Embed Size (px)
Citation preview

←確認用doi (左上Y座標:-17.647 pt)
1140 Vol. 44, No. 8Biol. Pharm. Bull. 44, 1140–1150 (2021)
© 2021 The Pharmaceutical Society of Japan
Regular Article
Inhibitory Effects of Antipsychotics on the Contractile Response to Acetylcholine in Rat Urinary Bladder Smooth MusclesKeisuke Obara,*,a Yuka Matsuoka,a Naoya Iwata,a Yukako Abe,a Yohei Ikegami,a Nanako Shioda,a Yume Hattori,a Shoko Hamamatsu,a Kento Yoshioka,a Fumiko Yamaki,a,b Kazuhiro Matsuo,c Takashi Yoshio,c and Yoshio Tanakaa
a Department of Chemical Pharmacology, Faculty of Pharmaceutical Sciences, Toho University; 2–2–1 Miyama, Funabashi, Chiba 274–8510, Japan: b Department of Pharmacy, Faculty of Pharmacy, Musashino University; 1–1–20 Shinmachi, Nishitokyo, Tokyo 202–8585, Japan: and c Department of Clinical Pharmacy, Faculty of Pharmaceutical Sciences, Toho University; 2–2–1 Miyama, Funabashi, Chiba 274–8510, Japan.Received April 24, 2021; accepted May 27, 2021
The clinical applications of antipsychotics for symptoms unrelated to schizophrenia, such as behavioral and psychological symptoms, in patients with Alzheimer’s disease, and the likelihood of doctors prescrib-ing antipsychotics for elderly people are increasing. In elderly people, drug-induced and aging-associated urinary disorders are likely to occur. The most significant factor causing drug-induced urinary disorders is a decrease in urinary bladder smooth muscle (UBSM) contraction induced by the anticholinergic action of therapeutics. However, the anticholinergic action-associated inhibitory effects of antipsychotics on UBSM contraction have not been sufficiently assessed. In this study, we examined 26 clinically available antipsychot-ics to determine the extent to which they inhibit acetylcholine (ACh)-induced contraction in rat UBSM to predict the drugs that should not be used by elderly people to avoid urinary disorders. Of the 26 antipsychot-ics, six (chlorpromazine, levomepromazine (phenothiazines), zotepine (a thiepine), olanzapine, quetiapine, clozapine (multi-acting receptor targeted antipsychotics (MARTAs))) competitively inhibited ACh-induced contractions at concentrations corresponding to clinically significant doses. Further, 11 antipsychotics (per-phenazine, fluphenazine, prochlorperazine (phenothiazines), haloperidol, bromperidol, timiperone, spiperone (butyrophenones), pimozide (a diphenylbutylpiperidine), perospirone, blonanserin (serotonin–dopamine antagonists; SDAs), and asenapine (a MARTA)) significantly suppressed ACh-induced contraction; however, suppression occurred at concentrations substantially exceeding clinically achievable blood levels. The re-maining nine antipsychotics (pipamperone (a butyrophenone), sulpiride, sultopride, tiapride, nemonapride (benzamides), risperidone, paliperidone (SDAs), aripiprazole, and brexpiprazole (dopamine partial agonists)) did not inhibit ACh-induced contractions at concentrations up to 10−5 M. These findings suggest that chlor-promazine, levomepromazine, zotepine, olanzapine, quetiapine, and clozapine should be avoided by elderly people with urinary disorders.
Key words antipsychotics; rat urinary bladder smooth muscle; anticholinergic effect; urinary disorder
INTRODUCTION
Antipsychotics are mainly utilized to treat schizophrenia; however, in recent years, its application has extended to other mental disorders, such as depression, behavioral and psycho-logical symptoms of dementia (BPSD), and gastrointestinal symptoms associated with chemotherapy.1–5) As a result, the prescription of antipsychotics has been increasing world-wide.6–8) Owing to the increase in human life span, elderly patients with mental disorders, Alzheimer's dementia, and cancer have also been increasing.9–11) Thus, the prescription of antipsychotics for elderly patients is expected to rapidly increase in the future. In support of this speculation, the pre-scription rate of antipsychotics for elderly patients in Japan was found to increase by ≥10% between 2006 and 2012.6)
In general, elderly patients are more likely to develop ad-verse effects than middle-age patients are. For example, elder-ly patients are more prone to antipsychotic-induced movement disorders12) and are at an increased risk of adverse events due to the intake of atypical antipsychotics (serotonin–dopamine antagonists (SDAs), multi-acting receptor targeted antipsychot-ics (MARTAs), dopamine partial agonists (DPAs)); this is be-
cause of age-related changes in pharmacokinetics and pharma-codynamics, current medical conditions, polypharmacy, and potential drug interactions.13) The U.S. Food and Drug Ad-ministration (FDA) issued an advisory and a subsequent black box warning regarding the risks of atypical antipsychotic use among elderly patients with dementia.14) Owing to the issu-ance of this black box warning, many clinical studies on the serious side effects of antipsychotics have been carried out.13) However, little information is available on the side effects that clearly lead to poorer QOL for patients but are not recognized as severe. Urinary disorders are one of the such side effects induced by antipsychotics.15) In elderly people, drug-induced as well as aging-associated urinary disorders are likely to occur.16) Drug-induced urinary disorders affect patient adher-ence,17) and thus should be avoided.
The most significant factor for drug-induced urinary disor-ders is a decrease in urinary bladder smooth muscle (UBSM) contraction due to anticholinergic actions.18) Among antipsy-chotics, there is no significant difference in the rate of side effects caused by anticholinergic actions between patients taking typical antipsychotics and those taking atypical anti-psychotics.15) However, little information is available on which
* To whom correspondence should be addressed. e-mail: [email protected]

Vol. 44, No. 8 (2021) 1141Biol. Pharm. Bull.
antipsychotics inhibit UBSM contractility through their pos-sible anticholinergic actions.
In this study, we determined the potential inhibitory effects of 26 clinically available antipsychotics on acetylcholine (ACh)-induced contractions in rat UBSM. We then compared the drug concentrations required to produce inhibitory effects against ACh-induced contractions with their clinically achiev-able concentration ranges to predict the antipsychotics that should be avoided in elderly patients with urinary disorders. We considered that rat UBSM is suitable for evaluating the anticholinergic potencies of drugs for the following reasons: 1) ACh-induced contractions in both rat and human UBSMs are mediated through M3 receptors, although the expression level of M2 receptors is higher than that of M3 receptors in their UBSMs19); 2) The binding properties of various muscarinic receptor antagonists (such as M1 receptor antagonist, pirenz-epine; M2 receptor antagonist, AF-DX 116; and M3 receptor antagonist, darifenacin) to rat UBSM are almost identical to their binding properties to human UBSM, although the binding properties of β3-adrenoceptor agonists/antagonists to rat UBSM differ from their binding properties to human UBSM.20)
MATERIALS AND METHODS
Animals Male Wistar rats (age, 8–10 weeks old; weight, 175–280 g; Japan SLC, Hamamatsu, Japan) were housed under controlled conditions (21–22°C, relative air humidity 50 ± 5%) and a fixed 12–12 h light–dark cycle (08 : 00–20 : 00), with food and water available ad libitum. This study was approved by the Toho University Animal Care and Use Committee (Ap-proval Nos. 17-53-294, 18-54-294, 19-55-294) and was con-ducted in accordance with the guidelines of the Laboratory Animal Center of Faculty of Pharmaceutical Sciences, Toho University.
