Embed Size (px)
Citation preview
Innovations in nebulized delivery
John Pritchard
Why nebulise ?
• Technical
– Easy to formulate
– Dose > 2mg to lung
– API is highly soluble
• hygroscopicity
– Drugs not easily micronised
– Early clinical trials
• Target patient groups
– Very poor lung function
– Acute exacerbation
– Very young or very old patients
– Not reliant on breathing technique
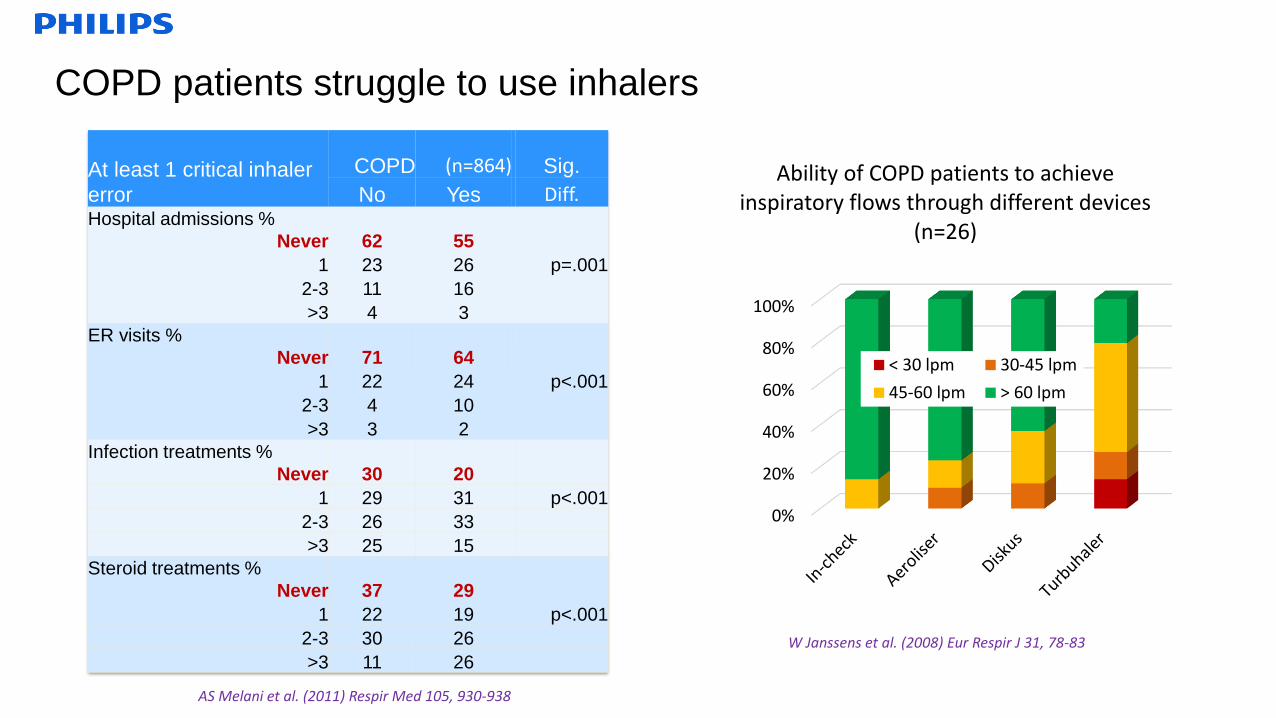
COPD patients struggle to use inhalers
At least 1 critical inhaler
error
COPD (n=864) Sig.
No Yes Diff.Hospital admissions %
Never 62 55
1 23 26 p=.001
2-3 11 16
>3 4 3
ER visits %
Never 71 64
1 22 24 p<.001
2-3 4 10
>3 3 2
Infection treatments %
Never 30 20
1 29 31 p<.001
2-3 26 33
>3 25 15
Steroid treatments %
Never 37 29
1 22 19 p<.001
2-3 30 26
>3 11 26
AS Melani et al. (2011) Respir Med 105, 930-938
W Janssens et al. (2008) Eur Respir J 31, 78-83
0%
20%
40%
60%
80%
100%
Ability of COPD patients to achieve inspiratory flows through different devices
(n=26)
< 30 lpm 30-45 lpm
45-60 lpm > 60 lpm
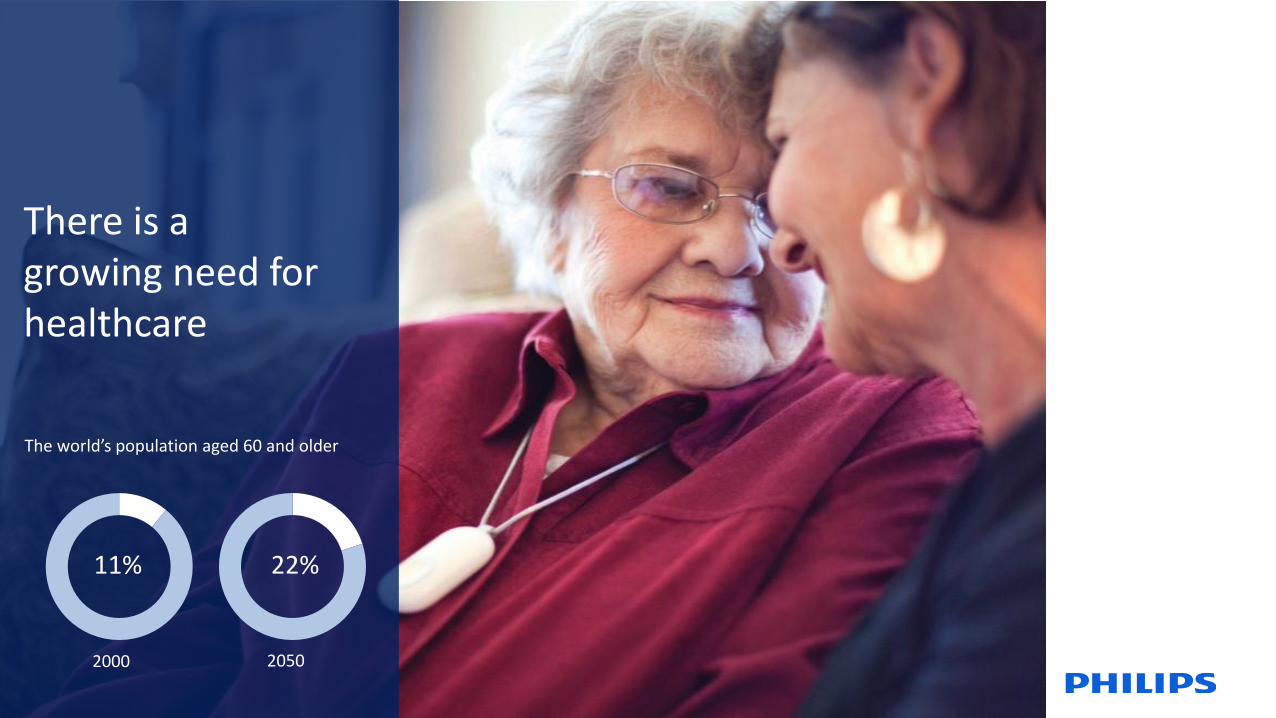
There is a growing need for healthcare
The world’s population aged 60 and older
2000 2050
11% 22%
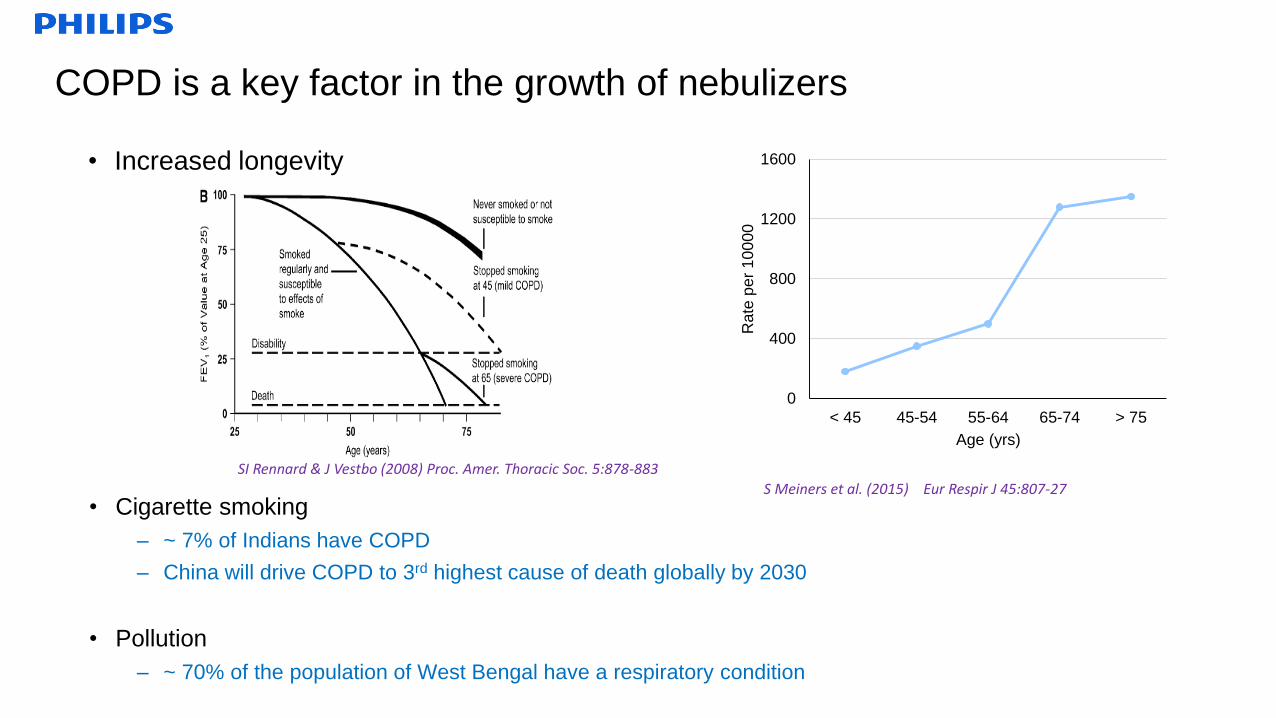
COPD is a key factor in the growth of nebulizers
