Embed Size (px)
Citation preview


INSTRUCTION TO AUTHORS
“People’s Journal of Scientific Research” is an official journal of People’s Group, whose purpose is to publish research papers, shortcommunication, review articles including book review and informative article on all scientific subjects including Medical & Dentalscience, Medical education, Nursing & Paramedical. The journal will be published twice a year (Jan & July).The Editor, reserves the right to improve on style, grammar & make corrections in the manuscript accordingly. The size of manuscript(including tables, references & figures/ photograph) will be limited to four printed pages.
· Manuscript be submitted in duplicate with two sets of illustration, photographs, tables.· Use one side of A4 white bond paper with margins of atleast 2.5 cm on each side.· Double – space throughout including title page, abstract, key words, text, acknowledgement, references, figure/photo-
graphs, legends and tables. Use atleast 12 point font size.· Manuscript submitted should also be accompanied with an electronic copy on CD (Rewritable).
Guide Lines for Manuscript Preparation1. Title Page should contain: concise and informative title, Name(s) of the author(s) with initials and surname, name of the
department, Institution & complete address with telephone number of the corresponding author.2. Abstract should not be more than 300 words & should be provided on a separate sheet. It should present the most important
results stating background, methods, results & conclusion.3. Key words (4 to 6).4. Introduction – should state purpose of study & give brief review of pertinent literature. Cite only those references that are
essential to justify the purpose of study.5. Materials & Methods – should follow the introduction & should provide enough information to permit repetition of work/
project, giving how the study was designed, carried out and data were analyzed. State whether study was approved by ethicalcommittee or not. Describe statistical methods used with required detail. Give actual p-values, define statistical terms,symbols and abbreviations.
6. Result section should describe the outcome of study giving relevant data. Avoid repeating in the text all the data depicted intables or illustrations: Tables (numbered in roman numerals) & illustration (Numbered in Arabic Numerals) should beprepared on separate sheets with headings or legends. Minimum size of illustration should be 8 x 10 cm & top of figureshould be marked on a label pasted on its back indicating number of figure, Author’s name & left side of figure. Cite thetables/ figures in the text at appropriate place.
7. Discussion ordinarily should not be more than 1/3 of total length of manuscript and should include summary of majorfindings, their relationship to other similar studies and publications of these findings in future research.
8. References - It should include only those publications which are mentioned in the text & must be arranged alphabetically.a. Papers published in journal / periodicals: Authors surnames followed by initials of first names; full title of paper; full name of journal; year of publication, volume/ issue (in Arabic Numerals) & first & last page numbers.b. When writing a reference in text the surname of the author with year in bracket should be given. If there are two authors, the surnames of both should be given & if there are more than two authors, then surname of first author followed by “et al”.eg. Rocs, D.B. Congenital anomalies associated with thoracic outlet syndrome. American Journal of Surgery, 1976; 132:771-778.c. Books: Authors surnames followed by initials of first name; full title of the books; In: name of chapter (if any); Editions & volume number; Name & Domicile of Publishers; Year of Publication; PP ( Page no. first & last page) eg. Weiner JS:Human Ecology. In: Human Biology, an introduction to human evolution, variation & growth. W.A. Harrison, J.S. Weiner & N.A. Barnicat (eds), Ist edition, Oxford University Press, Oxford ; 1964, PP 401-508.
9. The first author will receive five reprints of the article and a copy of the Journal.10. All manuscripts must be accompanied by the following statement:
“In consideration of PJSR accepting the manuscript in review, undersigned author (s) hereby transfer (s), assign, (s), orotherwise convey (s) all copyright ownership to PJSR in the other events that the same work may be published by PJSR. Theauthor (s) warrants that the article is original, is not under consideration by any other journal and has not been previouslypublished and the takes responsibility for the content.Furthermore, I/we warrant that all investigations reported in the publication were conducted in conformity with therecommendations from the Declaration of Helsinki and the International Guiding Principles for Biomedical Research involvinganimals. That the Ethical Committee clearance has been obtained for experiment on animals or trial involving human beings.”My work is a part / not a part of dissertation.Title of the paper:
Author’s name (s) with signature & date in order of appearance in manusent.
Article (s) should be sent to Dr. G.S. Longia, Editor, PJSR, Prof. & Head, Department of Anatomy,People’s Dental Academy, Bhanpur, Bhopal – 462010, Ph. No. 0755 4005366 (Office), E-mail :[email protected]

PEOPLE’S JOURNAL OF SCIENTIFIC RESEARCH
Chief EditorDr. G.S. Longia
Associated Editors Editorial Assistance
Dr. Sheela Longia Dr. Sangeeta Jain Mr. Atul Kashyap (Website)Dr. Sanjeev Tyagi Dr. S. Tamaskar Dr. L.S. Kot (Biostatics)
Advisory Board
Mr. Arun Gurtoo Capt. Ruchi VijaywargiaDr. G.C. Dixit Dr. P.R. SureshDr. M.K. Gupta Dr. Mukul TailangDr. V. W. Deshkar Lt. Col. (Retd) K. Prasad
Editorial Board
Dr. S. Agarwal Dr. Ashok MhaskeDr. S.D. Shukla Dr. Saroj GuptaDr. V.K. Bhardwaj Dr. P.K. RoyDr. Ajay Bhambal Dr. S.V. BhagwatDr. Surendra Agarwal Dr. Shubhangi MhaskeDr. Preeti Nair Dr. Parimala TyagiDr. Amitabh Kallury Dr. Sheetal HungundDr. S.S. Sandhu Mr. Bhaskar GuptaMrs. S. Johnson
Volume 1 July 2008

If I had the choice of educating a boy or a girl, I would educate the girl. If you educate a boy,you educate one, but if you educate a girl, you educate a generation.- Brigham Young
Education is the kindling of a flame, not the filling of a vessel.- Socrates
Education is a crutch with which the foolish attack the wise to prove that they are not idiots.- Karl Kraus
Education is a progressive discovery of our own ignorance.- Will Durant





Contents Vol 1 - July 08
Research Article
Conventional Dacryocystorhinostomy Versus Endonasal Dacryocystorhinostomy -A Comparative StudyS Gupta, R Goyal, AS Thakur & H Singh. .................................................................................................... 1
Cytogenetics in Recurrent AbortionsA.S. Mangalgiri & S.A. Pathak .................................................................................................................... 5
Antidiabetic Activity of Alcoholic Extract of Cinnamomum zeylanicum Leaves in Alloxon InducedDiabetic Rats.Mukul Tailang, Bhaskar K Gupta & Amirish Sharma.................................................................................. 9
Molecular Bases of –Thalassaemia in the Thalassaemic Population of Bhopal.C.B.S. Dangi, N.C. Sharma, R. Mishra & M. Sajid.................................................................................... 12
Case Report
Gastric Volvulus Due to Splenomegaly - A rare Entity.A Mhaske........................................................................................................................................................ 15
Servelle-Martorell Syndrome with Extensive Upper Limb involvement:A case ReportR Gupta & N Bhardwaj ............................................................................................................................... 18
Methemoglobinemia Mimics Complicated MalariaS Sarkar & D Sarkar ....................................................................................................................................... 22
Endodontic Enigma – Mandibular Second Premolar with Three Root Canals: AS Tyagi, KP Arjun Das & SV Bhagwat ....................................................................................................... 24
Thoraco-Abdominal Ectopia CordisAshwin V Apte ............................................................................................................................................. 27
Review Article
Clinical Anatomy of the Vocal CordA S Mangalgiri, R Razvi & G S Longia ....................................................................................................... 30
Oral submucous fibrosis - Current Concepts in EtiopathogenesisM K Gupta, S Mhaske, R Ragavendra & Imtiyaz ........................................................................................ 34
Informative Article
Improving quality of our life through biotechnologyS S Sandhu & R Thakur .............................................................................................................................. 40

The Hippocratic Oath
(Original Version)I SWEAR by Apollo the physician, AEsculapius,
and Health, and All-heal, and all the gods and goddesses,that, according to my ability and judgement, I will keep thisOath and this stipulation.
TO RECHON him who taught me this Art equallydear to me as my parents, to share my substance with him,and relieve his necessities if required; to look up his offspringin the same footing as my own brothers, and to teach themthis art, if they shall wish to learn it, without fee or stipulation;and that by precept, lecture, and every other mode ofinstruction, I will impart a knowledge of the Art to my ownsons, and those of my teachers, and to disciples bound by astipulation and oath according the law of medicine, but tonone others.
I WILL FOLLOW that system of regimen which,according to my ability and judgment, I consider for thebenefit of my patients, and abstain from whatever isdeleterious and mischievous. I will give no deadly medicineto any one if asked, nor suggest any such counsel; and in likemanner I will not give a woman a pessary to produce abortion.
WITH PURITY AND WITH HOLINESS I will passmy life and practice my Art. I will not cut persons laboringunder the stone, but will leave this to be done by men whoare practitioners of this work. Into whatever houses I enter, Iwill go into them for the benefit of the sick, and will abstainfrom every voluntary act of mischief and corruption; and,further from the seduction of females or males, of freemenand slaves.
WHATEVER, IN CONNECTION with myprofessional practice or not, in connection with it, I see orhear, in the life of men, which ought not to be spoken ofabroad, I will not divulge, as reckoning that all such shouldbe kept secret.
WHILE I CONTINUE to keep this Oath unviolated,may it be granted to me to enjoy life and the practice of theart, respected by all men, in all times! But should I trespassand violate this Oath, may the reverse be my lot!
The Hippocratic Oath
(Modern Version)I SWEAR in the presence of the Almighty and
before my family, my teachers and my peers that accordingto my ability and judgment I will keep this Oath andStipulation.
TO RECKON all who have taught me this artequally dear to me as my parents and in the same spirit anddedication to impart a knowledge of the art of medicine toothers. I will continue with diligence to keep abreast ofadvances in medicine. I will treat without exception all whoseek my ministrations, so long as the treatment of others isnot compromised thereby, and I will seek the counsel ofparticularly skilled physicians where indicated for thebenefit of my patient.
I WILL FOLLOW that method of treatment whichaccording to my ability and judgment, I consider for thebenefit of my patient and abstain from whatever is harmfulor mischievous. I will neither prescribe nor administer alethal dose of medicine to any patient even if asked norcounsel any such thing nor perform the utmost respect forevery human life from fertilization to natural death andreject abortion that deliberately takes a unique human life.
WITH PURITY, HOLINESS ANDBENEFICENCE I will pass my life and practice my art.Except for the prudent correction of an imminent danger, Iwill neither treat any patient nor carry out any research onany human being without the valid informed consent ofthe subject or the appropriate legal protector thereof,understanding that research must have as its purpose thefurtherance of the health of that individual. Into whateverpatient setting I enter, I will go for the benefit of the sickand will abstain from every voluntary act of mischief orcorruption and further from the seduction of any patient.
WHATEVER IN CONNECTION with myprofessional practice or not in connection with it I may seeor hear in the lives of my patients which ought not be spokenabroad, I will not divulge, reckoning that all such shouldbe kept secret.
WHILE I CONTINUE to keep this Oathunviolated may it be granted to me to enjoy life and thepractice of the art and science of medicine with the blessingof the Almighty and respected by my peers and society, butshould I trespass and violate this Oath, may the reverse bymy lot!

People’s Journal of Scientific Research 1 Vol 1 - July 08
Research Article
Conventional Dacryocystorhinostomy Versus EndonasalDacryocystorhinostomy -A Comparative StudySaroj Gupta, Rashmi Goyal, A.S.Thakur, Harpal SinghDepartment of Ophthalmology, People’s College of Medical Sciences and Research Center, Bhanpur, Bhopal-462010 (MP)
Abstract:The objective of present study was to compare the results of endonasal endoscopic dacryocystorhinostomy and
external dacryocystorhinostomy. It was a prospective non-randomized study. Forty consecutive patients having complaintsof watering with complete naso lacrimal duct obstruction were selected for the study. Dacryocystography was done in allthe cases. Selection of type of operation was left to the patient’s choice. All patients had preoperative counseling and boththe procedures were explained in detail with their advantages and disadvantages. Twenty patients underwent endonasaldacryocystorhinostomy and twenty had external dacryocystorhinostomy Silicon intubation was done in all cases ofendonasal dacryocystorhinostomy for three months after surgery. The final follow-up was done at 12 months after surgery.The patency of lacrimal passage was confirmed by syringing and patients were questioned about their symptoms. Therewas no significant difference in the results of both surgeries. The complication rate in both groups was almost equal. Thuswe came to the conclusion that these two different dacryocystorhinostomy techniques are acceptable alternatives.
Key Words:Chronic dacryocystitis, External dacryocystorhinostomy, Endonasal endoscopic dacryocystorhinostomy Silicon intubation.
Introduction:A persistent symptomatic naso lacrimal duct
obstruction is a very common affection sparing nospecific age group. Many surgeries have beenadvocated for this malady starting fromdacryocystectomy to dacryocystorhinostomy (DCR)with placements of various implants and tubes. StillDCR is the most accepted procedure today. It can bedone with external (Ex) or endonasal (En) access. Thebasic indication is same in all cases and either routecan be used.
ExDCR was first described by Toti in 1904and is the most widely practiced procedure. The adventof the nasal endoscopes brought fresh considerationto lacrimal sac surgery. It became possible toapproach the operation area from nasal side, thereby,avoiding facial scarring and unnecessary dissection ofboth orbicularis oculi and orbital periosteum. Thus,endoscopic surgery provided a new alternative for thetreatment of naso-lacrimal duct obstruction. Thisapproach was proposed by Caldwell as farback as 1893and developed by West (1910). In 1989 Mc Donogh—————————————————————Correspondence Author: Dr. Saroj Gupta, Department of Ophthalmo-logy, People’s College of Medical Science and Research Center,Bhanpur, Bhopal-462010 (MP)Phone: 0755-2420999, 9926550364E-mail.: [email protected]
& Meiring did first endoscopic transnasal DCR. Thereis considerable difference in opinion regardingsuccess rate of ExDCR and EnDCR. This study wascarried out to compare the results of External DCRwith Endonasal DCR. (Tarbet & Custer, 1995; Eloyet al, 1995; Nalgirkar & Sulache, 2005; Hartikainenet al, 1998). The aim of present study was to comparethe success rate of EnDCR with ExDCR.
Material and Methods:We performed a clinical prospective study
of 40 patients with diagnosis of naso- lacrimal ductobstruction admitted in our hospital from January ‘06to December ‘07. Preoperatively a detailedophthalmic and ENT examination was carried out torule out any other coexisting nasal pathology.Preoperative investigations included a completeheamogram, blood sugar, bleeding and clotting timeetc. Dacryocystography was done in all cases andthose having good lacrimal sac outline withobstruction in naso lacrimal duct were selected forthe study.
Selection of type of operation was left to thepatient’s choice. All patients had preoperativecounseling and both the procedures were explainedin detail with their advantages and disadvantages. Atotal of 20 patients were enrolled by simple

People’s Journal of Scientific Research 2 Vol 1 - July 08
Conventional Dacryocystorhinostomy Versus --------- S Gupta, R Goyal, AS Thakur & H Singh.
randomization in the ExDCR group and 20 patientsin the EnDCR group. There was predominance offemale over male patient (31:9) and age ranged from5 to 65 years.
Table I: Showing age distribution.
Age in years No. of cases (5 to 65) ExDCR EnDCR 1-10 1 1 11-20 - - 21-30 4 6 31-40 5 4 41-50 7 8 51 & above 3 1 Total 20 20
Table II: Showing sex distribution.
Group Male Female Total ExDCR 5 15 20 EnDCR 4 16 20 Total 9 31 40
Table III: Showing clinical picture of chronic dacryocystitis. S. No. Clinical picture No. of cases 1 Persistent watering 11 2 Mucopurulent regurgitation 17 3 Swelling in sac area (mucocoel) 8 4 Lacrimal fistula 4
Surgical Procedure- A. External DCR:
Surgery was performed under local anesthesiawith sedation, if required. Incision was taken overanterior lacrimal crest. Medial palpebral ligament wasidentified and orbicularis oculi was separated.Reflection of peiosteum and dissection of lacrimalsac from lacrimal fossa was done. Sac was excised tomake ‘H’ shaped anterior and posterior flaps. Bonyosteum of sufficient size was made with bone punch.Nasal mucosa was cut to make anterior and posteriorflaps. Subsequently anterior to anterior and posteriorto posterior flaps were sutured with 2 to 3 interruptedsutures by 6-0 vicryl.
B. Endonasal DCR: Surgery was performed preferably, under localanesthesia. In children and uncooperative patientsgeneral anesthesia was used. Nasal cavity was packed
with gauge soaked in 4% xylocain with 1:100,000adrenaline, 15 minutes before the procedure. Themucosa anterior to uncinate process was infiltratedwith 2% xylocain with 1:100,000 adrenaline.
A 300 rigid endoscope was used. Using thesickle knife a rectangular cuff of mucosa of 10mm x5mm just anterior to superior half of the uncinateprocess was incised. The mucosal cuff was thenelevated with a periosteal elevator and removed usinga pair of cutting forceps. The frontal process ofmaxilla and the very thin lacrimal bone is thenidentified. A 2 mm Kerrison punch was used to nibbleaway the thick bone at the frontal process of themaxilla. The bone removal was then continuednasally to expose the lacrimal sac. Lacrimal probingwas done to tent the medial wall of sac. The sac wasthen slit open with an angled knife. The medial wallof sac was then removed with a tissue punch.Syringing was done with saline and methyline blueto confirm the free flow and patency.
As a routine bicanalicular silicone intubationwas performed in EnDCR cases. A 24-25 gauge probealong with 30cm long silicon tube was used.
The probes are passed through the upper andthe lower canaliculi and through the lacrimal windowinto the nasal cavity. The two ends of the tube arethen tied together and sutured with 6-0 prolene suture.The excess length of tube is then cut. The tube wasremoved 6-8 weeks after the surgery depending uponthe patients comfort level.
As post-operative medica tion, nasaldecongestants and saline douching of the nasal cavityalong with topical antibiotic drops were given. Nasaldrops were given for 6 weeks to reduce crusting insidethe nose. The patients were asked to report after at2-3 weeks for endoscopic removal of crusts aroundthe lacrimal window. All patients of both the groupswere followed twice a week for 4 weeks and thenafter 3 months, 6 months and 1 year.
Results:Both the study groups were evaluated after a
period of 12months by sac syringing andsymptomatology of the patients (Table-IV). Patientshaving patent sac were found to be fully satisfied(ExDCR -95%, EnDCR-90%) while patients havingpartial block and clear fluid regurgitation weresymptomatically relieved and were also found to besatisfied (ExDCR -95%; EnDCR-95%). Patients with

