Embed Size (px)
Citation preview

1
Title page
Induction chemotherapy plus concurrent chemoradiotherapy in endemic
nasopharyngeal carcinoma: individual patient data pooled analysis of four
randomized trials
Running title: Pooled analysis of IC + CCRT for NPC
Authors list: Yu-Pei Chen, M.D.,1* Ling-Long Tang, M.D.,
1* Qi Yang, M.D.,
2,*
Sharon-Shuxian Poh, M.D.,3* Edwin P Hui, M.D.,
4* Anthony TC Chan, M.D.,
4
Whee-Sze Ong, MAppStats,5 Terence Tan, FRCR,
3 Joseph Wee, FRCR,
3 Wen-Fei Li,
M.D.,1 Lei Chen, M.D.,
1 Brigette BY Ma, M.D.,
4 Macy Tong, FRCR,
4 Sze-Huey Tan,
Ph.D.,5 Shie-Lee Cheah, FRCR,
3 Kam-Weng Fong, FRCR,
3 Kiattisa Sommat,
FRCR,3 Yoke Lim Soong, FRCR,
3 Ying Guo, M.D.,
6 Ai-Hua Lin, M.D.,
7 Ying Sun,
M.D., Ph.D.,1 Ming-Huang Hong, M.D.,
2 Su- Mei Cao, M.D.,
2† Ming-Yuan Chen,
M.D.,2†
AND Jun Ma, M.D.1†
Affiliations list:
1 Department of Radiation Oncology, Sun Yat-sen University Cancer Center, State
Key Laboratory of Oncology in South China, Collaborative Innovation Center for
Cancer Medicine, People’s Republic of China
2 Department of Nasopharyngeal Carcinoma, Sun Yat-sen University Cancer Center,
State Key Laboratory of Oncology in South China, Collaborative Innovation Center
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

2
for Cancer Medicine, People’s Republic of China
3 Division of Radiation Oncology, National Cancer Centre, Singapore
4 Partner State Key Laboratory of Oncology in South China, Sir Y K Pao Centre for
Cancer, Department of Clinical Oncology, Hong Kong Cancer Institute and Prince of
Wales Hospital, The Chinese University of Hong Kong
5 Division of Clinical Trials and Epidemiological Sciences, National Cancer Centre,
Singapore
6 Clinical Trials Centre, Sun Yat-sen University Cancer Centre, State Key Laboratory
of Oncology in South China, Collaborative Innovation Centre of Cancer Medicine,
Guangzhou, People’s Republic of China
7 Department of Medical Statistics and Epidemiology, School of Public Health, Sun
Yat-sen University, Guangzhou, People’s Republic of China
* These authors contributed equally to this work.
†Corresponding authors:
Jun Ma, Department of Radiation Oncology, Sun Yat-sen University Cancer Center,
State Key Laboratory of Oncology in South China, Collaborative Innovation Center
of Cancer Medicine, 651 Dongfeng Road East, Guangzhou 510060, People’s
Republic of China.
Tel.:+86-20-87343469; Fax:+86-20-87343295
E-mail: [email protected]
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

3
Ming-Yuan Chen, Department of Nasopharyngeal Carcinoma, Sun Yat-sen
University Cancer Center, State Key Laboratory of Oncology in South China,
Collaborative Innovation Center of Cancer Medicine, 651 Dongfeng Road East,
Guangzhou 510060, People’s Republic of China.
Tel.:+86-20-87343469; Fax:+86-20-87343295
E-mail: [email protected]
Su-Mei Cao, Department of Nasopharyngeal Carcinoma, Sun Yat-sen University
Cancer Center, State Key Laboratory of Oncology in South China, Collaborative
Innovation Center of Cancer Medicine, 651 Dongfeng Road East, Guangzhou 510060,
People’s Republic of China.
Tel.:+86-20-87343469; Fax:+86-20-87343295
E-mail: [email protected]
Key words: Induction chemotherapy; Concurrent chemoradiotherapy;
Nasopharyngeal carcinoma; Pooled analysis; Randomized controlled trial
Acknowledgements
We thank the anonymous reviewers and editors for their insightful comments and great
efforts to improve this manuscript. We thank the Clinical Trials Centre, Sun Yat-sen
University Cancer Centre, for assistance with data interpretation.
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

4
Grant Support
This work was supported by grants from the National Science & Technology Pillar
Program during the Twelfth Five-year Plan Period (2014BAI09B10), the Natural
Science Foundation of Guang Dong Province (2017A030312003), the National Key
R&D Program of China (2016YFC0902000), the National Natural Science Foundation
of China (81572658), the Innovation Team Development Plan of the Ministry of
Education (No. IR_17R110), and the Overseas Expertise Introduction Project for
Discipline Innovation (111 Project, B14035).
Conflict of Interest Statement
We declare that we have no conflicts of interest.
Word count: 3680
The total number of tables: 1
The total number of figures: 5
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

5
Translational Relevance
Due to uneven geographical distribution and small number of randomized trials
available, the value of additional induction chemotherapy (IC) to concurrent
chemoradiotherapy (CCRT) in nasopharyngeal carcinoma (NPC) remains
controversial. We performed an individual patient data (IPD) pooled analysis of four
randomized trials from endemic regions to comprehensively evaluate the precise role
of IC+CCRT in locoregionally advanced NPC. Our results indicate the benefits
associated with IC+CCRT versus CCRT alone, including significant improvements in
progression-free survival (PFS) and overall survival (OS), and a reduction in distant
failure; the benefit of IC did not differ among specific patient subgroups. No
statistically significant differences in survival between different IC regimens were
detected. This IPD pooled analysis demonstrate the superiority of additional IC over
CCRT alone in locoregionally advanced NPC, with the survival benefit mainly
associated with improved distant control. IC+CCRT may represent a promising
strategy for NPC in the era of intensity-modulated radiotherapy.
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

