ra i sed by current Federa l Indianh e a l t h e f fo r t s i s n e c e s s a r y if t h e C o n g r e s s i s t o f a s h i o n e f f e c t i v el e g i s l a t i v e s o l u t i o n s .
We w o u l d therefore request t h a t t h e O f f i c e o f T e c h n o l o g yA s s e s s m e n t c o n d u c t a s t u d y of h e a l t h t e c h n o l o g y a n d s e r v i c e s i n t h ec o n t e x t o f F e d e r a l I n d i a n h e a l t h p r o g r a m s a d m i n i s t e r e d b y t h e I n d i a nH e a l t h S e r v i c e ( I H S ) . To be m o s t helpful to t h e C o m m i t t e e , t h e s t u d yshould address: (1) the heal th s ta tus of American Indian and NativeAlaska people who are eligible for care through the IHS (whetherdirectly or by contract); (2) the most appropriate mix of medical andhealth services and technologies in light of the health needs of theeligible population; (3) the organization of health delivery systems,with emphasis on adequate and equitable access to services andtechnologies, health outcomes, and cost effectiveness: and (4)catastrophic health care needs, and current and alternative financingarrangements for those needs.
In conduct ing th is s tudy , we would urge you to assemble andconsu l t w i th an adv i so ry pane l of k n o w l e d g e a b l e i n d i v i d u a l s w h o a r er e p r e s e n t a t i v e o f t h e t r i b e s , t r i b a l h e a l t h o r g a n i z a t i o n s , a n d u r b a nI n d i a n p r o j e c t s t h r o u g h o u t t h e c o u n t r y t h a t r e c e i v e o r d e l i v e r c a r e

356 ● Indian Health Care
under current a r r a n g e m e n t s . The expert ise tha t such indiv iduals canbring to bear would, in our view be of invaluable assistance t o OTAi n a n a l y z i n g t h e i s s u e s t o b e c o n s i d e r e d b y t h e s t u d y .
w e u n d e r s t a n d that del ivery of the pr inted report may not bep o s s i b l e u n t i l the fal l of 1 9 8 5 . H o w e v e r , w e w o u l d r e q u e s t t h a t w er e c e i v e a n i n t e r i m . p r o g r e s s r e p o r t o n t h e s t u d y , i n t e r i m b r i e f i n g s o ns p e c i f i c i s s u e s a s t h e n e e d a r i s e s , a n d a f o r m a l b r i e f i n g i n J u l y o f1985.
W e look f o r w a r d t o y o u r r e s p o n s e . If you or members of the OTAs t a f f h a v e q u e s t i o n s c o n c e r n i n g t h i s r e q u e s t , p l e a s e c o n t a c t A n d yS c h n e i d e r o f t h e s t a f f o f t h e S u b c o m m i t t e e o n H e a l t h a n d t h eE n v i r o n m e n t a t 2 2 5 - 4 9 5 2 .
S i n c e r e l y y o u r s ,
& (u~~-7- --- ----- --------- -----
HENRY A. WAXMAN, ChairmanCommittee on Energy and Subcommi t t ee on Hea l thCommerce a n d t h e E n v i r o n m e n t
HAW:asl

App. E—Method of the Study . 357
SELECT COMMITTEE ON INDIAN AFFAIRS
WASHINGTON, D.C. 20610
June 19, 1984
Congressman Morris K. Udall ChairmanOffice of Technology AssessmentUnited States Congress600 Pennsylvania Avenue S. E.Washington, D.C. 20003
Dear Mo:
AS you know, the Senate Se lec t Commit tee on I n d i a n A f f a i r s h a sr e c e n t l y r e p o r t e d t o t h e S e n a t e f l o o r , a b i l l t o r e a u t h o r i z e t h eIndian Health Care Improvement Act of 1976 through f iscal year 1988.In cons ider ing the need for tha t l eg i s la t ion , a number o f i s suessurrounding the provis ion o f contrac t hea l th care were ra i sed , and i tis our unders tanding tha t a reques t for a s tudy o f those i s sues hasnow been formally submitted to you.
We are writing to join Congressman John Dingell , Chairman of theHouse Committee on Energy and Commerce, and Congressman Henry Waxman,Chairman of the House S u b c o m m i t t e e on Health and the Environment, inrequesting that the Office of Technology Assessment conduct a s tudy ofhea l th technology and serv ices in the contex t o f the Federa l Indianhealth care programs administered by the Indian Health Service, abureau of the Public Health Service within the Department of Healthand Human Services. We also wish to endorse the modifications to theproposed study that you have recommended on behalf of the HouseInterior and Insular Affairs Committee.
As Chairman and Ranking Minority member of the Senate SelectCommittee on Indian Affairs, we look forward to the opportunity tomake recommendations to the Office of Technology Assessment for theselection of the proposed advisory panel , and to make available to t h eof f i ce o f Technology Assessment , any mater ia l s or in format ion ,including Committee hearing records, that may be needed for the study.We have designated Indian Affairs Committee staff attorney, PatriciaZ e n , to provide any ass i s t ance t h a t t h e O f f i c e o f T e c h n o l o g yAssessment may require.
Warm regards,
Mark Andrewsv
John MelcherChairman Ranking Minority Member

358 ● Indian Health Care
Congress of the United StatesHouse of Representatives
Washington, D.C. 20515
Dr. John H. GibbonsD i r e c t o rOffice of Technology AssessmentU.S. CongressWashington , D .C . 20510
Dear Dr. Gibbons:
As Chairman and Vice Chairman of the Office of Technologyand Assessment Board , respec t ive ly , we take th i s oppor tuni ty t .comment on the request of the Committee on Energy and Commercefor a study by OTA in the f ield of Indian Health. Addi t iona l ly ,Mr. Udall , as Chairman of the Committee on Interior and InsularA f f a i r s , whose Committee has primary jurisdiction over Indian.Af fa i r s mat ters in the House o f Representa t ives , br ings to th i sissue a perspective and expertise which we feel OTA will be ableto a p p r e c i a t e a n d u t i l i z e t o t h e b e n e f i t o f s u c h a s t u d y as hasbeen requested by the Committee on Energy and Commerce.
We feel that we can support the request of the EnergyCommittee for such a study and that this study can be helpful tothe Congress and the Administration in meeting ourr e s p o n s i b i l i t y t o t h e I n d i a n t r i b e s f o r h e a l t h s e r v i c e s .However, in developing your schedule and plan for the OTAassessment , we ask tha t you take in to cons idera t ion thefollowing comments:
1. We are concerned about the implication in theEnergy letter that the study ‘be focused on therespons ib i l i ty o f the Uni ted S ta tes to provide hea l th caret o i n d i v i d u a l s o n t h e b a s i s o f t h e r a c i a l i d e n t i t y . TheI n d i a n h e a l t h c a r e r e s p o n s i b i l i t y o f t h e U n i t e d S t a t e s i sfounded upon the legal , m o r a l a n d h i s t o r i c a l r e l a t i o n s h i pbetween the Uni ted S ta tes and Indian t r ibes as po l i t i ca le n t i t i e s . I n t h i s r e g a r d , we re fer you to the dec i s ion o fthe Supreme Court in the case of Morton v. Mancari , 417Us. 535 (1974). We suggest that your study be guided bythe po l i t i ca l re la t ionsh ip o f the Federa l government andIndian t r ibes ra ther than by the rac ia l background o fi n d i v i d u a l r e c i p i e n t s o f h e a l t h s e r v i c e s .

