-
PI-
54
99
02
-AF
Jun
r20
19
Prof. Yann GouëfficDepartment of vascular surgery and
endovascular surgery
Goupe Hospitalier Paris Saint Joseph, France.
Insights on ELUVIA from the
IMPERIAL-trial and beyond: When
to prefer a stent-based approach?
-
PI-
54
99
02
-AF
Jun
r20
19
Y. Gouëffic reports:
- Research funding from Bard, Medtronic, Terumo, WL Gore
- Personal fees and grants from Abbott, Bard, Biotronik,
Boston
Scientic, Medtronic, Terumo, Vygon, WL Gore (medical
advisory
board, educational course, speaking)
Disclosures
-
PI-
54
99
02
-AF
Jun
r20
19
Femoropopliteal algorythm
PTA
Bare metal stent
Covered stent
Drug eluting stent
Drug eluting balloon
Vessel preparation
To define the lesion
Treatment
To define the approach
-
PI-
54
99
02
-AF
Jun
r20
19
Rational for DES
A drug to inhibit SMC
proliferation and migration
• The true lumen ( ) of the superficial femoral artery is still
open at 12 cm distance
• Dissection of the arterial wall located between the internal
elastic lamina and the atherosclerotic plaque ( )
• The newly formed route in the arterial wall was filled with
thrombus at all levels
• Reobstruction began at the distal part of the artery
Scaffolding to prevent subintimal
recoil
Scholtes, Circ Cardiovasc Interv. 2012 Iida, O. et al. Cath and
Cardiov Intv. 2011; 78:611–617.
Kimura T, et al. N Engl J Med 1996;334:561–567.
D0 D3 D7
-
PI-
54
99
02
-AF
Jun
r20
19
Zilver PTX vs POBA for TASC A/B femoropopliteal lesions
At 5 years, sustained clinical, morphological and
hemodynamic outcomes
Dake, Circ Cardiovasc Interv. 2011Dake, Circulation, 2016
Zilver® PTX® RCT
-
PI-
54
99
02
-AF
Jun
r20
19
First arm of randomizationPrimary end point
12-month rates of event-free survival andpatency in the primary
DES and PTA groups
Second arm of randomization- Sub groups (BMS/DES; 59/61)
- Secondary endpoints
Dake, Circ Cardiovasc Interv. 2011
479 patients to include
Sample size calculation of Zilver® PTX® RCT
-
PI-
54
99
02
-AF
Jun
r20
19
BATTLE trial French multicentric randomized clinical trial
comparing MISAGO® vs. ZILVER® PTX® for the treatment of
intermediate
femoropopliteal lesions (from February 2014 to September
2018)
10 centers: Clinique d'Antony (Jean-
Marc PERNES); CHU de Besançon
(Simon RINCKENBACH); CHU de
Bordeaux (Eric DUCASSE) ; CHU de
Clermont Ferrand (Eugenio ROSSET) ;
AP-HP, Hôpital Henri Mondor (Pascal
DESGRANGES) ; CHU de Lyon
(Patrick FEUGIER) ; CH de Bourgouin
(Patrick LERMUSIAUX); Clinique
Ollioules (Philippe COMMEAU) ; CHU
de Rennes (Alain CARDON) ; Clinique
Pasteur (Antoine SAUGUET); CHU de
Nantes (Yann GOUËFFIC)
**
*
**
**
* *
*Nantes University Hospital
BATTLE ClinicalTrials.gov number, NCT02004951
*
Gouëffic, JACC Intrv, In press
-
PI-
54
99
02
-AF
Jun
r20
19
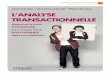
Freedom from in-stent restenosis* @ 12 months(primary endpoint)
(Kaplan Meier estimates)
*Defined by restenosis of >50% and by a peak systolic
velocity index >2.4 at the target
lesion. Assessment by an independent core laboratory (thromboses
were excluded)
Gouëffic, JACC Intrv, 2020
@ 12 months:
MISAGO®: 85.7%
ZILVER® PTX®: 90.3%
P=0.36
@ 24 months:
MISAGO®: 80.9%
ZILVER® PTX®: 85.8%
P=0.64
-
PI-
54
99
02
-AF
Jun
r20
19
The plateform and/or the absence of polymer could explain the