Assessment of the Effects of Antipsychotics on ACh-In-duced UBSM Contraction The effects of antipsychotics on UBSM contraction were assessed as previously described.21,22) Briefly, isolated rat UBSM strips were equilibrated under a 0.5 g resting tone for 20 min in a 20 mL organ bath contain-ing Locke–Ringer solution equilibrated with 95% O2 and 5% CO2 at 32 ± 1°C; the solution was comprised of the following (mM): NaCl, 154; KCl, 5.6; CaCl2, 2.2; MgCl2, 2.1; NaHCO3, 5.9; and glucose, 2.8. The UBSM preparation was contracted using 10−4 M ACh at least three times at 20 min intervals (preliminary procedures). After a 30 min equilibration period, ACh was incrementally applied to the bath medium until a maximum response was obtained; this contractile response was recorded twice at 30 min intervals. Following this pro-cedure, the concentration–response curves (CRCs) for ACh were plotted after pre-incubation with different concentrations (3 × 10−7 to 10−5 M) of each tested antipsychotic or verapamil (10−5 M) for 30 min. When dimethyl sulfoxide (DMSO) was used as a drug solvent, the experiment was conducted with a DMSO concentration of 0.5% in the bath solution, including the control experiment. All experiments were carried out in the presence of indomethacin (3 × 10−6 M).
Assessment of the Effects of Antipsychotics on UBSM Contraction Induced by High-KCl Locke–Ringer Solu-tion After the preliminary procedures, atropine (10−6 M), phentolamine (10−6 M), and propranolol (10−7 M) were added
to the bath medium. After a 30 min equilibration period, to produce sustained contractions, the strip was contracted with 80 mM high-KCl solution (containing atropine, prazosin, and propranolol) comprising (mM): NaCl, 79.6; KCl, 80; CaCl2, 2.2; MgCl2, 2.1; NaHCO3, 5.9; and glucose, 2.8. When the contractile response reached a steady state, each antipsychotic was incrementally applied to the bath medium. At the end of the experiment, the UBSM preparations were treated with verapamil (10−5 M).
Drugs The 26 antipsychotics tested in this study were: le-vomepromazine maleate, fluphenazine dimaleate, haloperidol, sultopride hydrochloride, and perospirone hydrochloride dihy-drate (FUJIFILM Wako Pure Chemical Corporation, Osaka, Japan); chlorpromazine hydrochloride, prochlorperazine di-maleate, pipamperone, (±)-sulpiride, tiapride hydrochloride, paliperidone, blonanserin, olanzapine, and aripiprazole (Tokyo Chemical Industry Co., Ltd., Tokyo, Japan); perphenazine, spiperone hydrochloride, quetiapine hemifumarate, clozapine, brexpiprazole, and pimozide (Cayman Chemical, Ann Arbor, MI, U.S.A.); bromperidol (MedChemExpress Co., Ltd., Mon-mouth Junction, NJ, U.S.A.); timiperone (Toronto Research Chemicals, Toronto, ON, Canada); nemonapride, and zotepine (Santa Cruz Biotechnology Inc., Dallas, TX, U.S.A.); risperi-done (Acros Organics, Geel, Belgium); and asenapine maleate (AdooQ BioScience LLC, Irvine, CA, U.S.A.). ACh chloride was purchased from Daiichi Sankyo Co., Ltd. (Tokyo, Japan). Atropine sulfate, indomethacin, propranolol hydrochloride, and (±)-verapamil were purchased from Sigma-Aldrich Co. (St. Louis, MO, U.S.A.). All other chemicals were commer-cially available and of reagent grade.
Fluphenazine and clozapine were dissolved in 0.1 N HCl to create a stock solution of 2 × 10−2 M. Thereafter, the stock so-lutions were further diluted with distilled water to the desired concentrations. The other antipsychotics were dissolved and diluted in pure DMSO. Indomethacin was dissolved in etha-nol to create a stock solution of 10−2 M. All other drugs were prepared as aqueous stock solutions and diluted with distilled water.
Data Analysis and Statistics CRCs for ACh-induced contractions and Schild plot analysis of anxiolytics versus ACh concentrations were performed using GraphPad Prism™ (GraphPad Software Inc., San Diego, CA, U.S.A.), as previ-ously described.21,22) All values are presented as mean ± stan-dard error of the mean (S.E.M.) or mean with 95% confidence intervals (CIs) for different numbers (n) of preparations. GraphPad Prism™ was used for the statistical analyses. Differ-ences among the CRCs were evaluated using post hoc Šidák’s test after two-way ANOVA. Statistical significance was set at p < 0.05.
RESULTS
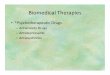
Effects of Phenothiazine Antipsychotics on ACh-Induced Contractions Figure 1 shows the effects of phenothiazine antipsychotics (3 × 10−7 to 10−5 M) on the CRCs of ACh. All tested phenothiazine antipsychotics (chlorpromazine, Fig. 1Aa; levomepromazine, Fig. 1Ba; perphenazine, Fig. 1Ca; fluphen-azine, Fig. 1Da; and prochlorperazine, Fig. 1Ea) were found to inhibit ACh-induced contractions. In the concentration range of 3 × 10−7 to 10−5 M, the slopes of the regression lines in the Schild plot of chlorpromazine (Fig. 1Ab) and levomeproma-

1142 Vol. 44, No. 8 (2021)Biol. Pharm. Bull.
zine (Fig. 1Bb) vs. ACh were 1.09 (95% CIs: 0.88–1.31, n = 5, chlorpromazine) and 0.91 (95% CI: 0.72–1.10, n = 5, levomepromazine); these values were not significantly differ-ent from unity. In the concentration range of 10−6 to 10−5 M, the slopes of the regression lines in the Schild plot of perphen-azine (Fig. 1Cb), fluphenazine (Fig. 1Db), and prochlorpera-zine (Fig. 1Eb) vs. ACh were 0.92 (95% CIs: 0.57–1.27, n = 5, perphenazine), 1.01 (95% CIs: 0.69–1.33, n = 5; fluphenazine), and 0.91 (95% CIs: 0.62–1.19, n = 5, prochlorperazine); these values were not significantly different from unity. Therefore, these phenothiazine antipsychotics were found to competi-tively antagonize ACh in the above concentration ranges. The pA2 values of chlorpromazine, levomepromazine, perphen-azine, fluphenazine, and prochlorperazine were 6.43 (95% CIs: 6.28–6.63, n = 5), 6.48 (95% CIs: 6.32–6.72, n = 5), 6.18 (95% CIs: 5.95–6.63, n = 5), 5.82 (95% CIs: 5.68–6.04, n = 5), and 6.17 (95% CIs: 5.97–6.50, n = 5), respectively.
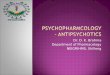
Effects of Phenothiazine Antipsychotics on ACh-Induced Contractions Figure 2 shows the effects of butyrophenone antipsychotics (3 × 10−7 to 10−5 M) on the CRCs of ACh. Of the tested butyrophenone antipsychotics, haloperidol (Fig.