• Increased longevity
• Cigarette smoking
– ~ 7% of Indians have COPD
– China will drive COPD to 3rd highest cause of death globally by 2030
• Pollution
– ~ 70% of the population of West Bengal have a respiratory condition
SI Rennard & J Vestbo (2008) Proc. Amer. Thoracic Soc. 5:878-883
0
400
800
1200
1600
< 45 45-54 55-64 65-74 > 75
Rate
pe
r 1
00
00
Age (yrs)
S Meiners et al. (2015) Eur Respir J 45:807-27
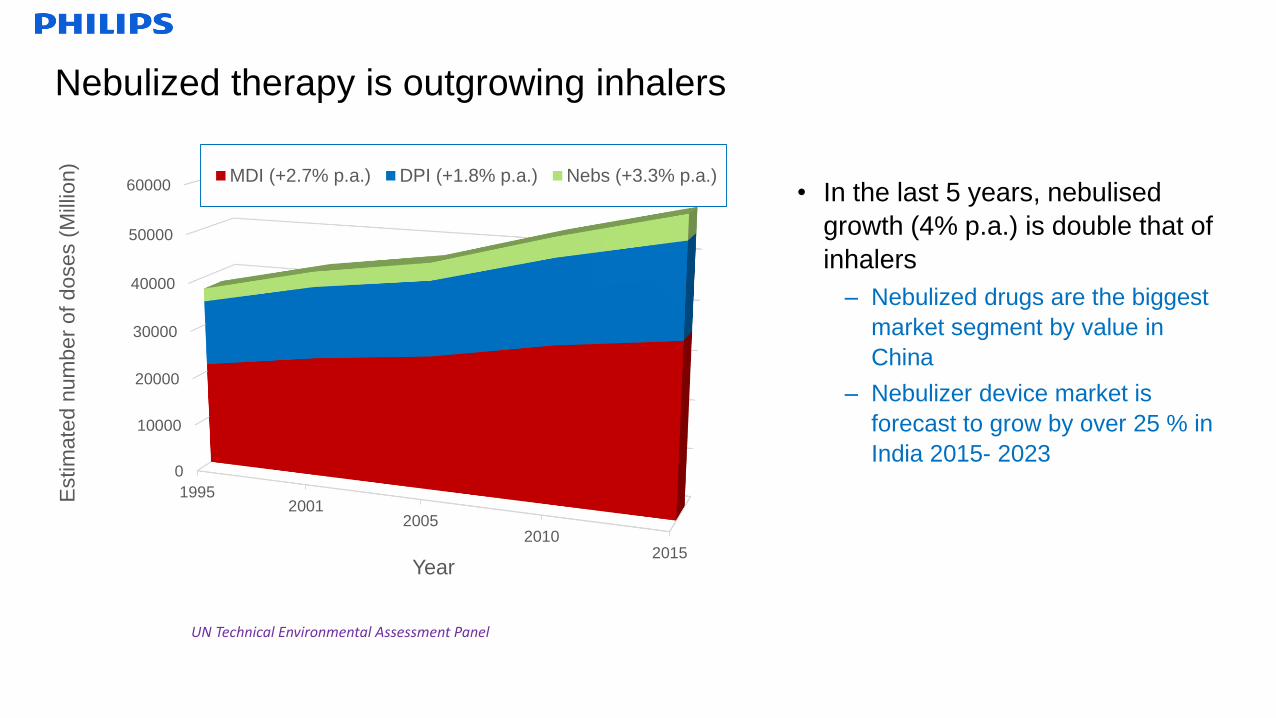
Nebulized therapy is outgrowing inhalers
• In the last 5 years, nebulised
growth (4% p.a.) is double that of
inhalers
– Nebulized drugs are the biggest
market segment by value in
China
– Nebulizer device market is
forecast to grow by over 25 % in
India 2015- 20230
10000
20000
30000
40000
50000
60000
19952001
20052010
2015
Estim
ate
d n
um
be
r of doses (
Mill
ion)
Year
MDI (+2.7% p.a.) DPI (+1.8% p.a.) Nebs (+3.3% p.a.)
UN Technical Environmental Assessment Panel
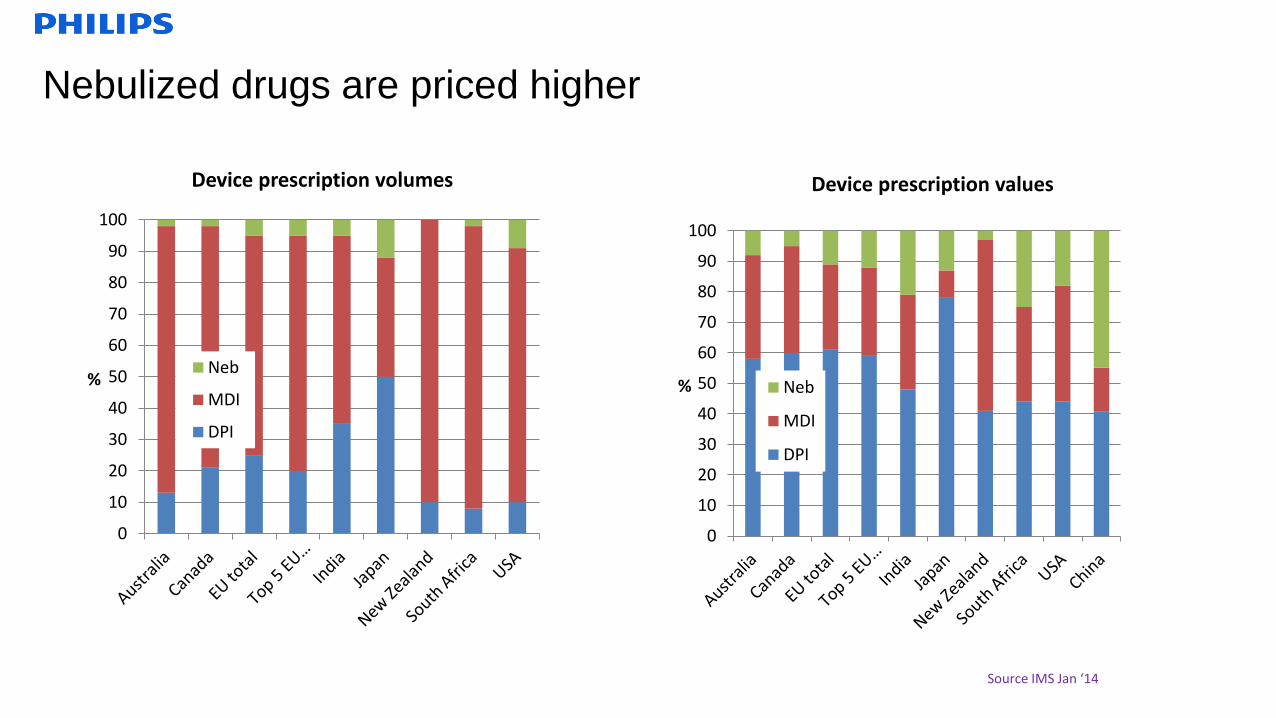
Nebulized drugs are priced higher
0
10
20
30
40
50
60
70
80
90
100
%
Device prescription volumes
Neb
MDI
DPI
Source IMS Jan ‘14
0
10
20
30
40
50
60
70
80
90
100
%
Device prescription values
Neb
MDI
DPI
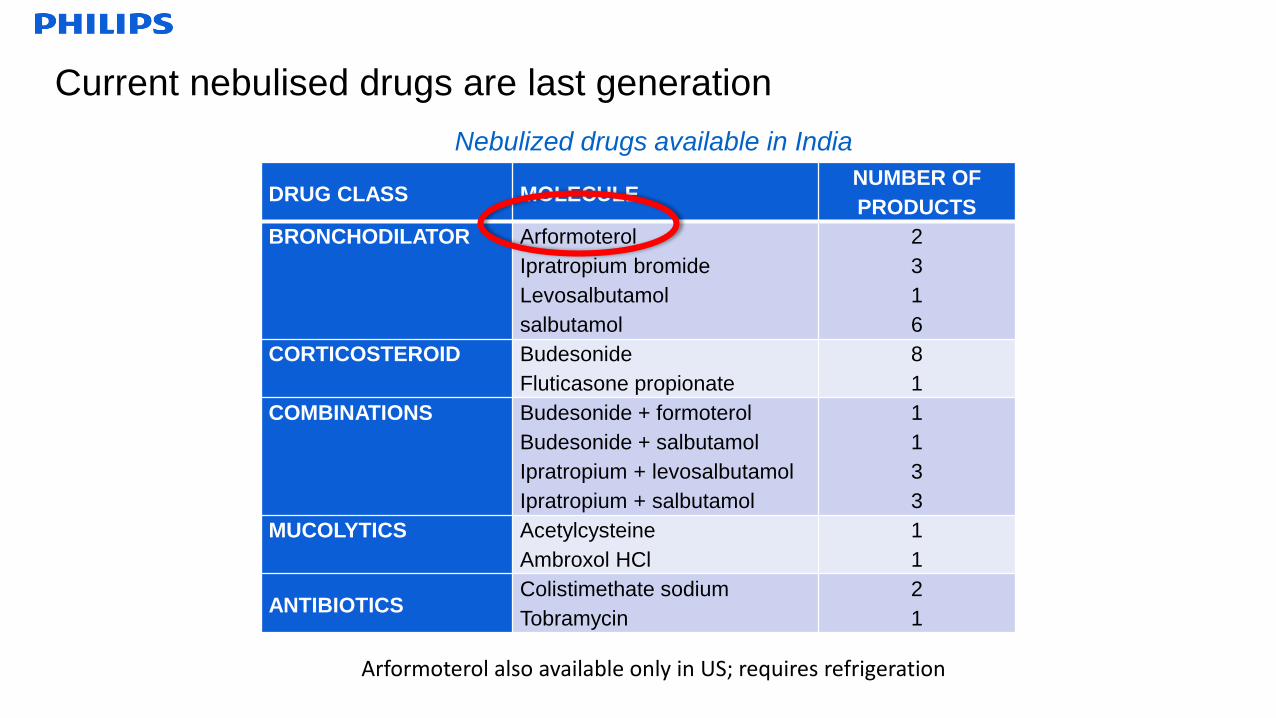
Current nebulised drugs are last generation
Nebulized drugs available in India
