Embed Size (px)
DESCRIPTION
Citation preview
INDIGENOUS DEMENTIA
PROJECT REPORT
FUNDED BY
December 2002

Dear Reader,
Indigenous Dementia Project
The Indigenous Dementia Project highlighted the research conducted in the Northern Territory on issues surrounding dementia. The project identified unmet needs, service gaps and issues in the Northern Territory for Indigenous peoples living with dementia, their families and carers. The main thrust of the consultant’s report shows that there are many barriers to overcome if dementia is to be given a higher priority among the many health issues pressing upon Indigenous communities. The long list of negatives in the report relating to service delivery and geography is not in doubt. Importantly a number of strategies have been identified as a positive approach, in promoting a better understanding of dementia among Indigenous communities, as well as improve service delivery. 1. Awareness – It was acknowledged by Alzheimer’s Australia that unless community awareness
was raised, the returns from training and other initiatives were likely to be that much lower. 2. Assessment Tool - There is a recognised need for a simple assessment tool that can be used
by relatively unskilled workers to recognise dementia in communities. At a national level, Alzheimer’s Australia is looking at ways of generating interest through one of the universities, in the development of an assessment tool. One option is to look at the tool based on work of by Dr Martin Prince, ADI, London.
3. Education - There was considerable scope for education and training initiatives. These
initiatives need to have an emphasis on Health and Community Care workers as well as Aboriginal health workers.
4. Representation – Alzheimer’s Australia to be represented at key Indigenous aged care and
mental health conferences during 2003/2004. These conferences will be a good opportunity to network with Indigenous service providers, improve understanding of Indigenous issues, and improve marketing of the work of Alzheimer’s Australia.
For further information contact Marianne Fitch Executive Director Alzheimer’s Australia NT on 89485228. To obtain a copy of The Indigenous Dementia Report please go to www.alzheimers.org.au go to NT on map of Australia.
Alzheimer’s Australia NT Unit 1, 18 Bauhinia Street Telephone 08 8948 5228 Dementia HelplineNightcliff NT 0810 Facsimile 08 8948 5229 1800 639 331 PO Box 515 Email [email protected] The Alzheimer’s Association Nightcliff NT 0814 of the Northern Territory Inc ABN 34 030 043 531
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 i
INDEX
PAGE
Executive Summary
1
1.0 Background 3 1.1 Objectives of the project 1.2 Requirements for stage one 2.0 Project Management 5 2.1 Project management 2.2 Project model 3.0 Unmet needs, service gaps and issues 9 3.1 Summary of data gathered 3.2 Diagnosis, assessment and management 3.3 Respite and residential care 3.4 Education, training and availability of information 3.5 Families and carers 3.6 People living with dementia 3.7 Culture and language 3.8 Service standards and standards of care 3.9 Models for service delivery 4.0 Indigenous Dementia data 18 4.1 Availability of data 4.2 General Northern Territory data 4.3 Dementia data 5.0 NT Indigenous Dementia Workshop 22 5.1 Workshop participants 5.2 Workshop issues 5.3 Workshop structure 5.4 Summary of workshop discussions 5.4.1 Diagnosis, assessment and early intervention/treatment 5.4.2 Families and carers 5.4.3 Funding of facilities and services 5.4.4 Respite care and residential care 5.4.5 Information, education and training 5.4.6 People living with dementia 6.0 Indigenous specific Dementia initiatives developed
around Australia 29
6.1 Better Medication Management by Aboriginal People with Mental Health Disorders Such As Dementia and Alcohol Related Brain Injury, Their Carers and Other Family Members: A Collaborative Project
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 ii
6.2 Department of Ageing, Disability and Home Care - Achievements under the NSW Action Plan on Dementia 1996–2001
6.3 Dementia training for Indigenous communities 7.0 Barriers to and strategies for convening a National Rural
and Remote Indigenous Dementia Forum 31
7.1 Barriers 7.2 Strategies to overcome barriers Attachments 34 A Reference List B Key Stakeholders, resources, expertise and support services C Sample Questionnaire D List of Abbreviations E Organisations Represented at the Darwin Workshop F Workshop issues G Conferences H Aged Care Planning data
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 1
Executive Summary This project is stage one of a two stage project. Stage one has been developed and scoped by Alzheimer’s Australia NT. Alzheimer’s Australia NT, the NT Department of Health and Community Services and the Commonwealth Department of Health and Ageing, jointly funded Stage One. Stage Two of the project is the proposed convening of a National Rural and Remote Indigenous Dementia Forum. The project was undertaken over approximately five months from the end of June 2002 to end of November 2002. The project involved the following key tasks: • Literature review • Identification of key stakeholders • Development and administration of a questionnaire • Interviews with service providers • NT Dementia Workshop • Identification of Indigenous dementia project or initiatives around Australia • Data collection and analysis • Report writing. The project identified unmet needs, service gaps and issues in the NT for Indigenous peoples living with dementia, their families and carers in relation to the following areas: • Diagnosis, assessment, early intervention/treatment and management
including the need for an assessment tool appropriate for languages and levels of education prevalent within Indigenous communities, role of interpreters and lack of access to medical specialists and Indigenous specific services.
• Respite and residential care including lack of options for and availability of services and facilities, lack of adequacy of facilities and services for Indigenous peoples particularly in relation to remote Indigenous communities.
• Education, training and availability of information across the gamut of areas from community awareness to helping people living with dementia.
• Families and carers including acknowledgment of the hard work of family carers, the poor quality of care being provided to some individuals, the need to provide support and respite and the lack of availability of suitable, trained, willing and reliable Indigenous carers.
• People living with dementia including the low rate of diagnosis of Indigenous dementia, the vulnerability of people, the need for aged care to be a higher profile issue within Indigenous communities and the need for tailored services / individual care planning.
• Indigenous culture and language including the complexities associated with cross-cultural service delivery, a perceived high level of tolerance,
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 2
acceptance and coping with dementia within Indigenous communities. • Service standards and standards of care including the adequacy of existing
services and the need for minimum standards of care to be enforced to safeguard the person and their health.
• Models for service delivery including issues to be taken into account in developing services.
• Funding of facilities and services including the difficulties associated with current discrete sources of funding for aged care, lack of flexibility and perceptions that funding of infrastructure gets priority.
The project failed to identify a source of data on dementia that presented a comprehensive view of the manner in which Indigenous communities and individuals are affected by the disorder and was forced to conclude that no such data is in existence. A range of data from different sources was brought together to sculpt a picture of Indigenous dementia in the Northern Territory. The project identified several other Indigenous dementia initiatives developed or in progress elsewhere in Australia. Barriers to convening a National Rural and Remote Indigenous Dementia Forum were identified as being: • Priorities of other health areas • Lack of funds for community based organisations • Lack of statistical data and research • Competing priorities for potential participants (other meetings / conferences) • Dementia not seen as a priority issue within remote communities • Small number of people diagnosed with dementia • Priorities of Aboriginal Medical Services and Health Boards. Combining with another relevant conference or forum was identified as the most effective strategy for overcoming the identified barriers. Organisations and groups that could be represented on a National Steering Committee for the development of a National forum were identified. (Provided to Alzheimer’s Australia NT under separate cover.)
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 3
1. Background 1.1 Objectives of the Project The objectives of the project as they appeared in the Consultants Brief were: • To develop an understanding of existing Dementia issues within Indigenous
communities including early identification of dementia, levels of assistance and types of service delivery.
• To identify unmet needs for indigenous people living with dementia, their families and carers.
• To identify service gaps for Indigenous people living with dementia, their families and carers.
• To outline training and service delivery requirements to address these issues.
1.2 Requirements for Stage One The requirements for stage one of the project are from the Consultants brief.
1.2.1 Stage One Undertake a mapping exercise of the Northern Territory (NT) urban, rural and remote Indigenous communities, Indigenous health and aged care organisations and other health and aged care organisations to: • Identify current key stakeholders, resources, expertise and support
services already available in the NT for Indigenous people living with dementia, their families and carers.
• Gather information about unmet needs, service gaps and issues in the NT, these will form the basis for discussion at an Indigenous Dementia Workshop.
• Identify key people, stakeholders and organisations, in the NT willing to participate in the workshop.
• Identify other Indigenous dementia initiatives that have been developed around Australia.
• Identify potential barriers both financial and structural to the successful convening of a National Rural and Remote Indigenous Dementia Forum and provide strategies to address such barriers.
• Identify key people Nationally to participate in the Steering Committee for the development of a National Rural and Remote Indigenous Dementia Forum.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 4
1.2.2 Northern Territory Workshop • Following the mapping exercise that a workshop be organised for
interested parties to address findings for the Northern Territory. • Identify generic issues that could be addressed at a National Rural
and Remote Indigenous Dementia Forum.
1.2.3 Key Outcome Stage One report will: • Identify key stakeholders, resources, expertise and support services
already available in the NT for Indigenous people living with dementia, their families and carers.
• Identify key people, stakeholders and organisations, in the NT willing to participate in the workshop.
• Provide a summary of the proceedings and recommendations of the NT Workshop.
• Produce a model of the mapping exercise for future resource. • Identify other Indigenous dementia projects or initiatives that have
been developed around Australia. • Provide recommendations in regards to the holding of the National
Rural and Remote Indigenous Dementia Forum. • Document potential barriers both financial and structural to the
successful convening of a National Rural and Remote Indigenous Dementia Forum and provide strategies to address such barriers.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 5
2. Project Management 2.1 Project Management Project management was the responsibility of Alzheimer’s Australia NT who established a Steering Committee comprising of representatives from Alzheimer’s Associations, Indigenous health organisations, Commonwealth Department of Health and Ageing and the NT Department of Health and Community Services. The role and responsibilities of the Steering Committee were to: • Review the draft consultants brief for the Indigenous Dementia Project. • Nominate a smaller tender selection committee to evaluate tenders. • Meet with the consultant at the completion of Stage One to receive the report
and recommendations. • Make recommendations to the Alzheimer’s Australia NT regarding Stage
Two of the project. 2.2 Project Model
2.2.1 Sources of data The project model was designed to incorporate as many sources for data collection as would be permitted by the budget and in the timeframe allowed for the project. Sources for data collection are shown in an overview of the model below. A possible source for data collection that could not be fully researched was direct contact with people living with dementia and their families. The intention was to use the various sources of data for two main purposes, namely to piece together a picture of Indigenous dementia issues and to enhance the validity of each source by reference to others.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 6
2.2.2 Literature Review The literature review was aimed at identifying any similar work undertaken within the Northern Territory or interstate in particular focusing on sources that might directly contribute to the outcomes of the project. Sources were located principally through Internet searching. Attachment A lists relevant sources of information on Indigenous health and dementia. Several of the sources listed contain extensive bibliographies of other works also potentially relevant.
