Embed Size (px)
Citation preview

402 Case reports
DiscussionHydrofluoric acid is commonly used in indus-try as a cleaning agent for metals and glass.'Burns resulting from contact with it maypresent early or late to the A&E department.Early presentation, with severe pain, occurswith concentrations of greater than 20%.2Burns resulting from more dilute forms of theacid may present with delayed onset of pain,erythema, and crust formation at the site of theburn. One of the characteristic features ofhydrofluoric acid burns is intense and oftendelayed pain. This may occur despite standardfirst aid treatment. The pathophysiology is saidto be the permeability of the fluoride ion,which enables it to rapidly penetrate skin, sub-cutaneous tissues, and bone. Rapid binding ofcalcium by the fluoride ion forms insolublesalts, and the ensuing drop in local tissuecalcium interferes with cellular function andcauses cell death. Cell death in turn releaseslarge amounts of potassium, which irritatesnerve endings, causing severe pain.Methods of treating these burns are aimed at
local pain control and prevention of progres-sive tissue damage. The most effective of thesehas repeatedly been shown to be the local infil-tration of calcium gluconate or application oftopical calcium carbonate to bind the fluorideion, forming an insoluble salt.'3 This removalof the free fluoride ion prevents progressive tis-sue necrosis and achieves simultaneous paincontrol. More recently, the identification ofsevere hypocalcaemia associated with fluorideloading has raised concerns over the life threat-ening, rather than limb threatening, nature ofthis injury."
Topical and local infiltration using gel orlocal injection are, however, not without prob-lems. Gel may be ineffective, particularly indelayed presentations. Local infiltration isoften found to be to exceedingly painful, andhas the added disadvantage of potential
compromise to the local circulation, possiblyrequiring concomitant fasciotomies whentreating digital burns.2 The use of local anaes-thetic infiltration is contraindicated, as the ces-sation ofpain is used as an indicator of effectivetreatment.' Intra-arterial infusion has beenadvocated, but is technically more demandingand potentially more hazardous.
Regional intravenous calcium injection using aBier's block technique satisfies all the aims ofeffective treatment of hydrofluoric acid burns.The 15 ml of 10% calcium gluconate, if releasedsuddenly, can cause flushing, headache, andarrhythmia, so we recommend the use of a dou-ble cuff tourniquet and cardiac monitoringduring the procedure. Despite these potentialproblems we feel that this amount of calcium issafe, given that there is rapid binding to fluoride.Furthermore, the risks must be balanced againstthe hazards of continued tissue destruction andthe need for adequate pain relief. Both thesepatients received rapid and complete analgesia,tissue necrosis was halted, and possible systemiceffects from either the burn or its treatment wereavoided. This procedure is technically much sim-pler and seemingly safer than intra-arterialinfusion. It is easy to perform in an A&E depart-ment when the patient first presents. Doctorsworking in A&E departments should be aware ofthis procedure, which can be used effectively totreat hydrofluoric acid burns to both upper andlower limbs.
1 Chick LR, Borah G. Calcium carbonate gel therapy forhydrofluoric acid burns of the hand. Plastic Reconstr Surg1990;86:935-9.
2 Anderson WJ, Anderson JR. Hydrofluoric acid burns of thehand: mechanism of injury and treatment. J Hand Surg1988; 13A:52-7.
3 Blunt CP. Treatment of hydrofluoric acid burns with injec-tion with calcium gluconate. Indust Med Surg 1964;33:869-71.
4 Kohnlein HE, Achinger R. A new method of treatment ofhydrofluoric acid burns of the extremities. Chir MaxillofacPlast 1982;6:297-305.
5 Sheridan RL, Ryan CM, Quinby WC, Blair J, Tomkins RG,Burke JF. Emergency management of major hydrofluoricacid burns. Burns 1995;21:62-4.
Stun gun injury
Peter Burdett-Smith
Accident andEmergency, The RoyalLiverpool UniversityHospitals, Liverpool,UKP Burdett-Smith
Correspondence to:Mr P Burdett-Smith,Consultant in A&EMedicine, The RoyalLiverpool UniversityHospitals, Prescot Street,Liverpool L7 8XP.
Accepted for publication13 June 1997
AbstractA case is presented of injury by a "stungun." The different types of electric shockdevices produced commercially are sum-marised and the potential injuries dis-cussed.(7 Accid Emerg Med 1997;14:402-404)
Keywords: stun gun; electrical burn
Case reportA 58 year old man attended the accident andemergency (A&E) department after beingattacked with what he described as a "cattle
prod" during a robbery. He described sparksbeing emitted from the device, which wasdeliberately applied to the dorsum of his righthand as he tried to defend himself. Examin-ation revealed a partial thickness electricalburn to the hand, with extensive soft tissueswelling. The wound was dressed and he wasreviewed in the clinic.
