Embed Size (px)
Citation preview
Clinical Endocrinology (1991). 34, 159-171
Review
ADONIS 030006649100033P
Insulin action 1991
Roy Taylor Human Metabolism Research Centre, Department of Medicine, Medical School, Frarnlington Place, Newcastle upon Tyne NE2 4HH, UK
(Received 20 July 1990; accepted 7 September 1990)
This review attempts to summarize current knowledge about how insulin works. The title reflects the rapidly moving nature of this field and acknowledges the remarkable advances of the last decade. Insulin plays a central role in endocrinology, interacting with all other hormones in a clinically important manner. It is also the model polypeptide whose signal transduction has been most extensively studied. In this review the transmission of the insulin signal across the cell membrane and the subsequent events will be discussed, leading to a summary of clinical aspects of insulin action.
The insulin receptor
Cellular physiology
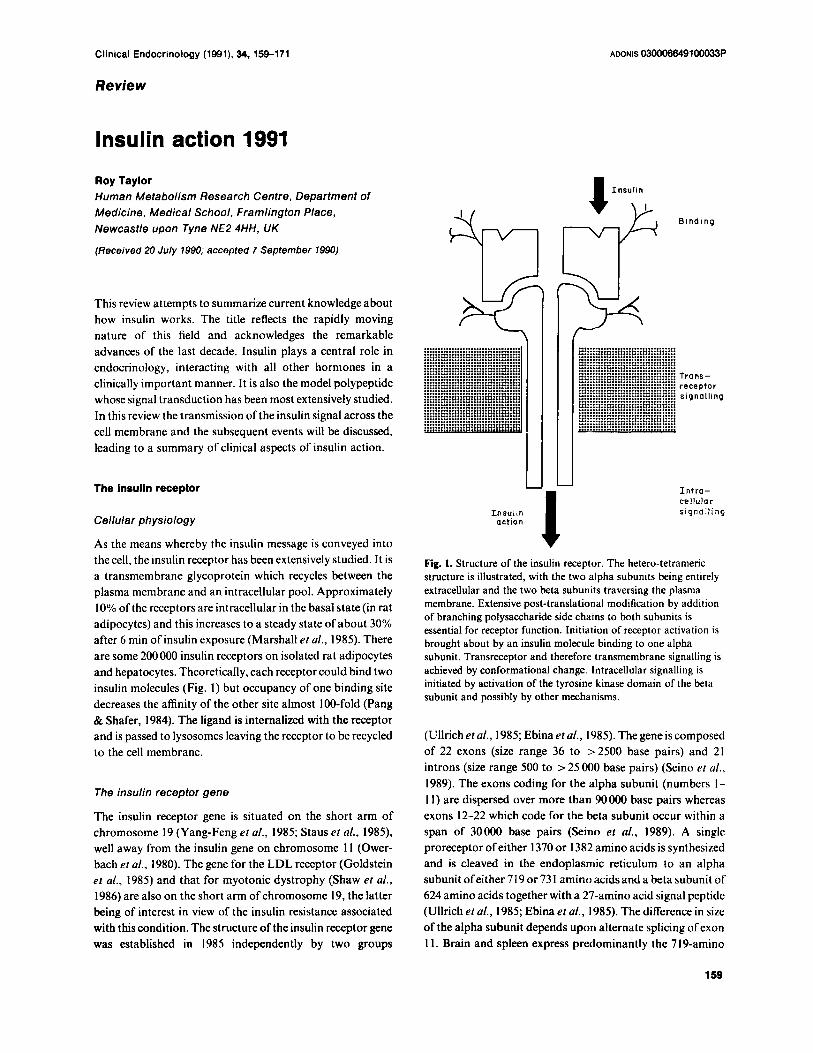
As the means whereby the insulin message is conveyed into the cell, the insulin receptor has been extensively studied. It is a transmembrane glycoprotein which recycles between the plasma membrane and an intracellular pool. Approximately 10% of the receptors are intracellular in the basal state (in rat adipocytes) and this increases to a steady state of about 30% after 6 min of insulin exposure (Marshall et al., 1985). There are some 200 000 insulin receptors on isolated rat adipocytes and hepatocytes. Theoretically, each receptor could bind two insulin molecules (Fig. 1) but occupancy of one binding site decreases the affinity of the other site almost 100-fold (Pang & Shafer, 1984). The ligand is internalized with the receptor and is passed to lysosomes leaving the receptor to be recycled to the cell membrane.
The insulin receptor gene
The insulin receptor gene is situated on the short arm of chromosome 19 (Yang-Feng el af., 1985; Staus et nl., 1985), well away from the insulin gene on chromosome 11 (Ower- bach el al., 1980). The gene for the LDL receptor (Goldstein et af., 1985) and that for myotonic dystrophy (Shaw et al., 1986) are also on the short arm of chromosome 19, the latter being of interest in view of the insulin resistance associated with this condition. The structure of the insulin receptor gene was established in 1985 independently by two groups
................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ............................ .. ..... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... . . A L
Insul in action i
Binding
................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ...................................
................................... Trans - ................................... ................................... receptor
................................... signalling ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... ................................... .................................
I n t r a - cellular signal l ing
Fig. 1. Structure of the insulin receptor. The hetero-tetrameric structure is illustrated, with the two alpha subunits being entirely extracellular and the two beta subunits traversing the plasma membrane. Extensive post-translational modification by addition of branching polysaccharide side chains to both subunits is essential for receptor function. Initiation of receptor activation is brought about by an insulin molecule binding to one alpha subunit. Transreceptor and therefore transmembrane signalling is achieved by conformational change. lntracellular signalling is initiated by activation of the tyrosine kinase domain of the beta subunit and possibly by other mechanisms.
(Ullrich eraf., 1985; Ebinaetal., 1985). Thegeneiscomposed of 22 exons (size range 36 to ~ 2 5 0 0 base pairs) and 21 introns (size range 500 to > 25 000 base pairs) (Seino el al., 1989). The exons coding for the alpha subunit (numbers I - 1 1) are dispersed over more than 90 000 base pairs whereas exons 12-22 which code for the beta subunit occur within a span of 30000 base pairs (Seino et al., 1989). A single proreceptor ofeither 1370 or 1382 amino acids is synthesized and is cleaved in the endoplasmic reticulum to an alpha subunitofeither719or731 aminoacidsanda betasubunit of 624 amino acids together with a 27-amino acid signal peptide (Ullrich et al., 1985; Ebina et al., 1985). The difference in size of the alpha subunit depends upon alternate splicing of exon 1 1. Brain and spleen express predominantly the 7 19-amino
1 59
160 R. Taylor
acid form whereas liver, kidney and adipose tissue express both forms (Seino & Bell, 1989). The implications of the existence of isoforms of the insulin receptor are unknown but could account for the observed heterogeneity of receptor size between different tissues.
After synthesis of the proreceptor on the endoplasmic reticulum, its asparagine residues are glycosylated largely with mannose, forming branching side chains. It is then transferred to the Golgi apparatus where proteolytic clea- vage forms separate alpha and beta subunits which undergo addition of glucosamine, fucose, sialic acid and fatty acyls (Forsayeth et al., 1986; Hedo et al., 1987; Herzberg et al., 1985). The subunits then dimerize by the formation of disulphide bonds to form heterotetrameric mature receptors (Fig. 1). The post-translational modifications are essential for insulin binding to occur (Forsayeth et al., 1986) and it may readily be appreciated that possibilitiesexist for function- ally significant aberrations to occur which are not reflected in the insulin receptor gene itself.
Transrnernbrane signalling
The means whereby the insulin signal is transmitted across the receptor were obscure until recently (Fig. I). It is now
a a
R Phe-88,89
Cys-rich (1 5531 2)
clear that the tyrosine kinase of the beta subunit is constitu- tively active, and that the alpha subunit exerts a tonic inhibitory effect to repress tyrosine kinase activity (Ellis et al., 1987). Insulin binding to the alpha subunit is likely to induce a conformational change which relieves the tonic inhibition.
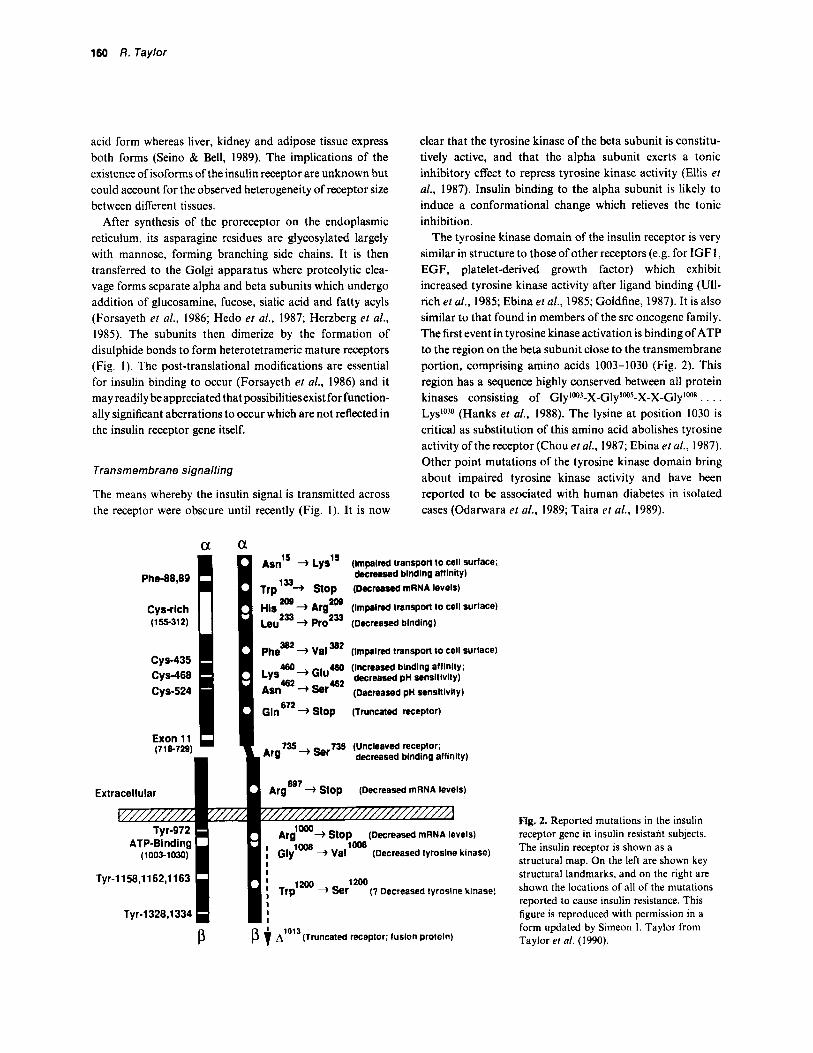
The tyrosine kinase domain of the insulin receptor is very similar in structure to those of other receptors (e.g. for IGFI, EGF, platelet-derived growth factor) which exhibit increased tyrosine kinase activity after ligand binding (Ull- rich et al., 1985; Ebina et al., 1985; Goldfine, 1987). It is also similar to that found in members of the src oncogene family. The first event in tyrosine kinase activation is binding of ATP to the region on the beta subunit close to the transmembrane portion, comprising amino acids 1003-1030 (Fig. 2). This region has a sequence highly conserved between all protein kinases consisting of Gly1w3-X-Gly'w5-X-X-Glylws . . . . LysloSo (Hanks et a[., 1988). The lysine at position 1030 is critical as substitution of this amino acid abolishes tyrosine activity of the receptor (Chou et al., 1987; Ebina et al., 1987). Other point mutations of the tyrosine kinase domain bring about impaired tyrosine kinase activity and have been reported to be associated with human diabetes in isolated cases (Odarwara et al., 1989; Taira et al., 1989).
