Embed Size (px)
Citation preview
2016
CNEA / Key Choice 1
1
Presented by:
Karen Marzlin DNP, RN, ACNPC-AG, CCNS, CCRN-CMC, CHFN
Cynthia Webner DNP, RN, ACNPC-AG, CCNS, CCRN-CMC, CHFN
www.cardionursing.com 2016
“Professional nursing practice can only advance as
much as individual nurses are aware that a
knowledge gap exists in their practice, feel
empowered to access further learning, and
integrate evidence based competencies into their
professional practice to provide safe, effective,
efficient, patient centered, equitable care.”
www.tigersummit.com
6 2016
2016
CNEA / Key Choice 2
7 2016
8
Acute Coronary Syndrome (ACS)
No ST Elevation
Non STEMI
Unstable Angina
ST Elevation
STEMI
2016
2016
CNEA / Key Choice 3
9
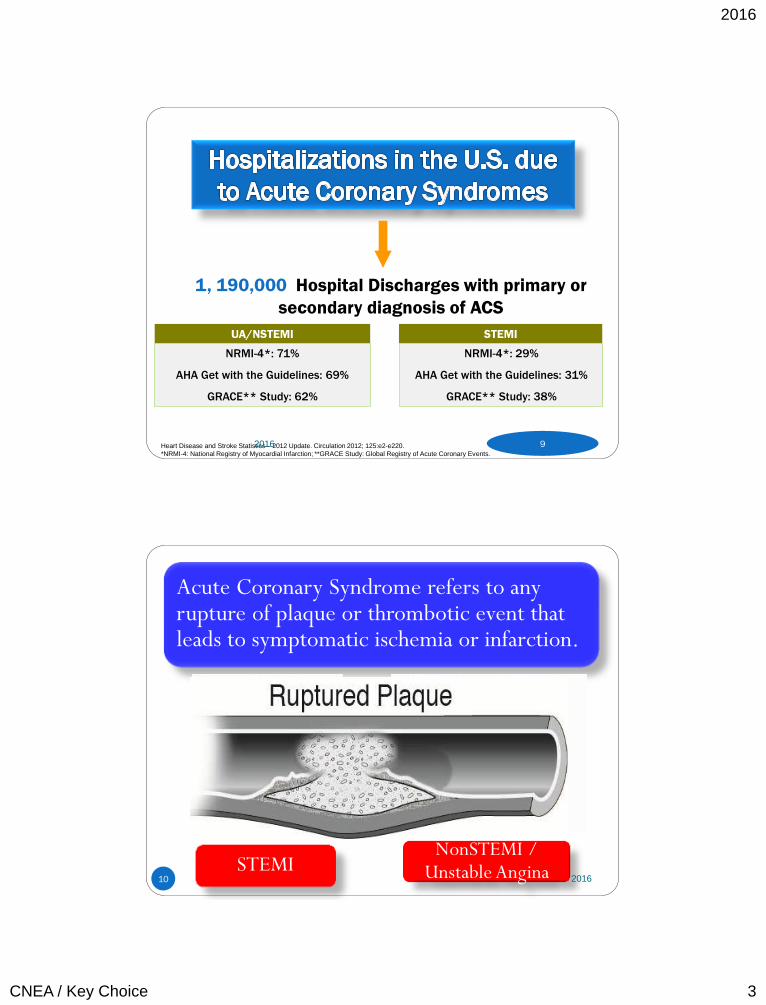
1, 190,000 Hospital Discharges with primary or
secondary diagnosis of ACS
UA/NSTEMI STEMI
NRMI-4*: 71%
AHA Get with the Guidelines: 69%
GRACE** Study: 62%
NRMI-4*: 29%
AHA Get with the Guidelines: 31%
GRACE** Study: 38%
Heart Disease and Stroke Statistics – 2012 Update. Circulation 2012; 125:e2-e220.
*NRMI-4: National Registry of Myocardial Infarction; **GRACE Study: Global Registry of Acute Coronary Events.
2016
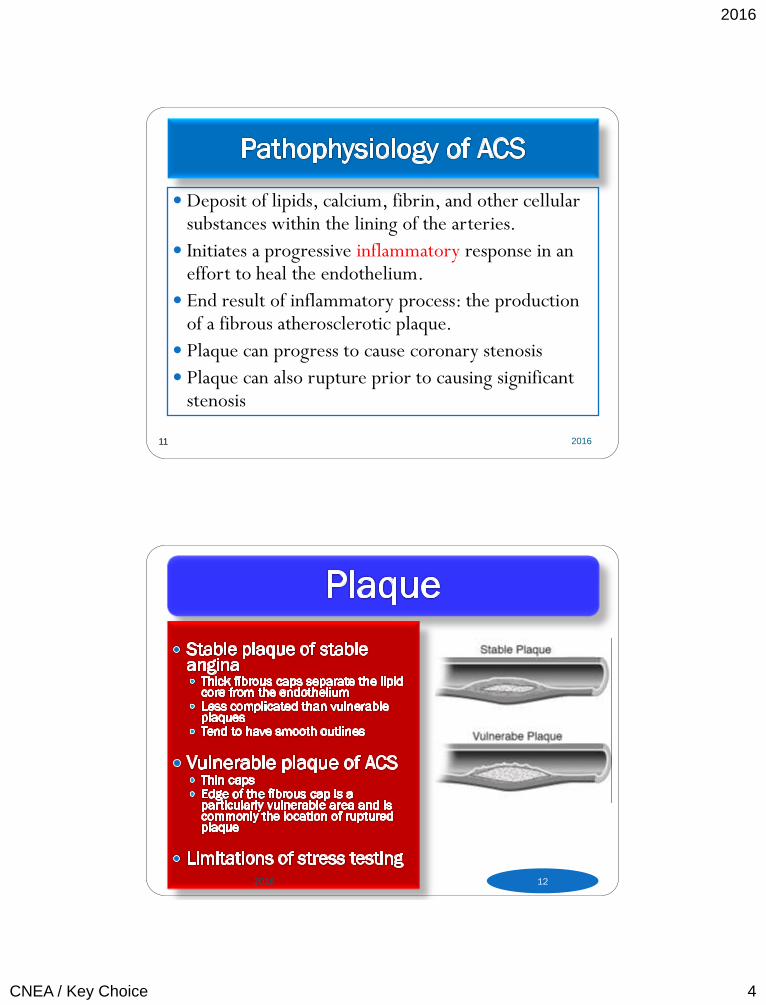
Acute Coronary Syndrome refers to any rupture of plaque or thrombotic event that leads to symptomatic ischemia or infarction.
STEMI NonSTEMI /
Unstable Angina 10 2016
2016
CNEA / Key Choice 4
11
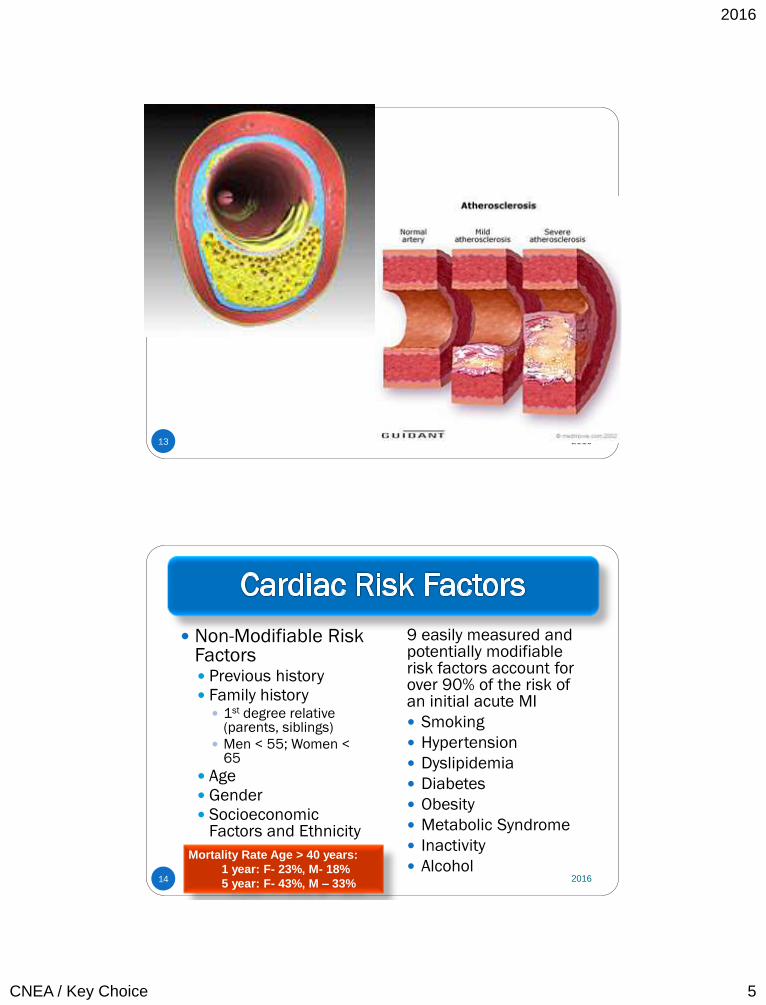
Deposit of lipids, calcium, fibrin, and other cellular substances within the lining of the arteries.
Initiates a progressive inflammatory response in an effort to heal the endothelium.
End result of inflammatory process: the production of a fibrous atherosclerotic plaque.
Plaque can progress to cause coronary stenosis
Plaque can also rupture prior to causing significant stenosis
2016
12 2016
2016
CNEA / Key Choice 5
13 2016
Non-Modifiable Risk Factors Previous history Family history
1st degree relative (parents, siblings)
Men < 55; Women < 65
Age
Gender
Socioeconomic Factors and Ethnicity
9 easily measured and potentially modifiable risk factors account for over 90% of the risk of an initial acute MI
Smoking
Hypertension
Dyslipidemia
Diabetes
Obesity
Metabolic Syndrome
Inactivity
Alcohol
Mortality Rate Age > 40 years:
1 year: F- 23%, M- 18%
5 year: F- 43%, M – 33% 14 2016
2016
CNEA / Key Choice 6
15 2016
Classic Symptoms
Stable angina
Unstable angina
MI
Symptom Variations
Women Elderly Diabetics
16 2016
2016
CNEA / Key Choice 7
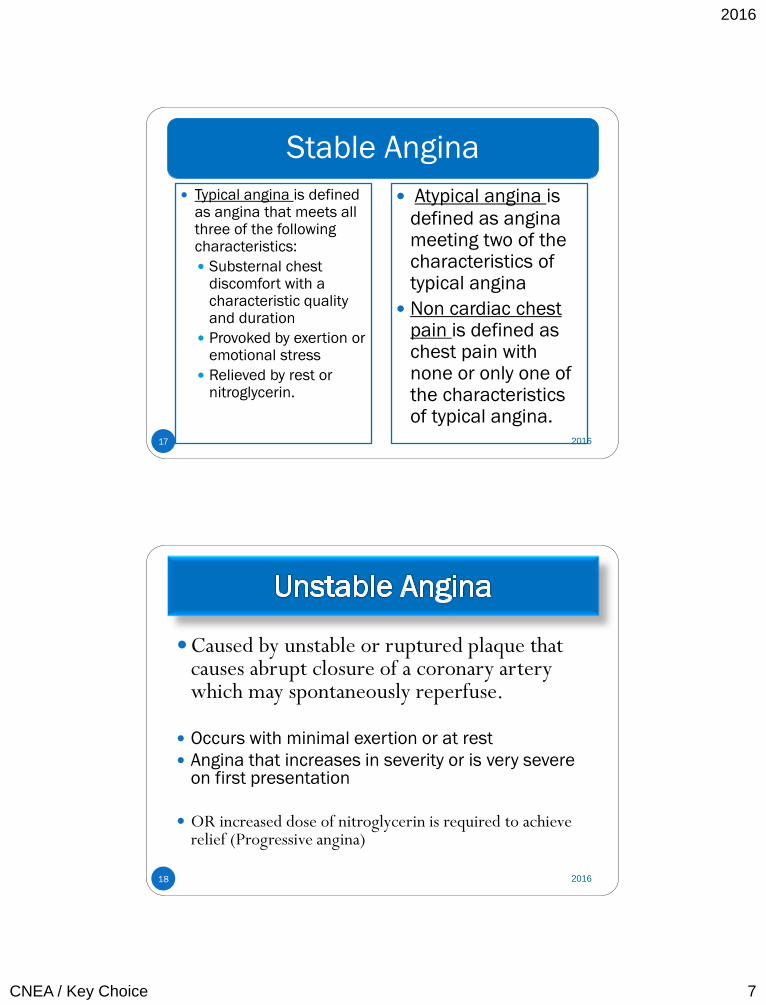
Stable Angina
17
Typical angina is defined as angina that meets all three of the following characteristics:
Substernal chest discomfort with a characteristic quality and duration
Provoked by exertion or emotional stress
Relieved by rest or nitroglycerin.
Atypical angina is
defined as angina meeting two of the characteristics of typical angina
Non cardiac chest pain is defined as chest pain with none or only one of the characteristics of typical angina.
2016
18
Caused by unstable or ruptured plaque that causes abrupt closure of a coronary artery which may spontaneously reperfuse.
Occurs with minimal exertion or at rest
Angina that increases in severity or is very severe on first presentation
OR increased dose of nitroglycerin is required to achieve relief (Progressive angina)
2016
2016
CNEA / Key Choice 8
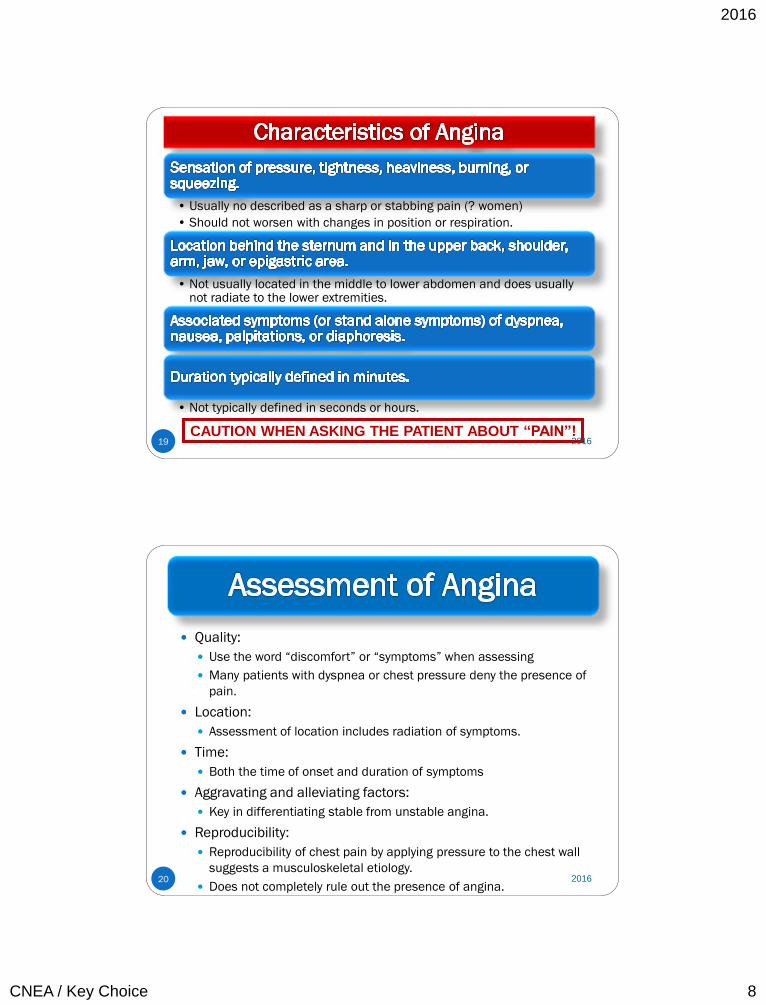
19
• Usually no described as a sharp or stabbing pain (? women)
• Should not worsen with changes in position or respiration.
• Not usually located in the middle to lower abdomen and does usually not radiate to the lower extremities.
• Not typically defined in seconds or hours.
CAUTION WHEN ASKING THE PATIENT ABOUT “PAIN”! 2016
20
Quality:
Use the word “discomfort” or “symptoms” when assessing
Many patients with dyspnea or chest pressure deny the presence of
pain.
Location:
Assessment of location includes radiation of symptoms.
Time:
Both the time of onset and duration of symptoms
Aggravating and alleviating factors:
Key in differentiating stable from unstable angina.
Reproducibility:
Reproducibility of chest pain by applying pressure to the chest wall
suggests a musculoskeletal etiology.
Does not completely rule out the presence of angina.
2016
2016
CNEA / Key Choice 9
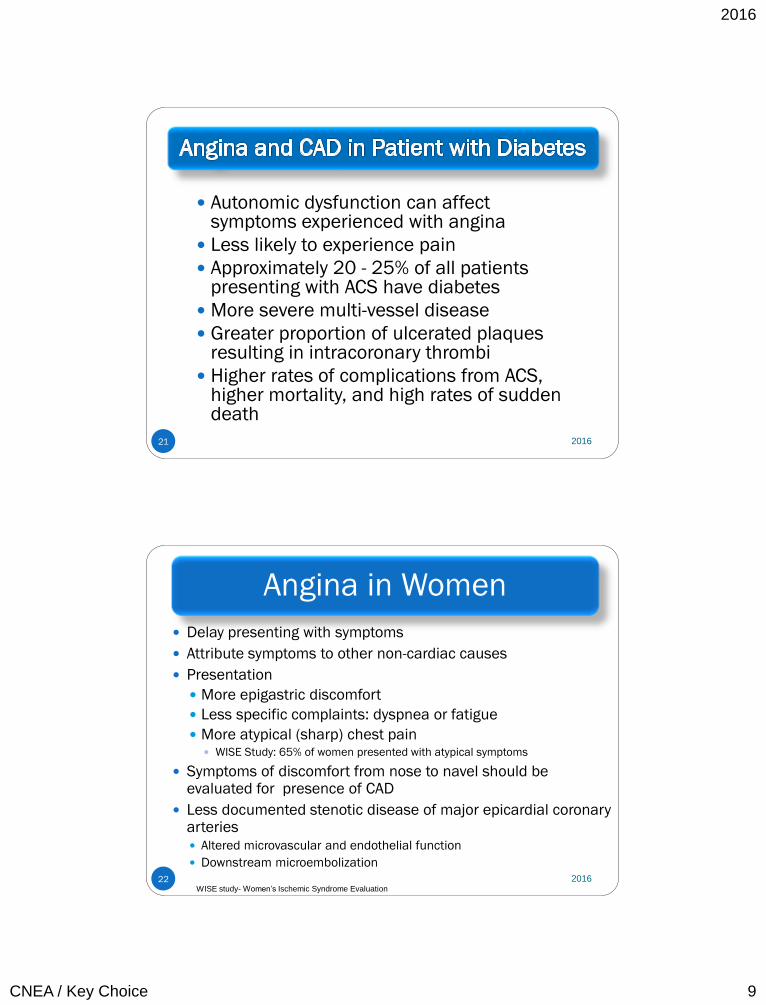
21
Autonomic dysfunction can affect symptoms experienced with angina
Less likely to experience pain
Approximately 20 - 25% of all patients presenting with ACS have diabetes
More severe multi-vessel disease
Greater proportion of ulcerated plaques resulting in intracoronary thrombi
Higher rates of complications from ACS, higher mortality, and high rates of sudden death
2016
Angina in Women
22
Delay presenting with symptoms
Attribute symptoms to other non-cardiac causes
Presentation
More epigastric discomfort
Less specific complaints: dyspnea or fatigue
More atypical (sharp) chest pain WISE Study: 65% of women presented with atypical symptoms
Symptoms of discomfort from nose to navel should be evaluated for presence of CAD
Less documented stenotic disease of major epicardial coronary arteries Altered microvascular and endothelial function
Downstream microembolization
WISE study- Women’s Ischemic Syndrome Evaluation
2016
2016
CNEA / Key Choice 10
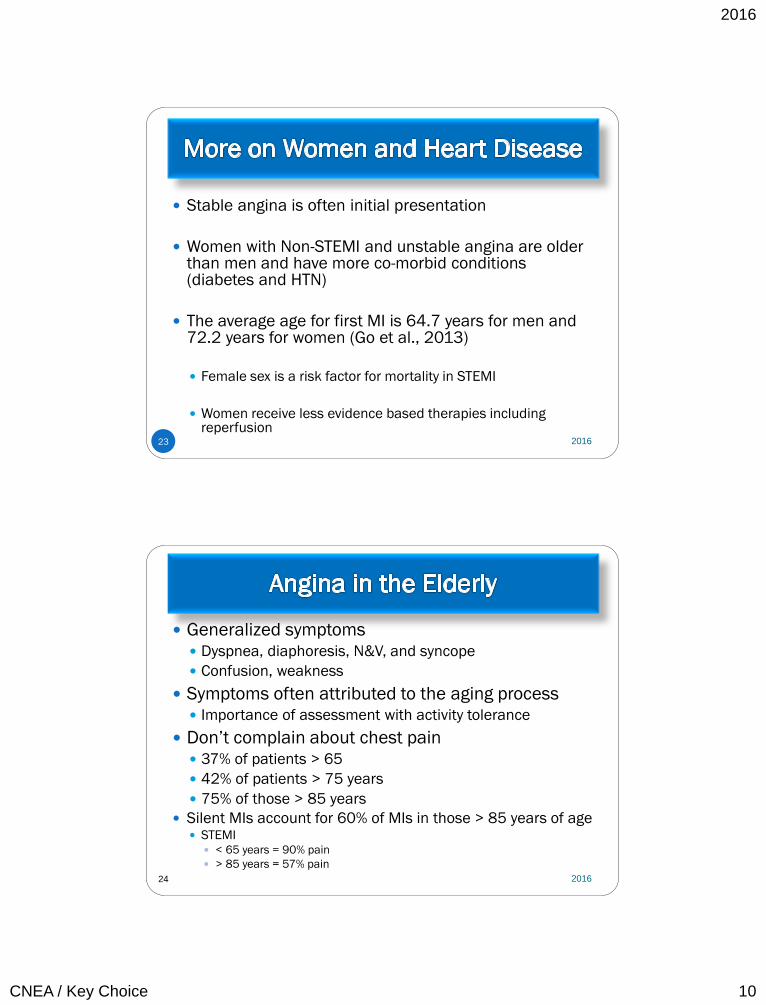
23
Stable angina is often initial presentation
Women with Non-STEMI and unstable angina are older than men and have more co-morbid conditions (diabetes and HTN)
The average age for first MI is 64.7 years for men and 72.2 years for women (Go et al., 2013)
Female sex is a risk factor for mortality in STEMI
Women receive less evidence based therapies including
reperfusion
2016
24
Generalized symptoms Dyspnea, diaphoresis, N&V, and syncope
Confusion, weakness
Symptoms often attributed to the aging process Importance of assessment with activity tolerance
Don’t complain about chest pain 37% of patients > 65
42% of patients > 75 years
75% of those > 85 years
Silent MIs account for 60% of MIs in those > 85 years of age STEMI
< 65 years = 90% pain
> 85 years = 57% pain
2016
2016
CNEA / Key Choice 11
25
LBBB complicates the recognition of STEMI
LBBB is present 33.8% of STEMI patients > 85 years.
STEMI recognized only 70% of time in patients > 85 years
Often co-existing heart failure with the ACS diagnosis
NSTEMI
44% not diagnosed on admission
HF with STEMI
< 65 years = 12%
> 85 years = 45%
Diagnosis of “Other”
< 65 years = 5%
> 85 years = 24%
2016
26
Decreased arterial compliance
Increased cardiac afterload
Diastolic dysfunction of the left ventricle
Inflammatory dysregulation
2016
2016
CNEA / Key Choice 12
27
Mobility and function Activities of daily living
Strength
Frailty: state of declining reserves in physical strength and functional status
Poor Nutrition Status Albumin
Weight loss
More co-morbid conditions
Altered renal and hepatic function
More co-morbid conditions
Altered renal and hepatic function
Poly pharmacy
Cognitive Impairment
Hearing Alterations
Vision Alterations
Isolation
Resources / Education
Socioeconomic
2016
28
> 75 years of age:
high risk for short
term death or non-
fatal MI.
In hospital death:
< 65 years: 1 in 100
> 85 years: 1 in 10
Morbidity and mortality
after STEMI also increased
due to electrical and
mechanical complications.
Heart failure and
pulmonary edema occur in
more than half of patients
> 75 years
Shock occurs in > 10% of
patients > 75 years.
2016
2016
CNEA / Key Choice 13
29 2016
29-38% of ACS patients
Complete occlusion of a vessel by a thrombus
Fibrin stable clot (red clot)
Classified more specifically by the portion of the left ventricle suffering injury.
Mortality is greatest within the first 24 to 48 hours of symptom onset
TREATMENT FOCUS = REPERFUSION 30 2016
2016
CNEA / Key Choice 14
Nationally under treated according to evidence based practice guidelines (Crusade Registry)
Pathophysiology often involves a platelet plug or white clot
Less stable clot
Opportunity for spontaneous reperfusion
Differentiated from unstable angina by troponin levels
TREATMENT FOCUS = ANTIPLATELET THERAPY 31 2016
32
Increase myocardial oxygen demand: Hyperthermia
Hypertension
Tachycardia
Conditions producing over stimulation of the sympathetic nervous system (cocaine use, hyperthyroidism)
Decrease myocardial oxygen delivery: Anemia
Pulmonary disease.
Increase myocardial oxygen demand and decrease myocardial oxygen supply: Aortic stenosis
Hypertrophic cardiomyopathy
Type 2 MI
2016
2016
CNEA / Key Choice 15
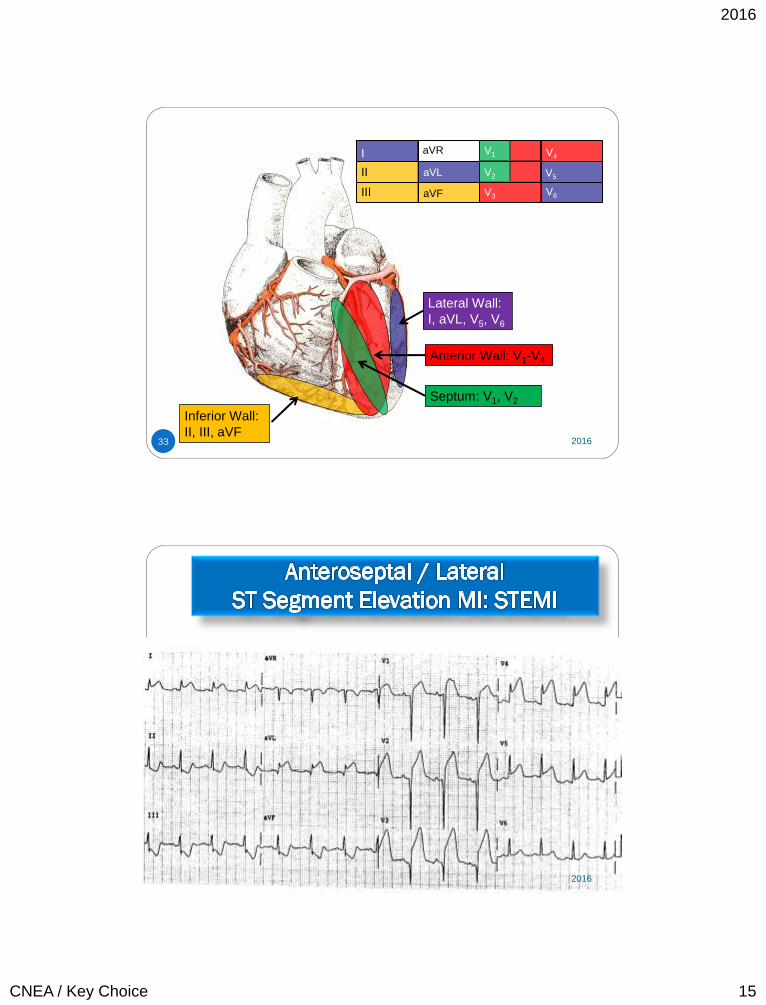
I
II
III
aVR
aVL
aVF
V1
V2
V3
V4
V5
V6
Inferior Wall:
II, III, aVF
Lateral Wall:
I, aVL, V5, V6
Anterior Wall: V1-V4
Septum: V1, V2
33 2016
34 2016
2016
CNEA / Key Choice 16
35 2016
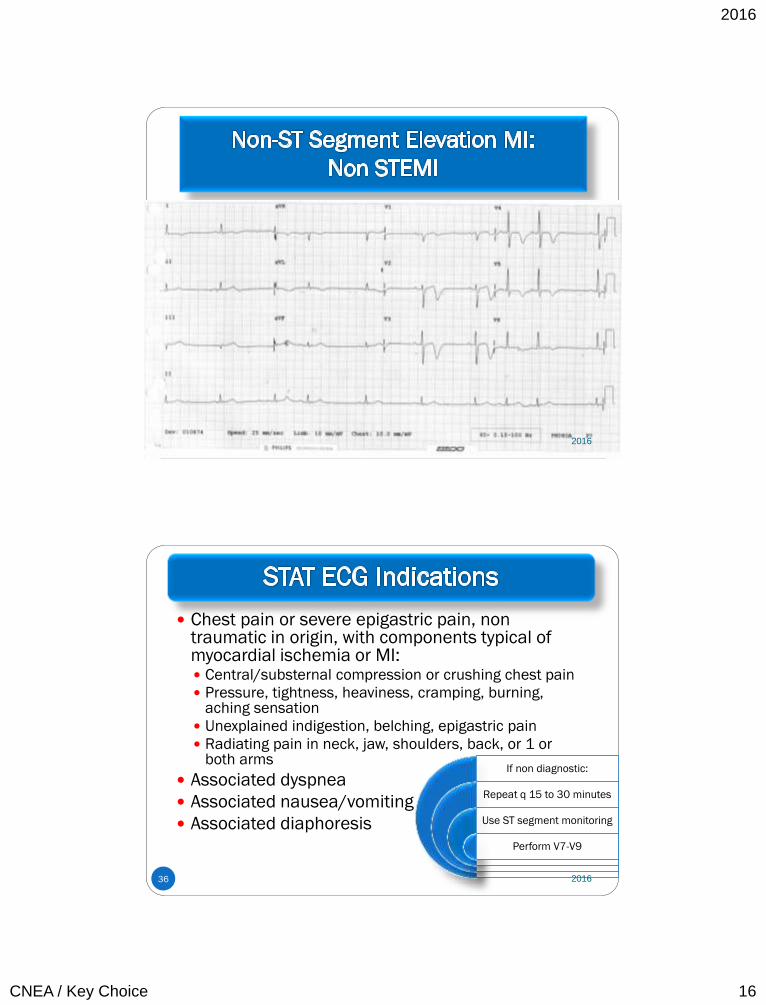
36
Chest pain or severe epigastric pain, non traumatic in origin, with components typical of myocardial ischemia or MI: Central/substernal compression or crushing chest pain
Pressure, tightness, heaviness, cramping, burning, aching sensation
Unexplained indigestion, belching, epigastric pain
Radiating pain in neck, jaw, shoulders, back, or 1 or both arms
Associated dyspnea
Associated nausea/vomiting
Associated diaphoresis
If non diagnostic:
Repeat q 15 to 30 minutes
Use ST segment monitoring
Perform V7-V9
2016
2016
CNEA / Key Choice 17
37 2016
38 2016
2016
CNEA / Key Choice 18
39 2016
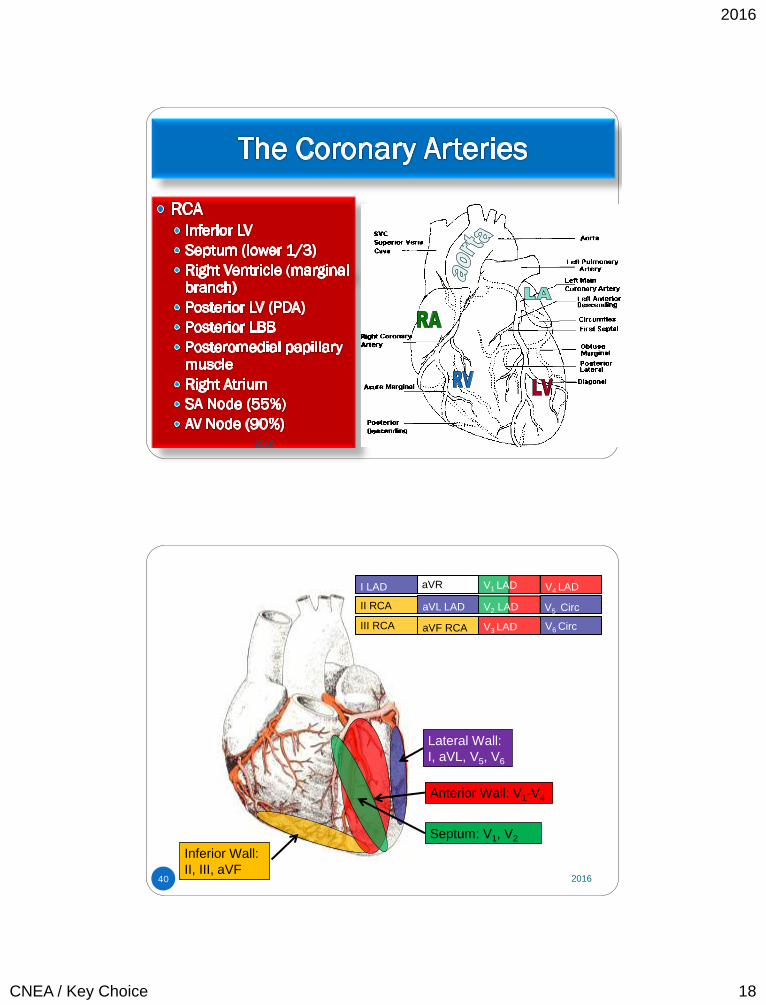
I LAD
II RCA
III RCA
aVR
aVL LAD
aVF RCA
V1 LAD
V2 LAD
V3 LAD
V4 LAD
V5 Circ
V6 Circ
Inferior Wall:
II, III, aVF
Lateral Wall:
I, aVL, V5, V6
Anterior Wall: V1-V4
Septum: V1, V2
40 2016
2016
CNEA / Key Choice 19
Found only in cardiac muscle
Most sensitive indicator of myocardial damage Capable of diagnosing small amounts of myocardial necrosis not
measured by rises in CK-MB levels
Approximately 30% of patients with non-ST elevation and normal CKMB levels will test positive for Non-STEMI
Of equal sensitivity and specificity
Troponin remains elevated for a long period Beneficial for late presentation Challenging for re-infarction
Positive troponin + ECG changes of injury / ischemia or
ACS symptoms = INFARCT 41 2016
Non infarct cardiac causes of elevated troponin: heart failure, left ventricular hypertrophy, tachyarrhythmias, pericarditis, cardiac trauma
Non CAD causes of troponin elevation (sepsis, pulmonary emboli, chronic kidney disease, chemotherapy, respiratory failure, burns, neurological disease )
Troponin I more specific in renal dysfunction Patients with ESRD commonly have elevated troponin T
Not a false positive - relates to overall dysfunction of the cardiorenal system
< 10% of patients with ESRD have elevated troponin I in absence of ACS
Elevated troponin levels are marker of risk and associated with an increased mortality – even when diagnosis is not myocardial infarction
Degree of troponin elevation correlates with risk of death
New high sensitivity troponin T
42 2016
2016
CNEA / Key Choice 20
43
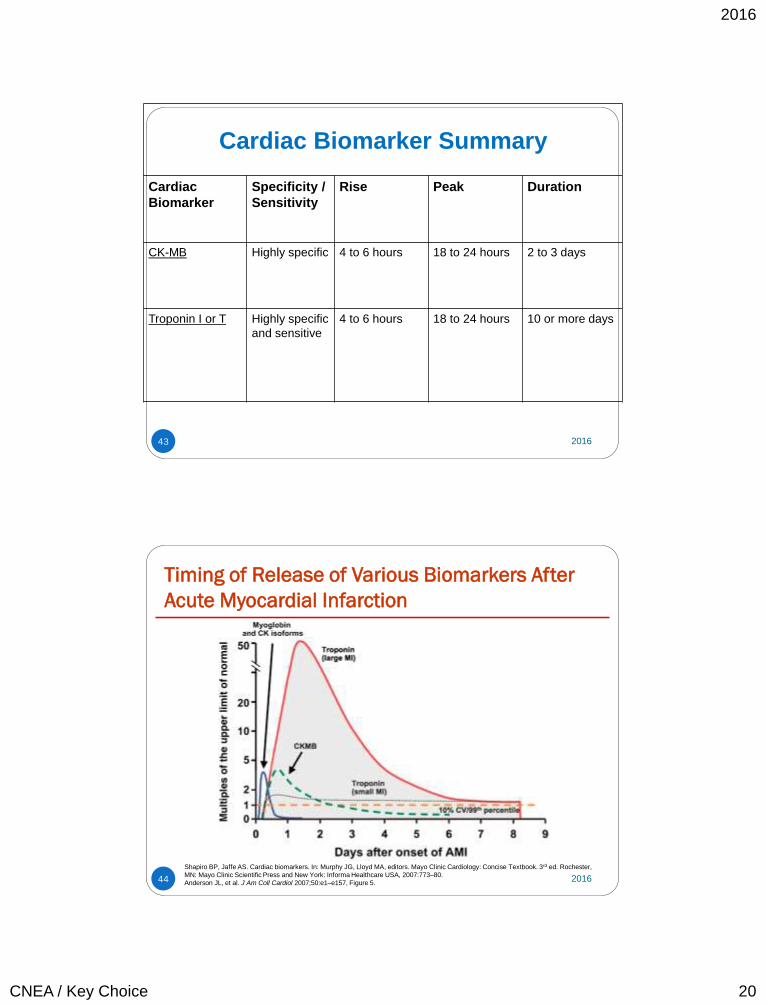
Cardiac Biomarker Summary
Cardiac
Biomarker
Specificity /
Sensitivity
Rise Peak Duration
CK-MB Highly specific 4 to 6 hours 18 to 24 hours 2 to 3 days
Troponin I or T Highly specific
and sensitive
4 to 6 hours 18 to 24 hours 10 or more days
2016
Timing of Release of Various Biomarkers After
Acute Myocardial Infarction
44
Shapiro BP, Jaffe AS. Cardiac biomarkers. In: Murphy JG, Lloyd MA, editors. Mayo Clinic Cardiology: Concise Textbook. 3rd ed. Rochester,
MN: Mayo Clinic Scientific Press and New York: Informa Healthcare USA, 2007:773–80.
Anderson JL, et al. J Am Coll Cardiol 2007;50:e1–e157, Figure 5. 2016
2016
CNEA / Key Choice 21
45
ASA: 325 mg (non enteric coated) If fibrinolytic therapy – 162-325 mg
P2Y12 inhibitor (loading dose before or at time of PCI) If fibrinolytic therapy - clopidogrel only
Anticoagulants (related to reperfusion strategy) If fibrinolytic – weight based heparin x 48 hours
Oral beta blockers ASAP IV if hypertensive or tachycardic
NTG – Sublingual vs IV Morphine Sulfate (Class I) Oxygen if hypoxemic (arterial oxygen saturation < 90%) High intensity statin therapy D/C NSAIDS ACE Inhibitors (within 24 hours)
Greatest benefit in anterior wall MI, LVEF < 40%, HTN, diabetes or chronic kidney disease
Aldosterone Antagonists Initiate within 7 days in those with LVEF <40% , HF , or diabetes
2016
46
It is reasonable to use an insulin-based regimen to achieve and maintain glucose levels less than 180 mg/dL while avoiding hypoglycemia* for patients with STEMI with either a complicated or uncomplicated course.
2016
2016
CNEA / Key Choice 22
47
Reperfusion is number one treatment strategy
Primary Coronary Intervention (PCI) preferred treatment strategy if within 90 minutes Goal: 90 minutes from 1st medical contact
Fibrinolytics within 30 minutes of hospital presentation (or 30 minutes from EMS to
fibrinolytics)
2016
48
The Winner!
2016
2016
CNEA / Key Choice 23
Interventional Revascularization: PCI (Primary Coronary Intervention (in STEMI) or
Percutaneous Coronary Intervention)
PTCA: Percutaneous transluminal coronary
angioplasty
Coronary Stent
BMS: Bare metal
DES: Drug eluting
Coronary Extraction Atherectomy
49 2016
50 2016
2016
CNEA / Key Choice 24
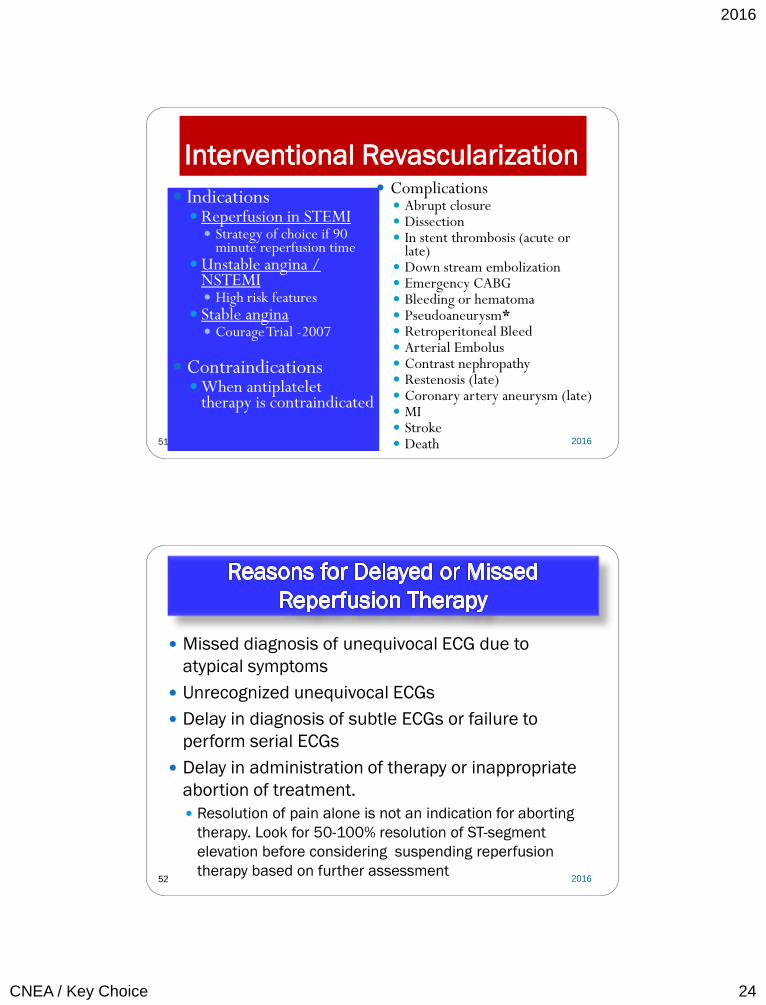
Interventional Revascularization
Indications Reperfusion in STEMI
Strategy of choice if 90 minute reperfusion time
Unstable angina / NSTEMI High risk features
Stable angina Courage Trial -2007
Contraindications When antiplatelet
therapy is contraindicated
Complications Abrupt closure Dissection In stent thrombosis (acute or
late) Down stream embolization Emergency CABG Bleeding or hematoma Pseudoaneurysm* Retroperitoneal Bleed Arterial Embolus Contrast nephropathy Restenosis (late) Coronary artery aneurysm (late) MI Stroke Death
51 2016
52
Missed diagnosis of unequivocal ECG due to
atypical symptoms
Unrecognized unequivocal ECGs
Delay in diagnosis of subtle ECGs or failure to
perform serial ECGs
Delay in administration of therapy or inappropriate
abortion of treatment.
Resolution of pain alone is not an indication for aborting
therapy. Look for 50-100% resolution of ST-segment
elevation before considering suspending reperfusion
therapy based on further assessment
2016
2016
CNEA / Key Choice 25
53 2016
54 2016
2016
CNEA / Key Choice 26
55
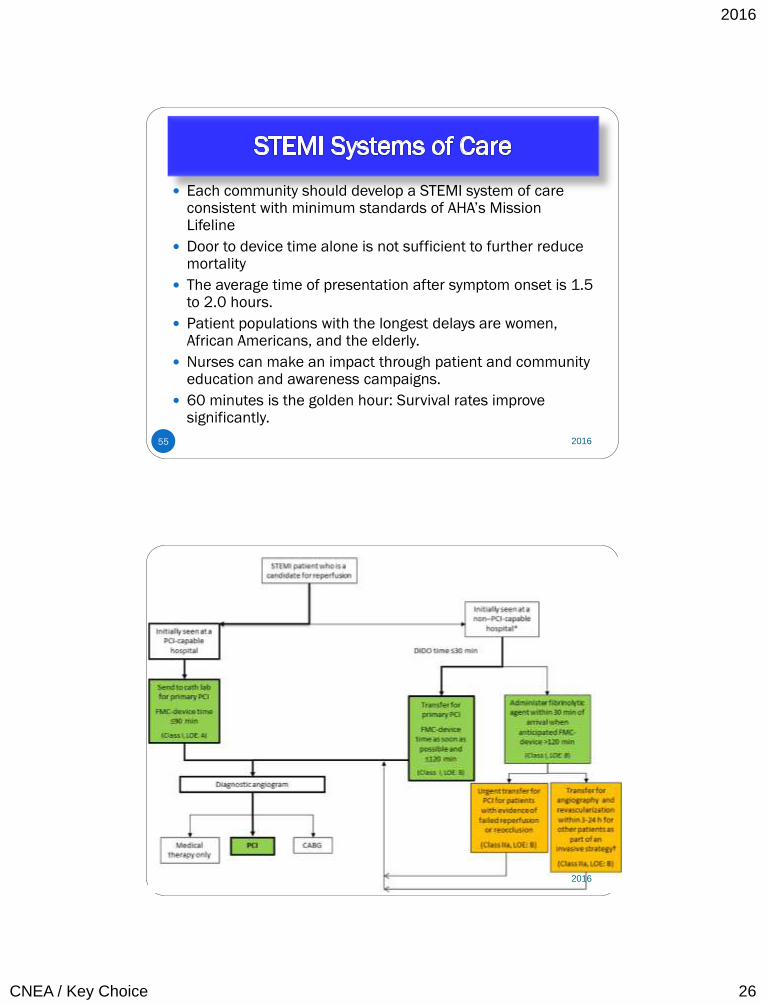
Each community should develop a STEMI system of care consistent with minimum standards of AHA’s Mission Lifeline
Door to device time alone is not sufficient to further reduce mortality
The average time of presentation after symptom onset is 1.5 to 2.0 hours.
Patient populations with the longest delays are women, African Americans, and the elderly.
Nurses can make an impact through patient and community education and awareness campaigns.
60 minutes is the golden hour: Survival rates improve significantly.
