Embed Size (px)
Citation preview

Journal of Pers~ality and Social Psychology Copyright 1989 by the American Psychological Association, Inc. 1989, Vol. 57, No. 3, 539-551 0022-3514/89/$00.75
Influence of Mood on Health-Relevant Cognitions
Peter Salovey and Deborah Birnbaum Yale University
Three experiments assessed the effects of mood on symptom appraisal, health behavior self-efficacy, outcome expectations, and perceptions of vulnerability. Ss in Experiments 1 and 2 were acutely ill, whereas Ss in Experiment 3 were healthy. In each experiment, happy, sad, and neutral moods were induced. In Experiment l, Ss who experienced sadness reported more aches and pains and greater discomfort than happy Ss. Sad Ss were less confident that they could carry out illness-alleviating behaviors. Experiments 2 and 3 demonstrated that mood's influence on vulnerability perceptions is moderated by health status. Although mood had little impact on perceptions of vulnerability among ill Ss, probability estimates of future negative health-relevant events among healthy Ss were mood sensitive. Seeing oneself as invulnerable to future negative events was accentuated among happy Ss and attenuated among sad Ss. Mood may be an important determinant of care seeking, adherence, and recovery from illness.
Psychotherapists and physicians frequently report the simul- taneous occurrence of psychological distress and physical com- plaints. Moreover, physicians are often confronted with patients who report a variety of physical symptoms with no obvious or- ganic basis. Conversely, psychotherapists often worry that their clients' psychological distress may in fact reflect or be secondary to a physical disorder.
In a comprehensive review of the literature on somatization, depression, and chronic physical illness, Katon (1984) noted that depressed individuals report somatic ailments in greater numbers than do nondepressed individuals. Similarly, health is often appraised less positively among persons with a history of depression (Maddox, 1962). The relationship between de- pressed mood and symptom appraisal holds even for individu- als not suffering from a diagnosable affective disorder. In gen- eral, perceived health status varies negatively with psychological distress (Tessler & Mechanic, 1978). Those individuals who feel relatively unhappy rate their health as poorer than do those who feel relatively happy.
Negative appraisals of one's health resulting from dysphoric mood may promote the seeking of treatment. Prospective stud- ies have demonstrated that psychological distress is an impor- tant determinant of who seeks medical services (Tessler, Me- chanic, & Dimond, 1976). Conversely, the seeking of medical
This project was supported in part by Biomedical Research Support Grant S07 RR07015 to Peter Salovey and by funding from the John D. and Catherine T. MacArthur Foundation Mental Health Network on Determinants and Consequences of Health-Promoting and Health- Damaging Behavior.
We would like to thank John D. Mayer, William McGuire, Judith Rodin, and two anonymous reviewers for their helpful comments on earlier versions of this article.
We determined the order of authorship by tossing a coin; both au- thors contributed equally to the research.
Correspondence concerning this article should be addressed to Peter Salovey, Department of Psychology, Yale University, Box 11A Yale Sta- tion, New Haven, Connecticut 06520.
care appears to decrease when hospitals provide psychological services that can address and perhaps alleviate the psychological distress of patients initially presenting physical complaints, al- though some of the studies of this question have been method- ologically limited (N. A. Cummings & Follette, 1976; Follette & Cummings, 1967; Jones & Vischi, 1979).
Although somatic symptoms and physical complaints may be manifestations of psychological distress, it may also he true that psychological difficulties can result from physical illnesses. Cor- relational work using time-series analysis indicates that changes in mood may be a consequence of current symptomatology (Persson & Sjoberg, 1987). For example, depression is often a consequence of chronic pain (Hendler, 1984; Holzman, Cline, & Rudy, in press; Kerns, Haythornthwaite, & Giiler, 1987; Turk, Rudy, & Stieg, 1987). In fact, negative mood or depres- sion may result from a variety of experiences with illness (Hol- lister, 1983; Murphy, 1982; G. Rodin & Voshart, 1986).
The hypothesis that psychological distress is a consequence of physical illness has not been accepted uncritically. Many the- orists posit that the illness itself is a product of an underlying (and primary) psychological disturbance. For example, Blumer and Heilbronn (1982) suggested that chronic pain disorders are actually the manifestation of underlying and unexpressed psy- chological depression. Although the methodology of these stud- ies has been criticized (Turk & Salovey, 1984), others have also established depression as a predictor of chronic pain com- plaints (Keefe, Wilkins, Cook, Crisson, & Muhlbaier, 1986).
The controversy concerning whether psychological distress precedes or is a consequence of physical illness has been ren- dered unresolvable, at least at present, because studies in this area are largely correlational and cross-sectional. What is re- quired are longitudinal studies of both psychologically dis- tressed patients and chronically ill individuals or laboratory an- alog studies in which either dysphoric mood or physical symp- toms can be manipulated and changes in the other variable observed. Although such longitudinal studies may emerge from several hospital-based pain clinics, surprisingly few laboratory studies have been conducted. One study that did induce happy
539

540 PETER SALOVEY AND DEBORAH BIRNBAUM
versus sad moods found that perceived health status varied in a mood-congruent direction. Subjects who experienced sad moods reported more symptoms and rated their current health status lower than did subjects induced to feel happy (Croyle & Uretsky, 1987). Although these results suggest that mood may be an important determinant of health appraisal, their interpre- tation is limited by the fact that a neutral mood control group was not included and the subject sample was healthy. It is not clear whether health appraisal is influenced by both depressed and elated moods (or by one and not the other) or whether mood would have a similar impact on the health appraisals of ill individuals, because variance in perceived health status among healthy subjects is low.
Although we have so far focused on relationships between mood and symptom appraisal, mood may also affect other health-relevant cognitions. One type of cognitive activity that predicts engaging in health-promoting behavior is holding be- liefs about one's capacity to engage successfully in such behav- iors. These beliefs, termed self-efficacy expectations by Bandura (1977), are important correlates of diverse health behaviors such as smoking cessation, eating, weight control, and adher- ence to preventive behavioral regimens (Bandura, in press; O'Leary, 1985). For example, in a study ofpsychosocial predic- tors of high-risk sexual activities, beliefs that one is capable of making recommended behavioral changes were found to be the most consistent predictors of AIDS risk-reducing behaviors (McKusick, Wiley, Coates, & Morin, 1986). A question, then, is whether mood significantly influences such beliefs. Although this hypothesis has not yet been tested in the health domain, correlational work by Kanfer and Zeiss (1983) suggests that de- pressed individuals have lower self-efficacy expectancies than do nondepressed individuals in a variety of situations. In addi- tion, induced mood appears to influence self-efficacy expecta- tions regarding behavior in domains such as romance, athletics (Kavanagh & Bower, 1985), and interpersonal helping (Salovey, 1986; Salovey & Rosenhan, 1989).
Another important health-relevant cognition concerns ex- pectations that engaging in certain behaviors will alleviate ill- ness or protect health. Individuals are more likely to engage in behaviors thought to be sufficiently salubrious (Turk, Rudy, & Salovey, 1984), and performing health behaviors is related to perceptions of the costs, benefits, and perceived effectiveness of those behaviors (Becker, 1974; Rogers & Mewborn, 1976). It seems likely that happy individuals would have greater expecta- tions that engaging in behaviors would be effective in alleviating illness or promoting health than would dysphoric individuals. Although this relationship has not been explored in the health domain, Wright and Mischel (1982) found that positive affect led individuals to form optimistic expectations about the out- come of future performances, and negative affect had the oppo- site effect.
Beliefs about one's vulnerability to illness are also related to health-relevant behavior. Beliefs about risk likelihood and risk severity have been found to contribute to interest in risk-reduc- ing behavior such as seeking medical treatment (Becker et al., 1977; K. M. Cummings, Jette, Brock, & Haefner, 1979; Kulik & Mahler, 1987; Weinstein, 1982, 1983). For example, denial of personal risk for the onset of AIDS has been found to be associated with high-risk sexual behavior (Weber, Coates, &
McKusick, 1986). These estimates of the likelihood of positive and negative future events appear to be influenced by mood. Subjects made to feel happy frequently underestimate the chances that a negative event will occur, and sad individuals often overestimate the likelihood of such events. Estimates of positive events are similarly mood congruent (Johnson & Tver- sky, 1983). Similar results have been observed in clinically de- pressed individuals (Pyszczynski, Holt, & Greenberg, 1987).
Underlying Mechanisms
Although not directly explored by our experiments, the im- pact of mood on health cognitions might be explained by some of the general influences of mood on cognitive processing. Neg- ative mood states have been hypothesized to result in a tendency to focus attention on the self and away from external stimuli (Brockner, Hjelle, & Plant, 1985; Ingrain & Smith, 1984; Pyszc- zynski & Greenberg, 1985, 1986, 1987; Salovey & Rodin, 1985; Smith & Greenberg, 1981; Smith, Ingrain, & Roth, 1985; Strack, Blaney, Ganellen, & Coyne, 1985). Mood induced self- focusing may be maintained because it serves to clarify the affective experience (Scheier & Carver, 1977; Scheier, Carver, & Gibbons, 1981). Individuals experiencing intense negative affect should thus be more attentive to physical symptoms and other bodily changes such as sweating, blushing, or a pounding heart. In turn, attention to these bodily experiences may serve to maintain the self-focused state (Fenigstein & Carver, 1978; Wegner & Giuliano, 1980).
Individuals undergoing an affective experience should also become aware of mood-congruent material from memory (for reviews of the impact of mood on memory, see Blaney, 1986; Gilligan & Bower, 1984; Isen, 1984; Mayer & Salovey, 1988; Singer & Salovey, 1988). While individuals experience a partic- ular mood, they are more likely to recall mood-congruent infor- mation, even though that material may not be related to the experience responsible for initiating the mood (Bower, 1981; Isen, Shalker, Clark, & Karp, 1978). Because judgments are of- ten based on what is most easily brought to mind (Tversky & Kahneman, 1973), mood may have a congruent effect on judg- ment (Mayer & Bremer, 1985; Mayer & Volanth, 1985). Mood may also influence judgment by its impact on the way memorial information is categorized (Isen & Daubman, 1984; Isen, Daubman, & Nowicki, 1987; Mayer, 1986). In the health do- main, mood should have an impact on health appraisal, risk estimates, and efficacy and outcome expectations by facilitating recall of pleasant versus unpleasant health and illness-related memories. Indeed, when individuals are asked to imagine a health-related scenario, mood has an especially strong effect on health appraisal and symptom reporting (Croyle & Uretsky, 1987).