2Aa), bromoperidol (Fig. 2Ba), timiperone (Fig. 2Ca), and spi-perone (Fig. 2Da) inhibited ACh-induced contractions. In the concentration range of 3 × 10−6 to 10−5 M, the slopes of the re-gression lines in the Schild plot of haloperidol (Fig. 2Ab) and timiperone (Fig. 2Cb) vs. ACh were 1.14 (95% CIs: 0.18–2.10, n = 5, haloperidol) and 0.96 (95% CIs: 0.28–1.63, n = 5, timi-perone), respectively; these values were not significantly dif-ferent from unity. In the concentration range of 10−6–10−5 M, the slope of the regression lines in the Schild plot of brom-peridol (Fig. 2Bb) vs. ACh was 0.96 (95% CI: 0.33–1.60, n = 5); this value was not significantly different from unity. Therefore, these butyrophenone antipsychotics competitively antagonized ACh in the above concentration ranges. The pA2 values of haloperidol, timiperone, and bromperidol were 5.43 (95% CIs: 5.21–6.51, n = 5), 5.88 (95% CIs: 5.59–7.44, n = 5), and 5.83 (95% CIs: 5.56–6.62, n = 5), respectively.
In contrast, the slope of the regression line in the Schild plot of spiperone (Fig. 2Db) vs. ACh was 0.47 (95% CIs: 0.24–0.70, n = 5); this value was significantly less than unity. Therefore, spiperone did not competitively antagonize ACh in the above concentration ranges.
Fig. 1. Effects of Phenothiazine Antipsychotics (3 × 10−7 to 10−5 M) on the ACh-Induced Contractions in Rat UBSMAa–Ea: Effects of chlorpromazine (Chl, Aa), levomepromazine (Lev, Ba), perphenazine (Perp, Ca), fluphenazine (Flu, Da), and prochlorperazine (Pro, Ea) on the con-
centration–response curves of ACh-induced contractions. Data are presented as mean ± S.E.M. (n = 5). Ab–Eb: Schild plot analysis of Chl (Ab), Lev, (Bb), Prep (Cb), Flu (Db), and Pro (Eb) vs. ACh. The slope and pA2 values are presented as means with 95% confidence intervals (CIs). ACh, acetylcholine; UBSM, urinary bladder smooth muscle.

Vol. 44, No. 8 (2021) 1143Biol. Pharm. Bull.
Pipamperone (Fig. 2E) was not found to affect the CRCs of ACh in the concentration range of 3 × 10−7 to 10−5 M.
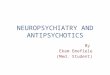
Effects of Benzamide Antipsychotics on ACh-Induced Contractions Figures 3A–D show the effects of benzamide antipsychotics (3 × 10−7 to 10−5 M) on the CRCs of ACh. The tested benzamide antipsychotics (sulpiride, Fig. 3A; sultopride, Fig. 3B; thiapride, Fig. 3C; nemonapride, Fig. 3D) did not af-
fect the CRCs of ACh in the concentration range of 3 × 10−7 to 10−5 M.
Effects of Zotepine and Pimozide on ACh-Induced Con-tractions Figures 3E and 3F show the effects of zotepine (a thiepine antipsychotic) and pimozide (a diphenylbutylpiperi-dine antipsychotic) (3 × 10−7 to 10−5 M) on the CRCs of ACh. Both zotepine (Fig. 3Ea) and pimozide (Fig. 3Fa) inhibited
Fig. 2. Effects of Butyrophenone Antipsychotics (3 × 10−7 to 10−5 M) on the ACh-Induced Contraction of Rat UBSMAa–E: Effects of haloperidol (Hal, Aa), bromperidol (Bro, Ba), timiperone (Tim, Ca), spiperone (Spi, Da), and pipamperone (Pip, E) on the concentration–response
curves of ACh-induced contractions. Data are presented as mean ± S.E.M. for n = 5. Ab–Db: Schild plot analysis of Hal (Ab), Bro, (Bb), Tim (Cb), and Spi (Db) vs. ACh. The slope and pA2 values are presented as means with 95% confidence intervals (CIs). ACh, acetylcholine; UBSM, urinary bladder smooth muscle.
Fig. 3. Effects of Benzamide Antipsychotics (A–D), a Thiepine Antipsychotic (E), and a Diphenylbutylpiperidine Antipsychotic (F) (3 × 10−7 to 10−5 M) on the ACh-Induced Contraction of Rat UBSM
A–Fa: Effects of sulpiride (Sulp, A), sultopride (Sult, B), tiapride (Tia, C), nemonapride (Nem, D), zotepine (Zot, Ea), and pimozide (Pim, Fa) on the concentration–response curves of ACh-induced contractions. Data are presented as mean ± S.E.M. (n = 5). Eb, Fb: Schild plot analysis of Zot (Eb) and Pim (Fb) vs. ACh. The slope and pA2 values are presented as means with 95% confidence intervals (CIs). ACh, acetylcholine; UBSM, urinary bladder smooth muscle.

1144 Vol. 44, No. 8 (2021)Biol. Pharm. Bull.
ACh-induced contractions. The slopes of the regression lines in the Schild plot of zotepine (Fig. 3Eb, 3 × 10−7 to 10−5 M) and pimozide (Fig. 3Eb, 3 × 10−7 to 3 × 10−6 M) vs. ACh were 0.98 (95% CIs: 0.76–1.19, n = 5, zotepine) and 1.01 (95% CIs: 0.70–1.32, n = 5, pimozide), respectively; these values were not significantly different from unity. Therefore, both zotepine and pimozide competitively antagonized ACh in the above concentration ranges. The pA2 values of zotepine and pimo-zide were 6.23 (95% CIs: 6.09–6.42, n = 5) and 7.04 (95% CIs: 6.77–7.52, n = 5), respectively.
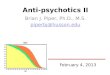
Effects of SDAs on ACh-Induced UBSM Contractions Figures 4A–D show the effects of SDAs (3 × 10−7 to 10−5 M) on the CRCs of ACh. Of the tested SDAs, perospirone (Fig. 4Ca) and blonanserin (Fig. 4Da) inhibited ACh-induced con-tractions. The slopes of the regression lines in the Schild plot of perospirone (Fig. 4Cb, 3 × 10−6 to 10−5 M) and blonanserin (Fig. 4Db, 3 × 10−7 to 10−5 M) vs. ACh were 1.05 (95% CIs: 0.26–1.84, n = 5, perospirone) and 1.08 (95% CIs: 0.81–1.34, n = 5, blonanserin), respectively; these values were not sig-nificantly different from unity. Therefore, these SDAs were found to competitively antagonize ACh in the above concen-tration range. The pA2 values of perospirone and blonanserin were 5.51 (95% CIs: 5.32–6.38, n = 5) and 6.48% (95% CIs: 6.29–6.77, n = 5), respectively.
Risperidone (Fig. 4A) and paliperidone (Fig. 4B) were not found to affect the CRCs of ACh in the concentration range of 3 × 10−7–10−5 M.
Effects of DPAs on ACh-Induced UBSM Contrac-tions Figures 4E and F show the effects of DPAs (3 × 10−7 to 10−5 M) on the CRCs of ACh. Aripiprazole (Fig. 4E) and brexpiprazole (Fig. 4F) did not affect the CRCs of ACh in the concentration range of 3 × 10−7 to 10−5 M.
