Embed Size (px)
Citation preview
Jonathan E. Efron, MD, FACS, FASCRS The Mark M Ravitch, MD Endowed Professorship in Surgery Chief of the Ravitch Division Associate Professor of Surgery Johns Hopkins University
Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond
Overview • Current Standard of Care
– Staging – Neoadjuvant Therapy – Technique
• MIS techniques • TEM/TAMMIS • Robotic Approach • Watch and Wait
Staging Determine extent of local
disease • History and physical exam
– pain • Digital rectal examination • Vaginal examination • Endoscopy • Imaging Studies
Imaging of Body
• CT Abdomen/Pelvis/Chest • CXR • MRI • US • ? PET scan
Current Neoadjuvant Recommendations in United States
• T3, NO or any T, N1 or 2 • Middle or Distal Rectum • Circumferential Margin • Long Course Therapy • Surgery 8-10 weeks
– Possibly 12 weeks
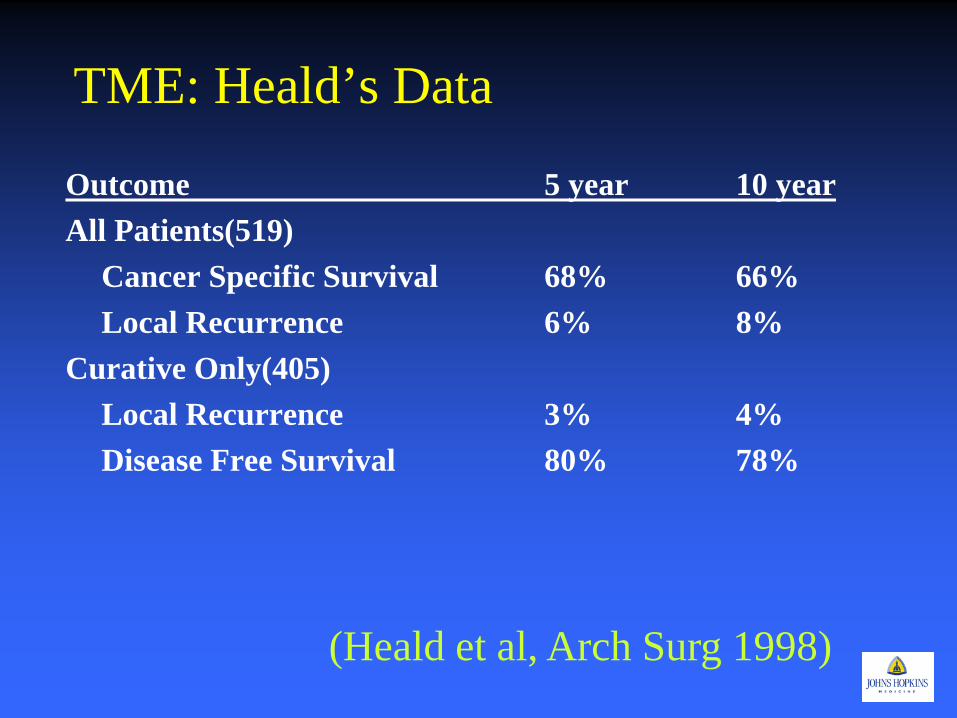
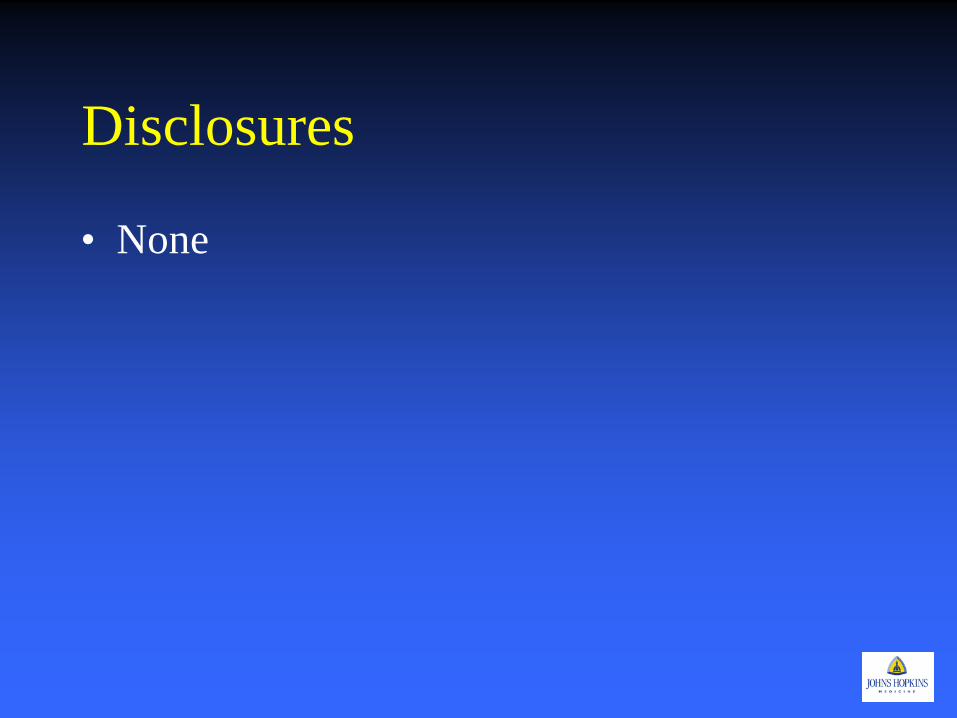
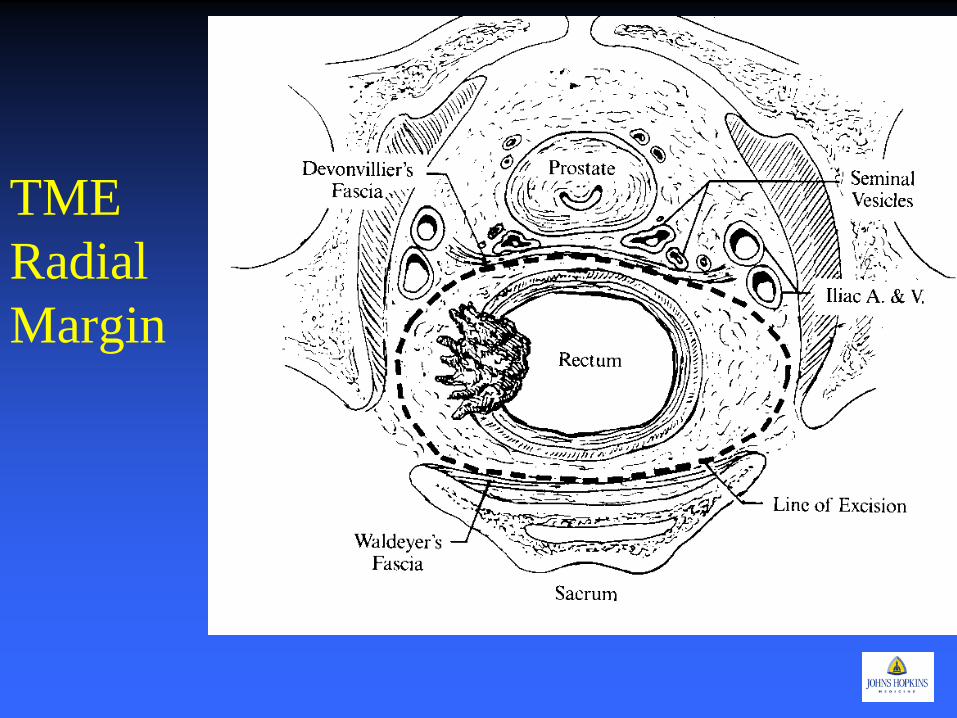
TME: Heald’s Data
Outcome 5 year 10 year All Patients(519) Cancer Specific Survival 68% 66% Local Recurrence 6% 8% Curative Only(405) Local Recurrence 3% 4% Disease Free Survival 80% 78%
(Heald et al, Arch Surg 1998)

Open TME Series: Local Recurrence
Author # series # patients Local recurrence rates
Wibe et al (NCR*) N/A 3516 6.4%LAR; 8.2% APR Ridgeway/Darzi 13 6058 6.6% Colquoun et al. 7 5%-9%
* Norwegian Cancer Registry (Gordon and Nivatvongs. Principles and Practice of Surgery for the Colon, Rectum, and Anus 3rd ed. 2007: 695.)
