Embed Size (px)
Citation preview

Insulin Access and AffordabilityWorking Group: Conclusions andRecommendationshttps://doi.org/10.2337/dci18-0019
There are more than 30 million Americans with diabetes, a disease that costs the U.S.more than $327 billion per year (1,2). Achieving glycemic control and controllingcardiovascular risk factors have been conclusively shown to reduce diabetes compli-cations, comorbidities, and mortality. To achieve these desired outcomes, the medicalcommunity now has available many classes of medications and many formulations ofinsulin to effectively manage the metabolic abnormalities for people with diabetes.However, the affordability of medications in general, and for insulin specifically, iscurrently of great concern to people with diabetes, their families, health care providers,insurers, and employers. For millions of people living with diabetes, including allindividuals with type 1 diabetes, access to insulin is literally a matter of life and death.The average list price of insulin has skyrocketed in recent years, nearly tripling between2002 and2013 (3). The reasons for this increase are not entirely clear but aredue inpartto the complexity of drug pricing in general and of insulin pricing in particular.As the price of insulin continues to rise, individuals with diabetes are often forced to
choosebetweenpurchasingtheirmedicationsorpayingforothernecessities,exposingthem to serious short- and long-term health consequences (4–9). To find solutionsto the issue of insulin affordability, there must be a better understanding of thetransactions throughout the insulin supply chain, the impact each stakeholder has onwhat people with diabetes pay for insulin, and the relative efficacy of therapeuticoptions. Thus, as the nation’s leading voluntary health organization whose mission is“to prevent and cure diabetes and to improve the lives of all people affected bydiabetes,” the American Diabetes Association (ADA) is committed to finding ways toprovide relief for individuals and families who lack affordable access to insulin.In the spring of 2017, the ADA Board of Directors convened an Insulin Access and
Affordability Working Group (Working Group) to ascertain the full scope of the insulinaffordability problem, to advise the ADA on the execution of strategies, and to providehigh-level direction to the ADA related to this issue. The composition of the WorkingGroup is provided in Supplementary Table 1. The Working Group identified increasedtransparency throughout the insulin supply chain and a number of other interventionsas important steps toward developing viable, long-term solutions to improve insulinaccess and affordability.Throughout 2017, theWorking Group assembled existing public information about
insulin prices and patient cost-sharing, and convened a series of meetings withstakeholders throughout the insulin supply chain to learn how each entity affects thecost of insulin for the consumer. TheWorking Group also had ongoing conversationswith researchers focused on insulin pricing at both the global and national levels. TheWorking Group talked with more than 20 stakeholders who were representatives ofpharmaceutical manufacturers, wholesalers, pharmacy benefit managers (PBMs),pharmacies, pharmacists, distributors, health plans, employers, and people withdiabetes and caregivers (Supplementary Table 2). Despite the attempt to interview asmany stakeholders as possible, it is important to note that due to time constraints andschedules, the Working Group may have inadvertently overlooked inviting somerelevant stakeholders, and there were a small number of individual stakeholderswho declined to meet with the Working Group. To guide the discussion with eachstakeholder interviewed, the Working Group developed a set of standard questionsfocused on determining the role each entity plays in the supply chain, the issues theentity faces, and recommendations for change (Supplementary Table 3).
1American Diabetes Association, Arlington, VA2Morehouse School of Medicine, Atlanta, GA3North Coast Health, Lakewood, OH4USC Schaeffer Center for Health Policy & Eco-nomics, Los Angeles, CA5University of Michigan, Ann Arbor, MI6Vanderbilt University Medical Center, Nashville,TN7University of Maryland School of Medicine,Baltimore, MD8Popper & Yatvin, Philadelphia, PA
Correspondingauthor:WilliamT.Cefalu,[email protected].
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dci18-0019/-/DC1.
*A complete list of the members of the InsulinAccess and Affordability Working Group can befound in the Supplementary Data online.
This ADA statement was reviewed and approvedby the American Diabetes Association Board ofDirectors in March 2018.
This article is featured in a podcast available athttp://www.diabetesjournals.org/content/diabetes-core-update-podcasts.
© 2018 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
See accompanying article, p. 1125.
William T. Cefalu,1 Daniel E. Dawes,2
Gina Gavlak,3 Dana Goldman,4
William H. Herman,5 Karen Van Nuys,4
Alvin C. Powers,6 Simeon I. Taylor,7 and
Alan L. Yatvin,8 on behalf of the Insulin
Access and Affordability Working Group*
Diabetes Care 1
ADASTA
TEMEN
T
Diabetes Care Publish Ahead of Print, published online May 8, 2018

BACKGROUND: SCOPE OF THEPROBLEM
Approximately 7.4million Americanswithdiabetes use one ormore formulations ofinsulin (10,11). Peoplewithdiabetes usinginsulin come fromvariedeconomic, racial,and ethnic backgrounds. Almost 20% ofAfrican Americans with diabetes use in-sulin,eitheraloneorwithoralmedications,as do 14% of Caucasians and 17% ofHispanics with diabetes (10). Of adultswith diabetes earning below the povertylevel, approximately 24% use insulin, ei-ther alone or with oral medications (11).Currently, there are only three insulin
manufacturers serving the U.S. market:Eli Lilly, NovoNordisk, and Sanofi. Almost100 years ago, the discovery of insulin,derived from animal sources, literallybegan to save human lives. The adventof genetic engineering brought humaninsulin formulations to patients with di-abetes in the 1980s. Rapid-acting andlong-acting human insulin analogs wereintroduced in the 1990s. The patents formany of the human insulin and humaninsulin analog formulations in currentclinical use have expired.Working Group members from the
USC Schaeffer Center for Health Policy&Economicshave significantexperience instudying medication pricing (12,13). UsingCenters for Medicare &Medicaid Servicesdata on National Average Drug Acquisi-tion Cost (NADAC), they identified 30 in-sulin products with NADAC data availablebetweenOctober 2012andDecember 2016and categorized them by product type:short-acting insulin vials, rapid-acting insulinvials, rapid-acting insulin pens, and long-acting insulin pens/vials (Table 1). For eachproduct, they collected monthly WholesaleAcquisition Cost (WAC) from First Databankand calculated average monthly WACand NADAC for each category by aver-aging across products in each category.They used Medicare Part D claims from2006 to 2013 to calculate the average in-sulinexpenditureandout-of-pocketspend-ing per insulin user and the Medicarespendingbyutilization (i.e., the total spend-ing divided by the number of insulin userstimes mean annual day supply).The average U.S. list price (WAC) of the
four insulin categories increased by 15%to 17% per year from 2012 to 2016 (Fig. 1).Over the same period, the price phar-maciespaid topurchase insulins (NADAC)increased at similar rates. Spending on
insulins byMedicare Part D has also shownan increasing and accelerating trend. Forexample, Medicare spending by utiliza-tion on rapid-acting insulin in vials hada compound annual growth rate (CAGR)of 10% per year between 2006 and 2013but a CAGR of 13% between 2011 and2013.Asspendingoninsulinshasincreased,so too have patient out-of-pocket costs.Between 2006 and 2013, average out-of-pocket costs per insulin user amongMedi-care Part D enrollees increased by 10% peryear for all insulin types (Fig. 2). Compar-atively,overall inflationduringthistimewas2.2%, medical care service costs increasedby 3.8%, and spending for all prescriptiondrugs increased by an average of 2.8%.
