Embed Size (px)
Citation preview

Infection Control and Prevention Annual Education

Director: Chris Abe RN, BSN, CIC, HEM
Epidemiologist: Alice Pong MD, CIC
IC Coordinators: Charlyne Neder LVN, CIC
Megan Medina RN, MSN, MBA, CIC
Sondra Lintz, RN, CNS, MSN, CIC
Molly Johnson, RN, BSN
BS Analyst: Anne Oconer, BS
We can be reached at any time by webpaging
Infection Control Group
Infection Control Team

Learning Objectives
Upon completion of this self study module, the learner will be able to: • Describe the impact of common Hospital Acquired Infections
(HAIs) on the healthcare system
• Identify Infection Control methods to minimize HAIs
• Describe proper hand hygiene technique
• Describe standard and transmission based precautions
• Identify the goals of the antimicrobial stewardship program
• Describe bloodborne pathogens and how to decrease exposure risks

• Infections that patients get while they are in the hospital for another condition
• Can be caused by bacteria, fungi, viruses, or other, less common pathogens
• Factors that contribute to Hospital Acquired Infection (HAI) risk are:
– Central lines
– Urinary catheters
– Surgery
– Transmission of disease between patients/healthcare workers
– Improper cleaning and disinfection practices
– Overuse/inappropriate use of antibiotics

Just the facts…
• More than 722,000 Healthcare Acquired Infections (HAI) occur annually in the U.S.
• Nearly 75,000 die as a direct or indirect cause of their infection.
• 1 in 25 hospital patients contract an HAI during the course of their hospital care
Magill, S. S., Edwards, J. R., Bamberg, W., Beldavs, Z. G., Dumyati, G., Kainer, M. A., & ... Fridkin, S. K. (2014). Multistate point-prevalence survey of health care-associated infections. The New England Journal Of Medicine, 370(13), 1198-1208.

Common HAIs include: • Central line associated bloodstream infections
– Average cost: $45,814
• Pneumonia
– Average cost: $40,144
• Urinary tract infections
– Average cost: $896
• Surgical site infections
– Average cost: $20,785
• Clostridium difficile infections
– Average cost: $11,285
Zimlichman, E., Henderson, D., Tamir, O., Franz, C., Song, P., Yamin, C.K., Keohane, C., Denham, C.R., Bates, D.W. (2013). Health care-associated infections: A meta-analysis of costs and financial impact on the US health care system. JAMA Internal Med, 173(22), 2039-2046.

HAIs are PREVENTABLE!
• Research shows when healthcare teams are aware of infections and take steps to prevent them, some targeted HAIs can decrease by more than 70%
• Prevention takes a conscious effort by everyone, working together to protect patients and save lives
Centers for Disease Control and Prevention. National and State Healthcare Associated Infections: Progress Report. https://www.cdc.gov/HAI/pdfs/progress-report/hai-progress-report.pdf

Impact of Hand Hygiene • Hand hygiene is the most important prevention and
control measure within the hospital.
• Most common mode of transmission of pathogens is by hands of healthcare workers
• 20,000 HAIs are preventable just by doing hand hygiene
Despite knowing the importance of doing hand hygiene, HCW adherence rarely exceeds 40%!

Technique Matters All staff in direct patient contact areas must:
Use alcohol-based sanitizer OR soap and water to routinely disinfect hands. Hand washing with soap and water is required when caring for patient with C. difficile or if hands are visibly soiled.

When To Do Hand Hygiene • Before and after contact with patients
or patient’s surroundings
• Immediately after removing gloves
• Before and after performing clean or
sterile procedures
• Between tasks at different body sites on
same patient (prevents cross contamination)
• Before and after eating, drinking, preparing food, applying cosmetics
• Whenever hands are visibly contaminated (soap and water)
Guideline for Hand Hygiene in Health-care Settings. MMWR 2002; vol. 51, no. RR-16.

Appearance Policy - Infection Prevention Guidelines
• Wear neat, clean clothes made from tightly woven and non-absorbable fabrics. Change clothes if they become soiled or contaminated.
• Bare below elbows – No rings or watches. If a ring is worn, should be limited to simple, flat bands with no grooves or stones.
• Tie long hair back.
• Follow good hand hygiene techniques. Nails must be kept short (1/4 inch) and clean. No artificial extended nails or chipped nail polish.

