Embed Size (px)
Citation preview

CLINICAL MICROBIOLOGY REVIEWS, Apr. 2002, p. 278–293 Vol. 15, No. 20893-8512/02/$04.00�0 DOI: 10.1128/CMR.15.2.278–293.2002Copyright © 2002, American Society for Microbiology. All Rights Reserved.
Integrated Approach to Malaria ControlClive Shiff*
The W. Harry Feinstone Department of Molecular Microbiology and Immunology, Johns Hopkins BloombergSchool of Public Health, Baltimore, Maryland 21205
INTRODUCTION .......................................................................................................................................................278GLOBAL STRATEGY FOR MALARIA CONTROL .............................................................................................279
Background..............................................................................................................................................................279Decentralization of Health Services .....................................................................................................................280Past Achievements ..................................................................................................................................................280Clouds on the Horizon ...........................................................................................................................................281
BASIC CONCEPTS OF MALARIA CONTROL ....................................................................................................281Biological Basis .......................................................................................................................................................281Strategies for Control.............................................................................................................................................282
Mortality control.................................................................................................................................................282Transmission control..........................................................................................................................................283Eradication of malaria .......................................................................................................................................283
TOOLS TO CARRY OUT MALARIA CONTROL ................................................................................................283Personnel and Strategy Development ..................................................................................................................283Environmental Management .................................................................................................................................284Intradomicile Application of Residual Insecticides ...........................................................................................284
Application...........................................................................................................................................................285Selection of insecticides .....................................................................................................................................285Planning ...............................................................................................................................................................285
Insecticide-Treated Mosquito Nets.......................................................................................................................285TECHNIQUES FOR IMPLEMENTATION OF ITN PROGRAMS ....................................................................286
Finance and Subsidy ..............................................................................................................................................286Reimpregnation .......................................................................................................................................................287Sustaining the Intervention...................................................................................................................................287
STRATEGIES BASED ON BIOLOGICAL CHARACTERISTICS OF MALARIA TRANSMISSION ...........287Barrier Spraying .....................................................................................................................................................287Structured Malaria Control ..................................................................................................................................289Evaluation of Efficacy.............................................................................................................................................289
INSECTICIDES, INSECTICIDE RESISTANCE, AND MALARIA CONTROL ...............................................289DIAGNOSIS OF INFECTION..................................................................................................................................290TRAVEL MEDICINE AND PROBLEMS DUE TO GLOBAL CLIMATE CHANGE.......................................290MALARIA VACCINES...............................................................................................................................................291FINALE: ROLL BACK MALARIA...........................................................................................................................291ACKNOWLEDGMENTS ...........................................................................................................................................291REFERENCES ............................................................................................................................................................291
INTRODUCTION
When one looks over the global distribution of malaria inthe 21st century, it is difficult to realize how widespread thedisease has been and how its distribution has diminished dur-ing the past 150 years. This is important because in manyplaces it may have the potential to return if appropriate cli-matic conditions prevail. Historically, malaria fever (ague) wasreported in one form or another from parts of southern andeastern England and seasonally in Holland, Germany, acrosscentral and southeastern Europe, much of Asia, India, China,almost all the Americas, and of course most tropical regions(20). In North America the disease existed in large areas ex-
tending as far north as New York and even Montreal (15).During the U.S. Civil War, possession of quinine was vital forthe warring forces to ensure that large numbers of the menwere not incapacitated by the disease (107). During the mid-19th century, evidence of malaria became more sporadic andthe disease receded from most of central Europe although itremained entrenched in the Mediterranean region and theBalkans (85). In the United States, major modifications ofmosquito habitat through the Tennessee Valley Authority ma-laria control program, habitat degradation, deforestation,flooding, and other effects of development restricted the hab-itat of the malaria mosquito Anopheles quadrimaculatus andled to the local decline of malaria (33). Its eventual disappear-ance was probably due to improvements in life-style, screenedhousing, and the eventual absence of the reservoir within thehuman population. During that period, the prevalence of ma-laria in temperate areas of Europe was declining without spe-
* Mailing address: The W. Harry Feinstone Department of Molec-ular Microbiology and Immunology, Johns Hopkins Bloomberg Schoolof Public Health, 615 N. Wolfe St., Baltimore, MD 21205. Phone: (410)955-1263. Fax: (410) 955-0105. E-mail: [email protected].
278
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

cial efforts (85), while in southern Europe and Turkey, wherethe disease was more endemic, elimination was achieved withthe advent of DDT. Expanded mosquito control programsduring the period from 1950 to 1970 finally brought success inmany parts of the world through the concerted efforts of theWorld Health Organization (WHO) (47). (Table 1)
In spite of these successes, the fabric of many of theseexpanded control programs began to unravel during the early1970s. The appearance of mosquitoes resistant to DDT andother residual insecticides (12), as well as the extreme difficul-ties involved in the supervision and financing of the variousprograms, led to problems which became overwhelming. Thiscan be seen in Sri Lanka, a country with high levels of epidemictransmission in the past. During an epidemic in 1934, 60,000new cases were being reported daily (19). Malaria eradicationcommenced in Sri Lanka in 1947, and in 1963, at the height ofthe eradication programs, only 17 cases were recorded through-out the country. Mass population movements into forestedareas and the withdrawal of intradomicilary spraying withDDT due to the advanced level of control achieved (i.e., tran-sition from attack phase to consolidation phase) contributed tofaltering control, and in 1969, over 500,000 cases were reportedin the country (42). This situation was not unique. Numerousother problems arose because of inadequate field research andalso because eradication was a concept dreamed up by over-enthusiastic authorities who showed little flexibility in theirdrive for completion of the plans (57).
Even in temperate countries from which malaria has disap-peared, the vector mosquitoes still exist as a sort of biologicaltime bomb. Particularly with the threat of global climatechange, all that is required is the reintroduction of sufficientnumbers of gametocyte carriers for the disease possibly to startup again in epidemic proportions (67).
At the advent of the new millennium, malaria continues toplague mankind as a burgeoning problem without any signs ofabatement (47). The current world malaria situation is proba-bly no better that it was 30 years ago, when the emphasis oneradication was replaced by a somewhat defeatist holding pro-gram (121). This new strategy allowed countries to adopt lessthan effective “control” programs, many which were basedentirely on the distribution of the cheap, effective drug chlo-
roquine. This has resulted, in part at least, in a series of prob-lematic situations which eventually led to the breakdown inhealth services and the loss of skilled personnel dedicated tothe study and control of malaria in areas of endemic infection.Additionally, there were biological problems which arose fromwidespread resistance of the parasite to the most effective andbest-tolerated drugs and selection of vector mosquitoes whichbecame resistant to many available insecticides.