DRUG CLASS MOLECULENUMBER OF
PRODUCTS
BRONCHODILATOR Arformoterol
Ipratropium bromide
Levosalbutamol
salbutamol
2
3
1
6
CORTICOSTEROID Budesonide
Fluticasone propionate
8
1
COMBINATIONS Budesonide + formoterol
Budesonide + salbutamol
Ipratropium + levosalbutamol
Ipratropium + salbutamol
1
1
3
3
MUCOLYTICS Acetylcysteine
Ambroxol HCl
1
1
ANTIBIOTICSColistimethate sodium
Tobramycin
2
1
Arformoterol also available only in US; requires refrigeration
2
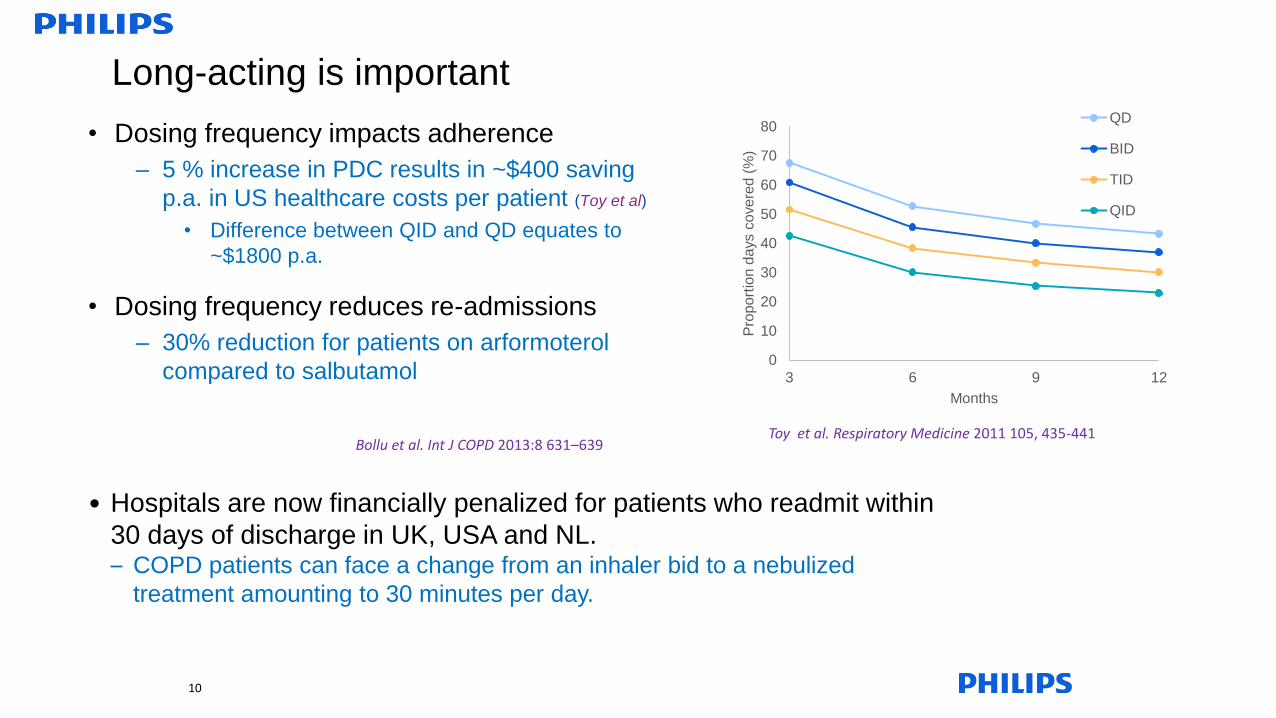
Long-acting is important
210
0
10
20
30
40
50
60
70
80
3 6 9 12
Pro
po
rtio
n d
ays c
ove
red
(%
)
Months
QD
BID
TID
QID
Toy et al. Respiratory Medicine 2011 105, 435-441Bollu et al. Int J COPD 2013:8 631–639
• Hospitals are now financially penalized for patients who readmit within
30 days of discharge in UK, USA and NL.– COPD patients can face a change from an inhaler bid to a nebulized
treatment amounting to 30 minutes per day.
• Dosing frequency impacts adherence
– 5 % increase in PDC results in ~$400 saving
p.a. in US healthcare costs per patient (Toy et al)
• Difference between QID and QD equates to
~$1800 p.a.
• Dosing frequency reduces re-admissions
– 30% reduction for patients on arformoterol
compared to salbutamol
2
There is no shortage of new drugs !
