Embed Size (px)
Citation preview
2017ASCLS Annual Meeting
Indianapolis, IN
The impact of a large fetomaternal bleed on the clinical laboratory.
Lesa Nelson MLS(ASCP)cm
Hendricks Regional HealthMichigan State University Graduate Student
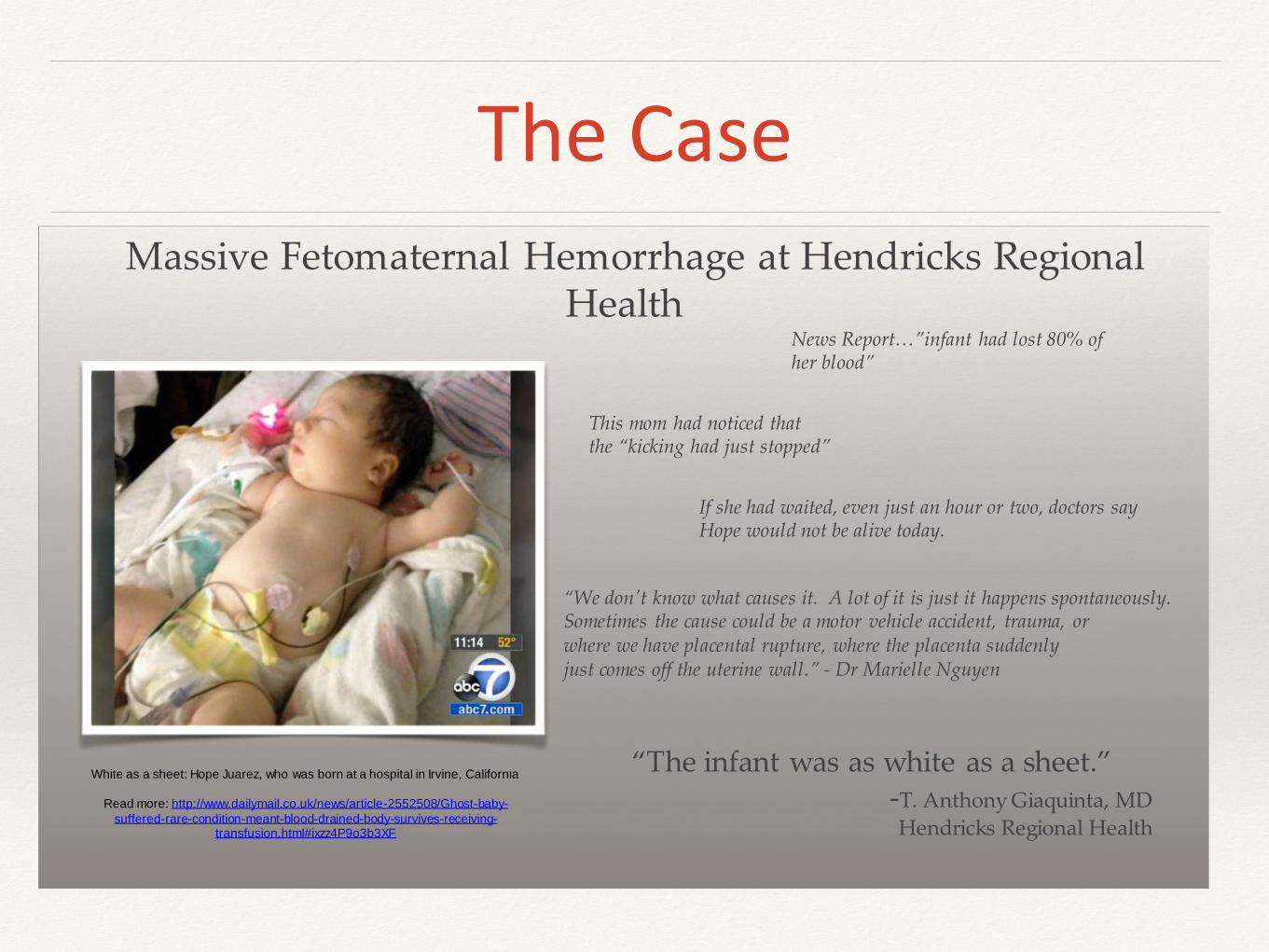
The CaseMassive Fetomaternal Hemorrhage at Hendricks Regional
Health
“The infant was as white as a sheet.”-T. Anthony Giaquinta, MD
Hendricks Regional Health
White as a sheet: Hope Juarez, who was born at a hospital in Irvine, California
Read more: http://www.dailymail.co.uk/news/article-2552508/Ghost-baby-
suffered-rare-condition-meant-blood-drained-body-survives-receiving-transfusion.html#ixzz4P9o3b3XF
News Report…”infant had lost 80% of her blood”
This mom had noticed that the “kicking had just stopped”
If she had waited, even just an hour or two, doctors say Hope would not be alive today.
“We don't know what causes it. A lot of it is just it happens spontaneously. Sometimes the cause could be a motor vehicle accident, trauma, or where we have placental rupture, where the placenta suddenly just comes off the uterine wall.” - Dr Marielle Nguyen
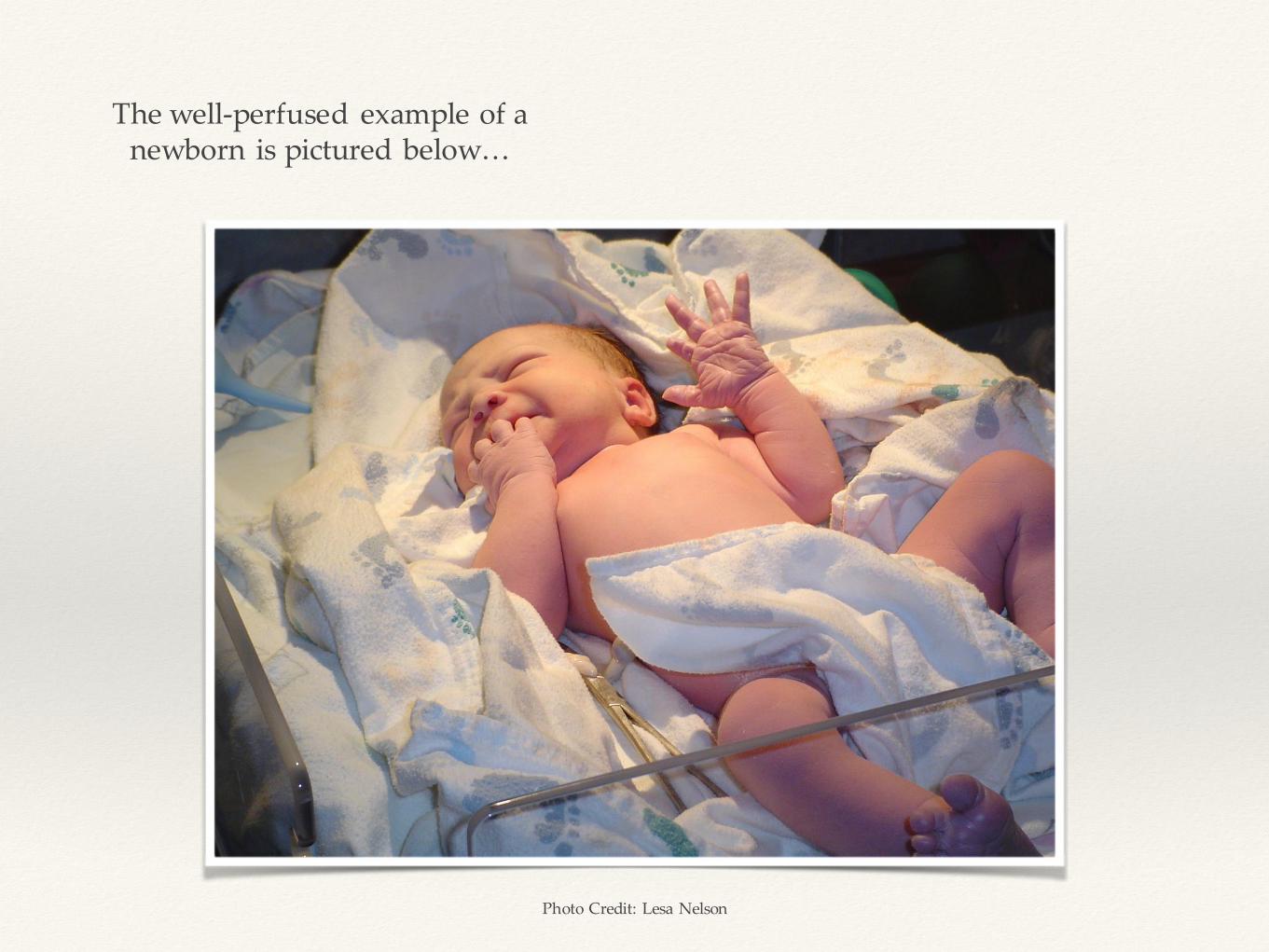
The well-perfused example of a newborn is pictured below…
Photo Credit: Lesa Nelson
Objectives
• Describe the events surrounding the case study
• Identify laboratory areas involved and review abnormal results
• Discuss treatment decisions
• Discuss Fetomaternal Hemorrhage
• Outcome of patient(s)
The Mother
• 27 years old
• OB History = G1 P1 Pr0 Ab0 LC1 (First Pregnancy)
“G” Gravada = Number of Pregnancies
“P” Para = Number of births of viable offspring
“Pr” PreTerm = Number of pre-term births (<37 weeks)
“A” Abortus = Number of abortions
“LC” Living Children = Number of children living
Dates of Interest
•Estimated Delivery Date: 2/19/2016
•Actual Delivery Date: 2/5/2016

Prenatal Results
Prenatal care was received, including testing, physical exams, and fetal monitoring.