Insulin affordability and accessibilityissues, however, are not restricted to theU.S. Data from the global ACCISS (Ad-dressing the Challenges and Constraintsof Insulin Sources and Supply) study foundseveraloverarching trends. First, even forthe same insulin product, there is a widerange of prices across the world. Second,there is a large price differential betweenthe lower prices of human insulin for-mulationsand thehigherpricesofhumaninsulin analog formulations on a globallevel. Third, therehasbeen increasinguseof human insulin analogs compared withnormal human insulin over the recentpast, which is greater in more developedparts of the world (14). This study alsoreported that the global insulin market isdominated by the same three large mul-tinational corporations thatmanufactureand sell insulin in the U.S. Those com-panies represent 99% of the total insulinbyvalue,96%bytotalmarketvolume,and88% of global product registrations.
COMPLEXITY OF THE INSULINSUPPLY CHAIN AND PRICINGMECHANISMS
Pricing of drugs in general, and for insulinspecifically, is very complex. Numerousstakeholders (i.e.,manufacturers,whole-salers, PBMs, pharmacies, health plans,andemployers) are involved in the insulinsupply chain, and the distribution andpayment systems involve multiple trans-actionsamongthesestakeholders(Fig.3).With this system, there is no one agreed-upon price for any insulin formulation.The price ultimately paid by the personwith diabetes at the point of sale resultsfrom the prices, rebates, and fees nego-tiated among the stakeholders. Stakehold-ers in the insulin supply chain have varying
degrees of negotiating power, which addsto the complexity. The following narrativerepresents the Working Group’s under-standing of the U.S. insulin delivery systemas obtained by research and in specificinterviews with the stakeholders.
Overview of Insulin Supply ChainDynamicsThecomplexityof the insulin supplychainis outlined schematically in Fig. 3. Theinsulin supply chain mirrors that of manyotherprescriptiondrugs.Asoutlined,man-ufacturers set the list price for each insulinproduct.Manufacturers typically sell theirmedications to wholesalers, who handledistribution to individual pharmacies. Butsometimes a pharmacy chain will dealdirectly with the manufacturer. Whole-salers typically purchase themedicationsfor close to the list price, often receiving ahandling fee from the manufacturer thatis calculated as a fixed percentage ofthe list price. Wholesalers then sell themedications topharmacies,with little tonomarkup. They may, however, charge thehigher list price. Pharmacies dispense themedication to individual patients and col-lectcost-sharingrequiredbythepatient’shealthplan (if any). Pharmacies then submita bill to the individual’s health insuranceplan (if any) to be reimbursed for the costof themedication dispensed to the patient,less any cost-sharing collected, plus a dispens-ing fee. If a patient does not have or usehealth insurance for themedication, thepharmacy typically charges thepatient apricerelatively close to its purchase price, witha markup.
Whilethemedicationitselftakesaratherdirect path from manufacturer to whole-saler to pharmacy to patient, the flow ofmoney is far less direct and transparent.Furthermore, PBMs often manage thepharmacybenefit portionof ahealthplanonbehalf of their clients. Their clients are thepayersforhealthcare,suchaslargeemploy-ers, health insurers providing pharmacybenefits to Medicare enrollees, health in-surers covering state Medicaid programenrollees, or health insurance plans solddirectly to individuals. It is important tonote, therefore, that PBMs’ primary cus-tomersarehealthplansandemployers,notpatients.
The Increasing List Prices of InsulinFormulationsMuch of the public discussion regardinginsulin affordability and accessibility hasfocusedon the rapidly increasing average
2 ADA Statement Diabetes Care

list prices of insulin over the past twodecades, which nearly tripled between2002 and 2013 (3). The list price is definedas the price manufacturers set for theirmedication (Table 2). Along with yearlyincreases, the published data also suggestthat when one insulin manufacturer in-creases the price for a given insulin for-mulation, the other insulinmanufacturersoften increase their prices by a similaramount shortly thereafter (15,16) (Fig. 4).
The Increasing Use of Higher-PricedInsulinsAnother important trend affecting overallcosts for insulin in the last decade is theshift in insulin utilization from the lessexpensive human insulins tomore expen-sive human insulin analogs (14,17–19) (Fig.5). While the prices of both types of insu-lin have increased, the difference in pricingbetween them has substantially added
to insulin costsdboth to the health caresystem and to many patients (17,18) (hu-man insulins are available at the pharmacyfor $25 to $100 per vial compared withhuman insulin analogs at $174 to $300per vial [19]). This is further discussedbelow in FORMULARY DECISIONS AND PATIENT
FINANCIAL BURDEN.
The Growing Gap Between the ListPrice and Net PriceWhile the list price is defined as thepricemanufacturers set for their medication,the list price is not ultimately what ispaid for the medication (with some excep-tions),nor is itwhatmanufacturers receivefor their products. The net price manu-facturers receive for their medicationsis the list price less any fees paid towholesalers, and/or discounts paid topharmacies, and any rebates paid toPBMs or health plans.
TheWorkingGroup found anumber ofexamples from public sources showingthat the net price to the insulin manu-facturers has grown at a slower rate, orhas gone down, compared to list prices.For example, the net price of the insulinformulation Lantus (glargine) increasedmore or less in parallel with the list pricefrom 2007 to 2013 (20). However, thenet price has decreased in recent years(2014–2016) (Fig. 6) (20). As a result,the net price increased by 57% between2007 and 2016, increasing 23% as fast asthe list price reported as a 252% increaseover the same period (Fig. 6).
Reports on other insulin products alsoillustrate the difference between the rapidincrease in list price as compared with theslower increase in net price to manufac-turer, a trend that may have started ear-lier for some insulin formulations (17,21).Bloomberg News reported an estimate by
Table 1—Categories of insulin
Category label onFigs. 1, 2, and 5 Description Delivery Productsdbrand namesa Productsdgeneric names
Short-acting insulin(vials)
Short-acting, intermediate-acting, or mixedintermediate/short-acting vials
Vial Humulin R, 10-mL vialHumulin R, 3-mL vialNovolin RNovolin R (Relion)Humulin N, 10-mL vialHumulin N, 3-mL vialNovolin NNovolin N (Relion)Humulin 70/30Novolin 70/30Novolin 70/30 (Relion)
Insulin regular, humanInsulin regular, humanInsulin regular, humanInsulin regular, humanInsulin NPH, human isophaneInsulin NPH, human isophaneInsulin NPH, human isophaneInsulin NPH, human isophaneInsulin NPH, human/regular insulin HMInsulin NPH, human/regular insulin HMInsulin NPH, human/regular insulin HM
Rapid-acting insulin(vials)
Rapid-acting or mixedintermediate/rapid-actingvials
Vial Humalog, 10-mL vialHumalog, 3-mL vialApidraNovoLogHumalog Mix 75/25Humalog Mix 50/50NovoLog Mix 70/30
Insulin lisproInsulin lisproInsulin glulisineInsulin aspartInsulin lispro protamine/lisproInsulin lispro protamine/lisproInsulin aspart protamine & aspart
Rapid-acting insulin(pens)
Rapid-acting or mixedintermediate/rapid-acting pens
Pen orcartridge
Humalog cartridgeHumalog KwikPen U-100Apidra SoloSTARNovoLog cartridgeNovoLog FlexPenHumalog Mix 75/25 KwikPenHumalog Mix 50/50 KwikPenNovoLog Mix 70/30 FlexPen
Insulin lisproInsulin lisproInsulin glulisineInsulin aspartInsulin aspartInsulin lispro protamine/lisproInsulin lispro protamine/lisproInsulin aspart protamine & aspart
Long-acting insulin(vials/pens)
Long-acting vialsand pens
Vial or pen LantusLevemirLantus SoloSTARLevemir FlexPen
Insulin glargineInsulin detemirInsulin glargineInsulin detemir
Categories of insulin products evaluated by the USC Schaeffer Center for Health Policy & Economics investigators as part of the InsulinAccess and Affordability Working Group. aIn the case of the Novo Nordisk products (Novolin R, Novolin N, Novolin 70/30), one is the NovoNordisk–branded product, while the other corresponds to the same drug sold under the Relion brand. Each has a different national drugcode and sells for a different price. In the case of the Eli Lilly products (Humulin R, Humulin N, Humalog), different vial sizes are referenced(3 mL vs. 10 mL).
