Embed Size (px)
Citation preview
Infections in Older Adults
Souha Kanj, MD, FACP, FIDSA, FRCP, FECMM, FESCMIProfessor of Medicine, Head Division of Infectious Diseases,
Chair Infection Control and Prevention Program, AUBMCConsultant Professor, Duke University Medical Center, NC, USA
Outline
Aging populations Burden of infections in the elderly
Influence of aging on infection
Antimicrobial characteristics in the elderly
Antimicrobial use at end of life
Specific infections in the elderly
Immunization of older adults Wrap-up
Outline
Aging populations
Changing Population Demographics
2015• 617 million
people > 65 y• 8.5% of world
population
2050• 1.6 billion
people > 65 y• 16.6% of world
population
He W. US Census Bureau; 2016Bartels SJ. N Engl J Med 2013;368:493
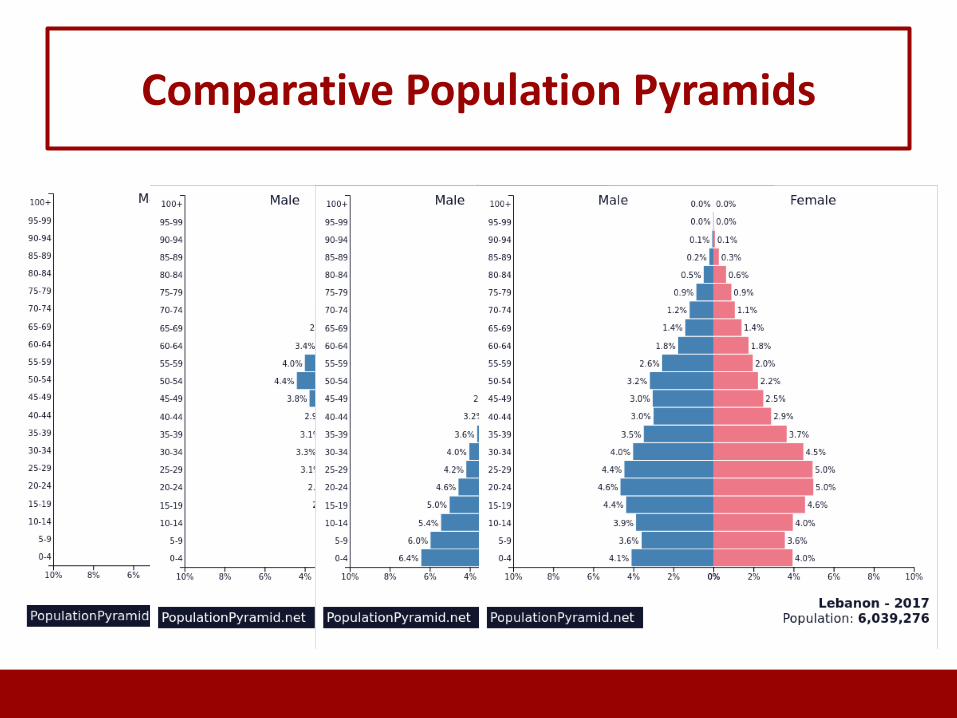
Comparative Population Pyramids
Definition of the “Older Adult”
• Changes over time• Generally accepted to be older than 65 years in developed
countries• United Nations definition: 60+ years• WHO definition in Africa: 50+ years• Recognition of age subsets:– Young old (65-74 y)– Old (75-84 y)– Old-old (85+ y)
Outline
Burdenofinfectionsintheelderly
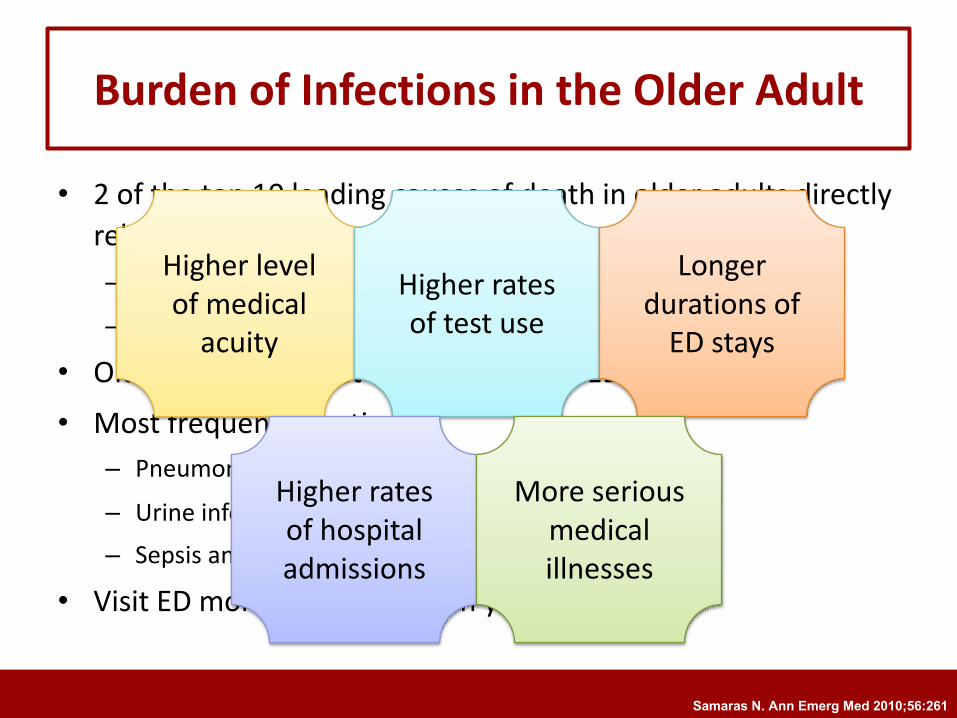
Burden of Infections in the Older Adult
• 2 of the top 10 leading causes of death in older adults directly related to infection– Influenza and pneumonia (infection of the lungs)
– Septicemia/bacteremia (bacteria in the blood)
• Older adults account for up to ¼ of all ED visits• Most frequent infections:
– Pneumonia (25%)
– Urine infection (22%)– Sepsis and bacteremia (18%)
• Visit ED more frequently than younger adults
Higher level of medical
acuity
Higher rates of test use
Longer durations of
ED stays
Higher rates of hospital admissions
More serious medical illnesses
Samaras N. Ann Emerg Med 2010;56:261
Outline
Influence of aging on infection
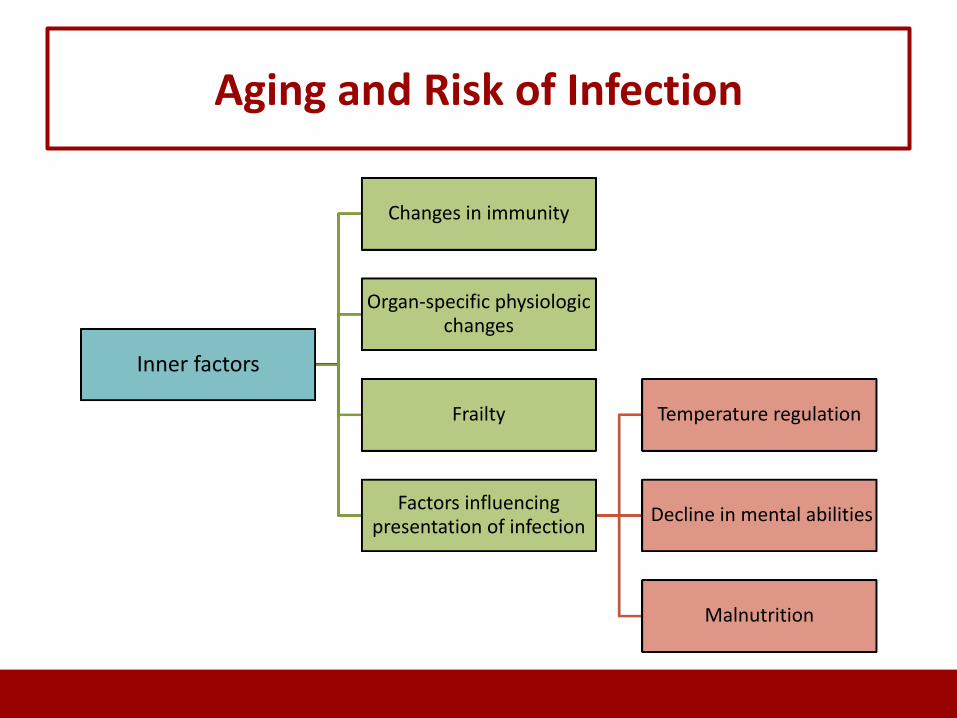