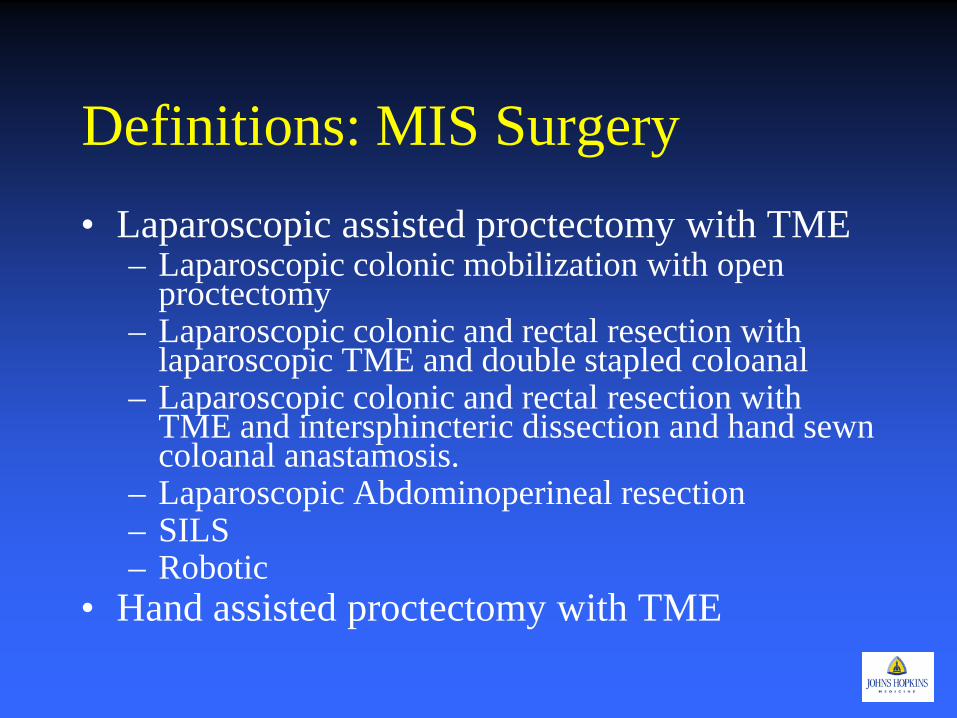
Definitions: MIS Surgery • Laparoscopic assisted proctectomy with TME
– Laparoscopic colonic mobilization with open proctectomy
– Laparoscopic colonic and rectal resection with laparoscopic TME and double stapled coloanal
– Laparoscopic colonic and rectal resection with TME and intersphincteric dissection and hand sewn coloanal anastamosis.
– Laparoscopic Abdominoperineal resection – SILS – Robotic
• Hand assisted proctectomy with TME
Measures of Quality and Outcome
• Short Term Complications – Mortality – Morbidity
• Pathological Assessment – TME specimen, circumferential margins – Lymph nodes
• Long Term Complications • Recurrence • Survival
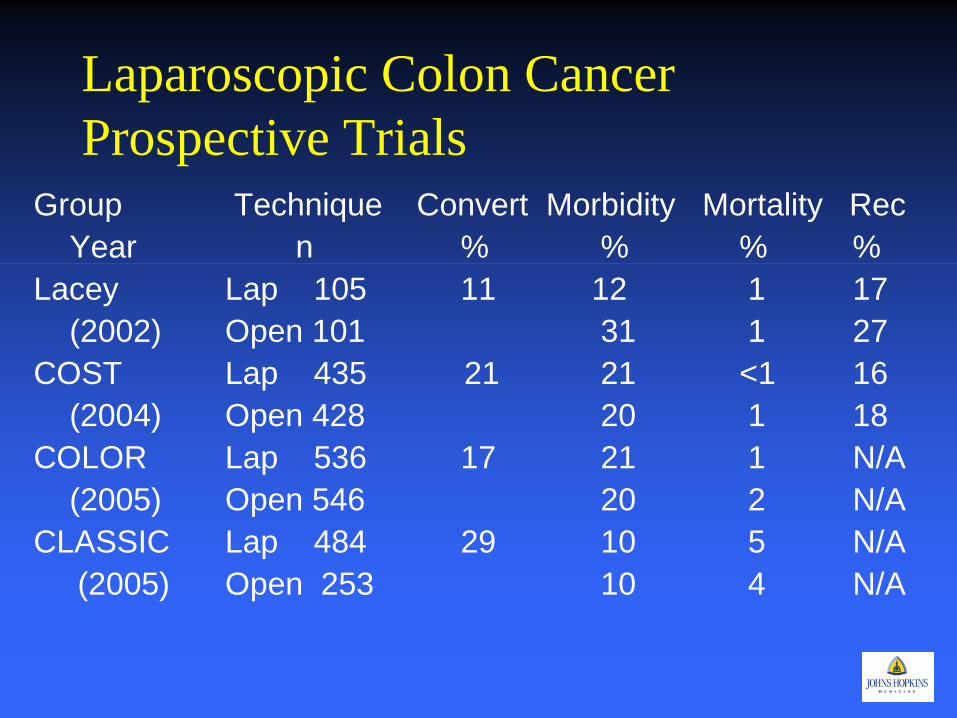
Laparoscopic Colon Cancer Prospective Trials
Group Technique Convert Morbidity Mortality Rec Year n % % % % Lacey Lap 105 11 12 1 17 (2002) Open 101 31 1 27 COST Lap 435 21 21 <1 16 (2004) Open 428 20 1 18 COLOR Lap 536 17 21 1 N/A (2005) Open 546 20 2 N/A CLASSIC Lap 484 29 10 5 N/A (2005) Open 253 10 4 N/A
MIS Surgery for Rectal Cancer
• Is MIS Total Mesorectal Excision possible? • How does the physiology of
pnuemoperitoneum and laparoscopic surgery effect the tumor biology? – It Doesn’t
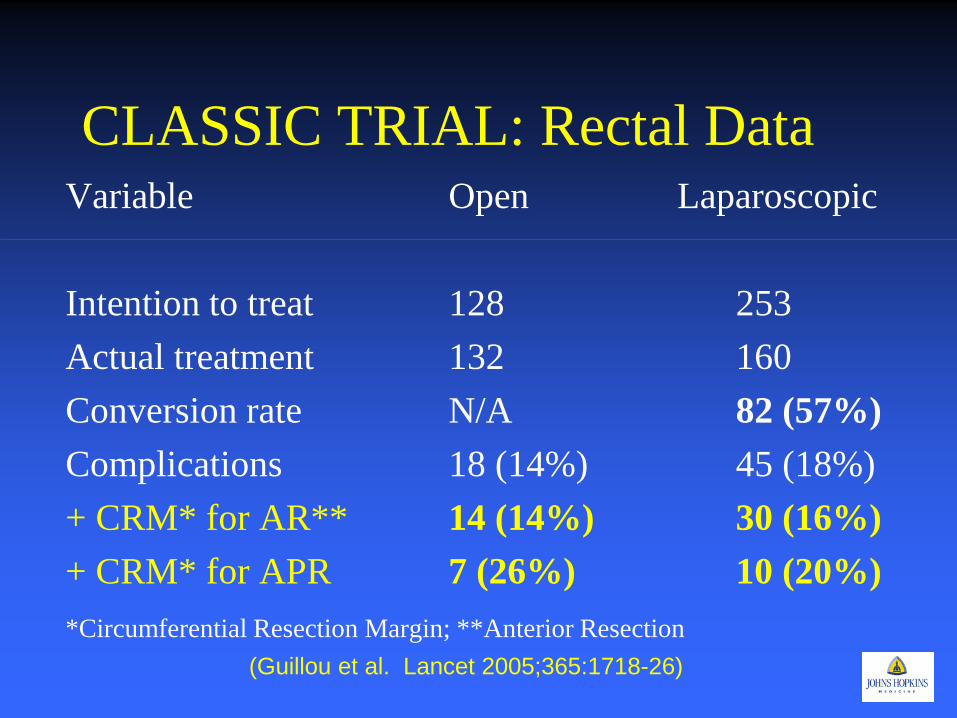
CLASSIC TRIAL: Rectal Data Variable Open Laparoscopic Intention to treat 128 253 Actual treatment 132 160 Conversion rate N/A 82 (57%) Complications 18 (14%) 45 (18%) + CRM* for AR** 14 (14%) 30 (16%) + CRM* for APR 7 (26%) 10 (20%) *Circumferential Resection Margin; **Anterior Resection (Guillou et al. Lancet 2005;365:1718-26)
CLASSIC Trial: Long Term Outcomes