absence
of a difference between MISAGO® vs. ZILVER® PTX®
Gouëffic, JACC Intrv, 2020
Zilver PTX does not use a polymer to release
paclitaxel, delivering approximately 95% of the
total drug within 24 h
of deployment, with sustained paclitaxel levels in
the artery wall over 56 days
-
PI-
54
99
02
-AF
Jun
r20
19
BSC PI Drug-Eluting Stent Clinical Program
IMPERIALMulticenter, RCT 2:1(Eluvia : ZilverPTX)
N = 465 2Y follow up complete
MAJESTICMulticenter, single-arm(Eluvia)
N = 57 3Y follow up complete
EMINENTMulticenter, RCT 2:1(Eluvia : BMS)
N = 750 Enrolling
REGALMulticenter registry(Eluvia)
N = 500 Enrolling
SPORTS*Multicenter, RCT 1:1:1 (Eluvia:DCB:BMS)
N = 222 Enrolling
SAVALMulticenter, RCT 2:1(DES BTK : PTA) & single-arm
N = 201 & N = 100
Enrolling
*These investigator-sponsored studies are supported by grant
funding from Boston Scientific. Boston Scientific is not
responsible for the collection, analysis or reporting of these
studies which remain the sole responsibility of the investigators.
Information for the use in countries with applicable product
registrations.SAVAL is an investigational device and not available
for sale in the US.
-
PI-
54
99
02
-AF
Jun
r20
19
Primary Investigators
Global: William A. Gray, MD
European: Stefan Müller-Hülsbeck, MD
Study Design
RCT
(Eluvia DES vs Zilver PTX)
Long Lesion Sub-study
(Eluvia)
Pharmacokinetic
Sub-study (Eluvia)
• 2:1 randomized
• Single-blind
• Non-inferiority trial
• Single arm
• Lesion length 140 mm-190 mm
• Single-arm
Patients
N=465
Eluvia N=309 vs
Zilver PTX N=156
N=50 N=13
InvestigationalCenters
65 study centers: US, Canada, New Zealand, Belgium, Germany,
Austria, Japan
IMPERIAL Clinical Study Overview
Gray WA, Lancet 2018.
-
PI-
54
99
02
-AF
Jun
r20
19
IMPERIAL Study Devices
Eluvia™ DES
Boston Scientific
Zilver® PTX®
Cook Medical
Stent Platform Innova Zilver Flex
Material Nitinol Nitinol
PolymerBiostable Fluorinated
Polymer Matrix (PROMUS polymer)
None
Drug
Dose DensityPaclitaxel
0.167µg/mm2Paclitaxel
3 µg/mm2
Deployment Self-expanding Self-expanding
SizesDiameter Length Diameter Length
6-7 mm 40-150 mm 6-8 mm 40-120 mm
BSC Data on file. Cook Medical (2014). Zilver PTX Drug-Eluting
Peripheral Stent Instructions for Use.
-
PI-
54
99
02
-AF
Jun
r20
19
CAUTION: The law restricts these devices to sale by or on the
order of a physician. Rx Only.
Spacing of interconnects
provides balanced stress
distribution for all deformation
modes
Stent Fracture rates in studies using the INNOVA Stent
platform:
• IMPERIAL (Eluvia): 0.3% at 12M• MAJESTIC (Eluvia): 0.0% at
24M
• SuperNOVA (Innova): 2.2% at 24M
Width, Length and angles
optimized for maximum
strength
Radial Force and Flexibility
must be matched by
excellent Fracture
Resistance
EluviaTM drug-eluting stent: stent architecture
Balanced geometry designed for even stress distribution and
optimal radial strength
-
PI-
54
99
02
-AF
Jun
r20
19
• Active Polymer Layer (PTx, PVDF-HFP)– Controls Release of
Paclitaxel
o Diffusion-controlled low-dose elution over time
• 0.167µg PTx/mm2 stent surface area
• Primer Layer (PBMA)– Promotes Adhesion of Active Layer to
Stent
• Conformal Coating for Both Layers
Eluvia Dual-Layer Coating Design
Boston Scientific Data on File.