2016
56 2016
2016
CNEA / Key Choice 27
Dual antiplatelet Anticoagulation Oxygen if SpO2< 90% NTG
IV in first 48 hours for persistent ischemia, HTN, HF Should not interfere with mortality reducing beta blockers or ace
inhibitors
MS (if NTG unsuccessful and other anti ischemic drugs on board )
Beta Blockers (within 24 hours) Start PO when hemodynamically stable May use IV if hypertensive
ACE Inhibitors (within 24 hours) In select patients – pulmonary congestion or LVEF < 40%) – may also
be used in other patients
High intensity statin
DC – NSAIDS
Medical Supportive Therapy:
Similar to STEMI
57 2016
58
Attacking Platelet is number one treatment strategy
Two antiplatelets agents are indicated
There are 3 types of antiplatelet agents
Aspirin
P2Y12 Receptor Antagonists
Intravenous GP IIb/IIIa Inhibitors
2016
2016
CNEA / Key Choice 28
59
Dual antiplatelet therapy for invasive strategies in medium to high risk patients ASA (and one of following) P2Y12 / ADP Receptor
blockers Clopidogrel Prasugral Ticagrelor * preferred over
clopidogrel
GP II b / III a Inhibitors
(*eptifibatide, * tirofiban, abciximab) * preferred agents Used only in special
circumstances
Antiplatelet therapy also in conservative treatment Prasugrel not unless
PCI is planned Abciximab not unless
PCI is planned
Dual antiplatelet
therapy is also
used after STEMI
and after any
coronary
intervention. 2016
60
Stent
Restenosis
Compared to
Stent Thrombosis
60 2016
2016
CNEA / Key Choice 29
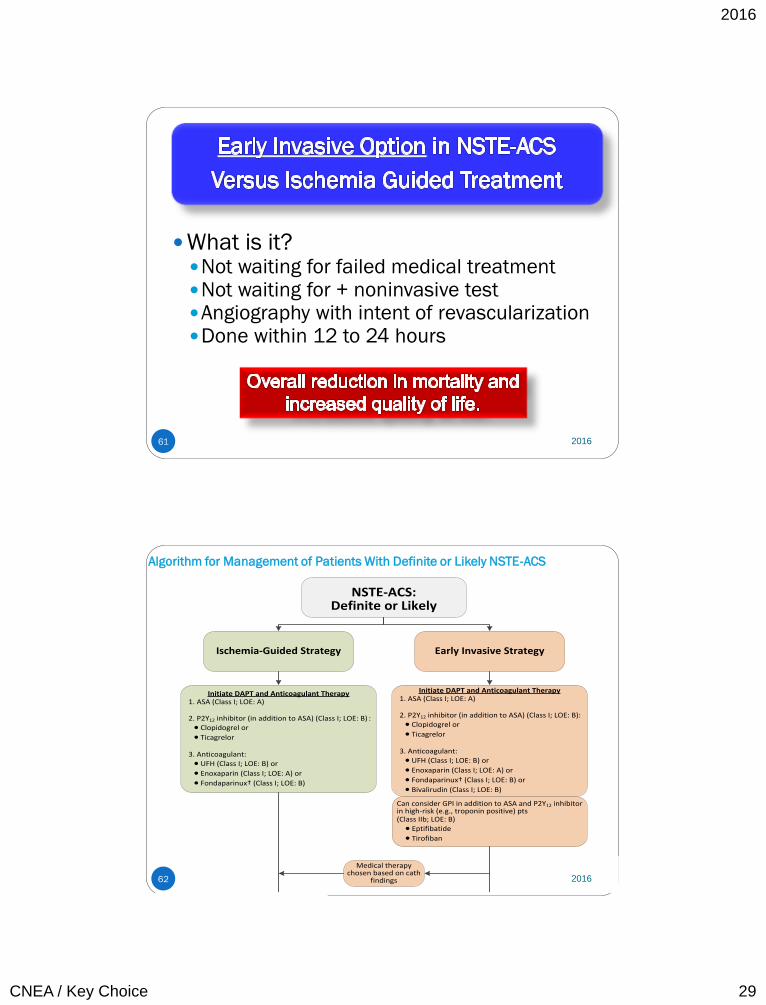
61
What is it? Not waiting for failed medical treatment Not waiting for + noninvasive test Angiography with intent of revascularization Done within 12 to 24 hours
2016
Algorithm for Management of Patients With Definite or Likely NSTE-ACS
NSTE-ACS: Definite or Likely
Ischemia-Guided Strategy Early Invasive Strategy
Initiate DAPT and Anticoagulant Therapy1. ASA (Class I; LOE: A)
2. P2Y12 inhibitor (in addition to ASA) (Class I; LOE: B) :· Clopidogrel or
· Ticagrelor
3. Anticoagulant:· UFH (Class I; LOE: B) or
· Enoxaparin (Class I; LOE: A) or
· Fondaparinux† (Class I; LOE: B)
Initiate DAPT and Anticoagulant Therapy1. ASA (Class I; LOE: A)
2. P2Y12 inhibitor (in addition to ASA) (Class I; LOE: B):· Clopidogrel or
· Ticagrelor
3. Anticoagulant:· UFH (Class I; LOE: B) or
· Enoxaparin (Class I; LOE: A) or
· Fondaparinux† (Class I; LOE: B) or
· Bivalirudin (Class I; LOE: B)
Medical therapy chosen based on cath
findings
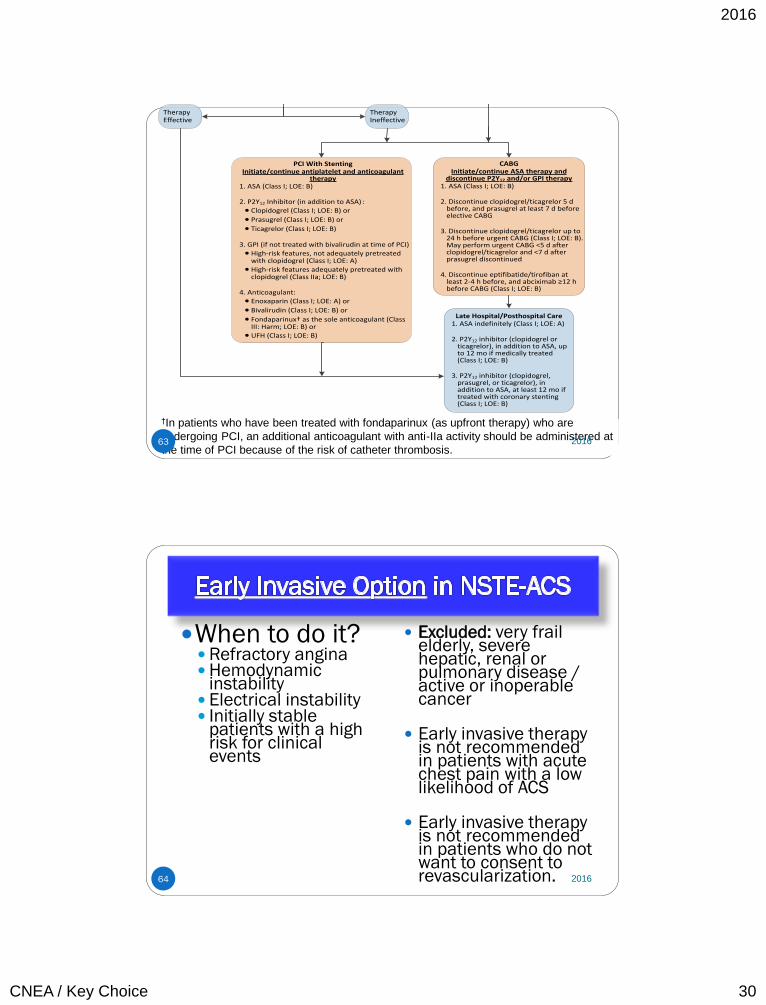
PCI With StentingInitiate/continue antiplatelet and anticoagulant
therapy1. ASA (Class I; LOE: B)
2. P2Y12 Inhibitor (in addition to ASA) :· Clopidogrel (Class I; LOE: B) or
· Prasugrel (Class I; LOE: B) or
· Ticagrelor (Class I; LOE: B)
3. GPI (if not treated with bivalirudin at time of PCI)· High-risk features, not adequately pretreated
with clopidogrel (Class I; LOE: A)· High-risk features adequately pretreated with
clopidogrel (Class IIa; LOE: B)
4. Anticoagulant:· Enoxaparin (Class I; LOE: A) or
· Bivalirudin (Class I; LOE: B) or
· Fondaparinux† as the sole anticoagulant (Class III: Harm; LOE: B) or
· UFH (Class I; LOE: B)
CABGInitiate/continue ASA therapy and
discontinue P2Y12 and/or GPI therapy1. ASA (Class I; LOE: B)
2. Discontinue clopidogrel/ticagrelor 5 d before, and prasugrel at least 7 d before elective CABG
3. Discontinue clopidogrel/ticagrelor up to 24 h before urgent CABG (Class I; LOE: B). May perform urgent CABG <5 d after clopidogrel/ticagrelor and <7 d after prasugrel discontinued
4. Discontinue eptifibatide/tirofiban at least 2-4 h before, and abciximab ≥12 h before CABG (Class I; LOE: B)
Late Hospital/Posthospital Care1. ASA indefinitely (Class I; LOE: A)
2. P2Y12 inhibitor (clopidogrel or ticagrelor), in addition to ASA, up to 12 mo if medically treated (Class I; LOE: B)
3. P2Y12 inhibitor (clopidogrel, prasugrel, or ticagrelor), in addition to ASA, at least 12 mo if treated with coronary stenting (Class I; LOE: B)
Can consider GPI in addition to ASA and P2Y12 inhibitor in high-risk (e.g., troponin positive) pts (Class IIb; LOE: B)
· Eptifibatide
· Tirofiban
TherapyIneffective
TherapyEffective
62 2016
2016
CNEA / Key Choice 30
NSTE-ACS: Definite or Likely
Ischemia-Guided Strategy Early Invasive Strategy
Initiate DAPT and Anticoagulant Therapy1. ASA (Class I; LOE: A)
2. P2Y12 inhibitor (in addition to ASA) (Class I; LOE: B) :
· Clopidogrel or
· Ticagrelor
3. Anticoagulant:
· UFH (Class I; LOE: B) or
· Enoxaparin (Class I; LOE: A) or
· Fondaparinux (Class I; LOE: B)
Initiate DAPT and Anticoagulant Therapy1. ASA (Class I; LOE: A)
2. P2Y12 inhibitor (in addition to ASA) (Class I; LOE: B):
· Clopidogrel or
· Ticagrelor
3. Anticoagulant:
· UFH (Class I; LOE: B) or
· Enoxaparin (Class I; LOE: A) or
· Fondaparinux† (Class I; LOE: B) or
· Bivalirudin (Class I; LOE: B)
Medical therapy chosen based on cath
findings
PCI With StentingInitiate/continue antiplatelet and anticoagulant
therapy1. ASA (Class I; LOE: B)
2. P2Y12 Inhibitor (in addition to ASA) :
· Clopidogrel (Class I; LOE: B) or
· Prasugrel (Class I; LOE: B) or
· Ticagrelor (Class I; LOE: B)
3. GPI (if not treated with bivalirudin at time of PCI)
· High-risk features, not adequately pretreated with clopidogrel (Class I; LOE: A)
· High-risk features adequately pretreated with clopidogrel (Class IIa; LOE: B)
4. Anticoagulant:
· Enoxaparin (Class I; LOE: A) or
· Bivalirudin (Class I; LOE: B) or
· Fondaparinux† as the sole anticoagulant (Class III: Harm; LOE: B) or
· UFH (Class I; LOE: B)
CABGInitiate/continue ASA therapy and
discontinue P2Y12 and/or GPI therapy1. ASA (Class I; LOE: B)
2. Discontinue clopidogrel/ticagrelor 5 d before, and prasugrel at least 7 d before elective CABG
3. Discontinue clopidogrel/ticagrelor up to 24 h before urgent CABG (Class I; LOE: B). May perform urgent CABG <5 d after clopidogrel/ticagrelor and <7 d after prasugrel discontinued
4. Discontinue eptifibatide/tirofiban at least 2-4 h before, and abciximab ≥12 h before CABG (Class I; LOE: B)
Late Hospital/Posthospital Care1. ASA indefinitely (Class I; LOE: A)
2. P2Y12 inhibitor (clopidogrel or ticagrelor), in addition to ASA, up to 12 mo if medically treated (Class I; LOE: B)
3. P2Y12 inhibitor (clopidogrel, prasugrel, or ticagrelor), in addition to ASA, at least 12 mo if treated with coronary stenting (Class I; LOE: B)
Can consider GPI in addition to ASA and P2Y12 inhibitor in high-risk (e.g., troponin positive) pts (Class IIb; LOE: B)
· Eptifibatide
· Tirofiban
TherapyIneffective
TherapyEffective
†In patients who have been treated with fondaparinux (as upfront therapy) who are
undergoing PCI, an additional anticoagulant with anti-IIa activity should be administered at
the time of PCI because of the risk of catheter thrombosis. 63 2016
64
When to do it? Refractory angina Hemodynamic
instability Electrical instability Initially stable
patients with a high risk for clinical events
Excluded: very frail elderly, severe hepatic, renal or pulmonary disease / active or inoperable cancer
Early invasive therapy is not recommended in patients with acute chest pain with a low likelihood of ACS
Early invasive therapy
is not recommended in patients who do not want to consent to revascularization.
2016
2016
CNEA / Key Choice 31
65
Recurrent angina / ischemia Rest or low level activity with medical treatment
Troponin +
New or presumed new ST depression
S&S HF or worsening mitral regurgitation
High risk findings on noninvasive testing EF < 35%, large anterior perfusion defect, multiple perfusion defects)
Hemodynamic instability
Sustained VT
PCI within 6 months
Prior CABG
Reduced LV Function
High risk TIMI or GRACE Score
2016
66
TIMI Risk Score Age > 65
3 or > risk factors for CAD
Prior 50% or > stenosis
ST deviation on ECG
2 or > anginal events in previous 24 hours
Use of ASA in prior 7 days
Elevated cardiac biomarkers
GRACE
Older age
Killip class
Systolic BP
Cardiac arrest during presentation
Serum creatinine
Positive initial cardiac markers
HR
2016
2016
CNEA / Key Choice 32
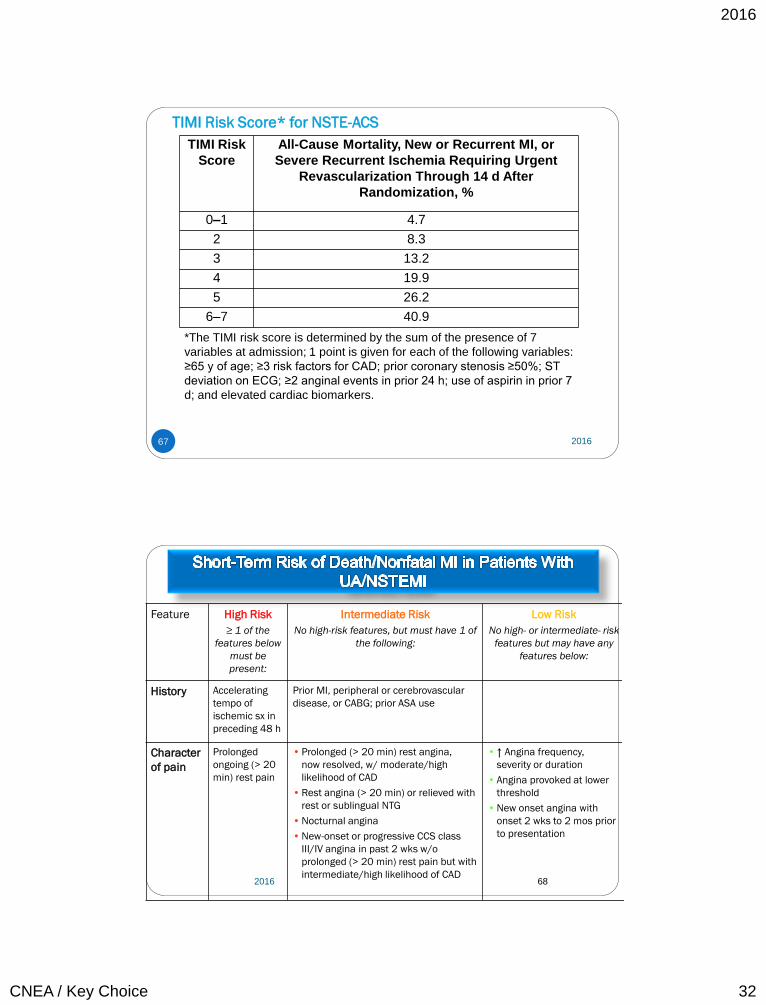
TIMI Risk Score* for NSTE-ACS
TIMI Risk
Score
All-Cause Mortality, New or Recurrent MI, or
Severe Recurrent Ischemia Requiring Urgent
Revascularization Through 14 d After
Randomization, %
0–1 4.7
2 8.3
3 13.2
4 19.9
5 26.2
6–7 40.9
*The TIMI risk score is determined by the sum of the presence of 7
variables at admission; 1 point is given for each of the following variables:
≥65 y of age; ≥3 risk factors for CAD; prior coronary stenosis ≥50%; ST
deviation on ECG; ≥2 anginal events in prior 24 h; use of aspirin in prior 7
d; and elevated cardiac biomarkers.
67 2016
68
Feature High Risk
≥ 1 of the
features below
must be
present:
Intermediate Risk
No high-risk features, but must have 1 of
the following:
Low Risk
No high- or intermediate- risk
features but may have any
features below:
History Accelerating
tempo of
ischemic sx in
preceding 48 h
Prior MI, peripheral or cerebrovascular
disease, or CABG; prior ASA use
Character
of pain
Prolonged
ongoing (> 20
min) rest pain
• Prolonged (> 20 min) rest angina,
now resolved, w/ moderate/high
likelihood of CAD
• Rest angina (> 20 min) or relieved with
rest or sublingual NTG
• Nocturnal angina
• New-onset or progressive CCS class
III/IV angina in past 2 wks w/o
prolonged (> 20 min) rest pain but with
intermediate/high likelihood of CAD
• ↑ Angina frequency,
severity or duration
• Angina provoked at lower
threshold
• New onset angina with
onset 2 wks to 2 mos prior
to presentation
2016
2016
CNEA / Key Choice 33
69
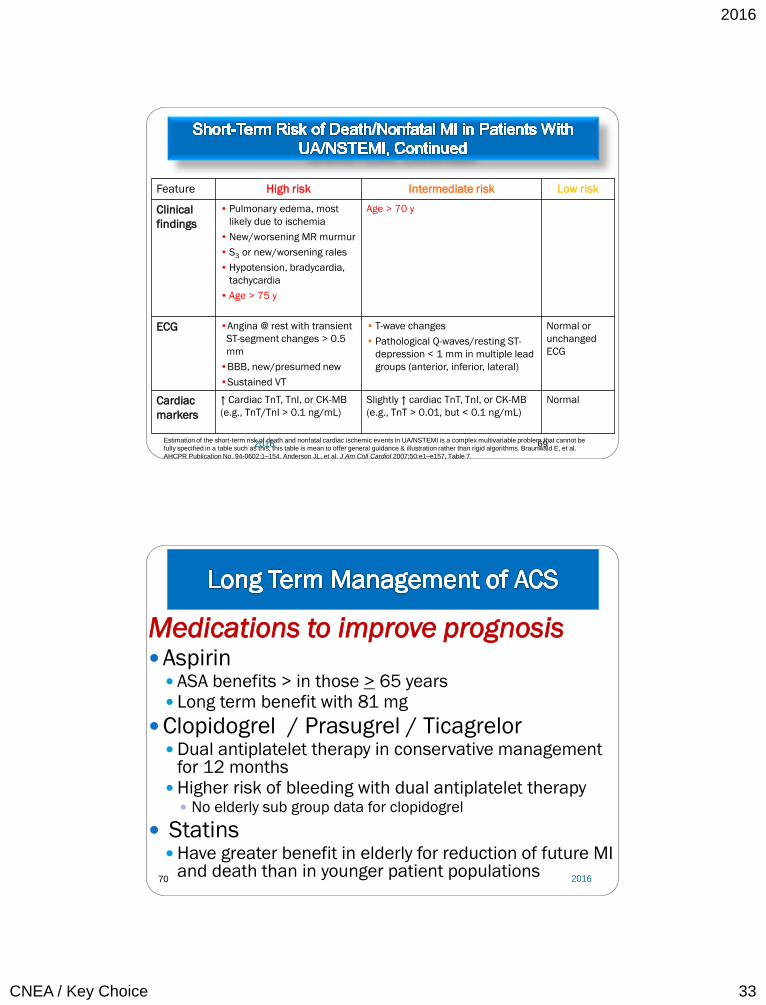
Feature High risk Intermediate risk Low risk
Clinical
findings
• Pulmonary edema, most
likely due to ischemia
• New/worsening MR murmur
• S3 or new/worsening rales
• Hypotension, bradycardia,
tachycardia
• Age > 75 y
Age > 70 y
ECG •Angina @ rest with transient
ST-segment changes > 0.5
mm
•BBB, new/presumed new
•Sustained VT
• T-wave changes
• Pathological Q-waves/resting ST-
depression < 1 mm in multiple lead
groups (anterior, inferior, lateral)
Normal or
unchanged
ECG
Cardiac
markers
↑ Cardiac TnT, TnI, or CK-MB
(e.g., TnT/TnI > 0.1 ng/mL)
Slightly ↑ cardiac TnT, TnI, or CK-MB
(e.g., TnT > 0.01, but < 0.1 ng/mL)
Normal
Estimation of the short-term risk of death and nonfatal cardiac ischemic events in UA/NSTEMI is a complex multivariable problem that cannot be
fully specified in a table such as this; this table is mean to offer general guidance & illustration rather than rigid algorithms. Braunwald E, et al.
AHCPR Publication No. 94-0602:1–154. Anderson JL, et al. J Am Coll Cardiol 2007;50:e1–e157, Table 7.
2016
70
Medications to improve prognosis Aspirin
ASA benefits > in those > 65 years Long term benefit with 81 mg
Clopidogrel / Prasugrel / Ticagrelor Dual antiplatelet therapy in conservative management
for 12 months Higher risk of bleeding with dual antiplatelet therapy
No elderly sub group data for clopidogrel
Statins Have greater benefit in elderly for reduction of future MI
and death than in younger patient populations
2016
2016
CNEA / Key Choice 34
71
Medications to improve prognosis Beta-blockers ACE inhibitors Definite in select patients / reasonable in
all ARBs if ACE-I intolerant
Aldosterone antagonists EF < 40 with HF or diabetes
2016
SL NTG Instruction
72
No more than 1 dose of SL NTG If chest discomfort is unimproved or is
worsening 5 min after 1 NTG call 9-1-1
immediately before taking additional NTG.
May take additional NTG while waiting EMS.
Chew ASA while waiting EMS.
In chronic stable angina if symptoms are significantly
improved by 1 dose of NTG may repeat NTG every 5
min for a maximum of 3 doses and call 9-1-1 if
symptoms have not resolved completely.
2016
2016
CNEA / Key Choice 35
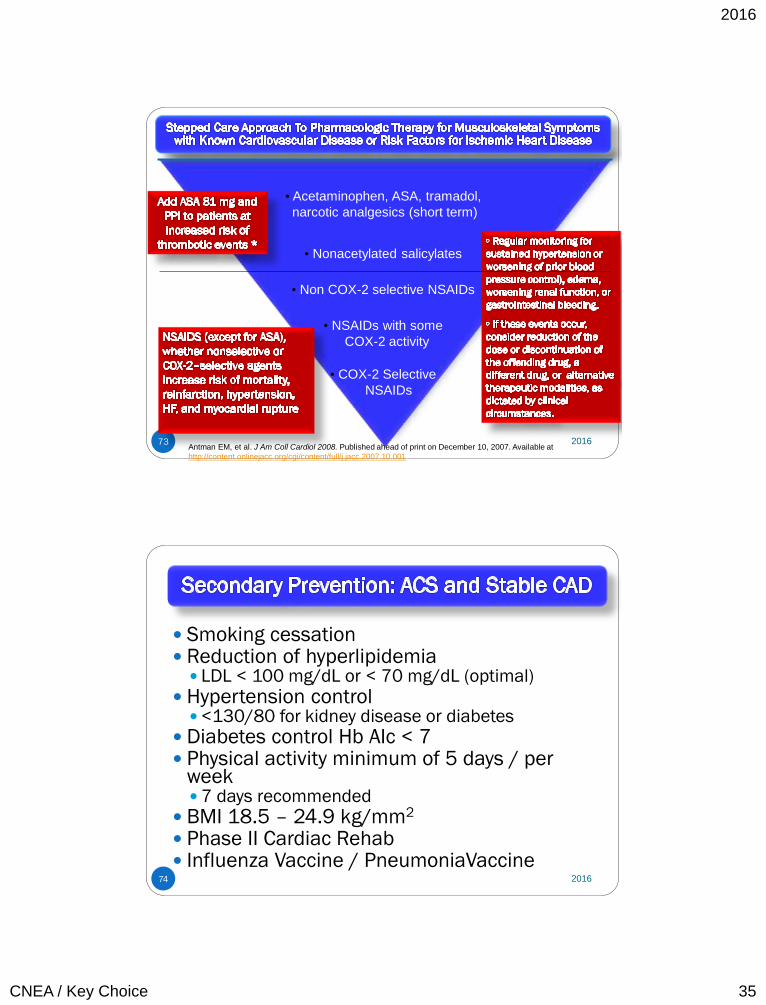
73
• Acetaminophen, ASA, tramadol,
narcotic analgesics (short term)
• COX-2 Selective
NSAIDs
• Nonacetylated salicylates
• Non COX-2 selective NSAIDs
• NSAIDs with some
COX-2 activity
Select patients at low risk
of thrombotic events
Prescribe lowest dose
required to control symptoms
* Addition of ASA may not be sufficient protection
Antman EM, et al. J Am Coll Cardiol 2008. Published ahead of print on December 10, 2007. Available at
http://content.onlinejacc.org/cgi/content/full/j.jacc.2007.10.001.
2016
74
Smoking cessation Reduction of hyperlipidemia
LDL < 100 mg/dL or < 70 mg/dL (optimal)
Hypertension control <130/80 for kidney disease or diabetes
Diabetes control Hb AIc < 7 Physical activity minimum of 5 days / per
week 7 days recommended
BMI 18.5 – 24.9 kg/mm2
Phase II Cardiac Rehab Influenza Vaccine / PneumoniaVaccine
2016
2016
CNEA / Key Choice 36
75
Use oxygen for hypoxemia
Assess response to beta-blocker therapy. HR / BP
Arrhythmia control
Assess for complications related to specific type of MI Assess heart sounds for new holosystolic murmurs
Risk for myocardial rupture
Observe for signs of left ventricular dysfunction, including hypotension or clinical signs of heart failure.
Monitor ECG for conduction disturbances and arrhythmias
Assess for presence of RV infarct 2016
76
Management of arterial access site
Assessment for contrast nephropathy
Restrict activity for the first 12 hours, and then begin Phase I Cardiac Rehabilitation (progressive mobility)
Referral to Phase II Cardiac Rehabilitation
Utilize cardiac monitoring ST-segment monitoring
Uninterrupted monitoring for first 24-48 hours
Address addiction to nicotine Consideration for nicotine withdrawal
Focus on holistic approach to anxiety reduction Include the family. Family visits do not have a negative
impact on vital signs or cardiac rhythm 2016
2016
CNEA / Key Choice 37
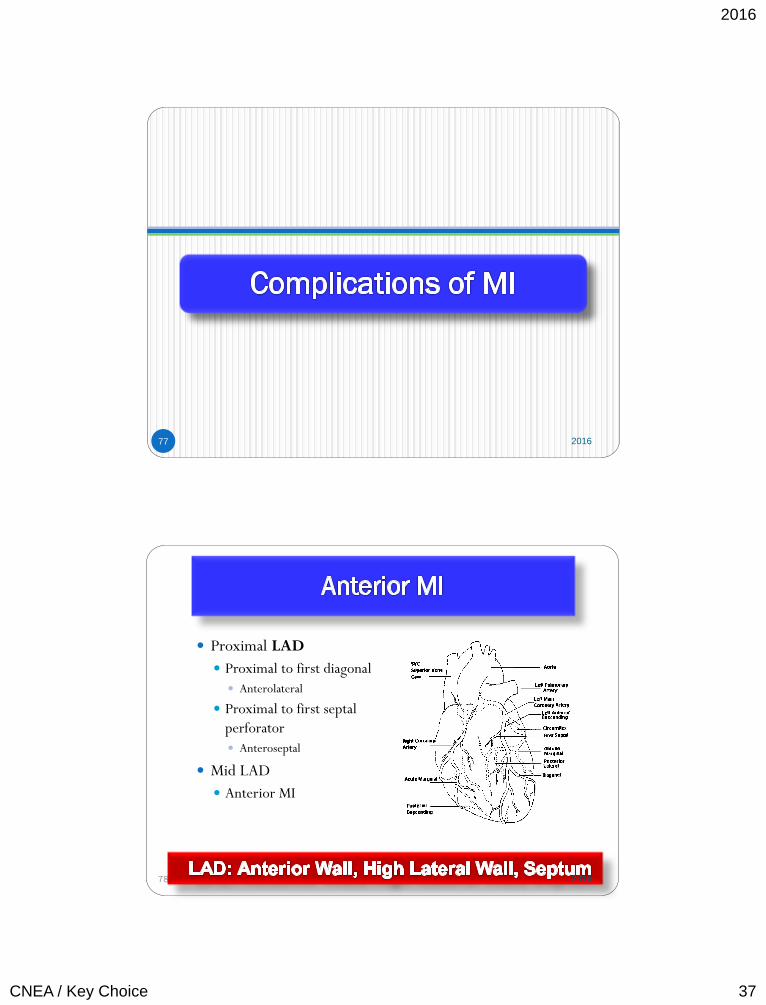
77 2016
Proximal LAD
Proximal to first diagonal
Anterolateral
Proximal to first septal
perforator
Anteroseptal
Mid LAD
Anterior MI
78
2016
2016
CNEA / Key Choice 38
Myocardium at risk
Mortality and morbidity
Post Infarction ejection fraction
79 2016
Tachycardia Sinus tachycardia
Atrial tachycardia
Ventricular tachycardia
Right BBB and left anterior hemiblock
Complete heart block
Ventricular septal defect New loud systolic
murmur
Cardiogenic shock
Long term ventricular modeling and heart failure
80 2016
2016
CNEA / Key Choice 39
RCA occlusion 80% to 85% of time
Marginal branch: Right ventricle
Posterior descending artery = Posterior wall of
LV
Concept of right versus left dominant
81 2016
82 2016
2016
CNEA / Key Choice 40
83
Cellular edema produces an inflammatory response.
Recruitment of some stem cells leads to some tissue
regeneration.
Damaged tissue is bruised and cyanotic.
Catecholamines are released from myocardial cells, thus
increasing the risk of arrhythmias.
Cardiac biomarkers are released.
White blood cells invade the necrotic tissue within 2 to 3 days.
Scavenger cells release enzymes to break down necrotic tissue.
The necrotic wall can become very thin during this phase, and
the patient is at risk for cardiac rupture.
2016
84
A weak collagen matrix forms by second week, myocardium is still vulnerable to
re-injury.
Scar formation has started by third week.
Necrotic area is completely replaced with scar tissue by week 6. Scar tissue does
not contribute to the contractile function of the myocardium.
Myocardial necrosis (transmural and non transmural) and stunned or hibernating
viable myocardium adversely affect the synergy of left ventricular contraction.
Surviving myocytes hypertrophy in an attempt to compensate for damaged
tissue.
Excessive non-contractile collagen is present in the newly hypertrophied
myocardium, leading to a ventricle that is stiff and noncompliant.
Regional wall motion dysfunction may improve due to recovery of post-ischemic
viable myocardium. Does not necessarily correlate with an improvement in
overall left ventricular ejection fraction.
Non-uniform left ventricular dilatation occurs. Occurs even in patients with
recovery of regional wall motion abnormalities. 2016
2016
CNEA / Key Choice 41
85 2016
86 2016
2016
CNEA / Key Choice 42
87
Cold extremities
Cyanosis
Oligurua
Decreased mentation
Large LV infarction (>
40% myocardium)
Right ventricular infarct
Mechanical
complication
Heart Failure:
• Cause: Ischemic, stunned, hibernating, or injured
myocardium.
• HF after a STEMI is a predictor of mortality.
• Functional mitral valve regurgitation can co-exist.
2016
88
V-fib preventable cause of
death
90% of sustained
arrhythmias occur in first
48 hours
Higher mortality than
arrhythmias early in course
ICD consultation if no
reversible cause
2016
2016
CNEA / Key Choice 43
89 2016
90 2016
2016
CNEA / Key Choice 44
91 2016
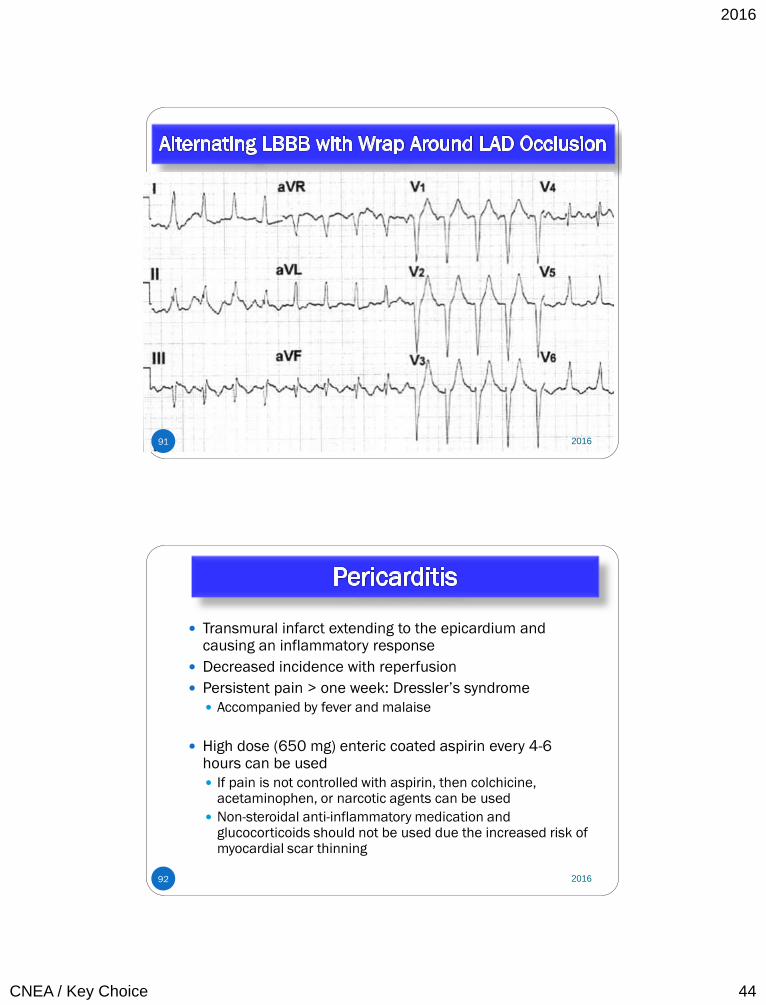
92
Transmural infarct extending to the epicardium and causing an inflammatory response
Decreased incidence with reperfusion
Persistent pain > one week: Dressler’s syndrome
Accompanied by fever and malaise
High dose (650 mg) enteric coated aspirin every 4-6 hours can be used
If pain is not controlled with aspirin, then colchicine, acetaminophen, or narcotic agents can be used
Non-steroidal anti-inflammatory medication and glucocorticoids should not be used due the increased risk of myocardial scar thinning
2016
2016
CNEA / Key Choice 45
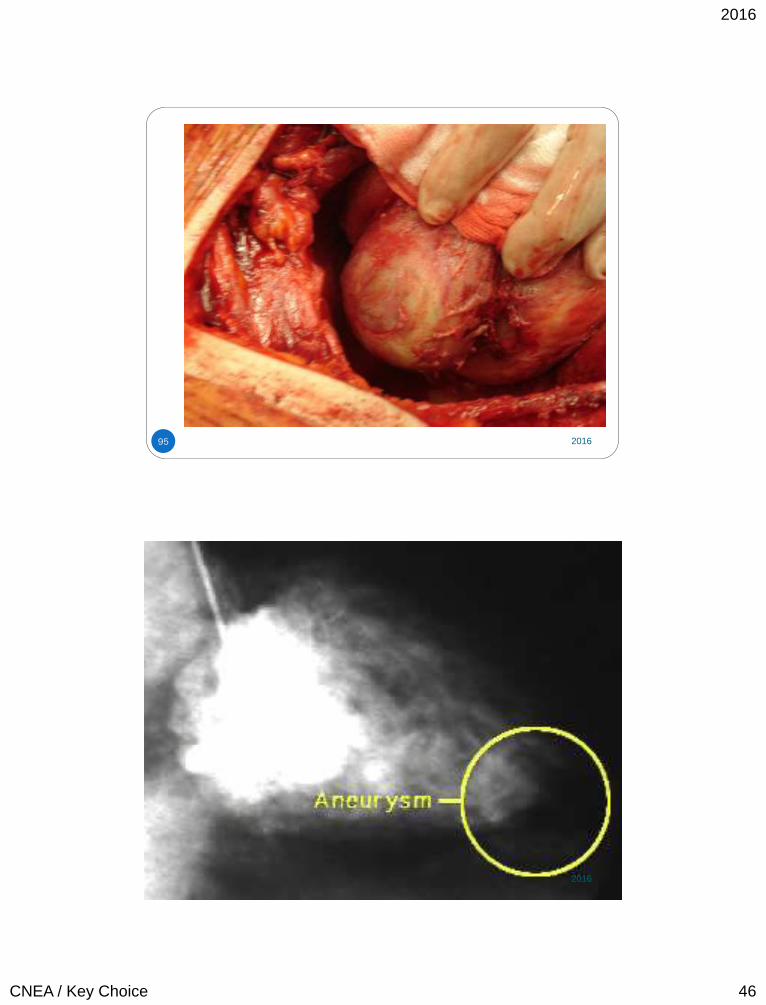
93
Occurs in approximately 5% of STEMI patients
If no reperfusion, the incidence of ventricular aneurysm is as high as 10% to 30%
More common with transmural anterior wall MI patients
Localized myocardial wall thinning and bulging of the left ventricle at the site of infarction
Stretched portion of the myocardium contains three layers and is connected to a ventricle by a wide neck
Expands during systole during the acute phase and thus contributes to mechanical dysfunction of the left ventricle Can contain thrombus
Site of junction can be source of ventricular arrhythmias
2016
94
Persistent ST elevation after AMI (anterior) often indicates true aneurysm
Often accompanied by deep QS waves and T wave inversion
Persistent ST elevation may be associated with systolic dyskinesis, akinesis, or a large area of necrosis, even in the absence of anatomic aneurysm
Considered chronic if
persist for > 6 weeks
ACE inhibitors can reduce
true aneurysm
development
NSAIDs can increase
development of aneurysms
Left-ventricular
aneurysmectomy
Heart failure
Ventricular arrhythmias
Thrombus on
anticoagulation 2016
2016
CNEA / Key Choice 47
97
Cardiac tamponade from
free wall rupture
Formation of left
ventricular diverticulum or
pseudoaneurysm from
free wall rupture
Left to right shunt from
septal rupture
Acute mitral regurgitation
from papillary muscle
rupture.
10% of MIs
15% of in hospital deaths
after MI
Without surgical
intervention, the mortality
rate for rupture is > 80%
at two weeks.
Two high risk periods
1st 24 hours
Within 1st week ( 3 to 5 days)
Associated with delayed
fibrinolytics and late
presentation Examples in next class! 2016
Post DISCHARGE AFTER MI
98 2016
2016
CNEA / Key Choice 48
After the patient achieves a rehabilitation level equivalent with
activities of daily living, he/she can begin a walking program
3 to 4 METS
Should be by time of discharge
Begin walking 5 to 10 minutes at a time
Patients should rate activity as moderate
Shortness of breath means overexertion. Other signs of
activity intolerance include: angina, dizziness, diaphoresis,
prolonged fatigue, and nausea.
The use of force to open windows or tight jar lids should be
avoided in patients with lifting restrictions.
99 2016
100 2016
2016
CNEA / Key Choice 49
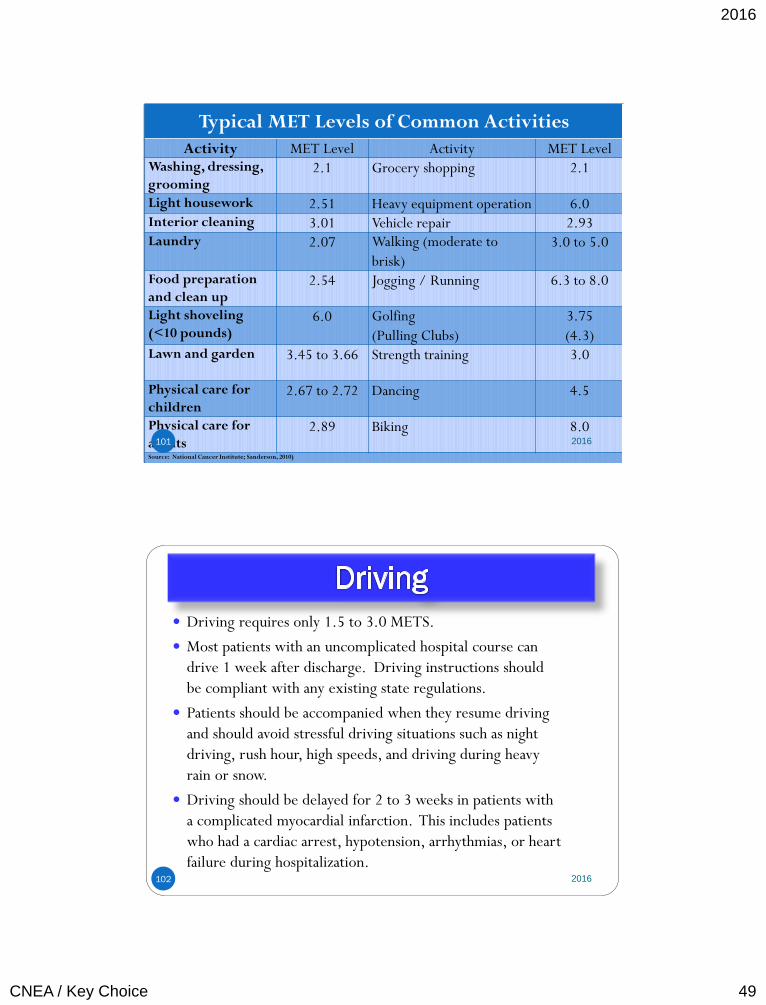
Typical MET Levels of Common Activities
Activity MET Level Activity MET Level Washing, dressing,
grooming 2.1 Grocery shopping 2.1
Light housework 2.51 Heavy equipment operation 6.0 Interior cleaning 3.01 Vehicle repair 2.93 Laundry 2.07 Walking (moderate to
brisk)
3.0 to 5.0
Food preparation
and clean up 2.54 Jogging / Running 6.3 to 8.0
Light shoveling
(<10 pounds) 6.0 Golfing
(Pulling Clubs)
3.75
(4.3) Lawn and garden 3.45 to 3.66 Strength training 3.0
Physical care for
children 2.67 to 2.72 Dancing 4.5
Physical care for
adults 2.89 Biking 8.0
Source: National Cancer Institute; Sanderson, 2010)
101 2016
Driving requires only 1.5 to 3.0 METS.
Most patients with an uncomplicated hospital course can
drive 1 week after discharge. Driving instructions should
be compliant with any existing state regulations.
Patients should be accompanied when they resume driving
and should avoid stressful driving situations such as night
driving, rush hour, high speeds, and driving during heavy
rain or snow.
Driving should be delayed for 2 to 3 weeks in patients with
a complicated myocardial infarction. This includes patients
who had a cardiac arrest, hypotension, arrhythmias, or heart
failure during hospitalization.
102 2016
2016
CNEA / Key Choice 50
Travel Patients can usually travel by air within 2 weeks if accompanied
by a travel companion, and if the patient has sublingual
nitroglycerin
If free of all angina symptoms and complications of their myocardial
infarction
Patients should also have airport transportation assistance to avoid
excessive stress and rushing in the airport
Patients should also take precautions when traveling to avoid the
development of deep vein thrombosis
103 2016
Sex After an acute coronary syndrome, stable patients can resume sexual
activity with their usual partner in one week to 10 days (Anderson et al., 2011).
Patients are uncomfortable asking about resuming sexual relationships, so instructions regarding sexual activity should be included as a routine part of all discharge instructions.
Patients with a history of angina during sexual relationships may be instructed to take nitroglycerin prior to engaging in sexual activities.
The average intimate session ranges from 2.5-4 METS for most people.
Walking at 2 mph on level ground is 2.5 METS. Mowing the lawn with a power mower or walking at 3.5 mph is 4 METS. Climbing up a flight of stairs is 8 METS.
The biggest risk with sex in the cardiac patient is the possibility of arrhythmias, which is associated with sympathetic activity increased during arousal. Patients with uncontrolled or untreated hypertension need to discuss specific guidelines with their physician (Sotile & Cantor-Cooke, 2003).
104 2016
2016
CNEA / Key Choice 51
Return to Work Low risk myocardial infarction (LVEF > 45%, successful
revascularization with PCI, age < 70 years) can generally return to work after 2 weeks.
Most myocardial infarction adverse events reach a low steady state at 10 weeks. This may guide decision making in some types of employment.
Patients who need to return to physically demanding activities can have an exercise stress test that compares their performance on the stress test to the METs required for the activity. This will provide information about the ability and safety of engaging in activities based on the MET level achieved during exercise stress test.
(Anderson et al., 2011).
105 2016
Cardiac Rehabilitation Goals:
Increase functional capacity
Reduce disability
Improve quality of life
Modify cardiac risk factors
Reduce morbidity and mortality.
Pooled data from a meta-analysis of studies involving the
exercise portion of cardiac rehabilitation show a benefit of
reduced all-cause mortality of approximately 25% when
compared to usual care.
In one study of over 600,000 Medicare patients, mortality
rates were 21% to 34% lower in patients who participated in
cardiac rehabilitation (Suaya, Stason, Ades, Normand, & Shepard, 2009).
106 2016
2016
CNEA / Key Choice 52
Cardiac Rehabilitation
Low-risk patients can implement an exercise prescription at
home or in a community setting. Low-risk patients include
those with absence of ischemia or arrhythmias on a stress test.
High-risk patients should be in medically supervised exercise
programs. They are defined as patients with ischemia or
serious arrhythmias on a stress test.
Under utilization of cardiac rehabilitation.
107 2016
Treating the Whole Patient
Depression
Approximately 1 in 5 patients hospitalized with MI have major depression. There is also evidence that depression continues for several months after discharge (Fihn et al., 2012; Bush et al., 2005).
There is strong evidence that patients who are depressed post MI have a higher rate of mortality from both cardiac and non-cardiac causes (Bush et al., 2005).
Anxiety and Stress
In post MI patients, interventions to reduce stress can reduce recurrent cardiac events by as much as 35-75% (Gibbons et al., 2002).
Social Support
Role Identity 108 2016
2016
CNEA / Key Choice 53
109
Cardiovascular
Assessment in
Emergency Situations
2016
110 2016
2016
CNEA / Key Choice 54
Key Assessment Tools
Integration with Obstructive Shock and Mechanical Emergencies
Pulling it All Together
111 2016
Heart Sounds An essential
assessment tool!