• 3 year results • 794 patients (526 laparoscopic; 268 open) • NO difference in 3 year survival • Differences in Survival
– Overall survival: 1.8% – Disease free Survival: -1.4% – Local recurrence: -0.8%
(Jayne et al. J Clin Oncol 2007;25(21):3061-8)
Randomized trial comparing lap and open surgery in patients with Rectal cancer
• 204 patients – Mid and low rectal cancers – Stage II and III – 103 laparoscopic – 101 open
• Blood loss: – > for open surgery
• Return of GI function and discharge: • Quicker in lap group • Complications and circumferential margins:
– no difference • Number of lymph nodes
– > in lap group • NO difference:
– Local recurrence – Overall survival – Disease free survival
(Valero et al. Br J Surg 2009;96(9): 982-9)
Cochrane Review: Laparoscopic versus open total mesorectal excision for rectal cancer
• Search from Jan 1990-Dec 2005 • 80 studies total; 48 included • 4224 patients • 3 grade 1b studies (individual randomized trials) • 12 grade 2b studies (individual cohort studies) • 5 grade 3b studies (case control studies) • 28 grade 4 studies (case series) • Only one randomized control trial with 3 and 5
year follow up. (Breukink et al Cochrane Database System Rev. 2006 (4):CD005200)
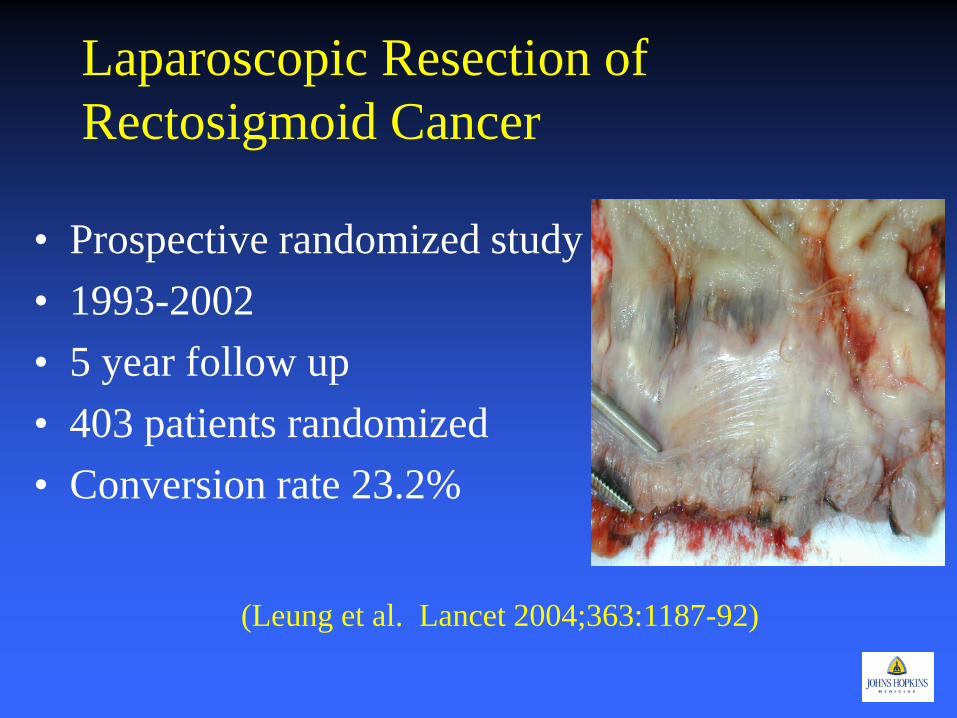
Laparoscopic Resection of Rectosigmoid Cancer
• Prospective randomized study • 1993-2002 • 5 year follow up • 403 patients randomized • Conversion rate 23.2%
(Leung et al. Lancet 2004;363:1187-92)
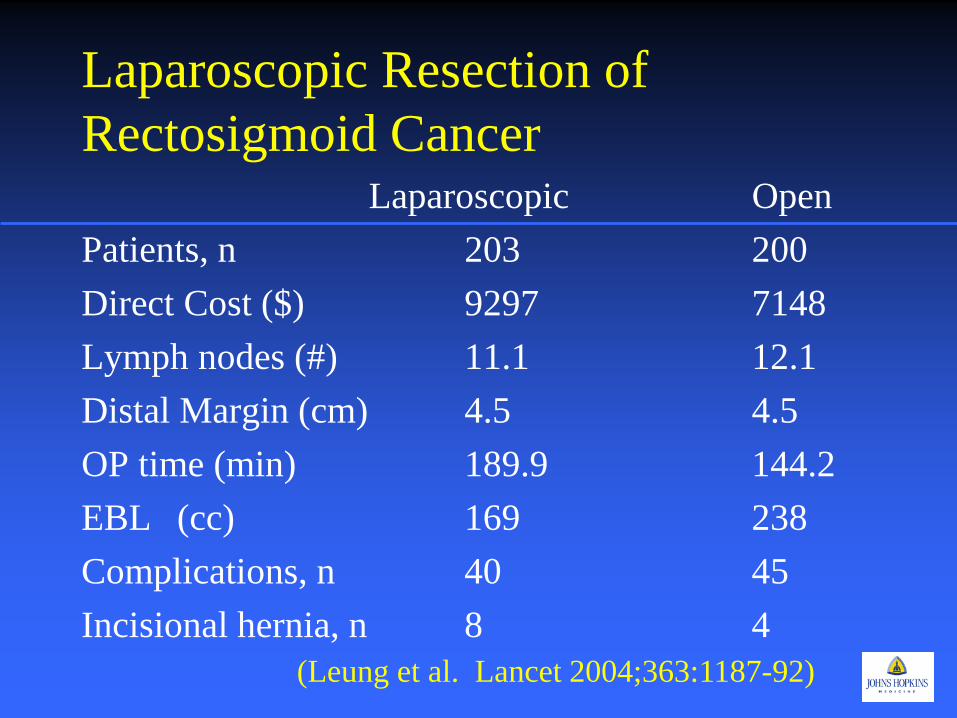
Laparoscopic Resection of Rectosigmoid Cancer Laparoscopic Open Patients, n 203 200 Direct Cost ($) 9297 7148 Lymph nodes (#) 11.1 12.1 Distal Margin (cm) 4.5 4.5 OP time (min) 189.9 144.2 EBL (cc) 169 238 Complications, n 40 45 Incisional hernia, n 8 4