6
Abstract
Purpose: Due to uneven geographical distribution and small number of randomized
trials available, the value of additional induction chemotherapy (IC) to concurrent
chemoradiotherapy (CCRT) in nasopharyngeal carcinoma (NPC) remains
controversial. This study performed an individual patient data (IPD) pooled analysis
to better assess the precise role of IC+CCRT in locoregionally advanced NPC.
Experimental Design: Four randomized trials in endemic areas were identified,
representing 1,193 patients; updated IPD were obtained. Progression-free survival
(PFS) and overall survival (OS) were the primary and secondary end-points,
respectively.
Results: Median follow-up was 5.0 years. The hazard ratio (HR) for PFS was 0.70 (95%
CI, 0.56-0.86; P = 0.0009; 9.3% absolute benefit at 5 years) in favor of IC+CCRT
versus CCRT alone. IC+CCRT also improved OS (HR 0.75, 95% CI 0.57-0.99, P =
0.04) and reduced distant failure (HR 0.68, 95% CI 0.51-0.90; P = 0.008). IC+CCRT
had a tendency to improve locoregional control compared with CCRT alone (HR,
0.70; 95% CI, 0.48-1.01; P = 0.06). There was no heterogeneity between trials in any
analysis. No interactions between patient characteristics and treatment effects on PFS
or OS were found. After adding two supplementary trials to provide a more
comprehensive overview, the conclusions remained valid and were strengthened. In a
supplementary Bayesian network analysis, no statistically significant differences in
survival between different IC regimens were detected.
Conclusion: This IPD pooled analysis demonstrate the superiority of additional IC
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

7
over CCRT alone in locoregionally advanced NPC, with the survival benefit mainly
associated with improved distant control.
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

8
Introduction
Nasopharyngeal carcinoma (NPC) is a squamous-cell carcinoma with a unique,
unbalanced endemic distribution, with an especially high prevalence in east and
southeast Asia (1). Non-keratinizing (World Health Organization [WHO] types 2 and
3) constitutes most cases of NPC in endemic areas (>95%), whereas keratinizing
disease (type 1) is more common in other regions of the world (1, 2). Unlike other
head and neck cancers, radiotherapy (RT) is the primary treatment modality for
non-disseminated NPC due to its anatomic location and radiosensitivity. The
introduction of intensity-modulated radiotherapy (IMRT) substantially improved
locoregional control, and distant metastasis is now the major pattern of treatment
failure in locoregionally advanced NPC (3).
In recent decades, numerous trials have investigated the value of adding
chemotherapy to RT in NPC. Concurrent chemoradiotherapy (CCRT) is now the
standard treatment for locoregionally advanced disease (1, 4); the updated
Meta-Analysis of Chemotherapy in Nasopharynx Carcinoma (MAC-NPC)
demonstrated CCRT with or without adjuvant chemotherapy (AC) was related to a 5
year survival benefit of 5-12% (5). However, the efficacy of AC after CCRT remains
uncertain, and our latest phase 3 trial observed no significant benefit for CCRT + AC
compared to CCRT alone (6). Moreover, the toxic effects and the low rate of
compliance to AC also need to be taken into account (4). Compared to AC, induction
chemotherapy (IC) offers the advantages of better tolerability and early eradication of
micrometastases (7), thus sequential IC followed by CCRT may represent a promising
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

9
strategy for NPC in the IMRT era.
Though four reported randomized controlled trials (RCTs) have compared IC +
CCRT versus CCRT alone in the endemic area, their conclusions remain controversial.
A trial at the Prince of Wales Hospital (PWH), Hong Kong, compared induction
docetaxel and cisplatin (TP) followed by CCRT with CCRT alone in stage III-IVB
NPC, and found IC significantly improved 3-year overall survival (OS) and had a
non-significant effect on progression-free survival (PFS) (8). The National Cancer
Centre Singapore (NCCS) trial adopted gemcitabine, carboplatin and paclitaxel (GCP)
IC, and no significant differences in survival or distant control were observed between
the IC + CCRT and CCRT alone arms (9). Recently, two multicenter phase 3 trials
from Guangzhou (GZ) have been reported: the GZ2008 trial found cisplatin and
fluorouracil (PF) IC significantly improved disease-free survival, with a marginally
significant effect on distant control (10), while the GZ2011 trial found TPF IC
improved failure-free survival, OS and distant control in locoregionally advanced
NPC (11). Recent meta-analyses by the MAC-NPC Collaborative Group did not show
IC + CCRT had obvious superiority over CCRT alone (5, 12). However, these studies
included trials reported before 2013; thus they could not confirm the value of IC +
CCRT considering new RCTs reported in recent years.
Therefore, these controversial results highlight the need to determine whether the
addition of IC to CCRT provides any additional benefit in NPC. Given the paucity of
studies and potentially insufficient power to detect small improvements in the specific
end-points of each trial, the investigators of the four endemic trials launched an
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

