Embed Size (px)
Citation preview

Correspondence and Reprint requests : Kam-Lun Ellis HonDepartment of Pediatrics, The Chinese University of Hong Kong,6/f, Clinical Science Building, Prince of Wales Hospital, Shatin,Hong Kong. Tel: (852)2632 2859. Fax: (852) 2636 0020.
[Received October 13, 2007; Accepted March 19, 2008]
Original Article
Ingestion - Associated Adverse Events NecessitatingPediatric ICU Admissions
Kam-Lun Ellis Hon, Ting-Fan Leung, Chi-Wan Emily Hung, Kam-Lau Cheung and Alexander KCLeung
Department of Paediatrics, The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, Hong Kong,The University of Calgary, Calgary, Alberta, Canada
ABSTRACT
Objective. To review the pattern of food-associated pediatric intensive care unit (PICU) admissions.
Methods. A retrospective chart review was conducted to analyse the pattern of food-associated PICU admissions at ateaching hospital between January 2004 and May 2007.
Results. Ten cases (7 boys and 3 girls, aged 9 month to 11.7 year) were identified. One girl developed progressivegeneralized urticarial rash and anaphylactic shock following consumption of bird nest drink. A boy presented with the classictriads of acute onset altered mental state, respiratory depression and small pupils following consumption of a bottle ofpresumed “green tea”, which was subsequently found to contain methadone. In the remaining 8 cases, dried mango,peanut, peanut-shell, fishmeat ball, pork chop, bread and bone were the culprits, impacting in the airway or oesophagus.All but one patient had short ICU stay (≤3 days). Ingestion-associated adverse events can be protean and may necessitatePICU admissions. All age groups can be affected. Solids are usually associated with symptoms from local obstruction orsuffocation, while fluids may be associated with systemic manifestations.
Conclusion. Presentations were generally acute, dramatic and unmistaken. The majority of patients made prompt anduneventful recovery and had short PICU stay. [Indian J Pediatr 2009; 76 (3) : 283-286] E-mail: [email protected].
Key words: Adverse events; Anaphylaxis; Bird’s nest; Bread; Mango; Peanut; Shock
Food is an important element for growth but rarely canbe a cause of morbidity in children. Children areexposed to a large variety of food. Reports on food-associated pediatric intensive care unit (PICU)admissions have been scarce in the literature. We reportten cases of food-associated adverse events requiringPICU admissions and describe their clinical coursesand morbidity.
MATERIALS AND METHODS
A retrospective chart review was conducted on allchildren with food-associated PICU admissions to thePrince of Wales Hospital between January 2004 andMay 2007. Cases were identified from the hospital’s
computerized auditing system and from the PICU’sdatabase of every admission to the unit. The hospital isa university-affiliated teaching hospital located at theNew Territories of Hong Kong. The ethics committee ofThe Chinese University of Hong Kong approved thisreview and patient consent was not required due to theretrospective nature of the study.
RESULTS
We identified ten cases (70% boys, aged 9 months to11.7 years) of ingestion-associated adverse eventsnecessitating PICU admissions. Only one patient wasan infant less than one year of age. There were a total of462 PICU admissions during the study period. Thesecases were reported to illustrate the wide spectrum ofmanifestations and diverse pathology (Table 1).Presentations were generally acute, dramatic andunmistaken. Prompt recovery was observed followingendoscopic removal of the culprit food. All but onepatients made prompt and uneventful recovery and hadshort PICU stay (≤ 3 days).
