Embed Size (px)
Citation preview
INFECTIOUS GLYCOSURIC DISEASE 1963 m FOLLOW-UP AND
FURTHER INVESTIGATIONS
H. G. Nelson
Outpatients' Department, Adelaide Hospital, Dublin and Drumcondra Hospital, Dublin.
Summary
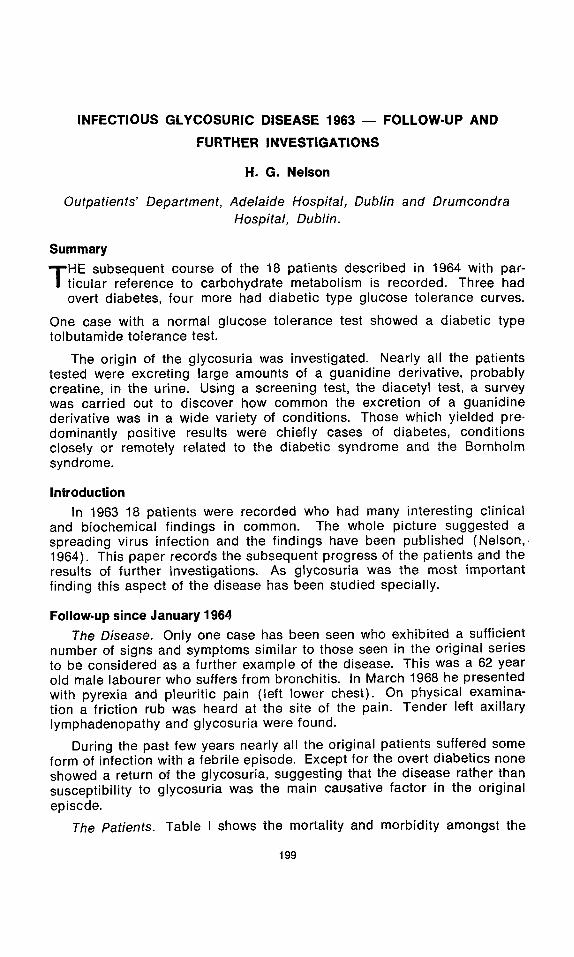
T HE subsequent course of the 18 patients described in 1964 with par- ticular reference to carbohydrate metabolism is recorded. Three had overt diabetes, four more had diabetic type glucose tolerance curves.
One case with a normal glucose tolerance test showed a diabetic type tolbutamide tolerance test.
The origin of the glycosuria was investigated. Nearly all the patients tested were excreting large amounts of a guanidine derivative, probably creatine, in the urine. Using a screening test, the diacetyl test, a survey was carried out to discover how common the excretion of a guanidine derivative was in a wide variety of conditions. Those which yielded pre- dominantly positive results were chiefly cases of diabetes, conditions closely or remotely related to the diabetic syndrome and the Bornholm syndrome.
Introduction
In 1963 18 patients were recorded who had many interesting clinical and biochemical findings in common. The whole picture suggested a spreading virus infection and the findings have been published (Nelson,, 1964). This paper records the subsequent progress of the patients and the results of further investigations. As glycosuria was the most important finding this aspect of the disease has been studied specially.
Follow-up since January 1964 The Disease. Only one case has been seen who exhibited a sufficient
number of signs and symptoms similar to those seen in the original series to be considered as a further example of the disease. This was a 62 year old male labourer who suffers from bronchitis. In March 1968 he presented with pyrexia and pleuritic pain (left lower chest). On physical examina- tion a friction rub was heard at the site of the pain. Tender left axillary lymphadenopathy and glycosuria were found.
During the past few years nearly all the original patients suffered some form of infection with a febrile episode. Except for the overt diabetics none showed a return of the glycosuria, suggesting that the disease rather than susceptibility to glycosuria was the main causative factor in the original episode.
