Embed Size (px)
Citation preview

INFLUENZA I
VERNON KNIGHI

T A B L E O F C O N T E N T S
D E F I N I T I O N . . . . . . . . . . . . . . . . . . 3
HISTORY . . . . . . . . . . . . . . . . . . . . 5
PROPERTIES OF THE V I R U S ." . . . . . . . . . . . . 5
S t r u c t u r e a n d Rep l i ca t ion . . . . . . . . . . . . 5 H e m a g g l u t i n i n a n d N e u r a m i n i d a s e . . . . . . . . . 7 N o m e n c l a t u r e of In f luenza V i r u s . . . . . . . . . . 10
EPIDEMIOLOGY . . . . . . . . . . . . . . . . . 13 A n t i g e n i c V a r i a t i o n , E p i d e m i c s a n d P a n d e m i c s . . . . 13 A n t i g e n s of In f luenza V i r u s be fo re 1934 . . . . . . . 15 C h a n g i n g M o r t a l i t y of I n f l u e n z a . . . . . . . . . . 16 F u t u r e O c c u r r e n c e of I n f l u e n z a E p i d e m i c s . . . . . . 20 Ep idemio log i c S u r v e i l l a n c e of I n f l u e n z a by V i r u s
I so l a t ion . . . . . . . . . . . . . . . . . 20
T H E DISEASE IN M A N . . . . . . . . . . . . . . . 2 6
P a t h o g e n e s i s . . . . . . . . . . . . . . . . . 26 Cl in ica l F e a t u r e s . . . . . . . . . . . . . . . 27 P u l m o n a r y Compl i ca t i ons . . . . . . . " . . . . . 27 Vi ra l C h e m o t h e r a p y . . . . . . . . . . . . . . 27 T r e a t m e n t of B a c t e r i a l P n e u m o n i a . . . . . . . . . 30 R e y e ' s S y n d r o m e . . . . ' . . . . . . . . . . . 31 O t h e r C o m p l i c a t i o n s . . . . . . . . . . . . . . 31 In f luenza a n d L e u k e m i a . . . . . . . . . . . . . 32
IMMUNOLOGY . . . . . . . . . . . . . . . . . . 3 3
Def in i t ion of Ce l l -Med ia t ed I m m u n e Resp o n s e . . . . . 33 Effect o f N a t u r a l I l lness a n d V a c c i n a t i o n on t h e Cel l -
M e d i a t e d I m m u n e S y s t e m . . . . . . . . . . . 33 S u p p r e s s i o n of C e l l - M e d i a t e d I m m u n i t y d u r i n g In f luenza l
I l l nes s . . . . . . . . . . . . . . . . . . 35 D e l e t e r i o u s Effect of C e l l - M e d i a t e d I m m u n i t y in
In f luenza . . . . . . . . . . . . . ' . . . . 36 A n t i b o d y R e s p o n s e in I n f l u e n z a . . . . . . . . . . 38
DIAGNOSIS . . . . . . . . . . . . . . . . . . . 4 0
PREVENTION . . . . . . . . . . . . . . . . . . 42 I m m u n i z a t i o n . . . . . . . . . . . . . . . . 42 A m a n t a d i n e Hydroch lo r i de . . . . . . . . . . . . 43
SUMMARY . . . . . . . . . . . . . . . . . . . 44

is Professor and Chairman, Department of Microbiology and Immunology and Head, Section of Infectious Diseases, Depart- ment of Internal Medicine at Baylor College of Medicine, Hous- ton, Texas. Doctor Knight received his M.D. degree from Harvard Medical School in 1943. With associates at the National Insti- tutes of Health in 1961, he began studies, continued at Baylor and supported by an NIH-established Influenza Research Center, ofrespiratory virus diseases. This research has included observa- tions on the pathogenesis, immunology and epidemiology of these diseases, evaluation of vaccines, viral chemotherapy, properties of viral aerosols and, currently, the problem of influenza.
IN RECENT YEARS, the volume of research on influenza has greatly increased, particularly in relation to the origin of epidemics and pandemics, the properties of the virus, the immunology of the disease, the development of improved vaccines and, to some extent, specific chemotherapy. This article will review the status of these developments.
DEFINITION
Influenza is an acute infectious disease of the respiratory tract caused by the influenza virus. It occurs in localized outbreaks, epidemics and world-wide pandemics. The fre- quent recurrences of the disease in persons of all ages, the high morbidity and the significant mortality distinguish it from other respiratory viral diseases and implicate it as one of the major unsolved problems of world health. Three immunologically distinct types of human influenza, A, B and C, have been identified. Type A strains cause pandem- ics every decade or so and are also responsible for epidem- ics every 2 -3 years in most localities. Influenza B causes more.limited epidemics every 4 - 6 years. Influenza C rare- ly causes detectable disease, although antibody to this vi- rus is widespread in the population.

GEOGR,,kPHIGAL AND HISTORICAL
PATHOLOGY:
DR. AUGUST HIRSCH, PAOIPP.-sIoa 0F ~JCDIC|~I& IN "r ~IIZSL~I'[Y OI" BZILIJL~'.
I'],ru~oIo~J~Cal ~urrey of e~m(c~ of ~nj~ue~za accord[~ to rOtOr(Is P~I~tn~j~ro?R t.I~C *Jcar$ 1 1 7 3 ~ 1 8 7 5 .1
Year.
I D I t + $ 7
1 4 ~ 4
14II S + S ~
1417 s $ ~ o
s$$7
s $ ~ s
Season of the El.ldem c.
Docember Auguet . bIarch. J~u~.ry .
March �9 �9 . .
F e b r . a ~ . September
July . August "i
July . . ~.ugu~t
September
October .
Autumn .
Amlt of E Dldee~{c Pte',IJeece..
Italy (,). Germany (~). E~gl,md (3). Italy an(1 Fraace (,). Italy (,). Italy (J) France: ~rontpcll;er (~). GermAn: ($). QermDj~.r! ~xony and Thur~gL~ (I). r~ae
Nethe' l~nds : Flauders 0). France: PadJ (0- Italy." ]~logm.~ (s), Forl[ (z), Yenlce (1),
Florence (§ France : Paris (5). France: P~r;s (x). General diffusion in ~urope (1, 1). Italy : ~ (I). Franc* (t). Engl~ud (s}. General d~-us[on ~ ~urop~ Sicily (O- Italy ( :) : Padua (I), Lomb~-dy (4)- Dalm~
Ua 0 ) . Switzerland (5)- France (6) : Poit/~ (7), MoutpeUier ($), Nis, meg(9).
Netherlands: Har~rwyk (so), ~ m o ~ r (s l ) Spain (ss).
General d]ff~s;on in Italy (s. s, 3").
TF~I~SL~TED I'I~OM THE SECOND Gs EDITION
] z
CHARLES CREIGHTON, M.D.
L O N D O N ;
T ] ] ~ .~EW SYDJ~NIIAM SOCIETY.
ISS3.
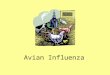
Fig. 1.-Composite of title page and first page of text of Hirsch's classic work on the history of influenza epidemics.
4

HISTORY
According to Hirsch, the first record of epidemics pre- sumed to be influenza began in A.D. 1173. A composite of the title page and the first portion of the text of the English translation of his book by Charles Creighton in 1883 is reproduced in Figure 1. One can imagine that the epidem- ics must have been substantial to have been recorded, quite possibly of pandemic magnitude. The epidemics in 1173 involved three countries, but it was 150 years before the next reference to influenza in 1323; thereafter, 4 per centu- ry were recorded until 1500, when general diffusion of the disease occurred in Europe in 1510 and 1557-1562, both possibly pandemics. In keeping with this possibility is the onset of disease in the summer, a feature of'recent pandem- ics in Europe and the United States.
Influenza epidemics occurred infrequently during the middle portion of the nineteenth century, but a major pan- demic began in 1889 and large epidemics occurred in 1898-1900 in the United States. Since then, world pan- demics occurred in 1918-1920, 1957-1960 and 1968- 1970.
PROPERTIES OF THE VIRUS
STRUCTURE AND REPLICATION
The structure of the influenza virus indicating the 10ca- tion of the antigens and other constituents is shown in Figure 2. In addition to replication in its natural host, in- fluenza virus grows in embryonated eggs, in mice after adaptation by serial passage, in monkey, hamster and bo- vine kidney, and in chick embryo fibroblast cells.
Figure 3 illustrates the time sequence and site of forma- tion of the various subunits of the virus in the cell. After adsorption and penetration, which may take an hour or more, an eclipse period begins, during which there is no morphologic evidence of virus in the cell. By about 3 hours, the nucleoprotein antigen appears in the nucleus and shortly thereafter neuraminidase and hemagglutinin anti- gens appear in the cytoplasm. Assembly and extrusion of

