Embed Size (px)
Citation preview

Innovation to InstitutionalizationNewborn Care in India
(2001-2010)
CARE-India’s experiences
Mukesh KumarProgram Director, CARE India

Objective• Integration of key-family practices for prevention
and timely management of neo-natal and childhood illnesses into existing national programs
• Appropriate and accessible care and information about prevention and management of neonatal and childhood illnesses from community-based service providers
• Better partnership between health facilities and the communities
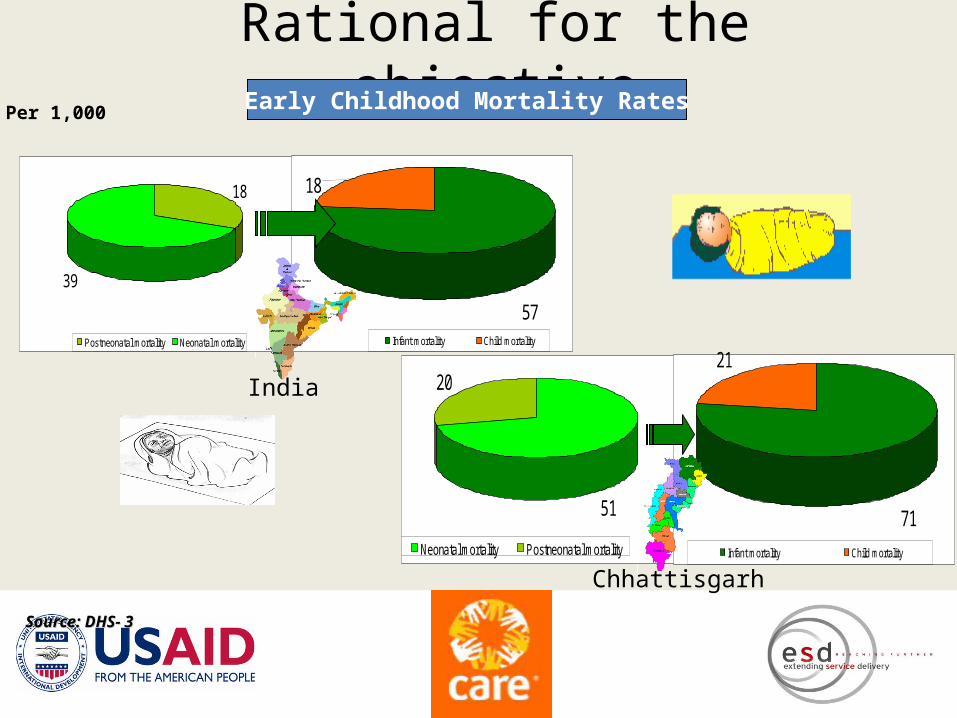
Rational for the objective
71
21
Infant mortality Child mortality
20
51
Neonatal mortality Postneonatal mortality
Per 1,000
Source: DHS- 3Source: DHS- 3
Early Childhood Mortality Rates
57
18
Infant mortality Child mortality
18
39
Postneonatal mortality Neonatal mortality
India
Chhattisgarh
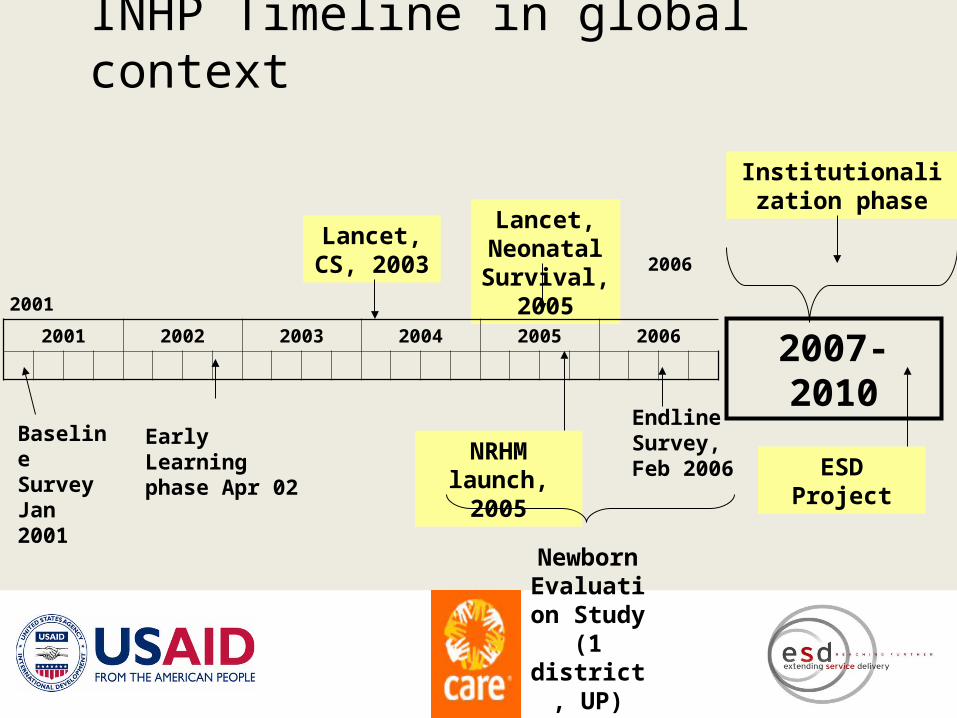