The Patients. Table I shows the mortality and morbidity amongst the
199
200 IRISH JOURNAL OF MEDICAL SCIENCE
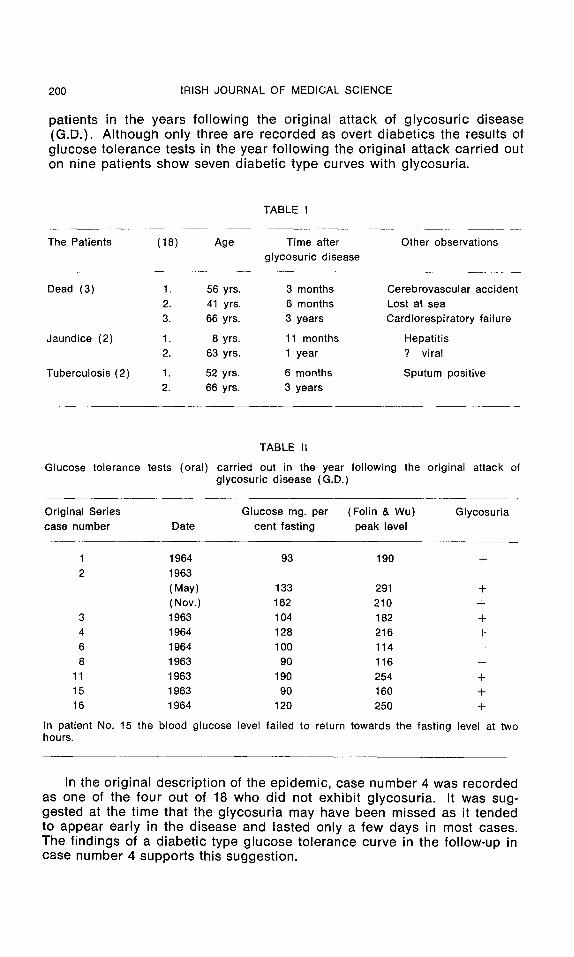
pat ients in the years f o l l ow ing the o r ig ina l a t tack of g l y c o s u r i c d isease (G.D.) . A l t h o u g h on ly three are recorded as overt d i abe t i cs the resul ts of g lucose to le rance tests in the year f o l l o w i n g the o r ig ina l a t tack carr ied out on n ine pat ien ts show seven d iabe t i c t ype curves w i th g lycosur ia ,
TABLE I
The Patients (18) Age Time after Other observations glycosuric disease
Dead (3) 1. 56 yrs. 3 months Cerebrovascular accident 2. 41 yrs. 6 months Lost at sea 3. 66 yrs. 3 years Cardiorespiratory failure
Jaundice (2) 1. 8 yrs. 11 months Hepatitis 2. 63 yrs. 1 year ? viral
Tuberculosis (2) 1. 52 yrs. 6 months Sputum positive 2. 66 yrs. 3 years
TABLE II
Glucose tolerance tests (oral) carried out in the year following the original attack of glycosuric disease (G.D.)
Original Series Glucose mg. per (Folin & Wu) Glycosuria case number Date cent fasting peak level
1 1964 93 190 + 2 1963
(May) 133 291 + (Nov.) 162 210 +
3 1963 104 182 + 4 1964 128 216 + 6 1964 1 O0 114 -- 8 1963 90 116 --
11 1963 190 254 -t- 15 1963 90 160 -I- 16 1964 120 250 +
In patient No. 15 the blood glucose level failed to return towards the fasting level at two hours.
In the o r ig ina l desc r ip t i on of the ep idemic , case n u m b e r 4 was recorded as one of the fou r out of 18 who did not exh ib i t g l ycosu r ia . It was sug- gested at the t ime that the g l ycosu r i a may have been missed as it tended to appear ear ly in the d isease and lasted on ly a f ew days in most cases. The f i nd ings of a d iabe t i c type g lucose to le rance curve in the fo l low-up in case number 4 suppor t s th is suggest ion .
INFECTIOUS GLYCOSURIC DISEASE 1963 201
Further Investigations
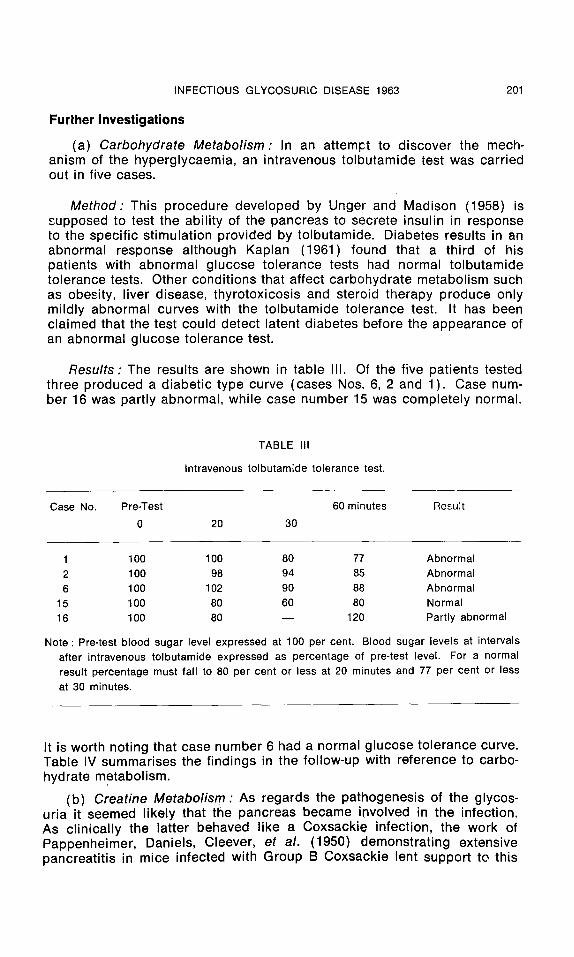
(a) Carbohydrate Metabolism" In an attempt to discover the mech- anism of the hyperglycaemia, an intravenous tolbutamide test was carried out in five cases.