Aging and Risk of Infection
Inner factors
Changes in immunity
Organ-specific physiologic changes
Frailty
Factors influencing presentation of infection
Temperature regulation
Decline in mental abilities
Malnutrition
Changes in Immunity
• Age-related dysfunction of the immune system which leads to enhanced risk of infection
• Total no. of immune cells stable
• But…
• Functional decline in immunity
Gavazzi G. Lancet Infect Dis 2002;2:659
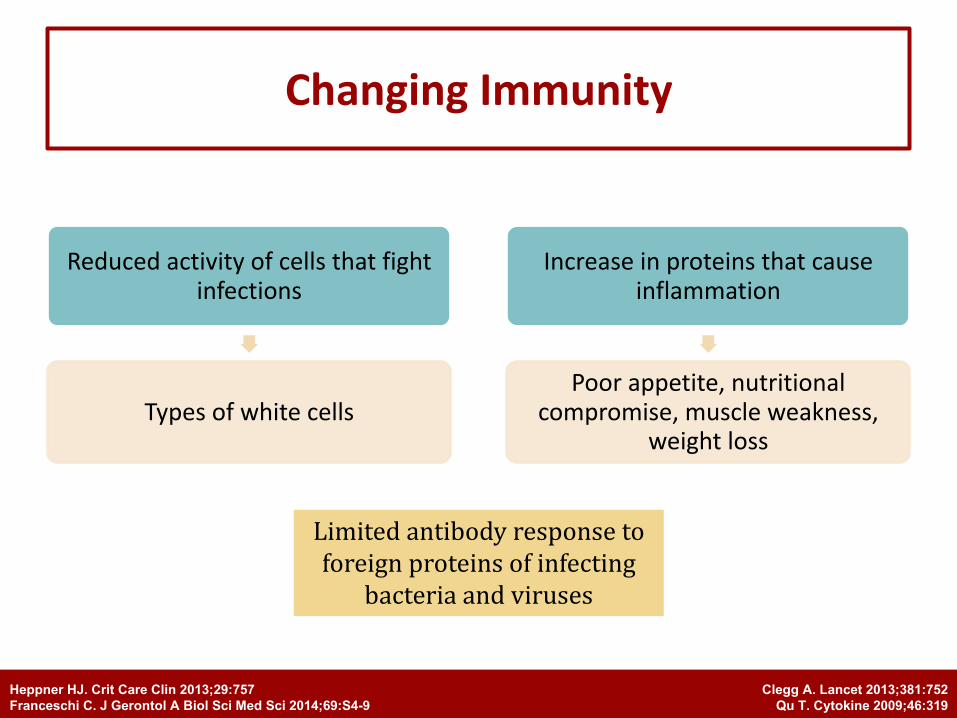
Changing Immunity
Reduced activity of cells that fight infections
Types of white cells
Increase in proteins that cause inflammation
Poor appetite, nutritional compromise, muscle weakness,
weight loss
Clegg A. Lancet 2013;381:752Qu T. Cytokine 2009;46:319
Heppner HJ. Crit Care Clin 2013;29:757Franceschi C. J Gerontol A Biol Sci Med Sci 2014;69:S4-9
Limitedantibodyresponsetoforeignproteinsofinfecting
bacteriaandviruses
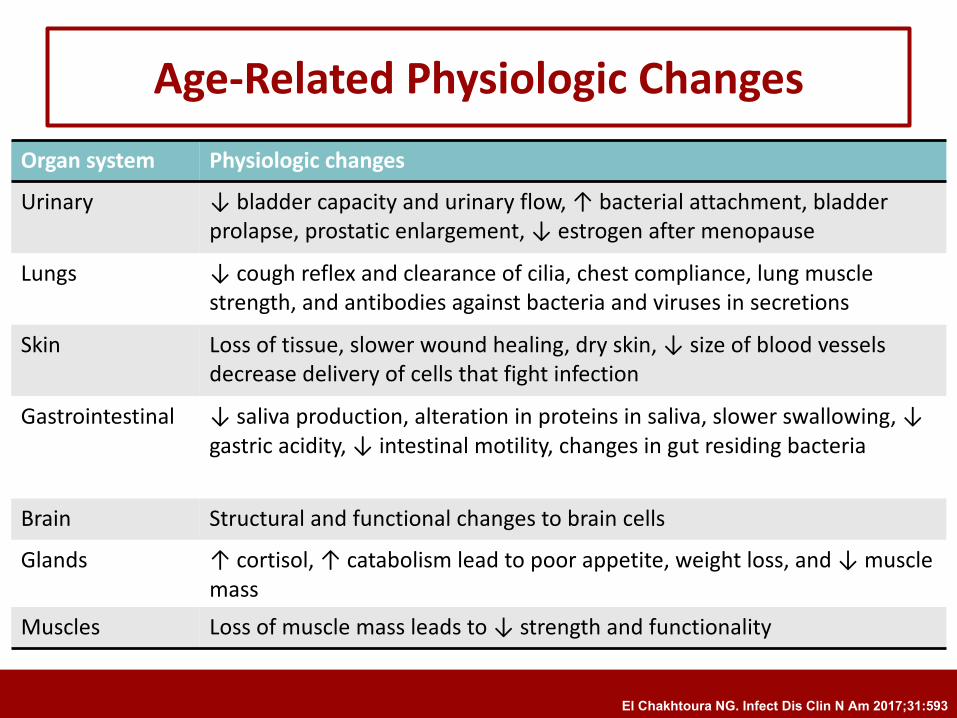
Age-Related Physiologic ChangesOrgan system Physiologic changesUrinary ↓ bladder capacity and urinary flow, ↑ bacterial attachment, bladder
prolapse, prostatic enlargement, ↓ estrogen after menopause
Lungs ↓ cough reflex and clearance of cilia, chest compliance, lung muscle strength, and antibodies against bacteria and viruses in secretions
Skin Loss of tissue, slower wound healing, dry skin, ↓ size of blood vessels decrease delivery of cells that fight infection
Gastrointestinal ↓ saliva production, alteration in proteins in saliva, slower swallowing, ↓ gastric acidity, ↓ intestinal motility, changes in gut residing bacteria
Brain Structural and functional changes to brain cells
Glands ↑ cortisol, ↑ catabolism lead to poor appetite, weight loss, and ↓ muscle mass
Muscles Loss of muscle mass leads to ↓ strength and functionality
El Chakhtoura NG. Infect Dis Clin N Am 2017;31:593
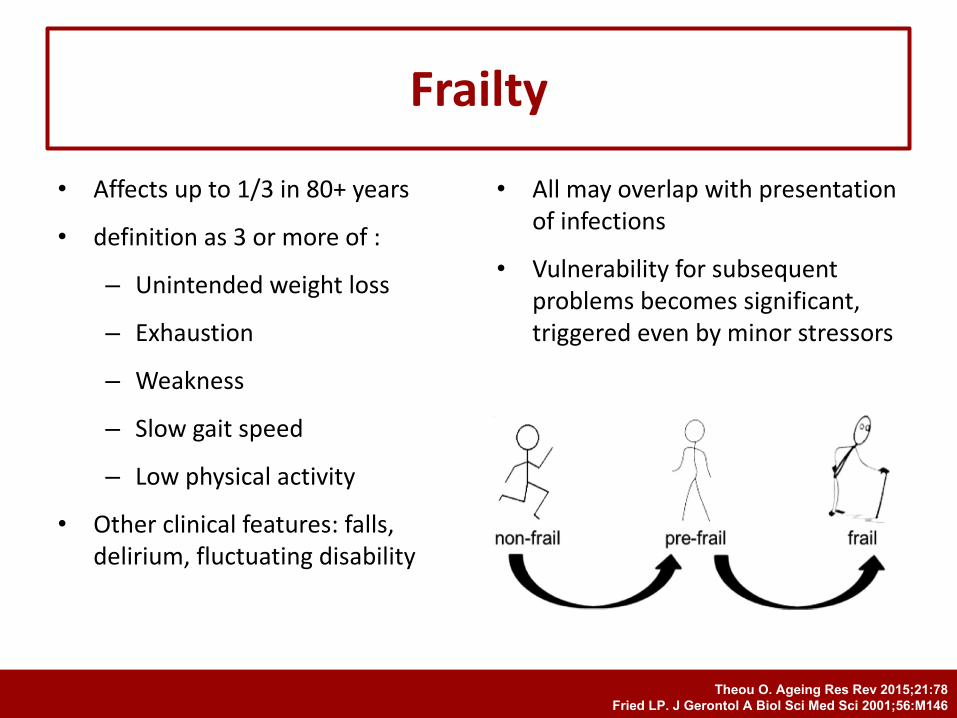
