Embed Size (px)
Citation preview

Tissue Engineering and Regenerative Medicine
Insulin-Producing Endocrine Cells Differentiated InVitro From Human Embryonic Stem Cells Function inMacroencapsulation Devices In Vivo
ALAN D. AGULNICK, DANA M. AMBRUZS, MARK A. MOORMAN, ANINDITA BHOUMIK,
ROSEMARY M. CESARIO, JANICE K. PAYNE, JONATHAN R. KELLY, CARL HAAKMEESTER, ROBERT SRIJEMAC,
ALISTAIR Z. WILSON, JUSTIN KERR, MAURO A. FRAZIER, EVERT J. KROON, KEVIN A. D’AMOUR
Key Words. Embryonic stem cells x Insulin-secreting cells x Diabetes x Drug delivery systems xCell therapy x Pancreas development
ABSTRACT
The PEC-01 cell population, differentiated from human embryonic stem cells (hESCs), contains pan-creatic progenitors (PPs) that, when loaded into macroencapsulation devices (to produce the VC-01candidate product) and transplanted intomice, canmature into glucose-responsive insulin-secretingcells and other pancreatic endocrine cells involved in glucose metabolism.Wemodified the protocolfor making PEC-01 cells such that 73%–80% of the cell population consisted of PDX1-positive (PDX1+)and NKX6.1+ PPs. The PPs were further differentiated to islet-like cells (ICs) that reproducibly con-tained 73%–89%endocrine cells, ofwhich approximately 40%–50%expressed insulin. A large fractionof these insulin-positive cells were single hormone-positive and expressed the transcription factorsPDX1 and NKX6.1. To preclude a significant contribution of progenitors to the in vivo function of ICs,we used a simple enrichment process to remove remaining PPs, yielding aggregates that contained93%–98% endocrine cells and 1%–3% progenitors. Enriched ICs, when encapsulated and implantedinto mice, functioned similarly to the VC-01 candidate product, demonstrating conclusively that invitro-produced hESC-derived insulin-producing cells can mature and function in vivo in devices. Ascaled version of our suspension culture was used, and the endocrine aggregates could be cryopre-served and retain functionality. Although ICs expressedmultiple importantb cell genes, the cells con-tained relatively low levels of several maturity-associatedmarkers. Correlating with this, the time tofunction of ICs was similar to PEC-01 cells, indicating that ICs required cell-autonomous maturationafter delivery in vivo, which would occur concurrently with graft integration into the host. STEMCELLS TRANSLATIONAL MEDICINE 2015;4:1–9
SIGNIFICANCE
Type1diabetes (T1D) affects approximately 1.25millionpeople in theU.S. alone and is deadly if notman-aged with insulin injections. This paper describes the production of insulin-producing cells in vitro anda newprotocol for producing the cells, representing another potential cell source for a diabetes cell ther-apy. These cells can be loaded into a protective device that is implanted under the skin. The device isdesigned to protect the cells from immune rejection by the implant recipient. The implant can engraftand respond to glucoseby secreting insulin, thuspotentially replacing theb cells lost in patientswith T1D.
INTRODUCTION
In type I diabetes, autoimmunity results in theloss of insulin-producing b cells in the pancreas,
leading to a loss of blood glucose control. The
standard treatment of insulin injection is life-
saving; however, daily glucose fluctuations re-
main higher than in healthy persons. This leaves
patients vulnerable to complications including
vascular and kidney disease, blindness, and lower
limb amputation. Transplantation of cadaveric
islets has made great progress in recent years
and can result in insulin independence or lower
insulin requirements [1]. This approach, however,
is greatly limited by donor availability and the
need for chronic immunosuppression.Human embryonic stem cells (hESCs) pos-
sess the key features of essentially unlimited
expansion and the theoretical ability to differen-
tiate to any cell type, thus there has been consid-
erable effort toward developing protocols to
produce b-like cells from hESCs for transplanta-
tion and drugdevelopment. Significant advances
have been made over the past 10 years in
ViaCyte, Inc., San Diego,California, USA
Correspondence: Alan D.Agulnick, Ph.D., ViaCyte, Inc.3550 General Atomics Court, SanDiego, California 92121, USA.Telephone: 858-455-3636;E-Mail: [email protected]
ReceivedApril 23, 2015; acceptedfor publication June 24, 2015.
©AlphaMed Press1066-5099/2015/$20.00/0
http://dx.doi.org/10.5966/sctm.2015-0079
STEM CELLS TRANSLATIONAL MEDICINE 2015;4:1–9 www.StemCellsTM.com ©AlphaMed Press 2015
TISSUE ENGINEERING AND REGENERATIVE MEDICINE
by KE
VIN
DA
MO
UR
on September 1, 2015
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
Published Ahead of Print on August 24, 2015 as 10.5966/sctm.2015-0079.

recapitulating pancreatic development in vitro with hESCs, us-ing the extensive knowledge gained from studies of pancreaticorganogenesis in model organisms [2]. We have previouslyshown that pancreatic endoderm cells (PECs) differentiatedfrom hESCs via a four-stage protocol can, when transplanted in-to immunodeficient mice, form functional b cells and reversestreptozotocin-induced diabetes [3, 4]; this result has beenreproduced by others [5]. We also demonstrated a scaledmanufacturing system capable of producing the required quan-tity and quality of PEC-01 cells (PECs derived from CyT49 hESCs)to enable clinical application [6].
To potentially circumvent the need for immune suppressionwhen implanting allogeneic hESC-derived pancreatic cells intopatients with type I diabetes, a particularly attractive approachis to encapsulate the cell product.We optimized a planarmacro-encapsulation device containing a semipermeable barrier(the Encaptra drug delivery system) that can be loaded withPEC-01 cells and implanted subcutaneously. The implantedcell/device combination product (the VC-01 candidate product;ViaCyte, Inc., SanDiego, CA, http://viacyte.com) canmature andfunction in mice (unpublished data), as described for nonencap-sulated grafts, and has the benefit of being easily retrievable.Others have recently published results using a similar device,the TheraCyte device (TheraCyte Inc., Laguna Hills, CA, http://www.theracyte.com/TheTechnology.htm), with similar outcomes[7, 8]. We are currently testing VC-01 in a clinical trial (Clinical-Trials.gov identifier NCT02239354).
PECs generated from hESCs in vitro are mixed populationsthat containmultipotent pancreatic progenitors (PPs), pancreaticendocrine progenitors and precursors, and pancreatic endocrinecells. Theendocrine cells inPECsoftenexpressmultiplehormonesand, in the case of cells expressing insulin, are deficient in expres-sion of essentialb cellmarkers (e.g.,NKX6.1 andPDX1) anddonotrespond appropriately to glucose stimulation. These polyhormo-nal cells havebeencharacterized indetail in recent studies [9–12].Our group has demonstrated previously that purified and reag-gregated cultures of PECs that were highly enriched for PPs anddepleted of endocrine cells can differentiate to endocrine line-ages in vivo including functional b cells, but purified and reaggre-gated polyhormonal endocrine cells do not [3]. This proves that PPsgenerated in vitro are sufficient to generateb cells in vivo.Whetherthe polyhormonal insulin-expressing cells are immature cells orwhether they are inappropriately differentiated and not analogousto cell types produced during normal pancreas development is notknown definitively.
In this study, we described the development of a seven-stage differentiation protocol that produced highly enrichedcultures of pancreatic endocrine cells in vitro (designated“ICs” [islet-like cells]). The first four stages of our IC protocolbuilt on our PEC-01 protocol and increased the PP content intothe range of 73%–80% while greatly reducing (polyhormonal)endocrine cell content. Stage 5was designed to efficiently directendocrine lineage commitment. Conditions supporting endo-crine differentiation were optimized in stages 6 and 7, resultingin cultures consisting of 73%–89% endocrine cells and less than10% PPs. Importantly, insulin-expressing cells produced by thismethod coexpressed other pancreatic hormones at a reduced fre-quencyandcoexpressedNKX6.1andPDX1atahigher frequencycom-pared with the standard four-stage protocol. Methods producingendocrine cells from hESCs with these expression attributes havebeen described recently [13, 14].
The stage 7 cells, when encapsulated and implanted intomice,were capable of producing b-like cells that functioned at a levelsimilar to that of implanted PEC-01 cells; however, becausea low but significant percentage of PPs was present in these cul-tures,we could not rule out that itwas PPs, and not endocrine cellsproduced in vitro, that resulted in functional cells in vivo. We useda dissociation/reaggregation process through which cell aggre-gateswere enriched for endocrine cells and depletedof PPs.Whenimplanted within devices, enriched ICs released human C-peptidein response to glucose, proving that highly purified endocrine cellsdifferentiated in vitro from hESCs can produce functional b-likecells. Importantly, the kinetics of functional maturation in vivoare similar to those of PEC-01 cells, indicating that IC insulin-expressing cells are immature prior to implant.
MATERIALS AND METHODS
All methods are described in the supplemental online data.
RESULTS
Data from 10 independent experiments (numbered 1–10) aredescribed.
Protocol Optimization for PancreaticProgenitor Content
In our four-stage suspension culture-based PEC-01 protocol, hESCdifferentiation progresses through the intermediate stages of defin-itive endoderm (stage 1), primitive gut tube (stage 2), and posteriorforegut (PF; stage 3) and then to a stage 4 population consisting of,on average (49 experiments), 32% PPs and 52% chromograninA-expressingendocrinecells, themajorityofwhicharepolyhormonal[6]. In developing the IC protocol, we initially aimed to increasethe PPs and reduce the endocrine content of the cell populationat the end of stage 4. In PEC-01 and many similar differentiationprotocols, neurogenin 3 (NEUROG3, also known as NGN3)—amaster regulator of endocrine development [15]—is induced duringstage 3. This occurs at the same time as PDX1 induction but wellbefore other critical PP markers, such as NKX6.1 and PTF1A (i.e., inPF cells, not PPs). It seemedplausible that induction of the endocrineprogram in PF cells by NGN3 expression could be an important con-tributor to the generation of polyhormonal endocrine cells. We hy-pothesized that suppressing NGN3 through stages 3 and 4 mightlead to decreased endocrine and increased PP content at the endof stage 4 and that,with further differentiation steps, endocrine cellsthat were more properly specified could be produced from PPs.
We modified the PEC-01 protocol by additionally treatingwith activin A, Wnt3A, and heregulin b1 at stage 3 (days 5–7)and with activin A and heregulin b1 at stage 4 (days 7–13). ThePEC-01and IC (stages 1–4) protocols are shown in schematic formin supplemental online Table 1. Relative to PEC-01, the IC popu-lation at stage 4 hadmore PPs (CHGA-negative [CHGA2], NKX6.1-positive [NKX6.1+], and PDX1+) and fewer endocrine (CHGA+)cells by flow cytometry (supplemental online Table 2). Specifi-cally, IC differentiations yielded, on average, approximately2.5-fold more PPs (75% vs. 32%) and more than 3-fold lower en-docrine (14% vs. 52%) cell content (supplemental onlineTable 2). An activin concentration of either 50 or 75 ng/ml atstage 3 was used in the experiments shown in supplementalonline Table 2. The higher concentrationmay have had a slightly
2 Insulin-Producing Endocrine Cells From hESCs
©AlphaMed Press 2015 STEM CELLS TRANSLATIONAL MEDICINE
by KE
VIN
DA
MO
UR
on September 1, 2015
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
Published Ahead of Print on August 24, 2015 as 10.5966/sctm.2015-0079.