Clinical Appearance Standards

Respiratory Hygiene & Cough Etiquette
Source containment of infectious respiratory secretions in symptomatic patients.
Beginning at initial point of encounter: • instruct symptomatic persons
to cover mouth/nose when sneezing/coughing
• use tissues and dispose in no-touch receptacle
• observe hand hygiene after soiling of hands with respiratory secretions
• wear surgical mask if tolerated or maintain spatial separation, >3 feet if possible
Do you feel sick? If you have any of the following symptoms:
• Fever in past 24 hours
• Unable to control cough
• Unable to control your secretions
• Nausea, vomiting, diarrhea
• Generally sick feeling
• Feeling unwell to the point of needing to wear a mask
Do not come to work! Stay home until you are feeling better – your coworkers and
patients will appreciate it!

Environmental Cleaning
• Wipe down high touch areas and keyboards once a shift
• Tape should not be used to secure items to surfaces
• No eating food in patient care areas. Only covered drinks allowed at nurses station (not in patient’s room)
• Purses and backpacks should not be stored on nursing station counters
• Remind families to minimize the amount of personal belongings stored in patient’s room
• EVS must be able to clean rooms daily.
• Report any ceiling tile stains or sink backups promptly to POM


• All equipment should be wiped down using Sani wipes
– Stethoscopes
– Otoscopes
– Ophthalmoscopes
– Mobile Devices (rover device)
– Other personal equipment
– Any equipment being shared between rooms/patients
• Bleach wipes must be used to clean all equipment used for C. difficile, Norovirus, Hepatitis A and Adenovirus patients
Cleaning of Equipment
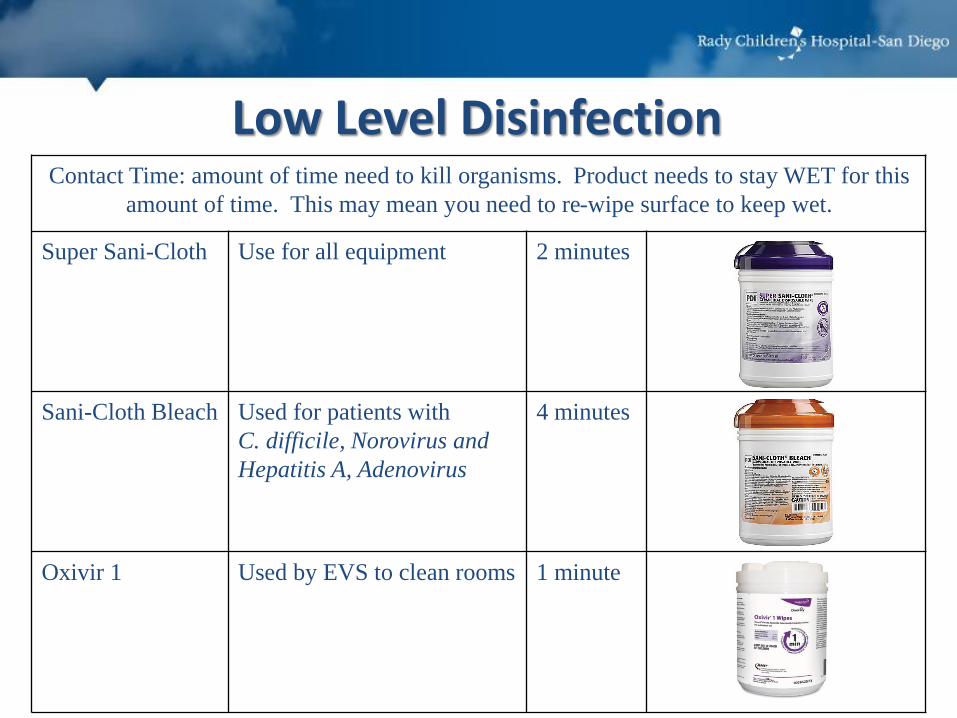
Contact Time: amount of time need to kill organisms. Product needs to stay WET for this
amount of time. This may mean you need to re-wipe surface to keep wet.
Super Sani-Cloth Use for all equipment 2 minutes
Sani-Cloth Bleach Used for patients with
C. difficile, Norovirus and
Hepatitis A, Adenovirus
4 minutes
Oxivir 1 Used by EVS to clean rooms 1 minute
Low Level Disinfection

Processing of equipment (surgical utensils, laryngoscope blades, airways) must begin right after use, before going to SPD for sterilization. • Place items in biohazard bin and
apply enzymatic spray. • Make sure instruments are open so
spray come in contact with all surfaces!
• Bins are stored in dirty utility rooms until picked up.
High Level Disinfection

Infection Prevention Bundles What are bundles?
• Small set of evidence-based interventions that, when implemented together, will result in improved outcomes
What do we use bundles for at RCHSD?
• Central Line Associated Blood Stream Infection (CLABSI) Prevention – Insertion & Maintenance of Central Lines
• Catheter Associated Urinary Tract Infection (CAUTI) Prevention – Insertion & Maintenance of Urinary Catheters
• Ventilator Associated Pneumonia (VAP) Prevention
• Surgical Site Infection (SSI) Prevention