Test Result
Syphillis Nonreactive
Hepatitis Negative
HIV Negative
Rubella Immune
GBS Culture Positive
HPV Positive
ABO /Rh O Negative
Antibody Screen Negative
Rhogam® Received at 28w gestation
Pre - Admission
• No complications during the course of prenatal care.
• Mother noticed a decrease in fetal movement on day of delivery, which prompted her arrival at Hendricks to be seen.
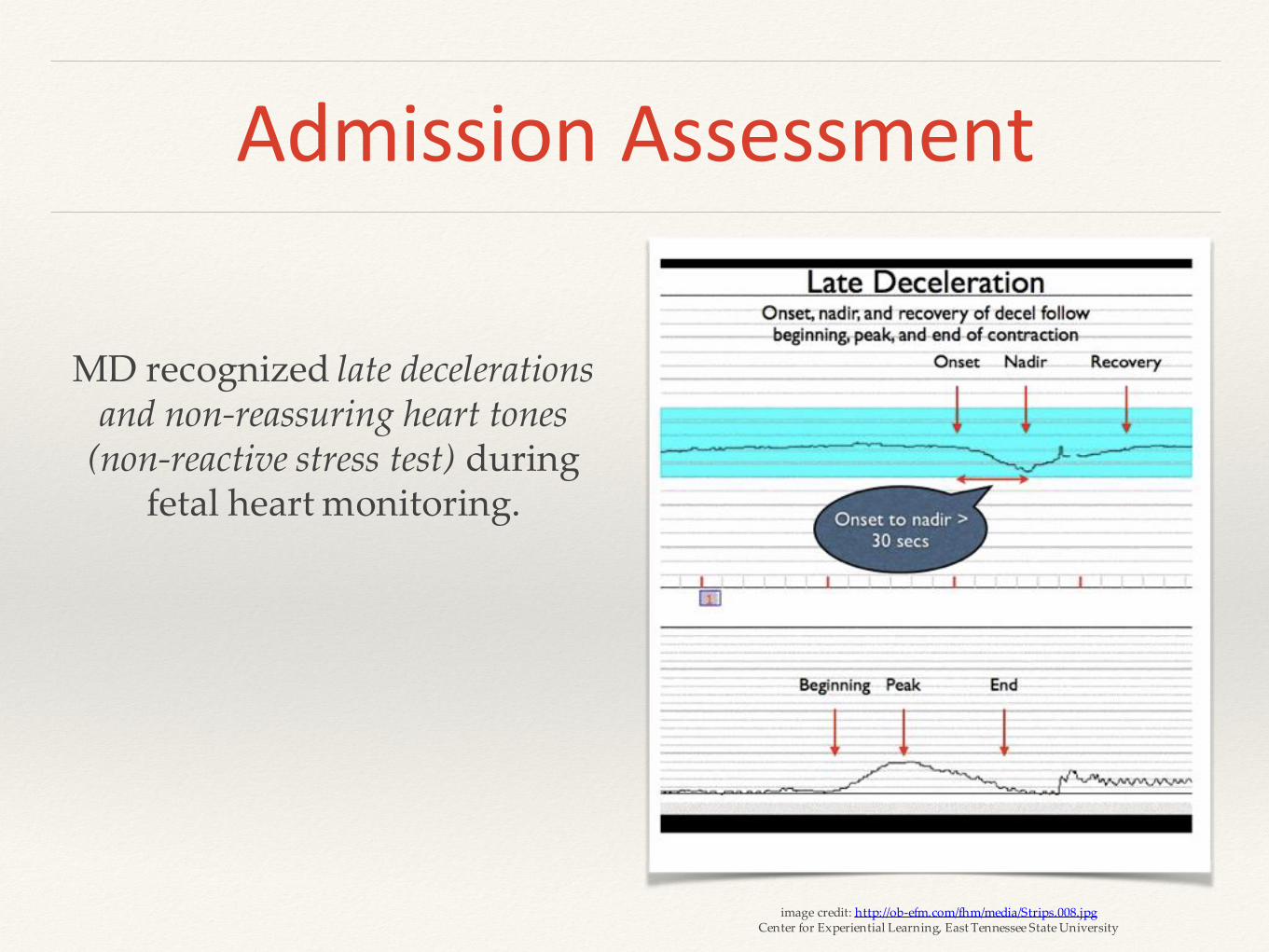
Admission Assessment
MD recognized late decelerations and non-reassuring heart tones
(non-reactive stress test) during fetal heart monitoring.
image credit: http://ob-efm.com/fhm/media/Strips.008.jpgCenter for Experiential Learning, East Tennessee State University
What is a Deceleration?
• Fetal Heart Rate (FHR) Changes
• Accelerations = increases in FHR, usually with fetal movement, vaginal exams, contractions, and other fetal stimulation.
• Decelerations = decreases in FHR below the baseline rate, late decelerations indicate the baby is not getting enough oxygen. Late decelerations occurring along with tachycardia mean that contractions may be contributing to the deprivation of oxygen to the baby.
3 Types of Decelerations
• Early - can be caused by fetal head compression during uterine
contraction.
• Variable - most common, vary in duration, time, and intensity. Typical
with premature rupture of membranes, decreased amniotic fluid volume, and cord compression.
• Late - Symmetric fall in fetal heart rate. Observed with a decrease in uterine
blood flow or placental dysfunction (can be caused by post-date gestation, preeclampsia, chronic hypertension, and diabetes mellitus).