Indian Journal of Pediatrics, Volume 76—March, 2009 283

Kam-Lun Ellis Hon et al
284 Indian Journal of Pediatrics, Volume 76—March, 2009
One case poised a subsequent diagnostic challenge indetermining the allergen when a 10-year-old girldeveloped a generalized urticarial rash, swelling oflips, abdominal pain, shortness of breath, sweating andirritability within 30 minutes following consumption ofbird’s nest with milk, and within 2 hours of eatingsome sushi and prawn. The father also consumed thebird’s nest and developed some abdominal pain but noskin reaction. The patient had a past history of allergicrhinitis, hyperactive airway disease, and urticaria afterconsumption of baby pigeon at the age of 6 years. At theemergency department, she was in shock, with a bloodpressure (BP) of 52/25 mmHg, pulse of 156 per minute,and capillary refill 4 seconds with warm peripheries.Glasgow Coma Scale (GCS) was 15 and she required 4L/min of oxygen by face-mask to maintain an oxygensaturation of 98%. She was immediately resuscitated
with intramuscular adrenaline (1 ml [mg] of 1 in 1000),intravenous fluid boluses (total 30 ml per kg),intravenous chlorpheniramine 5 mg and hydro-cortisone 100 mg. Her BP and pulse normalized andher rash, lip swelling and shortness of breath rapidlysubsided. Subsequent skin prick test was stronglypositive to the same brand of bird’s nest but negative tocow’s milk, egg, wheat, soybean, salmon, shrimp, craband beef.
Another case illustrated that history of illicit drugusage is often concealed. A previously healthy 11-year-old boy presented with sudden onset somnolence,small sluggish pupils and respiratory depression. Onarrival at the emergency department 10 minutes later,his GCS was 3 out of 15, BP 104/60 mmHg, pulse 88beats per minute, temperature 34.9°C and SaO2 91%.His pupils were small (2 mm), non-reactive and Doll’s
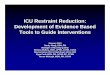
TABLE 1. Characteristics of the Ten Food-associated PICU Admissions
Age Sex Food Diagnosis Relevant risk factors Ventilation Inotropes Treatment PICU stay
10 Girl Bird’s nest Anaphylaxis Pigeon anaphylaxis, Nil Intramus- Intravenous chlorphen 1 daySuspension atopy (asthma and cul aradre- iramine and hydrocor
allergic rhinitis) naline tisone
0.8 Boy Mango Upper airway Esophageal stricture 2 days Nil Bronchoscopic removal, 2 daysobstruction intravenous dexamethasone
11 Boy Methadone CNS dep Parental divorce, 1 day Nil Intravenous naloxone 2 daysin a green -ression uncles methadonetea bottle user
2 Boy Peanut Aspiration Nil 2 days Nil Bronchoscopic removal, 2 daysintravenous dexamethasone
8 Boy Peanut shell Subglottic Patient and sister 2 days Nil Bronchoscopic removal, 2 daysimpaction mentally retarded intravenous dexamethasone
5 Girl Pork chop Esophageal Multiple congenital 2 days Nil Removal with oesophagos- 2 daysobstruction normalities copy, dilatation of esopha-
gus, bronchoscopy
6.7 Girl Fish ball Laryngeal Nil 2 days Nil Supportive 3 dayssuffocation
11 Boy Soft bread Oropharyngeal Mentally retarded From ad Intravenous Removal of bread at Died inobstruction and cerebral mission adrenaline, intubation, supportive PICU 5
palsy, wheel dopamine treatment for raised monthschair bound and dobuta- intracranial pressure and later
mine hypoxic brain injury,persistent vegetative state
2.6 Boy Fish ball Cricopharyn- Nil Nil Nil Fish ball removed from 2 daysgeal obstruc- cricopharyngeus by rigidtion laryngoscopy and esophago
scopy
1 Boy Bone and Bone in Nil 2 days Nil Removal of bone with rigid 3 daysmilk subaglottic laryngoscopy
area and milk intrachea

Ingestion – Associated Adverse Events Necessitating Pediatric ICU Admissions
Indian Journal of Pediatrics, Volume 76—March, 2009 285
eye reflex was negative. Arterial blood gas showed a pHof 6.9, pCO2 16.7 kPa, and pO2 8.95 kPa. Blood glucosewas 10.6 mmol/L. He was intubated and ventilated.Intravenous thiopentone and suxamethonium weregiven. Boluses of normal saline for hypotension (BP 73/36 mmHg) and ceftriaxone for coverage of septic riskwere given intravenously. An urgent CT scan of thebrain was normal. In the CT suite, the patient becamemore awake and was able to follow command. Aftermuch interrogation, the maternal uncle disclosed to theattending physician that he stocked some methadone ina “green tea” bottle in the refrigerator. In PICUintravenous naloxone (2 mg) was given with good effectand the patient was extubated. Subsequently, analoxone infusion was started at 0.01 mg/kg/hr andstepped up to 0.02 mg/kg/hr. The naloxone drip wasdiscontinued 19 hours later. High performance liquidchromatography and gas chromatography/massspectrometry confirmed the presence of methadone inthe urine and gastric aspirate. Retrospectively, thepatient admitted to have drunk a bottle of “green tea”from the refrigerator at home the evening before.
