Embed Size (px)
Citation preview

• Inhalational mercury toxicity with elevated blood mercury concentrations, occasionally severe and requiring critical care interventions, may occur following independent gold scavenging in the United States.
• In our small case series of acute inhaled mercury exposures reported to the Oregon Poison Center within the past 14 years, there was a range of symptoms often depending on extent of exposure.
• Standardized approaches to evaluation, particularly serum and/or urine mercury concentrations, as well as chelation guidelines seem to be lacking.
Toxicologists should be aware of the association of inhalational mercury toxicity and artisanal gold extraction.
RESULTS:• Between 2002–2015, there were nine cases of mercury exposure from extraction incidents reported to the Oregon Poison Center.
• Every incident involved trying to extract a precious metal for personal financial gain (i.e., not related to an industrial mining operation).
• By case description, all exposures were assumed to involve elemental mercury.
~ Eight (89%) patients were male, patient age ranging from 32 to 81 years.
~ Eight (89%) cases involved acute exposures.
~ Eight (89%) cases explicitly involved the patient heating a mercury-gold amalgam.
~ Seven of eight (88%) patients with acute exposures reported symptoms consistent with acute elemental mercury inhalation; two (29%) patients had severe toxicity requiring intubation. Risk factors for more severe toxicity seemed to include close and/or prolonged contact with vapor and not using personal protective equipment.
~ Six (67%) patients had measured whole blood mercury concentrations: two (33%) were normal, and four (67%) were markedly elevated. All four patients with elevated whole blood [mercury] received at least one dose of chelation therapy.
~ At least four of nine (44%) patients were known to be using methamphetamines at the time of their exposure.
BACKGROUND:• Mercury exposure has been well-described among artisanal and small-scale gold mining communities in developing countries1.
• Studies from Burkina Faso2, Indonesia3,4, Colombia5, Ghana6, and the Brazilian Amazon7 confirm exposures among workers and suggest increased risk of adverse health effects.
• These cohorts represent industrial mining communities, rather than individual extraction endeavors, and perhaps thus favor reports from developing countries where these industrial practices predominate.
• To date, a paucity of published cases has included patients in the United States, and inhalational mercury toxicity from such exposures remains speculative.
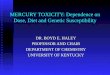
• Elemental mercury and gold ore dust combine to form a solid amalgam (Fig. 1); which is then heated to separate vaporized mercury (which is recollected via condensation) from residual gold.
• In contrast to terrestrial mining, individual prospectors may attempt to extract precious metals commonly gold) from secondary sources (commonly jewelry or electronic devices), often by adapting techniques such as amalgamation.
• This is a systematic retrospective review of the Oregon Poison Center Toxicall database.
• All cases of “mercury” or “mercury inhalation” exposures were reviewed and those involving attempted precious metal extraction were included in the analysis.
Patient Date/ Location
Age/Sex HPI Symptoms/
Signs[Mercury]
(Reference Range)
Treatment/s Meth?