(Leung et al. Lancet 2004;363:1187-92)
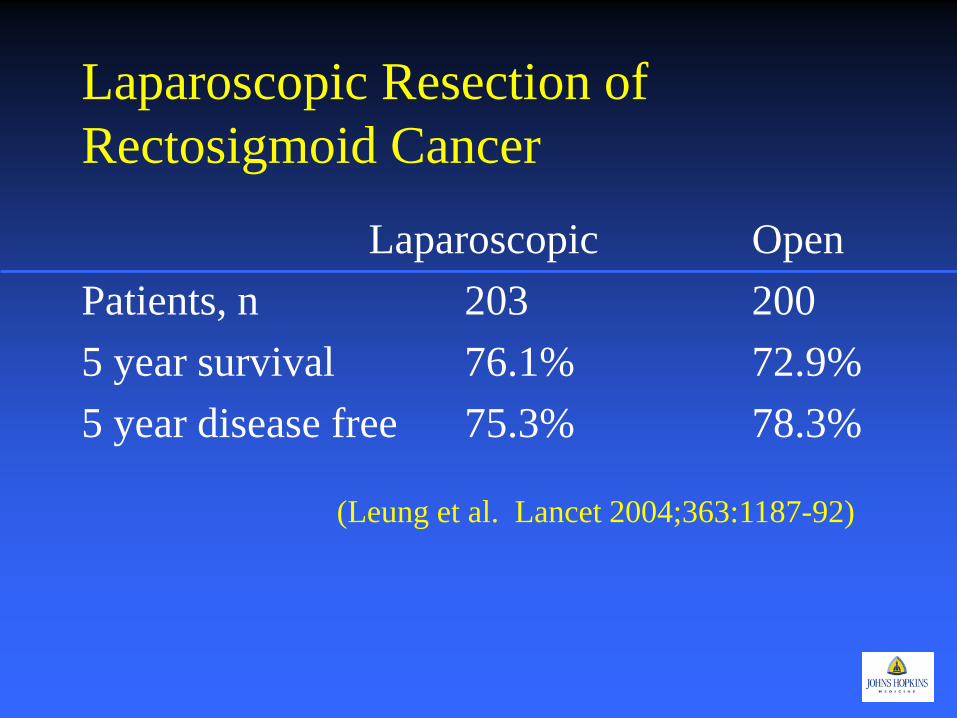
Laparoscopic Resection of Rectosigmoid Cancer
Laparoscopic Open Patients, n 203 200 5 year survival 76.1% 72.9% 5 year disease free 75.3% 78.3%
(Leung et al. Lancet 2004;363:1187-92)
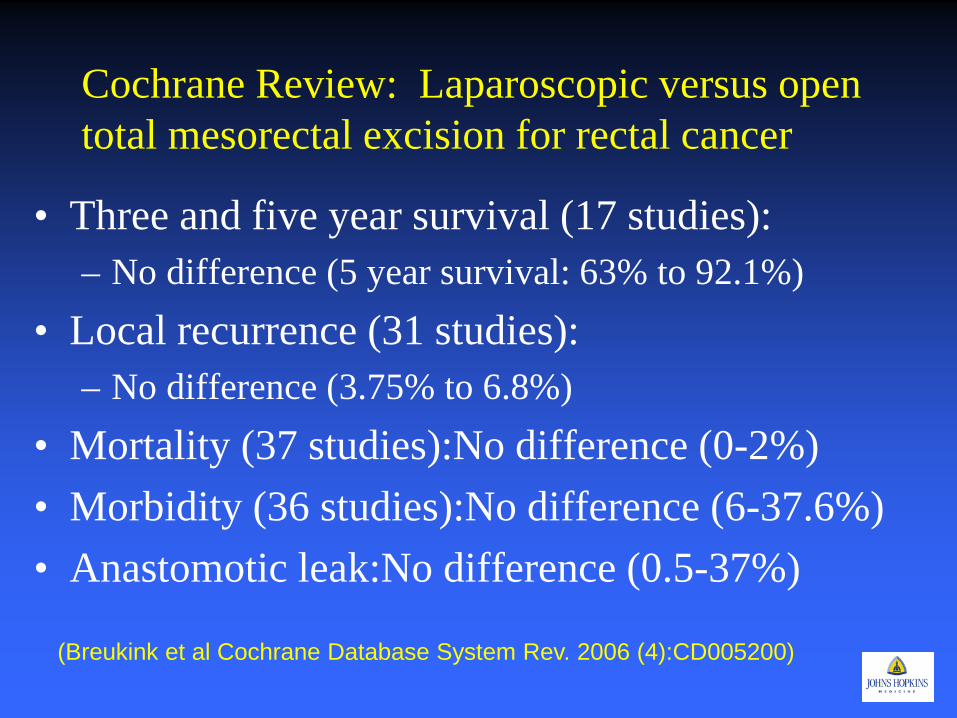
Cochrane Review: Laparoscopic versus open total mesorectal excision for rectal cancer
• Three and five year survival (17 studies): – No difference (5 year survival: 63% to 92.1%)
• Local recurrence (31 studies): – No difference (3.75% to 6.8%)
• Mortality (37 studies):No difference (0-2%) • Morbidity (36 studies):No difference (6-37.6%) • Anastomotic leak:No difference (0.5-37%)
(Breukink et al Cochrane Database System Rev. 2006 (4):CD005200)
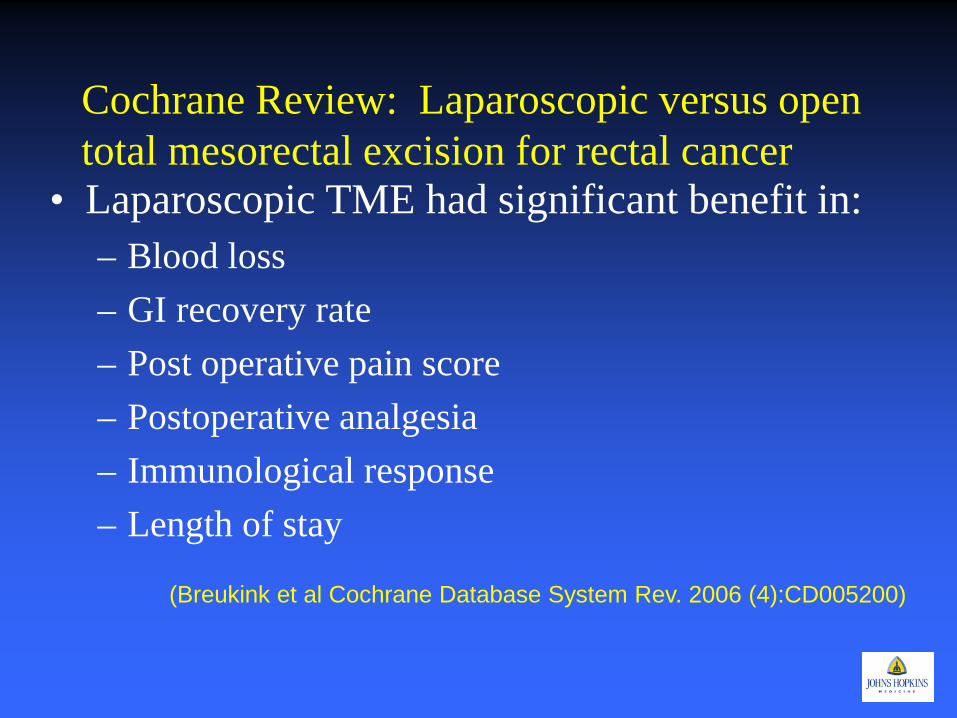
Cochrane Review: Laparoscopic versus open total mesorectal excision for rectal cancer
• Laparoscopic TME had significant benefit in: – Blood loss – GI recovery rate – Post operative pain score – Postoperative analgesia – Immunological response – Length of stay
(Breukink et al Cochrane Database System Rev. 2006 (4):CD005200)
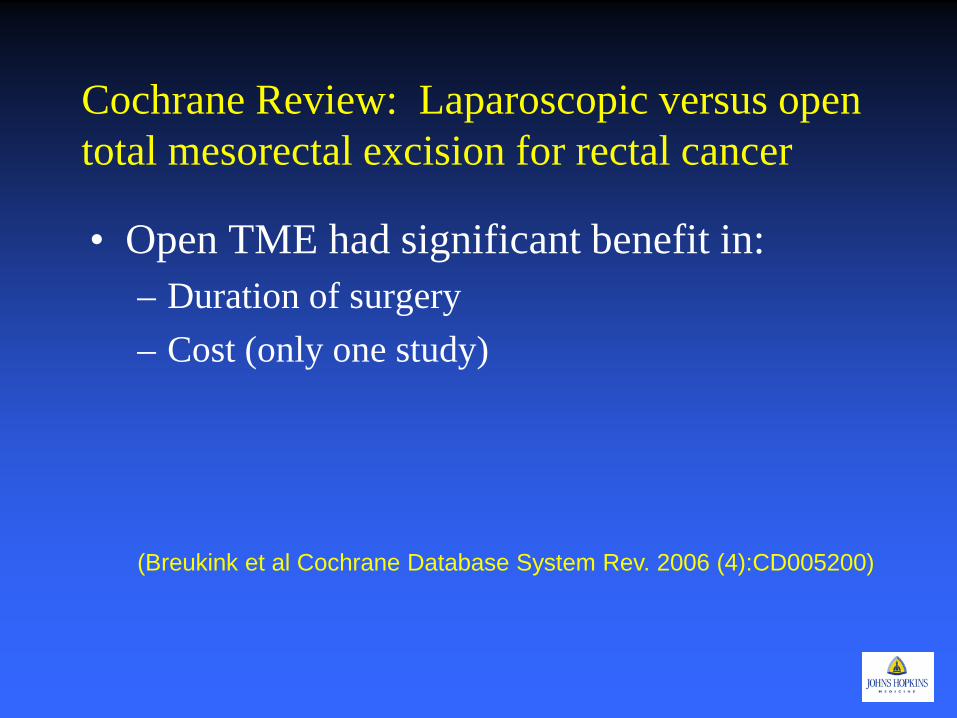
Cochrane Review: Laparoscopic versus open total mesorectal excision for rectal cancer
• Open TME had significant benefit in: – Duration of surgery – Cost (only one study)
(Breukink et al Cochrane Database System Rev. 2006 (4):CD005200)
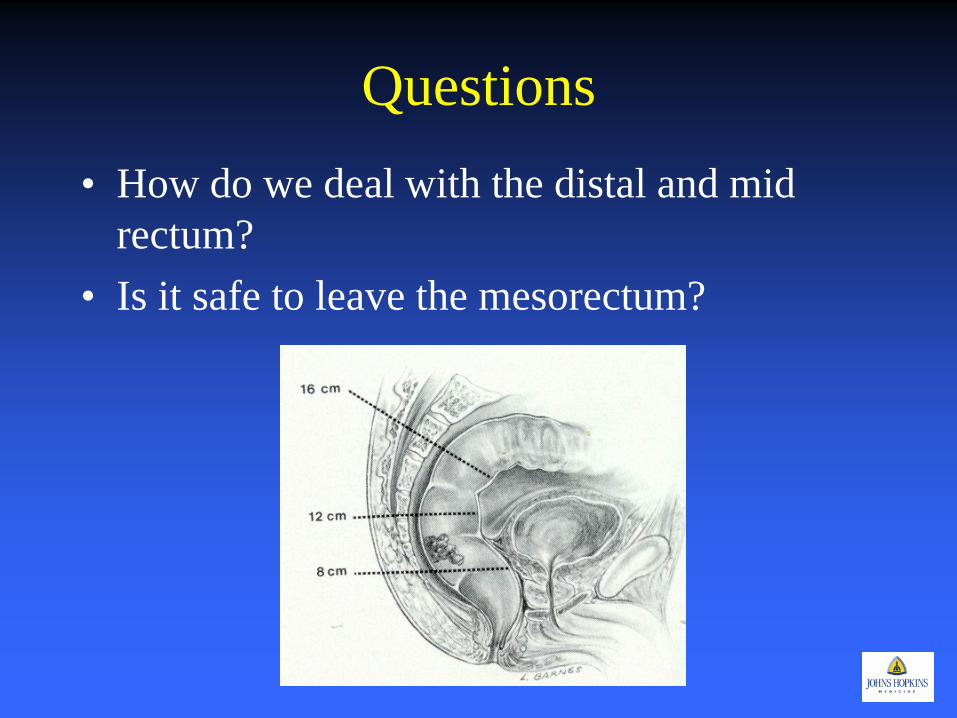
Questions • How do we deal with the distal and mid
rectum? • Is it safe to leave the mesorectum?