cys-435
cys-524 Cys-468
Exon 11 (716729)
As;' + L~S"
Trp la+ Stop
His Leu2= -) pro2= (Decreased blndlng)
pheN2 + Val 382 (Impelred transport to cell surface)
(Impaired transport to cell surtace; decreased blndlng affinity) (Decreased mRNA levels)
+ Argm (Impelred transport lo cell surface)
460 (Increased blndlng alllnlty; 460 4 &reared pn sensitivity)
(Decreased pH sensitivity)
G I ~ ~ ~ ~ + stop (Truncated receptor)
735 (Uncleaved receplor; Arg735+ Ser deereased blndlng afflnity)
Extracellular ArgEg7 4 stop (Decreased mRNA levels)
Tyr-1158,1162,1163 1200 + Ser (7 Decreased tyrosine kinase)
P p A'0'3(Truncated receptor; fuslon protein)
Fig. 2. Reported mutations in the insulin receptor gene in insulin resistant subjects. The insulin receptor is shown as a structural map. On the left are shown key structural landmarks. and on the right are shown the locations of all of the mutations reported to cause insulin resistance. This figure is reproduced with permission in a form updated by Simeon I . Taylor from Taylor er a/. (1990).

Insulin action 1910 161
The second event in tyrosine kinase activation is autophos- phorylation of the receptor on tyrosines in two groups at amino acids 1158, 1162, 1163, and 1328, 1334 (Tornqvist & Avruch, 1988). Substitutions of tyrosines 1162 and 1163 decrease kinase activity and insulin-stimulated glucose uptake (Ellis et al., 1986). Following ATP binding and tyrosine autophosphorylation the beta subunit is capable of phosphorylating substrates within the cell. Once autophos- phorylation has taken place the binding of insulin to the alpha subunit is no longer required for its continued activity and the receptor is inactivated only by dephosphorylation (Rosen ei al., 1983; Zick et al., 1983). Serine phosphorylation of the beta subunit occurs in intact cells (not isolated receptor preparations) and is presumed to exert a regulatory influence on receptor activity (Takayama ef al., 1980; Kasuga ei al., 1982).
Tyrosine phosphorylation via the kinase is the only known function of the insulin receptor at present. It remains uncertain whether all or only some of the intracellular effects of insulin are mediated by this means. The studies using site- directed mutagenesis discussed above and others using microinjected antibodies to phosphotyrosine have shown that 2-deoxyglucose uptake and glycogen synthesis stimula- tion by insulin is inhibited by prevention of tyrosine kinase activity (Ellis et al., 1986; Chou er al., 1987; Ebina et al., 1987; Goldfine, 1987; Morgan & Roth, 1987). On the other hand, replacement of tyrosines 1162 and 1163 does not alter the mitogenic effect of insulin (Debant et al., 1988). Further- more, anti-receptor antibodies which mimic insulin in stimu- lating glucose uptake and antilipolysis in adipocytes d o not all bring about activation of tyrosine kinase (Forsayeth et al., 1987; Soos et al., 1989; Hawley et al., 1989).
Observation that not all actions of insulin are modulated in parallel by treatment of insulin-resistant states suggested that divergent pathways of intracellular signal transmission operate (Boden et al., 1983; Pedersen et al., 1982; Taylor & Agius, 1988). Study of a mutant insulin receptor lacking 43 amino acids from the COOH terminal of the beta subunit (but showing normal kinase activity) has shown abolition of transduction of signal in stimulating acute metabolic re- sponses but enhancement of transduction of signal in stimulating cell growth (Maegawa et al., 1988). Transfection of a kinase-deficient receptor into a cell line brought about dominant inhibitory effect on insulin signalling via the native insulin receptors but allowed study of effects brought about by IGFl stimulation (McClain et al., 1990). IGFl was able to stimulate glucose uptake normally, but could not stimulate cell growth in the transfected cells. This suggests that the signalling pathway for mitogenesis is shared by the insulin and IGF I receptors and that they operate different signalling pathways for stimulation of acute metabolic events at least in
the cell line studied. These studies imply the existence of more than one signalling pathway mediated by the receptor tyrosine kinase, and leave open the possibility that signalling may occur by other means.
Signalling after the receptor
Set against the striking clarity with which signalling across the cell membrane may now be visualized, the link between the activated receptor and target enzymes remains an arcane subject of conjecture.
Insulin can bring about effects by achieving dephosphory- lation of some enzymes (Lamer, 1971; Coore et al., 1971; Kennelly & Rodwell, 1985) but phosphorylation of others (Alexander et ul., 1979; Brownsey & Denton, 1982). It may thus be postulated that insulin signalling involves a protein phosphorylation cascade which achieves the generation of one or more second messengers acting in ways analogous to cyclic nucleotides. However, second messengers mediating the acute effects of insulin must ultimately act upon a kinase or phosphatase.
Phosphoinositol glycan release
Analysis of several putative second messengers revealed the common presence of inositol (Salteil et al., 1986; Kelly ef al., 1986; Salteil, 1987). It is now clear that a novel glycosylated inositol derivative is involved, this being produced by hydrolysis of a membrane-linked phosphoinositol (Salteil, 1990). This hydrolysis is brought about by activation of a specific plasma-membrane-bound phospholipase-C. Whether release of the phosphoinositol glycan is entirely intracellular or also extracellular remains uncertain (Salteil ei al., 1988; Alvarez et al., 1988). It is of interest to note that lipoprotein lipase, which is released from adipocytes in uiuo in response to insulin, is released from cultured adipocytes with identical kinetics by insulin and phospholipase-C (Chan er al., 1988). This implies tight coupling to an exofacial phosphoinositol glycan.
The precise mode of linkage between the insulin receptor and the membrane-bound phospholipase-C remains uncer- tain. It could depend upon coupling by the G-protein system which acts as an integrator of individual hormone signals (Houslay el al., 1989). Some G-proteins are potential substrates for the insulin receptor kinase (O'Brien et a]., 1987). However, coupling may be achieved by non-covalent interaction within the membrane, and it may be postulated that the kinase-independent stimulation achieved by some anti-receptor antibodies could be mediated by conformation- a1 changes similar to those induced by autophosphorylation (Forsayeth et al., 1987; Soos et al., 1989; Hawley et al., 1989).

162 R. Taylor
Diacylglycerol is released along with the phosphoinositol glycan. This may act as a messenger in its own right by activating protein kinase C. However, non-specific acti- vation of protein kinase-C by phorbol esters inhibit some actions of insulin (Van der Werve et al., 1985). The production of a structurally distinct diacylglycerol (lacking the usual arachadonate) may underlie selective activation of isoforms of protein kinase-C capable of mediating the specific actions of insulin (Pelosin et al., 1987). Recently evidence has been produced suggesting that insulin induces diacylglycerol synthesis from phosphatidic acid in soleus muscle and diaphragm (Ishizuka etal., 1990). Not all studies confirm the involvement of phosphoinositol glycan and diacylglycerol in insulin action and it remains to be estab- lished whether this reflects differences between different cells, methodological factors, or the existence of this attractive signalling pathway (Spach et al., 1986; Taylor et al., 1985).
Phosphorylation cascade
Involvement of a phosphorylation cascade is suggested not only by the fact of the insulin receptor tyrosine kinase but also by the need for amplification of the insulin signal. Occupancy of some hundreds of receptors must bring about activation of approximately los target enzyme molecules within the cell. In cell-free systems tyrosine phosphorylation of many candidate molecules has been demonstrated (Har- ingetal., 1985; Nishidaetal., 1987; Sturgilletal., 1988;Sacks & McDonald, 1988). However, few have been shown to be phosphorylated on tyrosine in intact cells, including micro- tubule-associated proteins. These are attractive substrates in view of the ability of insulin to induce cellular changes in morphology (Kadowaki et al., 1986). By preincubating cells with 3zP and subsequently with insulin, several phosphopro- teins have been detected ranging in molecular weight from I5 to 240 kDa. One of the best characterized is pp185 which is rapidly phosphorylated by physiological concentrations of insulin and has been detected in several cell types (White et al., 1985, 1987; Maegawa et al., 1988). Cells transfected with insulin receptors lacking tyrosine kinase activity do not produce ppl85 in response to insulin stimulation (Maegawa er al., 1988). Interestingly, point mutation of tyrosine 960 allowed continued tyrosine kinase activity but abolished both pp185 synthesis and insulin action (White et al., 1988).