DISCUSSION
These ten cases illustrate the wide spectrum of food-associated adverse events which can occur followingthe ingestion of seemingly harmless food and drinks,and demonstrate that adverse events can result ineither regional dysfunction or systemic upset.
Regional dysfunction: Aspiration of food chunk canoccur, with the most common site being thecricopharyngeus level1-5. The mango case is particularlyinteresting in that it reminds clinicians to search for anyunderlying anatomical obstruction, which may beamenable to surgical treatment, when aspiration ofsolid food occurs. Relief of obstruction is associatedwith resolution of the symptoms. Mechanicalobstruction can also occur further downstream in thebronchi or lower airways, with resultant dyspnea orpersistent cough6. Expiratory chest radiograph films tolook for hyperinflation may be useful when thediagnosis is not immediately apparent6.
Aspiration usually occurs in toddlers 1,2,4,7. The two-year-old patient who choked on peanut is a classicexample. The incidence rate of nonfatal chokingepisodes in children was up to 30 per 100,000 in theUnited States, with more than 80% of cases occurring inchildren aged 4 or younger1. However, older childrenare not exempted. Children who suffer from braintumors, seizures or mental retardation are especiallyprone to choking and aspiration. The case regarding thepeanut shell aspiration also illustrates that graveconsequences such as subglottic stenosis can occurwhen diagnosis and treatment are delayed. Peanut is a
notorious cause of food-associated aspiration 1-4. Thefourth case demonstrates the importance of historytaking about possibility of foreign body aspiration in achild with respiratory symptoms and abnormal chestradiograph. The fifth case was unusual in that it wasthe peanut shell that causes the airway obstruction.Despite the older age, this boy was prone to aspirationin view of his mental retardation. In the sixth case, thesite of obstruction was the oesophagus rather than theairway in a child with predisposing oesophagealabnormality. The seventh, ninth and tenth casesillustrate that severe choking and upper airwayobstruction could occur in a healthy child without anypredisposing risk. The eighth patient with mentalretardation was exceedingly unfortunate and serves toremind healthcare providers that airway (A) patencytakes priority over breathing/ventilation (B) andcirculation (C) in the ABC of resuscitation. A foreignbody needs to be removed for effective resuscitation to beachieved.
Foreign body aspiration is a significant cause ofmorbidity and mortality yet readily treatable in thepediatric population. It must be suspected in childrenexperiencing sudden onset of respiratory distressassociated with coughing, gagging and stridor,especially when the rescuer is unable to secure a patentairway or effectively ventilate the child.7 Parents,grandparents and caregivers are strongly warnedagainst giving large chunk of any food to an infant.Anticipatory guidance should be offered especially inneurology outpatient clinics or in special schools, whilebasic life support and Heimlich manoeuvre should betaught to all caregivers, in particular those at riskgroups.
Systemic manifestations: Food-associated adverseevents may range from CNS depression to multi-organinvolvement as in anaphylactic shock. Inadvertentmethadone ingestion due to the illegal storage at homecan be difficult to diagnose as the relatives might notvolunteer the relevant information despite muchcoercion. Using common brand bottles to storemedication, in particular, to disguise the illegal storageof dangerous drugs, can be fatal to the young membersat home. Our case illustrates the danger of using brandbottle to store any life-threatening drugs or chemicals athome and, in particular, in the refrigerator wherechildren have ready accessibility. Methadoneintoxication in children has been previously reported.8
Having ruled out intracranial hemorrhage orinfarction, the classic triads of acute onset alteredmental state, respiratory depression and small pupilswould strongly suggest narcotic ingestion. A trial ofnaloxone may be diagnostic. Methadone has a longhalf-life (25 hours) and repeated administration ofnaloxone, in this case by continuous infusion, isrequired for treatment. Cardiopulmonary support and

Kam-Lun Ellis Hon et al
286 Indian Journal of Pediatrics, Volume 76—March, 2009
PICU monitoring are mandatory for optimal care.