• Affects up to 1/3 in 80+ years
• definition as 3 or more of :
– Unintended weight loss
– Exhaustion
– Weakness
– Slow gait speed
– Low physical activity
• Other clinical features: falls, delirium, fluctuating disability
• All may overlap with presentation of infections
• Vulnerability for subsequent problems becomes significant, triggered even by minor stressors
Frailty
Theou O. Ageing Res Rev 2015;21:78Fried LP. J Gerontol A Biol Sci Med Sci 2001;56:M146
Temperature Regulation
• Temperature regulation:
– Mean body T° ↓ with age, “the older, the colder”
– Fever predicting infection: 70% at 37.8°C– ↑ T° over baseline, occurs in most cases of infection in older adults
• Fever definition in older adults :
– Single oral T° > 37.8°C– Repeated oral T° > 37.2°C or rectal T° > 37.5°C– ↑ T° > 1.1°C over the baseline T°
Norman DC. Clin Infect Dis 2000;31:148Castle SC. Aging Immunol Infect Dis 1993;4:67
Mounting a fever is part of health defense and
absence of fever in response to a serious
infection is a poor sign
High KP. J Am Geriatr Soc 2009;57:375Kluger MJ. Infect Dis Clin North Am 1996;10:1
Decline in Mental Abilities
• In pneumonia, nonspecific presenting symptoms (e.g. generalized weakness, decreased appetite, falls, and delirium) more common in patients > 65 y
• When subjects with dementia were excluded, nonspecific symptoms similar in both groups
– Dementia, not age, explained the difference in clinical presentation of pneumonia
Johnson JC. J Am Geriatr Soc 2000;48:1316Schmidt R. Ann Neurol 2002;52:168
Malnutrition
• Affects 30% of older adults
• More prevalent in institutionalized and hospitalized individuals
• Related to depression, dental problems, disturbances of smell and taste, increased catabolism
• ↑ predisposition to infection
• Partially remediable with nutritional formulas:– ↑ influenza vaccine response
– Less fever
– Fewer newly prescribed antibiotics