10
individual patient data (IPD) pooled analysis. We aimed to better determine the
efficacy, compliance rates and toxicity, as well as treatment interactions within
specific patient subgroups, of adding IC to CCRT in locoregionally advanced NPC. To
our knowledge, this is the first IPD analysis to provide a comprehensive overview of
the precise role of additional IC in NPC.
Materials and Methods
Study selection
We searched PubMed and EMBASE for RCTs in NPC using “nasopharyngeal
neoplasms,” “nasopharyngeal tumors” and “nasopharyngeal cancers” as keywords
and “clinical trials” or “randomized controlled trial” as limits; the search was
supplemented by searching the bibliographies of the retrieved articles. The final
search date was June 24, 2017. To be eligible, trials had to be from endemic regions as
indicated by Chua and colleagues (e.g., east and southeast Asia, etc.) (13), have a
randomized design, include patients with non-metastatic NPC treated with definitive
conventional fractionated radiotherapy, and had to compare IC followed by CCRT
with CCRT alone.
The selection process is shown in Supplementary Figure S1. Eventually, four
RCTs were found to be eligible for this study: the PWH, NCCS, GZ2008 and GZ2011
trials (8-11). During the search process, we identified two other trials that assessed IC
followed by CCRT: one was conducted in an non-endemic area (the Hellenic
Cooperative Oncology Group [HeCOG] trial) (14), and the other compared IC +
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

11
CCRT with CCRT + AC (the NPC0501 trial) (15). These two RCTs were included in
supplementary analysis to provide a more comprehensive overview of the role of
additional IC.
Data collection
For the eligible RCTs, an updated IPD was established for patient and tumor
characteristics, treatment details, date of randomization, failure and death, pattern of
failure, cause of death, and adverse events during treatment. The studies were
conducted in compliance with the Declaration of Helsinki and local regulatory
requirements. Written informed consent was obtained from all patients; this study was
approved by the ethics committee or institutional review boards at each institution.
We examined the randomization process and intention-to-treat basis for each trial.
Randomization was assessed by checking the methods used and balance between
baseline characteristics. Patient follow-up was also compared between treatment
groups in each trial (16). The analyses were sent to the investigators for review and
validation, and all discrepancies were discussed by the investigators to reach
consensus.
For the two RCTs included in the supplementary analysis, we reviewed the
associated articles and previous IPD meta-analysis on NPC (5, 14, 15), then
summarized the trial characteristics and extracted survival data (obtained directly or
using the methods detailed by Parmar et al. (17)). We also assessed the quality of
these trials with respect to randomization and the intention-to-treat principle.
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

12
Outcomes
The primary end-point was PFS, calculated from date of randomization to
locoregional failure, distant failure or death from any cause, whichever occurred first.
The secondary end-points were OS, distant control (DC), locoregional control (LRC),
and cancer and non-cancer deaths. OS was calculated from date of randomization to
date of death from any cause. DC and LRC were defined as the time from
randomization to the occurrence of distant or locoregional failure, respectively.
Patients with locoregional failure as a first event were censored for distant failure, and
vice versa. If both distant failure and locoregional failure occurred at the same time,
patients were considered to have a distant failure event only. Patients without distant
and locoregional failure were censored at the date of death or last follow-up if still
alive. Persistent primary/nodal disease was classified as locoregional failure.
Surviving patients without any event for all end-points were censored at date of last
follow-up. Deaths attributed to known causes other than NPC for patients with no
reported progression were defined as non-cancer deaths. All other deaths were defined
as cancer deaths, including deaths from NPC, deaths from any cause in patients with
previous progression and deaths from unknown causes. This definition has been
adopted by the MAC-NPC Collaborative Group (5), as it prevents underestimation of
deaths related to cancer and is less biased than other methods (18).
Statistical analysis
We performed analysis based on the intention-to-treat principle. Survival analyses
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

13
were stratified by trial; the observed minus the expected number of deaths (O-E) and
its variance was used to calculate individual and overall pooled hazard ratios (HRs)
using a fixed effect model (17). Heterogeneity across trials was examined using the χ2
test and I2 statistic (19). Statistically significant heterogeneity was defined as a χ
2
P-value < 0.1 or an I2 statistic > 50%. If obvious heterogeneity existed, the
Dersimonian and Laird random effects model was adopted (20).
Median follow-up was calculated via the reverse Kaplan-Meier method (21). The
estimated Kaplan-Meier survival curves for the two treatment groups were plotted
(22), and the absolute benefits at 3 and 5 years and 95% confidence intervals (CIs)
were calculated (18). The interactions between treatment effect and patient subgroups
(i.e., sex, age, tumor category, nodal category, clinical stage, and radiotherapy
technique) were estimated with an interaction test, by adopting a single Cox model
stratified by trial and containing treatment effect, covariate (e.g., sex) effect, and
treatment–covariate interaction (one-stage model method) (23). An insignificant P
value in the interaction test indicates the effect in the experimental arm versus control
arm did not differ among that specific covariate group.
A supplementary analysis of PFS and OS between the experimental and control
groups was performed, including both the eligible and supplementary RCTs.
Moreover, to compare the potential differences in efficacy between different IC
regimens, we performed a supplementary Bayesian network analysis including all six
trials. The network analysis within a Bayesian framework using Markov chain Monte
Carlo methods were built using the model proposed by Woods and colleagues (24);
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

14
treatment effects were estimated by posterior means with corresponding 95% credible
intervals (CrIs) (25). The fixed effects model was adopted as it resulted in lower
deviance information criterion (DIC) statistics (DIC provides a measure of model fit
that penalizes model complexity, with lower values suggesting a simpler model) (26).
We did not assess the probability of treatment ranking as it could be produced even
without clear statistical meaning, which is misleading; detailed methods have been
described in our previous study (4). All tests were two-sided. Statistical analyses were
performed using STATA version 12.0 (Stata Corporation, College Station, TX, USA)
and WinBUGS 1.4.3 (MRC Biostatistics Unit, Cambridge, UK).
Results
Trial and patient characteristics
Table 1 summarizes the key features of the PWH, NCCS, GZ2008, and GZ2011 trials.
With respect to the intention-to-treat principle, all randomized patients in all four
trials were analyzed; data was not available for only eight patients in the NCCS trial,
who were either found ineligible on retrospective review or withdrew before receiving
treatment. Overall, a total of 1,193 patients were included in the current analysis, with
599 and 594 patients allocated to the IC + CCRT and CCRT arms, respectively. None
of the four trials demonstrated unbalanced baseline characteristics between treatment
arms. The median follow-up was 5.0 years; no major bias appeared between treatment
arms in any trial as indicated by the reverse Kaplan-Meier curves. All trials recruited
patients with WHO histological type 2 or 3 NPC. The patient characteristics for the
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