• Within the next couple of years, from major pharma companies there will be at least:
– 7 LAMA, 5 LABA, 7 ICS, 12 LABA/ICS, 5 LABA/LAMA
– Only ~ 1/3 in MDI format
• There are many more products being developed in growth markets
– Cipla offer 28 different products in over 100 countries including LABA/LAMA/ICS
• Few companies have addressed the nebulized segment
a) Develop a new molecule
b) Change the development paradigm
c) “Beyond the inhaler”
11
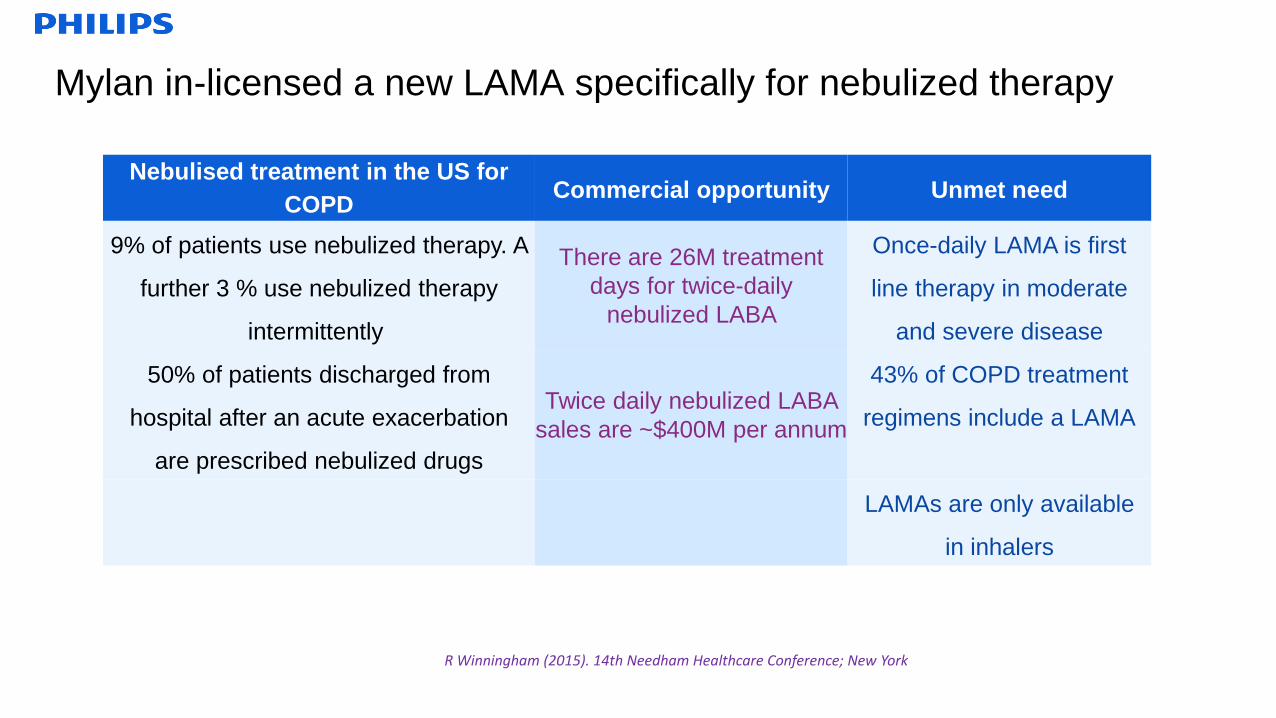
Mylan in-licensed a new LAMA specifically for nebulized therapy
Nebulised treatment in the US for
COPDCommercial opportunity Unmet need
9% of patients use nebulized therapy. A
further 3 % use nebulized therapy
intermittently
There are 26M treatment
days for twice-daily
nebulized LABA
Once-daily LAMA is first
line therapy in moderate
and severe disease
50% of patients discharged from
hospital after an acute exacerbation
are prescribed nebulized drugs
Twice daily nebulized LABA
sales are ~$400M per annum
43% of COPD treatment
regimens include a LAMA
LAMAs are only available
in inhalers
R Winningham (2015). 14th Needham Healthcare Conference; New York
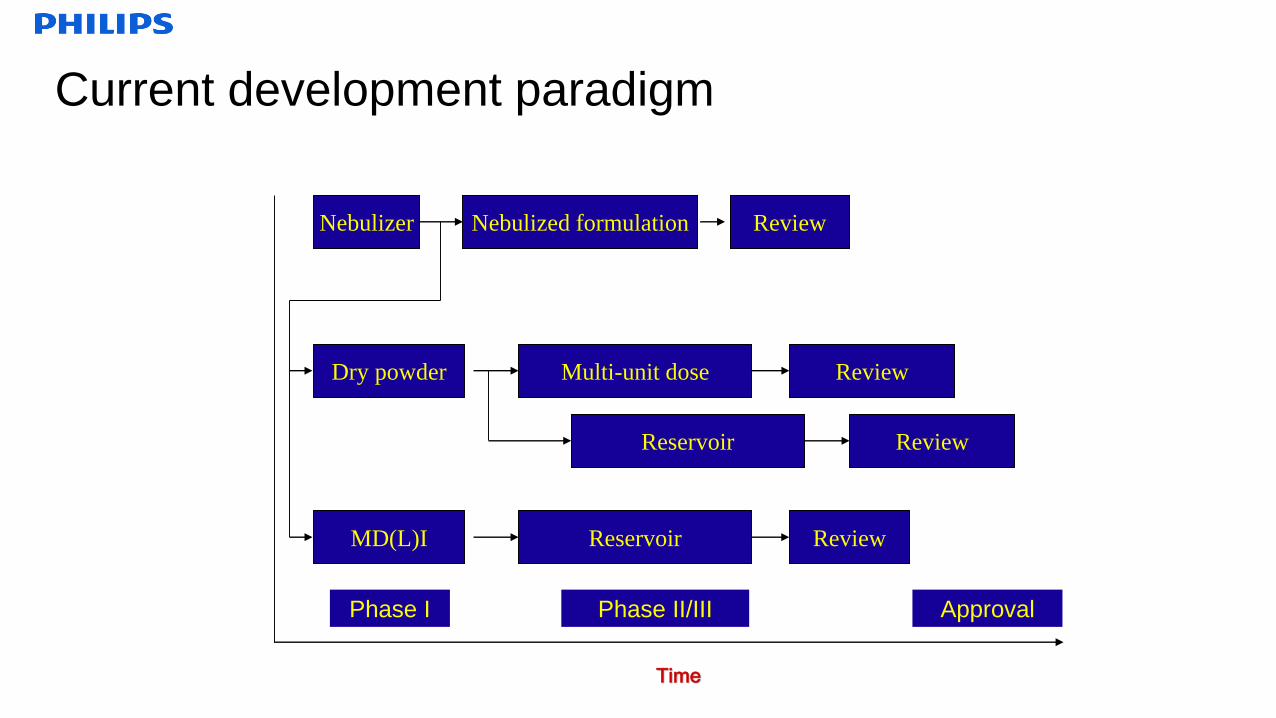
Current development paradigm
Time
Nebulizer