112 2016
2016
CNEA / Key Choice 55
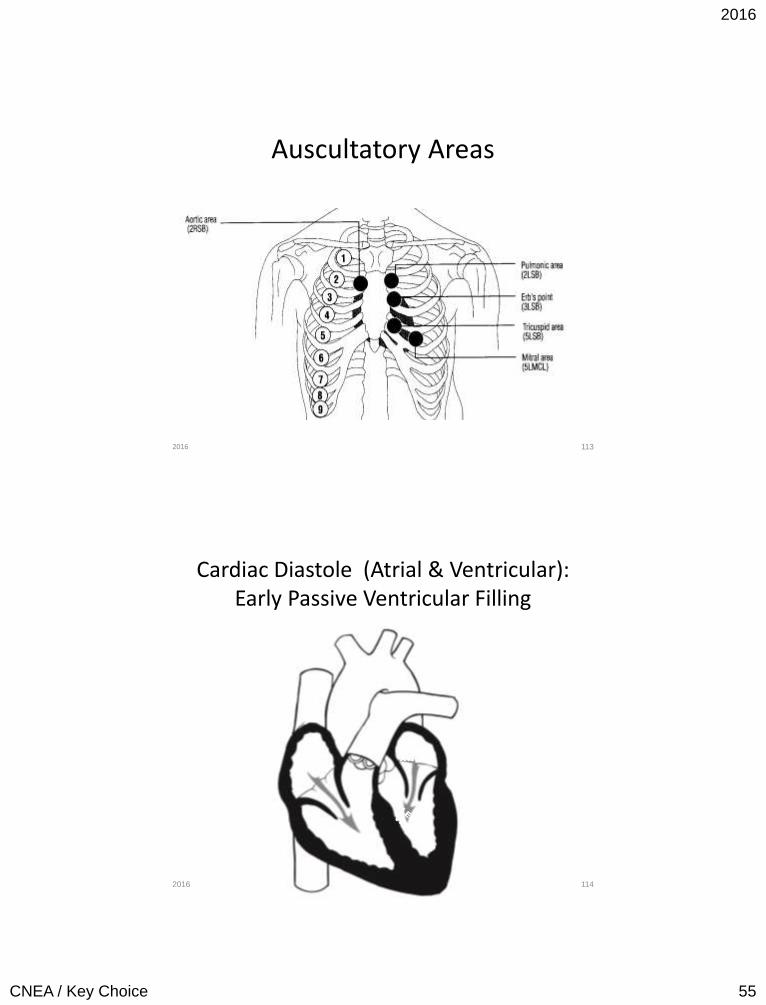
Auscultatory Areas
113 2016
Cardiac Diastole (Atrial & Ventricular): Early Passive Ventricular Filling
114
RIGHT
ATRIUM
LEFT
ATRIUM
AORTA
Pulmonary
Artery
2016

2016
CNEA / Key Choice 56
Atrial Systole & Ventricular Diastole: Late Active Ventricular Filling
115
Atrial Kick
RIGHT
ATRIUM
LEFT
ATRIUM
AORTA
Pulmonary
Artery
2016
Beginning Ventricular Systole: Isovolumic Contraction
116
RIGHT
ATRIUM
LEFT
ATRIUM
AORTA
Pulmonary
Artery
2016
2016
CNEA / Key Choice 57
Ventricular Systole: Ejection
117
RIGHT
ATRIUM
LEFT
ATRIUM
AORTA
Pulmonary
Artery
2016
Murmurs
• High blood flow through a normal or abnormal valve
• Forward flow through a narrowed or irregular orifice into a dilated chamber or vessel
• Backward or regurgitant flow through an incompetent valve
118 2016
2016
CNEA / Key Choice 58
Murmur Fundamentals
• Stenotic Murmurs – Valve does not open appropriately
– Heard during the part of the cardiac cycle when the valve is open
• Regurgitant Murmurs – Valve does not close appropriately
– Heard during the part of the cardiac cycle when the valve is to be closed
119 2016
Systolic Murmurs: What is Happening During Systole
• Tricuspid and Mitral Valve Closed
– Tricuspid Regurgitation
– Mitral Regurgitation
• Pulmonic and Aortic Valve Open
– Pulmonic Stenosis
– Aortic Stenosis
120 2016
2016
CNEA / Key Choice 59
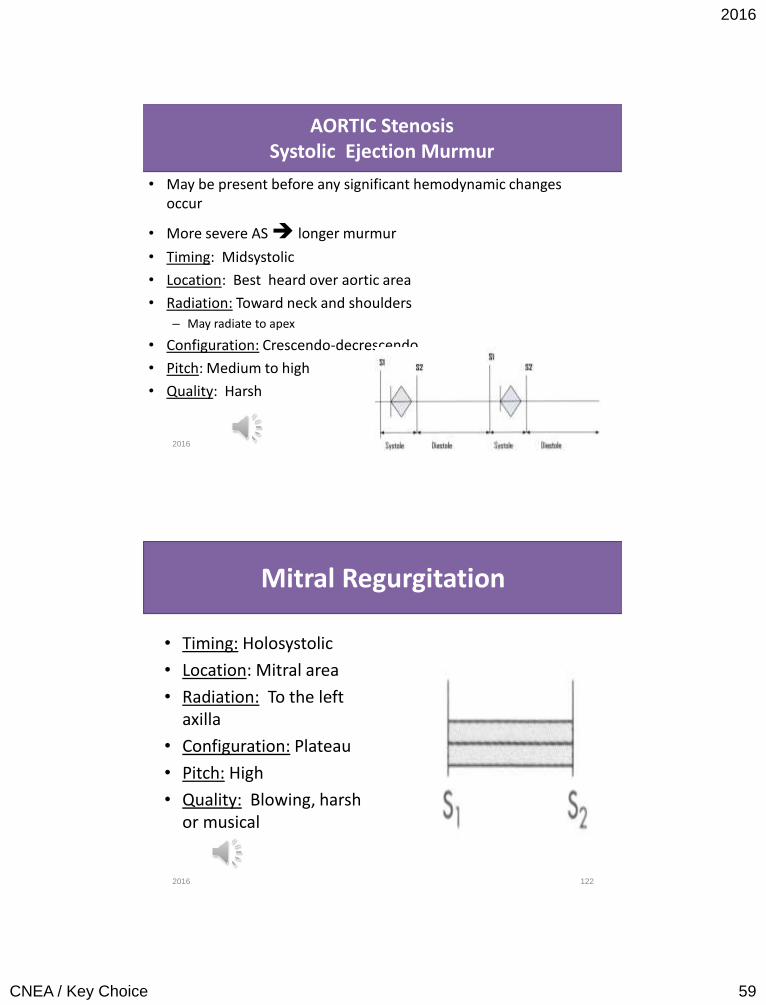
AORTIC Stenosis Systolic Ejection Murmur
• May be present before any significant hemodynamic changes occur
• More severe AS longer murmur
• Timing: Midsystolic
• Location: Best heard over aortic area
• Radiation: Toward neck and shoulders – May radiate to apex
• Configuration: Crescendo-decrescendo
• Pitch: Medium to high
• Quality: Harsh
121 2016
Mitral Regurgitation
• Timing: Holosystolic
• Location: Mitral area
• Radiation: To the left axilla
• Configuration: Plateau
• Pitch: High
• Quality: Blowing, harsh or musical
122 2016
2016
CNEA / Key Choice 60
BETWEEN AORTIC STENOSIS AND MITRAL REGURGITATION:
Which of these valvular disorders can develop acutely?
123 2016
Diastolic Murmurs: What is Happening During Diastole
• Tricuspid and Mitral Valves Open
– Tricuspid Stenosis
– Mitral Stenosis
• Pulmonic and Aortic Valves Closed
– Pulmonic Regurgitation
– Aortic Regurgitation
124 2016
2016
CNEA / Key Choice 61
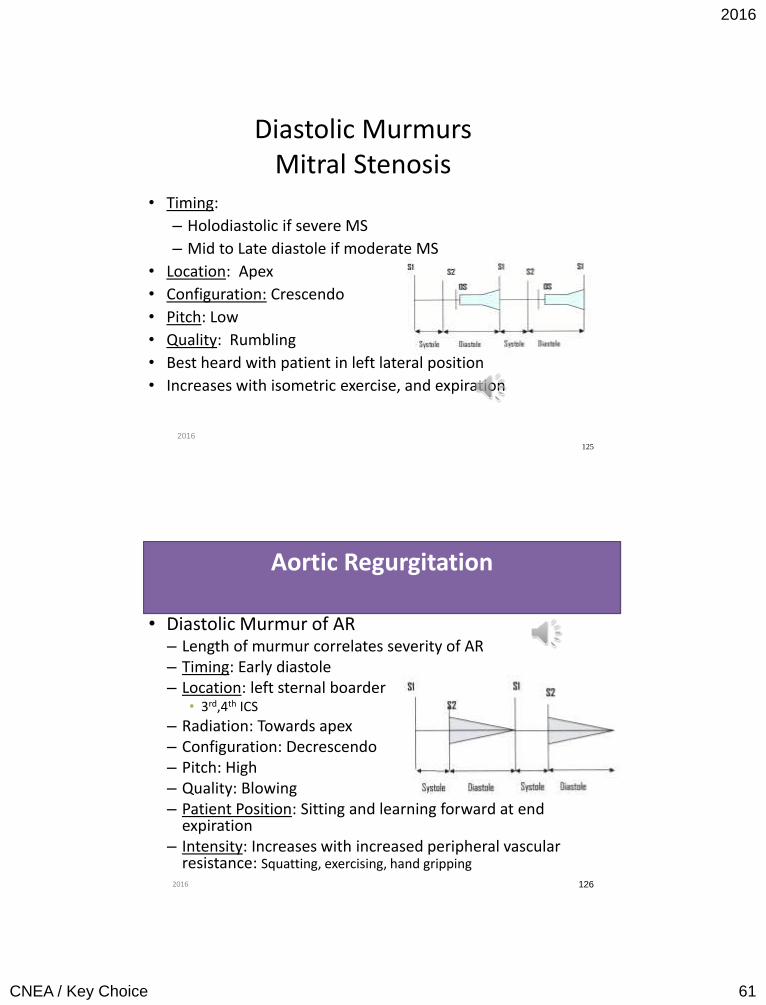
Diastolic Murmurs Mitral Stenosis
• Timing:
– Holodiastolic if severe MS
– Mid to Late diastole if moderate MS
• Location: Apex
• Configuration: Crescendo
• Pitch: Low
• Quality: Rumbling
• Best heard with patient in left lateral position
• Increases with isometric exercise, and expiration
125
2016
Aortic Regurgitation
• Diastolic Murmur of AR – Length of murmur correlates severity of AR – Timing: Early diastole – Location: left sternal boarder
• 3rd,4th ICS
– Radiation: Towards apex – Configuration: Decrescendo – Pitch: High – Quality: Blowing – Patient Position: Sitting and learning forward at end
expiration – Intensity: Increases with increased peripheral vascular
resistance: Squatting, exercising, hand gripping
126 2016
2016
CNEA / Key Choice 62
BETWEEN MITRAL STENOSIS AND AORTIC REGURGITATION:
Which of these valvular disorders can develop acutely?
127 2016
When you have Tachycardia Ask
Yourself:
128
Why is my patient
compensating?
2016
CO = SV x HR
2016
CNEA / Key Choice 63
Blood Pressure Monitoring
• Systolic: Maximum pressure when blood is expelled from the left ventricle – Represents stroke volume
• Diastolic: Measures rate of flow of ejected blood and vessel
elasticity – Represents state of arterioles
• Pulse Pressure: Difference between systolic and diastolic
pressure
• Mean pressure (MAP): calculated; pressure that determines end organ perfusion
129 2016
Blood Pressure Assessment
• Variation of up to 15mm Hg between arms is normal
• BP in legs - 10 mm Hg higher than arms
130 2016
2016
CNEA / Key Choice 64
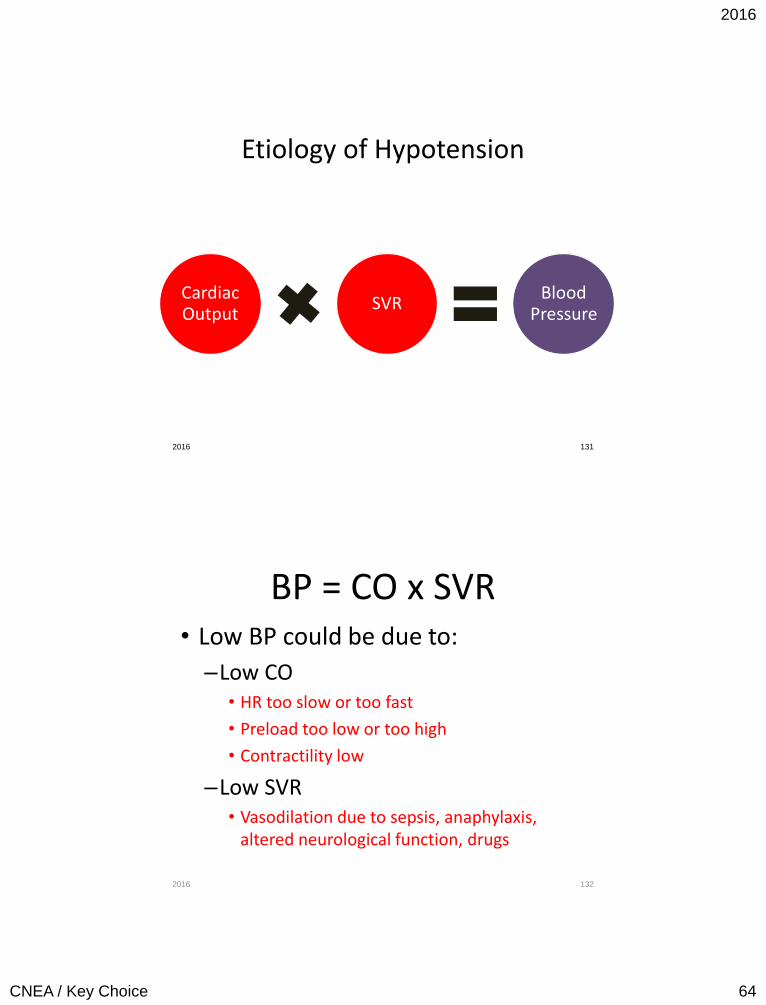
Etiology of Hypotension
Cardiac Output
SVR Blood
Pressure
2016 131
BP = CO x SVR • Low BP could be due to:
–Low CO • HR too slow or too fast
• Preload too low or too high
• Contractility low
–Low SVR • Vasodilation due to sepsis, anaphylaxis,
altered neurological function, drugs
2016 132
2016
CNEA / Key Choice 65
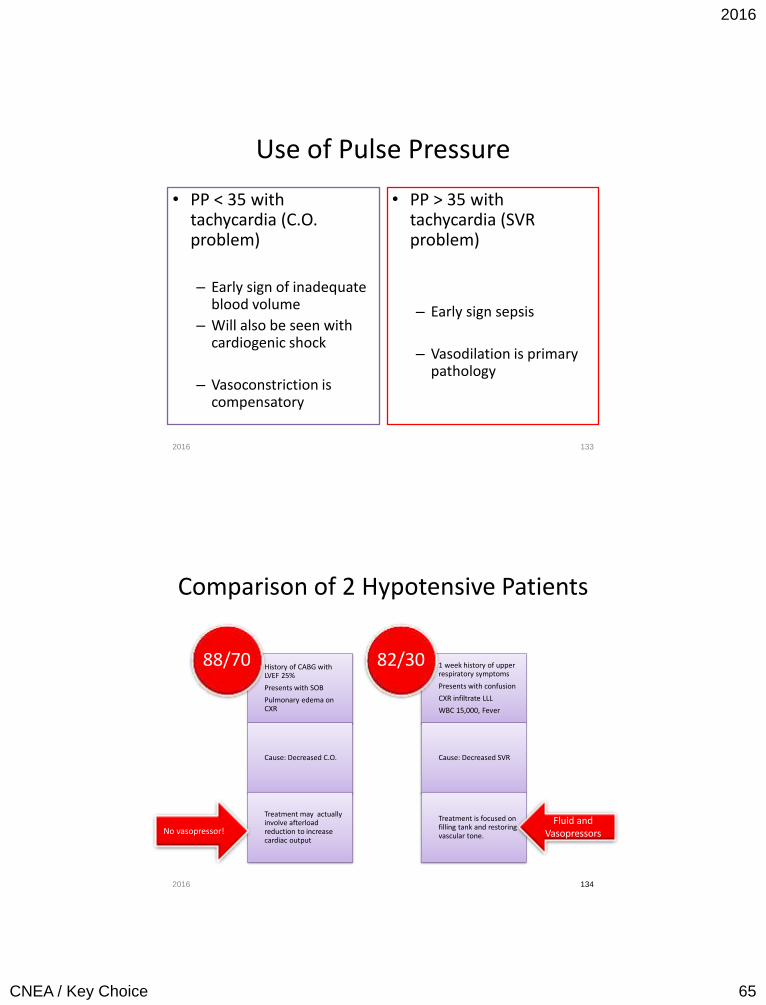
Use of Pulse Pressure
• PP < 35 with tachycardia (C.O. problem)
– Early sign of inadequate
blood volume
– Will also be seen with cardiogenic shock
– Vasoconstriction is compensatory
• PP > 35 with tachycardia (SVR problem)
– Early sign sepsis
– Vasodilation is primary pathology
2016 133
Comparison of 2 Hypotensive Patients
History of CABG with LVEF 25%
Presents with SOB
Pulmonary edema on CXR
Cause: Decreased C.O.
Treatment may actually involve afterload reduction to increase cardiac output
88/70 1 week history of upper respiratory symptoms
Presents with confusion
CXR infiltrate LLL
WBC 15,000, Fever
Cause: Decreased SVR
Treatment is focused on filling tank and restoring vascular tone.
82/30
2016 134
No vasopressor! Fluid and
Vasopressors
2016
CNEA / Key Choice 66
Pulsus Paradoxus • Patient is placed in a semirecumbent position • Respirations should be normal • BP cuff inflated to at least 20 mm Hg above the systolic pressure • Slowly deflated until the first Korotkoff sounds are heard only during
expiration. – Pulsus paradoxus is present at this pressure reading, if the cuff is
not further deflated and the first Korotkoff sound is not audible during inspiration.
• As the cuff is further deflated, the point at which the first Korotkoff sound is audible during both inspiration and expiration is recorded.
• If the difference between the first and second measurement is greater than 12 mm Hg, an abnormal pulsus paradoxus is present.
(Yarlagadda, Chakri, 2005 Cardiac Tamponade. Retrieved 3-22-06 from
www.emedicine.com) 135
May be present in cardiac tamponade.
2016
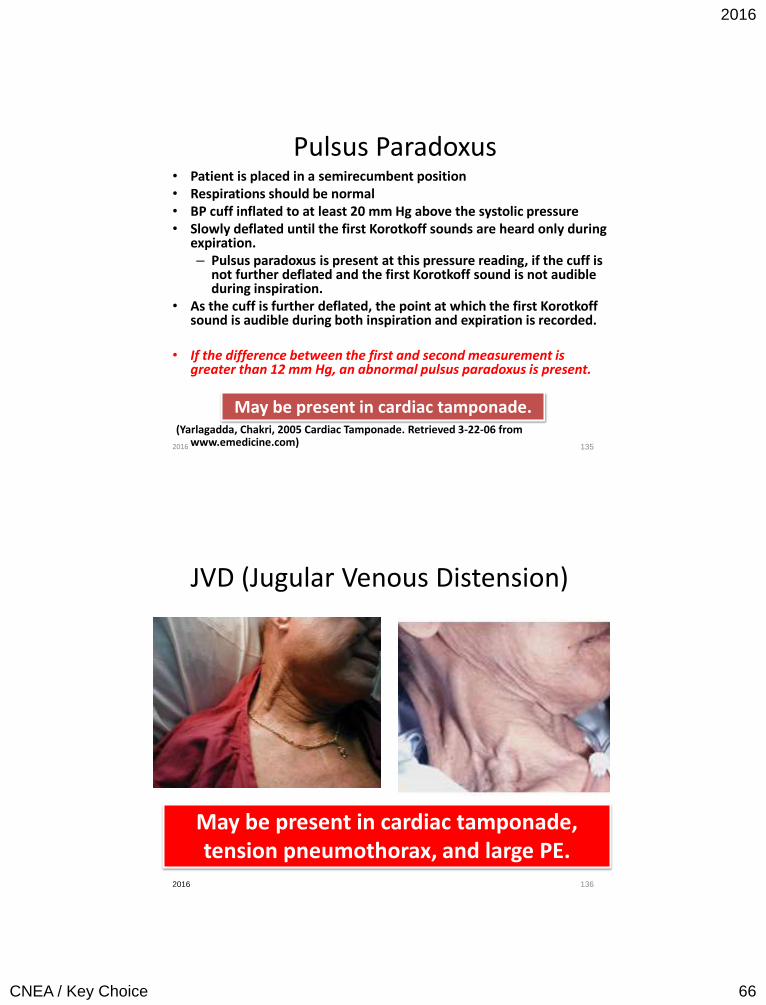
JVD (Jugular Venous Distension)
2016 136
May be present in cardiac tamponade, tension pneumothorax, and large PE.
2016
CNEA / Key Choice 67
Assessment Integration by Disease Process
Obstructive Shock and Mechanical Emergencies
137 2016
Cardiac Tamponade Who is at risk?
138
Trauma
Post CABG
Post MI
Pericarditis /
Effusion
2016
2016
CNEA / Key Choice 68
139 139
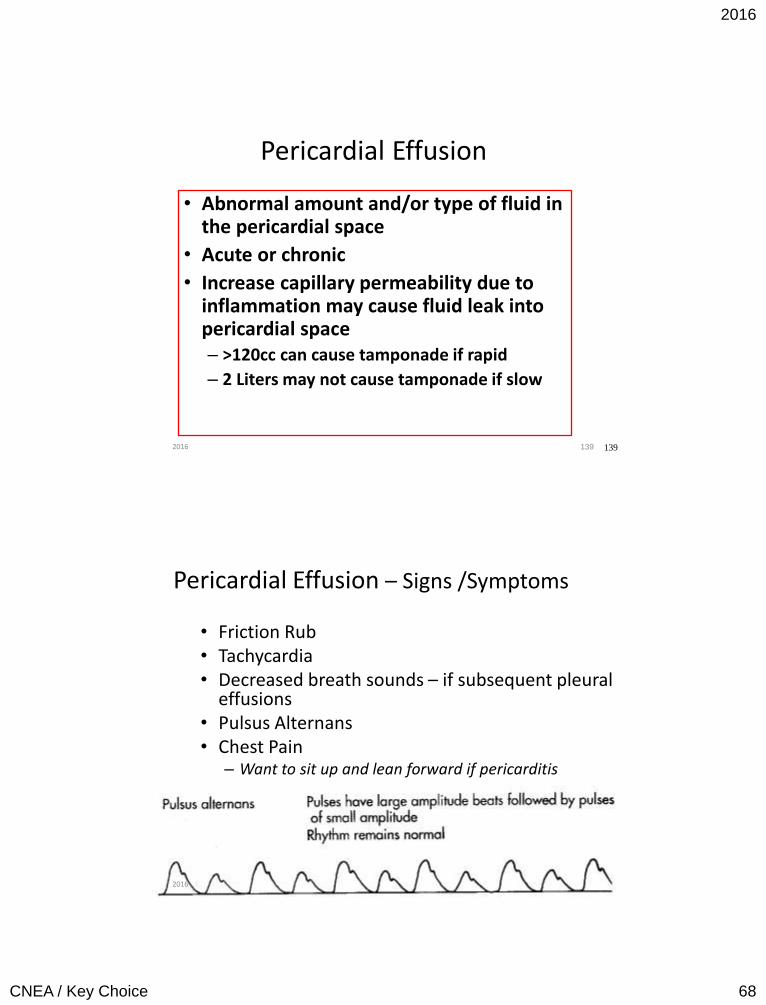
Pericardial Effusion
• Abnormal amount and/or type of fluid in the pericardial space
• Acute or chronic
• Increase capillary permeability due to inflammation may cause fluid leak into pericardial space – >120cc can cause tamponade if rapid
– 2 Liters may not cause tamponade if slow
2016
140 140
Pericardial Effusion – Signs /Symptoms
• Friction Rub • Tachycardia • Decreased breath sounds – if subsequent pleural
effusions • Pulsus Alternans • Chest Pain
– Want to sit up and lean forward if pericarditis
2016
2016
CNEA / Key Choice 69
141 2016
Cardiac Tamponade
• Clinical syndrome caused by accumulation of fluid in the pericardial space
• Results in reduction in ventricular filling and ultimately hemodynamic compromise
• Differentiation between pericardial
effusion and tamponade is hemodynamic status.
142 2016
2016
CNEA / Key Choice 70
Cardiac Tamponade: Signs and Symptoms
• Same as with pericarditis and pericardial effusion
• Feeling of impending doom • Beck’s Triad
• Hypotension, Distended neck veins, Muffled heart sounds
• Equalization of filling pressures (RAP, PAD, PAOP within 5mm of each other)
• Pulses paradoxus – Also observed in constrictive pericarditis, tension
pneumothorax, severe obstructive pulmonary disease, restrictive cardiomyopathy, PE, and RV infarct with shock.
143 Echocardiogram
2016
144 2016
2016
CNEA / Key Choice 71
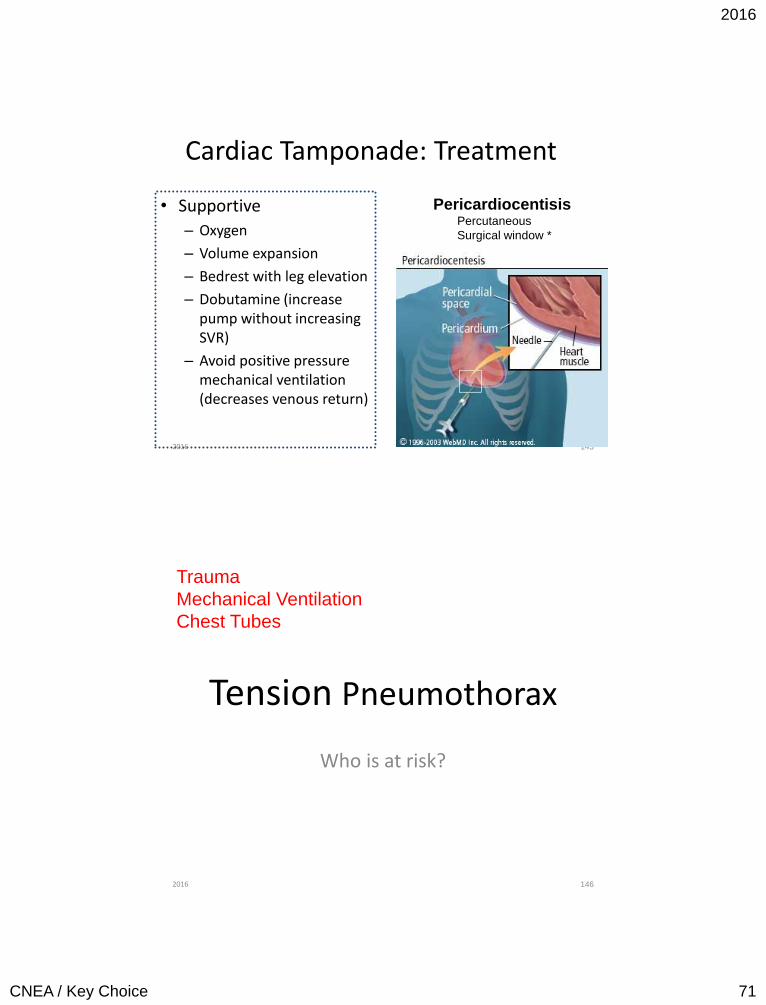
Cardiac Tamponade: Treatment
• Supportive
– Oxygen
– Volume expansion
– Bedrest with leg elevation
– Dobutamine (increase pump without increasing SVR)
– Avoid positive pressure mechanical ventilation (decreases venous return)
145
Pericardiocentisis Percutaneous
Surgical window *
2016
Tension Pneumothorax
Who is at risk?
146
Trauma
Mechanical Ventilation
Chest Tubes
2016
2016
CNEA / Key Choice 72
147
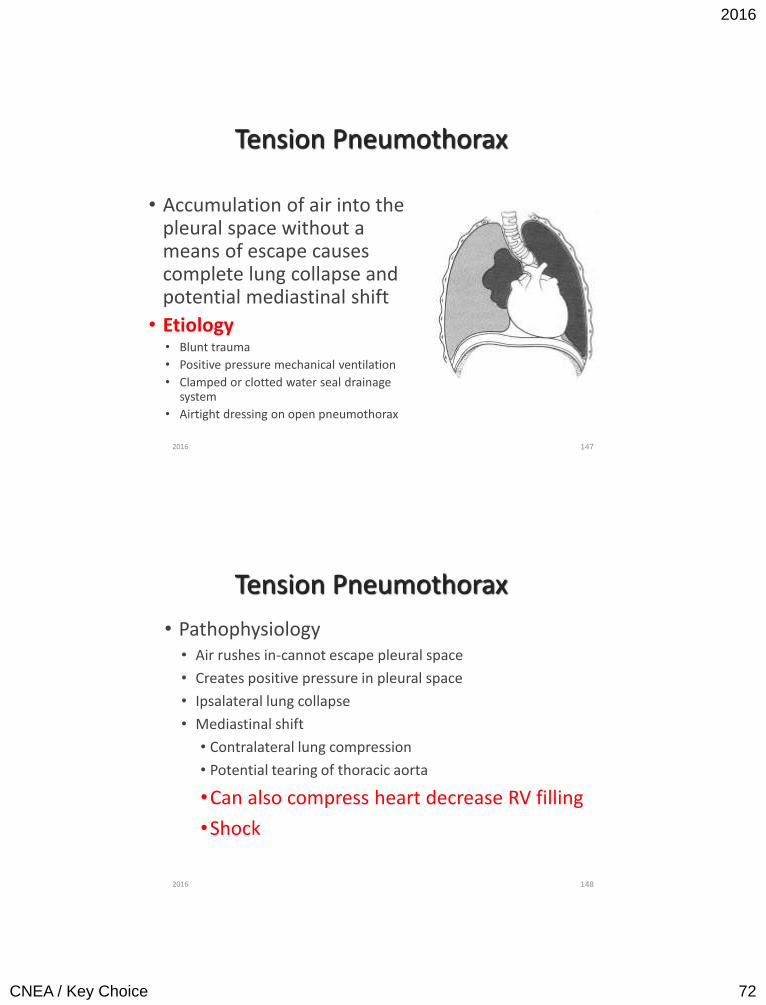
Tension Pneumothorax
• Accumulation of air into the pleural space without a means of escape causes complete lung collapse and potential mediastinal shift
• Etiology • Blunt trauma
• Positive pressure mechanical ventilation
• Clamped or clotted water seal drainage system
• Airtight dressing on open pneumothorax
2016
148
Tension Pneumothorax
• Pathophysiology • Air rushes in-cannot escape pleural space
• Creates positive pressure in pleural space
• Ipsalateral lung collapse
• Mediastinal shift
• Contralateral lung compression
• Potential tearing of thoracic aorta
•Can also compress heart decrease RV filling
•Shock
2016
2016
CNEA / Key Choice 73
Tension Pneumothorax: Signs and Symptoms
• Anxiety / agitation
• Diminished / absent breath sounds
• Dyspnea
• Tachypnea
• If mediastinal shift:
• Tracheal shift away from affected side
• LATE SIGN
• JVD
• Hypotension
149 2016
150
0Hypotension with Mechanical Ventilation
0 Sedation
0 Conversion to positive pressure ventilation. 0 Assure adequate circulating fluid
volume
0 Development of auto PEEP 0 Increase expiration time
0 Tension Pneumothorax 0 Chest tube required
2016
2016
CNEA / Key Choice 74
151
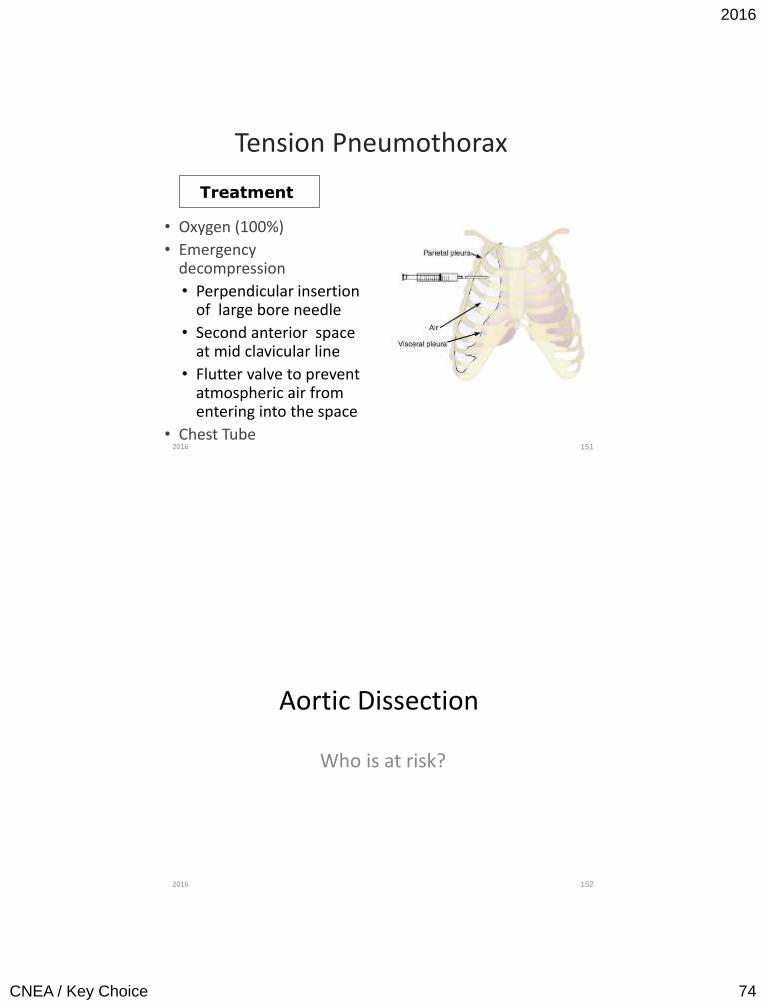
Tension Pneumothorax
• Oxygen (100%)
• Emergency decompression
• Perpendicular insertion of large bore needle
• Second anterior space at mid clavicular line
• Flutter valve to prevent atmospheric air from entering into the space
• Chest Tube
Treatment
2016
Aortic Dissection
Who is at risk?
152 2016
2016
CNEA / Key Choice 75
153
Risk Factors for Development of Thoracic Aortic Dissection
Conditions Associated With Increased Aortic Wall Stress
• Hypertension, particularly if uncontrolled • Pheochromocytoma
• Cocaine or other stimulant use
• Weight lifting or other Valsalva maneuver
• Trauma
• Deceleration or torsional injury (eg, motor vehicle crash,
fall)
• Coarctation of the aorta
Note: Information on this slide is adapted from Table 9 in full-text version of TAD Guidelines
2016
ISSUE:
Patient’s are usually asymptomatic until a catastrophic event occurs. Therefore: Identifying disease in high risk patients while still stable is a priority.
154 2016
2016
CNEA / Key Choice 76
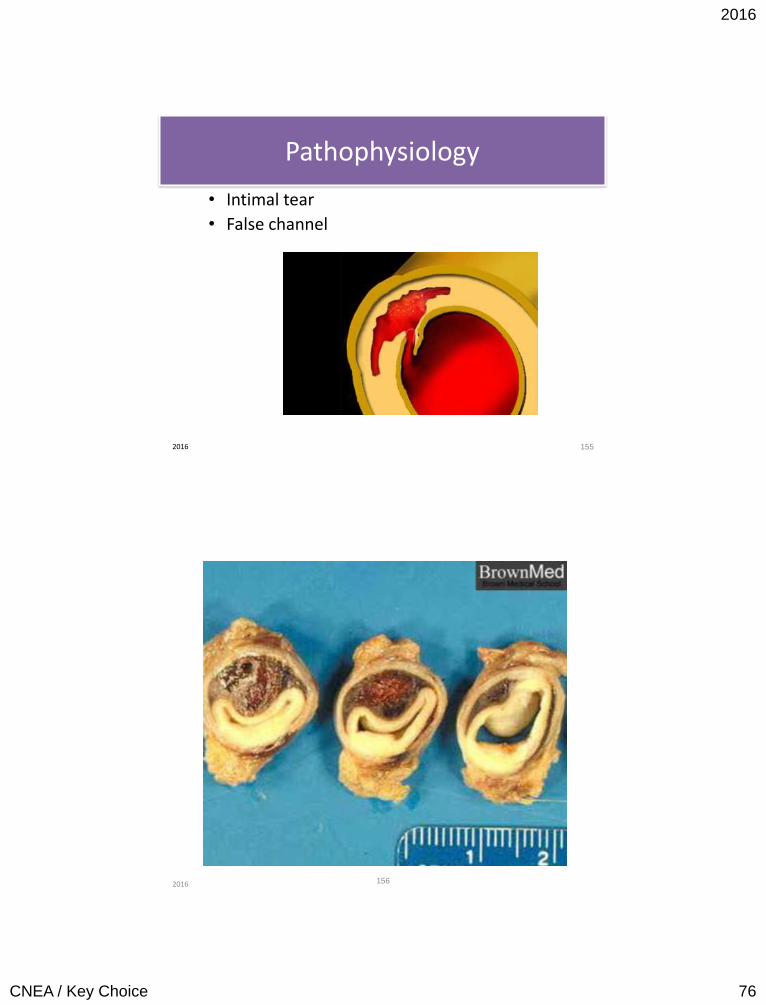
Pathophysiology
• Intimal tear
• False channel
155 2016
156 2016

2016
CNEA / Key Choice 77
Classification of Dissections
• Acute or chronic
• Type A Dissections: Dissections involving the ascending aorta.
• Type B Dissections: Dissections involving the descending thoracic aorta. These dissections begin distal to the left subclavian artery.
157 2016
Complications of Dissection
• Aortic regurgitation from retrograde dissection involving aortic valve or from aortic dilatation.
• MI from retrograde coronary artery dissection. • Cardiac tamponade from ascending aorta or aortic arch
rupture. • Intraplerual rupture from descending aortic dissection
ruptures into intrapleural space – most commonly left sided. • Retroperitoneal bleed from rupture of abdominal aorta
dissection. • Stroke from brachial artery compromise. • Paraplegia, reduced blood flow to kidneys, bowels, and lower
extremities from compromise of arterial branches.
158 2016
2016
CNEA / Key Choice 78
Clinical Presentation
Chest or back pain with variation in upper extremity blood pressure is key assessment finding in aortic dissection. Recurrent chest or back pain can indicate extension or rupture. The presence of aortic regurgitation in the setting of chest pain is also suspicious for aortic dissection.
159 2016
Estimation of Pretest Risk of Thoracic Aortic Dissection
* Loeys-Dietz syndrome, vascular Ehlers-Danlos syndrome, Turner syndrome, or other connective tissue disease.
†Patients with mutations in genes known to predispose to thoracic aortic aneurysms and dissection, such as FBN1, TGFBR1, TGFBR2, ACTA2, and MYH11.
160
High Risk Conditions
• Marfan Syndrome
• Connective tissue disease*
• Family history of aortic disease
• Known aortic valve disease
• Recent aortic manipulation (surgical or
catheter-based)
• Known thoracic aortic aneurysm
• Genetic conditions that predispose to AoD†
1
2016
2016
CNEA / Key Choice 79
161
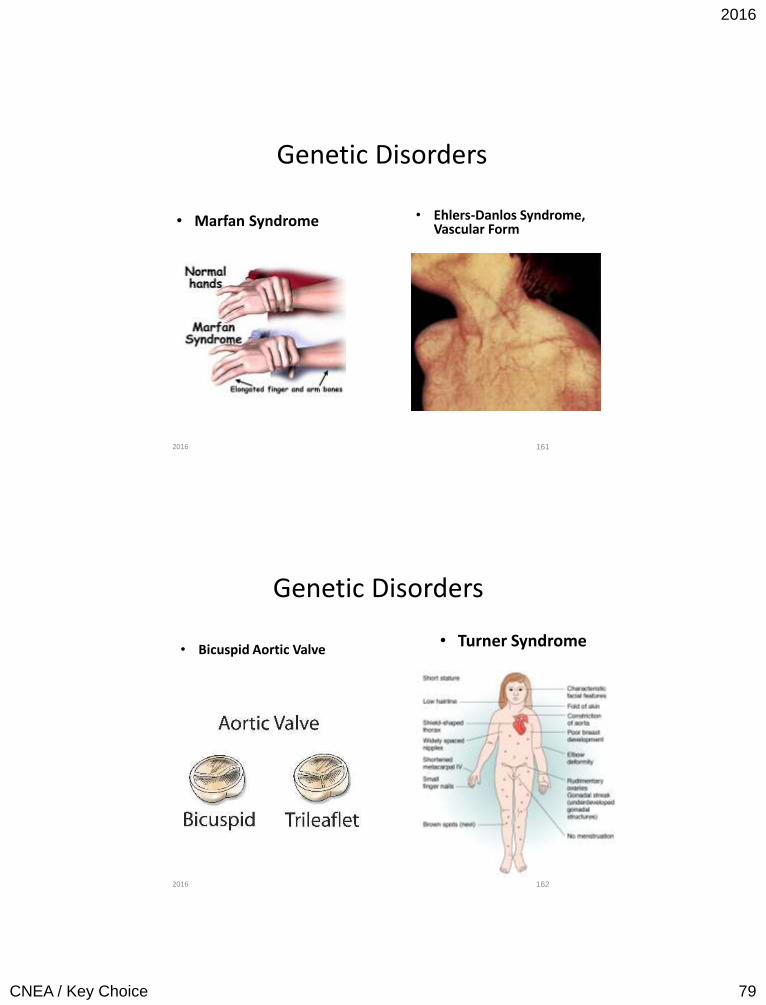
Genetic Disorders
• Marfan Syndrome
• Ehlers-Danlos Syndrome, Vascular Form
2016
162
Genetic Disorders
• Bicuspid Aortic Valve • Turner Syndrome
2016
2016
CNEA / Key Choice 80
Estimation of Pretest Risk of Thoracic Aortic Dissection
163
High Risk Pain Features
Chest, back, or abdominal pain features
described as pain that:
• is abrupt or instantaneous in onset.
• is severe in intensity.
• has a ripping, tearing, stabbing, or sharp
quality.
2
2016
Estimation of Pretest Risk of Thoracic Aortic Dissection
164
High Risk Examination Features
• Pulse deficit
• Systolic BP limb differential > 20mm Hg
• Focal neurologic deficit
• Murmur of aortic regurgitation (new or not
known to be old and in conjunction with pain)
3
2016
2016
CNEA / Key Choice 81
Risk-based Diagnostic Evaluation: Patients with High Risk of TAD
165
Patients at high-risk for TAD are those that present with at
least 2 high-risk features
The recommended course of action for high-risk TAD patients
is to seek immediate surgical consultation and arrange for
expedited aortic imaging.
• TEE (preferred if clinically unstable)
• CT scan (image entire aorta: chest to pelvis)
• MR (image entire aorta: chest to pelvis)
Expedited aortic imaging
2016
166 2016
2016
CNEA / Key Choice 82
167
Recommendations for Initial Management
a. In the absence of contraindications,
intravenous beta blockade should be
initiated and titrated to a target heart rate
of 60 beats per minute or less.
b. In patients with clear contraindications to
beta blockade, nondihydropyridine calcium
channel–blocking agents should be used as
an alternative for rate control.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
Initial management of thoracic aortic dissection should be
directed at decreasing aortic wall stress by controlling
heart rate and blood pressure as follows:
2016
168
Recommendations for Initial Management
c. If systolic blood pressures remain greater
than 120mm Hg after adequate heart rate
control has been obtained, then angiotensin-
converting enzyme inhibitors and/or other
vasodilators should be administered
intravenously to further reduce blood pressure
that maintains adequate end-organ perfusion.
d. Beta blockers should be used cautiously in the
setting of acute aortic regurgitation because
they will block the compensatory tachycardia.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
2016
2016
CNEA / Key Choice 83
169
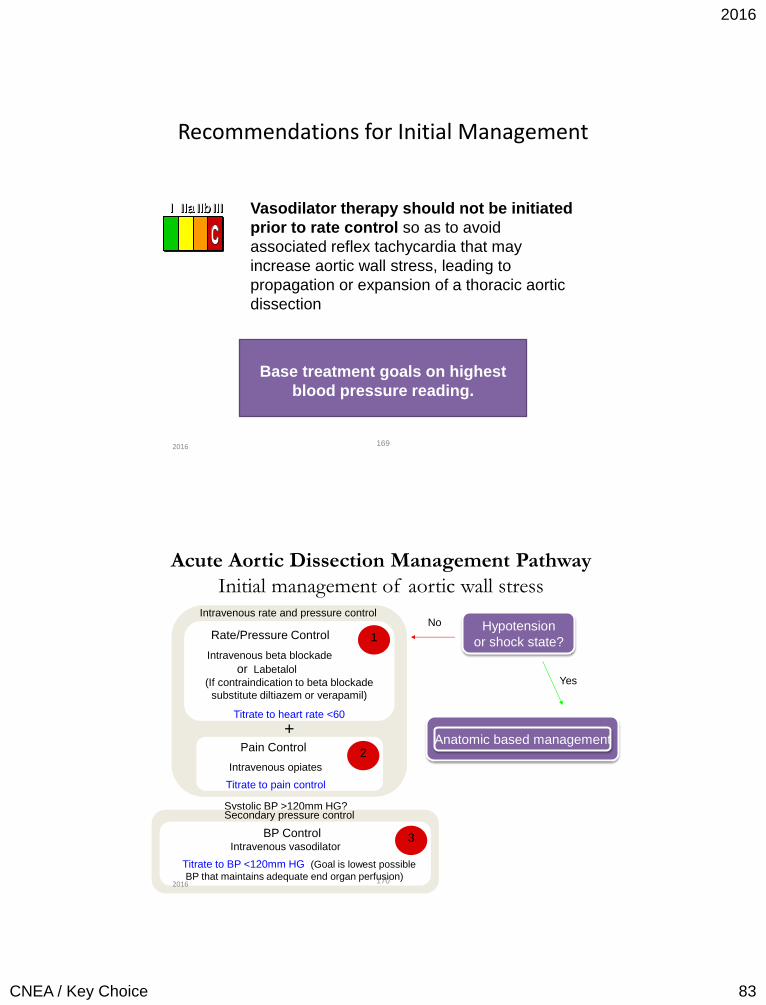
Recommendations for Initial Management
Vasodilator therapy should not be initiated
prior to rate control so as to avoid
associated reflex tachycardia that may
increase aortic wall stress, leading to
propagation or expansion of a thoracic aortic
dissection.
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
Base treatment goals on highest
blood pressure reading.
2016
Rate/Pressure Control
Intravenous beta blockade
or Labetalol
(If contraindication to beta blockade
substitute diltiazem or verapamil)
Titrate to heart rate <60
1
Pain Control
Intravenous opiates
Titrate to pain control
Intravenous rate and pressure control
2
+
Hypotension
or shock state?
No
Yes
Systolic BP >120mm HG?
BP Control Intravenous vasodilator
Titrate to BP <120mm HG (Goal is lowest possible
BP that maintains adequate end organ perfusion)
Secondary pressure control
3
Anatomic based management
Acute Aortic Dissection Management Pathway
Initial management of aortic wall stress
170 2016
2016
CNEA / Key Choice 84
Acute Aortic Dissection Management Pathway
171
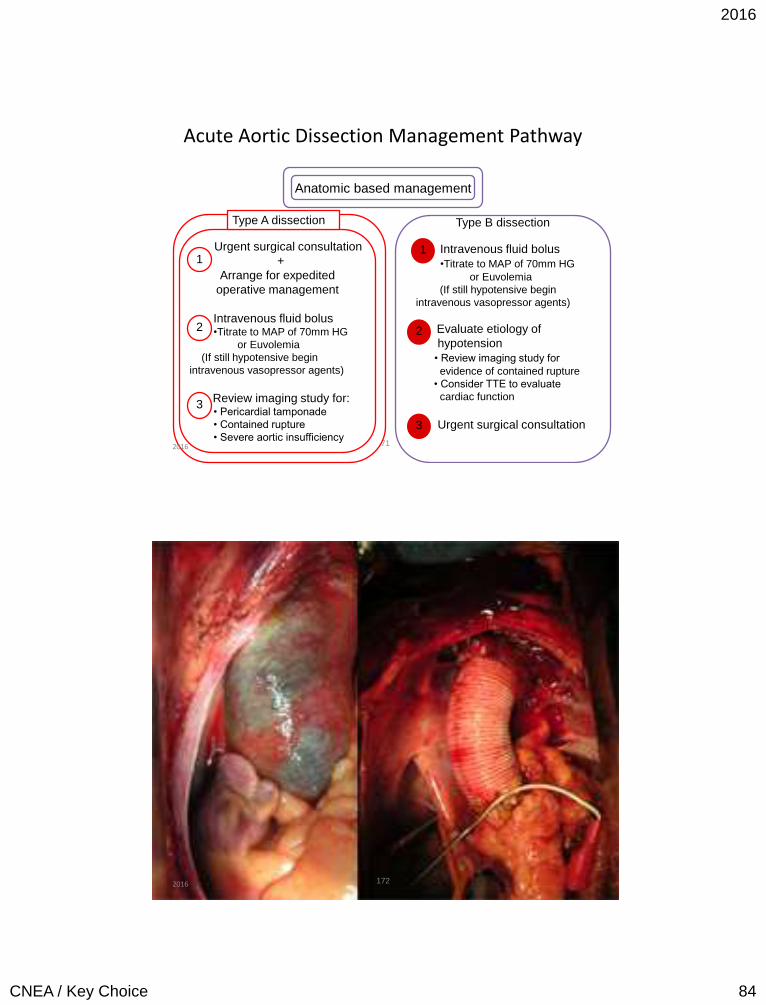
Anatomic based management
Urgent surgical consultation
+
Arrange for expedited
operative management
Intravenous fluid bolus •Titrate to MAP of 70mm HG
or Euvolemia
(If still hypotensive begin
intravenous vasopressor agents)
Review imaging study for: • Pericardial tamponade
• Contained rupture
• Severe aortic insufficiency
1
2
3
Type A dissection
Intravenous fluid bolus
•Titrate to MAP of 70mm HG
or Euvolemia
(If still hypotensive begin
intravenous vasopressor agents)
Evaluate etiology of
hypotension
• Review imaging study for
evidence of contained rupture
• Consider TTE to evaluate
cardiac function
Urgent surgical consultation
2
3
Type B dissection
1
2016
172 2016
2016
CNEA / Key Choice 85
173 2016
174 2016
2016
CNEA / Key Choice 86
Pulmonary Embolus
Who is at risk?