#1 Oct 2003/Reno, NV 81 M
Burning gold using mercury (approx 1 tablespoon) with 1:1 ratio; working on stove outdoors, wind shifted fumes into face
Pleuritic chest pain and abdominal pain, no dyspnea
Not performed / not available
Antibiotics Unknown
#2 July 2007/Albany, OR 43 M
"Self-employed gold miner" at home (uses mercury and lead) for "years"; no acute mercury exposure
Nausea, weight loss, vision abnormalities, fatigued
Serum: 5 mcg/L (0–10)
Antiemetics Unknown
#3 Apr 2011/Ashland, OR 45 M
Cooking gold-mercury mixture in kitchen, not wearing respirator; normally uses respirator outside with propane but ran out of propane so using kitchen; 3 episodes in past week
SOB, non-productive cough, strange taste, decreased hearing
Not performed / not available
Unknown(lost to follow-up)
Unknown
#4 Apr 2012/Grants Pass, OR 44 M
Gold mining in a sock using mercury (heats flake in a nylon stocking with mercury and sand with torch), wore gloves but no mask; first time doing this
Cough, SOB, painful red swollen hands, seizure, visual hallucinations, agitated
Serum: 7 mcg/L (0–9)
Dimercaprol started; patient left AMA
Positive UDS and patient admitted use
#5
Dec 2012/Northern California,
transferred to Medford, OR
32 M
"Separating iron ore" in garage using boiling (1 lb elemental) mercury, no personal protective equipment
Anxious, respiratory distress; CXR with opacifications
Serum: 340 mcg/L (0–10)
Intubated (x11 days), dimercaprol and succimer
Unknown
#6 Nov 2014/Anchorage, AK 61 M
"Boiling down gold in the [Alaskan] bush" 3.5 weeks ago, no personal protective equipment; history of "mercury poisoning"
Headaches, unusual odor, vertigo, no respiratory symptoms
Urine: 39 mcg/L (0–20)
Unknown (lost to follow-up)
Unknown
#7 Nov 2014/Portland, OR 46 M
Trying to extract gold from circuit board, endorses mercury vapor exposure, outside, wearing respirator, 30-min exposure, first time doing this
Cough, sore throat, chest pain; abnormal CXR
Serum: 346 mcg/L (0–10)
Succimer x 1 dose. Discharged after being non-compliant in hospital, then lost to follow-up
Positive UDS and patient admitted use
#8 Dec 2015 /Klamath Falls, OR 61 M
See case report SOB, HA, myalgias, hypoxia; abnormal CXR and CT
Serum: >200 mcg/L (0–9)
Intubated (x 3 days), antibiotics, dimercaprol and succimer
Positive UDS and patient admitted use
#9 Dec 2015/ Klamath Falls, OR 50 F
See case report HA, sore throat, myalgias, abdominal pain, nausea/vomiting; abnormal CXR and CT
Serum:>200 mcg/L (0–9)
Dimercaprol and succimer
Positive UDS and patient admitted use
To what extent do inhalational mercury exposure and toxicity occur among artisanal gold extractors in the Oregon Poison Center catchment area?
Figure 1: Gold-mercury amalgam
A 61 year-old male (patient #8) with a prior stroke and residual mild left-sided weakness and an otherwise healthy 50-year-old female (patient #9) presented to a rural southern Oregon hospital after exposure to mercury vapor.
In an effort to obtain money to purchase methamphetamines they had attempted to extract gold from computer chips, watch bands, and other jewelry from local thrift shops. The man claimed to have done this many times in the past using a coil apparatus, though not within the last 10 years.
On this occasional the couple used a butane torch to heat a jar filled with approximately 50 mL of elemental mercury, collected from old thermometers. Then in the enclosed space of their bedroom, without respirators or gloves, they slowly added the electronics and jewelry to the heated mercury.
After 2–3 hours the man’s grip slipped and he spilled the mixture onto the tile floor. After scraping up the liquid using an ID card, they both felt “ill” and decided to inject methamphetamine. For the next 48 hours they stayed in bed, suffering mild shortness of breath, sore throat, diffuse myalgia, and general malaise.
On presentation to the ED (post-exposure day 3), the 61 year-old male’s vital signs were T 37.8 C, HR 106, BP 123/78, RR 22, and SpO2 84% on room air, which improved to 90% on 3 LPM supplemental oxygen.
Chest x-ray revealed mildly hyperinflated lungs with nonspecific bilateral reticular interstitial opacities. Laboratory studies were notable for leukocytosis (WBC 18,700/µL, with neutrophilia of 80%) and methamphetamine-positive urine drug screen.
Initial mercury concentrations eventually resulted at >200 mcg/L (serum, reference range 0–9 mcg/L) and >800 mcg/L (spot urine, reference range 0–9 mcg/L); exact concentrations were not reported by the lab.
The patient was admitted and treated with dimercaprol, vancomycin and piperacillin/tazobactam. The patient required BiPAP, which he tolerated only intermittently, as well as non-rebreather mask oxygen at up to 15 LPM.