Standard and Transmission Based Precautions
Standard Precautions • Perform hand hygiene
• Use PPE whenever there is an expectation of possible exposure to infectious material
• Follow respiratory hygiene/cough etiquette principles
• Ensure appropriate patient placement
• Properly handle and properly clean and disinfect patient care equipment and instruments/devices
• Clean and disinfect the environment appropriately
• Handle textiles and laundry carefully
• Wear a surgical mask when performing lumbar punctures
• Follow safe injection practices
• Ensure healthcare worker safety including proper handling of needles and other sharps

Transmission-Based Precautions • Used in addition to Standard Precautions
• Used when Standard Precautions may be insufficient to prevent transmission of infectious agent
• Used for patients:
– Known to be infected with an infectious agent • Example: Patient who tested positive for influenza
– Suspected of being infected with an infectious agent • Example: Patient who has symptoms viral a respiratory illness
– Colonized with microorganisms • Example: Patient who has a history of MRSA
• Only the precautions needed to interrupt transmission of the infectious agent are used
• Based on CDC guidelines (see RCHSD policy SM 9-11)
• Includes Contact, Droplet and Airborne Precautions

Regulations & Recommendations for PPE
Occupational Safety and Health Administration (OSHA)
• Issues workplace health and safety recommendations regarding PPE
• Requires employers to: – Provide adequate PPE for employees
– Ensure that PPE is disposable or, if reusable, that it is cleaned, laundered, repaired and stored after use
• Specifies circumstances for which PPE is indicated
Center for Disease Control (CDC)
• Recommends when, what and how to use PPE

Barrier Protection: Personal Protective Equipment (PPE)
Gloves For touching blood, body fluids, secretions,
excretions, contaminated items; for touching mucous membranes and non-intact skin.
Gown During procedures and patient-care activities when contact of clothing/exposed skin with blood/body fluids, secretions, and excretions is anticipated.
Mask, eye protection (goggles), face shield
During procedures and patient-care activities likely to generate splashes or sprays of blood, body fluids, secretions, especially suctioning, endotracheal intubation

RCHSD Isolation Signs

MDROs & Antimicrobial Stewardship

Multi-Drug Resistant Organisms (MDROs)
• Microorganisms resistant to one of more classes of antimicrobial agents
• Organisms: – Methicillin resistant Staphylococcus aureus (MRSA)
– Vancomycin resistant enterococci (VRE)
– Extended spectrum beta lactamase (ESBL) producing bacteria
– Carbapenem resistant
enterobacteriaceae (CRE)
– Other drug resistant Gram
negative organisms
– Clostridium difficile (C. diff)
– Burkholderia cepacia

Patients At Risk For MDROs
• Immunocompromised patients
• Elderly patients
• Higher severity of illness
• Chronic conditions - hemodialysis
• Extended hospital stay
• Intensive Care Unit stay
• Prior antibiotic use
• Transfers from other acute/chronic care facilities
• Poor compliance with Infection Prevention practices

MDRO Prevention Strategies
• Accurate and prompt diagnosis and treatment of infection
• Implementation of appropriate isolation of patient and continued adherence to transmission based precautions
• Judicious use of antimicrobial agents (antimicrobial stewardship)

Goals of RCHSD AMS Program • Optimize dose and duration of antimicrobial use • Decrease overuse of antimicrobials • Decrease selection of multidrug resistant
organisms • Decrease C. difficile infections • Decrease drug side effects of antimicrobials • Decrease cost associated with overuse of
antimicrobials

RCHSD Antimicrobial Stewardship Program Specify and optimize dose, duration and indication of all antibiotics. Use stop dates for antibiotic orders
Follow Appropriate Antibiotic Use Guidelines (pharmacy website)
Antibiotic “time outs” – reassess the need for antibiotics at 48 hours from initiation
Switch from IV to oral antibiotics as soon as possible
Be aware of local hospital and community bacteria resistance patterns (antibiogram available on the Intranet and in EPIC)
Target antibiotic dosing to the site of infection
Bloodborne Pathogens

What Are Bloodborne Pathogens? • Any pathogens found in blood and body fluids that can cause
disease
• The most commonly transmitted blood borne diseases are:
– HIV
– Hepatitis B
– Hepatitis C
• Potential routes of exposure:
– Needle Sticks
– Punctures or cuts from dirty sharps or blades
– Direct contact of infected blood or body fluids with broken skin
– Splashing infected fluids in eyes, nose and mouth

Bodily Fluid Exposures
How can I protect myself?
• Avoid sharps when safer alternatives are available
• Use and activate sharps safety devices
• Wear personal protective equipment: gloves, gowns, face/eye protection
• Properly dispose of used sharps
• Avoid recapping

Bodily Fluid Exposures
If exposed …
• Wash injuries with soap and water
• Flush splashes to the nose, mouth or skin with water
• Irrigate eyes with clean water, saline or sterile irrigants
• Seek medical evaluation immediately
• Complete a Safety Report, notify your supervisor and notify Occupational Health and Safety (OHS).