The Present Experiments
The present article reports a set of experiments in which ill individuals were asked to experience elated, dysphoric, or neu- tral moods and then to report on their physical symptoms and discomfort, beliefs about their abilities to carry out health-pro- moting and illness-alleviating behaviors, expectations that these behaviors would be effective, and estimates of their (and others')

MOOD AND HEALTH 541
vulnerabil i ty to future health outcomes. We expected mood to have an impact on these health cognitions consistent with find- ings from the mood-congruent-recall and depressive-self-focus- ing literatures. In particular, we expected that
1. I!1 subjects who were induced to feel sad would report more physical symptoms and greater discomfort from these symptoms than would ill subjects induced to feel happy.
2. I11 subjects who were induced to feel sad would report lower self-efficacy and more pessimistic outcome expectations with respect to health-promoting and illness-aUeviating activi- ties than would individuals who were induced to feel happy.
3. Subjects who were induced to feel sad would perceive themselves as more vulnerable to future poor health outcomes than would subjects who were induced to feel happy. Similarly, happy subjects would perceive themselves as more likely to ex- perience more positive health outcomes than others, in contrast to sad subjects. The first two of these hypotheses were examined in Experiment 1, and the latter hypothesis was addressed in Experiments 2 and 3.
E x p e r i m e n t 1
College students experiencing the flu or common cold were recruited for a study on thoughts about health. They were asked to experience a happy, sad, or neutral mood state using an imag- ery-based mood induct ion procedure. Following mood induc- tion, the subjects appraised the variety and intensity of their physical symptoms and completed measures of self-efficacy and outcome efficacy regarding illness-alleviating behaviors. Mood and symptomatology were assessed both before and after mood induction.
Method
Subjects
Subjects were 66 undergraduates (34 men and 32 women) who re- sponded to a solicitation for individuals experiencing the common cold or flu. When subjects entered the lab, they completed a symptom per- ception checklist, which verified that they were currently experiencing symptoms of the cold or flu. Approximately two-thirds of the subjects were recruited from the introductory psychology subject pool and re- ceived credit toward their experimental participation requirement. The remainder were recruited from campus by means of posters and re- ceived $5 for their participation. Subjects were randomly assigned to one of three mood conditions. One additional subject was excluded from the analysis because she did not report any symptoms on the checklist.
you can. Picture the events happening to you. See all the details of the situation. Picture in your "mind's eye" the surroundings as clearly as possible. See the people or objects; hear the sounds; expe- rience the event happening to you. Think the thoughts you would actually think in this situation. Feel the same [happy, sad, neutral] feelings you would feel. Let yourself react as if you were actually there.
This mood induction procedure has been referred to as the autobio- graphical recollections method (Goodwin & Williams, 1982) or as self- generated imagery (Salovey & Rodin, 1985; Singer & Salovey, 1988). In a study by Brewer, Doughtie, and Lubin (1980), it was found to be more effective than Velten's (1968) mood inducing self-statements, a com- monly used technique. A previous study (Salovey & Singer; 1989) on mood and recall of childhood versus recent memories found that the mood induction procedure used here induced stable and reasonably intense moods.
Preliminary Measures
Mood state prior to the mood manipulation. Subjects' moods prior to the mood induction procedure were assessed with the Profile of Mood States (POMS) developed by McNair, Lorr, and Droppleman (1971 ). The POMS is a six-subscale measure with 65 adjectives forming the following mood subscales: Depression-Dejection, Vigor-Activity, Tension-Anxiety, Anger-Hostility, Fatigue-Inertia, and Confusion-Be- wilderment. Subjects used 5-point scales to indicate which adjectives described how they felt. The POMS has demonstrated adequate validity and reliability as a measure of mood (McNair et at., 197 I).
Symptomatology prior to the mood manipulation. A modified version of the Wahler Physical Symptoms Inventory (Wahler, 1968) was used to assess symptomatology. The inventory includes 28 symptoms (e.g., headache, stuffy nose, sore throat, aches and pains) and asks subjects to check those symptoms they are currently experiencing. Subjects also indicated those symptoms they experienced in the past week and rated the discomfort from those symptoms on 5-point scales. Wahler de- scribed this scale as having strong reliability and adequate validity as a measure of physical symptoms.
Manipulation Checks
Differential Emotions Scale. The Happiness subseale of Izard's (1971) Differential Emotions Scale (DES) consists of 16 adjectives placed on 7-point scales. The adjectives reflect both happiness and sad- ness. As a measure of happy versus sad affect, this instrument has dem- onstrated good internal consistency (Izard, 1971).
Six-Item Mood Check. In previous work involving happy and sad mood manipulation (Amrbein, Salovey, & Rosenhan, 1981; Rosenhan, Salovey, & Hargis, 1981; Salovey & Rosenhan, 1983; Salovey & Singex; 1989), six items presented in directionally counterbalanced orders on 7- point scales provided an extremely brief yet reliable measure of positive versus negative affect. This scale includes happy, exhilarated, sad, satis- fied, content, and disappointed.
Mood Manipulation
A tape-recorded mood induction procedure described by Wright and Misehel (1982) was used in this experiment. The tape, which lasted about 5 rain, first instructed subjects to relax, make themselves com- fortable, and focus their attention on the instructions they were about to hear. Subjects were told to vividly imagine a situation that would leave them feeling happy, sad, or neutral ("neither happy nor sad"). The instructions then proceeded as follows:
I would like for you to begin imagining a situation that would make you feel [happy, sad, or neutral]. Imagine the situation as vividly as
Dependent Variables
Symptom appraisal Subjects' symptom appraisals were assessed by a second administration of the Wahler Physical Symptoms Inventory.
Health behavior self-efficacy To assess health behavior self-efficacy, subjects were presented with 26 one-sentence health-promoting and ill- ness-alleviating behaviors and asked to rate their confidence that they could successfully carry out each. Subjects indicated their confidence on an I l-point scale ranging from 0 (not at all confident) to 100 (very confident). An average health behavior self-efficacy score was then com- puted. This measure, which we designed but which was based on Ban-
542 PETER SALOVEY AND DEBORAH BIRNBAUM
dura (1977), had good internal consistency; in the present experiment, Cronbach's alpha was .88.
Health behavior outcome expectations. Outcome expectations were assessed by presenting subjects with the same 26 behaviors and asking them to rate the likelihood that each would have prevented or would alleviate their current illness. Subjects indicated the probability on 1 l- point scales ranging from 0 to 100. In the present study, Cronbach's alpha for this measure was .89.
Procedure
Subjects were recruited for the experiment with posters soliciting vol- unteers who were presently "experiencing symptoms of the cold or flu?' The experiment was advertised as involving "imagination" a standard mood induction experimental cover story (e.g., Rosenhan et al., 1981).
Two to four subjects were tested in each session. Subjects were seated at separate desks with dividers placed between them so that they were unable to see or interact with each other. A set of headphones was placed on each desk. Before entering the laboratory, subjects were randomly assigned to one of the following three mood conditions: happy, sad, or neutral. On entering, subjects were told that the experiment was con- corned with how individuals think about events in their lives. They were told that they would imagine an event from their past and then complete a set of questionnaires concerning how individuals think about stresses and strains in their lives, especially those related to health. If they agreed to sign a consent form, the experiment commenced.
Because subjects were aware that they had been recruited because they were ill, the issue was specifically addressed by the experimenter. She told subjects that because many of the stresses and strains studied in this experiment were health related, we wanted subjects who were more likely to be actively thinking about their health. Subjects were unaware that their moods were being manipulated, however. Rather, they were told that the imagination task and the subsequent paragraph they would write about it (i.e., the mood induction procedure) were simply a means to understanding how people think about events in their lives.
Subjects first completed the POMS and the Wahler Physical Symp- toms Inventory. When subjects were finished, they were told that the imagination portion of the experiment was about to begin. Subjects then placed the headphones over their ears and listened to a tape de- signed to induce a happy, sad, or neutral mood. After this mood induc- tion ended, the tape instructed subjects to complete a new set of ques- tionnaires that had been placed on the desk in front of them. This packet contained (a) the DES, (b) a blank sheet asking subjects to briefly discuss what they had thought about during the mood induction procedure, ~ (c) the health behavior self-efficacy measure, (d) the health behavior out- come expectation measure, (e) a second Wahler Physical Symptoms In- ventory to assess changes in symptom appraisal, (f) a Behavioral Inten- tion scale, 2 and (g) the Six-Item Mood Check.
All subjects first completed the DES and then wrote briefly about the event they had imagined. The Six-Item Mood Check was always completed last. The remainder of the measures were presented to sub- jects in one of two random orders. 3 About halfway through the session, subjects were asked to take a minute to reflect back on what they had thought about during the imagination task. This mood booster was de- signed to increase the likelihood that the induced mood was maintained for the length of the experimental session. After subjects completed the Six-Item Mood Check, they ~-'re thanked and carefully debriefed to ensure that there were no lingering effects of the mood induction proce- dure. During debriefing, we asked subjects to generate guesses concern- ing our hypotheses. None of the subjects accurately discerned the goals of the study or realized that their moods had been intentionally manipu- lated. After subjects had answered our questions concerning these mat- ters, we described the purposes of the experiment to them and answered
their questions. We then discussed any lingering distress they might be experiencing and offered them the opportunity to listen to the happy mood induction tape. The entire study lasted less than 1 hr.
Resul ts
Prel iminary Analyses
Before examining the impact o f m o o d on the dependent vari- ables of this study, we conducted three prel iminary analyses. The first involved assessing whether the three m o o d groups differed before the m o o d manipulat ion. The second involved an analysis o f gender differences across all o f the variables o f the study, and the third was a reduct ion o f the 28 symptoms re- ported on the Wahler Physical Symptoms Inventory to several symptom factors.
Before m o o d induction, subjects assigned to the three m o o d groups were administered the Wahler Physical Symptoms In- ventory and the POMS in order to ensure that subjects assigned to the happy, sad, and neutral mood groups did not differ in the severity o f their illnesses or in their m o o d prior to the mood induction procedure. One-way analyses o f variance (ANOVAS) revealed that subjects assigned to the three mood groups did not differ in total number of symptoms reported at the start o f the experiment, F(2, 63) = 0.55, ns, in the discomfort at tr ibuted to those symptoms, F(2, 63) = 0.50, ns, or in their prior m o o d state on any of the POMS subscales, for example, for Depres- sion, F(2, 45) = 0.33, ns. However; the initial Wahler Physical Symptoms Inventory revealed that subjects on average reported nine symptoms on the checklist.