Laparoscopic TATA: Laparoscopic Transanal Transabdominal Approach
• 79/102 patients • 1998-2008 • Excluded:
– Stage IV – Tumors 3 cm from the anorectal ring – No neoadjuvant therapy
• Mean follow up: 34.2 months • Conversion rateL: 2.5% • Morbidity:
– Major: 11% – Minor:19%
• Local Recurrence: 2.5% • Distant Recurrence: 10.1%
(Marks J et al. Surg Endosc 2010 Nov 24(11):2700-7)
Transanal Endoscopic Microsurgery/TAMIS
• Trans anal excision – TEM superior to standard – ? TAMIS Equivalent
• Risk of lymph node metastasis – Recurrence
• T stage – T1 lesions – T2 lesions – T2 after neoadjuvant therapy
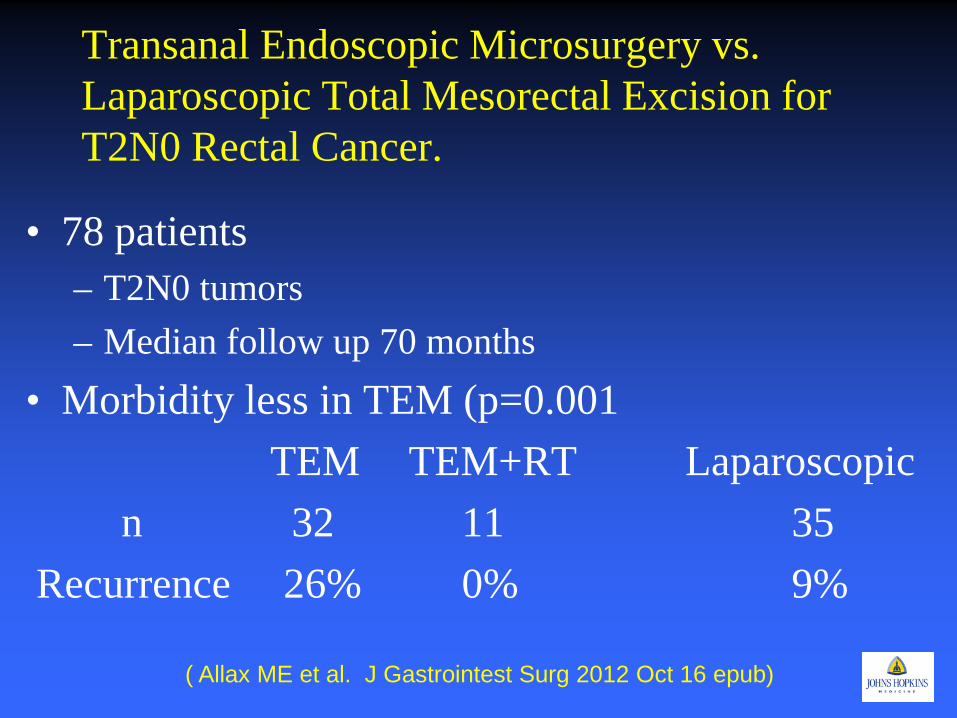
Transanal Endoscopic Microsurgery vs. Laparoscopic Total Mesorectal Excision for T2N0 Rectal Cancer.
• 78 patients – T2N0 tumors – Median follow up 70 months
• Morbidity less in TEM (p=0.001 TEM TEM+RT Laparoscopic n 32 11 35 Recurrence 26% 0% 9%
( Allax ME et al. J Gastrointest Surg 2012 Oct 16 epub)
TAMIS: Feasibility of transanal minimally invasive surgery for mid-rectal lesions.
• 16 patients – 3 T1 – 8 S/P neoadjuvant therapy – 4 neuroendocrine – 1 mucocele
• TAMIS technique • 7.5 cm from the anal verge (4-10cm) • No morbidity or mortality • LOS: 3 days
(Lim SB et al. Surg Endosc Nov 2012;26(11):3127-32)
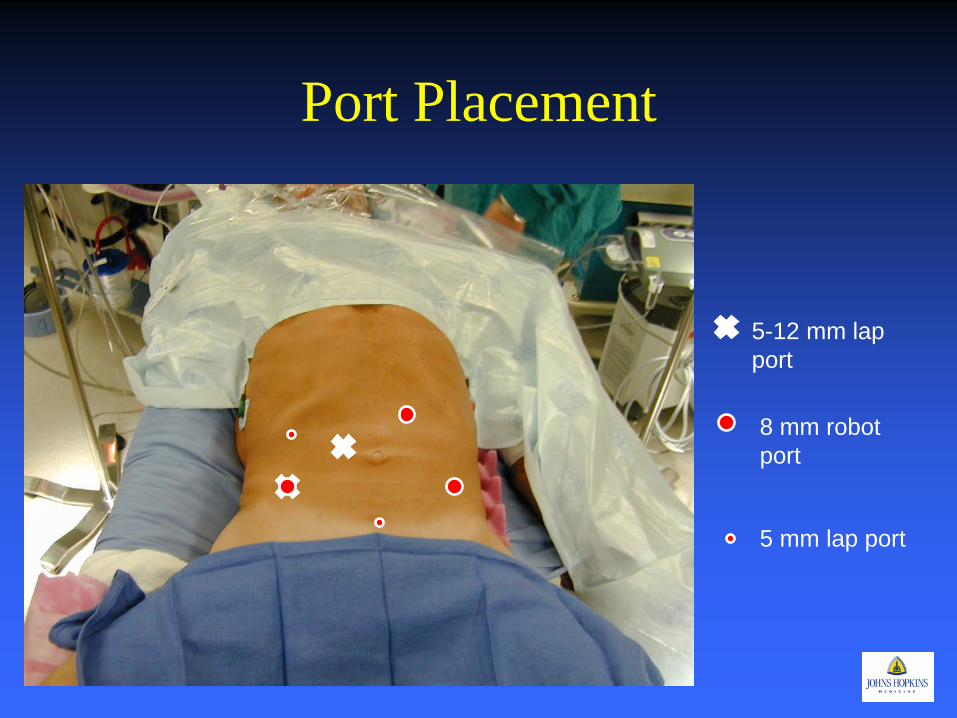
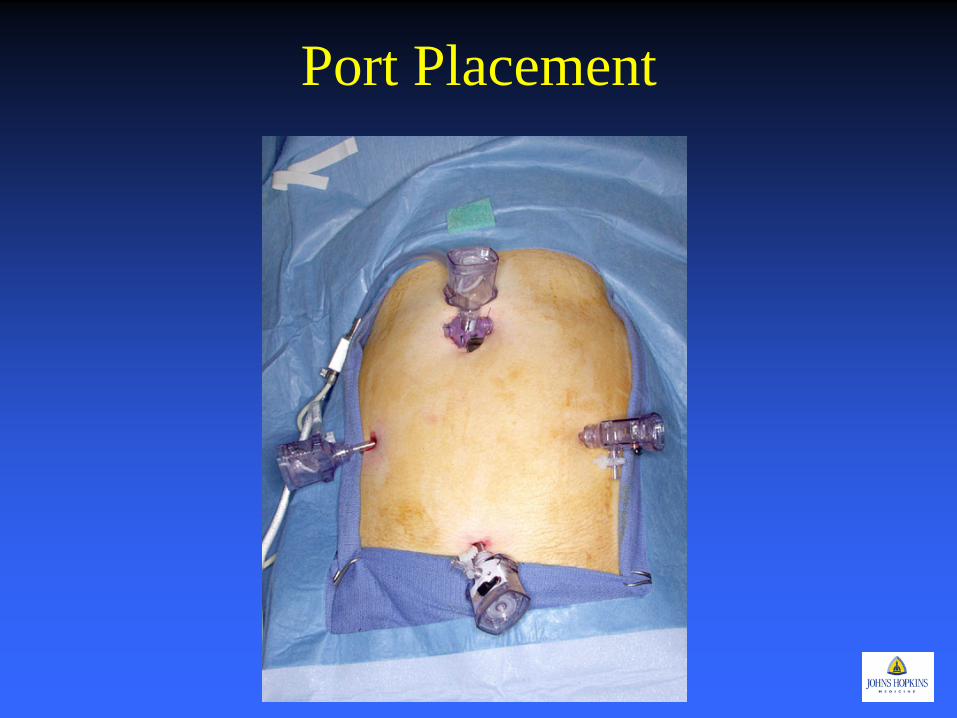
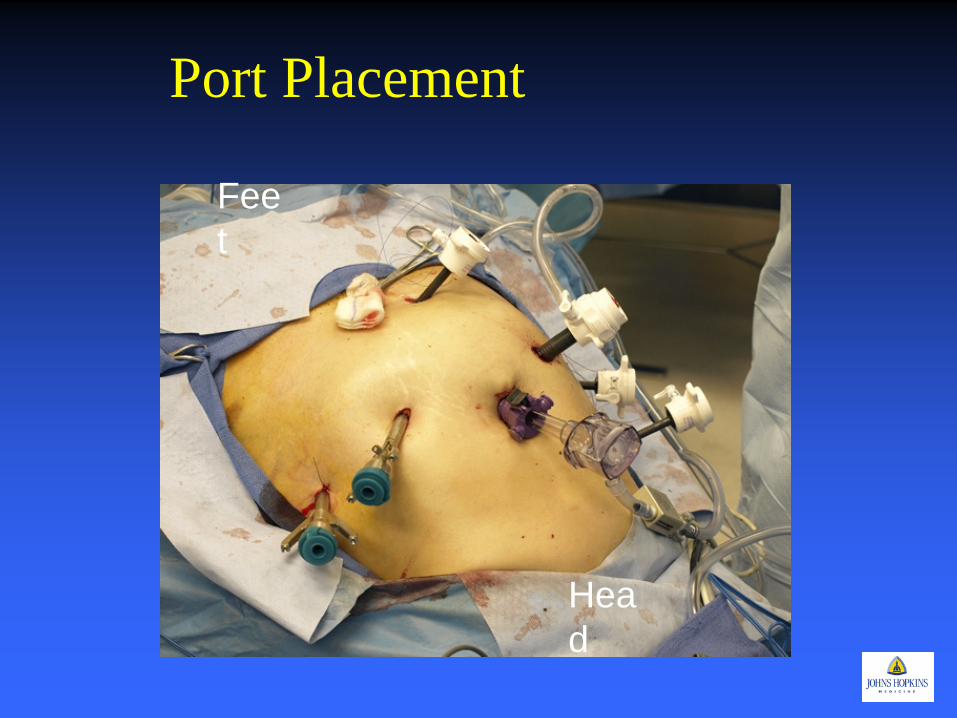
Port Placement
5-12 mm lap port
8 mm robot port
5 mm lap port
Short term Outcomes: Proctectomy • Retrospective study 2004-2007 • 39 patients robotic proctectomy • Low and Mid rectal cancer except T4 - 22 LAR - 11 inter-sphincteric - 6 APR • Complications - 0% mortality - 12.8% morbidity - 12.1 % anastomotic leak • Median OR time 285 minutes • Conversion rate 2.6 % • Median hospital stay 4 days • All negative circumferential margin • Median 13 LN removed • No local recurrence: median follow-up 13 months