WHO has attempted to address this deteriorating situationby holding a ministerial-level conference to develop a strategyto address malaria (123). This culminated in the global strategyfor malaria control entitled “Roll Back Malaria,” which is nowin the process of implementation. The strategy, which is notwithout critics (12) was developed mainly to address Africanconditions, where malaria is most serious. One of the arms ofthis approach calls for the use of antimalarial drugs in analmost unrestricted basis through clinics and health centersand even in the home following simple diagnosis. There is littleemphasis on an integrated approach to malaria control (Table2).
GLOBAL STRATEGY FOR MALARIA CONTROL
Background
Attitudes regarding malaria during the past century havefluctuated between hope during periods when worldwide con-trol seemed in reach, and despair as problems seemed tomount in spite of massive research efforts. For the most part,research thrusts have focused on the development of newdrugs and vaccines (7), with decreasing emphasis on conditionsin the field (124). Now, with the advent of the new century, weare faced with a situation which in many ways is far worse thanin the 1950s, when the plans for eradication were first intro-duced (119). Countries where infection is endemic have lostmuch of the infrastructure which could be used to mount asystematic attack on the parasite and its transmission. Parasiteresistance to available antimalarials is spreading and has ren-dered treatment increasingly difficult for most people exposedto infection (116). In some instances, the possibility of untreat-able multidrug-resistant malaria looms precariously (12).
TABLE 1. People affected by malaria eradicationa
WHO regionTotalb no. of
affectedpersons
No. of persons affected in:
Areas with no malariaor from which it
disappeared withoutspecific measures
Areas originallywith malaria
Areas where malariaeradication was
claimed
Areas where eradication programs were in progressin 1966
Consolidationphase Attack phase Preparatory
phase Total
Africa 212,883 16,318 196,595 3,223 2,733 490 3,223Americas 463,355 308,845 154,510 61,926 40,831 38,737 12,811 92,379South-east Asia 689,123 39,278 649,845 174,983 281,111 153,311 6,531 440,953Europe 739,311 409,207 330,104 269,536 29,946 9,224 39,170Eastern Mediterranean 238,009 60,207 177,802 6,459 11,339 57,900 24,017 93,256West Pacific 232,316 165,190 67,126 18,880 4,288 5,336 9,624
Total 2,574,997 999,045 1,575,952 535,007 370,248 264,998 43,359 678,605
a As of 31 December 1965. Data given by region, excluding China, North Korea, and North Vietnam. Table adapted from reference 129 with permission of thepublisher. WHO, World Health Organization.
b United Nations demographic.
VOL. 15, 2002 INTEGRATED APPROACH TO MALARIA CONTROL 279
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

During the past 40 years or so, major decisions were madewhich guided the world body in its quest to attack malaria andto address the overall health programs in developing nations(48). Successes with vaccines against other diseases promptedresearch to focus on the development of antimalaria vaccines(81). The research effort has helped us to learn much about thedisease and its epidemiology as well as the nature and molec-ular biology of malaria parasites; however, the task of devel-oping a vaccine has remained daunting. Only now are webeginning to investigate the genetic diversity among popula-tions of malaria parasites (11). Such studies will help us tounderstand more about the extent of parasite variability, whichmay impact not only on the way the disease is expressed butalso on how immunity may develop in the human population.This information will greatly affect the strategy of vaccine de-velopment and its use.
Decentralization of Health Services
In the meantime, the ability to control malaria has deterio-rated in countries with endemic infection (106). Within thesecountries, major donors of aid have directed efforts towardpromotion of decentralization of health programs, not specif-ically to handle malaria but to provide more services to therural poor. The process of decentralization has had an insidi-ous effect on the local infrastructure as the technical supportfor such developing nations to attack malaria, or even to de-velop rationally planned control interventions, has been eroded(48). Whereas the concept of decentralization is an appropri-ate basis for dispersing meager health services to the periph-ery, particularly in rural areas, when a professional scientificbody of experts is somehow decentralized the result can bedevastating. As with all scientific endeavour, a critical mass ofexperts is needed to facilitate the work. If these units arebroken up and decentralized, the professional interaction islost and the staff eventually will seek other, more stimulating
activities, leading to a brain drain. Moreover, these staff cannoteasily be replaced, particularly in the atmosphere of decreasingsalaries and bureaucratic deterioration seen in these countries.The study of malaria and its epidemiology and control is ahighly technical enterprise, requiring a body of experiencedscientists to maintain oversight and efficient monitoring of thelocal situations. Without these personnel, ministries of healthare not able to formulate rational malaria control strategiesand hence become dependent on imported technical advisorswho are usually unfamiliar with local conditions and whoseadvice may not be appropriate (103). It becomes difficult forthe ministries to plan effectively for the efficient use of dwin-dling resources, and conditions then deteriorate to the crisissituation we now observe. In the light of this state of affairs,one needs to consider the various options available to malaria-endemic nations to control malaria in the most effective man-ner in their own ecological regions. Hopefully, it is for othersto consider the hurdles that have been placed before thesenations so that appropriate help may be given in the immediatefuture.
Past Achievements
Malaria control as propounded by various expert commit-tees on malaria was a successful enterprise in many ways. It isfrequently forgotten that by 1966 malaria eradication programsglobally had freed some 525 million people (34% of the pop-ulation living in previously malarious areas) from the threat ofthis disease (Table 1). In the Americas, concerted malariacontrol efforts, using both vector control and treatment, hadachieved great success, with massive declines in infection beingseen throughout the region (21). The successful attacks onmalaria produced a strong infrastructure of personnel. Well-trained cadres of malaria control specialists were employedand carried out regular house spraying, treatment of casesdetected by active surveillance, and collection of statistics for
TABLE 2. Global strategy for malaria controla
Item Technical elements (WHO 1993) Implementation objectives Caveat
1 Provide early diagnosis and prompttreatment
Develop paradigms for presumptivediagnosis by mothers or ruralhealth workers; providetreatment in home and clinic(120)
Difficult to implement, particularly whensecond-line drugs are required. Manyfalse positives (10, 35)
2 Plan and implement selective andsustainable preventive measures,including vector control
Expand use of ITN’s, encouragepartnerships, train personnel
Lack of national implementation strategiesmay lead to disjointed programs; somepartners have specific goals (e.g.,UNICEF concentrates on pregnantwomen and children under 5 yr); this isnot malaria control; regular change ofpersonnelb
3 Detect, contain or preventepidemics
Develop epidemiologicalsurveillance
4 Strengthen local capacities in basicand applied research to permitand promote the regularassessment of a country’s malariasituation, in particular theecological, social, and economicdeterminants of the disease
Provide training opportunities forlocal scientists, regular planningon regional basis
Few training opportunities occur incountries with endemic infection alsodifficult to provide satisfactory careeropportunities leading to a brain drainb
a Adopted by Ministerial Conference, October 1992 (120).b Points of discussion at the July meeting of the WHO-Southern African Malaria Control programme, Victoria Falls, Zimbabwe, 22 to 29 July 2001.