The minimal phosphorylation cascade which may be postulated would involve the following steps: (1) the receptor tyrosine kinase phosphorylating and activating a serine kinase; (2) the activated serine kinase phosphorylating enzymes, which (3) finally result in dephosphorylation of serine or threonine residues on regulatory enzymes. The involvement of serine kinases is suggested by the observation
of extensive serine phosphorylation in '*P-labelled cells stimulated by insulin (Czech el al., 1988). Several serine kinases are known to be activated by insulin but their direct involvement in insulin signalling is uncertain. These include the S6 kinase (Jeno etaf., 1988) and glycogen synthase kinase 3 (see below) (Yang et al., 1989). A serine kinase associated with the high-density microsome fraction of adipocytes is notable in that it exhibits half-maximal stimulation at insulin concentrations one-tenth of those required for half-maximal activation receptor tyrosine kinase in intact cells (Yu el al., 1987). The insulin receptor itself is a substrate for a specific serine kinase which is regulated by the receptor tyrosine kinase activity, presumably as a n autoregulatory mechanism (Smith & Sale, 1988). Study of phosphorylation cascades resulting from receptor tyrosine phosphorylation is currently a promising and active area of research.
Glucose transporters
Transport of glucose into muscle and adipose tissue cells appears to be rate limiting for glucose metabolism under physiological conditions of insulin stimulation (Yki-Jarvi- nen et al., 1987; Pedersen et al., 1982). It may therefore be an important insulin regulatory step. Glucose transporters are facilitated diffusion channels and a specific insulin-sensitive transporter (GLUT4) exists in muscle and adipose tissue (James et al., 1989). Insulin mediates translocation of this transporter from an intracellular pool to the cell membrane (Cushman & Wardzala, 1980; Suzuki & Kono, 1980). The mechanism of induction of movement of the cytoskeleton or microtubular system is presently unknown. However, obser- vation of disproportionate stimulation of glucose transport compared with increase in plasma membrane transporter numbers has led to the concept that the efficiency of diffusion across the transporter is capable of being enhanced by insulin. The intrinsic activity of the transporters is decreased by isoproterenol, and this may be mediated by serine phosphorylation (Joost et al., 1986; James ct al., 1990). However, no phosphorylation or de-phosphorylation in response to insulin has yet been described. Hypothetically, non-covalent interactions between insulin receptor and glucose transporter (possibly via G-proteins) could explain increased efficiency of the transporters, but vesicles made from skeletal muscle have both insulin receptors and glucose transporters yet show no increased rate of glucose uptake with insulin stimulation (Sternlicht et al., 1988). Diacylglycerol in high concentration has been indirectly demonstrated to increase glucose transporter efficiency (Stralfors, 1988). In rat muscle, diacylglycerol increases glucose transport, possibly via protein kinase-C (Ishizuka et al., 1990).
Insulin action 1991 163
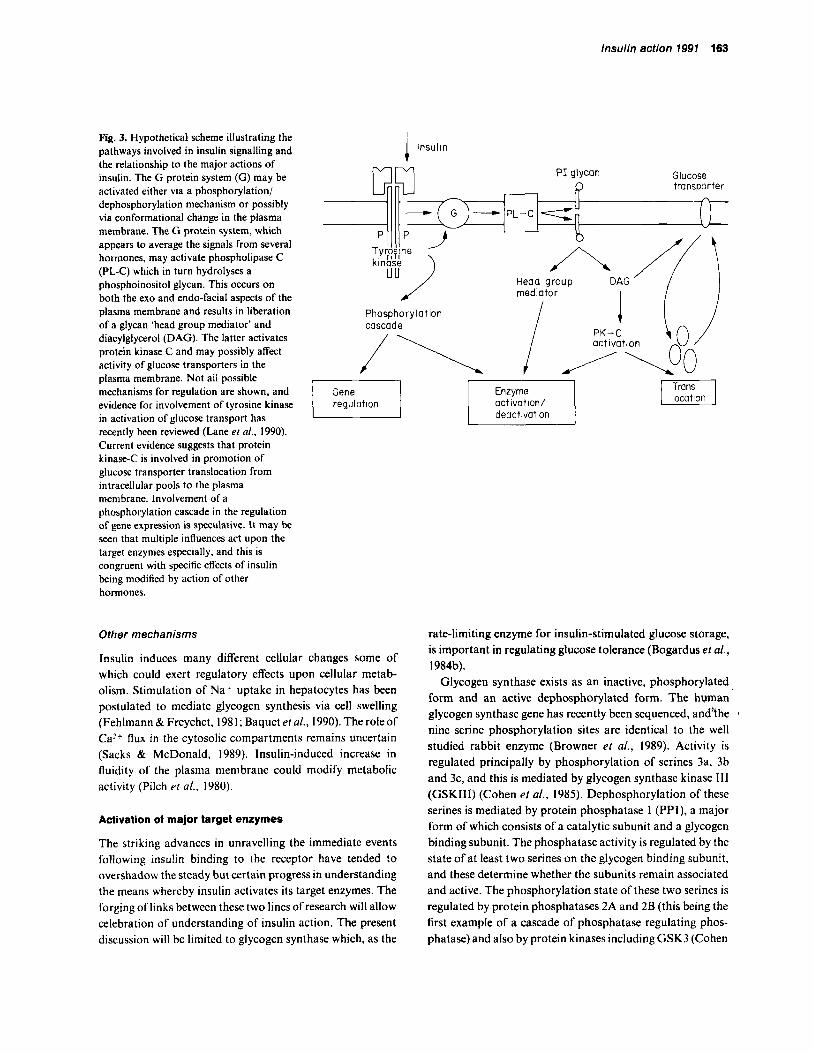
Fig. 3. Hypothetical scheme illustrating the pathways involved in insulin signalling and the relationship to the major actions of insulin. The G protein system (G) may be activated either via a phosphorylation/ dephosphorylation mechanism or possibly via conformational change in the plasma membrane. The G protein system, which appears to average the signals from several hormones, may activate phospholipase C (PL-C) which in turn hydrolyses a phosphoinositol glycan. This occurs on both the exo and endo-facial aspects of the plasma membrane and results in liberation of a glycan 'head group mediator' and diacylglycerol (DAG). The latter activates protein kinase C and may possibly affect activity of glucose transporters in the plasma membrane. Not all possible mechanisms for regulation are shown, and evidence for involvement of tyrosine kinase in activation of glucose transport has recently been reviewed (Lane et al., 1990). Current evidence suggests that protein kinase-C is involved in promotion of glucose transporter translocation from intracellular pools to the plasma membrane. Involvement of a phosphorylation cascade in the regulation of gene expression is speculative. It may be seen that multiple influences act upon the target enzymes especially, and this is congruent with specific effects of insulin being modified by action of other hormones.
insulin i
r I l regulation
Other mechanisms
Insulin induces many different cellular changes some of which could exert regulatory effects upon cellular metab- olism. Stimulation of Na+ uptake in hepatocytes has been postulated to mediate glycogen synthesis via cell swelling (Fehlmann & Freychet, 198 1 ; Baquet el al., 1990). The role of Ca2+ flux in the cytosolic compartments remains uncertain (Sacks & McDonald, 1989). Insulin-induced increase in fluidity of the plasma membrane could modify metabolic activity (Pilch et al., 1980).
Activation of major target enzymes
The striking advances in unravelling the immediate events following insulin binding to the receptor have tended to overshadow the steady but certain progress in understanding the means whereby insulin activates its target enzymes. The forging of links between these two lines of research will allow celebration of understanding of insulin action. The present discussion will be limited to glycogen synthase which, as the
deactivation
rate-limiting enzyme for insulin-stimulated glucose storage, is important in regulating glucose tolerance (Bogardus et al., 1984b).
Glycogen synthase exists as an inactive, phosphorylated form and an active dephosphorylated form. The human glycogen synthase gene has recently been sequenced, andrhe I
nine serine phosphorylation sites are identical to the well studied rabbit enzyme (Browner ef a/., 1989). Activity is regulated principally by phosphorylation of serines 3a, 3b and 3c, and this is mediated by glycogen synthase kinase 111 (GSKIII) (Cohen et al., 1985). Dephosphorylation of these serines is mediated by protein phosphatase 1 (PPI), a major form of which consists of a catalytic subunit and a glycogen binding subunit. The phosphatase activity is regulated by the state of a t least two serines on the glycogen binding subunit, and these determine whether the subunits remain associated and active. The phosphorylation state of these two serines is regulated by protein phosphatases 2A and 2B (this being the first example of a cascade of phosphatase regulating phos- phatase) and also by protein kinases including GSK3 (Cohen
164 R. Taylor
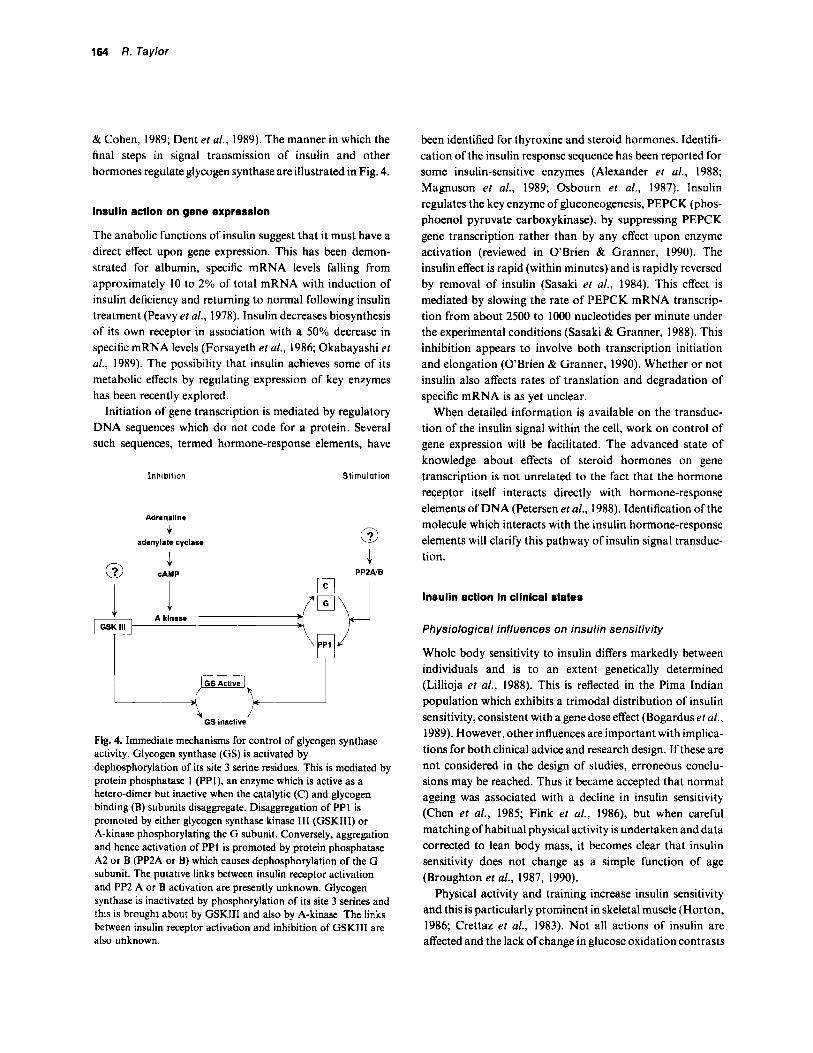
& Cohen, 1989; Dent et al., 1989). The manner in which the final steps in signal transmission of insulin and other hormones regulate glycogen synthase are illustrated in Fig. 4.
