Embed Size (px)
DESCRIPTION
Initiatives to Improve LTC Direct Care Workforce Retention: What is the Evidence Base?. Lauren D. Harris-Kojetin, PhD Institute for the Future of Aging Services www.futureofaging.org [email protected] AcademyHealth Annual Research Meeting Boston, MA June 26, 2005. - PowerPoint PPT Presentation
Citation preview
Initiatives to Improve LTC Direct Care Workforce Retention: What is
the Evidence Base?
Lauren D. Harris-Kojetin, PhDInstitute for the Future of Aging Services
AcademyHealth Annual Research MeetingBoston, MA
June 26, 2005
Presentation Overview
• Background• Purpose• Context/Conceptual Models• Research Synthesis
– Methods– Key findings on effective interventions
• Implications• Resources
Background
“Education and training of staff, supervision,environmental conditions, attitudes andvalues, job satisfaction and turnover of staff,salaries and benefits, leadership,management, and organizational capacityare all essential elements affecting quality ofcare to residents.”
IOM, Improving the Quality of Long-Term Care
• Over 2.4 M paraprofessional LTC workers form the core of the formal LTC system
• Turnover ranging from 45% to over 100%
• Between 2002 – 2012, 888,000 more DCW jobs
• 27 M Americans are projected to need LTC by 2050
• Significant societal factors converging “care gap”
• Variety of factors associated with LTC direct care workforce (DCW) recruitment & retention problems – inadequate training, job orientation & lack of
mentoring– poor public image of LTC direct care workforce– low pay & insufficient benefits– few opportunities for development within the
position– poor supervision– emotionally & physically hard work– workplace stress & burnout– personal life stressors– lack of respect from residents’ families– short staffing
Purpose
– States, providers & worker groups have designed & implemented a variety of initiatives intended to address DCW LTC problems
– Some of these initiatives have been evaluated
– Current state of evidence base on relationship between how LTC work is organized/structured & DCW turnover/retention
Context/Conceptual Models
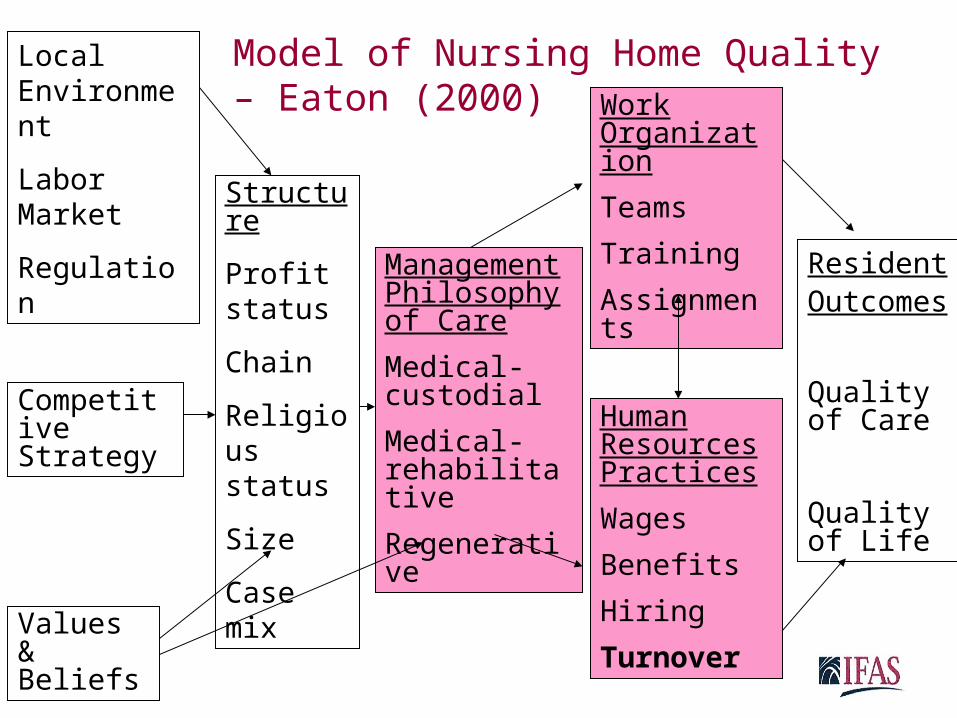
Local Environment
Labor Market
Regulation
Competitive Strategy
Values & Beliefs
Structure
Profit status
Chain
Religious status
Size
Case mix
Management Philosophy of Care
Medical-custodial
Medical-rehabilitative
Regenerative
Work Organization
Teams
Training
Assignments
Human Resources Practices
Wages
Benefits
Hiring
Turnover
ResidentOutcomes
Quality of Care
Quality of Life
Model of Nursing Home Quality – Eaton (2000)