~ R N A NUCLEOPROTEIN PROTEIN } POLYMERASE (?) NEURAMINIDASE MEMBRANE
~ ~ EMAGGLUTININ! HEMAGGLUTININ 2 ACTIVE HEMAGGLUTININ LIPID
i i . . . . . ~
HEMAGGLUTININ ACTIVE HEMAGGLUTININI HEMAGGLUTININ HEMAGGLUTININz "
Fig. 2.-- Diagrammatic representation of a segment of an influenza virus particle. The hemagglutinin and neuraminidase subunits, which protrude as "spikes" from the surface of the virus, are attached by their hydro- phobic regions to the lipid envelope. The ratio of hemagglutinin to neur- aminidase spikes varies from strain to strain (Webster et al,, 1968), but the relative distribution of these on the surface of the virus particle is not known. The orientation of the nucleoprotein RNA complex in the virion has not been fully elucidated; these complexes occur in segments when extracted from the virion but may be linked within the virion by labile bonds. Polymerase activity has been demonstrated within the core of the virion but the location is not known. (From Kilbourne, E. D. [ed.], The In- f luenza Viruses and Inf luenza [New York: Academic Press, 1975], p. 276.)
the new virus by budding from the plasma membrane begins by about the sixth hour.
Specific cytopathic effects of the virus do not occur, al- though, after many hours, cytoplasmic granules and round- ing of cells with fragmentation of the cell sheet may be observed. Despite the lack of early change in. the appear- ance of the cells, profound suppression of cell protein syn- thesis occurs in the first few hours after inoculation, and a similar pattern of events must take place in the infected respiratory epithelium of patients. This is illustrated in Figure 4. The top portion of the figure (A) shows the extent of incorporatipn of tritiated leucine into cell proteins in a 15-minute pulse and a 45-minute chase in uninfected chick

I I i i i I I I I O I 2 3 4 5 6
HOURS Fig. 3.-Time sequence of influenza virus replication: (1) adsorption,
(2) penetration, (3) uncoating, (4) eclipse, (5) viral nucleoprotein antigen pieces (intranuclear), (6) viral nucleoprotein helix, (7) hemagglutinin, (8) cytoplasmic ribonucleoprotein, (9) neuraminidase is formed in the cytoplasm, (10) budding virus and (11) pedunculated virus, viral outer coat continuous with host cell membrane. (From Knight, V., and Kasel, J. A.: Influenza Viruses, in Viral and Mycoplasmal Infections of the Respiratory Tract [Philadelphia: Lea & Febiger, 1973], Chap. 6, pp. 87-123.)
embryo fibroblast cells. The lower section (B) shows the production of viral proteins in similar cells several hours after inoculation with influenza virus. ShOwn also are pro- tein peaks produced from purified influenza virus run in the same gel. If peaks attributable to virus proteins are excluded, it is evident that, at most, very small amounts of cell protein are being produced.
Suppression of cell protein synthesis is characteristic of cells infected with many viruses, and whether or not the cell is visibly damaged by infection, the arrest of cell pro- tein synthesis undoubtedly is the first step in the develop- ment of lesions in the host animal.
HEMAGGLUTININ AND NEURAMINIDASE
The hemagglut inin (Fig. 3) functions primarily to attach virus to cells that later become infected. Sites on the hem- aggl.utinin glycoprotein attach to neuraminic acid radicals on the surface of cells, which is followed by penetration.

600
500
400
500
2OO
I00 (3-
i "1-
6OO
5OO
4O0
5OO
2O0
100
0
A . 7 2 , 0 0 0
B. ~ ~ 600
5O0 7 5 , 0 0 0
300 I I l i l t IW o.ooo ~ 200 D
I00
I0 20 :50 40 50 60 70 80 90 FRACTIONS
Fig. 4.--Protein biosynthesis measured by incorporation of tritiated leucine into chick embryo fibroblast cell culture and into chick embryo fibroblast culture infected with influenza A/PR8/34(HONI). Cells were harvested following a 15-minute pulse with leucine 3H and a 45-minute chase period. After sonication and treatment with hot sodium dodecyl sulfate to solubilize proteins, the proteins were separated by chromatog- raphy on a column of 7.5~ acrylamide gel with 8 m urea. A. distribution of cell proteins according to molecular weight. Two main peaks of cell proteins of 72,000 and 33,000 molecular weights were determined from marker proteins run concurrently on the gels. B, heavy black line shows peaks of proteins from infected cells after 15 hours of incubation. Viral proteins are identified by crosshatched peaks obtained from purified virus co-electrophoresed. The purified virus peaks demonstrate that substan- tially all of the proteins are of viral origin, indicating that viral infection has virtually stopped biosynthesis of cell protein. (From Knight, V., unpub- lished observations.)

!.' . . ~ . ~ ' . . . d ~- ~..- :~ ; :~ , : - . : :~ : . - " ~~ S.-
Fig. 5 . -A, rhesus monkey kidney cell culture (uninfected) with guinea pig red blood cells added. 13, rhesus monkey kidney cell culture infected with type A influenza virus with added guinea pig red blood cells. Note the clumping of red blood cells on the surface of the infected tissue culture cells. (Courtesy of J. A. Kasel, National Institute of Allergy and Infectious Diseases.) (From Knight, V., and Kasel, J. A.: Influenza Viruses, in Viraland Mycoplasmal Infections of the Respiratory Tract [Philadelphia: Lea & Febiger, 1973], Chap. 6. pp. 87-123.) g

Mucus also contains neuraminic acid, which can bind virus and prevent cell attachment; however, neuraminidase, the other surface structure on the influenza virus, is an enzyme that cleaves neuraminic acid radicals from the parent car- bohydrate molecules and thus frees the virus. Neuramini- dase also destroys virus receptors on cells, but this reaction takes place more slowly than cell penetration so that infec- tion of cells is not prevented.
The hemagglutinin also attaches to but does not infect red blood cells. Adsorption of red cells to infected cells is the basis for preliminary identification of influenza infec- t!on (Fig. 5) and for the titration of virus pools. As a result of removal of neuraminic acid receptor sites, red cells that have been agglutinated by influenza virus and freed by neuraminidase no longer will hemagglutinate.
The hemagglutinin is a tetramer of two pairs of glycopro- teins (Fig. 2). Major changes in antigenicity of influenza virus result from changes in antigenic determinants locat- ed on the hemagglutinin. Hemagglutination-inhibiting and neutralizing antibody are a response to the hemagglutinin.
Neuraminidase, also a tetramer of two pairs of glycopro- teins (Fig. 2) induces formation of antibody that has some protective role against infection. It undergoes less frequent antigenic change than the hemagglutinin.
NOMENCLATURE OF INFLUENZA VIRUSES
Influenza virus types A, B and C are classified as ortho- myxoviruses. They are subdivided according to type on the basis of the nucleoprotein (NP) antigen. This antigen ap- pears in extracts of infected tissues or cell cultures sepa- rate from virions, and because of its small size it is also referred to as soluble (S) antigen. Antibody to this antigen apparently has no role in immunity. Type A influenza vi- ruses from man, horses, swine and birds contain identical NP antigens.
The division of influenza type A strains into subtypes depends on the antigenic characteristics of the hemagglu- tinin and neuraminidase components on the surface of the virus. Current classification of influenza A viruses of hu- man origin is shown in Table 1, and the principal eras of
10

cO z < z
z~ ~
~ N N
N ~
mNt-- Zm Z
zm~m mwm
,...1
~ m
z ~
z -6
<
e~ -6 E z 5 .
S~ ocr~
o~ ~..=
influenza virus subtype predominance are shown in Figure 6. The hemagglutinin of the first influenza A virus isolated was designated H0 whereas the neuraminidase was given the designation N1. In 1947, 1957 and 1968, hemaggluti- nin antigen changes were successively designated H1, H2 and H3.
The new nomenclature also provides several types of in- formation about the origin of the virus. For example, the
11

A(H2-H3N2) era
AI swine era
- - - . . . . - ? 1814 - 1815 , A(H2N2)-like virus
1890.~--.-~ Hong Kong A(H3N2I-IIke and 1889 - A/equi(Heq2Neq2)- like virus
1 I
- - 1918- 1919 ~ Pandemic
I ~ A/swine-like virus
! 19f ~ A(HONI) vir us
1946 ~ ~ A(HINI) virus
i 1957 - 8 . ~ Pandemic A(H2N2) virus A(H3N2) era 1968
I ~ H0ng Kong (H3N2)virus related to A I equi(Heq2N2) virus
Fig. 6 . - D i a g r a m m a t i c representation of influenza eras. (Modified from Masurel, N., and Marine, W. M., 2 and Masurel, N.: Serological character- istics of a "new" serotype of influenza A virus: the Hong Kong strain, Bull WHO 41:467, 1969.)
first HON1 strain was isolated in Puerto Rico (PR) in 1934. The number 8 following the place name or its abbreviation is the culture accession number. A proper name sometimes is used instead of the place of isolation as a designation. The last number is the year of isolation.
Type B influenza viruses are genetically less mobile, and
12

TABLE 2.-TYPE B AND C INFLUENZA VIRUSES
REFERENCE STRAIN
B/l.~e/40 B/GL/1739/54 BIMd/1/59 Bfraiwan/2/62 B/Mass/3/66 B/Vic/98926/70 B/Mass/72 C/Taylor/1233/47
the limited information now available on the two antigens of this virus do not permit its detailed classification. Recent type B virus prototypes are listed in Table 2. Only one type C virus has been described.
EPIDEMIOLOGY
ANTIGENIC VARIATION, EPIDEMICS AND PANDEMICS
The changes in antigenicity of hemagglutinins of influ- enza virus A leading to new subtypes were described in the preceding section. Such large changes are referred to as antigenic "shift." There is, however, a continuing lesser degree of change within subtypes; this has been called anti- genic "drift." The lat ter apparently results from the selec- tion of mutants with some resistance to the antibody in the partially resistant population.
Serologic evidence of the antigenic drift of hemaggluti- nin antigens since introduction of the H3N2 subtype in 1968 is shown in Table 3. Thus, the ti ter of the Hong Kong/68 antiserum with homologous antigen was 1 : 1920 whereas it was 1:160 with the Port Chalmers antigen and 1:40 with the 1974 Scotland/74 variant. The Scotland variant has also drifted considerably from the Port Chalmers/73 strain. This drift is the basis for the inclusion of the Scotland strain in the 1975-1976 vaccine. The drift of neuramini- dase antigens since 1968 is shown in Table 4.
The appearance of strains with different antigenicity usually is followed by epidemics as the new antigen finds a
13