care.diabetesjournals.org Cefalu and Associates 3

an independent market research firm thatthe list price of Eli Lilly’s human insulin an-alog, Humalog, increased by 138% between2009 and 2015, while the net price to themanufacturer increased by 6% (21).Novo Nordisk also published data for
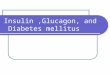
two of their insulin products, NovoLogand NovoLog FlexPen. Since the early2000s, the CAGRs for the list prices forNovoLog and NovoLog FlexPen (Fig. 7)have been in the range of 9.8–9.9% (22).This translated into large total increasesin the list prices: 353% (2001–2016) for
a NovoLog vial and 270% (2003–2016)for a FlexPen. In contrast, net pricesreceived by the manufacturer increasedat a more modest rate with CAGRs of3–36%dmore in line with the rate ofinflation for the overall economy. NovoNordisk, Eli Lilly, and Sanofi have reportedthat rebates have grown rapidly in recentyearsdrepresenting more than 40% ofU.S. gross sales in some cases (21,23). TheWorkingGroup found the transparency inlist versus net pricing for these two insulinformulationshelpful,butsimilardataonall
the other insulin productswill be necessaryfor clarity on this aspect of pricing in theinsulin supply chain.
This finding of greater increases in listprices than net prices raises the followingquestions. Who else has benefited orlost from the substantial increase in in-sulin list prices over the last decade? Andwhy has the financial burden for peoplewith diabetes who use insulin continuedto increasedespecially for those withoutinsurance who may have to pay the fulllist price?
Figure 1—Average WAC for insulins, by product category, 2012–2016. Source: USC Schaeffer Center analysis of First Databank data.
Figure 2—Average Medicare out-of-pocket spending for insulin, per user, by product category, 2006–2013. Source: USC Schaeffer Center analysis ofMedicare Part D claims data.
4 ADA Statement Diabetes Care

Role of Rebates and Discounts in thePricing of InsulinThe widening gap between the net andlist priceof insulin in recent years appearsto be the result of increasing rebatesanddiscountsnegotiatedbetween stake-holders. Manufacturers negotiate with aPBM for discounts from the list price tohave their medications placed on a lowercost-sharing tier and/or to avoid con-straints on utilization on the PBM’s clientformulary. In this process,manufacturersagree to fees and price concessions, typ-ically paid to the PBM after health planenrollees receive the manufacturer’smedication. These retroactive discounts orrebates are in addition to the fees paid toPBMs by the payers to provide the phar-macy benefit management services. Therate of increase in these rebates has ac-celerated to approach approximately halfof the list priceof insulin (21,23). PBMsalsonegotiate with pharmacies to determinehow much participating pharmacies willbe paid for medications dispensed toenrollees in the PBM client’s health plan.BecausePBMsdesigntheformularyfor
their clients, some stakeholders believePBMs have significant input into which
medications are on the formulary and atwhich tier, setting the parameters forpatient access to and cost-sharing forinsulins. Nationally, PBMs administer theprescriptionmedication benefit formorethan 266 million Americans, and thethreemajorPBMs (CVSCaremark, ExpressScripts, and OptumRx) manage about 70%of all prescription claims (13,24). Argu-ably, this gives PBMs considerable lever-age in any rebate/discount negotiationwith stakeholders.
Transparency and Flow of DollarsA consistent observation made to theWorkingGroupwas the lackof transparencythroughouttheinsulinsupplychain.Manyinterviewed stakeholders recommendedincreased transparency from entities acrossthe insulin supply chain. Manufacturersreported that without knowledge of thenegotiations that take place betweenPBMs and health plans, they are at adisadvantage in determining pricing fortheir insulin products. Manufacturersstate that the need to provide a higherrebate to achieve preferred formularypositioning impacts the list price of insu-lin. However, manufacturers do not know
where the dollars from increased rebates
flow.Health plans, pharmacists, and people
with diabetes also called for increasedtransparency,includingsheddingalightonhow the list price is set by the manufac-turer. Health plans stated thatwhile thereis no requirement to report factors thatdetermineincreasing listprices,privateandpublic payers are paying for themajority ofthecostsaslistpricescontinuetorise.Payerswould like more transparency in pharmacyacquisition prices and want more informa-tion on the therapeutic benefits of moreexpensive analog insulins. Pharmacists,patients, and providers also would likeformularydecisions tobemoretransparent.
After research and stakeholder discus-sions, it isstilluncleartotheWorkingGroupprecisely how the dollars flow and howmucheach intermediary profits. In the vastmajority of cases, discounts and rebatesnegotiated between PBMs and manufac-turers andbetweenPBMsandpharmacies,which affect the cost of insulin for peoplewith diabetes, are confidential. Even PBMclients are not privy to many of these ne-gotiations, nor do they know the net priceobtained by the PBM for insulins.
Figure 3—Schematic of insulin supply chain.
care.diabetesjournals.org Cefalu and Associates 5

How rebates and discounts are distrib-utedisalsounclear.Tolowerpatientcostsfor insulin, the rebates would need to bepassed through to individuals with di-abetes at the point of sale. Health planrepresentatives whomet with theWork-ing Group pointed out that this wouldminimize the incentive for PBMs to selectfor their formulary medications withhigher rebates. On the other hand, rep-resentatives of the PBMs told the Work-ingGroupthatwhentheyofferpartof therebates to their customers, it is morecommon for their customers to use therebates to lower overall premiums for
the plan than to use them to reducepatients’ cost-sharing for insulin at thepoint of sale. The Working Group couldnot confirm these claims.
An additional argument presented tothe Working Group was that the currentsystem appears to transfer profits fromone stakeholder to another. So, it is notclearwhoreallybenefits fromtherebatesand discounts provided to the variousstakeholders.
Formulary Decisions and IncentivesBased on the Working Group’s review ofthe insulin supply chain, it is clear that the
insulinmanufacturers still control the listprice of insulin, but ameaningful share ofthe negotiating power has shifted frommanufacturers to the PBMs. PBMs at-tempt to keepmedication costs down bymoving market share between compet-ing products, and their market power isdirectly related to their ability to provideexclusive formulary coverage for particu-lar brands of medications.
The PBMs told theWorking Group thatformulary determinations are first andforemost based on clinical considerations.However, when the PBM’s clinical expertsdetermine that one type of medication isnecessary on a given formulary tier butthere is no clinical preference for one brandor formulation over another, the PBMwillapproach manufacturers to seek rebatesin exchange for preferential formulary tier-ing. These types of negotiations help todeterminewhether aparticular insulinwillbe available at all to insured individualswith diabetes under a given health plan,and on which cost-sharing tier an insulinformulation will be placed. Sometimesa PBM will exclude a medication fromits national formulary if the PBM’s net costfor the medication is higher than a com-petitive or similar product. In addition toformulary placement, PBMs determinewhich and how many medications on theformulary are subject to utilization man-agement, suchasprior authorization, steptherapy, or quantity limits to steer pre-scribers and patients tomedications withbetter safety or efficacy profiles and/or lower net costs. PBMs may alsodevelop a list of preventive or essentialmedications, recommending the healthplan cover medications on the list with-out patient cost-sharing. Some types orbrands of insulins may be included onthese lists, but it varies from PBM to PBMand health plan to health plan.