—
App. E—Method of the Study Ž 359
Page 2 - John H. Gibbons
2 . This Federa l - t r iba l re la t ionsh ip must encompass anyreview of unmet health needs and resource al location andmust be ident i f i ed as the bas i s for a comprehens ive hea l thcare sys tem to meet tha t spec ia l respons ib i l i ty . Therev iew must a l so incorporate o ther fac tors bes idespopulation data, e . g . , g e o g r a p h i c l o c a t i o n , a c c e s s i b i l i t yto IHS and o ther hea l th serv ices , and lack o f loca li n f r a s t r u c t u r e ( r o a d s , water and sewer sys tems , e t c . ) .
3. We are supportive of Energy’s request for an OTAa s s e s s m e n t in the area o f t rea tment o f ca tas t rophici l l n e s s e s , but wi th two reservat ions . F i r s t , M r . U d a l ldoes not suppor t tha t por t ion o f the s tudy as a subs t i tu tef o r t h e c a t a s t r o p h i c i l l n e s s p r o v i s i o n i n t h e I n t e r i o rversion of H.R. 4 5 6 7 . It remains Mr . U d a l l ’ s i n t e n t t osecure enac tment o f tha t provis ion in to law. second, wehope tha t th i s por t ion o f the s tudy not be shaped so le ly bythe e lements o f the debate on tha t i s sue as a na t iona lh e a l t h c a r e i s s u e . T h e r e a r e s i g n i f i c a n t d i f f e r e n c e sbetween that issue as a national issue and as an issue andproblem for the Indian Hea l th Serv ice in prov id ing hea l thcare to Indians . I n t h i s r e g a r d , we refer you to thediscuss ion o f the H.R . 4567 provis ion in the d issent ingviews of Mr. Richardson, et al . in the Energy Committeer e p o r t o n t h e b i l l ( H . R e p t . 9 8 - 7 6 3 , P a r t 2 ) .
4. Finally, we would like to recommend for OTA on theselection of members of any Advisory Board for this study.
Again, we thank you for keeping us and our Committee staffsadvised on th i s mat ter . We would apprec ia te i t i f your o f f i cewould continue to stay in touch as the development of the studyprogresses.
with warm regards,
S i n c e r e l y ,
Vice ChairmanOffice of Technology Assessment

Appendix F
List of Acronyms and Glossary of Terms
Glossary of Acronyms
ADPL —average daily patient loadAFDC —Aid to Families with Dependent ChildrenAHCCCS—Arizona Health Care Cost Containment
AIPRC
ANCSAAPABEMAR
BIA
CHRCHSCHSDACRIHBDHEW
DHHS
DRGESRDGAOHMOHRSA
HUD
ICD-9
ICUIHCIAIHSISDMJCAH
JTPAMOAS
M&RNCI
NHSC
Ob-GynOFE
OMB
System—American Indian Policy Review Com-
mission—Alaska Native Claims Settlement Act—Administrative Procedures Act—backlog of essential maintenance and
repair—Bureau of’ Indian Affairs (U.S. Depart-
ment of the Interior)—community health representative—contract health services—contract health service delivery area–California Rural Indian Health Board—U.S. Department of Health, Education,
and Welfare—U.S. Department of Health and Human
Services—diagnosis-related group—end-stage renal disease—General Accounting Office (U.S. Congress)—health maintenance organization—Health Resources and Services Adminis-
tration (PHS, DHHS)—U.S. Department of Housing and Urban
Development—International Classification of Disease, 9th
Revision—intensive care unit—Indian Health Care Improvement Act–Indian Health Service (HRSA, PHS, DHHS)—Indian self-determination memos–Joint Commission on Accreditation of
Hospitals–Job Training Partnership Act—Memoranda of Agreement—maintenance and repair—National Cancer Institute (National Insti-
tute of Health, PHS)—National Health Service Corps (Bureau of
Health Care Delivery and Assistance,HRSA, PHS, DHHS)
—obstetrics-gynecology–Office of Facilities’ Engineering (HRSA,
PHS, DHHS)-–U.S. Office of Management and Budget
OTA
PCISPHSPIDRACRAMRPMSRRMSIDSSMSASS1TRAIS
VAWIC
–Office of Technology Assessment (U.S.Congress)
—Patient Care Information System–Public Health Service (DHHS)—program information document—resource allocation criteria—resource allocation methodology—Resource and Patient Management System—resource requirement methodology—sudden infant death syndrome—standard metropolitan statistical area—Supplemental Security Income—Tribal Resource and Assistance Informa-
tion System—U.S. Veterans Administration—Women, Infants, and Children [Program]
Glossary of Terms
Age-adjusted mortality rate: The death or mortalityrate adjusted for the age distribution of the popu-lation under study. Age adjustment allows a directcomparison of the overall mortality experience oftwo or more populations, or to examine mortalityover time in a single population, by using a singlestatistic. Age adjustment is necessary because pop-ulations differ in their proportions of people indifferent age categories, and different age groupshave different mortality rates; for example, deathrates for 25 to 34 year olds are much lower thanfor 55 to 64 year olds. Comparing populations with-out adjusting for the different age distributions ofpersons within each population (for example, a pop-ulation with a high proportion of persons over 55years of age versus a population with a high propor-tion of persons under 55 years of age) could leadto erroneous conclusions about the relative healthof the populations being compared (see also “crudemortality rate” and “mortality rate”),
Allotment: A Federal policy pursued in the late 19thand early 20th centuries to “civilize” Indians by: 1)assigning each adult Indian a specific amount ofland (usually 160 acres); 2) setting aside a smallamount of land for tribal purposes; 3) opening theresulting “excess” land to non-Indian settlement;and 4) holding the Indian land and proceeds fromsales of the “excess lands” in trust for Indians untilthey became assimilated (see also “assimilation”).
360

App. F—List of Acronyms and Glossary of Terms ● 361
Alternate resources: Sources of health care other thanthose of IHS’s contract care program that are avail-able and accessible to the individual requesting theservices or would be available and accessible uponapplication of the individual to the alternate re-sources, such as health care providers and institu-tions (including facilities operated by the IndianHealth Service), health insurance, or other healthcare programs that pay for health services (e. g.,Medicare or Medicaid) for which the individualmay be eligible.
Area: The designated organizational unit and its cor-responding geographical area through which IHSprograms are administered. There are 12 IHS areascovering the 32 Reservation States.
Assimilation: A Federal policy pursued in the late 19thand early 20th centuries, in which tribally held com-munal lands were broken up and individual Indianswere given allotments of land in order to inducethem to leave their traditional ways of life and tobecome “civilized” (see also “allotment”).
Blood quantum: The degree of Indian blood of an in-dividual. Most tribes require a minimum degree oftribal-specific Indian blood for membership,
Buy Indian contracts: Contracts under the Buy IndianAct of 1910 between the Federal Government (espe-cially BIA and IHS) and Indian businesses and orga-nizations for the purchase of goods and services,
Catastrophic health care fund: A revolving fund pro-posed in 1984 and 1985 congressional legislation toassist in paying for high-cost cases in the IHS con-tract care program. The fund would have contained$12 million, to be used to pay for contract care casesthat exceeded a threshold cost between $10,000 and$20,000 (see also “high-cost case”).
Commissioned Corps: Members of the Public HealthService Commissioned Corps, including physicians,dentists, nurses, administrators, and other health-related personnel.
Community health representative (CHR): Indian healthparaprofessionals who assist in providing healthcare, health promotion, and disease preventionservices to Indians.
Contract services: Health care purchased by the IHScontract care program for eligible Indians from non-IHS providers and facilities when direct services ofthe appropriate types are not available or accessi-ble (see also “direct services”).
Cooperative agreement: An instrument similar to agrant for the transfer of Federal funds and programoperation responsibilities to organizations such asIndian tribal governments. Cooperative agreementswere introduced by the Federal Grants and Coop-erative Agreement Act of 1977 (Public Law 95-224)and authorized for use in IHS and BIA self-deter-
mination (638) programs in 1984. The instrumentshad not been used by IHS as of the end of 1985.
Crude mortality rate: The death, or mortality rate,tabulated without being broken down into classes.The number of deaths in a population divided bythe total population, over a defined period of time(see also “mortality rate” and “age-adjusted mor-tality rate”).
Diagnosis-related groupings (DRGs): Groupings ofdiagnostic categories drawn from the InternationalClassification of Diseases and modified by the pres-ence or absence of a surgical procedure, patient age,presence or absence of significant comorbidities orcomplications, and other relevant criteria. DRGsare the case-mix measure mandated for Medicare’shospital prospective payment system by the SocialSecurity Amendments of 1983 (Public Law 98-21)(see also “prospective payment system”).
Direct services: Health care provided to eligible Indiansin IHS-operated facilities (see also “contract services”).
Equity fund: A fund established through additionalcongressional appropriations or through a set asideby IHS of a portion of its appropriations, and dis-tributed to benefit IHS service units identified as be-ing deficient in resources relative to other IHS serv-ice units.
Federal recognition: Refers to the relationship betweenIndian tribes and the Federal Government. Federalrecognition can be obtained by satisfying the cri-teria of the Federal Acknowledgement Processadministered through the U.S. Department of theInterior, by Federal statute enacted by Congress,or by court decree. Federally recognized tribes andtheir members are eligible for the special programsprovided by the United States to Indians becauseof their status as Indians (see also “Indian tribe”).
Health center: A relatively comprehensive ambulatorycare facility that is open at least 40 hours per week(see also “health station”).
Health location: Outpatient delivery sites that arestaffed periodically by traveling IHS health per-sonnel.
Health station: An ambulatory care facility, whichmay be a mobile unit, that is open fewer than 40hours per week and offers less complete ambula-tory services than a health center (see also “healthcenter”).
High-cost case: In care purchased by the IHS contractcare program from non-IHS providers, refers tothose cases that are much more expensive than theaverage contract care case, usually defined as ex-ceeding a specific threshold in costs to IHS, suchas $10,000 (see also “catastrophic health care fund”).
Historical budget approach: Also referred to as “pro-gram continuity” budgeting, this is the IHS policy