Insulin action on gene expression
The anabolic functions of insulin suggest that it must have a direct effect upon gene expression. This has been demon- strated for albumin, specific mRNA levels falling from approximately 10 to 2% of total mRNA with induction of insulin deficiency and returning to normal following insulin treatment (Peavy et al., 1978). Insulin decreases biosynthesis of its own receptor in association with a 50% decrease in specific mRNA levels (Forsayeth et al., 1986; Okabayashi et ul., 1989). The possibility that insulin achieves some of its metabolic effects by regulating expression of key enzymes has been recently explored.
Initiation of gene transcription is mediated by regulatory DNA sequences which do not code for a protein. Several such sequences, termed hormone-response elements, have
Inhibition Stimulation
Adrenaline
c adenylate cyclase 0
.1 @ cAMP
I I PPPAlB
Yl+ GS inactive
Fig. 4. Immediate mechanisms for control of glycogen synthase activity. Glycogen synthase (GS) is activated by dephosphorylation of its site 3 serine residues. This is mediated by protein phosphatase I (PPI), an enzyme which is active as a hetero-dimer but inactive when the catalytic (C) and glycogen binding (B) subunits disaggregate. Disaggregation of PPI is promoted by either glycogen synthase kinase 111 (GSKIII) or A-kinase phosphorylating the G subunit. Conversely, aggregation and hence activation of PPI is promoted by protein phosphatase A2 or B (PP2A or B) which causes dephosphorylation of the G subunit. The putative links between insulin receptor activation and PP2 A or B activation are presently unknown. Glycogen synthase is inactivated by phosphorylation of its site 3 serines and this is brought about by GSKIII and also by A-kinase. The links between insulin receptor activation and inhibition of GSKIII are also unknown.
been identified for thyroxine and steroid hormones. Identifi- cation of the insulin response sequence has been reported for some insulin-sensitive enzymes (Alexander et al., 1988; Magnuson et al., 1989; Osbourn et al., 1987). Insulin regulates the key enzyme of gluconeogenesis, PEPCK (phos- phoenol pyruvate carboxykinase), by suppressing PEPCK gene transcription rather than by any effect upon enzyme activation (reviewed in OBrien & Granner, 1990). The insulin effect is rapid (within minutes) and is rapidly reversed by removal of insulin (Sasaki et al., 1984). This effect is mediated by slowing the rate of PEPCK mRNA transcrip- tion from about 2500 to 1000 nucleotides per minute under the experimental conditions (Sasaki & Granner, 1988). This inhibition appears to involve both transcription initiation and elongation (OBrien & Granner, 1990). Whether or not insulin also affects rates of translation and degradation of specific mRNA is as yet unclear.
When detailed information is available on the transduc- tion of the insulin signal within the cell, work on control of gene expression will be facilitated. The advanced state of knowledge about effects of steroid hormones on gene transcription is not unrelated to the fact that the hormone receptor itself interacts directly with hormone-response elements of DNA (Petersen et al., 1988). Identification of the molecule which interacts with the insulin hormone-response elements will clarify this pathway of insulin signal transduc- tion.
Insulin actlon In cllnlcal states
Physiological influences on insulin sensitivity
Whole body sensitivity to insulin differs markedly between individuals and is to an extent genetically determined (Lillioja et al., 1988). This is reflected in the Pima Indian population which exhibits a trimodal distribution of insulin sensitivity, consistent with a gene dose effect (Bogardus et af., 1989). However, other influences are important with implica- tions for both clinical advice and research design. If these are not considered in the design of studies, erroneous conclu- sions may be reached. Thus it became accepted that normal ageing was associated with a decline in insulin sensitivity (Chen et al., 1985; Fink et al., 1986), but when careful matching of habitual physical activity is undertaken and data corrected to lean body mass, it becomes clear that insulin sensitivity does not change as a simple function of age (Broughton et al., 1987, 1990).
Physical activity and training increase insulin sensitivity and this is particularly prominent in skeletal muscle (Horton, 1986; Crettaz et al., 1983). Not all actions of insulin are affected and the lack ofchange in glucose oxidation contrasts

Insulin action 1991 165
with the increased glucose storage as glycogen (Bogardus et al., 1984a). Conversely, bed-rest decreases insulin sensitivity for glucose storage in muscle without major change in liver (Stuart et a[., 1988). Body composition influences overall insulin sensitivity, the latter being directly related to percent- age muscle mass and indirectly related to percentage adipose tissue mass (Yki-Jarvinen & Koivisto, 1983). The type of obesity must be considered, disproportionate intra-abdomi- nal adiposity being deleterious (Evans et al., 1984; Fujioka et a[., 1987). There may be a threshold effect whereby subjects below a body mass index of 27 kg/m2 do not show effects on insulin action by varying adiposity (Campbell & Gerich, 1990).
Both short-term overnutrition and fasting bring about decreased insulin-stimulated glucose metabolism (Mott et at., 1986; Newman & Brodows, 1983). The detailed response of muscle to fasting is of interest in that the insulin receptor tyrosine kinase activity retains a normal response to insulin and muscle insulin receptor numbers fall only slightly, suggesting that impairment of the insulin signal occurs at a subsequent step (Balage et al., 1990). In contrast, liver insulin receptors displayed a 50% decrease in insulin-stimulated kinase activity in the same study. This is a good example of the potential hazards in extrapolating events or mechanisms between tissues. A further example of this is the observation that the decrease. in insulin sensitivity of pregnancy is expressed only in muscle during mid pregnancy and in both muscle and liver during later pregnancy (Haugel et al., 1987).
Non-insulin dependent diabetes
In contrast to the hormone deficiency disease of insulin- dependent diabetes, the precise pathophysiology of non- insulin-dependent diabetes remains enigmatic. NIDDM does not present until insulin secretory defects are pro- nounced, but insulin insensitivity is a pre-existing feature (Kadowaki, 1984; Eriksson et al., 1989; Lillioja et al., 1988; reviewed in Taylor, 1989). NIDDM is characterized by markedly decreased insulin-stimulated glucose disposal as a consequence of failure of activation of glycogen synthase (Bogardus et al., 1984b; Johnson el al., 1990). This is usually assessed under the unphysiological conditions of euglycae- mic hyperinsulinaemia, but activation of muscle glycogen synthase is also abnormal after a mixed meal (Wright et al., 1988). Autophosphorylation of insulin receptors in muscle has been reported to be normal, but activation of the receptor tyrosine kinase, subnormal (Caro et al., 1987). The defect in kinase activation was only as severe as that for equivalently obese subjects, and this has been corroborated for less extremely obese NIDDM and control subjects (Arner et al., 1987). This does not explain the disproportionately
greater defect in stimulated glucose disposal in NIDDM, and awaits explanation. Increasing numbers of cases of NIDDM associated with mutations of the insulin receptor gene are being reported (Shimada et al., 1990; Taylor et al., 1990) (Fig. 2). Disorders of the primary structure of the insulin receptor are likely to explain only a minority of cases of impaired insulin action (Cama et al., 1990) although it must be considered that carriage of alleles for extreme insulin resistance, such as leprechaunism may affect as many as 1 in 1000 of the population (Taylor et al., 1990). Glucose transporters are being studied intensively at present, but there is no compelling evidence to suggest that abnormalities in these facilitated diffusion channels could relate to the aetiology of the disease.
Interest has recently centred upon amylin, a peptide which is co-secreted with insulin and which is a major component of the amyloid deposit typically seen associated with the beta cell membrane in NIDDM (Cooper et al., 1987). This obviously may interfere with insulin secretion and is highly likely to explain the insulin secretory defect. Amylin has also been suggested to bring about insulin insensitivity in rat muscle (Leighton & Cooper, 1988; Sowa et al., 1990; Molina et al., 1990). However, acute infusion of high-dose amylin in man did not affect glucose tolerance (Gilbey et al., 1989).
Slow transport of insulin from the vascular space to the plasma membranes of target cells may be important in certain insulin-resistant states. Insulin action upon heart muscle become abnormal if capillary endothelial insulin receptors are blocked (Bar & Sandra, 1988). In dogs, the concentration of insulin in thoracic duct lymph but not plasma correlates with insulin sensitivity during hyperinsulin- aemic clamps (Ader et al., 1990). Lillioja et al. (1987b) have demonstrated a direct relationship between muscle capillary density and degree of insulin resistance in obese NIDDM subjects.
Insulin action in other endocrine diseases
Adipose tissue from acromegalic patients exhibits subnormal insulin binding to receptors and insensitivity to insulin inhibition of lipolysis (Bolinder et al., 1986). In the fasting state, infusion of growth hormone decreased forearm glu- cose uptake as an effect of decreased glucose oxidation in favour of lipid oxidation rather than via interaction with insulin (Moller et al., 1990). During hyperinsulinaemia, a threefold increase in plasma growth hormone concentrations produced a shift to the right in the in-vivo insulin-dose response curve, suggesting a direct effect upon insulin action in muscle (Rizza et al., 1982a).
In Cushing’s syndrome, both liver and muscle display insensitivity to the regulation of glucose metabolism by

166 a. Taylor
Table 1. Insulin sensitivity in endocrine disease
Insulin sensitivity Reference
Addison's disease H ypopituitarism Hyperthyroidism Hypothyroidism Acromegaly Cushing's syndrome Phaeochromocytoma Hyperparathyroidism
Increased Increased Unchanged Unchanged Decreased Decreased Decreased Decreased
Kahn et al. (1 978) Goldfine et al. (1975) McCulloch er al. (1983) McCulloch et al. (1981) Bolinder et al. (1 986) Nosadini el al. ( 1983) Turnbull ei al. (1980) Prager et al. (1983)
insulin (Nosadini et al., 1983). This effect can be induced in normal subjects by 24-h infusion of hydrocortisone or oral administration of prednisone for 7 days (Rizza et al., 1982b; Pagano et al., 1983). The molecular mechanism of glucocor- ticoid effect upon insulin action is unknown.