15
four eligible trials are summarized in Supplementary Table S1 and the two
supplementary trials are described in Supplementary Table S2.
Efficacy of IC + CCRT versus CCRT
The disease status and patterns of failure are summarized in Supplementary Table S3.
Overall, 208/1,193 (17%) patients died and 311/1,193 (26%) patients experienced
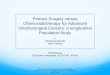
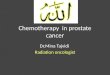
disease progression. IC + CCRT improved PFS compared to CCRT alone (HR, 0.70;
95% CI, 0.56-0.86; P = 0.0009; from 64.6% to 73.9% at 5 years] (Fig. 1A; Fig. 2A).
IC + CCRT also improved OS, with an HR of death of 0.75 (95% CI, 0.57 to 0.99; P
= 0.04) and 5.5% improvement at 5 years (Fig. 1B; Fig. 2B).
IC + CCRT was associated with a significantly lower rate of distant failure than
CCRT alone (HR, 0.68; 95% CI, 0.51-0.90; P = 0.008; absolute reduction from 84.8%
to 78.3% at 5 years) (Fig. 1C; Fig. 2C). No significant difference in locoregional
control was observed between IC + CCRT and CCRT alone, though IC + CCRT had a
tendency to improve LRC (HR, 0.70; 95% CI, 0.48-1.01; P = 0.06; Fig. 1D; Fig. 2D).
To confirm whether the results were sensitive to the choice of a fixed effects model as
opposed to a random effects model, we also calculated pooled HRs and corresponding
95% CIs using the random effects model. The results were the same as those
calculated with the fixed effects model. This is not surprising as the I2 statistic
(defined as variation in effect size attributable to heterogeneity) was equal to 0% for
all end-points (Fig. 1), which means no variation attributable to heterogeneity was
detected, and effect size was not affected by the model used.
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

16
In total, 193 (16%) cancer deaths and 15 (1%) non-cancer deaths occurred. IC +
CCRT tended to reduce the risk of death, with an absolute difference of 4.8% (from
20.1% to 15.3%) at 5 years; there was no obvious difference in non-cancer deaths
between the two arms (Fig. 3).
Treatment compliance and toxicity
Of the 599 patients randomized to the IC + CCRT arm, 578 (96%) received at least
one cycle of IC, and 542 (90%) received IC as planned despite relatively lower
compliance to the TPF regimen (88%; Supplementary Table S4). In total, 566/599
(94%) patients in the IC + CCRT arm and 564/594 (95%) in the CCRT arm initiated
concurrent chemotherapy. Compliance to concurrent chemotherapy was significantly
different between arms: more patients completed at least five/two cycles (if
eight/three cycles were planned) of concurrent chemotherapy in the CCRT arm than
the IC + CCRT arm (92% vs. 87%). No obvious differences in the numbers of
patients starting and completing RT were observed between the IC + CCRT and
CCRT alone arms.
Supplementary Table S5 summarizes the major grade 3-4 adverse events. During
IC, the most common toxic effect was neutropenia (35%), followed by leukopenia
(20%). Other toxicities were not common, with incidences lower than 10%. During
CCRT, adverse events were similar between the two arms, though the IC + CCRT
arm experienced significantly higher rates of grade 3 or 4 leukopenia (26% vs. 21%;
P = 0.03) and neutropenia (15% vs. 9%; P = 0.003).
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

17
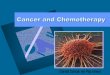
Subgroup analyses for PFS and OS
No significant heterogeneity was observed between trials for any end-point. In order
to determine whether the treatment effect of IC + CCRT versus CCRT alone differs
among specific covariate groups, we performed subgroup analyses for PFS and OS in
patients stratified by the following characteristics (covariates): sex (male, female), age
(< 40, 40-59, ≥ 60), tumor category (T1-2, T3-4), nodal category (N0-1, N2-3),
clinical stage (III, IV), and RT technique (2D-RT, IMRT). No interactions between
these covariates and treatment were observed (all P > 0.1; Fig. 4), which means the
benefit of additional IC did not differ among specific populations. However,
considering the oldest subgroup had relatively few patients, large-scale studies are
warranted to assess the benefit of IC in older patients.
Supplementary analyses
When the two supplementary trials (14, 15) were added to the pooled analysis, the
conclusions remained valid: compared to CCRT ± AC, IC + CCRT improved both
PFS (HR, 0.72; 95% CI, 0.60-0.85; P = 0.0002) and OS (HR, 0.77; 95% CI, 0.62-0.97;
P = 0.02) in locoregionally advanced NPC (Supplementary Fig. S2). Supplementary
Bayesian network analysis was performed to help identify potential differences in the
efficacy of different IC regimens. Supplementary Figure S3 shows the network
established for PFS and OS. Figure 5 summarizes the results of multiple treatment
comparisons; probably due to the lack of relevant trials, no significant differences
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