The second prel iminary analysis concerned the identification o f gender differences. A one-way multivariate analysis o f vari- ance (MANOVA) was conducted across all of the dependent vari- ables o f Exper iment 1 with subject gender as the sole indepen- dent variable. This analysis revealed that there were significant gender differences (Wilks's), = 0.26), F(37, 26) = 1.99, p < .05. Follow-up ANOVAs indicated that men and women significantly differed on only one dependent variable, health self-efficacy, F(1, 63) = 6.64, p < .01. Men tended to report greater self- efficacy for the illness-alleviating behaviors than did women (Ms = 58.75 vs. 49.24, respectively). Because there were no
To ensure that differences betwecn groups on the dependent vari- ables in all three experiments were due to the impact of mood and not to differences in imagery content during the mood induction procedure, we compared the events recalled by each of the three mood groups. We looked specifically for differences in health-relevant content and found that, in all three experiments, groups did not differ.
2 We assessed the relationship between mood and intention to engage in illness-alleviating behaviors using a 19-item scale asking subjects to rate the likelihood that they would engage in a variety of specific behav- iors, such as "take a prescription medicine." The variance on this mea- sure was quite restricted. Subjects had little intention of engaging in most of these behaviors. Not surprisingly, these ratings were unaffected by mood. Thus, no further analyses were conducted.
3 The measures in this experiment were presented to subjects in two different randomized orders. A one-way multivariate analysis of vari- ance (MANOVA) across all variables to assess differences due to order was not significant. Hence, the data were pooled over these two orders in all analyses.
MOOD AND HEALTH 543
other gender differences that even approached significance, and subsequent analyses revealed that gender never interacted sig- nificantly with induced mood, all subsequent analyses were pooled over gender.
Finally, because it was inefficient to consider the 28 symp- toms of the Wahler Physical Symptoms Inventory individually in their reactivity to induced mood, we submitted these items to a principal-components analysis with varimax rotation. We compared solutions for ratings of symptoms reported "today" and amount of discomfort due to the symptoms. Factors that were consistent across the two analyses were retained. Using this method, four factors were extracted. These four factors re- vealed symptom clusters common in individuals experiencing the flu or common cold: (a) aches and pains, (b) nasal conges- tion, (c) stomach discomfort, and (d) sleeping irregularities. All subjects reported at least some of these symptoms, but an exam- ination of the range of scores for each of these factors revealed that only subjects' ratings of aches and pains and nasal conges- tion varied widely; ratings on the other two factors fell within a narrow range of the scale. Because symptoms of nasal conges- tion, such as a stuffed nose, are relatively unambiguous, whereas evaluating aches and pains requires more subjective in- terpretion, we expected this latter symptom cluster to be more influenced by mood. Therefore, although we examined the effects of mood on ratings of all four symptom clusters, we fo- cused especially on ratings of aches and pains. We also exam- ined the influence of mood on the total symptom score reflect- ing subjects' ratings across all symptoms.
Mood Manipulation Checks
To examine whether subjects' assigned moods were induced properly and maintained for the duration of the experimental session, two mood measures, the DES and the Six-Item Mood Check, were embedded among the dependent variables of the experiment. A one-way MANOVA across these two variables re- vealed a significant difference due to mood induction condition (Wilks's ~, = 0.36), F(4, 120) = 20.02, p < .0001. Follow-up ANOVAS with linear contrast weights tested the hypothesis that subjects assigned to the happy condition would report greater positive affect than would subjects assigned to the neutral con- dition, who in turn would report greater positive affect than would subjects assigned to the sad conditions. These ANOVAS revealed that the three experimental groups significantly differed in mood reported on the DES and the Six-Item Mood Check, Fs(l, 63) = 111.58 and 29.55, p < .0001, respectively. As indicated by the means reported in Table 1, mood was properly induced and maintained for the duration of the session.
Impact of Mood on Health Cognitions
We began by examining the effects of mood on the appraisal of physical symptoms followed by an analysis of the influence of mood on self-efficacy and outcome expectations for illness- alleviating behaviors. The approach to data analysis was two- pronged. First, we examined mean differences due to mood in- duction. Then, recognizing that the experience of the induced mood might vary in intensity among subjects, we computed Pearson product-moment correlations between reported mood
Table 1 Mean Self-Reported Affect as a Function of Mood Induced in Experiment 1
Mood condition
Measure F Happy Neutral Sad
Differential Emotions Scale 111.58" M 5.22 3.86 2.54 SD 0.98 0.80 0.76 n 22 21 23
Six-Item Mood Check 29.55* M 4.72 3.77 3.12 SD 0.95 1.06 0.91 n 22 21 23
Note. Means in the table reflect ratings on a 7-point scale, with higher numbers indicating greater lx~sitive affect. *p < ,0001.
following mood induction (on the DES) and the various health cognitions across all subjects. We expected a correlational anal- ysis to be somewhat more powerful in this context because it preserves individual levels of responding.
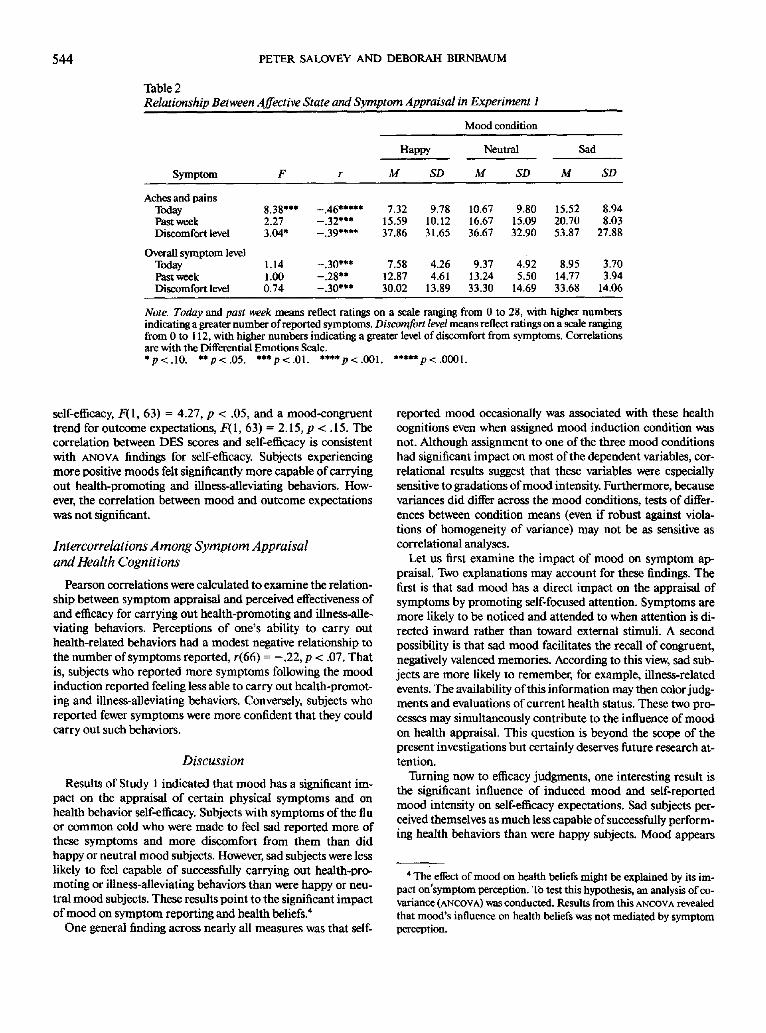
As indicated by the means reported in Table 2, mood had a pronounced effect on the number of aches and pains reported. One-way ANOVAS with linear contrast weights tested the hy- pothesis that sad subjects would report more aches and pains than would neutral subjects but that happy subjects would re- port fewer aches and pains than would neutral subjects. The results indicated that, as expected, sad subjects reported sig- nificantly more aches and pains (today) than did happy subjects, with the neutral mood subjects falling in between, F(1, 63) = 8.38, p < .005. Similar results were obtained for the amount of discomfort attributed to these aches and pains, although results only approached significance, F(I, 63) = 3.04, p < .09. Corre- lations between DES mores, present aches and pains, and dis- comfort from aches and pains corroborated the ANOVA results. As Table 2 indicates, as negative affect increased, the number of aches and pains reported and the discomfort attributed to those symptoms increased. Although the mean number of aches and pains experienced during the past week also varied in a mood-congruent direction, condition differences were not sta- tistically significant. There was a significant correlation between the DES scale and this measure, however.
Unlike aches and pains, mean overall symptom reporting was not significantly different among the mood conditions, although DES reports of mood were negatively correlated with total number of present and past-week symptoms and discomfort at- tributed to them. Finally, as expected, the impact of mood on the remaining three symptom factors other than aches and pains was not significant either between mood conditions using ANOVA$ or across conditions using Pearson correlations.