362 Ž Indian Health Care
of allocating its annual appropriations among the12 areas by granting each area its base budget fromthe previous year plus a share of any funding in-creases equal to the area’s proportion of the over-all IHS budget.
Incidence rate: The frequency of new occurrences ofdisease within a defined time interval in a definedpopulation. Incidence rate is the number of newcases of specific disease divided by the number ofpeople in a population over a specified period oftime, usually 1 year (see also “prevalence”).
Indian: Indians in the Continental United States, andIndians, Aleuts, and Eskimos in Alaska.
Indian preference: An absolute preference for personsof Indian descent in making appointments for Fed-eral employment in BIA and IHS, whether theplacement in the position involves initial appoint-ment, reappointment, reinstatement, transfer, re-assignment, promotion, or any other personnel ac-tion intended to fill a vacancy.
Indian tribe: Any Indian tribe, band, nation, group,Pueblo, rancheria, or community, including anyAlaska Native village, group, or regional or villagecorporation. A tribe may be federally recognized,State-recognized, or self-recognized and/or feder-ally terminated. In the context of the Federal-Indianrelationship, tribes must be federally recognized inorder to be eligible for the special programs andservices provided by the United States to Indiansbecause of their status as Indians (see also “Federalrecognition”).
Infant mortality rate: The number of deaths amongchildren less than 1 year old as a fraction of the to-tal number of live births in a year.
Montana Amendment: Refers to a demonstration pro-gram contained in 1984 legislation that was vetoedby the President, which would have prohibited IHSfrom applying its alternate resource rule to medi-cal or health assistance for indigent Indians in Mon-tana if the assistance was funded by the revenuesfrom any tax imposed on real estate, and the In-dian patient resided on a reservation or restrictedIndian land which was not subject to taxation. Alsoknown as the “Melcher Amendment,” after its spon-sor, Senator John Melcher (D-Mont. ) (see also“alternate resources, “ “primary provider, ” and “re-sidual payer”).
Morbidity: The condition of being diseased.Mortality rate: The death rate, often made explicit for
a particular characteristic; e.g., age, sex, or specificcause of death (see also “crude mortality rate” and“age-adjusted mortality rate”). A mortality rate con-tains three essential elements: 1) the number of peo-ple in a population group exposed to the risk ofdeath (the denominator); 2) a time factor; and 3)
the number of deaths occurring in the exposed pop-ulation during a certain time period (the numerator).
Neonatal: Pertaining to the first four weeks after birth.Perinatal: Pertaining to, or occurring in, the period
shortly before and after birth; variously defined asbeginning with the completion of the 20th to 28thweek of gestation and ending 7 to 28 days afterbirth.
Prevalence rate: The number of existing cases of a dis-ease in a defined population at a particular time orover a specified time period,
Primary provider: Refers to IHS’s description of alter-nate resources in its contract care program. Alter-nate resources or “primary providers” must be usedfirst before IHS will pay for contract care servicesby non-IHS providers (see also “alternate resources, ”“contract services, “ “residual payer, ” and “Montanaamendment”).
Prospective payment system: A hospital paymentmethod in which the amount that a hospital is paidfor services is set prior to the delivery of those serv-ices and the hospital is at least partially at risk forlosses or stands to gain from surpluses that accruein the payment period. Prospective payment ratesmay be per service, per capita, per diem, or per caserates. Medicare’s DRG payment system for in-patient hospital services is a particular form ofprospective payment (see also “diagnosis-relatedgroupings”).
Reservation: The geographic area set aside by treatyor other law for a federally recognized Indian tribe,including reservations, Pueblos, rancherias, or colo-nies, former reservations in Oklahoma, Alaska Na-tive regions established pursuant to the Alaska Na-tive Claims Settlement Act (43 U.S.C. 1601 et seq.),and Indian allotments.
Reservation State: A State in which there is at leastone federally recognized Indian tribe and in whichthe IHS therefore provides or finances health carefor eligible Indians. There were 32 such States asof 1986.
Residual payer: Refers to IHS’s position that othersources of payment available to the patient mustbe used first before IHS will pay for contract careservices by non-IHS providers (see also “alternateresources, ” “contract services, ” and “primaryprovider”).
Retrocession: The voluntary return of a contractedprogram, or portion thereof, to the Federal Gov-ernment pursuant to section 106(d) of the IndianSelf-Determination and Education Assistance Act(Public Law 93-638) (see also “self-determination”and “638 contract”),
Self-determination: A policy established in 1975 in theIndian Self-Determination and Education Assistance

App. F—List of Acronyms and Glossary of Terms . 363
Act (Public Law 93-638) to encourage maximum In-dian participation in the planning, conduct, andadministration of Federal programs and servicesprovided for Indians by IHS and BIA, by transfer-ring responsibilities for these programs and serv-ices from the Federal Government to Indian tribes(see also “retrocession” and “638 contract”).
Service population: The Indian population residing ingeographic areas that are served by IHS. Of the 1.4million Indians identified in the 1980 Census, ap-proximately 829,000, or 59 percent, resided in IHSservice areas. The estimated service population in1986 was 989,000 (see also “Reservation State”).
Service unit: The basic health care delivery unit thatcomprise an IHS area. A service unit may serve atribe or several tribes, and usually 10 to 20 serviceunits make up an IHS area (see also “area”).
Snyder Act: The basic authorizing legislation enactedin 1921 (42 Stat. 208; 25 U.S. C. section 13) for Fed-eral health and social services programs for Indians.
Termination: Refers to Federal policy after World WarII and continuing into the early 1960s, which hadseveral components: 1) induced resettlement ofthousands of reservation Indians into urban centerswhere they were to be trained and employed; 2) thetransfer of major functions, responsibilities, andjurisdiction over Indians to States from the FederalGovernment; and 3) the termination of the Federalrelationship with specific tribes, including endingservices and distributing tribal assets to individualtribal members.
Third-party payer: Refers to a party, other than theprovider or patient, which pays for the patient’s
health care, such as the patient’s health insurancecompany or governmental programs (e. g., Medi-care and Medicaid),
Transfer Act: Legislation (42 U.S.C. sections 2001 etseq. ) that transferred responsibility for Indian healthcare from the Bureau of Indian Affairs in the U.S.Department of the Interior to the Public HealthService in what is now the U.S. Department ofHealth and Human Services, creating IHS in 1955.
Tribal trust land: Lands held in trust for Indian tribesand administered for their benefit by the FederalGovernment (see also “trust responsibility”),
Trust responsibility: The responsibility assumed by theFederal Government, by virtue of treaties, statutesand other means, legally associated with the roleof trustee, to recognize, protect, and preserve tribalsovereignty and to protect, manage, develop, andapprove authorized transfers of interests in trust re-sources held by Indian tribes and Indian individuals.
Urban Indian programs: Programs administered by ur-ban Indian organizations and supported with IHSfunds that operate health centers and help urbanIndians gain access to other programs for whichthey might qualify, such as Medicaid and other pub-lic assistance sources.
638 contract; Contracts between Indian tribes or tribalorganizations and Federal agencies (i. e., IHS andBIA), under which tribes assume planning, opera-tion, and administration of programs and servicesfor Indians from the Federal Government (see also“self-determination” and “retrocession”), Author-ized by the Indian Self-Determination and Educa-tion Assistance Act of 1975 (Public Law 93-638).