EFM Monitoring
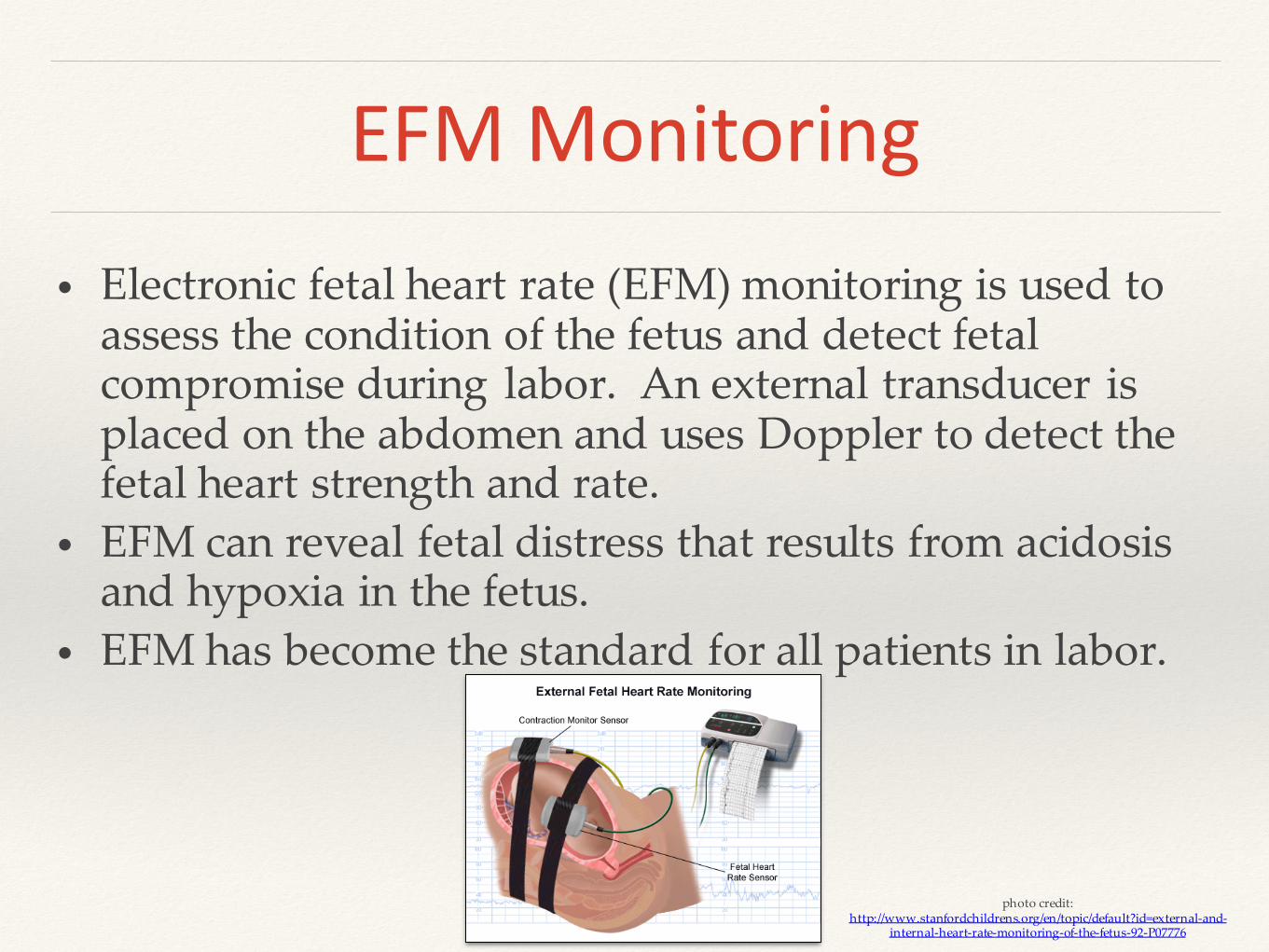
• Electronic fetal heart rate (EFM) monitoring is used to assess the condition of the fetus and detect fetal compromise during labor. An external transducer is placed on the abdomen and uses Doppler to detect the fetal heart strength and rate.
• EFM can reveal fetal distress that results from acidosis and hypoxia in the fetus.
• EFM has become the standard for all patients in labor.
photo credit: http://www.stanfordchildrens.org/en/topic/default?id=external-and-
internal-heart-rate-monitoring-of-the-fetus-92-P07776
Example
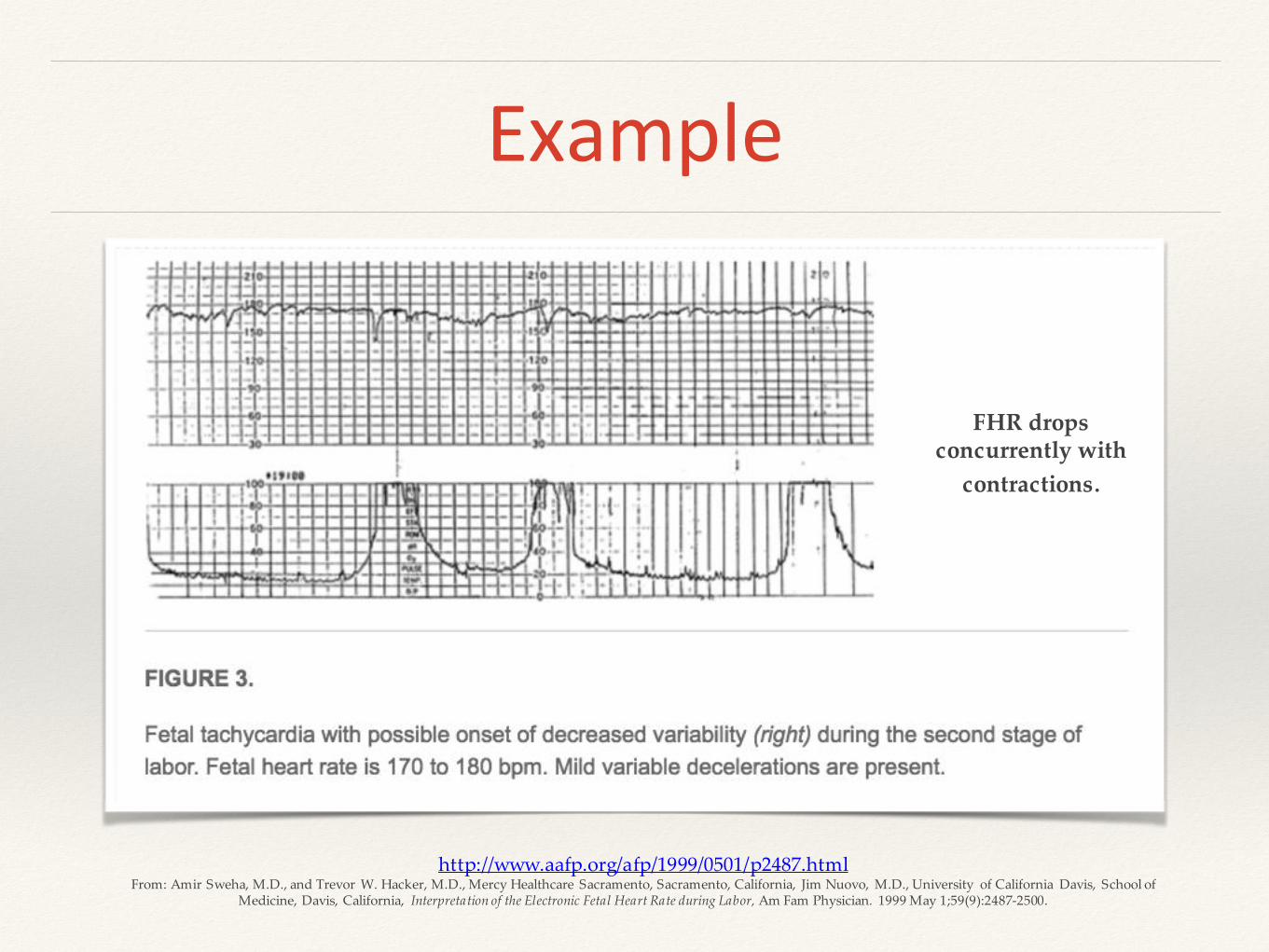
http://www.aafp.org/afp/1999/0501/p2487.htmlFrom: Amir Sweha, M.D., and Trevor W. Hacker, M.D., Mercy Healthcare Sacramento, Sacramento, California, Jim Nuovo, M.D., University of California Davis, School of
Medicine, Davis, California, Interpretation of the Electronic Fetal Heart Rate during Labor, Am Fam Physician. 1999 May 1;59(9):2487-2500.
FHR drops concurrently with
contractions.