280 SHIFF CLIN. MICROBIOL. REV.
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

assessment of the effects (50). In 1959, the Annual ParasiteIndex (the number of positive blood slides per 1,000 popula-tion) for the whole region of Latin America was 0.39. Sadly, by1996 the Annual Parasite Index had increased eightfold andwas 2.46 for the region; for people living in malarious areas, itwas 12.5 (21).
Clouds on the Horizon
By 1966 the problem of anopheline resistance to DDT hadbecome clear. There were 15 species resistant to DDT and 36resistant to dieldrin (127); equally important, chloroquine re-sistance was reported in Southeast Asia and South America(120). Although eradication programs had achieved consider-able success (Table 1), the WHO Expert Committee in 1968adopted a definition that “Areas with technical problems arethose where the planned single or combined attack measurescorrectly applied have failed to interrupt transmission.” By1973, the changes in programs were extensive, with a totallynew approach developed based on implementation of so-calledtactical variants, which identified a series of levels under whichcontrol programs should operate. These ranges from a relianceon chemotherapy alone to reduce mortality (Tactical Variant1) to a reliance mainly on chemotherapy and limited protectionfactors for reduction and prevention of mortality and morbid-ity, particularly in high-risk groups (Tactical Variant 2). Fi-nally, with Tactical Variant 4, countrywide malaria control wasthe ultimate objective (120, 121). This change of strategy beganthe decline in many national malaria control programs. Theeffect of this on the control programs in the Americas has beendisastrous—a profound decrease in house spraying and a de-pletion of trained operatives has resulted in an upsurge inmalaria (21, 45) To illustrate, 1,500 cases were reported fromLoreto Province in Peru in 1965 while 121,268 cases occurredin 1997 (44).
WHO surveillance has revealed that areas of western Asia,Armenia, Azerbaijan, and Tajikistan from which malaria hadbeen eradicated in the 1960s had started to report cases ofmalaria, with several thousand cases occurring in 1994 (12,126). Similar increases have been reported in Turkey (126) andIraq (126); more recently, in South Korea there has been alogarithmic increase in vivax malaria between 1993 and 1997(36). The reasons for this are difficult to summarize, but un-derlying the situation is a loss of international drive to considerthe malaria problem holistically, and part of that is the designbehind the Global Strategy for Malaria Control (12).
In a well-reasoned argument, Baird (12) supports the mes-sage of Butler and Roberts (21) and has delivered a warning topublic health administrators. Both authors think that the twofactors which contributed most significantly to the past controland reduction of malaria were (i) the use of DDT as an indoorspray to attack the vector mosquitoes and (ii) the widespreaduse of chloroquine as an effective chemotherapeutic. Theemergence of chloroquine resistance and the deterioration ofnational control programs that applied DDT (and other insec-ticides) have been coincident with the upsurge of malaria.Currently, the Global Strategy for Malaria Control, which wasdesigned as a lifeline for Africa (Table 2), emphasizes earlydiagnosis and prompt treatment as the major line of attack.While this is appropriate for immediate survival of severe
cases, there is no evidence that it will effectively reduce thetransmission of malaria. Lack of emphasis of the role of vectorcontrol as an intervention against malaria has restricted inte-grated approaches to malaria control (106). Authorities (12,21) feel that this strategy is setting the stage for further spreadand increase of malaria, not only because it deemphasizesvector control but also because it inevitably leads to misuse ofdrugs (home diagnosis and treatment), which will lead to anincrease in parasite resistance and further escalation of themalaria problem (10, 35, 94).
In light of these warnings, it is pertinent now to examine thetools available for malaria control and consider how they maybe used in an integrated approach to regulate this reemergingproblem of malaria in the new millennium.
BASIC CONCEPTS OF MALARIA CONTROL
Biological Basis
Malaria is a focal disease with extremely varied epidemiol-ogy based largely on the reservoir, which may or may not beasymptomatic, and the biting patterns and vectorial capacity ofthe vector mosquitoes. Initially, this complex relationship wasnot well understood, and after the discoveries by Grassi andRoss of the role of mosquitoes in the parasite cycle (20), theseinsects became the main target of control efforts (85). In theabsence of methods to kill adult mosquitoes, the strategy wasto reduce breeding sites. Accordingly, a considerable effort wasmade to drain swamps and marshes and to somehow limit thepopulations of mosquitoes, whether vectors or not. The Pon-tine marshes near Rome and the Hula swamps in Israel areoften used as examples of success in eliminating vector popu-lations (33). However, as pointed out by White these exampleswere not necessarily applicable elsewhere (118). The Sardinianproject (1946 to 1951) against Anopheles labranchiae confirmedthat it was difficult to eradicate an endemic vector by system-atic larvicide application or, even when insecticides were avail-able, by targeting adults by house spraying (58, 85). The pointis that if eliminating mosquito vectors is not an option, whatthen can be done?
Macdonald concentrated on mathematical models of ma-laria transmission and foresaw the importance of the prepatentperiod within the infected mosquito (61). Subsequently, byestimating the duration of prepatency in a mosquito after itsinfective blood meal and the variable life span of femaleanopheline mosquitoes, he reasoned that transmission couldbe interrupted by reducing mosquito survival to less than theduration of sporogony (the mosquito stage of the parasiteleading to the production of infective sporozoites). He sug-gested that this would be more effective in controlling trans-mission than merely reducing the mosquito density (61). Thisis, in fact, the main reason why indoor spraying is far superiorto larvicide application or space spraying to attack the mos-quito populations. To explain this concept, it is necessary tounderstand vectorial capacity.
Vectorial capacity (C) defines the efficiency of a mosquitospecies to act as a vector of the malaria parasite. It is expressedby the formula C � ma2pn/�loge p (38, 39), where C is vecto-rial capacity, m is the relative density of female anophelinemosquitoes to humans, a is the probability that a mosquito will
VOL. 15, 2002 INTEGRATED APPROACH TO MALARIA CONTROL 281
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

feed on a human in a day, ma is the number of times a personis bitten per day, pn is the proportion of the vector populationthat survives the incubation period of the parasite in the mos-quito, and 1/�loge p is the number of days that this proportionis expected to survive. The formula defines the critical role ofthe vector in determining the incidence of infection in anycommunity and supports the theory behind indoor use of con-tact insecticides or insecticide-impregnated bed nets. It calcu-lates the actual level of transmission as well as the epidemiol-ogy and pattern of illness seen in communities with endemicinfection (89). In this expression, pn greatly outweighs theimportance of mosquito density in relation to humans (ma).Thus, for the purpose of limiting transmission, it is more ef-fective to reduce mosquito longevity than to reduce mosquitodensity (118).