2.2.3 Statistical data
Statistical data, both published and unpublished were sources by the Consultants. Data is outlined in section 4.3 of this report. This data was to provide a quantitative perspective of dementia within Indigenous communities.
2.2.4 Survey
Key stakeholders were identified from a broad range of NT based organisations likely to be directly involved in the care, support or management of Indigenous people living with dementia, their families or carers or in the delivery of services within Indigenous communities. This identification relied in the first instance on existing contacts, networks and local knowledge of the Consultants including Aged Care Assessment Teams (ACAT), Residential Aged Care facilities, Community Aged Care Package (CACP) and Home &Community Care (HACC) providers, Respite Care Providers, Aboriginal Medical Services, Training Providers and funding bodies and policy makers. (See Attachment B) A questionnaire was developed to survey these stakeholders. Alzheimer’s Australia NT was consulted regarding the development and finalisation of the questionnaire. (See Attachment C) The questionnaire was then forwarded to stakeholders. In addition to surveying stakeholders, stakeholders were requested to ‘on-forward’ the questionnaire to other organisations of relevance to the project. Questionnaires were also distributed using a range of email lists available by subscription. The intention was to achieve the wide distribution of the questionnaire to potentially relevant organisations. Stakeholders are listed in Attachment B.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 7
2.2.5 Interviews
Following identification of key stakeholders as above, face-to-face interviews were conducted with a range of urban, rural and remote service providers. Interviews continued throughout the life of the project as time and resources permitted. The Consultants were able to contain project costs for some interviews with regional and remote service providers by combining interviews with visits to these providers for other purposes. Interviews in most locations were scheduled through direct contact with the providers. In some cases contact had to be made through an intermediary, eg. Town Clerk. In many cases arrangements were successful however in a handful of cases providers did not attend as arranged and this caused delays and rework for the Consultants. Based on the previous experience of the Consultants delays and rework of this nature can be expected for most projects due to providers having other priorities and in particular deaths in Indigenous communities (contact with communities can be severed for days following a death and a series of deaths can cause delays of up to months). Interviews were conducted using the structure of the survey questionnaire as a guide. Interviewees were encouraged to freely contribute their views, opinions and ideas.
2.2.6 Workshop Interest in attending an Indigenous dementia workshop was canvassed in interviews and the survey questionnaire. Where possible, interested people were contacted to assess a suitable date for the workshop that would meet the project timeframes. Invitations to the workshop were sent to all people who expressed interest in attendance and to a range of other organisations and individuals. Prior to the workshop some initial analysis of returned survey questionnaires was undertaken to identify issues that may form the basis for discussions in the workshop. These issues were submitted to Alzheimer’s Australia NT in the progress report. (See Attachment F) The workshop, held in Darwin, served the purpose of discussing and validating data collection to that point. Participants were divided into two groups. Each group was given a list of workshop issues and asked to discuss these issues with a view to identifying unmet needs and service gaps and providing additional information to refute or validate the issues.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 8
Each group recorded views and presented an oral report. A summary of proceedings from the workshop is presented as section 5 of this report.
2.2.7 Progress reporting The model included an open communication aspect enabling the Consultants and designated Alzheimer’s Australia NT representatives to seek an oral report on progress or raise queries about the project at all times. The Consultants also provided a formal written progress report and briefing during the course of the project (Friday 4 October) for designated Alzheimer’s Australia NT representatives.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 9
3. Unmet needs, service gaps and issues 3.1 Summary of Data gathered A total of 36 responses were obtained from organisations and individuals. Of the total responses:
• 19 completed questionnaires • 17 participated in interviews • 4 completed questionnaires and participated in interviews.
3.2 Diagnosis, assessment and management Of the total responses 58% of organisations (21) raised issues related to diagnosis, assessment and management of people living with dementia. An overwhelming number of these responses (81%) related to the lack of an assessment tool appropriate for Indigenous peoples and / or lack of access to appropriate assessment. Respondents expressed a range of views including: • Need for a suitable mini-mental assessment tool. • Need for a tool specifically designed for remote areas. • Assessment needs to include involvement of care recipients, family, health
workers and friends and needs to be conducted in the person’s community. • Lack of a tool that allows for differences in language, culture and education. Difficulties associated with development of a diagnosis and assessment tool that would be universally appropriate for all Indigenous peoples were acknowledged. Difficulties include: • Variation between urban and remote people. • Diversity of remote Indigenous peoples. • Low level of literacy of many Indigenous people. • Variation in daily living activities between urban and remote communities. In this context there was some support for development of a diagnosis and assessment model broadly based on gathering a history of the functional ability of a person and their background, including their routines, usual living standards, family history, community associations, likes, dislikes, functions they can no longer perform, etc. Such a model would rely on regular profiling of the person starting from age 45. The model would emphasise the use of a tool appropriate for the person’s level of education and whether there is a language in common to enable communication between interested parties. Health Clinics and HACC services were mentioned as a potentially valuable source for this information over a period of time. The cost of implementing such a tool needs to be a factor in design. A range of views was also expressed in relation to the use of interpreters in the diagnosis and assessment processes. Several respondents mentioned the expense associated with accessing interpreters and lack of reliability, availability
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 10
or ease of access to interpreters when needed. This was seen as limiting the use and appropriateness of current tools. The need for interpreters to provide an indication of the person’s ability to communicate in their preferred language was also mentioned. Although language can cause difficulties with assessment, the overall quality of assessment was not necessarily dependent on the involvement of interpreters as it was viewed as being vested in the development of rapport between the person of concern, their carers and the person conducting the assessment. Respondents viewed diagnosis and assessment as providing the information required for development of appropriate management or rehabilitative programs. Development of a management program is needed to commence the care process, help ensure a better quality of life for the person and their family carers and help define the need for other associated aged care workers. In particular if early diagnosis occurs, the person may still benefit from implementation of patterning behaviours before it is too late. Early detection of the disease would also enable existing patterns of behaviour to be monitored and documented to assist with formulation of care and management plans. Major management needs for dementia patients were described as: • Medication – prescribed medicines taken in accordance with correct routines • Incontinence programs • Insomnia • Wandering. Several factors were seen as influencing lack of early diagnosis, assessment and intervention including: • People who may have symptoms, such as memory loss, are not viewed as
‘sick’. • Diagnosis of other acute and chronic diseases takes priority. • Lack of a reliable basic level of health care in some communities. • Tolerance of changes in behaviour within Indigenous communities. • Aged care issues are not a priority. Lack of access to medical specialists or specialist support was consistently raised as an issue in terms of assessment and management of people living with dementia including lack of: • Specific Indigenous dementia services and dementia specific nurses. • Understanding and support by doctors especially of the need to refer to
respite. • Assessment by a specialist or through specialist services. • Professional support available through geriatric services, psycho-geriatrician,
geriatricians and gerontologists. • Neuropsychological testing or neuropsychiatric services. • Regular specialist review.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 11
3.3 Respite and residential care Fifty-eight percent (21) respondents raised issues related to respite or residential care, the main body of comments directed towards the lack of availability of services and facilities, lack of adequacy of facilities for Indigenous peoples and lack of support within homes and communities. Respondents consistently mentioned lack of availability of services and facilities particularly in relation to remote Indigenous communities. There was some support for an Indigenous specific facility in Darwin and broad support for respite within homes and communities for people living with dementia and their family carers. Comments included: • Lack of respite care and day centres • Nothing available in remote areas (East Arnhem and Port Keats were
specifically mentioned) • Current services not accessible to remote people • Need for purpose built and appropriately staffed facilities to care for
community members in their own home or in a communal or residential setting
• Need for Centre based respite within remote communities that people with dementia can attend thereby supporting family carers and contributing to the maintenance of care situations
• Need services that can accommodate sleepovers and providing assistance in the family home.
• Centre based day activity programs are needed in every community. • Services and facilities are available in Darwin but this sometimes causes
confusion and other difficulties for clients • Need for day care – diversional therapy and therapeutic activities • Emphasis on nursing home places rather than respite • Lack of residential and respite facilities and services appropriate for younger
people living with dementia. Several respondents specifically mentioned a lack of emergency respite / care. Often respite is being used as a last option when the family can’t cope. In addition emergency needs cannot always be accommodated by existing respite services. Several respondents indicated the need for Indigenous specific services and facilities: • Lack of activities appropriate for Indigenous peoples – eg. fishing • Lack of access to Indigenous foods (food is seen as an important part of
culture) • Capacity for Indigenous people to access structured respite is hampered by
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 12
lifestyle where other issues take priority • Indigenous people do not access mainstream day care facilities • Lack of culturally appropriate support services, care and facilities • Interpreters are not well used for residents or families • Need for Indigenous volunteers and paid carers prepared to visit regularly,
cook or do activities with people. Views supported Indigenous people being able to stay on their community. Engaging reliable and appropriate carers on communities was seen as the main barrier to this occurring. Where staying on their community was not possible a range of supportive alternatives were expressed including: • Community contact visits – visits from residential care to families,
communities and homelands. • Groups from communities being brought into town to visit people. • Recorded community events being sent in to people to enable them to
maintain their connection. Other issues related to respite or residential care included: • People are not aware of or are unwilling to pay fees for care. • People often present for care with little if any personal information so paid
carers know little about the person being cared for in terms of their family history, usual behaviours, likes/dislikes, routines, friends, etc.
• Families should be involved in a settling-in process to assist staff to understand the needs of the person.
• People should be encouraged to bring things from their home such as photos, paintings, songs on tape, videos in their own language, etc.
• Where appropriate, Aboriginal Liaison positions and workers in residential aged care facilities.