Sanford AM. Curr Opin Clin Nutr Metab Care 2017;31:54Langkamp-Henken B. J Am Geriatr Soc 2006;54:1861Carlsson M. J Nutr Health Aging 2013;17:186
Aging and Risk of Infection
Environmental factors
Place of residence
Inappropriate antibiotic use
Place of Residence
• In the United States, approximately 1.4 million people reside in nursing homes:– Nursing home residents share dining, recreation and therapeutic
facilities
– Highly dependent upon health care workers (HCWs) for assistance with daily activities
– Frequent patient transfers between nursing homes and hospitals
• Spread of resistant bacteria (that are difficult to treat with antibiotics) from one setting to the other
Harris-Kojetin L. Vital Health Stat 3 2016;38:1
Outline
Antibiotics Characteristics in the elderly
Special Considerations of Antibiotic Use in the Elderly
• Frail old patients are especially susceptible to the toxic effects of antibiotics because of diminished reserve:– ↓ baseline function of ≥ 1 organs
– ↑ incidence of chronic diseases
– Polypharmacy (↑ in adverse effects and drug interactions)
• Delayed and inadequate dosing of drugs correlates with development of resistance and death
Bellmann-Weiler R. Gerontology 2009;55:241Hubbard RE. Eur J Clin Pharmacol 2013;69:319
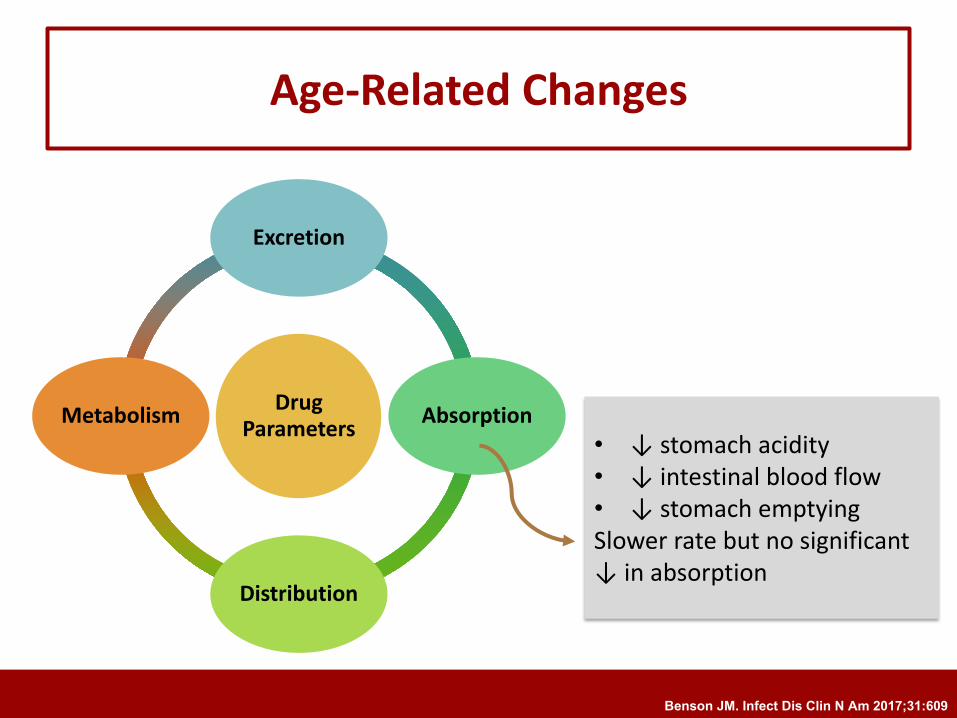
Age-Related Changes
Drug Parameters
Excretion
Absorption
Distribution
Metabolism• ↓ stomach acidity• ↓ intestinal blood flow • ↓ stomach emptyingSlower rate but no significant ↓ in absorption
Benson JM. Infect Dis Clin N Am 2017;31:609
Drug Parameters
Excretion
Absorption
Distribution
Metabolism
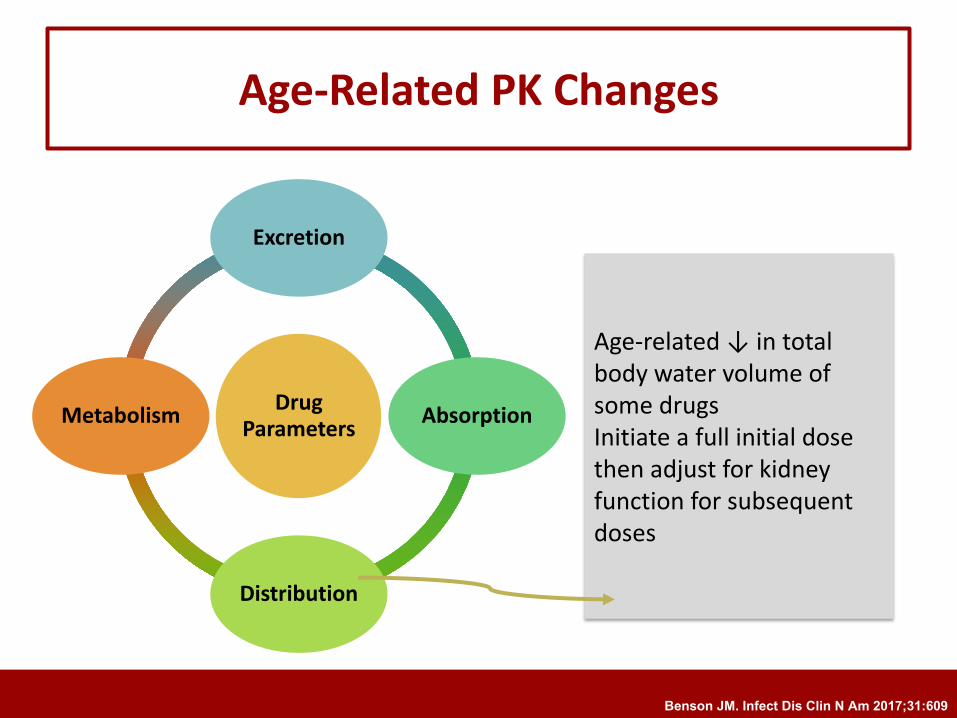
Age-Related PK Changes
Age-related ↓ in total body water volume of some drugsInitiate a full initial dose then adjust for kidney function for subsequent doses
Benson JM. Infect Dis Clin N Am 2017;31:609
Drug Parameters
Excretion
Absorption