TABLE 3.-ANTIGENIC CROSS REACTIONS OF VARIOUS INFLUENZA VIRUSES AS INDICATED BY HEMAGGLUTINATION
INHIBITION (HI) TESTS*
ANTIGEN
"FERRET ANTISERA
A/Hong Kong/8/68 1920 1920 80 80 80 <40 A/England/42/72 480 4840 640 60 320 60 A/Pt. Chalmers/l/73 160 640 1280 240 640 160 A/Georgia]101/74 160 320 320 640 240 60 A/Georgia/l/75 240 640 960 240 640 80 A/Scetland/840/74 40 160 160 40 80 640
*Average of two tests. To identify and characterize influenza strains, each virus isolate is tested
with reference antisera. The resulting HI titers are compared with the titers given by homologous virus controls (reading vertically). An isolate which reacts with a reference antiserum at a titer equal to that of the reference homologous virus (• one 2-fold dilution) is considered to resemble closely the reference virus in its hemagglutinin antigen.
Thus, HI testing with A/Port Chalmers/l/73 serum demonstrates that A/Georgia/i/75 (titer of 960) closely resembles A/Port Chalmers/ 1/73 (homologous titer 1280); while A/Georgia]101/74 and A/Scetland/840/74 with titers 4-fold arid 8-fold lower than the homologous A/Port Chalmers/ 1/73 titer show more antigenic drift from this reference strain.
From Morbidity and Mortality Weekly Report, p. 105, March 15, 1975.
susceptible populat ion in which to circulate, and in the course of a season or two, the new s t ra ins will be d is t r ibuted world wide.
The genet ic m e c h a n i s m of ant igenic shift, which appar- en t ly is l imited to inf luenza A, is less well understood, bu t it m a y be re la ted to the p h e n o m e n o n of viral recombina- tion. The genome of the inf luenza virus consists of seven loosely l inked segments , and it has been found t h a t influ- enza A viruses in mixed cu l tu re will produce progeny wi th var ious combinat ions of h e m a g g l u t i n i n and neu ramin idase ant igens. This p re sumab ly represents mix ing genome pieces of pa ren t viruses to form the new strains. By the use of suspending media con ta in ing ant ibody to an t igens t h a t are not desired, it is possible to direct the format ion of vi- rus so tha t ant igenic character is t ics are selected. Recombi-
14

TABLE 4.-NEURAMINIDASE INHIBITION TEST RESULTS.* CHICKEN ANTISERA
ANTIGEN
A/Hong Kong/8/68 2471 717 94 MEngland/42/72 631 4677 661 A/Pt. Chalmers/l/73 380 316 903 AJAllegheny/101174 436 724 1096 MSootland/840/74 479 346 479
*Average of two tests. ~Recombinant possessing A/equine/Prague/
1/56(Heql) and indicated N2 antigen. From Memorandum of June 25, 1975, Dowdle,
W. R., The WHO Collaborating Laboratory for Influenza, Atlanta.
nation has also been effected in vivo by inoculation of tur- keys with different strains of influenza A viruses. It ap- pears to many investigators that natura l ly occurring re- combination is the best explanation for the appearance of new subtypes with antigenic characteristics unrelated to the one that immediately preceded it.
ANTIGENS OF INFLUENZA VIRUS BEFORE 1934
An opportunity to make a serologic analysis of the anti- genic character of viruses responsible for some epidemics and pandemics in the half-century before 1934 became pos- sible as a result of an observation by Davenport and his associates. ~ They found that the antibody response to the virus responsible for an individual's first infection with influenza, which occurs during the first few years of life, will be recalled during later influenza infections along with the primary response to the current infecting strain. This event is referred to as "the doctrine of original antigenic sin." Thus, by testing the sera of persons who were only a few years of age at the time of earlier epidemics and pan- demics, inferences are possible concerning the antigenic character of the virus causing the epidemic. The value of
15

these analyses was greatly increased by the finding that antibody recalled from some infections in childhood shared antigens with viruses that were the cause of later epidem- ics. An analysis based on this thesis by Masurel and Marine 2 is described in Figure 6. Although the dates are inferential, there appears to b e a n antigenic relationship between viruses that circulated about 1875 and the sub- type responsible for the 1957 pandemic, and a relationship between viruses that caused the 1889-1890 pandemic and the 1968 Hong Kong virus. The hemagglutinin antigen of equine influenza that first appeared in horses in the United States in 1963 (A/equi/1/Miami/63/Hequi 2 Neq2) is re- lated to the human Hong Kong strain that appeared in 1968 and exhibits a serologic relationship to the Hong Kong-like strain that appears to have circulated about 1890. The hemagglutinin of the swine agent isolated in 1933,' by serologic evidence, is related to human strains that were prevalent in 1918, 1934 and 1946.
This evidence supports the concept of recycling of influ- enza virus antigens in an orderly sequence and shows a strong cross reactivity of human strains of influenza virus- es with those of two other animal species. Sharing of anti- gens between human influenza viruses and avian species has also been described. The mechanism by which influen- za virus antigens might reappear after many years when antibody to them has largely disappeared has not been defined, but recombination involving human and/or animal strains is an intriguing possibility.
CHANGING MORTALITY OF INFLUENZA
A consistent and substantial change in the character of influenza since the pandemic of 1918-1920 is a reduction in mortali ty and a reduction in the proportion of deaths due to respiratory causes (pneumonia, influenza, bronchi- t/s, emphysema). For example, in 1918-1920 it was esti- mated that there were 540,000 deaths due to influenza in the United States and that 90% of these were caused di- rectly by respiratory diseases (influenza and pneumonia). In the years 1957-1960 (Japanese influenza pandemic), more than 100,000 deaths were attr ibuted to influenza in the United States (Table 5), but only about one-third were
16

E~
o~
~ z
~ m
~ m Z ~
m Z
'1
r~
,.-1
o
I. d E . : ~ <
z 0
( )
0
F-t.1F.x.1F-t.1 ~.t.l r.~l F-t.1F..:.I Et.l ~
o
1 7

0
0
O0
X
0
E'-'
2 :
r~
I
,-1
C~
,--.~ LO t'O 0
~'xl o t'-,, 0
l~. ,q, QO co "q' ,-~
,~ t.O r~
0 c~
0
~ o ~ cJ ~j
~ o h R
18

directly attributable to respiratory causes (Table 6). 3 Thus, there was a fivefold reduction in total mortality, which would be about tenfold if corrected for the larger present population, and a sharp reduction in deaths due directly to respiratory causes. These trends began in the years imme- diately following the 1918-1920. pandemic and were pro- nounced before chemotherapy and antibiotics were avail- able.
In connection with the reduction in mortal i ty and death from respiratory causes, it is of interest to examine mortal- i ty according to age at death (Fig. 7). In 1892, in Massachu- setts, a sharp rise in mortal i ty occurred with increasing age after 55, with an enormous toll among persons over 70 years of age. In 1918 there were three peaks of high mor- tality: infancy, 20 -40 years of age and old age. The mortal- i ty in old age was considerably less than in 1892 and was, in fact, not greater than tha t among the 20-40-year age group. The suggestion has been made tha t mortali ty in the older age group was reduced because of the existence of antibody to the swine agent acquired in childhood some 70 years earlier. Housworth and Spoon 4 also showed a sparing of persons 75 years of age and older in the 1968-1969 pan-
Fig. 7.-Pneumonia and influenza mortality by age in certain epidemic years. (From Dauer, C. C., and Serfling, R. E.: Mortality from influenza 1957-1958, and 1957-1960, Am. Rev. Respir. Dis. 83:25, 1961.)
2, 000 [-- / 1892
I / haSSACHUSEITS
1,500 /
1918 c=
l ~ / ~ / " REGISTRATION AREA
/ UNIT~O STARES
500
O STATES
o - ----"?'- ---- --- ...... -" 0 I0 20 30 40 50 60 10 80 90
AGE
19

demic, presumably indicating prior experience with this agent in early childhood.
FUTURE OCCURRENCE OF INFLUENZA EPIDEMICS
Masurel and Marine 2 have suggested that by 1985 only persons 65 years and older will have antibody to the swine- like agent that caused the pandemic of 1918 and, therefore, a recycling of this agent would have its greatest impact on people less than 65 years of age. These observations sug- gest the possible occurrence of a pandemic caused by a swine-like agent in the period 1985-1991.
Before 1985, however, another major antigenic change in the present A strains is expected that could lead to a pan- demic before 1980. The appearance of an influenza virus in 1974 in Scotland that differed considerably from the 1973 Port Chalmers strain that is in present vaccines signaled the need for including this new virus strain in coming vac- cines. According to the WHO Laboratory, the rapid drift indicated by the difference between the 1973 Port Chal- mers and the 1974 Scotland strains resembles events that preceded the occurrence of the 1957 and 1968 pandemics.
EPIDEMIOLOGIC SURVEILLANCE OF INFLUENZA BY VIRUS ISOLATION
One of the major problems in influenza epidemiology is the early detection and measurement of intensity of epi- demics. The changing character of the occurrence of the disease from a primary cause of death to that of increasing mortal i ty from a variety of other diseases has been de- scribed. This change diminishes the value of the measure- ment of excess of mortali ty due to pneumonia and influenza as a means of quantifying epidemics and pandemics. Other indirect measures of the impact of influenza are surveys of absenteeism from school or work. These kinds of data are conveniently obtained because such information is required for other purposes as well, bu t there is increasing doubt that these measures can provide the information that is necessary to solve problems that have evolved from de- veloping knowledge of the disease and its cause.
20