People’s Journal of Scientific Research 3 Vol 1 - June 08
Complications:ExDCR - Hypertrophied external scar -1 - Closure of Osteum-1
EnDCR - Nasal synechia formation-1 (Tackled successfully as OPD procedure)
- Granulation at the ostium with narrowing-1
Discussion:Dacryocystitis is a very common affection
sparing no specific age group. Obstruction of naso-lacrimal duct can be approached either externally byan ophthalmologist or endonasally by the rhinologistor an ophthalmologist. The success rate of ExDCR hasbeen mentioned as 80% to 99% by Hartikainen et al,(1998). As mentioned earlier, EnDCR offers distinctadvantages over ExDCR. In our study the success rateof endonasal DCR was 90% after a single procedureand 95% after revision procedure, which was equal toExDCR. The success of an EnDCR is completelydependent on a thorough knowledge of the intranasalanatomy, experience of surgeon and careful operativetechniques. The success rate of both the procedure iscomparable.
Advantages of EnDCR over ExDCR:There is no facial scar. Physiological lacrimal
pump mechanism is persevered. Less operative time isrequired. Medial canthal ligament remains intact.Patient can be ambulated early. There is minimal bloodloss. If there is blockage or narrowing of ostium it canbe dealt with as OPD procedure. It is easy and lesspainful. It allows some common intranasal causes of
ExDCR failure to deal with concomitantly like DNS,nasal polyp, hypertrophied middle turbinate etc.More superior technique for revision cases.
Disadvantages of EnDCR:EnDCR needs sophisticated instruments.Thorough knowledge of the intranasal anatomyis must for an Ophthalmologist. Longer learningcurve.
Conclusion:A persistent nasolacrimal duct obstruction
can be treated with DCR by external or endonasalroute. The external route seems better in terms oflearning curve and cost of equipment. In our study,the success rate of EnDCR was 90% after a singleprocedure and 95% after revision procedure whichwas equal to ExDCR. This indicates that these twodifferent DCR techniques are acceptable alternatives.The success rate of EnDCR can be further improvedby the use of laser or antifibrotic agents likeMitomycin-C.
In our experience EnDCR has equal successrates associated with excellent aesthetic results,without any major complications.
Bibliography:
1. Caldwell GW : Two new operations for obstruction ofthe Nasal duct. New York Medical Journal,1893;57:581-582.
2. Eloy P, Bertrand B, Martinez M, Hoebeke M, Watelet.Jamart JB : Endonasal DCR: Indications, techniquesand results. Rhinology,1995; 33 (4): 229-233.
3. Hartikainen J, Antila J, Vaipula M, Puukka P, SeppaH, Grenman R : Prospective randomized comparisonof endonasal endoscopic dacryocystorhinostomy andexternal dacryocystorhinostomy. Laryngoscope,1998; 108(12) : 1861 -1866.
4. Mc Donogh M, Meiring JH : Endoscopic trasnsnasalDCR. Journal of laryingology & Otology ,1989;103(6):585-587.
5. Nalgirkar AR, Sulache AA : Comparative evaluationof results of endoscopic DCR and external DCR.Indian journal of Otolaryingology and Head & NeckSurgery, 2005; II: 363-365.
6. Tarbet KJ, Custer PL : External Dacryocystorhinos- tomy: Surgical success, patient satisfaction and
economic cost. Ophthalmology, 1995; 102 (7): 1065-1070.
Conventional Dacryocystorhinostomy Versus ——— S Gupta, R Goyal, AS Thakur & H Singh.
mucoid regurgitation or complete block were notrelieved of their symptoms and needed fur therintervention (5%).
Table IV: Showing results and symptomatology of patients
Grade Syringing ExDCR EnDCR Satisfaction level 1 Patent 19(95%) 18(90%) Fully satisfied 2 Partial Block with Symptomatically clear fluid - 1 relieved therefore regurgitation satisfied 3 Partial Block with - 1 Not relieved of mucoid regurgitation symptoms, so not satisfied 4 Complete Block 1 -

People’s Journal of Scientific Research 4 Vol 1 - June 08
7. Toti A : Nuovo metedo conservatore di cura dellesuppurazoni croniche del sacco lacrimale(Dacrioustornostoma). Clin. Mod. Firenze, 1904;10:385-387.
Conventional Dacryocystorhinostomy Versus --------- S Gupta, R Goyal, AS Thakur & H Singh.
8. West JM : A window resection of nasal duct in casesofstenosis. Transactions of the AmericanOphthalmological society, 1910;12(Pt. 2): 654-658.
My doctor gave me six months to live, but when I couldn’t pay the bill he gave me sixmonths more.Dick Wilson
The only equipment lack in the modern hospital? Somebody to meet you at the entrance witha handshake!Martin H. Fischer
The patient does not care about your science; what he wants to know is, can you cure him?Martin H. Fischer
The art of medicine is in amusing a patient while nature affects the cure.Voltaire

People’s Journal of Scientific Research 5 Vol 1 - July 08
Cytogenetics in Recurrent AbortionsAshutosh S. Mangalgiri, *S. A. PathakDepartment of Anatomy, People’s College of Medical Sciences & Research Centre, Bhanpur, Bhopal-462010, *Department of Anatomy, IndiraGandhi Medical College, Nagpur-440018.
Abstract:The present study comprised of 40 couples with bad obstetric history. Aim of the study was to find out
whether any specific chromosomal abnormalities exist in couples with recurrent abortions. Karyotyping with‘G’ banding was done. The study revealed that, out of 80 positive metaphases, chromosomal anomalies wereseen in 3 cases (3.75%). The abnormal karyotypes seen were 45XX,t(21;21), 45XY,t(13;21), 45XY,t(15;15).These translocations are known as Robertsonian translocations, which occur between D and G group ofchromosomes.
Key Words: Recurrent abortion, Translocation, Chromosomal aberrations.
Introduction:Recurrent abortion is defined as the occurrence
of three or more consecutive spontaneous abortions.Cytogenetic study should be considered after 2spontaneous pregnancy losses have occurred(Sider et al, 1988). The importance of recurrent abortionlies not only in the number of lives lost but also thepsychic trauma, injury and occasional mortality, whichresults from this cause. If there is history of previousabortions, it is likely that chromosomal aberrations willbe found with greater frequency in them.Various chromosomal abnormalities like reciprocaltranslocation, centric fusion and mosaicism have beenreported in cases with recurrent abortions. Schmid(1962) was the first to report the chromosomalabnormality in recurrent abortion cases.
A number of investigators have establishedcorrelation between recurrent abortions and parentalchromosomal aberrations (McKay et al 1967; Kadotaniet al, 1969; Lucas et al 1972; Kim et al, 1975; Lewis &Ridler,1977;Farah et al,1975; Sant-Cassia & Cooke,1981; Portnoi et al, 1988).
The present study was designed to see theincidence of chromosomal abnormalities and whetherany specific abnormality exist in couples with repeatedspontaneous abortions.-------------------------------------------------------------Corresponding Author: Dr. Ashutosh S. Mangalgiri, Department ofAnatomy, People’s College of Medical Sciences & Research Centre,Bhanpur, Bhopal-462010,Phone: +919827547597, 0755 4061597E-mail: [email protected]
Material & Methods:The present study was carried out on 40
couples attending Gynaecology OPD, with a historyof two or more spontaneous abortions. One ml ofvenous blood was drawn for lymphocyte culture undercomplete aseptic precautions in a heparinized syringe.It was then added to the culture medium consistingof RPMI 1640 media, triple distilled water, fetal calfserum, phytohaemagglutinin M and antibiotics.
Culture bottles were incubated at 370 C for72 hrs. Colchicine was then added to the culture bottleto arrest mitosis. At 69th hour it was centrifuged at1000 RPM for 10 min. Ten ml of 0.075M(0.56%)potassium chloride (KCl) prewarmed at 370 C wasadded to the above tubes and incubated for 30 min.Recentrifugation was done at 500 RPM for 5 min.The cells were fixed by adding freshly preparedfixative i.e. methanol and glacial acetic acid in theproportion of 3:1. Successive washings with thefixative were given until a colourless material wasobtained. Two to three drops of cell suspension wasdropped with a pasteur pipette on a wet, chilled (icecold), grease free slide held at an angle ofapproximately 300 to facilitate better spreading.Giesma banding was done with Trypsin digestionmethod (Seabright, 1971).
50 mitotic spreads from more than two slideswere screened and observed from every positivesample. Two best spreads from each case werephotographed and karyotypes prepared. Individualchromosome identification and reporting was doneas per the Paris Report (1971).
Research Article

Results:The cytogenetic study was carried out in 40
couples (80 individuals). We observed the chromosomalabnormalities in only three cases. Incidence was foundto be 3.75%.
Case 1: A 37 year old female who experienced fourfirst trimester and one second trimester abortions, wasreferred for chromosomal analysis. She was found tohave a 45 XX,t(21;21) translocation. Her husband’skaryotype was normal with no abnormality.
Case 2: A 29 year old female was referred forkaryotyping with history of two first trimester abortions.Karyptype was found to be 46 XX and no anomalywas seen. Her husband’s karyotype was found to have45XY,t(13;21) translocation.
Case 3: A couple was referred for chromosomalanalysis because three pregnancies had ended in firsttrimester abortions. Karyotype of wife was normal46XX. But husband was found to have 45 XY,t(15;15)translocation.
Discussion:Chromosomal aberrations have shown to be a
major etiological factor in the occurrence ofreproductive loss and fetal wastage. Parents who arecarriers of abnormal chromosomes are at higher risk ofproducing children with chromosomal abnormalities(Carr, 1971).
This study was designed to determine thechromosomal changes in couples with recurrentabortions. The abnormal karyotypes seen in 3cases were 45 XX, t(21;21) i.e. G/G translocation;
45 XY, t(13;21) i.e. D/G translocation and 45 XY,t(15;15) i.e. D/D translocation. All thesetranslocations were Robertsonian translocations.
In case 1: 45 XX, t(21;21) i.e. G/Gtranslocation was detected in a female. In such asituation, the possible gametes will be eithernullisomic or disomic for chromosome 21.Consequently all liveborn children will have Down’sSyndrome. This is one of the very rare situation inwhich offsprings are at a risk of greater than 50% forhaving an abnormality. Lewis & Ridler (1977) founda G/G translocation in a woman with a history ofrecurrent abortion. Maeda et al (1976) demonstrated22/22 translocation carrier in a woman with recurrentabortions. Farah et al (1975) found a balancedtranslocation t(22/22) in a woman who had 15abortions.
Fig. I: Showing Karyotype 45 XX, t(21;21)
Fig. II: Showing Karyotype 45 XY, t(13;21)
Fig. III: Showing Karyotype 45 XY, t(15;15)
People’s Journal of Scientific Research 6 Vol 1 - July 08
Cytogenetics in Recurrent Abortions --------------- A.S. Mangalgiri & S.A. Pathak.

In case 2: One parental balanced D/G (13;21)translocation was observed. In a phenotypically normalindividual with a translocation between 13 and 21chromosome, six possible outcome from suchfertilization are: Down’s Syndrome, normal 13/21carrier, normal progeny, monosomy 21, monosomy 13and trisomy 21. The last three out come areincompatible with life and could result in abortion. Thiscould explain previous spontaneous abortions in thiscase. Account of recurrent abortions attributable to D/G translocation have been reported by other workers.(Kuliyev, 1969; Kim et al, 1975; Byrd et al, 1977;Sant-Cassia & Cooke,1981).
Kim et al (1975) studied a series of 50 coupleswith recurrent abortions. One woman was found to bemosaic for 45 X / 46 XX / 47 XXX. Three womenwere found to be balanced translocation carriers, withone having D/G translocation. Sant-Cassia & Cook(1981) carried out chromosomal banding studies onboth the partners of 182 consecutive couples with twoor more spontaneous abortions. Seventeen abnormalkaryotypes were detected including D/G and D/Dtranslocation with frequency of 4.67%.
In case 3: D/D translocation was detected inmale with karyotype 45 XY, t(15;15). Lucas et al (1972)described a carrier with D/D translocation involvingboth number 15 chromosomes. In such a case, a gametecould only receive both the number 15 chromosomesinvolved in translocation or none of them. Onfertilization the resulting zygote would be eithertrisomic or monosomic for chromosome 15. As neitherproduct was compatible with viability, every pregnancyended in abortion.
Accounts of recurrent abortions attributable toD/D translocation have been reported by Stenchever
et al (1968), Pergament et al (1968), Mennuti et al(1978) and Neu et al (1979).
Stenchever et al (1968) found only onepatient with a D/D translocation carrier out of 36couples and 5 individuals. Pergament et al (1968)studied 39 couples and 4 women who had experiencedrepeated spontaneous abortions and stillbirths andfound one mother with a translocation, which provedto be a D/D translocation. In present work the totalfrequency of chromosomal aberrations in coupleswith recurrent spontaneous abortions studied was3.75 %, almost similar findings were observedby Papp et al (1974), Kim et al (1975) and Sant-Cassia & Cook (1981).
The findings reported and reviewed herestress the importance of cytogenetic evaluation ofcouples with history of recurrent spontaneousabortions. Similar views are expressed by manyworkers like Pergament et al (1968), Stenchever et al(1968), Kim et al (1975), Byrd et al (1977) and Portnoiet al (1988).
Although the small sample size in this studymay not warrant generalization, the incidence ofchromosomal abnormalities reported here correlateswith that found by other research workers (Table 1 ).
Since chromosomal anomalies have beenrecognized as a major cause of early spontaneousabortions, therefore, routine chromosomal bandingstudies are recommended and justified for both thepartners, with repeated spontaneous abortions inabsence of any apparent cause.
Bibliography:
1. Byrd JR , Askew DE, Mc Donough PG : Cytogeneticfindings in fifty five couples with recurrent fetalwastage. Fertility & Sterility,1977; 28 : 246 – 250.
2. Carr DH : Chromosomes and abortion. In: Advancesin Human Genetics - 2. Harris H & Hirschhorn, Eds;Plenium Press, New York, 1971; pp.201-257.
3. Farah LMS, Nazareth HR de S, Dolinikoff M, DelascioD : Balanced homologous translocation t(22q22q) ina phenotypically normal woman with repeatedspontaneous abortions. Human Geneics, 1975;28(4):357-360.
4. Kadotani T, Ohama K, Sato H : A chromosome survey in 71 couples with repeated spontaneous abortions and stillbirths. Proceedings of the Japanes Academy,
1969; 45: 180 – 184.
People’s Journal of Scientific Research 7 Vol 1 - July 08
Cytogenetics in Recurrent Abortions --------------- A.S. Mangalgiri & S.A. Pathak.
Table 1: Showing comparison of present study with otherworkers.
Authors No. of Cases Chromosomal abnormalities in
percentage (cases) Male FemaleSchmid (1962) 10 10 5.0 % (1)Mckay et al (1967) 42 42 2.3 % (2)Pergament et al (1968) 39 43 7.4 % (6)Kadotani et al (1969) 71 71 5.6 % (8)Wilson (1969) 50 50 10.0 % (10)Lucas et al (1972) 42 42 5.9 % (5)Papp et al (1974) 14 14 3.5 % (1)Kim et al (1975) 50 50 4.0 % (4)Sant-Cassia & Cook (1981) 182 182 4.1 % (15)Present study 40 40 3.75 % (3)

5. Kim HJ, Hsu LYF, Paciuc S, Cristian S, Quintana A,Hirschhorn K : Cytogenetics of fetal wastage. NewEngland Journal of Medicine, 1975; 293: 844 – 847.
6. Kuliyev AM : D/G translocation as a possible cause ofrepeated spontaneous abortions. Genetika, 1969; 5: 129.
7. Lewis BV, Ridler MAC : Recurrent abortion associatedwith a balanced 22;22 translocation or isochromosome22q in a monozygous twin. Human Genetics, 1977; 37(1): 81-85.
8. Lucas M, Wallace I, Hirschhorn K : Recurrent abortionsand chromosome abnormalities. Journal of Obstetrics& Gynaecology of Brithish Commonwealth, 1972; 79 :1119-1127.
9. Maeda T, Ohno M, Shimada N, Nishida M, Jabo T : A22/22 translocation carrier with recurrent abortionsdemonstrated by a Giemsa banding technique. HumanGenetics, 1976; 31(2): 243-245.
10. McKay RJ (Jr) , Hodgkin WE, Witte EH : Chromosomesof couples with repeated abortions (abstr.). PediatricResearch, 1967; 1 : 208.
11. Mennuti MT, Jingeleski S, Schwarz RH, Mellman WJ :An evaluation of cytogenetic analysis as a primary toolin assessment of recurrent pregnancy wastage. Obstetrics& Gynaecology, 1978; 53: 308.
12. Neu RL, Entes K, Bannerman RM : Chromosomeanalysis in cases with repeated spontaneous abortions.Obstetrics & Gynaecology, 1979; 53: 373- 375.
13. Papp Z, Gardo S, Dolhay B : Chromosome study ofcouples with repeated spontaneous abortions. Fertility& Sterility, 1974; 25 : 713 – 717.
People’s Journal of Scientific Research 8 Vol 1 - July 08
Cytogenetics in Recurrent Abortions --------------- A.S. Mangalgiri & S.A. Pathak
14. Pergament E, Kadotani T, Sato H : Chromosomestudies in repeated spontaneous abortions andstillbirths. American Journal of Obstetrics &Gynaecology, 1968; 100: 912 – 917.
15. Portnoi MF, Joye N , Akker JVD, Morlier G, TaillemiteJL : Karyotypes of 1142 couples with recurrentabortions. Obstetrics & Gynaecology, 1988; 72 : 31 –34.
16. Sant–Cassia LJ, Cooke P : Chromosome analysis ofcouples with repeated spontaneous abortions. BritishJournal of Obstetrics & Gynaecology, 1981; 88:52 –58.
17. Schmid W : A familial chromosomal abnormalityassociated with repeated abortions. Cytogenetics, 19621: 199.
18. Seabright M : A rapid banding technique for humanchromosomes. Lancet, 1971; 2 : 971.
19. Sider D, Wilson WG, Sudduth K, Atkin JF, Kelly TE: Cytogenetic studies in couples with recurrentpregnancy loss. South Medical Journal, 1988; 81: 1521– 1524.
20. Stenchever MA, Jarvis JA, Macintyre MN :Cytogenetics of habitual abortion. Obstetrics &Gynecology, 1968; 32 : 548 – 555.
21. Willson JA.: A prospective cytogenetic study ofrecurrent abortions. Journal of Medical Genetics,1969;6:5-13.