TheWorking Groupwas informed thatthe PBMs generally pass a portion of therebates received from manufacturersback to the employer or health planand that in some cases, less than 10%of the rebate is retained by the PBM.These statements were not confirmedby the Working Group. In addition tonegotiating rebates with manufacturers,PBMschargeemployers,plans,andphar-maciesadministrative fees foravarietyofservices. Specifically, health plans andemployers pay PBMs a fee for utilizationmanagement, such as prior authorizationrequests for plan enrollees. To ensure the
Table 2—Glossary of drug pricing and health insurance terms
Term Definition
Formulary List of drugs covered under the health insurance plan. Oftenhas tiers with increasing cost-sharing. Also includesutilization management requirements such as priorauthorization, step therapy, or quantity limits.
List price Thepricemanufacturers set for theirmedications.Also calledwholesale acquisition cost or launch price. This price isoften the basis for rebates, discounts, and feesthroughout the insulin supply chain.
Rebate Adiscountpaidafter thepatienthas received themedication.Typically, manufacturers pay rebates to PBMs forprescriptions filled by the PBM’s clients. Rebatesnegotiated between manufacturers and PBMs are oftencontingent on placement of the drug on the PBM’sformulary.
Benefits Healthcareitemsorservicescoveredunderahealthinsuranceplan.
Coinsurance Cost-sharing for covered benefits based on the percentage oftheplan’s cost (for example, 20%). For example, if the cost-sharing for a doctor’s office visit is 20% coinsurance, theenrollee will pay 20% of the plan’s cost for the visit.
Co-payment Cost-sharing for covered benefits that is a flat dollar amount($20, for example).
Cost-sharing The portion of the cost of benefits covered by insurance thatthe plan enrollee pays out of his/her pocket. This termgenerally includes deductibles, coinsurance, andco-payments, or similar charges, but it does not includepremiums.
Deductible Theamounthealth planenrollees pay for coveredhealth careservices before the insurance plan starts to pay. Witha $2,000 deductible, for example, the plan enrollee mustpay the first $2,000 of covered benefits before theinsurance plan will pay for care.
Premium The amount paid each month for a health insurance policy.Often health plan enrollees are responsible for payinga portion of the cost of the care they receive in addition tothemonthlypremiumamount(seecost-sharingdefinition).
Prior authorization Requires prescribers to obtain preapproval from the healthplan before a medication will be covered. Often requiresclinical information about the medical necessity of themedication.
Step therapy Requirespatients to tryand fail oncertainmedicationsbeforethe requested medication will be covered by the plan.Often requires clinical information about the patient’shistory with medications preferred by the health plan.
6 ADA Statement Diabetes Care

PBM does not have a financial incentivetied to the number of medications requiringutilization management, some employersor plans outsource the processing of uti-lization management requests and appro-vals to another company.The insulin manufacturers told the
Working Group that they are not privyto the negotiations that take place be-tween PBMs and health plans. Further,employers and health plans that workwith PBMs noted that they are not privy tothe net prices the PBM negotiates withmanufacturers on their behalf. Instead,the PBM guarantees at the beginning
of the plan year the total dollar amountof rebates it will pay to the employer orhealth plan.
The health plans the Working Groupinterviewed reported that plans andPBMs have an incentive to select med-ications for their formularies that offera higher rebate. It was also suggested totheWorkingGroup that the need to offerhigher rebates in order to achieve pref-erential formulary positioning from PBMscreates an incentive formanufacturers toraise the listprice. Inaddition,wholesalersare paid for their distribution servicesas a percentage of the list price of the
medications they handle, even thoughtheir handling costs may not differ fromone product to another. Thus, there areincentives throughout the insulin supplychain for high list prices.
In contrast, stakeholders have notedthat thecurrentstructureof theMedicaidbest price requirements limit the amountof discounts or rebates manufacturersprovide in the commercial market. If amanufacturer agrees to provide specificrebates to theMedicaidprogram,all of itsmedications will be covered (with someexceptions) (25). The basic Medicaid re-bate calculation defined in federal law is
Figure 4—NADAC for five rapid-acting insulin pen or cartridge products, 2012–2016. Source: USC Schaeffer Center analysis of Centers for Medicare &Medicaid Services NADAC data.
Figure 5—Medicaremarket share of four insulin product categories, 2006–2013. Source: USC Schaeffer Center analysis ofMedicare Part D claims data.
care.diabetesjournals.org Cefalu and Associates 7

the larger of a standardpercentageof themedication’s average net price, or theaverage net price minus the “best price”the manufacturer provided to anotherpayer. In addition, if a medication’s av-erage net price increased by more thaninflation, the manufacturer must pay anadditional rebate to Medicaid. If a man-ufacturer’s rebate agreement with anon-Medicaid PBM or health plan re-sults in a net price lower than the netprice Medicaid would receive using thestandard percentage rebate calculation,the manufacturer must use that rebateagreement amount to calculate themedication’s rebate for all Medicaidenrollees. Stakeholders shared that theMedicaid best price requirement essen-tially sets a floor for negotiations withPBMs and health plans since manufac-turers are hesitant to provide a verylarge rebate to non-Medicaid plans thatwill also have to be paid to Medicaid.
Formulary Decisions and Patient HealthIt is clear that decisions made from ne-gotiations between stakeholders that
affect formulary choice may not be inthebestfinancialormedical interestofthepatient. People with diabetes informedthe Working Group that they have littlechoice inmedication coverage, particularlyfor those enrolled in employer-sponsoredplans. PBMs often exclude from for-mularies the insulins made by the man-ufacturer who offers the lowest rebate.As a result of these negotiations, rulesfor coverage differ from plan to plan andyear to year, or even within the sameplan year. When insulins are excludedfrom the formulary, moved to a differ-entcost-sharing tier,or removedduringthe plan year (sometimes called “non-medical switching”), providers and peoplewith diabetes can be inconveniencedand patients’ health may be adverselyaffected. For example, patients with highcost-sharing may be less adherent torecommended medication dosing andadministration, resulting in harm to theirhealth (9,26–30). In addition, formularyexclusions and frequent formulary changescause uncertainty, increase financial costsfor patients, increase work required by
providers, and could be undermining pa-tient health (31,32).
The Working Group noted concernabout the increased burden on peoplewith diabetes and reduced adherence toeffective management strategies. TheADA was provided with numerous sto-ries and complaints from constituentsregarding this concern. One such exam-ple comes from Kathy Sego, who signedthe ADA’s Make Insulin Affordablepetition and whose son, Hunter, hastype 1 diabetes. Hunter requires approx-imately four vials of insulin per monthto properly manage his diabetes, at amonthly out-of-pocket cost of $1,948until the family meets the health plandeductible. Knowing the impact of thiscost on his family, Hunter, a collegestudent in 2016, began skipping insulindoses, which can lead to serious and evendeadly complications (33). Hunter Sego isone example of themany individuals whostruggle to obtain the insulin they need tosurvive.Whenpeople are unable toaffordtheir cost-sharing, many resort to ration-ing or skipping doses in order to maketheir insulin supply last longer, riskingtheir health and their lives.
Formulary Decisions and PatientFinancial BurdenFormulary exclusions and frequent formu-lary changes increase financial costs forpatients. In addition, patients are bearingmore of the cost of medications becauseof high-deductible plans, increased use ofcoinsurance, growing number of formularytiers, and fewer medications covered pertier (34–36). Sincenegotiateddiscounts orrebates are usually not passed directly topeople with diabetes, their financial ob-ligations for purchasing insulin are oftenbased on the list price. Clearly, this variesdepending on the type of insurance theperson has and the type of insulin pur-chased(seebelow)butspecifically impactsthose with a high deductible, those whohave to pay coinsurance, or thosewhoarein the Medicare Part D coverage gap.People without insurance are often re-quired to pay list price for insulins.