>.
7 ~ e F~2r:
II
w s!aaluasqv ft.
- ~ o
~ e X O N D - = ~ o 6
~ ~ r
" 5 o = 2 O Q . ~ .z*
<~ ox: 0 0 (,9}-- a) 0"~"
E d o ~ r - O o
"~ ~ ' "~ ~ E
-- >. cram .c
,.5 0 "--~
7~eo
E o o~-
< , E ~ _ ~
A greater appreciation of influenza epidemics and pan- demics will require continuing comprehensive case detec- tion by virus isolation on a year-around basis by a sam- pling procedure that will be representative of the popula- tion under study. An example of such surveillance and its advantages are illustrated in the study described in the fol- lowing section.
HOUSTON STUDY.- In the past year in Houston, a program was started under the sponsorship of the Influenza Re-
21

E E ~
II
1
luasqv o/~
~ o m o ~
o ~ - - .~- ~ ~ ~
~o~ < ~D CD ~ .
(D~ t- 0
1.~ O . Q ~ U) .
~ I D ' o .
o O ~ c --~ o ~ "6 c ~
Z a~ . - " ~
r ~ e ' o ~ e 2:} E~ o
o ~ = , , , o ~
--- e- .-- E
~ r-- '~-- "~ ~ -&,-- ~o ~- ~ c~ o ,
<
O ~ ~- ~D I - - ~ . . - - l ~ I o ~ ~~ ~Z='e ~
~" =E o'~g
search Center at Baylor College of Medicine and the Hous- ton City Health Department to obtain more detailed infor- mation on the occurrence of influenza. The 'program con- sisted of taking cultures for influenza virus from cases of febrile respiratory disease in selected physicians' offices and satellite clinics scattered widely about the city. In ad- dition, records were kept of admissions for pneumonia at a
22

children's hospital and two large general hospitals; the numbers of deaths from pneumonia and influenza in the city were available from the City Heal th Department. Re- ports of absenteeism due to illness were obtained from the Houston Independent School District and from a large de- par tment store chain.
The results of one season of study have shown the value of case detection of influenza by virologic examination and the limitation of some of the older methods of study tha t utilize only morbidity and mortali ty data. Figure 8 com- pares school absenteeism in 1974-1975 with a 5-year me- dian. The percentage of absenteeism is nearly identical in both groups and therefore does not suggest the occurrence of an influenza epidemic in 1974-1975. Figure 9 shows absenteeism in a department store chain from all illness and tha t caused by respiratory illness. There is a moderate increase in respiratory illness throughout the spring sea- son. This is about what was expected, and no prior data are available for comparison. This is not considered to be ade- quate evidence of an influenza outbreak.
In contrast, the number of admissions for pneumonia to three hospitals began to increase in late December, reached a peak in J anua ry 1975, with a slow decrease in March (Fig. 10). A number of these patients had i~afluenza Virus isolated from throat swabs. Graphed also is the number of pneumonia and influenza deaths in Houston during this period,* and the peak of their occurrence coincides with those of admissions for pneumonia and isolations of influ- enza virus from outpatients. These data, although sugges- tive, do not verify the occurrence of an epidemic. �9
However, surveillance by virus isolation from early De- cember 1974 to the end of March 1975 showed the contin- ued presence of a virus serologically similar to influenza A(H3N2)/Port Chalmers/1973 (Table 7). The peak occur- rence of positive cultures was in the period from January 12 to February 16, 1975, when one-fourth to one-half of throat swabs yielded influenza virus. Estimates of the fre- quency of disease based on virus isolations throughout the
*Deaths in this study were recorded on actual date of occurrence where- as data submitted to CDC are processed by date of receipt. Adequate data were not available to determine whether the deaths recorded by actual date of occurrence constituted an excess of mortality.
23

o-- -o SHI~F~(] VZN3rlI:INI (]NV VIN01~'n3Nd "ON
I I I I
: -'~]]~,l t l ]a SNOISSIW(]V VINOWn3Ncl 30 ~]QWnN
J
0 r- ___~ ~ o
o ~ o
00,- o mC) ~ o . ~-
~ ,... 0 .o ~ 1 7 6
F-O ~ O~
~o . , , - n O
O ~ o v
�9 7_ 0 - ~ E n
o o "~_ (n ( o = O O E- -E ~
:3 O") (:.) O
,r" O ~ O ' ~ {::).."r N ~ N ~ _ o c o c o
O~l-=._~ ~ =._ .~._= o
__ t- ~-
�9 ~ ' E r " ~ o o 5 - , - o ~ o o E ~ . ~ E i E ~
n', ~ o ~ - . o = o - : : O . ) {.-. O o
n ~ . , - o . 0 ~3
city suggested the occurrence of about 50,000 cases of influ- enza over a several-week period in Houston in January and February 1975. These findings were considered to be indic- ative of an epidemic of influenza. In a further effort to con- firm the epidemic, regional data on excess mortality from a several-state area including Texas, as submitted to CDC, were reviewed but did not indicate the occurrence of an epidemic. The Center for Disease Control, DHEW, Atlanta, then selectively examined mortality data for the city of
24

0 r.~
0
Z 0
,..-1 ~
I < Z ~ O m
O ~
Z ~
< b l
Z r.,.l
z I
t-:
r
N
r~
g
N 2
~ N
o
. . ~ c ~
25

Houston alone; these data, although indicating some excess of mortality, were not sufficient to indicate the occurrence of an epidemic.
It seems probable that many local epidemics of influenza will not be of a magnitude sufficient to cause enough excess mortali ty on a regional or even a municipal basis to be de- tectable as an epidemic. Therefore, study of such outbreaks will depend more on direct methods involving case finding and virologic diagnosis. It is hoped that future studies of this sort will increase our knowledge of the occurrence of epidemics and improve our ability to control them.
THE DISEASE IN MAN
PATHOGENESIS
Influenza virus is present in respiratory secretions of in- fected patients in titbrs ranging up to one million or more 50%-tissue-culture-infectious doses (TCID50) per ml and undoubtedly is discharged in particles produced by cough, sneezes and other expiratory actions. Although unstable at temperatures above 4 ~ C, the virus survives generation in aerosol, particularly at low humidity. Infection in volun- teers can be produced either by inhalation of small-particle aerosol or by intranasal introduction of suspensions of vi- rus. By small-particle aerosol, the 50% human infectious dose is about 3 TCID50. By the intranasal route, the 50% human infectious dose is tenfold or more greater than that. It seems apparent that infected persons would be capable of producing enough virus to cause infection by either route, i.e., small-particle aerosols produced by coughs and sneezes , or intranasal inoculation by large droplets or direct contact with infected secretions. However, the low infectious dose by small-particle aerosol, the tendency of small particles to remain in suspension and to diffuse widely, the rapidity of spread of the disease and the high attack rate all suggest an important role for small-particle aerosol in transmis- sion.
Once implanted, the virus multiplies in the respiratory epithelium. How far down the respiratory "tract infection occurs in uncomplicated influenza is not known. The find-
26

ing of increased resistance in peripheral airways and the frequent occurrence of high-pitched expiratory wheezes in patients with uncomplicated influenza suggest that i n - volvement of peripheral airways is not unusual.
CLINICAL FEATURES
The disease usually has an incubation period of 1 -5 days. Clinical onset often is sudden and may be associated with a dry, ticklish throat and rhinorrhea followed by coughing, systemic symptoms with fever, chills, myalgia and headache. Vomiting occurs occasionally, but abdom- inal pain and diarrhea do not ordinarily occur in influenza.
Despite prostrating illness, physical findings are mini- mal unless there is pneumonia. There is a slight polymor- phonuclear leukocytosis and lymphopenia .during the first day or so of illness followed by neutropenia, but the other laboratory findings usually are within normal limits.
PULMONARY COMPLICATIONS
Influenza in a healthy person usually is an acute, self- limited febrile illness lasting a few days and often is fol- lowed by a period of asthenia. Complications, when they occur, are largely due to pulmonary infection with the vi- rus alone or with secondary bacterial pneumonia. The fre- quency of pneumonia is variable in different epidemicsl but once pneumonia occurs, the prognosis is grave. Pneumococ- ci and drug-resistant staphylococci were frequent causes of bacterial pneumonia in recent epidemics, and the hemolyt- ic streptococcus and H. influenzae were reduced over their role in earlier epidemics. A phenomenon probably related to antimicrobial therapy was the occurrence in 1968-1969, and in some epidemics since then, of secondary pneumonia due to drug-resistant gram-negative bacteria.
VIRAL CHEMOTHERAPY
No special t reatment is required for the usual cases of influenza other than rest, analgesics and observation for
27