• Need for paid Indigenous carers. 3.4 Education, training and availability of information Sixty-seven percent of respondents (24) expressed views on the need for ongoing and supported education, training and information. Views ranged from the need to broaden community awareness of dementia to practical education, training and information on what can be done to help people living with dementia. Specific target groups included the following: • Staff of aged care facilities • Program staff on communities • Families and friends • Nurses • GPs
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 13
• Hospital staff • Health staff • Aboriginal health workers • Carers (paid and unpaid). Core areas of focus for education, training and information included: • Symptoms – what to look for • Dementia – what it is, stages and what to expect • Caring for a person with dementia • Challenging behaviours – advice and management • Guardianship and related issues • Services and resources available for people living with dementia, their
families and carers, how to use services and how to get access to support. Some respondents expressed the view that factual information should be presented while others emphasised using appropriate language and in a culturally appropriate manner. The related issue of Indigenous concepts and current level of understanding was raised. These issues were raised in the context of providing education, training and information on the subject (for paid and family carers) as well as in the context of a lack of understanding of Dementia. There is a need to ensure a better understanding of Dementia as well as development of relevant material that takes into consideration language and cultural issues. The need for staff of residential facilities to have cultural awareness training was also identified. This training does present some difficulties for service providers in terms of the cost of training and also staff turnover, which requires commitment to continuously investing in training as new staff commence. Several respondents commented on models for education and training including: • Classroom models are not effective due to low literacy levels. • One-to-one training by modelling is effective. • Sharing of skills and knowledge in communities. • Training placements with service providers. • Development of videos, booklets, training aids and material suitable to be
used using the Broadcasting for Remote Aboriginal Communities Scheme (BRACS).
3.5 Families and carers Of the total responses, 58% of organisations (21) raised issues relating to families and carers, either paid or unpaid. Respondents variously reported that most clients had good family networks or that sometimes there is a lack of family support for people. The hard work of family carers however was broadly acknowledged as well as the need to provide
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 14
support and respite to family carers. Issues relating to families and carers included: • Most carers are already caring for another person(s). • Family carers don’t access services for support. • Family carers don’t speak up for fear of losing services. • People living with alcohol related dementia are often more difficult to care for
and are frequently angry. • Paid carers need to understand culture, be caring, patient and have a sense
of humour. The lack of availability of suitable, trained, willing and reliable Indigenous paid carers was identified as well as the lack of continuity of paid carers. This was the case in urban and remote areas. One respondent expressed a view that there may be personal consequences resulting from a person with dementia dying and that this may be acting as a disincentive for Indigenous people to become carers. Some respondents noted incidences where Indigenous people had tended to be less aggressive with non-Indigenous staff. In addition to the resources and supports described elsewhere in this report, types of services and supports needed for families and carers were described as follows: • Community based • One-to-one • Person focused individualised help • 24 hours support • Help for families to visit relatives in town • Culturally relevant support • Access to comprehensive HACC programs to assist with daily living tasks • Assistance with providing a safe environment. 3.6 People living with dementia Early death, high morbidity rates and other chronic diseases were seen as contributing to a low rate of diagnosis of dementia in Indigenous peoples. In addition the contribution of alcohol and / or substance abuse (eg. petrol sniffing) as a leading cause of Indigenous dementia was commented on. Comments included: • Aboriginal people die younger and therefore there is less dementia. • Most dementia is alcohol related (some people as young as 20). • The person does not usually survive to be an older person due to the onset
of other chronic diseases including renal conditions and diabetes. • Early morbidity limits the number of Indigenous people with dementia to a
small percentage, as they do not attain the age for onset of the disease. • For an Aboriginal person there can be several contributing factors to the

© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 15
dementia including diabetes, past substance abuse, stroke, and head injury. • Other chronic diseases overpower or mask the dementia especially in the
early stages. • The highest incidence of causes of Dementia in Aboriginal communities is
alcohol related brain damage and vascular dementia. Comments on the vulnerability of people living with dementia included that: • They suffer from financial abuse from relatives and family carers. • They need assistance to ensure that homes are adequate and safe. • Financial abuse and other factors may prevent the person getting assistance
from hostel care at an early stage of the condition. • Unless people living with dementia are assisted with money management
they are often without money for food. • There are instances of where the family carer will not allow the person with
dementia to leave the community because their carers pension will cease and the money will no longer be available to the family.
• Respect and time is not afforded to the old people as it was in the past. • People need help to attend appointments including transport and sometimes
someone to go with them. • There are neglected old people and people with dementia on communities. Guardianship issues also received some mention in relation to: • who decides what is best for the client • who decides whether clients should remain in care or be returned to
communities. A prevailing view was that aged care is not a high priority issue and has a low profile in many Indigenous communities. 3.7 Culture and language Some respondents commented on the level of tolerance of Indigenous communities to behavioural changes caused by dementia. Comments centred on a perceived high level of tolerance and coping with dementia until challenging behaviours occur, someone is at risk or cultural protocols are broken. When this occurs people are usually referred away from the community. Examples cited included a person living with dementia who made a lot of noise, keeping the whole community awake at night, physical assault and a person who was inappropriately talking about cultural business such as talking men’s business in front of women. Tolerance was also attributed to cultural expectations that elderly people would not necessarily function at a high standard. Cultural norms tended to mean that unless the family identified a problem, changes to behaviour would be accepted and accommodated.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 16
Language and culture were less likely to be important in urban settings, where once a certain level of dementia was reached; the person’s Indigenous status was not the main issue. Other personal, lifestyle or health reasons were likely to influence whether a person accessed services. Language and cultural differences were cited as a major problem in diagnosis and assessment as discussed above. In terms of management of elderly Indigenous people living with dementia, paid carers need greater cultural awareness. For example, an insight into the types of activities in which an elderly Aboriginal person on a community might be involved on a day-to-day basis would assist with planning relevant activities in a day centre, respite or residential setting. Culturally specific care needs included the need to separate men’s and women’s health issues, food preferences as well as the need for relevant activities. Facilities that would accommodate the specific care needs of Indigenous people were mentioned for example, having an open fire.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 17
3.8 Service standards and standards of care Several respondents commented on standards of care of Indigenous people with dementia within their communities. In the main these comments related to the care of Indigenous people in remote areas however some also related to urban areas. There was a broad range of comments on dementia services, from services in Darwin being pretty good, services targeted for the remote areas being sadly lacking to their being no appropriate services in the NT. Many comments centred on the need for minimum standards of care to be enforced to safeguard the person and their health. In this context mention was made of the need for accountable, properly managed and functioning HACC and CACP services which are seen as a major factor in the level of care that is provided within Indigenous communities. When these services are working well they provide a necessary level of support for family carers, which in many cases allows the person living with dementia to stay on their community longer. However, lack of infrastructure and availability of paid carers within some communities makes ongoing support difficult. Remote services sometimes focus on meals only and don’t want to get into personal care. In addition when key people leave communities or go on leave services can fall down. In general terms there was support for the view that remote area Indigenous clients should be able to link into services available in the mainstream, without being taken out of their communities. Individual care planning was also raised. Groups don’t always work and there is some ‘stereotyping’ of dementia clients. Each person requires a care plan or management strategy and needs to be individually monitored. Services targeted towards meeting the needs of the person living with dementia as well as the family carers needs are necessary. Simple things can make a difference such as erecting a fence, fixing a gate or having firewood delivered, etc. 3.9 Models for service delivery Some respondents made brief comments on issues to be taken into account in developing models for service delivery including: • Services on communities depend very much upon individuals and the
continuity of people working on communities. • People on communities are dependant on on-to-one care as there are limited
group options. • Every community needs access to an aged care program and each program
needs access to a Community Services Officer to work alongside Indigenous staff for a period of time (2 – 5 years).
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 18
• Some collaboration between service providers may enable services to be
extended or established. • Many ‘urban’ Indigenous people access and manage well in mainstream
services. • One model doesn’t fit all. • Need for different services for remote and urban. • Care needs to be taken with issues such as the land from which services are
delivered and the groups or families expected to use the service. Funding of service delivery received some comment including that lack of finances is a major issue for all services and that aged care should be funded as one program. Separate and different funding for services such as CACP and HACC puts added pressure on services that sometimes struggle to provide care to people.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 19
4. Indigenous dementia data 4.1 Availability of data The project failed to identify a source of data on dementia that presented a comprehensive view of the manner in which Indigenous communities and individuals are affected by the disorder and was forced to conclude that no such data is in existence. Discussions with service providers and stakeholders suggest that this data is non-existent or that there is no direct information on the subject. A statement in The Health and Welfare of Territorians (THS, 2001) goes some way to confirming this conclusion:
“Understanding of mental health issues in the NT, as elsewhere in Australia, is impeded by the scarcity of information about the number of people with mental illnesses and the patterns of mental illness they suffer, as well as the numbers who seek help from general practitioners and use other community services. Better data collection systems are needed to assist in the planning of mental health service in the NT and enable Territorians to draw meaningful conclusions about their own mental health.”
4.2 General Northern Territory data Due to the lack of availability of comprehensive data, Alzheimer’s Australia NT directed that this report present available data that may help to sculpt a picture of the Northern Territory and Indigenous health generally by comparison with the rest of Australia. The Northern Territory ranges over 1.34 million square kilometres, occupying 17% of Australia’ coastline and total land mass. The land extends 1,610 kilometres, north to south and 934 kilometres east to west. (Northern Territory Population Strategy, Issues paper, 2002). As at June 2001, the estimated resident population of the NT was 200,000. Of this total, 104,300 were males and 95,700 females. The median age was 29.6, approximately 6 years less than the national median age. (Northern Territory Population Strategy, Issues paper, 2002). The estimated Indigenous population of the Northern Territory as at 30 June 2001 was 57,550, representing 28% of the total population of the NT. At a national level, Indigenous peoples represent 2.4% of the total Australian population. (Northern Territory Population Strategy, Issues paper, 2002). The majority of Aboriginal people live outside the NT’s urban centres. (The Health and Welfare of Territorians, 2001).