Effects of MARTAs on ACh-Induced UBSM Contrac-tions Figure 5 shows the effects of MARTAs (3 × 10−7 to 10−5 M) on the CRCs of ACh. All tested MARTAs (olanzap-ine, Fig. 5Aa; quetiapine, Fig. 5Ba; clozapine, Fig. 5Ca; and asenapine, Fig. 5D) inhibited ACh-induced contractions. In the concentration range of 3 × 10−6–10−5 M, the slopes of the regression lines in the Schild plot of olanzapine (Fig. 5Ab) and clozapine (Fig. 5Cb) vs. ACh were 0.97 (95% CIs: 0.67–1.28, n = 5, olanzapine) and 0.93 (95% CIs: 0.33–1.53, n = 5, clo-zapine), respectively; these values were not significantly dif-ferent from unity. In the concentration range of 3 × 10−6 to 10−5 M, the slope of the regression lines in the Schild plot of quetiapine (Fig. 5Bb) vs. ACh was 0.90 (95% CIs: 0.82–1.30, n = 5); this value was not significantly different from unity. Therefore, these MARTAs competitively antagonize ACh in the above concentration range. The pA2 values of olanzap-ine, quetiapine, and clozapine were 7.13 (95% CIs: 6.91–7.54, n = 5), 6.29 (95% CIs: 5.94–7.26, n = 5), and 7.19 (95% CIs: 6.80–8.87, n = 5), respectively.
At ≥10−6 M, the slopes of the regression line in the Schild plot of olanzapine (Fig. 5Ab) and clozapine (Fig. 5Cb) vs. ACh were 0.67 (95% CIs: 0.48–0.86, n = 5, olanzapine) and 0.51 (95% CIs: −0.14–1.17, n = 5, clozapine), respectively; these values were less than unity. Further, in the concentration range of 3 × 10−7 to 3 × 10−6 M, the slope of the regression line in the Schild plot of quetiapine (Fig. 5Bb) vs. ACh was 0.64 (95% CIs: 0.43–0.84, n = 5); this value was significantly less than unity.
In contrast, asenapine (Fig. 5D) inhibited ACh-induced con-tractions only at 10−5 M. However, asenapine did not shift the CRCs of ACh to the right. Instead, it inhibited the maximum response to ACh. The maximum response of CRCs of ACh
Fig. 4. Effects of Serotonin–Dopamine Antagonists (SDAs; A–D) and Dopamine Partial Agonists (DPAs; E, F) (3 × 10−7 to 10−5 M) on ACh-Induced Contraction of Rat UBSM
A–F: Effects of risperidone (Ris, A), paliperidone (Pal, B), perospirone (Pero, Ca), blonanserin (Blo, Da), aripiprazole (Ari, E), and brexpiprazole (Bre, F) on the concen-tration–response curves of ACh-induced contractions. Data are presented as mean ± S.E.M. (n = 5). Cb, Db: Schild plot analysis of Pero (Cb) and Blo (Db) vs. ACh. The slope and pA2 values are presented as means with 95% confidence intervals (CIs). ACh, acetylcholine; UBSM, urinary bladder smooth muscle.

Vol. 44, No. 8 (2021) 1145Biol. Pharm. Bull.
(control = 100%, 3 × 10−3 M) was suppressed to 68.0 ± 7.3% (n = 5) by pretreatment with asenapine (10−5 M).
Effect of Antipsychotics on UBSM Contraction Induced by High-KCl Locke–Ringer Solution Among the tested an-tipsychotics, 18 significantly inhibited ACh-induced contrac-tions. However, some of these antipsychotics did not display competitive antagonism with ACh. A possible mechanism underlying the non-competitive inhibition of ACh-induced contraction could be the inhibition of voltage-dependent L-type Ca2+ channels (VDCCs). Accordingly, this possibility was pharmacologically examined.
First, we investigated the effects of verapamil on ACh-induced contractions to elucidate whether the contractions were mediated via VDCCs. The following results were ob-tained from Fig. 6: the maximum response of the CRC of ACh (100%, 3 × 10−3 M ACh) was significantly inhibited to 52.0 ± 9.1% by verapamil (10−5 M) (n = 5). Thus, Ca2 + influx through VDCCs was demonstrated to be responsible for ACh-induced contractions in smooth muscle preparations.
We proceeded to determine the effects of 18 antipsychot-ics on 80 mM KCl-induced contraction to elucidate whether these antipsychotics could inhibit VDCC-mediated contraction (Table 1). Of the tested drugs, olanzapine hardly suppressed the contractions induced by the 80 mM KCl solution, whereas 17 antipsychotics, besides olanzapine, suppressed these contractions at 10−5 M by approximately 20–50% (Table 1). Pimozide suppressed 80 mM KCl-induced contraction by ap-proximately 10%, even at a concentration of 10−6 M (Table 1).
As the remaining contractions after each drug treatment were completely suppressed by verapamil (10−5 M) (data not shown), the contractions induced by 80 mM KCl solution were elicited via VDCCs.
DISCUSSION
In the present study, we sought to investigate the possible inhibitory effects of 26 clinically available antipsychotics on ACh-induced contractions in rat UBSM to predict the drugs that should not be used by the elderly population to avoid urinary disorders. Of the tested antipsychotics, two typical an-tipsychotics (chlorpromazine and levomepromazine) and four atypical antipsychotics (zotepine, olanzapine, quetiapine, and clozapine) significantly inhibited ACh-induced contractions at clinically significant doses. Such findings suggest that these six antipsychotics should be avoided in elderly people with
Fig. 6. Effect of Verapamil (10−5 M) on ACh-Induced Contraction of Rat UBSM
Data are presented as mean ± S.E.M. (n = 5). * p < 0.05, ** p < 0.01 vs. the control (post hoc Šidák’s test after two-way ANOVA). ACh, acetylcholine; UBSM, urinary bladder smooth muscle.
Fig. 5. Effects of Multi-Acting Receptor Targeted Antipsychotics (MARTAs) (3 × 10−7 to 10−5 M) on the ACh-Induced Contraction of Rat UBSMAa–D: Effects of olanzapine (Ola, Aa), quetiapine (Que, Ba), clozapine (Clo, Ca), and asenapine (Ase, D) on the concentration–response curves of ACh-induced contrac-
tions. Data are presented as mean ± S.E.M. (n = 5). Ab–Cb: Schild plot analysis of Ola (Ab), Que (Bb), and Clo (Cb) vs. ACh. The slope and pA2 values are presented as means with 95% confidence intervals (CIs). ACh, acetylcholine; UBSM, urinary bladder smooth muscle.

1146 Vol. 44, No. 8 (2021)Biol. Pharm. Bull.
urinary disorders.Chlorpromazine/Levomepromazine (Phenothiazines),
Zotepine (a Thiepine), Olanzapine/Quetiapine/Clozapine (MARTAs) Chlorpromazine, levomepromazine, zotepine, olanzapine, and clozapine inhibited ACh-induced contrac-tions in a competitive antagonistic manner. The calculated pA2 values were consistent with the pKi values obtained from our binding study where [3H]N-methyl scopolamine (NMS) was employed in the mouse cerebral cortex23) (Table 2). Therefore, we concluded that the inhibition of ACh-induced UBSM con-tractions by these antipsychotics was due to their anticholiner-gic effects. The pA2 values of the antipsychotics were found to be comparable with their plausible blood concentration levels, which are presented as minus logarithm values, or larger than the plausible blood concentration levels (clozapine). This finding indicates that these antipsychotics can reduce UBSM contractility by inhibiting muscarinic receptors, thereby in-ducing urinary functional disorders within their clinically applied antipsychotic dose ranges. The pA2 values/pKi values/plausible blood concentration levels (expressed as minus loga-rithm values) of each drug were (Table 2): 6.43/6.40/5.85–7.55 (chlorpromazine); 6.48/6.22/6.21–7.35 (levomepromazine); 6.23/6.21/6.14–7.04 (zotepine); 7.13/6.85/6.37–7.38 (olanzapine); and 7.19/6.83/5.23–6.30 (clozapine).