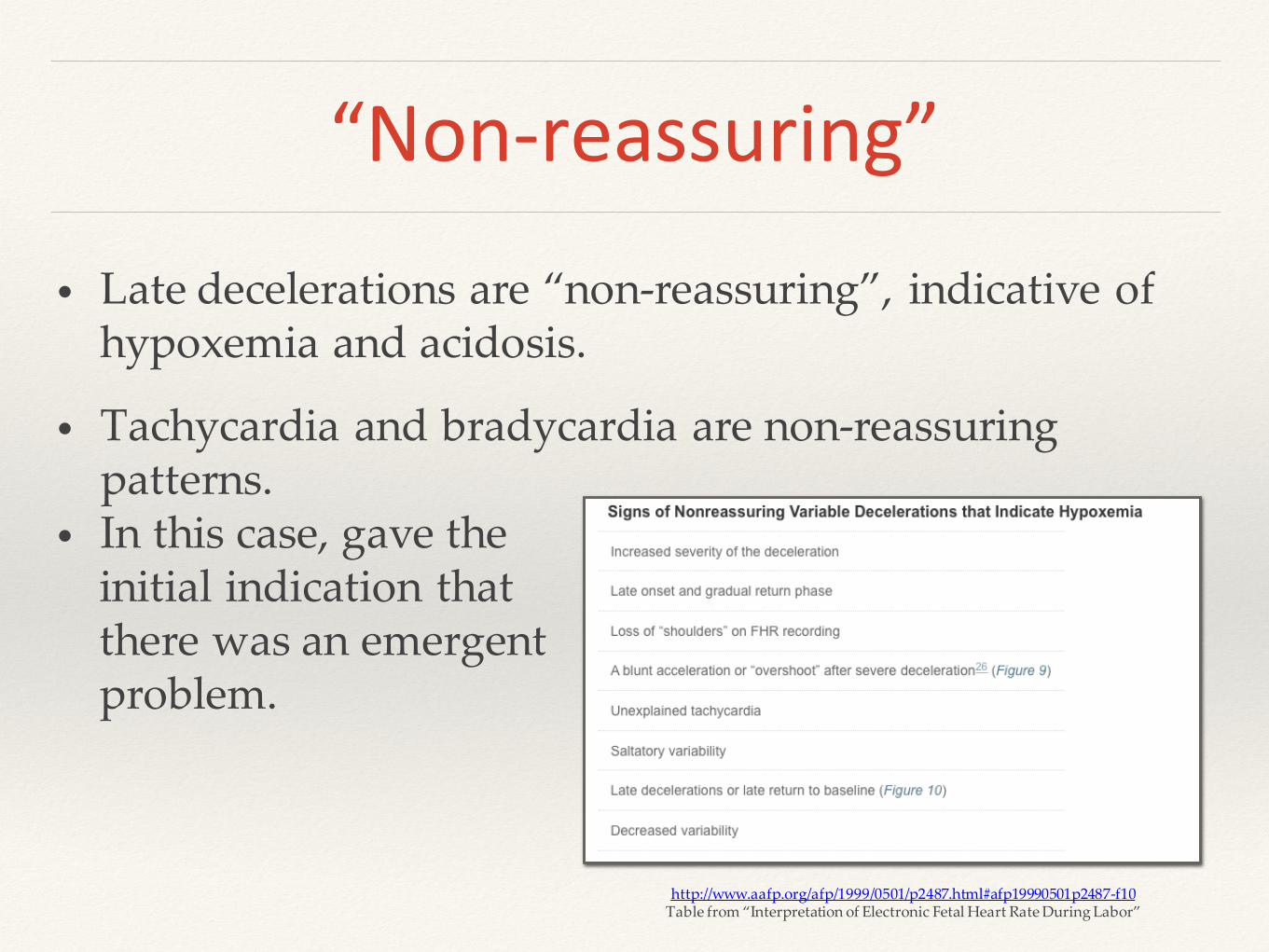
“Non-reassuring”
• Late decelerations are “non-reassuring”, indicative of hypoxemia and acidosis.
• Tachycardia and bradycardia are non-reassuring patterns.
• In this case, gave the initial indication thatthere was an emergent problem.
http://www.aafp.org/afp/1999/0501/p2487.html#afp19990501p2487-f10Table from “Interpretation of Electronic Fetal Heart Rate During Labor”
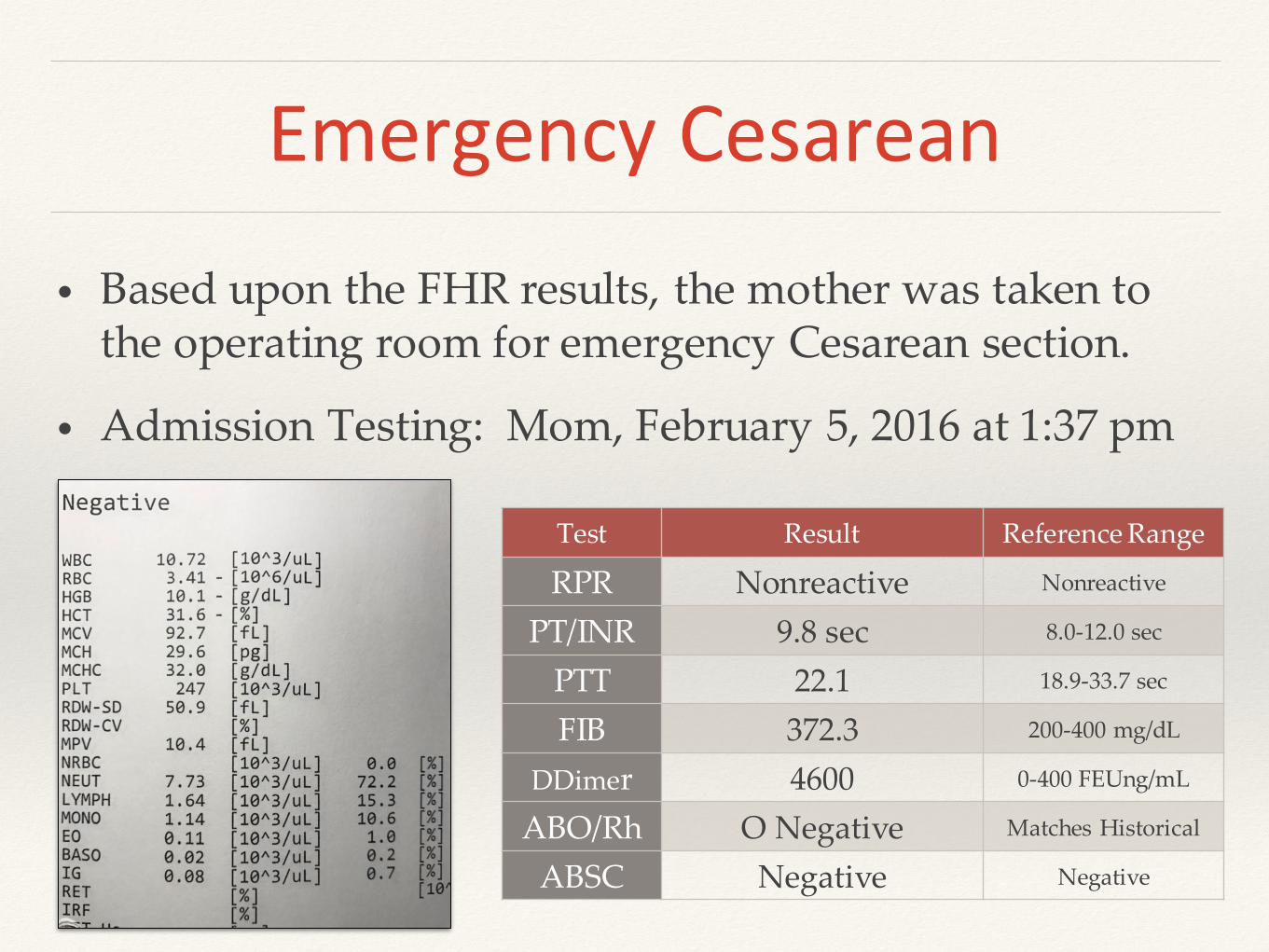
Emergency Cesarean
• Based upon the FHR results, the mother was taken to the operating room for emergency Cesarean section.