Stent
PBMA Primer Layer
Paclitaxel/PVDF-HFP Active Layer
-
PI-
54
99
02
-AF
Jun
r20
19
Polymer Selection: PVDF-HFP on PBMA
Biocompatible
PROMUS polymer:
PBMA-PVDF
• 20k clinical patients studied
• Over 10M WW implants
Durable
Durable coating during
deployment/fatigue testing
Tunable
Time
Dru
g R
elea
se
Ability To Tune Drug Release
Dep
loy
Forc
eBPolymer A DC E
Deployable
BSC evaluated multiple biostable & biodegradable
polymers
Boston Scientific Data on File.
-
PI-
54
99
02
-AF
Jun
r20
19• Drug release from the Eluvia system is sustained over
time
o >90% of drug is released at 1 year
• Drug release coincides with the restenotic cascade
Based on pre-clinical PK analysis. Data on file at Boston
Scientific.
*Dake MD, et al. J Vasc Interv Radiol. 2011;22(5):603-610.
*
Sustained Drug Release
-
PI-
54
99
02
-AF
Jun
r20
19
aSimulated use in a tortuous vessel model under clinically
relevant flow conditions.
Device sizes for particulates testing: 6mmx120mm stents,
6mmx80mm balloons. BSC Data on file.Data from ELUVIA, Zilver PTX,
Lutonix, Stellarex and IN.PACT DFUs. Abbreviations: DCB,
drug-coated balloon; DES, drug-eluting stent.
Paclitaxel-Eluting Paclitaxel-Coated
ELUVIA DESZilver PTX
Stent
DCB
IN.PACT Lutonix Stellarex
Biostable Polymer ✓
Excipient ✓ ✓ ✓
Amorphous Coating Morphology
✓ ✓
Paclitaxel Dose Density(µg/mm2)
0.167 3 3.5 2 2
Total Dose(6 mm x 120 mm)
409 µg 1103 µg 8448 µg 4500 µg 4721 µg
Diffusion-Controlled Elution ✓
Particulate Countsa
(≥10µm size)1381 11,928 567,432 210,320 193,968
Eluvia Differs from Peripheral Paclitaxel-Coated
Technologies
-
PI-
54
99
02
-AF
Jun
r20
19
IMPERIALPharmacokinetics Sub-study (N=13)
• All patients treated with Eluvia
• Plasma paclitaxel measured at 10 min, 30 min, and 1, 2, 3, 4,
6, 12, 24, 48 hours post-implant.
• Plasma paclitaxel unquantifiable (
-
PI-
54
99
02
-AF
Jun
r20
19
Treatment Difference for Primary Patency
Primary patency defined as duplex ultrasound PSVR ≤2.4, in the
absence of clinically-driven target
lesion revascularization or bypass of the target lesion, as
assessed by the DUS core lab.
Superior primary patency forEluvia vs Zilver PTX
Effectiveness I Primary Patency at 12 Months
Eluvia
(N=309)
Zilver PTX
(N=156)
77.5%
(110/142)
Δ
(95% CI)p value
86.8%
(243/280)
9.3%
(1.4%, 17.3%)0.0144
Gray WA, Lancet 2018.
IMPERIAL Trial: A global randomized controlled multi-center
trial with 2:1 randomization of the Eluvia™ Drug-
Eluting Stent against Cook Medical’s Zilver™ PTX™ Stent,
single-blind, non-inferiority design; independent core
lab adjudication. Superiority determined in a post hoc analysis
that was specified prior to unblinding. 12-Month
Primary Patency rate of 86.8% in the Eluvia arm vs. 77.5% in the
Zilver PTX arm (p-value = 0.0144).