increased effect (supplemental online Table 2) but also resultedin a lower cell yield (data not shown); therefore, activin at 50 ng/mlwas used in all other experiments. The IC protocol was also com-paredwith thePEC-01protocolbydigital RNAanalysis. Stage4 ICcul-tures had higher expression levels of PP genes (e.g., PDX1, NKX6.1,and SOX9) (Fig. 1A) and lower levels of endocrine genes (e.g., CHGA,INS, GCG, SST) (Fig. 1B) than did PEC-01 cultures. Looking at NGN3expression over time (Fig. 1C), amarked reductionwasobservedduring stage 3 in the IC protocol relative to PEC-01. SignificantNGN3 expression occurred during stage 4 in ICs; however, itremained well below that in PEC-01 populations. Consequently,we achieved a cell population that was enriched in PP cells and thathadmuchreduced(premature)endocrinecommitment fromwhichto optimize endocrine differentiation. Protocol stages 1–4were es-sentially the same for all experiments except for a modestly higherstage 3 activin concentration in experiments 1 and 9, as noted.
Endocrine Lineage Commitment From PPs
The next step, stage 5 (days 13–15), was designed tomaximize in-duction ofNGN3. It is well documented that theNotch pathway isa negative regulator ofNGN3 [16]. On ligand binding to Notch re-ceptor, g-secretase cleaves the receptor, releasing the Notch in-tracellular domain, which is part of a complex, including HES
(hairy and enhancer of split) proteins, that represses NGN3 tran-scription [17]; therefore, g-secretase inhibitors (GSIs) can inhibitNotch signaling activity and upregulate NGN3 expression. Wetested the GSI designated RO4929097 [18] for its ability to pro-mote endocrine differentiation from PPs. As seen in Figure 1D,NGN3was strongly induced by this GSI, with a peak of expressionatday15 (of thedays analyzed), followedbya reduction inexpres-sionbyday18 (i.e., 3 days afterGSIwithdrawal). ComparingNGN3levels at day 15 in nontreated versus GSI-treated cells, a 17-foldenhancement was observed with treatment (Fig. 1D). Stage 5treatments were the same in all experiments shown.
Optimization of Insulin Expression andEndocrine Maturation
During stages 6 and 7, we optimized for expression of insulin andmature b cell genes. A schematic of stages 5–7 is shown insupplemental online Table 3A. The resulting populations were an-alyzed by flow cytometry, digital gene expression, and immunoflu-orescence and for proinsulin and C-peptide content. Becausetesting was performed at intervals during the optimization pro-cess thedatapresented inthis studyhadvaryingtreatmentsatstages6 and 7. This is detailed in the supplemental online data (Methodssection) and in supplemental online Table 4. During the iterative
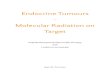
Figure 1. Digital RNA analysis of cell aggregates for pancreatic gene expression during the PEC-01 and IC protocols. Representative resultsfrom three ormore experiments are shown. The twobars depicted for each sample represent biological replicates. RNA levels are shown for PPmarkers (PDX1, PTF1A, NKX6.1, and SOX9) (A) and endocrinemarkers (CHGA, INS, GCG, and SST) (B)on day 13 (experiment 8). (C):RNA levels ofNGN3 over days 5–13 (stages 3 and 4; experiment 8). (D): NGN3 expression during stage 5 (days 13–15) and into stage 6 (day 18) of the ICprotocol (experiment6). Treatmentswere (+)GSI, GSI addedduring stage5; (2) GSI, noGSI added.Abbreviations:GSI,g-secretase inhibitor; IC,islet-like cells; NGN3, neurogenin 3; PEC, pancreatic endoderm cells derived from the PEC-01 protocol; PP, pancreatic progenitor.
Agulnick, Ambruzs, Moorman et al. 3
www.StemCellsTM.com ©AlphaMed Press 2015
by KE
VIN
DA
MO
UR
on September 1, 2015
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
Published Ahead of Print on August 24, 2015 as 10.5966/sctm.2015-0079.

process, some factors that had been beneficial in early experimentshad no positive effect in later versions of the protocol. Examples ofsuch factors are BMP4 and TTNPB, which were not used in the cur-rent IC protocol (supplemental online Table 4). The thyroid hormonetriiodothyronine was added based on studies suggesting involve-ment in b cell maturation [19]. Nicotinamide has been shown topotentiate differentiation of fetal islets in vitro [20]. The Rho-associated kinases (ROCKs) have roles inmultiple cellular functionssuchasadhesion,motility, proliferation,andapoptosis [21], and theROCK inhibitor (ROCKi) Y-27632 can increase survival of hESCs [22].
As shown in supplemental online Table 5, stage 7 IC populationsaveraged 78% endocrine cells, of which 45% were INS+ and 22%were GCG+ cells. Approximately 66% of the INS+ cells were GCG2
(i.e., single-hormone positive). SST has been observed to coexpresswith INS in hESC-derived endocrine cells [23], but there were veryfew SST+ cells present in IC cultures (described in “Histological anal-ysis of native and reaggregated ICs”). RNA analyses at stages 6 and 7(Fig. 2) showed the strong induction of early endocrine genes (e.g.,NGN3, PAX4), followed by hormone genes (e.g., INS, GCG and SST)andmatureb cellmarkers (e.g.,GCK, PCSK1 and SLC30A8).Wenotethat these maturity genes are not necessarily specific to b cells.Othermatureb cell geneswere expressed at very low levels relativeto islets (e.g., IAPP andMAFA; data not shown). The expression pat-terns ofPAX4 andARX are interesting regarding possible dominanceof GCG over INS expression in various paradigms [3, 9, 24].
Enrichment of Endocrine Cells via Dissociationand Reaggregation
A major goal of this work was to prove that endocrine cells pro-duced in vitrowere able tomature and function in vivo. To accom-plish this, a highly enriched endocrine preparation would be
required, to preclude any contribution from PPs present in het-erogeneous populations. We built on a relatively simple enrich-ment technique described previously [3]. That study showedthat PEC-01 aggregates could be enzymatically dissociated andthen reaggregated in rotating suspension culture. The resultingaggregates were enriched in endocrine cells and depleted ofPPs. In contrast, the inclusionofROCKi in the aggregationmediumallowed survival and incorporation of PP into the aggregates. WeremovedROCKi fromthe ICdifferentiationmediumon the last dayofstage6, thendissociatedandreaggregated ICsonthefirstdayofstage7, when the hormone genes were nearing peak expression. The cellswithintheresultingendocrine-enrichedclusterswerevery looselyad-hered, as observedpreviously [3]. The followingday,weaddedROCKinhibitorandasourceofextracellularmatrix in theformofverydilute,and thus soluble, Matrigel (Corning Inc., Corning, NY, https://www.corning.com). The combination of these two components greatly in-creasedthedegreeofcell-cell interactionwithintheclustersand,con-sequently, thestabilityof theaggregates (supplementalonlineFig. 1).
Reaggregated ICs were then differentiated through stage 7.Stages5–7 fornative (i.e., not reaggregated) ICs and reaggregatedICs are shown in schematic form in supplemental online Table 3.In Experiments 2 and 3, as measured by flow cytometry, reaggre-gated ICs contained 98% and 93% endocrine cells and 1% and 3%PPs, respectively (supplemental online Table 6). Compared withnative ICs, reaggregated ICsweremodestly enriched in endocrinemarkers (e.g., CHGA, INS, andGCG) and highly depleted for SOX9,a PP marker that is not expressed in endocrine cells (Fig. 3). Themature b cell genes PCSK1 and SLC30A8 were expressed in bothnative and reaggregated ICs at levels approaching (particularly inexperiment 3) those found in isolated human islets (Fig. 3). Asnoted, thesematurity genes are not necessarily specific tob cells.
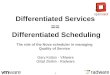
Figure2. RNAanalysisof ICaggregatesduringstages5–7ofdifferentiation (experiment7) showingearlyendocrine (NGN3,PAX4, andARX),hormone(INS, GCG, and SST), andmatureb cell (GCK, IAPP, andG6PC2) markers. Representative results from three ormore experiments are shown. The twobars depicted for each sample represent biological replicates. Abbreviations: GCG, glucagon; INS, insulin; NGN3, neurogenin 3; SST, somatostatin.
4 Insulin-Producing Endocrine Cells From hESCs
©AlphaMed Press 2015 STEM CELLS TRANSLATIONAL MEDICINE
by KE
VIN
DA
MO
UR
on September 1, 2015
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
Published Ahead of Print on August 24, 2015 as 10.5966/sctm.2015-0079.

