Embed Size (px)
Citation preview

Indonesia HIV-HRH Assessment
September 21, 2018

Welcome & Opening RemarksSubdirektorat HIV AIDS dan PIMS / CDC / MOH
USAID/Indonesia

IntroductionsHRH2030 Program

Assessment Objective
▪ Assess the HRH-related barriers at the policy and site levels that may be hindering HIV service delivery
▪ Gather evidence to recommend policy and site level interventions to improve HIV service delivery▪ HRH optimization to achieve Fast-Track targets
▪ Longer-term sustainability planning and HIV mainstreaming
▪ Consideration of differentiated service delivery (DSD) models

Workshop Overview
▪ Methods▪ Policy Assessment
▪ Site-level Assessment
▪ Results▪ Policy Assessment
▪ Site-level Assessment
▪ Preliminary recommendations
▪ Discussion & next steps

Methods


HRH2030 Policy and Site-level Assessment Approach in Indonesia

Policy Assessment Objectives
1. To identify relevant HRH policies, protocols, scopes of practice, and task shifting practices that hinder or support the key health worker types to implement and scale up HIV services
2. To identify policy and advocacy opportunities, challenges, priority actions, and implications for HRH programming to strengthen the implementation of HIV services

Policy research questions
For HIV policy implementation in Indonesia:
1. What are the major policy and regulatory barriers and opportunities in the HRH system for current implementation?
2. What are the policy implementation issues that influence the health workforce in delivering HIV services?
3. Learning from the implementation of SUFA, what HRH policy, regulatory, and legal adaptations will be needed for fully implementing Test and Treat program in the future?
4. What policy or regulatory changes should be prioritized to achieve more effective implementation?
5. What aspects in the policies, protocols, scopes of practice hinder or support the implementation of task-shifting practices in Indonesia?

*Adapted from the Policy
Implementation Assessment Tool:
(http://www.healthpolicyplus.com/a
rchive/ns/pubs/hpi/1155_1_PIAT_P
aper_Taking_the_Pulse_of_Policy_
acc.pdf)
1.Policy analysesa. Policy* search
Website of relevant institutionMLHR, MoH, MORTHE, Ministry of Labour
MLHR websiteValidate status of regulation
b. Policy Inventory
Primary Mainly concerns with
HIV/AIDS and HRH issues
Technical/derivativeFurther describes technical aspects
of a primary policy
Backgroundprovides context for
primary policy
Methods
c. Text analysis
2. Key informant
interviews

HRH2030 Policy and Site-level Assessment Approach in Indonesia

Site-level Assessment Sample
Site District
Volume of all HIV tests
conductedVolume of HIV+ tests
High Medium Low High Medium Low
PKM Kecamatan Tanjung Priok North X X
PKM Kecamatan Setiabudi South X X
PKM Kecamatan Gambir Central X X
PKM Kecamatan Tamansari West X X
PKM Kecamatan Penjaringan North X X
PKM Cengkareng West X X
PKM Cakung East X X
PKM Kecamatan Kramat Jati East X X
Ruang Carlo Central X X
PKM Kelurahan Kramat
(Kecamatan Senen)Central X X

Site-level tools
•Unit manager questionnaire Availability
•Rapid task analysisCompetency(self-reported)
•Client flow mappingAccessibility
Challenge identification
• Health worker focus group discussion

Unit manager questionnaire
▪ Semi-structured interview
▪ HRH Availability▪ Types, number and availability of cadres at facility
▪ Current health worker allocation per HIV service point
▪ Health worker capacity and preparation for providing quality HIV services
▪ Manager perspectives on▪ Reasons contributing to absenteeism, retention, and
productivity
▪ HRH barriers pertaining to service delivery
Adapted from the PEPFAR Rapid Site-level Health Workforce Assessment Tool
https://www.hrh2030program.org/pepfar_tool/