175 2016
176
Pulmonary Embolism
• Obstruction of blood flow to one or more arteries of the lung by a thrombus (other emboli – fat, air, amniotic fluid) lodged in a pulmonary vessel
• 2nd most common cause of sudden death
• 3rd most common cause of death in hospitalized patient
– 80% of unexpected hospital deaths
• Often recurrent
2016
CNEA / Key Choice 87
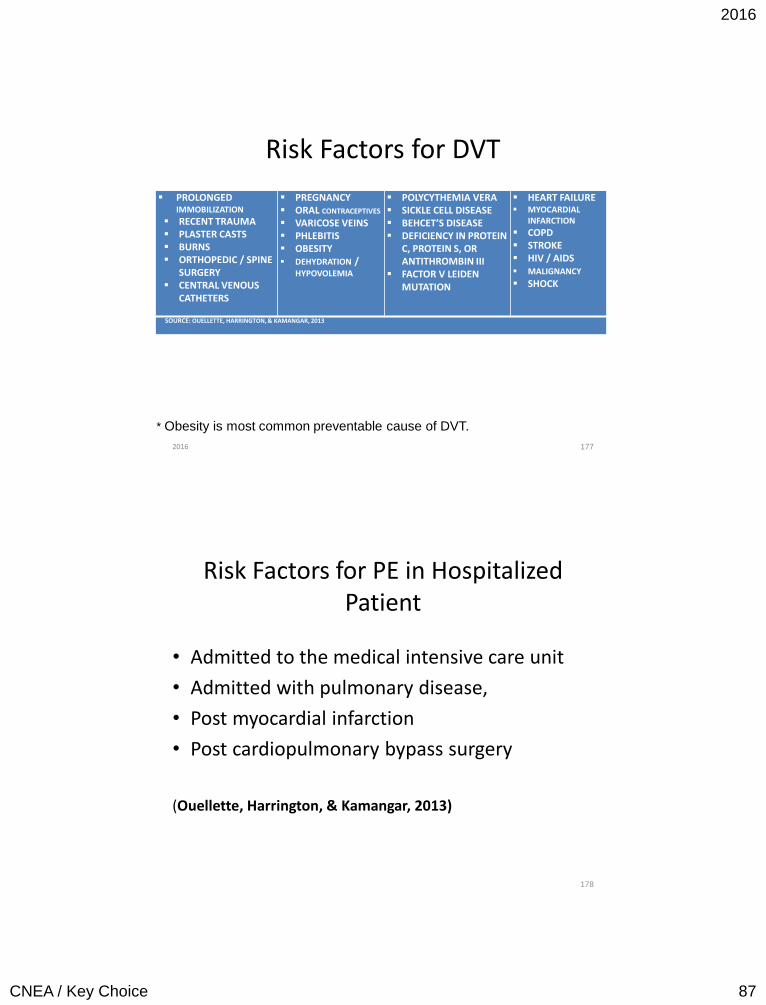
Risk Factors for DVT
177
PROLONGED IMMOBILIZATION
RECENT TRAUMA PLASTER CASTS BURNS ORTHOPEDIC / SPINE
SURGERY CENTRAL VENOUS
CATHETERS
PREGNANCY ORAL CONTRACEPTIVES
VARICOSE VEINS PHLEBITIS OBESITY DEHYDRATION /
HYPOVOLEMIA
POLYCYTHEMIA VERA SICKLE CELL DISEASE BEHCET’S DISEASE DEFICIENCY IN PROTEIN
C, PROTEIN S, OR ANTITHROMBIN III
FACTOR V LEIDEN MUTATION
HEART FAILURE MYOCARDIAL
INFARCTION
COPD STROKE HIV / AIDS MALIGNANCY SHOCK
SOURCE: OUELLETTE, HARRINGTON, & KAMANGAR, 2013
* Obesity is most common preventable cause of DVT.
2016
Risk Factors for PE in Hospitalized Patient
• Admitted to the medical intensive care unit
• Admitted with pulmonary disease,
• Post myocardial infarction
• Post cardiopulmonary bypass surgery
(Ouellette, Harrington, & Kamangar, 2013)
178
2016
CNEA / Key Choice 88
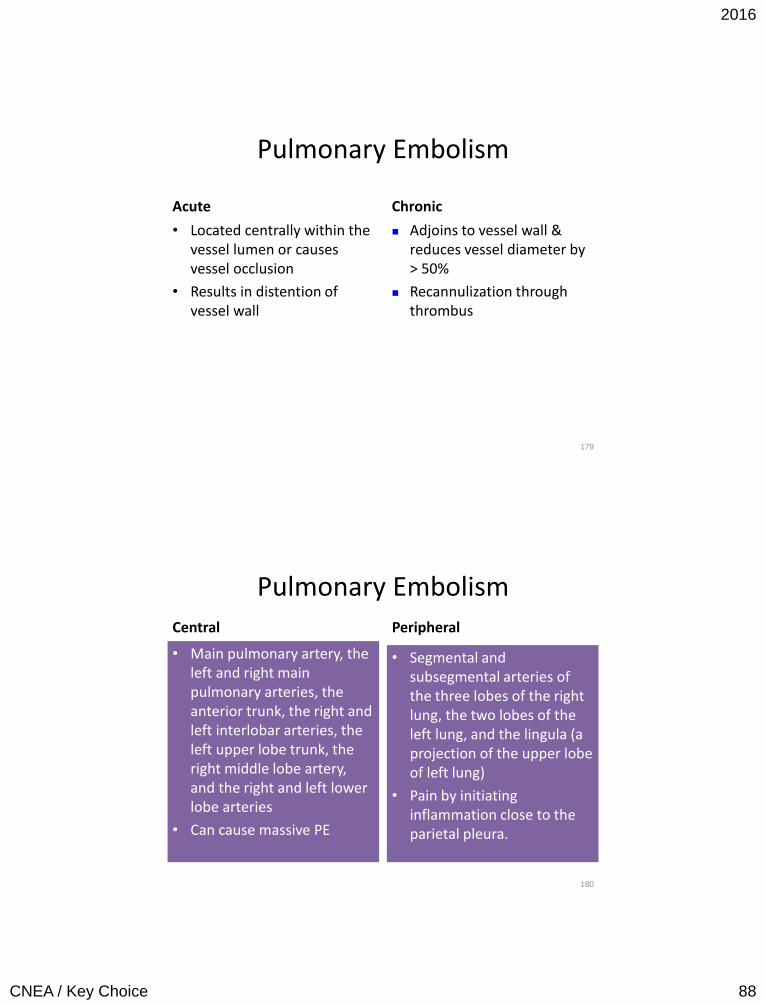
Pulmonary Embolism
Acute
• Located centrally within the vessel lumen or causes vessel occlusion
• Results in distention of vessel wall
Chronic
Adjoins to vessel wall & reduces vessel diameter by > 50%
Recannulization through thrombus
179
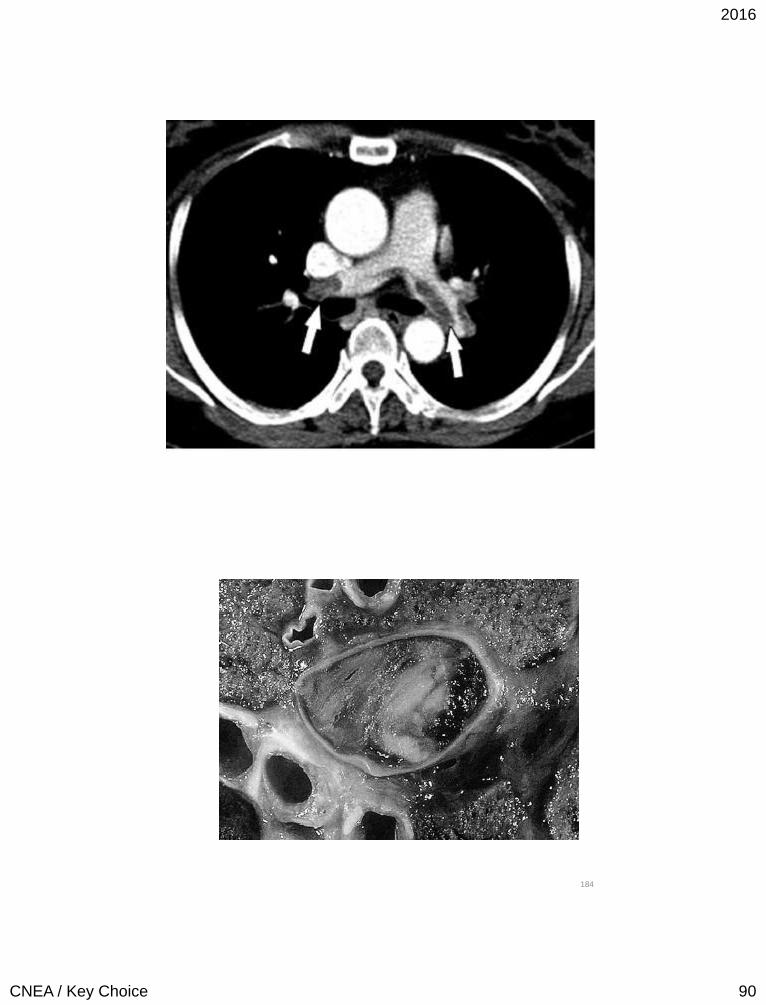
Pulmonary Embolism
Central
• Main pulmonary artery, the left and right main pulmonary arteries, the anterior trunk, the right and left interlobar arteries, the left upper lobe trunk, the right middle lobe artery, and the right and left lower lobe arteries
• Can cause massive PE
Peripheral
• Segmental and subsegmental arteries of the three lobes of the right lung, the two lobes of the left lung, and the lingula (a projection of the upper lobe of left lung)
• Pain by initiating inflammation close to the parietal pleura.
180
2016
CNEA / Key Choice 89
Massive PE
• Present in less than 5% of patients presenting with PE (Kucher, Rossi, De Rosa, & Goldhaber, 2006).
• Involves both the right and left pulmonary arteries or causes hemodynamic collapse
• Presenting systolic BP of < 90 mmHg
• Mortality rates ange from 30% to 60% and most deaths occur within the first 1 to 2 hours (Ouellette et al., 2013; Wood, 2002).
181
182
2016
CNEA / Key Choice 90
183
184
2016
CNEA / Key Choice 91
185
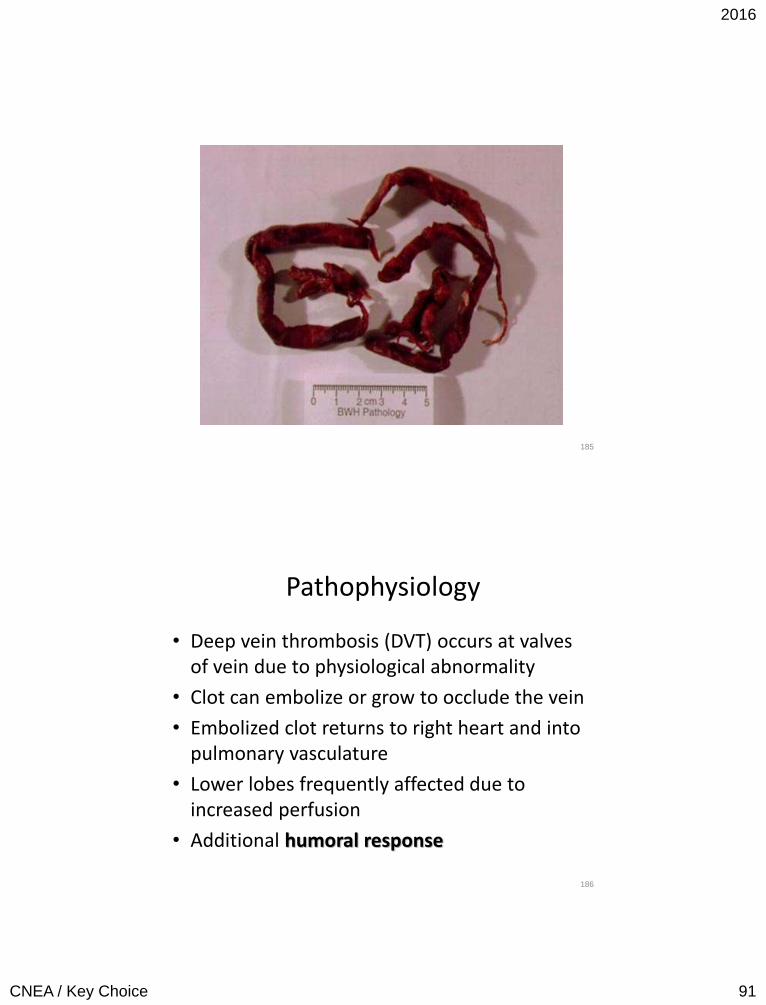
Pathophysiology
• Deep vein thrombosis (DVT) occurs at valves of vein due to physiological abnormality
• Clot can embolize or grow to occlude the vein
• Embolized clot returns to right heart and into pulmonary vasculature
• Lower lobes frequently affected due to increased perfusion
• Additional humoral response
186
2016
CNEA / Key Choice 92
Pathophysiology
• Increased PVR – Proximal clots
– Substances (thromboxane A and serotonin) released in humoral response also cause vasoconstriction
• PA pressures double to compensate
• Increased work load of RV – Right heart failure
– Leftward shift of septum
– Right coronary branches can be compressed
187
Pathophysiology • Increased V/Q ratio (alveolar dead space)
• Decreased V/Q ratio to other areas due to redistribution of blood flow
• Hypoxemia due to V/Q mismatching
• Increased minute ventilation to compensate for increased dead space – respiratory alkalosis – however, hypercapnea in massive
• Alveolar shrinkage (↓ CO2) – damage Type 2 alveolar cells – loss of surfactant – atelectasis – non cardiac pulmonary edema
• Pulmonary infarction rare due to dual blood supply
188
2016
CNEA / Key Choice 93
Clinical Presentation
• Pleuritic chest pain, shortness of breath, and hypoxemia is not present in the majority of patients
• May have no respiratory complaint
• Atypical presentation: flank pain, abdominal pain, delirium, syncope, and seizures
• Potential diagnosis in any patient with respiratory symptoms in whom there is not another clear etiology
• Suspect when there is respiratory alkalosis
189
Physical Exam Findings
• The most common physical sign, present in almost everyone with PE, is tachypnea (defined as respiratory rate > 16 per minute)
• Other:
– Dyspnea, rales, cough, hemoptysis
– Accentuated 2nd heart sound, presence of right sided S3 or S4, new systolic murmur of tricuspid regurgitation
– Tachycardia, low grade fever, diaphoresis
– Signs of thrombophlebitis, lower extremity peripheral edema
– Hypoxemia, cyanosis
190
2016
CNEA / Key Choice 94
More on Assessment
Massive PE
• Shock presentation
Multiple Emboli
• More signs of pulmonary hypertension and cor pulmonale
191
Diagnosis
• Cardiac troponins will be elevated in half of patients
with moderate to large PE (Konstantinides, 2008)
• Use of ultrasound to rule out DVT
• Computed tomography angiography (CTA) has become the standard test for the diagnosis of PE
• VQ scan is used as alternative
192
2016
CNEA / Key Choice 95
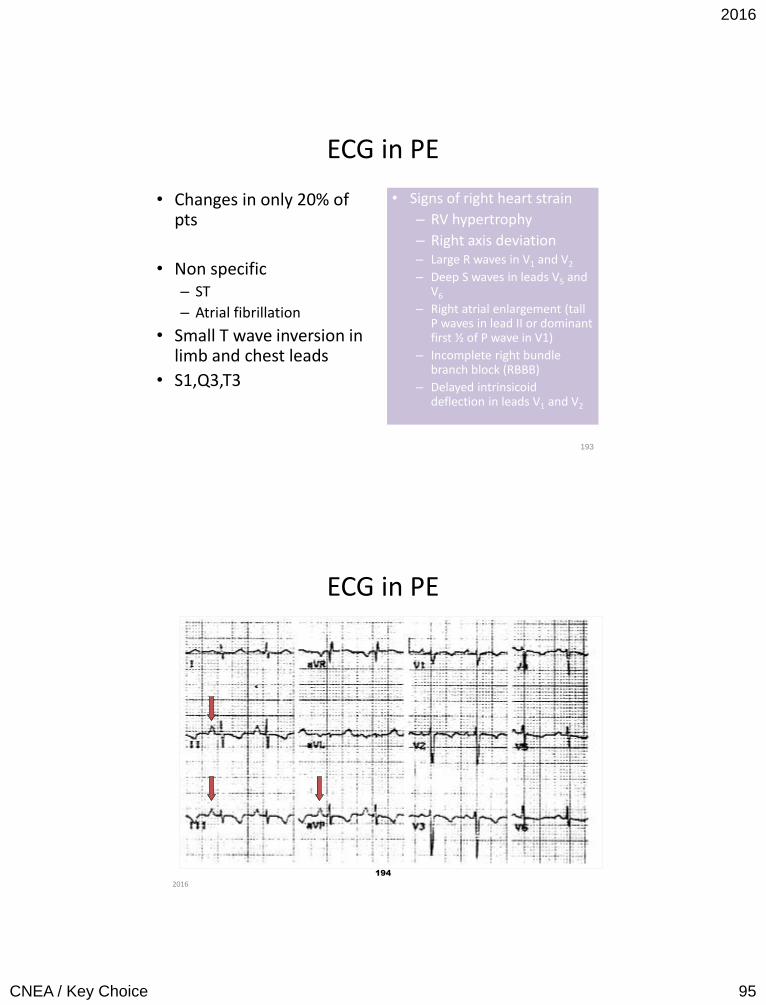
ECG in PE
• Changes in only 20% of pts
• Non specific – ST
– Atrial fibrillation
• Small T wave inversion in limb and chest leads
• S1,Q3,T3
• Signs of right heart strain
– RV hypertrophy
– Right axis deviation – Large R waves in V1 and V2
– Deep S waves in leads V5 and V6
– Right atrial enlargement (tall P waves in lead II or dominant first ½ of P wave in V1)
– Incomplete right bundle branch block (RBBB)
– Delayed intrinsicoid deflection in leads V1 and V2
193
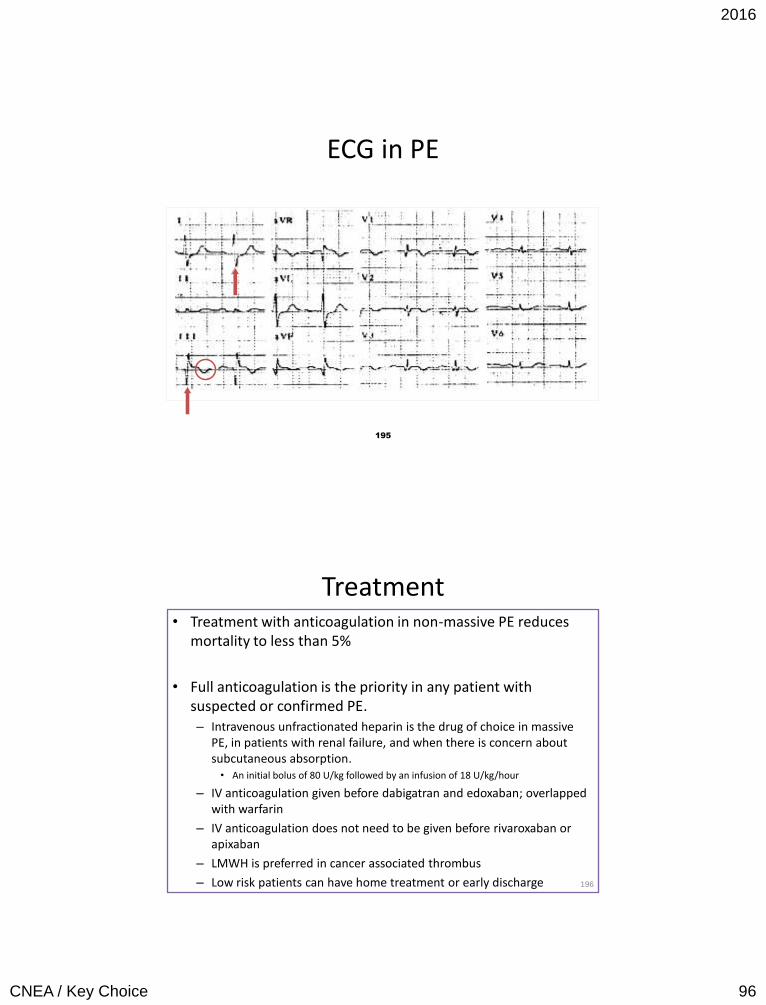
ECG in PE
194
2016
2016
CNEA / Key Choice 96
195
ECG in PE
Treatment • Treatment with anticoagulation in non-massive PE reduces
mortality to less than 5%
• Full anticoagulation is the priority in any patient with suspected or confirmed PE. – Intravenous unfractionated heparin is the drug of choice in massive
PE, in patients with renal failure, and when there is concern about subcutaneous absorption.
• An initial bolus of 80 U/kg followed by an infusion of 18 U/kg/hour
– IV anticoagulation given before dabigatran and edoxaban; overlapped with warfarin
– IV anticoagulation does not need to be given before rivaroxaban or apixaban
– LMWH is preferred in cancer associated thrombus
– Low risk patients can have home treatment or early discharge
196
2016
CNEA / Key Choice 97
Treatment
• Fibrinolytic therapy – Hemodynamic compromise as evidenced by
systolic BP < 90 mmHg and no high risk for bleeding
– Deterioration on anticoagulation and low bleeding risk
• Catheter assisted thrombosis removal if high bleeding risk / failed systemic therapy / shock – Surgical pulmonary embolectomy may also be considered
in select patients
197
Treatment • Includes PE, DVT, and VTE (venous thromboembolic event) • 3 month long term anticoagulation if no cancer and if
provoked – Dabigatran, rivaroxaban, apixaban, edoxaban preferred over
warfarin
• If unprovoked – minimum of 3 months and then evaluation for risk benefit ratio – High bleeding risk – 3 months – Low to moderate bleeding risk – extended anticoagulation
• Active cancer – LMWH preferred agent – Extended anticoagulation even in high bleeding risk
• LMWH if recurrent VTE on oral anticoagulation
2016
CNEA / Key Choice 98
Myocardial Rupture
Who is at Risk?
199 2016
Mechanical Rupture • Cardiac tamponade
from free wall rupture • Formation of left
ventricular diverticulum or pseudoaneurysm from free wall rupture
• Left to right shunt from septal rupture
• Acute mitral regurgitation from papillary muscle rupture.
– 10% of MIs
• 15% of in hospital deaths after MI
• Without surgical intervention, the mortality rate for rupture is > 80% at two weeks.
• Two high risk periods – 1st 24 hours – Within 1st week ( 3 to 5
days)
• Associated with delayed fibrinolytics and late presentation
2
0
0 2016
2016
CNEA / Key Choice 99
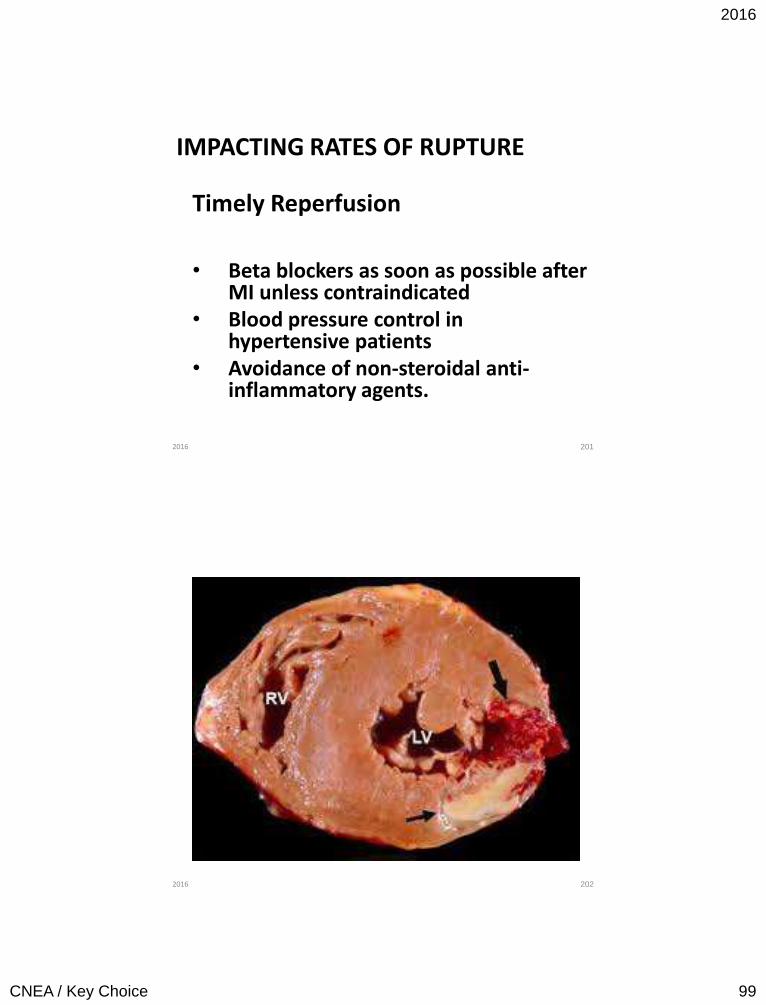
IMPACTING RATES OF RUPTURE
Timely Reperfusion
• Beta blockers as soon as possible after MI unless contraindicated
• Blood pressure control in hypertensive patients
• Avoidance of non-steroidal anti-inflammatory agents.
201 2016
202 2016
2016
CNEA / Key Choice 100
Free Wall Rupture
Incidence:
More common than ventricular septal rupture or papillary muscle rupture.
Warning Signs:
Recurrent chest pain and signs of regional pericarditis.
Consequences:
Hemipericardium, tamponade, electromechanical dissociation, and death.
203 2016
Risk Factors for Free Wall Rupture
• First MI, often relatively small • Anterior lateral wall MI • Advanced age • Female gender • Hypertension during acute phase • Absence of collateral blood flow • Q waves on ECG • Use of corticosteroids or non-steroidal anti-
inflammatory agents (NSAIDs) • Administration of fibrinolytics > 11 hours after
symptom onset. • Post infarction angina
204 2016
2016
CNEA / Key Choice 101
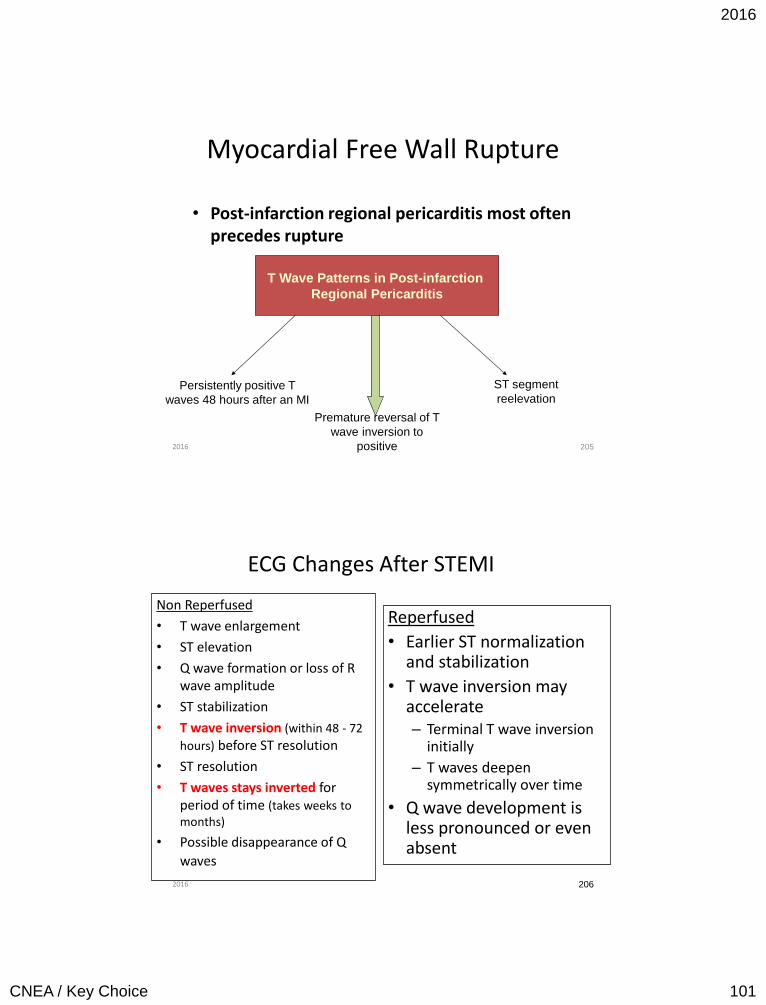
Myocardial Free Wall Rupture
• Post-infarction regional pericarditis most often precedes rupture
205
T Wave Patterns in Post-infarction
Regional Pericarditis
Persistently positive T
waves 48 hours after an MI
Premature reversal of T
wave inversion to
positive
ST segment
reelevation
2016
ECG Changes After STEMI
Non Reperfused
• T wave enlargement
• ST elevation
• Q wave formation or loss of R wave amplitude
• ST stabilization
• T wave inversion (within 48 - 72
hours) before ST resolution
• ST resolution
• T waves stays inverted for period of time (takes weeks to months)
• Possible disappearance of Q
waves
Reperfused
• Earlier ST normalization and stabilization
• T wave inversion may accelerate – Terminal T wave inversion
initially
– T waves deepen symmetrically over time
• Q wave development is less pronounced or even absent
206 2016
2016
CNEA / Key Choice 102
Types of Free Wall Rupture
Within 24 hours: Full thickness rupture.
1 to 3 days post MI: Erosion of myocardium.
Late: At border between MI and normal myocardium.
207 2016
208
• Sudden chest pain associated with coughing or straining.
• Transient bradycardia and other signs and symptoms of increased vagal tone prior to rupture.
• May have signs and symptoms of cardiac tamponade.
• Requires urgent surgical repair. – Resection of the infarcted
area – Closure of the ruptured
area with a patch or with the use of biological glues
• An emergency
pericardiocentesis may be required to stabilize the patient (not a definitive treatment)
2016
2016
CNEA / Key Choice 103
209
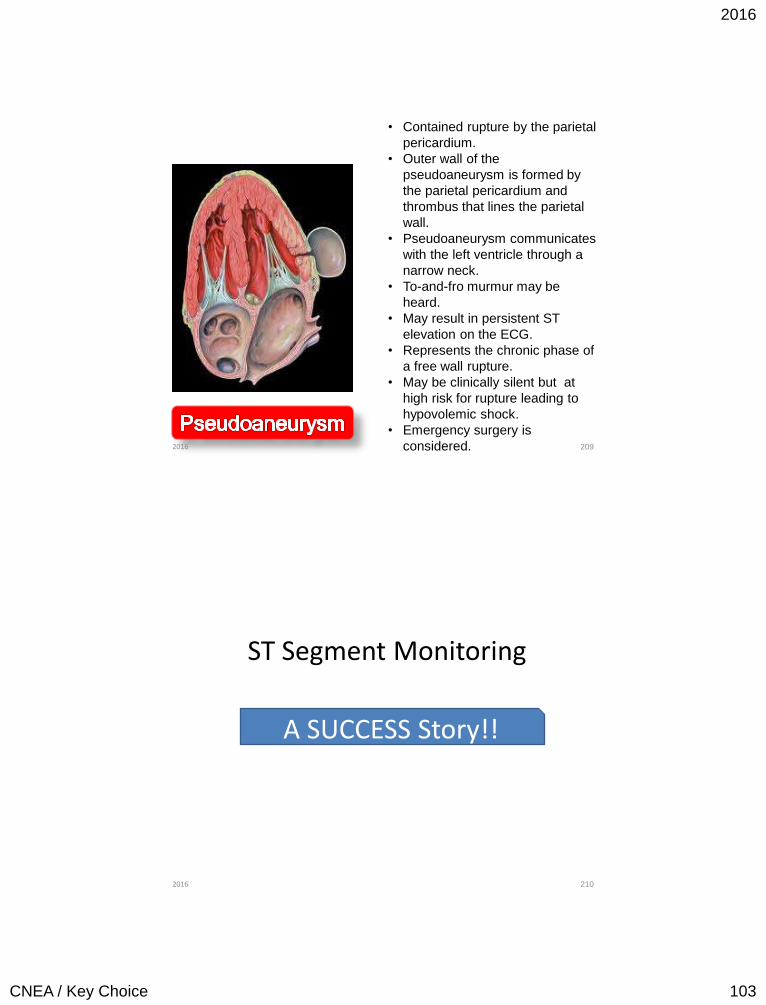
• Contained rupture by the parietal
pericardium.
• Outer wall of the
pseudoaneurysm is formed by
the parietal pericardium and
thrombus that lines the parietal
wall.
• Pseudoaneurysm communicates
with the left ventricle through a
narrow neck.
• To-and-fro murmur may be
heard.
• May result in persistent ST
elevation on the ECG.
• Represents the chronic phase of
a free wall rupture.
• May be clinically silent but at
high risk for rupture leading to
hypovolemic shock.
• Emergency surgery is
considered. 2016
210
ST Segment Monitoring
A SUCCESS Story!!
2016
2016
CNEA / Key Choice 104
211 2016
212 2016
2016
CNEA / Key Choice 105
213 2016
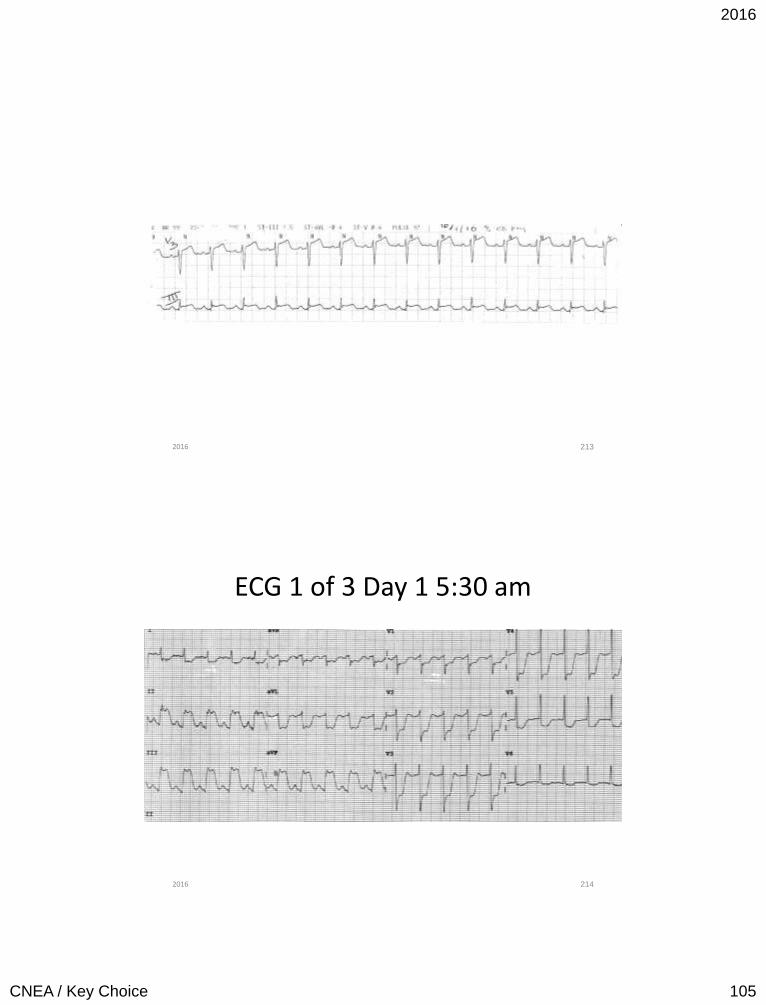
ECG 1 of 3 Day 1 5:30 am
214 2016
2016
CNEA / Key Choice 106
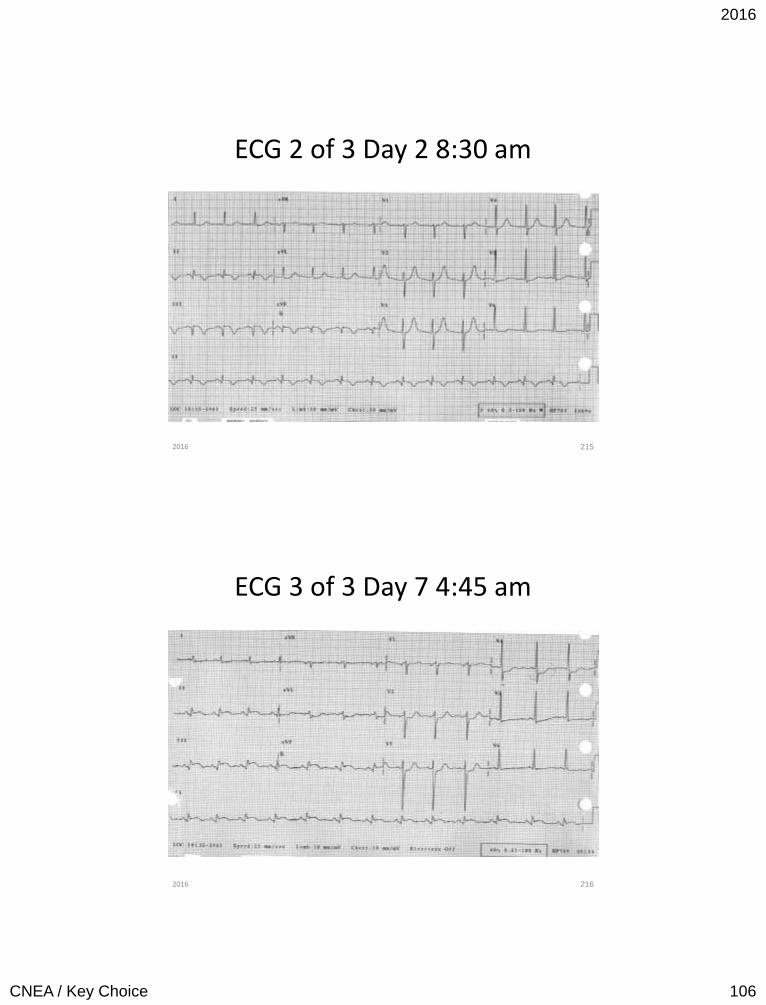
ECG 2 of 3 Day 2 8:30 am
215 2016
ECG 3 of 3 Day 7 4:45 am
216 2016
2016
CNEA / Key Choice 107
Ventricular Septal Rupture
• Without reperfusion average time frame is 5 days (2 to 8 days) post MI
• With fibrinolytic therapy post common time frame is within 24 hours
• Septum receives blood supply from branches of LAD and PDA arteries (apical septum)
• 60% ruptures with anterior MI and 40% with inferior posterior (posterior (inferior-basal)septum)
• Can be one large or a series of smaller defects
217 2016
Ventricular Septal Defect or Rupture
• Timing: Holosystolic
• Location: Left lower sternal border
• Radiation: Widely throughout the precordium
• Configuration: Plateau
• Pitch: High
• Quality: Harsh / Loud
218
New loud
holosystolic
murmur
(+ thrill)
2016
2016
CNEA / Key Choice 108
219 2016
220 220 2016
2016
CNEA / Key Choice 109
Ventricular Septal Defect
Left to Right Shunt
• Poor systemic perfusion
• Right ventricular volume overload
• Heart failure
• Shock
• State of right and left ventricle affect hemodynamic status.
Medical Management
• IABP
• IV nitroprusside for MAP 60 to 75 mmHg.
• Do not reduce pulmonary vascular resistance more than systemic vascular resistance.
Surgical Considerations
• Direct closure or closure with patch
• Higher risk with posterior defects
• Higher mortality when done urgently
• If unstable – morality is higher when surgery delayed
221 2016
222 222 2016
2016
CNEA / Key Choice 110
Papillary Muscle Rupture
223 2016
Papillary Muscle Rupture
5% Acute MI Mortality
Complete transection=death.
Without reperfusion:
2 to 7 days.
Reperfusion era: Median time 13 hours.
224 2016
2016
CNEA / Key Choice 111
225
Vicious Cycle • Acute mitral valve regurgitation Backward flow
Pulmonary edema
• Decreased forward flow Acute decrease in cardiac output
• Increased SVR to compensate
• More blood flow to area of least resistance
• Further decrease in cardiac output further increase in SVR
• Increase in pulmonary edema
• Further decrease in cardiac output Further increase in SVR
225 2016
Systolic Murmurs Mitral Regurgitation
226
New holosystolic murmur: Often radiating to LSB.
OR
May be absent due to equalizing
pressures.
If acute pulmonary edema and shock – suspect papillary muscle rupture or ischemia in
absence of murmur.
2016
2016
CNEA / Key Choice 112
Papillary Muscle Rupture
Medical Management
• Afterload reduction similar to septal rupture.
Surgical Intervention
• Mitral valve repair or replacement required.
• Operative mortality 20% - superior to medical management.
