Embed Size (px)
Citation preview

Inpatient management of common GI conditions
Sandee Bernklau, MSN, FNP-BC, CGRN

The multitasker

Where we are • Explosive growth in the inpatient role:• Due to medical residency requirements-less• Less physicians currently produced• Pressure from managed care organizations• LOS-decrease• Increasing patient acuity• Cost containment

NP/PA hospitalist• Have been shown to decrease LOS, cost of
care, and decrease patient mortality• Have more time/no procedural on
patient/family education• Less chance of readmission• According to the most recent Society of
Hospital Medicine figures, 16% of hospitalist groups now employ PAs, while 20% have hired NPs

Wachter and colleagues stated that” hospitalists learn to recognize outliers and anticipate problems, become familiar with the key players in the hospital…(medical/surgical consultants, discharge planners, nurses and clergy..), and become sufficiently invested in the hospital system to be accountable for its cost and quality to lead it quality improvement efforts.”

History of the inpatientAcuityLocationRadiationFactors that exacerbate or improveAssociated symptomsPast medical/surgical historyFamily historyAlcohol consumptionIntake of medications (NSAIDS)Menstrual history in womenWhen did they last eat????

Physical examination of the inpatientVitalsEyes for icterusAuscultation/percussion chestEvaluation of bowel sounds-presence/absencePalpation for masses, tenderness, peritoneal
signsSucussion splashRectal exam(Hemocult- a must)Pelvic exam for women

Iron deficiency Anemia

Anemia (iron deficiency)• One of the most common inpt consults• More that ¼ of the world’s population is
anemic- ½ secondary to iron deficiency• Shortage of iron stores = inability of RBCs to
deliver oxygen to the body• The development and speed-individuals
iron stores is:– Dependent on age, sex, rate of growth, iron
absorption and loss

Types of iron deficiency• Absolute-iron stores absent in bone
marrow-poor dietary intake, reduced absorption, blood loss
• Functional-insufficient availability of iron-2 causes– Anemia of inflammation(Chronic disease)-
infection, inflammation or malignancy– Treatment with erythropoiesis agents

Microcytosis

Diagnosing Anemia• Look at the patient• History most critical • Female versus male• Surgical history• Chronic disease• Childhood anemia• NSAIDs/anticoagulation/antiplatelet

Always evaluate, don’t assume• The NHANESI study, 9024 participants, men
and post menopausal women with IDA had increased risk for GI malignancy within 2 years for non IDA participants(CI 9-107)
• In 148 consecutive patients with IDA 12% were found to have a malignancy (CI 7-776)

Clinical manifestations• Many asymptomatic• Again remember source-clues to symptoms• Classic
– Fatigue– Shortness of breath– Pallor– Headache– Glossal pain, reduced salivary flow– Restless leg syndrome– PICA and Beeturia

Classic presentation• HGB low 8 g/dl• MCV low 75 fL• MCH low• Serum iron low 10 mcg/dl• TIBC/transferrin elevated 400 mcg/dl• Ferritin-gold standard-low-almost all
patients <10 IDA• Responds to iron replacement

Source search• History of ulcer disease• Celiac sprue• Family history of bleeding disorder• Family history of colonic malignancy• Recent blood donation• Marathon running• Suspected malignancy• Renal disease• Alcohol• Anticoagulation• Premenopausal women-12% GI bleed

Evaluation(GI)• Consider source• Patients with unexplained iron deficiency
anemia but a negative fecal occult blood test should be evaluated for a GI source of blood loss.
• Particularly important in men and postmenopausal women. Rule out celiac
• Colon/EGD• Capsule endoscopy if above negative + balloon
enteroscopy-capsule critical within 48 hrs of bleed• Consider hematology consult if work up negative

Treatment• Transfuse?-current recommendation
– If patient is hemodynamic ally unstable and end organ ischemia
– One unit of blood-300 ml=200 ml of RBC and 200 mg of iron.
– One unit will raise HCT by 3% and HGB by 1 gram.• Oral iron therapy preferred in stable pts-in
expensive, well tolerated• IV iron Venofer 200 mg IV weekly x 5-risk of
reaction, close monitoring more expensive• Consider hematology consult

Acute GI bleed

The GI bleed

GI bleed statistics• Acute, massive upper gastrointestinal bleeding-
incidence of 40 to 150 episodes per 100,000 persons annually, with a mortality rate of 6 to 10
• Acute, massive lower gastrointestinal bleeding-incidence of 20 to 27 episodes per 100,000 persons annually, with a mortality rate of 4 to 10 percent.
• Mortality rates increase-with advancing age, co morbidities, specifically renal and hepatic dysfunction, heart disease, and malignancies.