Rapid Task Analysis (1)
Service Areas
1: Examination of HIV, STI and hepatitis
2: ART Enrollment
3: ART Initiation
4: Adherence Counselling
5: Clinical Examination & Consultation
6: Recording and Reporting
7: Health Education
8: Integrated TB-HIV Services
9: Mobile Testing
10: PMTCT
11: Harm reduction
Health Worker Types
Doctor
Nurse
Lab Technician
Recording & reporting
officer
Pharmacy
Midwife
Cadre/community
counselor
“Core team” for site activation
Adapted from HRH2030 Rapid Task Analysis Questionnaire
https://www.hrh2030program.org/wp-content/uploads/2018/06/Rapid-Task-Analysis-Tool.pdf

In your opinion, to what extent is
your knowledge about this task?
Not acquired the basic knowledge
Only the basic knowledge
Necessary knowledge to perform the
task
Advanced knowledge
Rapid Task Analysis (2)
Is this
task
assigned
to you?
No
Yes
In your opinion, how confident
are you in performing the task? Need more opportunity to apply
knowledge
Can apply knowledge but still need help
Confident performing task, but not to
teach others
Confident performing task and teaching to
others
Have you
been trained
for this task?
No
Yes• Informal, on-the-job training
• Clinical mentoring
• Formal in-service training
• Pre-service training
How often do you perform
this task? Never
Seldom
A few times a month
A few times a week
Almost every day

Client flow mapping
▪ For ART refill patients with undetectable viral load
▪ Participatory observation▪ Where do they go?
▪ How long does it take?
▪ With which health workers do they interact during the visit?
▪ Where are the service delivery bottlenecks, if any?
▪ For reasons of ethics and confidentiality, CSCs were trained to use tablets to conduct client flow mapping

Health worker Focus Group Discussion (FGD)
▪ Client and health worker flow mapping from HW perspective▪ Who is involved at each service area?
▪ What are challenges at each service area?
▪ Root cause analysis by HRH category type:
Adapted from HRH2030 Optimizing Health Worker Performance and Productivity to Achieve the 95-95-95 Targets
https://www.hrh2030program.org/prodperftoolkit/
Health
worker
competency
gaps
Low
engagement
Poor
allocation of
staff or tasks
Inefficient
work
processes
Other
health
systems
issues

Results

HRH2030 Policy and Site-level Assessment Approach in Indonesia

Evolution of Policies for HIV Service Delivery

HRH Quantity & Quality HRH Management
Medical Practices
Law, HRH Law Competency, Registration,
Licensing
UU 17/2007,
RPJP HRH Development
UU 5/2014 ASN Legal foundation for ASN
management – PNS &PPPK
UU 23/2014 on
Regional Government Role of regional government in HRH
planning & development
PP 43/2016 SPM Quantity & quality standard of HRH
PP 11/2017 on Civil
Servants Managementmanagement of human resources for civil
servant)
PP 18/2016 on
Local Apparatus Offices & Technical Implementation Unit
perform the HRH planning)
HRH Procurement HRH Planning
PMK 26/2017Procurement of HRH by agreement
PMK 33/2015 Manual to determine HRH needs
PB 61/2014HRH planning and equity
Law or regulation
established by the House
of Representatives with
President's consent.
Law set by the President
to implement the act as it
should.
Based on certain content
for the purpose of the
administration of certain
affairs in government.
UU: Undang-undang
Act/Law
PP: Peraturan
Pemerintah
Government regulation
PMK: Perat uran
Menteri Kesehatan
Minister of Health
Regulation
HRH Regulation : Hierarchy of Legislations
UUD 1945 Constitutional Foundation

Ministry of
Research &
Higher
Education
Health
Professional
Education
Institutions
Health
Professional
Graduates
Ministry of Health Ministry of
Civil
Apparatus Empowerment
Ministry of
Home Affairs
BPPSDMPlanning
overall HRH
needs (#)
DG of Health
ServicesQuality of Care
(Accreditation)
DG of
CDCTechnical
Competence.
Technical Policies &
Program PlanningLocal
Government/
PHO / DHO
Puskesmas
&
Hospitals
Planning & Technical DirectionEducation Procurement
HRH Stakeholders in Policy Implementation
Management
Employed
Health
ProfessionalsCommand
Coordination
Professional
Councils
Regulation

