Embed Size (px)
Citation preview

PERIOPERATIVE “SWEET” SUCCESS
Inpatient Diabetes Program Glycemic Team
&
Moses Cone Pre-admission Testing Staff
• Literature shows that perioperative patients with diabetes,
with adequate glycemic control have decreased
complications such as hypoglycemia, hyperglycemia,
ketoacidosis, and other infections. It also helps maintain fluid
and electrolyte balance.
• Inconsistent practices were observed in patients with diabetes
in pre-admission testing (PAT), pre-operatively,
intraoperatively and post-operatively therefore standardized
blood glucose management was necessary
• HgbA1C inconsistently available prior to surgery
• Blood sugars not available during PAT appointment
• There was no distinction between Type 1 and Type 2
diabetes regarding medication management prior to
surgery
• Practice of insulin pump management prior to and during
surgery was inconsistent
• Lack of patient education regarding diabetes management
prior to surgery
• “Guidelines for Diabetes Management” were created based
on a literature review and expert consensus by
endocrinologists, anaesthesiology, and clinical nurse
specialists’ which included:
• Goals of Perioperative Diabetes Management
Avoidance of hypoglycemia and hyperglycemia
Prevention of ketoacidosis
Maintenance of fluid and electrolyte balance
Goal glucose reading between 140-200 mg/dl
• General Guidelines for surgery including: Pre-operative
Evaluation, Perioperative and Postoperative management
strategies.
• “Diabetes Medication Adjustment Guidelines Prior to
Procedure and Surgery” were also created for
standardized medication adjustments/instructions prior to
surgery.
• Collaborative meetings were held with anaesthesia, PAT
Nurses , and the Inpatient Diabetes Program to decide how
these guidelines would be initiated.
• It was decided that a Pilot would be initiated on the MC
campus with 4 PAT nurses to test the process and determine
the volume of diabetes patients and “current state” of
glycemic control.
BACKGROUND
“Current Practice” Prior to Pilot
• A1C ordered on all patients with diabetes.
• Capillary blood glucose (CBG) was checked on all patients at PAT appointment.
• CBG’s were evaluated on day of surgery.
• Assessed volume of patients who had diabetes
Methods:
Phase 1 Pilot (63 patients)
Perioperative management of blood glucose in adults with diabetes mellitus. Up To
Date. Literature review current through: Oct 2014.
University of Washington Medical Center, 2007 “How to Manage your Diabetes
Before and After Surgery”.
• Pilot group of 4 PAT nurses were trained on “Diabetes Medication Adjustment Guidelines” and how to
review with patient’s at PAT appointment.
• Phase 2 of Pilot was planned during a 3 week time period which included: A1C, CBG at PAT appointment,
Assessment of type of diabetes, and when to alert PA (CBG>250 mg/dL)
• RN’s reviewed patient written instructions and informed patients of “Pre-surgery insulin doses” and
diabetes medications based on guidelines.
Out of 257 patients 24.5% had diabetes
71.4% had capillary blood glucoses within the goal range of 71-180 mg/dl
REFERENCES
Next Steps:
• Results of 2 week Pilot were reported back to MD’s, PAT nurses, and collaborative team.
• “How to Manage Diabetes Before and After Surgery” patient education sheet was created and presented to
Cone Health Patient Education Committee for approval
Results
Methods:
Phase 2 Pilot (60 patients)
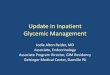
< 70 mg/dL 71-180 mg/dL 181-250 mg/dL >250 mg/dL
Phase 1 Pilot 3.00% 71% 14.20% 9.50%
Phase 2 Pilot 0 63% 28.30% 8.30%
3.00%
71%
14.20%9.50%
0
63%
28.30%
8.30%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
Capillary Blood Glucose (CBG) at PAT appointment
Phase 1 Pilot Phase 2 Pilot
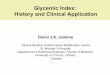
<7.9% 8.0-10.0% >10.0% A1C not done
Phase 1 Pilot 80% 12.20% 8.20% 22%
Phase 2 Pilot 74% 19% 6.30% 11.30%
80%
12.20%8.20%
22%
74%
19%
6.30%11.30%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
A1C Results at PAT appointment
Phase 1 Pilot Phase 2 Pilot
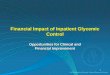
<70 mg/dL 71-180 mg/dL 181-250 mg/dL >251 mg/dL
Phase 1 Pilot 0 83% 11% 6%
Phase 2 Pilot 1.80% 94% 4% 0%
0
83%
11%6%
1.80%
94%
4%0%
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
CBG results: Day of Surgery
Phase 1 Pilot Phase 2 Pilot
• Phase 1 Pilot (63 pts.) versus Phase 2 pilot (60 pts.)• Phase 1 Pilot- 10 patients excluded - surgery cancellation (6) or no documented
CBG day of surgery (4)
• Phase 2 Pilot- 7 patients excluded- surgery cancellation
• Phase 2 of the Pilot showed an improvement in patient’s blood sugars the
day of surgery with 94% being within goal of (71-180 mg/dL)• There was one hypoglycemic event in the Phase 2 Pilot group on the day of surgery,
however insulin doses were decreased the day prior to surgery (prior to pilot insulin
doses were not reduced the day before surgery)
• RN’s did state that they observed increased time needed to review “ How
to Manage your Diabetes Before and After Surgery” therefore prompting
further discussion with leadership regarding appointment lengths.
• Overall the intervention proved successful and blood glucose levels the
day of surgery improved
• Further, A1C results allow MD’s and RN’s to better assess the patients
glycemic control prior to surgery and identify patients who need further
follow-up with PCP and diabetes education after surgery
Conclusions
Implications and Next Steps
• Revise patient instructions and train PACU RN’s regarding “Management
of Blood Sugars” after surgery
• Move pilot forms/assessment to EPIC environment to improve process
• Consider increasing appointment times in PAT for patients with diabetes
• Broaden scope of project to include other campuses within the health
system
• Consider interview of patients to assess their perception of process
Standardization of Care
Patient Education
Transformational
Leadership
Exemplary
Professional
Practice
Empirical
Outcomes
New
Knowledge,
Innovations and
Improvements