MD(L)I
Dry powder
Phase I ApprovalPhase II/III
ReviewNebulized formulation
Multi-unit dose Review
Reservoir Review
ReviewReservoir
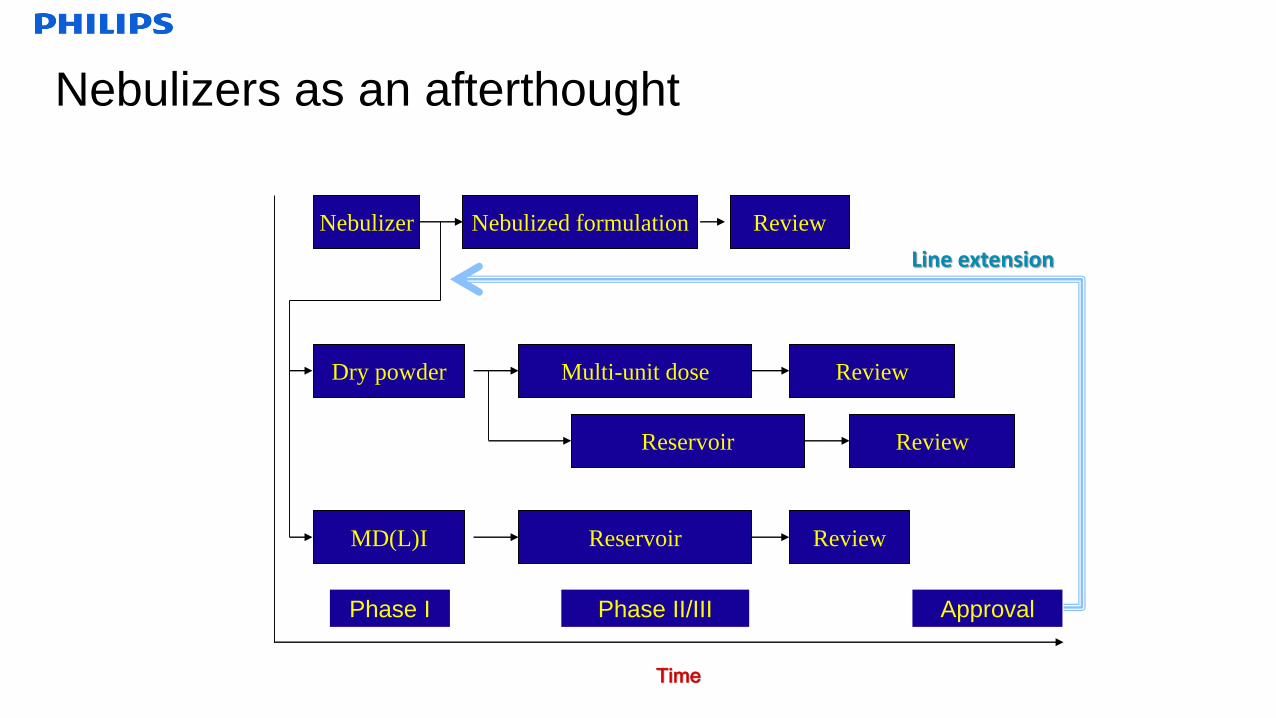
Nebulizers as an afterthought
Time
Nebulizer
MD(L)I
Dry powder
Phase I ApprovalPhase II/III
ReviewNebulized formulation
Multi-unit dose Review
Reservoir Review
ReviewReservoir
Line extension
Challenging the paradigm
• 8 % of respiratory drugs entering SAD/MAD get to market– Requires an inhaler to have already been developed
– Wastes significant development resource on compounds that fail in the clinic Delay formulation development until after PoC would avoid 12 FTE over 3 years and 10-20 kg of
drug substance
– However, would also delay launch by 2 years at a potential loss of sales of $1 Bn pa
– For compounds that do reach the market, it is often too late to start a nebulizer development before
patent expiry
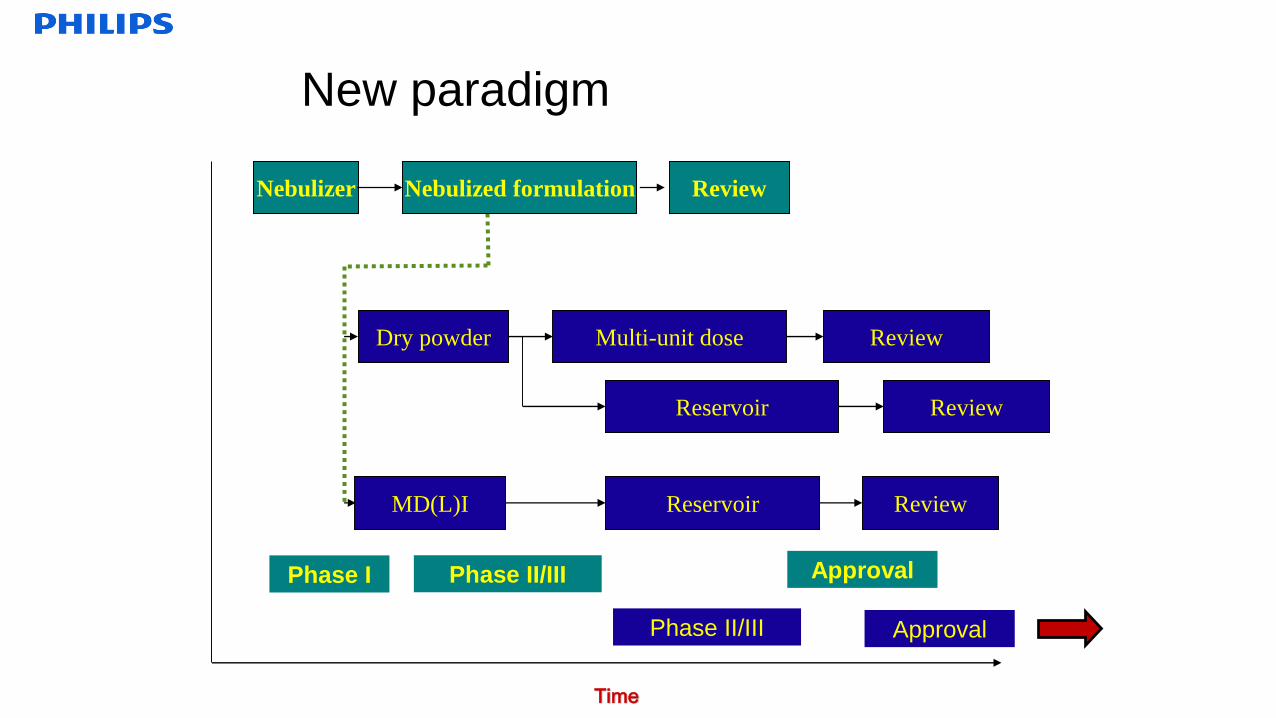
New paradigm
Time
Nebulizer
MD(L)I
Dry powder
Phase I ApprovalPhase II/III
ReviewNebulized formulation
Multi-unit dose Review
Reservoir Review
ReviewReservoir
Phase II/III Approval
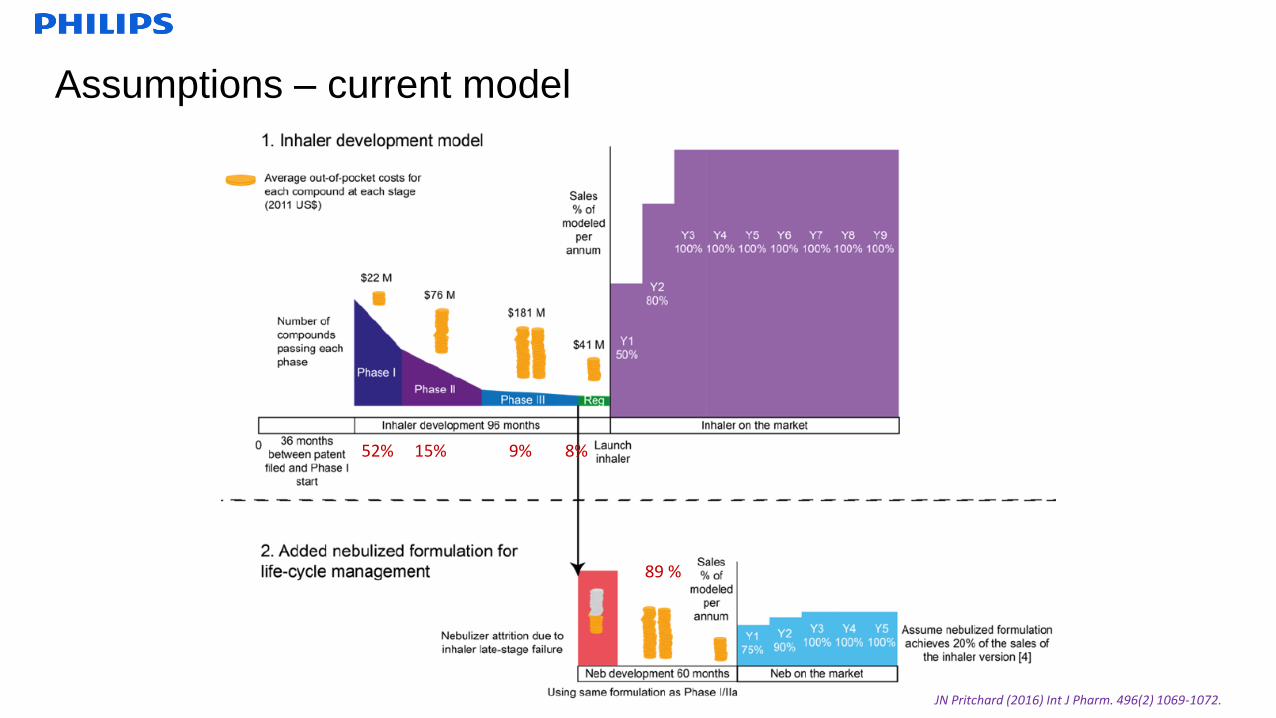
Assumptions – current model
JN Pritchard (2016) Int J Pharm. 496(2) 1069-1072.