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 20
The Northern Territory is composed of 6 Local Government municipalities, 30 Community Government Councils, 28 Incorporated Association Councils and 1 Special Purpose Council (Jabiru). There are 709 Aboriginal communities in the Northern Territory. Of the total 59 are considered to be major communities of over 100 people, are self-governing and have facilities generally expected in a small town such as a school, health centre, store, etc. Another 36 communities are also self-governing but smaller in size ranging from 20 to 100 people. A further 39 communities of variable size are considered to be town camps situated within or adjacent to a major urban area. A startling 575 Aboriginal communities are considered to be small family out-stations of up to 20 people, in permanent or semi-permanent residences with a water supply and shelter. (Northern Territory Aboriginal Communities, NTG, 2001) For 2001, the proportion of the NT population aged 65 years and over is estimated to be 3.8%. Over the period to 2021 this proportion is expected to increase to 6-7%. (Northern Territory Population Strategy, Issues paper, 2002) In 1996, 3% of Indigenous people were aged 65 years and over compared with 12% of the total Australian population. By 2006, the proportion of people of this age in the total Australian population is expected to rise to 13%, while the proportion of Indigenous people of this age is projected to remain at the same level. The stable proportion of Indigenous people reflects both their higher fertility and lower life expectancy. (Australia’s Older Population: Past, Present and Future, June, 1999) In relation to mortality rates for Northern Territory residents, the ABS has projected that by 2021 the overall life expectancy at birth will be 74.7 years for males and 78.5 years for females. (Northern Territory Population Strategy, Issues paper, 2002) The ABS reports that in 2000 in overall terms, Indigenous Australians had death rates at least twice as high as the total population. The median age at death for Indigenous Australians was 53 years. This age is approximately 25 years less than the median age for all deaths (78 years). (Northern Territory Population Strategy, Issues paper, 2002) From Department of Health and Ageing Aged Care Planning Data (2002) it can be seen that, for planning purposes, a Northern Territory aged care target population of 8,473 has been identified (see Attachment H). Planning data is derived from ABS population projections for the year 2001 and the 1996 Census and includes data for people aged 70 years and above and Indigenous people aged 50 – 69 years. (Aged Care Planning Data, 2002) For the purposes of aged care planning, the Northern Territory is divided into five regions, Alice Springs, Barkly, Darwin, East Arnhem and Katherine. Of the aged

© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 21
care target population of the Northern Territory, the Darwin region has the largest proportion (52%), followed by Alice Springs (24%), Katherine (10.5%), East Arnhem (8.7%) and Barkly (5.7%). (Aged Care Planning Data, 2002) In 2001, a little more than half of the aged care target group live in the major urban centres of the NT (4,320). Of these Darwin has the largest proportion (66%), followed by Alice Springs (22%), Katherine (6.5%) and Tennant Creek (5.5%). Among the total urban aged population, one third are of Indigenous origin. (Aged Care Planning Data, 2002) More than half of the total aged care target population (8,473) is comprised of Indigenous peoples aged between 50 – 69 years (52.95%). The aged 70 and above component of the total target population is smaller (47.05%) and includes Indigenous and non-Indigenous persons. In this latter group the proportion of non-Indigenous people is higher than that of Indigenous people. (Aged Care Planning Data, 2002) Of the total aged care target population: • 35.94% are Indigenous people aged 50 – 69 years living in rural and remote
areas • 17.01% are Indigenous people aged 50 – 69 years living in urban centres • 33.99% are aged 70 years and above living in urban centres • 13.06% are aged 70 years and above living in rural and remote areas. (Aged Care Planning Data, 2002) 4.3 Dementia data In 1996 Alzheimer’s Association Australian published data in relation to the 10 leading causes of disease burden in older Australians. This data rates dementia as the third highest and fifth highest source of disease burden for women and men respectively. The projections are that by 2016 dementia will rise in the rankings for both groups, in particular women where it may escalate to the highest ranked source of disease burden. (Jorm, A., 2001) In relation to the Northern Territory only two sources of data were identified and the publication source for one of these, NT Dementia Rates, could not be located. Given that this data contains citations for the sources from which the data was derived it may be possible to duplicate the results as a method for verifying its validity or otherwise however it was not within the scope of this project to do so. According to NT Dementia Rates, in June 2000 there were approximately 317 people aged 65 years or older living with dementia. By 2024 this is expected to increase 263% to approximately 833.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 22
In the NT between 1993 and 1997, Aboriginal males were admitted to hospital for treatment of mental illness slightly more often than non-Aboriginal males. Comparative admission rate for Aboriginal and non-Aboriginal women show little difference. For the same period, 17 Aboriginal males and 19 Aboriginal females were admitted to hospital in the dementia category. This is compared to 33 male and 46 females for non-Aboriginal persons. (The Health and Welfare of Territorians, 2001). Of NT non-Aboriginal hospitalisations for mental illness in people aged 55 years and over between 1993 and 1997, 18% were for dementia. In this period 70% of people hospitalised for dementia in the NT were aged 75 years or over. (The Health and Welfare of Territorians, 2001). In the same period, for Aboriginal people, hospitalisation from dementia was much less common although the reasons for this are not clear. From 1993 to 1997 the NT hospitalisation rate for dementia in Aboriginal people was 50 per 100,000, less than half that in non-Aboriginal people. (The Health and Welfare of Territorians, 2001) From 1993 to 1997, dementia was the most common reason for hospitalisation for mental illness for Territorians aged over 55 years. For Aboriginal people it was ranked as the fourth highest reason for admission by principal diagnosis. (The Health and Welfare of Territorians, 2001). In November 1999 Department of Health and Community Services (then Territory Health Services) commenced collection of ACAT data as part of the Community Care Information System (CCIS). Department of Health and Community Services reports on ACAT data at 6 monthly intervals. ACAT data is Northern Territory wide. Department of Health and Community Services staff extracted dementia data from CCIS at the request of the Consultants. Data relates to clients with dementia as a primary diagnosis or existing medical condition. This data shows that, from November 1999 to 30 June 2001, ACAT managed 170 assessments for a total of 130 clients. Of the total of 130 clients, 43 were Aboriginal or Torres Strait Islanders. This same CCIS regional data for dementia in the NT shows that the highest concentrations of people living with dementia are in Darwin (87), followed by Alice Springs (28), Barkley region (7), East Arnhem (4) and Katherine (3). Data specific for Indigenous Dementia status was not available for this report. However given that the population profile of remote NT areas would be primarily Indigenous, it could be assumed that, for remote areas, most of the assessments would be for Indigenous clients. This assumption would be less valid for Darwin and Alice Springs.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 23
5. Indigenous Dementia Workshop 5.1 Workshop participants People interested in participating in a workshop to discuss Indigenous dementia issues were initially identified through interviews and returned questionnaires. Where possible, interested people were contacted to assess a suitable date for the workshop that would meet the project timeframes. Invitations to the workshop were sent to all people who expressed interest in attendance and to a range of other organisations and individuals. Fourteen people participated in the NT workshop. 5.2 Workshop issues Interview records, returned questionnaires and community visits were analysed to identify potential issues that might form the basis of discussions at the workshop. 5.3 Workshop structure Participants were divided into two groups. Groups were provided with the list of workshop issues and asked to discuss these issues with a view to identifying unmet needs and service gaps and providing additional information to refute or validate the issues. A scribe for each group was nominated to record the views of the group members. The workshop concluded with each group providing an oral report. 5.4 Summary of workshop discussions
5.4.1 Diagnosis, assessment and early intervention/treatment
Diagnosis of Indigenous people living with dementia was seen as complex due to a range of problems particularly: • Lack of an Indigenous specific assessment tool • Higher priority chronic or acute health problems • High level of tolerance for early behavioural changes • Language and cross-cultural issues. These complexities tend to lead to people of concern not being diagnosed until they are in the late stages of dementia.
The lack of an Indigenous specific assessment tool was acknowledged by all present. However the complexities with design of such a tool were also acknowledged in terms of the types of dementia disorders, number
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 24
and diversity of Indigenous languages (some no longer spoken), the generally low level of literacy of Indigenous people within many communities, and the extent of variation between Indigenous people living in urban communities and their rural and remote counterparts in terms of requirements for daily living.
The general poor state of health of some Indigenous people also contributes to the complexity of diagnosis of dementia, particularly in rural and remote Indigenous communities. This is due to a tendency by health professionals to focus on the chronic and acute health conditions being suffered by a person. There are many reasons for this focus including: • Some conditions are life threatening and must be prioritised. • Health workers are often overworked, work in the particular
community for relatively short periods of time and may only see the person of concern infrequently.
• Lack of an appropriate assessment tool (as above). • Lack of training regarding mental health issues including dementia
and lack of experience with diagnosis and treatment. • Focus on conditions that can be ‘treated’ for which there is an
identifiable direct cause.
Both groups noted an apparent high level of tolerance/acceptance within Indigenous communities for a general reduction in capacity as a part of aging. This tolerance/acceptance results in family networks compensating for early behavioural changes due to Dementia. Indigenous communities do not necessarily therefore understand dementia as a disease and in this context lack of early intervention was not seen as problematic. There were several reported incidents of dementia becoming an issue only after the person began inappropriately raising culturally sensitive issues. In these and other cases, lack of understanding of dementia as a disease was seen as causing a range of tensions within the family network including blaming the person for their behaviour and not wanting to be involved in their care. Even when the dementia cannot be treated, families and carers provided with a better understanding of the condition through information are more capable of making care and support choices.
Language and cross-cultural issues can also add a degree of complexity to diagnosis of dementia. These issues tend to make development of a rapport with the person difficult at times and can add difficulty to gathering information about the usual behaviour and social circumstances of the person. Although these issues were complex those present agreed that in most cases arrangements could be made to observe cultural protocols and overcome language barriers. For example, Interpreters (formal or informal) are available to assist with language barriers and cultural protocols can be managed with the assistance of family members or
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 25
alternative staffing (eg. male / female).
5.4.2 Families and Carers
Issues raised in relation to family carers included the following: • Reluctant carers and carers who become carers by default • Quality of care being provided • Carers Allowance • Acceptability of external carers.
The issue of relatives and others looking after people living with dementia due to a lack availability of alternative care (reluctant carers) was discussed. Often these carers have little if any understanding of dementia and are burdened with providing care that may be beyond their capability in view of their own health or family circumstances. The primary responsibility for providing care usually falls to women who have other family responsibilities while men appear to undertake some other roles such as collecting and distributing firewood. In this context, the poor quality of care being provided to some individuals was also of concern. The issue of whether poor standards of care are negligent was discussed however in the cases described, the family carer had apparently provided care to the best of their ability and knowledge, without deliberate disregard or indifference to the persons condition.
Carers Allowance was also discussed. Participants were aware that some family carers are financially dependent on Carers Allowance and do not seek help from service providers because they do not want to do anything that may jeopardise their eligibility for the Allowance. This is sometimes to the detriment of the person with dementia. Paid external carers (non-Indigenous or Indigenous people from another community) are often acceptable as carers because they are free of relationship complications and can deal with all members of the family as an equal. They are able to put the care and management of the person living with dementia as their first priority because they do not have to satisfy other demands. However it is difficult to find carers to work within community based centres.