People’s Journal of Scientific Research 9 Vol 1 - July 08
Introduction:
Diabetes-mellitus is a chronic diseasecharacterized by elevated blood glucose levels anddisturbance in carbohydrate, fat and proteinmetabolism. These metabolic abnormalities result, inpart, from a deficiency of the blood sugar-loweringhormone insulin. This deficiency in insulin results intype 1 diabetes or insulin dependent diabetes mellitus(IDDM). Type 2 diabetes or non-insulin dependentdiabetes mellitus (NIDDM) is a result of hyperglycemiacaused by overproduction of glucose at the hepatic levelor because of abnormal - cell function or insulinresistance at target cells.(Fajans et al, 1997). Currentlyavailable synthetic antidiabetic agents produce seriousside effects like hypoglycemic coma (Stephen Davis,2006) and hepatorenal disturbances (Suba et al, 2004). Moreover, they are not safe for use during pregnancy(Rahman & Zaman, 1989). Hence, the search for saferand more effective hypoglycemic agents has continued.Several investigations have been conducted related toantidiabetic activity of Cinnamomum zeylanicum bark(family Lauraceae) and have shown positive effect.Cinnamon has been reported to have remarkablepharmacological effects in the treatment ofhyperglycemia (Kar et al, 2003;Verspohl et al, 2005).
The present study was aimed to investigate theanti-diabetic activity of an alcoholic extract ofCinnamomum zeylanicum leaves in alloxon induced-------------------------------------------------------------Corresponding Author: Dr. Mukul Tailang, Principal, People’s Instituteof Pharmacy & Research Centre, Bhanpur, Bhopal-462 010 (MP)Phone: 9425648344, 0755 4005028E-mail: [email protected]
Antidiabetic Activity of Alcoholic Extract of Cinnamomum zeylanicum Leaves inAlloxon Induced Diabetic Rats.Mukul Tailang, Bhaskar K. Gupta, Amrish Sharma.People’s Institute of Pharmacy & Research Centre, Bhanpur, Bhopal-462 010 (M.P.)
Abstract:The present study was carried out to investigate the antidiabetic potential of ethanolic extract of Cinnamomum
zeylanicum leaves. Oral administration of ethanolic extract in the doses of 100, 150 & 200 mg/kg body weight to whiteWistar albino rats significantly reduced their blood sugar level in allxon induced diabetic rats under acute and sub acutestudies.
Key Words: Cinnamomum zeylanicum, Alloxon induced, Antidiabetic study, Glucose oxidase method.
diabetic rats.
Material and Method:
1. Preparation of extract: The leaves of Cinnamo-mum zeylanicum (family Lauraceae) were procuredfrom the local market of Bhopal. The dried leaveswere pulverized and passed through 40 mesh sieve.The coarse powder was extracted with 95% v/vethanol at 600 - 750 C for 48 hours. The extract wasfiltered, concentrated and dried under reducedpressure by rotating evaporator (yield 6.3%) andresidue was kept in desicators. The suspension ofethanolic extract was prepared by using 0.5% Tween-80 in saline.
2. Animal: Healthy adult male Wistar albino ratsbetween 2-3 months of age and weighing 150-200gm were used for the present study. The animals werehoused individually in polypropylene cages,maintained under standard conditions (12-hr light and12-hr dark cycle, 25±5ºC and 40-60% humidity).They were fed with standard rat pellet diet (HindustanLever Limited. Mumbai) and provided water adlibitum.
3. Induction of non-insulin dependent diabetesmellitus (NIDDM): NIDDM was induced by asingle intraperitonial injection of 150mg/kg bodyweight of alloxon monohydrate in normal salinesolution. After two weeks, the surviving rats withfasting blood glucose level of more than 200mg/dlwere considered as alloxon induced diabetic rats(Gidado et al, 2005).
Research Article

4. Experimental design for antidiabetic study:The animals were divided into six groups. Eachgroup consisted of 6 animals.Group I – Control, non-diabetic.Group II – Control, diabetic.Group III – Diabetic, treated with standard drug(Glibenclamide 10mg/kg body weight/day).Group IV, V & VI – Diabetic, treated with ethanolicextract of Cinnamomum zeylanicum leaves (100, 150& 200mg/kg body weight/day respectively) orally.
This treatment was continued for sevendays.Blood samples from the rats were collected fromthe retro orbital plexus puncture method. Fasting bloodglucose level was estimated at 0, 1, 3 & 5 hours foracute studies and on 0, 1st, 3rd, 5th & 7th day for sub-acute studies. The Blood glucose levels weredetermined by Glucose oxidase method (Varley, 1988).
Result:
The hypoglycemic effects of the ethanolicextract of Cinnamomum zeylanicum leaves on fastingblood glucose levels of diabetic rats for both acute andsub-acute studies are shown in Tables 1&2 respectively.
On single oral administration of the extract for acutestudy a significant decrease in fasting blood sugarlevel was observed at dose 150 & 200 mg/kg bodyweight. The maximum reduction in blood glucose wasobserved after 5 hr at dose 200 mg/kg body weight.In sub acute treatment, on 7th day, the extract at doseof 150 & 200 mg/kg of body weight showedsignificant reduction in blood gulucose level ascompared to that of diabetic control group.
Statistical Analysis:The statistical analysis was carried out using
the one way ANOVA, as primary test followed byDunnett’s test by graphpad Instate.
Discussion:
The present study has detected theantidiabetic effect of the ethanolic extract ofCinnamomum zeylanicum leaves in alloxon induceddiabetic rats. Intraperitonial injection of alloxonmonohydrate caused diabetes mellitus in adult maleWistar albino rats. In acute treatment, the ethanolicextract was administered to over night fasted diabeticrats. A decline in blood sugar level was observed after1 hr, and the maximum effect was seen after 5 hr.
People’s Journal of Scientific Research 10 Vol 1 - July 08
Antidiabetic activity of alcoholic extract of Cinnamomum zeylanicum ------- Mukul Tailang, Bhaskar K Gupta & Amirish Sharma.
Table I (a) : Effect of ethanolic extract of Cinnamomum zeylanicum leaves on fastingblood glucose level of alloxan-induced diabetic rats (Acute studies).
Group Blood Gulucose level mg/dl (Mean ± SD) n = 6 0hr 1hr 3hr 5hr
I 104.59±1.41 104.51±1.40 102.81±1.35 101.23±1.36 II 220.54±1.42 218.19±1.52 215.93±1.53 214.18±1.52 III 218.19±1.61 215.59±1.52 204.79±1.69 197.32±1.81 IV 223.32±1.25 221.51±1.68 214.34±1.24 202.14±1.42 V 217.41±1.52 211.59±1.65 203.47±1.71 195.31±1.58 VI 222.32±1.52 217.37±1.65 201.53±1.85 190.22±1.91
Table I (b) - Showing satistical significance between control diabetic and treated groups (Acute studies).
Group One way analysis of variance (ANOVA) n = 6 0hr 1hr 3hr 5hr
II vs III (st. drug 10 mg/kg) p<0.05 p<0.05 p<0.01 p<0.0II vs IV (100 mg/kg) p<0.05 p<0.01 ns p<0.01II vs V (150 mg/kg) p<0.01 p<0.01 p<0.01 p<0.01II vs VI (200 mg/kg) ns ns p<0.01 p<0.01

In sub acute study, after oral administration ofCinnamomum zeylanicum leaves extract at dose 150 &200 mg/kg body weight, hyperglycemia was reducedapproximately by 22% and 33% respectively on 7th dayas compared to diabetic controls.
Whereas, the glibenclamide at a dose of 10mg/kg body weight reduced hyperglycemia by 30% on 7th
day.
Conclusion:The present study suggests that ethanolic extract of
Cinnamomum zeylanicum leaves posses a potentantidiabetic property as it significantly reduced thefasting blood sugar level in alloxon induced diabeticrats as compared to diabetic control group.
Long term studies of Cinnamomum zeylanicumleaves and its isolated compounds are necessary toelucidate the exact mechanism of action so as to developit as a potent antidiabetic drug.
Bibliography:
1. Fajans SS, Cloutier MC, Crowther RL : Clinical andetiological heterogeneity of idiopathic diabetes mellitus(Banting Memeoral Lecture). Daibetes, 1997;7:1112-1125.
People’s Journal of Scientific Research 11 Vol 1 - July 08
Antidiabetic activity of alcoholic extract of Cinnamomum zeylanicum ------- Mukul Tailang, Bhaskar K Gupta & Amirish Sharma.
Table II (a) : Effect of ethanolic extract of Cinnamomum zeylanicum leaves on fasting bloodglucose level of alloxan-induced diabetic rats (Sub-acute studies).
Group Blood Gulucose level mg/dl (Mean ± SD) n = 6 0day 1 day 3 day 5 day 7 day
I 104.59±1.41 104.10±1.51 103.79±1.62 103.59±1.82 105.10±1.52 II 220.54±1.42 220.32±1.58 221.30±1.65 220.71±1.58 222.31±1.69 III 218.19±1.61 202.91±1.35 185.46±1.59 163.73±1.52 152.53±2.13 IV 223.32±1.25 214.68±1.63 203.22±1.95 196.52±1.62 189.82±1.52 V 217.41±1.52 206.53±1.25 195.66±1.62 184.79±1.25 169.57±1.52 VI 222.32±1.52 206.68±1.62 186.68±1.55 162.22±1.52 148.90±1.65
Group One way analysis of variance (ANOVA) n = 6 0day 1 day 3 day 5 day 7 day
II vs III (st. drug 10 mg/kg) p<0.05 p<0.01 p<0.01 p<0.01 p<0.01II vs IV (100 mg/kg) p<0.05 p<0.01 p<0.01 p<0.01 p<0.01II vs V (150 mg/kg) p<0.01 p<0.01 p<0.01 p<0.01 p<0.01II vs VI (200 mg/kg) ns p<0.01 p<0.01 p<0.01 p<0.01
Table II(b) : Showing satistical significance between control diabetic and treated groups (Sub-acute studies).
2. Gidado A, Ameh, D.A., Atawodi, S.E : effect ofNauclea latifolia leaves aqueous extracts on bloodglucose levels of normal and alloxon-induced diabeticrats. African Journal of Biotechnology, 2005; 4 (1):91-93
3. Kar A, Choudhary BK, Bandyopadhyay NG :Comparative evaluation of hypoglycemic activity ofsome Indian medicinal plants in alloxan diabetic ratsJournal of Ethenopharmacol, 2003; 84(1):105-108.
4. Rahman Q, Zaman K : Medicinal Plants withhypoglycemic activity. Journal of Ethnopharmacol,1989;26:1-55.
5. Stephen N. Davis : Insulin, Oral hypoglycemic agentand the Pharmacology of endocrine Pancreas. In:Goodman & Gillman’s The Phamacological Basis ofTherapeutics. Laurence L. Burnton, John S. Lazo,Keith L. Parker, Eds; 11th Edn; McGraw-Hill MedicalPublishing Division, New York, 2006;pp.1613-1641.
6. Suba V, Murugesan T, Arunachalam G, Mandal SC,Sahu BP.: Antidaibetic potential of Barleria lupilinaextract in rats. Phytomed, 2004;11:202-205
7. Varley Harold : Practical clinical biochemistry. 4th Edn.; C B S Publishers & Distributors, Delhi, 1988; p 84.
8. Verspohl E.J, Katrin B, Neddermann E.: Anti-diabeticeffect of Cinnamomum cassia and Cinnamomumzeylanicum in vivo and in vitro. PhytotherapyResearch, 2005;19(3):203 - 206 .

If I had the choice of educating a boy or a girl, I would educate the girl. If you educate a boy,you educate one, but if you educate a girl, you educate a generation.- Brigham Young
Education is the kindling of a flame, not the filling of a vessel.- Socrates
Education is a crutch with which the foolish attack the wise to prove that they are not idiots.- Karl Kraus
Education is a progressive discovery of our own ignorance.- Will Durant
People’s Journal of Scientific Research 12 Vol 1 - July 08

People’s Journal of Scientific Research 13 Vol 1 - July 08
Molecular Bases of –Thalassaemia in the Thalassaemic Population of Bhopal.C.B.S. Dangi, *N.C. Sharma , **R. Mishra & M. SajidHuman Genetic Laboratory, Centre for Scientific Research and Development, People’s Group, Bhanpur, * Department of Genetics, BarkatullahUniversity, ** Department of Pediatrics, Gandhi Medical College, Bhopal.
Abstract:Beta- Thalassaemia is a group of heterogeneous recessive disorders common in many parts of the world and one
of a major haemoglobinopathy of wide occurrence in the Indian sub-continent. It is distributed to different degrees indifferent sub-populations. The treatment of this disorder is quite expensive and counseling seems to be the only way forcontrolling it. Genetic analysis for Beta - Thalassaemia disorder is carried out by Amplification Refractory MutationSystem (ARMS) technique. Blood samples of 50 cases of thalassaimia were obtained from patient attending PediatricsOPD of Gandhi Medical College & Delta Pathology laboratory, Bhopal and were tested. Out of seven common -thalassaemia mutation, IVS1 [Intra Venous Sequences] nt 5 [nucleotides] (G C)], IVS1 nt 1 (G T), Deletion 619 bp(basic pair) and Cap+1(A C) were found in population of Bhopal in 39.52%, 16.27%, 18.59%, 6.97% respectively. Earlydetection of thalassaemia is, therefore, important not only from treatment point of view, but also for the prevention bygenetic counseling.
Key Words : - thalassaemia, Central India, Mutation, Genetic counseling, Prenatal diagnosis.
Introduction:Thalassemias are the most common monogenic
gene disorders in the world. – Thalassaemia is a groupof heterogeneous autosomal recessive disorders, wherecomplete absence or reduced synthesis of – globinchain occurs in haem protein of haemoglobin. Sometimes the excessive production of – globin chainsleads to its deposition in RBC resulting in less orineffective erythropoiesis (Weatherall, 1994; Steinberet al, 2001). Patients of thalassemias present with awide variability of clinical presentation varying fromsevere forms ( - thalassaemia major) to a very mild oralmost symptom less condition. This variability isowing to the presence of a large number of geneticmodifiers affecting the disease. In last two decades over200 types of different mutations have been studiedthrough out the world (Weatherall, 1994). Patients aregenerally treated with blood transfusions and ironchelation therapy. Pharmacological therapies havevarying degrees of success depending on the geneticmodifiers of the disease present in the patients (Borgna-Pignatti et al, 2004; Telfer et al, 2006). Studiesundertaken to identify all the modifiers that affect -thalassaemia will lead to more appropriate geneticcounseling during-------------------------------------------------------------------Corresponding Author: Dr. C.B.S. Dangi, Human Genetic Laboratory,Centre for Scientific Research and Development, People’s Group, Bhanpur,Bhopal-462010 (MP)Phone: 0755 4005200 Extn. 4053, 9425013170
prenatal diagnosis and enable targeted andpersonalized treatment regimen for patients in thefuture.
Material & Methods:Blood samples of 50 cases from patients
attending Paediatrics OPD of Gandhi Medical Collegeand Delta Pathology Laboratory, Bhopal, were tested.The samples were either from confirmed cases ofThalassaemia or carrier patients of such cases seekingprenatal diagnosis. Out of 50 samples, 43 cases wereconfirmed, rest of the 7 cases remained unidentified.Genomic DNA was extracted using standard methodsfrom intravenous peripheral blood collected in EDTA-coated tubes. Complete blood count was determinedusing five part cell counter of Sysmax and HbA2 &HbF was determined by HPLC (VARIANT)manufactured by Bio Red, France. Mutation detectionwas carried out by the method of Fortina et al (1992)which is based on the combination of multiplexingand amplification refractory system. Five commonmutations were screened by four separate reactionscontaining either four normal or four mutant primers.Polymerase chain reaction (PCR) mixtures contained1 g of genomic DNA, 100mM Tris HCl (pH 8.3),50mM KCl, 100 ìM dNTP mixtures, 1.5mM MgCl2
and 0.01 % (w/v) gelatin in a total volume of 50 µl.The mixtures were heated for 5 minutes at 950C
Research Article

followed by the addition of four units of Taq DNApolymerase. Twenty five PCR cycles of 950C for 1minute and combined annealing and extension at 660 Cfor 2 minutes with the last cycle of 3 minutes at 660Cwere carried out. The - globin strip assay kit was usedto confirm the results obtained by the multiplex PCRmethod as well as detecting those mutations not coveredby the above method (Newton et al, 1989; Maggio etal, 1993). In this study, PCR amplification was carriedout using biotinylated pr imers, followed byhybridization of the PCR product to a test stripcontaining allele-specific oligonucleotide probesimmobilized as an array of parallel lines. Boundbiotinylated sequences were detected using streptavidinphosphatase and color substrate. The amplified geneswhen separated on Gel electrophoresis, seven distinctbands were obtained out of which four bands were moreprominent.
Result & Discussion:Out of seven common - Thalassaemia
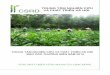
mutations confiremed by Gel electrophorosis (Shaji etal, 2003), 4 different - Thalassaemia mutations wereidentified in the present study of randomly selectedThalassaemia patients in Bhopal. They are IVS1 nt 5(G C), IVS1 nt 1 (G T), Del 619 bp. & Cap+1(A C) in 39.5%, 16.27%, 18.59 % & 6.97 %respectively in studied group (Fig.1)
A similar study was conducted in six differentstate of India (Varawalla et al, 1991; Table 1). In Punjabthe frequency of mutation was 34%, 14.9%, 15.7% and
Cap+1 (A C)
M 1 2 3 4 5 6 7
M 1 2 3 4 5 6 7
IVS1 nt 5 (G C)
M 1 2 3 4 5 6 7
M 1 2 3 4 5 6 7
IVS1 nt 1 (G T)
Del 619 bp
People’s Journal of Scientific Research 14 Vol 1 - July 08
Molecular Bases of –Thalassaemia -------- C.B.S. Dangi, N.C. Sharma, R. Mishra & M. Sajid.
3.7%. Apart from these mutation in 1.6% cases anadditional mutation -88 (C T) was also reported. InGujrat IVS1 nt 1(G C), IVSI nt 5 (G C) and 619 bpdel was detected in 16.8%, 41.1% & 25.9% casesrespectively. In Maharashtra approximately 60% ofmutations were of IVS1nt 5(G C) type. Cap+1(A C)mutation was not observed in Maharashtra andGujrat but is was observed in 6.97% cases in thepresent study. In contrast to our study in U.P. &Haryana two mutations were observed and they were-88 (C T) & 619 bp del. IVS1 nt 1 (G C) mutationwas observed in16.27 % cases in the present studywhile it was 85.9% in Tamil Nadu (Varawalla et al,1991).
The character wise analysis of the presentstudy revealed that 16.3% (7) cases were compoundheterozygous, 51.2% (22) cases were heterozygousand 32.5% (14) were homozygous variety. In anotherstudy conducted in India, revealed 60.8%hetrozygous, 32.0% & 34.0 % cases were of differenthomozygous conditions (Panigrahi et al, 2005, 2006).
Community wise analysis of mutations haveshown varying result in the present study. Mutation619 bp del was found in Sindhi community, IVS1 nt5 (G C) in Jain and Cap+1(A C) in Muslimcommunity. Population wise Punjabis have mix casesof homo and heterozygous IVS1 nt 5 (G C) mutationin 12%. Hindus too have high ratio of IVS1 nt 5(G C) mutation in 51.6%. Sindhi community showedmixed results of two mutations i.e. IVS1 nt 5 (G C)and Del 619 bp in 12.9%. Rest of the mutation wereof mixed frequency.
A study conducted on population of westBengal reflect that the case of Thalasseamia major ismost common among the religious group having intercommunity marriages as in the case of Muslims(55.26%) and in tribal people it is 29.87% (Sur &Mukhopadhyay 2006).
Name of Punjab Guj Maha- UP Haryana Tamil Bhopalmutation rastra Nadu (Pres. study)Cap+1 3.7% - - - - - 6.97%(A C)IVS1 nt 1 14.9% 16.8% 1.8% - - 85.9% 16.27%(G C)IVS1 nt 5 34% 41.1% 59.6% - - - 39.52%(G C)-88 (C T) 1.6% - - 4.9% 1.7% - -619 bp del 15.7% 25.9% 5.3% 3.3% 16.9 % 1.0% 18.57%
Table I: Showing comparative percentage of the mutation found in population of various states of India.(Varawalla et al, 1991) & Present study.
Fig.I: Mutation found in 43 patients.