Distribution
Metabolism
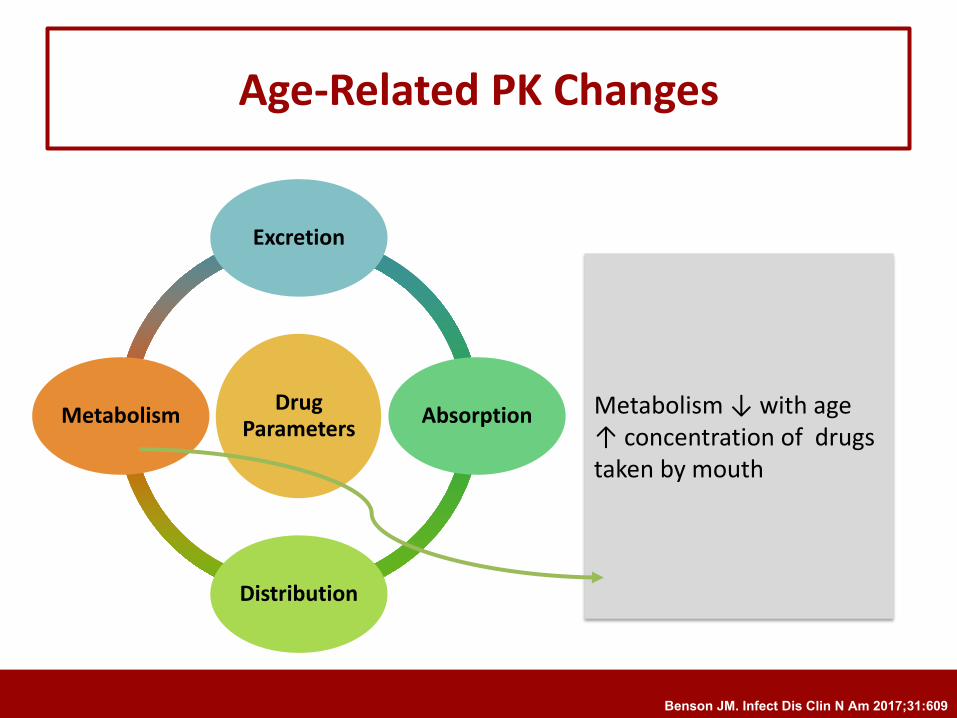
Age-Related PK Changes
Metabolism ↓ with age↑ concentration of drugs taken by mouth
Benson JM. Infect Dis Clin N Am 2017;31:609
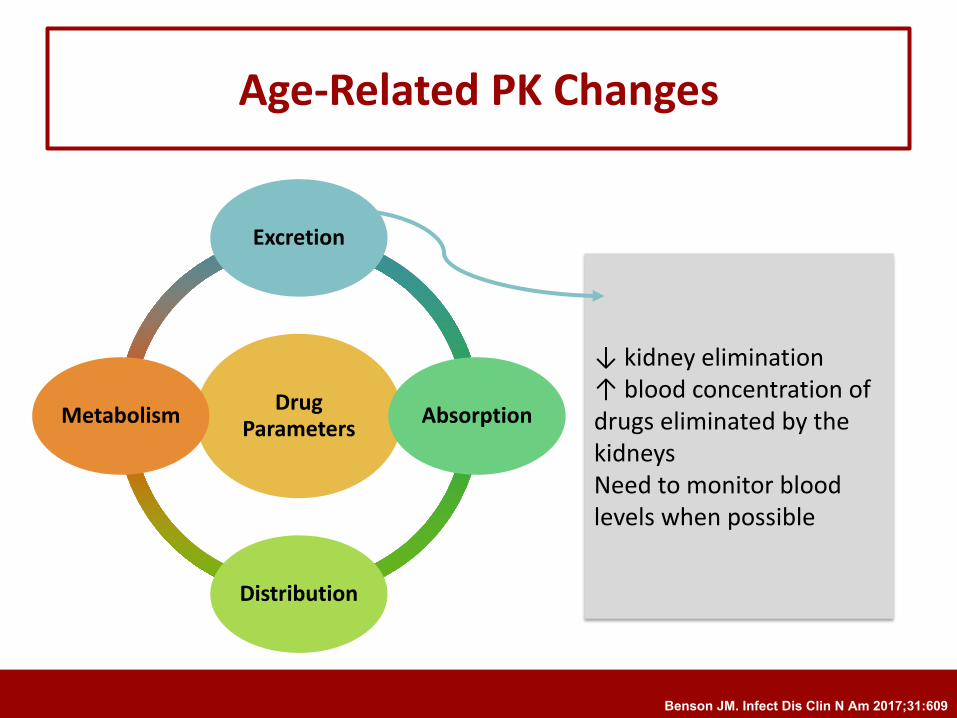
Drug Parameters
Excretion
Absorption
Distribution
Metabolism
Age-Related PK Changes
↓ kidney elimination↑ blood concentration of drugs eliminated by the kidneysNeed to monitor blood levels when possible
Benson JM. Infect Dis Clin N Am 2017;31:609
Considerations in the Older Adult
For some drugs
• Decrease the dose• Maintain or increase dosing frequency
For other drugs
• Maintain same dose• Decrease dosing interval
Benson JM. Infect Dis Clin N Am 2017;31:609
Outline
Antibiotic use at end of life
Overuse of Antibiotics at End of Life
• Up to 88% of patients receive abx in the final weeks of life!!!• No documented infection in 40-80%
• Noninfectious fever important reason to initiate abx• Abx one of the last interventions to be withdrawn or withheld
in terminally-ill patients• Perceived to carry a lower potential for harm
Baghban A. Infect Dis Clin N Am 2017;31:639
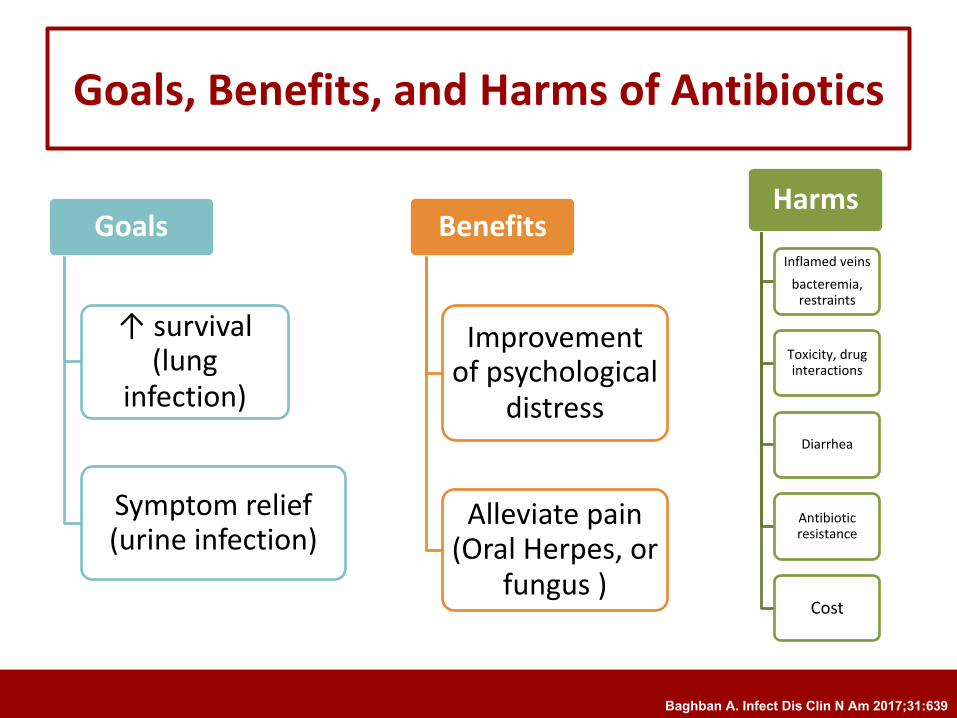
Goals, Benefits, and Harms of Antibiotics
Goals
↑ survival (lung
infection)
Symptom relief (urine infection)
Benefits
Improvement of psychological
distress
Alleviate pain (Oral Herpes, or
fungus )
Harms
Inflamed veinsbacteremia,
restraints
Toxicity, drug interactions
Diarrhea
Antibiotic resistance
Cost
Baghban A. Infect Dis Clin N Am 2017;31:639
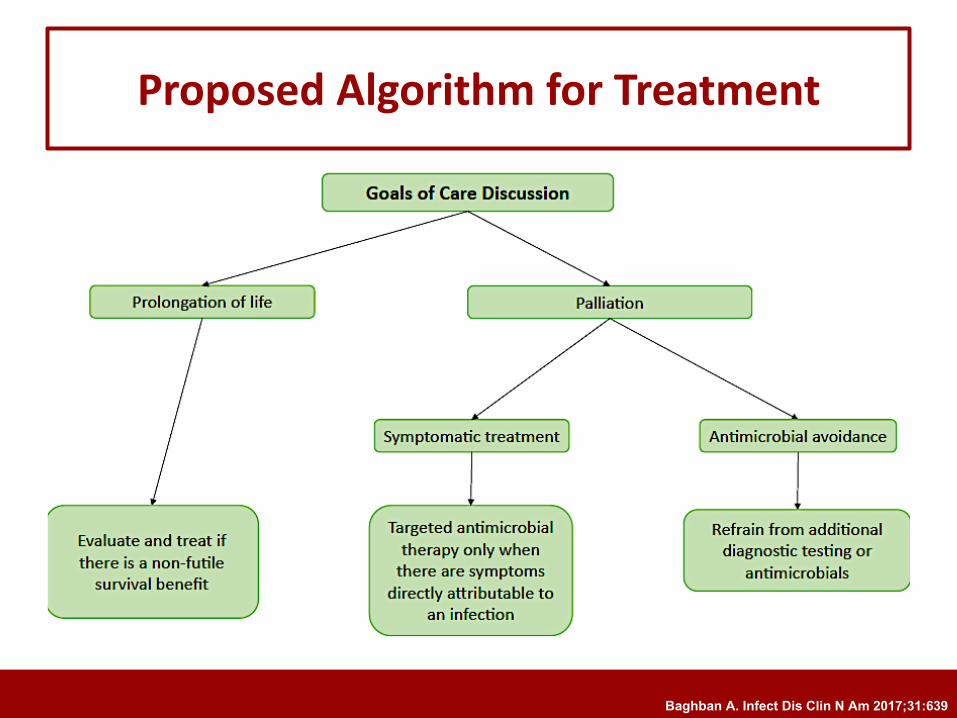
Proposed Algorithm for Treatment
Baghban A. Infect Dis Clin N Am 2017;31:639
Outline
Specific infections in the elderly
Urine
Lung
Influenza
Shingles
Diarrhea
HIVSTDs
Select Infections in the Older Adult
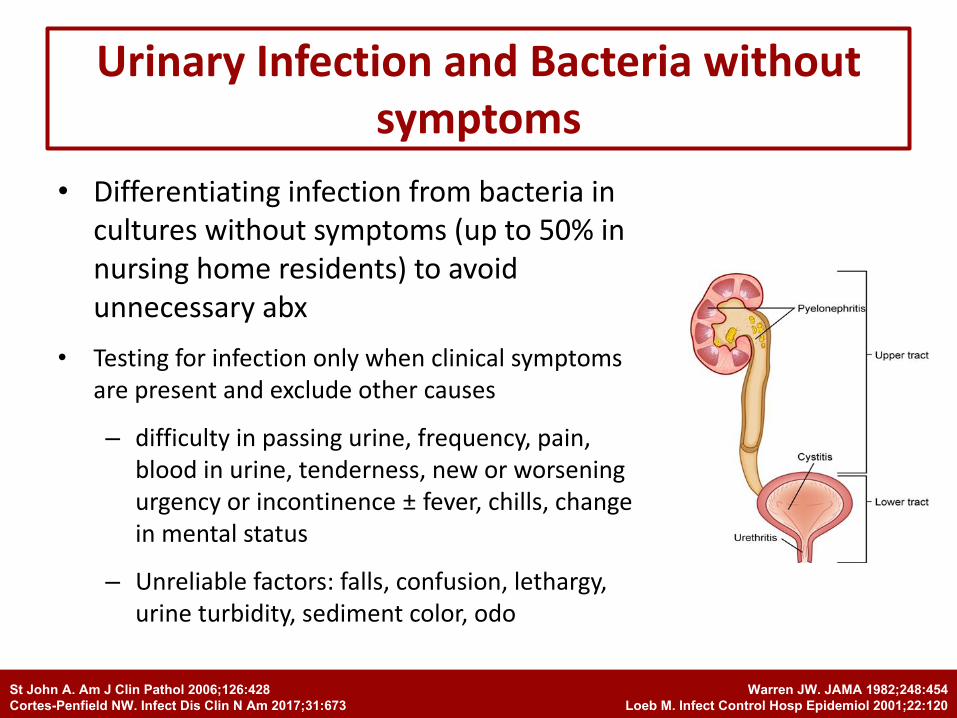
Urinary Infection and Bacteria without symptoms