Acute GI bleed• Goal: assess severity, potential source,
conditions that may affect subsequent treatment
• Factors predictive of an upper GI bleed– Melena, coffee ground emesis
• Lower GI bleed– Gross hematochezia, passage of blood clots– Left colon bright red, right colon-maroon
Severe GI bleeding-blood during NG tube drainage, tachycardia, HGB < 8g/dl

Where to look

Bleeding manifestations• Hematemesis-either red blood or coffee-
ground emesis-proximal ligament of treitz• Frank bloody emesis-more brisk vs coffee
ground• 90% melena- bleed proximal to ligament of
treitz• Melena can be seen with as little as 50 ml of
blood

Putting together the puzzle• History is everything• Medical history-Cardiac/CVA• Anticoagulation• Use of NSAIDs• Liver disease-variceal • Bleeding disorders• Congenital disorders• Previous GI bleeding history• Symptoms also help determine source

Less common causes of GI bleeding• Less common causes of upper gastrointestinal bleeding include:
Hemobilia
Hemosuccus pancreaticus
Aortoenteric fistula
Cameron lesions
Dieulafoy's lesion
Hemobilia

Variceal bleeding• Hemodynamic recessucitation• Blood products-replace low PLT and
coagulopathy• Some studies have shown that Factor VIIa
(recombinant) aides in control of bleeding• Vasopressin(off label), Octreotide gtts• Consider antibiotics-SBP raises mortality in
bleeds

Obscure GI bleeding• 10-20% of cases bleeding not clear source• Recurrent bleeding occurs in 5% of these
cases• Main challenge-high miss rate during initial
evaluation• Overt-perceptible bleeding• Occult-IDA with or without + FOB test

Evaluation• If hemodynamically unstable hospitalize• STAT CBC• Fluid resuscitation-essential prior to
endoscopy• Transfuse HGB < 7 g/dl• Current literature goal >9 g/L –
comorbities-CAD• consider gastric lavage

Transfusion study• Randomized study by et.al-921 adults UGI
bleed-two groups-restrictive HGB <7 g/L transfuse, unrestrictive HGB < 9 g/L
• Pts in restrictive group more likely to avoid transfusions, received less blood, lower mortality( 5 vs 9%, 95% CI)
• Retrospective study 1677 pts, nonvariceal UGI bleed, blood transfusion in 24 hours of bleed risk of rebleeding(OR 1.8, 95% CI)

Evaluation(cont.)• Melena-EGD/push enteroscopy• Hematochezia-colon-unprepped ideal• Several studies have demonstrated that
colonoscopy identifies definitive bleeding sites in more than 70 % of patients.
• If negative-capsule endoscopy-highest yield if performed within 24 hours of bleed
• Consider tagged RBC scan-yield• Angiography

Risk stratification• Hemodynamic stability• Hemoglobin < 10 g/L in CAD• Active bleeding• Large ulcer > 1 to 3 cm• Ulcer location
• Rockall score and Blatchford score

Capsule endoscopy• Multiple retrospective studies found CE
superior to push enteroscopy for occult GI bleeding
• Meta analysis CE vs PE-yield 56% vs 26%(Triester et. al, 2005)
• CE was also found to have better identification of both vascular and inflammatory lesions
• DBE is found to be superior to CE 73% vs 44%-after + CE findings(May & Schneider, 2006)

Treatment• If possible avoid offending agent• Acid suppression-Preferred PPI infusion,
Protonix gtt- 80 mg bolus followed by 8mg/hr(however PPI does not prevent further bleeding, stigmata or death)
• Somatostatin/Octreotide gtt for variceal• Depo-sometimes for GI bleeds• Anticoagulation-stop? Continue?-
cardiology/neuro involved

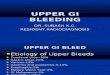
Selective angiogram of the gastroduodenal artery shows contrast material extravasation into the duodenal lumen (arrow).