Histological Analysis of Native and Reaggregated ICs
As noted, previously studied polyhormonal insulin-expressingcells lacked expression of NKX6.1 and PDX1. In contrast, many,if notmost, stage 7 INS+ cells coexpressed these transcription fac-tors, as seen by immunofluorescence, in native IC, reaggregatedIC, and cryopreserved IC samples, shown in Figure 4 (experiment 3)and supplemental online Figures 2–4 (experiments 2, 3, and 4, re-spectively). Depletion of PPs in reaggregated samples can be ob-served (supplemental online Fig. 2). In correlation with notedflow cytometry data, when costained for INS, GCG, and SST,most of the stage 7 cells expressed only one hormone, althoughpolyhormonal cells were observed (Fig. 4; supplemental onlineFigs. 2–4). There were very few SST+ cells in the cultures. Thesedata indicate that stage 7 endocrine cells aremore appropriatelyspecified compared with polyhormonal cells and that cryopres-ervation and thaw or enrichment by reaggregation maintainsthis phenotype.
Proinsulin Processing by ICs Compared WithHuman Islets
To further assess the maturity of stage 7 insulin-producing cells,we quantified the amount of C-peptide (which is generated byprocessing of proinsulin to insulin) present in the cells andthe percentage of proinsulin that was fully processed com-pared with purified human islets (Fig. 5). The mean values for
C-peptide levels, in micrograms of C-peptide per microgram ofDNA (i.e., normalized to cell content), were 0.31 for islets and0.15 for ICs (Fig.5A).Themeanpercentagesofproinsulinprocessedin islets and ICs were 96% and 90%, respectively (Fig. 5B). We con-cluded that ICs produced very significant levels of insulin andC-peptide (albeit approximately twofold lower than islets) andpro-cessed proinsulin essentially as efficiently as human islets do.
In Vivo Assessment of IC Populations
We tested whether ICs could mature and exhibit glucose-stimulated insulin secretion (GSIS) in the in vivo setting. Fivecohorts of SCID/beige mice were implanted with ICs loaded intoEncaptra macroencapsulation devices in 3 experiments (experi-ments 2–4). In experiment 2, native ICswere comparedwith reag-gregated ICs; experiment 3 compared native ICs that had beencryopreservedwith reaggregated ICs; andexperiment 4 consistedof native ICs only. The results of GSIS assays in grafted mice fromexperiments 2 and 3, tested at 8, 12, and 16 weeks after trans-plant, are shown in Figure 6. The serum C-peptide values plottedin Figure 6, and additional values from experiment 4 are shown insupplemental online Table 7. The IC-implanted mouse cohortdata were compared with our database of mice similarlyimplanted with VC-01 in unrelated experiments. At 8 weeks,the median glucose-stimulated C-peptide values were compara-ble for all cohorts and ranged from 326 to 539 pmol/l with the
Figure 3. RNA analysis of IC aggregates at stage 7 of differentiation (experiments 2 and 3) comparing pancreatic gene expression in native ICs(IC), native ICs that had been cryopreserved and thawed (Cryo), and reaggregated ICs (RA) to purified human islets. Representative results fromthree ormore experiments are shown. The two bars depicted for each sample represent biological replicates. Abbreviations: Expt., experiment;GCG, glucagon; IC, islet-like cells; INS, insulin; SST, somatostatin.
Agulnick, Ambruzs, Moorman et al. 5
www.StemCellsTM.com ©AlphaMed Press 2015
by KE
VIN
DA
MO
UR
on September 1, 2015
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
Published Ahead of Print on August 24, 2015 as 10.5966/sctm.2015-0079.

VC-01 controls at 375 pmol/l. As described (supplemental onlineTable 6), the reaggregated IC populations contained 98% (experi-ment2)and93%(experiment3)CHGA+endocrinecells. Importantly,these data prove that in vitro differentiated insulin-producing cellscan mature and function in vivo. These cohorts were not tested attime points earlier than 8weeks because in pilot experimentswithICs, we did not see a robust GSIS response prior to this time (datanot shown); however, these earlier experiments, which were notyet well optimized, also had relatively lowGSIS values at later timepoints (datanot shown). At 12weeks after implant, theGSIS valuesincreased considerably in all cohorts,withmedian values for the IC-engrafted groups between 468 and 848 pm serum C-peptide at60 minutes following glucose injection. There was no clear corre-lationbetweenmedianC-peptide values and native, reaggregated,or cryopreserved cell implants. The median value for the PEC-01
grafts was considerably higher, at 1830 pmol/l C-peptide, com-paredwith the IC grafts; however, the significanceof this is unclearbecause of the relatively small number of animals implanted withICs. Stimulated C-peptide values increased again at 16 weeks afterimplant, and the native IC and VC-01 groups had similar medianglucose-stimulated C-peptide values. At this time point therewas a trend toward the reaggregated IC cohorts havingmedian val-ues below those of the native IC groups and the PEC-01 controls.This would not be particularly surprising considering the harsh na-ture of the reaggregation process; however, as noted, the numberof animals implantedwas too few to be definitive. In summary, ICs,including populations that were essentially pure endocrine cells orthat had been cryopreserved, were capable of maturing in a devicein vivo and subsequently responding appropriately to glucose stim-ulation by releasing insulin.
Figure 4. Immunostaining of stage 7 islet-like cell (IC) aggregates (experiment 3, day 27). (A, B): Immunofluorescence for colocalization of INS,NKX6.1, andPDX1 innative IC aggregates (A) and reaggregated ICs (B). (C, D): Immunofluorescence for INS,GCG, and SST innative IC aggregates (C)and reaggregated ICs (D). Scale bars = 50mm. Abbreviations: DAPI, 49,6-diamidino-2-phenylindole; GCG, glucagon; INS, insulin; SST, somatostatin.
6 Insulin-Producing Endocrine Cells From hESCs
©AlphaMed Press 2015 STEM CELLS TRANSLATIONAL MEDICINE
by KE
VIN
DA
MO
UR
on September 1, 2015
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
Published Ahead of Print on August 24, 2015 as 10.5966/sctm.2015-0079.

Histological Analysis of Explanted IC Grafts
IC grafts were removed between 18 and 24 weeks after implant.GSIS assay results in the week of or the week prior to explant areshowninsupplementalonlineTables8–10(experiments2–4, respec-tively). Robust function was maintained through the latest timepoint examined (24 weeks) (supplemental online Table 9). High-functioning grafts were chosen for immunofluorescent staining(Fig. 7; supplemental online Figs. 5, 6) (experiments 2, 3, and 4, re-spectively). Almost all INS+ cells expressed both PDX1 and NKX6.1.Hormones were very rarely, if ever, coexpressed. As with IC aggre-gates in vitro, there were few SST+ cells in the IC grafts. The immu-nofluorescent analyses of grafts from native, reaggregated, andcryopreserved native IC appeared substantially similar.
DISCUSSION
We developed an in vitro differentiation protocol that producespancreaticendocrinecells fromhESCs.Thisprotocolbuiltonourpre-vious 4-stage protocol [6] bymodifying stages 3 and 4 such that theNKX6.1+/PDX1+ PP pool was increased to 73%–80% (supplemental
online Table 2). This was accomplished with the addition of activinA, Wnt3A, and heregulin b1. We previously found that activin A iscapable of suppressing NGN3 and increasing PP content; however,at effective concentrations, activin A treatment resulted in a reduc-tion of cell yield (data not shown). Wnt3A was capable of counter-acting this cell loss, allowing theuseof relativelyhighconcentrationsofactivinAand, in fact, resulted inanet increase in cells at theendofstage3(datanotshown).Wehavenotaddressedwhether thiseffectof Wnt3A was due to increased proliferation, decreased cell death,decreasedmigration of cells from aggregates (and into themediumand subsequently aspirated on daily feeding), or a combination ofthese. Wnt signaling has been shown to promote proliferation ofPPs in the developingmouse pancreas [25], and activin family signal-ing has been implicated in pancreas specification [26], althoughbecause of the complexity of these pathways, the particular ligandsused in vivo are not well established. Others have used relativelylowconcentrationsofactivinAsimilarly in theirhESC-to-pancreaticcelldifferentiation protocols [10]. Heregulinb1 also decreased the loss ofcells, although not as potently as didWnt3A. In addition, low concen-trations of heregulinb1were used because higher concentrations in-creased expression of CDX2, a posterior gutmarker (data not shown).
When differentiated through stage 7, IC populations could bemacroencapsulated, implanted, and matured in vivo to glucose-responsive b-like cells (Fig. 6). The ability to form functional graftswhile protected from cell-cell interactions with the immune systemis a critical component of any potential allogeneic cell therapy for di-abetes. Furthermore, as proof of the efficacy of in vitro-derivedendocrine cells, we showed that enriched ICs, largely depleted ofPPs, can function similarly to native ICs (Fig. 6; supplemental onlineTable 6). Because ICs contain some polyhormonal cells, as seen insupplemental online Table 5, it is possible that they can mature andcontribute to in vivo function. The small fraction of PPs remainingin enriched ICs (supplemental online Table 6) likely contribute, at
Figure5. Proinsulin processing by stage 7 IC aggregates andhumanislets. Samples tested were three lots of purified human islets, des-ignated a, b, and c, as IC-a (experiment 9, day 34), IC-b (experiment10, day 28), and IC-c (experiment 10, day 33). (A): Enzyme-linked im-munosorbent assay (ELISA) for C-peptide content (in micrograms)normalized to DNA content (in micrograms). (B): Percentage of pro-insulin processed, calculated using the ratio of C-peptide to C-peptideplus proinsulin (both determined by ELISA). Error bars represent theSEM of C-peptide. Abbreviations: C-PEP, C-peptide; IC, islet-like cells.
Figure 6. Enzyme-linked immunosorbent assay of human C-peptidelevels in sera of implanted mice. Mice implanted with Encaptra-loaded aggregates were analyzed at the indicated postengraftmenttimes (8, 12, or 16 weeks) for human C-peptide at fasting and60 minutes after intraperitoneal glucose administration. HumanC-peptide released by IC implants was compared with our historicaldata frommicewith VC-01 implants. The x-axis labels for IC implantsare as follows: IC (native ICs, experiment 2), Cryo (native ICs that hadbeen cryopreserved and thawed, experiment 3), RA-1 (reaggre-gated ICs, experiment 2), RA-2 (reaggregated ICs, experiment 3).C-peptide values are shown both in picomoles per liter and nano-grams per milliliter. Horizontal bars show median serum C-peptidecontent. Abbreviation: IC, islet-like cells.
Agulnick, Ambruzs, Moorman et al. 7
www.StemCellsTM.com ©AlphaMed Press 2015
by KE
VIN
DA
MO
UR
on September 1, 2015
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
Published Ahead of Print on August 24, 2015 as 10.5966/sctm.2015-0079.