• Differentiating infection from bacteria in cultures without symptoms (up to 50% in nursing home residents) to avoid unnecessary abx
• Testing for infection only when clinical symptoms are present and exclude other causes
– difficulty in passing urine, frequency, pain, blood in urine, tenderness, new or worsening urgency or incontinence ± fever, chills, change in mental status
– Unreliable factors: falls, confusion, lethargy, urine turbidity, sediment color, odo
Warren JW. JAMA 1982;248:454
Loeb M. Infect Control Hosp Epidemiol 2001;22:120
St John A. Am J Clin Pathol 2006;126:428
Cortes-Penfield NW. Infect Dis Clin N Am 2017;31:673
• Leading cause of death among old patients
• > 40% of hospitalizations • 4 fold ↑ risk > 65 y vs. < 45 y• > 80% require hospitalization• Unidentified bacteria in 77% of
patients• Longer list of bacteria than in young
patients
• Predictors of death:– Residence in nursing home– stroke– Liver disease– Immunosuppression– Malnutrition– Severe pneumonia – Hospital admission
Bacterial Pneumonia (Lung Infection)
Henig O. Infect Dis Clin N Am 2017;31:689
Bacterial Pneumonia:Diagnosis
• Mental status changes might be the only sign
• Pneumonia should be considered with any of: – confusion, delirium, disorientation, loss of appetite, urinary
incontinence, recurrent falls, functional decline, exacerbation of underlying illnesses, low oxygen
• Imaging may be inadequate: Chest X Ray inconclusive
• Blood cultures, sputum culture before antibiotics
Henig O. Infect Dis Clin N Am 2017;31:689
• Many deaths from influenza due to pneumonia or cardiac complications
• Much more common in older adults
• Can spread easily among elderly patients
• 67% become housebound, 1/4 are bedbound
• Classic symptoms
• fever, cough, general aches for 3-7 d
• Presentation in elderly neither classic nor simple
– Only 40-65% fever
– 94% runny nose
– Shortness of breath
– Exacerbation of heart failure
– Exacerbation of bronchitis