18
were detected between the different IC regimens. Still, it should be noted that
compared with no IC, only TPF regimen significantly improved both PFS [HR, 0. 70;
95% credible intervals (CrIs), 0.49-0.95] and OS (HR, 0.59; 95% CrI, 0.37-0.92),
suggesting TPF IC may be more effective.
Discussion
This IPD pooled analysis of patients from endemic regions shows the benefits
associated with the use of IC followed by CCRT in locoregionally advanced NPC,
including significant improvements in PFS and OS and a reduction in distant failure.
The absence of interactions between patient characteristics and treatment effects
indicates the benefit of additional IC does not differ among specific populations. The
efficacy of IC + CCRT remained valid and was even strengthened after adding the
supplementary trials, further supporting the conclusions.
Recently, the MAC-NPC Collaborative Group reported no significant differences
between IC + CCRT and CCRT alone with respect to treatment outcomes in NPC in a
network meta-analysis, though additional IC tended to improve distant control (12).
However, this study included trials reported before 2013 and did not include trials
using new IC regimens (e.g., GCP, TPF). Considering the publication of new trials in
recent years, we conducted this pooled analysis to confirm the role of IC followed by
CCRT. We primarily focused on trials conducted in endemic regions. In the original
trial reports, the PWH trial found additional IC significantly increased 3-year OS from
68% to 94%, but failed to detect a significant improvement in PFS (despite an
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

19
obvious trend) (8). The NCCS trial observed a small but insignificant increase in
3-year OS, disease-free survival and distant metastasis-free survival (the absolute
differences were 2%, 8%, and 4%, respectively) (9). The multicenter GZ2008 trial
observed an 8% improvement in 3-year disease-free survival and a marginally
significant increase in distant metastasis-free survival (4% improvement), but no early
OS benefit (10). The GZ2011 trial detected 8% and 6% improvements in 3-year
failure-free survival and OS after IC (both P = 0.03), respectively (11). Combination
of IPD from these four trials enabled a more precise and comprehensive estimation of
the magnitude of the benefits provided by IC + CCRT compared with CCRT alone.
The results of this study demonstrate the superiority of additional IC over CCRT
alone in terms of PFS and OS, with the survival benefit mainly associated with
improved distant control. Considering the wide-spread use of IMRT, it is not
surprising that no significant improvement in locoregional control was observed. To
further validate the conclusions, we included two additional trials (HeCOG and
NPC0501 trials) in the supplementary analysis. The superior efficacy of IC + CCRT
versus CCRT alone remained unchanged, and no heterogeneity was observed.
Considering the varied regimens used for IC, these conclusions should be interpreted
with caution; to provide more information on the efficacy of different IC regimens,
we further conducted a supplementary Bayesian network analysis. Though no
statistically significant differences in PFS or OS between different IC regimens were
detected, the results may favor TPF over other regimens. The efficacy of adding
docetaxel to the PF induction regimen has been demonstrated in locally advanced
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

20
head and neck cancers via large-scale phase 3 trials and IPD pooled analysis (27-29).
The unobvious superiority of one IC regimen over others may be result of a lack of
trials directly comparing different IC regimens. Though TPF has the potential to be a
better choice in IC for NPC, it is still of great significance to identify the optimal IC
regimen. The gemcitabine-based IC regimen may also be effective, as it provides a
significant advantage in advanced NPC (30). Several trials (NCT01872962 and
NCT02512315) are being undertaken to assess other IC regimens, such as
gemcitabine plus cisplatin, and this data should be publicly available in the near future.
Moreover, further trials are required to directly compare different IC regimens.
Compliance to IC was satisfactory, about 90% of patients completed their planned
cycles despite the relatively lower compliance to TPF (88%). During CCRT,
relatively fewer patients in the IC + CCRT arm completed more than half of their
planned cycles of concurrent cisplatin compared to the CCRT alone arm (87% vs.
92%), probably due to patient refusal and treatment toxicities (11). Overall,
compliance to IC and CCRT was satisfactory compared to that of locally advanced
head and neck cancers (about 80% of patients received IC as planned, with about 40%
being able to receive concomitant chemotherapy, and about 70% starting planned RT),
which could promote the clinical use of additional IC in NPC (29). The major grade 3
and 4 toxicities in the IC + CCRT arm were leukopenia (26%), mucositis (24%),
neutropenia (15%), vomiting (12%) and nausea (11%), which were manageable and
reversible; with the exception of leukopenia and neutropenia, adverse events were
similar between arms. Moreover, no obvious differences in deaths due to toxicities
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

21
were observed between groups, further reflecting the acceptable toxicity of additional
IC.
The strengths of this pooled analysis are related to its size and its use of the IPD
that allowed re-analysis of each trial (e.g., standardized multiple end-points).
Nevertheless, we should state the limitations of this analysis. First, these trials
included different IC regimens. However, all regimens were platinum-based, and no
heterogeneity was observed for any end-points. Second, we should be cautious when
interpreting OS benefits. For some of the trials included, the failure to achieve a
significant increase in OS may be explained by a high salvage rate, which dilutes the
OS benefit, or relatively small sample sizes. With increased statistical power, our IPD
analysis could help to detect a significant improvement in OS. Still, whether
additional IC could provide a long-term OS benefit needs to be explored further when
more trials with long-term follow-up results are available. However, the MAC-NPC
Collaborative Group recently demonstrated that PFS and DC were valid surrogate
end-points for OS (31). Thus, considering the significant improvements in PFS and
DC observed for IC+CCRT, additional IC may also provide a long-term survival
benefit. Third, considering the uneven geographical distribution of NPC and the small
number of RCTs available, we also included the HeCOG trial (from a non-endemic
area) and NPC0501 trial (which also included adjuvant chemotherapy) in the
supplementary analyses, which may cause potential bias. Still, the conclusions
remained valid after including these supplementary trials, with no heterogeneity
detected. The supplementary analyses help to provide a more comprehensive
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