most,asmall fractionofthe invivoactivity.Anothercriticalcomponentofapotential cell therapy is theability to cryopreserveand recover thecell product, and that ability was demonstrated in this study (Fig. 6).
Two important reports thatpancreatic endocrine cells producedfromhESCs in vitro can also function in vivowere published recently[13, 14]. The in vivo studies in the reportswere performedwithnon-encapsulated cells. Remarkably, the endocrine cells produced invitrowere shown to respond to glucose in vitro in both publications,with an approximately twofold stimulation index (which was similarto human islet controls). We do not see a reproducible response toglucose by insulin-producing cells generated with our IC protocol(data not shown). We have not directly compared the cells gener-ated by the three protocols; nonetheless, some interesting observa-tions can be made. All three protocols produce endocrine cells thatare approximately 50% INS+, and a high proportion of these are
GCG2. In addition, a high proportion of INS+ cells also are positivefor theb cell markers PDX1 and NKX6.1. These important attributesare all in contrast to previously reported polyhormonal cells derivedfrom hESCs. All three protocols produce relatively high proportionsof PPs by the end of stage 4, (.55% in [13], 62% in [14] as shown inone flowcytometryplot, andanaverageof75%shown in this study).Wenoted that the timeatwhichendocrine inductionwaspromotedby addition of a GSI was the same (day 13) among the 3 protocols.This may be related to the previously described [27] competencewindows of pancreatic progenitors for the formation of the variousendocrine cell types. Consequently, cells produced by all three regi-mens have very important similarities despite relatively divergentprotocols. Concerning the time required to first observe in vivo func-tion,we consistently sawa significant GSIS response at 8weekswithboth IC and PEC-01 protocols, not far from the 6 weeks reported by
Figure 7. Immunostaining of IC grafts in Encaptra devices at 22 weeks after implantation (experiment 2). (A, B): Immunofluorescence forcolocalization of INS, NKX6.1, and PDX1 in grafts of native ICs (A) and reaggregated ICs (B). (C, D): Immunofluorescence for INS, GCG, andSST in grafts of native ICs (C) and reaggregated ICs (D). Scale bars = 50mm. Abbreviations: DAPI, 49,6-diamidino-2-phenylindole; GCG, glucagon;IC, islet-like cells; INS, insulin; SST, somatostatin.
8 Insulin-Producing Endocrine Cells From hESCs
©AlphaMed Press 2015 STEM CELLS TRANSLATIONAL MEDICINE
by KE
VIN
DA
MO
UR
on September 1, 2015
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
Published Ahead of Print on August 24, 2015 as 10.5966/sctm.2015-0079.

Rezania et al. [14]. This indicates that ICs require additional develop-mental maturation to acquire a b cell-like glucose response. Takentogether, our data strongly suggest that the insulin-expressing cellswithin ICsmostclosely resemble immatureb cells.Thesecells shouldprove to be a great starting point for gaining a better understandingof the final steps of b cell maturation.
ACKNOWLEDGMENTS
We thank the California Institute for Regenerative Medicine forfunding support in the form of Strategic Partnership AwardSP1-06513. Confocalmicroscopywas performed at theUniversityof California San Diego School of Medicine Microscopy Core,which uses funding fromNational Institute of Neurological Disor-ders and Stroke P30 Core Grant NS047101.
AUTHOR CONTRIBUTIONS
A.D.A.: conception and design, collection and assembly ofdata, data analysis and interpretation, wrote the manuscript,
final approval of manuscript; D.M.A.: design, collection and as-sembly of data, data analysis and interpretation, manuscriptwriting; M.A.M.: design, data analysis; A.B.: design, collectionand assembly of data, data analysis; R.M.C.: assembly of data,data analysis J.K.P., J.R.K., C.H., R.S., A.Z.W., J.K., and M.A.F.:collection and assembly of data; E.J.K.: design, data analysisand interpretation; K.A.D.: design, data analysis and interpre-tation, manuscript writing, final approval of manuscript
DISCLOSURE OF POTENTIAL CONFLICTS OF INTEREST
All authors are employees of ViaCyte Inc. A.D.A. has uncom-pensated patents assigned to ViaCyte Inc., has compensatedresearch funding, and is an uncompensated ViaCyte, Inc.shareholder. D.M.A. has uncompensated stock options.M.A.M., A.B., R.M.C., J.K.P., J.R.K., C.H., R.S., A.Z.W., J.K.,and M.A.F. have compensated research funding and uncom-pensated stock options. E.J.K. and K.A.D. have compensatedresearch funding and are uncompensated ViaCyte, Inc.shareholders.
REFERENCES
1 McCall M, Shapiro AM. Update on islettransplantation. Cold Spring Harb Perspect Med2012;2:a007823.
2 Pagliuca FW, Melton DA. How to makea functional b-cell. Development 2013;140:2472–2483.
3 Kelly OG, Chan MY, Martinson LA et al.Cell-surface markers for the isolation of pan-creatic cell types derived from human embry-onic stem cells. Nat Biotechnol 2011;29:750–756.
4 KroonE,Martinson LA, KadoyaKet al. Pan-creatic endoderm derived from human embry-onic stem cells generates glucose-responsiveinsulin-secreting cells in vivo. Nat Biotechnol2008;26:443–452.
5 Rezania A, Bruin JE, Riedel MJ et al. Mat-uration of human embryonic stem cell-derivedpancreatic progenitors into functional islets ca-pable of treating pre-existing diabetes in mice.Diabetes 2012;61:2016–2029.
6 Schulz TC, Young HY, Agulnick AD et al. Ascalable system for production of functionalpancreatic progenitors from human embryonicstem cells. PLoS One 2012;7:e37004.
7 Bruin JE, Rezania A, Xu J et al. Maturationand function of human embryonic stem cell-derived pancreatic progenitors in macroencap-sulation devices following transplant into mice.Diabetologia 2013;56:1987–1998.
8 Kirk K, Hao E, LahmyR et al. Human embry-onic stem cell derived islet progenitors matureinside an encapsulation devicewithout evidenceof increased biomass or cell escape. Stem CellRes (Amst) 2014;12:807–814.
9 Basford CL, Prentice KJ, Hardy AB et al.The functional and molecular characterisationof human embryonic stem cell-derived insulin-positive cells compared with adult pancreaticbeta cells. Diabetologia 2012;55:358–371.10 Bruin JE, Erener S, Vela J et al. Character-
ization of polyhormonal insulin-producing cellsderived in vitro from human embryonic stemcells. Stem Cell Res (Amst) 2014;12:194–208.11 HrvatinS,O’DonnellCW,DengFetal.Dif-
ferentiated human stem cells resemble fetal,not adult, b cells. Proc Natl Acad Sci USA2014;111:3038–3043.12 Xie R, Everett LJ, Lim HW et al. Dynamic
chromatin remodeling mediated by polycombproteins orchestrates pancreatic differentia-tion of human embryonic stem cells. Cell StemCell 2013;12:224–237.13 Pagliuca FW,Millman JR, Gurtler M et al.
Generation of functional human pancreatic bcells in vitro. Cell 2014;159:428–439.14 RezaniaA, Bruin JE, AroraP et al. Reversal
of diabetes with insulin-producing cells derivedin vitro from human pluripotent stem cells. NatBiotechnol 2014;32:1121–1133.15 Rukstalis JM, Habener JF. Neurogenin3:
A master regulator of pancreatic islet differ-entiation and regeneration. Islets 2009;1:177–184.16 Afelik S, Jensen J. Notch signaling in the
pancreas: Patterning and cell fate specifica-tion. Wiley Interdiscip Rev Dev Biol 2013;2:531–544.17 Jorissen E, De Strooper B. Gamma-
secretase and the intramembrane proteolysisof Notch. Curr Top Dev Biol 2010;92:201–230.18 Huynh C, Poliseno L, SeguraMF et al. The
novel gamma secretase inhibitor RO4929097
reduces the tumor initiating potential of mela-noma. PLoS One 2011;6:e25264.19 Aguayo-MazzucatoC, ZavackiAM,Marine-
larena A et al. Thyroid hormone promotespostnatal rat pancreatic b-cell develop-ment and glucose-responsive insulin se-cretion through MAFA. Diabetes 2013;62:1569–1580.20 Otonkoski T, Beattie GM, Mally MI
et al. Nicotinamide is a potent inducer of en-docrine differentiation in cultured human fe-tal pancreatic cells. J Clin Invest 1993;92:1459–1466.21 Olson MF. Applications for ROCK ki-
nase inhibition. Curr Opin Cell Biol 2008;20:242–248.22 Watanabe K, Ueno M, Kamiya D et al. A
ROCK inhibitor permits survival of dissociatedhuman embryonic stem cells. Nat Biotechnol2007;25:681–686.23 D’AmourKA,BangAG,EliazerSetal.Produc-
tion of pancreatic hormone-expressing endocrinecells from human embryonic stem cells. NatBiotechnol 2006;24:1392–1401.24 Spijker HS, Ravelli RB, Mommaas-
Kienhuis AM et al. Conversion of mature hu-man b-cells into glucagon-producing a-cells.Diabetes 2013;62:2471–2480.25 Murtaugh LC. The what, where, when
and how of Wnt/b-catenin signaling in pan-creas development. Organogenesis 2008;4:81–86.26 Wiater E, Vale W. Roles of activin family
in pancreatic development and homeostasis.Mol Cell Endocrinol 2012;359:23–29.27 Johansson KA, Dursun U, Jordan N et al.
Temporal control of neurogenin3 activity inpancreas progenitors reveals competence win-dows for the generation of different endocrinecell types. Dev Cell 2007;12:457–465.
See www.StemCellsTM.com for supporting information available online.
Agulnick, Ambruzs, Moorman et al. 9
www.StemCellsTM.com ©AlphaMed Press 2015
by KE
VIN
DA
MO
UR
on September 1, 2015
http://stemcellstm
.alphamedpress.org/
Dow
nloaded from
Published Ahead of Print on August 24, 2015 as 10.5966/sctm.2015-0079.