INHP Timeline in global context
Baseline Survey Jan 2001
Endline Survey, Feb 2006
2001
2006
Lancet, CS, 2003
Lancet, Neonatal Survival,
2005
NRHM launch, 2005
Newborn Evaluation Study
(1 district,
UP)
Early Learning phase Apr 02
2001 2002 2003 2004 2005 2006
Institutionalization phase
2007-2010
ESD Project
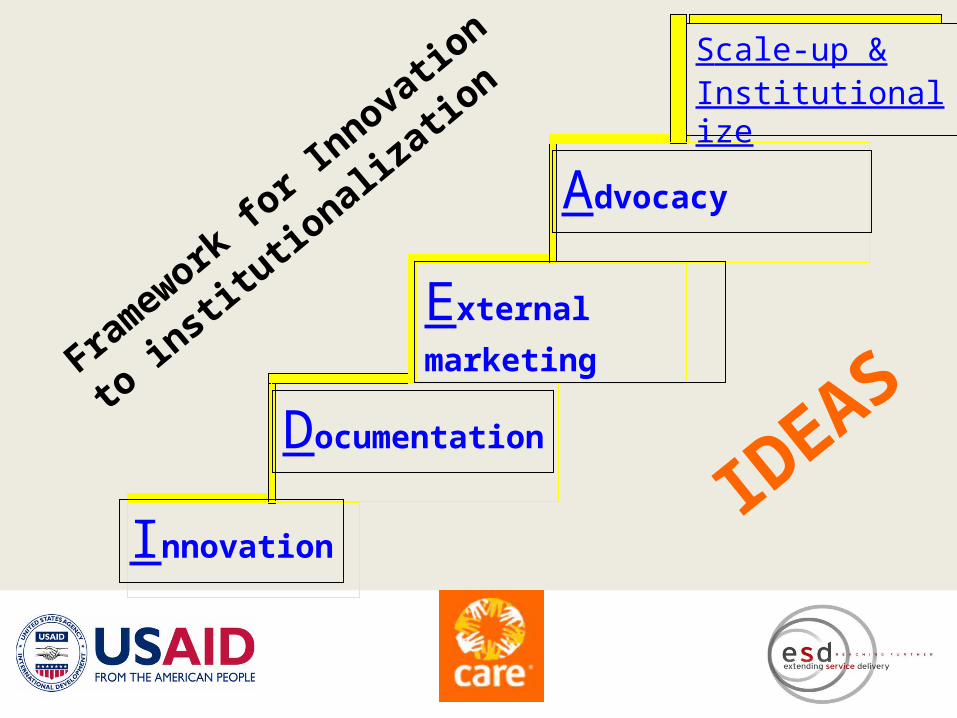
Innovation
Documentation
External marketing
Advocacy
Scale-up & Institutionalize
Fram
ework
for I
nnovatio
n
to in
stitu
tional
izat
ion
IDEAS

Early learning Sites( 150 Villages across eight
states)
Demonstration sites- Approx. 10,000 villages
Key Interventions Promoted
• Tetanus Toxoid along with basic ANC for mothers.• Essential home-based newborn care:
Clean delivery, cord care, handling Adequate thermal care (warmth) Early and exclusive breastfeeding
• Early recognition of and extra care for the weak (premature/LBW) newborn.