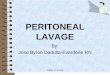
Colonic bleed

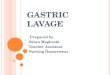
Positive capsule endoscopy

Abdominal pain

Location

Acuity• Critical factor if onset < 1 hour
– Perforated ulcer– Ruptured abscess– Ruptured hematoma– Esophageal rupture– Dissecting aneurysm– Ectopic pregnancy– Mesenteric infarction

Acuity (cont.)• Onset > 1 hour
– All sudden onset pain +– SB obstruction– Acute pancreatitis– Acute cholecystitis– Nephrolithiasis– Acute diverticulitis

History/Physical exam findings• History
-Location/radiation?-How long pain-hours, days, weeks, years?-Associated symptoms-Past medical history-Medication history-Surgical history-What makes it better/worse?
• PE findings-Scars?-surgeries?-Jaundice/icteris-Eccymosis-grey turner?-Abdominal distention-Fever, tachycardia, shortness of breath?-Change in bowel habits, color-heme-Nausea/vomiting-Abnormal labs-LFTs, anemia, Leukocytosis-Abdominal tenderness-Bowel sounds

Cullen’s sign and Grey Turner
Cullen’s sign
Grey Turner’s sign

Evaluation• Routine labs-CBC, CMP,
CRP, ESR, Amylase and Lipase, PT/INR
• U/A• Pregnancy test• Obstructive series• US• CT• Rectal examination

Mesenteric ischemia• Acute and severe onset-diffuse abdominal
pain• 1-2% of the population• Hx critical-known CAD, ischemia,
cardiovascular disease• Mesenteric venous thrombosis rare source
– Seen in previously healthy individuals

Evaluation(Mesenteric ischemia)• CT angiography/MR
angiography of the celiac artery or mesenteric vessels
• Sigmoidoscopy for ischemic colitis

Additional sources of pain to consider• Ruptured aneurysm• Ectopic pregnancy• Leiomyomas• Sickle cell• Celiac artery compression• Painful rib syndrome• Abdominal wall pain syndrome• Fitz-Hugh-Curtis syndrome

Treatment• Treatment based on findings: acute-surgical
abdomen-surgical team consult• Upper abdominal-EGD/imaging-rule out
biliary disease• Lower-colonoscopy-imaging/CT• Consider associated symptoms to determine
best course. Laboratory/vitals help determine acuity

Acute Pancreatitis

Pancreatitis Etiology

Classification• Atlanta classification:
– Interstitial edematous acute pancreatitis-acute inflammation with tissue necrosis
– Necrotizing acute pancreatitis-inflammation associated with pancreatic parenchymal necrosis/and or peripancreatic necrosis

Severity• Mild-absence of organ failure or systemic
complications• Moderate-no organ failure/or transient(<
48 hours)• Severe-Persistent organ failure(>48 hours)
with multiple organ systems involved(i.e. lungs, kidneys)

Early assessment• Early assessment critical• Evaluate for fluid loss• Affected organs/systemic manifestations
– Lungs– Kidney– Ca+ levels– Heart
• APACHE II score• SIRS• Modified Marshall Score for organ dysfunction

APACHE II

SIRS

Fluid replacement• Aggressive hydration
– Isotonic crystalloid solution(NS, LR)– LR vs. NS-has been shown to reduce SIRS(84 vs 0%)– Give at rate of 5 to 10 mL/kg per hour– Assess heart, lungs, kidney first for failure– For tachycardia or suggestion of shock-20 mL/kg
over 30 min followed by 3 ml/kg/hour for 8-12 hours
– Evaluate for Ca+, consider NS in those cases– Evaluate for ATN- urine output-be suspicious

Pain control •Hypovolemia-leads to vascular leak, hemoconcentration-ischemic pain•Opiods-intravenous•Fentanyl-good with renal impairment•Dilaudid-0.2 -1 mg q 2-3 hrs not opiod naïve•Morphine-avoid can irritate

Monitoring• First 24 to 48 hours-
close monitoring-may require ICU bed
• O2 Sat >95%-goal-risk of ARDs
• Blood gas if < 90%• Urine output(> 0.5 to 1
cc/kg/hr)• Electrolytes-watch Ca+,
glucose, mag