Methods Ethics Statement The CyT49 cell line (NIH Registration Number 0041) was ethically derived from a donated embryo with informed consent. Animal experiments were performed at Neurocrine Biosciences, Inc., San Diego, CA and were approved by their Institutional Animal Care and Use Committee, protocol # V-12-01. Human Embryonic stem cell (hESC) culture. The CyT49 hESC line (NIH registration number 0041) was cultured as described [6]. Briefly, hESC were grown in monolayer culture in DMEM/F12 with Glutamax, plus 10% (v/v) xeno-free serum replacement, 1% (v/v) non-essential amino acids, 1% (v/v) penicillin/streptomycin (all from Life Technologies), 10 ng/mL Heregulin-
1 (Peprotech), and 10 ng/mL Activin A (R&D Systems). Cultures were dissociated to single cells with Accutase (Innovative Cell Technologies) and re-plated every 3 to 4 days. 10% (v/v) soluble-phase human AB serum (Valley Biomedical) was added to the medium for cell attachment on the first day of each passage only. Cells were used for differentiation studies between passages 27 and 33 only. hESC aggregation. Cells were placed in suspension culture in 6-well plates essentially as described [6], or alternatively in 500 mL bottles for larger experiments. Briefly, hESC monolayers were dissociated with Accutase (Innovative Cell Technologies), collected and resuspended at 1x106 cells/mL in StemPro hESC SFM (Life Technologies; combined DMEM/F12 containing Glutamax, StemPro hESC supplement, BSA, and 1% (v/v) Penicillin/streptomycin; omitted FGF-2 and 2-Mercaptoethanol). The single cell suspensions were dispensed to non-TC treated 6-well plates (5.5 mL/well) and rotated at 95 rpm on an Innova 2000 rotator (New Brunswick Scientific), or dispensed to 500 mL Nalgene filter receiver storage bottles (150 mL/bottle) and rotated at 65 rpm on a Sartorius Certomat RM-50 rotator (configured with a 5 cm axis of rotation). Cells were rotated overnight in a 37oC/8% CO2 incubator and formed
aggregates of approximately 100-200M. hESC aggregate differentiation. Differentiation to PEC-01 in 6-well plates was essentially as described in [6]; alternatively, the protocol was scaled-up for use in 500mL bottles. Stages 1 and 2 of IC differentiation were identical to PEC-01. Stage 1 (2 days; protocol days 0-2): hESC aggregates were collected, centrifuged at 500 rpm for 1 minute, and washed with stage 1/2 base medium (RPMI 1640 supplemented with 1% (v/v) Glutamax, 1% (v/v) penicillin/streptomycin (all from Life Technologies), and 0.2% (v/v) FBS (Hyclone)). Aggregate pellet volume was measured and used to determine the number of
vessels required for differentiation. 6-well plates required 33 mL medium and 80 L cells, and
bottles required 150 mL medium and 350 L cells. Cells were distributed in Stage 1/2 base medium supplemented with ITS-G (Life Technologies, 1:5000 dilution), Activin A (100ng/mL, R&D Systems), and Wnt3a (50ng/mL, R&D Systems). Plates were rotated at 95 rpm, and bottles

at 70 rpm, in a 37oC/8% CO2 incubator. On day 1, cells were fed with the same medium minus Wnt3a. Medium was changed daily; feeding volumes were 4.5 mL for plates and 140 mL for bottles. Stage 2 (3 days; protocol days 2-5): Day 2 used Stage 1/2 base medium with ITS-G (Life
Technologies, 1:1000 dilution), TGF RI Kinase inhibitor IV (2.5 M, EMD Bioscience), and KGF (25
ng/mL, Peprotech). Days 3 and 4 used same medium minus TGFRI kinase inhibitor. Plates were rotated at 95 rpm on days 2 and 3 and at 105 rpm on day 4; and bottles were rotated at 70 rpm. Stage 3 (2 days; protocol days 5-7): PEC-01 stage 3 was shortened from 3 to 2 days, to coincide with IC stage 3. Stage 3/4/5 base medium was DMEM high glucose with 1% (v/v) Glutamax, 1% (v/v) penicillin/streptomycin, and 1% (v/v) B-27 supplement (all from Life Technologies). For PEC-01, cells were fed with stage 3/4/5 base medium plus TTNPB (3 nM, Sigma-Aldrich), KAAD-
cyclopamine (0.5 M, Toronto Research Chemicals), and Noggin (50 ng/mL, R&D Systems). IC medium additionally contained Activin A (50 or 75 ng/mL, R&D Systems), Wnt3a (50 ng/mL,
R&D Systems), and Heregulin-1 (5 ng/mL, Peprotech). Plates were rotated at 105 rpm and bottles at 70 rpm. Stage 4 (6 days; protocol days 7-13): For PEC-01, stage 3/4/5 base medium plus Noggin (50 ng/mL, R&D Systems), KGF (50 ng/mL, Peprotech), and EGF (50 ng/mL, Peprotech) was used. IC
medium additionally contained Activin A (5 ng/mL, R&D Systems) and Heregulin-1 (5 ng/mL, Peprotech) on days 7-10 only. Plates were rotated at 105 rpm on day 7 and at 95 rpm on days 8-13; and bottles were rotated at 68 rpm. Stage 5 (2 days; protocol days 13-15): Stages 5-7 are performed for IC only. Cells were treated with stage 3/4/5 base medium with Noggin (50 ng/mL, R&D Systems), KGF (50 ng/mL,
Peprotech), EGF (50 ng/mL, Peprotech), -secretase inhibitor (GSI) RO4929097 (0.5 M,
Cellagen Technology), and Rho-associated protein kinase inhibitor (ROCKi) Y-27632 (10 M, Tocris Bioscience). B-27 could be substituted with the combination (referred to as B-27 substitute) of ITS-G (0.5% (v/v), Life Technologies), chemically defined lipid concentrate (0.5% (v/v), Life Technologies), and BSA (0.2% (wt/v), Millipore). Aggregates were typically collected from bottles and redistributed to plates at this stage (can also be done at stages 6 or 7) to facilitate multi-variable testing. Plates were rotated at 100 rpm and bottles at 70 rpm. Stage 6 (5 days; protocol days 15-20) and Stage 7 (6-14 days; protocol days 20-34): Stage 6/7 base medium was CMRL 1066 (with an additional 3.5g/L glucose added) or DMEM high glucose, supplemented with 1% (v/v) Glutamax, 1% (v/v) penicillin/streptomycin, and 1% (v/v) B-27 supplement (all from Life Technologies). B-27 could be substituted with the combination (referred to as B-27 substitute) of ITS-G (0.5% (v/v) , Life Technologies), chemically defined lipid concentrate (0.5% (v/v), Life Technologies), and BSA (0.2% (wt/v), Millipore). Cells were fed at stages 6 and 7 with stage 6/7 base medium further supplemented as detailed by experiment in Supplementary Table 4. The additional supplements included combinations of ROCKi (Y-27632,