• Recognition and referral of sick newborn
Scale up phase
Project universe = 95,000 AWC, 747 blocks, 78 districts, 9 states, 100 m + population
Modifications
– Did pilot test the intervention package with the help of ICDS and RCH functionaries in ‘early learning sites’.
– Referral of sick and weak neonates were promoted only if there were health facilities
Program Approaches to Promote NBC
Home visits and advice by AWW, ANM, Volunteers with emphasis on: Late pregnancy, first day, first week Family, not just the mother Immediate care at birth Recognition of preterm / LBW at birth, marked for
extra careHome visit planner for AWW and close supervisionSupplemented by varied BCC and community-based monitoring efforts
What did CARE do?
• Facilitation and catalysis:– Capacity building: ICDS, RCH, volunteers,
community bodies– System strengthening: functional
convergence, Supportive supervision (ICDS) – Behavior Change Communication
• Advocacy:– Prioritizing neonatal care– Measuring and Monitoring

Progress made
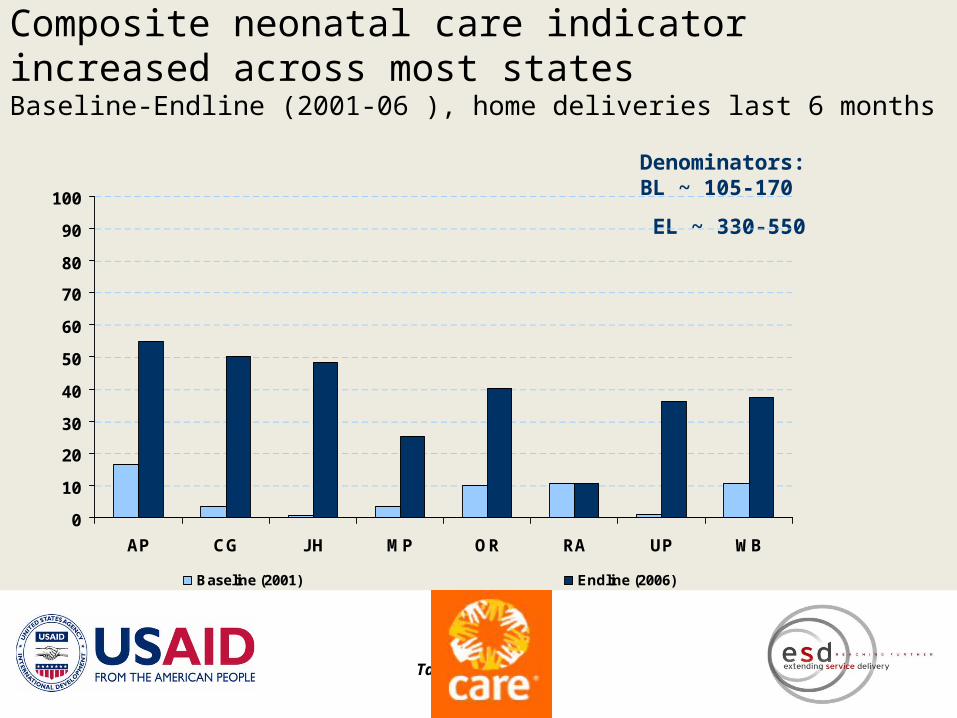
Composite neonatal care indicator increased across most statesBaseline-Endline (2001-06 ), home deliveries last 6 months
Table 3.1
Denominators: BL ~ 105-170
EL ~ 330-550
0
10
20
30
40
50
60
70
80
90
100
AP CG JH MP OR RA UP WB
Baseline (2001) Endline (2006)

Factors that possibly influenced change
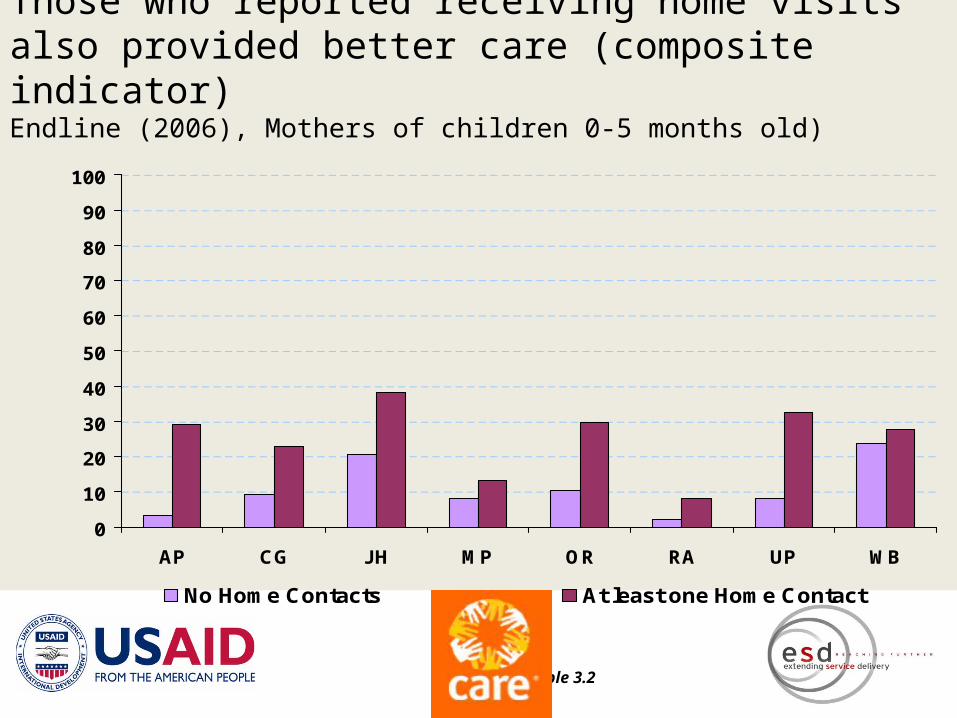
Those who reported receiving home visits also provided better care (composite indicator)Endline (2006), Mothers of children 0-5 months old)
Table 3.2
0
10
20
30
40
50
60
70
80
90
100
AP CG JH MP OR RA UP WB
No Home Contacts At least one Home Contact
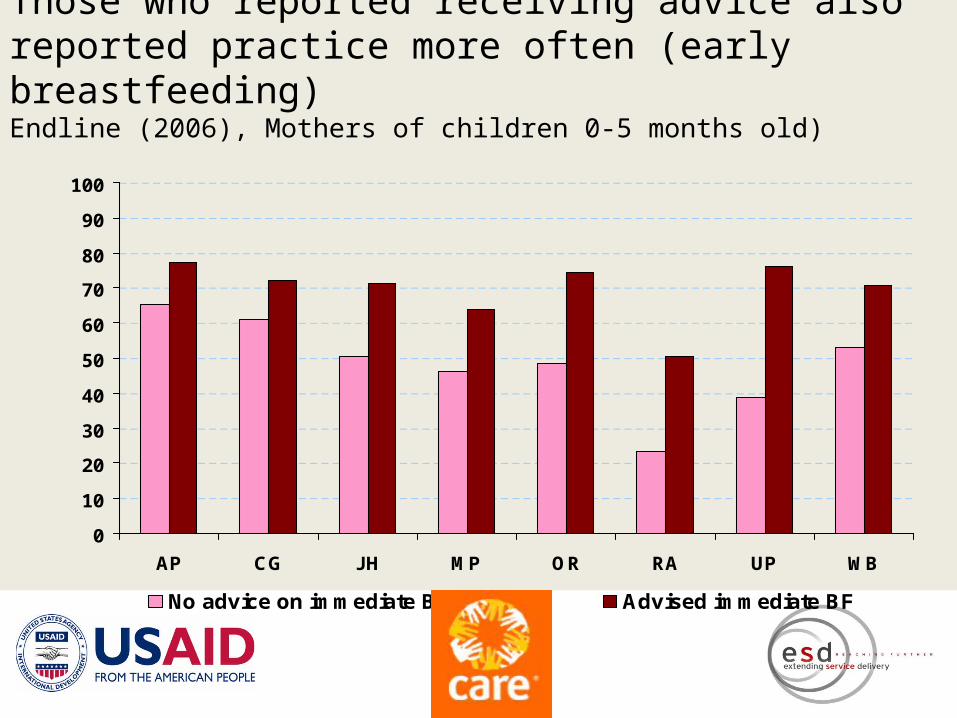
Those who reported receiving advice also reported practice more often (early breastfeeding)Endline (2006), Mothers of children 0-5 months old)
Table 3.2
0
10
20
30
40
50
60
70
80
90
100
AP CG JH MP OR RA UP WB
No advice on immediate BF Advised immediate BF
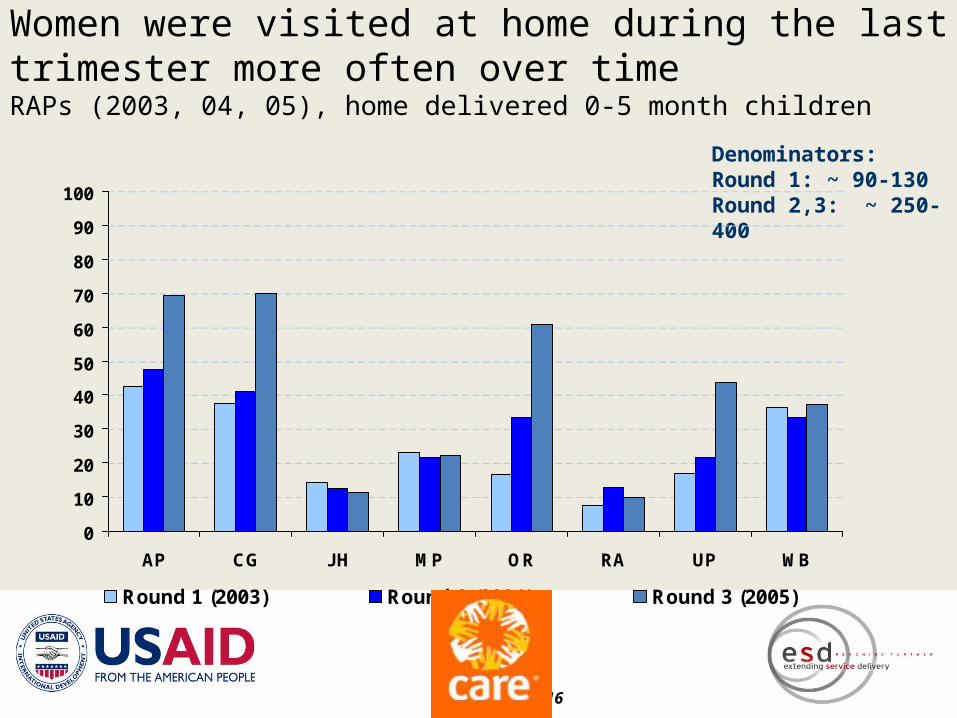
Women were visited at home during the last trimester more often over timeRAPs (2003, 04, 05), home delivered 0-5 month children