In the concentration range of 3 × 10−6 to 10−5 M, quetiapine competitively inhibited ACh-induced contractions, and its pA2 value was calculated to be 6.29. This value was one order of magnitude larger than the calculated pKi value (5.31) (Table 2), but consistent with the pKi value for the muscarinic M3 receptor (6.65) obtained from the binding experiment using [3H] NMS.24) Our calculated pKi value for [3H] NMS in the mouse cerebral cortex corresponded to the quetiapine’s pKi
value for M5 receptor25); however, we do not have any reason-able explanations for this. Nonetheless, the pA2 value (6.29) of quetiapine was in its plausible blood concentration levels and was expressed as the minus logarithm (−log M: 5.92–7.95). This finding suggests that clinically applied quetiapine re-duces UBSM contractility and urinary disorders by inhibiting muscarinic receptors.
In the concentration range of ≥ 10−6 M, olanzapine and clozapine did not show competitive inhibitory effects on ACh as the slope of the regression line in the Schild plot was sig-nificantly less than unity (0.67 and 0.51, respectively). The ap-parent non-competitive effects of these antipsychotics against ACh could be explained by their different affinities for the M2/M3 receptors. Although UBSM expresses both the M2/M3 receptors, the receptor subtype responsible for UBSM con-tractions is M3.26) Both olanzapine and clozapine have higher affinity for M3 than M2. The pKi values for olanzapine were 7.89/7.32 (M3/M2) while those for clozapine were 8.15/7.32 (M3/M2).25) Based on these previous results, we infer the fol-lowing for the muscarinic receptor subtypes responsible for inducing inhibition vs. ACh-induced contraction by olanzapine and clozapine: in the low concentration ranges (3 × 10−7 to 10−6 M), both antipsychotics selectively bind to M3 and pro-duce competitive antagonistic effects against ACh and inhibi-tion of ACh-induced UBSM contraction. In contrast, at higher concentrations (≥ 10−6 M), both antipsychotics could bind to M2, which is not responsible for inducing ACh-induced contraction, and thus, did not show apparently competitive antagonistic effects against ACh.
In the low concentration range (3 × 10−7 to 3 × 10−6 M), quetiapine did not exhibit any competitive inhibitory effects against ACh, as the slope of the regression line in the Schild
Table 1. Effects of Antipsychotics (10−7 to 10−5 M) on 80 mM KCl Solution-Induced Contractions in Rat Urinary Bladder Smooth Muscle
Category/Generic nameInhibition of high-K-induced contraction (%)
10−7 M 10−6 M 10−5 M
Phenothiazine antipsychoticsChlorpromazine 0.1 ± 0.2 3.1 ± 1.7 38.0 ± 8.5Levomepromazine 1.3 ± 1.9 4.3 ± 1.8 40.8 ± 2.5Perphenazine 0.7 ± 0.9 2.2 ± 0.7 20.2 ± 3.8Fluphenazine 0.6 ± 0.8 4.2 ± 2.8 27.7 ± 5.8Prochlorperazine 0.7 ± 0.7 2.0 ± 0.7 25.2 ± 2.0
Butyrophenone antipsychoticsHaloperidol 1.1 ± 1.6 2.4 ± 1.1 46.3 ± 6.0Bromperidol 0.7 ± 0.4 2.1 ± 0.6 41.9 ± 5.3Timiperone 0.0 ± 0.1 2.1 ± 0.7 42.7 ± 10.7Spiperone 2.7 ± 2.8 4.4 ± 1.6 26.1 ± 4.4
Thiepin antipsychoticZotepine 1.0 ± 0.9 2.1 ± 0.5 22.3 ± 4.4
Diphenylbutylpiperidine antipsychoticPimozide 2.2 ± 1.9 10.9 ± 2.4 49.6 ± 4.7
Serotonin–dopamine antagonists (SDAs)Perospirone 1.5 ± 2.2 3.5 ± 1.0 25.5 ± 4.9Blonanserin 1.8 ± 1.8 8.5 ± 6.1 36.8 ± 10.7
Multi-acting receptor-targeted antipsychotics (MARTAs)Olanzapine 0.4 ± 1.1 1.1 ± 0.7 7.3 ± 2.7Quetiapine 1.1 ± 0.9 1.7 ± 0.7 18.9 ± 4.6Clozapine 0.4 ± 1.1 0.7 ± 0.7 32.2 ± 3.7Asenapine 1.2 ± 1.1 3.8 ± 0.7 56.4 ± 6.3
Data are presented as mean ± S.E.M. (n = 5).

Vol. 44, No. 8 (2021) 1147Biol. Pharm. Bull.
plot was significantly less than unity (0.64). Such finding might be explained by the different affinities of quetiapine between M2 and M3: quetiapine has a higher affinity for M2 (pKi = 6.20) than M3 (pKi = 5.88).24) Therefore, in the low concentration ranges (3 × 10−7 to 3 × 10−6 M), quetiapine is speculated to bind to non-contractile M2 and M3, and thus exert apparently non-competitive effects against ACh. In con-trast, at higher concentrations (3 × 10−6 to 10−5 M), where the binding of quetiapine to M2 becomes saturated, quetiapine displayed competitive antagonism against ACh on contractile M3, and thus, produced inhibitory effects against ACh-induced contraction in a competitive manner.
Prochlorperazine/Perphenazine/Fluphenazine (Phenothi-azines), Haloperidol/Bromperidol/Timiperone (Butyrophe-nones), Pimozide (a Diphenylbutylpiperidine), and Blonan-serin (SDA) Prochlorperazine, timiperone, and blonanserin suppressed ACh-induced contraction in a competitive fashion, and their calculated pA2 values were close to their pKi values obtained from our binding experiments23) (Table 2). As a re-sult, we concluded that the inhibitory effects of these antipsy-
chotics on ACh-induced contraction were mainly due to their anticholinergic effects. The pA2/pKi values of each antipsy-chotic were (Table 2): 6.17/5.68 (prochlorperazine), 5.88/5.39 (timiperone), and 6.48/6.09 (blonanserin).
In our previous study, the pKi values could not be calculated for perphenazine, fluphenazine, haloperidol, and bromperidol (pKi < 5.39).23) However, the pA2 values of perphenazine (6.18) and fluphenazine (5.82) were found to be approximately com-parable to their pKi values (5.31, perphenazine; and 5.39, flu-phenazine), which were calculated from the binding study for rat cerebral cortex using [3H] quinuclidinyl benzilate (QNB).27) In addition, the pA2 value of haloperidol (5.43) was almost comparable to its pKi value (5.80) calculated from the bind-ing study for the rat submandibular gland using [3H] NMS.24) Therefore, the inhibitory effects of perphenazine, fluphen-azine, and haloperidol on ACh-induced contraction could be mainly caused by their anticholinergic effects. We speculated that bromperidol inhibited ACh-induced contraction through the same mechanism (anticholinergic effects) as haloperidol because bromperidol has a bromine atom that replaces the
Table 2. Comparison of the pA2 Values of Drugs vs. ACh, Their pKi Values vs. Muscarinic Receptor, and the Clinically Achievable Blood Concentra-tion of Antipsychotics
Category/Generic name pA2 values vs. ACh pKi values vs. muscarinic receptor
Clinically achievable blood concentration (−log M) Ref.