10 M, Tocris Bioscience), Nicotinamide (10 mM, Stem Cell Technologies), Triiodothyronine (T3) (25 nM, Sigma-Aldrich), TTNPB (1 nM, Sigma-Aldrich), BMP4 (10 ng/mL, Peprotech), Matrigel (0.05% (v/v), BD Biosciences), and IGF2 (50 ng/mL, R&D systems). Many iterative experiments have led to a current procedure which includes, of the above ‘additional supplements’, ROCKi and Nicotinamide at stage 6, and ROCKi, Nicotinamide, Matrigel, and T3 at stage 7. The start day of stage 7 was not critical and occasionally occurred 1 day later or earlier than day 20. Plates were rotated at 100 rpm and bottles at 70 rpm. Re-aggregation for endocrine cell enrichment: Re-aggregation was performed similarly as described [3]. All experiments that included a re-aggregation step utilized DMEM-containing stage 6/7 base medium at stage 6 and on the day of re-aggregation; re-aggregation in CMRL-containing medium has not been optimized. Re-aggregation occurred on day 20, but could also be performed at least 1 day earlier or later. Cells were fed with medium without ROCKi on the day prior to, and the day of re-aggregation. Aggregates were washed twice in DPBS (without calcium and magnesium, Life Technologies) with centrifugation at 500 rpm for 1 minute. Drawing of aggregates into pipettes or tips is avoided from this step until after dissociation as aggregates become very sticky at this point. Cell pellet volume was measured and used to determine reagent volume for the next step. Aggregates were dissociated with Accumax (Innovative Cell Technologies) at room temperature; 4 mL enzyme solution and 2 mL DPBS
(without calcium and magnesium) were used per 100 L pellet volume. Aggregates were triturated with a P1000 pipettor after 10 minutes of digestion, and every 2-3 minutes thereafter, until a single cell suspension is achieved. The reaction must be monitored closely to avoid excessive cell lysis. Three volumes of DMEM-containing stage 6/7 base medium were added and mixed with cells, and an aliquot was removed to obtain a cell count. Cells were centrifuged at 1000 rpm for 5 minutes. Cells were resuspended at 1x106 cells/mL in DMEM-containing stage 6/7 base medium (which does not contain ROCKi) plus DNAse I (10 Units/μl, Roche). 5 mL cell suspension was added per well of each 6-well plate, and the plates were rotated at 95 rpm. The following day, cells were very gently collected (cells are loosely adherent), allowed to settle, washed with stage 6/7 base medium, resuspended, and distributed to plates in stage 7 medium. The composition of stage 7 medium is detailed in Supplementary Table 4, and contained ROCKi and Matrigel for all re-aggregated conditions. Cryopreservation and thaw of cell aggregates: Stage 7 IC aggregates were collected, centrifuged at 500 rpm for 1 minute, and washed in cryopreservation solution containing CMRL with 60% (v/v) xeno-free Serum Replacement, 25mM HEPES (all from Life Technologies), and 10% (v/v) DMSO (OriGen Biomedical). Cells were resuspended in cryopreservation solution, aliquoted into freezing vials, held for 30 minutes at 4oC, and then placed on ice. The vials were transferred to a controlled-rate freezer (Planer, Kryo 560-16) which was equilibrated to 0 oC. The cells were brought to -9 oC at a rate of 2oC /min, held at this temperature for 10 minutes, and the vials were seeded manually. The temperature was held at -9 oC for another 10 minutes and then decreased at a rate of 0.2oC /minute down to -40oC. The freezing chamber was subsequently cooled at a rate of 25oC /minute down to -150oC. The vialed cells were moved to the vapor phase of a liquid nitrogen storage freezer. To recover cells for culture and implant, vials were rapidly thawed in a 37oC water bath. The cells were transferred to a 15 mL sterile

tube containing base medium, mixed gently, and centrifuged at 1000 rpm for 5 minutes. The cells were resuspended in stage 7 medium with DNAse I (10 Units/μl, Roche) and placed in rotation culture. The following days, cells were fed with stage 7 medium. The IC condition in Experiment #3 denoted as ‘native, cryo’ was cryopreserved on day 23 and thawed on the same day (thus keeping the day of differentiation consistent between both conditions in the experiment). Flow Cytometric Analysis: Undifferentiated hESC, hESC-derived DE aggregates, or hESC-derived pancreatic aggregates were washed in PBS and then enzymatically dissociated to single cell suspensions at 37oC using Accumax (Innovative Cell Technologies). MACS Separation Buffer (Miltenyi Biotec #130-091-221) was added, and the suspension was passed through a 40 μM filter and pelleted. Cells were fixed for 30 minutes in 4% (wt/v) paraformaldehyde, washed in FACS Buffer (PBS, 0.1% (wt/v) BSA, 0.1% (wt/v) NaN3), and stored in IC Buffer (PBS, 1% (wt/v) BSA, 0.1% (wt/v) NaN3). Cells were permeabilized with Perm Buffer (PBS, 0.2% (v/v) Triton X-100, 5% (v/v) normal donkey serum, 0.1% (wt/v) NaN3) for 30 minutes on ice and then washed with IC buffer. Cells were incubated with primary antibodies diluted with Block Buffer (PBS, 0.1% (v/v) Triton X-100, 5% (v/v) normal donkey serum, 0.1% (wt/v) NaN3) overnight at 4oC. Cells were washed in IC buffer and then incubated with secondary antibodies for 60 min at 4oC. Cells were washed with IC Buffer and then in FACS Buffer. Cells were resuspended in FACS buffer for flow acquisition. Antibodies and dilutions used for staining were: Primary: rabbit anti-CHGA (DAKO, A0430, 1:1000), mouse anti-NKX6.1 (Developmental Studies Hybridoma Bank, F55A12, 1:750), goat anti-PDX1 (Abcam, ab47383, 1:2000), guinea pig anti-insulin (DAKO, A0564, 1:1000), mouse anti-glucagon (Sigma-Aldrich, G2654, 1:2000), and goat anti-somatostatin (Santa Cruz, 7819, 1:500); Secondary (all were made in donkey): Alexa Fluor 488 anti-rabbit (Jackson, 711-546-152, 1:5000), DyLight 488 anti-rabbit (Jackson, 711-486-152, 1:1000), Alexa Fluor 488 anti-mouse (Molecular Probes, A21202, 1:2000), PE anti-mouse (Jackson, 715-116-151, 1:100 or 1:500), Cy5 anti-guinea pig (Jackson, 706-176-148, 1:2000), DyLight 488 anti-goat -(Jackson, 705-486-147, 1:1000), Alexa Fluor 647 anti-goat (Jackson, 705-606-147, 1:6000), and PE anti-goat (Jackson, 705-116-147, 1:1000). Flow cytometry data were acquired with a FACSCalibur (BD Biosciences), using excitation lines at 488 nm and 635 nm and detecting fluorescence at 530+/-15 nm, 585+/-21 nm, and 661+/-8 nm. Data were analyzed using FlowJo software (Tree Star, Inc.). Intact cells were identified based on forward (low angle) and side (orthogonal, 90u) light scatter. To account for the varying levels of autofluorescence observed in these complex samples, additional gating of intact cells (2–3 subpopulations) was performed, and cells were subsequently analyzed for fluorescence intensity. Background was estimated using unstained, secondary-antibody alone, or irrelevant antibody controls, as appropriate. In some figures, a representative flow cytometry plot is shown from one of the sub-populations. Numbers reported on plots and in tables represent the percentage of total cells from the intact cells gate. Gene expression analysis: Total RNA was isolated from duplicate biological samples using the
ABI Prism 6100 Nucleic Acid Prep Station (Applied BioSystems) and associated ABI materials and reagents per manufacturer’s instructions. Gene Expression was determined using 100ng
per sample of total RNA in the NanoString Technologies nCounter analysis system per

manufacturer’s instructions utilizing custom code sets designed at ViaCyte, Inc. and produced
by NanoString Technologies. Briefly, per sample reaction, sample RNA (100ng) was combined with reporter code set and capture probe set and allowed to hybridize overnight at 65°C. The
next day, purification and binding reactions were performed in the nCounter PrepStation. Subsequently, the cartridge containing hybridized, purified target RNA bound to fluorescent
barcode was placed into the nCounter Digital Analyzer for counting at 1155 FOV per sample. Once the samples were analyzed on the nCounter® Digital Analyzer, a Reporter Code Count (RCC) output file was generated containing the count data for the controls and probe/target complexes in the samples. The RCC file was imported into the Genedata Analyst™ software program (Genedata AG., Switzerland) using the NanoString parser developed by Genedata AG., for RCC files. The parser directly imports the RCC file, annotates all gene data by accession number including positive and negative controls, and performs a quality control analysis of the experiment. The quality control analysis results are reported in the Genedata Analyst™ program as “good” or “bad”, which corresponds to passing or failing, respectively, of the
nCounter assay quality control criteria. Within the program, the gene expression data was then normalized using a fixed target value for the geometric mean of the housekeeping genes (ACTB, PPIG, POLR2A, and TBP) multiplexed into the custom code set. The normalized gene expression values can then be directly compared between samples in the same experiment as well as samples in other experiments (that use the same codeset) since all data is normalized to the same fixed target value. Data in figure 1 was generated using codeset A while figures 2 and 3
utilized codeset B.
Content analysis of IC aggregates and human islets: Three different lots of human islets were purchased from ProCell Biotech, LLC. IC aggregates and human islets were homogenized using
the Bullet Blender®. To each sample tube, 200 L of RNase-free zirconium-oxide beads (Next
Advance, Inc.) were added along with 300 L of cold TE buffer (20 mM Tris-HCl, pH 7.5, 50 mM
NaCl, 1 mM EDTA) supplemented with 1 L of SUPERase• In™ RNase Inhibitor (Life Technologies). The tubes were placed in the Bullet Blender® and run twice with the speed control set at 8 for 4 minutes. The tubes were placed in ice for at least 1 min between each
run. Once homogenized, the lysates were divided into 2 fractions: #1) 40 L of lysate was diluted 1:2 in water in the presence of protease inhibitors, for protein content analysis; and #2)
15 L of the lysate was diluted 1:20 in UltraPure™ DNase/RNase-Free Distilled Water (Life Technologies) for measurement of DNA concentration. DNA was quantified using the PicoGreen® dsDNA Quantitation Kit (Life Technologies). C-peptide content was measured using the C-peptide ELISA kit, product number 10-1136-01 (Mercodia) and proinsulin was measured using the Proinsulin ELISA kit, product number 10-1118-01 (Mercodia). The ELISA’s were performed according to the manufacturer’s instruction manuals. Immunofluorescent Staining: Differentiated hES cell–derived aggregates were fixed with 4% (wt/v) paraformaldehyde for 1 hour at room temperature, washed with PBS, and then equilibrated in 30% sucrose at 4°C overnight. Aggregates were mounted with Optimal Cutting Temperature Compound (Tissue-Tek) to make frozen blocks and were cut into 8 μm sections. Devices were fixed in 10% (v/v) neutral buffered formalin (Fisher Scientific) for 6-30 hours at