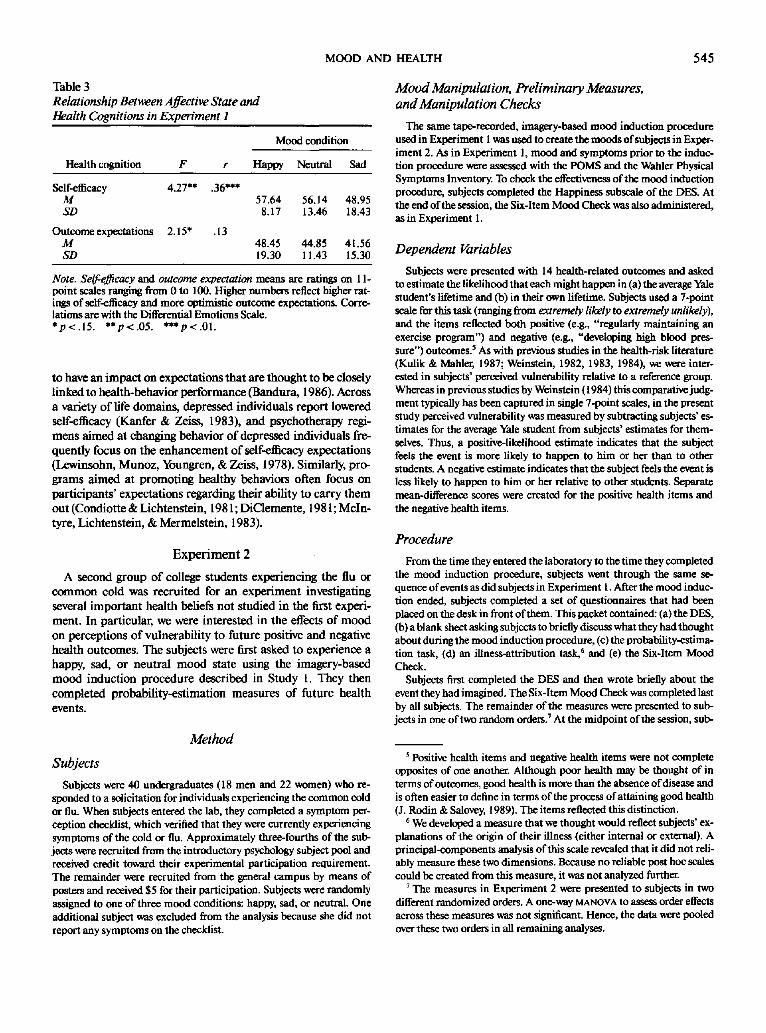
Table 3 displays differences among the three groups in the confidence subjects expressed regarding their ability to carry out a variety of health-related behaviors (self-efficacy) and in their expectations that these behaviors would be effective (out- come expectations). Univariate ANOVAS with linear contrast weights indicated significant mood-congruent differences for
544 PETER SALOVEY AND DEBORAH BIRNBAUM
Table 2 Relationship Between Affective State and Symptom Appraisal in Experiment 1
Mood condition
Happy Neutral Sad
Symptom F r M SD M SD M SD
Aches and pains Today 8.38*** -.46***** 7.32 9.78 10.67 9.80 15.52 8.94 Past week 2.27 -.32*** 15.59 10 .12 16 .67 15 .09 20.70 8.03 Discomfort level 3.04* -.39**** 37.86 31 .65 36.67 32.90 53.87 27.88
Overall symptom level Today 1 .14 -.30*** 7.58 4.26 9.37 4.92 8.95 3.70 Past week 1.00 -.28** 12.87 4.61 13.24 5.50 14.77 3.94 Discomfort level 0.74 -.30*** 30.02 13 .89 33.30 14 .69 3 3 . 6 8 14.06
Note. Today and past week means reflect ratings on a scale ranging from 0 to 28, with higher numbers indicating a greater number of reported symptoms. Discomfort level means reflect ratings on a scale ranging from 0 to 112, with higher numbers indicating a greater level of discomfort from symptoms. Correlations are with the Differential Emotions Scale. *p<.10. **p<.05. ***p<.01. ****p<.001. *****p<.0001.
self-efficacy, F(1, 63) = 4.27, p < .05, and a mood-congruent trend for outcome expectations, F(1, 63) = 2.15, p < . 15. The correlation between DES scores and self-efficacy is consistent with ANOVA findings for self-efficacy. Subjects experiencing more positive moods felt significantly more capable of carrying out health-promoting and illness-alleviating behaviors. How- ever, the correlation between mood and outcome expectations was not significant.
lntercorrelations Among Symptom Appraisal and Health Cognitions
Pearson correlations were calculated to examine the relation- ship between symptom appraisal and perceived effectiveness of and efficacy for carrying out health-promoting and illness-alle- viating behaviors. Perceptions of one's ability to carry out health-related behaviors had a modest negative relationship to the number of symptoms reported, r(66) = - .22 , p < .07. That is, subjects who reported more symptoms following the mood induction reported feeling less able to carry out health-promot- ing and illness-alleviating behaviors. Conversely, subjects who reported fewer symptoms were more confident that they could carry out such behaviors.
Discussion
Results of Study 1 indicated that mood has a significant im- pact on the appraisal of certain physical symptoms and on health behavior self-efficacy. Subjects with symptoms of the flu or common cold who were made to feel sad reported more of these symptoms and more discomfort from them than did happy or neutral mood subjects. However, sad subjects were less likely to feel capable of successfully carrying out health-pro- moting or illness-alleviating behaviors than were happy or neu- tral mood subjects. These results point to the significant impact of mood on symptom reporting and health beliefs. 4
One general finding across nearly all measures was that self-
reported mood occasionally was associated with these health cognitions even when assigned mood induction condition was not. Although assignment to one of the three mood conditions had significant impact on most of the dependent variables, cor- relational results suggest that these variables were especially sensitive to gradations of mood intensity. Furthermore, because variances did differ across the mood conditions, tests of differ- ences between condition means (even if robust against viola- tions of homogeneity of variance) may not be as sensitive as correlational analyses.
Let us first examine the impact of mood on symptom ap- praisal. Two explanations may account for these findings. The first is that sad mood has a direct impact on the appraisal of symptoms by promoting self-focused attention. Symptoms are more likely to be noticed and attended to when attention is di- rected inward rather than toward external stimuli. A second possibility is that sad mood facilitates the recall of congruent, negatively valenced memories. According to this view, sad sub- jects are more likely to remember, for example, illness-related events. The availability of this information may then color judg- ments and evaluations of current health status. These two pro- cesses may simultaneously contribute to the influence of mood on health appraisal. This question is beyond the scope of the present investigations but certainly deserves future research at- tention.
Turning now to efficacy judgments, one interesting result is the significant influence of induced mood and self-reported mood intensity on self-efficacy expectations. Sad subjects per- ceived themselves as much less capable of successfully perform- ing health behaviors than were happy subjects. Mood appears
4 The effect of mood on health beliefs might be explained by its im- pact on'symptom perception. To test this hypothesis, an analysis of co- variance (ANCOVA) was conducted. Results from this Ar~COVA revealed that mood's influence on health beliefs was not mediated by symptom perception.
MOOD AND HEALTH 545
Table 3 Relationship Between Affective State and Health Cognitions in Experiment 1
Mood condition
Health cognition F r Happy Neutral Sad
Self-efficacy 4.27** .36*** M 57.64 56.14 48.95 SD 8.17 13.46 18.43
Outcome expectations 2.15* .13 M 48.45 44.85 41.56 SD 19.30 11.43 15.30
Note. Self-e.ff~cacy and outcome expectation means are ratings on 1 l- point scales ranging from 0 to 100. Higher numbers reflect higher rat- ings of self-efficacy and more optimistic outcome expectations. Corre- lations are with the Differential Emotions Scale. *p< .15 . **p<.05. ***p<.01.
to have an impact on expectations that are thought to be closely linked to health-behavior performance (Bandura, 1986). Across a variety o f life domains, depressed individuals report lowered self-efficacy (Kanfer & Zeiss, 1983), and psychotherapy regi- mens aimed at changing behavior o f depressed individuals fre- quently focus on the enhancement o f self-efficacy expectations (Lewinsohn, Munoz, Youngren, & Zeiss, 1978). Similarly, pro- grams aimed at promoting healthy behaviors often focus on participants ' expectations regarding their ability to carry them out (Condiotte & Lichtenstein, 1981; DiClemente , 1981; Mcln- tyre, Lichtenstein, & Mermelstein, 1983).
E x p e r i m e n t 2
A second group of college students experiencing the flu or c o m m o n cold was recruited for an exper iment investigating several impor tant health beliefs not studied in the first experi- ment. In particular, we were interested in the effects o f mood on perceptions o f vulnerabili ty to future positive and negative health outcomes. The subjects were first asked to experience a happy, sad, or neutral m o o d state using the imagery-based m o o d induction procedure described in Study 1. They then completed probabili ty-estimation measures o f future health events.
Method
Subjects
Subjects were 40 undergraduates (18 men and 22 women) who re- sponded to a solicitation for individuals experiencing the common cold or flu. When subjects entered the lab, they completed a symptom per- ception checklist, which verified that they were currently experiencing symptoms of the cold or flu. Approximately three-fourths of the sub. jects were recruited from the introductory psychology subject pool and received credit toward their experimental participation requirement. The remainder were recruited from the general campus by means of posters and received $5 for their participation. Subjects were randomly assigned to one of three mood conditions: happy, sad, or neutral. One additional subject was excluded from the analysis because she did not report any symptoms on the checklist.
Mood Manipulation, Preliminary Measures, and Manipulation Checks
The same tape-recorded, imagery-based mood induction procedure used in Experiment 1 was used to create the moods of subjects in Exper- iment 2. As in Experiment 1, mood and symptoms prior to the induc- tion procedure were assessed with the POMS and the Walaler Physical Symptoms Inventory. To check the effectiveness of the mood induction procedure, subjects completed the Happiness subscale of the DES. At the end of the session, the Six-Item Mood Check was also administered, as in Experiment I.
Dependent Variables
Subjects were presented with 14 health-related outcomes and asked to estimate the likelihood that each might happen in (a) the average Yale student's lifetime and (b) in their own lifetime. Subjects used a 7-point scale for this task (ranging from extremely likely to extremely unlikely), and the items reflected both positive (e.g., "regularly maintaining an exercise program") and negative (e.g., "developing high blood pres- sure") outcomes? As with previous studies in the health-risk literature (Kulik & Mahler, 1987; Weinstein, 1982, 1983, 1984), we were inter- ested in subjects' perceived vulnerability relative to a reference group. Whereas in previous studies by Weinstein (1984) this comparative judg- ment typically has been captured in single 7-point scales, in the present study perceived vulnerability was measured by subtracting subjects' es- timates for the average Yale student from subjects' estimates for them- selves. Thus, a positive-likelihood estimate indicates that the subject feels the event is more likely to happen to him or her than to other students. A negative estimate indicates that the subject feels the event is less likely to happen to him or her relative to other students. Separate mean-difference scores were created for the positive health items and the negative health items.
Procedure
From the time they entered the laboratory to the time they completed the mood induction procedure, subjects went through the same se- quence of events as did subjects in Experiment I. After the mood induc- tion ended, subjects completed a set of questionnaires that had been placed on the desk in front of them. This packet contained: (a) the DES, (b) a blank sheet asking subjects to briefly discuss what they had thought about during the mood induction procedure, (c) the probability-estima- tion task, (d) an illness-attribution task, 6 and (e) the Six-Item Mood Check.