22
overview of the value of IC+CCRT in NPC.
The National Comprehensive Cancer Network (NCCN) currently recommends
CCRT + AC for locoregionally advanced NPC (Category 2A); CCRT alone is also an
option (Category 2B) (32). IC + CCRT is recommended as a Category 3 option.
According to the European Society for Medical Oncology (ESMO), platinum-based
IC can be considered for locally advanced disease, but in no case should it negatively
affect the administration of CCRT (33). This updated IPD pooled analysis provides
important information to clarify the precise value of IC + CCRT in NPC. Our study
highlights the importance of identifying high risk patient groups that may benefit most
from IC + CCRT; certain biomarkers such as plasma Epstein-Barr virus (EBV) DNA
load may be helpful for participant selection (NCT02135042). In the future when data
from other trials is available, the MAC-NPC Collaborative Group could provide a
more comprehensive overview to help better understand the optimal treatment
modality for NPC.
In conclusion, this IPD pooled analysis indicates the benefits associated with the
addition of IC to CCRT in locoregionally advanced NPC; the precise value of IC in
specific patient subgroups and the optimal regimens still need further assessment.
References
1. Chua ML, Wee JT, Hui EP, Chan AT. Nasopharyngeal carcinoma. Lancet. 2015.
2. Ou SH, Zell JA, Ziogas A, Anton-Culver H. Epidemiology of nasopharyngeal
carcinoma in the United States: improved survival of Chinese patients within the
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

23
keratinizing squamous cell carcinoma histology. Ann Oncol. 2007;18:29-35.
3. Mao YP, Tang LL, Chen L, Sun Y, Qi ZY, Zhou GQ, et al. Prognostic factors and
failure patterns in non-metastatic nasopharyngeal carcinoma after intensity-modulated
radiotherapy. Chinese journal of cancer. 2016;35:103.
4. Chen YP, Wang ZX, Chen L, Liu X, Tang LL, Mao YP, et al. A Bayesian network
meta-analysis comparing concurrent chemoradiotherapy followed by adjuvant
chemotherapy, concurrent chemoradiotherapy alone and radiotherapy alone in patients
with locoregionally advanced nasopharyngeal carcinoma. Ann Oncol.
2015;26:205-11.
5. Blanchard P, Lee A, Marguet S, Leclercq J, Ng WT, Ma J, et al. Chemotherapy
and radiotherapy in nasopharyngeal carcinoma: an update of the MAC-NPC
meta-analysis. Lancet Oncol. 2015;16:645-55.
6. Chen L, Hu CS, Chen XZ, Hu GQ, Cheng ZB, Sun Y, et al. Concurrent
chemoradiotherapy plus adjuvant chemotherapy versus concurrent chemoradiotherapy
alone in patients with locoregionally advanced nasopharyngeal carcinoma: a phase 3
multicentre randomised controlled trial. Lancet Oncol. 2012;13:163-71.
7. Chua DT, Ma J, Sham JS, Mai HQ, Choy DT, Hong MH, et al. Long-term
survival after cisplatin-based induction chemotherapy and radiotherapy for
nasopharyngeal carcinoma: a pooled data analysis of two phase III trials. J Clin Oncol.
2005;23:1118-24.
8. Hui EP, Ma BB, Leung SF, King AD, Mo F, Kam MK, et al. Randomized phase II
trial of concurrent cisplatin-radiotherapy with or without neoadjuvant docetaxel and
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

24
cisplatin in advanced nasopharyngeal carcinoma. J Clin Oncol. 2009;27:242-9.
9. Tan T, Lim WT, Fong KW, Cheah SL, Soong YL, Ang MK, et al. Concurrent
chemo-radiation with or without induction gemcitabine, Carboplatin, and Paclitaxel: a
randomized, phase 2/3 trial in locally advanced nasopharyngeal carcinoma.
International journal of radiation oncology, biology, physics. 2015;91:952-60.
10. Cao SM, Yang Q, Guo L, Mai HQ, Mo HY, Cao KJ, et al. Neoadjuvant
chemotherapy followed by concurrent chemoradiotherapy versus concurrent
chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: A
phase III multicentre randomised controlled trial. Eur J Cancer. 2017;75:14-23.
11. Sun Y, Li WF, Chen NY, Zhang N, Hu GQ, Xie FY, et al. Induction chemotherapy
plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in
locoregionally advanced nasopharyngeal carcinoma: a phase 3, multicentre,
randomised controlled trial. Lancet Oncol. 2016;17:1509-20.
12. Ribassin-Majed L, Marguet S, Lee AW, Ng WT, Ma J, Chan AT, et al. What Is the
Best Treatment of Locally Advanced Nasopharyngeal Carcinoma? An Individual
Patient Data Network Meta-Analysis. J Clin Oncol. 2016:JCO2016674119.
13. Chua ML, Wee JT, Hui EP, Chan AT. Nasopharyngeal carcinoma. Lancet.
2016;387:1012-24.
14. Fountzilas G, Ciuleanu E, Bobos M, Kalogera-Fountzila A, Eleftheraki AG,
Karayannopoulou G, et al. Induction chemotherapy followed by concomitant
radiotherapy and weekly cisplatin versus the same concomitant chemoradiotherapy in
patients with nasopharyngeal carcinoma: a randomized phase II study conducted by
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