room temperature then processed for paraffin embedding using the Leica ASP300S Advanced Smart Processor. Devices were cut into 5 µM sections which were deparaffinized and rehydrated in preparation for staining. For the Insulin/PDX1/NKX6.1 co-staining, both frozen (cell aggregates) and paraffin (grafts in devices) sections underwent heat-induced epitope retrieval prior to staining. Sections were washed with PBS twice for 10 minutes followed by PBST (PBS/0.2% (v/v) Tween20; Thermo Fisher Scientific) for 15 minutes. Blocking was done for 1 hour at room temperature with 5% (v/v) normal donkey serum (Jackson ImmunoResearch Labs)/PBSTr (PBS/0.1% (v/v) Triton X-100 (Sigma)). Primary and secondary antibodies were diluted in 1% (wt/v) BSA (Sigma)/ PBSTr. Primary antibodies were incubated at 4°C overnight and secondary antibodies for 1 hour 15 minutes in a moisture chamber at room temperature. The following primary antibodies and dilutions were used: guinea pig anti-insulin, 1:500 (Dako, A0564); rabbit anti-somatostatin, 1:300 (Dako, A0566); mouse anti-glucagon, 1:200 (Sigma, G2654); mouse anti-NKX6-1, 1:20 (Developmental Studies Hybridoma Bank, F55A12, used for staining of frozen sections); goat anti-NKX6-1, 1:500 (LSBio, LS-C124275, used for paraffin sections); and rabbit anti-PDX1, 1:500 (Epitomics, 3470-1). The following secondary antibodies were used at a dilution of 1:500: Cy3-conjugated donkey anti-goat, Cy5-conjugated donkey anti-guinea pig (both from Jackson ImmunoResearch Laboratories), Alexa Fluor-488 donkey anti-rabbit, and Alexa Fluor-555 donkey anti-mouse (both from Life Technologies). Imaging was done by confocal microscopy (Olympus FV1000) and acquired with Olympus FluoView software. Digital processing of images was performed using Adobe Photoshop. Manipulations included cropping a portion of an image from a larger field and adjusting the levels of each color channel on the entire image.
Encapsulation and Transplantation: Encaptra-20 devices were wetted with base culture
medium. IC were collected and gravity settled in 1.5 mL tubes and 10 L aliquots of cell pellet (approximately 3 x 106 cells) were pipetted to individual tubes containing approximately 0.5mL base medium. An aliquot of cells and medium was delivered through the device loading port with a catheter/syringe assembly. The device port was sealed with medical-grade silicone adhesive and trimmed. SCID beige mice were anesthetized with ketamine/xylazine and supplemental isoflurane. For implant, a lateral dorsal incision was made, and a subcutaneous pocket was created by blunt dissection with a hemostat. The loaded device was placed in the pocket, and the incision was closed with surgical clips. IC were implanted at day 29 (Experiment #2), day 27 (Experiment #3), or day 26 (Experiment #4) of in vitro differentiation. Glucose Stimulated Insulin Secretion (GSIS) Assay: Graft function was assessed by performing measurement of serum human C-peptide in response to glucose administration essentially as described [6]. Prior to the GSIS assay, mice were fasted for approximately 15–18 hours. Glucose was administered via intraperitoneal injection of a 30% dextrose (Hospira) solution at a dose of 3.0 g/kg body weight, and blood was collected prior to (fasting) and at 30 and/or 60 minutes
after glucose administration. Blood samples of approximately 50 L were collected by retro-orbital sinus puncture under isoflurane anesthesia and transferred to microtainer tubes (BD Biosciences, cat#365956) containing blood/serum separation gel. Serum was collected after spinning these tubes at 4000–6000 x g for 10 minutes. Human C-peptide was measured using the Mercodia Ultrasensitive Human C-peptide ELISA, cat#10-1141-01. We regard the lower limit

of accurate quantitation of human C-peptide in serum samples to be 50 pM [4]. The level of cross-detection of mouse C-peptide is <1%, or a maximum of 30 pM in glucose stimulated control mice. The level of cross-detection of human insulin is <0.0006% and of proinsulin is <1.8%.

Supplemental Information – Agulnick et al.
Supplemental Figures
Figure S1. Grayscale images of cell aggregates that were re-aggregated on day 20 of in vitro differentiation (Experiment #1). (A): Cell aggregates on day 21 (1 day post re-aggregation). (B): Aggregates on day 23 (3 days post re-aggregation). (C): Aggregates on day 23 which have been treated with dilute MG. (D): Aggregates on day 23 which have been treated with ROCKi. (E): Aggregates on day
23 which have been treated with both MG and ROCKi. Scale bars = 500 m. Abbreviations: MG, Matrigel; ROCKi, Rho-associated protein kinase inhibitor Y-27632.

Figure S2. Immunostaining of stage 7 IC aggregates (Experiment #2, day 29). (A,B): Immunofluorescence for co-localization of INS, NKX6.1, and PDX1 in native IC (A) and re-aggregated IC (B). (C,D): Immunofluorescence for INS, GCG, and SST in native IC (C) and re-aggregated IC (D). Scale bars = 50 µm. Abbreviations: DAPI, 4',6-diamidino-2-phenylindole; GCG, glucagon; INS, insulin; SST, somatostatin.

Figure S3. Immunostaining of stage 7 IC aggregates (Experiment #3, day 27). (A): Immunofluorescence for co-localization of INS, NKX6.1, and PDX1 in native IC that had been cryopreserved and thawed. (B): Immunofluorescence for INS, GCG, and SST in native IC that had been cryopreserved and thawed. Scale bars = 50 µm. Abbreviations: DAPI, 4',6-diamidino-2-phenylindole; GCG, glucagon; INS, insulin; SST, somatostatin.

Figure S4. Immunostaining of stage 7 IC aggregates (Experiment #4, day 26). (A): Immunofluorescence for co-localization of INS, NKX6.1, and PDX1 in native IC. (B): Immunofluorescence for INS, GCG, and SST in native IC. Scale bars = 50 µm. Abbreviations: DAPI, 4',6-diamidino-2-phenylindole; GCG, glucagon; INS, insulin; SST, somatostatin.

Figure S5. Immunostaining of IC grafts in Encaptra devices 24 weeks after implantation (Experiment #3). (A,B): Immunofluorescence for co-localization of INS, NKX6.1, and PDX1 in grafts derived from IC that had been cryopreserved and thawed (A) or IC that had been re-aggregated (B). (C,D): Immunofluorescence for INS, GCG, and SST in grafts from IC that had been cryopreserved and thawed (C) or IC that had been re-aggregated (D). Scale bars = 50 µm. Abbreviations: DAPI, 4',6-diamidino-2-phenylindole; GCG, glucagon; INS, insulin; SST, somatostatin.

Figure S6. Immunostaining of IC grafts in Encaptra devices 18 weeks after implantation (Experiment #4). (A): Immunofluorescence for co-localization of INS, NKX6.1, and PDX1 in grafts of native IC. (B): Immunofluorescence for INS, GCG, and SST in grafts of native IC. Scale bars = 50 µm. Abbreviations: DAPI, 4',6-diamidino-2-phenylindole; GCG, glucagon; INS, insulin; SST, somatostatin.

Supplemental Tables – Agulnick et al.
Stage: 1 2 3 4
Definitive Endoderm (DE) Primitive Gut Tube (PG)
Posterior Foregut (PF) Pancreatic Progenitor (PP)
Days: 2 (0-2) 3 (2-5) 2 (5-7) 6 (7-13)
Base Medium: RPMI 0.2% FBS DMEM 1% B-27
Factors:
PEC-01
Activin A, WNT3A KGF,
TGFI (day 2 only)
TTNPB, Cyclopamine, Noggin
Noggin, KGF, EGF
IC
TTNPB, Cyclopamine, Noggin, Activin A,
WNT3A,
Heregulin 1
Noggin, KGF, EGF, Activin A,
Heregulin 1
Markers: SOX17, CXCR4 HNF1, HNF4 PDX1, HNF6, SOX9 PDX1, SOX9, PTF1A,
NKX6.1
Table S1. Description of the differentiation of hESC to definitive endoderm through pancreatic progenitors (stages 1-4) in both the PEC-01 and IC protocols, including media and factors used and stage-specific markers. Abbreviations: IC, islet-like cells; PEC-01, pancreatic endoderm cells; TGFβi, TGF-β RI kinase Inhibitor IV; ITS, Insulin-Transferrin-Selenium used at different concentrations in Stage-1 and -2.
Experiment, Condition
Total Endocrine [CHGA+]
CHGA- NKX6.1+ PDX1+
[PP]
CHGA- NKX6.1- PDX1+
[PDX1-only]
Residual
#1, ActA [75] 6.5 72.7 8.4 12.4
#6, ActA [50] 16.7 73.2 6.1 4.0
#9, ActA [50] 20.4 73.8 1.6 4.2
#9, ActA [75] 14.3 80.2 1.5 4.0
Mean (n=4) 14 75 4 6
Table S2. Flow cytometric analysis of cell aggregates on day 12 or 13 of the IC differentiation protocol across three Experiments ( #1, #6 and #9). Cell subsets quantified, expressed as percentage of total live cells, were: endocrine (CHGA+), pancreatic progenitor (CHGA-/ NKX6.1+/ PDX1+), and PDX1-only (CHGA-/ NKX6.1-/ PDX1+), cells. Abbreviations: [ActA], activin A concentration at stage 3 in ng/mL; CHGA, chromogranin A; PP, pancreatic progenitor.

A
Stage: 5 6 7
Endocrine Progenitor
Endocrine Precursor
Endocrine
Days: 2 (13-15) 5 (15-20) 6-14 (20-34)
Base Medium: DMEM 1% B-27 CMRL 1% B-27
Factors: Noggin, KGF, EGF,
GSI, ROCKi Nic, ROCKi
Nic, MG, ROCKi, T3
Markers: NGN3, NKX2.2 Hormones PCSK1, SLC30A8
B
Stage: 5 6 re-agg 7
Endocrine Progenitor
Endocrine Precursor
Endocrine
Days: 2 (13-15) 5 (15-20) 1 (20-21) 5-13 (21-34)
Base Medium: DMEM 1% B-27 CMRL 1% B-27
Factors:
Noggin, KGF, EGF, GSI, ROCKi
Nic, ROCKi Nic Nic, MG
ROCKi, T3
Markers: NGN3, NKX2.2 Hormones PCSK1, SLC30A8
Table S3. Description of the differentiation of pancreatic progenitors to endocrine cells (stages 5-7) in the IC protocol (A) and the IC protocol with re-aggregation on day 20 (B), including media and factors used and stage-specific markers. Abbreviations: GSI; γ-secretase inhibitor RO4929097; MG, Matrigel; NGN3, neurogenin 3; Nic, Nicotinamide; ROCKi, Rho-associated protein kinase inhibitor Y-27632; T3, Triiodothyronine.