Subjects first completed the DES and then wrote briefly about the event they had imagined. The Six-Item Mood Check was completed last by all subjects. The remainder of the measures were presented to sub- jects in one of two random orders. 7 At the midpoint of the session, sub-
5 Positive health items and negative health items were not complete opposites of one another. Although poor health may be thought of in terms of outcomes, good health is more than the absence of disease and is often easier to define in terms of the process of attaining good health (J. Rodin & Salovey, 1989). The items reflected this distinction.
6 We developed a measure that we thought would reflect subjects' ex- planations of the origin of their illness (either internal or external). A principal-components analysis of this scale revealed that it did not reli- ably measure these two dimensions. Because no reliable post hoc scales could be created from this measure, it was not analyzed further.
7 The measures in Experiment 2 were presented to subjects in two different randomized orders. A one-way MANOVA to assess order effects across these measures was not significant. Hence, the data were pooled over these two orders in all remaining analyses.
546 PETER SALOVEY AND DEBORAH BIRNBAUM
jects were asked to take a minute to reflect on what they had thought about during the imagination task. This was done to increase the likeli- hood that the induced mood was maintained for the length of the exper- imental session. After subjects completed the Six-Item Mood Check, they were thanked and carefully debriefed, as in Experiment 1.
Results
Preliminary Analyses
Before examining the impact of mood on the dependent vari- ables of this experiment, we conducted two preliminary analy- ses. The first involved examining whether the three mood groups differed in mood or symptoms prior to the mood manip- ulation. The second was an examination of gender differences in probability estimations.
Before mood induction, subjects assigned to the three mood groups were administered the Wahler Physical Symptoms In- ventory and the POMS in order to ensure that subjects assigned to the happy, sad, and neutral mood groups did not differ in the severity of their illnesses or in their mood prior to the mood induction procedure. One-way ANOVAS revealed that subjects assigned to the three mood groups did not initially differ in total number of symptoms reported at the start of the experiment, F(2, 37) = 0.77, ns, in the discomfort attributed to those symp- toms, F(2, 37) = 0.71, ns, or in their prior mood state on any of the POMS subscales, for example, for Depression, F(2, 37) = 0.3 l, ns. However, the initial Wahler Physical Symptoms Inventory revealed that subjects were, in fact, experiencing about eight different symptoms at the start of the experiment.
The second preliminary analysis concerned the identification of gender differences across the variables of this experiment. Two-way ANOVAS, with both mood and gender as independent variables, revealed no main effects for gender on any probability estimate, as well as no significant interactions. Hence, the data were pooled over gender in subsequent analyses.
Mood Manipulation Checks
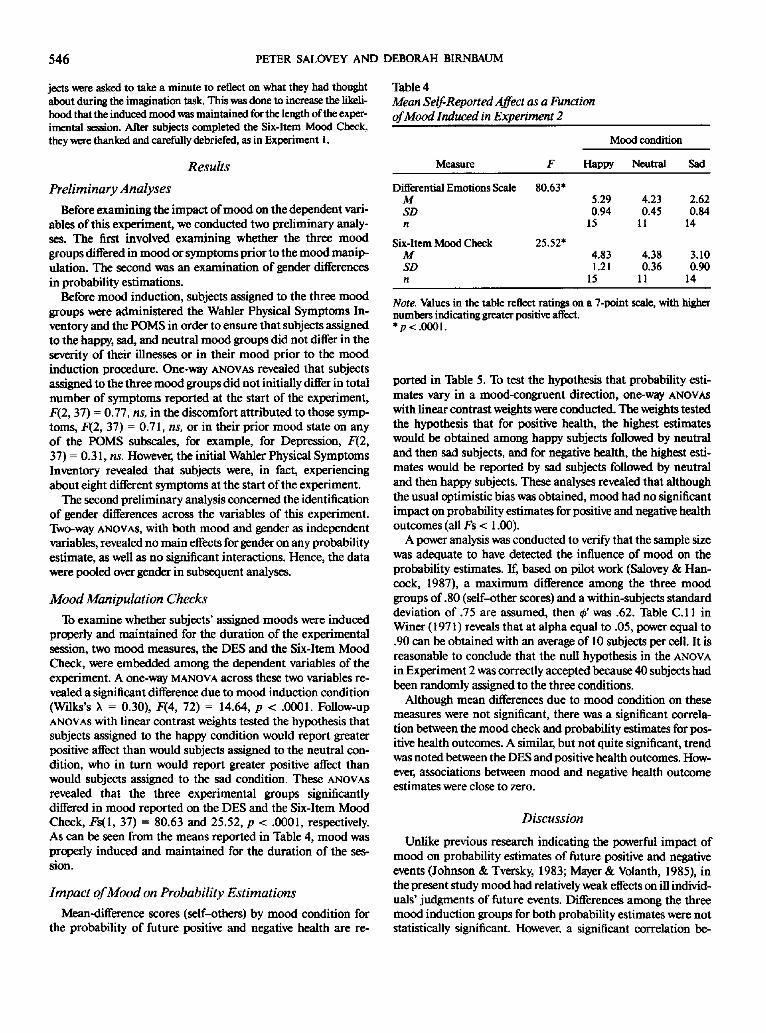
To examine whether subjects' assigned moods were induced properly and maintained for the duration of the experimental session, two mood measures, the DES and the Six-Item Mood Check, were embedded among the dependent variables of the experiment. A one-way MANOVA across these two variables re- vealed a significant difference due to mood induction condition (Wilks's ~, = 0.30), F(4, 72) = 14.64, p < .0001. Follow-up ANOVAS with linear contrast weights tested the hypothesis that subjects assigned to the happy condition would report greater positive affect than would subjects assigned to the neutral con- dition, who in turn would report greater positive affect than would subjects assigned to the sad condition. These ANOVAS revealed that the three experimental groups significantly differed in mood reported on the DES and the Six-Item Mood Check, Fs(l, 37) = 80.63 and 25.52, p < .0001, respectively. As can be seen from the means reported in Table 4, mood was properly induced and maintained for the duration of the ses- sion.
Impact o f Mood on Probability Estimations
Mean-difference scores (self-others) by mood condition for the probability of future positive and negative health are re-
Table 4 Mean Self-Reported Affect as a Function of Mood Induced in Experiment 2
Mood condition
Measure F Happy Neutral Sad
Differential Emotions Scale 80.63* M 5.29 4.23 2.62 SD 0.94 0.45 0.84 n 15 11 14
Six-Item Mood Check 25.52* M 4.83 4.38 3.10 SD 1.21 0.36 0.90 n 15 I1 14
Note. Values in the table reflect ratings on a 7-point scale, with higher numbers indicating greater positive affect. *p< .0001.
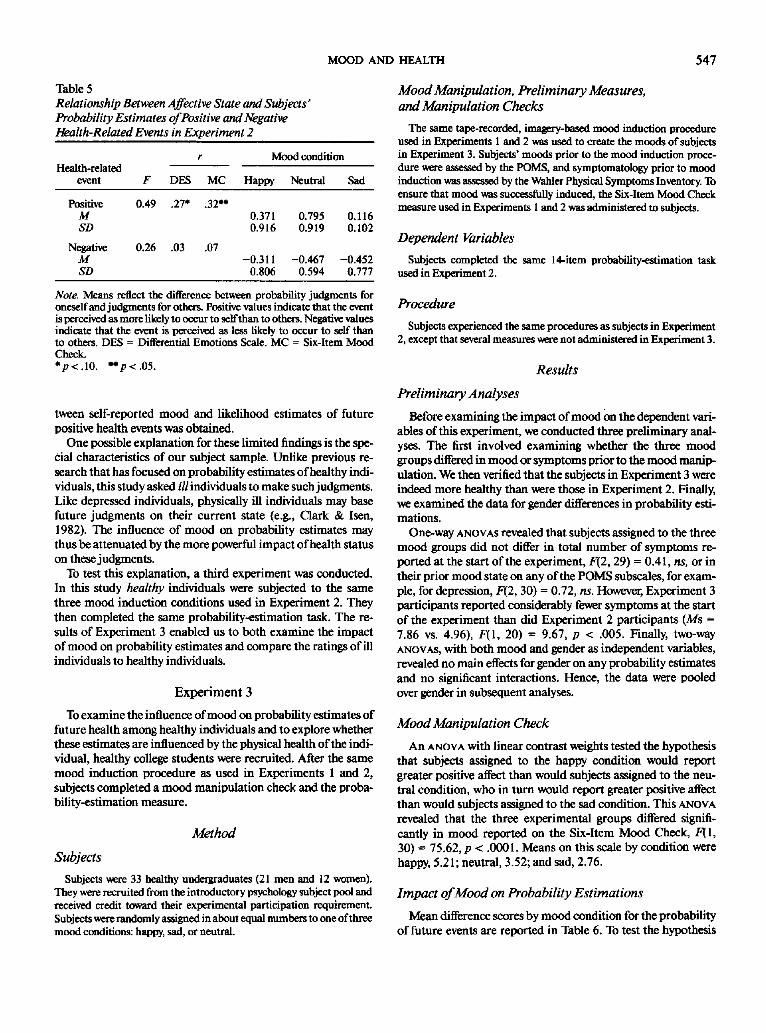
ported in Table 5. To test the hypothesis that probability esti- mates vary in a mood-congruent direction, one-way ANOVAS with linear contrast weights were conducted. The weights tested the hypothesis that for positive health, the highest estimates would be obtained among happy subjects followed by neutral and then sad subjects, and for negative health, the highest esti- mates would be reported by sad subjects followed by neutral and then happy subjects. These analyses revealed that although the usual optimistic bias was obtained, mood had no significant impact on probability estimates for positive and negative health outcomes (all Fs < 1.00).
A power analysis was conducted to verify that the sample size was adequate to have detected the influence of mood on the probability estimates. If, based on pilot work (Salovey & Han- cock, 1987), a maximum difference among the three mood groups of.80 (self-other scores) and a within-subjects standard deviation of .75 are assumed, then # w a s .62. Table C.11 in Winer (1971) reveals that at alpha equal to .05, power equal to .90 can be obtained with an average of l 0 subjects per cell. It is reasonable to conclude that the null hypothesis in the ANOVA in Experiment 2 was correctly accepted because 40 subjects had been randomly assigned to the three conditions.
Although mean differences due to mood condition on these measures were not significant, there was a significant correla- tion between the mood check and probability estimates for pos- itive health outcomes. A similar, but not quite significant, trend was noted between the DES and positive health outcomes. How- ever, associations between mood and negative health outcome estimates were close to zero.