Figure 3.16
Denominators: Round 1: ~ 90-130 Round 2,3: ~ 250-400
0
10
20
30
40
50
60
70
80
90
100
AP CG JH MP OR RA UP WB
Round 1 (2003) Round 2 (2004) Round 3 (2005)
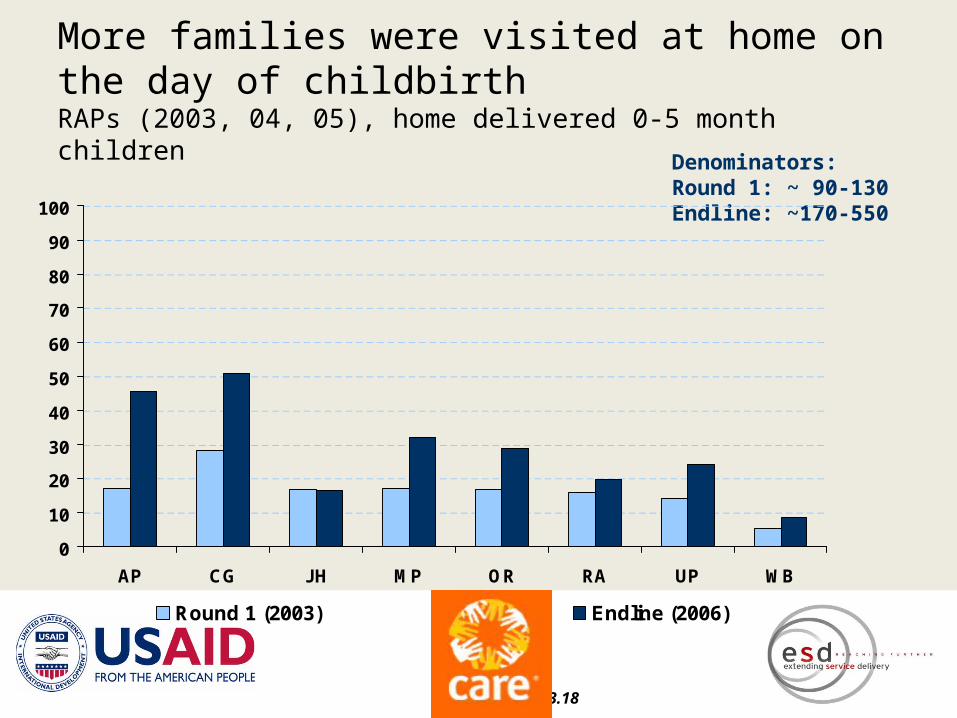
More families were visited at home on the day of childbirthRAPs (2003, 04, 05), home delivered 0-5 month children
Figure 3.17, 3.18
Denominators: Round 1: ~ 90-130 Endline: ~170-550
0
10
20
30
40
50
60
70
80
90
100
AP CG JH MP OR RA UP WB
Round 1 (2003) Endline (2006)
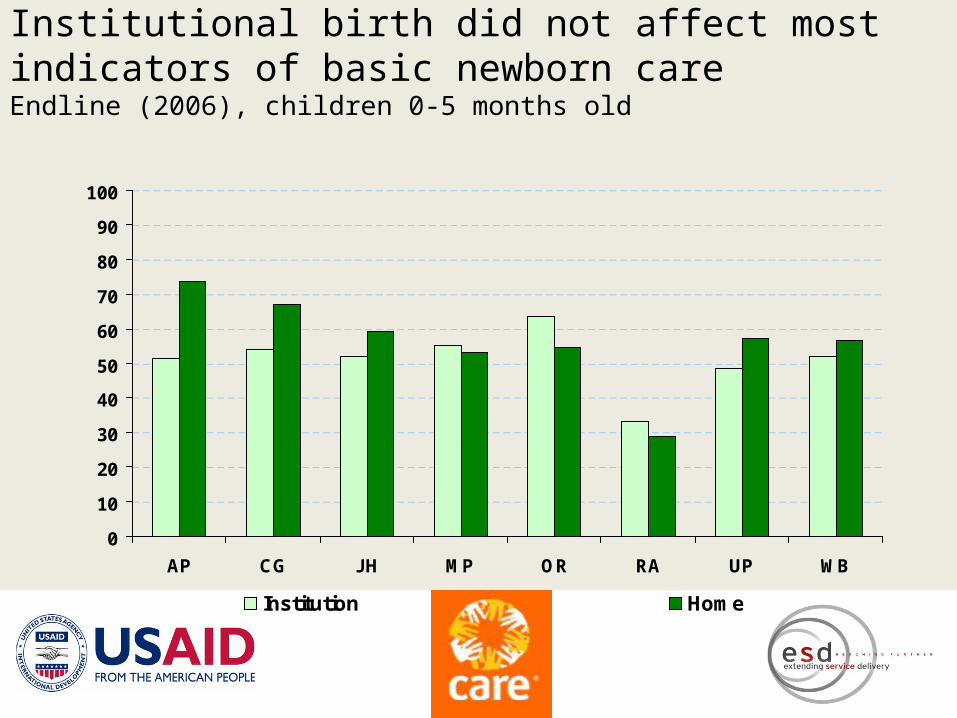
Institutional birth did not affect most indicators of basic newborn careEndline (2006), children 0-5 months old
Figure 3.14
0
10
20
30
40
50
60
70
80
90
100
AP CG JH MP OR RA UP WB
Institution Home
Institutionalization phase(2007-2010)
ESD project started in Chhattisgarh to institutionalize best practices through IMNCI program of Govt. of India
Total Districts: 16Blocks : 168AWCs : 33000
Chhattishgarh
Activities