Policies on HRH Education
▪ HIV competencies are integrated into pre-service education policies for doctors, nurses, midwives▪ Standar Kompetensi Dokter Indonesia – SKDI, 2012
▪ Standar Kompetensi Perawat, 2007
▪ Standar Kompetensi Bidan, 2007
▪ In-service training required for health worker re-registration
▪ Lab technicians, recording and reporting, and pharmacy staff▪ Nurses can perform some pharmacy tasks in the absence of pharmacy
staff
Policy Implementation for HRH Education
▪ Pre-service education standardization of comprehensive
HIV curricula is limited, particularly in private schools
▪ Variant quality of pre-service curricula
▪ Wide range of HIV in-service training programs established
▪ Targeted selection of in-service trainees and post-training
follow-up may not be consistently practiced
▪ In-service training curricula

Policy Implementation on HRH Regulation, Planning and Procurement
▪ Initial licensure/passing competency exams can be challenging for many new health graduates
▪ Registration processes frequently delayed
▪ Limited use and interoperability of local HRH databases for planning
▪ Challenge to coordinate across stakeholders to hire health workers, specifically related to planning and procurement

Policies on HRH Management Remuneration, incentives and benefits
▪ Civil servant, non-civil servant and private health workers
▪ Compensation vs workload, timing incentives payment
▪ Operational incentives for performing activities outside the health facilities (Puskesmas BOK, DHO)
▪ MOH Regulation No. 21/2016 (60% of fees for medical providers and operational costs) - Local Government’s capability (to adapt the national regulation to the local level and manage the funding for the Puskesmas)

Existing Policies• MOH Regulation No. 64/2015 – technical direction/guidance
• Permenkes No. 21/2013 jo. Permenkes No. 87/2014 – monitoring of quality of
HIV care
• The Act on Health (Law of Health No. 26/2009) - drugs can only be prescribed
by physicians (Law of Medical Practices No. 29/2004)
• Article 65 of Law 36/2014 - Delegation of authority/action (the transfer of
medical authority to health professionals/non-medical)
• Article 29, Article 32 of Law 38/2014 - Delegation of medical authority to nurses
(the transfer of medical authority to nurses has a special legal basis/lex specialist)
• Duty of nurses with certain limitations
Policies on HRH Management
Quality of care and performance

Implementation issues
• Variant the monitoring practices, budget availability
• Only about 50% of health facilities in Indonesia are accredited
• Accreditation as an objective vs maintain quality of care, lack of
human resources at the health facilities to apply and meet the
accreditation standards
• Indonesia Medical Association (Ikatan Dokter Indonesia/IDI) rarely
audits and evaluates quality of care including prescribing practices
Policies on HRH Management
Quality of care and performance

Site-level Results
•Unit manager questionnaire Availability
•Rapid task analysisCompetency(self-reported)
•Client flow mappingAccessibility
Challenge identification
• Health worker focus group discussion