Discussion
Unlike previous research indicating the powerful impact of mood on probability estimates of future positive and negative events (Johnson & Tversky, 1983; Mayer & Volanth, 1985), in the present study mood had relatively weak effects on ill individ- uals' judgments of future events. Differences among the three mood induction groups for both probability estimates were not statistically significant. However, a significant correlation be-
MOOD AND HEALTH 547
Table 5 Relationship Between Affective State and Subjects" Probability Estimates of Positive and Negative Health-Related Events in Experiment 2
r Mood condition Health-related
event F DES MC Happy Neutral Sad
Positive 0.49 .27* .32** M SD
Negative 0.26 .03 .07 M SD
0.371 0.795 0.116 0.916 0.919 0.102
-0.311 -0.467 -0.452 0.806 0.594 0.777
Note. Means reflect the difference between probability judgraents for oneself and judgments for others. Positive values indicate that the event is perceived as more likely to occur to self than to others. Negative values indicate that the event is perceived as less likely to occur to self than to others. DES = Differential Emotions Scale. MC = Six-Item Mood Check. *p<.10. **p<.05.
tween self-reported mood and likelihood estimates of future positive health events was obtained.
One possible explanation for these limited findings is the spe- cial characteristics of our subject sample. Unlike previous re- search that has focused on probability estimates of healthy indi- viduals, this study asked ill individuals to make such judgments. Like depressed individuals, physically ill individuals may base future judgments on their current state (e.g., Clark & Isen, 1982). The influence of mood on probability estimates may thus be attenuated by the more powerful impact of health status on these judgments.
To test this explanation, a third experiment was conducted. In this study healthy individuals were subjected to the same three mood induction conditions used in Experiment 2. They then completed the same probability-estimation task. The re- suits of Experiment 3 enabled us to both examine the impact of mood on probability estimates and compare the ratings of ill individuals to healthy individuals.
E x p e r i m e n t 3
To examine the influence of mood on probability estimates of future health among healthy individuals and to explore whether these estimates are influenced by the physical health of the indi- vidual, healthy college students were recruited. After the same mood induction procedure as used in Experiments 1 and 2, subjects completed a mood manipulation check and the proba- bility-estimation measure.
Method
Subjects
Subjects were 33 healthy undergraduates (21 men and 12 women). They were recruited from the introductory psychology subject pool and received credit toward their experimental participation requirement. Subjects were randomly assigned in about equal numbers to one of three mood conditions: happy, sad, or neutral.
Mood Manipulation, Preliminary Measures, and Manipulation Checks
The same tape-recorded, imagery-based mood induction procedure used in Experiments 1 and 2 was used to create the moods of subjects in Experiment 3. Subjects' moods prior to the mood induction proce- dure were assessed by the POMS, and symptomatology prior to mood induction was assessed by the Wahler Physical Symptoms Inventory. To ensure that mood was successfully induced, the Six-Item Mood Check measure used in Experiments I and 2 was administered to subjects.
Dependent Variables
Subjects completed the same 14-item probability-estimation task used in Experiment 2.
Procedure
Subjects experienced the same procedures as subjects in Experiment 2, except that several measures were not administered in Experiment 3.
Results
Preliminary Analyses
Before examining the impact of mood on the dependent vari- ables of this experiment, we conducted three preliminary anal- yses. The first involved examining whether the three mood groups differed in mood or symptoms prior to the mood manip- ulation. We then verified that the subjects in Experiment 3 were indeed more healthy than were those in Experiment 2. Finally, we examined the data for gender differences in probability esti- mations.
One-way ANOVAS revealed that subjects assigned to the three mood groups did not differ in total number of symptoms re- ported at the start of the experiment, F(2, 29) -- 0.41, ns, or in their prior mood state on any of the POMS subscales, for exam- ple, for depression, F(2, 30) = 0.72, ns. However, Experiment 3 participants reported considerably fewer symptoms at the start of the experiment than did Experiment 2 participants (Ms = 7.86 vs. 4.96), F ( l , 20) = 9.67, p < .005. Finally, two-way ANOVAS, with both mood and gender as independent variables, revealed no main effects for gender on any probability estimates and no significant interactions. Hence, the data were pooled over gender in subsequent analyses.
Mood Manipulation Check
An ANOVA with linear contrast weights tested the hypothesis that subjects assigned to the happy condition would report greater positive affect than would subjects assigned to the neu- tral condition, who in turn would report greater positive affect than would subjects assigned to the sad condition. This ANOVA revealed that the three experimental groups differed signifi- cantly in mood reported on the Six-Item Mood Check, F( I , 30) -- 75.62, p < .0001. Means on this scale by condition were happy, 5.21; neutral, 3.52; and sad, 2.76.
Impact of Mood on Probability Estimations
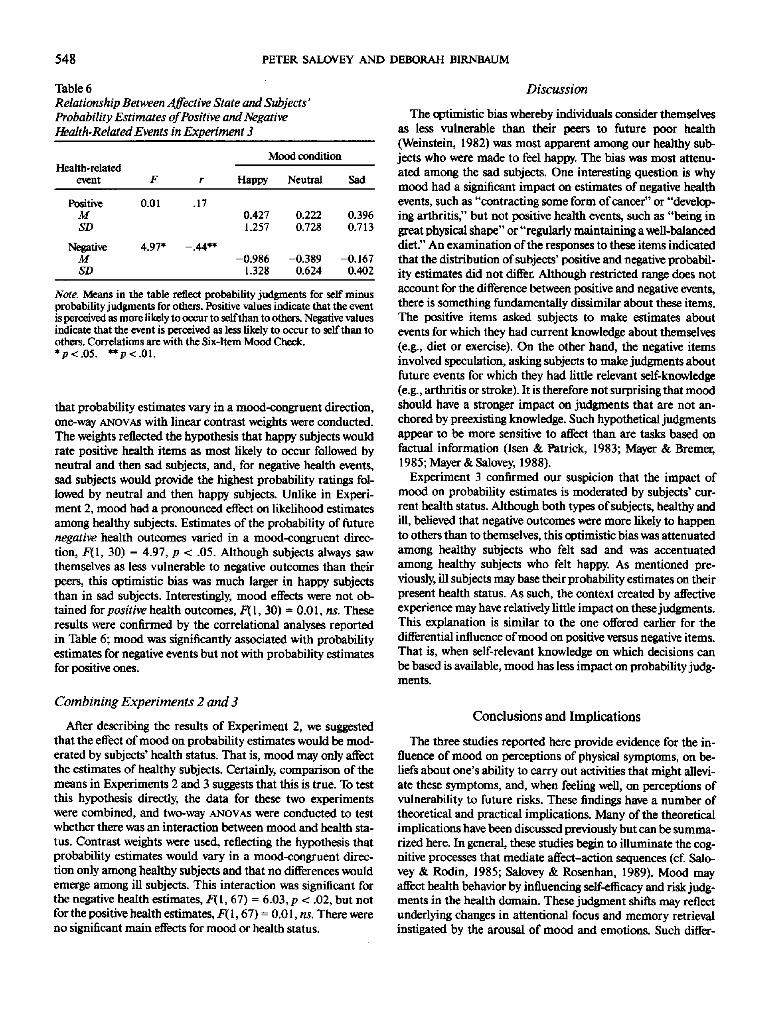
Mean difference scores by mood condition for the probability of future events are reported in Table 6. To test the hypothesis
548 PETER SALOVEY AND DEBORAH BIRNBAUM
Table 6 Relationship Between Affective State and Subjects" Probability Estimates of Positive and Negative Health-Related Events in Experiment 3
Mood condition Health-related
event F r Happy Neutral Sad
Positive 0.01 .17 M SD
Negative 4.97* -.44** M SD
0.427 0.222 0.396 1.257 0.728 0.713
-0.986 -0.389 -0.167 1.328 0.624 0.402
Note. Means in the table reflect probability judgments for self minus probability judgments for others. Positive values indicate that the event is perceived as more likely to occur to self than to others. Negative values indicate that the event is perceived as less likely to occur to self than to others. Correlations are with the Six-Item Mood Cheek. *p < .05. **p < .01.
that probability estimates vary in a mood-congruent direction, one-way ANOVAS with linear contrast weights were conducted. The weights reflected the hypothesis that happy subjects would rate positive health items as most likely to occur followed by neutral and then sad subjects, and, for negative health events, sad subjects would provide the highest probability ratings fol- lowed by neutral and then happy subjects. Unlike in Experi- ment 2, mood had a pronounced effect on likelihood estimates among healthy subjects. Estimates of the probability of future negative health outcomes varied in a mood-congruent direc- tion, F(I, 30) = 4.97, p < .05. Although subjects always saw themselves as less vulnerable to negative outcomes than their peers, this optimistic bias was much larger in happy subjects than in sad subjects. Interestingly, mood effects were not ob- tained for positive health outcomes, F(1, 30) -- 0.0 I, ns. These results were confirmed by the correlational analyses reported in Table 6; mood was significantly associated with probability estimates for negative events but not with probability estimates for positive ones.
Combining Experiments 2 and 3
After describing the results of Experiment 2, we suggested that the effect of mood on probability estimates would be mod- erated by subjects' health status. That is, mood may only affect the estimates of healthy subjects. Certainly, comparison of the means in Experiments 2 and 3 suggests that this is true. To test this hypothesis directly, the data for these two experiments were combined, and two-way ANOVAS were conducted to test whether there was an interaction between mood and health sta- tus. Contrast weights were used, reflecting the hypothesis that probability estimates would vary in a mood-congruent direc- tion only among healthy subjects and that no differences would emerge among ill subjects. This interaction was significant for the negative health estimates, F(I, 67) = 6.03, p < .02, but not for the positive health estimates, F(I, 67) = 0.01, ns. There were no significant main effects for mood or health status.
Discussion
The optimistic bias whereby individuals consider themselves as less vulnerable than their peers to future poor health (Weinstein, 1982) was most apparent among our healthy sub- jects who were made to feel happy. The bias was most attenu- ated among the sad subjects. One interesting question is why mood had a significant impact on estimates of negative health events, such as "contracting some form of cancer" or "develop- ing arthritis;' but not positive health events, such as "being in great physical shape" or "regularly maintaining a well-balanced diet." An examination of the responses to these items indicated that the distribution of subjects' positive and negative probabil- ity estimates did not differ. Although restricted range does not account for the difference between positive and negative events, there is something fundamentally dissimilar about these items. The positive items asked subjects to make estimates about events for which they had current knowledge about themselves (e.g., diet or exercise). On the other hand, the negative items involved speculation, asking subjects to make judgments about future events for which they had little relevant self-knowledge (e.g., arthritis or stroke). It is therefore not surprising that mood should have a stronger impact on judgments that are not an- chored by preexisting knowledge. Such hypothetical judgments appear to be more sensitive to affect than are tasks based on factual information (Isen & Patrick, 1983; Mayer & Bremer, 1985; Mayer & Salovey, 1988).