Population of this region is conscious andwilling to accept prenatal diagnosis as a mean of controlof thalassaemia.
Bibliography:
1. Borgna-Pignatti C, Rigolotto S, De Stefano P, Zhao H,Capellini MD, Del Vecchio G : Survival andcomplications in patients with thalassaemia major treatedwith transfusion and deferoxamine. Haematologica,2004; 89:1187-1193.
2. Fortina P, Dotti G, Conant R, Monokian G, Pareella T,Itctchcock W, Rappaport E, Schwartz E, Surry S :Detection of the most common mutations causing -thalassaemia in Mediterraneans using a multiplexamplification refractory mutation system (MARMS).PCR Methods Applications, 1992; 2(2):163–166.
3. Maggio A, Giambona A, Cai SP, Wall J, Kan YW, ChehabFF : Rapid and simultaneous typing of hemoglobin S,hemoglobin C, and seven Mediterranean beta-thalassaemia mutations by covalent reverse dot-blotanalysis: application to prenatal diagnosis in Sicily.Blood,1993; 81(1):239–242.
4. Newton C R, Graham A, Heptinstall L E, Powell, SJ,Summers C, Kalasheker N, Smith JC, Markham AF :Analysis of any point mutation in DNA. Theamplification refractory mutation system (ARMS).Nucleic Acids Research, 1989; 17: 2503-2516.
5. Panigrahi S, Agarwal T, Gupta P, Singhal M, Pradhan M: Hemoglobin E-beta Thalassaemia: Factors affectingPhenotype. Indian Pediatrics, 2005; 42:351-352.
People’s Journal of Scientific Research 15 Vol 1 - July 08
6. Panigrahi I, Agarwal S, Pradhan M, Choudhry DR,Choudhry VP and Saxena R : Molecularcharacterization of thalassaemia intermedia in Indians.Haematologica (the hematology journal), 2006; 91(9):1279-1280.
7. Shaji VR, Eunice SE, Balasubramanian P, SrivastavaA, Chandy M : Rapid Detection of -Globin GeneMutations and Polymorp-hisms by TemporalTemperature Gradient Gel Electrophoresis. ClinicalChemistry, 2003; 49: 777–781.
8. Steinber MH, Forget BG, Higgs DR Nagel RL :Disorders of haemoglobin. In: Genetics,Pathophysiology and Clinical management. CambridgeUniversity Press, U.K. ; 2001.
9. Sur D, Mukhopadhyay SP : Prevalence of thalassaemiatrait in the state of West Bengal. Journal of IndianMedical Association, 2006; 104(1):11-15.
10. Telfer P, Coen PG, Christou S, Hadjigavriel M,Kolnakou A, Pangalou E, Pavlides N, Psiloines M,Simamonian K, Skordos G, Sitarou M, AngastiniotisM : Survival of medically treated thalassaemia patientsin Cyprus. Trends and risk factors over the period 1980- 2004. Haematologica, 2006; 91:1187-1192.
11. Varawalla N Y, Old J M, Sarkar R, Venkatesan R,Weatherall D J : Distribution and population geneticsof the Thalassaemia patients in Indian states, BritishJournal of Haematology, 1991; 78: 2421 –2424.
12. Weatherall SJ. G, Nienhuis AW, Majerus PH, VarmusH : The Molecular Bases of Blood Diseases. 2nd Edn.W. B. Saunders, Philadelphia,1994; pp.157–205.
Molecular Bases of –Thalassaemia -------- C.B.S. Dangi, N.C. Sharma, R. Mishra & M. Sajid.

Ah, great it is to believe the dream as we stand in youth by the starry stream; but a greaterthing is to fight life through and say at the end, the dream is true!- Edwin Markham
I like the dreams of the future better than the history of the past.- Patrick Henry
All our dreams can come true, if we have the courage to pursue them.- Walt Disney
Dreams are today’s answers to tomorrow’s questions.- Edgar Cayce
People’s Journal of Scientific Research 16 Vol 1 - July 08

Case Report
Gastric Volvulus Due to Splenomegaly - A rare Entity.Ashok MhaskeDepartment of Surgery,People’s College of Medical Sciences and Research Centre, Bhanpur, Bhopal. 462010 , (M.P.)
Abstract:Gastric volvulus is a rare condition which typically presents with intermittent episodes of abdominal pain. The
volvulus occurs around an axis made by two fixed points, organo-axial or mesentero-axial. Increased pressure within thehernial sac associated with gastric distension can lead to ischemia and perforation. Acute obstruction of a gastric volvulusis thus a surgical emergency.We present an unusual case of gastric volvulus secondary to tropical splenomegaly. Tropicalsplenomegaly precipitating gastric volvulus is not documented till date.
Key Words: Gastric volvulus, Tropical splenomegaly.
Introduction:Gastric volvulus is abnormal rotation of the
stomach of more than 180 degrees. It can cause closedloop obstrcution and at t imes can result inincarceration and strangulation. Berti first describedgastric volvulus in 1866; to date, it remains a rareclinical entity. Berg performed the first successfuloperation on a patient with gastric volvulus in 1896.Borchardt (1904) described the classic triad of severeepigastric pain, retching without vomiting andinability to pass a nasogastric tube. We are presentinga case of gastric volvulus secondary to huge tropicalsplenomegaly (which acted as a pendulous) with laxityof ligaments which underwent surgical repair. To thebest of our knowledge, this report is the first articleabout a gastric volvulus secondary to tropicalsplenomegaly.
Case Report:A 28 years old lady presented to the
Department of Surgery with complaints of intermittentpain in abdomen, vomiting with distension for lastseven years. She was treated by antacids multipletimes (details of specific drugs could not be gathered)but the symptoms recurred intermittently. There wasno history of fever in the past.
Since last fifteen days she had pain in theupper abdomen aggravated with nausea andintermittent vomiting of gastric contents. She reported--------------------------------------------------------------------------------------Corresponding Author: Dr. Ashok Mhaske, Professor & Head,Department of Surgery, People’s College of Medical Sciences & ResearchCentre, Bhanpur, Bhopal-462010 ( M.P.)Phone No.: 9993376700, 0755 4005241E-mail:[email protected]
to general practitioner but as symptoms persisted shewas referred to our tertiary care centre for expertopinion and management.
On examination, vital parameters andhydration was adequate with marked tenderness inepigastric region with vague lump. Her routineinvestigations were inconclusive but she did partiallyresponded to antispasmodic and antacid drugs.
Ultrasound of abdomen and Barium studiesrevealed gastric volvulus (Fig.1 & 2) withsplenomegaly for which she was taken up forabdominal exploration. Abdominal explorationconfirmed organoaxial gastric volvulus due to hugespleen. Laxity of supporting ligaments was evident;volvulus was precipitated by splenomegaly (actingas pendulous) on which rotation occurred. Nogangrenous changes were noted. Splenectomy withgastropexy was done. Post operative course wasuneventful. Histopathological report revealed tropicalsplenomegaly. She is under our follow-up and isasymptomatic.
Anatomy and Aetiology:The stomach is maintained in its normal
position by four ligaments. The lesser curvature and
Fig. I: Showing organoaxial gastric volvulus.
People’s Journal of Scientific Research 17 Vol 1 -July 08

People’s Journal of Scientific Research 18 Vol 1 - July 08
liver are joined by the gastrohepatic ligament, thegreater curvature is attached to spleen and transversecolon by the gastrosplenic and gastrocolic ligaments,and the cardia is held fixed by the phrenicoesophagealligament. Some form of ligament abnormality (extremelaxity, absence or disruption) is essential to allowrotation; the direction of rotation is determined bywhich ligaments are lax and which points remainrelatively fixed.
Fig. III: Showing splenomegaly acting a pedulous for volvulus.
Fig. IV : Showing dilated & derotated stomach after splenectomy
Discussion:Gastric volvulus (Latin volvere, to roll) is
rotation of full or part of the stomach by more than180º, which may lead to a closed-loop obstructionand possible strangulation. We report a case of gastricvolvulus secondary to splenomegaly, diagnosed onimaging and managed surgically.
Gastric volvulus can be classified on the basisof its location in reference to the diaphragm and onthe basis of the axis of rotation. Subdiaphragmatic, orprimary volvulus accounts for approximately one thirdof cases and it is not associated with diaphragmaticdefects. Supradiaphragmatic or secondary volvulusaccounts for approximately two thirds of cases and itis associated with diaphragmatic defects.
Gastric volvulus is also classified on the basisof its axis of rotation. In the more common,organoaxial volvulus, the stomach rotates on itslongitudinal axis. This axis is defined as the lineconnecting the cardia and pylorus. The greatercurvature moves from an inferior to a superiorposition. When compared with other types of gastricvolvulus, organoaxial volvulus is more commonlyassociated with strangulation. In our case though itwas organoaxial volvulus timely interventionprobably prevented strangulation.
In mesenteroaxial volvulus, the stomachrotates about a vertical axis passing through the middleof the greater and lesser curvatures. The pylorus movesanteriorly and superiorly, whereas the greatercurvature remains inferior. Mesenteroaxial volvulusis more often seen in young children and is associatedwith ligamentous laxity but not with diaphragmaticdefects (Stavros et al, 2006).
The signs and symptoms of gastric volvulusdepend on the type of volvulus (primary or secondary)and chronicity, as well as the degree of obstruction.
Chronic volvulus may be detectedincidentally on plain chest radiographs or on uppergastrointestinal studies. Symptoms and signs are notspecific and may include vague intermittent abdominalpain upper abdominal fullness etc. Our patient seemsto be of chronic type with acute superimposition.
Acute cases represent a surgical emergency.Triad of typical symptoms and signs is described byBorchardt (1904):
Severe upper abdominal pain and distentionViolent retching with an inability to vomitInability to pass a nasogastric tube into the
stomachBarium study is highly sensitive and specific.
However, the diagnosis may be missed in cases ofintermittent torsion.
In mesenteroaxial volvulus, the distendedstomach appears spherical on supine images. Two air-filled or fluid levels are visible on the upright film i.e.
Gastric Volvulus due to Splenomegaly ------------- A Mhaske.
Fig. II: Showing organoaxial gastric volvulus.

People’s Journal of Scientific Research 19 Vol 1 - July 08
in the fundus and in the antrum. In addition, the uprightimage often demonstrates a beak where thegastroesophageal junction is seen on normal images. Ifbarium moves through the gastroesophageal junction,the upside-down configuration of the stomach and thedegree of obstruction can be documented. Organoaxialvolvulus is difficult to diagnose on plain images. Thestomach lies horizontally and contains a single air-fluidlevel on upright views. No characteristic beak isobserved. Decreased air is noted within the remaining Gastro - intestinal tract. Barium study shows that theesophagogastric junction is lower than normal. Markedgastric dilatation and the slow passage of contrastmaterial through the site of twisting are noted.
Reduction of acute gastric volvulus is firstattempted with nasogastric decompression. However,this is often unsuccessful, particularly in cases oforganoaxial volvulus with obstruction. Surgical goalsinclude reduction, prevention of recurrence, and thecorrection of predisposing factors. Specifically,treatment involves anterior gastropexy or gastrostomyin order to fix the stomach in its anatomically correctposition. In our case gastropexy was done to preventrecurrence after derotation and predisposing enlargedspleen removed.
Several reports were published over the lastcentury describing patients from tropical areaswith massive splenomegaly. After excluding knowncauses of splenomegaly, tropical splenomegalysyndrome was defined as a separate entity. Thiscondition was later redefined as hyperreactive malarialsyndrome (HMS; Vikramjit, 2007). This is prevalentin native residents of regions where malaria is endemicand in visitors to those regions. Patients with HMS havehigh levels of antibody for Plasmodium falciparum,Plasmodium vivax, or Plasmodium malar iae.Deposition of large immune complexes in Kupffer cellsin the liver and spleen, leads to reticuloendothelial cellhyperplasia, and hepatosplenomegaly.
The hallmark of HMS is splenomegaly, whichis usually moderate to massive. The spleen is firm andregular, with notches that may be well palpable.The enlarged spleen may be seen to protrude againstthe abdominal wall. Patients are usually afebrile atpresentation. This seems to be the presentation in ourcase.
Wandering spleen is a rare conditioncharacterized by the absence or underdevelopment of
Gastric Volvulus due to Splenomegaly ------------- A Mhaske.
one or all of the ligaments that hold the spleen in itsnormal position in the left upper quadrant of theabdomen. (Ugolini et al, 2000). Wandering spleen andgastric volvulus share a common cause, the absenceof an intraperitoneal visceral ligament. As there werelax ligaments, this possibility cannot be entertainedin our case.
Massive tropical splenomegaly presenting withgastric volvulus is not documented till date. In ourcase we had splenomegaly (tropical splenomegaly)which acted as pendulous for rotation of stomach ,laxity of attachments predisposed to rotation; timelysurgical intervention prevented complication in thiscase.
Conclusion:Gastric volvulus is a rare disease. Clinical and
radiological assessment can make the diagnosis withreliability in most cases but it is the rare presentationwhich requires a high index of suspicion from thetreating clinician to avert delay or error in diagnosingthe disease. Massive tropical splenomegalyprecipitating as gastric volvulus is not documentedyet. We report this rare case which was managedsuccessfully with surgical intervention for gastricvolvulus.
Bibliography:
1. Berti A.: Singulare attortigliamento dele’ esofagocol duodeno seguita da rapida morte. Gazzeta Medica Italiana,1866;9:139-141.2. Borchardt M.: Aus Pathologie und therapiedes magen- nvolvulus.Archive Kun Chirurgica,1904;74:243.3. Mohamed A, Richard WG.: Gastric volvulus.e-Medicine specialities General Surgery: Abdomen, Article last updated-August 15, 2006.4. Stavros G, Vasilis V, Stylianos G, Sotiris B.: Acute Gastric Volvulus: Diagnosis and Management over 10 Years. Digestive Surgery, 2006;23:169- 172.5. Ugolini G, Potenti FM, Pricolo VE: Gastric outlet obstruction secondary to wandering spleen. Surgery, 2000;128(3):480-481.6. Vikramjit S K.:Tropical Splenomegaly Syndrome. e-Medicine, Specialties Pediatrics. General Medicine, Hematology, Article last updated- November 19, 2007.

I see my purpose in life as making the world a happier place to be in.- David Niven
It is not the years in your life but the life in your years that counts.- Adlai Stevenson
Life is a dream for the wise, a game for the fool, a comedy for the rich, a tragedy for the poor.- Sholom Aleichem
Every man and woman is born into the world to do something unique and somethingdistinctive and if he or she does not do it, it will never be done.- Benjamin E. Mays
Life is like a game of poker: If you don’t put any in the pot, there won’t be any to take out.- Moms Mabley
People’s Journal of Scientific Research 20 Vol 1 - July 08

Case Report
People’s Journal of Scientific Research 21 Vol 1 - June 08
Servelle-Martorell Syndrome with Extensive Upper Limb involvement:A case ReportRajesh Gupta, Nalini BharadwajDepartment of Radio Diagnosis, People’s College of Medical Sciences & Research Center, Bhanpur, Bhopal-462010 (M.P.)
Abstract:Servelle-Martorell syndrome is characterized by venous or rarely arterial malformations with limb hypertrophy
and bony hypoplasia. Extensive involvement of the upper limb is a rare feature of Servelle-Martorell syndrome. Cases withminimal upper limb involvement have been described in the literature. A young man presented with gradually increasingmultiple swellings over the right upper limb and periscapular region with functional difficulty. The arm muscles wereatrophic. The bones of forearm and hand were hypoplastic and tender. We report a case of Servelle-Martorell syndrome withextensive involvement of the entire right upper limb and periscapular region.
Key Words: Venous malformation.
Introduction:Servelle-Martorell syndrome is characterized
by limb hypertrophy owing to venous and rarely,arterial, malformations with skeletal abnormalities(hypoplasia). Similar conditions such as Klippel-Trenaunay, Parkes-Weber and Blue rubber bleb nevussyndromes can present with limb and bonehypertrophy. Magnetic resonance is the best imagingmethod for diagnosis. Adequate radiologicalinvestigations with collaborative clinical findings arecrucial to establish correct diagnosis. The prognosisof this disorder is uncertain. Therapy is predominantlyconservative. In the presence of aneurysmalcomplications or severe shunting, surgery may beindicated. Servelle-Martorell syndrome has beenreported rarely in the literature.
Venous malformations (VM) are present atbirth, although not always evident. They are bluish,soft and compressible and can be localized orextensive. They are usually present on the face, limbsor trunk. However, VM can also involve oronaso-pharynx, genitalia, bladder, brain, spinal cord, liver,spleen, lungs, skeletal muscles and bones.
Extensive involvement of whole right upperlimb is very uncommon. We present a rare case ofextensive venous malformations involving rightperiscapular region and upper limb.
————————————————————————————Corresponding Author: Dr. Rajesh Gupta, Assistant Professor,Department of Radio Diagnosis, People’s College of Medical Sciences& Research Center,Bhanpur, Bhopal-462010 (M.P.)Phone No.: 0755-2682474e-mail: [email protected]
Case Report:A 23 year old male presented with history
of gradual diffuse enlargement of right upper limbfor last 15 years and functional difficulty. Theswelling was small to begin with and progressivelyincreased in size. Patient often complained of painand stiffness in the affected areas. On clinicalexamination multiple swollen areas of various sizeswere seen over right upper limb. They were soft andcompressible. The right forearm was shorter inlength than left side.
Plain radiographs of the right upper limbshowed soft tissue masses and areas of calcification.The forearm bones revealed hypoplasia on right side.
Fig.I: Photograph showing extensive nodular soft tissue swellingsinvolving whole right upper limb and periscapular region

People’s Journal of Scientific Research 22 Vol 1 - July 08
Musculoskeletal ultrasound showed multipledilated tortuous anechoic lesions involving the rightupper limb and periscapular region. Echogenic lesionswith shadowing suggestive of phleboliths were seeninside the anechoic lesions. The forearm muscles werethinned and replaced by these anechoic lesions.
Color Doppler study showed no flow withinthe lesion but, while performing a Valsalva maneuver,there was sluggish flow within the lesion suggestiveof dilated torturous venous channels involving thesuperficial venous system. The arterial systemappeared normal.
Discussion:Servelle-Martorell syndrome is also known
as phlebectatic osteohypoplastic angiodisplasia(Weiss et al, 2000). The ectasia and aneurysmaldilatation of the superficial veins may result in amonstrous deformity of the extremity. An abnormalvein location, partial or complete lack of valves, and/or venous hypoplasia or aplasia has been observed indeep venous system.. Intra-osseous vascularmalformations may lead to hypoplasia of the bonewith the destruction of spongiosa and cortical bone,resulting in shortening and hypoplasia of the limb(Weiss et al, 2000). Intra-osseous vascular ectasiasmay lead to joint destruction. Radiographs candemonstrate multiple soft-tissue swellings, hypoplasiaof the bones and multiple phleboliths in the venousectasias. The prognosis of this disorder is uncertain.
Fig. II : AP Radiograph of right arm showing soft tissue swelling &multiple calcifications.
Fig. III: AP Radiograph of both Hands showing soft tissue swelling withmultiple calcifications on right side. Ulna and first, second metacarpalbones are hypopalstic
Venous vascular malformations span a widespectrum, varying from isolated cutaneous ectasiasto voluminous lesions involving manifold tissues andorgans. They are soft and compressible, and showno alteration in skin temperature, thrill or bruits.These are frequently and incorrectly termed‘cavernous hemangiomas’. Pure venousmalformations usually exhibit blue coloration of theskin or in the overlying mucosa, while the combinedvenous malformations and capillaries exhibit a huethat ranges from dark-red to violet (Enjolras &Mulliken, 2000; Fishman & Mulliken, 1993).
The venous malformations revealed lowflow. The condition deteriorates with pregnancy ortrauma (Enjolras & Mulliken, 1998; Burns et al,1991). There may be demineralization, hypoplasiaor lytic changes in the underlying bones in up to 71%of cases (Enjolras & Mulliken, 1998).Venous thrombosis is a regular complication, and thethrombi may be palpated at the point of pain. Anotherpossible complication is the development ofconsumption coagulopathy due to stasis in the ectaticvascular canals. The possibility of consumptioncoagulopathy must be investigated prior toundertaking any invasive procedures(Fishman &Mulliken, 1993; Burns et al, 1991).
Diagnosis is made in majority of cases byclinical features. A simple radiograph may revealphleboliths and bone hypoplasia at the age of 2 or 3years. Magnetic resonance is the best investigation
Servelle-Martorell syndrome with extensive upper limb ------------ R Gupta & N Bhardwaj.