Phenothiazine antipsychoticsChlorpromazine 6.43 (6.28–6.63) 6.40 ± 0.08 5.85–7.55 37)Levomepromazine 6.48 (6.32–6.72) 6.22 ± 0.07 6.21–7.35 37)Perphenazine 6.18 (5.95–6.63) <5.39 7.43–9.00 37)Fluphenazine 5.82 (5.68–6.04) <5.39 7.59–8.87 37)Prochlorperazine 6.17 (5.97–6.50) 5.68 ± 0.14 7.87–9.55 38)
Butyrophenone antipsychoticsHaloperidol 5.43 (5.21–6.51) <5.39 6.19–7.90 37)Bromperidol 5.83 (5.56–6.62) <5.39 7.25–8.28 39)Timiperone 5.88 (5.59–7.74) 5.39 ± 0.09 7.62–8.06 40)Spiperone — <5.39 7.88* 41)Pipamperone — <5.39 6.22 42)
Benzamide antipsychoticsSulpiride — <5.39 5.48–6.69 43)Sultopride — <5.39 5.12–7.04 43)Tiapride — <5.39 5.25–5.55 44)Nemonapride — <5.39 8.44–9.33** 45)
Thiepin antipsychoticZotepine 6.23 (6.09–6.42) 6.21 ± 0.03 6.14–7.04 46)
Diphenylbutylpiperidine antipsychoticPimozide 7.04 (6.77–7.52) 5.64 ± 0.09 7.39–8.97 47)
Serotonin–dopamine antagonists (SDA)Risperidone — <5.39 6.53–8.61 47)Paliperidone — <5.39 6.70–7.53 48)Perospirone 5.51 (5.32–6.38) <5.39 7.82–9.70 49)Blonanserin 6.48 (6.32–6.72) 6.09 ± 0.13 8.61–9.26 50)
Dopamine partial agonists (DPAs)Aripiprazole — <5.39 5.71–7.65 47)Brexpiprazole — <5.39 6.11–6.83 51)
Multi-acting receptor-targeted antipsychotics (MARTA)Olanzapine 7.13 (6.91–7.54) 6.85 ± 0.14 6.37–7.38 48)Quetiapine 6.29 (5.94–7.26) 5.31 ± 0.12 5.92–7.95 52)Clozapine 7.19 (6.80–8.87) 6.83 ± 0.09 5.23–6.30 53)Asenapine — <5.39 7.70–8.53 54)
*Data from rabbit. **Total concentration of nemonapride and its metabolites. pKi values vs. the muscarinic receptor were obtained from our previous report using [3H]N-methyl scopolamine in the mouse cerebral cortex.23) Ref.: references from which the clinically achievable blood concentrations were obtained.

1148 Vol. 44, No. 8 (2021)Biol. Pharm. Bull.
chlorine atom possessed by haloperidol in its structure.The pA2 value of pimozide (7.04) was one order of mag-
nitude larger than the pKi value (5.64) obtained from our binding experiments23) (Table 2) and the value (6.10) obtained from binding experiments in the human brain using [3H] QNB (6.10).28) These findings imply that pimozide inhibited ACh-induced contractions primarily through anticholinergic action-unrelated mechanisms, despite exhibiting anticholinergic ac-tions at higher concentrations.
In addition to pimozide, the pA2 values of most other anti-psychotics were slightly higher than their pKi values (Table 2). Therefore, mechanisms besides those used to elucidate their anticholinergic effects might be responsible for their inhibi-tory effects against ACh-induced contractions. One plausible mechanism could be the inhibition of VDCCs, which was supported by the evidence that these antipsychotics suppressed the depolarizing contraction induced by 80 mM KCl (Table 1). Consistently, fluphenazine was reported to exhibit Ca2+ channel blocking effects29); haloperidol and pimozide were re-ported to suppress Ca2+ currents30); and phenothiazines31) and butyrophenones32) were reported to exert calmodulin inhibi-tory effects. Thus, in addition to anticholinergic actions, the antipsychotic suppression of ACh-induced contractions might be mediated via the VDCC-inhibitory actions and/or calmodu-lin inhibitory actions. However, the concentrations required to inhibit ACh-induced contractions were markedly higher than the clinically achieved blood concentrations (pA2 values<−log [clinical blood concentrations]) of these antipsychotics (Table 2). Therefore, these antipsychotics do not induce or worsen urinary disorders as long as their clinically applied doses are administered. However, it should be noted that the higher lev-els of unmetabolized drugs and metabolites of these drugs in urine than in the blood might cause urinary disorders by act-ing from within the urinary bladder.
Spiperone (a Butyrophenone), Perospirone (SDA), and Asenapine (MARTA) Spiperone, perospirone, and asenap-ine apparent-competitively or non-competitively suppressed ACh-induced contractions. However, the results of our previ-ous study and others revealed that their pKi values for the muscarinic receptor were lower than their blood concentra-tions, presented as minus logarithm, or lower than experimen-tally detectable levels: spiperone, pKi<5.3923); perospirone, pKi<5.39,23) pKi<633); asenapine, pKi<5.39,23) pKi≤5.34)
Nonetheless, these drugs were found to inhibit depolarizing contractions in the 80 mM KCl solutions (Table 1). Therefore, we concluded that the inhibition of ACh-induced contractions by these drugs was mediated by their non-anticholinergic ac-tions, such as the inhibition of VDCC/calmodulin. Based on prior reports, these drugs possess the following effects: spiper-one, Ca2+ current inhibitory effect29); asenapine, action potential duration-reducing effects on Purkinje fibers35); and butyrophe-nones, calmodulin inhibitory effects.32) However, the clinically achievable blood concentrations of these drugs are markedly lower than the concentrations needed to suppress ACh-induced contractions (Table 2). Therefore, these antipsychotics are un-likely to induce urinary disorders at the clinical doses.
Pipamperone (a Butyrophenone), Sulpiride/Sultopride/Tiapride/Nemonapride (Benzamides), Risperidone/Paliperi-done (SDAs), and Aripiprazole/Brexpiprazole Pipamper-one, sulpiride/sultopride/tiapride/nemonapride, risperidone/paliperidone, and aripiprazole/brexpiprazole suppressed ACh-
induced contractions up to 10−5 M. However, their pKi values (pKi<5.39) could not be obtained because of their marginal effects on [3H] NMS in the cerebral cortex.23) Sulpiride and aripiprazole did not suppress ACh-induced contractions in guinea pig UBSM.36) Additionally, the plausible blood con-centration levels of all drugs were found to be markedly lower than 10−5 M (Table 2). Therefore, these antipsychotics were not found to cause anticholinergic action-mediated urinary disor-ders within the doses administered clinically.