25
the Hellenic Cooperative Oncology Group (HeCOG) with biomarker evaluation. Ann
Oncol. 2012;23:427-35.
15. Lee AW, Ngan RK, Tung SY, Cheng A, Kwong DL, Lu TX, et al. Preliminary
results of trial NPC-0501 evaluating the therapeutic gain by changing from
concurrent-adjuvant to induction-concurrent chemoradiotherapy, changing from
fluorouracil to capecitabine, and changing from conventional to accelerated
radiotherapy fractionation in patients with locoregionally advanced nasopharyngeal
carcinoma. Cancer. 2015;121:1328-38.
16. Stewart LA, Clarke MJ. Practical methodology of meta-analyses (overviews)
using updated individual patient data. Cochrane Working Group. Stat Med.
1995;14:2057-79.
17. Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform
meta-analyses of the published literature for survival endpoints. Stat Med.
1998;17:2815-34.
18. Systemic treatment of early breast cancer by hormonal, cytotoxic, or immune
therapy. 133 randomised trials involving 31,000 recurrences and 24,000 deaths among
75,000 women. Early Breast Cancer Trialists' Collaborative Group. Lancet.
1992;339:1-15.
19. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat
Med. 2002;21:1539-58.
20. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials.
1986;7:177-88.
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

26
21. Schemper M, Smith TL. A note on quantifying follow-up in studies of failure
time. Control Clin Trials. 1996;17:343-6.
22. Pocock SJ, Clayton TC, Altman DG. Survival plots of time-to-event outcomes in
clinical trials: good practice and pitfalls. Lancet. 2002;359:1686-9.
23. Fisher DJ, Copas AJ, Tierney JF, Parmar MK. A critical review of methods for the
assessment of patient-level interactions in individual participant data meta-analysis of
randomized trials, and guidance for practitioners. J Clin Epidemiol. 2011;64:949-67.
24. Woods BS, Hawkins N, Scott DA. Network meta-analysis on the log-hazard scale,
combining count and hazard ratio statistics accounting for multi-arm trials: a tutorial.
BMC medical research methodology. 2010;10:54.
25. Wandel S, Juni P, Tendal B, Nuesch E, Villiger PM, Welton NJ, et al. Effects of
glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee:
network meta-analysis. Bmj. 2010;341:c4675.
26. Spiegelhalter DJ, Best NG, Carlin BP, Linde AVD. Bayesian measures of model
complexity and fit. J R Stat Soc. 2002;64:583-639.
27. Vermorken JB, Remenar E, van Herpen C, Gorlia T, Mesia R, Degardin M, et al.
Cisplatin, fluorouracil, and docetaxel in unresectable head and neck cancer. The New
England journal of medicine. 2007;357:1695-704.
28. Posner MR, Hershock DM, Blajman CR, Mickiewicz E, Winquist E, Gorbounova
V, et al. Cisplatin and fluorouracil alone or with docetaxel in head and neck cancer.
The New England journal of medicine. 2007;357:1705-15.
29. Blanchard P, Bourhis J, Lacas B, Posner MR, Vermorken JB, Cruz Hernandez JJ,
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

27
et al. Taxane-cisplatin-fluorouracil as induction chemotherapy in locally advanced
head and neck cancers: an individual patient data meta-analysis of the meta-analysis
of chemotherapy in head and neck cancer group. J Clin Oncol. 2013;31:2854-60.
30. Zhang L, Huang Y, Hong S, Yang Y, Yu G, Jia J, et al. Gemcitabine plus cisplatin
versus fluorouracil plus cisplatin in recurrent or metastatic nasopharyngeal carcinoma:
a multicentre, randomised, open-label, phase 3 trial. Lancet. 2016;388:1883-92.
31. Rotolo F, Pignon JP, Bourhis J, Marguet S, Leclercq J, Tong Ng W, et al.
Surrogate End Points for Overall Survival in Loco-Regionally Advanced
Nasopharyngeal Carcinoma: An Individual Patient Data Meta-analysis. J Natl Cancer
Inst. 2017;109.
32. NCCN Clinical Practice Guidelines in Oncology: Head and Neck Cancers,
Version 2. 2017 Available at: https://www.nccn.org/professionals/physician_gls/pd
f/head-and-neck.pdf. Accessed <1st July, 2017>.
33. Chan AT, Gregoire V, Lefebvre JL, Licitra L, Hui EP, Leung SF, et al.
Nasopharyngeal cancer: EHNS-ESMO-ESTRO Clinical Practice Guidelines for
diagnosis, treatment and follow-up. Ann Oncol. 2012;23 Suppl 7:vii83-5.
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

28
Figure legends
Figure 1. Forest plots for (A) progression-free survival, (B) overall survival, (C)
distant control and (D) locoregional control. The estimated hazard ratio (HR) for each
individual trial is indicated by the center of the squares and the horizontal line
indicates the 95% confidence interval (CI). The closed diamonds show the overall HR
and 95% CI. HR < 1 and 95% CI excluding 1 indicate improved survival/control for
the experimental versus control arm. A fixed effect model was used. CCRT,
concurrent chemoradiotherapy; GZ, Guangzhou; IC, induction chemotherapy; NCCS,
National Cancer Centre Singapore; O-E, observed minus expected deaths or events;
PWH, Prince of Wales Hospital.
Figure 2. Survival curves for (A) progression-free survival, (B) overall survival, (C)
distant control and (D) locoregional control. CCRT, concurrent chemoradiotherapy;
IC, induction chemotherapy.
Figure 3. Survival curves for cancer and non-cancer deaths. CCRT, concurrent
chemoradiotherapy; IC, induction chemotherapy.
Figure 4. Effect of IC + CCRT versus CCRT alone on (A) progression-free survival
and (B) overall survival, stratified by patient characteristics. 2D-RT, two-dimensional
radiation therapy; CCRT, concurrent chemoradiotherapy; IC, induction chemotherapy;
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