Special Topics in Infection Control

MRSA Screening Since January 1, 2009, California Law (SB 1058- Nile’s Law) requires MRSA screening with in 24 hours of admission for certain patient populations
Patients that required screening at RCHSD include: • Inpatient surgeries for Ortho, Cardiac & Neuro surgeries • All patient discharged after an admission greater than 30 days • Any patient admitted from a skilled nursing facility • All PICU, NICU & ACU admissions • Patients receiving inpatient dialysis treatment • Patients at high risk for MRSA
- chronic TPN
- High risk pulmonary patients
Any patient admitted to RCHSD with a history of MRSA required Contact Isolation - see SM 9-19: MRSA Screening and Prevention Program

Tuberculosis • San Diego County reported 226 cases active TB in 2018 –
7 cases per 100,000 people – 13 cases were children under 15 years old (4 in children <5)
– 26 cases were Adults 15-24 years old
– 121 cases were Adults aged 25-64
– 66 cases were 65 and older
• RCHSD reported 10 cases of active
Tuberculosis in 2019 – 0 Exposure Incident to Active TB
– 0 Staff Personnel Exposed
– 0 Conversions to TB After Exposure

• Patient and family members wear surgical
mask until placed in proper room.
• Negative Pressure room is required, door
should remain closed.
• No additional visitors allowed.
• Staff must wear a fit tested N95 mask.
• Notify Infection Control as soon as possible so we can provide further guidance/restrictions.
When TB is Suspected

Exposure Management
• All employee exposures are managed by Infection Control (IC) and Occupational Health (OHS)
– Infection Control confirms exposure and completes risk assessment
– OHS provides any monitoring and follow-up
• In case of patient exposure, Infection Control will also do risk assessment and provide recommendations/ guidance to physicians for patient follow-up.

Outbreaks • Infection Control team is in close communication
with San Diego Public Health Department
• When there is an outbreak – goal is to prevent transmission within our facility (and provide guidance to community physicians to prevent exposure in offices)
• Send out reminders to physicians and staff to be on alert and to report any suspected cases to Infection Control

Influenza and Immunization
• Our Employee immunization rate for Influenza is % 99.86
• Annual flu immunization is an important way to reduce the risk of transmission and acquisitions of the flu from health care workers and our patients!

Find Resources &
Data @
RCHSD’s intranet
Infection Prevention Resources

Thank You
for Preventing the Spread of
Infection!

Test Questions 1. What percent Reduction can be achieved when utilizing bundles to decrease Hospital Acquired Infections? a. 90% b. 70% c. 25% d. 50% 2. Which of the following is TRUE regarding hand hygiene practices? a. Hand hygiene is the most important prevention and control measure within the hospital. b. Most common mode of transmission of pathogens is by hands of healthcare workers c. 20,000 HAIs are preventable just by doing hand hygiene d. All of the Above 3. The precautions sign outside of the double room door says Contact and Droplet. You are just dropping of a few items in the patient’s room on the far side of double room. What is the appropriate PPE to wear a. Just a Mask b. Mask, gown, and gloves c. None you are just running in and don’t plan to touch anything anyway d. Just gloves 4. Your new admission is a patient admitted to rule out Tuberculosis. The patient has just arrived and the negative pressure room will not be available for another 30 minutes. Where do you place the patient? a. In the waiting room b. In a private room c. Have the family wait in the hospital lobby d. In a private room with a HEPA filter from Clinical Equipment Distribution (CED)until the negative room is clean. 5. You wipe down the counter in a Clostridium difficile patient’s room. Which product do you use and how long must it remain wet (contact time)? a. Oxivir 1 minute b. Saniwipes, 2 minutes c. Bleach, 4 minutes d. Soap and water, 1 minute 6. True or False. You are feeling ill. Yesterday you had a fever of 102, you have a cough and a runny nose and generally feel bad. You are scheduled to work
tonight. It is ok for you to work since your fever was yesterday and you can just wear a mask and power through. FALSE!
Key 1. a, 2. d, 3. B, 4. d, 5. c, 6. FALSE