References

References
1. Alaska Area Native Health Boards, “Memoran-dum Regarding the Office of Technology Assess-ment Study on Indian Health, ” Anchorage, AK,June 1985.
2. American Hospital Association, American Hos-pital Association Guide to the Health Care Field,1984 edition (Chicago, IL: AHA, 1984).
3. American Hospital Association, Hospita) Statis-tics, 1984 edition (Chicago, IL: AHA, 1984).
4. American Indian Health Care Association, “Re-sponse to OTA Report on Indian Health Care, ”letter to the Office of Technology Assessment,Washington, DC, Oct. 27, 1985.
5, American Indian Health Care Association, TheUrban Indian Health Program (St. Paul, MN:American Indian Health Care Association, nodate).
6. Anderson, N., Tribal Chairman, The San CarlosApache Tribe, San Carlos, AZ, personal com-munication, Nov. 25, 1985.
7. Arfsten, M., Acting Directorr American Indian
8
9,
10.
11.
12
13.
14.15.
Health Care Association, St. Paul, MN, per-sona] communication, Oct. 27, 1985.Armbrust, J., Contract Care Section, AlaskaArea Office, Indian Health Service, Health Re-sources and Services Administration, PublicHealth Service, U.S. Department of Health andHuman Services, Anchorage, AK, personalcommunication, October 1985.Beckwith, C. A., Special Assistant to the Direc-tor, California Program Office, Indian HealthService, Health Resources and Services Admin-istration, Public Health Service, U.S. Depart-ment of Health and Human Services, Sacra-mento, CA, personal communications, August-September 1985.Beiser, M., and Attneave, C. L., “Mental Dis-orders Among Native American Children: Ratesand Risk Periods for Entering Treatment, ” Am.). Psychiatry 139(2):193-198, Feb. 1982.Berman, A., An Analysis of Suicidal and Non-Natural Deaths Among the Duck Valley Reser-vation Indians (Washington, DC: AmericanUniversity Press, 1979).Brookings Institution, The Problem of IndianAdministration (Baltimore, MD: Johns HopkinsPress, 1928).Bryan v. Itasca County, Minnesota, 426 U.S.373 [1975].Bullock v. Carter, 405 U.S. 134 [1972].Bush, M., Branch Chief, Tribal Enrollment Of-fice, Bureau of Indian Affairs, U.S. Department
of the Interior, Washington, DC, personal com-munication, October 1985.
16. Carpenter, K., Grants and Contracts Office, In-dian Health Service, Health Resources and Serv-ices Administration, Public Health Service, U.S.Department of Health and Human Services,Rockville, MD, personal communication, Sept.19, 1985.
17. Casebolt, J., Director, Program Planning Branchr
18.
19.
20.
21.
22.
23.
Office of Planning, Evaluation and Legislation,Indian Health Service, Health Resources andServices Administration, Public Health Service,U.S. Department of Health and Human Serv-ices, Rockville, MD, personal communications,December 1984.Chambers, R. P., “Judicial Enforcement of theFederal Trust Responsibility to Indians, ” Stan.L. Rev. 27:1213-1248, May 1975.Charleston, G. M., Myers, J. G., and Charleston,K., Indian Alcoholism Program Evaluation Fis-cal Year 1984 (Oklahoma City, OK: DatastatComputer Center, 1985).Cherokee Intermarriage Cases, 203 U.S. 76[1904].Cherokee Nation v. Georgia, 30 U.S. [5 Pet. ]1 [1831].Citizens to Preserve Overton Park v. Vo)”e, 401U.S. 402 [1971],Cohen, F. S., Handbook of Federal Indian Law(Albuquerque, NM: University of New MexicoPress, 1971).
24. Colombel, P., Human Resources Management
2526
27
28
Branch, Indian Health Service, Health Re~ourcesand Services Administration, Public HealthService, U.S. Department of Health and HumanServices, presentation at the American PublicHealth Association Conference, Washington,DC, Nov. 20, 1985.Dandridge v. Williamsr 397 U.S. 471 [1970].D’Angelo, A. J., Chief Program Statistics Branch,Indian Health Service, Public Health Service,Health Resources and Services Administration,U.S. Department of Health and Human Serv-ices, personal communication, January 1986.Davidson, R. W., Facilities Management Branch,Indian Health Service, Health Resources andServices Administration, Public Health Service,U.S. Department of Health and Human Serv-ices, Albuquerque, NM, personal communica-tion, Jan. 3, and Summer 1985.Delaware Indians v. Cherokee Nation, 193 U.S.127 [1904].
367

368 ● Indian Health Care
28a. Delaware Tribal Business Committee v. Weeks,43 Us. 73 [1977].
29. Deloria, V., “The Popularity of Being Indian:
30
31.
A New Trend in Contemporary Indian Society, ”Centerboard: The Journal of the Center for Hu-man Relations Studies 2(1):6-12, Spring 1984.“Dental Caries in American Indian and AlaskaNative Children, ” Morbidity and MoralityWeekly Report 34(26):400-401, July 5, 1985.“Early Detection of Primary HepatocelluiarCarcinoma –Alaska,” Morbidity a;d MortaJityWeekly Report 33(5):53-54, Feb. 10, 1984.
32. Edelman, S., Office of Tribal Activities, IndianHealth Service, Health Resources and ServicesAdministration, Public Health Service, U.S. De-partment of Health and Human Services, Rock-ville, MD, personal communication, Jan. 22,1986.
33, Elrod, M., Division of Indian Resource Liaison,Office of Tribal Activities, Indian Health Serv-ice, Health Resources and Services Administra-tion, Public Health Service, U.S. Department ofHealth and Human Services, Rockville, MD,personal communications, Jan. 22, Mar. 11, andMar. 17, 1986.
34. Fischler, R. S., “Child Abuse and Neglect inAmerican Indians, ” Child Abuse and Neglect9(1):95-106, October 1983.
35. Fritz, H., The Movement for Indian Assimila-tion, 1860-1890 (Westport, CT: GreenwoodPress, 1963).
36. Gibson, R. M., and Waldo, D. R., “NationalHealth Expenditures, 1981, ” Health Care Financ-ing Review 4(l): 1-35, September 1982.
37. Gila River Pima-Maricopa Indian Community
38
39.
v. United States, 427 F. id 1194, 1198 (Ct. Cl~,197o), cert. denied, 400 U.S. 819 [1970].Gimon, J., Health Manpower Support Branch,Indian Health Service, Health Resources andServices Administration, Public Health Service,U.S. Department of Health and Human Serv-ices, Rockville, MD, personal communication,Sept. 25, 1985.Gohdes, D. M., “Diabetes Among American In-dians: A Growing Problem, ” inte%al document,Albuquerque, NM, no date.
40. Gonzalez, M., and Henderson, J. Y., “HealthCare for Tribal Citizens: A Criticism of Whitev. Califano, ” Amer. Indian L. Rev. 7:245, 1979.
41. Graham v. Richardson, 403 U.S. 365 [1971].42. Griggs v. Duke Power Co., 401 U.S. 424 [1971].43. Gutierrez, M., Executive Director, California
Rural Indian Health Board, Sacramento, CA,personal communications, August 1985, andOct. 29, 1985.
44. Gutierrez, M., Executive Director, CaliforniaRural Indian Health Board, Sacramento, CA,letter to Gerald Ivey, Acting Director, IndianHealth Service, Aug. 27, 1985.
45. Hammond, J., Contract Health Care Branch, Di-vision of Health Support Activities, IndianHealth Service, Health Resources and ServicesAdministration, Public Health Service, U.S. De-partment of Health and Human Services, Rock-ville, MD, personal communication, Sept. 3,1985.
46. Hanson, I., Portland Area Office ContractHealth Service Program Management, IndianHealth Service, Health Resources and ServicesAdministration, Public Health Servicer U.S. De-partment of Health and Human Services, Port-land, OR, personal communication, Apr. 5,1985.
47. Herman, D. J., “Oral Disease Prevention/OralHealth Promotion, ” The IHS Primary Care Pro-vider 9(12): 1-4, December 1984.
48. Hill, G. L., “Comparison of Two Urban HealthCenters: Toward a Successful Model, ” presentedat the 14th Annual Meeting of the Associationof American Indian Physicians, Scottsdale, AZ,Aug. 14, 1985.
49. Information Systems Strategic Planning TaskForce, “The Indian Health Service 5-year Stra-tegic Information Systems Plan Initiated FiscalYear 1984, ” prepared for the Indian Health Serv-ice, Health Resources and Services Administra-tion, Public Health Service, U.S. Department ofHealth and Human Services, Rockville, MD,undated.
50. Ivey, G., “Policy Memo—Patient Care DataReporting Requirements for the Tribal Contrac-tors, ” memorandum to Indian Health ServiceArea/Program Directors, Rockville, MD, Nov.6, 1985.
51. Ivey, G,, Acting Director, Indian Health Serv-
52
53.
ice, Health Resources and Services Administra-tion, Public Health Service, U.S. Department ofHealth and Human Services, Rockville, MD,personal communication, Nov. 21, 1985.Jacobs, J,, National Health Service Corps, U.S.Department of Health and Human Services,Rockville, MD, personal communication, Feb.5, 1986,Jojola, T., University of New Mexico, NativeAmerican Studies Center, Albuquerque, NM,personal communication, Feb. 21, 1986.
54. Josephy, A. W., The Indian Heritage of Amer-ica (New York: Knopf, 1968).
55. JRB Associates, Inc., “IHS Patient Care Infor-mation System Assessment, ” prepared for the