Experiment 3 confirmed our suspicion that the impact of mood on probability estimates is moderated by subjects' cur- rent health status. Although both types of subjects, healthy and ill, believed that negative outcomes were more likely to happen to others than to themselves, this optimistic bias was attenuated among healthy subjects who felt sad and was accentuated among healthy subjects who felt happy. As mentioned pre- viously, ill subjects may base their probability estimates on their present health status. As such, the context created by affective experience may have relatively little impact on these judgments. This explanation is similar to the one offered earlier for the differential influence of mood on positive versus negative items. That is, when self-relevant knowledge on which decisions can be based is available, mood has less impact on probability judg- ments.
Conclusions and Implicat ions
The three studies reported here provide evidence for the in- fluence of mood on perceptions of physical symptoms, on be- liefs about one's ability to carry out activities that might allevi- ate these symptoms, and, when feeling well, on perceptions of vulnerability to future risks. These findings have a number of theoretical and practical implications. Many of the theoretical implications have been discussed previously but can be summa- rized here. In general, these studies begin to illuminate the cog- nitive processes that mediate affect-action sequences (cf. Salo- vey & Rodin, 1985; Salovey & Rosenhan, 1989). Mood may affect health behavior by influencing self-efficacy and risk judg- ments in the health domain. These judgment shifts may reflect underlying changes in attentional focus and memory retrieval instigated by the arousal of mood and emotions. Such differ-
MOOD AND HEALTH 549
ences in the motivating properties of alfective arousal have been termed emotional intelligence (Salovey & Mayer, 1988).
Because psychological distress appears to intensify the illness experience, mood may have an important influence on deci- sions to seek medical services and treatment. Sick persons who feel sad may be more likely to seek medical care, regardless of the origin of the aifective state. As noted by Croyle and Uretsky (1987), the mood states of ill individuals may also influence physicians' diagnoses, as these are often partially based on pa- tients' appraisals of their own health. The impact of psychologi- cal distress on patients' evaluation of their health may also pose difficulties for the physician who needs to distinguish predomi- nantly somatically based symptoms from those rooted in psy- chological factors. Physicians are often unaware of the extent to which physical well-being may be influenced by affect (Katon, 1984; Nielson & Williams, 1980). As Tessler and Mechanic (1978) noted, " i f practitioners are to be responsive to patients' definitions and perceptions of their needs, they must give atten- tion not only to tangible evidence of illness hut also to patients' total life circumstances" (p. 262).
In addition to influencing treatment-seeking behavior, pa- tients' mood states may also affect their adherence to treatment regimens. Although ill individuals who feel sad may be more likely to report symptoms and seek medical care, our data sug- gest that they may be less likely to believe they can successfully carry out illness-alleviating behaviors. In addition, they are somewhat more likely to have pessimistic expectations regard- ing the effectiveness of these behaviors. Adherence to treatment regimens, particularly those that require a great deal of patient participation, may thus be determined in part by the patient 's affective state. This nonadherence may subsequently prolong the illness experience. Indeed, research indicates that negative mood may, in fact, retard recovery from illness (Bruhn, Chand- ler, & Wolf, 1969; Imboden, Canter, Cluff, & Trevor, 1959).
Mood may also influence the course of the illness. Imboden, Canter, and Cluff ( 1961 ) suggested that because features of psy- chological distress, such as fatigue and weakness, are similar to symptoms common in physical disorders, depressed mood is often misattributed to the physical illness, even after the so- matic basis for the illness has "run its course" This misinterpre- tation of psychological distress as physical distress and the bias- ing influence of mood on the recall of mood-congruent, illness- relevant material (Isen, 1984) may explain why psychological distress slows recovery from physical illness (Croyle & Uretsky, 1987). The relationship between depressed mood and the pro- gression of illness has been noted by Friedman and Booth-Kew- ley (1987), who, in their analysis of the "disease-prone personal- ity," argued that
the treatment of medical patients by health psychologists and clini- cal psychologists seems prudent and worthwhile. At the very least, such interventions may improve the psychological adjustment among a high risk population. Such intervention may also have a beneficial effect on the progression or recurrence of serious chronic illness. (p. 552)
References
Amrhein, J., Salovey, P., & Rosenhan, D. L. (1981). Joy and sadness generate attributional vulnerability in men. Unpublished manuscript, Stanford University, Stanford, CA.
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behav- ioral change. PsychologicalReview, 84, 191-215.
Bandura, A. (1986). Social foundations of thought and action. Engle- wood Cliffs, N J: Prentice-Hall.
Bandura, A. (in press). Self-efficacy mechanisms in physiological activa- tion and health-promoting behavior. In J. Madden, S. Matthysse, & J. Barchas (Eds.), Adaptation, learning, and affect. New York: Raven Press.
Becket, M. H. (Ed.). (1974). The health belief model and personal health behavior. Thorofare, NY: Charles B. Slack.
Becker, M. H., Haefner, D. P., Kasl, S. V., Kirscht, J. P., Maiman, L. H., & Rosenstock, I. M. (1977). Selected psychosocial models and corre- lates of individual health-related behaviors. Medical Care, 15, 27--46.
Blaney, P. H. (1986). Affect and memory: A review. Psychological Bulle- tin, 99, 229-246.
Bhimer, D., & Heilbronn, M. (1982). Chronic pain as a variant of de- pressive disease: The pain-prone disorder. Journal of Nervous and Mental Disease, 170, 381-406.
Bower, G. H. (1981). Mood and memory. American Psychologist, 36, 129-148.
Brewer, D., Donghtie, E. B., & Lubin, B. (1980). Induction of mood and mood shift. Journal of Clinical Psychology,, 36, 215-226.
Brockner, J., Hjelle, L., & Plant, R. W. (1985). Self-focused attention, self-esteem, and the experience of state depression. Journal of Person- ality, 53, 425-434.
Bruhn, J. G., Chandler, B., & Wolf, S. (1969). A psychosocial study of survivors and nonsurvivors of myocardial infarction. Psychosomatic Medicine, 31, 318-319.
Clark, M. S., & Isen, A. M. (1982). Toward u n ~ d i n g the relation- ship between feeling states and social behavior. In A. Hastorf& A. M. Isen (Eds.), Cognitive social psychology (pp. 73-108). Amsterdam: Elsevier.
Condiotte, M. M., & Lichtenstein, E. (1981). Self-efficacy and relapse in smoking cessation programs. Journal of Consulting and Clinical Psychology,, 49, 648-658.
Croyle, R. T., & Uretsky, M. B. (1987). Effects of mood on self-appraisal of health status. Health Psycholog£ 6, 239-253.
Cummings, K. M., Jette, A. M., Brock, B. M., & Haefner, D. P. (1979). Psychosocial determinants of immunization behavior in a swine in- fluenza campaign. Medical Care, 17, 639-649.
Cummings, N. A., & FoUette, W. T. (1976). Brief psychotherapy and medical utilization. In H. Darken (Ed.), The professionalpsychologist today(pp. 165-174). San Francisco: Jossey-Bass.
DiClemente, C. C. (1981). Self-efficacy and smoking cessation mainte- nance: A preliminary report. Cognitive Therapy and Research, 5, 175-187.
Fenigstein, A., & Carver, C. S. (1978). Self-focusing effects of false heart- beat feedback. Journal of Personality and Social Psychology,, 36, 1241-1250.
Follette, W. E, & Cummings, N. A. (1967). Psychiatric services and medical utilization in a prepaid health plan setting. Medical Care, 5, 25-35.
Friedman, H. S., & Booth-Kewley, S. B. (1987). The "disease-prone personality": A meta-analytic view of the construct. American Psy- chologist, 42, 539-555.
Gilligan, S. G., & Bower, G. H. (1984). Cognitive consequences of emo- tional arousal. In C. Izard, J. Kngan, & R. Zajonc (Eds.), Emotions, cognition, and behavior (pp. 547-588). New York: Cambridge Uni- versity Press.
Goodwin, A. M., & Williams, J. M. G. (1982). Mood induction re- search: Its implications for clinical depression. Behavioral Research and Therap£ 20, 373-382.
Hendler, N. (1984). Depression caused by chronic pain. Journal of Clin- ical Psychiatry, 45, 30-36.
550 PETER SALOVEY AND DEBORAH BIRNBAUM
Hollister, L. E. (1983). Treating depressed patients with medical prob- lems. In J. M. Davis & J. W. M_aa$ (Ed$.), Affective disorders (pp. 393- 408). Washington, DC: American Psychiatric Press.
Holzman, A. D., Cline, J. C., & Rudy, T E. (in press). Chronic pain and depression: Application of a cognitive-behavioral model. Clinical Journal of Pain.
Imboden, J. B., Canter, A., & Cluff, L. E. ( 1961). Separation experiences and health records in a group of normal adults. Psychosomatic Medi- cine, 25, 433-440.
Imboden, J. B., Canter, A., Cluff, L. E., & Trevot; R. W. (1959). Brucel- losis: III. Psychologic aspects of delayed convalescence. Archives of Internal Medicine, 103, 406--414.
Ingrain, R. E., & Smith, T. W. (1984). Depression and internal versus external focus of attention. Cognitive Therapy and Research, 8, 139- 152.
Isen, A. M. (1984). Toward understanding the role of affect in cognition. In R. Wyer & T. SruU (Eds.), Handbook of social cognition (Vol. 3, pp. 179-236). HiUsdale, NJ: Erlbaum.
Isen, A. M., & Daubman, IC A. (1984). The influence of affect on cate- gorization. Journal of Personality and Social Psychology,, 47, 1206- 1217.
Isen, A. M., Daubman, K. A., & Nowicki, G. P. (1987). Positive affect facilitates creative problem solving. Journal of Personality and Social Psychology,, 52, 1122-1131.
Isen, A. M., & Patrick, R. (1983). The effects of positive feelings on risk taking: When the chips are down. Organizational Behavior and Human Performance, 31, 194-202.