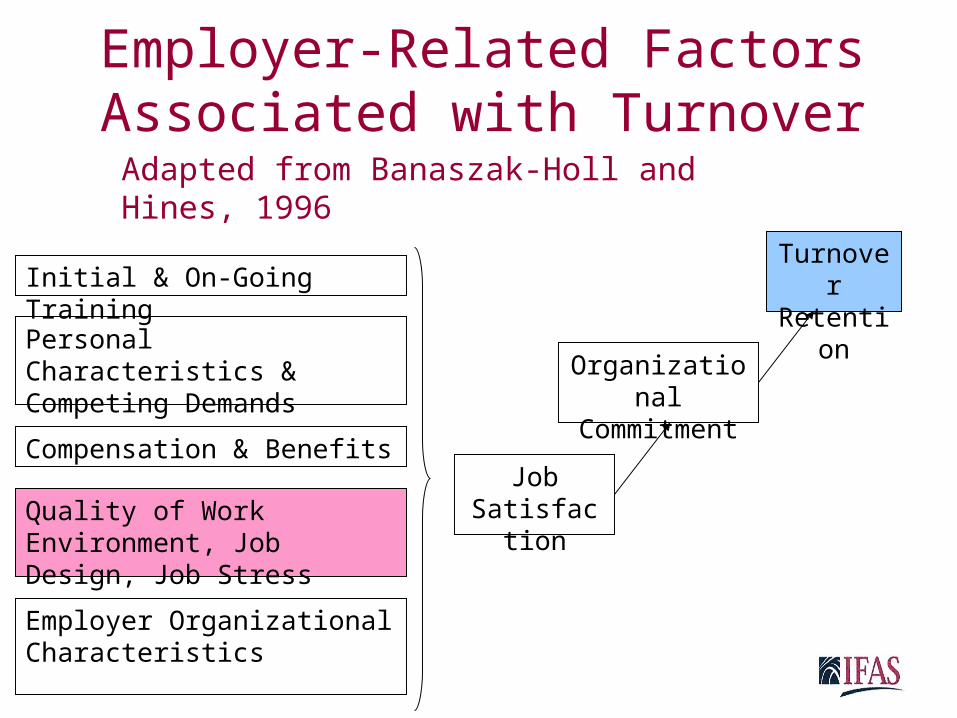
Employer-Related Factors Associated with Turnover
Job Satisfaction
Organizational Commitment
TurnoverRetention
Personal Characteristics & Competing Demands
Compensation & Benefits
Quality of Work Environment, Job Design, Job Stress
Initial & On-Going Training
Employer Organizational Characteristics
Adapted from Banaszak-Holl and Hines, 1996
Research Synthesis
Recent Insights about Frontline Long-Term Care
Workers: A Research Synthesis 1999-2003Lauren Harris-Kojetin, PhD
Debra Lipson, MHSAJean Fielding, MGSKristen Kiefer, MPP
Robyn I. Stone, DrPH
Funded by ASPE, DHHS
Methods
• Search sources: Ageline, PubMed, Internet searches, personal communications, conferences, initiatives in Stone (2001)
• Eligible materials: Published & gray literature
• Search terms (examples): LTC workforce, labor force, recruiting, paraprofessional, job tenure, work environment, intervention
• Timeframe: 1999 – 2003• Outcomes: turnover and/or retention• Data collection: Study documents
abstracted & categorized by intervention type, evaluation design & results
Types of Interventions Evaluated
1999 - 2003• Alternative labor pools• Career ladders• Culture change• Enhanced staff-family communication• Multi-faceted initiatives• Peer mentoring• Self-managed work teams• Wage enhancements
Types of Initiatives Evaluated1999 – 2003 (continued)
• 15 interventions reviewed– 2 had not (yet) had outcome evaluation – 2 did not measure actual turnover or
retention– 8 showed non-significant, negative, or
inconclusive results or did not use robust quasi-experimental design
– 3 showed significant positive turnover/retention results using a pre-post comparison group design
Key Findings on Effective Interventions
Growing Strong Roots – Peer Mentoring
• Trained, experienced certified nursing assistants (CNAs) matched with new CNAs
• Training & manuals for project coordinators & mentors
• Booster training & newsletters for mentors
• Mentoring active 8 weeks• Salary increase for mentor
Growing Strong RootsEvaluation Results
• 12 nursing homes in New York state
• Statistically significant improvement in retention among those mentored – 18 point increase in average
retention rate while increase not significant among comparison group
WIN A STEP UP – Education & Payment
Incentives• 10 modules on clinical skills,
interpersonal skills, and communication• Nurse aides (NAs) get $70 per completed
module• Facilities must agree to commit staff time
& give either retention bonus ($75) or wage increase (> $0.25/hr) 3 months after completion of modules