-
PI-
54
99
02
-AF
Jun
r20
19
Effectiveness I Primary Patency at 12 Months
Kaplan-Meier Analysis of Primary Patency
Primary patency defined as duplex ultrasound PSVR ≤2.4, in the
absence of clinically-driven target
lesion revascularization or bypass of the target lesion, as
assessed by the DUS core lab.Gray WA, LINC 2020.
-
PI-
54
99
02
-AF
Jun
r20
19
Significant reduction TLR with Eluvia DES at 2 years
Circulatory System Surgery Devices Panel June 20, 2019 Boston
Scientific Presentation.BSC Data on File. As-treated ELUVIA and PTx
Control data from IMPERIAL RCT. FDA PTA reference based on FDA
Executive Summary (median of PTA arms). Abbreviations: DES,
drug-eluting stent; TLR, target lesion
revascularization; PTx, paclitaxel.
IMPERIAL outcomes at 2 Years
No significant primary patency at 2 years
-
PI-
54
99
02
-AF
Jun
r20
19
Primary Patency at 24 Months (Eluvia Treatment Arm)
-
PI-
54
99
02
-AF
Jun
r20
19
IMPERIAL with a clinically relevant
comparator contributes level 1 evidence to
support the use of DES to treat LEAD
IMPERIAL supports the effectiveness of
the longer paclitaxel elution profile of the
Eluvia stent in preventing restenosis while
maintaining similar safety to a
contemporary comparator.
IMPERIAL conclusions
Gray W, Lancet, 2018
-
PI-
54
99
02
-AF
Jun
r20
19
IMPERIALMulticenter, RCT 2:1(Eluvia : ZilverTMPTXTM)
N = 465 2Y follow up complete
MAJESTICMulticenter, single-arm(Eluvia)
N = 57 3Y follow up complete
EMINENTMulticenter, RCT 2:1(Eluvia : BMS)
N = 750 Enrolling
REGALMulticenter registry(Eluvia)
N = 500 Enrolling
SPORTS*Multicenter, RCT 1:1:1 (Eluvia:DCB:BMS)
N = 222 Enrolling
SAVALMulticenter, RCT 2:1(SAVAL : PTA) & single-arm
N = 201 & N = 100
Enrolling
BSC PI Drug-Eluting Stent Clinical Program
-
PI-
54
99
02
-AF
Jun
r20
19
Clinical Study Overview: EMINENT
Title A Randomized Trial Comparing the ELUVIA™ Drug-Eluting
Stent versus Bare Metal Self-Expanding Nitinol Stents in the
Treatment of Superficial Femoral and/or Proximal Popliteal
Arteries
Coordinating Principal Investigators
Prof. Yann Goueffic, Nantes, France
Prof. Giovanni Torsello, Münster, Germany
Objective To confirm superior effectiveness of the ELUVIA
Drug-Eluting Vascular Stent System (ELUVIA Stent) for treating
Superficial Femoral Artery (SFA) and/or Proximal Popliteal Artery
(PPA) lesions up to 140 mm in length when compared against bare
metal stents, and collect additional data including health
economics data.
Study Design Prospective, multi-centre, single-blind,
superiority trial (RCT)Randomized 2:1 (Eluvia : Self Expanding
BMS)*Powered for 10% Primary Patency superiority*
Subjects 750 subjects to receive treatment Total lesion length
(or series of lesions) ≥ 30 mm and ≤140 mmRutherford 2-4Stenosis
≥70% by visual angiographic assessment
EMINENT Clinical Study
CAUTION: The law restricts these devices to sale by or on the
order of a physician. Rx Only.