Method: This procedure developed by Unger and Madison (1958) is supposed to test the ability of the pancreas to secrete insulin in response to the specific stimulation provided by tolbutamide. Diabetes results in an abnormal response although Kaplan (1961) found that a third of his patients with abnormal glucose tolerance tests had normal tolbutamide tolerance tests. Other conditions that affect carbohydrate metabolism such as obesity, liver disease, thyrotoxicosis and steroid therapy produce only mildly abnormal curves with the tolbutamide tolerance test. It has been claimed that the test could detect latent diabetes before the appearance of an abnormal glucose tolerance test.
Results" The results are shown in table II1. Of the five patients tested three produced a diabetic type curve (cases Nos. 6, 2 and 1). Case num- ber 16 was partly abnormal, while case number 15 was completely normal.
TABLE III
Intravenous tolbutamide tolerance test.
Case No. Pre-Test 60 minutes Result 0 20 30
1 100 100 80 77 Abnormal 2 100 98 94 85 Abnormal 6 100 102 90 88 Abnormal
15 100 80 60 80 Normal 16 100 80 - - 120 Partly abnormal
Note: Pre-test blood sugar level expressed at 100 per cent. Blood sugar levels at intervals after intravenous tolbutamide expressed as percentage of pre-test level. For a normal result percentage must fall to 80 per cent or less at 20 minutes and 77 per cent or less at 30 minutes.
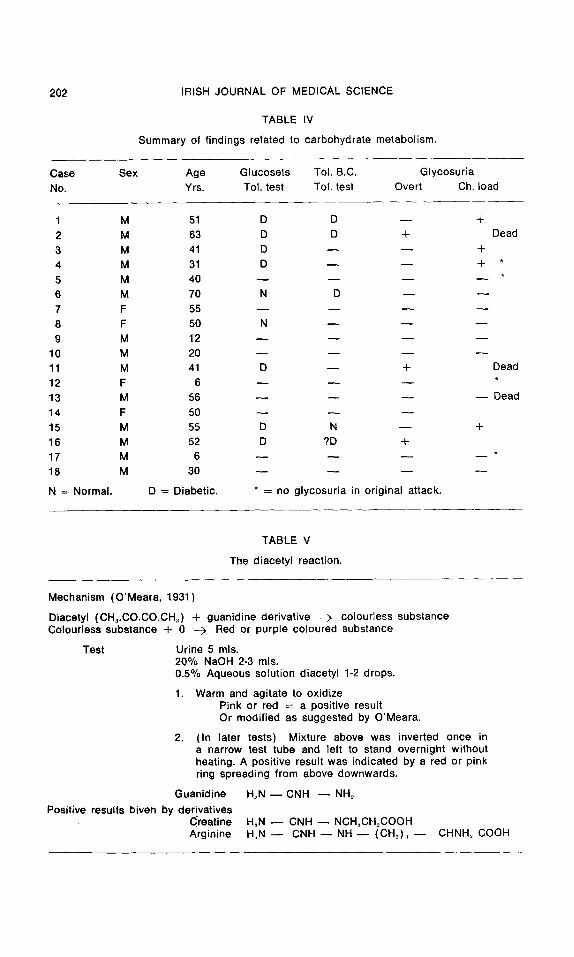
It is worth noting that case number 6 had a normal glucose tolerance curve. Table IV summarises the findings in the follow-up with reference to carbo- hydrate metabolism.
(b) Creatine Metabolism: As regards the pathogenesis of the glycos- uria it seemed likely that the pancreas became involved in the infection. As clinically the latter behaved like a Coxsackie infection, the work of Pappenheimer, Daniels, Cleever, et ah (1950) demonstrating extensive pancreatit is in mice infected with Group B Coxsackie lent support to this
202 IRISH JOURNAL OF MEDICAL SCIENCE
TABLE IV
Summary of f indings related to carbohydrate metabol ism.
Case Sex Age Glucosets Toi. B.C. Glycosur ia
No. Yrs. Tol. test ToI. test Overt Ch. load
1 M 51 D D - - +
2 M 63 D D + Dead
3 M 41 D - - - - +
4 M 31 D - - - - + *
5 M 40 . . . .
6 M 70 N D - - - -
7 F 55 . . . .
8 F 50 N - - - - - -
9 M 12 . . . .
10 M 20 . . . . 11 M 41 D - - + Dead
12 F 6 - - - -
13 M 56 . . . . Dead
14 F 50 - - - - - -
15 M 55 D N - - -t-
16 M 52 D ?D +
17 M 6 . . . .
18 M 30 . . . .
N -- Normal. D = Diabetic. * = no g lycosur ia in or iginal attack.
TABLE V
The diacetyl reaction.
Mechanism (O'Meara, 1931)
Diacetyl (CH~.CO.CO.CH.~) + guanid ine der ivat ive --> colour less substance Colour less substance + 0 --> Red or purple co loured substance
Test Urine 5 mls. 20% NaOH 2-3 mls. 0.5% Aqueous solut ion diacetyl 1-2 drops.
1. Warm and agitate to oxid ize Pink or red = a posit ive result Or modi f ied as suggested by O'Meara.
2. (In later tests) Mixture above was inverted o n c e in a narrow test tube and left to stand overnight without heating. A posit ive result was indicated by a red or pink ring spreading from above downwards.