(Pigazzi et al. Ann Surg Oncology 2007.)
Robotic Proctectomy: 3 Year Follow Up • 64 patients (Stage l – lll) • Mean OR time: 270 min • Conversion rate: 9.4% • Anastamotic leak: 4/52 (7.7%) • Median lymph nodes: 14.5 • Median distal margin: 3.4 cm • Circumferential margins: - • Recurrence:
– Local: 2/64 (3%) – Overall: 6/64 (9%) – 3 year overall survival: 96.2% – 3 year disease free survival: 73.7%
(Baek et al. Ann Surg 2010 May: 251(5):882-6)

Robot-Assisted Laparoscopic Surgery of the Colon and Rectum • Review of Literature for Robotic colon and
rectal surgery • 39 studies
– 13 ileocecal resections – 220 right colectomies – 190 left colectomies/sigmoid resection – 440 anterior resections – 149 APR/intersphincteric resections – 11 subtotal colectomies
(Stavros et al. Surg Endosc 2012 26:1-11)
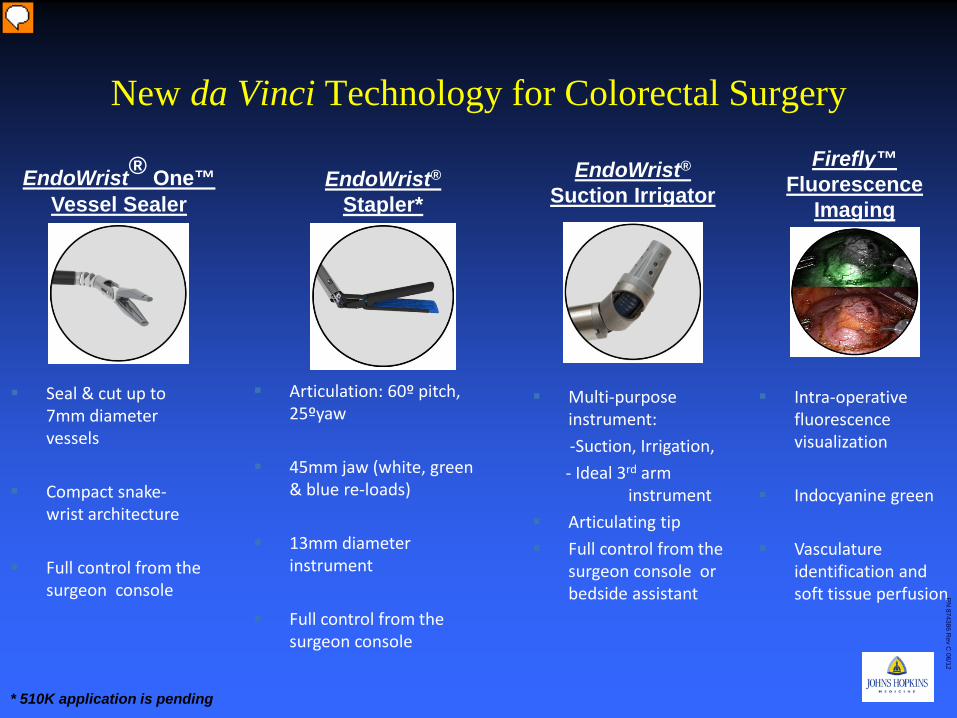
New da Vinci Technology for Colorectal Surgery
Seal & cut up to 7mm diameter vessels
Compact snake-wrist architecture
Full control from the surgeon console
Articulation: 60º pitch, 25ºyaw
45mm jaw (white, green & blue re-loads)
13mm diameter instrument
Full control from the surgeon console
EndoWrist® One™ Vessel Sealer
EndoWrist® Stapler*
* 510K application is pending
EndoWrist® Suction Irrigator
Multi-purpose instrument:
-Suction, Irrigation, - Ideal 3rd arm
instrument Articulating tip Full control from the
surgeon console or bedside assistant
Firefly™ Fluorescence
Imaging
Intra-operative fluorescence visualization
Indocyanine green
Vasculature identification and soft tissue perfusion
PN
874386 Rev C
06/12
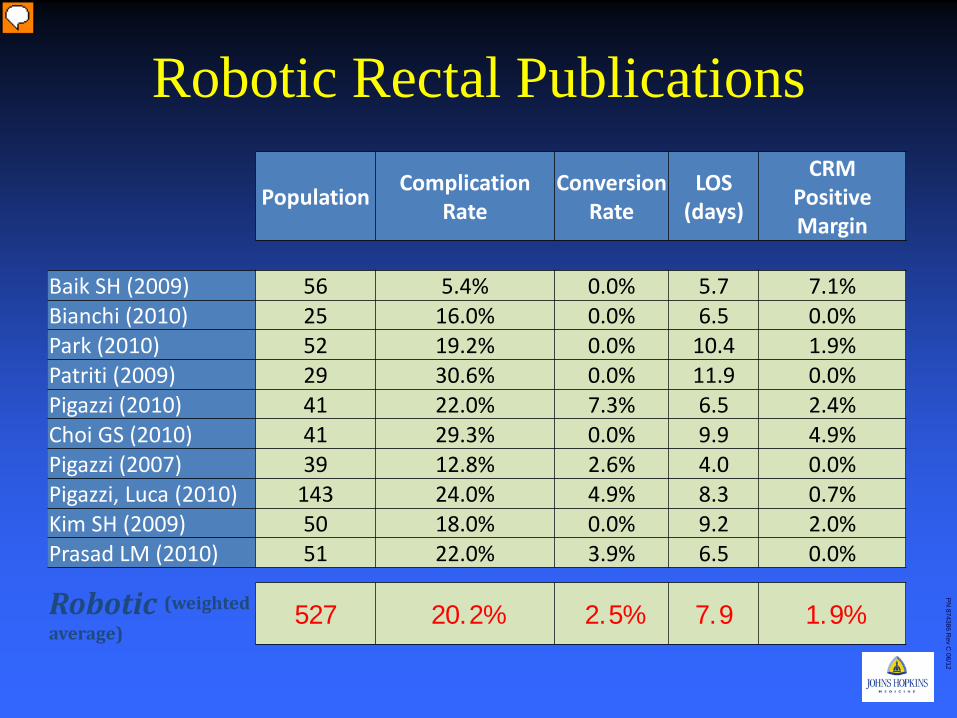
Robotic Rectal Publications
Population Complication Rate
Conversion Rate
LOS (days)
CRM Positive Margin