Nutritional support• Mild pancreatitis, NPO IV hydration-24 to 48
hours• Feed if hungry-always a good sign-must be
absent of ileus• Start with clear liquids, advance to low fat soft
diet• Moderate to severe consider NJ vs enteral
– Avoid oral feeding due to gastroduodenal inflammation and or extrinsic inflammation from infection

Enteral feeding• For moderate to severe acute pancreatitis • Randomized trial 208 patients-severe
pancreatitis NG at 24 vs oral at 72 hrs –no difference in rates of infection or complications
• High protein low fat semi-elemental-Peptamen AF start slow 25 ml/hr
• Presence of fluid collections not always contraindication for enteral feedings

Parental feeding• Reserved for pts that do not tolerate oral or
enteral• Observational study 2920 MV patients given
enteral nutrition with early or late parental nutrition found a mortality(35 vs 28%) vs enteral alone.
• Randomized trial 4640 pts receiving enteral nutrition with supplemental parental-pts receiving late parental supplementation lower risk of infection or complications(23 vs 26%)

Complications• Pancreatic necrosis/pseudocyst formation• Splanchnic venous thrombosis• Pseudoaneurysm• Exacerbate underlying conditions• Renal failure• ARDS• Development of pre-diabetes/diabetes

Pancreatic fluid collections• Tend to develop early• Watch and wait• Most resolve within 7-10 days• Watch for fever and pseudocyst formation

Pancreatic necrosis• Leading course of morbidity and mortality in
necrotic pancreatitis• 1/3 of patients with necrotic pancreatitis will
develop• Suspected in patients with pancreatic or
extrapancreatic necrosis who deteriorate (clinical instability or sepsis physiology, increasing white blood cell count, fevers) or fail to improve after 7 to 10 days of hospitalization
• Get therapeutic/IR/surgical team involved• Wait for culture before using antibiotics

Management of underlying conditions• Gallstone pancreatitis-
ERCP/EUS/cholecystectomy-in future• Pancreatic pseudocyst-cyst gastrostomy –
determine if candidate-utilize therapeutic team
• Alcohol-prevention-use• Hypertriglyceridemia• Hypercalcemia

Acute cholecystitis• Acute cholecystitis: most prevalent surgical
entity• Most common cause: Cholelithiasis • An autopsy 11-35% of Americans have• 1-2% of the patients develop symptoms
annually• 700,000 cholecystectomies are performed
annually

Symptomatic cholelithiasis• Gallbladder pain in presence of gallstones• Gallstones results of cholesterol and calcium
salts• Cholesterol or pigmented stones (tarry:
Sickle cell, hemolytic diseases)• Brown stones-Asian populations• In US 70-80% cholesterol variety• Choledocholithiasis: Stone in bile duct=
ERCP

Risk Factors for Cholecystitis• Hispanic• Obese• 40s-50s• Pregnant• Post partum• Comorbidity-sickles-hemolytic disease

Symptoms• Biliary colic: constellation of symptoms• Occurs when gallbladder contracts against
an outlet obstruction (stone). • Described as sharp, cramping, RUQ with
radiation to scapula.• Usually occur after large, fat rich food.• Night waking• Nausea, chills, malaise, bloating, belching or
occasional diarrhea.

Physical exam findings• Murphy’s sign + (pain in the right
midclavicular line upon deep inspiration)• Right upper quadrant pain tenderness• In-between episodes may be pain free

Diagnostic Evaluation• Labs: Lfts, amylase, lipase• US for dilated CBD(common bile duct) and
presence stones- can sometimes be seen• CT scan• MRCP• Normal bile duct <6 mm allow 1 mm for
each decade of life past 60 years old• Post chole-give 1-2 mm for CBD

Treatment• Cholecystectomy-urgency based on how
sick/toxic• Some wait- with low fat diet and avoid
heavy meals• Counsel patients that are waiting on
reporting symptom change• Confirm no Choledocholithiasis

Acute Ascending CholangitisAscending cholangitis is an infection of the
biliary tract with the potential to cause significant morbidity and mortality. Many patients with acute cholangitis respond to antibiotic therapyDescribed a triad of fever, jaundice, and right
upper quadrant pain. More severe cases add septic shock and confusion.-Due to biliary obstructionRequires urgent referral for treatmentCannot be left alone/ICU admissionWill die within hours if left untreated