References . 369
Health Resources and Services Administration,Public Health Service, U.S. Department ofHealth and Human Services, Rockville, MD,1984.
56. Kanter, Williams, Merin & Dickstein, GeneralCounsel to the California Rural Indian HealthBoard, memorandum to Lawrence Miike, Proj-ect Director, Office of Technology Assessment,U.S. Congress, Washington, DC, Aug. 29, 1985.
57. Kauffman, J,, comments on the PBS Broadcast,“Make My People Live: The Crisis in IndianHealth,” Mar. 27, 1984.
58. Kaufman, S. F., Program Statistics Branch, Of-fice of Planning, Legislation and Evaluation, In-dian Health Service, Health Resources and Serv-ices Administration, Public Health Service, U.S.Department of Health and Human Services,Rockville, MD, personal communications, Sept.9, Sept. 27, Oct. 9, Oct. 23, and November1985.
59, Keith, S. N., Bell, R. M., Swanson, A. G., et al.,
60
61
62
“Effects of Affirmative Action in MedicalSchools: A Study of the Class of 1975,” N. Engl.J. Med. 313(24):1519-1525, Dec. 12, 1985.Kelso, J. H., Acting Administrator, Health Re-sources and Services Administration, PublicHealth Service, U.S. Department of Health andHuman Services, Washington, DC, “PublicHealth Service Review and Comments on theOffice of Technology Assessment Draft Reporton Indian Health Care, ” personal communica-tion, Dec. 11, 1985.Kerrigan, M., Director, Office of Third PartyHealth Resource Management, Phoenix Area In-dian Health Service, Health Resources and Serv-ices Administration, Public Health Service, U.S.Department of Health and Human Services,Rockville, MD, personal communication, Aug.13, 1985.King-Shaw, R., Facilities Planning and Con-struction Section, Indian Health Service, HealthResources and Services Administration, PublicHealth Service, U.S. Department of Health andHuman Services, Rockville, MD, personal com-munication, Aug. 22, 1985.
63. Kircher, T., Nelson, J., and Burdo, H., “The Au-topsy as a Measure of Accuracy of the DeathCertificate,” New Eng]. -1. Med. 313(20):1263-69,November 1985.
64. Klausner, S. Z., and Foulks, E. F., Eskimo Capi-talists: Oil, Politics and Alcohol (Totowa, NJ:Allanheld, Osmun, 1982).
65. Lewis v. Weinberger, 415 F. Supp. 652 [D. C. N. M.,1976].
66. Lex, B., “Alcohol Problems in Special Popula-
tions, ” The Diagnosis and Treatment of Alco-holism, 2d cd., J.H. Mendelson and N.K. Mello(eds. ) (New York, NY: McGraw Hill, 1985).
66a. Lone Wolf v, Hitchock, 187 U.S. 553 [1903].67. Lund, E., President, Southeast Alaska Regional
Health Corp., Juneau, AK, personal communi-cations, April/May 1985.
68, Lund, E., President, Southeast Alaska RegionalHealth Corp., Juneau, AK, letter to Jake White-crow, Executive Director, National Indian HealthBoard, Denver, CO, May 10, 1985.
69. Macro Systems, Inc., “Indian Health Service,Contract Health Services, Final Report, ” pre-pared for the Office of the Assistant Secretaryfor Planning and Evaluation, U.S. Departmentof Health and Human Services, Washington,DC, March 1984.
70, Macro Systems, Inc., “Final Report of an Assess-ment of Private Insurance Coverage and Medi-care/Medicaid Reimbursement Among IndiansEligible for Health Care Provided by the IndianHealth Service, ” prepared for the Office of theAssistant Secretary for Planning and Evaluation,U.S. Department of Health and Human Serv-ices, Washington, DC, June 1984.
71. Maier, P., “Second Thoughts on Our First Cen-tury,” New York Times Book Review, July 7,1985, pp. 1, 20-21.
72, Mail, P. D., “American Indian Alcoholism:What Is Not Being Done?” The IHS PrimaryCare Provider 9(3):1-5, March 1984.
73. Martin v. Mancari, 417 U.S. 535 [1974].74. Martinez v. Santa Clara Pueblo, 436 U.S. 49
[1978].75. Martinez v. Southern Llte Tribe, 249 F. 2d 915
[lOth Cir., 1957], cert. den’d. 356 U.S. 960[1957], rehearing den’d. 357 U.S. 924 [1958].
76. Mason, R. D., Mail, P. D., Palmer, I., et al.,Briefing Book for the Alcoholism Program Re-view (Albuquerque, NM: Indian Health Serv-ice Alcoholism Program Branch, Jan. 21, 1985).
77. May, P. A., and Hymbaugh, K. J., “A PilotProject on Fetal Alcohol Syndrome AmongAmerican Indians, ” Listening Post: A Periodi-cal of the Mental Health Programs Indian HealthService 5(3):3-16, October 1985.
78. McCloskey, R. J., Chief, Legislation and Regu-lations Branch, Office of Planning and Evalua-tion, Indian Health Service, Health Resourcesand Services Administration, Public HealthService, U.S. Department of Health and HumanServices, Rockville, MD, personal communica-tions, Nov. 27, 1985, Jan. 3, Jan. 7, Jan. 8, andJan. 20, 1986.
79. McCloud, D., Senior Attorney, Public Health

370 ● Indian Health Care
80.
81.82.
83.
84.
8 5
86,
Division, U.S. Department of Health and Hu-man Services, memorandum to the Director, Of-fice of Legislation and Regulations, IndianHealth Service, Health Resources and ServicesAdministration, Public Health Service, U.S. De-partment of Health and Human Services, com-menting on the Office of Technology Assess-ment’s draft report on Indian Health Care,Rockville, MD, Nov. 25, 1985.McCloud, D., Senior Attorney, Public HealthDivision, U.S. Department of Health and Hu-man Services, Rockville, MD, personal commu-nication, Feb. 6, 1986.McLaughlin v. Florida, 379 U.S. 184 [1964].McNabb v. Heckler et al., No. CU-83-051-GF(D, Mont. 1986).Mellgren, L., Office of the Assistant Secretaryfor Planning and Evaluation, U.S. Departmentof Health and Human Services, Washington,DC, personal communications, Fall 1985.Millar, W., Director, Health Services Manage-ment Branch, Nashville Program Office, IndianHealth Service, Health Resources and ServicesAdministration, Public Health Service, U.S. De-partment of Health and Human Services, Nash-ville, TN, personal communications, July 18 and19, 1985.Milossz, C., Visions From San Francisco Bay,translated by R. Lourie (New York, NY: Farrar,Straus & Giroux, Inc., 1983).Mitchell, J., Director, Division of Health Sup-port Activities, Office of Program Operations,Indian Health Service, Health Resources andServices Administration, Public Health Service,U.S. Department of Health and Human Serv-ices, Rockville, MD, personal communications,November 1984.
87. Moran, J., Director, Division of Grants andProcurement Management, Health Resourcesand Services Administration, Public HealthService, U.S. Department of Health and HumanServices, Rockville, MD, personal communica-tion, Jan. 22, 1986,
88, Morton v. Mancari, 417 U.S. 535 [1974].89. Morton v. Ruiz, 415 U.S. 199 [1974].90. National Diabetes Advisory Board, The Preven-
tion and Treatment of Five Complications of Di-abetes (Atlanta, GA: 1983).
91. National Indian Health Board, “IHS Slated for$10.8 Million Cut in ’86 Under Gramm-Rud-man, ” NIHB Health Reporter 4(20):1-4, January1986.
92. National Research Council and the Institute ofMedicine, Injury in America (Washington, DC:National Academy Press, 1985).
93. National Tribal Chairmen’s Association, testi-mony before hearing of U.S. Congress, Houseof Representatives, House Committee on In-terior and Insular Affairs, H.R. 1426, IndianHealth Care Improvement Act of 1985, Wash-ington, DC, Mar. 19, 1985.
94. Nixon, R., Public Papers of the Presidents of theUnited States, Containing the Public Messages,Speeches, and Statements of the President, 1970,Special Message to the Congress on Indian Af-fairs, July 8, 1970 (Washington, DC: U.S. Gov-ernment Printing Office, 1971).
95. Northwest Portland Area Indian Health Board,“Comments on Office of Technology Assess-ment Draft Report, ” Portland, OR, personalcommunication, December 1985.
96. Oyama v. California, 332 U.S. 633 [1948].97, Passel, J. S., “Provisional Evaluation of the 1970
Census Count of American Indians, ” Demogra-phy 13(3):397-409, August 1976.
98. Patterson v. Council of Seneca Nation, 245 NY
99.
100
233, 157 NE 734 [1927].Pearson, B. F., Associate Director, Office ofAdministration and Management, Indian HealthService Headquarters, presentation made dur-ing a session on “How Indian Health ServiceSpends Its Money, ” Seventh National Indian/Alaska Native Health Conference, Albuquer-que, NM, Nov. 13, 1985.Petersdorf, R. G., Adams, R. D., Braunwald, E.,et al. (eds. ), Harrison’s Principles of InternalMedicine, Ioth ed. (New York: McGraw Hill,1983).
101. Program to Consolidate Health Services forHigh-Risk Young People at Georgetown Univer-sity, “The High-Risk Young People’s Program:A Progress Report, ” Information Exchange, Fall1985.
102. Prucha, F. P., Americanizing the American In-dian (Cambridge, MA: Harvard UniversityPress, 1973).
103. Prucha, F.P. (cd.), Documents of the UnitedStates Indian PoZicy (Lincoln, NE: University ofNebraska Press, 1975).
104. Rincon Band of Mission Indians v. CaliLano, 464F. Supp. 934 [N.D. Cal., 1979], aff’d., 618 F.2d 569 [9th Cir., 1980].
105. Roe v. Wade, 410 U.S. 113 [1973].106. Scholder v. United States, 428 F. 2d 1123 [9th
Cir., 1970], cert. denied, 400 U.S. 942 [1970].107. Seidl, T. C., Assistant Area Director for Plan-
ning and Evaluation, Portland Indian HealthService Area Office, Health Resources and Serv-ices Administration, Public Health Service, U.S.Department of Health and Human Services,