5.4.3 Funding of facilities and services
Funding issues were broadly discussed in relation to the types of facilities and services that the government is prepared to resource. Some participants supported more flexibility in the manner in which funds could be allocated towards infrastructure such as fencing and outdoor
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 26
facilities. There is a perception that funding of infrastructure is given priority and this is seen as limiting the funding available for service providers to deliver flexible services to meet individual needs. Examples of ‘failed’ attempts to provide facilities or services within communities were discussed. In one case the funding body had apparently engaged in extensive and protracted community consultations. While consultation was seen as necessary and important, there was no guarantee that the result would be a facility or service that would be enduring and would meet individual needs. In another case a building had been sitting idle (‘trashed’) within weeks of completion. An example of a successful remote Indigenous service was attributed to strong leadership within the community, not necessarily related to traditional ownership of the country. Access to any health service is difficult in some Indigenous communities where the clinic may not be staffed every day and health workers are forced to manage very high workloads under conditions that are sometimes difficult. Substantial travel can be involved to access a doctor or specialist and it can be difficult to arrange an escort for some patients. Some participants stated that the whole health system is under enormous stress due to lack of resources. Funding of HACC and CACP services within Indigenous communities was seen as potentially advantageous however these services are limited and the service providers often do not have capacity or the desire to be involved in personal care. In addition some service providers may be constrained by cultural factors in their relationships with others. Diversity of Indigenous communities and the extent to which communities fluctuated between functional and dysfunctional makes it difficult for the government and service providers alike to develop and fund models for service provision that will meet individual care needs over the long term. The prevailing view is that what works in one community may not necessarily work in another and that what is working well today may not necessarily be working well tomorrow. However difficult it may be for funding bodies and service providers, the long-term goals of providing community based care are sound, the needs are demonstrated and the view is that service providers and governments need to act quickly.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 27
5.4.4 Respite care and residential care
Lack of availability, flexibility and the cost of respite care and residential care were raised as critical issues.
Some participants believe that the concepts and purpose of respite care are not widely or well understood. This has lead to the present situation where respite tends to be used as emergency care or a last resort care option for people living with dementia who have developed behaviours that are difficult to manage. Most people are being referred to respite only after an acute episode where nursing respite was required rather than respite that could be provided in a hostel type environment. The cost of providing respite care was discussed. There were some concerns that the cost of overnight or weekend respite care out of the home makes it prohibitive for many families.
The lack of respite services and facilities in remote NT Indigenous communities was of particular concern to participants. Participants cited a number of contributing factors including: • Lack of appropriate infrastructure within communities to
accommodate respite – eg. lack of hostel type accommodation, lack of visitor accommodation
• Conditions within some communities make it difficult to attract workers for community based respite services
• Need to quantify and justify the need for a service • Indigenous people from within the community are often constrained
by cultural requirements / protocols that influence how they relate to others within the community – eg. who they are permitted to care for.
In addition the possibility of a lack of acceptability of out-of-home care within remote communities was mentioned because it may be seen as equivalent to stating that the family carer is not providing adequate care for the person. The carer may therefore feel shamed or inadequate. Lack of respite facilities and services within Indigenous communities is being compensated for to some extent within family networks by various family members taking it ‘in-turns’ to care for the person living with dementia. Lack of services has also previously resulted in some cases of people being referred to services in Darwin. As there is usually no previous relationship with the service provider this has caused additional problems including:
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 28
• for the person living with dementia, becoming even more confused and anxious
• for the service provider, there is no social history available and often scant information about the person making it difficult to provide appropriate care.
Some participants suggested that more creative use could be made of electronic technologies including telephone, video-tapes, live-links, photos and audio mediums. This could assist people transferred away from their communities.
Several alternative service models were discussed as having possibility for application in the NT. One service is mobile, using a caravan that is set up adjacent to homes to provide the respite care. There was general agreement that services should be developed and provided in a community development framework rather than a health and welfare framework. Whether or not any particular model would work in the NT, respite care services must be funded adequately to enable them to have the flexibility to provide individually tailored services in the community that are not cost prohibitive for families.
5.4.5 Information, education and training
Participants validated the need for wider information provision, education and training. Information for families and carers in the early stages is seen as very important to developing their understanding of the progressive nature of the condition and the type of care that the person living with dementia is likely to need. Participants described some difficulties in explaining dementia to Indigenous carers and families such as: • the causes can be multi-faceted (alcohol or substance abuse,
vascular, head injury, age) • no perception that dementia is a disease • families are fearful of being involved • families may have very limited understanding of basic medical
terminology and concepts • language barriers. Use of x-rays to assist in communicating the concepts has been helpful and further development of an information package using illustration is desirable.
Hands-on education and training of paid and family carers is supported. Trained carers can make a substantial difference to the standard of care
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 29
provided to the person living with dementia.
Education and training of Aboriginal Health Workers and other health professionals is also needed. Workers who are educated about and trained in management of dementia would be able to assist with: • in-community management of people living with dementia • supporting families and paid carers • establishing relationships with persons of concern over time to
provide information about changes in the person’s behaviour.
It was suggested that ‘adding-on’ to other established or existing vehicles rather than attempting to ‘go-it-alone’ would be the preferred method to implement information, education and training.
5.4.6 People living with dementia
The main message from participants is that all Indigenous people living with dementia are not the same and therefore scope is needed to provide individually tailored services. Tailored services would be greatly facilitated if a tool to gather and record a person’s social history could be applied. Currently no such tool is applied within the NT. Other concerns directly relating to people living with dementia included: • elder abuse – physical and financial • people being removed from their communities • people being sent back to communities where they are not
adequately supported or accepted.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 30
6.0 Indigenous specific Dementia initiatives developed around Australia
The following Indigenous specific Dementia initiatives were identified through contact with Stakeholders. The extent to which these initiatives may be relevant in a Northern Territory context requires careful evaluation in view of the diversity of Indigenous peoples in terms of culture, language and lifestyle, current levels of understanding of Dementia, literacy levels and the infrastructure and supports available within NT Indigenous communities. 6.1 Better Medication Management by Aboriginal People with Mental
Health Disorders Such As Dementia and Alcohol Related Brain Injury, Their Carers and Other Family Members: A Collaborative Project
Organisations involved in this project are the School of Nursing, Flinders University; Aboriginal Alcohol and Drug Council and South Australian Network for Research on Ageing. The project timetable is February 2000 – June 2003. This is a qualitative collaborative research project to investigate the particular experiences, needs and contexts of Aboriginal people with mental health disorders such as dementia, Korsakoff’s psychosis, alcohol related brain injury, and those of their carers and other family members. There will be a particular emphasis on management of medications, other substance use and related issues. The findings will inform the development and implementation of culturally appropriate policies and practices to enhance safety of medication use, health and well being of Aboriginal clients, carers and other family members. The research will be conducted throughout SA. 6.2 Department of Ageing, Disability and Home Care - Achievements
under the NSW Action Plan on Dementia 1996–2001 An Aboriginal dementia awareness and training project conducted across NSW in 2000-2001 by the Home Care Service of NSW increased knowledge of dementia amongst key Aboriginal workers and service providers. A second phase of this project will build on the resources and outcomes from the first phase. 6.3 Dementia training for Indigenous communities This resource was developed by the Aboriginal Drug and Alcohol Council (SA) and the Alzheimer's Association (SA). The aim of the resource is to equip health and community workers with the skills and information to support people with dementia and their carers.

© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 31
The resource is in the form of a kit containing a video, book, a personal life history booklet, an alcohol and brain damage booklet, a dementia, memory loss and confusion booklet, information handouts, and overheads. (NOTE: Alzheimer’s Australia NT has evaluated this resource.)
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 32
7.0 Barriers to and strategies for convening a National Rural and Remote Indigenous Dementia Forum
7.1 Barriers
7.1.1 Priorities of other health areas eg. Chronic diseases There is a high prevalence of chronic disease or acute health problems amongst older Indigenous people. Many conditions can be life threatening and require a high level of care, the priority of treating these conditions tends to outweigh the priority of dealing with secondary conditions such as dementia. Therefore it is also the case in terms of funding and allocation of resources both human and financial. If medical professionals are limited in the number of conferences or forums they can attend due to work priorities and/or limited funding it is highly likely that conferences or forums dealing with other conditions would be chosen. 7.1.2 Lack of funds for community based organisations For small community based organisations there is limited access to funds for travel and expenses to attend conferences. The staff of these organisations should be the target audience for the conference due to their vital role in the care of the indigenous clients with dementia in remote and urban areas. 7.1.3 Lack of statistical data and research The limited availability of data specific to Indigenous people living with dementia would tend to limit the choice of Keynote presenters and others for delivery of concurrent sessions. Although the other side of this is that how to improve this area could make for an interesting topic in itself. 7.1.4 Competing priorities for potential participants – eg. Other
meetings / conferences As at 12 November 2002 there were 10 Aged Care or related conferences to be held in Australia listed on the Aged & Community Services Australia website. This does not include specific local or interstate forums and meetings for service providers such as the meeting planned by DHA for March 2003. (See Attachment G)
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 33
7.1.5 Dementia not seen as a priority issue within remote
communities Due to the tolerance of early signs of dementia and acceptance by many that behavioural changes are just part of getting old, dementia is not seen as a serious issue. Gaining commitment of family or carers to leave their community to attend a conference could be difficult. 7.1.6 Small numbers of people diagnosed with dementia Although this research was not intended to gather definitive numbers of Indigenous people in the NT diagnosed with dementia it did gather some interesting anecdotal numbers. These numbers were very small with common examples of one or two people in a community or more commonly none. Of course there are probably many undiagnosed cases as mentioned earlier in this report. In addition the small number of people diagnosed with dementia are potentially widely spread throughout a vast geographical distance. This could mean that the potential audience for a conference / forum is also small.
7.1.7 Priorities of Aboriginal Medical Services and Health Boards
Throughout this project it has proven extremely difficult to get access to personnel from Aboriginal Medical Services or the peak body. Following an extensive amount of phone calls, emails and faxes we were only successful in gaining interviews with two services Congress in Alice Springs and Miwatj in Nhulunbuy. We in fact travelled to Katherine for an appointment and the representative failed to attend the agreed appointment time. The other priorities of these services and the fact that their core business is primary health make it difficult for them to be able to give time to other areas such as this project. This difficulty could also extend to attending a conference / forum.