Health plans noted that out-of-pocketinsulin costs could be lower for somepeople with diabetes if health savingsaccount–eligible high-deductible healthplans could exempt insulin from thedeductible. Manufacturers agree thatexempting insulin from the plan’s de-ductible is a critical step in lowering
Figure 6—Report of changes in list and net prices for Lantus. Reprinted by permission of theWallStreet Journal, Copyright © 2016, Dow Jones & Company, Inc. All Rights Reserved Worldwide.License number 4321941207734 (20).
8 ADA Statement Diabetes Care

out-of-pocket insulin costs. Until there isa systematic plan that addresses a changein benefit design to lower out-of-pocketinsulin costs for people with diabetes,human insulinmay be a valid alternativeto more expensive analog insulins forsomepatients (19,37). Inthisregard, therewould need to be significant education ofpeople with diabetes and health care pro-viders on the appropriate use of humanand analog insulins, and careful selectionof people who may benefit from analoginsulin.While data on average patient out-of-
pocket spending for insulinarenotwidelyavailable, one study found that patientout-of-pocket expenses for insulin dou-bledover a 10-year period.Using a privateinsurance administrative claims databasefor all insulin prescriptions filled at leastonce, the median out-of-pocket cost topatients went from $19 per vial of insulin
in 2000 to $36 per vial of insulin in2010 (38). In addition, Working Groupmembers with the USC Schaeffer Centerfound that average Medicare Part D ben-eficiary out-of-pocket costs for all insulintypes doubled between 2006 and 2013,from $27 per month to $65 per month.However, it should be noted that theseresults are average costs and do notcapture fluctuations in cost-sharing thatpatients experience throughout the year(suchas during thedeductiblephase), andthey do not capture patient costs whentheir insulin is not on their health plan’sformulary. In addition, these studies do notinclude people who are uninsured. Moreinformation is needed to better quantifyinsulin costs for people with diabetes.
Biosimilar InsulinsAnother issue raised by stakeholderswasthe lack of competition in the insulin
manufacturing sector and whether intro-duction of biosimilar insulins will lead tolower prices. The Working Group spokewithmanufacturers whowant to introducea biosimilar insulin into the U.S. marketwho said the increased regulatory bur-den associated with the development,as well as U.S. Food and Drug Admin-istration (FDA) approval, of biosimilarsis deterring manufacturers from pro-ducing biosimilar insulins.
Insulin is a biologic medication madefrom living cells and far more complex tomanufacture than small-molecule med-ications, which are made by combiningdifferent chemical ingredients (37). Be-fore 2010, a regulatory path was not inplace to allow for the development ofbiosimilarmedications, as therehasbeenfor decades for small-molecule drugs. If abiologic medication no longer had patentprotection, another company couldman-ufacture its own version. In order to ob-tain FDA approval, the company wouldnot be able to rely exclusively on safetyand efficacy data from the originalmanufacturer’s research, as is the casewith small-molecule generic drugs. To ad-dress this problem, Congress enacted theBiologics Price Competition and InnovationAct (BPCIA) as part of the Affordable CareAct in 2010. Under the BPCIA, companiesdeveloping alternatives to biologic med-ications (called “biosimilar”medications)must prove that their medication is“highly similar” to the original biologicand that there are no “clinicallymeaning-ful” differences from the original biologic(39). According to the FDA, “[t]his generallymeans that biosimilar manufacturersdo not need to conduct as many expen-sive and lengthy clinical trials, potentiallyleading to faster access to these prod-ucts, additional therapeutic options, andreduced costs for patients” (39). Themanufacturer of a biosimilar medicationcan submit additional data to the FDA tobe deemed “interchangeable” with theoriginal biologic medication. These datamust show that the biosimilar is “ex-pected to produce the same clinical re-sult” as the original biologic medicationand that “switching between the pro-posed interchangeable product and thereference product does not increasesafety risks or decrease effectivenesscompared to using the reference productwithout such switching” (39). Dependingon state laws, if a biosimilar is deemedinterchangeablebytheFDA,apharmacist
* Adjusted for inflation** 2016 reflects September YTD
0
50
100
150
200
250
300
350
400
450
500
Inde
x
Solid Line: List Price* Dashed Line: Net Price*
NovoLog® Vial
Net Price* CAGR +2.1%
+353%
+36%
0
50
100
150
200
250
300
350
400
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016**
Inde
x
Solid Line: List Price* Dashed Line: Net Price*
NovoLog® FlexPen
Net Price* CAGR +0.2%
+3%
+270%
Figure 7—Reported changes in NovoLog list and net prices. Adapted from Hobbs (22). YTD, yearto date.
care.diabetesjournals.org Cefalu and Associates 9

may fill a prescription written for theoriginal version with the biosimilar ver-sion,much like theycurrentlydoforothertypes of medications with so-called ge-neric medications. Prior to passage ofBPCIA, alternative versions of originalbiologic medications were referred toas“follow-onbiologics.”Asofthiswriting,there are no biosimilar insulins on themarket, but to date, three follow-on bi-ologic human insulin analogs have beenapproved by the FDA (40–42). Discussionwith stakeholders revealed differingopinions on howmuch biosimilars wouldlower the price of insulin. Currently, theonly follow-on biologic insulin on themarket was introduced with a list priceapproximately 15% less than the originalversion (43,44).
Patient Assistance ProgramsThe Working Group also reviewed in-formation regarding the value of phar-maceutical patient assistance programsas a solution to help peoplewith diabetesafford their insulin. However, it is beyondthe scope of this current report to pro-vide details, benefits, and value of all theavailable programs. Peoplewith diabeteswill need to discuss this option with theirphysician and health plan (if applicable)to determine what, if any, benefit thesepatient assistance programs could pro-vide to them individually. Although theWorking Group didnot address this optionin detail, it was not deemed to be a long-term or comprehensive answer to the risingcost of insulin for the vastmajority of peoplewith diabetes.
Continued Innovation for DiabetesTherapiesOne issue of importance to people withdiabetes is the need for continued in-novation in diabetes management andprevention. New technologies, pharma-cotherapies, and strategies continue tobeneededtopreventthedisease, todiminishadversesideeffects likehypoglycemiaandweight gain, to promote adherence, andto prevent complications. Such innova-tion would generate substantial value topeople with diabetes both now and inthe future (45). One of the best ways toencourage innovation is to better link re-imbursement to value (46). With value-based insurance design, the amount ofcost-sharing for a medical treatment orservice is set according to its value ratherthan its cost. Value-based insurancedesignprovides coverage for evidence-based
treatments that improve health by low-ering or eliminating patient cost-sharing.Efforts to encourage value-based insur-ance design, wherein cost-sharing is linkedto population health outcomes, may im-prove adherence and lower patient finan-cial burden (47).
PATIENT COST-SHARING:INSURANCE TYPE MATTERS
There are many factors that impact howmuch people with diabetes pay for in-sulin, including the amount and type ofinsulin and delivery system they use. An-other major factor is whether the personhasinsuranceand,ifso,whattype.Whetherthe person’s health insurance plan or itsPBM has negotiated rebates with insulinmanufacturers also impacts the costto people with diabetes. In the U.S.,there are many different types of healthinsurance.