• Admission Testing: Mom, February 5, 2016 at 1:37 pm
Test Result Reference Range
RPR Nonreactive Nonreactive
PT/INR 9.8 sec 8.0-12.0 sec
PTT 22.1 18.9-33.7 sec
FIB 372.3 200-400 mg/dL
DDimer 4600 0-400 FEUng/mL
ABO/Rh O Negative Matches Historical
ABSC Negative Negative
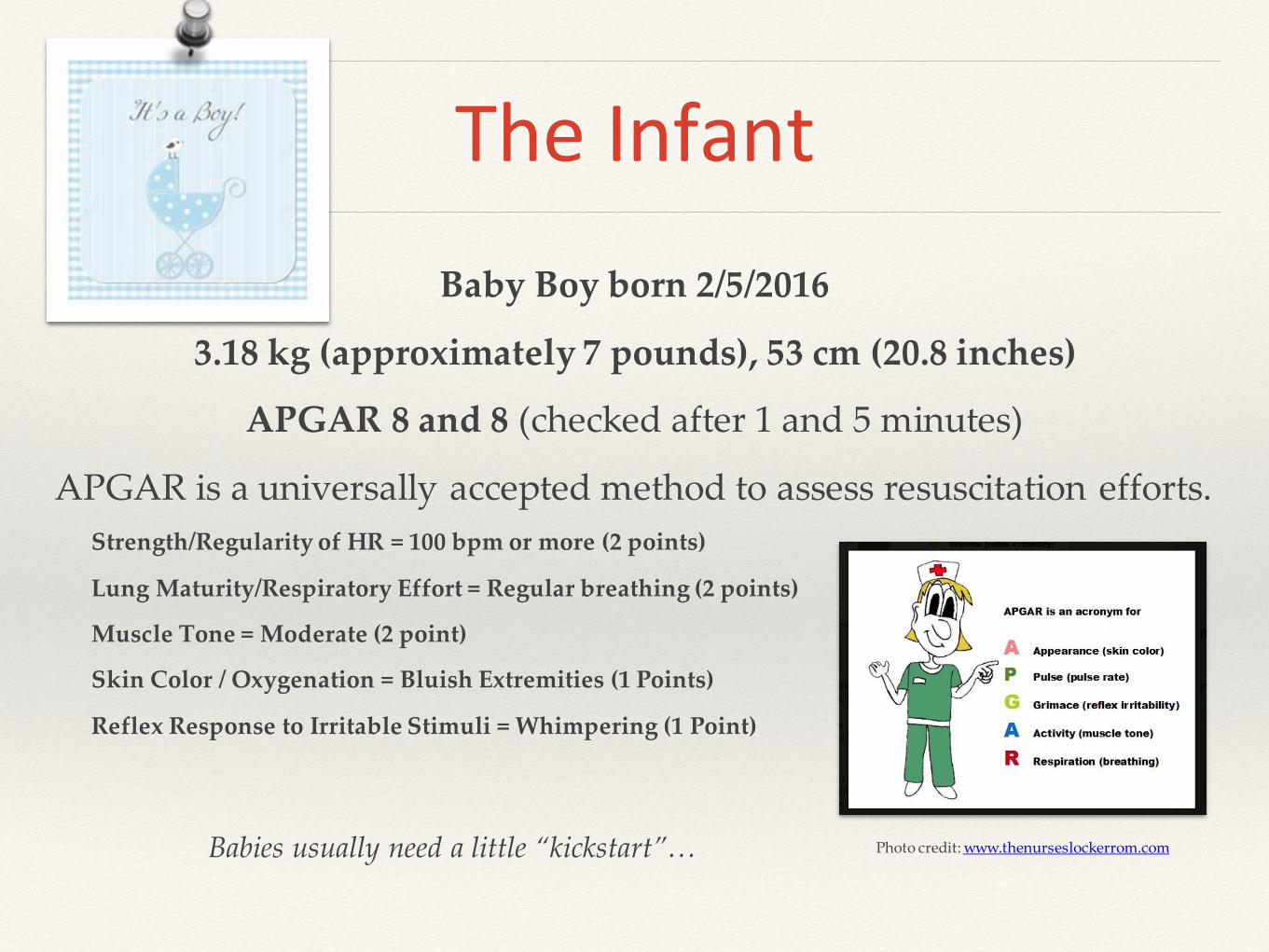
The Infant
Baby Boy born 2/5/2016
3.18 kg (approximately 7 pounds), 53 cm (20.8 inches)
APGAR 8 and 8 (checked after 1 and 5 minutes)
APGAR is a universally accepted method to assess resuscitation efforts.
Strength/Regularity of HR = 100 bpm or more (2 points)
Lung Maturity/Respiratory Effort = Regular breathing (2 points)
Muscle Tone = Moderate (2 point)
Skin Color / Oxygenation = Bluish Extremities (1 Points)
Reflex Response to Irritable Stimuli = Whimpering (1 Point)
Photo credit: www.thenurseslockerrom.comBabies usually need a little “kickstart”…

Infant Assessment
Pale appearance (should be reddish/pink)
Tachycardia 180-190’s (should be 120-160’s)
Normal Blood Pressure
Acidotic (pH 7.13, bicarb 8.4) (pH <7.25 caused by hypoxia induced anaerobic metabolism.)
No obvious external bleeding from infant observed.
*Bloody amniotic fluid was noted at time of incision.
*No hydrops fetalis detected upon ultrasound (abnormal fluid accumulation in 2 or more fetal compartments)
“Compensated Hypovolemic Shock”…per Dr. Giaquinta.
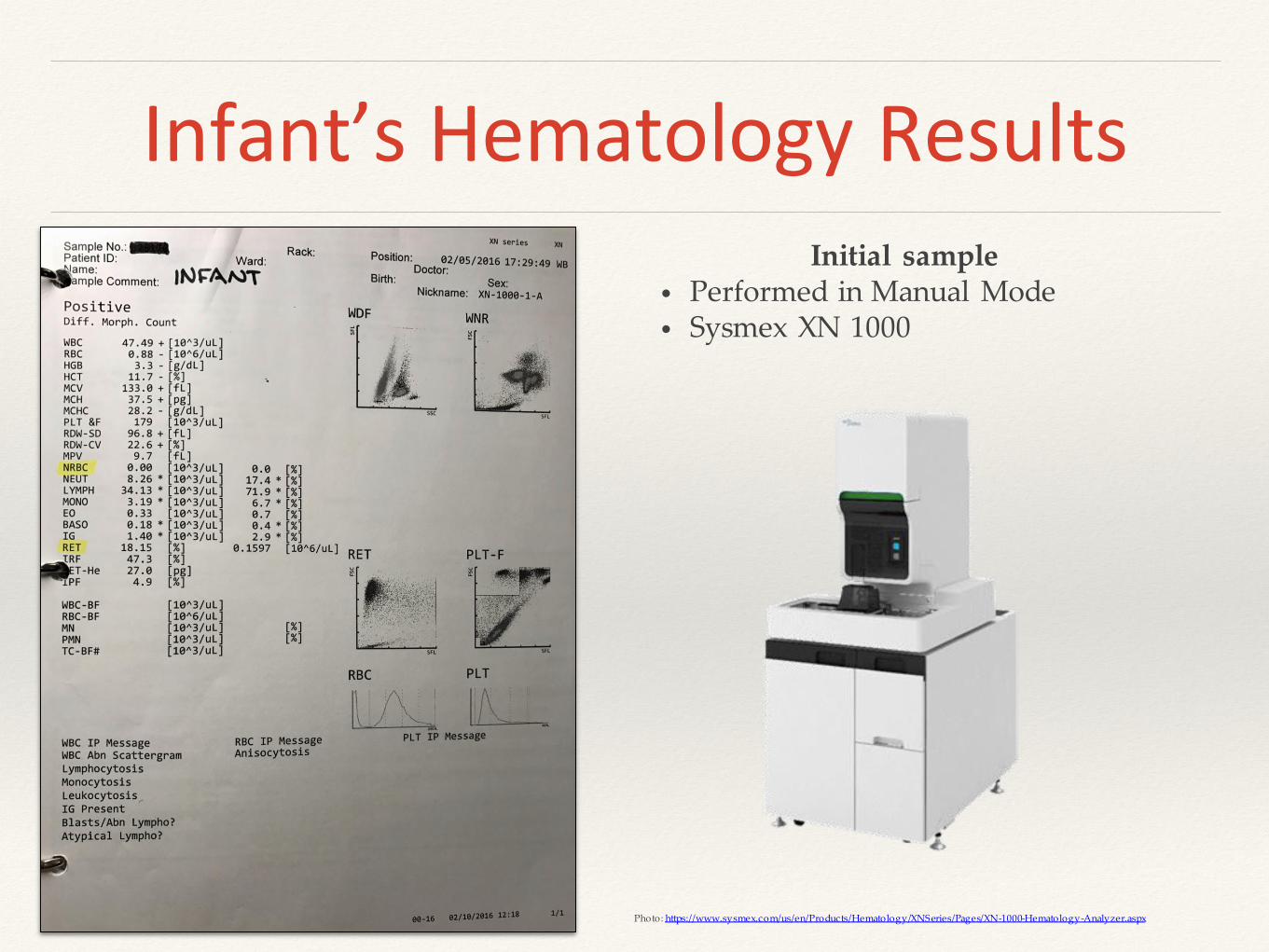
Infant’s Hematology ResultsInitial sample
• Performed in Manual Mode• Sysmex XN 1000
Photo: https://www.sysmex.com/us/en/Products/Hematology/XNSeries/Pages/XN-1000-Hematology-Analyzer.aspx

What do you see on the CBC?
• Elevated WBC• Low Red Cells• Critically Low Hemoglobin• Critically Low Hematocrit• Nucleated Red Cells…WBC correction
WBC = XN count x100 / 100 + NRBC
Also noted on the slide review/differential:
• 3+ Polychromasia• 3+ Schistocytes and Burr Cells• 3+ Anisocytosis• 2+ Macrocytes• Few Erythroblasts noted
• The slide was reviewed by the pathologist and a consult was made with the physician.