References Ž 371
Portland, OR, personal communication, Oct. 8,and Dec 10, 1985.
108. Shapiro v. Thompson, 394 U.S. 618 [1969].109. Shore, J. H., “American Indian Suicide—Fact
and Fantasy, “ Psychiatry 38:86-91, Feb. 1975.110. Shore, J. H., remarks at Plenary Session of In-
dian Health Service Mental Health Program Re-view, Portland, OR, Jan. 17-19, 1984.
111. Sievers, M.L. “Hypertension in Native Ameri-
112<
113.
114.
115
116
117.
118.
119,
120,
cans, ” The IE/S Primary Care Provider 9(7):6-7, July 1984.Singyke, R., Director, Alaska Area Health Serv-ice, Indian Health Service, Health Resources andServices Administration, Public Health Service,U.S. Department of Health and Human Serv-ices, Anchorage, AK, “Comments on the Officeof Technology Assessment Draft Report on In-dian Health Care, ” personal communication,Nov. 25, 1985.Smith, N., Executive Director, Indian HealthBoard of Minneapolis, Inc., Minneapolis, MN,personal communication, oct. 29, 1985.Snipp, M., University of Maryland, Departmentof Sociology, College Park, MD, personal com-munication referring to an unpublished 1980census monograph entitled “American Indians, ”Feb. 21 and 27, 1986.State of New Mexico, Health and EnvironmentDepartment, Health Services Division, 1982-1983 New Mexico Selected Health Statistics(Santa Fe, NM: State of New Mexico, October1985).State of South Dakota, Department of Health,Center for Health Statistics, State Planning andDevelopment Agency, South Dakota Vital Sta-tistics and Health Status: 1984 (Capital Cityr SD:State of South Dakota, August 1985).Taylor, W., Division of Health Facilities Plan-ning, Office of Management, Health Resourcesand Services Administration, Public HealthService, U.S. Department of Health and HumanServices, Rockville, MD, personal communica-tion, August 1985.TCI, Inc., “Indian Self-Determination Study, ”prepared for the Bureau of Indian Affairs, As-sistant Secretary of the Interior, Indian Affairs,Washington, DC, May 1984.The Grace Commission, “Report on: ContractHealth Services Program of the Indian HealthService, ” Issue PHS-2, internal document, Wash-ington, DC, Oct. 1, 1982.The Navajo Nation, Navajo Tribal Council,“Calling Upon the Congressional Office of Tech-nology Assessment to Provide Congress With aComprehensive Report on the Disparities Be-
121
tween Indian Health Service Area Funding Al-locations and Workloads, ” Resolution CJY-54-85, Window Rock, AZ, July 25, 1985.The President’s Commission on Mental Health,“A Good Day to Live for One Million Indians:Report of the Special Populations Subpanel onMental Health of American Indians and AlaskaNatives, ” Volume IV Appendix, Task PanelReports (Washington, DC: U.S. GovernmentPrinting Office, 1978).
122. Thurmon, R., Health Care Administration
123
124
Branch, Office of Program Operations, Divisionof Health Support Activities, Indian HealthService, Health Resources and Services Admin-istration, Public Health Service, U.S. Depart-ment of Health and Human Services, Rockville,MD, personal communications, November 1984,September 1985, Oct. 3, Oct. 4, and Oct. 10,1985.Thurmon, R., Health Care AdministrationBranch, Office of Program Operations, Divisionof Health Support Activities, Indian HealthService, Health Resources and Services Admin-istration, Public Health Service, U.S. Depart-ment of Health and Human Services, Rockville,MD, disk data made available to the Office ofTechnology Assessment, Oct. 3, 1985.Townsley, H. C., remarks at Plenary Session ofIndian Health Service, Mental Health ProgramReview Portland, OR, Jan. 17-19, 1984.
125. United States v. Patrick, 73 F. 800 [1895].125a. United States v. Sioux Nation, 448 U.S. 371
[1980].126. United States v. Washington, 476 Fed. Supp.
1101 [1974].127. University of Pennsylvania Law Review, “Fed-
128
eral Plenary Power in Indian Affairs After Weeksand Sioux Nation, ” U. Penn. L. Rev. 131:235-270, November 1982.U.S. Congress, American 1ndian Policy ReviewCommission, Report on Indian Hea]th, TaskForce Six: Indian Health, Final Report to theAmerican Indian Policy Review Commission(Washington, K: U.S. Government PrintingOffice, 1976).
129. U.S. Congress, American Indian Policy Review
130
Commission, Report on Indian Law, Task ForceNine: Codification, Revision, and Consolida-tion, Final Report to the American Indian Pol-icy Review Commission (Washington, DC: U,S.Government Printing Office, 1976).U.S. Congress, American Indian Policy ReviewCommission, Final Report of the American In-dian Policy Review Commission (Washington,DC: U.S. Government Printing Office, 1977).

372 ● Indian Health Care
131.
132.
132a
133,
134,
135
136.
137<
U.S. Congress, General Accounting Office,Congressional Monitoring of Planning for In-dian HeaZth Care Facilities Is StilZNeeded, Pub.No. GAO/HRD-80-28 (Washington, DC: U.S.Government Printing Office, Apr. 16, 1980).U.S. Congress, General Accounting Office, In-dian Health Service Not Yet Distributing FundsEquitabZy Among Tribes, Pub. No. GAO/HRD-82-54 (Washington, DC: U.S. GovernmentPrinting Office, July 2, 1982).U.S. Congress, General Accounting Office, re-port on Study of Contract Health Services Pro-gram Claims Processing in the Indian HealthService, as cited in U.S. Department of Healthand Human Services, Public Health Service,Health Resources and Services Administration,Indian Health Service, Director’s Task Force onContrast Health Services, Rockville, MD, Feb-ruary 1983.U.S. Congress, House of Representatives, IndianHealth Care Amendments of 1984, ConferenceReport to accompany S. 2166, Report No. 98-1126 (Washington, DC: U.S. Government Print-ing Office, Oct. 2, 1984).U.S. Congress, House of Representatives, Com-mittee on Appropriations, Department of the In-terior and Related Agencies Appropriation Bill,1984, Report 98-253 (Washington DC: U.S.Government Printing Office, 1984).U.S. Congress, House of Representatives, Com-mittee on Energy and Commerce, Indian HealthCare: An Overview of the Federal Government’sRole, staff report for the Subcommittee onHealth and the Environment, Committee Print98-Y (Washington, DC: U.S. Government Print-ing Office, April 1984).U.S. Congress, House of Representatives, Com-mittee on Energy and Commerce, Indian HealthCare Amendments of 1985, H. Rpt. 99-94, Pt.2 (Washington, DC: U.S. Government PrintingOffice, 1985).U.S. Congress, House of Representatives, Com-mittee on~nterior and Insula-r Affairs, Reauthor-izing and Amending the Indian Health CareImprovement Act, Report No. 99-94, Part 1(Washington, DC: U.S. Government PrintingOffice, May 1985).
138. U.S. Congress, Office of Technology Assess-ment, “Survey of Urban Indian Health Pro-grams, ” internal document, Washington, DC,1985.
139. U.S. Congress, Office of Technology Assess-ment, Children’s Mental Health: Problems and
Treatment (Washington, DC: U.S. GovernmentPrinting Office, forthcoming).
140, U.S. Congress, Office of Technology Assess-
141
—ment, Health Program, “Replacing the RosebudSioux Hospital, “ internal document, Washing-ton, DC, August 1985.U.S. Conm-ess, Senate, Select Committee on In-dian Affairs, Oversight of the Federal Acknowl-edgement Process, hearings, S. Hrg. 98-690(Washington, DC: U.S. Government PrintingOffice, July 21, 1983).
142. U.S. Department of Commerce, Bureau of theCensus, Statistical Abstract of the United States:1975 (Washington, DC: U.S. Government Print-ing Office, 1975).
143. U.S. Department of Commerce, Bureau of theCensus, Statistical Abstract of the United States:1978 (Washington, DC: U.S. Government Print-ing Office, 1978).
144. U.S. De~artment of Commerce, Bureau of the
145
146
Census, >980 Census of Population: Character-istics of the Population, General PopulationCharacteristics, U.S. Summary, PC80-1-B1(Washington, DC: U.S. Department of Com-merce, May 1983).U.S. Department of Commerce, Bureau of theCensus, General Housing Characteristics, U.S.Summary 1980 (Washington, DC: U.S. Depart-ment of Commerce, May 1983).U.S. Department of Commerce, Bureau of theCensus, ‘General Social and Economic Charac-teristics, U.S. Summary 1980, PC80-1-C1 (Wash-ington, DC: U.S. Department of Commerce,December 1983).
147, U.S. Department of Commerce, Bureau of theCensus, 1980 Census of Population: AmericanIndian Areas and Alaska Native Villages: 1980,Supplementary Report, PC80-51-13 (Washing-ton, DC: U.S. Department of Commerce, Au-gust 1984).
148. U.S. Department of Commerce, Bureau of theCensus, American Indian Areas and Alaska Na-tive VilZages: 1980, PC80-S1-13 (Washington,DC: U.S. Department of Commerce, August1984),
149. U.S. Department of Commerce, Bureau of theCensus, Marital Characteristics, PC80-2-4C(Washington, DC: U.S. Department of Com-merce, March 1985).
HO. U.S. Department of Commerce, Bureau of theCensus, Ancestry of the Population by State:1980, PC8O-S1-1O (Washington, DC: U.S. De-partment of Commerce, April 1985).