O
w
I r >-
, /
~ ~ o --2
C
o.
~ ! !
~ n
121 W 0 I - -
' I
Z - -
z ~ ~o ~
J ~ j
-J 0
o z-
o
m. O
~ i ~
~4~ q W e t ~-
~'(xl
~
I I l l l
O-
IjJO
~J v
I
Lu Z
-J .
o "E cz -- O~d ~
' - 6 - 9
E - ~ ~
22aa
�9 ~ ~2
c ~
o o
3 ~ - N
~ ,- . O -.~ 0_
I T _ - ~ '
~o~
~ o
the possible occurrence of complications. Amantadine hy- drochloride (Symmetrel) has, however, been shown to re- duce the fever and symptoms of the disease but has little effect on virus shedding, at least in doses that have been used (100 mg twice daily in adults). The course of influenza illness in 2 patients, one treated with amantadine, is shown in Figure 11. The more rapid defervescence in the treated patient is in accord with results of studies with large groups of patients, as is the apparent lack of effect of
2 8

t reatment on virus shedding. Larger doses of amantadine (300-400 mg per day) have been used extensively in treat- ment of parkinsonism and in some cases of influenzal pneu- monia in adults with infrequent toxicity, which usually consists of tremors, drowsiness and, rarely, syncope. Sei- zures have occurred on rare occasions in some patients, possibly representing a toxic effect of amantadine. A possi- ble accentuation of congestive failure in some cases of Pa~'- kinson's disease treated with amantadine is also under evaluation. Amantadine is poorly excreted in renal failure, with consequent accentuation of toxicity. Dosages should be materially reduced in such patients. Experience is limit- ed in the t rea tment-of influenzal pneumonia with large doses of amantadine, but the problem should be investi- gated more thoroughly.
AEROSOL TREATMENT OF EXPERIMENTAL INFLUENZA INFEC-
TION IN MICE. -- Stephen and his associates 5 recent ly have made some observations on the t rea tment of experimental influenza in mice by small-particle aerosol that may have potential use in man (Fig. 12). They found that r imantad- ine, an analogue of amantadine, was significantly protec- tive when given as a continuous small-particle aerosol for several days beginning 72 hours after viral inoculation. By this time, lung virus titers had reached or passed their peak titers of 10 T-5-108.0 egg infectious doses of virus per lung. Only 10% of untreated controls survived inocula- tion with the mouse-adapted strain influenza A/Aichi/ 2/68(H3N2). Animals given r imantadine by the intraperi- toneal route or by single 80-minute dosage periods of small- par t ic le aerosol per day showed a significant increase in survival approximating 40%. However, animals t reated continuously from 72 to 168 hours after inoculation showed a survival rate of about 70%. If a single dose of kanamycin was given on day 6, survival rate was increased still fur- ther. Amantadine and ribovarin given in continuous small- particle aerosol produced a similar result. It ~;r also noted that lung titers of virus and lung lesion scores were sig- nificantly lowered in animals t reated with amantadine and ribovarin.
Many factors must be evaluated before studies of this sort can be made in man, but the marked favorable effect of
29

I00'
75,
21-DAY SURVIVAL OF MICE INFECTED WITH INFLUENZA . AND TREATED WITH RIMANTADINE DAYS 3 - 7
>.
~o
RIM~kNTADINE (8 mg/kg/doy)
,im ,it
RLMANTADINE -'1" KANAMYGIN (Smg/kg/doy),,~,(I6.4 mg/kg do,/6}
~ SPA (80 role/day| SPA pCONTINUOUS)
(once dolly}
)1l me p,cO.OI GOMPARED TO VIRUS GONTROL . . . .
Fig. 12.-Comparison of treatment of influenza infection in the mouse with rimantadine by small-particle aerosol (SPA) (95% particles < 6.5 /~m diameter) and by the intraperitoneal route (IP). Continuous aerosol was given for 24 hours daily from day 3 to day 7 of infection. All treated groups showed significantly greater survival than did controls. The high- est survival occurred with continuous aerosol. Results by aerosol were somewhat improved by the addition of kanamycin. These results indicate that continuous small-particle aerosol given late in infection provided a highly significant degree of protection that was superior to that afforded by the medication given by the intraperitoneal route. (From Walker, J. S., unpublished results, with permission.)
three different drugs given by continuous aerosol suggests the need for further study. The distribution and retention of small-particle aerosols in the respiratory tract of man are summarized in reference 6.
The usual case of influenzal pneumonia appears several days after onset of influenza illness, and current modes of therapy in these cases is singularly unsuccessful; thus, this disease might be benefited by a treatment that could be started late in illness.
TREATMENT OF BACTERIAL PNEUMONIA
The treatment of bacterial pneumonia with antibiotics should be as indicated for the bacterial species causing the
30

infection. The prognosis, however, is worse in patients with bacterial pneumonia complicating influenzal pneumonia than when it occurs alone, especially that due to drug:re- sistant staphylococci.
REYE'S SYNDROME
This clinicopathologic ent i ty .has been observed most commonly as a rare sequel to influenza B, chickenpox and some other respiratory viral diseases of childhood. A few cases complicating influenza A have also been described. It is characterized by a usually mild prodromal viral ill- ness followed progressively by vomiting, abdominal pain, cerebral dysfunction and coma. The mortality is at least 40%. The primary lesions appear to be hepatic, with degen- erative changes in hepatic cells that include swelling of mitochondria with loss of cristae, loss of glycogen granules, frequent fatty cytoplasmic deposits and reduced urea for- mation with accumulation of ammonia and possibly other toxic metabolites in the blood3 The latter result from defi- cient function of the hepatic enzymes of the urea cycle, or- nithine transcarbamylase and/or carbamyl phosphate syn- thetase. Other liver function tests are not markedly abnor- mal and there usually is no jaundice. The cerebral edema responsible for the encephalopathic picture is nonspecific and appears attributable to a toxic effect of ammonia and possibly other substances. Recent studies in 2 cases have shown virus-like particles in liver cells resembling herpes- viruses and myxoviruses.
Treatment has consisted of measures to reduce intra- cranial pressure, such as the use of dexamethasone and injections of urea and mannitol. Peritoneal dialysis has been used to reduce the characteristically elevated blood ammonia concentrations.
OTHER COMPLICATIONS
In addition to Reye's syndrome, infrequent neurologic complications of both influenza A and B have been ob- served. They include myelopathy, polyneuritis and tempo- rary motor paralysis of the legs. Cardiac complications also
31

occur uncommonly and include pericarditis, interst i t ial myocarditis and congestive failure. The last usually occurs in persons with pre-existing hear t disease and thus would be counted as a worsening of the pre-existing condition. Studies tha t report unusual complications often have suf- fered from inadequate diagnostic information about the. virus infection. Diagnostic facilities are improving in many areas, and it is expected tha t more useful information on complications will be forthcoming.
INFLUENZA AND LEUKEMIA
Austin and his associates s recently have reported an ex- cess of acute lymphocytic leukemia (ALL) in cohorts of chil- dren born following influenza epidemics. The increase was noted in the 0 - 4 a g e group, and the greatest excess, 3.2 • tha t in a control population, occurred in children who were in the first t r imester of gestation during the influenza epidemics (Table 8). The association of influenza and subse- quent ALL was substantial and, if not due to influenza di- rectly, likely would be due to some other factor associated with influenza epidemics. The association was also present when leukemia of all types was included in the analysis.
TABLE 8.-AVERAGE ANNUAL CRUDE INCIDENCE RATE AND RELATIVE RISK OF ALL* AND TOTAL LEUKEMIA BY COHORT AND TRIMESTER OF INFLUENZA EXPOSURE FOR CHILDREN UNDER AGE 5, SAN FRANCISCO-OAKLAND SMSA, 1969-1973
COHORT AVERAGE ANNUAL Flu
CRUDE INCIDENCE RATE AND N o n - T r i m e s t e r
RELATIVE RISK flu 1s t 2d 3d Total
ALL Incidence Ratet 3.19 10.32 8.21 2.99 6.94 Relative Risk 3.2 2.6 0.9 2.2
Total Leukemia Incidence Ratet 3.43 11.79 9.70 2.99 7.89 Relative Risk 3.4 2.8 0.9 2.3
*Acute lymphocytic leukemia. tRates per 100,000 population. From Austin, D. F., et al2
32