Enrollment Complete
-
PI-
54
99
02
-AF
Jun
r20
19
IMPERIALMulticenter, RCT 2:1(Eluvia : ZilverTMPTXTM)
N = 465 2Y follow up complete
MAJESTICMulticenter, single-arm(Eluvia)
N = 57 3Y follow up complete
EMINENTMulticenter, RCT 2:1(Eluvia : BMS)
N = 750 Enrolling
REGALMulticenter registry(Eluvia)
N = 500 Enrolling
SPORTS*Multicenter, RCT 1:1:1 (Eluvia:DCB:BMS)
N = 222 Enrolling
SAVALMulticenter, RCT 2:1(SAVAL : PTA) & single-arm
N = 201 & N = 100
Enrolling
BSC PI Drug-Eluting Stent Clinical Program
-
PI-
54
99
02
-AF
Jun
r20
19
Clinical Study Overview: REGAL
Title A Real World Evaluation of ELUVIA™ Drug-Eluting stent in
All-Comers Superficial Femoral Artery and Proximal Popliteal Artery
Disease
Primary Investigator Prof Carlo Setacci, Siena, Italy
Objective Collect additional data including health economics
data to support the use of the ELUVIA Drug-Eluting Vascular Stent
System for treating Superficial Femoral Artery (SFA) and/or
Proximal Popliteal Artery (PPA) lesions
Study Design Prospective, multi-centre, single-arm, open-label
registry
Subjects 500 subjects at up to 30 study centres in up to 10 EU
countries• Stenotic, restenotic or (re)occluded lesion(s) in the
femoro-popliteal arteries suitable for endovascular
treatment
Primary Effectiveness Endpoint
Primary patency • Freedom from more than 50% stenosis based on
PSVR ≤ 2.4• Assessed by duplex ultrasound (DUS) at 12 months
post-procedure
Primary Safety Endpoint Major Adverse Event (MAE) rate defined
as:• All cause death through 1 month• Target limb major amputation
through 12M• Target lesion revascularization (TLR) through 12M
Follow-Up Index, 1m, 6m, 1-year (primary endpoint), and 2-years
(standard of care)
REGAL Clinical Study Enrolling
-
PI-
54
99
02
-AF
Jun
r20
19
IMPERIALMulticenter, RCT 2:1(Eluvia : ZilverTMPTXTM)
N = 465 2Y follow up complete
MAJESTICMulticenter, single-arm(Eluvia)
N = 57 3Y follow up complete
EMINENTMulticenter, RCT 2:1(Eluvia : BMS)
N = 750 Enrolling
REGALMulticenter registry(Eluvia)
N = 500 Enrolling
SPORTS*Multicenter, RCT 1:1:1 (Eluvia:DCB:BMS)
N = 222 Enrolling
SAVALMulticenter, RCT 2:1(SAVAL : PTA) & single-arm
N = 201 & N = 100
Enrolling
BSC PI Drug-Eluting Stent Clinical Program
-
PI-
54
99
02
-AF
Jun
r20
19
Clinical Study Overview: SPORTS
Title Sequent Please Drug Coated Balloons Versus Primary Stent
Application in Long SFA Lesions
Primary Investigator / Sponsor
Gunnar Tepe, MD - RoMed Klinikum Rosenheim, Germany
InnoRa GmbH
ObjectiveCompare angiographic and clinical outcome of PTA with a
paclitaxel coated balloon versus nitinol stent (paclitaxel-eluting
or bare metal) with regard to restenosis development
Study Design Prospective, multicenter, RCT 1:1:1 (Eluvia DES:
SeQuent Please PCB : Nitinol stent)
Subjects
Up to 222 patients
• Rutherford stage 2-4
• Occlusion or stenosis ≥70% of diameter and ≥13 cm length in
the SFA and/ or PI-segment of popliteal artery
Investigational Centers Up to 11 centers in Germany
Primary EndpointPercent diameter stenosis at 1 year post
intervention in successfully treated patients by quantitative
angiography
These investigator-sponsored studies are supported by grant
funding from Boston Scientific. Boston Scientific is not
responsible for the collection, analysis or reporting of these
studies which remain the sole responsibility of the investigators.
Information for the use in countries with applicable product
registrations. CAUTION: The law restricts these devices to sale by
or on the order of a physician. Rx Only.
ClinicalTrials.gov Identifier: NCT03332264
SPORTS Enrolled
-
PI-
54
99
02
-AF
Jun
r20
19
Prof. Yann GouëfficDepartment of vascular surgery and
endovascular surgery
Goupe Hospitalier Paris Saint Joseph, France.
Insights on ELUVIA from the
IMPERIAL-trial and beyond: When
to prefer a stent-based approach?