This point needs to be reiterated continuously because it isforgotten frequently by those who recommend source reduc-tion, “environmental management,” and other ill-defined con-cepts (93) which serve little purpose other than to deflectscarce resources to abating populations of nuisance mosqui-toes. It is interesting that as early as 1931, systematic housespraying with pyrethrum was introduced (53). The concept was“not intended to destroy all Anopheles gambiae, but only thosewhich are infected. . .largely to be found indoors” (118).
The duration of mosquito survival after an infective biteforms the fundamental basis for the use of indoor spraying orof insecticide-impregnated bed nets to control transmission.The duration of sporogony, the period following ingestion ofinfective gametocytes by a susceptible mosquito prior to thematuration of sporozoites and their migration to the salivaryglands, is dependent on the prevailing temperature conditions.For Plasmodium falciparum, sporogony development in themosquito is inhibited when the ambient temperature falls be-low about 20°C and lasts approximately 10 days at tempera-tures between 25 and 30°C. With P. vivax, development is morerapid at the higher temperature (approximately 6 days) butproceeds, although slowly, even at temperatures around 16°C(61). With all blood-fed mosquitoes, and particularly membersof the genus Anopheles, the females become heavy and vulner-able after a feed, flying to a nearby surface, where they rest andcommence digestion (40). Usually the meal is taken during thenight, and the mosquitoes will seek a secluded corner or hardsurface as a refuge. If this surface is treated with insecticide,the mosquito may acquire a lethal dose. However, even if only
a partial (sublethal) dose is acquired, the mosquito may survivebut must take a blood meal every 2 to 3 days in order toaccomplish oviposition and ensure survival of the species.Thus, before a mosquito can transmit malaria parasites, it willvery probably return to feed two or three times, and at eachoccasion it is vulnerable to exposure to insecticide. The role ofthe insecticide applied to the walls of a hut, room, or mosquitonet is not necessarily to kill the mosquito immediately but toprovide a sufficient dose to kill the mosquito before the infec-tion becomes patent (41). In spite of the current high level ofresearch into the biology of the malaria parasite, control ofmalaria transmission for the foreseeable future will continue todepend on these basic principles.
Strategies for Control
Malaria control is too complex to be addressed by a singleapproach, and any attempt to do so is fraught with danger. Itis important to tailor the strategy to the prevailing ecologicaland epidemiological conditions (78). To illustrate this, defini-tions of the four main patterns of epidemiology (Table 3) arebased on indicators which can be measured in the community.Of significance, the immune status of the population and thepatterns of malaria seen will be different in these four situa-tions and will also affect the strategy for control. Therefore,these will be dictated by the prevailing transmission patternsand will be orientated to the following outcomes: (i) mortalitycontrol, (ii) transmission control, and (iii) eradication.
Mortality control. The major impact of malaria in any com-munity is that of the death of individuals. To prevent a persondying from the disease, appropriate treatment is necessary.The strategy of mortality control involves detecting presump-tive cases, determining which cases are parasite positive, andadministering effective treatment. Such a strategy has littleimpact on morbidity due to malaria and has little or no effecton the overall transmission of the disease. In areas of holoen-demic infection, this morbidity results in a major burden on thepopulation (66).
Mortality control is the main thrust of the current “GlobalMalaria Control Strategy” (Table 2) (123). Since it relies onchemotherapy, no particular program is required, nor is thereany need for nationwide strategies and the development oflocal priorities. All that is required is some means for recordkeeping and a system for distribution of the drugs of choice to
TABLE 3. Classification of levels of endemicity of malaria transmission
Endemicity level Transmission Parasite rate (%)a Comment
Hypoendemic malaria Low: subperiodic or sporadic Usually �10% Mosquito populations unstable, usually difficultto detect; serious epidemics may occur
Mesoendemic malaria Seasonal or periodicfollowing good rains
11–50, dependingon surveytiming
Mosquito populations fluctuate, detectableseasonally; seasonal outbreaks occur; somedetectable immunity in the population
Hyperendemic malaria Intense transmission(seasonal) each year
51–75 Seasonal fluctuation in malaria cases; severesequelae frequent in young children; someimmunity in adults
Holoendemic malaria Transmission may occurthroughout the year withperiods of hightransmission
�75 Mosquitoes detectable throughout the yearalthough with seasonal peaks; high levels ofanemia in very young children; immunityseen in adults
a Rate in children aged 5 to 10 years.
282 SHIFF CLIN. MICROBIOL. REV.
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

the peripheral clinics. Training is minimal and could also in-volve local commercial outlets for antimalaria drugs. It is aneffective stopgap strategy to cope with epidemics of malariawhen emergency situations arise (125). In crisis situations suchas severe flooding or epidemic outbreaks, it is the strategy ofchoice because the tools can be mustered simply and quickly.The main problem is that chemotherapy alone is not a meansof controlling malaria and is not sustainable in the long term.There are good data to indicate that treatments obtained fromunskilled sources are frequently inappropriate and often inef-fective and may promote drug resistance in the parasite pop-ulation (18, 35, 76). The first-line drugs in current use, chlo-roquine and pyrimethamine-sulfadoxine, are becoming lesseffective due to increasing resistance. Replacement drugs arecostly and may not be acceptable for use in understaffed clinics.Effective diagnosis would help with this problem. However,despite the availability of rapid diagnostics that are readilyinterpreted by unskilled clinic workers (71, 91), little effort ismade to introduce them into widespread use. Persistence withchemotherapy alone will buy time but will create very seriousproblems in the future.
This global strategy was endorsed by the technical expertisepresent to advise Ministers at the Amsterdam Conference, butit was not without its critics. The Hon Timothy Stamps, Min-ister of Health for Zimbabwe, noted “If one considers the finaltables in the Global Strategy, one can only presume these to besterile impractical assumptions of a disintegrating scientifictechnology. No significant guidance was offered for countrieslike Zimbabwe which needs to protect her precious humanresources.” As a result of the adoption of the Global Strategy,the Zimbabwe Ministry of Finance refused to continue withthe old programs and reduced annual expenditure on malariacontrol from 3 million to 0.8 million U.S. dollars (106). Suchconcerns are currently expressed, perhaps with greater discre-tion but nevertheless with the same urgency, by Baird (12).