Acknowledgments The authors would like to thank Mr. Yunfeng Ban for his expert technical assistance. This study was partly supported by the Joint Research Grants of the Toho University Faculty of Pharmaceutical Sciences (K.O.).
Conflict of Interest The authors declare no conflict of interest.
REFERENCES
1) Bosnjak SM, Dimitrijevic J, Djordjevic F. Cancer and chemothera-py-induced nausea and vomiting: a focus on olanzapine. Curr. Opin. Support. Palliat. Care, 10, 180–188 (2016).
2) Chiesa D, Marengoni A, Nobili A, Tettamanti M, Pasina L, Franchi C, Djade CD, Corrao S, Salerno F, Marcucci M, Romanelli G, Man-nucci PM. Antipsychotic prescription and mortality in hospitalized older persons. Psychogeriatrics, 17, 397–405 (2017).
3) Lally J, MacCabe JH. Antipsychotic medication in schizophrenia: a review. Br. Med. Bull., 114, 169–179 (2015).
4) Trifiró G, Sultana J, Spina E. Are the safety profiles of antipsy-chotic drugs used in dementia the same? An updated review of observational studies. Drug Saf., 37, 501–520 (2014).
5) Zhou X, Keitner GI, Qin B, Ravindran AV, Bauer M, Del Giovane C, Zhao J, Liu Y, Fang Y, Zhang Y, Xie P. Atypical antipsychotic augmentation for treatment-resistant depression: a systematic re-view and network meta-analysis. Int. J. Neuropsychopharmacol., 18, pyv060 (2015).
6) Kochi K, Sato I, Nishiyama C, Tanaka-Mizuno S, Doi Y, Arai M, Fujii Y, Matsunaga T, Ogawa Y, Furukawa TA, Kawakami K. Trends in antipsychotic prescriptions for Japanese outpatients dur-ing 2006–2012: a descriptive epidemiological study. Pharmacoepi-demiol. Drug Saf., 26, 642–656 (2017).
7) Hálfdánarson O, Zoëga H, Aagaard L, et al. International trends in antipsychotic use: A study in 16 countries, 2005–2014. Eur. Neuro-psychopharmacol., 27, 1064–1076 (2017).
8) Raschi E, Poluzzi E, Godman B, Koci A, Moretti U, Kalaba M, Bennie M, Barbui C, Wettermark B, Sturkenboom M, De Ponti F. Torsadogenic risk of antipsychotics: combining adverse event reports with drug utilization data across Europe. PLOS ONE, 8, e81208 (2013).
9) Deak F, Freeman WM, Ungvari Z, Csiszar A, Sonntag WE. Recent developments in understanding brain aging: implications for Al-zheimer’s disease and vascular cognitive impairment. J. Gerontol. A Biol. Sci. Med. Sci., 71, 13–20 (2016).
10) Kudryavtseva AV, Krasnov GS, Dmitriev AA, Alekseev BY, Kardy-mon OL, Sadritdinova AF, Fedorova MS, Pokrovsky AV, Melnikova NV, Kaprin AD, Moskalev AA, Snezhkina AV. Mitochondrial dysfunction and oxidative stress in aging and cancer. Oncotarget, 7, 44879–44905 (2016).
11) Karel MJ, Gatz M, Smyer MA. Aging and mental health in the decade ahead: what psychologists need to know. Am. Psychol., 67, 184–198 (2012).
12) Caligiuri MR, Jeste DV, Lacro JP. Antipsychotic-induced movement disorders in the elderly: epidemiology and treatment recommenda-

Vol. 44, No. 8 (2021) 1149Biol. Pharm. Bull.
tions. Drugs Aging, 17, 363–384 (2000).13) Gareri P, Segura-Garcia C, Manfredi VG, Bruni A, Ciambrone
P, Cerminara G, De Sarro G, De Fazio P. Use of atypical anti-psychotics in the elderly: a clinical review. Clin. Interv. Aging, 9, 1363–1373 (2014).
14) Dorsey ER, Rabbani A, Gallagher SA, Conti RM, Alexander GC. Impact of FDA black box advisory on antipsychotic medication use. Arch. Intern. Med., 170, 96–103 (2010).
15) Ozbilen M, Adams CE, Marley J. Anticholinergic effects of oral antipsychotic drugs of typicals versus atypicals over medium- and long-term: systematic review and meta-analysis. Curr. Med. Chem., 19, 5214–5218 (2012).
16) Verhamme KMC, Sturkenboom MCJM, Stricker BHC, Bosch R. Drug-induced urinary retention: incidence, management and pre-vention. Drug Saf., 31, 373–388 (2008).
17) Uher R, Farmer A, Henigsberg N, et al. Adverse reactions to anti-depressants. Br. J. Psychiatry, 195, 202–210 (2009).
18) Obara K, Chino D, Tanaka Y. The recovery effects of distigmine on guinea pig detrusor underactivity induced by anticholinergic drugs. Ōyō Yakuri/Pharmacometrics, 91, 25–39 (2016).
19) Anisuzzaman AS, Morishima S, Suzuki F, Tanaka T, Yoshiki H, Sathi ZS, Akino H, Yokoyama O, Muramatsu I. Assessment of muscarinic receptor subtypes in human and rat lower urinary tract by tissue segment binding assay. J. Pharmacol. Sci., 106, 271–279 (2008).
20) Palea S, Rekik M, Rouget C, Camparo P, Botto H, Rischmann P, Lluel P, Westfall TD. Fenoterol functionally activates the β3-adrenoceptor in human urinary bladder, comparison with rat and mouse: implications for drug discovery. Eur. J. Pharmacol., 690, 202–206 (2012).
21) Obara K, Ao L, Ogawa T, Ikarashi T, Yamaki F, Matsuo K, Yo-shio T, Tanaka Y. Assessment of inhibitory effects of hypnotics on acetylcholine-induced contractions in isolated rat urinary bladder smooth muscle. Biol. Pharm. Bull., 42, 280–288 (2019).
22) Obara K, Ao L, Shimada T, Horiguchi S, Ikarashi T, Ogawa T, Yo-shioka K, Yamaki F, Matsuo K, Yoshio T, Tanaka Y. Pharmacologi-cal characteristics of anxiolytics on acetylcholine-induced contrac-tions in rat detrusor smooth muscle. Pharmacology, 105, 369–376 (2020).
23) Obara K, Horiguchi S, Shimada T, Ikarashi T, Yamaki F, Matsuo K, Yoshio T, Tanaka Y. Characterization of binding of antipsychotics to muscarinic receptors using mouse cerebral cortex. J. Pharmacol. Sci., 140, 197–200 (2019).
24) Bymaster FP, Calligaro DO, Falcone JF, Marsh RD, Moore NA, Tye NC, Seeman P, Wong DT. Radioreceptor binding profile of the atypical antipsychotic olanzapine. Neuropsychopharmacology, 14, 87–96 (1996).
25) Bymaster FP, Felder CC, Tzavara E, Nomikos GG, Calligaro DO, McKinzie DL. Muscarinic mechanisms of antipsychotic atypical-ity. Prog. Neuropsychopharmacol. Biol. Psychiatry, 27, 1125–1143 (2003).
26) Frazier EP, Peters SLM, Braverman AS, Ruggieri MR Sr, Michel MC. Signal transduction underlying the control of urinary bladder smooth muscle tone by muscarinic receptors and beta-adreno-ceptors. Naunyn Schmiedebergs Arch. Pharmacol., 377, 449–462 (2008).