• Reticulocyte Count was not ordered/reported… RETIC = 18.2% (0.5 -1.8%)
IRF = 47.3% (2.3 - 13.4%)
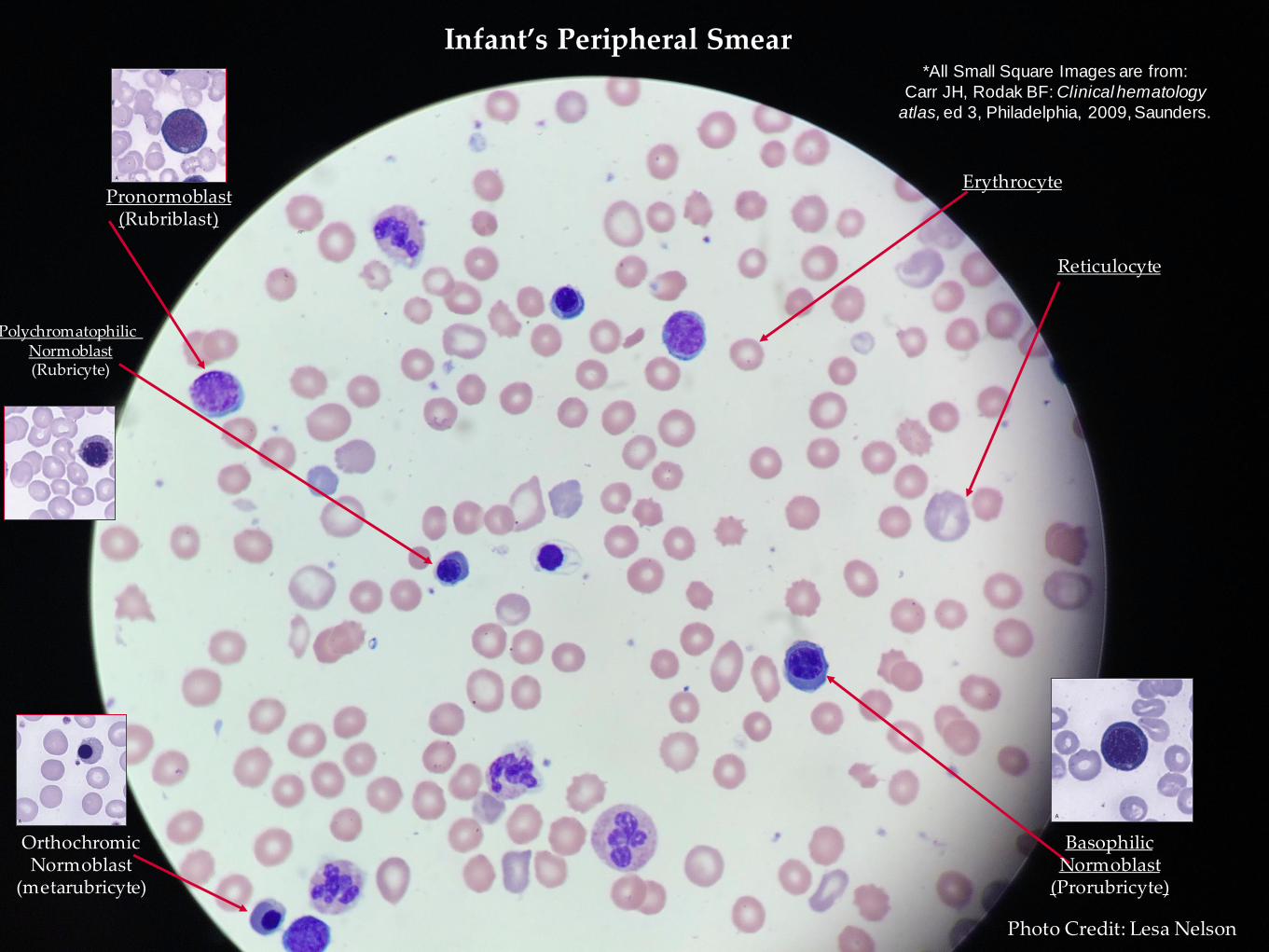
Reticulocyte
ErythrocytePronormoblast
(Rubriblast)
Basophilic Normoblast
(Prorubricyte)
OrthochromicNormoblast
(metarubricyte)
Polychromatophilic Normoblast(Rubricyte)
Infant’s Peripheral Smear*All Small Square Images are from:
Carr JH, Rodak BF: Clinical hematology
atlas, ed 3, Philadelphia, 2009, Saunders.
Photo Credit: Lesa Nelson
Blood Bank
Infant Cord Blood Test Results:
O Positive
DAT Negative
Image Credit: www.nzblood.co.nz
Mom’s Blood Type is…
O Negative

Treatment
The infant was transfused with one unit of O Neg, CMV Negative, Irradiated, Leukoreduced Packed Red Cells at a volume of 10 mL/kg…approximately 32 mL was transfused. The transfusion was started at Hendricks Regional Health in Danville, IN….
Image Credit: https://blood.ca/en/hospitals/component-modifications
Image credit: http://www.usatoday.com/story/news/2015/03/16/blood-needed-o-negative/24870849/

The transfusion was completed while being transported to Riley Hospital for Children in
Indianapolis, IN.
Photo Credit: https://www.flickr.com/photos/88417894@N06/
Infant Treatment at Riley
The admission exam of the infant at Riley revealed the following:
• Clear breath sounds, mild tachypnea
• Regular Heart Rate and Rhythm, 2-3 second capillary refill
• Crying upon exam, Normal strength and tone, positive grasp, spontaneous movements in all extremities.
• Initial H&H on 2/5/16 at Riley = 6.5 g/dL & 19% respectively and was transfused with an additional unit of RBC’s while at Riley.
Discharge Assessment
• Sepsis was ruled out by negative blood culture results.
• Coagulation testing was normal, acidosis resolved.
• Color upon discharge was pink/perfused, neurologic exam was normal for age, regular heart rate and rhythm, high pitched-cry.
• Discharge H&H on 2/8/16 at Riley was 13 g/dL & 39% respectively
What about Mom?
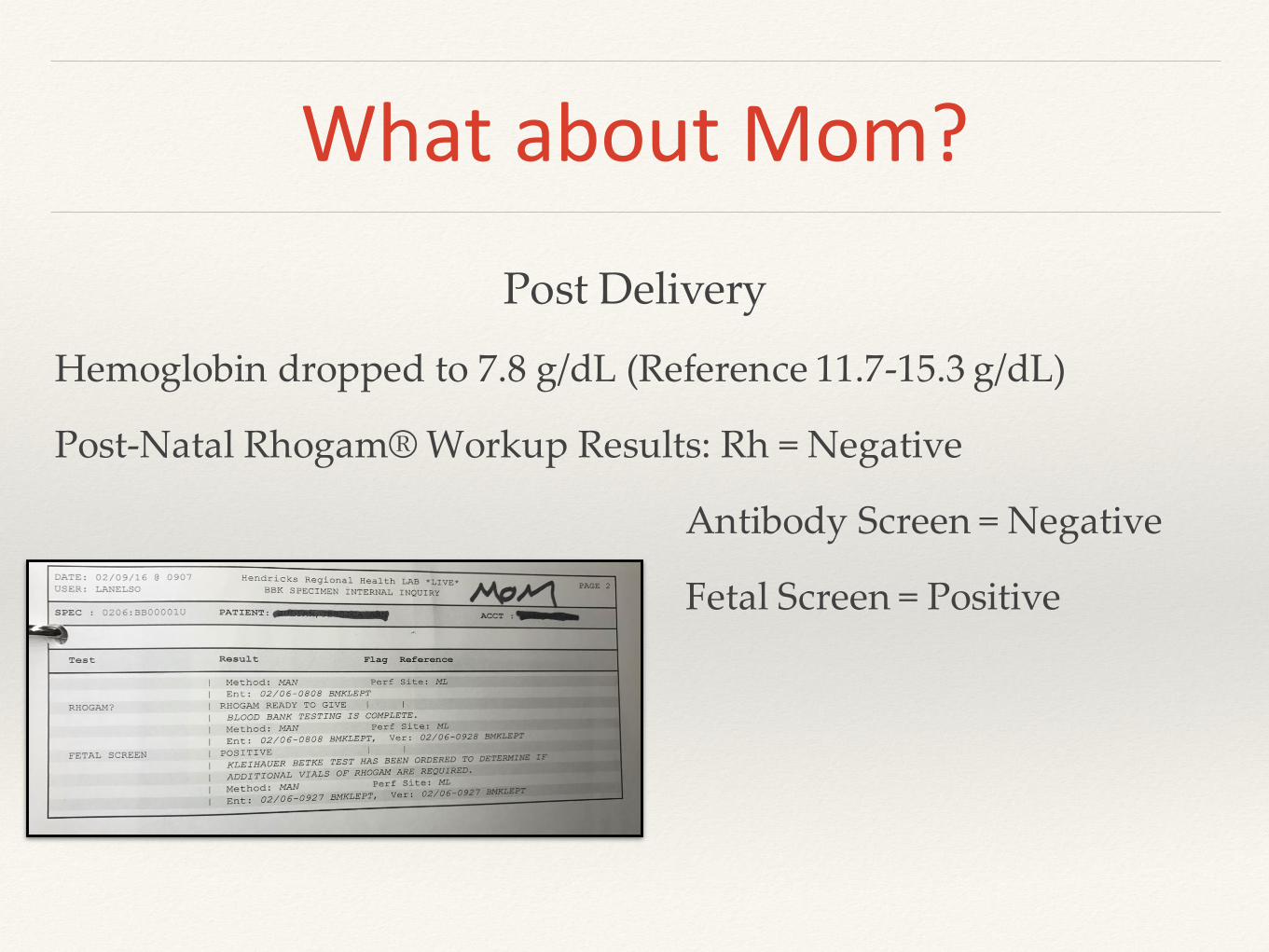
Post Delivery
Hemoglobin dropped to 7.8 g/dL (Reference 11.7-15.3 g/dL)
Post-Natal Rhogam® Workup Results: Rh = Negative
Antibody Screen = Negative
Fetal Screen = Positive

Fetal Screen
A Fetal Screen is performed on all Rh Negative mothers at Hendricks Regional Health.