227 2016
228 228
ECG 1of 3
2016
2016
CNEA / Key Choice 113
229 229
ECG 2 of 3
2016
230 230
ECG 3 of 3
2016
2016
CNEA / Key Choice 114
231 231
2016
Emergency Decision Making
232 2016
2016
CNEA / Key Choice 115
Cardiac Tamponade
Risk factors : (Trauma, Post OHS / procedure, MI - lateral wall, HTN during acute phase, late
presentation)
Checklist
√Beck’s triad (hypotension / JVD / muffled heart sounds
√ Pulses Paradoxus
√ Pulses / Electrical Alternans
233 2016
Risk Factors: (Trauma, Conversion to positive pressure ventilation, existing chest tube)
Checklist
√Diminished to absent lung sounds
√Hypotension
√JVD
√Mediastinal shift (very late sign)
234 2016
2016
CNEA / Key Choice 116
Pulmonary Embolus
Risk Factors: (Venous stasis, hypercoagulability, injury to vascular endothelium, any hospitalized patient without pharmacological prophylaxis)
Checklist
√Tachypnea (most common sign)
√Respiratory Alkalosis
√ECG signs: Right axis deviation, RBBB, Tall P waves inferior leads , T wave inversion (limb and precordial leads), Prominent S waves 1 and aVL, S1, Q3, T3
√ST / New atrial arrhythmia
235 2016
Aortic Dissection
Risk Factors: HTN, aortic cannulation, genetic abnormalities, known aortic valve disease, known thoracic aneurysm
Checklist
√Tearing or ripping description of chest or back pain
√Diastolic murmur of aortic regurgitation
√Bilateral arm BP variation
√ 4 extremity pulse variation
√ Neurological deficit or Co-existing Inferior MI
236 2016
2016
CNEA / Key Choice 117
237
Mechanical Complications of MI
• Septal Rupture • Papillary Muscle Rupture
High Risk
• Anteroseptal MI
Check List
• Loud holosystolic murmur
• RV volume overload
• Systemic hypoperfusion
High Risk
• Inferior posterior or posterior MI
Check List
• Holosystolic murmur (can be absent)
• Acute pulmonary edema
2016
238
BE THE BEST THAT YOU CAN BE EVERY DAY. YOUR PATIENTS ARE
COUNTING ON IT!
www.cardionursing.com
2016
2016
CNEA / Key Choice 118
239 2016
UNDERSTANDING WHY WE DO WHAT WE DO
240 2016
2016
CNEA / Key Choice 119
241 2016
Flow is determined by:
√Pressure
√ Resistance
√ Volume 242 2016
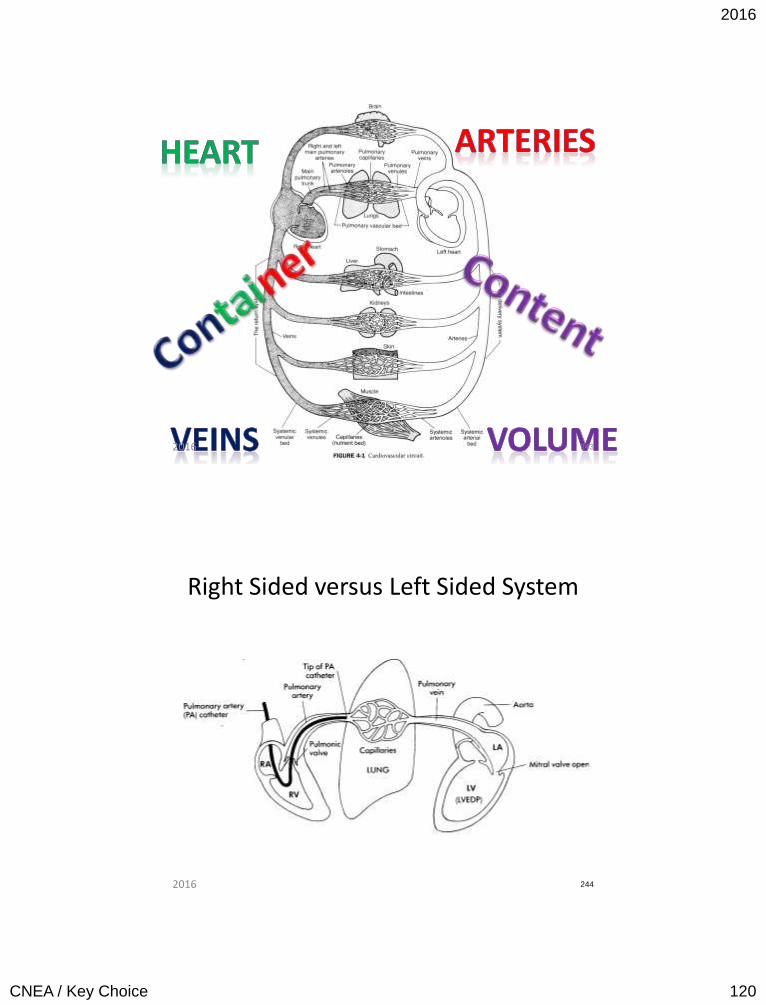
2016
CNEA / Key Choice 120
243 2016
Right Sided versus Left Sided System
244 2016
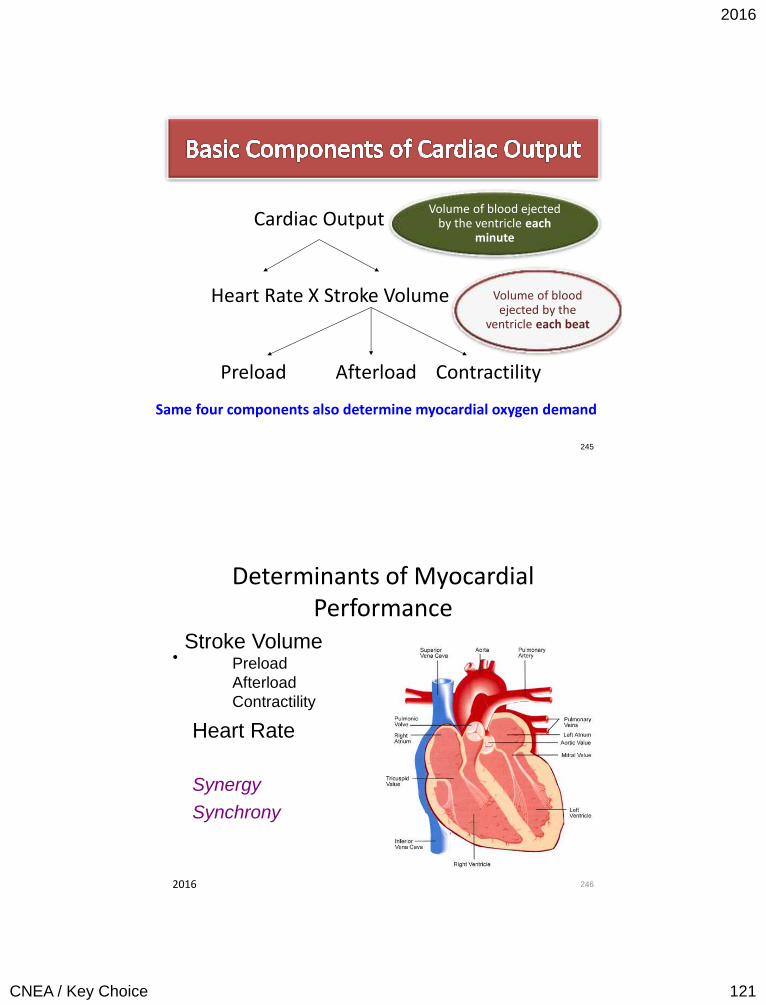
2016
CNEA / Key Choice 121
Cardiac Output
Heart Rate X Stroke Volume Preload Afterload Contractility Same four components also determine myocardial oxygen demand
245
Volume of blood ejected by the ventricle each
minute
Volume of blood ejected by the
ventricle each beat
Determinants of Myocardial Performance
•
246
Heart Rate
Synergy
Synchrony
Stroke Volume Preload
Afterload
Contractility
2016
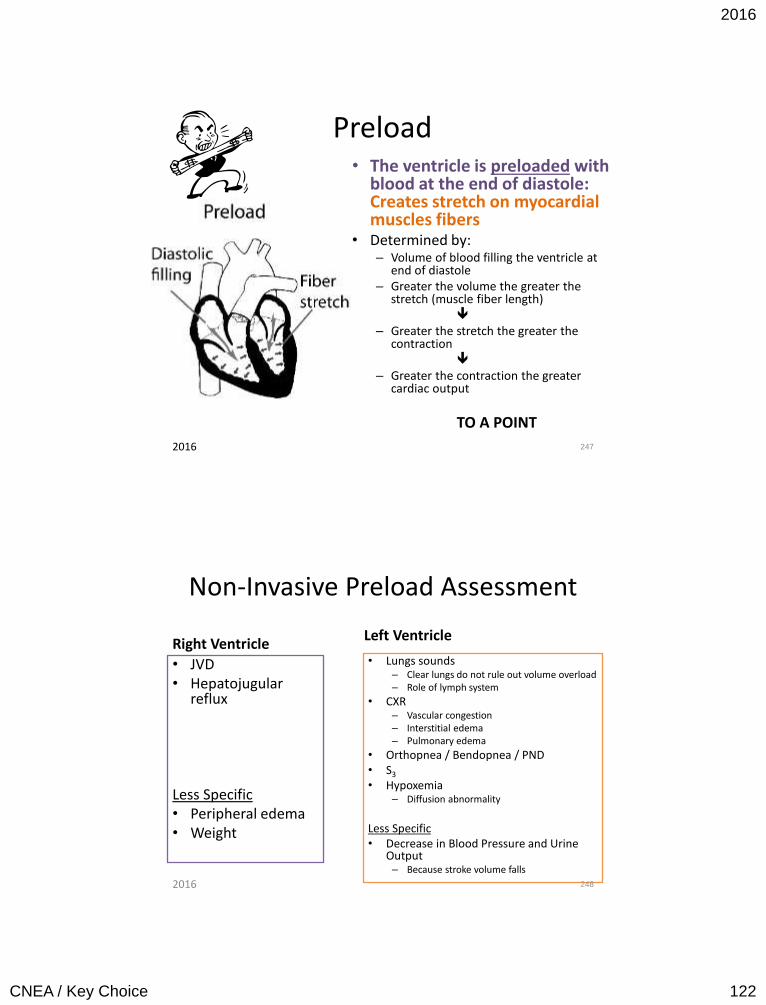
2016
CNEA / Key Choice 122
Preload • The ventricle is preloaded with
blood at the end of diastole: Creates stretch on myocardial muscles fibers
• Determined by: – Volume of blood filling the ventricle at
end of diastole – Greater the volume the greater the
stretch (muscle fiber length) – Greater the stretch the greater the
contraction – Greater the contraction the greater
cardiac output
TO A POINT
247 2016
Non-Invasive Preload Assessment
Right Ventricle
• JVD • Hepatojugular
reflux Less Specific • Peripheral edema • Weight
Left Ventricle
• Lungs sounds – Clear lungs do not rule out volume overload – Role of lymph system
• CXR – Vascular congestion – Interstitial edema – Pulmonary edema
• Orthopnea / Bendopnea / PND • S3
• Hypoxemia – Diffusion abnormality
Less Specific • Decrease in Blood Pressure and Urine
Output – Because stroke volume falls
248 2016
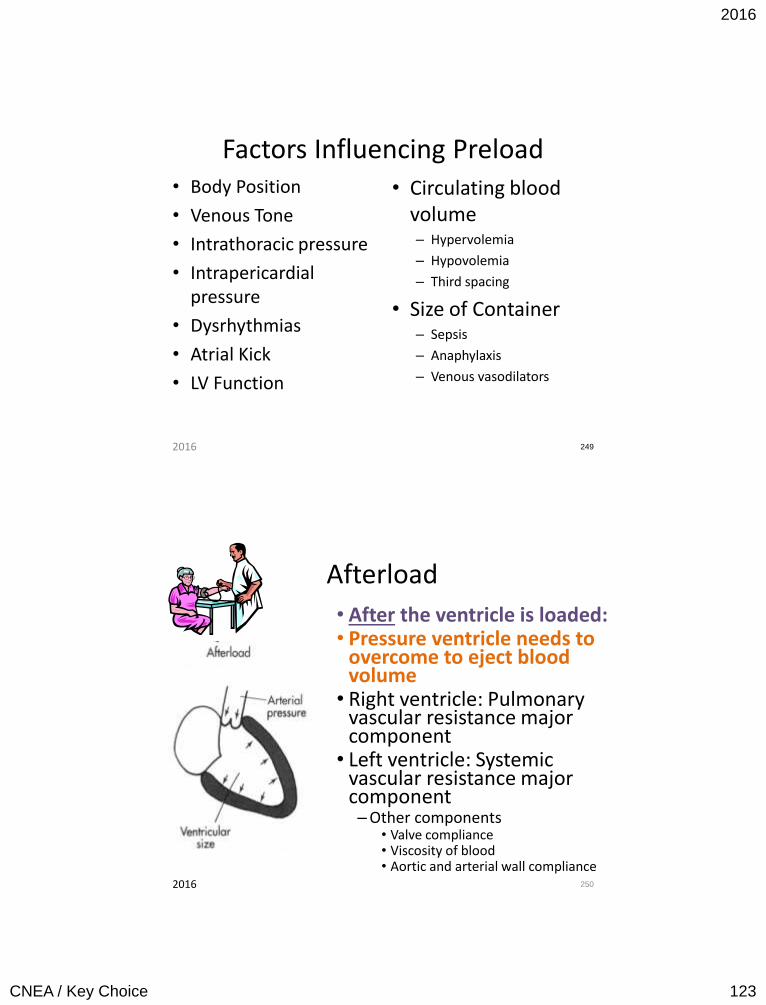
2016
CNEA / Key Choice 123
Factors Influencing Preload • Body Position
• Venous Tone
• Intrathoracic pressure
• Intrapericardial pressure
• Dysrhythmias
• Atrial Kick
• LV Function
• Circulating blood volume – Hypervolemia
– Hypovolemia
– Third spacing
• Size of Container – Sepsis
– Anaphylaxis
– Venous vasodilators
249 2016
Afterload
• After the ventricle is loaded: • Pressure ventricle needs to
overcome to eject blood volume
• Right ventricle: Pulmonary vascular resistance major component
• Left ventricle: Systemic vascular resistance major component – Other components
• Valve compliance • Viscosity of blood • Aortic and arterial wall compliance
250 2016
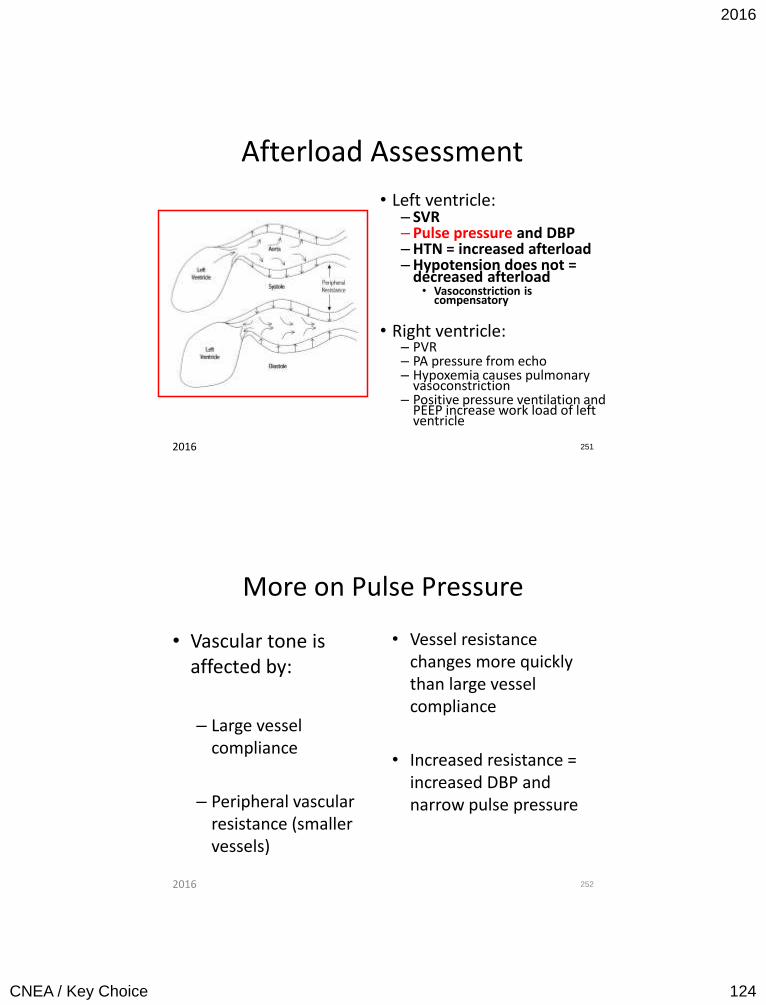
2016
CNEA / Key Choice 124
Afterload Assessment
• Left ventricle: – SVR – Pulse pressure and DBP – HTN = increased afterload – Hypotension does not =
decreased afterload • Vasoconstriction is
compensatory
• Right ventricle: – PVR – PA pressure from echo – Hypoxemia causes pulmonary
vasoconstriction – Positive pressure ventilation and
PEEP increase work load of left ventricle
251 2016
More on Pulse Pressure
• Vascular tone is affected by:
– Large vessel compliance
– Peripheral vascular resistance (smaller vessels)
• Vessel resistance changes more quickly than large vessel compliance
• Increased resistance = increased DBP and narrow pulse pressure
252 2016
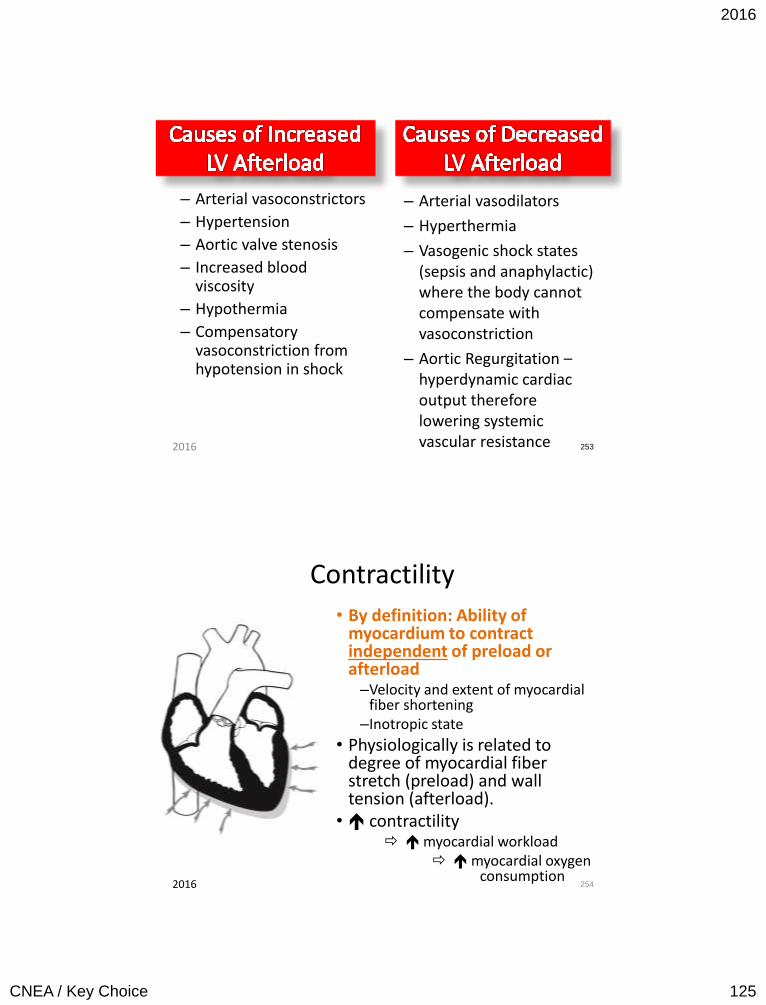
2016
CNEA / Key Choice 125
– Arterial vasoconstrictors
– Hypertension
– Aortic valve stenosis
– Increased blood viscosity
– Hypothermia
– Compensatory vasoconstriction from hypotension in shock
– Arterial vasodilators
– Hyperthermia
– Vasogenic shock states (sepsis and anaphylactic) where the body cannot compensate with vasoconstriction
– Aortic Regurgitation – hyperdynamic cardiac output therefore lowering systemic vascular resistance
253 2016
Contractility
• By definition: Ability of myocardium to contract independent of preload or afterload
–Velocity and extent of myocardial fiber shortening
–Inotropic state
• Physiologically is related to degree of myocardial fiber stretch (preload) and wall tension (afterload).
• contractility myocardial workload myocardial oxygen
consumption
254 2016
2016
CNEA / Key Choice 126
Important Points about Contractility
• No accurate way to measure contractility
• Low cardiac output does not necessarily mean
diminished contractility (i.e. hypovolemia)
• Correct preload and afterload problems first in a patient with a low ejection fraction.
• Increasing contractility with medications will also increase myocardial oxygen demand.
255
Noninvasive Assessment: Ejection Fraction
2016
Factors Altering Contractility
• Decreased contractility
– Excessive preload or afterload
– Drugs – negative inotropes
– Myocardial damage
– Ischemia
– Cardiomyopathy
– Hypothyroidism
– Changes in ionic environment: hypoxia, acidosis or electrolyte imbalance
256
• Increased contractility
– Drugs
• Positive inotropes
– Hyperthyroidism
– Adrenal Medulla Tumor
2016
2016
CNEA / Key Choice 127
Heart Rate
• Mathematically heart rate increases cardiac output
• Physiological limit where increased heart rate will decrease cardiac output due to decreased filling time (decreased preload)
257 2016
Backwards Failure:
Pulmonary Congestion
Forwards Failure:
Hypoperfusion
258 2016

2016
CNEA / Key Choice 128
Warm and Dry
Normal Perfusion
No Congestion
Warm and Wet
Normal Perfusion
Congestion
Cold and Dry
Low Perfusion
No Congestion
Cold and Wet
Low Perfusion
Congestion
259 2016
Treatment
Congestion with Adequate Perfusion
• Reduce Preload
Hypoperfusion with No Congestion
• Increase contractility – Must have adequate
preload
Hypoperfusion with Congestion
• Reduce Afterload
2016 260
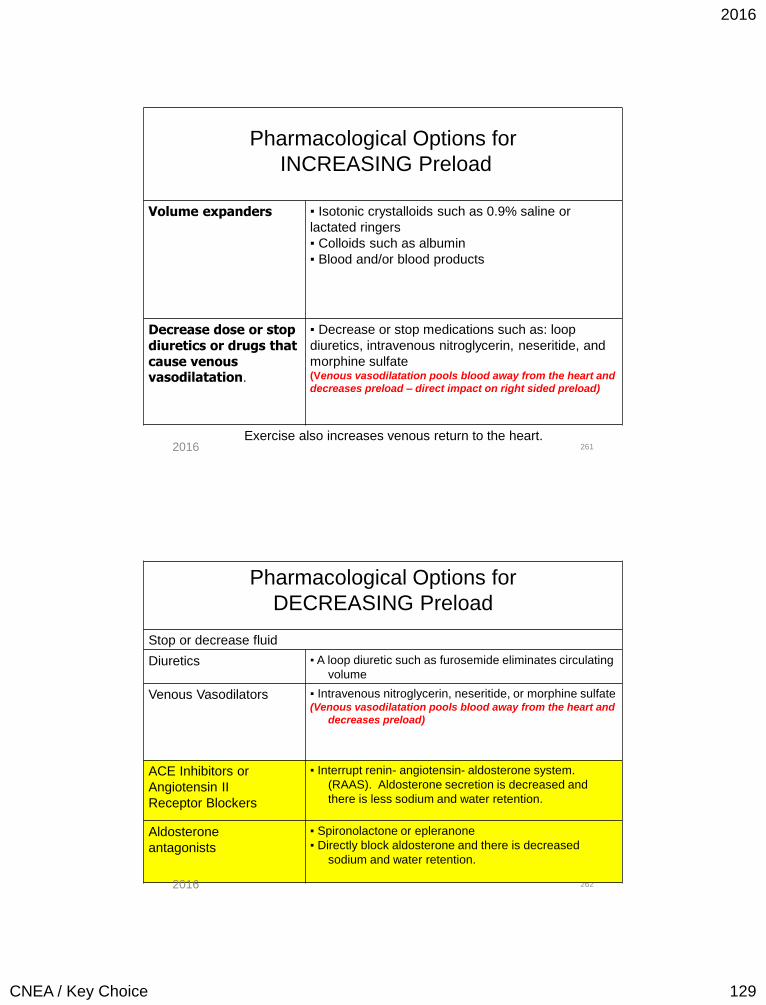
2016
CNEA / Key Choice 129
261
Pharmacological Options for
INCREASING Preload
Volume expanders ▪ Isotonic crystalloids such as 0.9% saline or
lactated ringers
▪ Colloids such as albumin
▪ Blood and/or blood products
Decrease dose or stop diuretics or drugs that cause venous vasodilatation.
▪ Decrease or stop medications such as: loop
diuretics, intravenous nitroglycerin, neseritide, and
morphine sulfate (Venous vasodilatation pools blood away from the heart and
decreases preload – direct impact on right sided preload)
Exercise also increases venous return to the heart. 2016
262
Pharmacological Options for
DECREASING Preload
Stop or decrease fluid
Diuretics ▪ A loop diuretic such as furosemide eliminates circulating
volume
Venous Vasodilators ▪ Intravenous nitroglycerin, neseritide, or morphine sulfate (Venous vasodilatation pools blood away from the heart and
decreases preload)
ACE Inhibitors or
Angiotensin II
Receptor Blockers
▪ Interrupt renin- angiotensin- aldosterone system.
(RAAS). Aldosterone secretion is decreased and
there is less sodium and water retention.
Aldosterone
antagonists
▪ Spironolactone or epleranone
▪ Directly block aldosterone and there is decreased
sodium and water retention.
2016
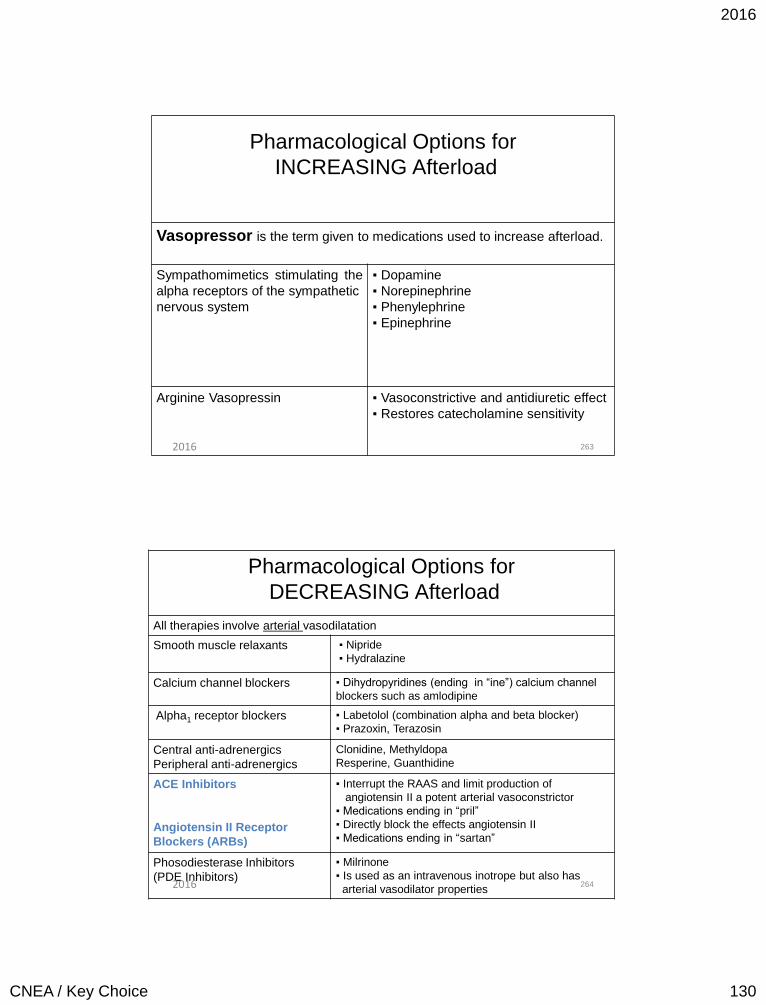
2016
CNEA / Key Choice 130
263
Pharmacological Options for
INCREASING Afterload
Vasopressor is the term given to medications used to increase afterload.
Sympathomimetics stimulating the
alpha receptors of the sympathetic
nervous system
▪ Dopamine
▪ Norepinephrine
▪ Phenylephrine
▪ Epinephrine
Arginine Vasopressin ▪ Vasoconstrictive and antidiuretic effect
▪ Restores catecholamine sensitivity
2016
264
Pharmacological Options for
DECREASING Afterload
All therapies involve arterial vasodilatation
Smooth muscle relaxants ▪ Nipride
▪ Hydralazine
Calcium channel blockers ▪ Dihydropyridines (ending in “ine”) calcium channel
blockers such as amlodipine
Alpha1 receptor blockers
▪ Labetolol (combination alpha and beta blocker)
▪ Prazoxin, Terazosin
Central anti-adrenergics
Peripheral anti-adrenergics
Clonidine, Methyldopa
Resperine, Guanthidine
ACE Inhibitors
Angiotensin II Receptor
Blockers (ARBs)
▪ Interrupt the RAAS and limit production of
angiotensin II a potent arterial vasoconstrictor
▪ Medications ending in “pril”
▪ Directly block the effects angiotensin II
▪ Medications ending in “sartan”
Phosodiesterase Inhibitors
(PDE Inhibitors)
▪ Milrinone
▪ Is used as an intravenous inotrope but also has
arterial vasodilator properties 2016
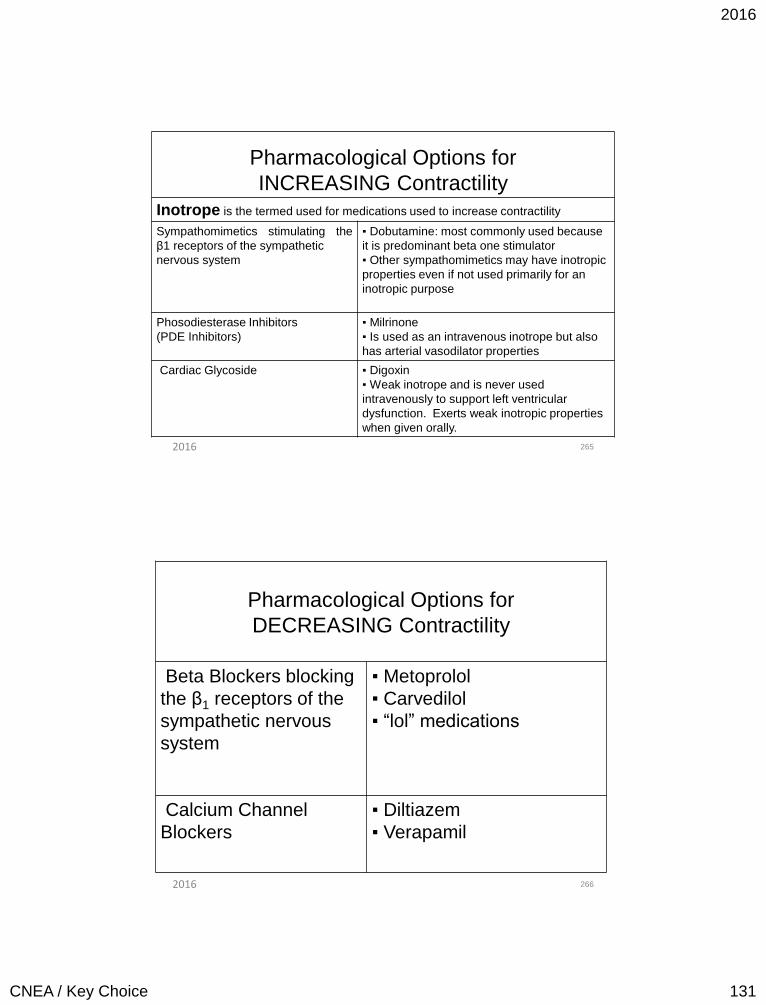
2016
CNEA / Key Choice 131
265
Pharmacological Options for
INCREASING Contractility
Inotrope is the termed used for medications used to increase contractility
Sympathomimetics stimulating the
β1 receptors of the sympathetic
nervous system
▪ Dobutamine: most commonly used because
it is predominant beta one stimulator
▪ Other sympathomimetics may have inotropic
properties even if not used primarily for an
inotropic purpose
Phosodiesterase Inhibitors
(PDE Inhibitors)
▪ Milrinone
▪ Is used as an intravenous inotrope but also
has arterial vasodilator properties
Cardiac Glycoside ▪ Digoxin
▪ Weak inotrope and is never used
intravenously to support left ventricular
dysfunction. Exerts weak inotropic properties
when given orally.
2016
266
Pharmacological Options for
DECREASING Contractility
Beta Blockers blocking
the β1 receptors of the
sympathetic nervous
system
▪ Metoprolol
▪ Carvedilol
▪ “lol” medications
Calcium Channel
Blockers
▪ Diltiazem
▪ Verapamil
2016
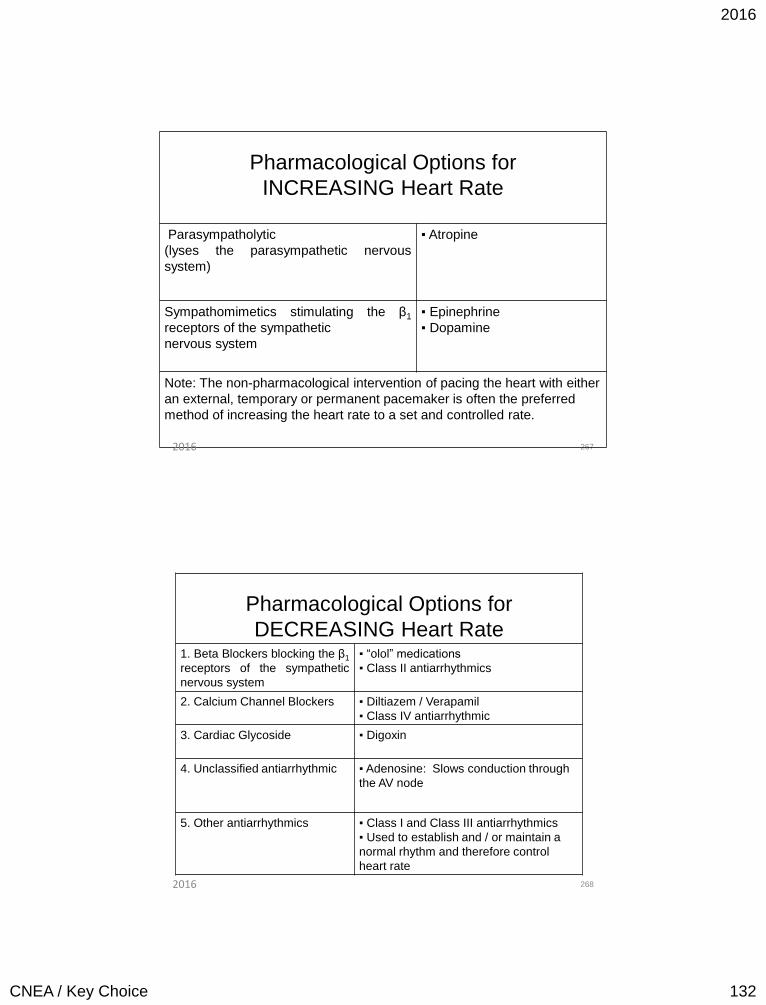
2016
CNEA / Key Choice 132
267
Pharmacological Options for
INCREASING Heart Rate
Parasympatholytic
(lyses the parasympathetic nervous
system)
▪ Atropine
Sympathomimetics stimulating the β1
receptors of the sympathetic
nervous system
▪ Epinephrine
▪ Dopamine
Note: The non-pharmacological intervention of pacing the heart with either
an external, temporary or permanent pacemaker is often the preferred
method of increasing the heart rate to a set and controlled rate.
2016
268
Pharmacological Options for
DECREASING Heart Rate 1. Beta Blockers blocking the β1
receptors of the sympathetic
nervous system
▪ “olol” medications
▪ Class II antiarrhythmics
2. Calcium Channel Blockers ▪ Diltiazem / Verapamil
▪ Class IV antiarrhythmic
3. Cardiac Glycoside ▪ Digoxin
4. Unclassified antiarrhythmic ▪ Adenosine: Slows conduction through
the AV node
5. Other antiarrhythmics ▪ Class I and Class III antiarrhythmics
▪ Used to establish and / or maintain a
normal rhythm and therefore control
heart rate
2016
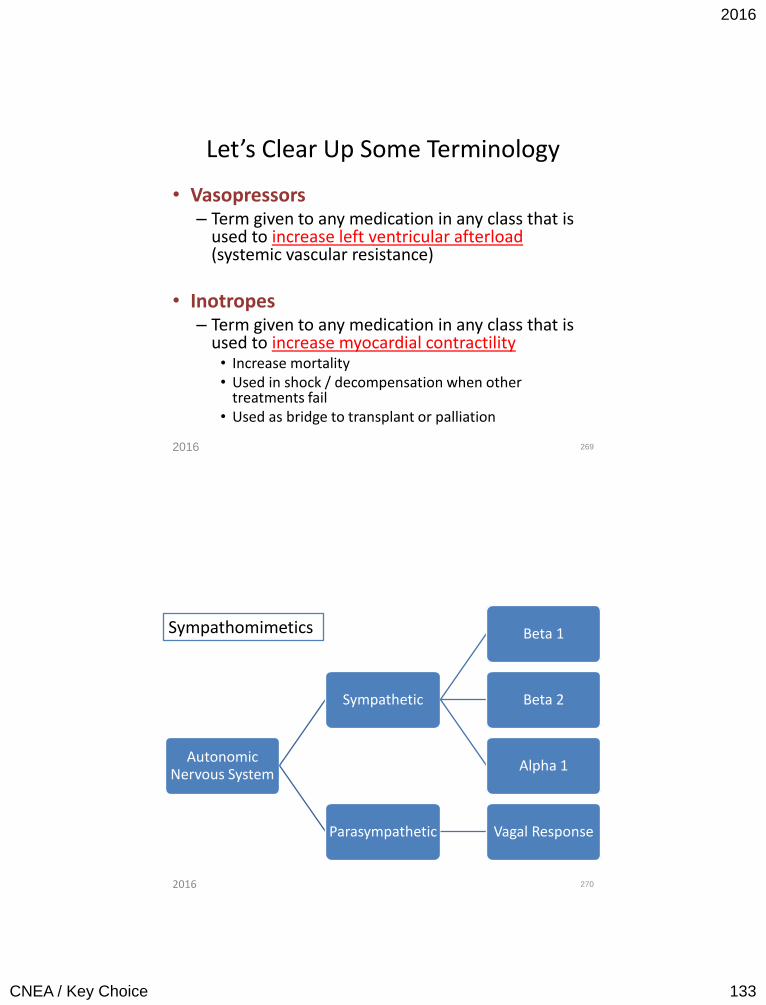
2016
CNEA / Key Choice 133
Let’s Clear Up Some Terminology
• Vasopressors – Term given to any medication in any class that is
used to increase left ventricular afterload (systemic vascular resistance)
• Inotropes – Term given to any medication in any class that is
used to increase myocardial contractility • Increase mortality • Used in shock / decompensation when other
treatments fail • Used as bridge to transplant or palliation
269 2016
Autonomic Nervous System
Sympathetic
Beta 1
Beta 2
Alpha 1
Parasympathetic Vagal Response
270
Sympathomimetics
2016
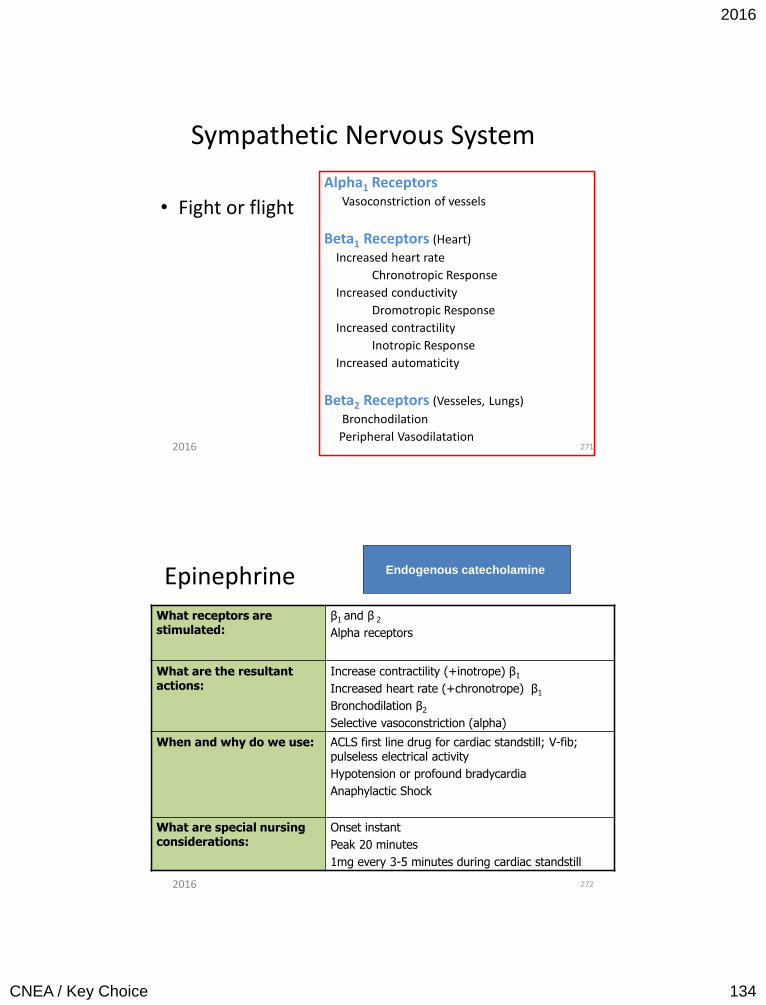
2016
CNEA / Key Choice 134
Sympathetic Nervous System
• Fight or flight
Alpha1 Receptors Vasoconstriction of vessels
Beta1 Receptors (Heart)
Increased heart rate
Chronotropic Response
Increased conductivity
Dromotropic Response
Increased contractility
Inotropic Response
Increased automaticity
Beta2 Receptors (Vesseles, Lungs)
Bronchodilation
Peripheral Vasodilatation 271 2016
Epinephrine
What receptors are stimulated:
β1 and β 2
Alpha receptors
What are the resultant actions:
Increase contractility (+inotrope) β1
Increased heart rate (+chronotrope) β1
Bronchodilation β2
Selective vasoconstriction (alpha)
When and why do we use: ACLS first line drug for cardiac standstill; V-fib; pulseless electrical activity
Hypotension or profound bradycardia
Anaphylactic Shock
What are special nursing considerations:
Onset instant
Peak 20 minutes
1mg every 3-5 minutes during cardiac standstill
272
Endogenous catecholamine
2016
2016
CNEA / Key Choice 135
Dobutamine
273
What receptors are stimulated:
Primarily β1
Some alpha1 receptor stimulation
Some β2 stimulation
Modest β2 (more β2 than alpha1)
What are the resultant actions:
Increase contractility (+ inotrope) (β1)
Increase AV node conduction
Modest vasodilation
When and why do we use: Used as an inotrope (resultant preload reduction) with modest afterload reduction
(ACC / AHA Guidelines for Heart Failure*)
What are special nursing considerations:
Onset 1 to 2 minutes; Peak 10 minutes
Half-life 2 minutes
Note: Blood pressure response is variable; β2 causes vasodilatation; β1 increases cardiac output and may increase BP
Synthetic Compound
2016
274 2016
2016
CNEA / Key Choice 136
2016 275
Continuous intravenous dobutamine is associated with an increased risk of death in patients with advanced heart failure: Insights from the Flolan International Randomized Survival Trial (FIRST)
Intermittent dobutamine treatment in patients with chronic refractory congestive heart failure: a randomized, double-blind, placebo-controlled study. (PMID:9663183) Intermittent dobutamine infusions in patients with refractory CHF have no effect on the need for hospitalization or on survival.
Dopamine
What receptors are stimulated:
Dopaminergic at low doses (0.5-2.0 mcg/kg/min)
β1 also at moderate doses ( 2.0-10.0 mcg/kg/min)
Pure alpha stimulation at high doses > 10mcg/kg/min
What are the resultant actions:
Increase GFR at low doses
Increase contractility at moderate doses (greater effects on contractility than heart rate)
Vasoconstriction (alpha) at high doses
When and why do we use:
Refractory hypotension / shock
* Not indicated for routine treatment or prevention of acute renal failure
What are special nursing considerations:
VT, atrial tachyarrhythmias
Onset 1-2 minutes; Peak 10 minutes
Maximal effects @20/mcg/kg/min
Large IV line or central line
Phentolamine for extravasation: 5 to 10 mg diluted in 10ml 0.9 NS, inject into area with fine needle
Leave cannula and needle in place, aspirate not flush line, dry warm compress 276
Mimics endogenous dopamine;
metabolic precursor
of norepinephrine and epinephrine
2016
2016
CNEA / Key Choice 137
Norepinephrine What receptors are stimulated:
Primarily alpha stimulation
Some β1
(In lower doses β1 can be more dominant)
What are the resultant actions:
Potent vasoconstrictor (increased afterload)
Some increased contractility (+inotrope)
When and why do we use: Refractory hypotension / shock
(used as a vasopressor but will have inotropic properties)
What are special nursing considerations:
Onset: rapid; very short half-life
Duration 1-2 minutes (BP checks q2 minutes while titrating)
Large IV line or central line
Phentolamine for extravasation: 5 to 10 mg diluted in 10ml 0.9 NS, inject into area with fine needle
Leave cannula and needle in place, aspirate not flush line, dry warm compress
277
Endogenous precursor
of epinephrine
2016
Phenylephrine
What receptors are stimulated:
Direct effect: Dominant alpha stimulation
No substantial β1 effect at therapeutic doses
Indirect effect: Releases norepinephrine
What are the resultant actions:
Vasoconstriction (increased afterload)
When and why do we use: As a vasopressor for Unresponsive hypotension
What are special nursing considerations:
Pressor effect occurs almost immediately
Persists for 10 to 15 minutes
278
Synthetic compound
2016
2016
CNEA / Key Choice 138
Pearls for Practice
• Titrate up based on onset of action & peak action
• Wean based on duration of action / half life
• Consider systolic, diastolic, pulse pressure and mean
• Vasoconstriction with a reduced ejection fraction increases work load of failing left ventricle!
279 2016
Comparison of Dopamine to Norepinephrine in Shock
280
• Backer et al. • Multi Center Randomized
Controlled Trial • New England Journal of
Medicine • March 4th 2010
• There were no significant differences between the groups in the rate of death at 28 days or in the rates of death in the ICU, in the hospital, at 6 months, or at 12 months
• More patients with arrhythmia in the dopamine group
• Rate of death was higher in predefined subgroup analysis for patients with cardiogenic shock treated with dopamine.
2016
2016
CNEA / Key Choice 139
Arginine Vasopressin: Non Sympathomimetic Vasopressor
• Vasoconstrictive effects – Allowing for regional
vasodilation
• Antidiuretic effects • Restoration of
catecholamine sensitivity
• Low dose exogenous – 0.04 units / min
• Use in refractory shock – Also consider
methylene blue – Also consider adrenal
insufficiency • Hydrocortisone
281 2016
Milrinone: Phosphodiesterase Inhibitors
• Creates + inotropic effect by increasing availability of calcium • Inhibits the degradation of
cyclic AMP which is indirectly responsible for increasing the influx of calcium through the calcium channel
• Smooth muscle relaxant (venous and arterial vasodilator)
• Indications: – Refractory heart failure
(can be used in combination with dobutamine)
– Left ventricular failure in MI
– Patients waiting transplant
• Side Effects: – Ventricular arrhythmias – Atrial tachyarrhythmias
• Nursing Considerations: – Onset IV: Immediate – Peak: 10 minutes
282 2016
2016
CNEA / Key Choice 140
Milrinone
283
Used as an
Inotrope
BUT…..
Also has……
Preload
Reduction
Afterload
Reduction
2016
OPTIME Trial
• Milrinone approved by FDA based on hemodynamic data • Future trials need to address outcome data • OPTIME
– Prospective trial, randomized, placebo controlled – 951 patients – Patients had indication for but not all required inotrope for end
organ perfusion. – Results: No difference in LOS, No difference in subjective
improvement – Treatment failures more common in milrinone group due to
hypotension, more atrial fibrillation in milrinone – Not powered for mortality differences
– Conclusion: Hemodynamic improvement does not translate into clinical improvement
284 2016
2016
CNEA / Key Choice 141
A Closer Look at Venous Versus Arterial Vasodilators
285
Venous
Vasodilators
Arterial
Vasodilators
2016
A Closer Look at Venous Versus Arterial Vasodilators
• Some medications do both
• Some depend on dose • Nesiritide
• NTG
• Nitroprusside
• CA Channel blockers
• PDE Inhibitors
• ACE Inhibitors
• Other Vasodilators
286 2016
2016
CNEA / Key Choice 142
Nesiritide (Natrecor) • Recombinant form of
human B type natriuretic peptide (BNP)
– BNP is a naturally occurring
cardiac neurohormone secreted by the heart in the body’s response to heart failure
– BNP allows the heart to
participate in the regulation of vascular tone and extracellular volume status
– The BNP system and the renin-angiotensin system counteract each other in heart failure
– BNP levels are elevated in
heart failure
287
Onset: 15 minutes Peak: Within an hour
2016
Nesiritide (Natrecor)
• Balanced arterial and venous vasodilatation
– Causes rapid reduction in right and left sided ventricular filling pressures (preload reduction)
– Reduces afterload
• Indicated for acutely decompensated heart failure patients who have dyspnea at rest
288
• Patient must have systolic BP > 90 mmHg
• PAOP should be estimated to be > 20 mmHg
2016
2016
CNEA / Key Choice 143
Nesiritide (Natrecor) • Given by IV bolus and
maintenance infusion
• Bolus 2mcg/kg
• Infusion 0.01mcg/kg/min - usually 24-48 hours
• Caution with higher doses
289
Monitor BP, hemodynamic assessment,
urine output, and renal function closely
during administration.
• Prime IV tubing with 5 ml of solution – prior to bolus or infusion
• Bolus to be taken from reconstituted IV bag and not from vial)
2016
Neseritide: Where do we stand?
• Sackner-Bernstein JD, Kowalski M, Fox M, Aaronson K: Short-term risk of death after treatment with nesiritide for decompensated heart failure: a pooled analysis of randomized controlled trials. JAMA 2005, 293:1900-1905.
– In the 3 trials, 485 patients were randomized to nesiritide
and 377 to control therapy. Death within 30 days tended to occur more often among patients randomized to nesiritide therapy (35 [7.2%] of 485 vs 15 [4.0%] of 377 patients; risk ratio from meta-analysis.
– P value did not achieve .05 or less.
290 2016
2016
CNEA / Key Choice 144
Randomized Trial • Effect of Nesiritide in Patients with Acute Decompensated
Heart Failure • O'Connor et al. • July 7 2011
• 7141 patients
• Nesiritide was not associated with an increase or a decrease in the rate of death and rehospitalization.
• It was not associated with a worsening of renal function, but it was associated with an increase in rates of hypotension.
• Neseritide cannot be recommended for routine use.