27) Hals PA, Hall H, Dahl SG. Muscarinic cholinergic and histamine H1 receptor binding of phenothiazine drug metabolites. Life Sci., 43, 405–412 (1988).
28) Richelson E, Souder T. Binding of antipsychotic drugs to human brain receptors: focus on newer generation compounds. Life Sci., 68, 29–39 (2000).
29) Sah DW, Bean BP. Inhibition of P-type and N-type calcium chan-nels by dopamine receptor antagonists. Mol. Pharmacol., 45, 84–92 (1994).
30) Ito K, Nakazawa K, Koizumi S, Liu M, Takeuchi K, Hashimoto T,
Ohno Y, Inoue K. Inhibition by antipsychotic drugs of L-type Ca2+ channel current in PC12 cells. Eur. J. Pharmacol., 314, 143–150 (1996).
31) Kamei A, Mizumoto Y, Takehana M. The relationship between properties of antipsychotic drugs and cataract formation. Biol. Pharm. Bull., 17, 237–242 (1994).
32) Prokopenko RA, Mogilevich SE, Luik AI, Naydyenova IY, Batrak GN, Hawryluk BR, Degtiar VY. Effects of haloperidol and chlor-promazine on smooth muscle contractility, platelet aggregation and neuronal calcium current. Gen. Physiol. Biophys., 14, 349–357 (1995).
33) Maruoka Y, Ohno Y, Kato T, Hirose A, Tatsuno T, Nakamura M. Effects of SM-9018, a potential atypical neuroleptic, on the central monoaminergic system in rats. Jpn. J. Pharmacol., 62, 419–422 (1993).
34) Shahid M, Walker GB, Zorn SH, Wong EHF. Asenapine: a novel psychopharmacologic agent with a unique human receptor signa-ture. J. Psychopharmacol., 23, 65–73 (2009).
35) A Product monograph for Saphris® tablets provided by Merck Canada Inc. (Kirkland, QC, Canada).
36) Uno J, Obara K, Suzuki H, Miyatani S, Chino D, Yoshio T, Tanaka Y. Inhibitory effects of antidepressants on acetylcholineinduced contractions in isolated guinea pig urinary bladder smooth muscle. Pharmacology, 99, 89–98 (2017).
37) Winek CL, Wahba WW, Winek CL Jr, Balzer TW. Drug and chemi-cal blood-level data 2001. Forensic Sci. Int., 122, 107–123 (2001).
38) Tashiro M, Naito T, Kagawa Y, Kawakami J. Simultaneous deter-mination of prochlorperazine and its metabolites in human plasma using isocratic liquid chromatography tandem mass spectrometry. Biomed. Chromatogr., 26, 754–760 (2012).
39) Someya T, Muratake T, Hirokane G, Shibasaki M, Shimoda K, Takahashi S. Interindividual variation in bromperidol metabolism and relationship to therapeutic effects. J. Clin. Psychopharmacol., 20, 175–180 (2000).
40) Shimoda K, Someya T, Morita S, Hirokane G, Yokono A, Shiba-saki M, Takahashi S. Plasma concentrations of timiperone and its reduced metabolite in the patients on timiperone. Psychiatry Clin. Neurosci., 52, 535–540 (1998).
41) An interview form for Spiropitan® tablets was provided by Eisai Co., Ltd. (Tokyo, Japan).
42) Potgieter GE, Groenewoud G, Jordaan PJ, Hundt HK, Schall R, Kummer M, Sewarte-Ross G. Pharmacokinetics of pipamperone from three different tablet formulations. Arzneimittelforschung, 52, 430–434 (2002).
43) Tokunaga H, Kudo K, Imamura T, Jitsufuchi N, Ohtsuka Y, Ikeda N. Plasma concentrations of antipsychotic drugs in psychiatric inpa-tients. Nihon Hoigaku Zasshi, 51, 417–422 (1997).
44) Roos RA, de Haas EJ, Buruma OJ, de Wolff FA. Pharmacokinetics of tiapride in patients with tardive dyskinesia and Huntington’s dis-ease. Eur. J. Clin. Pharmacol., 31, 191–194 (1986).
45) Mihara K, Kondo T, Suzuki A, Yasui N, Nagashima U, Ono S, Otani K, Kaneko S. Prolactin response to nemonapride, a selective antagonist for D2 like dopamine receptors, in schizophrenic patients in relation to Taq1A polymorphism of DRD2 gene. Psychopharma-cology, 149, 246–250 (2000).
46) Noda K, Suzuki A, Okui M, Noguchi H, Nishiura N, Nishiura N. Pharmacokinetics and metabolism of 2-chloro-11-(2-dimethylaminoethoxy)-dibenzo[b,f ]thiepine (zotepine) in rat, mouse, dog and man. Arzneimittelforschung, 29, 1595–1600 (1979).
47) van der Weide K, van der Weide J. The influence of the CYP3A4*22 polymorphism and CYP2D6 polymorphisms on serum concentra-tions of aripiprazole, haloperidol, pimozide, and risperidone in psychiatric patients. J. Clin. Psychopharmacol., 35, 228–236 (2015).
48) Wang ST, Li Y. Development of a UPLC-MS/MS method for routine therapeutic drug monitoring of aripiprazole, amisulpride, olanzapine, paliperidone and ziprasidone with a discussion of their

1150 Vol. 44, No. 8 (2021)Biol. Pharm. Bull.
therapeutic reference ranges for Chinese patients. Biomed. Chro-matogr., 31, e3928 (2017).
49) Gen K, Morokawa Y, Inoue Y, Miyake N, Sekiguchi G, Akomoto T, Suzuki H, Ishizeki K, Takagi H, Tanaka A, Aoba A. Daily dosage of Perospirone, concentrations of nonmetabolized drug and metabo-lite ID-15036 in plasma, and anti-dopamine (D2) and anti-serotonin (5-HT2A) activities in plasma. Jpn. J. Clin. Psychopharmacol., 9, 1581–1589 (2006).
50) Suzuki H, Gen K. The relationship between the daily dose, the plasma concentration of blonanserin, and its plasma anti-dopamine D2 and anti-serotonin 5-HT2A activity. Hum. Psychopharmacol., 25, 342–346 (2010).
51) Ishigooka J, Iwashita S, Higashi K, Liew EL, Tadori Y. Pharma-cokinetics and safety of brexpiprazole following multiple-dose
administration to Japanese patients with schizophrenia. J. Clin. Pharmacol., 58, 74–80 (2018).
52) van der Weide K, van der Weide J. The influence of the CYP3A4*22 polymorphism on serum concentration of quetiapine in psychiatric patients. J. Clin. Psychopharmacol., 34, 256–260 (2014).
53) Rajji TK, Mulsant BH, Davies S, Kalache SM, Tsoutsoulas C, Pol-lock BG, Remington G. Prediction of working memory performance in schizophrenia by plasma ratio of clozapine to N-desmethylclozap-ine. Am. J. Psychiatry, 172, 579–585 (2015).
54) Dogterom P, Timmer C, de Greef R, Spaans E, de Vries D, van Vliet A, Peeters P. Asenapine safety, tolerability, and pharmacoki-netics after single and multiple doses in healthy volunteers. Clin. Pharmacol. Drug Dev., 1, 131–143 (2012).