Number of health workers by typeof required “core team” for HIV site activation

PKMHIV Services
Q3, to be verified
Core
teamKnowledge Confidence to perform % Training
New positives
Enrolled in ART
Currently on ART
+
=
-
Advanced
Sufficient
Basic
None
Confident, capable to mentor
Confident
Confident but need support
Needs practice
Across all HWs &
tasks
A 8 6 82 + 0% 73% 20% 7% 11% 41% 36% 11% 66%
B 20 15 237 + 5% 73% 19% 3% 57% 8% 27% 8% 79%
C 0 0 61 + 0% 56% 38% 6% 21% 44% 15% 21% 53%
D 10 6 111 + 0% 85% 12% 2% 20% 32% 34% 15% 95%
E 20 11 171 + 0% 68% 32% 0% 16% 60% 12% 12% 88%
F 10 9 265 + 4% 71% 24% 0% 27% 53% 18% 2% 78%
G 2 7 81 + 12% 81% 8% 0% 46% 31% 23% 0% 88%
H 13 12 241 + 34% 47% 19% 0% 38% 53% 9% 0% 75%
Summary dashboard of 8 Puskesmas KecamatanAll health workers across all tasks
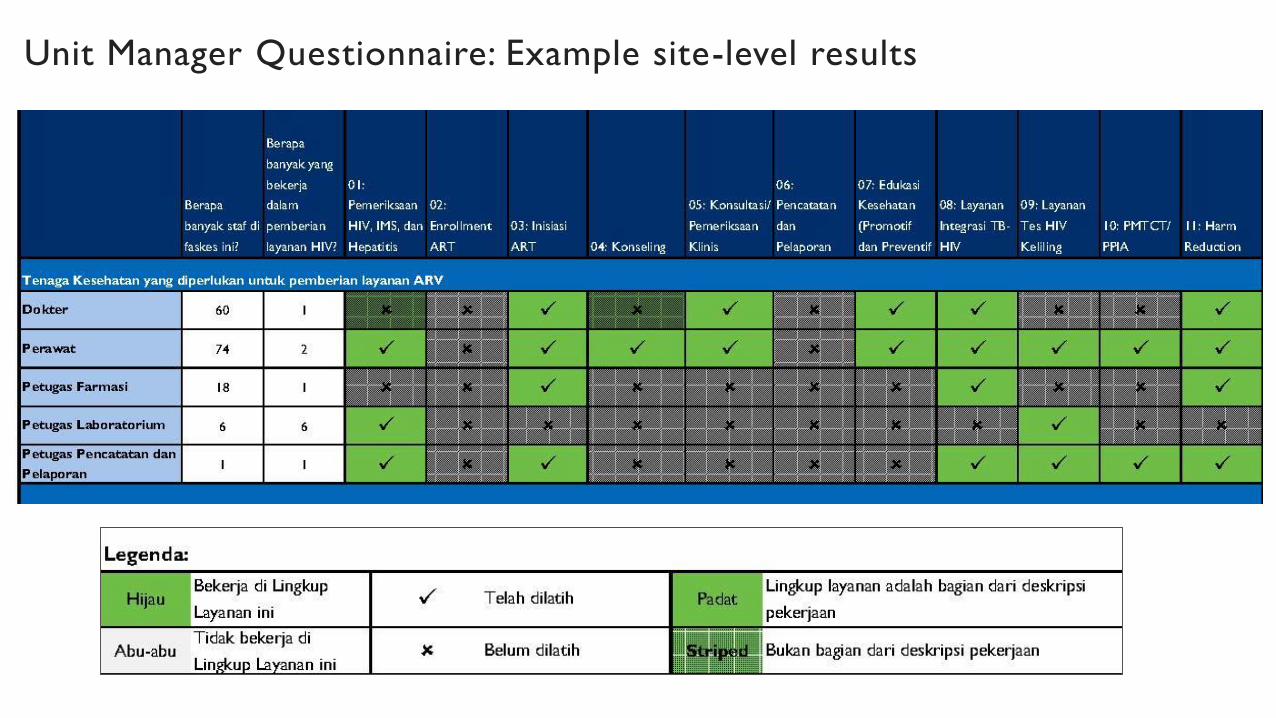
Unit Manager Questionnaire: Example site-level results

Rapid Task Analysis: Example aggregate results
Doctors’ self-reported HIV knowledge, training, skills, and frequency by task (n=13)

Nurses’ self-reported HIV knowledge, training, skills, and frequency by task (n=12)

Doctors’ self-reported HIV knowledge, training, skills, and frequency by assigned task

Nurses’ self-reported HIV knowledge, training, skills, and frequency by assigned task

Nurses’ self-reported HIV knowledge, training, skills, and frequency by assigned
task: HIV diagnosis
Of nurses assigned to HIV
diagnosis, (n=3), 1 reported
having no knowledge
S/he had been trained in HIV
diagnosis
S/he reported needing practice
to perform HIV diagnosis
S/he reported performing the task
a few times a month

Nurses’ self-reported HIV knowledge, training, skills, and frequency by
assigned task: PMTCT
Of 12 surveyed, 1 nurse
reported being assigned to ARV
management of pregnant
women, and having basic
knowledge
S/he has not been
trained for PMTCT.
S/he needs support to
perform PMTCT.
S/he performs
PMTCT somewhat
frequently.