References ● 373
151. U.S. Department of Commerce, Bureau of theCensus, unpublished tables from the Racial Sta-tistics Branch, 1980 Supplementary Census forAmerican Indians, Washington, DC, July 21,1985.
152. U.S. Department of Commerce, Bureau of theCensus, 1980 Census Population: Volume 2,Subject Reports, American Indians, Eskimos,Aleuts on Identified Reservations and in theHistoric Areas of Oklamoma (Excluding Ur-banized Areas), PC80-2-lD, Part 1 (Washing-ton, DC: U.S. Department of Commerce, No-vember 1985).
153. U.S. Department of Commerce, Bureau of theCensus, 1980 Census of Population: Character-istics of the Population General Social and Eco-nomic Characteristics, United States Summary,PC80-1-C1 (Washington, DC: U.S. GovernmentPrinting Office, December, 1983).
154. U.S. Department of Health, Education, and
155
156
Welfare, - “The Changing Legal Status of theTribal Indian, ” report of the Task Force on In-dians, Monograph #5, Region VIII, Denver, CO,1976.U.S. Department of Health, Education, andWelfare, Public Health Service, Health Servicesfor American Indians (Washington, DC: U.S.DHEW, 1957).U.S. Department of Health Education and Wel-fare, Public Health Service, Health ServicesAdministration, Indian Health Service, Alco-holism: A High Priority Health Problem, DHEWPub. No. (HSA) 77-1OOI (Washington, DC: U.S.DHEW, 1977).
157. U.S. Department of Health, Education, andWelfare, Public Health Service, Health ServicesAdministration, Indian Health Service, SelectedVital Statistics for Indian Health Service Areasand Service Units, 1972 to 1977, DHEW Pub.No. (HSA) 79-1005 (Rockville, MD: HSA,1979) .
158. U.S. Department of Health and Human Serv-ices, National Institute of Health, Child Healthand Human Development: An Evaluation . . .SZDS (Washington, DC: NIH, May 1983).
159. U.S. Department of Health and Human Serv-ices, Office of the Secretary, Office of the Gen-eral Counsel, Public Health Division, draft pro-posed rules of eligibility for services from theIndian Health Service, internal document, Wash-ington, DC, no date.
160. U.S. Department of Health and Human Serv-ices, Public Health Service, Centers for Disease
Control, Suicide Surveillance, 1970-1980 (At-lanta, GA: CDC, March 1985).
161. U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Summary Report,Indian Health Service Mental Health ProgramReview Plenary Session, Portland Oregon, Jan-uary 17-19, 1984 (Rockville, MD: U.S. DHHS,May 1984).
162. U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, “Indian Health,Justification of Appropriation Estimates forCommittee on Appropriations, Fiscal Year1985, ” internal document, Rockville, MD, nodate.
163, U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, “Indian Health,Justification of Appropriation Estimates forCommittee on Appropriations, Fiscal Year1986, ” internal document, Rockville, MD, nodate.
164. U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Bureau of HealthCare Delivery and Assistance, NHSCFact Sheet,March 1985.
165. U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Bureau of HealthProfessions, Division of Disadvantaged Assis-tance, Health Status of Minorities and Low In-come Groups, DHHS Pub. No. (HRSA) HRS-P-DV 85-1 (Washington, DC: U.S. DHHS,1985).
166. U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Discharge Summary, Fiscal Year 1979,Indian Health Service and Contract GeneralHospitals (Rockville, MD: IHS, 1979).
167. U.S. Department of Health and Human Serv-
168
ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, “Priority System for Health FacilityConstruction, ” Docs. 0820B and 2046T, inter-nal document, Rockville, MD, Sept. 19, 1981.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian Hea~thService, “Indian Health Manual, ” internal doc-ument, Rockville, MD, 1983.

374 ● Indian Health Care
169
170
171
171a
172
U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, “Resource Allocation Criteria, VolumeI: RAC Reference Manual, and Volume II: RACWorkbook,” internal document, Rockville, MD,Jan. 3, 1983.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Urban Indian Health Program Evalua-tion Report Fiscal Year 1983 (Tucson, AZ: IHS,February 1984).U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, “Annual Report to Congress on the In-dian Civil Service Retirement Act, Public Law96-135, Fiscal Year 1983, ” internal document,Rockville, MD, May 22, 1984.
. U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, “Annual Report to Congress on the In-dian Civil Service Retirement Act, Public Law96-135, Fiscal Year 1984, ” internal document,Rockville, MD, 1985.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Response to the Subcommittee onHealth and the Environment, Committee onEnergy and Commerce, House of Representa-tives, U.S. Congress, Washington, DC, internaldocument, Summer 1984.
. U.S. Department of Health and Human Serv-173<
ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, revisions to “Indian Health Manual,”transmitted by E.R. Rhoades, memorandum,Rockville, MD, Nov. 27, 1984.
174. U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, memorandum from the chief of the Fa-cilities Management Branch to IHS area/pro-gram directors, Albuquerque, NM, Dec. 10,1984.
175. U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, “Special Report on 15 Leading Causesof Outpatient Care by Area, Service Unit, State,and County, “ internal document, Albuquerque,NM, 1985,
175a.
176.
177
178.
179
180.
181
182.
183,
U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, computer tape supplied to the Office ofTechnology Assessment, Washington, DC, 1985.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, “Findings From an Oral Health Surveyof Native Americans, “ internal document, Rock-ville, MD, Jan. 31, 1985,U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, “History of Sanitation Facilities Con-struction, ” internal document, Rockville, MD,Feb. 15, 1985.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, “Fiscal Year 1987, Justification of Ap-propriation Estimates for Committees on Ap-propriations, ” vol. X, Indian Health, internaldocument for Appropriations hearings, Wash-ington, DC, Spring 1986.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Indian Health Service: A Comprehen-sive Health Care Program . . . (Washington,DC: U.S. DHHS, no date).U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Dental Services Branch, “Computationof Units Provided Activity, ” internal document,Rockville, MD, Mar. 28, 1985.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Director’s Task Force on ContractHealth Services, “Report of the IHS Director’sTask Force on Contract Health Services asTransmitted by the Director, Indian HealthService, ’r internal document, Rockville, MD,February 1983.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Director’s Task Force on ContractHealth Services, “Director’s Task Force on Con-tract Health Services, Task D, Concept Paper, ”internal document, Rockville, MD, September1983.U.S. Department of Health and Human Serv-