Hemolytic disease of the newborn resulting from maternal sensitization to the Rh (D) antigen on fetal red cells can be prevented by use of Rh immune globulin (Rhogam®) within 72 hours of delivery of an Rh positive infant. When the fetal blood volume that enters maternal circulation exceeds 30 mL, more than one vial of Rhogam® will need to be administered.

http://www.rhogam.com/images/content/Teaching-Chart-Large.jpg
The Rhogam® brand is used at Hendricks Regional Health.
Mother’s Fetal Screen
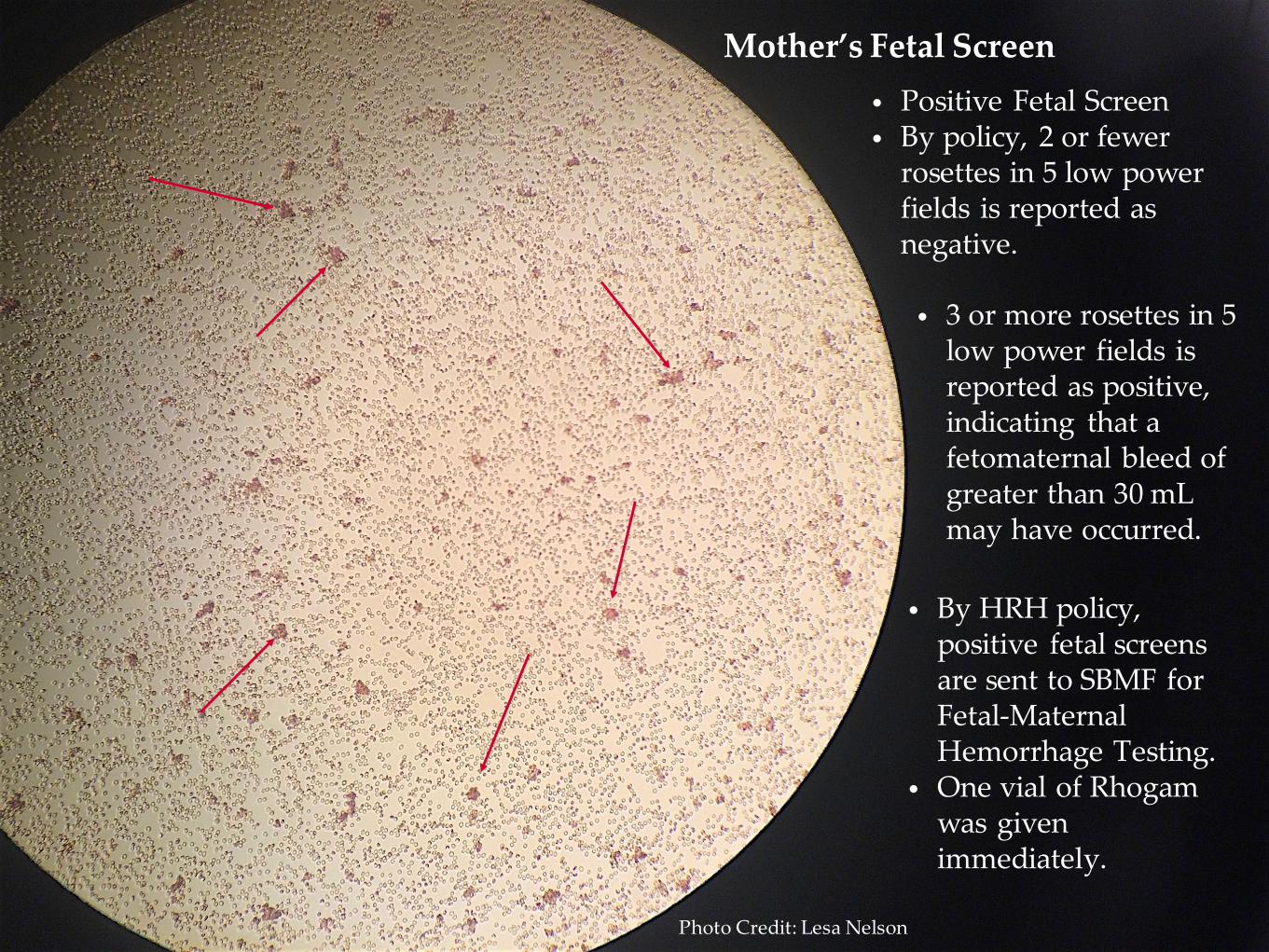
• Positive Fetal Screen• By policy, 2 or fewer
rosettes in 5 low power fields is reported as negative.
• 3 or more rosettes in 5 low power fields is reported as positive, indicating that a fetomaternal bleed of greater than 30 mL may have occurred.
• By HRH policy, positive fetal screens are sent to SBMF for Fetal-Maternal Hemorrhage Testing.
• One vial of Rhogam was given immediately.
Photo Credit: Lesa Nelson
Fetomaternal Hemorrhage Testing
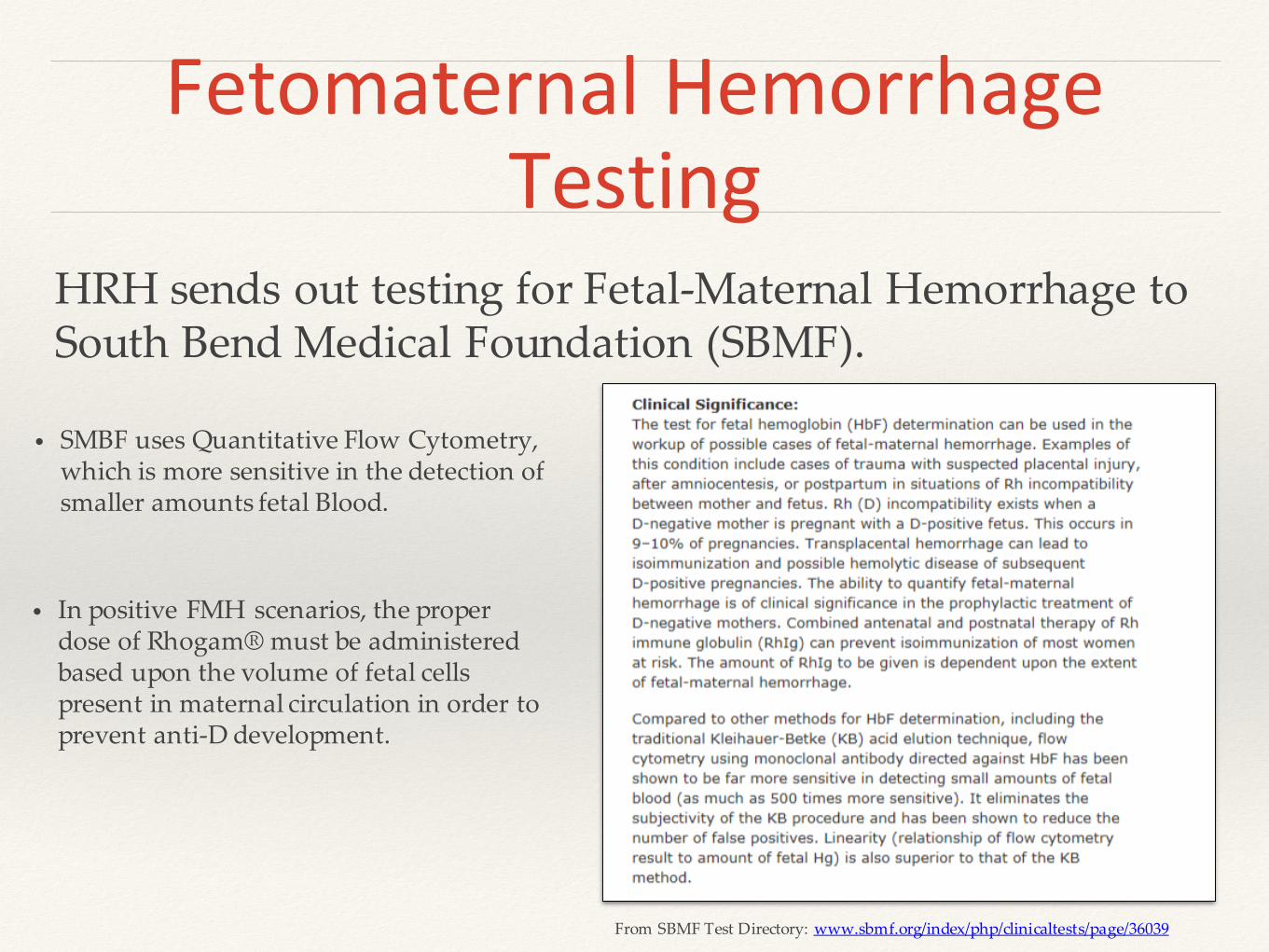
HRH sends out testing for Fetal-Maternal Hemorrhage to South Bend Medical Foundation (SBMF).