Experiment Stage 6 Stage 7
1 DMEM; B-27; ROCKi DMEM; B-27; ROCKi; MG
2 DMEM; B-27; ROCKi; MG; Nic; BMP4 DMEM; B-27; ROCKi; MG; BMP4; TTNPB; IGF2
3 DMEM; B-27; ROCKi; Nic; BMP4 CMRL; B-27; ROCKi; MG; BMP4; TTNPB; IGF2
4 CMRL; B-27; ROCKi; MG; Nic; BMP4; TTNPB CMRL; B-27; ROCKi; Nic; BMP4; TTNPB; IGF2
5 CMRL; B-27; ROCKi; Nic; BMP4; TTNPB CMRL; B-27; ROCKi; Nic; BMP4
6 CMRL; B-27 substitute; ROCKi; Nic; BMP4 CMRL; B-27 substitute; Nic; BMP4; T3
7 CMRL; B-27 substitute; ROCKi; Nic; BMP4 CMRL; B-27 substitute; ROCKi; MG; Nic; BMP4; T3
8 CMRL; B-27 substitute; ROCKi; Nic CMRL; B-27 substitute; ROCKi; MG; Nic; BMP4
9 CMRL; B-27 substitute; ROCKi; Nic CMRL; B-27 substitute; ROCKi; MG; Nic; T3
10 CMRL; B-27; ROCKi; Nic CMRL; B-27; ROCKi; Nic; T3
Current CMRL; B-27; ROCKi; Nic CMRL; B-27; ROCKi; MG; Nic; T3
Table S4. Summary of late-stage media and factors used in Experiments #1-10. Abbreviations: B-27 substitute, see description in supplemental methods; MG, Matrigel; Nic, Nicotinamide; ROCKi, Rho-associated protein kinase inhibitor Y-27632; T3, Triiodothyronine. The bottom row (labeled ‘Current’) represents our current best protocol for IC stages 6 and 7. We note that this protocol has not yet been tested in an in vivo model.
Experiment, Condition
Total Endocrine [CHGA+]
Total INS+
Total GCG+
INS+ GCG-
INS+ GCG+
INS-only as a % of total INS+
#4 85.2 49.3 23.5 34.3 15.0 70
#5 73.2 42.8 18.2 30.8 12.0 72
#5, B-27 sub 77.8 37.5 20.3 25.2 12.2 67
#7, B-27 sub 74.2 46.0 22.9 30.2 15.9 66
#7 77.6 51.5 25.5 29.0 20.0 56
Mean (n=5) 78 45 22 30 15 66
Table S5. Flow cytometric analysis of IC aggregates during stage 7 across Experiments #4, #5, and #7. Results, expressed as percentage of total live cells (except in last column; see below), include: chromogranin A, insulin, and glucagon positive cells as well as singly-positive insulin (INS+/ GCG-), and insulin/glucagon co-positive (INS+/ GCG+) cells. In the last column only, results are expressed as a percent of total insulin-positive cells. Abbreviations: CHGA, chromogranin A; INS, insulin; GCG, glucagon; B-27 sub, B-27 supplement was substituted as described in the supplemental methods.

Experiment, Condition
Total Endocrine [CHGA+]
CHGA- Nkx6.1+ Pdx1+ [PP]
CHGA- Nkx6.1- Pdx1+
[PDX1-only]
Residual
#2, Native 87.1 10.4 2.2 0.2
#2, Re-agg 98.2 1.4 0.6 -0.2
#3, Native 88.6 5.4 4.4 1.7
#3, Re-agg 92.9 3.4 2.1 1.7
#3, Native/Cryo 90.0 5.2 3.5 1.4
Table S6. Flow cytometric analysis for pancreatic cell content in IC aggregates (Experiments #2 and #3). Conditions tested were: Native (non-re-aggregated IC), Re-agg (re-aggregated IC), and Native/Cryo (native IC that had been cryopreserved and thawed). Cell subsets quantified, expressed as percentage of total live cells, were: endocrine (CHGA+), pancreatic progenitor (CHGA-/ NKX6.1+/ PDX1+), and PDX1-only (CHGA-/ NKX6.1-/ PDX1+) cells. Abbreviations: CHGA, chromogranin A; PP, pancreatic progenitor.

Expt# Cohort Subgroup
Serum C-peptide following glucose challenge (pM)
8 weeks 12 weeks 16 weeks
fasting 30’ 60’ fasting 30’ 60’ fasting 30’ 60’
2
1 Native
489 ND 1012 606 1480 2676 516 2183 3423
205 ND 408 440 542 799 1014 2593 2478
87 ND 198 99 131 207 413 753 740
396 ND 499 281 434 752 724 1192 2053
95 ND 142 84 21 177 346 273 418
Median: 205 NA 408 281 434 752 516 1192 2053
2 Re-agg
385 ND 1217 418 1084 1091 484 1046 636
352 ND 1151 484 1104 1666 958 2073 2929
127 ND 302 388 866 1321 769 2066 1228
137 ND 349 355 678 605 766 1024 1494
141 ND 239 162 179 326 473 586 786
119 ND 215 199 225 319 502 614 929
Median: 139 NA 326 371 772 848 634 1035 1079
3
3 Native/
Cryo
0 ND 65 81 318 136 325 522 926
162 ND 469 269 321 632 456 1370 2387
144 ND 367 442 538 578 658 1168 1830
231 ND 500 466 1354 908 779 2076 2347
313 ND 1137 761 470 2536 1586 4043 5969
252 ND 548 406 374 861 912 2194 3636
Median: 197 NA 485 424 422 747 719 1723 2367
4 Re-agg
222 ND 503 315 394 527 727 1207 1872
199 ND 316 343 513 388 668 1330 1510
318 ND 580 310 453 948 690 1115 1800
391 ND 602 319 333 594 239 997 655
141 ND 311 113 229 312 227 559 629
253 ND 575 211 136 410 423 809 1157
Median: 238 NA 539 313 363 468 545 1056 1334
4 5 Native
263 ND 428 232 ND 681 ND ND ND
325 ND 487 244 ND 983 ND ND ND
376 ND 623 436 ND 1175 ND ND ND
293 ND 585 240 ND 681 ND ND ND
463 ND 543 347 ND 536 ND ND ND
396 ND 654 581 ND 1231 ND ND ND
284 ND 344 164 ND 470 ND ND ND
260 ND 302 45 ND 183 ND ND ND
Median: 309 NA 515 242 NA 681 NA NA NA
Table S7. Serum human C-peptide levels (pM) in glucose-stimulated mice implanted with IC aggregates at 8, 12, and 16 weeks post-implantation (Experiments #2, #3, and #4). The subgroups tested were: Native (non-re-aggregated IC), Re-agg (re-aggregated IC), and Native/Cryo (IC that had been cryopreserved and thawed). Serum C-peptide levels were measured at fasting and 30 and 60 minutes after intraperitoneal glucose administration. Abbreviation: pM, picomoles/L.

Expt# Cohort Subgroup
Serum C-peptide following glucose challenge
21 weeks
fasting 30 min 60 min
2
1 Native
933 1437 1798
724 1935 1669
617 1395 1632
755 2397 2437
488 230 462
Median: 724 1437 1669
2 Re-agg
436 1308 1458
609 1701 2691
622 1809 1495
454 932 1123
268 332 542
Median: 454 1308 1458
Table S8. Serum human C-peptide levels (pM) in glucose-stimulated mice implanted with IC aggregates at 21 weeks post-implantation (Experiment #2). The subgroups tested were: Native (non-re-aggregated IC) and Re-agg (re-aggregated IC). Serum C-peptide levels were measured at fasting and 30 and 60 minutes after intraperitoneal glucose administration. Abbreviation: pM, picomoles/L.

Expt# Cohort Subgroup
Serum C-peptide following glucose challenge
24 weeks
fasting 30 min 60 min
3
3
Native/ Cryo
483 969 782
707 1234 1642
817 1440 2187
794 1834 1237
1482 4336 5659
1172 2057 2154
Median: 806 1637 1898
4 Re-agg
1124 2000 1825
1043 2375 1371
969 1220 1269
796 1119 848
548 1112 871
Median: 969 1220 1269
Table S9. Serum human C-peptide levels (pM) in glucose-stimulated mice implanted with IC aggregates at 24 weeks post-implantation (Experiment #3). The subgroups tested were: Native/Cryo (IC that had been cryopreserved and thawed) and Re-agg (re-aggregated IC). Serum C-peptide levels were measured at fasting and 30 and 60 minutes after intraperitoneal glucose administration. Abbreviation: pM, picomoles/L.
Expt# Cohort Subgroup
Serum C-peptide following glucose challenge
18 weeks
fasting 30 min 60 min
4 5 Native
348 677 1209
579 2084 2794
579 1084 3673
441 753 2819
913 985 1995
1078 1944 3015
252 761 1146
106 226 391
Median: 510 873 2395
Table S10. Serum human C-peptide levels (pM) in glucose-stimulated mice implanted with IC aggregates at 18 weeks post-implantation (Experiment #4). The subgroup tested was: Native (non-re-aggregated IC). Serum C-peptide levels were measured at fasting and 30 and 60 minutes after intraperitoneal glucose administration. Abbreviation: pM, picomoles/L.