291 2016
Nitroglycerin
• Minimal mortality benefit – Nitrates may be more helpful in patients > 70 years in reduction
of death and heart failure @ 6 month follow up
• Symptom benefit
• Mixed venous and arterial vasodilator – Dosage < 1mcg/kg/min = venous vasodilator
• Decrease preload
– Dosage > 1mcg/kg/min = arterial and venous vasodilator • Decrease preload and afterload
– Sublingual tablets provide high enough dosage to dilate arteries and veins
• Decrease preload and afterload 292
Mortality reducing agents should always take precedence over non mortality reducing agents: I.E. Beta blockers precede nitrate use
2016
2016
CNEA / Key Choice 145
Nitrate Contraindications
• Systolic BP < 90 mm Hg or < 30 mm Hg below baseline
• Bradycardia < 50 BPM
• Tachycardia > 100 BPM (in absence of clinical HF)
• Right ventricular infarct
• Within 24 hours of sildenafil
• Within 48 hours of taldalafil
293
Question female patients: Pulmonary HTN
2016
Nitroglycerin • Onset IV: 1-2 minutes • Duration: 3-5 minutes
• Side Effects: H/A, Hypotension, flushing
Treat H/A with pain meds and decrease dose
• Pain activates the SNS
• Caution: Severe diastolic dysfunction
– Hypertrophic cardiomyopathy – Severe aortic stenosis
294 2016
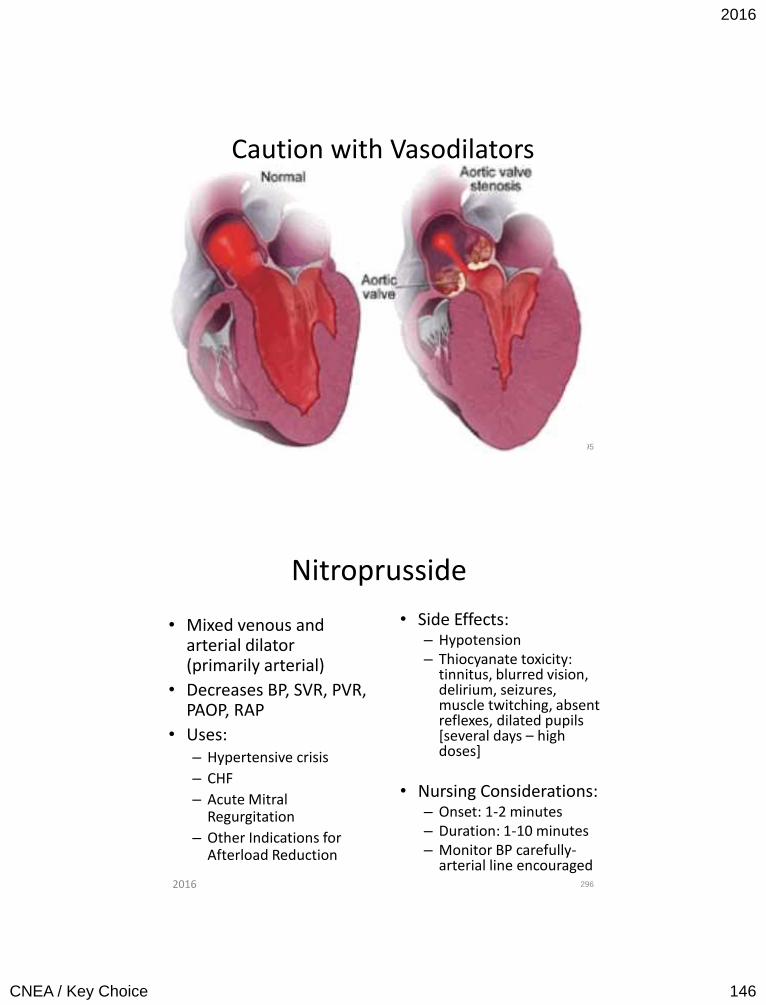
2016
CNEA / Key Choice 146
Caution with Vasodilators
2016 295
Nitroprusside
• Mixed venous and arterial dilator (primarily arterial)
• Decreases BP, SVR, PVR, PAOP, RAP
• Uses: – Hypertensive crisis
– CHF
– Acute Mitral Regurgitation
– Other Indications for Afterload Reduction
• Side Effects: – Hypotension – Thiocyanate toxicity:
tinnitus, blurred vision, delirium, seizures, muscle twitching, absent reflexes, dilated pupils [several days – high doses]
• Nursing Considerations: – Onset: 1-2 minutes – Duration: 1-10 minutes – Monitor BP carefully-
arterial line encouraged
296 2016
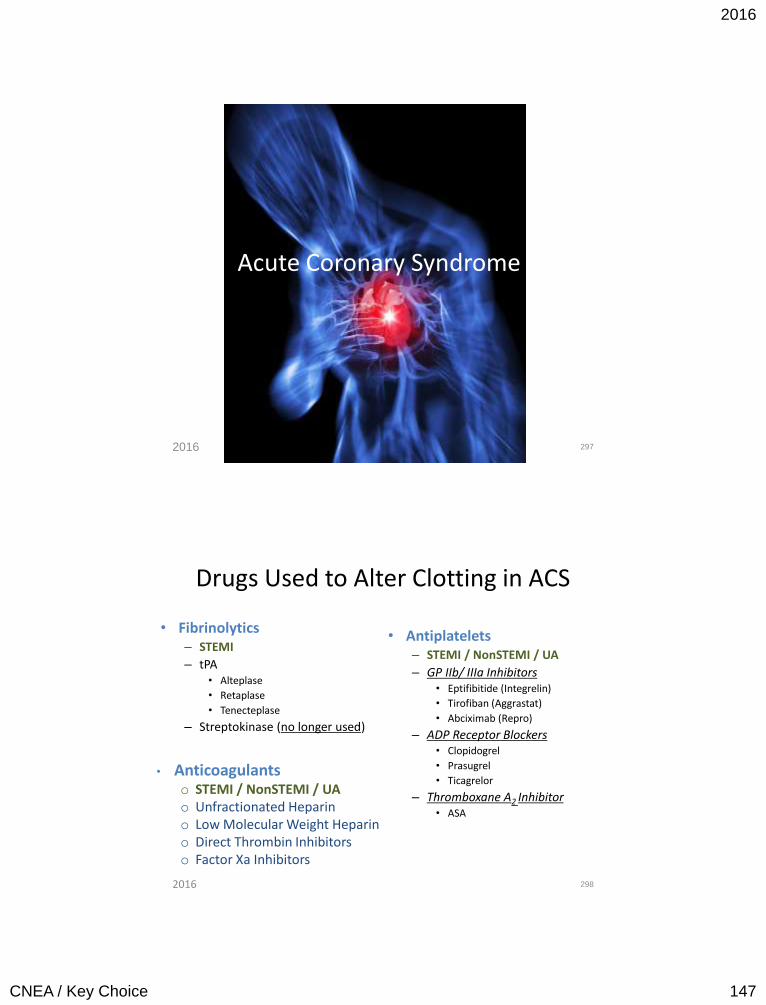
2016
CNEA / Key Choice 147
Acute Coronary Syndrome
297 2016
Drugs Used to Alter Clotting in ACS
• Fibrinolytics – STEMI
– tPA • Alteplase
• Retaplase
• Tenecteplase
– Streptokinase (no longer used)
• Antiplatelets – STEMI / NonSTEMI / UA
– GP IIb/ IIIa Inhibitors • Eptifibitide (Integrelin)
• Tirofiban (Aggrastat)
• Abciximab (Repro)
– ADP Receptor Blockers • Clopidogrel
• Prasugrel
• Ticagrelor
– Thromboxane A2 Inhibitor • ASA
298
• Anticoagulants o STEMI / NonSTEMI / UA o Unfractionated Heparin o Low Molecular Weight Heparin o Direct Thrombin Inhibitors o Factor Xa Inhibitors
2016
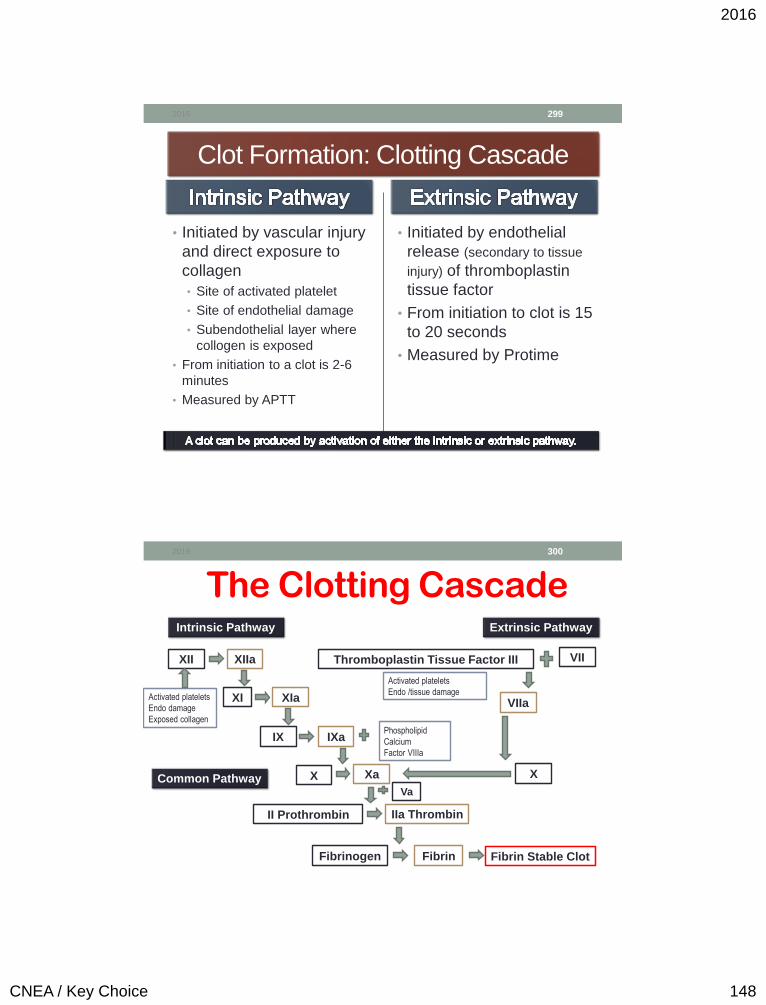
2016
CNEA / Key Choice 148
Clot Formation: Clotting Cascade
• Initiated by vascular injury
and direct exposure to
collagen
• Site of activated platelet
• Site of endothelial damage
• Subendothelial layer where
collogen is exposed
• From initiation to a clot is 2-6
minutes
• Measured by APTT
• Initiated by endothelial
release (secondary to tissue
injury) of thromboplastin
tissue factor
• From initiation to clot is 15
to 20 seconds
• Measured by Protime
2016 299
2016 300
The Clotting Cascade Intrinsic Pathway Extrinsic Pathway
XII XIIa
XI XIa
IX IXa
X Xa
Va
II Prothrombin IIa Thrombin
Fibrinogen Fibrin
VII Thromboplastin Tissue Factor III
VIIa
X
Activated platelets
Endo damage
Exposed collagen
Activated platelets
Endo /tissue damage
Phospholipid
Calcium
Factor VIIIa
Common Pathway
Fibrin Stable Clot
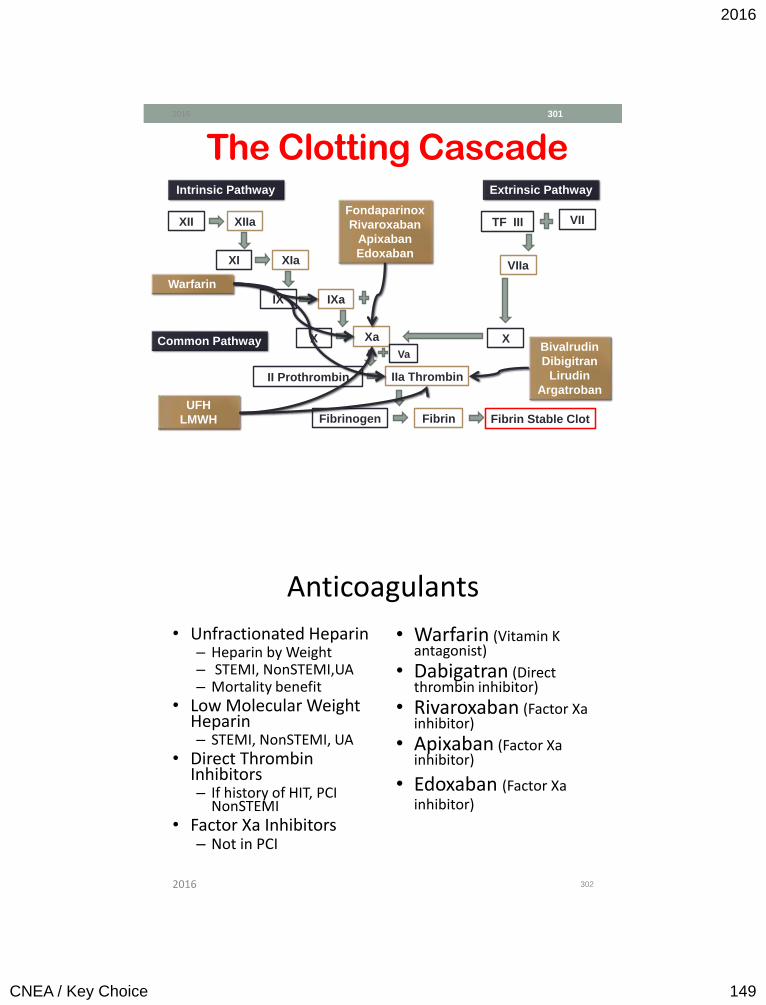
2016
CNEA / Key Choice 149
2016 301
The Clotting Cascade Intrinsic Pathway Extrinsic Pathway
XII XIIa
XI XIa
IX IXa
X Xa
Va
II Prothrombin IIa Thrombin
Fibrinogen Fibrin
VII TF III
VIIa
X Common Pathway
Fibrin Stable Clot
Warfarin
UFH
LMWH
Bivalrudin
Dibigitran
Lirudin
Argatroban
Fondaparinox
Rivaroxaban
Apixaban
Edoxaban
Anticoagulants
• Unfractionated Heparin – Heparin by Weight – STEMI, NonSTEMI,UA – Mortality benefit
• Low Molecular Weight Heparin – STEMI, NonSTEMI, UA
• Direct Thrombin Inhibitors – If history of HIT, PCI
NonSTEMI • Factor Xa Inhibitors
– Not in PCI
• Warfarin (Vitamin K antagonist)
• Dabigatran (Direct thrombin inhibitor)
• Rivaroxaban (Factor Xa inhibitor)
• Apixaban (Factor Xa inhibitor)
• Edoxaban (Factor Xa inhibitor)
302 2016
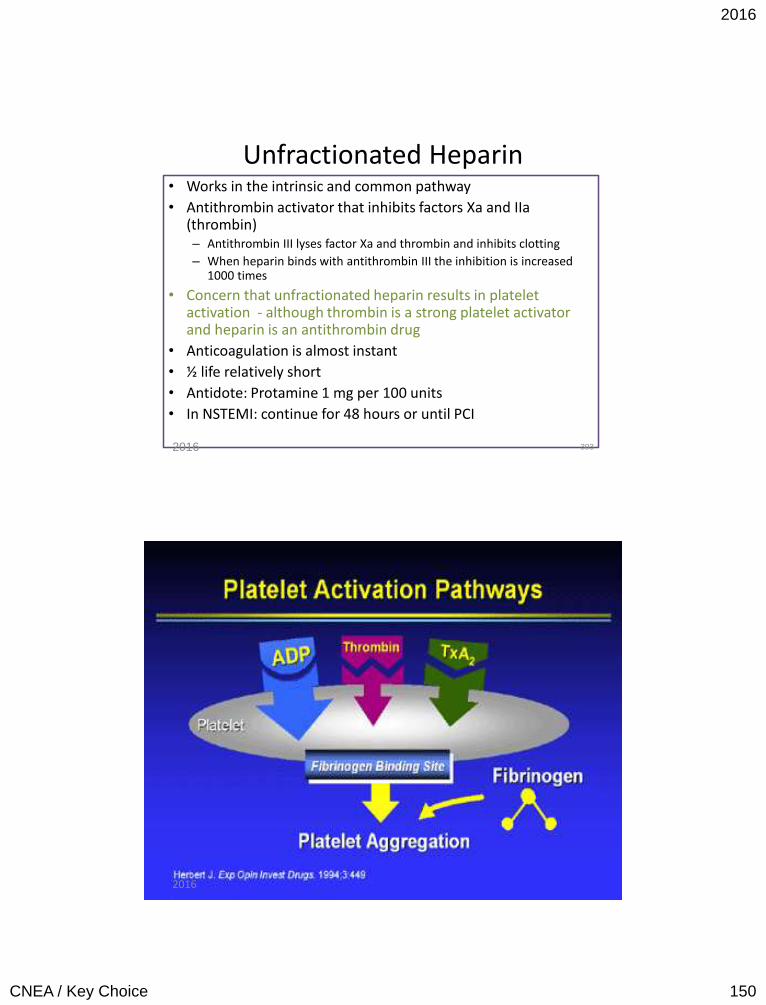
2016
CNEA / Key Choice 150
Unfractionated Heparin • Works in the intrinsic and common pathway
• Antithrombin activator that inhibits factors Xa and IIa (thrombin) – Antithrombin III lyses factor Xa and thrombin and inhibits clotting
– When heparin binds with antithrombin III the inhibition is increased 1000 times
• Concern that unfractionated heparin results in platelet activation - although thrombin is a strong platelet activator and heparin is an antithrombin drug
• Anticoagulation is almost instant
• ½ life relatively short
• Antidote: Protamine 1 mg per 100 units
• In NSTEMI: continue for 48 hours or until PCI
2016 303
304 2016
2016
CNEA / Key Choice 151
More About Heparin • Different dose and aPTT for ACS versus venous thrombotic event
• aPTT (activated partial thromboplastin time) is used to monitor effectiveness and safety • Goal is aPTT 1.5 -2Xs the control
• Weight based heparin dosing reaches goal 90% of time compared to 77% with standard therapy
• OR – Anti factor Xa levels • 0.3-0.7 IU/ml
• Baseline aPTT, PT/INR, platelets and CBC
• Increased bleeding can occur with renal failure • Heparin has dual clearance mechanism
2016 305
Complications of Heparin
• Bleeding • Mild thrombocytopenia – HIT 1
• Mild thrombocytopenia occurs in 10-20% of patients
• Severe thrombocytopenia – HIT 2 • occurs in 1-2% of patients • Heparin Induced Thrombocytopenia (HIT) • Platelet aggregation resulting in venous or arterial
thrombosis (HITT – Thrombocytopenia with thrombosis) • Determining patients at risk is unpredictable • Generally occurs 5 to 10 days after initiation of heparin
• Could be sooner if recent exposure to heparin • DC heparin if platelets fall below 100,000 (or > 50%
reduction from baseline) • Severe thrombocytopenia is due to an immune response
2016 306
2016
CNEA / Key Choice 152
More on Heparin Induced
Thrombocytopenia • Immune system forms antibodies against heparin when bound to protein
platelet factor 4 [PF4] – antibodies bind to PF4-heparin complexes and induce platelet activation
• Immunoassay identify antibodies against PF4
• Detected in ELISA testing
• Function Assay
• Heparin-induced platelet aggregation assay (HIPA)
• Platelet activation test
• HIT antibodies are usually IgG class
• Take 5 days to form
• IgG antibodies associated with platelet activation and increased thrombin generation
• Antibodies not necessarily associated with thrombotic risk
• Can disappear 3 months after exposure
• Antibodies bind to platelets and trigger the development of thrombosis.
2016 307
Treatment of HIT 1. Discontinue and avoid all heparin.
2. Give a non-heparin alternative anticoagulant: Direct thrombin inhibitors.
3. Postpone warfarin pending substantial platelet count recovery (give vitamin K if warfarin has already been started). Warfarin is associated with protein C deficiency and increased risk for microthrombosis
4. Avoid platelet transfusions – leads to platelet activation.
5. Test for HIT antibodies (ELISA and washed assay)
6. Investigate for lower-limb deep-vein thrombosis.
2016 308

2016
CNEA / Key Choice 153
• Enoxaparin, dalteparin, tinzaparin, and nadroparin
• Smaller in size • Antithrombin by inhibiting factor Xa • Causes less inactivation of thrombin and less bleeding than standard heparin
• More predictable anticoagulant response • No need to monitor APTT
• Anti Xa levels can be drawn 4 hours after SQ dose
• Lower incidence of heparin induced thrombocytopenia • Less platelet activation concern than with UFH
2016 309
Low Molecular Weight Heparin
Low Molecular Weight Heparin
• Can be self administered with Sub – Q administration
• ½ life 4-6 hours
• Protamine reverses 60% of drug effect
• Renal failure results in increased risk of bleeding because
LMWH is renally cleared • Special dosing for chronic renal insufficiency with enoxaparin
2016 310
2016
CNEA / Key Choice 154
Enoxaparin Dosing
• Prevention of DVT • 40 mg SC daily in most situations
• 30 mg SC daily for renal adjustment (CR Clearance < 30 ml/min)
• NSTE-ACS (or as adjunct in STEMI) • 1 mg/kg SC q12 hours
• 1mg/kg SC daily if CR Clearance < 30 ml/min
• IV loading dose of 30 mg – in select patients
• Continued for duration of stay or until PCI
• Embolism with Atrial Fib • 1 mg/kg SC q12 hours
• Venous thrombosis / DVT • 1mg/kg SC q12 or 1.5 mg/kg daily depending of specific
circumstances
2016 311
Enoxaparin Administration
• Full length of 27 gauge ½ needle (prepackaged) should be injected
• Skin fold held until needle withdrawn
• Use anterolateral or posterorlateral walls of abdomen
• Rotate sites frequently
• Do not massage site
2016
CNEA / Key Choice 155
Direct Thrombin Inhibitor
• Ability to inactivate fibrin bound thrombin
• Less binding to plasma proteins, therefore more reliable anticoagulation effect
• Indications
• HIT /HITT
• Approved in NSTE-ACS (Use only in patients with early invasive strategy) / PCI • Non inferior to heparin with a
GPIIb/IIIa with less bleeding
• Monitor in the cath lab with ACT
• Lipirudin / desirudin (hirudin)
• Argatroban
• Bivalirudin* • 0.10 mg/kg loading
• 0.25 mg/kg per hour
• Until diagnostic angiography or PCI is performed
2016 313
• Neutralizes Factor Xa and interrupts the clotting cascade
• Does not inhibit thrombin
• No reported HIT / HITT
• Indications • Venous thromboembolism and PE
• DVT prophylaxis
• ACS
• Contraindicated in severe renal dysfunction • No laboratory monitoring is needed – PT/aPTT not sensitive
• No antidote (Recombinant factor VIIa can help reverse anticoagulation effect)
2016 314
Synthetic Factor Xa Inhibitor
Fondaparinux (Arixtra)
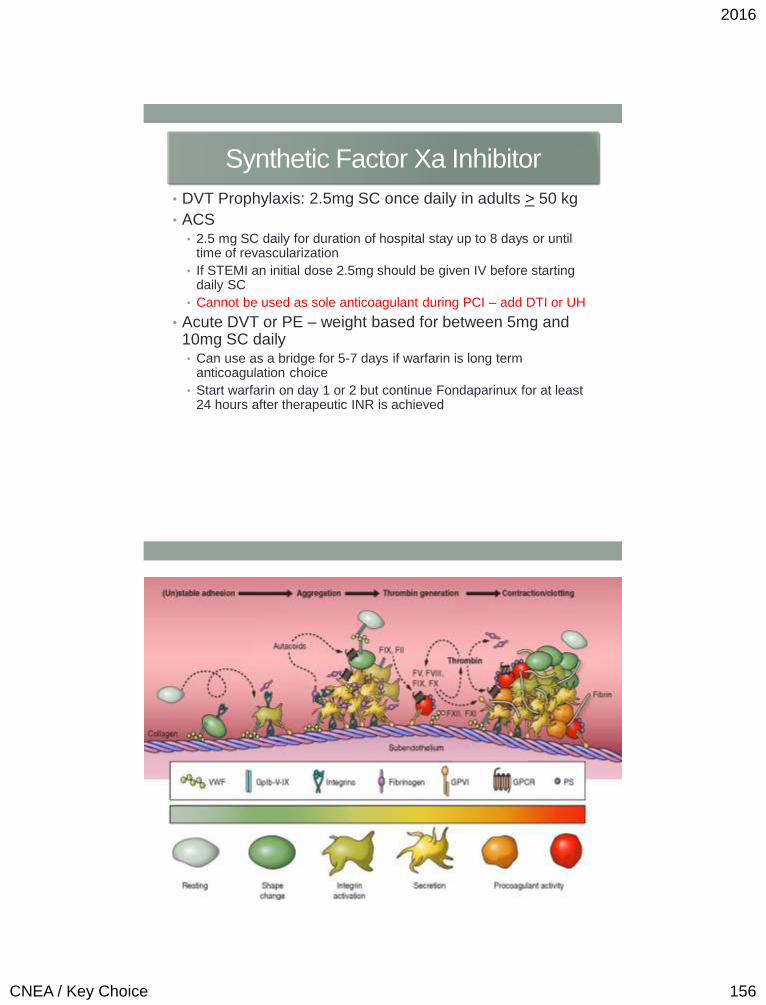
2016
CNEA / Key Choice 156
Synthetic Factor Xa Inhibitor
• DVT Prophylaxis: 2.5mg SC once daily in adults > 50 kg
• ACS • 2.5 mg SC daily for duration of hospital stay up to 8 days or until
time of revascularization
• If STEMI an initial dose 2.5mg should be given IV before starting daily SC
• Cannot be used as sole anticoagulant during PCI – add DTI or UH
• Acute DVT or PE – weight based for between 5mg and 10mg SC daily • Can use as a bridge for 5-7 days if warfarin is long term
anticoagulation choice
• Start warfarin on day 1 or 2 but continue Fondaparinux for at least 24 hours after therapeutic INR is achieved
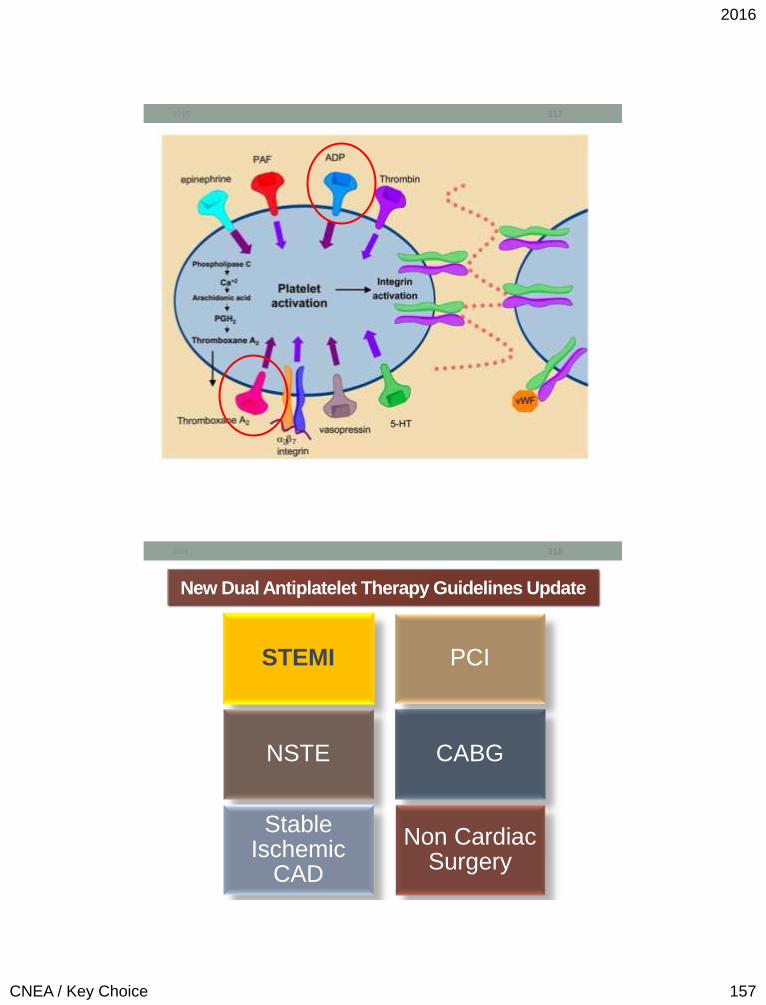
2016
CNEA / Key Choice 157
2016 317
New Dual Antiplatelet Therapy Guidelines Update
STEMI
NSTE CABG
Stable Ischemic
CAD
Non Cardiac Surgery
PCI
318 2016
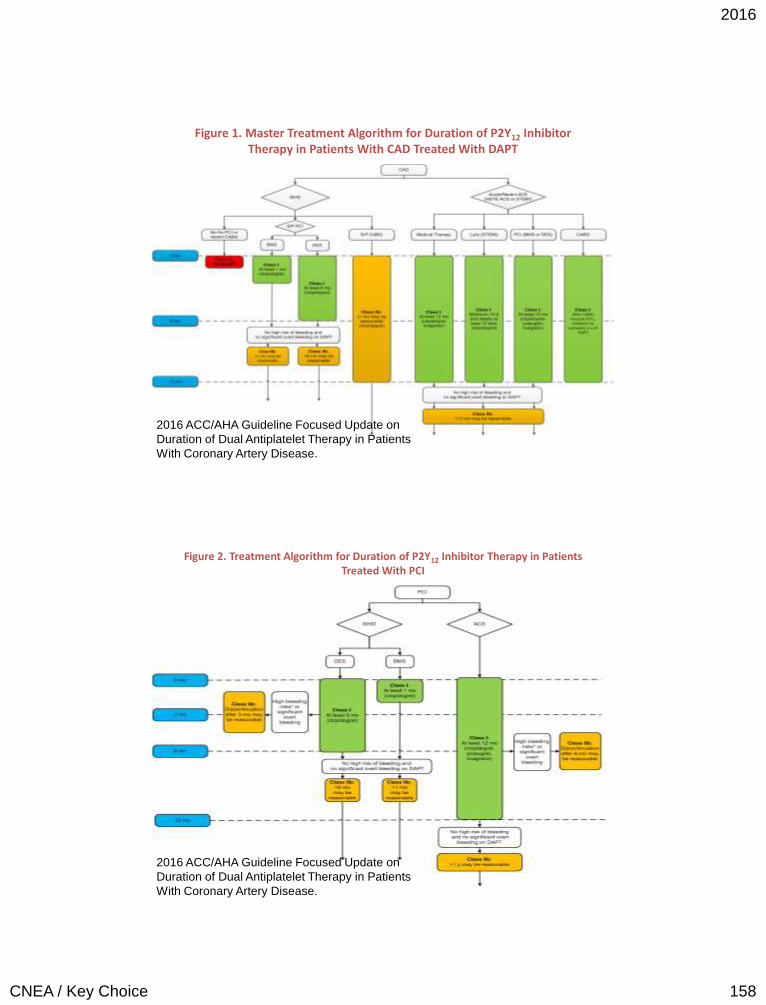
2016
CNEA / Key Choice 158
Figure 1. Master Treatment Algorithm for Duration of P2Y12 Inhibitor Therapy in Patients With CAD Treated With DAPT
2016 ACC/AHA Guideline Focused Update on
Duration of Dual Antiplatelet Therapy in Patients
With Coronary Artery Disease.
Figure 2. Treatment Algorithm for Duration of P2Y12 Inhibitor Therapy in Patients Treated With PCI
2016 ACC/AHA Guideline Focused Update on
Duration of Dual Antiplatelet Therapy in Patients
With Coronary Artery Disease.

2016
CNEA / Key Choice 159
Figure 3. Treatment Algorithm for Management and Duration of P2Y12 Inhibitor Therapy in Patients Undergoing CABG
2016 ACC/AHA Guideline Focused Update on
Duration of Dual Antiplatelet Therapy in Patients
With Coronary Artery Disease.
Figure 4. Treatment Algorithm for Duration of P2Y12 Inhibitor Therapy in Patients With SIHD (Without ACS Within the Past Several Years)
2016 ACC/AHA Guideline Focused Update on
Duration of Dual Antiplatelet Therapy in Patients
With Coronary Artery Disease.
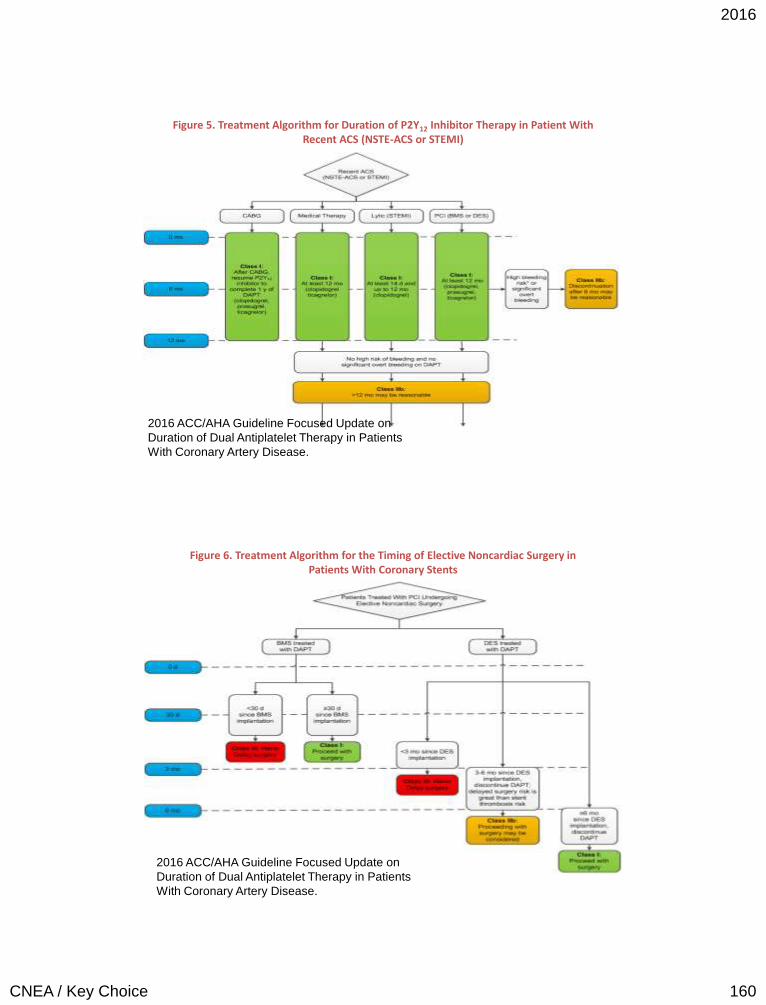
2016
CNEA / Key Choice 160
Figure 5. Treatment Algorithm for Duration of P2Y12 Inhibitor Therapy in Patient With Recent ACS (NSTE-ACS or STEMI)
2016 ACC/AHA Guideline Focused Update on
Duration of Dual Antiplatelet Therapy in Patients
With Coronary Artery Disease.
Figure 6. Treatment Algorithm for the Timing of Elective Noncardiac Surgery in Patients With Coronary Stents
2016 ACC/AHA Guideline Focused Update on
Duration of Dual Antiplatelet Therapy in Patients
With Coronary Artery Disease.
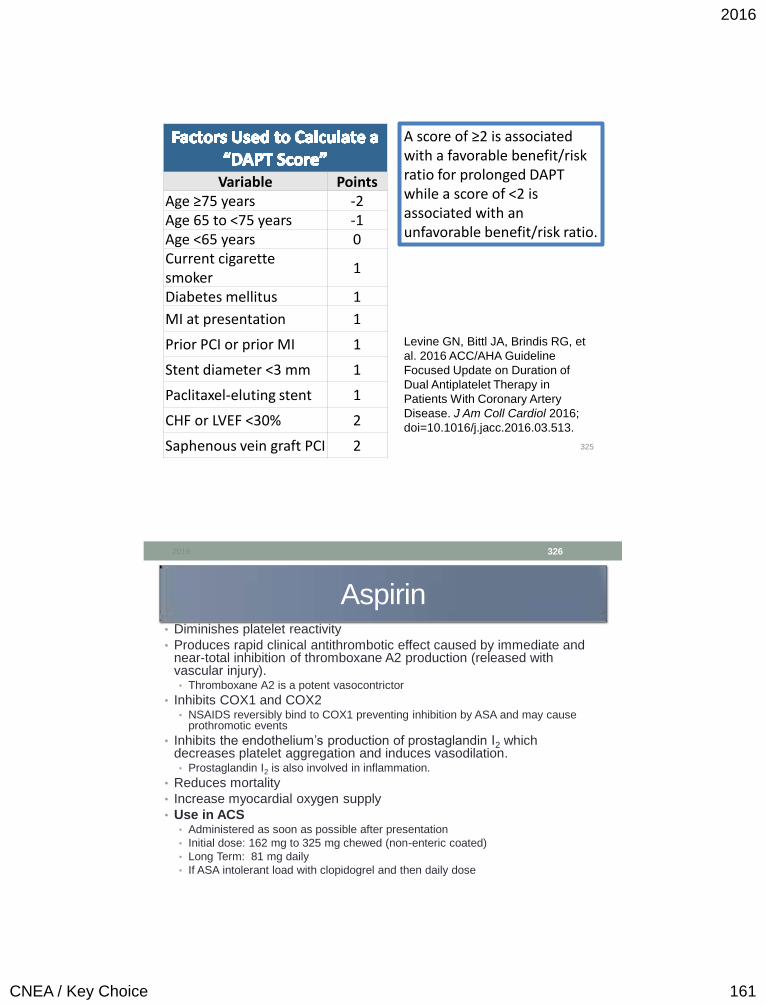
2016
CNEA / Key Choice 161
2016 325
Variable Points Age ≥75 years -2 Age 65 to <75 years -1 Age <65 years 0 Current cigarette smoker
1
Diabetes mellitus 1
MI at presentation 1
Prior PCI or prior MI 1
Stent diameter <3 mm 1
Paclitaxel-eluting stent 1
CHF or LVEF <30% 2
Saphenous vein graft PCI 2
A score of ≥2 is associated with a favorable benefit/risk ratio for prolonged DAPT while a score of <2 is associated with an unfavorable benefit/risk ratio.
Levine GN, Bittl JA, Brindis RG, et
al. 2016 ACC/AHA Guideline
Focused Update on Duration of
Dual Antiplatelet Therapy in
Patients With Coronary Artery
Disease. J Am Coll Cardiol 2016;
doi=10.1016/j.jacc.2016.03.513.
Aspirin • Diminishes platelet reactivity
• Produces rapid clinical antithrombotic effect caused by immediate and near-total inhibition of thromboxane A2 production (released with vascular injury). • Thromboxane A2 is a potent vasocontrictor
• Inhibits COX1 and COX2 • NSAIDS reversibly bind to COX1 preventing inhibition by ASA and may cause
prothromotic events
• Inhibits the endothelium’s production of prostaglandin I2 which decreases platelet aggregation and induces vasodilation. • Prostaglandin I2 is also involved in inflammation.
• Reduces mortality
• Increase myocardial oxygen supply
• Use in ACS • Administered as soon as possible after presentation
• Initial dose: 162 mg to 325 mg chewed (non-enteric coated)
• Long Term: 81 mg daily
• If ASA intolerant load with clopidogrel and then daily dose
2016 326
2016
CNEA / Key Choice 162
P2Y12 Receptor Inhibitors /
ADP Receptor Blockers • Clopidogrel (Plavix)
• 600 mg initial dose
• 75 mg daily
• Prasugrel (Effient) • 60 mg initial dose
• 10mg daily
• Contraindicated: > 75, < 60 kg, previous TIA, CVA
• Ticagrelor (Brilinta) • 180mg initial dose
• 90mg twice daily
• Not to be given with ASA doses > 100mg
• Adenosine Diphosphate (ADP) - Stored in platelets and released upon platelet activation
• ADP interacts with P2Y12 chemoreceptors to enhance adhesiveness and aggregation of platelets through the activation of the GP IIb/IIIa pathway
2016 327
P2Y12 Receptor Inhibitors /
ADP Receptor Blockers • Thienopyridines
• Clopidogrel
• Prasugrel
• Non thienopyridine
• Ticagrelor
2016 328
2016
CNEA / Key Choice 163
Thienopyridines
• Thienopyridines are a class of ADP / P2Y12 receptor
blockers • Clopidogrel (Plavix)
• Prasugrel (Effient)
• Irreversibly inhibits P2Y12 receptor
2016 329
Clopidogrel Indications
• Alternative to ASA therapy in those who cannot take ASA
• Option in NSTE-ACS for the second antiplatelet agent
• Ticagrelor and prasugrel have upgraded indications
• Recommended agent in elective PCI with bare metal stent
2016
CNEA / Key Choice 164
Clopidogrel
Issue of Non Responders • ACCF/AHA Clopidogrel Clinical Alert
• FDA Boxed Warning March 2010
• Role of genotype testing or routine platelet function testing
• Class II b recommendation pending results of randomized controlled
clinical trials.
• Prodrug
• 2 step process
• Involves several CYP450 isoenzymes
• CYP2C19 isoenzyme responsible for almost half of the first step formation
• 3 major genetic polymorphisms are associated with loss of function
• Observational studies have shown an association between an increased
risk of adverse cardiovascular events and the presence of one
nonfunctioning allele
2016 331
Clopidogrel and PPIs
11/8/2010: Expert Consensus Document
• Using proton pump inhibitors (PPIs) and antiplatelet drugs
(thienopyridines) together is an appropriate way of
treating patients with cardiovascular (CV) disease who
are at high risk of upper gastrointestinal (GI) bleeds,
despite recent concerns about an adverse interaction
between these two types of drugs, according to an Expert
Consensus Document released jointly today by the
American College of Cardiology (ACC), the American
College of Gastroenterology (ACG), and the American
Heart Association (AHA).
2016 332
2016
CNEA / Key Choice 165
Clopidogrel and PPIs
2012: World Journal of Gastroenterology • Because PPI induced risk reduction clearly overweighs
the possible adverse cardiovascular risk in patients with
high risk of gastrointestinal bleeding, combination of
clopidogrel with the less CYP2C19 inhibiting pantoprazole
should be recommended.
• Several pharmacodynamic studies found a significant decrease of the
clopidogrel platelet antiaggregation effect for omeprazole, but not for
pantoprazole.
• More recent RCT and retrospective co-hort studies have not resulted
in same concerns with PPIs as observational studies suggested.
2016 333
Prasugrel
• TRITON TIMI 38 Trail • 13,608 patients with moderate to high risk ACS – all referred for
PCI; 3,534 STEMI
• Randomized to clopidogrel 300mg load and 75mg daily or prasurgrel 60mg load and 10mg daily
• Median follow up 14 ½ months
• Prasugrel (compared to Clopidogrel) associated with • Significant 2.2% reduction in absolute risk and a 19% reduction in
relative risk in the composite endpoint of death due to CV disease, nonfatal MI, or nonfatal stroke during the follow up period
• Significant increase in TIMI major hemorrhage (1.8% vs 2.4%)
• Prasugrel approved 2009
2016 334
Wiviott et al., 2007. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J
Med 2007; 357:2001-2015
2016
CNEA / Key Choice 166
Prasugrel • TRILOGY
• Prasugrel versus clopidogrel in patients with NSTEMI or unstable angina who were not treated with PCI
• 7,243 patients
• No statistically significant difference in primary outcome (composite of: death from cardiovascular causes, myocardial infarction, or stroke) among patients under the age of 75 years
• A weak trend toward a reduced risk in the prasugrel group after 12 months (P = 0.07)
• Rates of severe and intracranial bleeding were similar in the two groups in all age groups. This is different than TRITON TIMI 38. Dose was adjusted in Trilogy for weight < 60 kg and age > 75 years.
• Conclusion: More research needed
• Higher recommendation for prasugrel in NSTE over clopidogrel in early invasive option only
2016 335
Take Away Prasugrel Points
• Less concern with PPI administration
• Less concern regarding non responders • Prodrug but not as
dependent on CYP2C19 isoenzyme
• Only used in patients with planned PCI • No benefit to
administration before the time of angiography
• Increased bleeding risk
• > 75 years old
• <60 KG
• Cannot be used: • Previous CVA / TIA
2016 336
2016
CNEA / Key Choice 167
Ticagrelor (Non-Thienopyridine)
• Reversibly binds to P2Y12 receptor
• Not a PRO drug: does not requiring metabolic activation
• FDA approved July 2011
• Prevention of thrombotic events in patients with acute
coronary syndromes.
• Loading dose 180 mg then 90 mg twice daily
• Contraindicated in history of intracranial bleeding, active
pathological bleeding, severe hepatic impairment
• Higher recommendation for ticagrelor in NSTE over
clopidogrel in either ischemia guided or early invasive
option
2016 337
Clopidogrel versus Ticagrelor • PLATO trial
• Better anti-ischemic effect compared to clopidogrel
• No significant increase in major bleeding
• Faster onset and shorter duration than clopidogrel (known as reversible mode of action)
• BID dosing is a potential concern for compliance
• North American effect – thought to be due to higher dose ASA • Must not be given with maintenance ASA doses >
100mg
• Although shorter ½ life – recommendation to be held 5 days before surgery.
2016 338
Wallentin, L. et al., 2009. Ticagrelor versus clopidogrel in patients with acute coronary
syndromes. N Engl J Med; 361:1045-1057
Take Aways
2016
CNEA / Key Choice 168
Guideline Directed Medical Therapy for ACS / CAD
Dual Antiplatelet Therapy • ASA • Clopidogrel/Prasugrel/Ticagrelor
Beta Blocker ACE Inhibitor
– Based on additional criteria
Eplerenone – Based on additional criteria
Statin – Regardless of baseline LDL-C
SL Nitroglycerin
Medications to control ischemia for medical
management / angina
• Beta-blockers
• Calcium channel blockers
• Long acting nitrate
• Ranolazine (Ranexa)
339 2016
Beta Blockers in ACS • Immediate as well as long term mortality benefit
• Immediate beta-blocker therapy – Reduces the magnitude of infarction and incidence of associated
complications
• Decreases myocardial oxygen demand
– Reduces rate of reinfarction
– Reduces frequency of life-threatening ventricular tachyarrhythmias.
• Long term benefit post ACS – Decreases myocardial oxygen demand
• HR Benefit
– Enhances overall well being
– Slows disease progression
– Inhibits ventricular remodeling and apoptosis
– Inhibits adverse effects of SNS
– Reduces mortality and repeat hospitalizations
340 2016
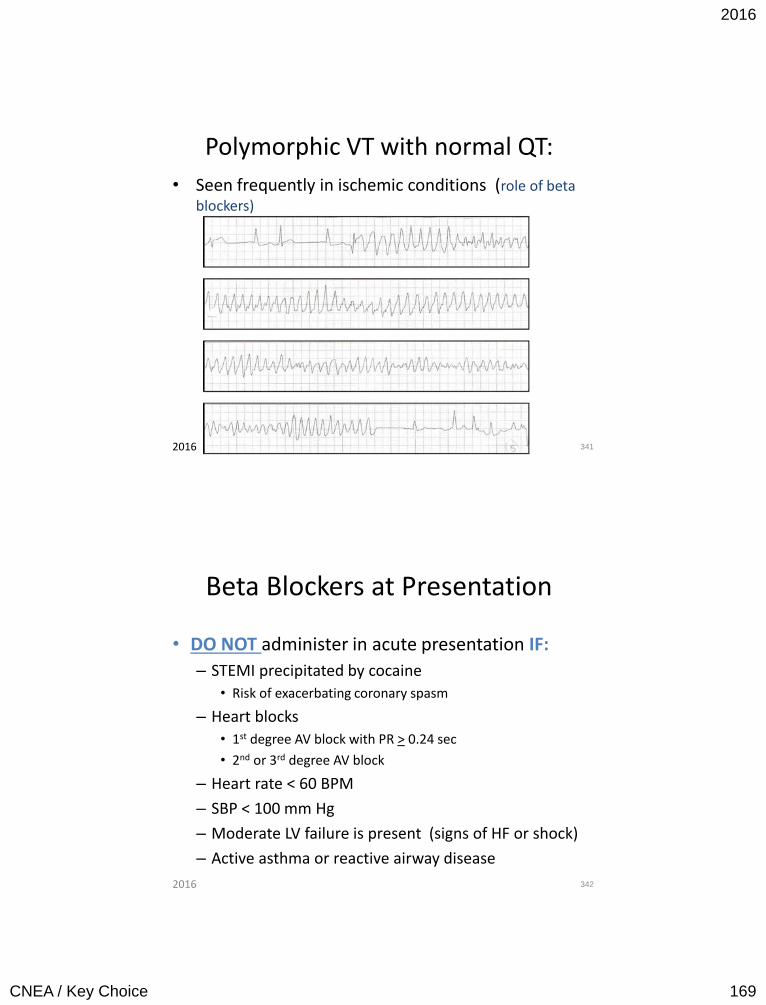
2016
CNEA / Key Choice 169
Polymorphic VT with normal QT:
• Seen frequently in ischemic conditions (role of beta blockers)
341 2016
Beta Blockers at Presentation
• DO NOT administer in acute presentation IF:
– STEMI precipitated by cocaine
• Risk of exacerbating coronary spasm
– Heart blocks
• 1st degree AV block with PR > 0.24 sec
• 2nd or 3rd degree AV block
– Heart rate < 60 BPM
– SBP < 100 mm Hg
– Moderate LV failure is present (signs of HF or shock)
– Active asthma or reactive airway disease
342 2016
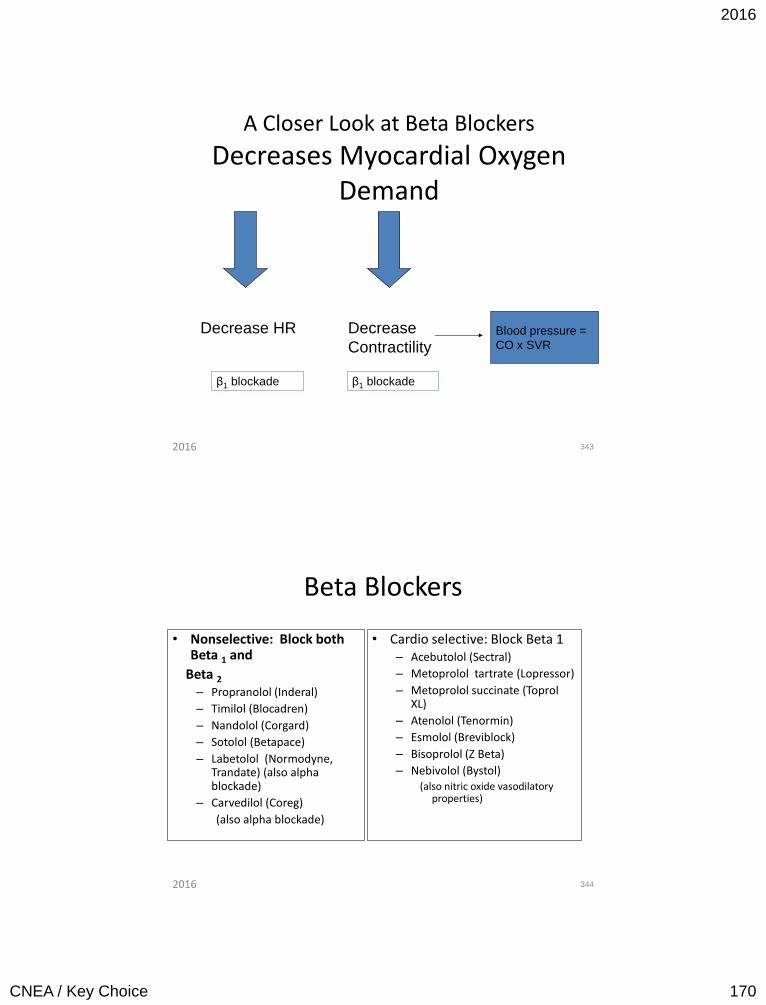
2016
CNEA / Key Choice 170
A Closer Look at Beta Blockers
Decreases Myocardial Oxygen Demand
343
Decrease HR Decrease
Contractility
β1 blockade β1 blockade
Blood pressure =
CO x SVR
2016
Beta Blockers
• Nonselective: Block both Beta 1 and
Beta 2
– Propranolol (Inderal)
– Timilol (Blocadren)
– Nandolol (Corgard)
– Sotolol (Betapace)
– Labetolol (Normodyne, Trandate) (also alpha blockade)
– Carvedilol (Coreg)
(also alpha blockade)
• Cardio selective: Block Beta 1 – Acebutolol (Sectral)
– Metoprolol tartrate (Lopressor)
– Metoprolol succinate (Toprol XL)
– Atenolol (Tenormin)
– Esmolol (Breviblock)
– Bisoprolol (Z Beta)
– Nebivolol (Bystol) (also nitric oxide vasodilatory
properties)
344 2016
2016
CNEA / Key Choice 171
345
• Start beta blocker prior ACE-inhibitor – Beta blockers most important medication to
reduce mortality early – However, cannot be given in patients at high risk
for shock
• Do not start beta blocker and ACE-I at the same time
• Hold ACE inhibitors for BP < 100 mm Hg systolic
or < 30 mm Hg below baseline. – Ideally ACE-I should be initiated within 24 hours
2016
Beta Blockers Recommended by Disease State
Post MI
• Atenolol
• Carvedilol
• Metoprolol
• Propanolol
• Timololol
Heart Failure • Bisoprolol
• Carvedilol
• Metoprolol Succinate (XL)
346 2016
2016
CNEA / Key Choice 172
• Altered responses and vulnerability to drugs with:
– Hypotensive action (nitrates, calcium blockers)
– Cerebral effects (beta blockers)
• Caution with renally cleared drugs
347 2016
• Indicated for treatment of chronic angina • Mechanism of action in treating angina is
unknown – Possible relaxation of myocardium
• Does not impact heart rate or blood pressure • Dose: 500-1000mg BID • May prolong QTc interval • May worsen renal failure – DC if marked increase
in serum creatinine • Contraindicated in hepatic cirrhosis
348 2016
2016
CNEA / Key Choice 173
349 2016
• The 2013 ACC/AHA Expert Panel included all 16 members of the National Heart, Lung, and Blood Institute Adult Treatment Panel (ATP) IV.