Guanidine H~N - - CNH ~ NH2
Positive results biven by der ivat ives C'reatine Arginine
H.N - - CNH - - NCH:,CH=COOH H , N - - C N H - - N H - - ( C H = ) : , - - CHNH~ COOH
INFECTIOUS GLYCOSURIC DISEASE 1963 203
suggestion. However, these workers specifically state that the islets seemed to escape amidst widespread necrosis of acini. Also, during the acute phase of the original infection no rise in the serum amylase level could be detected.
Two other possible origins for the glycosuria were considered with the clinical and biochemical findings in mind. These were liver and muscle. To lend support to the latter, detection and estimation of urinary creatine was attempted in case 8. The result revealed that a large quantity was being excreted. As the estimation is a tedious procedure, a screening test was sought. Professor R. A. Q. O'Meara suggested the diacetyl reaction. The mechanism, method and interpretation of this test is shown in table V.
Results
i. Glycosuric Disease. Twelve out 13 cases of glycosuric disease gave repeated strongly positive tests when these were carried out during or soon after the active phase of the disease. The one negative was a single test carried out on case number 14 about four months after the onset of the disease. In the follow-up, those showing persistent glycosuria con. tinued to yield positive results in the majority of tests.
The possible importance of this glyccsuria/diacetyl positive relation- ship immediately raised the question of how commonly was this test positive in practice. Thus a survey was carried out from 1963 to 1965 on the reaction in various conditions encountered in general practice.
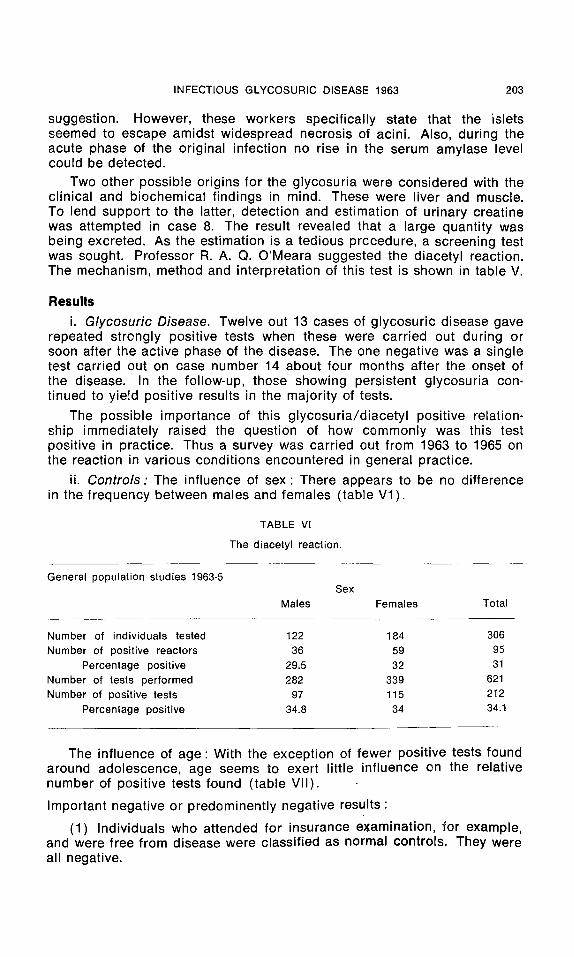
ii. Controls: The influence of sex: There appears to be no difference in the frequency between males and females (table V1 ).
TABLE Vl
The diacetyl reaction.
General population studies 1963-5 Sex
Males Females Total
Number of individuals tested Number of positive reactors
Percentage positive Number of tests performed Number of positive tests
Percentage positive
122 184 306 36 59 95
29.5 32 31 282 339 621
97 115 212 34.8 34 34.1
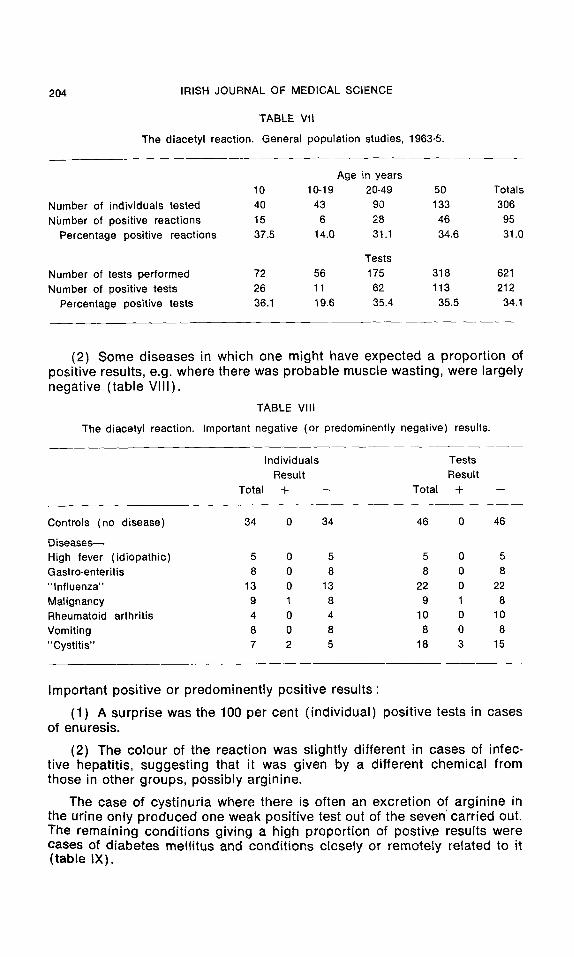
The influence of age: With the exception of fewer positive tests found around adolescence, age seems to exert little influence on the relative number of positive tests found (table VII).