7.2 Strategies to overcome barriers The Consultants suggest that the most effective strategy to overcome the identified barriers is to ‘combine’ with another conference or forum already scheduled. A ‘combined’ conference is envisaged as being achieved by the inclusion of an extra day of the conference. An alternative would be to include a plenary session, concurrent sessions or workshops depending upon the format of the event.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 34
The National Residential & Flexible Aged Care Service Providers Conference scheduled for 25th to 27th March 2003 in Alice Springs is viewed as an ideal opportunity, however this is a short time frame and conference preparations may be well advanced, unable to accommodate changes to the program or format that may be required. Other opportunities are the Aged & Community Services Australia Conference in Perth 19th to 22nd October 2003 or the National Carers Conference in Canberra 18th to 19th September 2003. Alzheimer’s would need to act quickly to gain input. Combining with another forum would offer potential speakers and participants considerable cost and time-savings. It would also provide the opportunity for participants who may not normally consider attending an Indigenous Dementia specific forum to do so at minor additional cost.
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 35
Attachment A References
1. Aged and Community Services Australia, Dementia, Fact Sheet No. 5. www.agedcare.org.au/factsheets.
2. Aged Care Planning Data. Department of Heath and Ageing, 2002 3. Australian Institute of Health and Welfare, date, Indigenous peoples,
Older Australians at a glance. www.aihw.gov.au/publications/welfare/oag02.
4. Australia’s Older Population: Past, Present and Future (June, 1999). Special Article published in Australian Demographic Statistics, June Quarter 1999, ABS cat no. 3101.0.
5. Australia’s Welfare, 1999 6. Chronic Diseases and Risk Factors. ABS Special Article, Year Book
Australia, 2001. 7. Condon JR, Warman G, Arnold L (editors), The Health and Welfare of
Territorians. Epidemiology Branch, Territory Health Services, Darwin, 2001.
8. Jorm, A., Dementia: a major health problem for Australia. Position Paper, Alzheimer’s Association of Australia, September 2001.
9. Mental Health. Australian Institute of Health and Welfare, www.healthinfonet.ecu.edu.au, originally published in Australia’s Health 2002.
10. Northern Territory Aboriginal Communities, Department of Lands, Planning and Environment, Northern Territory Government, July 18th, 2001
11. Northern Territory Population Strategy, Issues paper. Department of the Chief Minister, Northern Territory Government, August 2002.
12. NT Dementia Rates. Unknown author, unknown publisher, unknown publication date.
13. Overview of the health status of Indigenous Australians. Office for Aboriginal and Torres Strait Islander Health, Department of Health and Aged Care, (date unknown), www.health.gov.au/about/cmo/indhea.htm.
14. Pollitt, PA (1997) The Problem of Dementia in Australian Aboriginal and Torres Strait Islander Communities: An Overview, International Journal of Geriatric Psychiatry, Vol 12, 155–163.
15. Rosewarne, R., (date unknown), Dementia and older Australians, Older Australians at a glance. www.aihw.gov.au/publications/welfare/oag02.
16. Sheldon, M., (1997) Psychiatric Assessment in Remote Aboriginal Communities of Central Australia, www.aams.org.au/mark_sheldon/index.htm.
17. Swan, P. and Raphael, B., 1995, Ways Forward, National Aboriginal and Torres Strait Islander Mental Health Policy, National Consultancy Report. AGPS, Canberra.

© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 36
ATTACHMENT B Key Stakeholders, resources, expertise and support services
SERVICE ROLE Aboriginal Medical Services
Provide primary health care. Access to doctors, nurses and Aboriginal health workers
Adult Guardianship Adult Guardianship determines the eligibility for guardianship and appoint a suitable guardian
Advocacy Services Advocacy Services are available to residents of aged care homes, people assessed as eligible for residence in an aged care home and who are waiting for a place and recipients of Community Aged Care Packages The Service provides: • Information about the aged persons rights and strategies
for ensuring these rights are upheld; • Referrals to other organisations and services; • Support such as attending a meeting with the person,
helping prepare for a meeting or to write a letter; • Representation if the aged person would like the advocacy
service to speak on their behalf, and • Education sessions for community groups and service
providers on topics such as advocacy and duty of care. Advocacy services work with individuals and groups. They also work with the aged persons representatives such as families and friends
Aged Care Assessment Teams
Aged Care Assessment Teams are groups of professionals, such as doctors, nurses, occupational therapists and social workers. In Darwin and Alice Springs there are Dementia Support Workers. In Darwin, Katherine and Alice Springs there are also Aboriginal Liaison Officers. Team members can provide an expert assessment of dementia and help to determine the level of care the person will need, and provide information about services such as respite at home, in a day care centre or residential care services.
Alzheimer’s Australia NT
Provide education and support services to people with dementia and their carers. They assist and promote support groups and provide both a telephone and face-to-face counselling service.
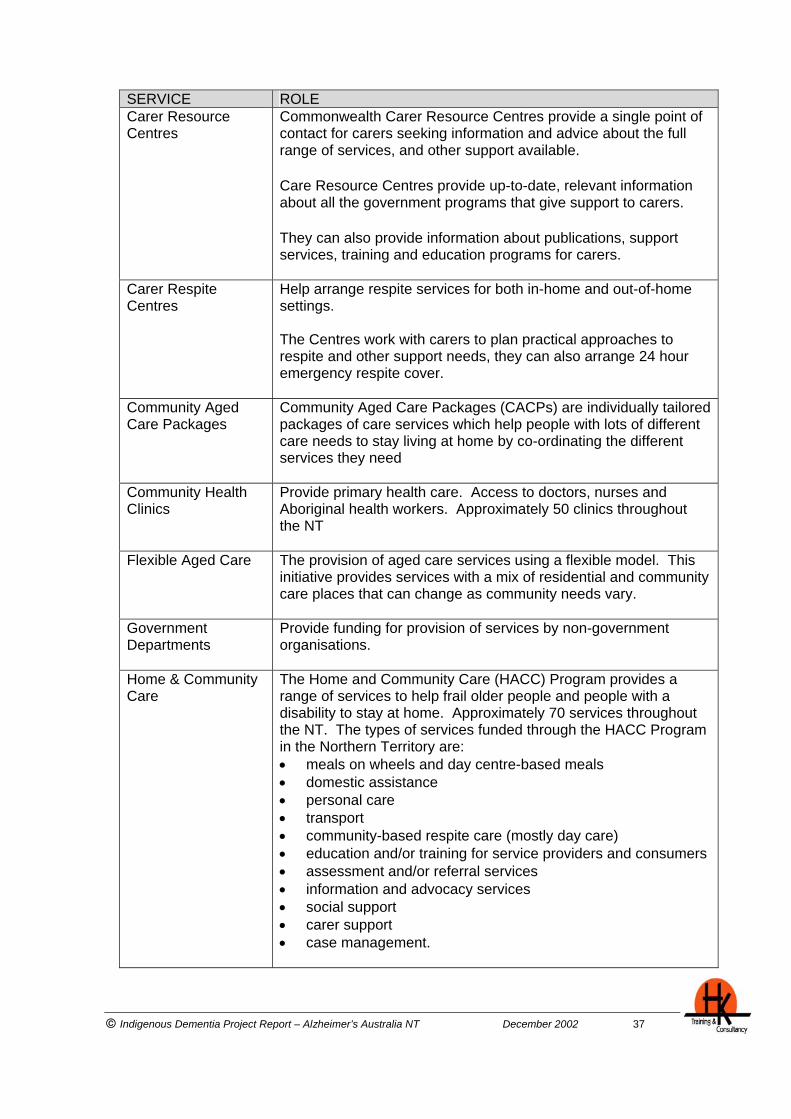
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 37
SERVICE ROLE Carer Resource Centres
Commonwealth Carer Resource Centres provide a single point of contact for carers seeking information and advice about the full range of services, and other support available.
Care Resource Centres provide up-to-date, relevant information about all the government programs that give support to carers.
They can also provide information about publications, support services, training and education programs for carers.
Carer Respite Centres
Help arrange respite services for both in-home and out-of-home settings. The Centres work with carers to plan practical approaches to respite and other support needs, they can also arrange 24 hour emergency respite cover.
Community Aged Care Packages
Community Aged Care Packages (CACPs) are individually tailored packages of care services which help people with lots of different care needs to stay living at home by co-ordinating the different services they need
Community Health Clinics
Provide primary health care. Access to doctors, nurses and Aboriginal health workers. Approximately 50 clinics throughout the NT
Flexible Aged Care The provision of aged care services using a flexible model. This initiative provides services with a mix of residential and community care places that can change as community needs vary.
Government Departments
Provide funding for provision of services by non-government organisations.
Home & Community Care
The Home and Community Care (HACC) Program provides a range of services to help frail older people and people with a disability to stay at home. Approximately 70 services throughout the NT. The types of services funded through the HACC Program in the Northern Territory are: • meals on wheels and day centre-based meals • domestic assistance • personal care • transport • community-based respite care (mostly day care) • education and/or training for service providers and consumers • assessment and/or referral services • information and advocacy services • social support • carer support • case management.