52% 15% 9% 8%
89 %
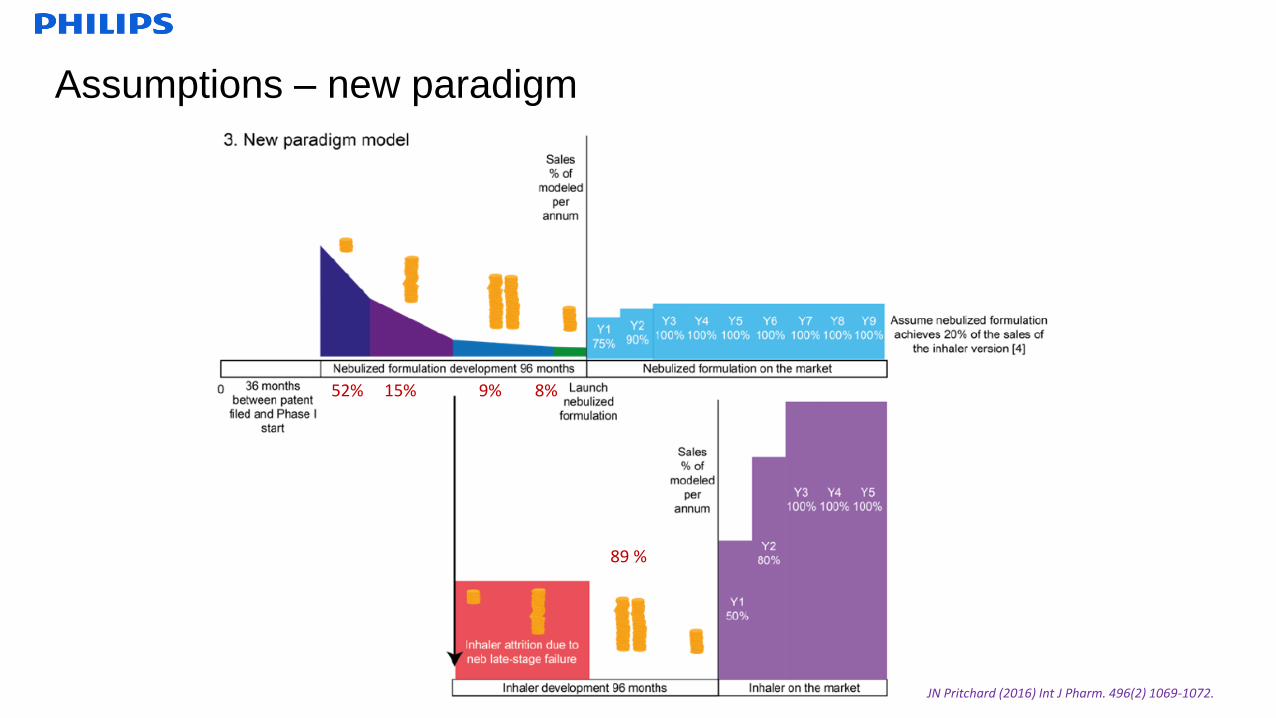
Assumptions – new paradigm
JN Pritchard (2016) Int J Pharm. 496(2) 1069-1072.
52% 15% 9% 8%
89 %
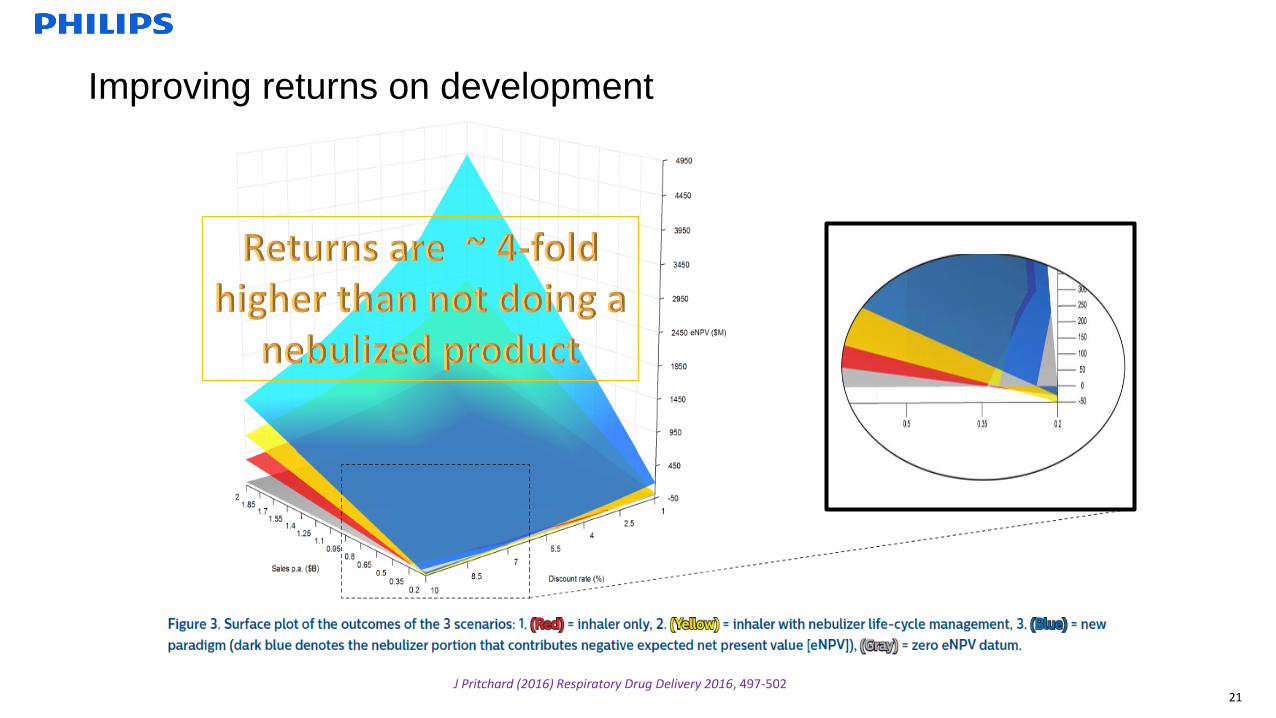
21J Pritchard (2016) Respiratory Drug Delivery 2016, 497-502
Improving returns on development
Changing the paradigm - to realise the value of nebulized drugs
• 8 % of respiratory drugs entering SAD/MAD get to market– Requires an inhaler to have already been developed
– Wastes significant development resource on compounds that fail in the clinic Delay formulation development until after PoC would avoid 12 FTE over 3 years and 10-20 kg of
drug substance
– However, would also delay launch by 2 years at a potential loss of sales of $1 Bn pa
– For compounds that do reach the market, it is often too late to start a nebulizer development before
patent expiry
Pritchard Int J Pharm 2015, 496:1069–72
• Take the FTIM nebulised formulation right through to market
– Treats the severe patients Underserved today
Most consuming of healthcare resource
• Financial penalties for readmission following exacerbation
Easiest to demonstrate efficacy and pharmacoeconomic benefit
– Improves bottom line ~ $8M saved in development costs (@4*PhI) & ~ $7M increased sales profit p.a.