• NAs who complete > 7 modules & stay at facility > 3 months after training get matching $75 bonus from WIN A STEP UP
WIN A STEP UPPilot Evaluation Results
• 4 nursing homes, 1 home health agency, 1 adult care home in NC
• Annual turnover rates significantly lower for NAs in the program compared to those in the matched comparison group (15% to 32%)
Wellspring – Quality Improvement & Organizational
Change • Alliance super structure• Leadership & clinical training modules• Shared advanced practice nurse• Coordinator in each facility• Care resource teams• Systematic collection & use of outcome
data• Non-hierarchical management
philosophy
WellspringEvaluation Results
• Wellspring facilities fared better than other Wisconsin facilities on retention & turnover – Wellspring CNA retention increased
by 6% while other homes decreased by 6%
– CNA turnover rates increased for both Wellspring & other homes, but increase was smaller for Wellspring
Summary – What Works?• 3 of 15 interventions using a pre-post
comparison group design had significant improvements in retention and/or turnover– Management buy in & sustained
commitment – Facilities commit to give staff time– Direct supervisors committed to working
with DCWs– Follow-up & support beyond initial training– Financial incentives to DCW in 2 of 3
interventions– Clear, consistent messages & expectations
Implications
Strengthen Evidence Base• Evaluate innovative workforce
improvement models• Examine linkages among workforce &
quality of care & life outcomes• Strengthen evaluation designs
– Measure longer-term effects– Measure variation within facilities (units,
shifts)– Measure actual behavioral outcomes– Measure outcomes consistently– Use of a comparison group
• Examine other LTC settings• Determine transferability of evidence-
based models across settings
Promote Evidence Base
• Provide technical assistance to LTC providers to implement & sustain new models– Give on-going feedback to providers
• Determine how to replicate effective interventions beyond the initial demonstration (inform technical assistance)
• Determine how to sustain interventions• “Incentivize” the use of evidence-based models
– Make the case for evidence-based workforce interventions with payors, regulators and providers
Resources
• Synthesis paper available at:http://aspe.hhs.gov/daltcp/reports/insight.pdf• Measuring Long-Term Care Work: A
Guide to Selected Instruments to Examine Direct Care Worker Experiences and Outcomes
Give me your business card for print copy





