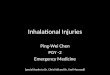
A chest CT demonstrated diffuse groundglass opacities consistent with acute pneumonitis (Figures 2 and 3). He was treated with furosemide, bronchodilators and methylprednisolone. On hospital day 4 he was intubated for impending respiratory failure.
Bronchoscopy revealed no pulmonary hemorrhage. He was transitioned to 2, 3-dimercaptosuccinic acid (succimer) via orogastric tube on hospital day 6. He was extubated on hospital day 7, still requiring 4 LPM.
A repeat CT showed diffuse perihilar reticular opacities with subpleural sparing, improved groundglass opacities, and evolution of interstitial scarring. He was discharged on hospital day 16 on levofloxacin, home oxygen (at 3 LPM), prednisone taper, and succimer.
Total succimer regimen was 500 mg TID for 5 days followed by 500 mg BID for 14 days. On day of discharge (post-exposure day 19, succimer day 8), serum mercury concentration was 64 mcg/L and urine mercury concentration was 200 mcg/L. On post-discharge day 10 (post-exposure day 29, succimer day 18) a 24-hour urine mercury concentration was 305 mcg/L. Additional follow-up evaluations are pending.
CASE REPORT
BACKGROUND RESULTS
RESEARCH QUESTION
METHODS
DISCUSSION
CONCLUSION
Figure 2: Inhalational mercury CT coronal Figure 3: Inhalational mercury CT transverse
1. Gibb H and O’Leary KG. Mercury Exposure and Health Impacts among Individuals in the Artisanal and Small-Scale Gold Mining Community: A Comprehensive Review. Envirn Health Perspect. 2014;122(7):667-72.2. Tomicic C, Vernez D, Belem T, Berode M. Human mercury exposure associated with small-scale gold mining in Burkina Faso. Int Arch Occup Environ Health. 2011;84(5):539-46.3. Sari MM, Inoue T, Matsumoto Y, Yokota K. Measuring total mercury due to small-scale gold mining activities to determine community vulnerability in Cihonje, Central Java, Indonesia. Water Sci Technol. 2016;73(2):437-44.4. Nakazawa K, Nagafuchi O, Kawakami T, Inoue T, Yokota K, Serikawa Y, Cyio B, Elvince R. Human health risk assessment of mercury vapor around artisanal small-scale gold mining area, Palu city, Central Sulawesi, Indonesia. Ecotoxicol Environ Saf. 2016;124:155-62.
5. Rodriguez-Villamizar LA, Jaimes DC, Manquian-Tejos A, Sanchez LH. Human mercury exposure and irregular menstrual cycles in relation to artisanal gold mining in Colombia. Biomedica. 2015;35:38-45.6. Rajaee M, Long RN, Renne EP, Basu N. Mercury Exposure Assessment and Spatial Distribution in A Ghanaian Small-Scale Gold Mining Community. Int J Environ Res Public Health. 2015;12(9):10755-82.7. Castilhos Z, Rodrigues-Filho S, Cesar R, Rodrigues AP, Villas-Boas R, de Jesus I, Lima M, Faial K, Miranda A, Brabo E, Beinhoff C, Santos E. Human exposure and risk assessment associated with mercury contamination in artisanal gold mining areas in the Brazilian Amazon. Environ Sci Pollut Res. 2015;22(15):11255-64.
References
Matthew J. Noble and Robert G. HendricksonOregon Poison Center, Department of Emergency Medicine, Oregon Health & Science University, Portland, Oregon
Inhalational mercury toxicity from artisanal gold extraction reported to the Oregon Poison Center, 2002–2015







![Neuroprotection by Melatonin on Mercury Induced Toxicity ...Neuroprotection by Melatonin on Mercury Induced Toxicity in the Rat Brain. 377 sari (1981) [47]. The method of Lowry . et](https://img.pdfslide.net/doc/110x75/5e9cc620eecd3003874e80cd/neuroprotection-by-melatonin-on-mercury-induced-toxicity-neuroprotection-by.jpg)