Important negative or predominently negative results :
(1) Individuals who attended for insurance examination, for example, and were free from disease were classified as normal controls. They were all negative.
204 IRISH JOURNAL OF MEDICAL SCIENCE
TABLE VII
The diacetyl reaction. General population studies, 1963-5.
Number of individuals tested Number of positive reactions
Percentage positive reactions
Number of tests performed Number of positive tests
Percentage positive tests
Age in years 10 10-19 20-49 50 Totals 40 43 90 133 306 15 6 28 46 95 37.5 14.0 31.1 34.6 31.0
Tests 72 56 175 318 621 26 11 62 113 212 36.1 19.6 35.4 35.5 34.1
(2) Some d iseases in which one might have expected a propor t ion of posi t ive results, e.g. where there was probab le muscle wast ing, were largely negat ive ( tab le VI I I ) .
TABLE VIII
The diacetyl reaction. Important negative (or predominently negative) results.
Individuals Tests Result Result
Total + -- Total +
Controls (no disease) 34 0 34 46 0 46
Diseases-- High fever (idiopathic) 5 0 5 5 0 5 Gastro-enteritis 8 0 8 8 0 8 "Influenza" 13 0 13 22 0 22 Malignancy 9 1 8 9 1 8 Rheumatoid arthritis 4 0 4 10 0 10 Vomiting 8 0 8 8 0 8 "Cystitis" 7 2 5 18 3 15
Important pos i t ive or p redominent ly pos i t ive resu l ts :
(1) A surpr ise was the 100 per cent ( ind iv idua l ) pos i t ive tests in cases of enuresis.
(2) The co lour of the react ion was s l ight ly d i f ferent in cases of infec- t ive hepat i t is, suggest ing that it was given by a d i f ferent chemica l f rom those in other groups, possib ly arg in ine.
The case of cys t inur ia where there is often an excret ion of arg in ine in the ur ine only p roduced one weak pos i t ive test out of the seven ~ carr ied out. The remain ing condi t ions g iv ing a high proport ion of postiv.e results were cases of d iabetes mel l i tus and cond i t ions c lose ly or remote ly related to it ( tab le IX).
INFECTIOUS GLYCOSURIC DISEASE 1963
TABLE IX
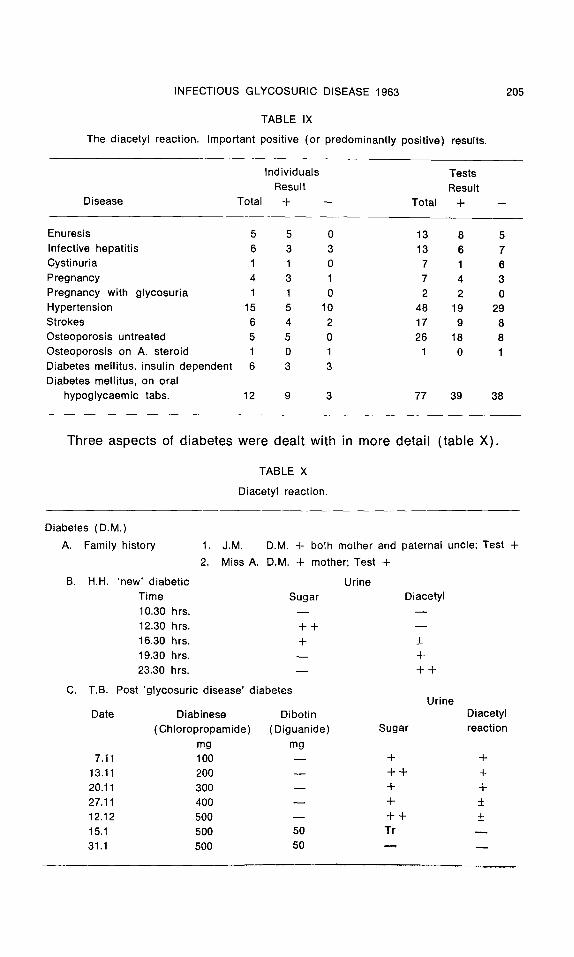
The diacetyl reaction. Important positive (or predominantly posit ive) results.