• Commissioned by NHLBI in June 2013
• Guidelines replace ATP III
350 2016
2016
CNEA / Key Choice 174
• Focus is no longer on targeting the LDL-C – Treat to level of risk not to target LDL-C
• New guidelines focus on 4 groups of patients who can benefit from statin therapy with a good safety margin
• Benefit includes reduction in atherosclerotic cardiovascular disease events (ASCVD) – Nonfatal MI, CHD Death, nonfatal stroke
351 2016
• Individuals with clinical ASCVD – acute coronary syndromes – History of MI – Stable or unstable angina – Coronary or other arterial revascularization – Stroke/TIA – Peripheral arterial disease presumed to be of
atherosclerotic origin
• Without New York Heart Association (NYHA) class II-IV heart failure or receiving hemodialysis.
• High intensity statin – adults < 75
352 2016
2016
CNEA / Key Choice 175
• Individuals with primary elevations of low-density lipoprotein cholesterol (LDL-C) ≥190 mg/dl.
353 2016
• Individuals 40-75 years of age with diabetes, and LDL-C 70-189 mg/dl without clinical ASCVD.
354 2016
2016
CNEA / Key Choice 176
• Individuals without clinical ASCVD or diabetes, who are 40-75 years of age with LDL-C 70-189 mg/dl, and have an estimated 10-year ASCVD risk of 7.5% or higher
• Pooled Cohort Equations for ASCVD risk prediction.
– Men and women; black and non-Hispanic white
• May use non Hispanic White calculator for other populations (may under estimate risk in certain populations)
– Ages 40 to 79
– Identifies cohorts most likely to benefit from statin therapy
355 2016
• Required information to estimate ASCVD risk: – Age – Sex – Race – Total cholesterol – HDL cholesterol – Systolic blood pressure – Blood pressure lowering medication use – Diabetes status – Smoking status.
Source: Based on the Pooled Cohort Equations2 and the work of Lloyd-Jones, et al., Circulation, 2006
356 2016
2016
CNEA / Key Choice 177
• No recommendations for treatment outside the 4 groups.
• No recommendation to start or stop statins in NYHA Class II-IV systolic HF that is ischemic in etiology
• In patients with a 10-year risk < 7.5%, other factors can be considered: – Family history – LDL-C>160mg/dL – HS C-reactive protein >2mg/dL – Coronary calcium score >300 – ABI < 0.9 – Etc.
357 2016
• Atorvastatin (Lipitor)
• Provastatin (Pravachol)
• Fluvostatin (Lescol)
• Simvastatin (Zocor)
• Lovastatin (Mevacor)
• Rosuvastin (Crestor)
• Inhibition of HMG-CoA reductase
• HMG –CoA reductase catalyzes an early step in cholesterol biosynthesis
Decrease mortality Reduce risk of major coronary events by 30% Stimulate plaque regression
358 2016
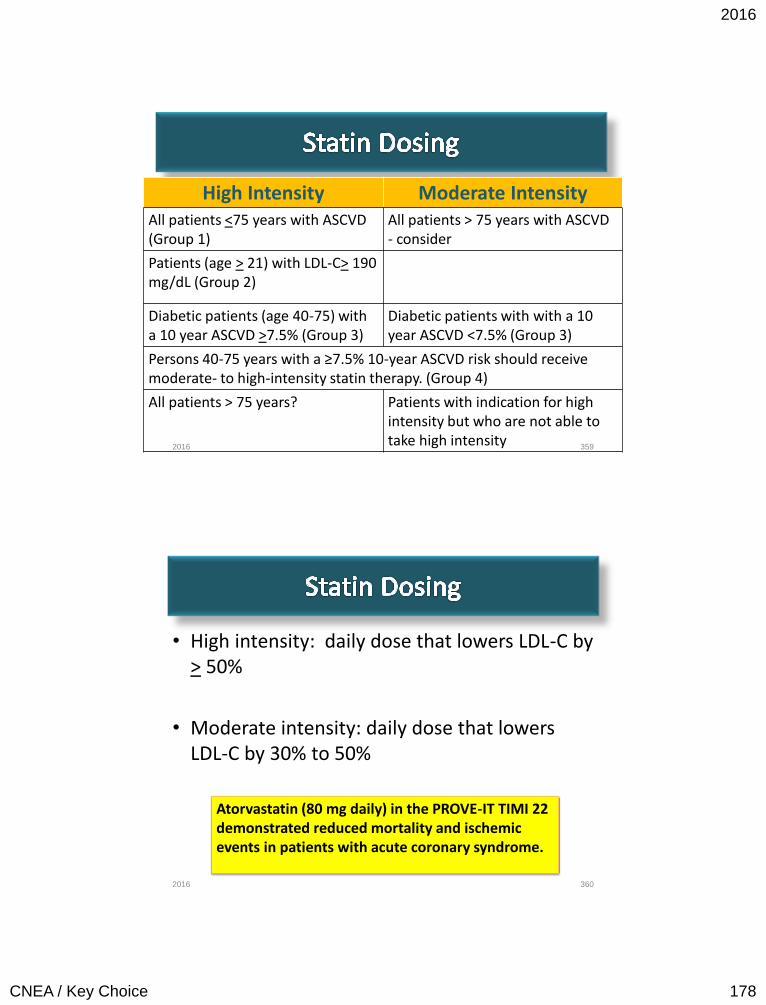
2016
CNEA / Key Choice 178
High Intensity Moderate Intensity All patients <75 years with ASCVD (Group 1)
All patients > 75 years with ASCVD - consider
Patients (age > 21) with LDL-C> 190 mg/dL (Group 2)
Diabetic patients (age 40-75) with a 10 year ASCVD >7.5% (Group 3)
Diabetic patients with with a 10 year ASCVD <7.5% (Group 3)
Persons 40-75 years with a ≥7.5% 10-year ASCVD risk should receive moderate- to high-intensity statin therapy. (Group 4)
All patients > 75 years?
Patients with indication for high intensity but who are not able to take high intensity
359 2016
• High intensity: daily dose that lowers LDL-C by > 50%
• Moderate intensity: daily dose that lowers LDL-C by 30% to 50%
360
Atorvastatin (80 mg daily) in the PROVE-IT TIMI 22 demonstrated reduced mortality and ischemic events in patients with acute coronary syndrome.
2016
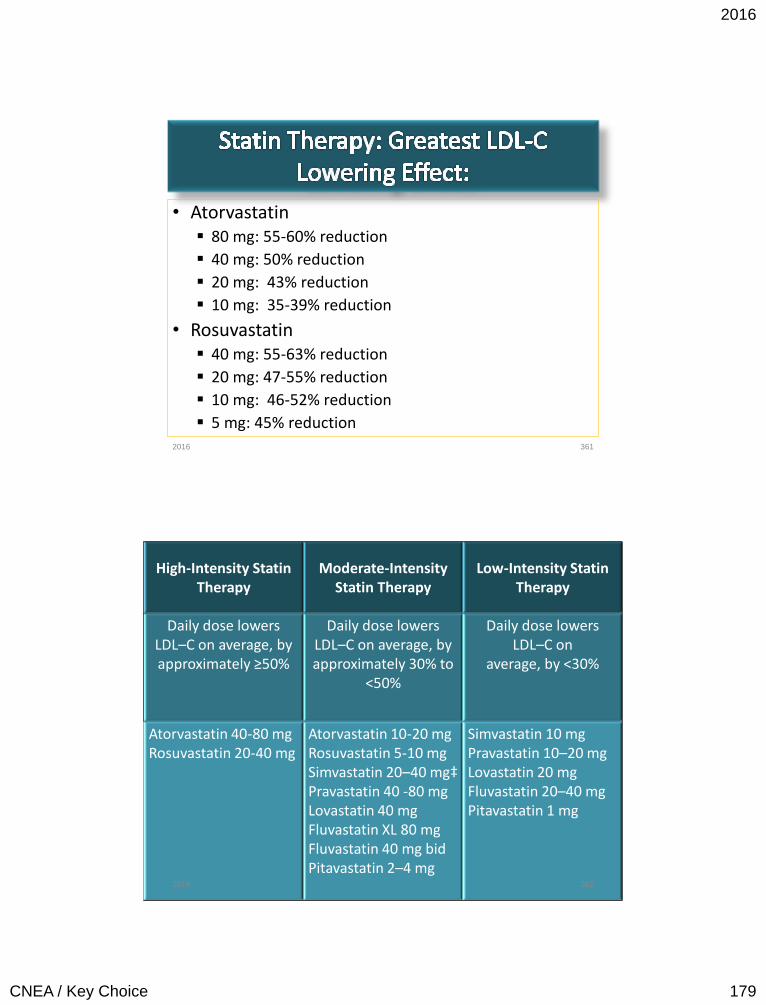
2016
CNEA / Key Choice 179
• Atorvastatin 80 mg: 55-60% reduction
40 mg: 50% reduction
20 mg: 43% reduction
10 mg: 35-39% reduction
• Rosuvastatin 40 mg: 55-63% reduction
20 mg: 47-55% reduction
10 mg: 46-52% reduction
5 mg: 45% reduction
361 2016
High-Intensity Statin Therapy
Moderate-Intensity Statin Therapy
Low-Intensity Statin Therapy
Daily dose lowers LDL–C on average, by approximately ≥50%
Daily dose lowers LDL–C on average, by approximately 30% to
<50%
Daily dose lowers LDL–C on
average, by <30%
Atorvastatin 40-80 mg Rosuvastatin 20-40 mg
Atorvastatin 10-20 mg Rosuvastatin 5-10 mg Simvastatin 20–40 mg‡ Pravastatin 40 -80 mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2–4 mg
Simvastatin 10 mg Pravastatin 10–20 mg Lovastatin 20 mg Fluvastatin 20–40 mg Pitavastatin 1 mg
362 2016
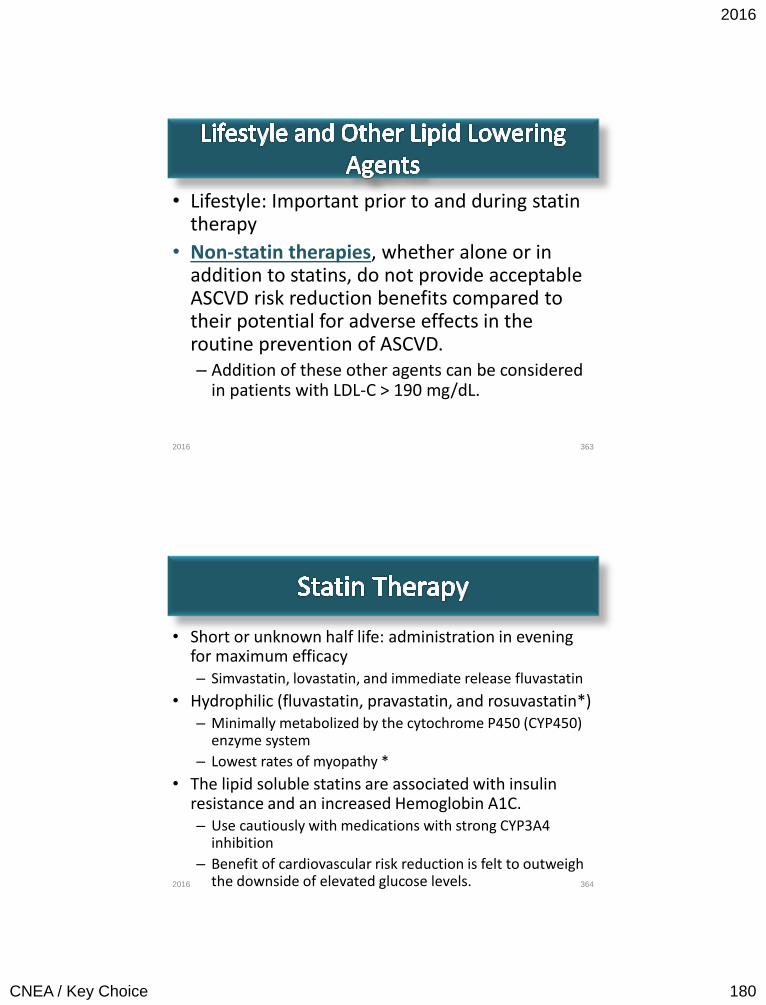
2016
CNEA / Key Choice 180
• Lifestyle: Important prior to and during statin therapy
• Non-statin therapies, whether alone or in addition to statins, do not provide acceptable ASCVD risk reduction benefits compared to their potential for adverse effects in the routine prevention of ASCVD. – Addition of these other agents can be considered
in patients with LDL-C > 190 mg/dL.
363 2016
• Short or unknown half life: administration in evening for maximum efficacy – Simvastatin, lovastatin, and immediate release fluvastatin
• Hydrophilic (fluvastatin, pravastatin, and rosuvastatin*) – Minimally metabolized by the cytochrome P450 (CYP450)
enzyme system
– Lowest rates of myopathy *
• The lipid soluble statins are associated with insulin resistance and an increased Hemoglobin A1C. – Use cautiously with medications with strong CYP3A4
inhibition
– Benefit of cardiovascular risk reduction is felt to outweigh the downside of elevated glucose levels.
364 2016
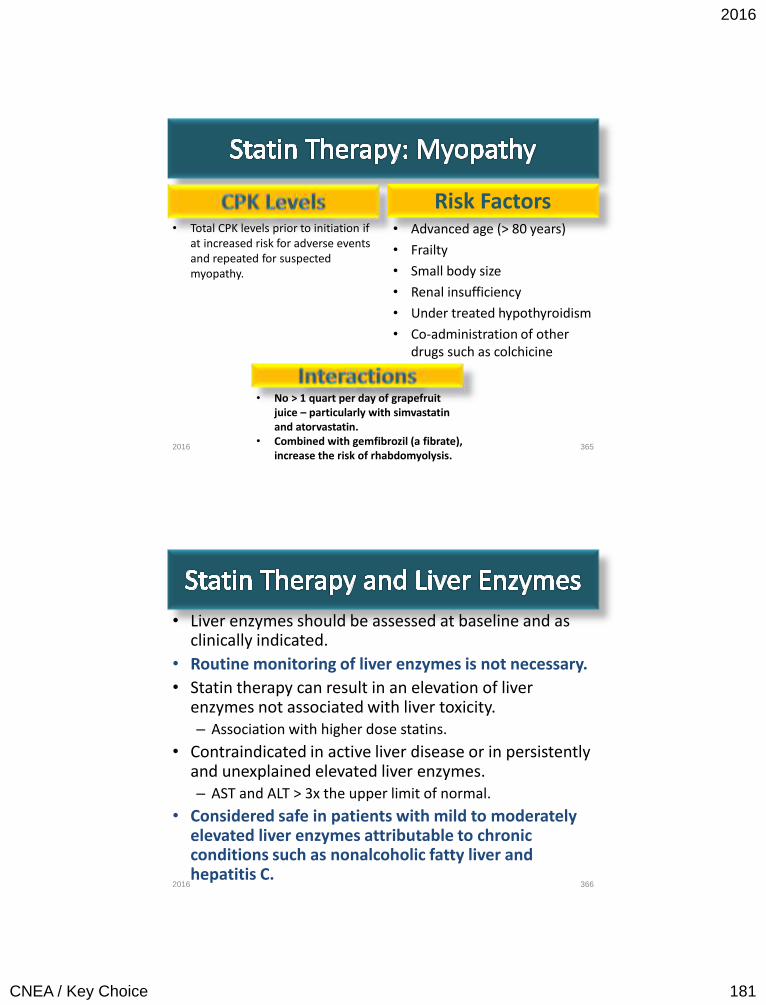
2016
CNEA / Key Choice 181
• Total CPK levels prior to initiation if at increased risk for adverse events and repeated for suspected myopathy.
• No > 1 quart per day of grapefruit juice – particularly with simvastatin and atorvastatin.
• Combined with gemfibrozil (a fibrate), increase the risk of rhabdomyolysis.
Risk Factors • Advanced age (> 80 years)
• Frailty
• Small body size
• Renal insufficiency
• Under treated hypothyroidism
• Co-administration of other drugs such as colchicine
365 2016
• Liver enzymes should be assessed at baseline and as clinically indicated.
• Routine monitoring of liver enzymes is not necessary.
• Statin therapy can result in an elevation of liver enzymes not associated with liver toxicity. – Association with higher dose statins.
• Contraindicated in active liver disease or in persistently and unexplained elevated liver enzymes. – AST and ALT > 3x the upper limit of normal.
• Considered safe in patients with mild to moderately elevated liver enzymes attributable to chronic conditions such as nonalcoholic fatty liver and hepatitis C.
366 2016
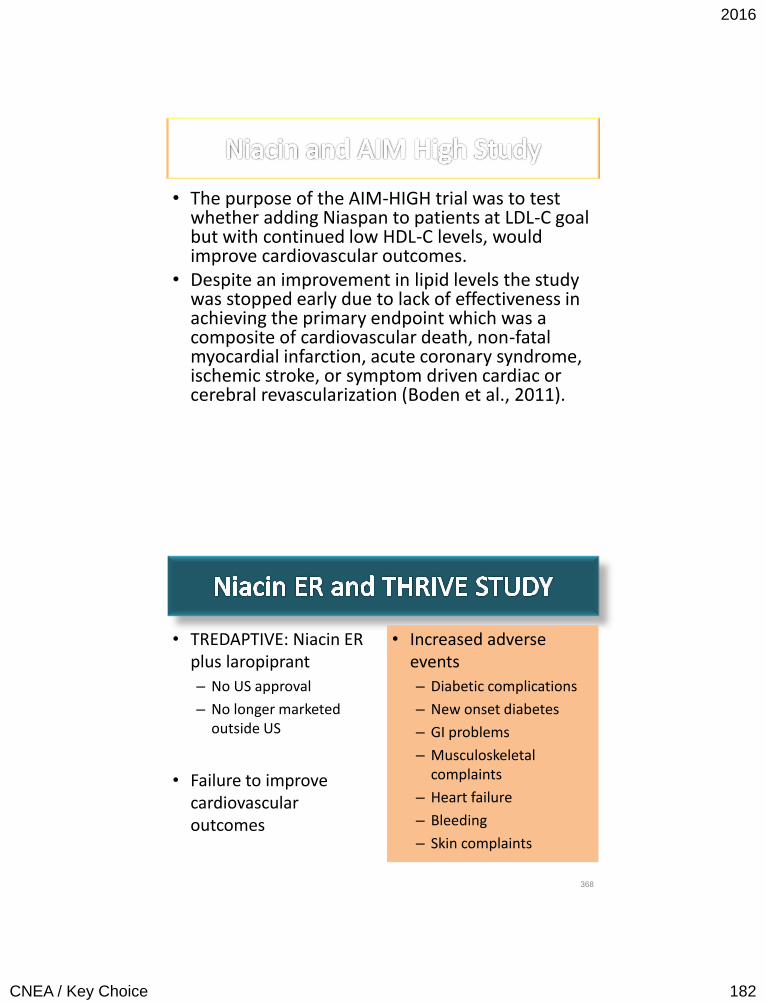
2016
CNEA / Key Choice 182
• The purpose of the AIM-HIGH trial was to test whether adding Niaspan to patients at LDL-C goal but with continued low HDL-C levels, would improve cardiovascular outcomes.
• Despite an improvement in lipid levels the study was stopped early due to lack of effectiveness in achieving the primary endpoint which was a composite of cardiovascular death, non-fatal myocardial infarction, acute coronary syndrome, ischemic stroke, or symptom driven cardiac or cerebral revascularization (Boden et al., 2011).
• TREDAPTIVE: Niacin ER plus laropiprant
– No US approval
– No longer marketed outside US
• Failure to improve cardiovascular outcomes
• Increased adverse events
– Diabetic complications
– New onset diabetes
– GI problems
– Musculoskeletal complaints
– Heart failure
– Bleeding
– Skin complaints
368
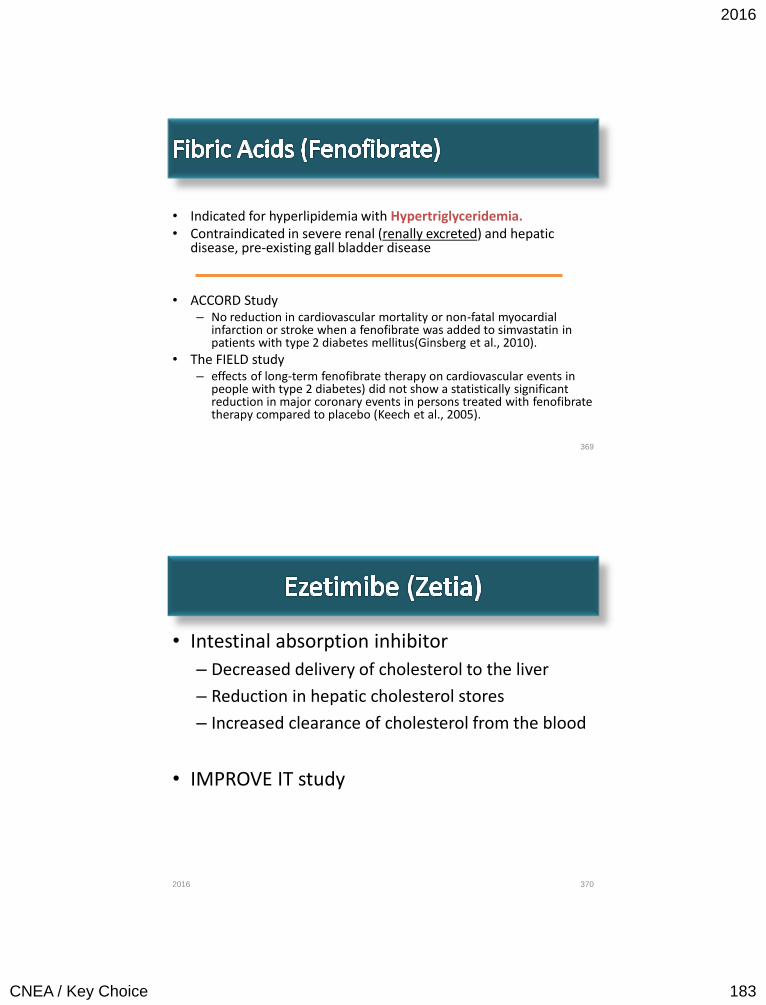
2016
CNEA / Key Choice 183
• Indicated for hyperlipidemia with Hypertriglyceridemia. • Contraindicated in severe renal (renally excreted) and hepatic
disease, pre-existing gall bladder disease • ACCORD Study
– No reduction in cardiovascular mortality or non-fatal myocardial infarction or stroke when a fenofibrate was added to simvastatin in patients with type 2 diabetes mellitus(Ginsberg et al., 2010).
• The FIELD study – effects of long-term fenofibrate therapy on cardiovascular events in
people with type 2 diabetes) did not show a statistically significant reduction in major coronary events in persons treated with fenofibrate therapy compared to placebo (Keech et al., 2005).
369
• Intestinal absorption inhibitor
– Decreased delivery of cholesterol to the liver
– Reduction in hepatic cholesterol stores
– Increased clearance of cholesterol from the blood
• IMPROVE IT study
370 2016

2016
CNEA / Key Choice 184
371 2016
• Drug is an antibody that targets a specific protein (PCSK9) – PCSK9 reduces the number of receptors on the liver
that remove LDL cholesterol from the blood. – By blocking PCSK9’s ability to work, more receptors
are available to get rid of LDL cholesterol from the blood
• Average reduction in LDL cholesterol ranging from 36 to 59 percent, compared to placebo
• Alirocumab (Praluent) • Evolocumab (Repatha)
372 2016
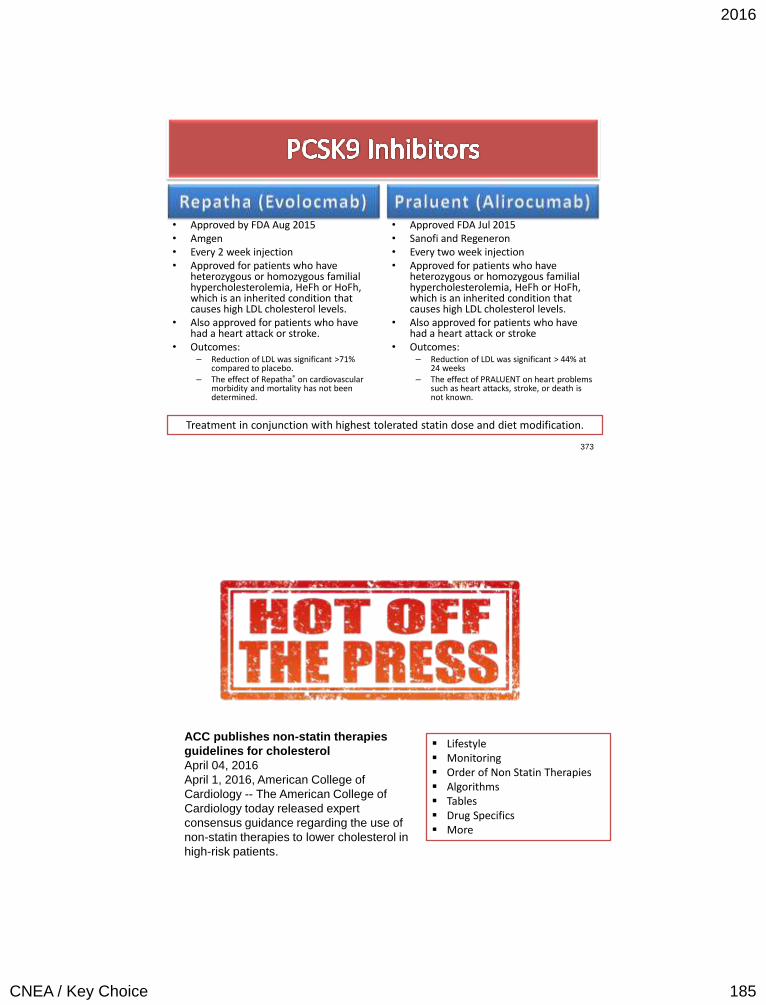
2016
CNEA / Key Choice 185
• Approved by FDA Aug 2015 • Amgen • Every 2 week injection • Approved for patients who have
heterozygous or homozygous familial hypercholesterolemia, HeFh or HoFh, which is an inherited condition that causes high LDL cholesterol levels.
• Also approved for patients who have had a heart attack or stroke.
• Outcomes: – Reduction of LDL was significant >71%
compared to placebo. – The effect of Repatha® on cardiovascular
morbidity and mortality has not been determined.
• Approved FDA Jul 2015 • Sanofi and Regeneron • Every two week injection • Approved for patients who have
heterozygous or homozygous familial hypercholesterolemia, HeFh or HoFh, which is an inherited condition that causes high LDL cholesterol levels.
• Also approved for patients who have had a heart attack or stroke
• Outcomes: – Reduction of LDL was significant > 44% at
24 weeks – The effect of PRALUENT on heart problems
such as heart attacks, stroke, or death is not known.
373
Treatment in conjunction with highest tolerated statin dose and diet modification.
ACC publishes non-statin therapies
guidelines for cholesterol
April 04, 2016
April 1, 2016, American College of
Cardiology -- The American College of
Cardiology today released expert
consensus guidance regarding the use of
non-statin therapies to lower cholesterol in
high-risk patients.
Lifestyle Monitoring Order of Non Statin Therapies Algorithms Tables Drug Specifics More
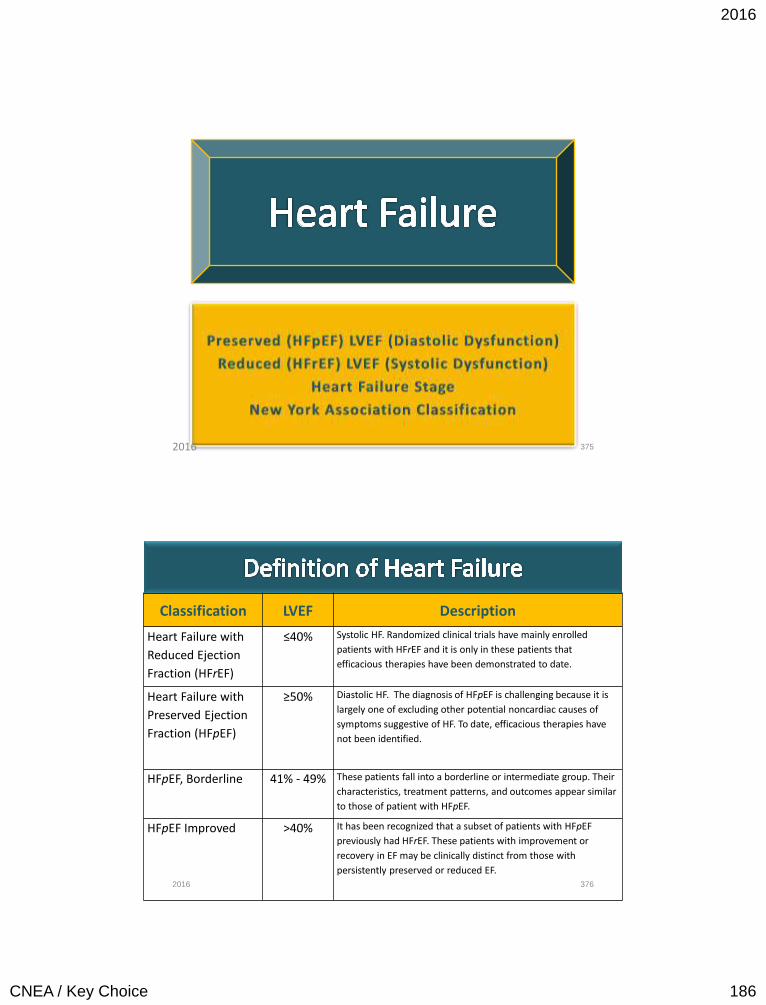
2016
CNEA / Key Choice 186
375 2016
Classification LVEF Description
Heart Failure with
Reduced Ejection
Fraction (HFrEF)
≤40% Systolic HF. Randomized clinical trials have mainly enrolled
patients with HFrEF and it is only in these patients that
efficacious therapies have been demonstrated to date.
Heart Failure with
Preserved Ejection
Fraction (HFpEF)
≥50% Diastolic HF. The diagnosis of HFpEF is challenging because it is
largely one of excluding other potential noncardiac causes of
symptoms suggestive of HF. To date, efficacious therapies have
not been identified.
HFpEF, Borderline 41% - 49% These patients fall into a borderline or intermediate group. Their
characteristics, treatment patterns, and outcomes appear similar
to those of patient with HFpEF.
HFpEF Improved >40% It has been recognized that a subset of patients with HFpEF
previously had HFrEF. These patients with improvement or
recovery in EF may be clinically distinct from those with
persistently preserved or reduced EF.
376 2016
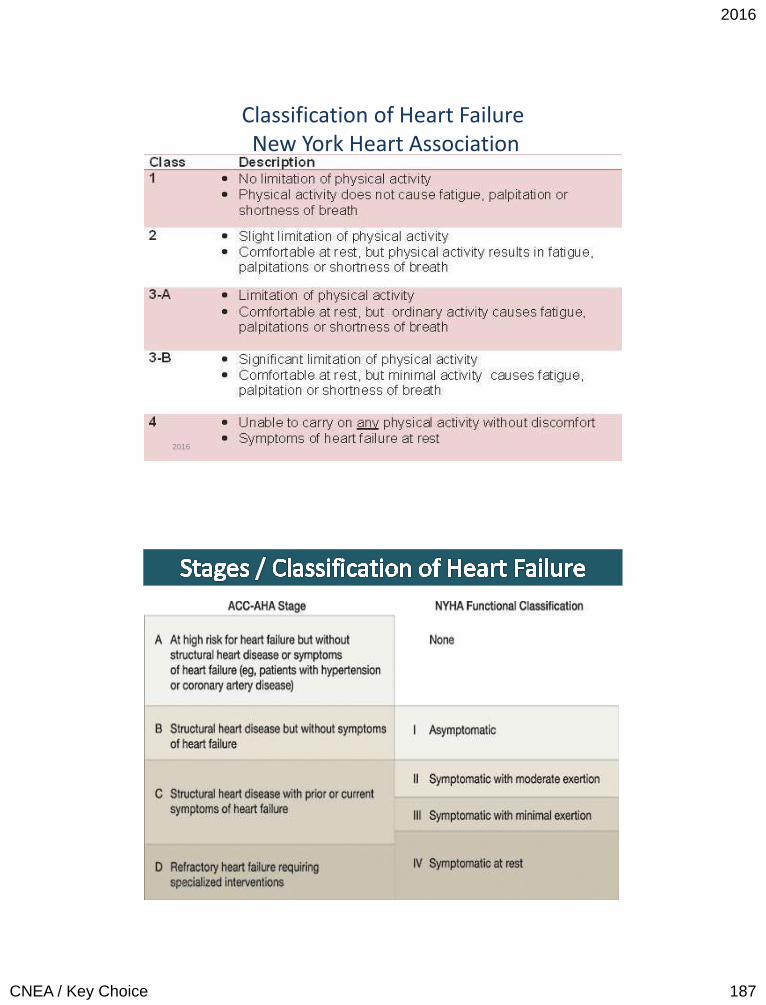
2016
CNEA / Key Choice 187
377
Classification of Heart Failure New York Heart Association
2016
378 2016
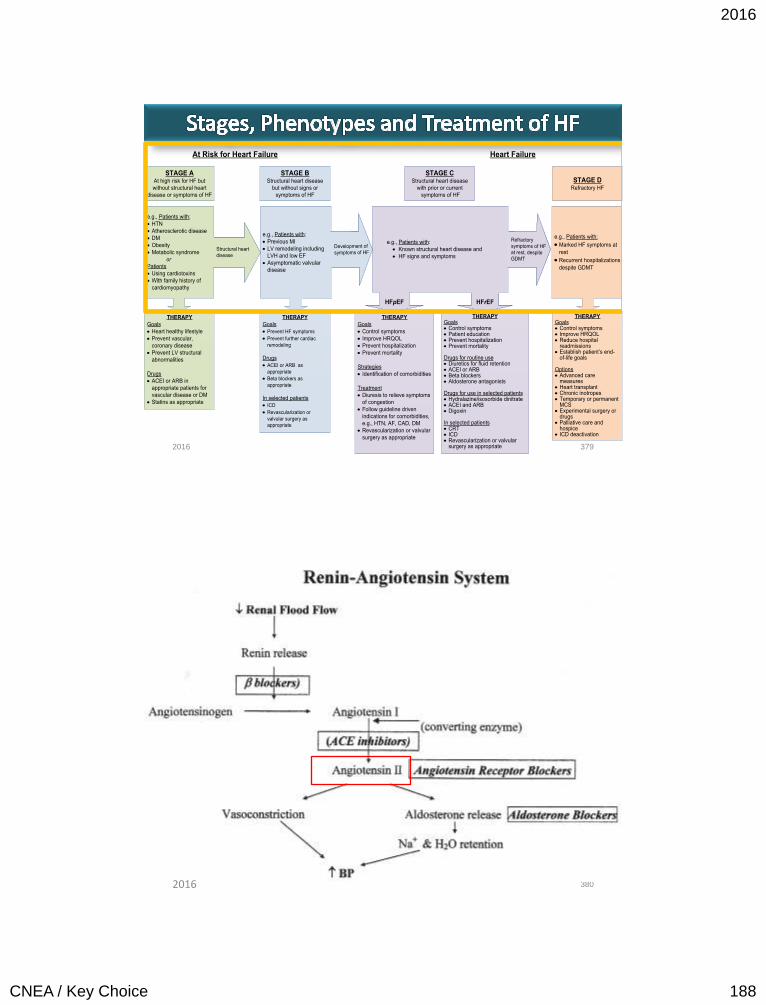
2016
CNEA / Key Choice 188
STAGE AAt high risk for HF but
without structural heart
disease or symptoms of HF
STAGE BStructural heart disease
but without signs or
symptoms of HF
THERAPY
Goals
· Control symptoms
· Improve HRQOL
· Prevent hospitalization
· Prevent mortality
Strategies
· Identification of comorbidities
Treatment
· Diuresis to relieve symptoms
of congestion
· Follow guideline driven
indications for comorbidities,
e.g., HTN, AF, CAD, DM
· Revascularization or valvular
surgery as appropriate
STAGE CStructural heart disease
with prior or current
symptoms of HF
THERAPYGoals· Control symptoms· Patient education· Prevent hospitalization· Prevent mortality
Drugs for routine use· Diuretics for fluid retention· ACEI or ARB· Beta blockers· Aldosterone antagonists
Drugs for use in selected patients· Hydralazine/isosorbide dinitrate· ACEI and ARB· Digoxin
In selected patients· CRT· ICD· Revascularization or valvular
surgery as appropriate
STAGE DRefractory HF
THERAPY
Goals
· Prevent HF symptoms
· Prevent further cardiac
remodeling
Drugs
· ACEI or ARB as
appropriate
· Beta blockers as
appropriate
In selected patients
· ICD
· Revascularization or
valvular surgery as
appropriate
e.g., Patients with:
· Known structural heart disease and
· HF signs and symptoms
HFpEF HFrEF
THERAPY
Goals
· Heart healthy lifestyle
· Prevent vascular,
coronary disease
· Prevent LV structural
abnormalities
Drugs
· ACEI or ARB in
appropriate patients for
vascular disease or DM
· Statins as appropriate
THERAPYGoals· Control symptoms· Improve HRQOL· Reduce hospital
readmissions· Establish patient’s end-
of-life goals
Options· Advanced care
measures· Heart transplant· Chronic inotropes· Temporary or permanent
MCS· Experimental surgery or
drugs· Palliative care and
hospice· ICD deactivation
Refractory symptoms of HF at rest, despite GDMT
At Risk for Heart Failure Heart Failure
e.g., Patients with:
· Marked HF symptoms at
rest
· Recurrent hospitalizations
despite GDMT
e.g., Patients with:
· Previous MI
· LV remodeling including
LVH and low EF
· Asymptomatic valvular
disease
e.g., Patients with:
· HTN
· Atherosclerotic disease
· DM
· Obesity
· Metabolic syndrome
or
Patients
· Using cardiotoxins
· With family history of
cardiomyopathy
Development of
symptoms of HFStructural heart
disease
379 2016
380 2016
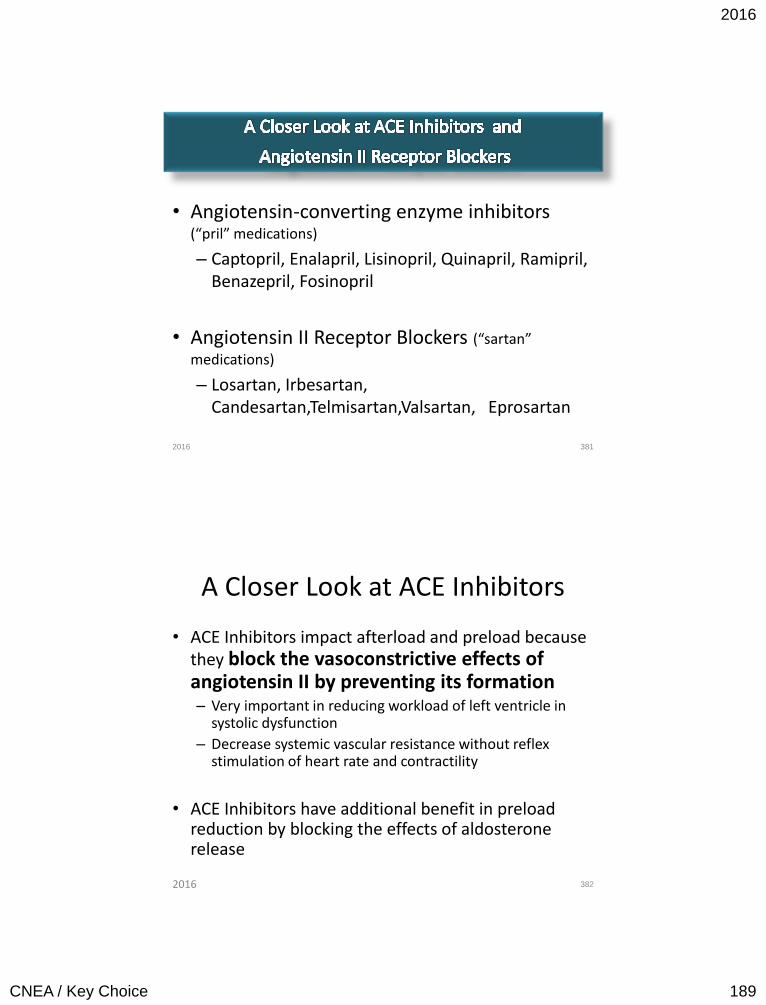
2016
CNEA / Key Choice 189
• Angiotensin-converting enzyme inhibitors (“pril” medications)
– Captopril, Enalapril, Lisinopril, Quinapril, Ramipril, Benazepril, Fosinopril
• Angiotensin II Receptor Blockers (“sartan”
medications)
– Losartan, Irbesartan, Candesartan,Telmisartan,Valsartan, Eprosartan
381 2016
A Closer Look at ACE Inhibitors
• ACE Inhibitors impact afterload and preload because they block the vasoconstrictive effects of angiotensin II by preventing its formation – Very important in reducing workload of left ventricle in
systolic dysfunction
– Decrease systemic vascular resistance without reflex stimulation of heart rate and contractility
• ACE Inhibitors have additional benefit in preload reduction by blocking the effects of aldosterone release
382 2016
2016
CNEA / Key Choice 190
A Closer Look at ACE Inhibitors
• Overall cardioprotective, vasculoprotective effect, and renal protective – Prevents ventricular remodeling
– Reduce mortality in patients with systolic heart failure
– Reduction of left ventricular mass in LV hypertrophy
– Slows progression of both renal disease in diabetes and hypertensive nephrosclerosis
383 2016
• Renal protective in chronic kidney disease • However, can cause acute kidney injury (AKI) in patient’s at risk
(i.e. low stroke volume) due to preventing the compensatory mechanism of efferent vasoconstriction – When there is decreased blood flow into the glomerulus via the afferent arterioles,
the efferent arterioles constrict to raise glomerular filtration pressure on the back end
– ACE-I prevent efferent vasoconstriction
• Creatinine can be allowed to be 35% above baseline without stopping the drug. – As forward flow to the glomerulus improves – there is less
need for efferent vasoconstriction to compensate and glomerular filtration will stabilize
• Will cause acute renal failure in patients with bilateral renal artery stenosis – Dilation of efferent glomerular arterioles with no ability to dilate afferent arterioles
which results in decreased glomerular filtration – In bilateral renal artery stenosis there is fixed flow into the glomerulus – an
improvement in stroke volume will not improve flow into the glomerulus •
384 2016
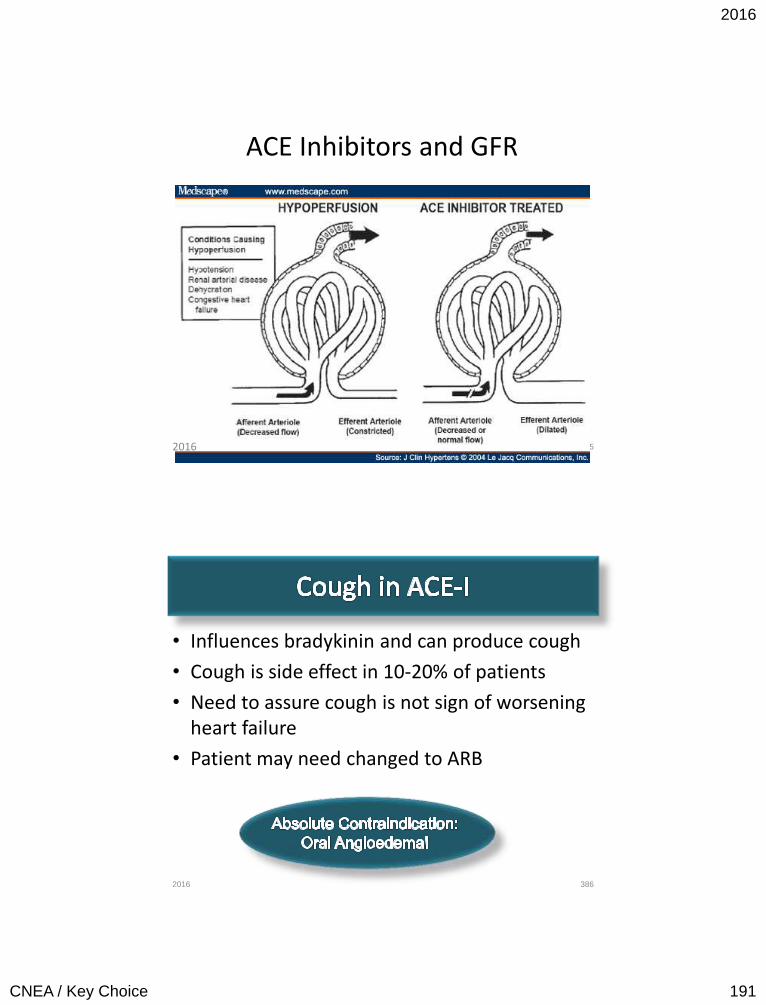
2016
CNEA / Key Choice 191
ACE Inhibitors and GFR
385 2016
• Influences bradykinin and can produce cough
• Cough is side effect in 10-20% of patients
• Need to assure cough is not sign of worsening heart failure
• Patient may need changed to ARB
386 2016
2016
CNEA / Key Choice 192
ACE Inhibitor Monitoring and Contraindications
• Assess renal function and potassium within 1 to 2 weeks of initiation if outpatient
• High risk features for AKI: diabetes, hyponatremia, hypotension, azotemia, potassium supplementation, combination with aldosterone antagonist.