Transmission control. The transmission control strategy rec-ognizes that malaria is an important cause of morbidity as wellas mortality. The disease is extremely debilitating and extractsa high price from the communities affected. Children are ane-mic and unable to concentrate at school (90, 98), and society asa whole is debilitated. Whereas appropriate treatment is oneaspect of the transmission control strategy, vector control isalso a major player, and, properly applied, these aspects to-gether have an impact on both the mortality and morbidity ofmalaria. This approach is effective in most epidemiologicalconditions (Table 3) and is an effective control strategy for asustained attack on the malaria problem. It is adaptable to theuse of insecticide-treated mosquito nets as well as indoorspraying of insecticide (26, 30, 50). It can be implemented inspecific circumstances where malaria is a local priority or on awide scale as part of a major program of intervention. Trans-mission control requires coordination and the development ofstrategic plans to intervene against malaria (50). A high level ofexpertise is needed with personnel trained in epidemiology andvector control as well as in planning, mapping, and communi-cations to coordinate and supervise the operations. However,these would be the prerequisites in countries which have madecommitments to controlling malaria.
Concerns have been raised by some health authorities (24,66) that transmission control will eventually reduce local im-
munity acquired from longstanding infection in the population.This is true. Effective transmission control will reduce theincidence of infection and reinfection in the community, andeventually people will lose their acquired immunity. Therefore,such interventions should be planned in a sustainable manner.It is incumbent on the local government to recognize this whenmaking commitments to malaria control. However, the tech-nique can be incorporated into national malaria controlschemes on a stage-structured basis in areas of high priority. Itis even possible to create barriers to seasonal encroachment ofvector populations and the potential for transmission to invadepopulated areas or towns (51).
Eradication of malaria. Eradication can be considered onlyin certain areas, e.g., in places where malaria has been eradi-cated and where it has been reintroduced and in areas ofhypoendemic malaria where there are sufficient resources toundertake the process and where there is little likelihood offuture introduction. The advantage of an eradication programis that it is time limited and, once it has achieved its objective,can be terminated with little further oversight (119). In Table1 the relative successes of the various malaria control activitiescommenced in the mid-20th century period are outlined.Clearly, eradication programs were extremely successful, buteradication could not be achieved in many places and thetechnique must be considered not appropriate in most areas ofendemic infection.
TOOLS TO CARRY OUT MALARIA CONTROL
Personnel and Strategy Development
Malaria control is a scientific, technical activity that requiresskilled and dedicated staff with training in epidemiology, en-tomology, mapping and planning, and manpower manage-ment. Since much work is in the field, it requires personnelprepared to undertake field work. This is not an arena for pureclinicians or laboratory scientists, and although all play a rolein the fight against malaria, the control operations are therealm of malariologists (45). The most important tools to con-trol malaria consist of properly trained personnel with author-ity to coordinate and carry out their scientific work (94).
The rest of the tools to control malaria are still fundamen-tally similar to those used for eradication and control pro-grams, i.e., the use of insecticides directed against adult mos-quitoes to reduce the pressure of transmission in the humanpopulation and effective treatment to cure cases as they arediagnosed. In spite of years of research, there are no newtechniques; in fact, with the advent of drug-resistant P. falci-parum, we now have a less effective battery of drugs which canbe applied safely in community-wide programs (37, 48).
What has been learned over the past several decades is thatspecific control strategies should be developed for specificcountry conditions and that there is not a “one set fits all”method available. We now understand the ecological condi-tions which affect and regulate the distribution and abundanceof mosquito populations (41). Essentially, efforts to controlmalaria must be sustainable and rely on the double-prongedattack while the sustainability of programs will depend greatlyon the local resources available and should not depend only ondonor support. The extent of a sustainable control program
VOL. 15, 2002 INTEGRATED APPROACH TO MALARIA CONTROL 283
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

will, of necessity, depend mainly on local resources, which willthen dictate local priorities. The simplest approach, therefore,is to rely on widespread chemotherapy in populations at risk.However, wherever possible (and even in areas of restrictedpriority) this should be combined with vector control (96). Theuse of vector control is not an ancillary factor that can beconveniently disregarded. It is essential not only to reducetransmission but also to prevent the development of drug re-sistance within the parasite population (76). There are goodexamples from Zimbabwe of the synergistic effects of the twomethods where integrated malaria control has been in effect inselected areas for over 50 years (111; K. Day, personal com-munication). In a recent nationwide survey, chloroquine resis-tance has been found to occur with any frequency in only threedistricts in spite of its use as the first-line drug for all that timeand in spite of the advent of widespread chloroquine-resistantP. falciparum parasites in surrounding countries, e.g., Zambia(16, 69, 76). Additionally, combined vector control and pro-phylaxis using Deltaprim (pyramethine-dapsone) has been un-der way on a large sugar estate covering a resident populationof 50,000 persons for over 40 years. The local Chief MedicalOfficer indicates that there is no transmission of malaria orbreakthrough in prophylaxis on the estate, whereas transmis-sion does occur in adjacent areas (A. Morar, 2001, personalcommunication).
Environmental Management
In a variety of texts, environmental management is proposedto reduce the number of breeding sites and overall populationsof vector species (93, 96, 122). As mentioned above, there havebeen some situations where source reduction was effective(85). However, on the whole, anopheline mosquitoes are op-portunistic breeders that favor open sunlit pools or smallstreams and rivulets (Table 4). In most cases it is impractical tosuggest source reduction as an effective control effort foranophelines. Since anophelines are opportunists, their popu-lations expand during rainy spells and they breed in such avariety of situations that any attempts to limit the extent ofsuitable habitat will not be very successful. Importantly, it isnot the number of mosquitoes that is critical in the cycle but,rather, the length of mosquito survival which contributes to theefficient transmission of malaria (40, 60).
Controlling mosquito breeding sites by using spreading oilsor by source reduction is often promoted by health authorities
as a means of limiting nuisance mosquitoes. This is commend-able since the pests are a considerable irritant to the humanpopulation as well as to domestic animals; however, most peri-domestic breeding mosquitoes are culicines, which are notinvolved in the transmission of human malaria. However, un-der certain conditions, e.g., in India, where important vectors(A. culicifacies and A. stephensi) are swamp or pool dwellers,drainage, the use of larvivorous fish (guppies), or even intro-duction of polystyrene beads into some habitats may effectivelyreduce some populations of mosquitoes by reducing the sur-vival of larvae and pupae (97). However, the reduction is tem-porary if not properly managed, and even in India this strategydoes not control an alternative vector, A. fluviatalis; hence, ithas only limited effect on malaria transmission (108).