29
IMRT, intensity-modulated radiotherapy.
Figure 5. Bayesian network analysis of (A) progression-free survival and (B) overall
survival. Upper triangles denote pooled hazard ratios (HRs); treatments in rows were
compared with those in the columns. Numbers in parentheses indicate the
corresponding 95% CIs. Red numbers indicate the HRs with Bayesian P < 0.05. A
fixed effect model was used. CCRT, concurrent chemoradiotherapy; CEP, cisplatin,
epirubicin and paclitaxel; GCP, gemcitabine, carboplatin and paclitaxel; IC, induction
chemotherapy; PF, cisplatin and fluorouracil; PX, cisplatin and capecitabine; TP,
docetaxel and cisplatin; TPF, TP and fluorouracil.
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

30
Table 1. Summary of the Four Randomized Controlled Trials Included in the Pooled Analysis
Variable PWH Trial NCCS Trial GZ2008 Trial GZ2011 Trial
Region Hong Kong Singapore Mainland China Mainland China
No. of patients 65 172 476 480
IC + CCRT arm 34 86 238 241
CCRT arm 31 86 238 239
Inclusion period Nov 2002 to Nov 2004 Sep 2004 to Aug 2012 Jun 2008 to Feb 2015 Mar 2011 to Aug 2013
No. of centers 1 1 4 10
Randomization method Central randomization Central randomization Sealed envelopes Sealed envelopes
Stratification Stage (III vs. IV) N stage (N0-1 vs. N2-3) T and N stages (T4N0-1 vs. T1-3N2-3
vs. T4N2-3)
Center, and stage (III vs. IV)
Histology, WHO classification 2-3 2-3 2-3 2-3
Clinical stage III-IVB
(5th AJCC/UICC)
III-IVB
(5th AJCC/UICC)
III-IVB (except T3N0-1)
(6h AJCC/UICC)
III-IVB (except T3-4N0)
(7th AJCC/UICC)
Induction chemotherapy
Regimen TP (2 cycles) GCP (3 cycles) PF (2 cycles) TPF (3 cycles)
Dose Docetaxel 75 mg/m2 d1; cisplatin 75
mg/m2 d1; q3wks
Gemcitabine 1000 mg/m2 d1, d8; carboplatin AUC =
2.5 d1, d8; paclitaxel 70 mg/m2 d1, d8; q3wks
Cisplatin 80 mg/m2 d1; fluorouracil 800
mg/m2 d1-5; q3wks
Docetaxel 60 mg/m2 d1; cisplatin 60
mg/m2 d1; fluorouracil 600 mg/m2
d1-5; q3wks
Concurrent chemotherapy Cisplatin 40 mg/m2 d1, q1wk×8 Cisplatin 40 mg/m2 d1, q1wk×8 Cisplatin 80 mg/m2 d1, q3wks×3 Cisplatin 100 mg/m2 d1, q3wks×3
Radiotherapy*
Technique IMRT (26% of patients), 2D-RT
(74% of patients)
IMRT (98% of patients), 2D-RT (2% of patients) IMRT (43% of patients), 2D-RT (47%
of patients)
IMRT (100% of patients)
Dose 66 Gy (2 Gy/fr) for primary tumor,
residual boost of 7.5 Gy,
IMRT: 69.96 Gy (2.12Gy/fr) for primary tumor and
positive nodes, 60 Gy (1.82 Gy/fr) for negative nodes;
≥ 66 Gy (2–2.33 Gy/fr) for primary
tumor, ≥ 50 Gy for neck lymph nodes
≥ 66 Gy (2–2.27 Gy/fr) for primary
tumor, ≥ 50 Gy for neck lymph nodes
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

31
parapharyngeal boost of 20 Gy 2D-RT: 70 Gy (2 Gy/fr), for primary tumor and
positive nodes, 60 Gy (2 Gy/fr) for negative nodes
Median follow-up (months) 102 (IQR 97-113) 40 (IQR 25-60) 56 (IQR 40-71) 63 (IQR 56-67)
2D-RT = two-dimensional radiation therapy; AJCC = American Joint Committee on Cancer; AUC = area under the curve; CCRT = concurrent
chemoradiotherapy; fr = fraction; GCP = gemcitabine, carboplatin, and paclitaxel; GZ = Guangzhou; IC = induction chemotherapy; IMRT =
intensity-modulated radiotherapy; IQR = interquartile range; NCCS = National Cancer Centre Singapore; PF = cisplatin and fluorouracil; PWH = Prince of
Wales Hospital; q1wk = every 1 week; q3wks = every 3 weeks; TP = docetaxel and cisplatin; TPF = TP and fluorouracil; UICC = International Union Against
Cancer; WHO = World Health Organization.
* The guideline for radiotherapy is described in details in the primary publications of each trial (8-11).
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656

Published OnlineFirst February 5, 2018.Clin Cancer Res Yu-Pei Chen, Ling-Long Tang, Qi Yang, et al. pooled analysis of four randomized trials
datain endemic nasopharyngeal carcinoma: individual patient Induction chemotherapy plus concurrent chemoradiotherapy
Updated version
10.1158/1078-0432.CCR-17-2656doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2018/02/03/1078-0432.CCR-17-2656.DC1
Access the most recent supplemental material at:
Manuscript
Authorbeen edited. Author manuscripts have been peer reviewed and accepted for publication but have not yet
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/early/2018/02/03/1078-0432.CCR-17-2656To request permission to re-use all or part of this article, use this link
Research. on July 3, 2020. © 2018 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on February 5, 2018; DOI: 10.1158/1078-0432.CCR-17-2656