References Ž 375
184
185
186
187.
188
189
190.
ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Division of Health Systems Develop-ment, Urban Indian Health Program EvaluationReport FY 1983 (Tucson, AZ: IHS, February1984) .U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Division of Health Systems Develop-ment, (_Jrban Inclian Flealth F’rogram EvaluationReport FY 1984 (Tucson, AZ: IHS, June 1985).U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Division of Health Systems Develop-ment, Evaluation Report Charts and Graphs FY1984 (Tucson, AZ: IHS, June 1985).U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Division of Health Systems Develop-ment, “Interim Report: Descriptive Analysis ofTribal Health Systems, October 1, 1984—September 30, 1985, ” internal document, Tuc-son, AZ, Feb. 14, 1986.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Nashville Program Office, “Summaryof 638 Contract Points, ” internal document,Nashville, TN, Sept. 24, 1984.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Office of Planning, Evaluation and Leg-islation, Program Statistics Branch, IndianHealth Service Chart Series Book June 1984(Rockville, MD: IHS, 1984).U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Office of Planning, Evaluation and Leg-islation, Program Planning Branch, “Listing ofTribal Deficiency Levels and Rankings Follow-ing Distribution of the Fiscal Year 1984 EquityFund, ” internal document, Rockville, MD, April1984.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Office of Planning, Evaluation, andLegislation, Program Statistics Branch, “Facil-ity Planning Forecasting Guidelines, ” internaldocument, Rockville, MD, August 1984.
191
192,
193<
194,
195,
196,
U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Office of Planning, Evaluation and Leg-islation, Program Statistics Branch, IndianHealth Service Chart Series Book April 1985(Rockville, MD: IHS, 1985).U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Office of Planning, Evaluation and Leg-islation, Program Statistics Branch, Tables ofEstimated Population and Percent Distributionof the Total Indian and Alaska Native Popula-tion for Reservation States by Age and Sex, 1980Census Data, internal document, Rockville,MD, February 1985.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Office of Planning, Evaluation and Leg-islation, Program Statistics Branch, “PercentDistribution of the Total Indian and Alaska Na-tive Population for 32 Reservation States by Ageand Sex, 1980 Census, ” internal document,Rockville, MD, Aug. 29, 1985.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Office of Planning, Evaluation and Leg-islation, Progam Statistics Branch, Summary ofLeading Causes for Outpatient Visits, IndianHealth Service Facilities, Fiscal Year 1984 (Rock-ville, MD: IHS, no date).U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Office of Planning, Evaluation and Leg-islation, Program Statistics Branch, Patient CareStatistics Staff, “Utilization of Indian HealthService and Contract Hospitals, Fiscal Year1984, ” internal document, Rockville, MD, 1985.U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Office of Tribal Activities, ]ndianHealth Notes 2(14), July 26, 1984.
197. U.S. Department of Health and Human Serv-ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Oklahoma Area Office, “OklahomaArea Contract Health Service CatastrophicFund,” internal document, Oklahoma City, OK,undated.
198. U.S. Department of Health and Human Serv-

376 Ž Indian Health Care
ices, Public Health Service, Health Resourcesand Services Administration, Indian HealthService, Portland Area Office, “Catastrophic Re-port, Portland Area Indian Health Service, Fis-cal Year 1984, ” Portland, OR, May 1, 1985.
199. U.S. Department of Health and Human Serv-ices, Public Health Service, National Center forHealth Statistics, Annotated Bibliography ofCause of Death Validation Studies: 1958-1980,Data Evaluation and Methods Research Series2, No. 89, DHHS Pub. No. (PHS) 82-1363(Hyattsville, MD: PHS, 1982).
200. U.S. Department of Health and Human Serv-ices, Public Health Service, National Center forHealth Statistics, “1981 Summary: NationalAmbulatory Medical Care Survey, ” AdvanceData From Vital and Health Statistics, No. 88(Hyattsville, MD: PHS, Mar. 16, 1983).
201. U.S. Department of Health and Human Serv-ices, Public Health Service, National Center forHealth Statistics, “Advance Report of Final Mor-tality Statistics, 1981, ” A40nthly Vital StatisticsReport 33(3) :supp., June 22, 1984.
202. U.S. Department of Health and Human Serv-ices, Public Health Service, National Center forHealth Statistics, Health, United States, 2984,DHHS Pub. No. (PHS) 85-1232 (Washington,DC: U.S. Government Printing Office, Decem-ber 1984).
203. U.S. Department of Health and Human Serv-ices, Public Health Service, National Center forHealth Statistics, “1984 Summary: National Hos-pital Discharge Survey, ” Advance Data FromVital and Health Statistics, No. 112, DHHS Pub.No. (PHS) 85-1250 (Hyattsville, MD: PHS,Sept. 27, 1985).
204. U.S. Department of the Interior, Bureau of In-dian Affairs, Division of Law Enforcement Serv-ices, Tribal and Bureau Law Enforcement Serv-ices Automated Data Report, January 1, 1980-December 31, 1980 (Washington, DC: BIA, nodate).
205. U.S. Department of the Interior, Bureau of In-dian Affairs, Division of Law Enforcement Serv-ices, Tribal and Bureau Law Enforcement Serv-ices Automated Data Report, January 1, 1981-December 31, 1981 (Washington, DC: BIA, nodate).
206. U.S. Department of the Interior, Bureau of In-dian Affairs, Division of Law Enforcement Serv-ices, Tribal and Bureau Law Enforcement Serv-ices Automated Data Report, January 1, 1982-December 31, 1982 (Washington, DC: BIA, nodate).
207. U.S. Department of the Interior, Bureau of In-dian Affairs, Division of Law Enforcement Serv-ices, Tribal and Bureau Law Enforcement Serv-ices Automated Data Report, January 1, 1983-December 31, 2983 (Washington, DC: BIA, nodate).
208. U.S. Department of the Interior, Bureau of In-dian Affairs, Office of Financial Management,“Local Estimates of Resident Indian Populationand Labor Force Status: December 1981, ” inter-nal document, Washington, DC, January 1982.
209. U.S. Department of the Interior, Bureau of In-dian Affairs, Office of Financial Management,“Local Estimates of Resident Indian Populationand Labor Force Status, January 1985, ” inter-nal document, Washington, DC, 1985.
21o. Washburn, W. E., “The Historical Context ofAmerican Indian Legal Problems, ” Law andCont. Prob. 40:4, 1976.
211. Westermeyer, J., “Erosion of Indian MentalHealth in Cities, ” Minnesota Medicine 59(6),June 1976.
212. White v. C’a]ifano, 9th Cir. [1978].213. Whiting v. United States, Civ. No. 75-3007
[D. S. D., 1975].214. Wiggins, C., Health Services Planning Section,
Program Planning Branch, Office of Planning,Evaluation and Legislation, Indian Health Serv-ice, Health Resources and Services Administra-tion, Public Health Service, U.S. Department ofHealth and Human Services, Rockville, MD,personal communications, Sept. 4, 1985, Dec.16, 1985, and February/March 1986.
215. Williams, R., “638 Contract Data SummarySheets by Area, 1979-1985,” prepared for the In-dian Health Service, Health Resources and Serv-ices Administration, Public Health Service, U.S.Department of Health and Human Services, in-ternal document, Rockville, MD, Nov. 12, 1985.
216. Williams, R., Program Analyst, Division of In-dian Resources Liaison, Indian Health Service,Health Resources and Services Administration,U.S. Department of Health and Human Serv-ices, Rockville, MD, personal communication,Nov. 7, 1985.
217. Wilson, M., “The Federal Trust Responsibilityand Obligation to Provide Health Care to In-dian People,” Research Institute on Legal Assis-tance of the Legal Services Corp., internal doc-ument, Mar. 10, 1980.
218. Wiszneauckas, D. G., Division of Grants andContracts, Office of Resource Management, Of-fice of the Assistant Secretary for Health, Pub-lic Health Service, U.S. Department of Health

References ● 377
and Human Resources, Rockville, MD, personalcommunication, Nov. 5, 1984.
219. Wolford, E. W., “RPMS (Resource and PatientManagement System) Overview, ” memorandumto Associate Administrator, Office of Planning,Evaluation and Legislation, Health Resourcesand Services Administration, Public HealthService, U.S. Department of Health and HumanServices, Rockville, MD, Nov. 20, 1985.
220. Worcester v. Georgia, 31 U.S. [6 Pet. ] 515[1831].
221. Yamashita, S. K., and Cole, H., The FuturesGroup, Demographic Project on Model, pre-
pared for the Office of Technology Assessment,U.S. Congresss, Washington, DC, 1985.
222. Young, L., Office of Associate Administrator forOperations and Management, Health Resourcesand Services Administration, Public HealthService, U.S. Department of Health and HumanServices, Rockville, MD, personal communica-tions, November 1984.
223. Young, J. L., Ries, L. G., and Pollack, E. S., “Can-cer Patient Survival Among Ethnic Groups inthe United States, ” Journal of the National Can-cer Institute 73(2):341-352, August 1984.