People’s Journal of Scientific Research 23 Vol 1 - July 08
to delimit vascular malformation (Enjolras &Mulliken, 1998).
The majority of the reported cases had alimited area of involvement (Weiss et al, 2000).The extensive involvement of the entire right upperlimb and the periscapular region made this case rare.
Nonoperative management is adequate formost patients with Servelle-Martorell syndrome. Thisincludes external compression with graduatedcompression stockings and garments. Compressiontherapy can be helpful in protecting the limb, evenfrom minimal trauma that can cause bleeding of thelarge superficial malformations. Patients withsignificant edema of the lower limbs can be treatedwithdiuretics.
Sclerotherapy with local injection of 95%alcohol or 1% sodium tetradecyl sulphur may be usedfor small lesions. Surgical resection may then beperformed following successful obliteration. Theembolization of arteries sustaining the malformationis contraindicated since it may provoke tissuenecrosis.
Patients with recurrent attacks of cellulitesmay benefit from prophylactic antibiotic therapy.Anticoagulants are indicated after deep veinthrombosis or pulmonary embolus. Patients withrecurrent superficial thrombophlebitis frequentlyrequire daily administration of aspirin or ibuprofen;however, this may promote problems with bleeding.
Surgery should not be done to improvecosmetic look at the expense of function. Aneurysmalcomplications or severe shunting may be anindication of the requirement for surgery. Surgicalexcision is the definitive therapy, often renderedimpossible, however, by anatomic, esthetic andfunctional limitations (Enjolras & Mulliken, 1998).Amputation of a grossly hypertrophied, poorlyfunctioning digit may be necessary but a moreproximal foot, hand or limb amputation is rarelyrequired. Symptomatic varicosities or localizedvenous malformations can be removed in selectedpatients with good results provided that there is afunctioning deep vein system. It should be recognizedthat complete excision of extensive malformationswith debulking procedures is seldom possible.
Debulking procedures can damage venousand lymphatic structures and lead to increased edemaof the affected part, scar formation, recurrence,chronic wound infection, and chronic weeping lymph
edema (Cliff & Mortimer, 2000).
Fig. IV: High resolution ultrasound of Right arm with 12 Mhz probeshowing anechic spaces with calcification
Fig. V: Sonography reveals irregular anechic spaces with calcification.
Fig. VI:. Sonography of dorsal aspect of hand reveal irregularanechoic spaces.
Servelle-Martorell syndrome with extensive upper limb ------------ R Gupta & N Bhardwaj.

People’s Journal of Scientific Research 24 Vol 1 - July 08
Conclusion:Servelle-Martorell syndrome is a rare
condition, the diagnosis of which can be confused withKlippel-Trenaunay, Parkes-Weber and blue rubber blebnevus syndromes. Venous malformations are presentin all these conditions; bony hypoplasia is characteristicof Servelle-Martorell syndrome. Although it is rare,extensive limb involvement may be seen in Servelle-Martorell syndrome. Magnetic resonance imaging isuseful in assessing the extent of venous malformations.Conservative treatment is recommended in most cases.Sclerotherapy, with or without surgery, is recommendedin cases of functional impairment, even if recurrencesare frequent.To conclude, it is very important to have a correctdiagnosis for the vascular anomalies before thetreatment. Proper understanding of the natural courseand multidisciplinary approach is essential to tacklethese complex anomalies. Management of large VMrequire role of expert interventional Radiologist It isdifficult to cure these lesions, and the aim is to controlthem and treat the associated complications.
Servelle-Martorell syndrome with extensive upper limb ------------ R Gupta & N Bhardwaj.
Bibliography:1. Burns AJ, Kaplan LC, Mulliken JB : Is there an
association between hemangiomas and syndromes withdysmorphic features? Pediatrics, 1991; 88:1257-1267.
2. Cliff SH , Mortimer OS : Disorders of Lymphatics. In:Textbook of Pediatric Dermatology. BlackwellScience, Oxford; 2000, pp.1017-1034.
3. Enjolras O, Mulliken JB : Vascular tumours andvascular malformations (new issues). Advances inDermatology, 1998; 13:375-423.
4. Enjolras O, Mulliken JB : Vascular malformations. In:Textbook of Pediatric Dermatology. BlackwellScience, Oxford, 2000; pp.975-996.
5. Fishman SJ, Mulliken JB : Hemangiomas and vascularmalformations of infancy and childhood. PediatricClinics of North America, 1993; 40:1177-1200.
6. Weiss T, Madler U, Oberwittler H, Kahle B, Weiss C,Kubler W : Peripheral vascular malformation(Servelle-Martorell). Circulation, 2000; 101(7):82-83.

Case Report
People’s Journal of Scientific Research 25 Vol 1 - July 08
Introduction:Methemoglobinemia is an uncommon
condition seen in clinical practice. Whereas, malariain our country is one of the commonest reason foradmission to hospital. Here, we present a case reportof drug induced methemoglobinemia which resembledthe presentation of complicated malaria so closely thatwithout the high index of suspicion, monitoring andinvestigating facilities of a tertiary care center, thediagnosis would not have been suspected and made.Incorrect diagnosis and inappropriate treatment couldhave caused more harm to the patient. This case isreported with the objective of increasing awareness thatsometimes uncommon condition can closely resemblecommonly seen ones and can be missed.
Case Report:A 6 year old boy presented to the Department
of Pediatrics with a history of moderate grade fever for10 days, vomiting for 2 days with altered blood once.He had passed cola colored urine that morning althoughthe total urine output was normal. On examination hehad marked pallor, tachypnea, (30/min), pulse was 130/ min. normovolemic, had normal blood pressure andmild Jaundice. Oxygen saturation was 58% in roomair. Chest was clear, heart sounds were normal, liverwas just palpable and he was fully conscious andoriented. He had received oral Chloroquine prescribed--------------------------------------------------------------------Corresponding Author: Dr. Shruti Sarkar, Assistant Professor,Department of Pediatrics, Peoples College of Medical Science andResearch Center, Bhopal, 462010 (MP)Ph.: 0755- 4005229, Mobile 09826433108, 09977701964E-mail: [email protected]
Methemoglobinemia Mimics Complicated MalariaShruti Sarkar, Dipankar SarkarDepartment of Pediatrics, Peoples College of Medical Sciences and Research Centre, Bhanpur, Bhopal- 462010 (MP.)
Abstract:Methemoglobinemia is an uncommon condition seen in clinical practice. It is generally caused by exposure to
drugs, chemicals or solvents. Many drugs are implicated in the causation of Methemoglobinemia one of which isChloroquine. We present here a case of Methemoglobinemia following Chloroquine which was given for the treatment offever. The clinical presentation resembled closely to that of complicated Malaria. This case is presented with the objectiveof increasing awareness that uncommon illnesses can sometimes resemble closely to a very commonly seen condition andhence can be missed.
Key Words: Methemoglobinemia, Complicated Malaria
by a local doctor before presenting to our hospital.There was no history of exposure to other drug,chemical or solvent. Our clinical impression was ofMethemoglobinemia. We also investigated him for thecause of fever. He was given inhaled oxygen, packedcell transfusion, IV Ceftriaxone, Amikacin and IVfluids. Investigations showed Hb-6.1, WBC - 35,000(neutrophils- 83%) and platelets- 6.1 lacs. CRP waspositive in 1:4 dilution. Blood urea and creatinine werenormal. Urine had 20 to 30 pus cells/ HPF but noRBCs. Peripheral smear showed evidence ofhemolysis with reticulocytosis of 6%. G6PD activitywas normal. Blood gas showed partial pressure ofoxygen to be 110 mm Hg. Smear for malaria andmalaria antigen test were negative. Our impressionwas of Methemoglobinemia and probable UTI. Dueto financial constraints of the family Methemoglobinlevel estimation was sent on 3rd day of admission after2 units of packed cells had been transfused. It wasfound to be raised at 27.5%, confirming the diagnosisof Methemoglobinemia. We added oral Ascorbic acidto the treatment. He was afebrile on 3rd day ofadmission and urine became clear. He made steadyprogress from 3rd day onwards and was discharged on8th day with clear written instructions regarding thedrugs to be avoided. Our final diagnosis wasChloroquine induced Methemoglobinemia withUrinary Tract Infection.
Discussion:Oxidant exposure is generally the cause of
acquired Methemoglobinemia as seen in exposureto drugs, chemicals or solvents or indirectly as in

People’s Journal of Scientific Research 26 Vol 1 - July 08
sepsis. (Mansourie & Lurie, 1993; Hall et al, 1986;Ohashi et al, 1998; Kennedy et al, 1997). By oxidationthe ferrous molecule in the hemoglobin gets oxidizedto ferric, the resultant molecule is Methemoglobin,which is incapable of binding oxygen.
Levels greater than 2 % are non physiologicalor abnormal. Symptoms generally appear when levelsexceeds 15% and levels > 70 % may cause death(Rehman,2001). Spectral properties of Methemoglobinare different and it interferes with pulse oximetryreadings which are characteristically very low. Arterialblood gas partial pressures are very high because ofhigh flow oxygen therapy. Hemolytic anemia withintravascular hemolysis may follow drug inducedMethemoglobinemia as was seen in this patient.( Hallet al, 1986; Rehman, 2001).
This case illustrates an uncommon conditioni.e. Methemoglobinemia precipitated by a verycommonly used drug that is Chloroquine. The clinicalscenario described here is very much similar to that ofcomplicated malaria, the treatment on the contrary istotally different.( Bolyai et al, 1972).
Chloroquine is a very widely used drug in Indiaespecially in the periphery. Chloroquine inducedMethemoglobinemia has been reported before. (Cohenet al, 1968; Sharma & Varma, 2003). The point beingmade here is that Chloroquine inducedMethemoglobinemia with intravascular hemolysis asseen in our patient mimics the clinical picture ofcomplicated Malaria. One should have a high index ofsuspicion and low threshold for investigations wherecases are complicated. In the periphery, whereinvestigation facilities are limited and even simplemonitoring facilities like pulse oximetry areunavailable, early referral to higher centers in the eventof complications is recommended.
Bibliography:
1. Bolyai JZ, Smith RP, Gray CT.: Ascorbic acid and chemically induced methemoglobinemias. Toxicology & Applied Pharmacology,1972;21: 176-185.2. Cohen RJ, Sachs JR, Wicker DJ, Conrad ME.: Methemoglobinemia provoked by malaria chemoprophylaxis in Vietnam. New England Journal of Medicine, 1968;279:1127-1131.3. Hall AH, Kurig KW, Rumack BH.: Drug and chemical-induced methemoglobinemia. Clinical features and management. Journal of Medical Toxicology, 1986; 1:253-260.4. Kennedy N, Smith CP, Mc. Whinney P.: Faulty sausage production causing Methemoglobinemia. Archives of Disease in Childhood, 1997;76:367- 368.5. Mansourie A, Lurie AA.: Concise review:methmo -globinemia. American Journal of Hematology, 1993;42:7–12.6. Ohashi K, Yukioka H, Hayashi M, Asada A.: Elevated methemoglobinin patients with sepsis. Acta Anaesthesiologica Scandinvica,1998;42: :713-716.7. Rehman H U.: Methemoglobinemia. The Western Journal of Medicine, 2001 ; 175 : 193-196.8. Sharma N, Varma S.: Unusual life-threatening adverse drug effects with Chloroquine in a young girl. Journal of Postgraduate Medicine, 2003; 49:187-187.
Methemoglobinemia Mimics Complicated Malaria --------------- S Sarkar & D Sarkar.

Case Report
People’s Journal of Scientific Research 27 Vol 1 - July 08
Endodontic Enigma – Mandibular Second Premolar with Three Root Canals: ACase ReportSanjeev Tyagi, K.P. Arjun Das, S.V. BhagwatDepartment of Conservative Dentistry & Endodontics, People’s Dental Academy, Bhanpur, Bhopal-462010 (M.P.)
Abstract:Location and thorough instrumentation of all the canals in the root of a diseased tooth normally ensure success of
the endodontic therapy. Present case was referred for endodontic therapy of mandibular second premolar. Clinical andradiographic examination revealed inadequate root canal filling. Three canals were located. Endodontic therapy wasperformed under aseptic conditions.
Key Words: Pre-molar, Three root canals, Re-root canal treatment.
Introduction:Detailed knowledge of root canal
anatomy and awareness of the configuration of thepulp canal are essential when practicing root canaltherapy. There are evidences that root canalmorphology is almost limitless in its variability. Theunusual number of canals should always be expectedin various teeth. Untreated root canals may causefailure of the treatment.
Mandibular second premolars are known tohave a single canal. According to El-Deeb (1982) themandibular premolars may show wide variation intheir root canal anatomy. The incidence of their havingtwo or three canals was reported to vary from 0 to34.3%. (Zillich & Dowasn ,1973; Vertucci, 1978; Yanget al, 1988).
Case reports describing four canals inmandibular second premolar have been occasionallypublished (Yang et al, 1988; Wong, 1991). Thus, theknowledge & recognition of atypical anatomy isimportant even though it is not usually encountered.
The aim of this article is to report anuncommon condition of mandibular second premolarwith three distinct canals.
Case report:A 28 years old female with severe pain in right
mandibular region was referred to the Department—————————————————————Correspondence Author: Sanjeev Tyagi , Associate Professor,Department ofConservative Dentistry & Endodontics, People’s DentalAcademy, Bhanpur, Bhopal-462010 (M.P.)Phone: +91-9893456642E-mail.: [email protected]
of Conservative Dentistry and Endodontics forevaluation of root canal therapy. Clinical examinationrevealed that the mandibular second premolar toothresponded positively to percussion but not topalpation. Radiographic examination revealed shortand inadequate root canal filling. (Fig. 1).
Fig. I: Pre-operative radiograph showing the poor root canal filling.
The tooth was isolated with rubber dam, theold amalgam filling was removed and the accesscavity preparation was re-established. The gutta-percha was removed using Hedstrom file size 15without solvent. Three canals were located : buccally,lingually and an extra canal in the middle. Theworking length was checked radiographically(Fig. 2).
The canals were conventionally instrumentedwith a # 35K file using crown-down pressureless

People’s Journal of Scientific Research 28 Vol 1 - July 08
Fig. II : Working length radiograph showing files in the three rootcanals.
technique. Canal was irrigated with 5.25% sodiumhypochlorite, dried with sterile paper points and sealedwith formacresol. The access opening was closed withCavit. Antibiotics along with analgesics and anti-infammatory drugs were prescribed for 3 days.
The patient returned asymptomatic after 3days. Tooth was isolated with rubber dam, the canalswere instrumented with # 35 K file and irrigated withsodium hypochlorite and saline. Patient was recalledafter 4 days. On fifth day, tooth was irrigated withsodium hypochlorite and saline to remove all theremnants of the formacresol and then dried with paperpoints. Master cone was selected and the canals werefilled with gutta percha and AH26 sealer cement usinglateral condensation. Access opening was sealed withamalgam restoration. Post-operative radiograph wastaken to confirm the quality of the filling (Fig. 3).The patient was referred to the prosthetic clinic forcrown construction.
Fig. III : Obturation of the three root canals.
Patient was asked to come for follow upafter one month. At the end of one month sheconveyed that she was unable to come for followup but that she was asymptomatic.
Discussion:Inadequate debridement and/or incomplete
obturation of the root canals were found to be thecommonest cause of root canal therapy failures(Grossman, 1972). If a canal is originally cleanedbut incompletely filled, tissue fluids from the adjacentarea could cause chronic inflammatory response inthe periradicular tissue (Seltzer et al, 1967).
In this case three canals were identified, outof which only one was filled inadequately. Short canalfillings usually offer no serious problem inretreatment. That is why a Hedstrom file was usedwithout solvent. If a canal is inadequately filled, it isgenerally due to insufficient canal preparation. In astudy of endodontic failures, from histologyperspective, Seltzer et al (1967) reported inflammedor necrotic pulp tissue in teeth in which endodontictherapy had failed. They found tissues in canals thatwere not instrumented during treatment.
Although the success rate of retreatment offailed therapy is high, it may be lower than that forinitial endodontic therapy (Sjogren et al, 1990). Non-surgical retreatment is always preferable and shouldbe attempted before resorting to surgery. Theobjective of retreatment is to perform endodontictherapy in order to return the treated tooth to functionand comfort, and to allow the supporting structuresto heal completely. Retreatment of the present casewas performed using the crowndown pressurelesstechnique. It has been advocated by Marshall &Pappin (1980) in which Gates Glidden drills and largesize files should first be used in the coronal two thirdsof the canal and then smaller files are progressivelyused from the crown-down until the desired length isreached. This technique has the advantage ofenlarging and cleaning the coronal area beforeproceeding deeply into the apical regions from wheremajority of the infected tissue is removed (Marshall& Pappin, 1980; Saundars & Saundars, 1992).Furthermore, it provides unobstructed access forinstruments to follow. This would help to minimizepost-operative discomfort by preventing theinoculation of periradicular tissues with bacteria andnecrotic tissue that might be pushed out by hand files.
Endodontic enigma – Mandibular second premolar ----------- S Tyagi, KP Arjun Das & SV Bhagwat.

People’s Journal of Scientific Research 29 Vol 1 - July 08
A thorough knowledge of the pulp spacemorphology is essential for successful endodontictherapy. This may help to reduce endodontic failurecaused by incomplete obturation. An extra root canalmay be detected by careful clinical and radiographicinvestigation of the floor of the pulp chamber.(Zillich& Dowsan, 1973). Finally, variations in root canalmorphology must be considered before starting theroot canal therapy.
Bibliography:
1. Al-Fouzan K : The microscopic diagnosis and treatmentof a mandibular second premolar with four canals.International Endodontic Journal, 2001; 34:406-410.
2. Bram S, Fleisher R : Endodontic therapy in a mandibularsecond bicuspid with four canals. Journal ofEndodontic, 1991; 17:513-515.
3. ElDeeb M : Three root canals in mandibular secondpremolars. Literature review and case report. Journalof Endodontic, 1982; 8:376-377.
4. Grossman L : Endodontic failures. Dental Clinics ofNorth America, 1972; 16:50-70.
5. Marshall F, Pappin J : A crown-down pressurelesspreparation root canal enlargement technique. InTechnique manual. Oregon Health & SciencesUniversity, Portland, Oregon, 1980.
6. Rhodes J : A case of unusual anatomy: A mandibularsecond premolar with four canals. InternationalEndodontic Journal, 2001; 34:645-648.
7. SaundersW, Saunders E : Effect of non-cutting tippedinstruments on the quality of root canal preparationusing a modified double flared technique. Journal ofEndodontic, 1992; 18:32-36.
8. Seltzer S, Bender I, Smith J, Freedman I, Nazimov H: Endodontic failures: An analysis based on clinical,roentgenographic findings. Oral Surgery, 1967;23:517- 530.
9. Seltzer S, Bender I, Smith J, Freedman I, Nazimov H: Endodontic failures: An analysis based on clinical,roentgenographic and histologic findings. OralSurgery,1967; 23:500-510.
10. Sjogren U, Hagglund B, Sundqvist G, Wing K :Factors affecting the long-term results of endodontictreatment. Journal of Endodontic, 1990; 16:498-504.
11. Slowey R : Radiographic aids in the detection of extraroot canals. Oral Surgery, 1974; 37:762-772.
12. Vertucci F : Root canal morphology of the mandibularpremolars. Journal of America dental association,1978; 94:47-50.
13. Wong M : Four root canals in a mandibular secondpremolar. Journal of Endodontic, 1991; 17:125-126.
14. Yang Z, Yang S, Lin Y, Shay J, Chi C : C-shaped rootcanals in mandibular second molars in Chinesepopulation. Endodontic and Dental Traumatology,1988; 4:160- 163.
15. Zillich R, Dowasn J : Root canal morphology ofmandibular first and second premolar. Oral Surgery,1973; 36:738-744.
Endodontic enigma – Mandibular second premolar ----------- S Tyagi, KP Arjun Das & SV Bhagwat.