Work by others on this subject has shown both positive and negative results2
IMMUNOLOGY
Most work on the immunology of influenza has dealt with the role of antibody. The most frequent uses of anti- body determinations are to judge the response to immuni- zation and to estimate the susceptibility to infection, and the predictive value for these purposes is high. Influenza is more immunologically complex than is implied by these measurements, however, and recently, with the develop- ment of new knowledge in immunology, a re-examination of cell-mediated immunity in this disease has begun.
DEFINITION OF CELL-MEDIATED IMMUNE RESPONSE
This response is produced by soluble factors elaborated by sensitized thymus-derived lymphocytes (T cells) follow- ing re-exposure to antigens free in tissues or exposed on the surface of cells. These factors cause the accumulation of macrophages and lymphocytes at sites of antigen localiza- tion, changes that are characteristic of the cell-mediated response, and lead to the destruction of antigen and anti- gen-bearing cells, such as those infected with viruses. Other populations of T cells have regulatory functions that can suppress or enhance the cell-mediated immune re- sponse: T cells responsible for causing the cell-mediated immune response undergo increased formation of DNA detected by increased incorporation of radioactive thymi- dine into the cell.
EFFECT OF NATURAL ILLNESS AND VACCINATION ON THE CELL-MEDIATED IMMUNE SYSTEM
Habershon and his associates TM showed that influenza virus used as a skin test antigen evoked a cell-mediated type response in 24-48 hours in 12 of 42 normal subjects in whom influenza A was used as antigen and in 17 of 42 to influenza B; 9 of 42 were positive to both antigens. Correla- tion of these tests with the presence of hemagglutination
33

inhibition antibody titers suggested an association of posi- tive skin tests with prior infection with influenza. Further- more, when challenged with live at tenuated influenza vi- rus (A/H3N2), 5 of 14 skin test negative but none of the 13 subjects skin test positive to the A virus were infected. The authors also observed that at tenuated vaccine or natura l illness in a small number of persons studied did not convert the skin test to positive. This suggests tha t repeated or very intense st imulation is required to convert the skin test to positive and presumably, therefore, to stimu- late cell-mediated immunity, and that the latter may
Fig. 13.-Lymphocyte thymidine uptake in response to Hang Kong influenza antigen according to a history of previous vaccination, influen- zal illness or both. (From Cate, T. R., and Kelly, J. R.'. 1)
8.0 7.0 6.0 5.0
4.0
Foccine ~iUS Influenza
Lymphocyte Thymidine 3.0
Uptake, Influenza
(Exp/C0nt.) 2.0
1.0
0.8
II
!nfluenza IVaccine Alone IAIone
0
o c~
o o
.3 Neither
34

have some protective effect against infection when present. Cate and Kelly H examined thymidine uptake of lympho-
cytes from per'sons currently well, who had received an inactivated influenza vaccine several months previously, some of whom had also contracted influenza shortly there- after (Fig. 13). When influenza virus was used to stimulate thymidine uptake, they found an increased response of cells from patients who had been vaccinated and had con- tracted influenza as well, and this lymphocyte response correlated positively with the serum hemagglutination in- hibition antibody titer. In contrast, the lymphocyte prolif- erative response to influenza virus correlated negatively with interferon titers of the lymphocyte culture supernates, largely because cells from subjects who had been vaccinat- ed tended to release less interferon than those from unvac- cinated donors. When phytohemagglutinin was substituted for influenza antigen, the greatest response was among persons who had been vaccinated several months previous- ly, whether or not they were ill. These data suggest that influenza vaccination and infection have significant but differing effects on the cell-mediated immune response.
SUPPRESSION OF CELL-MEDIATED IMMUNITY DURING INFLUENZAL ILLNESS
In 1919, Bloomfield and Mateer TM noted a depression of skin sensitivity to tuberculin in patients with influenza , and a similar depression to various skin test antigens was described by others during measles and influenza virus infection. The findings were taken to indicate suppression of cell-mediated immunity.
In 1974, Kantzler and associates 13 reported a depression in the skin test response to tuberculin and other antigens during infection of volunteers with an attenuated live in- fluenza vaccine and during infection following challenge with a virulent strain of A2 influenza. A majority of the subjects who were infected also demonstrated suppression of thymidine uptake by their lymphocytes to stimulation with phytohemagglutinin, a test that correlates with the functional capacity of the thymus-dependent system.
Experience with transplantation and immunosuppressed hosts due to other causes suggests possible consequences of
35

immune suppression from influenza or other virus infec- tions. These include increased hazard of reactivation of tuberculosis and other infections and increased occurrence of neoplasia.
DELETERIOUS EFFECT OF CELL-MEDIATED IMMUNITY IN INFLUENZA
In contrast to the possible benefit of cell-mediated immu- nity in influenza, studies in mice by Cate and Mold '4 pro- vide evidence of a deleterious effect depending on the method of sensitization with the virus. They found that a large number of spleen and lymph node cells (25 million) from mice immunized with formalin-inactivated influenza virus, when given intravenously, increased the mortality of recipient mice following homologous challenge (Fig. 14). It
Fig. 14 . - Survival curves after intranasal challenge with influenza A PR8 for mice who had been transfused with 25 million washed node and spleen cells from either donors vaccinated subcutaneously with for- malinized influenza A PR8 (VAC) or unsensitized donors (CON). The num- bers in parentheses indicate the number of mice represented by the curve and vertical lines between the curves indicate that the proportions of surviving mice on that day were significantly different by chi-square anal- ysis (P < 0.05). (From Cate, T. R., and Mold, N. G.")
-~ 75
_ 5 0 r
a_ 25
I00 ~-'~'-~-~ .k~
- ",,I',
- wc,o,, "-kk!_k_k_I 22 0 I I I I I I I I ! I J I I I I
5 I0 15 Day After Virus Challenge
36

was also observed that t reatment of the spleen and node cells with anti thymocyte serum before injection abolished the apparent cell-mediated excess mortality. That cell-me- diated immunity can be deleterious in influenza infection was further suggested by the studies by Suzuki and asso- ciates 15 (Fig. 15). In that study, injection of antithymo- cyte serum reduced the mortal i ty with experimental in- fluenza infection in mice from 100% to 50%. They also found that desp!te the continued presence of virus in high titers in the lungs of mice treated with anti thymocyte se- rum, consolidation was minimal whereas control mice showed extensive consolidation. These findings are consis-
Fig. 15 . -Ef fec t of ALG on virus growth and humoral ant ibody response in inf luenza-infected mice. Two groups of mice were infected intranasally with 5 LDs0 of inf luenza virus. Each group then received either 5 mg/kg of ALG or NRG intraperi toneal ly according to the fo l lowing schedule: twice on the day of infection and once daily for 4 consecutive days (see text). ALG-treated group: O = EIDs0/0.2 ml; /k = HAl t i ter/ml; and [ ] = mortality. Control group: �9 = EIDs0/0.2 ml; • = HAl t i ter/ml; and [ ] = mortality. (ALG = ant i lymphocyt ic globul in; NRG = normal rabbit globul in; HAl = hemagglut inat ion inhibit ion; EIDso = 50% egg infectious dose.) (From Suzuki, F., et al. is)
(logo)
I0.0
9.0 o ~
8.C -1- -~?.r O
6.C
._c 5.0
4.(3 ,w,--
,,, 3.0 iw .
~ z o
�9 Control
o ALG treatment !1
,,
o/ ~ . / M o r t a l i t y , u ~ ' D . . ~
# e S
0 ; !
I " ! I
I 2 3 4 5 6 7 8 9
1.0
Days afler infection
{%!
IO0
9O
8O
6O
50 - -
30
I0
3 7

tent with those from lymphocytic choriomeningitis infec- tion in mice where anti thymocyte globulin leads to a viremic but nonlethal infection in adult mice, similar to the state of tolerance produced when suckling mice are given the virus.
In both of the above studies, anti thymocyte serum or globulin abolished a factor tha t -increased mortali ty of mice from influenza, and it was shown by Cate and Mold to be transferable in node and spleen cells from mice given inac- tivated vaccine. Antibody seems not to have played an important role in these events. A major question posed by these studies is, if it is due to a cell-mediated response, which of the T cell populations of mice are responsible for the deleterious effect? Mixed lymphocyte responses to al- loantigen stimulation in mice can be suppressed by spleen cells and enhanced by lymph node cells. '6 Since both spleen and lymph node cells were injected by Cate and Mold, el- ther population could have functioned. Enhahced cell-me- diated response at this time seems the best explanation. No immediate parallel in man to t h e foregoing experiments with influenza in man comes to mind, but it must be re- called that a role for cell-mediated immunity in this dis- ease has received limited attention. If cell-mediated immu- nity is suppressed with any regulari ty in human influenza, it conceivably is a protective reaction that would prevent the damaging effects such as those that occur in its pres- ence in mice. This is a subject of obvious interest and sig- nificance.
ANTIBODY RESPONSE IN INFLUENZA
Three antigens of influenza are commonly used to mea- sure antibody response. The nuc|eoprotein antigen reacts with antibody in complement fixation tests to identify in- fluenza types A, B and C. The surface or coat proteins, hemagglutinin and neuraminidase, are used to identify
subtypes . Antibody to hemagglutinin is measured in hem- agglutination-inhibition tests or neutralizing antibody tests, and antibody to neuraminidase is measured in an enzyme-inhibition test.
Persons infected with influenza or immunized with whole virions or subunit vaccines containing both surface compo-
38