Women with polycystic ovary syndrome have been noted to be resistant to insulin but uncertainty has surrounded the role of obesity and hyperandrogenism. In a well character- ized group of polycystic ovary syndrome patients defects in muscle and liver insulin sensitivity have been shown to be present in comparison with weight matched controls and this effect persists after correction for lean body mass (Dunaif et al., 1989). Hyperandrogenism plays no part in the genesis of the insulin insensitivity (Geffner er al., 1986).
Essential hypertension is not normally considered an endocrine disease, but it is associated with decreased insulin sensitivity for glucose disposal in muscle (Ferrannini et al., 1987). If the insulin insensitivity extended to all actions of insulin this finding would not be of pathogenic significance as any renal effects would be blunted. However, insulin sensiti- vity of ion transport, as reflected by fall in plasma potassium during insulin infusion, is normal in essential hypertension (Ferrannini et al., 1987). It has been hypothesized that the mild hyperinsulinaemia required to maintain glucose homeostasis under these circumstances could cause mild, chronic renal sodium retention and hence increased blood pressure in the long term (Reaven & Hoffman, 1987). Resistance to insulin-stimulation of glucose uptake, despite normal insulin receptor tyrosine kinase activity, is a feature of adipocytes from spontaneously hypertensive rats (Reaven et al., 1989).
Conclusions
Elucidation of the molecular structure of the insulin receptor has allowed rapid advances in the understanding of the immediate post-binding events in insulin action. Details of
primary regulation of some key target enzymes are now clear. The stage is set for establishment of links between these two research areas. The revealed network of insulin signal transmission is likely to be amenable to regulation at several points, and therapeutic possibilities for non-insulin-depen- dent diabetes may be predicted.
Acknowledgements
I am grateful to Dr S. J. Yeaman, Human Metabolism Research Centre, Newcastle upon Tyne for reading the manuscript and to Dr S. I. Taylor, National Institutes of Health, Bethesda for unpublished information on insulin receptor mutations.
References
Ader, M., Yang, J.Y. & Bergman, R.N. (1990) Efficiency of transepithelial transport is a determinant of insulin sensitivity in vivo. Diabetes, 39, 12A.
Alexander, M.C., Kowaloff, E.M., Witters, L.A., Dennihy. D.T. & Avruch, J. (1979) Purification of a hepatic 120.000-dalton hor- mone stimulated '*P peptide and its identification as ATP-citrate lyase. Yournal of Biological Chemistry, 254,8052-8056.
Alexander, M.C., Lomanto, M., Nasrin, N. & Ramaika, C. (1988) Insulin stimulates glyceraldehyde-3-phosphate dehydrogenase gene expression through cis-acting DNA sequences. Proceeding.? of the National Academy of Science, USA, 85,5092-5096.
Alvarez, J.F., Varela, I., Ruiz-Albusac, J.M. & Mato, J.M. (1988) Localization of the insulin-sensitive phosphatidylinositol glyca? at the outer surface of the cell membrane. Biochemical und Biophysical Research Communication, 152, 1455- 1462.
Arner, P., Pollare, T., Lithell, H. & Livingston, J.N. (1987) Defective insulin receptor tyrosine kinase in human skeletal muscle in obesity and Type 2 (non-insulin-dependent) diabetes mellitus. Diabetologia, 30,437-440.
Balage, M., Grizard, J., Sornet, C., Simon, J., Dardevet, D. & Manin, M. (1990) Insulin binding and receptor tyrosine kinase activity in rat liver and skeletal muscle: Effect of starvation. Metabolism, 39, 366-373.
Baquet, A., Huel, L., Meijer, A.J., Van Woerkom, G.M. & Plomp, P.J.A.M. (1990) Swelling of rat hepatocytes stimulates glycogen synthesis. Journal of Biological Chemistry, 265,855-959.
Bar, R.S. & Sandra, A. (1988) Insulin receptors in vascular endothelium. In Insulin receptors. Part A Me1hod.s .for Studv of Sfructure and Function (eds C. R. Kahn & L. C. Harrison), pp. 267-279. A.R. Liss, New York.
Boden, G., Ray, R.K., Smith, R.H. & Owen, O.E. (1983) Carbo- hydrate oxidation and storage in obese non-insulin-dependent diabetic patients. Diabetes, 32, 962-987.
Bogardus, C., Lillioja, S., Nyomba, B.L., Zurlo, F.. Swinburn, B.. Puente, A.E., Knowler, W.C., Ravussin, E.. Mott. D.M. & Bennett, P.H. (1989) Distribution of in vivo insulin action in Pima Indians as mixture of three normal distributions. Diaberes, 38,
Bogardus, C., Lillioja, S . , Stone, K. & Mott, D. (l984b) Correlation between muscle glycogen synthase activity and in vivo insulin action in man. Journal of Clinical Investigation. 73, 1185-1 190.
1423-1432.

Insulin action 1991 167
Bogardus, C., Ravussin, E., Robbins, D.C., W o k , R.R., Horton, E.S. & Sims, E.A.H. (1984a) Effects of physical training and diet therapy on carbohydrate metabolism in patients with glucose intolerance and non-insulin-dependent diabetes mellitus. Dia- betes, 33, 3 l l &-3 l 8.
Bolinder, J., Ostman, J., Werner, S. & Amer, P. (1986) Insulin action in human adipose tissue in acromegaly. Journal of Clinical Investigation. 77, 1201-1206.
Broughton, D.L., Alberti, K.G.M.M. & Taylor, R. (1987) Periph- eral tissue insulin sensitivity in healthy elderly subjects. Geronto-
Broughton, D.L., James, O.F.W., Alberti, K.G.M.M. & Taylor, R. (1991) Peripheral and hepatic insulin sensitivity in healthy elderly subjects. European Journal of Clinical Investigation (in press).
Browner, M.F., Nakano, K., Bang. A.G. & Fletterick, R.J. (1989) Human muscle glycogen synthase cDNA sequence: A negatively charged protein with an asymmetric charge distribution. Proceed- ings of the National Academy of Science, USA, 86, 143-1447.
Brownsey, R.W. & Denton, R.M. (1982) Evidence that insulin activates fat cell acetyl CoA carboxylase by increased phosphory- lation at a specific site. Biochemical Journal, 202, 77-86.
Cama, A,, Patterson. A.P.. Kadowaki, T., Kadowaki, H., Siegel, G., D’Ambrosio, D., Lillioja, S., Roth. J. & Taylor, S.I. (1990) The amino acid sequence of the insulin receptor is normal in an insulin- resistant Pima Indian. Journal of Clinical Endocrinology and Merabulism. 70, I 155- I 161.
Campbell, P.J. & Gerich, J.E. (1990) Impact of obesity on insulin action in volunteers with normal glucose tolerance: Demonstra- tion of a threshold for the adverse effect of obesity. Journal of Clinical Endocrinology and Metabolism, 70, I 114-1 I 18.
Caro, J.F., Sinha, M.K., Raju, S.M., Ittoop, O., Pories, W.J., Flickinger. E.G., Meelheim. D. & Dohm, G.L. (1987) Insulin receptor kinase in human skeletal muscle from obese subjects with and without noninsulin dependent diabetes. Journal of Clinical Inoesiigation. 79, 1330-1337.
Chan, B.L., Lisanti, M.R., Rodriguez-Boulan, E. & Saltiel, A.R. (1988) Lipoprotein lipase is anchored to the cell surface by glycosyl-phosphatidylinositol. Science, 241, 1670-1672.
Chen, M., Bergman, R.N., Pacini, G. & Porte, D. (1985) Pathogene- sis of age-related glucose intolerance in man: insulin resistance and decreased B-cell function. Journal of Clinical Endocrinology and Metabolism, 60, 13-20,
Chou. C.K.. Dull, T.J., Russell. D.S., Gherzi, R., Lebwohl. D. & Ullrich, A. (1987) Human insulin receptors at the ATP-binding site lack protein tyrosine kinase activity and fail to mediate postreceptor effects of insulin. Juurnul of Biological Chemistry. 362 , 1842-1847.
Cohen. P. & Cohen, P.T.W. (1989) Protein phosphatases come of age. Journal of Biological Chemisirj, 264, 21435-2 1438.
Cohen, P.. Parker, P.J. & Woodgett, J.R. (1985) The molecular mechanism by which insulin activates glycogen synthease in mammalian skeletal muscle. In Molecular Basis oflnsulin Acrion (ed. M. P. Czech). pp. 213-233. Plenum Press, New York.
Cooper, G.J.S., Willis. A.C.. Clark. A.. Turner, R.C., Sim, R.B. & Reid. K.B.M. (1987) Purification and characterization of a peptide from amyloid-rich pancreases of type 2 diabetic patients. Proceedings of ihc Naricml Academy of Science. USA, 84, 8628- 8632.
Coore. H.G., Denton. R.M., Martin, B.R. & Randel, P.J. (1971) Regulation of adipose tissue pyruvate dehydrogenase by insulin and other hormones. Biochemistry, 125, I 15-127.
l0g.V. 33, 357-362.
Crettaz, M., Horton, E.S., Warzala, L.J., Horton, E.D. & Jeanre- naud, B. (1983) Physical trainingofZucker rats: lack ofalleviation of muscle insulin resistance. American Journal ofPhysiology, 244, E414420.
Cushman, S.W. & Wardzala, L.J. (1980) Potential mechanisms of insulin action on glucose transport in the isolated rat adipose cell: apparent translocation of intracellular transport systems to the plasma membrane. Journal of Biological Chemistry, 255, 4758- 4762.
Czech, M.P., Klarlund, J.K., Yagaloff, K.A., Bradford, A.P. & Lewis, R.E. (1988) Insulin receptor signaling: activation of multiple serine kinases. Journal of Biological Chemistry, 263, 11017-1 1020.
Debant, A,, Clauser, E., Ponzio, G., Filloux, C., Auzan, C., Contreres, J-0. & Rossi, B. (1988) Replacement of insulin receptor tyrosine residues 1162 and 1163 does not alter the mitogenic effect of the hormone. Proceedings of the National Academy of Science, USA, 85,8032-8036.