Almost half of Americans have healthinsurance provided through their em-ployer or a family member’s employer(48). Employer coverage is generally reg-ulated by federal law, but employers haveleeway in determining which benefits tocover and how much to charge enrollees.Medicaid, a health insurance program forlow-income individuals, covers more than68 million Americans (20% of the popula-tion) (49). Each statemanages and admin-isters the Medicaid programs for theirresidents; however, they are required tofollow federal guidelines, which includelimits to the out-of-pocket costs to ben-eficiaries. Medicare, the federal healthcare program for Americans over age65 years, people with disabilities underage 65 years, and people with end-stagerenal disease, covers about 14% of Amer-icans (48). Federal rules dictate the bene-fits covered under Medicare and howmuch enrollees pay, including MedicarePart D, the program’s prescription drugbenefit. Approximately 7% of Americanspurchase insurance on their own directlyfrom an insurer or through state healthinsurance exchanges (called individualmarket insurance) (48). Federal and statelaws dictate which benefits are coveredin individual market insurance plans aswell asenrollees’annualspendingoncare.Roughly2%ofAmericansarecoveredunderother government programs like militaryor Veterans Administration coverage, and9%havenohealth insurance coverage (48).
To further understand how havinginsurance and insurance type impact
an individual’s insulin costs, the WorkingGroup provides several case scenarios,using an insulin with a list price of $480per vial as an example. (See Table 2 for aglossary of health insurance terms.)
The Uninsured PersonAn uninsured person with diabetes willpay the full $480 for the insulin, regardlessof any rebates offered by the manufac-turer. He or she could directly receivepayment assistance from the manufac-turer or a pharmaceutical patient assis-tance program, but eligibility for thoseprogramsvaries basedon the individual’sincome, state, and medication.
The Person With CommercialInsuranceA person with diabetes who has com-mercial insurance may pay less than the$480 list price, but the amount paiddepends upon the person’s insurancecontract. If the person is required to payan annual deductible that has not yetbeen reached (for example, if this is thepatient’s first expenditure in the new year),the person with diabetes will pay the full$480 list price for the insulin until theperson spends enough to meet the de-ductible. Once the deductible is met, ifthe person’s insurance contract specifiesafixedco-payment,heorshewillpayaflatamount,forexample,$50perprescription,even if the person with diabetes usesmultiple vials of the same insulin productpermonth.However, if the insuranceplanrequires coinsurance, the person with di-abeteswill pay a percentage, for example,20% of the cost of each vial of insulin. Im-portantly, the coinsurance is based onthe listpriceof the insulin, not thenet costafter any rebates or discounts negotiatedby thePBM. In this case, theout-of-pocketcost by the person with diabetes for theinsulin is $96 per vial (20% of the $480 listprice).
The Person With MedicareA Medicare beneficiary with Part D pre-scription drug coverage could face anarrayofdifferentbenefitdesignsandout-of-pocket expenditures, depending onthe type of plan in which the personwith diabetes enrolls, where the pre-scription is filled, and the phase of cov-erage. For example, in 2018 under thestandard benefit (see Fig. 8 for overviewof Medicare standard benefit structure)(50), beneficiaries face a deductible of$405andacoinsurance rateof25%.Thus,
10 ADA Statement Diabetes Care

onthefirstfill, thefirst$405ispaidout-of-pocket, plus 25% of the remaining costof the drug (25% of $75) for a total of$423.75. The 25% coinsurance rate ap-plies to additional fills until the personreaches the plan’s initial coverage limit($3,750 inmost plans in 2018) and entersthe coverage gap, commonly known asthe “donut hole.” Historically, beneficia-ries paid 100% of the Part D plan’s brand-name drug costs in the donut hole, buttheAffordableCareActhasreducedsomeof that burden. In 2018, beneficiaries pay35% of the Part D plan’s brand-namedrug costs (or $168 per prescriptionin this example) in the coverage gapuntil their annual out-of-pocket expensereaches $5,000. After that, beneficiariespay 5% of a drug’s list price ($24) for theremainderof the calendar year. Beginningin 2019, beneficiaries in the standardplan will pay 25% (or $120 per vial in thisexample) of the cost of their brand-nameprescription drugs once they meet theirdeductibleuntiltheyreachtheout-of-pocketmaximum.
The Person With MedicaidFor a person with diabetes withMedicaiddrug coverage, co-payments are generallylimited to a nominal amount ($1–$5) fordrugs on the preferred drug list.Medicaiddrug coverage varies from state to state,however, all states include some insulinson their preferred drug lists. If a Medicaidenrollee needs a medication not on thestate’s preferred drug list, the prescriber can
submit a request on his or her behalf statingthe medical need for the drug.
CONCLUSIONS ANDRECOMMENDATIONS
Afterdiscussionswithmorethan20stake-holders in the insulin supply chain, theWorkingGroupremainsconcernedbythecomplexity of the system. As outlined,there are numerous stakeholders in-volved in the delivery of insulin, withmultiple opaque transactions betweenand among these stakeholders (Fig. 3). Itwas also the consensus of the WorkingGroup that incentives throughout theinsulin supply chain facilitate and mayeven promote high list prices. The follow-ing sections provide the conclusions andrecommendations of theWorking Group.
Conclusionsc List prices of insulin have risen precipi-
tously in recent years. Between2002 and2013, the average price of insulin nearlytripled.
c The current pricing and rebate systemencourages high list prices.+ As list prices increase, the profits of
the intermediaries in the insulinsupply chain (wholesalers, PBMs,pharmacies) increase since each mayreceive a rebate, discount, or fee cal-culatedasapercentageof the listprice.
c There is a lack of transparency through-out the insulin supply chain. It is unclearprecisely how the dollars flow and howmuch each intermediary profits.
+ Manufacturers are rarely paid thelistpriceforinsulin.Theso-callednetpricedwhichreflectswhattheman-ufacturers receivedis much lower;however, in most cases, the dataare not available.
+ In the vast majority of cases, dis-counts and rebates negotiated be-tweenPBMsandmanufacturersandbetween PBMs and pharmacies,which affect the cost of insulinfor the person with diabetes, areconfidential.▪ PBM clients (often large employersinmost cases) are not privy to thesenegotiations,nordo theyknowthenet price obtained by the PBM forinsulins.
+ Formulary considerations and deci-sions are not transparent.
c PBMs have substantial market power.+ PBMs’ primary customers are healthplans and employers, not patients.
+ PBMs negotiate rebates from man-ufacturers using formulary place-ment as leverage.▪ PBMs often exclude from formular-ies the insulins made by the manu-facturer who offers the lowest rebate.
▪ As a result of negotiation, rules forcoverage differ from plan to plan andyear to year, or even within the sameplan year.
▪ When insulins are excluded fromthe formulary, moved to a different
cost-sharing tier, or removedduring
the plan year, it places a burden on
people with diabetes and providers
and may have a negative health
impact.+ PBMs receive administrative feesfrom their clients (health insuranceplans) for utilization managementservices (prior authorization, etc.).Often it is the PBM that determineswhich and how many drugs on theformulary are subject to utilizationmanagement.
c People with diabetes are financiallyharmedbyhigh listpricesandhighout-of-pocket costs.+ Regardless of the negotiated netprice, the cost of insulin for peoplewith diabetes is greatly influencedby the list price for insulins.▪ Out-of-pocket costs vary dependingupon the type of health insuranceeach individual has and the type ofinsulin prescribed. The costs can beFigure 8—Standard Medicare prescription drug benefit, 2018 (50).
care.diabetesjournals.org Cefalu and Associates 11

significantly higher for people whoare uninsured, who have an in-surance plan with a high deduct-ible, or who are in the MedicarePart D donut hole.
+Manufacturer rebates often are notdirectly passed on to people withdiabetes.
c Patients’medical carecanbeadverselyaffected by formulary decisions.+ People with high cost-sharing are lessadherent to recommended dosing,which results in short- and long-termharm to their health.
+ Formulary exclusions and frequentformulary changes cause uncertainty,increase financial costs for peoplewith diabetes, and could have seri-ous negative consequences on thehealth of people with diabetes.
c The regulatory framework for develop-mentandapprovalofbiosimilar insulinsis burdensome for manufacturers.+ There are not enough biosimilarinsulins on the market.