Z
~[--,
Z ~
m Z E
Z o
,.-.1
u
0
z
Z 0
r//)...~
'- o .
"~~ ~
o ( . = ~ 0
o ,"~o
39

nents develop serum antibody to both antigens. Compari- sons of results of antibody to ti trations to strains of influen- za that appear sequentially in the population are the basis for the determination of antigenic "shift" and "drift." Anti- body produced by infection or immunization with older strains shows a reduced protective effect against more re- cently derived strains roughly in proportion to the extent of drift.
Antibody to influenza virus also occurs in respiratory tract secretions, where it is presumed to be optimally posi- tioned as the first barrier to infection. A comparison of the response to intranasal and subcutaneous immunization with inactivated A2/Hong Kong/68 vaccine is shown in Table 9.
Intranasal administration of vaccine produced a greater response of nasal secretory antibody than that following subcutaneous vaccination, although only 5 of 9 given in- tranasal vaccine had significant increases in antibody titer. By both routes of administration there were substantial and uniform increases in serum antibody. When this infor- mation is coupled with the knowledge that nasal secretory antibody disappears more rapidly than serum antibody, the subcutaneous route seems to be the most advantageous for inactivated vaccines.
Live at tenuated vaccines have the potential to s t imulate substantial rises in nasal secretory and serum antibody ti- ters, but various technical problems have prevented the use of this method of immunization.
DIAGNOSIS
In the United States, surveillance of influenza is increas- ingly effective, and warnings are given of imminent epi- demics. Moreover, when influenza appears in a community, the at tack rate is high, and influenza likely will be the predominant cause of febrile respiratory illness. These cir- cumstances allow a presumptive diagnosis of influenza in cases of respiratory illness with a high probability of suc- cess. Specific diagnosis can be conveniently made by virus isolation, since virus shedding precedes the onset of illness by a few hours and continues at a high ti ter for 1 - 2 days before it diminishes (Fig. 11). (Note virus titrations in res- piratory secretions in cases described in Fig. 11.)
4O

Inf luenza vi ruses o rd ina r i ly have been isolated in rhesus monke y k idney cell cu l tu re or in embry o n a t ed eggs. The presence of v i rus is detected by nonspecific tests, hemad- sorpt ion of gu inea pig red cells to the surface of the t issue cu l tu re (Fig. 5) or hemagg lu t i na t i on of chicken red cells by a l lantoic f u i d f rom the inocula ted egg. Specific identifica- t ion requires f u r t h e r serologic tests.
Specific immunof luorescence provides a more rapid me thod of diagnosis of influenza. Le igh ton tubes con ta in ing cover slips covered wi th rhesus k idney cell cu l tu re or t issue cu l tu re tubes are inocula ted wi th the specimen. One or 2 days af ter inoculat ion, coverslips or cell ma te r i a l are scraped from the tube, dried, fixed and examined by indi- rect immunofluorescence. A n t i s e r u m to severa l v i ruses m a y be tes ted on different fixed prepara t ions . Resul ts of the di- agnosis of inf luenza by immunof luorescence are demon- s t r a t ed in recent s tudies f rom th i s l abora to ry in Table 10. Among 14 vo lun teers chal lenged wi th a s t r a in of inf luenza A2/Hong Kong/68 (H3N2), 10 yie lded posit ive resul ts by specific immunof luorescence wi th in 24 hours and 3 more became posit ive at 72 hours. In cont ras t , only 2 of 14 were posi t ive by hemadsorp t ion (a nonspecific test) in 24 hours, a l though 6 more were posit ive in 48 hours. On occasion, it is possible to he tec t virus by specific immunof luores- cence direct ly in secret ions. This can be done in an hour or so and is especial ly useful in pa t ien t s wi th inf luenzal pneumonia .
TABLE 10.-DETECTION OF INFLUENZA VIRUS TYPE A BY IMMUNOFLUORESCENCE (IF) IN NORMAL VOLUNTEERS
NO. OF PATIENTS ILLNESS
7 Febrile 6 Afebrile 1 No illness
INFLUENZA A(II3N2)/HONG XONO/68 NUMBER OF IF? HAd~ PATIENTS 72
WIT~ VIRUS 24 48 72 24 48 hr ISOLATED* hr hr hr hr hr or later
7 .7 2 5 5 2 3 1 4 1 1
TOTALS 10 0 3 2 6 4
*Virus was isolated from nasal secretion specimens. ?IF = Specific indirect immunofluorescence of influenza Ar Kong/68. ~:ttAd = Hemadsorption of guinea pig crythrocytes. From Knight, V., Brasicr, F., Greenberg, S. B., and Jones, D. B.: Immunofluores-
cent diagnosis of acute viral infection, South. Med. J. 68:765, 1975.
41

Serologic tests are used commonly in diagnosis of influ- enza, but the necessity for having convalescent specimens to show antibody rise with the incident delay limits the v a l u e of these procedures. A complement fixation test based on the ribonucleoprotein antigen often is used to de- termine the type of virus responsible for infection. Hemag- glutination-inhibition and neutralizing antibody tests that depend on the hemagglutinin antigen are used commonly to identify subtypes and current strains responsible for infection.
PREVENTION
IMMUNIZATION
The prevention of influenza by immunization has been an objective since the discovery of the viral cause of the disease. It must also be considered that the effort was at- tended by a significant degree of success, namely, that vac- cines produced against current strains of virus or their near predecessors afford substantial protection against infection and illness. The chief limitations to total success are antigenic shift and drift. If these changes did not occur and require the preparation of new vaccines at l - 3 - y e a r intervals, nearly total immuni ty could be achieved.
The need for repeated immunization (and there are dif- ferences of opinion as to how long the interval can be) cre- ates a difficult logistic problem in preparation and distribu- tion of vaccine. The present situation is that amounts of vaccine that will immunize about 10% of the population are prepared each year. Vaccine use, by present methods of distribution, is determined by public demand, which, in turn, derives from the people and their physicians' concern about the disease. The need for frequent reimmunization, reactions to vaccination and vaccine failure on some occa- sions all combine to reduce utilization of vaccine.
There are at least three strategies that can be considered in this circumstance. First, to administer vaccine each year to the high-risk group, predominantly those over 65 and those of all ages with chronic pulmonary, cardiovascular and other chronic diseases. This is the current recommen- dation. Second, to increase the amount of vaccine prepared
42

each year and devise means to get it administered in a way to induce herd immunity in the most advantageous man- her. Davenport 17 believes that schoolchildren, who are sub- ject to high attack rates of influenza, should be a focal point of preventive effort. Third, at the level of research, efforts should be increasingly directed toward an understanding of the evolutionary nature of influenza virus antigens, and to develop means of preparing vaccines with greater and lon- ger-lasting protective effect.
All approaches to prevention of influenza would be fa- vored by development of methods of earlier detection of new strains and the onset of epidemics caused by them. It should be noted that there exists a world-wide surveillance network that has served increasingly to report the occur- rence of influenza and to obtain virus from new outbreaks of the disease.
In terms of vaccine development, the most significant event in recent years has been the purification of vaccine by ultracentrifugation and ultrafiltration to remove bacte- ria, white blood cells and fragments of chick embryo tissue. The increased purity has resulted in a reduction in reac- tions to the vaccine. As a consequence, doses of vaccines have been increased about two-fold in the past few years. In the 1975-1976 season, the vaccine included influenza A (Port Chalmers/1973) 350 chick cell agglutinating units (CCA), A (Scotland/1974) 350 CCA and B/Hong Kong/1972 500 CCA for a total dose of 1200 CCA. Dowdle 's has tested dosages as high as 4800 CCA of A strains of influenza: 4800 CCA produced double the antibody response ~observed to 1200 CCA, and 6 - 7 times that of earlier vaccines. If, by such efforts, higher titers and longer-lasting antibody are produced and the antigenic range is broadened, as is con- sidered possible, the vaccine should find greater appeal.
AMANTA'DINE HYDROCHLORIDE
This drug given in doses of 100 mg twice daily has been shown to prevent influenza in families and in patients in the hospital. O'Donoghue and associates 19 gave amantadine to 34 of 73 serologically negative patients admitted to a hospital during an influenza A epidemic in 1972. In the treated group there were 2 cases of asymptomatic influenza
43

and 12 cases (clinical and subclinical) in the control group, a significant difference. Treatment was continued through- out the period of hospitalization, which lasted 2 - 3 weeks. Galbreath and associates ~~ also noted a significantly lower rate of clinical and subclinical infection in family members treated with amantadine than in controls. In neither of the above studies was drug toxicity of significance.
These and other published reports indicate the value of amantadine prophylaxis against A strains of influenza; it is not active against influenza B. When new type A epidemic strains appear, they will be tested for their susceptibility to amantadine. If they are susceptible, as all have been since the drug was introduced, it is reasonable to use amanta- dine as prophylaxis at a dose of 100 mg twice daily. Treat- ment should be continued until the epidemic has subsided. Four to 6 weeks should be adequate in most cases. This means of prevention of influenza has not been widely used and probably should be used more often, especially in the older population, whose antibody response to immunization may be less than optimal31
SUMMARY
The most universally employed measurement of the impact of epidemics and pandemics is the excess of mortali- ty due to influenza and pneumonia. Other criteria are ab- senteeism from school and work, and all three will show positive indications when epidemics are of substantial size. During the 1974-1975 influenza season in Houston, school and industrial absenteeism and the increase in influenza and pneumonia deaths, despite a newly devised statistical procedure, did not signal an epidemic. However, a system of community surveillance of febrile respiratory illness with cultures for influenza virus during late January and early February 1975 gave unmistakable evidence of an influenza epidemic, with more than 600 virus isolations and an estimated occurrence of 50,000 cases of the disease. It is believed that this type of study can explore facets of the epidemiology of the disease not hitherto adequately examined. From this surveillance, which will continue through the summer months, it is hoped to gain further knowledge of the occurrence of antigenic drift and shift,
44