UPPER TEETH EXTRACTION AFFECTS THE EYES:
There are numerous reasons for this perception mainly because pain and swelling of an upper toothradiates towards the cheek bones and lower portion of the eyes; therefore the correlation.The teeth are nomally extracted in middle/old age when the eyesight is in any case getting weaker.
DENTISRY IS PAINFUL TREATMENT:
With advancement in materials, techniques, instruments etc. dental treatments have now becomevery comfortable for the patients. In fact in skilled hands its virtually a painless procedure leavingaside the anxiety of the patient wchich also can be dealt with in a practical fashion.
AMAZING INVENTIONS
The American botanist BENJAMIN MINGE DUGGER discovered the broad spectrum tetracyclineantibiotic in 1948 at the age of seventy - six. A living example of patience, persistence andperseverance.Twenty thousand plants are listed by World Health Organisation as being used for therapeuticpurposes.
People’s Journal of Scientific Research 30 Vol 1 - July 08

People’s Journal of Scientific Research 31 Vol 1 - July 08
Case Report
Thoraco-Abdominal Ectopia Cordis: A Rare Entity. Case Report and Review ofLiterature.Ashwin V ApteDepartment of Surgery, People’s college of Medical Sciences and Research Center, Bhanpur, Bhopal-462 010.
Abstract:Ectopia cordis is a rare congenital abnormality characterised by partial or complete displacement of
the heart outside the thoracic cavity. It can be associated with other congenital abnormalities. The present casewas a two hours old male child and a product of non-consanguineous marriage. Child had thoraco-abdominalectopia cordis. Condition of child detoriated rapidly and succumbed before any investigation and surgicalintervention could be performed.
Key Words: Ectopia Cordis Thoracoabdominalis, Sternal Cleft.
Introduction:Ectopia cordis is defined as complete or partial
displacement of the heart out side the thoracic cavity.It is a rare congenital defect in fusion of the anteriorchest wall resulting in extra thoracic location of theheart (Hornberger et al, 1996; Kim et al, 1997). Itoccurres in 5.5 to 7.9 per 1 million live births(Hornberger et al, 1996). This anomaly is classifiedinto five types : cervical, cervicothoracic, thoracic,abdominal, and thoracoabdominal (Kim et al, 1997).The two most common forms of ectopia cordis are thethoracic and thoracoabdominal type (Amato et al, 1995;Hochberg et al, 1995). The thoracic ectopia cordisconstitute the classic naked heart with no overlyingsomatic structures. The thoracoabdominal type isfrequently associated with Cantrell’s pentalogy, whichinclude bifid sternum, deficiency of the diaphragm,defect of diaphragmatic pericardium, defect of theanterior abdominal wall, and intracardiac defects(Amato et al, 1995; Abdallah et al, 1993).
Case Report:A fullterm 2 hours old male boy weighing 2.4
kg was shifted to our hospital with Ectopia Cordis. Hewas born to a 26 year old mother by caesarian sectiondue to fetal distress. There was no history of consangu-ineous marriage, antenatal infection, drug ingestion,--------------------------------------------------------------------Corrseponding Authors: Ashwin V Apte, Associate Professor,Department of Surgery, People’s college of Medical Sciences and ResearchCenter, Bhanpur Bhopal.Phone No.: 0755 4004078, 9826033422E-mail: [email protected]
exposure to radiation etc. Priliminary examinationof the baby revealed peri-oral cyanosis with heart rateof 140/min and respiratory rate of 50/ min. The heartof baby was lying outside the thoracic cavity & devoidof pericardium with a Sternal Cleft. The apex of heartwas pointing anteriorly. Baby also had associatedsupraumblical omphalocele which contained the liverand bowel with a thin membrane covering theomphalocele. The sternum was bifid in lower half,with an inter-ridge distance of 5 cm, through whichthe heart was protruding for 4-5 cm. (Fig. 1).
Baby was resuscitated on admission andinitial management included covering of the heart andomphalocele with sterile-soaked dressing andsystemic antibiotics coverage.
Fig 1: Baby with Ectopia Cordis Thoracoabdominalis showing nakedheart lying outside the thoracic cavity and associated exomphalos.
The baby deteriorated rapidly and inspite ofsupportive management baby unfortunately diedwithin few hours of birth before any investigationsand surgical intervention could be undertaken. At ourhospital performing a medical autopsy is not a routinepractice & obtaining consent for the same is difficult,

therefore, the underlying cardiac defects and associatedmalformations could not be ascertained.
Discussion:Ectopia cordis is a rare and striking congenital
heart defect, which was first observed 5000 years ago(Taussing, 1982). The term ectopia cordis was firstcoined by Haller in 1706. The defect is described asmalposition of the heart, partially or completely outsidethe thorax. According to the position of the misplacedheart, ectopia cordis can be classified into five types:1) cervical, in which the heart is located in the neckwith sternum that is usually intact; 2) thoracicocervical,in which the heart is partially in the cervical region butthe upper portion of the sternum is split; 3) thoracic, inwhich the sternum is completely split or absent, andthe heart lies partially or completely outside the thorax;4) thoraco-abdominal, which usually accompaniesCantrell’s syndrome; 5) abdominal, in which the heartpasses through a defect in the diaphragm to enter theabdominal cavity.(Kim et al, 1997; Dobell et al, 1982).
Genesis of ectopia cordis has not been fullyexplained, although several theories have been offered(Dobell et al, 1982). Predominent theory states thatthere is primary failure of descent & mid line fusion ofthe lateral body folds (Humpl et al, 1999); early ruptureof chorion & / or yolk sac causing failure of midlinefusion, amniotic band syndrome (Dobell et al, 1982;VanAllen & Myhre, 1985).
The majority of ectopia cordis patients haveassociated intracardiac defects. Ventricular septaldefect, atrial septal defect, tetralogy of Fallot, anddiverticulum of the ventricle are the most commonlyencountered heart lesions (Amato et al, 1995; Leca etal, 1989). The severity and the complexity of theintracardiac defect contribute largely to the poorprognosis associated with this malformation(Amato etal, 1995).
It has been also observed that the ultimatesurvival of these patients depend more on the presenceor absence of intrinsic cardiac defects rather thansurgical techniques. Most of infants are stillborn or diewithin first few hrs or days of life (Humpl et al, 1999;Shamberger, 1998).
The overall objectives of ectopia cordismanagement are: closure of the chest wall defect,including the sternal defect, repair of the associatedomphalocele, placement of the heart into the thorax,
and repair of the intracardiac defect (Dobell et al,1982; Leca et al, 1989).
Ectopia cordis is a rare congenitalmalformation which may require a staged procedureto achieve a complete repair. The prognosis of thiscondition has been poor historically. With theadvances in all aspects of medicine, the number ofinfants with ectopia cordis who undergo successfulsurgical repair and survive is steadily increasing.
Bibliography:
1. Abdallah HI, Marks LA, Balsara RK, Davis DA, RussoPA : Staged repair of pentalogy of Cantrell with tetralogyof Fallot. Annal of Thoracic Surgery, 1993; 56:979-980.
2. Amato JJ, Zelen J, Talwakar NG : Single - stage repairof thoracic ectopia cordis. Annal of Thoracic Surgery,1995; 59:518-520.
3. Dobell AR, William HBU, Long RW : Staged repair ofectopia cordis. Jouranl of Pediatric Surgery,1982;17:353-358.
4. Haller (1706) cited in Ectopia Cordis thoracalis withfacial cleft. Indian Journal of Radiology & Imaging,2003;13(4):415-416.
5. Hochberg J, Ardenghy MF, Gustafson RA, Murray GF: Repair of thoracoabdominal ectopia cordis withmyocutaneuous flaps and intraoperative tissueexpansion. Plastic Reconstructive Surgery,1995;95:148-151.
6. Hornberger LK, Colan SD, Lock JE, Wessel DL, MayerJE (Jr) : Outcome of patients with ectopia cordis andsignificant intracardiac defects. Circulation, 1996; 94(9 Suppl.):II32-37.
7. Humpl T , Huggan P, Hornberger L K, McCrundle BW: Presentation & outcomes of ectopia cordis. TheCanadian Journal of Cardiology, 1999, 15 (12):1353-1357.
8. Kim KA, Vincent WR, Muenchow SK, Wells WJ,Downesy SE : Successful repair of ectopia cordis usingalloplastic materials. Annal of Plastic Surgery, 1997;38:518-522.
9. Leca F, Thibert N, Khoury W, Fermont L, Laborde F,Dumez Y : Extrathoracic heart (ectopia cordis): Reportof two cases and review of literature. InternationalJournal of Cardiology, 1989; 22:221-228.
10. Shamberger RC : Congenital chest wall deformities.In: Pediatric Surgery (vol. 1), O ‘Neill JH, Rowe MI,Grosfeld JL, Fonkalsrud EW, Coran AG. Eds; 5th Edn.Mosby year book inc, St. Louis, 1998; pp.787-817.
11. Taussing HB : World survey of the common cardiacmalformation: developmental error of genetic variant.American Journal of Cardiology, 1982;50:544-559.
People’s Journal of Scientific Research 32 Vol 1 - July 08
Thoraco-Abdominal Ectopia Cordis --------- Ashwin V Apte.

12. Van Allen MI, Myhre S : Ectopia cordis thoracalis withcraniofacial defects resulting from early amnion rupture.Teratology, 1985, 32 (1):19-24.
Thoraco-Abdominal Ectopia Cordis --------- Ashwin V Apte.
People’s Journal of Scientific Research 33 Vol 1 - July 08

People’s Journal of Scientific Research 34 Vol 1 - July 08
AMAZING INVENTIONS
Penicillin, the first antibiotic, ws dicovered in 1928 by accident. A shallow glass dish forbacteriological experiments was uncovered unintentionally by ALEXANDER FLAMING in hislaboratory in England. An experimenter upstairs was careless with the mold he was using and somedrifted through an open window and landed in Fleming’s Staphylococci culture. The following day, thescottish bacteriologist found in the dish a clear area where the penicillin, the mould had been killing thebacteria.
Men can have hemophillia, but can’t pass it on to their children. Women may not even show symptomsof hemophilia, yet pass on the ‘royal disease’.
The above episodes have been collected from the book of Facts (vol. 1) by Issac Astimov.

People’s Journal of Scientific Research 35 Vol 1 - July 08
Review Article
Clinical Anatomy of the Vocal CordAshutosh S. Mangalgiri, *Raza Razvi, **G. S. LongiaDepartment of Anatomy, People’s College of Medical Sciences & Research Centre, *People’s College of Dental Sciences & Research Centre &**People’s Dental Academy, Bhanpur, Bhopal-462010 (M.P.)
Abstract:Larynx is a multifunctional organ. Laryngeal cavity is divided into the supra-glottic, glottic and sub-glottic
cavity by vestibular fold (False vocal cords) and vocal folds (True vocal cords). Various conditions are responsible forvocal cord paralysis; commonest one is recurrent laryngeal nerve injury during neck surgeries. Possible complicationsshould be kept in mind by surgeons and anesthetists. In this paper we have discussed various conditions causing vocalcord paralysis.
Key Words: Larynx, Vocal cords, Recurrent laryngeal nerve, Paralysis.
Introduction:Laryngeal primordia appears at approximately
33 days of gestation. At this stage auditus becomes ‘T’shaped by the growth of epiglottis in anterior directionwhile arytenoid cartilages grow in the lateral direction.The adult larynx is about 5 cm in length in males andshorter in females. Longer length in males is due tolarger growth after puberty. Larynx descends from thelevel of C5 vertebra at the age of 2 years to C6 – C7 inadult position. During this descend the relationshipbetween the internal and external parts of the larynx ismaintained. The position of true vocal cords remainsmidway between the thyroid notch and lower borderof thyroid cartilage. The narrowest part of larynx inchildren is subglottic region and rima glottidis in adults(O’ Neill et al, 1998).
The larynx serves three basic functions. Firstit protects the respiratory passage against invasion ofthe food and foreign bodies. Secondly it maintains thepatency of airway thereby helps in respiration and lastlyit also serves as organ of phonation. Most primitiveand primary function of the larynx is protection of thelower airway. Larynx first evolved as sphincter forprevention of ingress of water into the airway oflungfish, but with subsequent evolution of the dilators,active opening is permitted (Negus, 1949).
The inlet of the larynx is set obliquely facingbackwards (Fig.1). The inlet bounded anteriorly by—————————————————————————————Corresponding Author: Dr. Ashutosh S. Mangalgiri, Associate Professor,Department of Anatomy, Peoples College of Medical Science and ResearchCentre, Bhopal, 462010 (M.P.)Ph: +919827547597, 0755 4061597E-mail: [email protected]
the upper border of the epiglottis. The aryepiglotticfold containing aryepiglottic muscles and corniculateand cuneiform cartilages. The inlet is related laterallyon each side to the piriform recess of thelaryngopharynx. The cavity of the larynx is dividedinto the supraglottic, glottic and sub-glottic cavity,by two pairs of horizontal folds, the vestibular andvocal folds as shown in figure 2. Vestibular folds arealso termed as false vocal cords and vocal folds aretermed as true vocal cords. Each vocal fold consistsof central part formed by muscle, intermediate partformed by conus elasticus consisting of layers ofcollagen and elastic tissue which in turn is coveredby epithelium and superficial layer of lamina propria(Reinke’s space) as shown in figure 3 (Cummings etal, 2005).
Discussion:Various pathological conditions are
responsible for vocal cord paralysis. The mostcommon cause of the vocal cord paralysis is recurrentlaryngeal nerve injury (Fernandes & Mesqnita,1997;Shindo et al, 2005). Most of the recurrent laryngealnerve injuries occur during neck and mediastinalsurgeries. Neoplasms, tracheal intubation, blunttrauma, inflammation and some idiopathic conditionare other common causes. Although, rarely directinfiltration of recurrent laryngeal nerve by laryngealtumors causes vocal cord paralysis (Million,1992).Skalicky et al (2007) stressed about theprotection of the nervous laryngeus recurrens fromiatrogenic damage. Many central nervous systemdisorders and various congenitle abnormalities maycause vocal cord paralysis viz. transient ischaemic

People’s Journal of Scientific Research 36 Vol 1 - July 08
Fig. I: Photograph showing in let of larynx.
Fig. II: Photograph of sagittal section through larynx showing differentparts.
attacks, hydrocephalus, syringobulbia, Arnold –Chairi,malformations, Shy - Drager syndrome, multiple-system atrophy and amyotrophic lateral sclerosis (Terriset al, 1992; Hillel et al, 1999; Cummings et al, 2005;Boey et al, 1995; Glucan et al, 2005). Endotrachealintubation causes unilateral paralysis of vocal cord dueto acute trauma ( Terrence, 2007 ) and bilateral paralyisdue to prolonged use of endotracheal tube (Gibbin &Egginton, 1981). Chen et al (2007) reported radiationinduced cranial nerve paralysis in head and neck cancermay play a significant role in vocal cord paralysis.
Fig. III: Photograph showing epithelial layer, sub-epithelial laminapropria, crico-vocal membrane (conus elasticus) with vocal process asseen by dissection of larynx.
Vocal cord paralysis may be unilateral orbilateral. Unilateral vocal cord paralysis is morecommon than the bilateral. Etiology of the unilateraland bilateral vocal cord paralysis is almost the samebut with a varying percentage (Benninger et al, 1994;Hillel et al,1999). Unilateral paralysis is seen inalmost 75% of cases (Terris et al, 1992). In unilateralvocal cord palsies, left sided palsies (in 56% cases)are more common than the right because of the longercourse and extension of the recurrent laryngeal nervein the mediastinum (Jacob et al, 1987). Nerurkar etal (2006) in a series of 85 patients with unilateralparalysis of vocal cords observed left sided palsy in68 patients and right sided in 17 patients. In 90 % ofcases of unilateral vocal cord paralysis, there is aninvolvement of recurrent laryngeal nerve (Terris etal, 1992).
Chen et al (2007) studied 291 patients, outof which 259 patients presented with unilateral vocalcord paralysis and 32 with bilateral vocal cordparalysis. These were attributed to surgical in 40.2%,neoplastic in 29.9%, idiopathic in 10.7%, traumaticin 8%, central in 3.8%, radiation induced in 3.4%,inflammatory in 2%, cardiovascular in 1.7% and othercauses in 0.3% cases. Hulscher et al (1999) in hisretrospective study of 241 patients who underwenttranshiatal oesophagoctomy observed thirty-onepatients with recurrent laryngeal nerve paralysis outof which 3 had bilateral and 28 with unilateral palsies.
Clinical Anatomy of the Vocal Cord —————————— A S Mangalgiri, R Razvi & G S Longia.

People’s Journal of Scientific Research 37 Vol 1 - July 08
Ishimoto et al (2002) encountered unilateralvocal cord paralysis in 19 patients and bilateral vocalcord paralysis in one patient postoperatively in 62patients of thoracic aortic aneurysm.
Yoskovitch & Kantor (2001) reported a uniquecase of unilateral vocal cord paralysis due todegenerative cervical spine disease resulting in extrinsiccompresson of recurrent laryngeal nerve.
Bilateral vocal cord paralysis was observedfollowing anterior cervical discectomy and fusion.(Hachwa & Halim, 2006; Manski et al, 1998).
Witt (2003) observed a case of sarcoidosis withcranial polyneuritis with bilateral paratracheal andmediastinal adenopathy resulting in bilateral vocal cordparalysis. Aydin et al (2002) observed a case of bilateralvocal cord paralysis caused by cervical spinalosteophytes compressing the recurrent laryngeal nerve.Bilateral vocal cord immobility can be life threateningfor some patients. Weksler et al (2001) reported anunusual bilateral vocal cord paralysis followingpreoperative bupivacaine infiltration for pain controlof tonsil surgery. Knowledge of such uncommoncomplications should be kept in mind by anaesthetistsand surgeons.
Sometimes weakness or a paradoxical motionof vocal cords may mimic paralysis (Hillel at al, 1999).In such cases of paradoxical motion, vocal foldsapproximate together during inspiration, instead ofopening normally. Therefore, it is essential to considerparadoxical movements as a differential diagnosis ofbilateral vocal cord paralysis.
In 0.3% to 1% cases an unusual ‘non-recurrent’laryngeal nerve may arise from the vagus nerve, usuallyon right side. This may get injured during surgery ordue to laryngeal pathology leading to paralyticcondition of vocal cords (Stranding, 2005).
Growths on vocal cords varies from simplebenign nodule to malignant growth in the form of polyps(Fig. 4), which may lead to dysfunction of the vocalcords. This infiltration may be direct or indirect frommetastasis. A well recognised form of papillarycarcinoma of thyroid directly infiltrating the larynx wasreported by Mcaffrey et al (1994). Varghese et al (2003)reported an unusual metastasis of papillary carcinomaindirectly affecting vocal folds. Many researchersreported vocal cord dysfunction as a consequence ofthe laryngeal tuberculosis mimicking carcinoma larynx(Hunter et al, 1981; Bull, 1966). Glottic tumors willnot show the signs of spread of metastasis to adjacent
lymph nodes at presentation because glottis is verypoorly endowed with lymphatic vessels (Stranding,2005).
Clinical Anatomy of the Vocal Cord —————————— A S Mangalgiri, R Razvi & G S Longia.
Fig. IV: Photograph showing vocal cord polyp as seen by directlaryngoscopy. [By courtesy of Dr. Devendra Mahore, Professor of ENT,Govt. Medical College, Nagpur.]
Conclusion:Paralysis of the vocal fold is most common
laryngeal pathology. A detailed clinical history andmeticulous examination on head and neck is necessaryto evaluate vocal cord paralysis. It is essential thatanaesthesiologists and surgeons should be well versedwith the topographic anatomy of the larynx and allpossible complications should be kept in mind beforesurgeries.
Bibliography:
1. Aydin K, Ulug T, Simsek T : Bilateral vocal cord par- alysis caused by cervical spinal osteophytes. British
Journal of Radiology, 2002; 75: 990-933.2. Benninger MS, Crumley RL, Ford CN, Gould WJ,
Hanson DG, Ossoff RH, Sataloff RT : Evaluation andtreatment of the unilateral paralyzed vocal cord.Otolaryngology Head Neck Surgery, 1994; 111:497–508.
3. Boey HP, Cunningham MJ, Webe AL : Central nervoussystem: Imaging in evaluation of children with truevocal cord paralysis. Annals of Otology, Rhinology &Laryngology, 1995; 104: 76.
4. Bull TR : T. B. of Larynx. British Medical Journal,1966; 2: 991.
5. Chen H, Jen Y, Wang C, Lee J, Lin Y : Etiology ofVocal Cord Paralysis. Journal for Oto-Rhino-Laryngology, 2007; 69:167-171.