+ Prices for biosimilar insulins are notlikely to be lower unless there aremultiple biosimilars that can be sub-situted for the brand-name analoginsulin, rather than only one.
c Prescribing patterns have favorednewer, more expensive insulins.+ Newer insulins, including analogs,
are more expensive than older in-sulins including human insulins.
+ Human insulin may be an appropriatealternative to more expensive analoginsulins for somepeoplewithdiabetes.
Recommendationsc Providers, pharmacies, and health
plans should discuss the cost of insulinpreparations with people with diabe-tes tohelpunderstandtheadvantages,disadvantages, and financial implica-tions of potential insulin preparations.
c Providers should prescribe the lowest-priced insulin required to effectivelyand safely achieve treatment goals.+Thismay includeusinghuman insulin
in appropriately selected patients.+ Providers should be aware of the
risingcostof insulinpreparationsandhowthisnegativelyimpactsadherencetotheclinicaltreatmentbypeoplewithdiabetes.
+ Providers should be trained to appro-priately prescribe all forms of insulinpreparations based on evidence-based medicine.
c Cost-sharing for insured people withdiabetesshouldbebasedonthelowestprice available.
c Uninsuredpeoplewith diabetes shouldhave access to high-quality, low-costinsulins.
c Researchers should study the compara-tive effectiveness and cost-effectivenessof the various insulins.
c Listprice for insulins shouldmorecloselyreflectnetprice,andrebatesbasedonlistpriceshouldbeminimized.Thecurrentpay-ment system should rely less on rebates,discounts, and fees based on list price.
c Healthplansshouldensurethatpeoplewith diabetes can access their insulinwithout undue administrative burdenor excessive cost.+Payers, insurers,manufacturers, and
PBMs should design pharmacy for-mularies that include a full range ofinsulin preparations, including hu-man insulin and insulin analogs, inthe lowest cost-sharing tier.
c PBMsandpayers shoulduse rebates tolower costs for insulin at the point ofsale for people with diabetes.
c There needs to be more transparencythroughout the insulin supply chain.
c Payers, insurers,manufacturers, PBMs,and people with diabetes should en-courage innovation in thedevelopmentof more effective insulin preparations.
c TheFDAshould continue to streamlinethe process to bring biosimilar insulinsto market.
c Organizations such as the ADA shoulddo the following:+Advocateforaccesstoaffordableand
evidence-based insulin preparationsfor all people with diabetes.
+ Ensure that health providers receiveongoing medical education on howto prescribe all insulin preparations,including human insulins, based onscientific and medical evidence.
+Developand regularlyupdate clinicalguidelinesor standardsofcarebasedon scientific evidence for prescribingall forms of insulins and make theseguidelines easily available to healthcare providers.
+Make information about the advan-tages, disadvantages, and financial im-plications of all insulin preparationseasilyavailabletopeoplewithdiabetes.
Duality of Interest. D.G. has received researchsupport from the ADA to examine trends in insulin
pricing. D.G. is also a consultant to Precision HealthEconomics and owns equity in its parent company,Precision Medicine Group. W.H.H. serves as Chair,Data Safety Monitoring Board, Merck Sharp &Dohme, and as a consultant for Janssen ScientificAffairs, LLC. K.V.N. received research support fromtheADAtoexaminetrends in insulinpricingandhasconsulted for Precision Health Economics. A.C.P.has served on the Board of Directors for the ADA.S.I.T. has served as a consultant for Ionis Pharma-ceuticals; has received research support providedto University of Maryland School of Medicine byRegeneron Pharmaceuticals; and owns stock inCelgene, Amgen, and Abbott Laboratories. A.L.Y.served on the Board of Directors for the ADA andowns stock in Amgen and Bristol-Myers Squibbthrough a broker-managed account. No otherpotential conflicts of interest relevant to thisarticle were reported.
References1. Centers for Disease Control and Prevention.National Diabetes Statistics Report, 2017. Atlanta,GA, Centers for Disease Control and Prevention,U.S. Department of Health and Human Services,20172. American Diabetes Association. Economiccosts of diabetes in the U.S. in 2017. DiabetesCare 2018;41:917–9283. Hua X, Carvalho N, TewM, Huang ES, HermanWH, Clarke P. Expenditures and prices of anti-hyperglycemic medications in the United States:2002-2013. JAMA 2016;315:1400–14024. American Diabetes Association. Insulin stories[Internet].Availablefromhttps://makeinsulinaffordable.org/insulin-stories/. Accessed 1 March 20185. Picchi A. Soaring insulin prices have diabeticsfeeling the pain [article online]. CBS News Money-Watch,25August2016.Availablefromhttps://www.cbsnews.com/news/soaring-insulin-prices-have-diabetics-feeling-the-pain/. Accessed 1 March20186. Lipska K. Break up the insulin racket [articleonline]. New York Times, 20 February 2016. Avail-able fromhttps://www.nytimes.com/2016/02/21/opinion/sunday/break-up-the-insulin-racket.html. Accessed 4 March 20187. SchneiderA.Insulinpricespikeleavesdiabetespatients in crisis [article online]. Montana Stan-dard, 21 August 2016. Available from http://mtstandard.com/news/local/insulin-price-spike-leaves-diabetes-patients-in-crisis/article_74cd6b23-7d9d-5f36-9df0-9c72c5de9f1a.html. Accessed 5March 20188. RamseyL.A93-year-olddrugthatcancostmorethanamortgagepayment tellsuseverythingthat’swrong with American healthcare [article online].Business Insider, 16 September 2016. Availablefrom http://www.businessinsider.com/insulin-prices-increase-2016-9. Accessed 5March 20189. QuickStats:Percentage*ofadultsaged$45yearswho reduced or delayedmedication to savemoney†
in the past 12 months among those who wereprescribed medication, by diagnosed diabetesstatus and age§ - National Health Interview Sur-vey,2015.MMWRMorbMortalWklyRep2017;66:67910. United States Diabetes Surveillance System.Diabetic medication use [Internet], 2015. Atlanta,GA, Centers for Disease Control and Prevention.Available from https://gis.cdc.gov/grasp/diabetes/DiabetesAtlas.html#. Accessed 5 March 2018
12 ADA Statement Diabetes Care