• SMBF uses Quantitative Flow Cytometry, which is more sensitive in the detection of smaller amounts fetal Blood.
• In positive FMH scenarios, the proper dose of Rhogam® must be administered based upon the volume of fetal cells present in maternal circulation in order to prevent anti-D development.
From SBMF Test Directory: www.sbmf.org/index/php/clinicaltests/page/36039

Fetal-Maternal HemorrhageTest Result
371 mL is a significant fetal maternal bleed.

• A 2 volume neonate exchange = 500 mL
• The expected blood volume of this approximately 7 pound infant is 42mL/pound, or about 294 mL.
• The typical volume of one unit of packed red cells.
• Mom needs 13 doses/vials/injections of Rhogam® ???!!!
www.clipartfest.com
Perspective…

Rhophylac®
to the
Rescue
About Rhophylac®
• Administered intravenously as outpatient. Obtained from neighboring hospital…not stocked at Hendricks Regional Health.
• 1 - 300 mcg Rhophylac® will suppress < 15 mL of Rh positive red cells.
• The Fetal Bleed, indicating whole blood in this case was 371 mL. One dose of Rhogam was administered postpartum, which covers 30 mL of fetal whole blood.
• 341 mL of fetal blood would need to be considered when calculating Rhophylac® dosage. Based upon the dosing information, one dose plus 20 mcg/ml of red cells would need to be administered intravenously.
• Calculated dosage = 11.37 vials, rounded to the next whole vial = 12 vials or 3600 mcg
• The equivalent of 13 vials was administered to this patient. (3900 mcg + initial 300 mcg dose = 4200 mcg total)
• The dose was received at the tail end of the 72 hour period.
• Information and table from: http://www.rhophylac.com/Product-Information-Administration-Guide.aspx
Fetomaternal Hemorrhage
• A fetomaternal hemorrhage is the passage of fetal blood across the
placenta into maternal circulation.
• According to UpToDate, “No universally accepted threshold defines
the volume of fetal erythrocytes in maternal circulation that
constitutes a massive fetomaternal hemorrhage”. (A wide range of
10-150 mL volumes have been proposed.)
• Pathogenesis is unclear, but the following have been found to increase
the likelihood that fetal cells would be found in maternal circulation:
❖ Parenchymal and retroplacental hemorrhage
❖ Intervillous thrombi
❖ Infarction
FMH Incidence
FMH <20-30 mL in 1 in 200-300 live births
FMH >80 mL in 1 in 1000 live births
FMH >150 mL in 1 in 5000 deliveries
Statistics from Moise, Kenneth, MD, Massive fetomaternal hemorrhage, UpToDate, Topic 6806, version 6.0, January 2016
Risk Factors for FMH
Multiple Gestation
Nuchal Cord (wrapped around fetal neck)
Low Birth Weight
What can cause a FMH?
Trauma:
MVA, Fall, Amniocentesis
Spontaneous:
Cause can typically not be determined
This case
Silent Fetal-Maternal Hemorrhage• No risk factors
• No indication until decreased fetal movement noticed
• Fetomaternal bleed not suspected until time of or after delivery
• No pathology requested on the placenta
Significant Bleed
• 371 ml represents the amount of fetal blood present in mother’s circulation at the time
This case
Chronic• Large amount of fetal cells in maternal circulation.
• Slide shows compensation, high reticulocytes, nucleated red cells,
anisocytosis, macrocytosis, polychromasia
• Tachycardia, normal blood pressure, poor perfusion, pale, weak
• According to Sebring, “neonatal anemia likely from a bleed 1-2 or more days prior to delivery is based upon the presence of RBC precursors and elevated reticulocyte count”. (Sebring ES1, Polesky HF., Fetomaternal
hemorrhage: incidence, risk factors, time of occurrence, and clinical effects, Transfusion. 1990 May;30(4):344-57.)
Patient Outcome - Mom
Received IV Rhophylac® and was discharged without complications.
Discharge instructions were to have antibody screen performed 6 months post delivery to monitor potential
development of anti-D, but she has not had testing performed at this institution since February 2016.
Patient Outcome - Baby
Discharge instructions included monitoring for brain injury as a result of hypoxia and acidosis.
Patient was seen in 11/2016 for a wellness visit. He is developing normally and shows no neurological or
physical deficits.
References
Rhogam® Website, http://www.rhogam.com/rhogam-dosing.
Rhophylac® Website http://www.rhophylac.com.
South Bend Medical Foundation Website, Test Directory, www.sbmf.org.
News report on infant with hemorrhage, http://www.dailymail.co.uk/news/article-2552508/Ghost-baby-suffered-rare-condition-meant-blood-drained-body-survives-receiving-transfusion.html
Ahmed, Masood, and Mohammad Abdullatif. “Fetomaternal Transfusion as a Cause Of Severe Fetal Anemia Causing Early Neonatal Death: A Case Report.” Oman Medical Journal 26.6 (2011): 444–446. PMC. Web. 5 Nov. 2016.
Stroustrup, Annemarie, Callie Plafkin, and David A. Savitz. "Impact of Physician Awareness on Diagnosis of Fetomaternal Hemorrhage." Neonatology 105.4 (2014): 250-5. ProQuest. Web. 5 Nov. 2016.
Amir Sweha, M.D., and Trevor W. Hacker, M.D., Mercy Healthcare Sacramento, Sacramento, California, Jim Nuovo, M.D., University of California Davis, School of Medicine, Davis, California, Interpretation of the Electronic Fetal Heart Rate during Labor, Am Fam Physician. 1999 May 1;59(9):2487-2500.
Sam Pourbabak, Chad R. Rund, Kendall P. Crookston, Three Cases of Massive Fetomaternal Hemorrhage Presenting Without Clinical Suspicion, Archives of Pathology & Laboratory Medicine, vol. 128 number 4, pp. 463-465, 2004.
Alexis R. Peedin, Marshall A. Mazepa, Yara A. Park, Eric T. Weimer, John L. Schmitz, Jay S. Raval, Two cases of asymptomatic massive fetomaternal hemorrhage, Volume 52, Issue 2, April 2015, Pages 208–210 Transfusion and Apheresis Science
Harris, J.L. et al., Mechanisms of late decelerations of the fetal heart rate during hypoxia, American Journal of Obstetrics & Gynecology , Volume 144 , Issue 5 , 491 - 496
Moise, Kenneth, MD, Massive fetomaternal hemorrhage, UpToDate, Topic 6806, version 6.0, January 2016.
Sebring ES1, Polesky HF., Fetomaternal hemorrhage: incidence, risk factors, time of occurrence, and clinical effects, Transfusion. 1990 May;30(4):344-57.

Acknowledgements
Lynn Devich and Dave Petrous, IRB Approval
Many thanks to T. Anthony Giaquinta, MD, HRH Pediatric Hospitalist for guidance.
Robert P. Hooker, MD, HRH Pathologist
Edward Wills, MD, HRH Pathologist
Westside Physicians for Women
Photo Credit: Hendricks Regional Health Marketing Dept.

Questions?





