Dent, P., Campbell, D.G., Hubbard, M.J. & Cohen, P. (1989) Multisite phosphorylation of the glycogen-binding subunit of protein phosphatase-lG by cyclic AMP-dependent protein kinase and glycogen synthase kinase-3. Federation of European Biochemi- cal Socieries, 248, 67-72.
Dunaif, A,, Segal, K.R., Futterweit, W. & Dobrjansky, A. (1989) Profound peripheral insulin resistance, independent of obesity, in polycystic ovary syndrome. Diabetes, 38, 1 165- 1 174.
Ebina, Y., Araki, E., Taira, M., Shimada, F., Mori, M., Craik, C.S., Siddle, K., Pierce, S.B., Roth, R.A. & Rutter, W.J. (1987) Replacement of lysine residue 1030 in the putative ATP-binding region of the insulin receptor abolishes insulin- and antibody- stimulated glucose uptake and receptor kinase activity. Proceed- ings of the National Academy of Science, USA, 84, 704-708.
Ebina, Y., Ellis, L., Jarnagin, K., Edery, M., Graf, L., Clauser, E., Ou, J.H., Maslarz, F., Kan, Y.W., Goldfine, I.D., Roth, R.A. & Rutler, W.J. (1985) The human insulin receptor cDNA: the structural basis for hormone-activated transmembrane signalling. Cell, 40,747-758.
Ellis, L., Clauser, E., Morgan, D.O., Edery, M., Roth, R.A. & Rutter, W.J. (1986) Replacement of insulin receptor tyrosine residues I 162 and I163 compromises insulin-stimulated kinase activity and uptake of 2-deoxyglucose. Cell, 45, 721-732.
Ellis, L., Morgan, D.O., Clauser, E., Roth. R.A. & Rutter, W.J. (1 987) A membrane-anchored cytoplasmic domain of the human insulin receptor mediates a constitutively elevated insulin-inde- pendent uptake of 2-deoxyglucose. Molecular Endocrinology, 1,
Eriksson, J., Franssila-Kallunki, A., Ekstrand, A,, Saloranta, C., Widen, E., Schalin, C. & Groop, L. (1989) Early metabolic defects in persons at increased risk for non-insulin dependent diabetes mellitus. New England Journal of Medicine, 321, 337-343.
Evans, J., Hoffmann, R.G., Kalkoff, R.K. & Kissebah, A.H. (1984) Relationship of body fat topography to insulin sensitivity and metabolic profiles in premenopausal women. Metabolism, 33,68- 75.
Ferrannini, E., Buzzigoli, G., Bonadonna, R., Giorico, M.A., Oleggini, M., Graziadei, L., Pedrinelli, R., Brandi, L. & Bevilac- qua, S. (1987) Insulin resistance in essential hypertension. New England Journal of Medicine, 317, 350-357.
Fehlmann, M. & Freychet, P. (1981) Insulin and glucagon stimula- tion of (Na+-K+)-ATPase transport activity in isolated rat hepatocytes. Journal of Biological Chemistry, 256, 7449- 7453.
15-24,
168 R. Taylor
Fink, R.I., Wallace, P. & Olefsky, J.M. (1986) Effects on aging on glucose-mediated glucose disposal and glucose transport. Journal of Clinical Investigation, 77, 2034-2040.
Forsayeth, J.R., Caro, J.F., Sinha, M.K., Maddux, B.A. & Goldfine, I.D. (1987) Monoclonal antibodies to the human insulin receptor that activate glucose transport but not insulin receptor kinase activity. Proceedings of the National Academy of Science, USA, 84,
Forsayeth, J., Maddux, B. & Goldfine, I.D. (1986) Biosynthesis and processing of the human insulin receptor. Diabetes, 35,837-846.
Fujioka, S . , Matsuzawa, Y., Tokunaga, K. & Tarui, S. (1987) Contribution of intra-abdominal fat accumulation to the impair- ment of glucose and lipid metabolism in human obesity. Metab- olism, 36, 54-59.
Geffner, M.E., Kaplan, S.A., Bersch, N., Golde, D.W., Landow, E.M. & Chang, R.J. (1986) Persistence of insulin resistance in polycystic ovarian disease after inhibition of ovarian steroid secretion. Fertility and Sterility, 43, 327-333.
Gilbey, S.G., Bretherton-Watt, D., Beacham, J., Ghatei, M.A. & Bloom, S.R. (1989) High dose amylin in man: unexpected failure to affect intravenous glucose tolerance. Diaberic Medicine, 6(Suppl. 2) 5A.
Goldfine, I.D. (1975) Binding of insulin to thymocytes from suckling and hypophysectomised rats: Evidence for 2 mechanisms regulat- ing insulin sensitivity. Endocrinoiogy, 97,948-954.
Goldfine, I.D. (l987b) The insulin receptor: Molecular biology and transmembrane signaling. Endocrine Reviews, 8,235-243.
Goldstein, J.L., Brown, M.S., Anderson, R.C., Russel, D.W. & Schneider, W.J. (1985) Receptor-mediated endocytosis: concepts emerging from the LDL receptor system. In Annual Review of Cell Biology (ed. G . E. Palade), pp. 1-40. Annual Reviews Inc. Palo Alto, CA.
Hanks, S.K.. Quinn, A.M. & Hunter, T. (1988) The protein kinase family: conserved features and deduced phylogeny of the catalytic domains. Science, 241, 42-52.
Haring, H.U., White, M.F., Kahn, C.R., Ahmad, S., Depaoli- Roach, A.A. & Roach, P.J. (1985) Interaction of the insulin receptor kinase with serine/threonine kinase in uirro. Journal of Cell Biochemistry, 28, 17 1 - 182.
Hauguel, S., Gilbert, M. & Girard, J. (1987) Pregnancy-induced insulin resistance in liver and skeletal muscles of the conscious rabbit. American Journal of Physiology, 252, EI65-EI69.
Hawley, D.M., Maddux, B.A., Patel, R.G., Wong, K-Y., Mamula, P.W., Firestone, G.L., Burnetti, A., Verspohl, E. &Goldfine, 1.D. (1989) Insulin receptor monoclonal antibodies that mimic insulin action without activating tyrosine kinase. Journal of Biological Chemistry, 264,2438-2444.
Hedo, J.A., Collier, E. & Watkinson, A. (1987) Myristyl and palmityl acylation of the insulin receptor. Journal of Biological Chemistry, 262,954-957.
Herzberg, V.L., Grigorescu, F., Edge, AS., Spiro, R.G. & Kahn, C.R. ( 1985) Characterization of insulin receptor carbohydrate by comparison of chemical and enzymatic deglycosylation. Bio- chemical and Biophysiology Research Communication, 129, 789- 796.
Hjollund, E., Beck-Nielsen, H., Pedersen, O., Richelsen, B. & Sorensen, J.S. (1985) Defective non-insulin mediated and insulin mediated glucose transport and metabolism in adipocytes from obese and lean patients with untreated type 2 diabetes mellitus. Diabetic Medicine, 2,468-473.
Horton, E.S. (1986) Exercise and physical training: effects on insulin
3448-345 1.
sensitivity and glucose metabolism. Diabetes/Metabolism Reviews, 2, I - 18.
Houslay, M.D., Pyne, J.F., OBrien, R.M., Siddle, K. & Strazs- sheim, D. (1989) Guanine nucleotide regulatory proteins in insulin’s action and in diabetes. Biochemical Society Transactions,
Ishizuka, T., Cooper, D.R., Hernandez, H., Buckley, D., Standaert, M. & Farese, R.V. (1990) Effects of insulin on diacylglycerol- protein kinase C signalling in rat diaphragm and soleus muscles and relationship to glucose transport. Diabetes, 39, 181-190.
James, D.E., Hiken, F. & Lawrence, J.C. (1990) Isoproterenol stimulates phosphorylation of the insulin-regulatable glucose transporter in rat adipocytes. Proceedings of the National Aca- demy of Science, USA (in press).
James, D.E., Strube, M. & Mueckler, M. (1989) Molecular cloning and characterization of an insulin-regulatable glucose trans- porter. Nature, 33, 83-87.
Jeno, P., Ballou, L.M., Novak-Hofer, I. & Thomas, G. (1988) Identification and characterization of a mitogen-activated S6 kinase. Proceedings of the National Academy of Science, USA, 85, 406410.
Johnson, A.B., Argyraki, M., Thow, J.C., Jones, I.R., Broughton, D., Miller, M. &Taylor, R. (1991) Impaired activation of skeletal muscle glycogen synthase in NIDDM is unrelated to the degree of obesity. Metabolism (in press).
Joost, H.G., Weber, T.M., Cushman, S.W. & Simpson, I.A. (1986) Insulin-stimulated glucose transport in rat adipose cells: modula- tion of transporter intrinsic activity by isoproterenol and adeno- sine. Journal of Biological Chemistry, 261, 10033-10036.
Kadowaki, T. (1984) Risk factors for worsening to diabetes in subjects with impaired glucose tolerance. Diabetologia, 26,4449.
Kadowaki, T. , Koyasu, S., Nishida, E., Sakai, H., Takaku. F., Yahara, I. & Kasuga, M. (1986) Insulin-like growth factors, insulin and epidermal growth factor cause rapid cytoskeletal reorganization in KB cells. Journal of Biological Chemistry. 261,
Kahn, C.R., Goldfine, I.D., Neville, D.M. & Demeyts, P. (1978) Alterations in insulin binding induced by changes in oitw in the levels of glucocorticoids and growth hormone. Endocrinology,
Kasuga, M., Zick, Y., Blithe, D.L., Karlsson, F.A., Haring, H.U. & Kahn, C.R. (1982) Insulin stimulation of phosphorylation of the beta subunit of the insulin receptor. Journal of Biological Chemistry, 257,9891-9894.
Kelly, K.L., Mato, J.M. & Jarett, L. (1986) The polar head group of a novel insulin-sensitive glycophospholipid mimics insulin action on phospholipid methyltransferase. FEBS Letters. 209,238-242.
Kelly, K.L., Merida, I., Wong, E.H.A., Dicenzo, D. & Mato. J.M. (1987) A phospho-oligosaccharide mimics the effect of insulin to inhibit isoproterenol-dependent phophorylation of phospholipid methyltransferase in isolated adipocytes. Journal of Biological Chemistry, 262, 15285-15290.