Any program to control malaria must be tailored to thespecies of vectors which are involved in transmission. Antima-laria interventions should be implemented in a coordinatedmanner by an authority which has the technical support andpolitical power to carry out the programs. In several countries,particularly in Africa, numerous projects are operated througha number of agencies which are uncoordinated and which mayhave a variety of agendas. Each might provide some localeffect, but none will be sustainable without a national programwhich is developed to meet the goals of the local people (gov-ernment) and which will be sustained and supervised by gov-ernmental agencies. Sporadic, uncoordinated short-term inter-ventions are not part of a goal-orientated integrated malariacontrol intervention. Even the Global Strategy acknowledgesthe coordinating role of government (123). This is necessary toset priorities which will benefit the nation and help develop astrategy and to fund and implement the control program (124).
Intradomicile Application of Residual Insecticides
Intradomicile application of residual insecticides, also referredto as indoor spraying, has been the mainstay of malaria controloperations since the early parts of the last century. Because therationale for this method is based on the feeding and restinghabits of most malaria vectors, it is important first to understandthese characteristics of the species of concern. While crepuscular(twilight) feeding patterns have been noted in a few instances, themajority of important vectors feed late at night, with peak bitingactivities between the hours of 20:00 and 05:00 nightly (117).Although some species prefer to feed outdoors, endophagy (in-door feeding) is most common (78, 117).
TABLE 4. Larval breeding sites of Anopheles spp.
Type of habitat Characteristics
Permanent or semipermanent standing freshwater ......................Large open marshes or marshy margins to lakes and pondsSmall ponds, pools or borrow-pits; spring-fed pools and seepagesStanding water in fields, rice fields, open wells, forest pools or swamps
Transient freshwater collections......................................................Open pools in fields, stagnant water in streambeds and cattle hoof-prints, poolsin car tracks and road ruts
Permanent or semi-permanent running freshwater......................Open streambeds with vegetation or running over gravelFlowing water in canals and ditches, streams in forests and plantations
Brackish water ...................................................................................Marshes, ponds and swamps (not tidal), ponds near salt pans and vleis (dambo)Tidal swamps
Container habitats (seldom used by anophelines)........................Rock holes, tree holes, plant axils and epiphytic water-bearing plantsDiscarded containers (natural and artificial), tins, and tiresCrab holes and cracks in drying mud; water cisterns
284 SHIFF CLIN. MICROBIOL. REV.
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

Application. The proper application of insecticide is nottrivial and, if incorrectly carried out, may be quite ineffective.Although applications can be done by unskilled personnel, ahigh level of supervision is necessary (50, 96). The work isdifficult and usually involves hot and sometimes cramped con-ditions; people tire easily and need encouragement. Addition-ally, inefficient spraying and even misuse of the insecticidecould occur if supervision is lacking or conniving. To preventor control this, it is necessary for rigorous inspection to becarried out frequently.
Since spray operations are critical in regulating the actualtreatment of the walls and eaves and around immovable fur-niture, a period of training is necessary (96). Wettable powderformulations cause abrasion of the spray nozzles, and so theseneed to be inspected regularly to ensure correct application ofthe spray (118). Ideally, spray solutions should be made up ata concentration which will treat a specific number of rooms(Table 5). Before application of insecticide, all furniture, hang-ing clothing, cooking utensils, food, and other items should beremoved from the house and left covered outside. Indoorspraying is a very intrusive operation. Strangers are admittedinto one’s private space, which is often a major problem to thehomeowner. It also involves heavy lifting to remove items offurniture and personal effects prior to the spraying. If there areno real perceived benefits such as destruction of pests or nui-sance insects, people soon object to the work, and so it isimportant to ensure an ongoing public-relations effort to ex-plain procedures and motivate the community.
Selection of insecticides. A variety of insecticides are cur-rently available, and the most appropriate for specific condi-tions must involve careful study by entomologists (Table 5) andsupport of local opinion. For example, the use of DDT orsimilar wettable powder may introduce transport costs, sincethe formulation is heavy and difficult to transport by bicycle. Inthe past, organophosphate insecticides such as malathion (Ta-ble 5) were substituted for the organochlorines DDT and BHC(118, 128). However, the cost and increased household disrup-tion involved with the repeated applications needed for effec-tive mosquito control have made these compounds unpopular.If these insecticides are replaced by Deltamethrin or Icon,much less material is required and a daily supply can be easilytransported by bicycle (5, 110). Other features such as odorand wall staining are important and must be reviewed with the
community. Finally, there is the element of cost; however,decisions about supply and expense are usually the subject ofcommercial tenders, and final selection is often done by inde-pendent sources.
Planning. Planning indoor spraying operations requires con-siderable effort on the part of the health authorities and in-volves careful mapping of all houses, location of the roads androutes of access, and generation of the daily work allocation toensure that the community is appropriately warned before thearrival of the spray teams etc. There should be means foridentification of houses so that the records of the spray teamscan be checked on the ground. All the logistics, supplies, andtransport needs must be delineated and budgeted so that theteams and supervisors all know their duties, allowing the dailyschedule to be properly carried out (50, 111).
Insecticide-Treated Mosquito Nets
The development of synthetic pyrethroid insecticides whichare stable and remain effective for long periods enabled ento-mologists to test the idea of impregnating mosquito nets ofvarious textures and fabrics as a vehicle for residual insecticide.Much has been written about this technique, which is now wellunderstood and has proven effective (26, 29, 52, 54) (Table 6).The initial seminal research was carried out in a series of hutsin Tanzania (52). The well-designed experiments of Lines et al.answered several important questions before the rationale forthe use of insecticide-treated mosquito nets (ITNs) could beestablished (56). In a series of trials with volunteers sleepingeither under treated nets or under or adjacent to a treated netor in huts with no nets at all, the effects on the viability ofexiting mosquitoes was discerned through the use of windowand eave exit traps. Nets treated with permethrin were used forthis work, and the excito-repellency of this insecticide wasdiscernible in the results. Blood-fed mosquitoes were found inexit traps, but there was higher mortality among mosquitoesexiting rooms with treated nets than among mosquitoes exitingrooms where no treatment was used. This effect was seen withnets of various dimensions, nets with holes, or torn nets andeven when nets were improperly tucked in or when peopleslept on wood frames without mattresses (56).
It is important to return to the basic concept of transmissioncontrol, i.e., reduction of vector life span. Conceptually, the
TABLE 5. Comparison of six insecticides used for house sprayinga (WHOPES-approved products)
Feature Organochlorine(DDT 75% WP)
Organophosphates Carbamates Pyrethroids
Malathion50% WP
Fenitrothion40% WP
Baygon 75%WP (propoxur)
Ficam 80% WP(bendiocarb)
K-othrine 2.5%(deltamethrin)
Icon 10% WP(�-cyhalothrin)
Application rate (g of ai/m2)c 2 2 1 2 0.4 0.025 0.025Residual efficacy duration (mo) 6–12 2–3 4 2–3 2–3 6–12 6–12Cost (US$)/kg (product) 3 7 8 20 80 40 75Cost (US$)/house (200 m2) 1.6 5.6 4 10.5 8 8 3.75Operational cost ratiob 1.1 5.6 2.5 7 1 2 0.23Stains walls? Yes Yes Yes Yes No No NoControls other pests? No Some Some Yes Yes Yes YesOdor? No Yes Yes Yes No No NoRefusals? Yes Yes Yes Yes No No No
a Adapted from reference 118 with permission of the publisher. These insecticides are WHOPES-approved products.b The operational cost ratio is defined as the cost per house/freight-saving factor and is given in U.S. dollars for 1996.c ai, active ingredient.