Capacity Building of ICDS state, district and project level program leaders was done through ongoing forums and structured CB events.
Different communication materials (leaflets/booklets /modules) developed and distributed in close collaboration with state resource center, department of women and child development.
Communication Campaign organized through multi-media channels & structured home contacts by AWW / ANM / Volunteers.
Mainstreaming C-IMNCI & HTSP into ICDS / RCH program at district & state level through PIP development process and Kuposan Mukti Abhiyan (state sponsored malnutrition eradication drive)
Institutionalization– Incorporating C-IMNCI components into the training
modules for Supervisors and Outreach workers jointly developed with SRC.
– Undertook training of key ICDS functionaries in collaboration with W & CD
– Incorporated the key messages into website developed for the department
– District level advocacy efforts undertaken for discussion of key components during ongoing forums
Challenges– Programming in civil unrest areas
– Varied capacities of outreach workers
– Competing priorities of health department
– Engagement of AWWs / ICDS block functionaries time for back to back training

Lessons
What does this imply?
1. Current programs can deliver
• The changes were brought about by ICDS and RCH staff
• Change was brought about in “difficult” states and districts
• Efforts were multi-dimensional: all other services continued
• What worked was probably:– Focus on effective interventions– Strengthening accountability mechanisms –
internal, external
2. Can ICDS continue to contribute to neonatal care?• It can, and must:
– ICDS has a mandate for addressing mortality
– Basic neonatal care is simple– AWW is available to the community– AWW has greater credibility than ASHA– AWW is backed by a mature, well-defined
support structure– AWW has proven she can deliver
3. Let us do what is doable
• More aggressive interventions have yet to be shown to be scalable
• Basic care must be scaled up until more effective ones are available
• Much needs to be done, and time is slipping by….