People’s Journal of Scientific Research 38 Vol 1 - July 08
Clinical Anatomy of the Vocal Cord —————————— A S Mangalgiri, R Razvi & G S Longia.
6. Cummings CW, Flint PW, Harker LA, Haughey BH,Richardson MA, Robbins KT, Schuller DE, Thomas JR: Cummings Otolaryngology Head and Neck Surgery.Vol. 3, 4th Edn., Elsevier Mosby, USA, 2005; pp: 2026-2053.
7. Fernandes L, Mesqnita A : Stridor presentation in lary- ngeal tuberculosis. Indian Journal of Tuberculosis, 1997;
44:93-94.8. Gibbin, KP, Egginton, MJ : Bilateral vocal cord paralysis
following endotracheal intubation. British Journal ofAnaesthesia, 1981; 53 (10): 1091-1092.
9. Gulcan H, Onal C, Arslan S, Bayindir T : Bilateral vocalcord paralysis in newborns with neuraxial malformations.– Two case reports. Neurologia Medico Chirurgica(Tokyo), 2005; 45:536- 539.
10. Hachwa B, Halim-Armanios M : Bilateral vocal cordinjury following anterior cervical discectomy: could abetter preoperative exam have prevented it? LibyanJournal of Medicine, 2006; 1(2):156-161.
11. Hillel AD, Benninger M, Blitzer A, Crumley R, Flint P,Kashina HK, Sanders I, Schaefer S : Evaluation andmanagement of bilateral vocal cord immobility.Otolaryngology Head Neck Surgery, 1999; 121:760–65.
12. Hulscher JBF, Van Sandick JW, Devriese PP, VanLanschot JJB, Obertop H : Vocal cord paralysis aftersubtotal oesophagectomy. British Journal of Surgery,1999; 86(12): 1583–1587.
13. Hunter AM, Miller JW, Wightman AJA, Mome NW :Changing pattern of laryngeal tuberculosis. Journal ofLaryngology and Otology, 1981; 95:393.
14. Ishimoto S, Ito K, Toyama M, Kawase I, Kondo K,Oshima K, Niimi S : Vocal Cord Paralysis After Surgeryfor Thoracic Aortic Aneurysm. Chest, 2002; 121:1911-1915.
15. Jacobs CJM, Harnsberger HR, Lufkin RB, Osborn AG,Smoker WRK, Parkin JL : Vagal neuropathy: evaluationwith CT and MR imaging. Radiology, 1987; 164:97–102.
16. Manski TJ, Wood MD, Dunsker SB : Bilateral vocalcord paralysis following anterior cervical discectomy andfusion : Case report. Journal of neurosurgery,1998; 89(5): 839-843.
17. Mcaffrey TV, Bergstralh EJ, Hay ID : Locally invasivepapillary thyroid carcinoma. Head Neck, 1994; 16:165-172.
18. Million RR : The Larynx ……. so to speak: EverythingI wanted to know about laryngeal cancers, I learnedin the last 32 years. International Journal of RadiationOncology Biology Physics, 1992; 23:691.
19. Negus V : The comparative anatomy and physiologyof of the larynx. Hafner Publishing company, NewYork, 1949; pp. 190.
20. Nerurkar N, Tandon S, Kalel K, Joshi A, Gharat P,Bradoo R : Unilateral Vocal Fold Paralysis -- An IndianScenario. Bombay Hospital Journal, 2006; 48 (4).
21. O’Neill Jr. JA, Rowe MI, Grosfeld JL, FonkalsrudEW, Coran AG : Paediatric Surgery, Vol 1, 5th Edn.,Mosby, London, 1998; pp.701-726.
22. Skalicky T, Treska V, Spindlen V, Vodicka J, SimanekV, Wirthova M, Cambal M : The surgical anatomy ofthe nervous laryngeus recurrens. Bratislavske LekarskeListy, 2007; 108 (6): 269-270.
23. Shindo M, Wu J, Park E : Surgical anatomy of therecurrent laryngeal nerve revisited. Otolaryngology –Head and Neck, 2005; 133 (4): 514 - 519.
24. Stranding S : Gray’s Anatomy: In Larynx, Chp. 36,39th
Edn., Elsevier Churchill Livingstone, London, 2005;pp: 633 – 646.
25. Terrence Jose Jerome J : An Unusual Complication OfNasotracheal Intubation- Unilateral Vocal Cord Palsy.The Internet Journal of Anesthesiology, 2007; 12 (1).
26. Terris DJ, Arnstein DP, Nguyen HH : Contemporaryevaluation of unilateral vocal cord paralysis,Otolaryngology Head Neck Surgery, 1992; 107: 84-89.
27. Varghese BT, Mathews A, Pandey M, Pradeep VM :Unusual metastasis of papillary thyroid carcinoma tolarynx and hypopharynx a case report. World Journalof surgical Oncology, 2003; 1:7.
28. Weksler N, Nash M, Rozentsveig V, Schwartz A, Schily M, Gurman GM : Vocal cord paralysis as a conseque- nce of peritonsillar infiltration of with bupivacaine. Acta Anaesthesiologica Scandinavica, 2001; 45(8): 1042-1044.29. Witt R L: Sarcoidosis presenting as bilateral vocal fold paralysis. Journal of voice, 2003; 17(2): 265 – 268.30. Yoskovitch A, Kantor S : Cervical osteophytes presen- ting as unilateral vocal fold paralysis and dysphagia. The Journal of Laryngology & Otology, 2001; 115: 422-424.

People’s Journal of Scientific Research 39 Vol 1 - July 08
Review Article
Oral submucous fibrosis - Current Concepts in EtiopathogenesisM.K. Gupta*, Shubhangi Mhaske, Raju Ragavendra , ImtiyazDepartment of Oral & Maxillofacial Surgery*, Department of Oral & Maxillofacial Pathology, Peoples Dental Academy, Bhanpur, Bhopal-462010 (M.P.)
Abstract:Oral submucous fibrosis (OSF) is now accepted globally as an Indian disease, having highest malignant potential
than any other oral premalignant lesions. The understanding of the exact role of alkaloids and other etiological agents withrespect to pathogenesis will help the management and minimize the blind clinical trials and treatment modalities. Thisarticle provides an overview of the etiopathogenesis with stress on the recent concepts related to this chronic “IndianDisease”.
Key Words: Areca nut, Arecoline, Cytokines, HLA typing, Oral precancer, Oral submucous fibrosis.
Introduction:Oral submucous fibrosis (OSF), now globally
accepted as an Indian disease, has one of the highestrates of malignant transformation amongst potentiallymalignant oral lesions and conditions. The conditionhas also been described as idiopathic scleroderma ofmouth, idiopathic palatal fibrosis and sclerosingstomatitis. It was first described three decades agoby Pindborg & Sirsat (1966). The hallmark of thedisease is submucosal fibrosis that affects most partsof the oral cavity, pharynx and upper third of theesophagus leading to dysphagia and progressivetrismus due to rigid lips and cheeks.
The disease is predominantly seen in Asiancountries, prevalence being more in India (Fig. 1).
Fig. I: Grey areas demonstrate regions which have betel quid chewinghabits in south-east Asia with India being the most affected country.
--------------------------------------------------------------------------------------Correspondence Author: Dr. Shubhangi Mhaske, Associate Professor& Head, Department of Oral & Maxillofacial Pathology, Peoples DentalAcademy, Bhanpur, Bhopal-462010 (M.P.)Ph. 9893778647E-mail : [email protected]
Recent epidemiological data indicates that the numberof cases of OSF has risen rapidly in India from anestimated 250,000 cases in 1980 to 2 million casesin 1993. The reasons for the rapid increase of thedisease are reported to be due to an upsurge in thepopularity of commercially prepared areca nutpreparations (pan masala) in India(Ranganathan etal, 2004) and an increased uptake of this habit byyoung people(Gupta et al, 1998) due to easy access,effective price changes and marketing strategies.
Oral Submucous fibrosis is diagnosed on thebasis of clinical criteria including oral ulceration,paleness of the oral mucosa and burning sensation(particularly in the presence of spicy foods), harden-ing of the tissue and presence of characteristic fibrousbands. The fibrosis involves the lamina propria andthe submucosa and may often extend into the under-lying musculature resulting in the deposition of densefibrous bands giving rise to the limited mouth open-ing which is a hallmark of this disorder.
Etiology:Epidemiological data and intervention
studies suggest that areca nut is the main aetiologicalfactor for OSF (Pindborg et al, 1984; Seedat & VanWyk, 1988; Sinor et al, 1990; Maher et al, 1994; Murtiet al 1995; Merchant et al, 1997; Shah & Sharma,1998; Yang et al, 2001; Farrand et al, 2001; IARC,2004; Jacob et al, 2004). Other etiological factorssuggested are chillies, lime, tobacco, nutritionaldeficiencies such as iron and zinc, immunologicaldisorders, and collagen disorders. Extensive researchis being done on the Indian supari ( areca nut /betel nut, Fig. 2).

People’s Journal of Scientific Research 40 Vol 1 - July 08
Fig. II:Areca nut –Indian supari is the main cause for submucousfibrosis
Areca nut:The term areca nut is used to denote the
unhusked whole fruit of the areca nut tree and termbetel nut is used exclusively to refer to the inner kernelor seed which is obtained after removing husk. Thebetel nut has psychotropic and anti helminthic propertydue to presence of areca alkaloids. Four alkaloids havebeen conclusively identified in biochemical studies,arecoline, arecaidine, guvacine & guvacoline, of whicharecoline is the main agent. These alkaloids havepowerful parasympathetic properties which produceeuphoria and counteract fatigue.
Nitrosation of arecoline leads to the formationof areca nut specific nitrosamine namelynitrosoguvacoline, nitrosoguvacine and 3-methylnitrosominopropionitrile, which alkylate DNA.Metabolism of these areca nut specific nitrosamine leadto formation of cyanoethyl, which binds with o’methylguanine in DNA. Prolonged exposure to this irritantleads to malignant transformation.
Recently suggested pathogenesis of oralsubmucous fibrosis is by dual action of areca nut. It issuggested that arecoline not only stimulates fibroblasticproliferation and collagen synthesis but also decreasesit’s breakdown. This suggests that arecoline is the activemetabolite in fibroblast stimulation.
Areca and slaked lime :In a habitual betel nut chewer, oral submucous
fibrosis may be caused by the amount of tannic acidcontained in the betel nut, the influence of mixedcalcium powder and the conditional action of arecolinecontent in betel nut, affecting the vascular supply of
oral mucosa and causing neurotropic disorder .Thisview was further supported by the finding that,addition of slaked lime Ca(OH)2 to areca nut in panfacilitates hydrolysis of arecoline to arecaidine (morepotent than arecolin) making this agent available inthe oral environment.
Tobacco & Lime:These are known irritants and causative
factors in oral malignancy. They may act as localirritants. The commercially freeze dried products suchas Pan masala, Gutka and Mawa (areca, tobacco andlime) have high concentrates of areca nut per chewand appear to cause OSF more rapidly than by selfprepared conventional betel quid which containsmaller amounts of areca nut. (Shah & Sharma, 1998;Sinor et al, 1990).
Chillies: The use of chillies (Capsicum annum and
Capsicum frutescence) has been thought to play anetiological role in oral submucous fibrosis. Capsaicin,which is vanillylamide of 8-methyl-6-nonenic acid,is the active ingredient of chillies, play an etiologicalrole in oral submucous fibrosis (Rajendran, 1994).
Nutritional deficiency:A subclinical vitamin B complex deficiency
has been suspected in cases of OSF withvesiculations and ulcerations of oral cavity. Thedeficiency could be precipitated by the effect ofdefective nutrition due to impaired food intake inadvanced cases and may be the effect, rather than thecause of the disease (Rajendran, 1994).
Defective iron metabolism:Microcytic hypochromic anemia with high
serum iron has been reported in submucous fibrosis(Rajendran, 1994).
Collagen disorders:Oral submucous fibrosis is thought to be a
localized collagen disease of oral cavity. It is linkedto scleroderma, rheumatoid arthritis, Duputreyen’scontracture and intestinal fibrosis. A link betweenscleroderma and oral submucous fibrosis has alsobeen suspected on the basis of similarity of histologi-cal characteristics (Tsai et al, 1999; Tilakratne et al,2005).
Oral submucous fibrosis - Current Concepts -------------------- M K Gupta, S Mhaske, R Ragavendra & Imtiyaz.

Oral submucous fibrosis - Current Concepts -------------------- M K Gupta, S Mhaske, R Ragavendra & Imtiyaz.
Immunological disorders:Raised ESR and globulin levels are indicative
of immunological disorders. Serum immunoglobulinlevels of IgA, IgG and IgM are raised significantly inoral submucous fibrosis. These raised levels suggestan antigenic stimulus in the absence of any infection.Circulating autoantibodies are also present in somecases of oral submucous fibrosis (Canniff et al, 1985).
Pathogenesis:I Collagen accumulation:Oral submucous fibrosis results from increasedproduction of collagen by fibroblasts. In addition tothis there is decreased breakdown leading toaccumulation of excessive amount of collagen.
a) Increased Collagen Production:Under the influence of areca nut, fibroblasts
differentiated into phenotypes that produce morecollagen. The alkaloids present in areca nut, arecadineand arecoline are responsible for this. Arecoline getsconverted in to arecadine which is the activemetabolite. There is dose dependent increase inproduction of collagen by fibroblasts under influenceof these factors (Flow chart-1;Meghji et al, 1987; Kuoet al, 1995).
Various cytokines are increased in oralsubmucous fibrosis. These are: Transforming growthfactor (TGF- ), Platlet derived growth factor (PDFG)and Basic fibroblast growth factor (bFGF). These arefibrogenic growth factors that stimulate collagenproduction. Another cytokine that has anticollageneffect is Interfran- (IFN- ). This is decreased in OSF.Thus overall there is stimulation of collagen synthesisthrough different mechanisms (Haque et al, 1998).
Flow chart 1: Role of areca alkaloids in OSF (Ghom & Mhaske, 2008).
b) Stabilization of collagen structure and decreasedcollagen breakdown:
One of the mechanisms that can lead toincreased fibrosis is by reduced degradation ofcollagen by forming a more stable collagen structure.Betel nut contains tannin. Tannin has ability tostabilize collagen by cross-linking it. With theprogression of the disease type III collagen is almostcompletely replaced by type I (Utsunomiya et al,2005). Type I collagen is more resistant todegradation than type III. An important finding fromthese studies is the identification of excess -1 chainsrelative to -2, suggesting an alteration of collagenmolecules during the progression of the disease.Although, the biological function of this trimer isnot known, it is regarded as more resistant todegradation than the normal collagen molecule (Tsaiet al, 1999).
Another component of betel nut that aids thiscross-linking is copper. It is a constituent of enzymelysyl oxidase. This enzyme also causes cross-linkingand makes collagen resistant to degradation bycollagenase. Due to action of tannin and copper,collagen that is produced in OSF is highly resistantto remodeling and phagocytosis (Tsai et al, 1999).
It is fibroblast that brings about remodelingand phagocytosis of collagen. As in OSF, thesefibroblasts are affected and phenotypically changed,they cannot degrade collagen. Studies on the effectsof arecoline on both normal and OSF fibroblasts inculture revealed an elevated rate of collagen synthesisby OSF fibroblasts as compared to normal fibroblasts.
Flow chart 2: Role of areca nut in oral submucous fibrosis (Ghom &Mhaske, 2008)
People’s Journal of Scientific Research 41 Vol 1 - July 08

People’s Journal of Scientific Research 42 Vol 1 - July 08
Oral submucous fibrosis - Current Concepts -------------------- M K Gupta, S Mhaske, R Ragavendra & Imtiyaz.
Although the reason for this elevation is not clear, someauthors proposed that it could reflect the clonal selectionof a highly fibrogenic cell population in the alteredtissue under the influence of local factors such asinterleukin-1 from inflammatory cells (Utsunomiya etal, 2005). This leads to decrease in phagocytosis &accumulation of collagen in oral mucosa (Flow chart2).Glycogen consumption is physiologically related tocellular activity of muscle fibres. Over activity ofmuscles results in excessive glycogen consumption,leading to its depletion. In areca nut chewers there isoveractivity of muscles due to repeated, continuouschewing and use of heavy force to crush the hard nut.This increased muscle activity along with diminishedblood supply, following connective tissue changes leadsto muscle degeneration and fibrosis.
II Increased expression of fibrogenic cytokines:The most important finding in the various
studies was the demonstration of increased expressionof fibrogenic cytokines namely TGF -1, PDGF andbFGF in OSF tissues compared to normal (Haque et al,1998). These observations may suggest that the diseaseprocess in OSF may be an altered version of woundhealing as recent findings show that the expression ofvarious ECM molecules are similar to those seen inmaturation of granulation tissue.(Utsunomiya et al,2005)
III Genetic polymorphisms predisposing to OSF:Polymorphisms of the genes coding for TNF-
has been reported as a significant risk factor for OSF.TNF - is known to stimulate fibroblastic proliferationin vitro (Vilcek et al, 1986). Evidences suggest thatcollagen-related genes are altered due to ingredients inthe quid.The genes COL1A2, COL3A1, COL6A1,COL6A3 and COL7A1 have been identified as definiteTGF- targets and induced in fibroblasts at early stagesof the disease. The transcriptional activation of theseprocollagen genes by TGF- suggests that it maycontribute to increased collagen levels in OSF(Rajalalitha & Vali, 2005).
IV OSF as an autoimmune disorder:OSF is also thought to be an autoimmune
disease. The presence of various autoantibodies invarying titers is reported in several studies confirmingautoimmune basis to the disease. Few studies havereported on HLA typing of OSF patients and controls.
Higher frequencies of OSF are found in HLA A10,DR3 and DR7 types when compared to an ethnically,regionally and age-matched control group (Cannifet al, 1985; Kuo et al, 1995). Although the data onvarious HLA types, raised autoantibodies and thedetection of immune complexes tend to indicate anautoimmune basis for the disease, substantial numberof cases and matched controls may be required toverify these finding (Tilakaratne et al, 2005)Precancerous nature and malignanttransformation:
The precancerous nature of OSF was firstdescribed by Paymaster in 1956 when he observedslow growing squamous cell carcinoma (SCC) in onethird of the patients with the disease. This wasconfirmed by various other workers. Pindborg in1972 put forward five criterias to prove that thedisease is precancerous (Pindborg et al, 1984). Theyincluded, high occurrence of OSF in oral cancerpatients, higher incidence of SCC in patients withOSF, histological diagnosis of cancer without anyclinical suspicion in OSF, high frequency ofepithelial dysplasia and higher prevalence ofleukoplakia among OSF cases.
Most of the earlier studies have focused onthe prevalence of epithelial dysplasia in OSF. It hasso far been the most reliable indicator for predictingpotential malignant transformation of an oralprecancerous lesion though new markers areemerging (Warnakulasuriya, 2001). Epithelialdysplasia in OSF tissues appeared to vary from 7 to26% depending on the study population (Pindborget al, 1967; Murti et al, 1995; Lee et al, 2003).However, according to the current awareness of thedisease and some refined criteria for gradingdysplasia, it is reasonable to assume that theprevalence of dysplasia is more towards the midwayof the reported range. Malignant transformation rateof OSF was found to be in the range of 7–13%.
The hypothesis that dense fibrosis and lessvascularity of the corium, in the presence of analtered cytokine activity creates a uniqueenvironment for carcinogens from both tobacco andareca nut to act on the epithelium is widely beingaccepted. It could be assumed that carcinogens fromareca nut accumulate over a long period of time eitheron or immediately below the epithelium allowingthe carcinogens to act for a longer duration before itdiffuses into deeper tissues.