Choledocholithiasis• Gallbladder pain in presence of gallstones• Gallstones results of cholesterol and calcium
salts• Cholesterol or pigmented stones (tarry:
Sickle cell, hemolytic diseases)• Brown stones-Asian populations• In US 70-80% cholesterol variety• Choledocholithiasis: Stone in bile duct=
ERCP

DiverticulitisDiverticulosis is a disorder of the GI tract-sac
like outpouchings of mucosa/submucosa through muscle layer.Found along colon’s mesenteric border-
descending colon/sigmoid colon/rectum-weakeningOccurs in 50-70% of people > 50 years old70% cases benignBleeding may occur due abrasion or erosion in
adjacent arteryDiverticulosis progresses to acute
Diverticulititis in 20% of cases

Diverticular Disease(Epidemiology)• < 10% in younger then 40• Up to 65% in those over 85• Rare in Africans• Most common in Westernized societies

Symptoms of Acute Diverticulitis• Lower left quadrant tenderness(with or
without guarding)• Low grade fever• Leukocytosis• Rarely may present with abscess
formation/perforation

Management of Acute Diverticulitis• Bowel rest: low residue food, NPO or clear
liquids, depending on severity of symptoms• Opioid analgesics• Broad spectrum antibiotics• Surgery consult-if patient has more then
two attacks or does not respond to conventional therapy
• CT scan of abdomen• Colonoscopy contraindicated in acute attack

Antibiotics for Acute Diverticulitis• Ampicillin 1-2 gram IV every 4-6 hours 500
mg po every 6 h x 7-10 days• Cefotetan 1 gram IV q 12 h• Ciprofloxacin 400 mg IV every 8-12 hrs, po
500-750 every 12 h x 7-10 days• Metronidazole 500 mg IV every 8-12 h, po
250-500 mg every 6 h x 7-10 days• Gentamicin 3.5 mg/kg/day IV every 8 h for
7-10 days

Special populations

GeriatricsAging population(> 65 years old, more then ½
get admitted in ED)Less likely to present in classic presentationAcute abdominal pain carries a 10% mortality
in elderlyHigh risk of ischemia due to CAD and poor
circulatory disorders, DM.Take NSAIDS (ulcers/perforation)Anticoagulation useAbdominal aortic aneurysm –if in doubt scan
their abdomen/send to the emergency room

Pregnancy• Should be considered emergency• Can be related to GI, gyne, urologic or obstetric• Anatomical changes that normally occur during
pregnancy may make diagnosis difficult• Enlarging uterus• Alteration in GI function/motility• Decreased progesterone-decreased LES
pressure ↑ heartburn/GERD

Evaluating the Gravid Patient“Don’t penalize her for being pregnant!”Radiologist/anesthesiologists dreadLeads to delayed diagnosis and treatmentUS and MRI not associated with ionizing
radiation-no ill effect to fetus documentedNo radiological procedure shown to cause
harm < 5 rads no fetal harmMost risk to fetus between 8 and 15 weeksAlways shield abdomen

Estimated Fetal Exposure to Radiology

Surgical abdomen during pregnancy• Avoid elective surgery• Appendicitis-most common no obstetrical
surgical intervention during pregnancy• Affects 1 in 1500 pregnancies• Symptoms: RLQ pain, anorexia, nausea, and
vomiting. Some may have fever.• WBC may normally increase with
pregnancy-increasing bands-more suggestive

Appendicitis• Results from appendiceal dilation secondary
to obstruction. • Obstructions: lymphoid hyperplasia,
fecalith, tumor, foreign body• Other causes: pelvic infections, ovarian
torsion, ectopic pregnancy, diverticulitis, Crohn’s disease

Appendicitis (cont.)• Delayed treatment increases morbidity• An unruptured appendix fetal loss 3-5%• Fetal loss rate of 20-25% and maternal loss
4% with ruptured appendix• Prompt imaging aides in diagnosis-CT scan
or US

Gallbladder disease in pregnancy• Biliary sludge and gallstone formation
common• Occurs in up to 31% and 2% respectively• 28% will manifest with pain• Evaluate with labs(LFTs, WBC and US)• Ductal dilation and stone will be visualized• Acute cholecystitis-hospital admit/IV
hydration and antibiotics • Treatment non-operative and supportive