Figure 1, taken 10 days after the assault,shows the haematoma secondary to the deepsoft tissue injury. Just visible are the contactpoints of the electrodes on the skin. Thehaematoma was aspirated and the injuryresolved in four weeks.
on 23 August 2018 by guest. P
rotected by copyright.http://em
j.bmj.com
/J A
ccid Em
erg Med: first published as 10.1136/em
j.14.6.402 on 1 Novem
ber 1997. Dow
nloaded from

Case reports
DiscussionThere are three main types of device designedto (deliberately) impart an electric shock: stunguns, shock batons, and cattle prods.' Theyshare the same basic design but differ in energyoutput and potential for injury.
STUN GUNDeveloped in America in 1979, stun guns arehand held, battery operated devices, with avariety of names such as "Cosmic Defender"and "Lightning Strike." Similar in design tocattle prods, with two electrodes approximately5 cm apart, they are designed to be pressedagainst the victim's skin and an electric shock isadministered when the switch is pressed. Avariety of warning devices are incorporatedinto some models, including two furtherelectrodes placed approximately 2 cm apartand facing together, which produce visiblearcing, and lights or audible warnings to wouldbe assailants. In some models, the elec-trodes are sharp and designed to penetrate theskin.A development of this principle is the
"Taser" (Thomas A Swift's electric rifle), usedin the USA by police officers.2 This resembles alarge torch, but beneath the light source arehoused cassettes containing two darts withbarbed hooks at one end and a spool of finewire connecting them to the device proper.When the trigger is pressed, the darts are firedup to a distance of 15 feet, and are designed toembed in clothing or the skin. Pressing thetrigger activates the current, causing tetany ofthe muscles, usually causing the victim to fall.The current is effective through up to 5 cm ofclothing. After the victim has been restrained,
Figure 1 Haematoma secondary to the deep soft tissueinjury. Just visible are the contact points of the electrodes onthe skin.
the wires have to be cut, and the patient takento hospital for the darts to be removed underlocal anaesthesia. In North America they areconsidered useful weapons for dealing withpeople deranged by the effects of drugs,especially PCP (phencyclidine), as the alterna-tive method of subduing is the .38 special witha 50% mortality! It is also possible to removethe cassettes from the Taser and insert extend-ible 12 inch electrodes, allowing the instru-ment to be used as a stun gun.
ELECTRIC SHOCK BATONThis implement looks like a police baton butwith two stud electrodes at one end. These aredesigned to be pressed against the skin. Theinstrument is not designed to incapacitate, butto encourage the victim to move! A variant ofthis design is the electric "wand" which haswires wrapped around the length, and somemodels incorporate both.
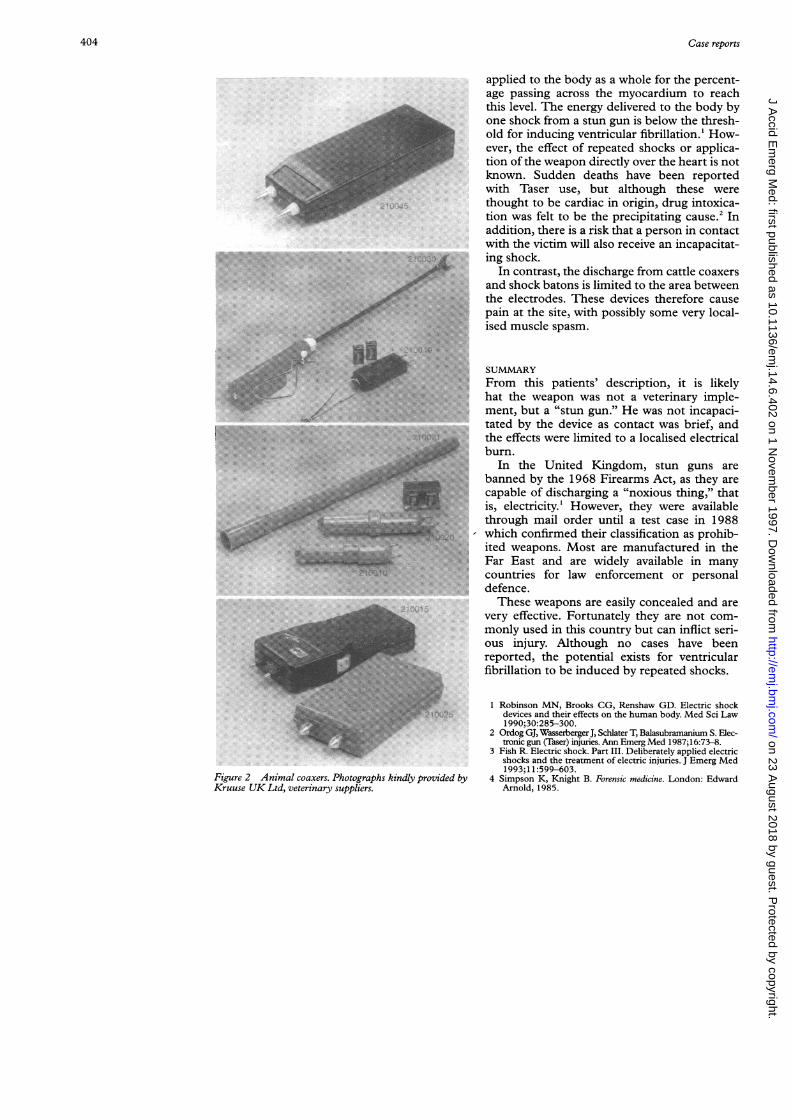
CATTLE PRODCorrectly termed animal "coaxers", thesedevices have the same basic design as the stungun but the audible and visual warnings are ofcourse unnecessary. There is a huge variety ofdesign (fig 2) and seemingly no restriction ontheir sale. As well as "coaxing," immobilisationand even anaesthesia of cattle by electricalmeans is practised in some countries, but notthe United Kingdom. These latter devices arenecessarily large and unlikely to be used asweapons against humans.