Kennelly, P.J. & Rodwell, V.W. (1985) Regulation of 3-hydroxy-3- methylglutaryl coenzyme A reductase by reversible phos- phorylation-dephosphorylation. Journal of Lipid Research, 26,
Klarlund, J.K., Bradford, A.P., Milla, M.G. & Czech, M.P. (1990) Purification of a novel insulin-stimulated protein kinase from rat liver. Journal of Biological Chemistry, 265,227-234.
Lane, M.D., Flores-Riveros, J.R., Hresko, R.C., Kaestner, K.H., Liao, K., Janicot, M., Hoffman, R.D., McLenithan, J.C., Kaeste-
17,627-629.
I614 I - 16147.
103, 1054-1063.
903-914.

lnsutin action 7997 169
lic, T. & Christy, R.J. (1990) Insulin receptor tyrosine kinase and glucose transport. Diabeies Care, 13, 565-575.
Larner. J . (1971) Insulin and glycogen synthase. Diaheies, 21,428- 438.
Leighton. B. & Cooper, G.J.S. (1988) Pancreatic amylin and calcitonin gene-related peptide cause resistance to insulin in skeletal muscle in rtiro. Nature, 335, 632-635.
Lillioja, S., Mott. D.M.. Zawadzki, J.K. ei al. (1987a) In vivo insulin action is familial characteristic in nondiabetic Pima Indians. Diabetes. 36, I329 - 1335.
Lillioja. S., Mott, D.M.. Howard, B.V., Bennett, P.H., Yki- Jarvinen. H., Freymond, D., Nyomba, B.L.. Zurlo, F., Swinburn, B. & Bogardus, C. (1988) Impaired glucose tolerance as a disorder of insulin action. New England Journal of Medicine, 318, 1217- 1225.
Lillioja, S., Young, A.A.. Culter. C.L., Ivy. J.L., Abbott, G.H.. Zadowaki. J.E., Yki-Jarvinen, H., Christin, L., Secomb, T.W. & Bogardus. C. (1987b) Skeletal muscle capillary density and fiber type area: Possible determinants of in vivo insulin resistance in man. Journal of Clinical Invesiigaiion, 80,4 15424.
McClain, D.A. (1990) Insulin action in cells expressing truncated of kinase-defective insulin receptors: Dissection ofmultiple hormone signalling pathways. Diabetes Care, 13, 302-316.
McCulloch, A.J., Home, P.D., Heine, R., Ponchner, M., Hanning, 1.. Johnston, D.G., Clark, F. &Alberti, K.G.M.M. (1983) Insulin sensitivity in hyperthyroidism: Measurement by the glucoseclamp technique. Clinical Endocrinology, 18, 327-333.
McCulloch, A.J., Johnston, D.G.. Burrin, J.M., Hodson, A.W., Clark, F., Waugh, C., Orskov, H., Alberti. K.G.M.M. (1981) Diurnal hormone-metabolic profiles in hypothyroidism. Clinical Endocrinology, 15, 607-61 9.
Maegawa, H., Olefsky, J.M., Thies. S., Boyd. D., Ullrich, A. & McClain. D.A. (1988) Insulin receptors with defective tyrosine kinase inhibit normal receptor function at the level of substrate phosphorylation. Journal of Biological Chemisiry, 263, 12629- 12637.
Magnuson. M.A., Andreone, T., Printz, R.L., Koch, S. & Granner, D.K. (1989) Rat glucokinase gene: structure and regulation by insulin. Proceedings of the Naiionul Academy of Science, USA, 86,
Marshall, S., Heidenreich, K.A. & Horikoshi, H. (1985) Stoichio- metric translocation of adipocyte insulin receptor from the cell- surface to the cell-interior. Journal of Biological Chemistry, 260, 4 128-4 135.
Molina. J.M., Cooper, G.J.S., Leighton, B. &Olefsky, J.M. (1990) Induction of insulin resistance in aiuo by amylin and CGRP. Diabeies. 39, 260-265.
Moller, N., Jorgensen, J.O., Alberti, K.G.M.M.. Glyvbjerg, A. & Schmitz, 0. (1990) Short-term effects of growth hormone on fuel oxidation and regional substrate metabolism in normal man. Journal of Clinical Endocrinology and Meiabolism, 70, 1 179-1 186.
Morgan, D.O. & Roth, R.A. (1987) Acute insulin action requires insulin receptor kinase activity: introduction of an inhibitory monoclonal antibody into mammalian cells blocks the rapid effects of insulin. Proceedings of ihe National Academy of Science,
Mott. D.M.. Lillioja, S. & Bogardus, C. (1986) Overnutrition induced decrease in insulin action for glucose storage: in viuo and in oiiro in man. Metabolism. 35, 160-165.
Newman, W.P. & Brodows, R.G. (1983) Insulin action during acute
4838-4842.
USA, 84,41-45.
starvation: evidence for selective insulin resistance in normal man. Metabolism, 32, 590-596.
Nishida, E., Hoshi, M., Miyata, Y., Sakai, H., Kadowaki, T., Kasuga, M., Saijo, S.. Ogawara, H. & Akiyama, T. (1987) Tyrosine phosphorylation by the epidermal growth factor recep- tor kinase induces functional alterations in microtubule-asso- ciated protein 2. Journal qf Biological Chemisiry, 262, 16200- 16204.
Nosadini, R., Del Prato, S., Tiengo, A,, Valerio. A,, Muggeo, M., Opocher, G., Mantero, F.. Duner, E., Marescotti, C., Mjollo. F. & Belloni, F. (1983) Insulin resistance in Cushing's syndrome. Journal of Clinical Endoerinotogy and Metabolism, 51,529-536.
OBrien, R.M. & Granner, D.K. (1990) PEPCK gene as model of inhibitory effects of insulin on gene transcription. Diabeies Cure,
OBrien. R.M., Siddle, K.. Houslay, M.D. & Hall, A. (1987) Interaction of the human insulin receptor with the ras oncogene product p21. FEBS Letters, 217, 253-259.
Odawara, M., Kadowaki, T.. Yamamoto, R.. Shibasaki. Y., Tobe, K., Accili, D., Bevins. C., Mikami, Y., Matsuura, N., Akanuma. Y.. Takaku, F., Taylor, S.I. & Kasuga, M. (1989) Human diabetes associated with a mutation in the tyrosine kinase domain of the insulin receptor. Science. 245, 66-68.
Okabayashi, Y., Maddux, B.A., McDonald, A.R., Logsdon, C.D.. Williams, J.A. & Goldfine, I.D. (1989) Mechanisms of insulin- induced insulin-receptor downregulation: decrease of receptor biosynthesis and mRNA levels. Diabeies. 38, 182-187.
Osborn, L., Rosenberg, M.P., Keller. S.A. & Meisler, M.H. (1987) Tissue-specific and insulin-dependent expression of a pancreatic amylase gene in transgenic mice. Molecular Cell Biology, 7,326- 334.
Owerbach, D., Bell, G.I., Rutler, W.J. & Shaes, T.B. (1980) The insulin gene is located on chromosome I I in humans. Naiure, 286, 82.
Pagano, G.. Cavallo-Perin. P., Cassader, M.. Bruno, A,, Ozzello, A,. Masciola, P., Dall'Omo, A.M. & Imbimbo, B. (1983) An in vivo and in vitro study of the mechanism of prednisone-induced resistance in healthy subjects. Journal of Clinical Invesiigaiion, 12,
Pang, D.T. & Shafer, J.A. (1984) Evidence that insulin receptor from human placenta has a high affinity for only one molecule of insulin. Journal of Biological Chemistry, 259,8589-8596.
Peavy, D.E., Taylor, J.M. & Jefferson, L.S. (1978) Correlation of albumin production rates and albumin mRNA levels in livers of normal, diabetic, and insulin-treated diabetic rats. Proceedings qf the Naiional Academy of Science, USA, 75, 5879-5883.
Pedersen, 0.. Hjollund, E. & Linkskov, H.O. (1982) Insulin binding and action on fat cells from young healthy females and males. American Journal of Physiology, 243, E I 58- E 167.
Pelosin, J-M., Vilagrain, I. & Chambaz, E.M. (1987) A single form of protein kinase C is expressed in bovine adrenocortical tissue, as compared to four chromatographically resolved isozymes in rat brain. Biochemical and Biophysical Research Communication, 147,
Petersen, D.D., Magnuson, M.A. & Granner, D.K. (1988) Location and characterization of two widely separated glucocorticoid response elements in the phosphoenolpyruvate carboxykinase. Molecular Cell Biology. 8,96-104.
Pilch, P.F., Thompson, P.A. & Czech, M.P. (1980) Coordinate modulation of D-glUCOSe transport activity and bilayer fluidity in
13,327-339.
I8 14- 1820.
382-391.
170 R. Taylor
plasma membranes from control and insulin treated cells. Pro- ceedings of the National Academy of Science, USA, 77,915-918.
Prager, R., Kovarik, J., Schernthaner, G., Woloszcuk, W. & Willvonseder, R. (1983) Peripheral insulin resistance in primary hyperparathyroidism. Metabolism, 32, 800-805.
Reaven, G.M. & Hoffman, B.B. (1987) A role for insulin in the aetiology of hypertension. Lancet, ii, 435-436.
Reaven, G.M., Chang, H., Hoffman, B.B. & Azhar, S. (1989) Resistance to insulin-stimulated glucose uptake in adipocytes isolated from spontaneously hypertensive rats. Diabetes, 38,
Rizza, R.A., Mandarino, L.J. & Gerich, J.E. (1982a) Effects of growth hormone on insulin action in man: mechanisms of insulin resistance, impaired suppression of glucose production, and impaired stimulation of glucose utilization. Diabetes, 31,663-669.
Rizza, R.A., Mandarino, L.J. & Gerich, J.E. (1982b) Cortisol- induced insulin resistance in man: impaired suppression of glucose production and stimulation of glucose utilization due to a postreceptor defect of insulin action. Journal of Clinical Endocri- nology and Metabolism, 54, 131-137.
Rosen, O.M., Herrera, R., Olowe, Y., Petruzzelli, L.M. & Cobb, M.H. (1983) Phosphorylation activates the insulin receptor tyrosine protein kinase. Proceedings of the National Academy of Science, USA, 80,3237-3240.
