Embed Size (px)
DESCRIPTION
Inherited Renal Diseases Part II. Maria Ferris and Deb Gipson 10/23/01. Outline. Lowe Syndrome Fabry disease Cystinosis Cystinuria Hyperoxaluria Alports. Fabry Disease. X-linked recessive disorder (Xq22-24) Defect is in the alpha-1 galactosidase A - PowerPoint PPT Presentation
Citation preview

Inherited Renal DiseasesPart II
Maria Ferris and Deb Gipson
10/23/01

Outline
• Lowe Syndrome
• Fabry disease
• Cystinosis
• Cystinuria
• Hyperoxaluria
• Alports

Fabry Disease• X-linked recessive disorder (Xq22-24)
• Defect is in the alpha-1 galactosidase A
• Diagnosis by assay of peripheral blood leukocyte level of alpha-galactosidase
– Hemizygous(M) level is near 0
– Heterozygote (F) level may be in the low normal range. Check urinary ceramide digalactoside and trihexoside.
– Fetus: determine level in amniocyte

Fabry Disease• Males: wide range of clinical abnormalities• Females: variable range of clinical expression,
may have lipid storage in cells and be completely asymptomatic (lyonization)
• Race: White most common• Incidence: 1:40,000• Intracellular accumulation of the
glycosphingolipid galabiosylceramide

Fabry: Deposition– *Endothelial, perithelial, smooth muscle of
blood vessels– Kidney: glomerluar and tubular
epithelium– Corneal epithelium– Myocardium– Autonomic NS: ganglion cells– RES: bone marrow, liver, spleen, lymph
nodes– Lungs, synovial lining and testes

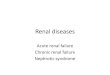
Fabry: Clinical Manifestations
– angiokeratoma (age 10-20) appearance dark red macules or papules
– acroparesthesias exacerbated by fever and exercise (childhood)
– anhidrosis (tears and saliva)– Nausea, abdominal pain, diarrhea– ophthalmic abnormalities: corneal opacity,
posterior cataracts,– ischemic cerebrovascular disease: seizure, TIA,
stroke– ischemic heart disease: MI, dysrhythmias

Angiokeratoma

Kidney
– mild proteinuria (0.5-2g/d) in the 3rd
decade
– Uremia and hypertension in the 4-5th
decade
– ESRD as early as 2nd decade
– Urine: myelin bodies, mild hematuria

Pathology • Uniform-size empty vacuoles (formalin)– Most striking in visceral
epithelial cells of glomeruli– Less in renal arterioles,
tubular epithelium, mesangium, interstitium
• Birefringence and Maltese-cross w/ polarized optics (fresh or frozen)
• Progressive disease: segmental and global glomerulosclerosis

Pathology • IF is negative
• EM: cellular inclusions in all glomerular cells– Zebra bodies or myelin figures
– Onion skin appearance
– Located in lysosomes
• Foot process effusion w/ heavy proteinuria
• DDX: – Pulmonary Scilicosis W/ hematuria and proteinuria: inclusions in
glomeruli
– Clororquine therapy: inclusions in glomeruli
– Aminoglycoside: inclusions in tubules

M&M in Fabry Disease
• Natural Hx: death at mean age of 42 from uremia
• Treated for ESRD: most common causes of death are cerebrovascular and cardiovascular
• After transplant, the glycosphingolipid deposits recur but do not limit renal function
• New Rx: IV alpha-galactosidase q 2 weeks. Approved in Europe last month. Awaiting FDA approval in US

Alport Syndrome
• Inheritance– Classic X-linked dominant– AR– AD
• Gene: COL4A5 encodes for the alpha 5 chain of type IV collagen
• Gene frequency 1:10,000

Alport Clinical Features• Hematuria: microscopic may be persistent, gross
hematuria is intermittent if present. Onset 0-10 yrs• Proteinuria: absent in the first few years of life and
then becomes gradually progressive.• Hypertension-progressive• Renal survival
– Males: nearly all affected progress to ESRD; Age is variable
– Females: better prognosis (X-linked variety); presence of gross hematuria in childhood, nephrotic syndrome, and diffuse GBM thickening are poor prognostic signs