PHYSICSStun guns, including the Taser, produce a peakvoltage of up to 50 000 volts when discharged,in a series of short duration, high peak pulses,between 10 and 15 per second.3 This deliversapproximately 0.8 joules of energy. The batonsand coaxers deliver a regular alternatingcurrent, with peak voltages very much lower ataround 200 volts.'The effects of these currents on the victim
depends on the resistance of the skin, whichdepends in turn on pressure of contact,whether the skin is intact, and if it is wet. Itappears that the electrical impulse is not justlocalised to between the electrodes, but spreadsfrom the point of contact along channels of lowresistance, that is, neurovascular bundles,throughout the body. Thus a discharge ofhalf a second will repel the victim, but adischarge of one to two seconds will causetetany of most of the skeletal muscle and thevictim will fall. A discharge of three to five sec-onds will leave the victim unable to functionfor up to 15 minutes. Stiffness and pain in themuscles at the site are common after paralysishas worn off.'Concern has been expressed as to the poten-
tial for these devices to induce ventricularfibrillation. The heart may be fibrillated by thepassage of as little as 0.1 A applied for 0.5 sec-onds.4 However, a larger current needs to be
403
on 23 August 2018 by guest. P
rotected by copyright.http://em
j.bmj.com
/J A
ccid Em
erg Med: first published as 10.1136/em
j.14.6.402 on 1 Novem
ber 1997. Dow
nloaded from
404 Case reports
j~~~~~~~~~~~~~~~~~~~~~~~~~~~~~... .. ....S~~~~~~~~~~~~~~~~~~~~~~~~~~~~~...........
......''"''''....,.s:.:..
': fS.S,,: ~.
,f'~t*
S~~~~~~~~~~~~~~~~~~~~~~~5
....
..
ttI,:,zllSElS,glStl:;,.-.:.... .. ...........,,j .. ' ' '!'' E': ....~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~............. ... ... ....... ..fl;...
* ...... ..''....: ..
Figure 2 Animal coaxers. Photographs kindly provided byKruuse UK Ltd, veterinary suppliers.
applied to the body as a whole for the percent-age passing across the myocardium to reachthis level. The energy delivered to the body byone shock from a stun gun is below the thresh-old for inducing ventricular fibrillation.' How-ever, the effect of repeated shocks or applica-tion of the weapon directly over the heart is notknown. Sudden deaths have been reportedwith Taser use, but although these werethought to be cardiac in origin, drug intoxica-tion was felt to be the precipitating cause.2 Inaddition, there is a risk that a person in contactwith the victim will also receive an incapacitat-ing shock.
In contrast, the discharge from cattle coaxersand shock batons is limited to the area betweenthe electrodes. These devices therefore causepain at the site, with possibly some very local-ised muscle spasm.
SUMMARYFrom this patients' description, it is likelyhat the weapon was not a veterinary imple-ment, but a "stun gun." He was not incapaci-tated by the device as contact was brief, andthe effects were limited to a localised electricalburn.
In the United Kingdom, stun guns arebanned by the 1968 Firearms Act, as they arecapable of discharging a "noxious thing," thatis, electricity.' However, they were availablethrough mail order until a test case in 1988which confirmed their classification as prohib-ited weapons. Most are manufactured in theFar East and are widely available in manycountries for law enforcement or personaldefence.These weapons are easily concealed and are
very effective. Fortunately they are not com-monly used in this country but can inflict seri-ous injury. Although no cases have beenreported, the potential exists for ventricularfibrillation to be induced by repeated shocks.
1 Robinson MN, Brooks CG, Renshaw GD. Electric shockdevices and their effects on the human body. Med Sci Law1 990;30:285-300.
2 Ordog GJ, WasserbergerJ, Schlater T, Balasubramanium S. Elec-tronic gun (Taser) injuries. Ann Emerg Med 1987;16:73-8.
3 Fish R. Electric shock. Part III. Deliberately applied electricshocks and the treatment of electric injuries. J Emerg Med1993;1 1:599-603.
4 Simpson K, Knight B. Forensic medicine. London: EdwardArnold, 1985.
on 23 August 2018 by guest. P
rotected by copyright.http://em
j.bmj.com
/J A
ccid Em
erg Med: first published as 10.1136/em
j.14.6.402 on 1 Novem
ber 1997. Dow
nloaded from





