• Rapid test positivity as low as 19%
Influenza in the Elderly
Talbot HK. Infect Dis Clin N Am 2017;31:757
• Elderly are candidates for
treatment
• Within 48 h of symptom onset
– Tamiflu
– Flumivir in Lebanon
• Benefits:
– Symptom relief
– ↓ hospital hospital length of
stay
– ↓ death
• Response to vaccination lower in
older patients
• Vaccine efficacy > 50 y 40-60% to
prevent hospitalization when
strains are similar
• 2 licensed vaccines for patients ≥
65 y in the US
1. High dose vaccine
2. MF59 adjuvanted vaccine
• Antiviral prophylaxis after
exposure
Treatment and Prevention of Influenza
Talbot HK. Infect Dis Clin N Am 2017;31:757
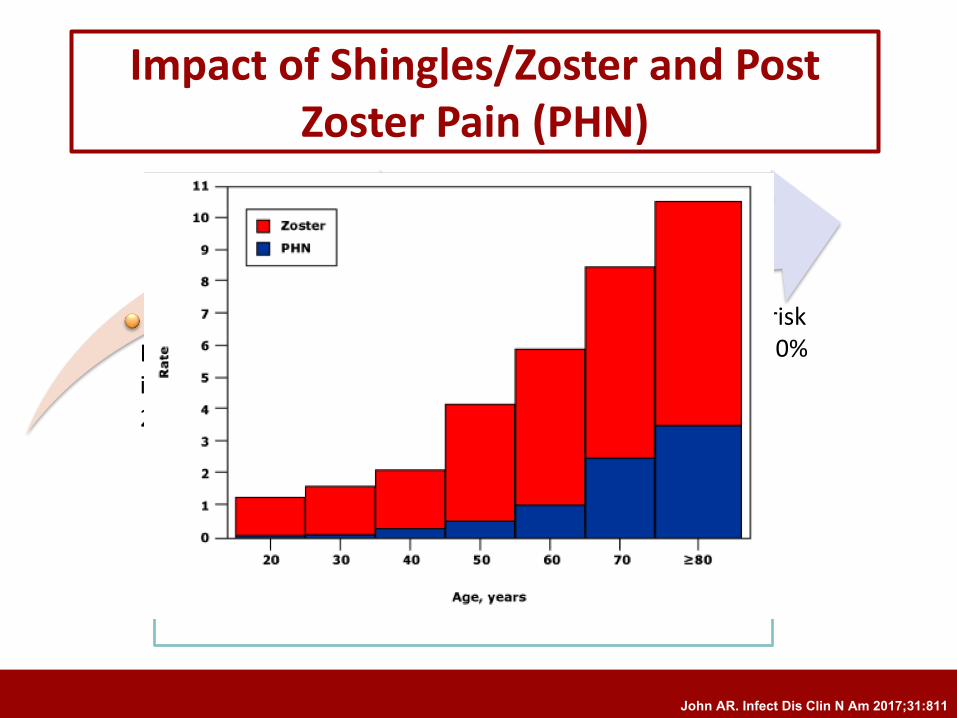
Lifetime incidence20-30%
By 80 y, lifetime incidence 50%
Impact of Shingles/Zoster and Post Zoster Pain (PHN)
Risk of PHN5-30%
By 85 y, risk of PHN 50%
Other complications beyond 50 y:vessel damage causing stroke, bleeding, vision loss,
local neurologic deficits
John AR. Infect Dis Clin N Am 2017;31:811

Locations of Shingles
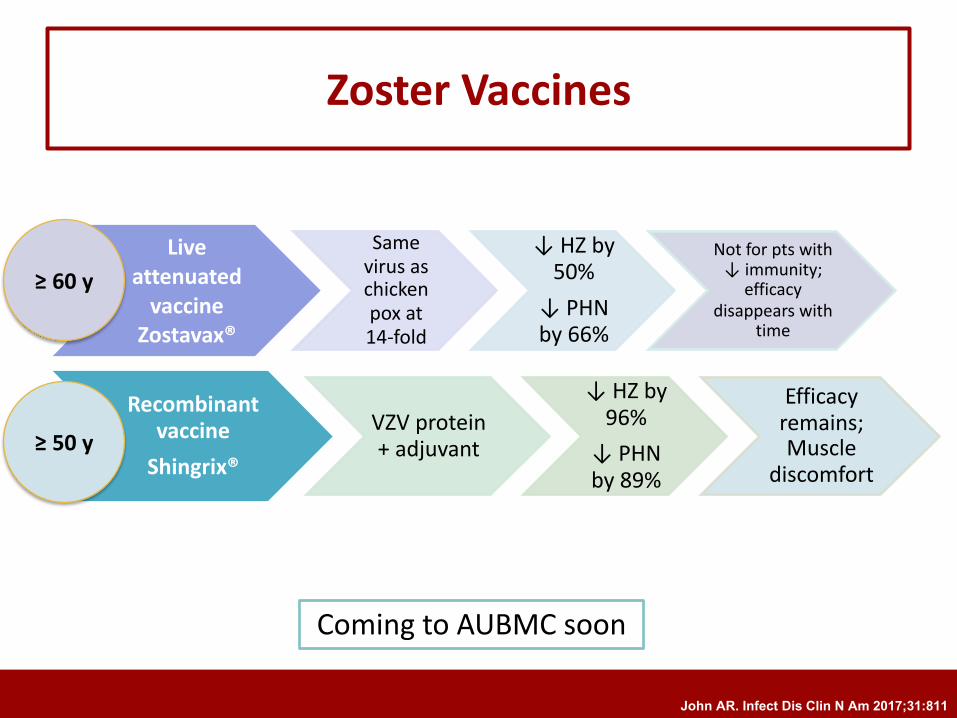
Zoster Vaccines
Live attenuated
vaccineZostavax®
Same virus as chicken pox at 14-fold
↓ HZ by 50%
↓ PHN by 66%
Not for pts with ↓ immunity;
efficacy disappears with
time
Recombinant vaccine
Shingrix®
VZV protein + adjuvant
↓ HZ by 96%
↓ PHN by 89%
Efficacy remains; Muscle
discomfort
≥ 60 y
≥ 50 y
John AR. Infect Dis Clin N Am 2017;31:811
Coming to AUBMC soon
• Elderly are at higher risk
– have ↓ stomach acidity
– ↓ defenses
• Diarrhea can be due to
– Virus
– Bacteria
– Parasites
– Drug side effects including a bacteria from taking antibiotics (Clostridium difficile)
Diarrhea can lead to :• Fever• Belly pain• Dehydration• Kidney injury from dehydration If diarrhea persists we need to know the cause• Implications for:
– Testing– Treatment
• (antibiotics versus no)– Need for isolation
Diarrhea in the Elderly