.... but from a historic perspective
• Cost of Goods– Device
• US: minimum $ 30, typically $ 100, eFlow $ 1500, iNeb $ 3000
• India: range from $15 to > $1000
– Delivery efficiency can be poor if not breath-actuated
• Variable performance from different nebulisers– Multiple devices need to be covered during clinical programme
– Device specific registration and promotion
• Restricted formulary
– Increased sales and marketing costs
• Hardware is not patient-friendly– Transportation, cleanliness (microbiology), delivery time
– Pharmaceutical discharge to the environment
– Maintenance
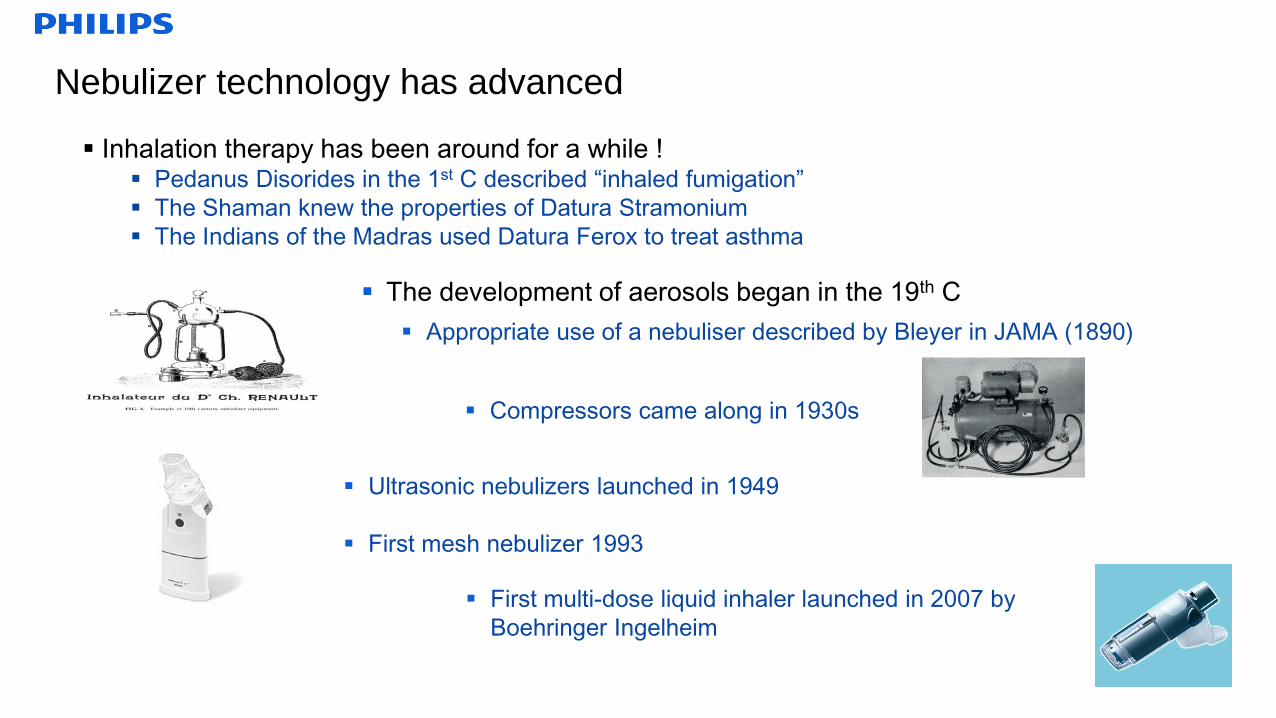
The development of aerosols began in the 19th C
Appropriate use of a nebuliser described by Bleyer in JAMA (1890)
Nebulizer technology has advanced
Inhalation therapy has been around for a while ! Pedanus Disorides in the 1st C described “inhaled fumigation”
The Shaman knew the properties of Datura Stramonium
The Indians of the Madras used Datura Ferox to treat asthma
Compressors came along in 1930s
Ultrasonic nebulizers launched in 1949
First mesh nebulizer 1993
First multi-dose liquid inhaler launched in 2007 by
Boehringer Ingelheim
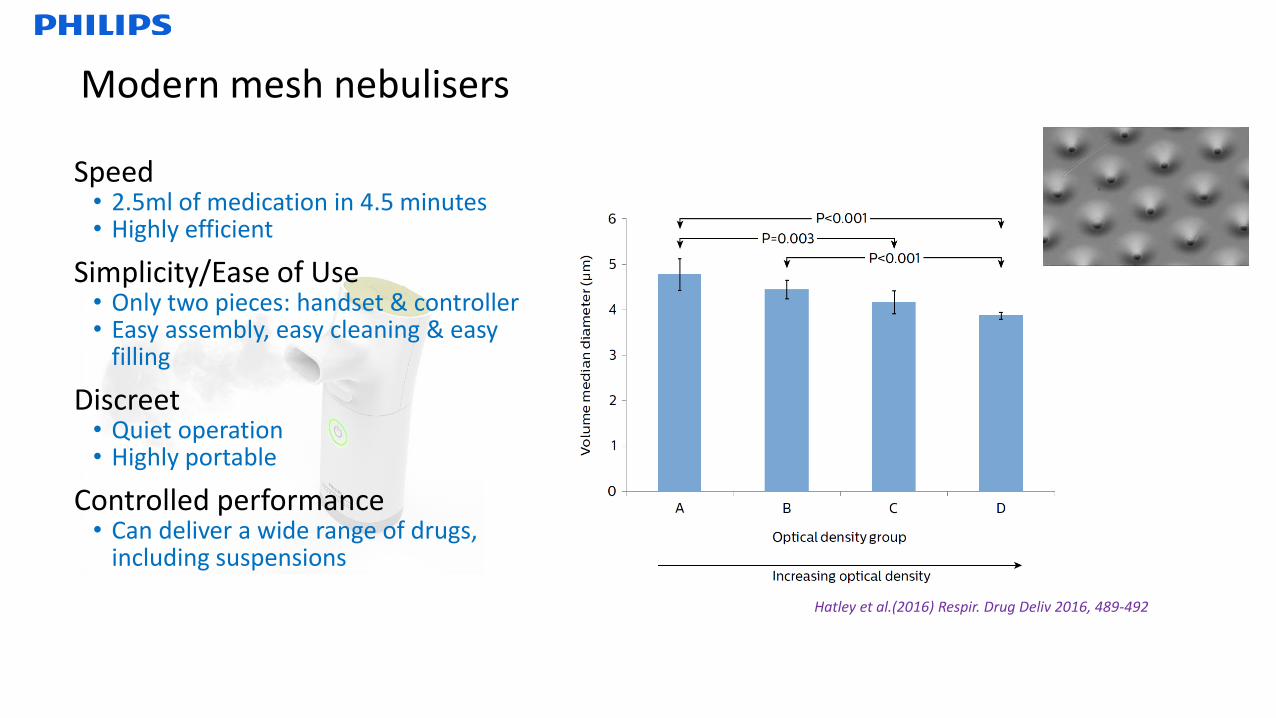
Modern mesh nebulisers
Hatley et al.(2016) Respir. Drug Deliv 2016, 489-492
Speed• 2.5ml of medication in 4.5 minutes • Highly efficient
Simplicity/Ease of Use• Only two pieces: handset & controller • Easy assembly, easy cleaning & easy
filling
Discreet• Quiet operation • Highly portable
Controlled performance• Can deliver a wide range of drugs,
including suspensions
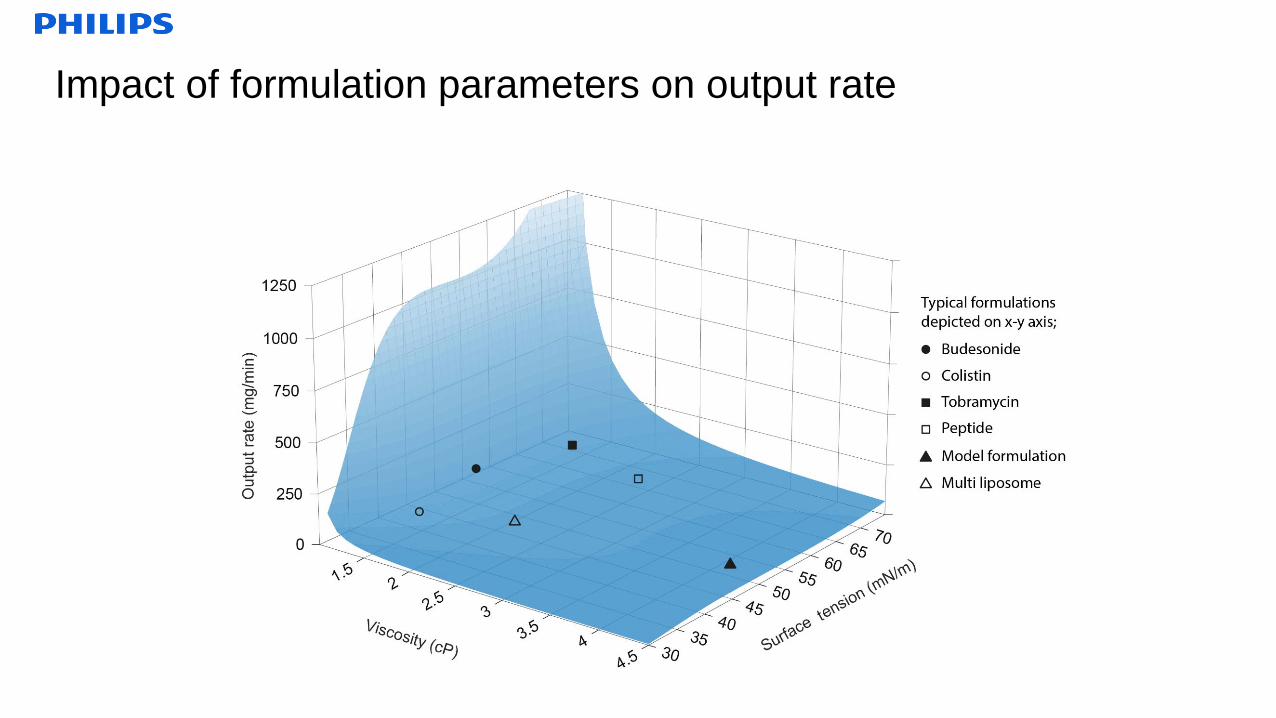
Impact of formulation parameters on output rate
10
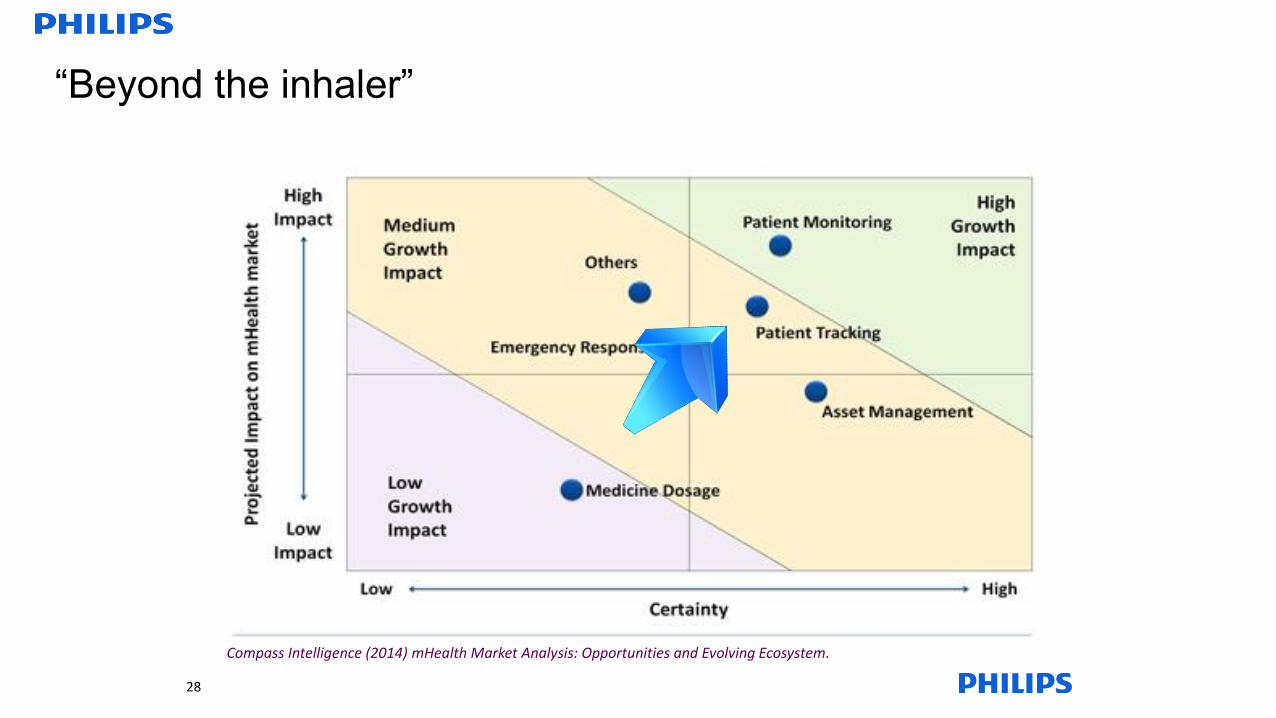