Baik SH (2009) 56 5.4% 0.0% 5.7 7.1% Bianchi (2010) 25 16.0% 0.0% 6.5 0.0% Park (2010) 52 19.2% 0.0% 10.4 1.9% Patriti (2009) 29 30.6% 0.0% 11.9 0.0% Pigazzi (2010) 41 22.0% 7.3% 6.5 2.4% Choi GS (2010) 41 29.3% 0.0% 9.9 4.9% Pigazzi (2007) 39 12.8% 2.6% 4.0 0.0% Pigazzi, Luca (2010) 143 24.0% 4.9% 8.3 0.7% Kim SH (2009) 50 18.0% 0.0% 9.2 2.0% Prasad LM (2010) 51 22.0% 3.9% 6.5 0.0%
Robotic (weighted average)
527 20.2% 2.5% 7.9 1.9%
Population Complication Rate
Conversion Rate
LOS (days)
CRM Positive Margin
PN
874386 Rev C
06/12
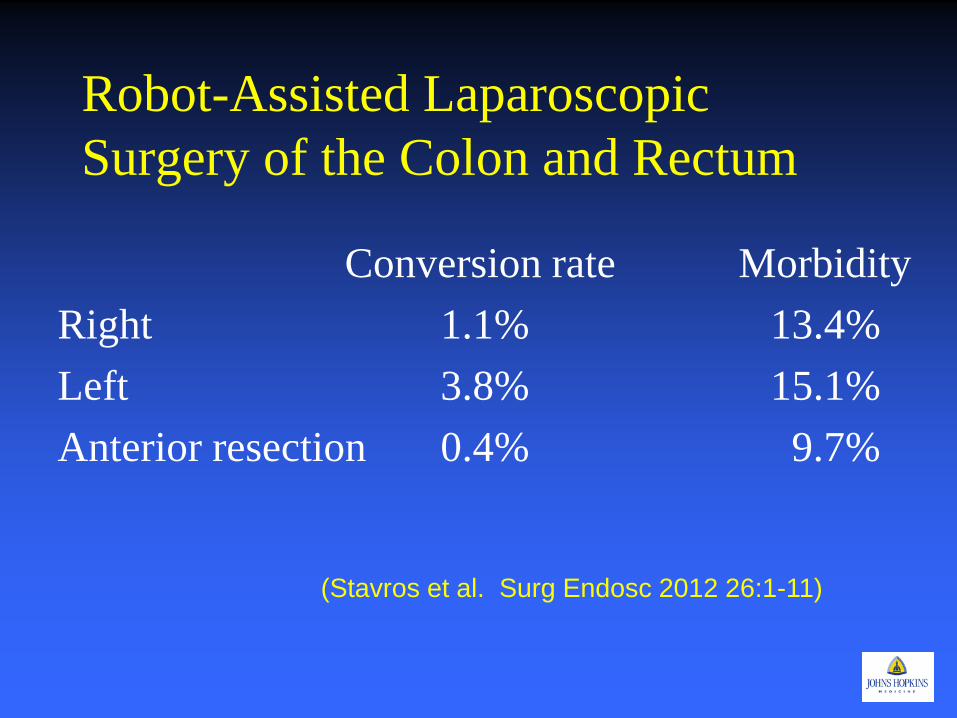
Robot-Assisted Laparoscopic Surgery of the Colon and Rectum
Conversion rate Morbidity Right 1.1% 13.4% Left 3.8% 15.1% Anterior resection 0.4% 9.7%
(Stavros et al. Surg Endosc 2012 26:1-11)
SILS
• Minimal data • Retrospective small series and case reports • No definitive benefit over other MIS
techniques • Most data on Right colectomies for colon
cancer
© 2012 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2
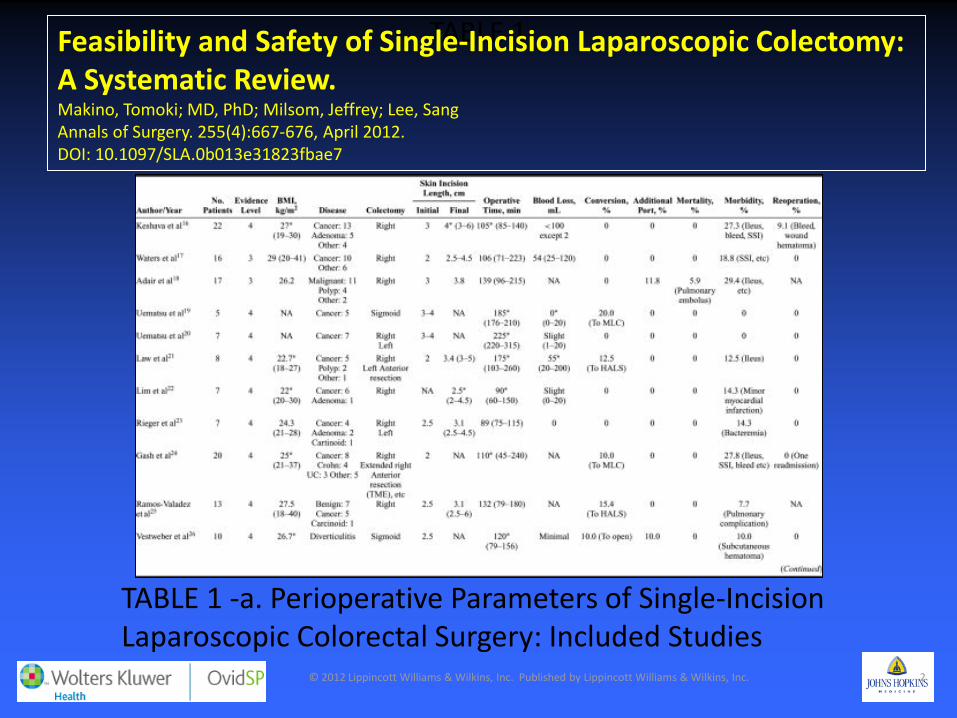
TABLE 1 Feasibility and Safety of Single-Incision Laparoscopic Colectomy: A Systematic Review. Makino, Tomoki; MD, PhD; Milsom, Jeffrey; Lee, Sang Annals of Surgery. 255(4):667-676, April 2012. DOI: 10.1097/SLA.0b013e31823fbae7
TABLE 1 -a. Perioperative Parameters of Single-Incision Laparoscopic Colorectal Surgery: Included Studies
© 2012 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2
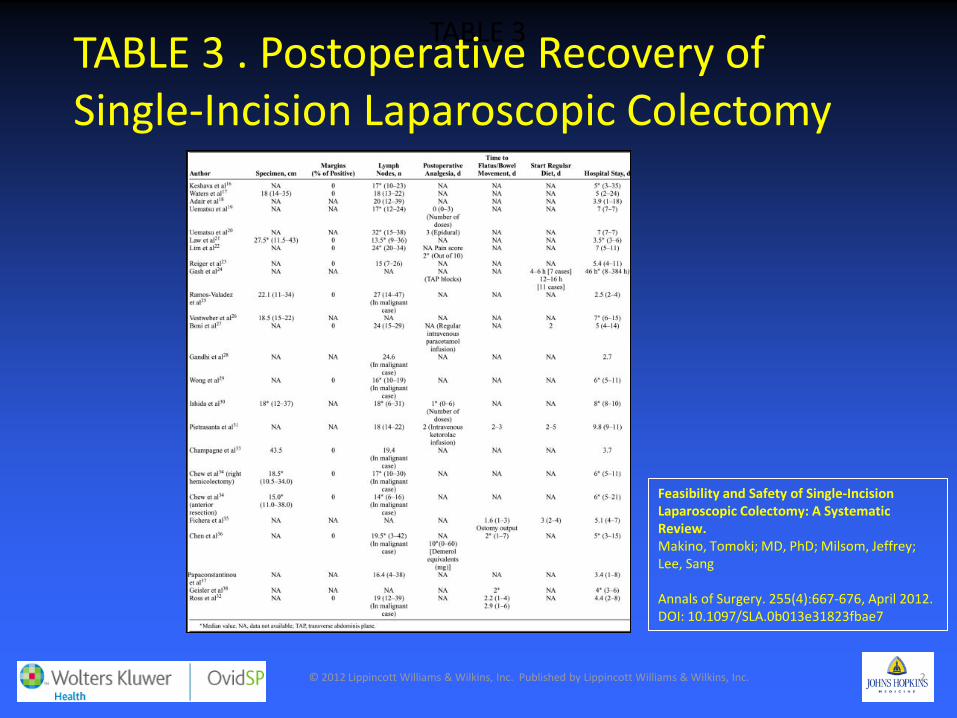
TABLE 3
Feasibility and Safety of Single-Incision Laparoscopic Colectomy: A Systematic Review. Makino, Tomoki; MD, PhD; Milsom, Jeffrey; Lee, Sang Annals of Surgery. 255(4):667-676, April 2012. DOI: 10.1097/SLA.0b013e31823fbae7
TABLE 3 . Postoperative Recovery of Single-Incision Laparoscopic Colectomy

The Future “To boldly go where no man has gone before”
Captain James T. Kirk
“Steel isn’t the answer to a systemic biological disease”
Gershon Efron MD
NOTES:Mini-laparoscopy-assisted transrectal low anterior resection (LAR): a preliminary study.