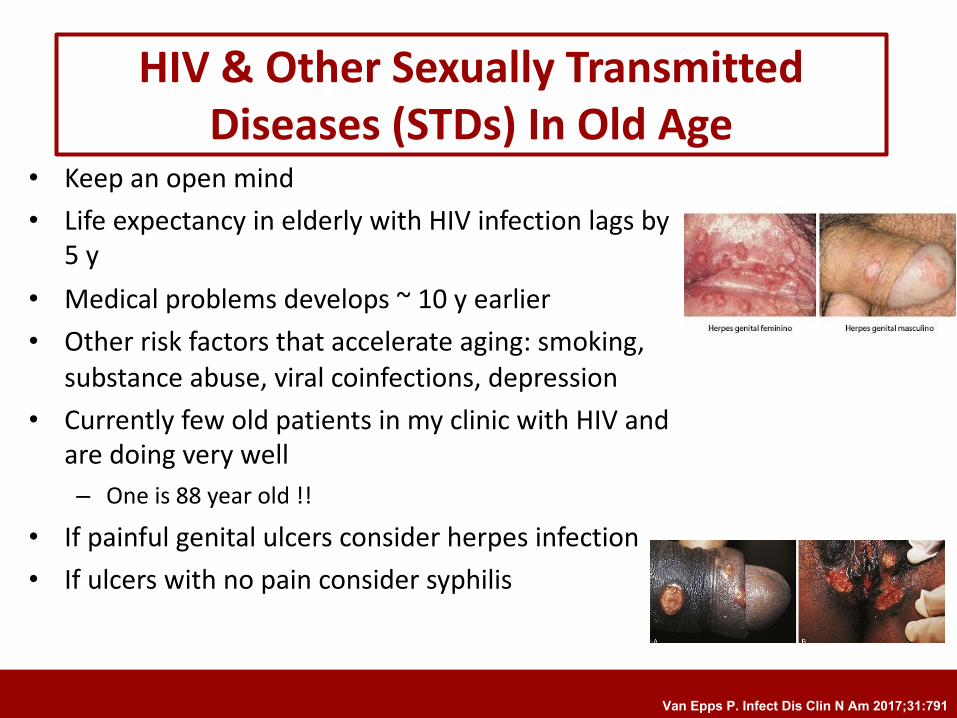
HIV & Other Sexually Transmitted Diseases (STDs) In Old Age
• Keep an open mind• Life expectancy in elderly with HIV infection lags by
5 y• Medical problems develops ~ 10 y earlier• Other risk factors that accelerate aging: smoking,
substance abuse, viral coinfections, depression• Currently few old patients in my clinic with HIV and
are doing very well– One is 88 year old !!
• If painful genital ulcers consider herpes infection• If ulcers with no pain consider syphilis
Van Epps P. Infect Dis Clin N Am 2017;31:791
Outline
Vaccines of older adults
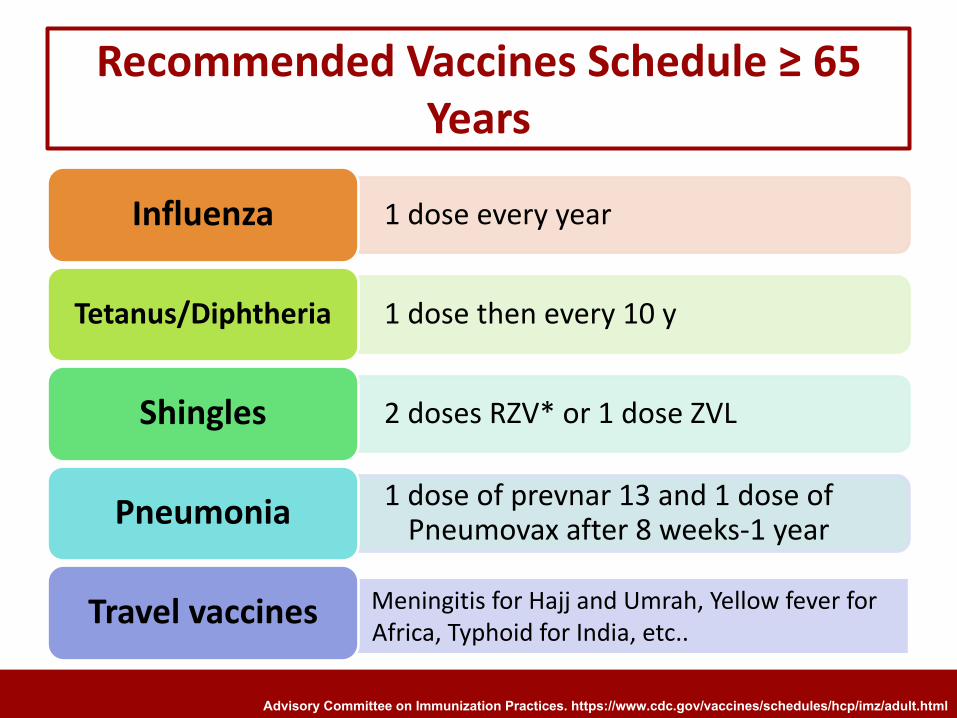
Meningitis for Hajj and Umrah, Yellow fever for Africa, Typhoid for India, etc..
Recommended Vaccines Schedule ≥ 65 Years
1 dose every yearInfluenza
1 dose then every 10 yTetanus/Diphtheria
2 doses RZV* or 1 dose ZVLShingles
1 dose of prevnar 13 and 1 dose of Pneumovax after 8 weeks-1 yearPneumonia
Travel vaccines
Advisory Committee on Immunization Practices. https://www.cdc.gov/vaccines/schedules/hcp/imz/adult.html
Key Messages
• Old people are at higher risk for infections• Infections can lead to serious complications including death• The presentation of infections is different than in younger people• Antibiotics have different properties in older people and variation in
choice, dose, duration should be monitored• Overuse of antibiotics can lead to resistant bacteria and diarrhea
– Treat when symptoms happen not for positive culture• Prevention is important• Eat well, exercise• Update vaccination













![Biomarkers for diagnosing serious bacterial infections in older ......bacteraemia in older adults [+ve LR range 1.50 to 2.60]. A CRP≥50mg/L only raises the probability of bacteraemia](https://img.pdfslide.net/doc/110x75/60b29041652da54ccf7015a6/biomarkers-for-diagnosing-serious-bacterial-infections-in-older-bacteraemia.jpg)