205
Individuals Tests
Result Result Disease Total Jr -- Total Jr
Enuresis 5 5 0 13 8 5 Infective hepatit is 6 3 3 13 6 7 Cystinuria 1 1 0 7 1 6 Pregnancy 4 3 1 7 4 3 Pregnancy with glycosuria 1 1 0 2 2 0 Hypertension 15 5 10 48 19 29 Strokes 6 4 2 17 9 8 Osteoporosis untreated 5 5 0 26 18 8 Osteoporosis on A. steroid 1 0 1 1 0 1 Diabetes mellitus, insulin dependent 6 3 3 Diabetes mellitus, on oral
hypoglycaemic tabs. 12 9 3 77 39 38
Three aspects of diabetes were dealt with in more detail (table X).
TABLE X
Diacetyl reaction.
Diabetes (DM.) A. Family history J.M,
Miss A. D.M. + mother; Test +
B. H.H. 'new' diabet ic Urine Time Sugar Diacetyl
10.30 hrs. - -
12.30 hrs. Jr -t- - - 16.30 hrs. + _+ 19.30 hrs. - - +
23.30 hrs. - - + +
C. T.B. Post 'glycosuric disease' d iabeies Urine
Date Diabinese Dibotin Diacetyl (Chloropropamide) (Diguanide) Sugar reaction
mg mg 7.11 100 - - + +
13.11 200 - - + + + 20.11 300 - - Jr -I- 27.11 400 - - + _+ 12.12 500 - - Jr Jr +_
15.1 500 50 Tr 31.1 500 50 N
1.
2.
D.M. -I- bolh mother and paternal uncle; Test -I-
206 IRISH JOURNAL OF MEDICAL SCIENCE
Two cases (J.M. and Miss A.) who were d iabetes f ree but gave a posi- t ive fami ly h is tory y ie lded posi t ive results. In one recent ly d iagnosed matur i ty onset d iabet ic , the assoc ia t ion of the appea rance of sugar and a diacety l pos i t ive chemica l in the ur ine th roughou t the day was invest igated. It was noted that sugar appeared ear ly in the day wh i le the guan id ine de- r ivat ive appeared later.
Finally, the ef fect of t rea tment on the d iacety l test was noted in one of the cases of g l ycosur i c d isease who deve loped overt d iabetes. The test became weak ly pos i t ive as the full dose of ch lo rp ropamide was reached (500 mg) and then became abrupt ly negat ive on in t roduc t ion of Dibot in (a d iguan ide ) . It is in terest ing that a guan id ine der ivat ive should d isappear f rom the ur ine on in t roduct ion of a d iguan ide into the system.
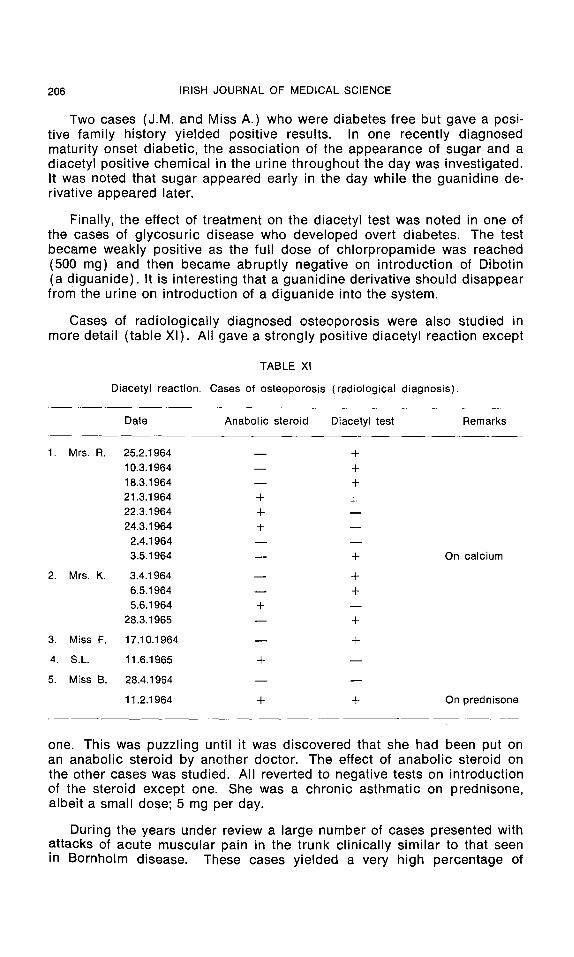
Cases of rad io log ica l l y d iagnosed os teoporos is were also studied in more detai l ( tab le Xl ) . All gave a s t rong ly posi t ive d iacety l react ion excep t
TABLE Xl
Diacetyl reaction. Cases of osteoporosis (radiological diagnosis).
Date Anabolic steroid Diacetyl test Remarks
1. Mrs. R. 25.2.1964 - - § 10.3.1964 - - + 18.3.1964 - - + 21.3.1964 -I- _+ 22.3.1964 -I- - - 24.3.1964 + - -
2.4.1964 - - - - 3.5.1964 - - -t- On calcium
2. Mrs. K. 3.4.1964 - - -t- 6.5.1964 - - -I- 5.6.1964 -t- - -
28.3.1965 - - +
3. Miss F. 17.10.1964 - - §
4. S . L . 11.6.1965 § - -
5. Miss 13. 28.4.1964 - - - -
11.2.1964 -t- § On prednisone
one. This was puzz l ing until it was d iscovered that she had been put on an anabo l i c s tero id by another doctor . The ef fect of anabo l i c steroid on the other cases was studied. All rever ted to negat ive tests on in t roduct ion of the stero id excep t one. She was a chron ic as thmat ic on predn isone, a lbei t a small dose; 5 mg per day.