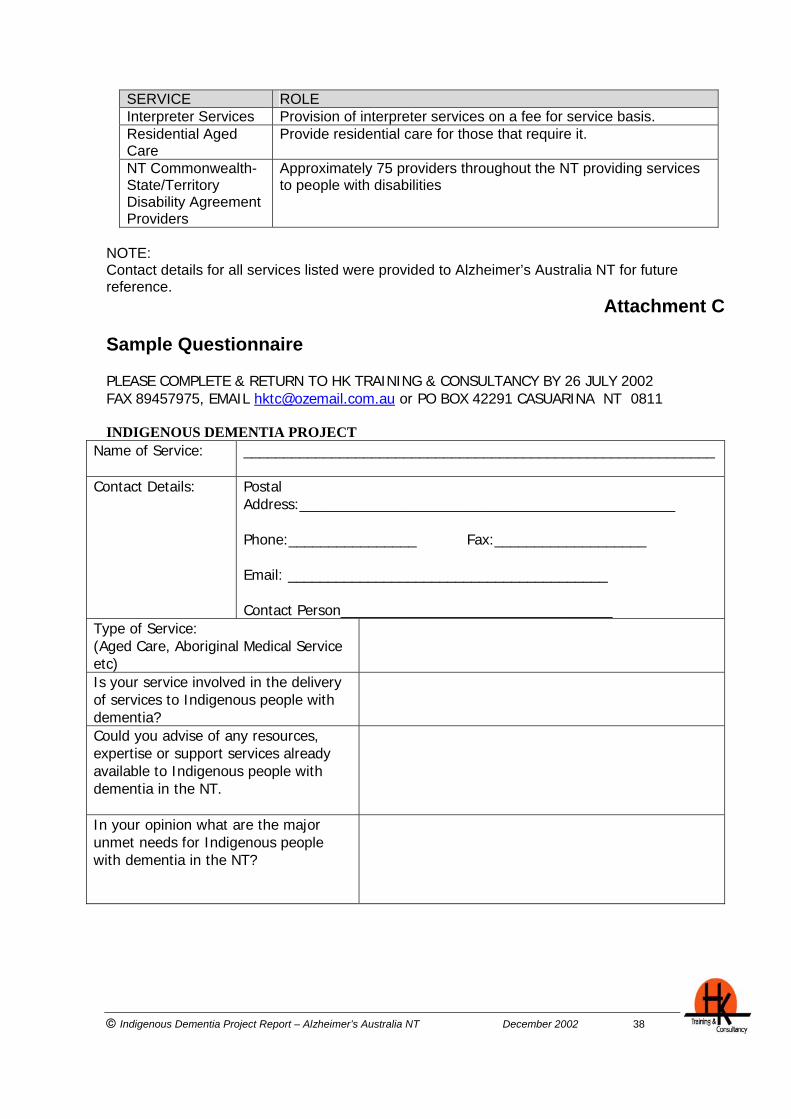
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 38
SERVICE ROLE Interpreter Services Provision of interpreter services on a fee for service basis. Residential Aged Care
Provide residential care for those that require it.
NT Commonwealth-State/Territory Disability Agreement Providers
Approximately 75 providers throughout the NT providing services to people with disabilities
NOTE: Contact details for all services listed were provided to Alzheimer’s Australia NT for future reference.
Attachment C Sample Questionnaire PLEASE COMPLETE & RETURN TO HK TRAINING & CONSULTANCY BY 26 JULY 2002 FAX 89457975, EMAIL [email protected] or PO BOX 42291 CASUARINA NT 0811
INDIGENOUS DEMENTIA PROJECT
Name of Service: ___________________________________________________________
Contact Details:
Postal Address:_______________________________________________ Phone:________________ Fax:___________________ Email: ________________________________________ Contact Person__________________________________
Type of Service: (Aged Care, Aboriginal Medical Service etc)
Is your service involved in the delivery of services to Indigenous people with dementia?
Could you advise of any resources, expertise or support services already available to Indigenous people with dementia in the NT.
In your opinion what are the major unmet needs for Indigenous people with dementia in the NT?
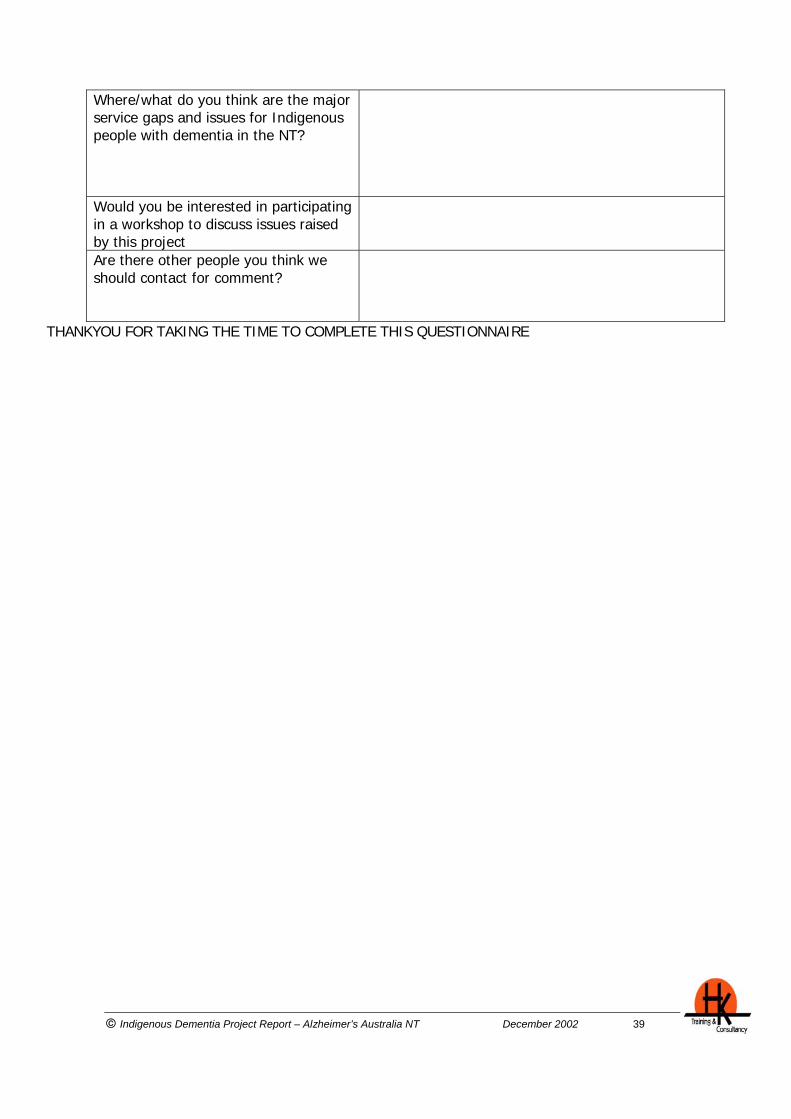
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 39
Where/what do you think are the major service gaps and issues for Indigenous people with dementia in the NT?
Would you be interested in participating in a workshop to discuss issues raised by this project
Are there other people you think we should contact for comment?
THANKYOU FOR TAKING THE TIME TO COMPLETE THIS QUESTIONNAIRE
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 40
Attachment D List of Abbreviations ABS Australian Bureau of Statistics ACAT Aged Care Assessment Team BRACS Broadcasting for Remote Aboriginal Communities Scheme CACP Community Aged Care Packages CCIS Community Care Information System DHA Commonwealth Department of Health and Ageing DHaCs Northern Territory Department of Health and Community ServicesGP General Practitioner HACC Home and Community Care NSW New South Wales NT Northern Territory SA South Australia THS Territory Health Service
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 41
Attachment E Organisations Represented at the Darwin Workshop Territory Care and Support Commonwealth Department of Health and Ageing (2 participants) ACAT Darwin (4 participants) Red Cross Homecare Services Darwin Community Legal Service Alzheimer’s Australia NT (4 participants) Respite Options for Senior Territorians
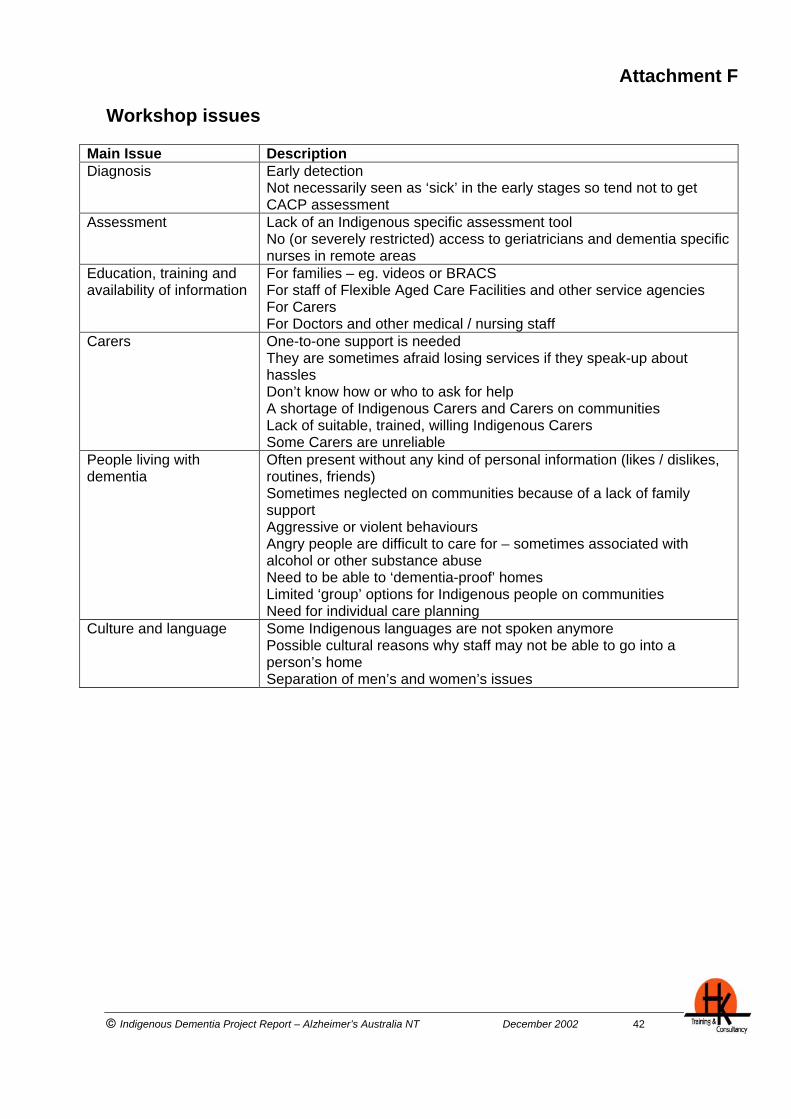
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 42
Attachment F Workshop issues
Main Issue Description Diagnosis Early detection
Not necessarily seen as ‘sick’ in the early stages so tend not to get CACP assessment
Assessment Lack of an Indigenous specific assessment tool No (or severely restricted) access to geriatricians and dementia specific nurses in remote areas
Education, training and availability of information
For families – eg. videos or BRACS For staff of Flexible Aged Care Facilities and other service agencies For Carers For Doctors and other medical / nursing staff
Carers
One-to-one support is needed They are sometimes afraid losing services if they speak-up about hassles Don’t know how or who to ask for help A shortage of Indigenous Carers and Carers on communities Lack of suitable, trained, willing Indigenous Carers Some Carers are unreliable
People living with dementia
Often present without any kind of personal information (likes / dislikes, routines, friends) Sometimes neglected on communities because of a lack of family support Aggressive or violent behaviours Angry people are difficult to care for – sometimes associated with alcohol or other substance abuse Need to be able to ‘dementia-proof’ homes Limited ‘group’ options for Indigenous people on communities Need for individual care planning
Culture and language
Some Indigenous languages are not spoken anymore Possible cultural reasons why staff may not be able to go into a person’s home Separation of men’s and women’s issues