“Beyond the inhaler”
Compass Intelligence (2014) mHealth Market Analysis: Opportunities and Evolving Ecosystem.
28
Device Training Sustaining
Match inhaler to
patient
Use the patient’s
“language”
Electronic
instruction
Forgiving of poor
technique
Check inspiratory
manoeuvre
Check adherence and
reminders
16
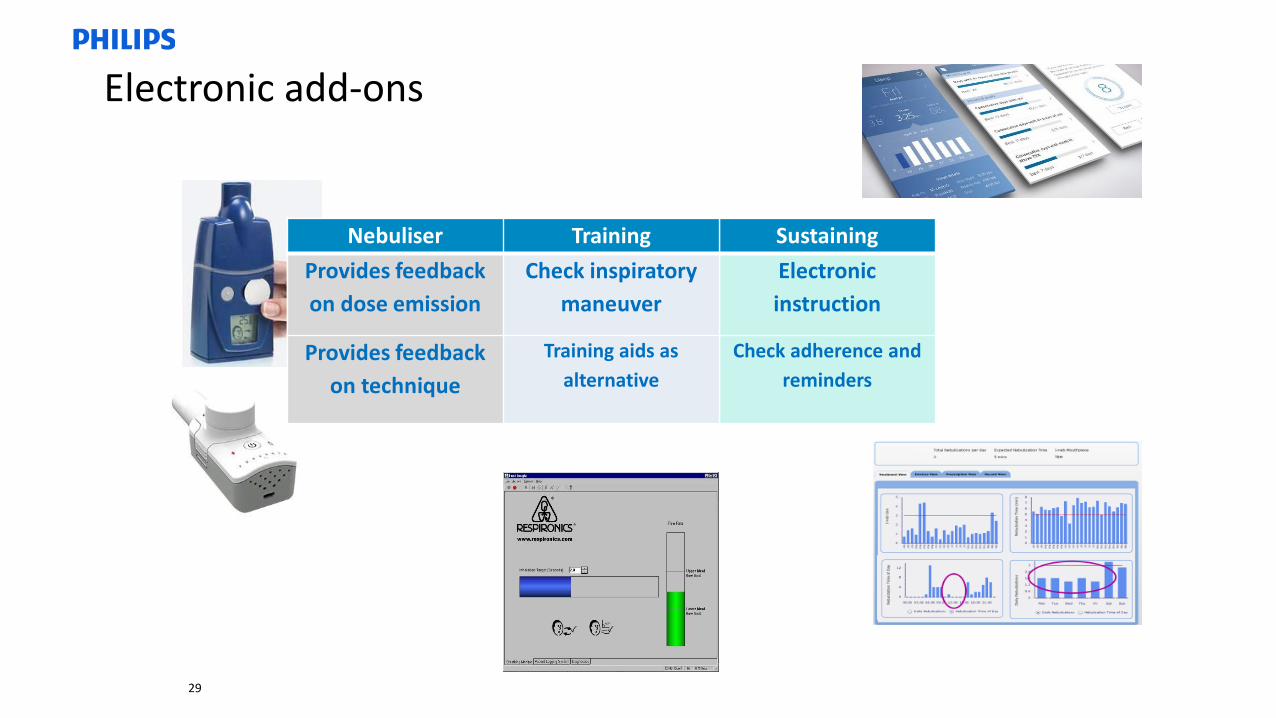
Electronic add-ons
Nebuliser
Provides feedback
on dose emission
Provides feedback
on technique
Nebuliser Training
Provides feedback
on dose emission
Check inspiratory
maneuver
Provides feedback
on technique
Training aids as
alternative
29
Redressing the drawbacks
• Delivery inefficiency
– Breath-actuation
– Low residual volume
• HeteroHomogeneous performance from different nebulisers
– Now regarded as drug-device combinations, other than for well-characterized, prescribed drugs
which have had prior approval from CDER eg. Salbutamol, ipratropium bromide, sodium
cromoglycate.
• For the review of the device component, a manufacturer may either submit a “device module” as component of the
NDA or IND or submit a separate 510(k).
– Tighter controls on device performance
• Hardware is not patient-friendly
– Battery-powered devices
– Simple construction
– Short treatment times
– Low maintenance
– Adherence management
.
Summary
• Despite drawbacks in performance, the
nebulizer drug market has outgrown the
inhaler market, and is currently growing faster
• Driven by Asian markets and by COPD
increasing
• There is a lack of long-acting drugs available
in nebulized form
• Bring the nebulized version to market first to
avoid missing the opportunity
• The technology has advanced
• Look “beyond the inhaler” to provide additional
protection
N B U R






