Doctors’ self-reported HIV knowledge, training, skills, and frequency by
assigned task: Advanced clinical ART exam
Of doctors assigned to
advanced ART clinical exam
(n=10), 80% reported having
sufficient knowledge
7 of the these 8 have
been trained to do
advanced clinical ART
exams
7 of the these 8 feel
confident to perform
clinical ART exams
Most doctors perform
advanced clinical ART
exams regularly

Client Flow mapping results:
Time spent in waiting rooms / total time spent at facility by ART refill clients (n=18)
Of those observed, clients spent an
average of 53% of their time waiting
versus receiving care.

Health worker FGDs: Challenge identification▪ Health worker competency gaps
▪ PKM management planning and budgeting for staff in-service training
▪ Increase the number and capacity of Counselor
▪ Low engagement▪ Stigma is not only felt by HIV client but also felt by the HIV core team
▪ Puskesmas management's commitment to "see" that HIV services
are as important as other health service units
▪ Poor allocation of staff or tasks▪ Additional task
▪ Tasks distribution between health workers in the HIV team
▪ Inefficient work processes▪ Manual recording system
▪ SIHA
▪ Integration of recording and reporting systems
▪ Other health system issues▪ Almost all Puskesmas doesn’t have a special room for counseling
▪ Some Puskesmas have the equipment for Viral Load test, but are constrained in procuring cartridges
▪ Unclear Reagan allocation for the CATIN (Calon Pengantin) program.

Discussion & Questions

Preliminary Recommendations
▪ Site-level data review and discussion▪ Health workforce challenges and local potential solutions
▪ Review HIV service delivery to identify gaps and take quality improvement approach (HRH2030 Toolkit; see next slide)
▪ Coordinate strategic in-service skills development in consideration of workload, FTE implications, staff rotations and turnover
▪ Determine evidence needs/workload limits to support incremental task sharing or differentiated care;▪ MMS could be considered at high-volume sites (where pharmacy workload high),
especially when monthly refills present hardship for the client
▪ Scale up tools application through capacity building; use locally available data streams to inform

Optimizing Health Worker Performance and Productivity
to Achieve 95-95-95 Targets
www.hrh2030program.org/prodperftoolkit
Future Opportunities
▪ Distribution of HRH management responsibilities
▪ Increased practical, interprofessional learning and supportive supervision
▪ Anticipate and plan for workload increase for lab/pharmacy staff across other (non-HIV) services
▪ Repeat HIV-HRH assessment to inform future workload needs that may required differentiated care models
▪ Consider strategic use of district and site level funds, e.g., capitation funds
▪ Adapt and apply the policy and site-level assessment methodology across all services

Discussion & Next Steps
▪ Conduct local dissemination of site-level results and support development of site-level solutions and/or improvement plans
▪ Build capacity to routinely apply tools at PEPFAR-supported sites (Jakarta, Papua)
▪ Make Power BI dashboard with detailed site-level results available to USAID, MOH, and partners (LINKAGES)

Closing remarksSubdirektorat HIV AIDS dan PIMS / CDC / MOH
USAID/Indonesia

Acknowledgements
Rachel Deussom, Astri Ferdiana, Caroline Francis, Katy Gorentz, Endang Budi Hastuti, Aulia Human, Ciptasari Prabawanti,
Anton Purnama, Tetty Rachmawati, Edhie Rahmat, Elisabeth Rottach, Nanda Sirajulmunir, Revy Sjahrial
Ministry of Health Indonesia | Provincial Health Office, DKI Jakarta | District Health Offices, East, Central, North, South
and West Jakarta | Participating health facilities

Terima kasih!





