• 3 patients • One 10 mm port, one 5 mm port, one 2mm
port • Transanal TME • Double purse string stapled anastamosis. • LOS: 5 days • 1 patient readmitted for dehydration
(Lacy A et al. Surg Endosc 2012 Jul 18, E pub)
Incisionless: No Surgery • Predictors of complete response
– Tumor markers – Inflammatory markers – Treatment regimine
• Adequate post treatment assessment: determine cpr – MRI – PET/CT – Endoscopy
Watch and Wait: Habr-Gama Evaluation and
Treatment • T2/T3 lesions • Chemo Radiation
therapy • 12 week observation • Assessment of cCR
– Physical Exam – Endoscopy – CEA – CT scan – Excisional Biospy – MRI
Follow up
• Every month – Rigid proctoscopy – Digital exam – CEA – CT scan
• Every 6 weeks to 6 Months – PET/CT – MRI
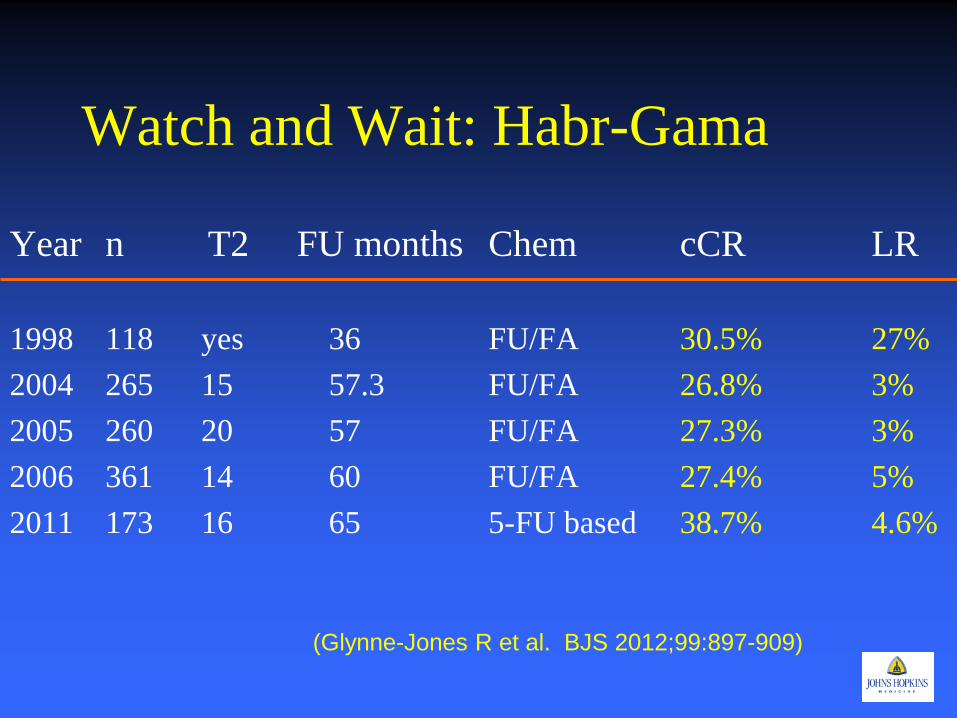
Watch and Wait: Habr-Gama
Year n T2 FU months Chem cCR LR 1998 118 yes 36 FU/FA 30.5% 27% 2004 265 15 57.3 FU/FA 26.8% 3% 2005 260 20 57 FU/FA 27.3% 3% 2006 361 14 60 FU/FA 27.4% 5% 2011 173 16 65 5-FU based 38.7% 4.6%
(Glynne-Jones R et al. BJS 2012;99:897-909)
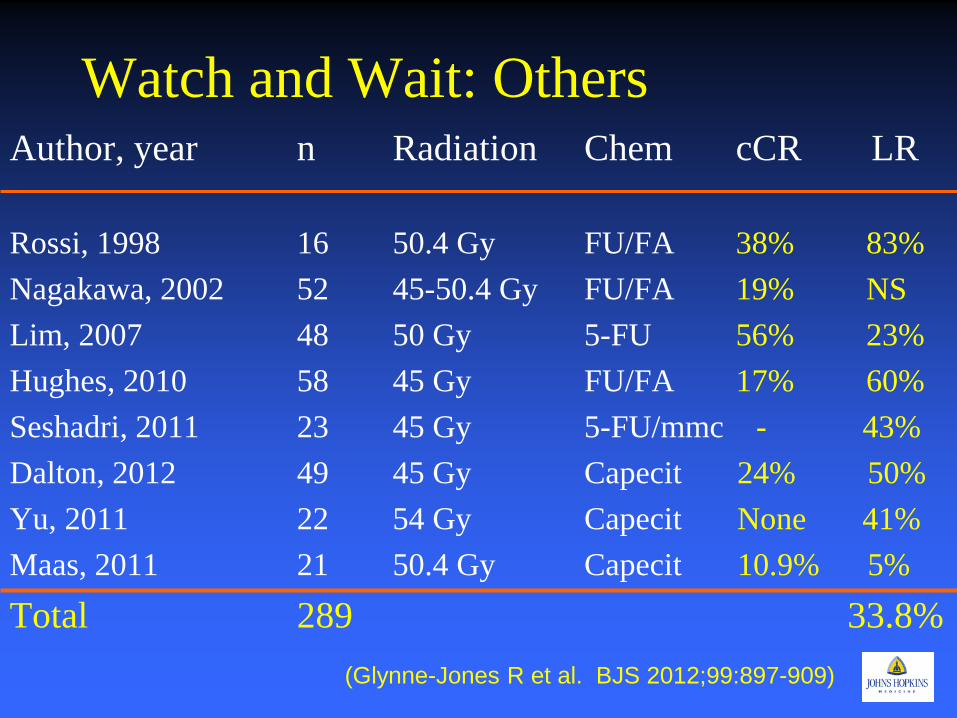
Watch and Wait: Others Author, year n Radiation Chem cCR LR Rossi, 1998 16 50.4 Gy FU/FA 38% 83% Nagakawa, 2002 52 45-50.4 Gy FU/FA 19% NS Lim, 2007 48 50 Gy 5-FU 56% 23% Hughes, 2010 58 45 Gy FU/FA 17% 60% Seshadri, 2011 23 45 Gy 5-FU/mmc - 43% Dalton, 2012 49 45 Gy Capecit 24% 50% Yu, 2011 22 54 Gy Capecit None 41% Maas, 2011 21 50.4 Gy Capecit 10.9% 5% Total 289 33.8%
(Glynne-Jones R et al. BJS 2012;99:897-909)
Where we stand • Some evidence to suggest similar oncological
results when comparing MIS to open TME. • Evidence to show benefits seen with other MIS
colectomy procedures. • Guidelines for laparoscopic colectomies for cancer
should be extrapolated • Possibly avoid in obese patients or those with
large bulky tumors. • Requires advance laparoscopic and colorectal
experience • Preliminary Data on Watch and Wait
– Needs Replication
Where are we going? • Need randomized trials to confirm suspicions. • Japan: JCOG 0404
– Randomized trial comparing lap and open colon and rectal cancer
• Color II – International randomized trial comparing lap and open
rectal cancer • US ACOSOG funded trial
– 500 patient randomized trial comparing lap and open rectal resections
• Multicenter Prospective Data Base on Watch and Wait Patients
• Robotic Prospective Trials – International/Korea
December 19, 2012 57
Johns Hopkins Hospital: New Clinical Buildings
Opened April 30, 2012
Johns Hopkins Hospital Opened 1883