• Note * difference between AKI (hold regardless of creatinine) and CKD may give until creatinine of > 3.0)
387
ESRD: ACE Inhibition ok . SBP most often limiting factor. Need reasonable SBP for
dialysis. Cautions/Contraindications
Bilateral renal artery stenosis Creatinine > 3 mg /dL Potassium > 5.0 mEq/L Systolic BP < 80 mmHg 2016
• ACE Inhibitors remain the first choice for inhibition of RAAS
• ARB’s are a reasonable alternative to ACE Inhibitor if intolerant to ACE Inhibitor due to cough or angioedema
• Reasonable alternative to ACE I as 1st line therapy for patients with mild / moderate HF & reduced LVEF, especially if already take ARB for other reason (HTN)
• Directly blocks angiotensin II
• Combination of ACE I and ARB – not recommended
388 2016
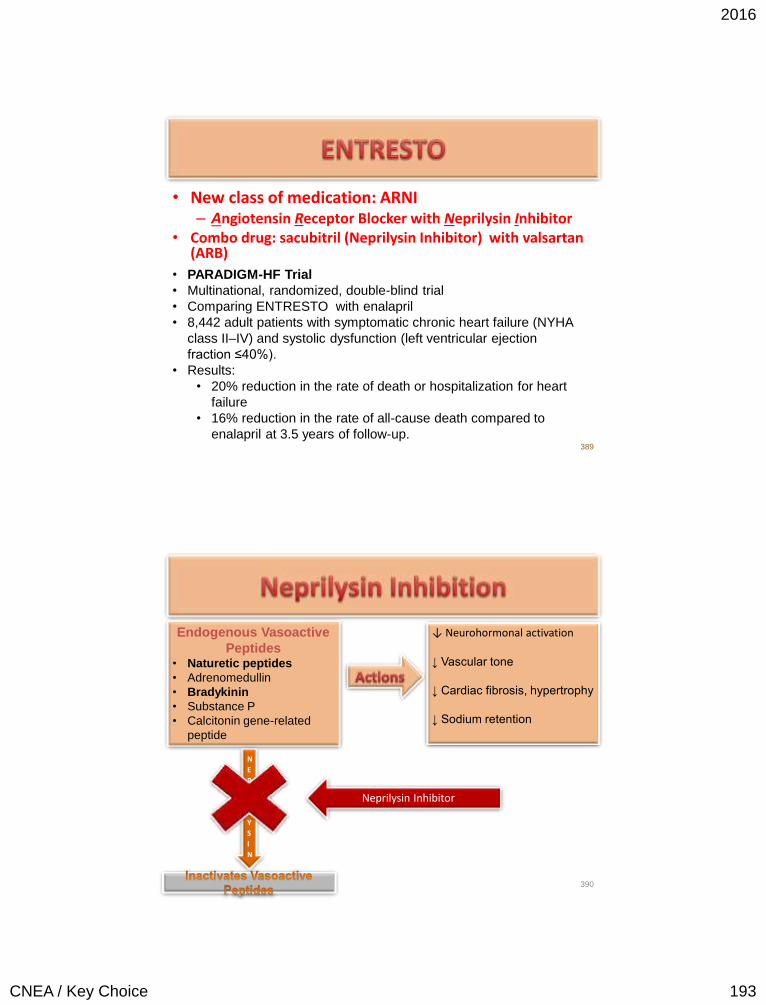
2016
CNEA / Key Choice 193
• New class of medication: ARNI – Angiotensin Receptor Blocker with Neprilysin Inhibitor
• Combo drug: sacubitril (Neprilysin Inhibitor) with valsartan (ARB)
389
• PARADIGM-HF Trial
• Multinational, randomized, double-blind trial
• Comparing ENTRESTO with enalapril
• 8,442 adult patients with symptomatic chronic heart failure (NYHA
class II–IV) and systolic dysfunction (left ventricular ejection
fraction ≤40%).
• Results:
• 20% reduction in the rate of death or hospitalization for heart
failure
• 16% reduction in the rate of all-cause death compared to
enalapril at 3.5 years of follow-up.
390
Endogenous Vasoactive
Peptides • Naturetic peptides
• Adrenomedullin
• Bradykinin
• Substance P
• Calcitonin gene-related
peptide
↓ Neurohormonal activation ↓ Vascular tone
↓ Cardiac fibrosis, hypertrophy
↓ Sodium retention
N
E
P
R
I
L
Y
S
I
N
Neprilysin Inhibitor
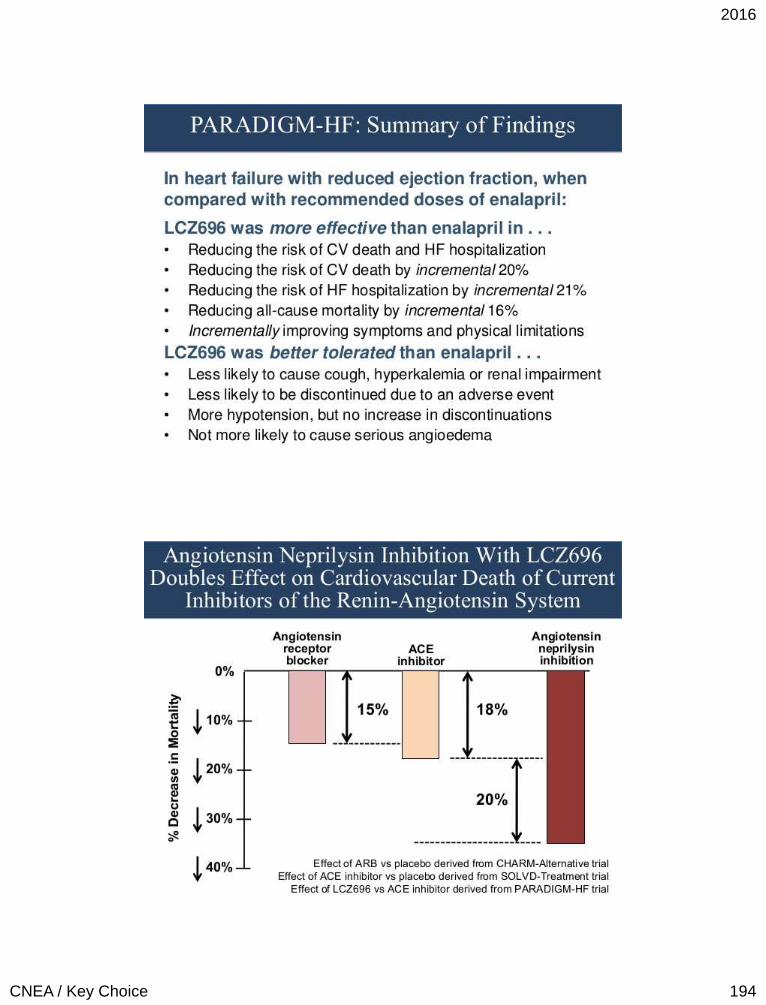
2016
CNEA / Key Choice 194
391
392
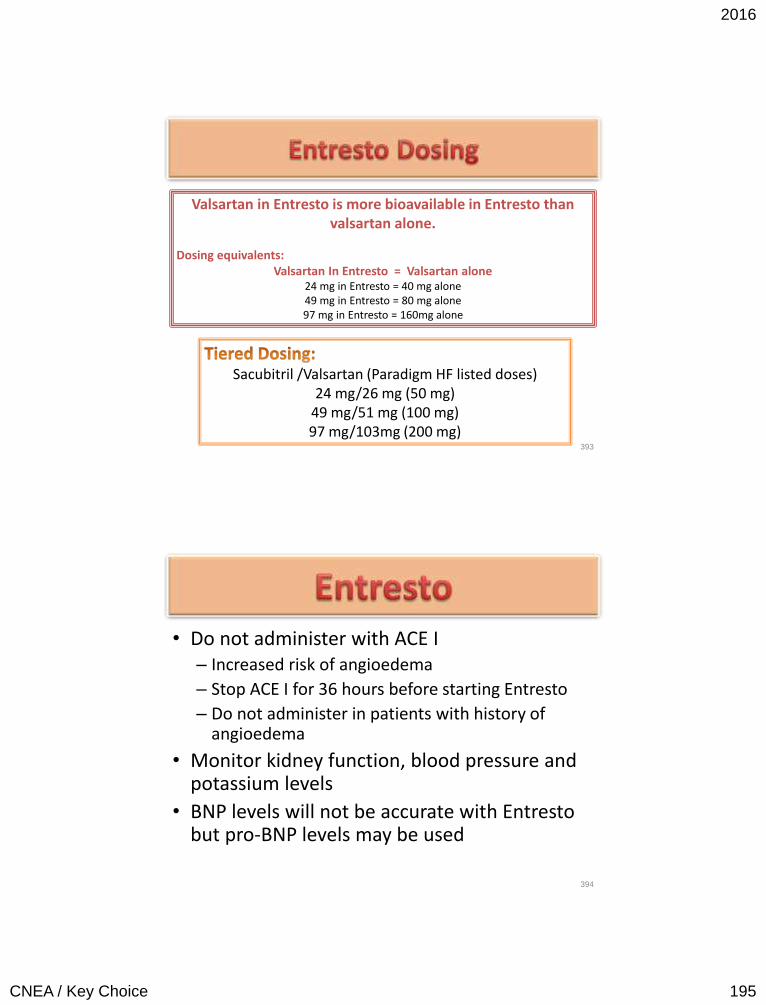
2016
CNEA / Key Choice 195
393
Sacubitril /Valsartan (Paradigm HF listed doses) 24 mg/26 mg (50 mg)
49 mg/51 mg (100 mg) 97 mg/103mg (200 mg)
Valsartan in Entresto is more bioavailable in Entresto than valsartan alone.
Dosing equivalents: Valsartan In Entresto = Valsartan alone
24 mg in Entresto = 40 mg alone 49 mg in Entresto = 80 mg alone 97 mg in Entresto = 160mg alone
• Do not administer with ACE I – Increased risk of angioedema
– Stop ACE I for 36 hours before starting Entresto
– Do not administer in patients with history of angioedema
• Monitor kidney function, blood pressure and potassium levels
• BNP levels will not be accurate with Entresto but pro-BNP levels may be used
394
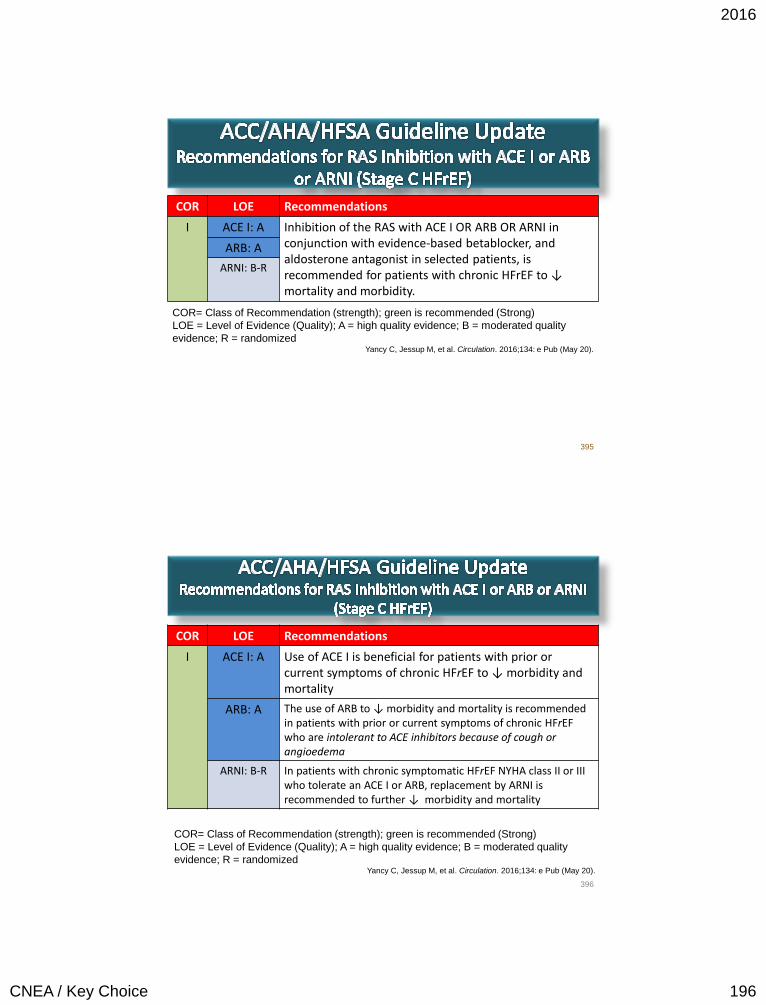
2016
CNEA / Key Choice 196
COR LOE Recommendations
I ACE I: A Inhibition of the RAS with ACE I OR ARB OR ARNI in conjunction with evidence-based betablocker, and aldosterone antagonist in selected patients, is recommended for patients with chronic HFrEF to ↓ mortality and morbidity.
ARB: A
ARNI: B-R
395
COR= Class of Recommendation (strength); green is recommended (Strong)
LOE = Level of Evidence (Quality); A = high quality evidence; B = moderated quality
evidence; R = randomized Yancy C, Jessup M, et al. Circulation. 2016;134: e Pub (May 20).
COR LOE Recommendations
I ACE I: A Use of ACE I is beneficial for patients with prior or current symptoms of chronic HFrEF to ↓ morbidity and mortality
ARB: A The use of ARB to ↓ morbidity and mortality is recommended in patients with prior or current symptoms of chronic HFrEF who are intolerant to ACE inhibitors because of cough or angioedema
ARNI: B-R In patients with chronic symptomatic HFrEF NYHA class II or III who tolerate an ACE I or ARB, replacement by ARNI is recommended to further ↓ morbidity and mortality
396
COR= Class of Recommendation (strength); green is recommended (Strong)
LOE = Level of Evidence (Quality); A = high quality evidence; B = moderated quality
evidence; R = randomized Yancy C, Jessup M, et al. Circulation. 2016;134: e Pub (May 20).
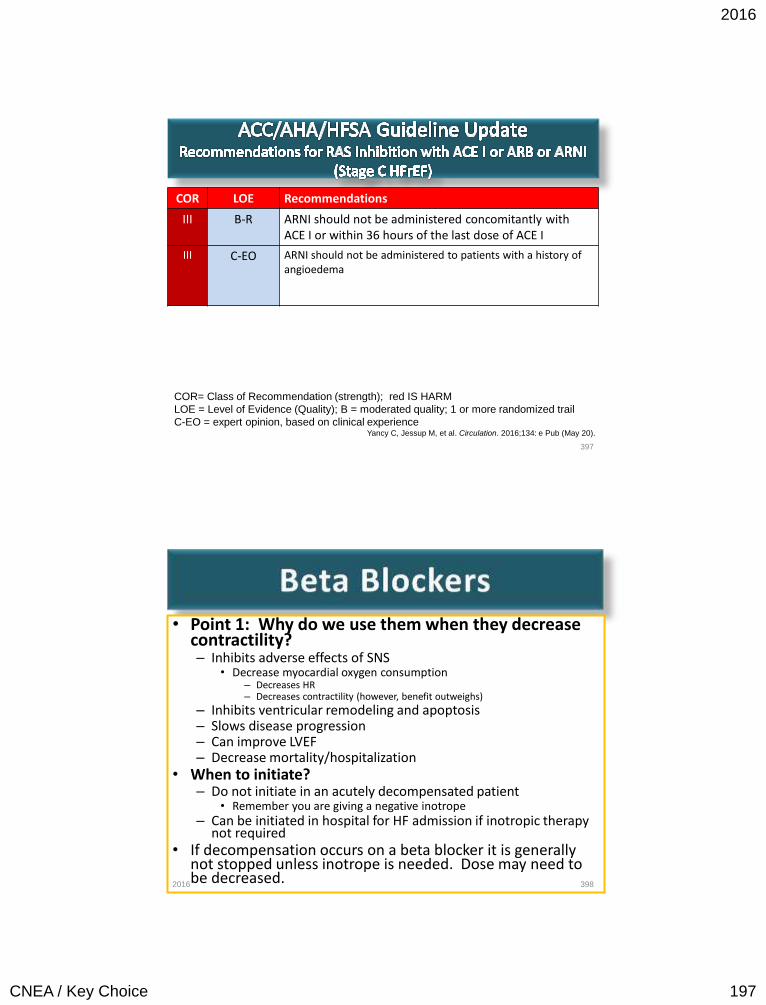
2016
CNEA / Key Choice 197
COR LOE Recommendations
III B-R ARNI should not be administered concomitantly with ACE I or within 36 hours of the last dose of ACE I
III C-EO ARNI should not be administered to patients with a history of angioedema
397
COR= Class of Recommendation (strength); red IS HARM
LOE = Level of Evidence (Quality); B = moderated quality; 1 or more randomized trail
C-EO = expert opinion, based on clinical experience Yancy C, Jessup M, et al. Circulation. 2016;134: e Pub (May 20).
• Point 1: Why do we use them when they decrease contractility? – Inhibits adverse effects of SNS
• Decrease myocardial oxygen consumption – Decreases HR – Decreases contractility (however, benefit outweighs)
– Inhibits ventricular remodeling and apoptosis – Slows disease progression – Can improve LVEF – Decrease mortality/hospitalization
• When to initiate? – Do not initiate in an acutely decompensated patient
• Remember you are giving a negative inotrope – Can be initiated in hospital for HF admission if inotropic therapy
not required • If decompensation occurs on a beta blocker it is generally
not stopped unless inotrope is needed. Dose may need to be decreased.
398 2016
2016
CNEA / Key Choice 198
• Even better in combination with ACE Inhibitor – Started after initiation of ACE-I but before getting to target
dose of ACE-I
• Must be used with diuretic if any recent or current fluid retention
• Start very low doses with gradual up-titration • Titration to target dose essential
• Pearl: If hypotension – consider administration opposite of ACE-I or decrease in diuretic dose
• Pearl: Fatigue may be multifactorial – address over diuresis, sleep apnea and screen for depression
399 2016
• Cannot assume class effect • Bisoprolol – β1
– CIBIS III randomized trial – 2005 (enalapril)
• Metoprolol succinate - β1
– MERIT-HF randomized trial – 1999 (placebo)
• Carvedilol - β1, β2, α1
– CAPRICORN randomized trial – 2001 (placebo)
– COMET randomized trial – 2003 (metoprolol tartrate)
400 2016
2016
CNEA / Key Choice 199
• Mineralocorticoid Receptor Antagonist (MRA)
• ACC/AHA Class IA Recommendation
• LVEF < 35% with NYHA Class II-IV Heart Failure to reduce mortality and morbidity
401
RALES Trial (1999) – 1663 pts
• NYHA Class III-IV
• LVEF < 35%
• Standard rx. vs standard rx.
with spironolactone
• 30% ↓ in mortality
• 35% ↓ in hospitalization
EMPHASIS-HF (2011) – 2737 pts
• NYHA Class II
• LVEF < 35%
• Standard rx. vs standard rx. with
epleranone
• 24% ↓ in all cause mortality
• 42% ↓ in HF hospitalization
• Promotes retention of sodium
• Promotes loss of potassium and magnesium
• Potentiates catecholamines
• Inhibits the parasympathetic nervous system
• Decreases arterial compliance
• Promotes direct remodeling
• Has prothrombotic properties
• Causes vascular inflammation and injury
402
2016
CNEA / Key Choice 200
• Potassium sparing medications
• Any potassium supplements should be stopped after initiating - consider potassium based
salt substitutes
• Counsel patients about avoiding foods high in potassium
Lab Monitoring • Potassium, sodium
and renal function
checked 2-3 days after
initiation and again at
7 days then at the one
month mark. If stable
then every 3 months.
• Adding or increasing
ACE I or ARB should
increase potassium
and creatinine
surveillance. 403
• Non selective aldosterone blocker – Blocks aldosterone and
androgen; stimulates progesterone
• RALES Trial
• Selective aldosterone receptor antagonist
• EMPHASIS-HF
• EPHESUS (Post MI)
404
Major side effect:
gynecomastia (10%), sexual
dysfunction and menstrual
problems due to non
selectivity
Eliminates most
gynecomastia and sexual side
effects associated with
aldactone
2016
CNEA / Key Choice 201
• The combination of hydralazine and isosorbide dinitrate (ISDN) is recommended to REDUCE MORBIDITY AND MORTALITY for : – Self-described African Americans with NYHA class III–IV HFrEF
receiving optimal therapy with ACE inhibitors and beta blockers, unless contraindicated (Class I, LOE: A)
– Anyone with current or prior symptomatic HFrEF who cannot be given an ACE inhibitor or ARB because of drug intolerance, hypotension, or renal insufficiency, unless contraindicated (Class IIa, LOE: B)
405
Self-identified African Americans are thought to have a less
active renin-angiotensin system and a lower bioavailability
of nitric oxide than those self-identified as white.
• African American Heart Failure Trail (2004) - A-HeFT
• 1050 self-described African American patients
• NYHA Class III or IV
• LVEF < 35% or < 45 with a dilated left ventricle
• Currently on standard therapy with BB for at least 3 months prior to enrollment
• Randomized to standard therapy + placebo (1 tablet TID) or standard therapy + 37.5mg of hydralazine and 20mg of ISDN (combined in one tablet TID)
• Dose increased to 2 tablets TID if no side effects with 1 tablet TID
• Trial ended early due to significantly higher rate of mortality in placebo group
– 43% reduction in rate of death from any cause
– 33% reduction in the rate of first hospitalization for heart failure in treatment group
– Significant improvement in quality of life score in treatment group
406
2016
CNEA / Key Choice 202
• Initiation: • Hydralazine 37.5 mg / ISDN
20mg 3 times daily
• Target dose: – Total DAILY dose of
Hydralazine 225 mg (75mg TID) and ISDN 120 mg (40mg TID)
• Bidil – combo drug: – Hydralazine 37.5mg / ISDN
20mg
– 1 up to 2 tablets TID
• Adherence difficult
• Adverse Reaction – Headache
– Dizziness
– GI complaints
407
Consider slower titration to enhance
tolerance
Digoxin • Stage C Recommendations
– Added in patients with persistent symptoms already on ACE Inhibitor, Beta-blocker and diuretic
• Positive inotropic effect – weak effect • Enzyme inhibition in noncardiac tissues – reduces
sympathetic flow • Improved symptoms, exercise tolerance and quality of life • No reduction in mortality • Beta-blocker better for rate control • Low dose: 0.125mg daily • No need for loading dose • Narrow therapeutic range in HF
– 0.5 to 0.9 ng/ml 408 2016
2016
CNEA / Key Choice 203
Impact of HR on Heart Failure
• In patients with coronary artery disease and left-ventricular dysfunction, a heart rate of 70 beats per minute (bpm) or higher was associated with a 34% increased risk of cardiovascular death and a 53% increase in admission to hospital for heart failure compared with heart rate lower than 70 bpm1
• Heart rate is also directly related to risk of death, cardiovascular death, or admission to hospital in patients with heart failure2
• Heart-rate reduction is associated with improved outcomes3
409
1. Fox K et al. on behalf of the BEAUTIFUL investigators. Heart rate as a prognostic risk
factor in patients with coronary artery disease and leftventricular systolic dysfunction
(BEAUTIFUL): a subgroup analysis of a randomised controlled trial. Lancet 2008; 372:
817–21
2. Pocock SJ, et al. Predictors of mortality and morbidity in patients with chronic heart
failure. Eur Heart J 2006; 27: 65–75.
3. Flannery G et al. Analysis of randomized controlled trials on the effect of magnitude of
heart rate reduction on clinical outcomes in patients with systolic chronic heart failure
re
• Sinus node inhibition • Inhibition of the Hyperpolarization –activated
cyclic nucleotide-gated channels (If channel or f-channel or “Funny” channel)
• If current is an inward Na+/K+ current that activates pacemaker cells of the SA Node
• Ivabradine binds the “Funny” channel in a current dependent fashion
• Slows diastolic depolarization → slows the firing of the SA Node → slows heart rate
410
Ivabradine (Corlanor)
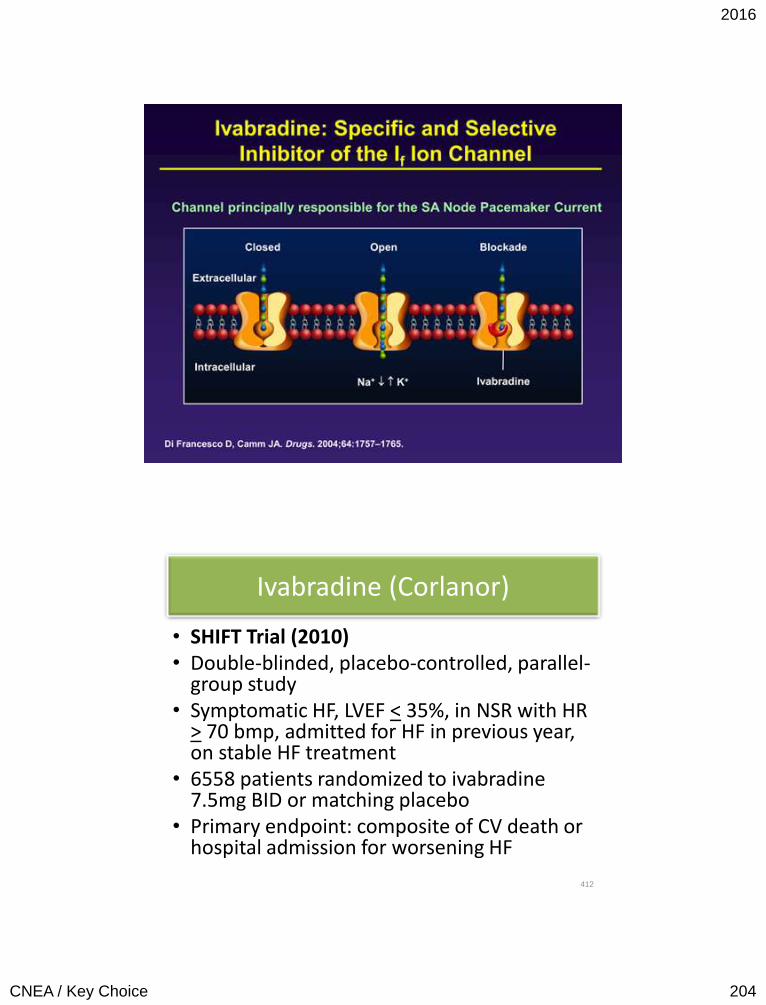
2016
CNEA / Key Choice 204
411
Ivabradine (Corlanor)
• SHIFT Trial (2010) • Double-blinded, placebo-controlled, parallel-
group study • Symptomatic HF, LVEF < 35%, in NSR with HR
> 70 bmp, admitted for HF in previous year, on stable HF treatment
• 6558 patients randomized to ivabradine 7.5mg BID or matching placebo
• Primary endpoint: composite of CV death or hospital admission for worsening HF
412
2016
CNEA / Key Choice 205
Ivabradine (Corlanor)
• Median follow up 22.9 months • Mean HR lowered to • Statistically significant outcomes:
– Composite endpoint (CV death or Hospitalization for HF): 18% reduction with Ivabradine
– Hospitalization for worsening HF: 26% reduction with Ivabradine – Deaths due to HF: 26% reduction in Ivabradine group (CV deaths
and all cause deaths not statistically significant) – The higher the baseline heart rate the better the outcome – Quality of Life scores better with ivabradine
• Side Effect: Phosphenes (visual disturbances) reported in 3% of ivabradine group (1% in placebo – p<0.0001)
413
ACC/AHA/HFSA Guideline Update Recommendations for Ivabradine (Stage C HFrEF)
COR LOE Recommendations
IIa B-R Ivabradine can be beneficial to reduce HF hospitalization for patients with symptomatic (NYHA class II-III), stable chronic HFrEF (LVEF < 35%) who are receiving GDEM, including beta blocker at maximum tolerated dose, and who are in NSR with a heart rate of > 70 bmp at rest.
414
COR= Class of Recommendation (strength); yellow, is reasonable/useful (Moderate)
LOE = Level of Evidence (Quality); B = moderated quality; 1 or more randomized trials;
GDEM: Guideline-directed evaluation and management Yancy C, Jessup M, et al. Circulation. 2016;134: e Pub (May 20).
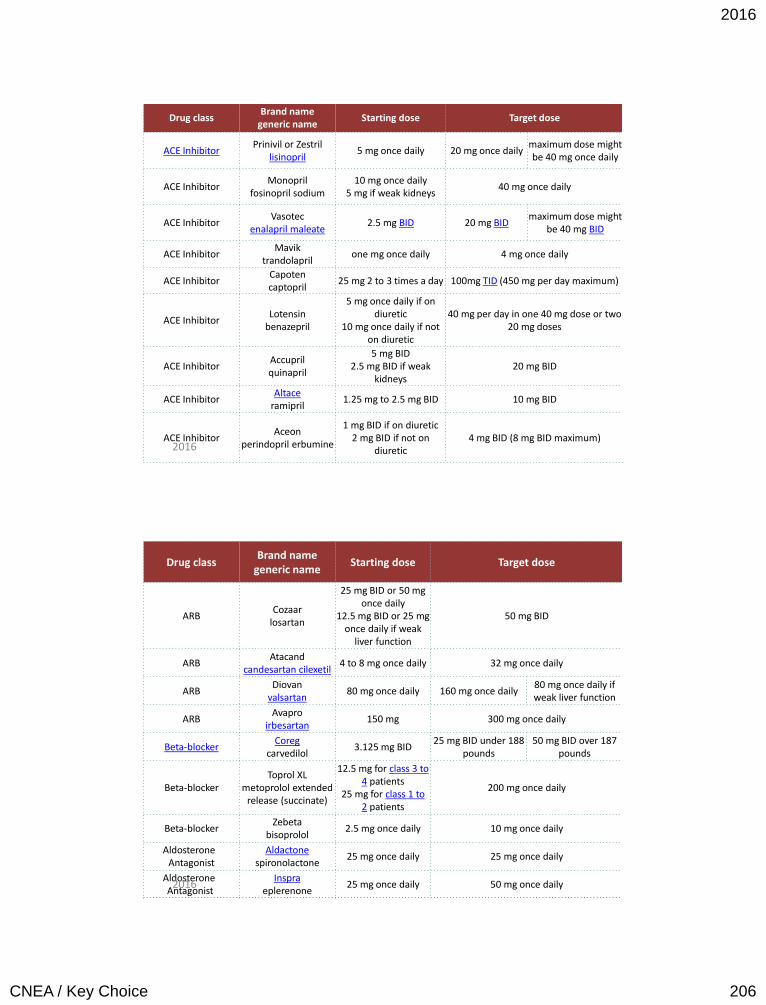
2016
CNEA / Key Choice 206
415
Drug class Brand name
generic name Starting dose Target dose
ACE Inhibitor Prinivil or Zestril
lisinopril 5 mg once daily 20 mg once daily
maximum dose might be 40 mg once daily
ACE Inhibitor Monopril
fosinopril sodium 10 mg once daily
5 mg if weak kidneys 40 mg once daily
ACE Inhibitor Vasotec
enalapril maleate 2.5 mg BID 20 mg BID
maximum dose might be 40 mg BID
ACE Inhibitor Mavik
trandolapril one mg once daily 4 mg once daily
ACE Inhibitor Capoten captopril
25 mg 2 to 3 times a day 100mg TID (450 mg per day maximum)
ACE Inhibitor Lotensin
benazepril
5 mg once daily if on diuretic
10 mg once daily if not on diuretic
40 mg per day in one 40 mg dose or two 20 mg doses
ACE Inhibitor Accupril quinapril
5 mg BID 2.5 mg BID if weak
kidneys 20 mg BID
ACE Inhibitor Altace
ramipril 1.25 mg to 2.5 mg BID 10 mg BID
ACE Inhibitor Aceon
perindopril erbumine
1 mg BID if on diuretic 2 mg BID if not on
diuretic 4 mg BID (8 mg BID maximum)
2016
416
Drug class Brand name
generic name Starting dose Target dose
ARB Cozaar
losartan
25 mg BID or 50 mg once daily
12.5 mg BID or 25 mg once daily if weak
liver function
50 mg BID
ARB Atacand
candesartan cilexetil 4 to 8 mg once daily 32 mg once daily
ARB Diovan
valsartan 80 mg once daily 160 mg once daily
80 mg once daily if weak liver function
ARB Avapro
irbesartan 150 mg 300 mg once daily
Beta-blocker Coreg
carvedilol 3.125 mg BID
25 mg BID under 188 pounds
50 mg BID over 187 pounds
Beta-blocker Toprol XL
metoprolol extended release (succinate)
12.5 mg for class 3 to 4 patients
25 mg for class 1 to 2 patients
200 mg once daily
Beta-blocker Zebeta
bisoprolol 2.5 mg once daily 10 mg once daily
Aldosterone Antagonist
Aldactone spironolactone
25 mg once daily 25 mg once daily
Aldosterone Antagonist
Inspra eplerenone
25 mg once daily 50 mg once daily 2016
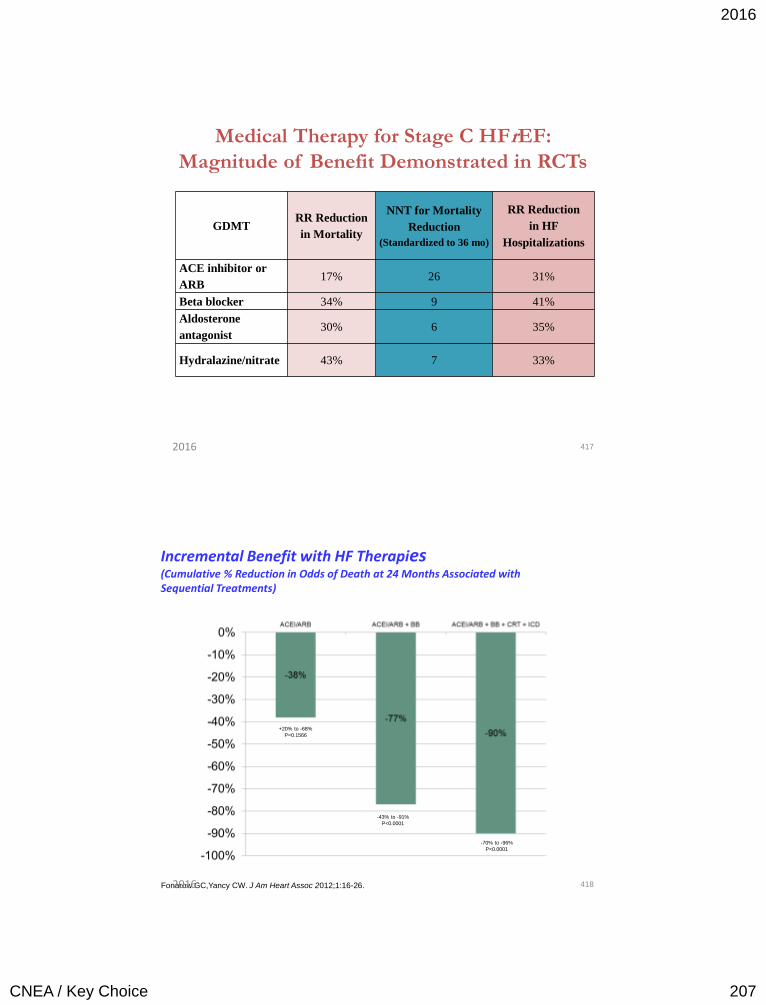
2016
CNEA / Key Choice 207
Medical Therapy for Stage C HFrEF:
Magnitude of Benefit Demonstrated in RCTs
GDMT RR Reduction
in Mortality
NNT for Mortality
Reduction
(Standardized to 36 mo)
RR Reduction
in HF
Hospitalizations
ACE inhibitor or
ARB 17% 26 31%
Beta blocker 34% 9 41%
Aldosterone
antagonist 30% 6 35%
Hydralazine/nitrate 43% 7 33%
417 2016
Incremental Benefit with HF Therapies (Cumulative % Reduction in Odds of Death at 24 Months Associated with Sequential Treatments)
+20% to -68%
P=0.1566
-43% to -91%
P<0.0001
-70% to -96%
P<0.0001
Fonarow GC,Yancy CW. J Am Heart Assoc 2012;1:16-26. 418 2016
2016
CNEA / Key Choice 208
Diuretics • Decrease congestive
symptoms
– No mortality benefit
• First line: Loop diuretics – Thiazide diuretic my be added
• Potassium and magnesium monitoring
• Use with moderare NA restriction
• Fluid restriction criteria
• Monitor response to therapy
– Adequate diuresis
• BNPt goal
• JVP assessment
• Orthopnea
– Over diuresis
• Hypotension
• Dizziness
• Orthostatic BP
419 2016
Diuretic Therapy
Outpatient
• Weight loss goal of 0.5 to 1.0 kg per day
• Patients can be educated for adjustable diuretic dosing • Weight gain
• Weight loss
• Change in oral intake or during periods of illness
Diuretic Resistance
• Diuretic resistance – Reasons
• High sodium levels
• NSAIDs
• Severe renal impairment
• Renal hypoperfusion
– Strategies • IV instead of PO
• Continuous infusion versus intermittent dosing if BP is a concern
• Change the loop diuretic
• Addition of thiazide
420 2016
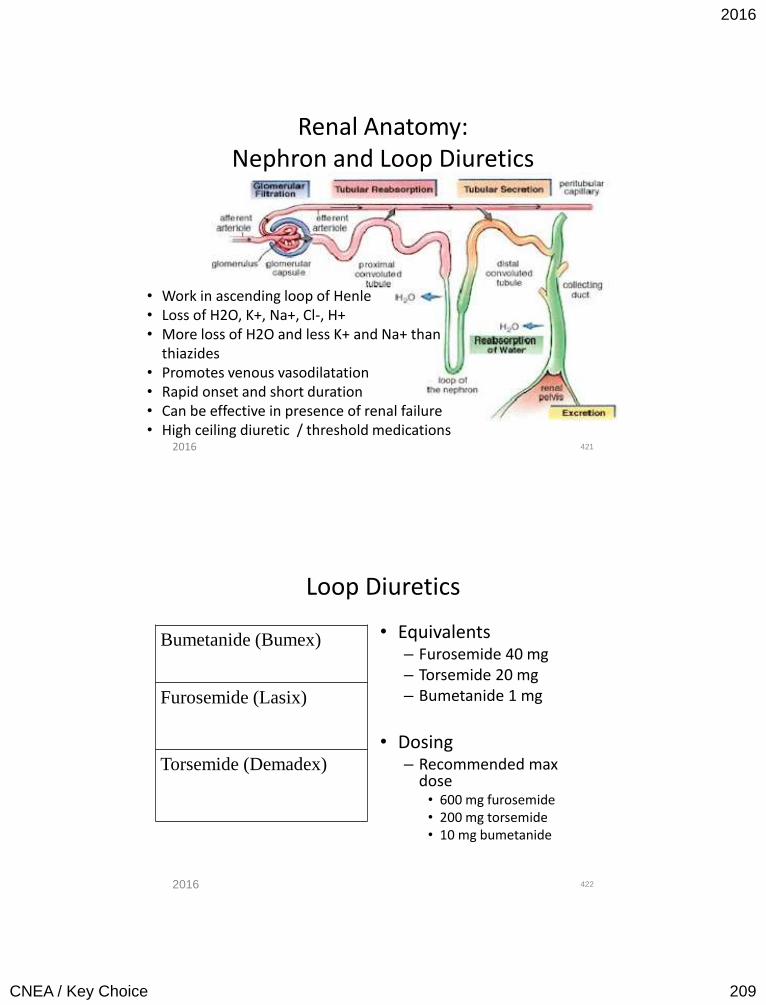
2016
CNEA / Key Choice 209
Renal Anatomy: Nephron and Loop Diuretics
421
• Work in ascending loop of Henle • Loss of H2O, K+, Na+, Cl-, H+ • More loss of H2O and less K+ and Na+ than
thiazides • Promotes venous vasodilatation • Rapid onset and short duration • Can be effective in presence of renal failure • High ceiling diuretic / threshold medications 2016
Loop Diuretics
• Equivalents – Furosemide 40 mg – Torsemide 20 mg – Bumetanide 1 mg
• Dosing
– Recommended max dose
• 600 mg furosemide • 200 mg torsemide • 10 mg bumetanide
422
Bumetanide (Bumex)
Furosemide (Lasix)
Torsemide (Demadex)
2016
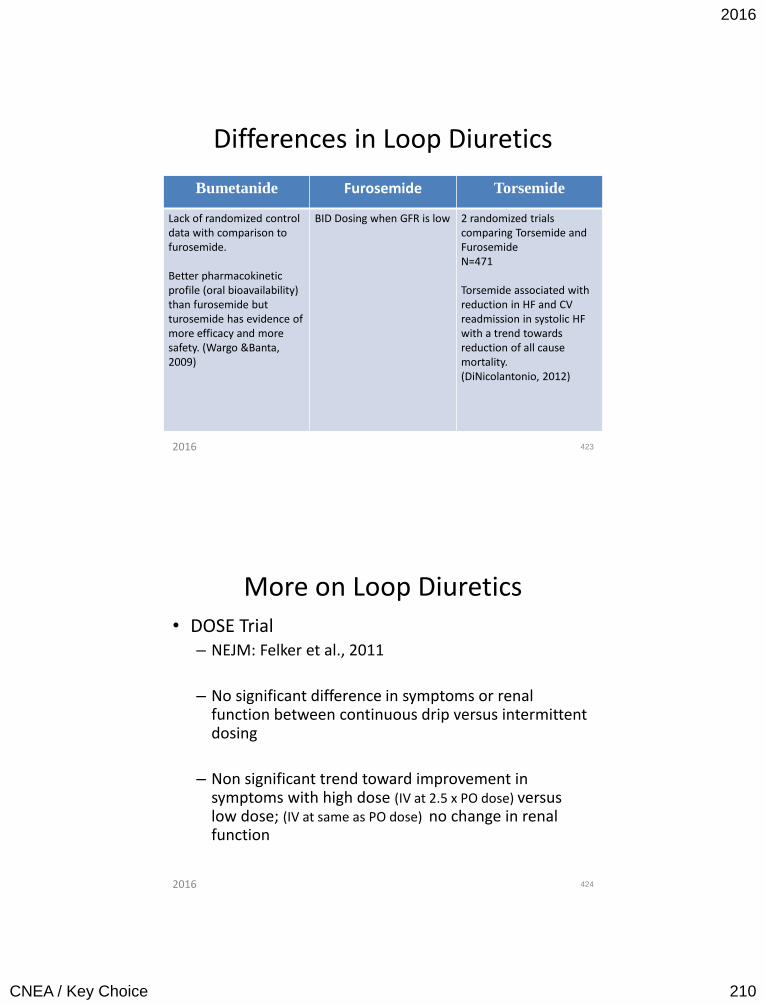
2016
CNEA / Key Choice 210
Differences in Loop Diuretics
Bumetanide Furosemide Torsemide
Lack of randomized control data with comparison to furosemide. Better pharmacokinetic profile (oral bioavailability) than furosemide but turosemide has evidence of more efficacy and more safety. (Wargo &Banta, 2009)
BID Dosing when GFR is low 2 randomized trials comparing Torsemide and Furosemide N=471 Torsemide associated with reduction in HF and CV readmission in systolic HF with a trend towards reduction of all cause mortality. (DiNicolantonio, 2012)
423 2016
More on Loop Diuretics • DOSE Trial
– NEJM: Felker et al., 2011
– No significant difference in symptoms or renal function between continuous drip versus intermittent dosing
– Non significant trend toward improvement in symptoms with high dose (IV at 2.5 x PO dose) versus low dose; (IV at same as PO dose) no change in renal function
424 2016
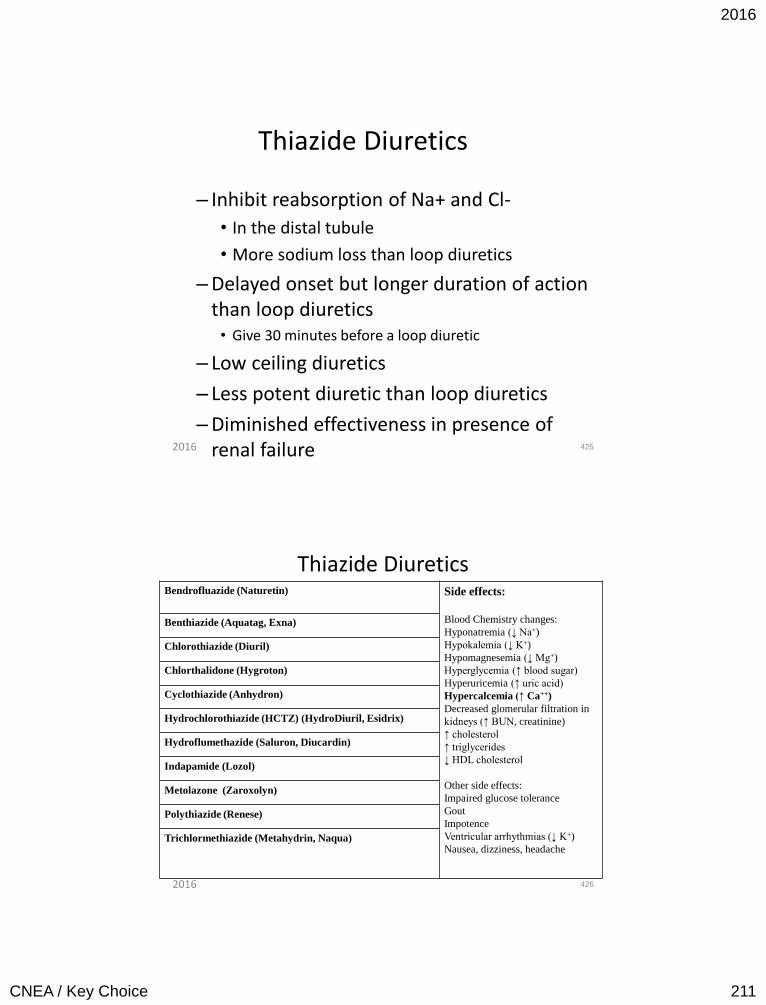
2016
CNEA / Key Choice 211
Thiazide Diuretics
– Inhibit reabsorption of Na+ and Cl-
• In the distal tubule
• More sodium loss than loop diuretics
– Delayed onset but longer duration of action than loop diuretics
• Give 30 minutes before a loop diuretic
– Low ceiling diuretics
– Less potent diuretic than loop diuretics
– Diminished effectiveness in presence of renal failure 425 2016
Thiazide Diuretics Bendrofluazide (Naturetin) Side effects:
Blood Chemistry changes:
Hyponatremia (↓ Na+)
Hypokalemia (↓ K+)
Hypomagnesemia (↓ Mg+)
Hyperglycemia (↑ blood sugar)
Hyperuricemia (↑ uric acid)
Hypercalcemia (↑ Ca++)
Decreased glomerular filtration in
kidneys (↑ BUN, creatinine)
↑ cholesterol
↑ triglycerides
↓ HDL cholesterol
Other side effects:
Impaired glucose tolerance
Gout
Impotence
Ventricular arrhythmias (↓ K+)
Nausea, dizziness, headache
Benthiazide (Aquatag, Exna)
Chlorothiazide (Diuril)
Chlorthalidone (Hygroton)
Cyclothiazide (Anhydron)
Hydrochlorothiazide (HCTZ) (HydroDiuril, Esidrix)
Hydroflumethazide (Saluron, Diucardin)
Indapamide (Lozol)
Metolazone (Zaroxolyn)
Polythiazide (Renese)
Trichlormethiazide (Metahydrin, Naqua)
426 2016
2016
CNEA / Key Choice 212
Diuretics and Renal Function
• Role of venous congestion in worsening renal function
• Role of volume depletion / hypotension and worsening renal function
427 2016
Cardiorenal Syndrome
• Moderate to severe renal dysfunction with fluid overload
– Continue to treat with diuretics
• In severe fluid overload renal dysfunction my improve with continued treatment
• May need to hold ACE I secondary to AKI
• Venous congestion plays a role in worsening renal function (not just hypoperfusion)
428 2016
2016
CNEA / Key Choice 213
Pharmacology for Atrial Fibrillation will be discussed during atrial
fibrillation class in the AM.
429 2016
BE THE BEST THAT YOU CAN BE
EVERY DAY. YOUR PATIENTS ARE
COUNTING ON IT!
www.cardionursing.com
430 2016