Dur ing the years under rev iew a large number of cases presented wi th at tacks of acu te muscu lar pain in the t runk c l in ica l ly s imi lar to that seen in Bornho lm disease. These cases y ie lded a very high pe rcen tage of

INFECTIOUS GLYCOSURIC DISEASE 1963 207
s t r o n g l y p o s i t i v e resu l t s . In f o u r i n c i d e n t s t h e a p p e a r a n c e of p o s i t i v e t es t s w i t h i n t h e f a m i l y w a s s t u d i e d in m o r e de ta i l . It s h o u l d be n o t e d in t h e t h i r d i n c i d e n t o n e son w h o o n l y d e v e l o p e d a h e a d c o l d w i t h o u t t h e m y a l g i a g a v e o n e n e g a t i v e tes t ( t a b l e s X l l a n d X l I I ) .
TABLE XII
The diacetyl reaction.
Bornholm-like disease : Original 'Glycosuric disease' - - 12 out of 13 persons tested gave a strong positive reaction.
Cases presenting with acute muscular pain similar in character to Bornholm disease.
Patients Tests Site No. + - - No. + - - Dorsi-lumbar 6 5 1 13 9 4 Chest 8 8 0 14 9 5 Abdomen 12 11 1 18 12 6
TABLE XIII
Bornholm-like disease, contd.
Family examples
Date Patient Symptoms Test Patient Symptoms Test Patient Symptoms Test
6.4 P.G. + + M.G. - - - - 7.4 (Brother) + + (Sister) - - - - 8.4 + + + - -
10.4 + + + + 12.4 + + + +
25.6 M.D.S. + + E.D.S. - - - - 29.6 (Mother) (Father) + +
2.7 + +
Previous tests M.N.S. - - - - A.S. - - - - 27 .11 (Mother) + + (Son) 28.11 + + + + 30.11 + + - - - -
5.2 J.C. + + M.C. + + 7.2 (Sister) - - - - (Sister) - - - -
D.D.S. (Son)
+ +
D.S. - - - - (Son)
Cold - -
S.C. + _+_ (Sister) - - - -
Discussion
In t he a b s e n c e of any k n o w n a e t i o l o g y i t is d i f f i c u l t to f i nd a s a t i s f a c t o r y n a m e f o r t h i s d i s e a s e . I have , h o w e v e r , t a k e n t h e m o s t i n t e r e s t i n g a n d d i s t i n c t i v e b i o c h e m i c a l f i n d i n g , i.e. g l y c o s u r i a a n d p r e - f i x e d i t w i t h t h e
208 IRISH JOURNAL OF MEDICAL SCIENCE
almost certain fact that it is an infectious disease (original series, cases 17 & 18).
Davies and Bell (1967) published the description of a case with clinical and biochemical abnormalities which fitted closely the description of orig- inal cases of glycosuric disease. Up to date this appears to be the only publication supporting the existence of this disease.
Dr. J. E. Craighead of the Harvard Medical School reporting to the American Association of Pathologists in 1968 claimed to have shown ex- perimentally that the encephalomyocarditis virus (EMC) can cause or trigger transient diabetes in mice by attacking the islets of Langerhans. This virus is classified with the enteroviruses and is closely linked with the Coxsackie and polio viruses. Dr. Craighead has now turned his attention to the former of these two and is studying their effect on the human pancreas.
Gamble, Kinsley, Fitzgerald, et al. (1969) reported the results of their studies on viral antibodies in recent cases of diabetes and compared them with similar studies in established cases and normal controls. They found that in diabetics of recent onset who were insulin-dependent, there was a higher titre of antibody to Coxsackie B virus particularly of type 4, than in either normal subjects or patients with diabetes of longer duration.
Two of these authors (Gamble and Taylor, 1969) at the same time reported on studies of the seasonal incidence of diabetes mellitus. A significant variation in annual totals of new cases of diabetes seen could not be demonstrated or excluded, but the pattern of the variation present showed significant positive correlation with the annual prevalence data for Coxsackie virus type B4, but not for other types of virus infection.