Isen, A. M., Shalker, T., Clark, M., & Karp, L (1978). Positive affect, accessibility of material in memory, and behavior. A cognitive loop? Journal of Personality and Social Psycholog)g, 36, 1-12.
Izard, C. E. ( 1971 ). The face of emotion. New York: Appleton-Century- Crofts.
Johnson, E. J., & Tversky, A. (1983). Affect, generalization, and the perception of risk. Journal of Personality and Social Psychology,, 45, 20-33.
Jones, K., & Vischi, T. (1979). Impact of alcohol, drug abuse, and men- tal health treatment on medical care utilization: Review of the re- search literature. Medical Care, 17(Suppl. 12), 1-82.
Kanfer, R., & Zeiss, A. M. (1983). Depression, interpersonal standard setting, and judgments of self-efficacy. Journal of Abnormal Psychol- ogy, 92, 319-329.
Katon, W. (1984). Depression: Relationship to somatization and chronic medical illness. Journal of Clinical Psychiat~ 45, 4-11.
Kavanagh, D. J., & Bower, G. H. (1985). Mood and self-efficacy: Impact of joy and sadness on perceived capabilities. Cognitive Therapy and Research, 9, 507-525.
Keefe, E J., Wilkins, R. H., Cook, W. A., Crisson, J. E., & Muhlhaier, L. H. (1986). Depression, pain, and pain behavior. Journal of Con- sulting and Clinical Psychology,, 54, 665-669.
Kems, R. D., Haythornthwaite, J., & CAller, E. (1987, August). Cogni- tive mediators of the relationship between chronic pain and depres- sion. Paper presented at the 95th Annual Convention oftbe Ameri- can Psychological Association, New York.
Kulik, J. A., & Mahler, H. I. M. (1987). Health status, perceptions of risk, and prevention interest for health and nonbealth problems. Health Psychology, 6, 15-27.
Lewinsohn, P. M., Munoz, R. E, Youngren, M. A., & Zeiss, A. M. (1978). Controlyour depression. Englewood Cliffs, NJ: Prentice-Hall.
Maddox, G. L. (1962). Some correlates of differences in self-assessment of health status among the elderly. Journal of Gerontology, 17, 180- 185.
Mayer, J. D. (1986). How mood influences cognition. In N. E. Sharkey (Ed.), Advances in cognitive science (Vol. 1, pp. 290-314). Chichester, England: Ellis Horwood.
Maye~ J. D., & Breme~ D. (1985). Assessing mood with affect-sensitive tasks. Journal of Personality Assessment, 49, 95-99.
Mayer, J. D., & Salovey, E (1988). Personality moderates the interaction of mood and cognition. In IC Fiedler & J. Forgas (Eds.), Affect, cogni- tion, and social behavior (pp. 87-99). Toronto: Hogrefe.
Mayer, J. D., & Volanth, A. J. (1985). Cognitive involvement in the emo- tional response system. Motivation and Emotion, 9, 261-275.
Mclntyre, K. O., Lichtenstein, E., & Mermelstein, R. J. (1983). Self- efficacy and relapse in smoking cessation: A repfication and exten- sion. Journal of Consulting and Clinical Psychology, 51, 632-633.
McKusick, L., W'dey, J., Coates, T. J., & Morin, S. E (1986). Predictors of AIDS behavioral risk reduction: The AIDS behavioral research project. Paper presented at the New Zealand AIDS Foundation Pre- vention Education Planning Workshop, Auckland, New Zealand.
McNair, D., I.off, M., & Droppleman, L. ( 1971). EDITS manual for the Profile of Mood States. San Diego, CA: Educational and Industrial Testing Service.
Murphy, E (1982). Social origins of depression in old age. British Jour- nal of Psychiatry, 141, 135-142.
Nielson, A. C., & Williams, T A. (1980). Depression in ambulatory medical patients. Archives of General Psychiatry, 37, 999-1004.
O'Leary, A. (1985). Self-efficacy and health. Behavior Research and Therapy, 23, 437-451.
Persson, L-O., & Sjoberg, L. (1987). Mood and somatic symptoms. Journal of Psychosomatic Research, 31, 499- 51 I.
Pyszczynski, T., & Greenberg, J. ( 1985). Depression and preferences for self-focusing stimuli following success and failure. Journal of Person- ality and Social Psychology, 49, 1066-1075.
Pyszczynski, T., & Greenberg, J. (1986). Evidence for a depressive self- focusing style. Journal of Research in Personality, 20, 95-106.
Pyszczynski, T, & Greenberg, J. (1987). Self-regulatory perseverafion and the depressive self-focusing style: A self-awareness theory of de- pression. Ps~hological Bulletin, 102, 122-138.
Pyszczynski, T., Holt, K., & Greenherg, J. (1987). Depression, self-fo- cused attention, and expectancies for future positive and negative events for self and others. Journal of Personality and Social Psychol- ogy, 52, 994-1001.
Rodin, G., & Voshatt, K. (1986). Depression in the medically ill: An overview. American Journal of Psychiat~ 143, 696-705.
Rodin, J., & Salovey, E (1989). Health psychology. AnnualReview of Psychology,, 40, 533-579.
Rogers, R. W., & Mewborn, C. R. (1976). Fear appeals and attitude change: Effects of a threat's noxiousness, probability of occurrence, and the efficacy of coping responses. Journal of Personality and Social Psychology, 34, 54-61.
Rosenhan, D. L., Salovey, P., & Hargis, K. (1981). The joys of helping: Focus of attention mediates the impact of positive affect on altruism. Journal of Personality and Social Psychology, 40, 899-905.
Salovey, P. (1986). The effects of mood and focus of attention on self- relevant thoughts and helping intention. Unpublished doctoral disser- tation, Yale University, New Haven, CT.
Salovey, P., & Hancock, M. E. (1987). The effects of state mood, trait depression, and cognitive set on personal health appraisal. Unpub- lished manuscript, Yale University, New Haven, CT.
Salovey, P., & Mayer, J. D. (1988). Emotional intelligence. Manuscript submitted for publication.
Salovey, P., & Rodin, J. (1985). Cognitions about the self." Connecting feeling states and social behavior. In P. Shaver (Ed.), Self, situations, and socia7 behavior: Review of personality and social psychology (Vol. 6, pp. 143-166). Beverly Hills, CA: Sage.
Salovey, P., & Rosenhan, D. L. (1983, August). Effects ofjoy, attention, and recipient "s status on helpfulness. Paper presented at the 91 st An- num Convention of the American Psychological Association, Ana- heim, CA.

MOOD AND HEALTH 551
Saiovey, P., & Rosenhan, D. L. (1989). Mood and prosocial behavior. In H. L. Wagner & A. S. R. Manstead (Eds.), Handbook of social ps~haphysiology (pp. 371-391). Chicheste~ England: Wiley.
Salovey, P., & Singer, J. A. (1989). Mood congruency effects in recall of childhood versus recent memories. Journal of Social Behavior and Personality, 4, 99-120.
Seheier, M. E, & Carver, C. S. (1977). Self-focused attention and the experience of emotion: Attraction, repulsion, elation, and depres- sion. Journal of Personality and Social Psychology, 35, 625-636.
Seheier, M. E, Carver, C. S., & Gibbons, E X. (1981). Self-focused at- tention and reactions to fear. Journal of Research in Personality, 15, 1-15.
Singer, J. A., & Salovey, E (1988). Mood and memory: Evaluating the network theory of affect. Clinical Psychology Review, 8, 211-251.
Smith, T. W., & Greenberg, J. (1981). Depression and self-focused at- tention. Motivation and Emotion, 5, 323-33 I.
Smith, T. W., Ingrain, R. E., & Roth, D. L. (1985). Self-focused atten- tion and depression: Self-evaluation, affect, and life-stress. Motivation and Emotion, 9, 381-389.
Strack, S., Blaney, P. H., Ganellen, R. J., & Coyne, J. C. (1985). Pessi- mistic self-preoccupation, performance deficits, and depression. Journal of Personality and Social Psychology,, 49, 1076-1085.
Tessler, R., & Mechanic, D. (1978). Psychological distress and perceived health status. Journal of Health and Social Behavior, 19, 254-262.
Tessle~ R., Mechanic, D., & Dimond, M. (1976). The effect ofpsycho- logical distress on physician utilization: A prospective study. Journal of Health and Social Behavior, 17, 353-364.
Turk, D. C., Rudy, T. E., & Salovey, E (1984). Health protection: Atti- tudes and behaviors of LPNs, teachers, and college students. Health Psychology,, 3, 189-210.
Turk, D. C., Rudy, T. E., & Stieg, R. L. (1987). Pain and depression: 1. "Facts:' Pain Management, 1, 17-26.
Turk, D. C., & Salovey, P. (1984). "Chronic pain as a variant of depres- sive disease": A critical reappraisal. Journal of Nervous and Mental Disease, 172, 398-404.
Tversky, A., & Kahneman, D. (1973). Availability: A heuristic for judg- ing frequency and probability. Cognitive Psychalogy, 5, 207-232.
Velten, E. A. (1968). A laboratory task for induction of mood states. Behavior Research and Theral~,, 6, 473-482.
Wahler, H. J. (1968). The Physical Symptoms Inventory: Measuring levels of somatic complaining beliavior. Journal of Clinical Psychol- ogy, 24, 207-211.
Weber, J., Coates, T. J., & McKusick, L. (1986). Denial may hinder AIDS risk reduction: The AIDS behavioral research project. Unpub- lished manuscript, University of California, San Francisco.
Wegner, D. M., & Giuliano, T. (1980). Arousal-induced attention to sel£ Journal of Personality and Social Psychalog~, 38, 719-726.
Weinstein, N. D. (1982). Unrealistic optimism about susceptibility to health problems. Journal of Behavioral Medicine, 5, 441-460.
Weinstein, N. D. (1983). Reducing unrealistic optimism about illness susceptibility. Health Psychology, 2, 11-20.
Weinstein, N. D. (1984). Why it won't happen to me: Perceptions of risk factors and susceptibility. Health Psychology, 3, 431-457.
Winer, B. J. (1971). Statistical principles in experimental design (2nd ed.). New York: McCffaw-Hill.
Wright, J., & Miscbel, W. (1982). Influence of affect on cognitive social learning person variables. Journal of Personality and Social Psychal- ogy, 43, 901-914.
Received June 14, 1988 Revision received November 21, 1988
Accepted February 14, 1989 •




