The case of bird’s nest anaphylaxis hasdemonstrated another pathway for CNS depressionrelated to ingestion, which occurs secondary tocirculatory collapse in anaphylactic shock. Goh et alreported that the most common food triggeringangioedema and food-induced anaphylaxis inSingaporean children was due to consumption ofbird’s nest.9 The bird’s nest may contain difficult-to-digest glycoproteins and fibers and may causeanaphylaxis in infants and young children.9, 10 Thedemand of bird’s nest as a Chinese delicacy on table ishigh. Over 19.9 million nests were consumedworldwide in 1989.11 Bird nest’s soup is a Chinesedelicacy frequently consumed as a traditional remedyfor asthma and respiratory ailments. We recently foundthat more than one-quarter of children with severeeczema have been given bird’s nest.12 In contrary to thereports in the western population, peanut allergy isrelatively uncommon in the Chinese population.9, 10 Inthe past ten years in this tertiary hospital in HongKong, with a catchment population of 1 million people,there was no peanut anaphylaxis requiring PICUadmission.
CONCLUSION
This report serves to alert the public and physicians ofthe protean life-threatening manifestations of food-associated accidents. It appears that fluids (such as birdnest suspension and methadone drinks) are morecommonly associated with systemic manifestations(anaphylaxis and altered mental state) and solids areassociated with obstruction and suffocation/
aspiration. Timely treatment would be life-saving.
REFERENCES
1 Gotsch K, Anmest JL, Holmgreen P, Gilcrist J. Nonfatalchoking-related episodes among children - United States,2001. Morb Mortal Wkly Rep 2002; 51:945-948.
2 Wolach B, Raz A, Weinberg J, Mikulski Y, Ben Ari J, SadanN. Aspirated foreign bodies in the respiratory tract ofchildren: Eleven years experience with 127 patients. Int JPediatr Otorhinolaryngol 1994; 30:1-10.
3 Yeh LC, Li HY, Huang TS. Foreign bodies intracheobronchial tree in children: a review of cases over atwenty-year period. Changgeng Yi Xue Za Zhi 1998; 21:44-49.
4 Rothmann BF, Boeckman CR. Foreign bodies in the larynxand tracheobronchial tree in children. Ann Otol RhinolLaryngol 1980; 89:434-436.
5 Gay BB Jr, Atkinson GO, Vanderzalm T, Harmon JD,Porubsky ES. Subglottic foreign bodies in pediatricpatients. Am J Dis Child 1986; 140:165-168.
6 Leung AK, Robson WL, Tay-Uyboco J. Chronic cough inchildren. Can Fam Physician 1994; 40:531-537.
7 Leung AK, Cho H. Diagnosis of stridor in children. Am FamPhysician 1999; 60:2289-2296.
8 Binchy JM, Molyneux EM, Manning J. Accidental ingestionof methadone by children in Merseyside. BMJ 1994;308:1335-1336.
9 Goh DL, Lau YN, Chew FT, Shek LP, Lee BW. Pattern offood-induced anaphylaxis in children of an Asiancommunity. Allergy 1999; 54:84-86.
10 Bjorksten B. The epidemiology of food allergy. Curr OpinAllergy Clin Immunol 2001; 1:225-227.
11 Lau ASM, Melville DS. International trade in swiftlet nestswith special reference to Hong Kong. Cambridge: TrafficInternational, 1994.
12 Hon KL, Leung TF, Kam WY, Lam MC, Fok TF, Ng PC.Dietary restriction and supplementation in children withatopic eczema. Clin Exp Dermatol 2005; 31:187-191.