and of the details of the early origin and progress of epi- demics.
Current speculation is that there will be another world pandemic before 1980 caused by a derivative of A strains presently circulating; in 1985-1991, a pandemic is predict- ed to be caused by a virus antigenically related to the swine agent of 1918.
The purity of vaccines has been increased in recent years through ultracentrifugation and. high-efficiency filtration, so that dosages can be increased while severity of reactions is reduced. The current level of dosage of vaccine for adults is 1200 chick cell agglutinating units, almost double what it was a dozen years ago. Recently, vaccines have been pre- pared more rapidly by the use of viral recombinants that incorporate the surface antigens of newly emerged epidem- ic strains into the core of older strains that grow well in embryonated eggs. This practical device greatly reduces the lead time in the preparation of new vaccines.
The main problem in immunization against influenza is the need to reimmunize every 1-3 years. This creates an enormous requirement for vaccine and therefore a problem of selection of recipients. Currently, it is recommended that aged persons and those with cardiovascular, pulmonary and other chronic illnesses should receive the vaccine. Pregnant women are not more susceptible than others to the disease, and they should receive vaccine only if they have some other indications for immunization. Schoolchil- dren probably are important in transmission of the disease, but at present there is no special recommendation to im- munize them. Young children occasionally have severe fe- brile convulsions when immunized against influenza, and those with this history probably should not be immunized.
Amantadine is useful as a prophylactic agent in A(H3N2) influenza infections, and several reports suggest therapeutic benefits as well. Its benefits probably have not been fully utilized. Studies with larger doses should be made in the treatment of influenzal pneumonia. In experi- mental influenza A infections in mice, amantadine and some other agents were remarkably successful when given as continuous small-particle aerosol from the third to the seventh day. The possibility of aerosol treatment of in- fluenzal pneumonia in man should be examined.
45

Evidence was presented that influenza epidemics were associated with increased leukemia in children. The study was well designed and executed, and the results cannot be easily dismissed despite the fact that some older studies did not show this relationship.
Studies of the cell-mediated immunologic system in in- fluenza reveal a suppression during acute illness and sen- sitization following immunization and/or infection with influenza virus. Skin test studies suggest that sensitization to influenza virus may be very common in the population. Mice adoptively immunized with node and spleen cells from donors that had been vaccinated against influenza had a higher mortali ty than controls when challenged with the homologous virus; this effect was abolished by exposure of the donor cells to anti thymocyte serum. Although these studies suggest involvement of the cell-mediated immuno- logic system in host response to influenza, it is not clear whether the effect of this involvement will be protective or harmful for the host, or differ under varying conditions.
Reye's syndrome is a clinicopathologic complex charac- terized by mitochondrial lesions in hepatic cells, deficient function of one or two hepatic enzymes of the urea cycle, increase of blood ammonia, and possibly other metabolites, and frequently fatal encephalopathy. It has occurred most often following influenza B and some other virus infections, and only occasionally is described after influenza A infec- tion. Treatment has consisted primarily of measures to reduce intracranial pressure.
ADDENDUM
Since this article was written, an outbreak of swine in- fluenza virus infection in recruits occurred in February 1976 at Fort Dix, New Jersey. There were 13 documented cases with 1 fatality, and serologic surveys in recruit pla- toons sugges ted that a total of 500 cases may have oc- curred. Although sporadic cases of swine-type influenza virus in man have occurred over the years, there usually was evidence of contact with pigs, the patients often had illnesses that could impair host defenses and the disease did not spread secondarily among the human population. There was a concurrent outbreak of A/Victoria influenza at
46

Fort Dix, and it has been proposed that the capacity of the swine-type infection to spread from man to man may have resulted from recombination between the swine and A/Victoria agents. As a result of this epidemic, a nation- wide program is planned to vaccinate substantially all of the people in the United States. Some 150 million doses of swine vaccine will be manufactured. In addition, nearly 20 million doses of a vaccine containing the swine agent and A/Victoria strain will be prepared for use by high-risk or elderly persons.
A return of swine influenza as a cause of epidemics and pandemics in man had not been anticipated until about 1990, when the numbers of those who had the disease in the 1918-1930 epidemics will be substantially reduced. At present, about 85% of persons 50 years of age or older have antibody to the swine agent. These people probably have some protection against the disease; and epidemics, if they occur, are likely to largely involve those under 50 years of age.
Whether the Fort Dix outbreak heralds the appearance of epidemic disease in the coming year in the United States and possibly elsewhere is not certain; but the possibility of such epidemics in the next year or so could not be excluded, and the difficult decision to initiate a national vaccination campaign was made by public health authorities. This will be the most massive effort to immunize against influenza ever attempted, and developments in this unique experi- ment in prophylaxis will provide valuable insights into many aspects of preventive medicine and public health.
REFERENCES
1. Davenport, F. M., Hennessy, A. V., and Francis, T., Jr.: Epidemiologic and immunologic significance of age distribution of antibody to anti- genic variants of influenza virus, J. Exp. Med. 98:641, 1953.
2. Masurel, N., and Marine, W.: Recycling of Asian and Hong Kong in- fluenza A virus hemagglutinins in man, Am. J. Epidemiol. 97:44, 1973.
3. Housworth, J., and Langmuir, A. D.: Excess mortality from epidemic influenza, 1957-1966, Am. J. Epidemiol. 100:40, 1974.
4. Housworth, J., and Spoon, hi.: The age distribution of excess mortality during A2 Hong Kong influenza epidemics compared with earlier A2 outbreaks, Am. J. Epidemiol. 94:348, 1971.
5. Stephen, E. L., Dominik, J. W., Moe, J. B., Spertzel, R. O., and Walk- er, J. S.: Treatment of influenza infection of mice using rimantadine
47

hydrochlorides by the aerosol and intraperitoneal routes, Antimicrob. Agents Chemother. 8:154, 1975.
6. Knight, V.: Airborne Transmission and Pulmonary Deposition of Re- spiratory Viruses in Viral and Mycoplasmal Infections ofthe Respira- tory Tract, in Knight, V. (ed.), Viral and Afycoplasmal Infections of the Respiratory Tract (Philadelphia: Lea'& Febiger, 1973), Chap. 1, pp. 1-9 .
7. Tang, T. T., Siegesmund, K. A., Sedmak, G. V., Casper, J. T., Varina, R. R., and McCreadie, S. R.: 'Reye syndrome: A correlated electron microscope, viral and biochemical observation, JAMA 232:1339, 1975.
8. Austin, D. F., Karp, S., Dworsky, R., and Henderson, B. W.: Excess leukemia in cohorts of children born during influenza epidemics, Am. J. Epidemiol. 101:77, 1975.
9. Randolph, V. L., and Heath, C.: Influenza during pregnancy in rela- tion to subsequent childhood leukemia and lymphoma, Am. J. Epide- miol. 100:399, 1974.
10. Habershon, R. B., Molyneaux, M. E., Stavin, G., Leewi, G., and Tyr- tell, D. A. J.: Skin tests with influenza virus, J. Hyg. (Camb.) 71:755, 1973.
11. Cate, T. R., and Kelly, J. R.: Hong Kong Influenza Antigen Sensitivity and Decreased Interferon Response of Peripheral Lymphocytes, in Hobby, G. L. (ed.), Antimicrobial Agents and Chemotherapy-1970 (Bethesda: American Society for Microbiology, 1971), pp. 156-160.
12. Bloomfield, A. L., and Mateer, J. G.: Changes in skin sensitiveness to tuberculin during epidemic influenza, Arm Rev. Tuberc. 3:166, 1919.
13. Kantzler, G. B., Lanteria, S. F., Cusumano, C. L., Lee, J. D., Ganguly, R., and Waldman, R.: Immunosuppression during influenza virus infection, Infect. Immun. 10:996, 1974.
14. Cate, T. R., and Mold, N. G.: Increased influenza pneumonia mortality of mice adoptively immunized with node and spleen cells sensitized by inactivated but not live virus, Infect. Ifilmun. 11:908, 1975.
15. Suzuki, F., Ohya, J., and Ishida, N.: Effect of antilymphocyte serum on influenza virus infection in mice, Proc. Soc. Exp. Biol. Med. 146:78, 1974.
16. Rich, S. S., and Rich, R. R.: Regulatory mechanisms in cell-mediated immune responses. I. Regulation of mixed lymphocyte reactions by alloantigen-activated thymus derived lymph0cytes, J. Exp. Med. 140: 1588, 1974.
17. Davenport, F. M. Control of influenza, Med. J. Aust. Special Supp. ix 33, 1973.
18. Dowdle, W. R.: New approaches to the control of influenza, Med. J. Aust. Special Supp. 1:38, 1973.
19. O'Donoghue, J. hi., Ray, C. G., Terry, D. W., Jr.~ and Beaty, H.: Pre- vention of nosocomial infection with amantadine, Am. J. Epidemiol. 97:276, 1973.
20. Galbreath, S. W., Schild, G. C., Oxford, J. S., and Watson, G. I.: Pro- tective effect of aminoamantadine on influenza A2 infections in the family environment, Lancet 2:1026, 1969.
21. Howells, C. H. L., Vesselinova-Jenkins, C. K., Evans, A: D., and James, J.: Influenza vaccination and mortality from bronchopneumo- nia in the elderly, Lancet 1:381, 1975.
48