VOL. 15, 2002 INTEGRATED APPROACH TO MALARIA CONTROL 285
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

nets serve as a vehicle for the insecticide. Any ingressing mos-quito must probe the protecting surface until either it is re-pelled or finds a hole to enter. This may happen with a treatednet, and the mosquito can take a blood meal. When satiated,the insect must then probe again, trying to find an exit. Duringthe process it will acquire a dose of insecticide. This may not beimmediately lethal, but over several feeding excursions theinsect will probably acquire sufficient insecticide to die andthus not transmit the infection (40).
The use of ITNs is a new and somewhat revolutionary tool foreffective vector control. There is very little infringement on per-sonal privacy, and the application of insecticide does not involveseasonal upheaval of furniture, clothing, etc. The method evenprovides effective protection from a major source of nuisance,that of nightly disturbance by mosquitoes (102), as well as de-stroying bed bugs and other pests (114). However, it is necessaryto note that untreated or improperly treated nets alone do notprovide effective protection from mosquito bites, and toutingthem as a means of personal protection may be misleading. Mos-quitoes can feed through the net when body parts touch thenetting, and access through small holes is well known.
Although ITNs are effective (52), there has to be extensivecoverage and use of nets to achieve a substantial reduction inmalaria transmission, in the same way that this needed forindoor spraying to be effective (17, 30). In a Tanzanian project,household coverage approached 75%, and contributed to areduction in slide positivity (relative risk, 0.45) and febrileepisodes (relative risk, 0.38) and improved weight gain in chil-dren younger than 5 years who slept under treated nets (90,98). There was also a major impact on the density of infectedmosquitoes in the protected areas (99, 113). There is littledoubt about the efficacy of the system in reducing both childmortality and morbidity (3, 82). The use of ITNs could beintegrated into any national malaria control strategy. Depend-ing on the behavior patterns of the local vector species, ITNscould replace indoor spraying in many instances (74). Themain problem to be addressed is the process of implementingand sustaining operations which are dependent on communitysupport. Whereas indoor spraying can be carried out by gov-ernment edict in a centrally planned, vertical-type program,
ITNs can be introduced only in a systematic manner via awell-informed and committed community. Public informationis a necessity and must be seen as an ongoing activity.
TECHNIQUES FOR IMPLEMENTATIONOF ITN PROGRAMS
Finance and Subsidy
Any discussion about financing public health programsraises the important issue of subsidy, particularly when onesection of society bears the impact. To what extent can theoverall cost be shared? In developed countries, impoverishedcommunities are seldom expected to bear the entire brunt of apublic health intervention which in the long run will benefit thenation as a whole. This reviewer asks, should not those com-munities embracing malaria control activities for both personaland public good be entitled to some subsidy to defray theirindividual costs? One proceeds with an assumption of a re-sponse in the affirmative, even in light of certain agenciesrequiring full cost recovery. While such cost recovery mayappease many economists, this is not the basis of public health.
There are several approaches for financing the distributionof ITNs as a means of vector control, ranging from outrightgifts to sale of the items at commercial or subsidized prices. Inthe first situation, there is the hope that recipients will respectthe items and use them for the purpose of malaria control.Alternatively, agencies are encouraging the sale of treated netsas a commercial activity promoted by advertising, together withsome health education and some form of cost recovery (9). Itis now accepted that the concept of sale and private ownershipof mosquito nets is likely to be acceptable and result in theirgeneral use (9, 65, 105). Current information indicates thatwith the more active pyrethroids, e.g., deltamethrin, annualtreatment will be sufficient (28). Merely handing out the netsdoes not mean they will be used, and there is considerable riskthat many of the free nets will be sold on the open market bythe recipients rather than used for protection against malaria.More importantly, if they are part of an overall strategy formalaria control, then the system will not achieve its overall
TABLE 6. Implementation of malaria control by using ITNs
Activity Critical implementation conditions Implementation process
Strategy Concept should be incorporated in a national malariacontrol program based on vector control
Nets and insecticide sold or distributedto target communities
Promotion (type 1) Education to inform and convince population; supervisionand coordination by community leaders (or malariaaction committee)
Community involvement
Promotion (type 2) Role for trained technical support staff; overall supervisionand monitoring of all implementation activities
Strong, motivated support scientists;need overall authority forcoordination and control
Affordability Public are asked to bear some costs; need for marketing ofcommodities and subsidy to purchasers; arrangementsfor assisting impoverished persons
Honest and transparent financialtransactions under coordinatingauthority
Insecticide use Proper treatment and reimpregnation of nets is essential;education of target communities, careful supervision,and motivation needed
Supervision and control by dedicatedtechnical personnel
Evaluation Trained epidemiologists, entomologists, and support staffmust be employed by malaria control authority
Deployment of trained staff to collectdata; adequate facilities includingtransport; computerized support
286 SHIFF CLIN. MICROBIOL. REV.
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

objective. With personal ownership in mind, there are twomain approaches to consider.
The first is the sale of subsidized ITNs, with the proceeds orprofits being converted into a community-held revolving fundthat pays for sustaining community participation, purchase,and distribution of replacement nets as needed (79). If netsretail at approximately 75% of the street price, people are notinclined to sell or otherwise dispose of them (9, 102). Thesenets and additional insecticide can be obtained with somesubsidy through the commercial sector, and the whole enter-prise would be overseen by trained research and control offic-ers who are retained by the Ministry of Health. Such a systemwas developed by the Bagamoyo Bednet Project (65).
The second is the promotion and sale of necessary itemsthrough a process of “social marketing” within the community.The nets and insecticide are packaged attractively and madeavailable for sale through commercial outlets, although thepromotional activities and some of the distribution costs areunderwritten via large donor agencies (62, 105). A largeproject under the name KINET has reported success in south-ern Tanzania but with subsidies of 33 and 83% for the nets andinsecticide, respectively (9). Reports available on these activi-ties usually focus on the success of sales but omit anythingabout reimpregnation activities (105).
These systems both require an input of external financialsupport because the full commercial cost of both nets andinsecticide will preclude ownership and use by large sections ofthe public. If ownership of ITNs is limited to those who canafford them or to a small section of the community such aspregnant women, these individuals may get some personalprotection but the efforts will not contribute to malaria controland could not be considered an effective element of a publichealth intervention against malaria.