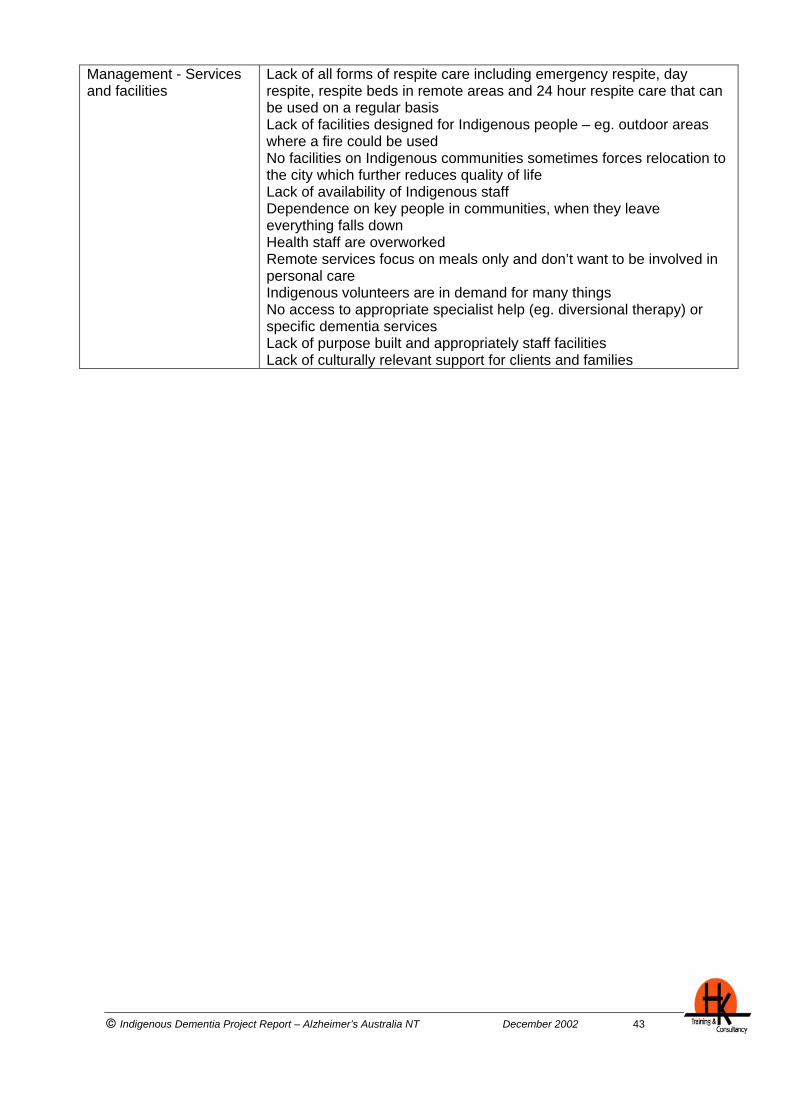
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 43
Management - Services and facilities
Lack of all forms of respite care including emergency respite, day respite, respite beds in remote areas and 24 hour respite care that can be used on a regular basis Lack of facilities designed for Indigenous people – eg. outdoor areas where a fire could be used No facilities on Indigenous communities sometimes forces relocation to the city which further reduces quality of life Lack of availability of Indigenous staff Dependence on key people in communities, when they leave everything falls down Health staff are overworked Remote services focus on meals only and don’t want to be involved in personal care Indigenous volunteers are in demand for many things No access to appropriate specialist help (eg. diversional therapy) or specific dementia services Lack of purpose built and appropriately staff facilities Lack of culturally relevant support for clients and families
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 44
Attachment G Conferences
February 2003
Biennial Congress of the World Federation for Mental Health 21 - 26 February 2003 Melbourne Convention Centre, Melbourne Contact: ICMS Pty Ltd, 84 Queensbridge Street, Southbank 3006 Phone: (03) 9682 0244 Fax: (03) 9682 0288 [email protected] www.icms.com.au/wfmh2003
March 2003
7th National Rural Health Conference "The Art and Science of Healthy Community 1 - 4 March 2003 Hotel Grand Chancellor, Hobart, Tasmania Contact: 7th National Rural Health Conference, PO Box 280 Deakin West, ACT, 2600. Fax (02) 6285 4670 [email protected] www.ruralhealth.org.au 12th Annual Tri-State Conference "Innovation Excellence in Aged Care" 2nd - 4th March 2003, Albury Contact VAHEC Ph: 03 9820 0888 Fax: 03 9804 5133 [email protected] Alzheimer's Australia National Conference "Today's challenges, tomorrow's choices" 18 - 21 March 2003 Melbourne Convention Centre, Melbourne www.alzvic.asn.au Aged Care Queensland State Conference 25 - 28 March, 2003, Conrad Jupiters, Gold Coast www.acqi.org.au/conferences.htm
April 2003
2003 HACC Service Providers State Conference "Dare to be Different" 7 - 8 April 2003, Launceston, Tasmania Contact: Community Options SErvice (North), 233B Charles Street, Launceston [email protected]
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 45
May 2003
"Live Life" Asia Pacific Regional Conference on Prevention of Elderly Suicide "Prevention of Elderly Suicide" A Transdisciplinary Challenge" The Hong Kong Council of Social Service, Hong Kong Psychogeriatric Association, Social Welfare Department 28 - 30 May 2003 Hong Kong Contact: Conference Secretariat: (852) 2864 2946 (852) 2865 4916 [email protected]
July 2003
International Nursing Conference 2003 Nursing in a Technological World, 1 - 4 July 2003, Hilton Hotel, Brisbane, Queensland [email protected]
September / October 2003
28th International Congress on Law and Mental Health International Academy of Law and Mental Health, New South Wales Department of Health, Commonwealth Department of Health and Ageing, New South Wales Attorney-General's Department 28 September - 3 October 2002 Sydney Contact: Capital Conferences Phone: 02 99996577 Fax: 02 9999 5733 [email protected] www.ialmh.org 16th National Conference - 2003 Aged & Community Services Australia - Perth 19 - 22 October, 2003 18-19 Sep 2003 Canberra, ACT National Carers Conference
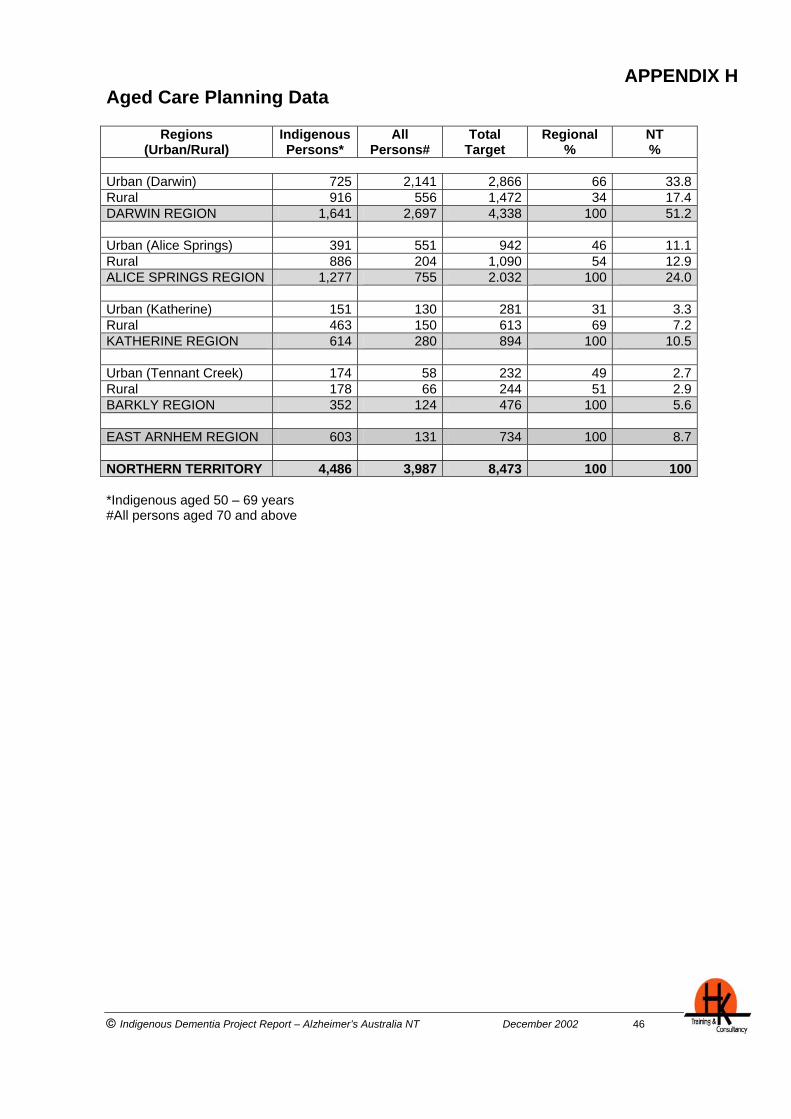
© Indigenous Dementia Project Report – Alzheimer’s Australia NT December 2002 46
APPENDIX H Aged Care Planning Data
Regions (Urban/Rural)
Indigenous Persons*
All Persons#
Total Target
Regional %
NT %
Urban (Darwin) 725 2,141 2,866 66 33.8Rural 916 556 1,472 34 17.4DARWIN REGION 1,641 2,697 4,338 100 51.2 Urban (Alice Springs) 391 551 942 46 11.1Rural 886 204 1,090 54 12.9ALICE SPRINGS REGION 1,277 755 2.032 100 24.0 Urban (Katherine) 151 130 281 31 3.3Rural 463 150 613 69 7.2KATHERINE REGION 614 280 894 100 10.5 Urban (Tennant Creek) 174 58 232 49 2.7Rural 178 66 244 51 2.9BARKLY REGION 352 124 476 100 5.6 EAST ARNHEM REGION 603 131 734 100 8.7 NORTHERN TERRITORY 4,486 3,987 8,473 100 100 *Indigenous aged 50 – 69 years #All persons aged 70 and above