Alport Syndrome• Sensorineural hearing loss: onset by age 15 in males.
Detect by audiometry. Progressive. In females progressive hearing loss is a poor prognostic sign
• Ocular defects: 15-30%– Anterior lenticonus– Corneal endothelial vesicles
• Platelet defects: megathrombocytopenia + platelet dysfunction (AD)
• Diffuse leiomyomatosis: upper GI tract, tracheobronchial tree, females genital. Posterior subcapsular cataracts. (AD)

Alport Nephropathology: Light– < 5 years: nearly nl w/ occasional interstitial foam cells
and fetal glomeruli– mesangial widening– focal thickening of Bowman’s capsule– focal endothelial and mesangial proliferation– split capillary walls– progressive glomerular sclerosis– TBM thickening– interstitial fibrosis and foam cells; tubular atrophy– occasional crescents– capsular tuft synechiae

Nephropathology
• IF
– Typically negative
– Increased deposition w/ sclerosis
• EM
* Variable thickening, thinning, basket weaving, and lamellation of the GBM

Alport Syndrome

Alport: Prognosis
• Post transplant– 5% Anti-GBM nephritis– responds to therapy– likely to recur in next allograft
• Hearing deficit– may progress to total deafness
• Treatment– supportive

Primary Hereditary Hyperoxaluria• Type I
– hyperoxaluria w/ glycolic aciduria – alanine: glyoxylate aminotransferase deficiency (peroxisome)– autosomal recessive; 1:60,000-120,000
• Type II– hyperoxaluria w/ L-glyceric aciduria – D-glycerate dehydrogenase deficiency (cytosol)– very rare
• Type III– Intestinal hyperoxaluria (hyperabsorptive)

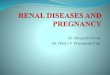
(1)glycine cleavage enzyme; (2) alanine: glyoxylate aminotransferase; (3) D-glyceric acid dehydrogenase; (4) glycerate kinase; (5) trimethylamine oxidase; (6) lactate dehydrogenase; (7) glycolate oxidase; (8) NKH* = nonketotic
hyperglycinemia; TH4 =tetrahydrofolate. Behrman: Nelson Textbook of Pediatrics, 16th ed. 2000

Metabolic PathwayDefective in PH-I
glyoxalate
oxalate glycine
PyridoxineAlanine:glyoxylate aminotransferase
(liver)

Primary Hyperoxaluria-I: Laboratory
• Elevated urinary sodium, oxalate, glycolic acid, and glyoxylic acid
• Laboratory Normal Values– Blood oxalate 10-140 mg/dl– Urine oxalate 10-40 mg/day– Oxalate/Creatinine urine
• Infants < 0.3 mg/mg• 1-5 yo < 0.1 mg/mg• >5 yo < 0.05 mg/mg

Pathology
• Hyperoxalemia: wide spread deposition of oxalate = oxalosis
• Renal deposition: nephrolithiasis, tubulointerstitial nephropathy, renal failure
• Light Microscopy: calcium oxalate crystalline deposits in tubule, interstitium, interstitial fibrosis, late focal glomerular sclerosis. Stone in calyceal system are birefringent

Extrarenal deposition• blood vessel walls• bone • bone marrow
(myelopthesis)• joints• heart• spleen• liver• thymus
• pituitary
• adrenal
• pancreas
• parathyroids
• thyroid
• brain
• heart (conduction defects)

Primary Hyperoxaluria

Primary Hyperoxaluria - ITreatment
• Early diagnosis
• Dietary restriction of glycine and high oxalate foods (spinach, rhubarb, beet roots, iced tea)
• Pyridoxine
• Hydration to limit stone formation (2.5 L/m2)
• + Mg and phosphate supplementation
• Liver / Kidney transplant