Sacks, D.B. & McDonald, J.M. (1988) Insulin-stimulated phos- phorylation of calmodulin by rat liver insulin receptor prep- aration. Journal of Biological Chemistry, 263,2377-2383.
Sacks, D.B. & McDonald, J.M. (1989) Calcium and insulin action. In Molecular and Cellular Biology of Diabetes Mellitus. Volume 2. Insulin Action (eds. B. Draznin, S. Melmed & D. LeRoith), pp. 193-202. A.R. Liss, New York.
Saltiel, A.R. (1987) Insulin generates an enzyme modulator from hepatic plasma membranes: regulation of CAMP phosphodiester- ase, pyruvate dehydrogenase and adenylate cyclase. Endocrino-
Saltiel, A.R. (1990) Second messengers of insulin action. Diabetes Cure, 13, 244-256.
Saltiel, A.R., Fox, J.A., Sherline, P. & Cuatrecasas, P. (1986) Insulin stimulates the release from liver plasma membranes of a chemical modulator of pyruvate dehydrogenase. Science, 233,867-972.
Saltiel, A.R., Osterman, D.G. & Darnell, J.C. (1988) Role of glycosyl phosphoinositides in insulin action. Cold Spring Harbor Symposium on Quantitative Biology, 53, 955-963.
Sasaki, K., Cripe, T.P., Koch, S.R., Andreone, T.L., Petersen, D.D., Beale, E.G. & Granner, D.K. (1984) Multihormonal regulation of phosphoenolpyruvate carboxykinase gene transcription. Journal of Biological Chemistry, 259, 15242- 1525 1.
Sasaki, K. & Granner, D.K. (1988) Regulation of phosphoenolpyru- vate carboxykinase gene transcription by insulin and CAMP: reciprocal actions on initiation and elongation. Proceedings of the National Academy of Science. USA, 85, 2954-2958.
Seino, S. & Bell, G.1. (1989) Alternative splicing of human insulin receptor messenger RNA. Biochemical and Biophysical Research Communicurion, 159, 312-316.
Seino. S., Seino, M., Nishi, S. & Bell, G.1. ( 1 989) Structure of the human insulin receptor gene and characterization of its promoter. Proceedings of rhe National Academy of Science, USA, 86, 114- 118.
Shaw, D.J., Meredith, A.C., Brook, J.D., Sarfaranzi, M., Harley, H.G., Husson, S.M., Bell, G.I. & Harper, P.S. (1986) Linkage relationship of the insulin receptor gene with the complement
1155-1160.
logy, 120,967-972.
component 3, LDL receptor, apolipoprotein C2 and myotonic dystrophy loci on chromosome 19. Human Genetics, 74,267-269.
Shimada, F., Taira, M., Suzuki, Y., Hashimoto, J., Nozaki, O., Taira, M., Tatibana, M., Ebina, Y., Tawata, M.. Onaya, T., Makino, H. & Yoshida, S. (1990) Insulin-resistant diabetes associated with partial deletion of insulin-receptor gene. Lancet, 335,1179-1181.
Smith, D.M. &Sale, G.J. (1988) Evidence that a novel serine kinase catalyses phosphorylation of the insulin receptor in an insulin- dependent and tyrosine kinase-dependent manner. Biochemical Journal, 256,903-909.
Soos, M.A.,OBrien, R.M.,Brindle,N.P.J.,Stigter, J.M.,Okamoto, A.K., Whittaker, J. & Siddle, K. (1989) Monoclonal antibodies to the insulin receptor mimic metabolic effects of insulin but do not stimulate receptor autophosphorylation in transfected NIH 3T3 fibroblasts. Proceedings of the National Academy of Science, USA,
Sowa, R., Sanke, T., Hirayama, J., Tabata, H., Furuta, H., Nishimura, S. & Nanjo, K. (1990) Islet amyloid polypeptide amide causes peripheral insulin resistance in uivo in dogs. Diabetologia, 33, 118-120.
Spach, D.H., Nemenoff, R.A. & Blackshear, P.J. (1986) Protein phosphorylation and protein kinase activities in BCM-I myo- cytes. Journal of Biological Chemistry, 261, 12750- 12753.
Staus, S.D., Pan, K.J., Kull Jr F.C., Jacobs, S. & Mohandas, T. (1985) Human insulin receptor gene. Diaberes, 34,816-820.
Sternlicht, E., Barnard, R.J. & Grimditch, G.K. (1988) Mechanism of insulin action on glucose transport in rat skeletal muscle. American Journal of Physiology, 254, E633-638.
Stralfors, P. (1988) Insulin stimulation of glucose uptake can be mediated by diacylglycerol in adipocytes. Nature. 335, 554-556.
Stuart, C.A., Shangraw, R.E., Prince, M.J., Peters, E.J. & Wolfe, R.R. (1988) Bed-rest induced insulin resistance occurs primarily in muscle. Metabolism, 37, 802-806.
Sturgill, T.W., Ray, L.B., Erikson, E. & Maller, J.L. (1988) Insulin- stimulated MAP-2 kinase phosphorylates and activates ribosomal protein S6 kinase 11. Nature, 334, 715-718.
Suzuki, K. & Kono, T. (1980) Evidence that insulin causes translocation of glucose transport activity to the plasma mem- brane from an intracellular storage site. Proceedings of the National Academy of Science, USA, 77, 2542-2545.
Takayama, S., White, M.F., Luris, V. & Kahn, C.R. (1 980) Phorbol esters modulate insulin receptor phosphorylation and insulin action in cultured hepatoma cells. Proceedings of the National Academy of Science, USA, 81, 7797-7801.
Taira, M., Taira, M., Hashimoto N., Shimada, F., Suzuki. Y., Kanatsuka, A., Nakamura, F., Ebina, Y., Tatibana, M., Makino, H. & Yoshida, S. (1989) Human diabetes associated with a deletion of the tyrosine kinase domain of the insulin receptor. Science, 245, 63-66.
Taylor, D., Uhing, R.J., Blackmore, P.F., Prpic, V. & Exton, J.H. (1985) Insulin and epidermal growth factor do not affect phos- phoinositide metabolism in rat liver plasma membranes and hepatocytes. Journal of Biological Chemistry, 260,201 1-2014.
Taylor, R. (1989) Aetiology of non-insulin dependent diabetes. British Medical Bulletin, 45, 73-91.
Taylor, R. & Agius, L. (1988) The biochemistry of diabetes. Biochemical Journal, 250,625-640.
Taylor, S.I., Kadowaki, T., Kadowaki, H., Accili. D., Cama, A. & McKeon, C. (1990) Mutations in insulin-receptor gene in insulin- resistant patients. Diabetes Care, 13, 257-279.
86,5217-5221.

Insulin action 1991 171
Tornqvist, H.E. & Avruch, J. (1988) Relationship ofsitespecificbeta subunit tyrosine autophosphorylation to insulin activation of the insulin receptor (tyrosine) kindse activity. Journal of Biological Chemistry, 263,4593-460 1.
Turnbull. D.M.. Johnston, D.G., Alberti, K.G.M.M. & Hall, R. (1980) Hormonal and metabolic studies in a patient with pheo- chromocytoma. Journal of Clinical Endocrinology and Metab- ofism, 51,930-933.
Ullrich. A,, Bell. J.R., Chen, E.Y., Herrera. R., Petruzzelli, L.M., Dull, T.J., Gray, A,, Coussens, L., Liao, Y-C., Tusbokawa, M., Mason, A,, Seeburg, P.H., Grunfeld, C.. Rosen, O.M. & Rama- chandran, J. (1985) Human insulin receptor and its relationship to the tyrosine kinase family of oncogenes. Nature, 313,756.
van de Werve, G.. Proielto, J. & Jenrenaud, B. (1985) Tumor- promoting phorbol esters increase basal and inhibit stimulated lipogenesis in rat adipocytes without decreasing insulin binding. Biochemical Journal, 225, 523-527.
White, M., Stegmann, E.W., Dull, T.J., Ullrich, A. & Kahn, C.R. (1987) Characterization of an endogenous substrate of the insulin receptor in cultured cells. Journal of Biological Chemistry, 262,
White, M.F.. Livingston, J.N., Backer, J.M., Lauris, V., Dull, T.J., Ullrich, A. & Kahn, C.R. (1988) Mutation of the insulin receptor at tyrosine 960 inhibits signal transmission but does not affect its tyrosine kinase activity. Cell. 54,641-649.
White, M.F., Maron, R. & Kahn, C.R. (1985) Insulin rapidly
9769-9777.
stimulates tyrosine phosphorylation of M,-185,000 protein in intact cells. Nurure, 318, 183-186.
Wright, K.S., Beck-Nielsen, H., Kolterman, O.G. & Mandarino, L.J. (1988) Decreased activation of skeletal muscle glycogen synthase by mixed-meal ingestion in NIDDM. Diaberes, 37,436- 440.
Yang-Feng, T.L., Francke, U. & Ullrich, A. (1985) Gene for human insulin receptor: localization to site on chromosome 19 involved in pre-B-cell leukemia. Science, 228, 728-731.
Yang, S.D., Ho, L.T., Fung, T.J. & Yu, J.S. (1989) Insulin induces activation of kinase FA in membranes and thereby promotes activation of ATP. Mg-dependent phosphatase on adipocytes. Biochemical and Biophysical Reseurch Communication, 158, 762- 768.
Yki-Jarvinen, H. & Koivisto, V.A. (1983) Effects of body composi- tion on insulin sensitivity. Diubetes, 32, 965-969.
Yki-Jarvinen, H., Young, A.A., Lamkin, C. & Foley, J.E. (1987) Kinetics of glucose disposal in whole body and across the forearm in man. Journal of Clinical Inoesrigation, 79, I7 13- I7 19.
Yu, K.T., Khalaf, N. & Czech, M.P. (1987) Insulin stimulates a membrane-bound serine kinase that may be phosphorylated on tyrosine. Proceedings of the National Academy of Science. USA, 84,3972-3976.
Zick, Y., Whittaker, J. & Roth, J. (1983) Insulin stimulated phosphorylation of its own receptor. Journal of Biolugicul Chemistry, 258, 343 1-3437.





