It is assumed that if these virus infections produce or precipitate dia- betes they do so by attacking the islets. In the cases of glycosuric disease
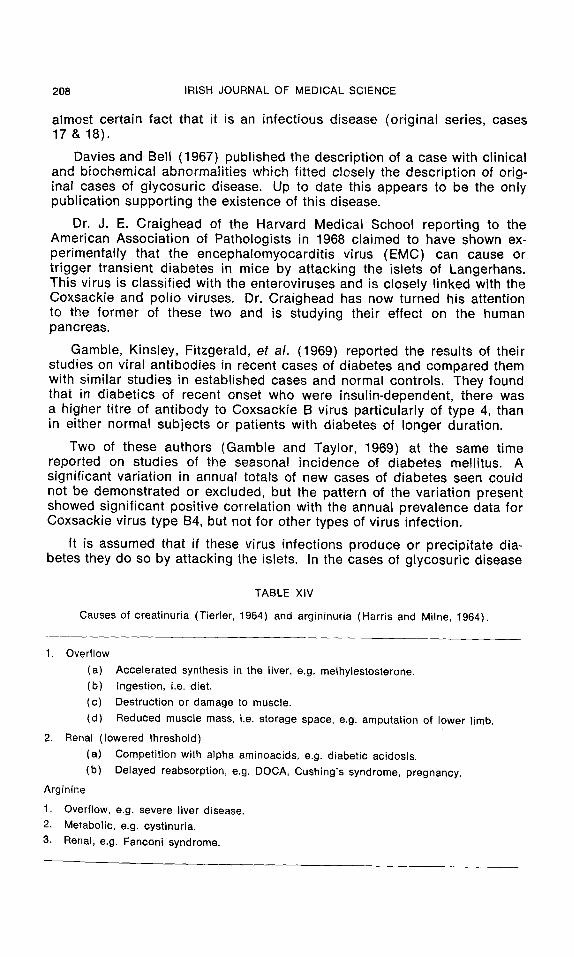
TABLE XIV
Causes of creatinuria (Tierler, 1964) and argininuria (Harris and Milne, 1964).
1. Overflow
(a) Accelerated synthesis in the liver, e.g. methylestosterone. (b) Ingestion, i.e. diet.
(c) Destruction or damage to muscle.
(d) Reduced muscle mass, i.e. storage space, e.g. amputation of lower limb.
2. Renal (lowered threshold)
(a) Competition with alpha aminoacids, e.g. diabetic acidosis. (b) Delayed reabsorption, e.g. DOCA, Cushing's syndrome, pregnancy.
Arginine
1. Overflow, e.g. severe liver disease. 2. Metabolic, e.g. cystinuria.
3. Renal, e.g. Fanconi syndrome.
INFECTIOUS GLYCOSURIC DISEASE 1963 209
described above the acinar tissue of the pancreas appeared to escape as no change could be demonstrated in the level of serum amylase in the cases tested. Alternatively in mumps the islets appear to escape.
As regards the results with the diacetyl reaction it appears that the most likely substances giving positive tests are the guanidine derivatives creatine and arginine as these occur naturally in the body.
Table XlV shows the main conditions under which one or other of these amino-acids may appear in the urine. The most likely cause in the disease under consideration is 1 (c), destruction or damage to muscle. Cause 2(a) is unlikely, as diabetic acidosis was not demonstrated in any of the cases. As is noted above a different colour reaction was observed in cases of infective hepatitis. It is probable that this type of colour is that given by arginine and that the other type of reaction found in the remainder of the cases was given by creatine.
The glycosuric disease and "Bornholm syndrome" appear to be asso- ciated with the excretion of large amounts of creatine. To a lesser extent so also are diabetes mellitus, particularly the maturity onset type and conditions associated closely or remotely with the diabetic syndrome (e.g. osteoporosis).
I wish to thank Professor R. A. Q, O'Meara for his help with this work and Dr. David Mitchell and Dr. Eric Horgan for reading the draft of the paper and giving helpful criticism.
References
Craighead, J. E. 1968. As reported in Antibiotic News, vol. 5, No. 4, p. 3. Davies, D. M. and Bell, S. M. 1967. Another case of Nelson's disease. J. Irish med. Ass.
60, 363. Gamble, D. R., Kinsley, M. L., Fitzgerald, M. G., Bolton, R. and Taylor, K. W. 1969. Viral
Antibodies in Diabetes Mellitus. Brit. med. J., 3, 627. Gamble, D. R. and Taylor, K. W. 1969. Seasonal Incidence of Diabetes Mellitus. Brit. med.
J., 3, 631. Harris, H. and Milne, M. D. in Biochemical Disorders in Human Disease, 2nd ed., Thomp-
son, R.H.S. and King, E. J., London. J. & A. Churchill. Kaplan, N. M. 1961. Diagnosis of Diabetes Mellilus. Arch. intern. Med., 107, 212. Nelson, H. G. 1964. An Epidemic in a Dublin Practice.--A New Virus Infection. J. Irish
med. Ass., 329, 118. O'Meara, R. A. Q. 1931. The mechanism of the Voges-Proskauer reaction and the diacetyl
reaction for proteins. Brit. J. exp. Path. 12, 346. Pappenheimer, A. M., Daniels, J. B., Cleever, F. G. and Weller, T. H. 1950. Lesions caused
in suckling mice by certain viruses isolated from cases of so called non-paralytic polio- myelitis and of pleurodynia. J. exp. Med. 92, 169.
Unger, R. F. and Maddison, L. L. 1958. The Intravenous Sodium Tolbutamide Tolerance Test. Diabetes, 7, 455.
Zierler, K. L. in Biochemical Disorders in Human Disease. 2rid ed. Thompson, R. H. S. and King, E. J. London : J. & A. Churchill.