People’s Journal of Scientific Research 43 Vol 1 - July 08
Oral submucous fibrosis - Current Concepts -------------------- M K Gupta, S Mhaske, R Ragavendra & Imtiyaz.
Conclusions:Various available data suggests that the main
causative agents for OSF are the constituents of arecanut, mainly arecoline, whilst tannin may have asynergistic role. Arecoline will interfere with themolecular processes of deposition and/or degradationof extracellular matrix molecules such as collagen. Dueto this interference, phagocytic capacity of fibroblastis reduced, because of up or down regulation of keyenzymes such as lysyl oxidase and alteration inexpression of various ECM molecules. The process mayalso be influenced by increased secretion ofinflammatory cytokines, growth factors and decreasedproduction of anti-fibrotic cytokines. Although theabove mechanisms may explain the induct ion,maintenance and progression of fibrosis in OSF, furtherresearch is required in order to identify the mechanismleading to carcinogenesis in this fibrotic oral mucosa.Nutritional deficiencies may not play a primary rolebut it could synergize the symptomotology bycontributing to epithelial atrophy. Although theinvolvement of HLA and genetic predisposition hasbeen reported, specific haplotypes have not beendetermined. The individual mechanisms operating atvarious stages of the disease–initial, intermediate andadvanced–need further study in order to proposeappropriate therapeutic interventions.
Bibliography:
1. Canniff JP, Batchelor JR, Dodi K, Harvey W.: HLA typing in oral submucous fibrosis. Tissue Antigen, 1985; 26:138- 142.2. Farrand P, Rowe RM, Johnston A, Murdoch H.:
Prevalence, age of onset and demographic relationshipsof different Areca nut habits amongst children in TowerHamlets, London. British Dental Journal, 2001;190:150–154.
3. Ghom A, Mhaske S.: Premalignant lesions and conditions(Chapter 12) In: Textbook of oral pathology. 1st Edn,Jaypee Brothers Medical Publishers (P) Ltd, New Delhi, 2008; pp.194-201
4. Gupta PC, Sinor PN, Bhonsle RB, Pawar VS, Mehta HC.Oral submucous fibrosis in India: a new epidermic.National Medical Journal of India, 1998;11:113–116.
5. Haque MF, Harr is M, Meghji S, Barrett AW.:Immunolocalization of cytokines and growth factors inoral submucous fibrosis. Cytokine, 1998;10:713–719.
6. International Agency for Research on Cancer (IARC).:Betel-quid and areca nut chewing and some areca nutderived nitrosoamines. Lyon IARC, 2004; 85: 123–129.
7. Jacob BJ, Straif K, Thomas G, Ramadas K, Mathew B,Zhang ZF, Rangaswamy S, Hashibe M.: Betel quidwithout tobacco as a risk factor for oral precancers.Oral Oncology, 2004; 40:697–704.
8. Kuo MYP, Chen HM, Hahn LJ, Hsieh CC, ChiangCP.: Collagen biosynthesis in human OSF fibroblastcultures. Journal of Dental Research, 1995;74:1783–1788.
9. Lee CH, Ko YC, Huang HL, Chao YY, Sheih TY, LinLM.: The precancer risk of betel chewing, tobacco useand alcohol consumption in oral leukoplakia and oralsubmucous fibrosis in Southern Taiwan. BritishJournal of Cancer, 2003; 88:366–372.
10. Maher R, Lee AJ, Warnakulasuriya KA, Lewis JA,Johnson NW.: Role of areca nut in the causation oforal submucous fibrosis: a case control study inPakistan. Journal of Oral Pathology & Medicine,1994;23:65–69.
11. Meghji S, Scutt A, Harvey W, Canniff JP.: An in vitrocomparison of human fibroblasts from normal and oralsubmucous fibrosis tissue. Archives of Oral Biology,1987;32:213–215.
12. Merchant AT, Haider SM, Fikree FF.: Increased severityof oral submucous fibrosis in young Pakistani men.British Journal of Oral Maxillofacial Surgery, 1997;35:284–287.
13. Murti PR, Bhonsle RB, Gupta PC, Daftary DK,Pindborg JJ, Metha FS.: Aetiology of oral submucousfibrosis with special reference to the role of areca nutchewing. Journal of Oral Pathology & Medicine,1995;24:145–152.
14. Murti PR, Bhonsle RB, Pindborg JJ, Daftary DK, GuptaPC, Mehta FS.: Malignant transformation rates in oralsubmucous fibrosis over a 17 year period. CommunityDentistry & Oral Epidemiology, 1985;13:340–341.
15. Paymaster JC.: Cancer of the buccal mucosa: A clinicalstudy of 650 patients. Cancer, 1956;9:431–435.
16. Pindborg JJ, Poulsen E, Zachariah J.: Oral epithelialchanges in thirty Indians with oral cancer and oralsubmucous fibrosis. Cancer, 1967;20:1141–1146.
17. Pindborg JJ, Murti PR, Bhonsle RB, Gupta PC, DaftaryDK, Metha FS.: Oral submucous fibrosis as aprecancerous condition. Scandinavian Journal ofDental Research, 1984;92:224–229.
18. Pindborg JJ, Sirsat SM.: Oral submucous fibrosis. OralSurgery Oral Medicine & Oral Pathology, 1966; 22:764–779.
19. Rajalalitha P, Vali S.: Molecular pathogenesis of oralsubmucous fibrosis–collagen metabolic disorder.Journal Oral Pathology & Medicine, 2005;34:321–328.
20. Rajendran R.: Oral submucous fibrosis: etiology,pathogenesis and future research. Bulletin of World

People’s Journal of Scientific Research 44 Vol 1 - July 08
Oral submucous fibrosis - Current Concepts -------------------- M K Gupta, S Mhaske, R Ragavendra & Imtiyaz.
Health Organisation, 1994;72 (6): 985-996.22 Ranganathan K, Uma Devi M, Joshua E, Kirankumar K,
Saraswathi TR.: Oral submucous fibrosis: a case controlstudy in Chennai South India. Journal Oral Pathology& Medicine, 2004;33:274–277.
23. Saeed B, Haque MF, Meghji S, Harris M.: HLA typingin oral submucous fibrosis. Journal of Dental Research,1997;76:1024.
24 Seedat HA, Van Wyk CW.: Betel nut chewing and oralsubmucous fibrosis in Durban. South African MedicalJournal, 1988;74:572–575.
25. Shah N, Sharma PP. Role of chewing and smoking haibtsin the aetiology of oral submucous fibrosis (OSF): a casecontrol study. Journal Oral Pathology & Medicine,1998;27:475–479.
26. Sinor PN, Gupta PC, Murti PR, Bhonsle RB, DaftaryDK, Mehta FS, Pindborg JJ.: A case-control study oforal submucous fibrosis with special reference to theaetiologic role of areca nut. Journal Oral Pathology &Medicine, 1990;19:94–98.
27. Tilakaratne WM, Klinikowski MF, Saku T, Peters TJ,Warnakulasuriya S.: Oral submucous fibrosis :Reviewon aetiology and pathogenesis. Oral Oncology, 2005;42:561-568.
28. Tsai CC, Ma RH, Shieh TY. Deficiency in collagenand fibronectin phagocytosis by human buccal mucosafibroblasts in vitro as a possible mechanism for oralsubmucous fibrosis. Journal Oral Pathology &Medicine, 1999;28:59–63.
29. Utsunomiya H, Tilakaratne WM, Oshiro K, MaruyamaS, Suzuki M, Ida-Yonemochi H, Cheng. J, Sabu T.:Extracellular matrix remodeling in oral submucousfibrosis; its stage-specific modes revealed by immuno-histochemistry and in situ hybridization. Journal OralPathology & Medicine, 2005;34(8):498–507.
30. Vilcek J, Palombella VJ, Henrikson-DeStefano D.Fibroblast growth factor enhancing activity of tumournecrosis factor and its relationship to other polypeptidegrowth factors. Journal of Experimental Medicine,1986;163:632–643.
31. Warnakulasuriya S.: Histological grading of oralepithelial dysplasia: revisited. Journal of Pathology,2001;194:294–297.
32. Yang YH, Lee HY, Tung S, Shieh TY.: Epidemiologicalsurvey of oral submucous fibrosis and leukoplakia inaborigines of Taiwan. Journal Oral Pathology &Medicine, 2001;30:213–219.

People’s Journal of Scientific Research 45 Vol 1 - July 08
Informative Article
Improving quality of our life through biotechnologyS.S. Sandhu, Rupesh ThakurCentre for Advance Research & Development, People’s Group, Bhanpur, Bhopal – 462010 (M.P.)
Key words: Genetic engineering, Gene therapy, Transgenic animals, Fermentation, Vaccines.
Introduction:Biotechnology is any technological application
that uses biological systems, living organisms, orderivatives thereof, to make or modify products orprocesses for specific use. It applies the knowledge ofbiology to enhance and improve the environment,health, and food supply. Using biotechnology, scientistswork to develop environment-friendly alternatives tofossil fuels and plastics; new medicines, vaccines anddisease diagnostic tools and higher yielding and morenutrient-rich crop plants (Miller, 1991). Biotechnologyaffects every part of our lives in the 21st Century. Sometechnologies used for human welfare are:
Bioprocessing:The use of bacteria, yeast, mammalian cells
and/or enzymes to manufacture products. Large scalefermentation and cell cultures carried out in hugebioreactors manufacture useful products like Insulin,vaccines, vitamins, antibiotics, amino acids etc(Mudgett, 1996).
Monoclonal antibodies (MCAb):Our immune system makes proteins called
antibodies which are produced by cells called B-lymphocytes. -lymphocytes produce antibodies whenour immune system detects a foreign substance that hasinvaded our body. Monoclonal antibodies (MCAb) formedicine are produced by cloning a single cell.Therapeutically, MCAb are used for Home Pregnancytests, to diagnose infectious diseases such asstreptococcal infection and gonorrhoea; to detectcancer(they bind to tumour cells) and to detect diseasesin plants and animals, food contaminants andenvironmental pollutants (Hubbard, 1983).
------------------------------------------------------------Corresponding Author: Prof. S.S. Sandhu, Head of Department,Centre for Advance Research & Development, People’s Group, Bhanpur,Bhopal-462010 (MP)Phone: +919424395270E-mail: [email protected]
Cell culture technologies:Plant cell culture in which growing cells in
containers or large bioreactors are achieved. Plantcell cultures are used to grow genetically engineeredplants that contain useful traits, such as resistance toinsect pests (Hansen & Wright, 1999).
Animal Cell Culture is used for breedinglivestock. Bovine zygotes from genetically superiorbull and cows can be produced in large numbers tobe implanted into surrogate cows (MacDonald, 1996).
Human Embryonic Stem Cell (ESC) areundifferentiated cells that have the potential todevelop into any cell in the human body. One sourceof ESC is the inner cell mass of the human blastocyst.Other sources of ESC are being discovered anddeveloped (Wilmut et al, 1997).
Tissue engineering technology:This is a combination of cell biology and
materials science where semi synthetic tissues in thelaboratory are created using natural collagen andsynthetic polymers to produce artificial skin. The goalis to create complex organs as replacement fordiseased or injured organs (Mironov et al., 2003).
Genetic engineering technology:It makes the use of recombinant DNA
technology that is the recombining of genetic materialfrom two different sources. It is the next step, afterselective breeding, in changing the genetic makeupof organisms (Schmidt, 1994). Products of geneticengineering are: a) Transgenic bacteria – bacteria thatproduces human insulin; b) Transgenic plants – plantsthat glow in the dark (firefly gene), plants that areresistant to disease, to frost; Transgenic animal – micewith human genes; animal with extra copies of growthhormone genes, that grows faster and produces leanermeat and chicken resistant to bacteria that causes foodpoisoning (Hammer et al, 1985).

People’s Journal of Scientific Research 46 Vol 1 - July 08
Improving quality of our life through biotechnology----------------- S S Sandhu & R Thakur.
Bioinformatics technology:Use and organization of information about
biology. This is an interface of computer science,mathematics and molecular biology. Objective is to usedatabase management to map and compare genomes,determine protein structure, design drugs, identifygenes, etc (Forslund & Sonnhammer, 2008).
DNA chip technology:This is a combination of the semiconductor
industry and molecular biology which consists of atagged DNA on a microchip that can be read usinglasers, computers and microscopes and allows tens ofthousands of gene to be analyzed on a single microchipand used to detect mutations and diagnose geneticdiseases (Lemieux et al, 1998).
In the coming years, most of the commercialapplication of biotechnology will be in four markets:Medical, Agricultural, Environmental and IndustrialSystems. Though Medical and Agricultural areas aremore relevant from the international market point ofview, in the Indian context, environment and industrialproducts are also likely to present immenseopportunities in the short term - both for traditionaland modern Biotechnology products.
Medical Biotechnology:To detect and diagnose many diseases and
medical conditions more quickly and with greateraccuracy, designer drugs, gene therapy to correctgenetic disease, cell therapy to produce replacementtissues and organs, antibiotics, cancer therapy tosuppress tumour genes and prevent or cure cancer,design and production of vaccines (Feber, 2001).Vaccine delivery systems (goats that produce milk witha malaria antigen in it). Vaccines have also made animportant effort in helping to control disease epidemics.Forensics: DNA fingerprinting allows for theidentification of individuals by analyzing section ofDNA that varies widely from one individual to another(Findley et al, 1997). Human Genetics: Stem cellresearch has proven potential to help over 10 millionpeople with osteoporosis, 43 million arthritis sufferers,and 250,000 people paralyzed by spinal cord injuries(Gardner, 2002).
Agricultural Biotechnology:It is the single largest influence on farming
since the cultivator ; increased yields per plant,
increased resiliency to chemicals such as pesticides,easier to grow economic gains for farmers, endingworld hunger, biopesticides and biofertilisers. Today,there are over 200 million acres of crops in over 17countries that have been improved by biotechnology.Designer plants – genetically modified organisms(GMO) with inserted genes. Genetically modifiedplants can be resistant to disease, frost, and insects.GMO can be a factory for pharmaceuticals: tobaccoplant that produces haemoglobin. Plants that yield ahealthier and higher than normal crop to improve ourfood supply, animal feeds / supplements fromagricultural products and natural products inhealthcare (Potrykus, 1990).
Animal Biotechnology:Livestock that is engineered to resist disease
-no more mad cow disease, cattle that produces humanpharmaceutical products and cattle with increasedmuscle mass and less fat for healthier food supply.Flavours / fine chemicals / amino acids / nutrientsupplements from animal waste (Schwerin et al,
1995).Environmental Biotechnology:
Cleaning up pollution throughbioremediation: the use of microbes to digest andconvert unwanted waste material into harmlesssubstances, cleaning oil spills using living organism,helping the environment: burn cleaner, made lesstoxic, biodegradable, recyclable and low to zerogreenhouse gas emissions, reduced use of chemicals/pesticides, reduced ground water contamination,reclaiming of polluted or salt-affected land, increasedagricultural productivity reducing the need for landclearing, thus protecting biodiversity, detection,removal and treatment of toxins in water, air, foodand soil, and conversion of waste into energy. Theuse of biotechnology has the potential for bothpositive and negative impacts on the environment.Biotechnology can be used to support work onrecovering endangered species. (Miller, 1991).
Industrial Biotechnology:Production of antibiotics , vitamins,
detergents, new textile fibres, biodegradable plastics,biomass fuels: biodiesel and bioethanol, biorefineries:lower emissions, economical benefits: cheaper

People’s Journal of Scientific Research 47 Vol 1 - July 08
Improving quality of our life through biotechnology----------------- S S Sandhu & R Thakur.
production and government incentives (Lipinsky,1981). Recombinant DNA technology is used forproducing various compounds in micro organisms. Italso plays an important role in fermentation processesand has applications from food area to development ofvarious products (Bristow, 1993).
Conclusion:Biotechnology has grown more in the last 15
years than almost any other field of science. Thisgrowth is due to the fact that it has helped benefitvirtually every aspect of our lives. Its benefits maypotentially one day be able to reach out to help virtuallyany person, in any profession, in a positive way.Although there are some clear concerns with thedifferent aspects of biotechnology, governmentregulations have helped make sure that the technologieswe use are safe and have constructive affects on us andour environment and that the positive benefits we gainfrom biotechnology far outweigh any moral and socialimplications.
Bibliography:
1. Bristow A F : Recombinant DNA derived insulinanalogues as potentially useful therapeutic agents.Trends in Biotechnology, 1993; 11:301–305.
2. Feber D : Gene therapy: Safer and virus-free? Science,2001; 294:1638–1642.
3. Findlay I, Taylor A, Quircke P, Frazier R, Urquhart A :DNA fingerprinting from single cells. Nature, 1997;389:555–556.
4. Forslund K, Sonnhammer E L L : Predicting proteinfunction from domain content. Bioinformatics, 2008;24:1681–1687.
5. Gardner R L : Stem cells: potency, plasticity and publicperception. Journal of Anatomy, 2002; 200(3):277–82.
6. Hammer R E, Pursel V G, Rexroad CE, Wall RJ, BoltD J, Ebert K M, Palmiter R D, Brinster RL : Productionof transgenic rabbits, sheep and pigs by microinjection.Nature, 1985; 315:680–683.
7. Hansen G, Wright M S : Recent advances in thetransformation of plants. Trends in Plant Science,1999; 4:226–231.
8. Hubbard R : Monoclonal antibodies: production,properties and application. In: Topics in Enzyme andFermentation Biotechnology (Wiseman, A. ed.) 1983;pp. 163–196. Ellis Harwood, Chichester.
9. Lemieux B A, Aharoni A, Schena M : Overview ofDNA chip technology. Molecular Breeding, 1998;4:277–289.
10. Lipinsky E S : Chemicals from biomass: petrochemicalsubstitution options. Science, 1981; 212:1465–1471.
11. MacDonald C : Animal cell technology. Trends inBiotechnology, 1996; 14:325–326.
12. Miller M : The promise of biotechnology. Journal ofEnvironmental Health, 1991; 54:13–14.
13. Mironov V, Boland T, Trusk T, Forgacs G, MarkwaldR R : Organ printing: computer-aided jet-based 3Dtissue engineering. Trends in Biotechnology, 2003;21:157–161.
14. Mudgett R E : Solid state ferementation. In: Manualof Induatrial Microbiology and Biotechnology(Demain, A. L., Solomon, N. A., eds.), 1996; pp. 66–83. American Society of Microbiology, WashingtonDC.
15. Potrykus I : Gene transfer to plants: Assessment andperspectives. Physiologia Plantarium, 1990; 79:125–134.
16. Schmidt K : Genetic engineering yields first pest-resistant seeds. Science, 1994; 265:739.
17. Schwerin M, Brockmann G, Vanselow J, Seyfert H M: Perspective of molecular genome analysis in livestockimprovement–an overview. Animal Research andDevelopment, 1995; 42:14–26.
18. Wilmut I, Schnieke A E, McWhir J, Kind A J, CampbellH S : Viable offspring derived from foetal and adultmammalian cells. Nature, 1997; 385:810–813.