11. Saydah SH. Medication use and self-carepractices in persons with diabetes. In Diabetesin America, 3rd ed. Cowie CC, Casagrande SS,Menke A, et al, Eds. Bethesda, MD, NationalInstitutes of Health, 2017(NIH publ. no. 17-1468)12. GoldmanDP,JenaAB,PhilipsonT,SunE.Druglicenses: anewmodel forpharmaceutical pricing.Health Aff (Millwood) 2008;27:122–12913. Sood N, Shih T, Van Nuys K, Goldman D. Theflow of money through the pharmaceutical dis-tribution system. Los Angeles, USC Leonard D.Schaeffer Center for Health Policy & Economics,June 201714. Beran D, Ewen M, Laing R. Constraints andchallenges in access to insulin: a global perspec-tive. LancetDiabetes Endocrinol 2016;4:275–28515. TsaiA.Therisingcostof insulin [articleonline].Diabetes Forecast, March 2016. Available fromhttp://www.diabetesforecast.org/2016/mar-apr/rising-costs-insulin.html. Accessed 5 March 201816. Ramsey L. The prices for life-saving diabetesmedications have increased again [article online].Business Insider, 15 May 2017. Available fromhttp://www.businessinsider.com/insulin-prices-increased-in-2017-2017-5. Accessed20March201817. Johnson CY. Why treating diabetes keepsgetting more expensive [article online].Washing-ton Post, 31October 2016. Available fromhttps://www.washingtonpost.com/news/wonk/wp/2016/10/31/why-insulin-prices-have-kept-rising-for-95-years/?utm_term5.9c77afd62bb0. Accessed 28February 201818. Luo J, Avorn J, Kesselheim AS. Trends inMedicaid reimbursements for insulin from 1991through 2014. JAMA Intern Med 2015;175:1681–168619. LipskaKJ,HirschIB,RiddleMC.Humaninsulinfor type 2 diabetes: an effective, less-expensiveoption. JAMA 2017;318:23–2420. Roland D, Loftus P. Insulin prices soar whiledrugmakers’ share stays flat [article online].Wall Street Journal, 7 October 2016. Availablefromhttps://www.wsj.com/articles/insulin-prices-soar-while-drugmakers-share-stays-flat-1475876764.Accessed 5 March 201821. LangrethR,KellerM,CannonC.Decodingbigpharma’s secret drug pricing practices [articleonline]. Bloomberg, 29 June 2016. Available fromhttps://www.bloomberg.com/graphics/2016-drug-prices/. Accessed 5 March 201822. Hobbs T. Our perspectives on pricing andaffordability [Internet], November 2016. NovoNordisk. Available from http://www.novonordisk-us.com/blog/perspectives/2016/november/our_perspectives.html. Accessed 6March 201823. Boss v. CVS Caremark, U.S. District Court,District of N.J. Case no. 2:17-cv-01823, complaintfiled 17 March 201724. Pharmaceutical CareManagement Association.What is a PBM? [Internet]. Available from https://www.pcmanet.org/our-industry/.Accessed20March201825. United States Code. 2008 Edition, Title 42,Section1396r-8. Payment for coveredoutpatientdrugs.Washington,DC,U.S.GovernmentPrintingOffice, 2008
26. Karter AJ, Parker MM, Solomon MD, et al.Effect of out-of-pocket cost on medication ini-tiation, adherence, and persistence among pa-tientswith type 2 diabetes: theDiabetes Study ofNorthern California (DISTANCE). Health Serv Res2017;53:1227–124727. Iuga AO, McGuire MJ. Adherence and healthcare costs. Risk Manag Healthc Policy 2014;7:35–4428. Egede LE, Gebregziabher M, Dismuke CE,et al. Medication nonadherence in diabetes:longitudinal effects on costs and potential costsavings from improvement. Diabetes Care 2012;35:2533–253929. Salas M, Hughes D, Zuluaga A, Vardeva K,Lebmeier M. Costs of medication nonadherencein patients with diabetes mellitus: a systematicreviewandcriticalanalysisof the literature.ValueHealth 2009;12:915–92230. GoldmanDP, Joyce GF, Zheng Y. Prescriptiondrug cost sharing: associations with medicationandmedical utilization and spending and health.JAMA 2007;298:61–6931. KesselheimAS,HuybrechtsKF,ChoudhryNK,et al. Prescription drug insurance coverage andpatienthealthoutcomes:asystematicreview.AmJ Public Health 2015;105:e17–e3032. RaischDW,Klaurens LM,HaydenC,Malagon I,Pulliam G, Fass R. Impact of a formulary changein proton pump inhibitors on health care costsand patients’ symptoms. Dig Dis Sci 2001;46:1533–153933. Tribble SJ. Flurry of federal and state probestarget insulin drugmakers and pharma middlemen[article online]. Kaiser Health News 30 October2017. Available from https://khn.org/news/flurry-of-federal-and-state-probes-target-insulin-drugmakers-and-pharma-middlemen/. Accessed5 March 201834. KaiserFamilyFoundationandHealthResearch& Educational Trust. Employer Health Benefits2017 Annual Survey [Internet], 19 September2017. Available from https://www.kff.org/health-costs/report/2017-employer-health-benefits-survey/.Accessed 26 February 201835. Thorpe KE, Allen L, Joski P. Out-of-pocketprescription costs under a typical silver planare twice as high as they are in the averageemployer plan. Health Aff (Millwood) 2015;34:1695–170336. Medicare Payment Advisory Commission.Status report on Part D. In Report to Congress:Medicare Payment Policy [Internet], March 2016.Washington, DC, Medicare Payment AdvisoryCommission. Available from http://www.medpac.gov/docs/default-source/reports/chapter-13-status-report-on-part-d-march-2016-report-.pdf?sfvrsn50.Accessed 26 February 201837. Dowlat HA, Kuhlmann MK, Khatami H,Ampudia-Blasco FJ. Interchangeability amongreference insulin analogues and their biosimi-lars: regulatory framework, study design andclinical implications. Diabetes Obes Metab 2016;18:737–74638. Lipska KJ, Ross JS, Van Houten HK, Beran D,Yudkin JS, Shah ND. Use and out-of-pocket costs
of insulin for type 2 diabetes mellitus from 2000through 2010. JAMA 2014;311:2331–233339. U.S. FoodandDrugAdministration.Biosimilardevelopment, review, and approval [Internet].Available from https://www.fda.gov/Drugs/DevelopmentApprovalProcess/HowDrugsare-DevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/Biosimilars/ucm580429.htm. Accessed 28 February 201840. U.S. Food and Drug Administration. Basaglar(insulin glargine injection) [Internet], 26 April 2016.Available from https://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/205692Orig1s000TOC.cfm. Accessed 28 February 201841. U.S. Food and Drug Administration. FDAapproves Admelog, the first short-acting “follow-on” insulin product to treat diabetes [news release],11December2017. Silver Spring,MD,U.S. FoodandDrug Administration, 201842. Merck. Merck announces U.S. FDA grantstentative approval for LUSDUNA Nexvue (insulinglargine injection), a follow-on biologic basalinsulin [press release], 20 July 2017. Keniworth,NJ, Merck & Co43. Ault A. Rising insulin costs in US get pushbackas Basaglar launches [article online]. MedScape,15 December 2016. Available from https://www.medscape.com/viewarticle/873353. Accessed5 March 201844. Ramsey L. A cheaper versionof the lifesavingdiabetes medication just launched in the US[article online]. Business Insider, 15 December2016. Available from http://www.businessinsider.com/insulin-cheaper-generic-2016-12.Accessed5 March 201845. Lakdawalla DN, Eber MR, Forma FM, et al.Measuring the value of better diabetes manage-ment. Am J Manag Care 2013;Mar-Apr:19 SpecNo. 2:E1146. Blumenthal DM, Goldman DP, Jena AB. Out-comes-based pricing as a tool to ensure access tonovel but expensive biopharmaceuticals. AnnIntern Med 2017;166:219–22047. Spaulding A, Fendrick AM, Herman WH,et al. A controlled trial of value-based insurancedesigndtheMHealthy:FocusonDiabetes(FOD)trial. Implement Sci 2009;4:1948. Kaiser Family Foundation. Health insurancecoverage of the total population [Internet], 2016.TheHenryJ.KaiserFamilyFoundation.Availablefromhttps://www.kff.org/other/state-indicator/total-population/?currentTimeframe50&sortModel5%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D. Accessed 26 February 201849. Centers for Medicare & Medicaid Services.January 2018 Medicaid and CHIP enrollment datahighlights [Internet]. Available from https://www.medicaid.gov/medicaid/program-information/medicaid-and-chip-enrollment-data/report-highlights/index.html. Accessed 26 February201850. KaiserFamilyFoundation.TheMedicarePartDprescriptiondrugbenefit [Internet],October2017.Available from http://files.kff.org/attachment/Fact-Sheet-The-Medicare-Part-D-Prescription-Drug-Benefit. Accessed 26 February 2018
care.diabetesjournals.org Cefalu and Associates 13