Reimpregnation
A key element in the ITN program is the need for nets to beretreated regularly with insecticide. Without reimpregnation,the nets will lose their function as vector control agents (Table6). It is essential that concerted efforts be made to ensure thatpeople understand that the nets must be retreated regularly(annually) and that they should bring the nets to a center tohave this done (or treat the nets themselves) (72, 73, 102). Thistask requires effort on behalf of the community and the super-visory staff. Also, logistics concerned with procurement, distri-bution, and use of insecticides must be put in place. Misuse ofthe insecticides must be scrutinized to ensure proper retreat-ment activities, and cash flow must be transparent and properlymanaged. In rural areas where community participation is anintegral part of the program, financial remuneration for theworkers may be necessary; this can best be done with a revolv-ing fund where the interest accruing may be used for paymentof services rendered by the committee (65, 102).
The issue of regular retreatment of nets has been the subjectof much research and debate (9, 27, 29, 75). It is now consid-ered that ITNs operate with similar efficiency to indoor spray-ing programs but with certain advantages (Table 6). Industryhas developed single-dose tablets of deltamethrin (KO-Tabs)for individual use, but these packages are more expensive thangroup treatments. Large-scale treatments usually cost about 20
to 30 cents (U.S. currency) per net for the insecticide. Re-cently, nets produced under the name Permanet and treatedwith a propriety formulation of deltamethrin have beenclaimed to remain insecticidal for up to 4 years. Curtis (C. F.Curtis, abstract from the Vector Control Workshop hosted bythe London School of Hygiene and Tropical Medicine in Sep-tember 2001, abstr. 2.2, 2001) has tested these pretreated poly-ester nets, but there has not been sufficient time to determinethe duration of insecticidal efficacy. In comparative trials, theknockdown time for bioassay with mosquitoes (300 s) wassimilar for both Permanet and normal nets treated with thesame dose of deltamethrin; even after 20 successive launder-ings, the knockdown time was similar (600 s), and data suggestthat the Permanet polyester nets were more wash resistantthan conventional nets treated with deltamethrin (28). Thisinformation does not disprove the efficacy claims of Permanet,but this is an area of critical research.
Sustaining the Intervention
Interested and motivated communities are important to sus-tain an intervention. For this to be effective, people shouldknow what is expected of them and what they will receive inreturn. There should be a clear statement of activities, respon-sibilities, and rates of remuneration for people who providetime to do the work (65). This can be done if the scopes ofwork are defined and codified in a “constitution” that is agreedupon collectively. This was done in Bagamoyo, and the finaldocument approved by the various communities contained de-tails of membership, specifying the membership composition(i.e., the number of women, teachers, and medical personnel)and means of election. Each job category, the activities in-volved, the number of formal meetings to be held, their fre-quency, and the specific activities which were to be reviewedwere described (65). To maintain a consistent level of remu-neration, the interest accruing from the revolving fund was tobe distributed among the personnel according to the numberof hours worked and individual achievements. This work pro-gram was to be reviewed by a medical official, e.g., the malariaofficer, a member of the local Ministry of Health staff. Moneycould be removed from the fund established in the Bagamoyodistrict only with a cheque bearing three signatures, two fromthe committee and one from the malaria officer, thus ensuringthat funds were, for the most part, used appropriately.
The alternative method proposed for sustaining interven-tions, that of social marketing, while popular with donor agen-cies, has also raised queries (9, 105). Despite considerablepublic relations work and initial advertising, there is no evi-dence as yet that it will be effective in controlling malaria in anynational program or that the system will be sustained withoutcontinual financial input from the donors.
STRATEGIES BASED ON BIOLOGICALCHARACTERISTICS OF MALARIA TRANSMISSION
Barrier Spraying
Under certain conditions, particularly when there are strongseasonal fluctuations in vector mosquito populations and thespecies survive the winter by seeking refuge in warmer, humid
VOL. 15, 2002 INTEGRATED APPROACH TO MALARIA CONTROL 287
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

areas, barriers to mosquito invasion can be created by limitedbut intense vector control operations. Properly designed, thesewill help prevent the periodic invasions of areas of hypoen-demic infection or areas vulnerable to severe epidemics. Suchareas are usually in proximity to regions where transmission ismore stable or even permanent. Designing systematic controloperations in the areas prone to invasion can prevent themigration of mosquitoes into vulnerable areas, thus reducingthe threat of serious epidemics in highly populated areas. Ar-eas of hypoendemic infection are usually cooler (or drier) thanareas of mesoendemic infection and therefore may be denselypopulated or may be of considerable economic importance.Outbreaks in populated areas can have catastrophic effects onpublic health and the economy of the country where infectionis endemic. The use of barrier spraying programs to preventthe movement of vector mosquitoes from their dry season orwinter refuges can be effective in curtailing the spread of ma-laria into vulnerable areas. However, to be effective, barrierspraying requires detailed knowledge of the mosquito popula-tions, their winter refuges, and the seasonal conditions whichallow their spread into adjacent areas.
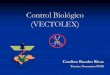
An example used in Zimbabwe was based on Leeson’s obser-
vations that A. gambiae sensu lato and A. funestus found winterrefuges in the northeast of that country (51) (Fig. 1). In the spring,as conditions warmed in the areas above 900 m, vector speciesbegan to invade the upland areas and could be collected in poolsalong river valleys, progressively moving into more temperateareas. From these refuges, malaria spread into the adjacent farm-ing and urban areas with devastating effects. A concerted systemof intradomicilary spraying across these lines of invasion just priorto the seasonal warming period served to protect invasions ofhigh-density population areas, which were of economic impor-tance to the country (5, 6). The importance of altitude and tem-perature in the seasonal ebb and flow of malaria under hypo- andmesoendemic conditions was stressed by Taylor and Mutambu(111). These data support the successful malaria control opera-tions which guided the Ministry of Health in Zimbabwe for over50 years and which have only recently been inadvertently disman-tled. This dismantling is a result of the drive to decentralizationrequired by international donors and has contributed to recentincreases in transmission (1.8 million cases of clinical malariarecorded in 1998) (8).
The concept of barrier spraying can be applied in numerousepidemiological situations, provided that there is sufficient ex-
FIG. 1. Map of Zimbabwe showing regions of malaria endemicity. The regions of differing malaria endemicity are shown in color. The red area,mainly below the 600-m contour except in the elevated mountain ranges, is holoendemic; the orange areas, also around the same elevation, aremore seasonal and dependent on rainfall; in the green areas, transmission is unstable and seasonal; transmission in the yellow areas, above the1,200-m contour, is hypoendemic or nonexistent. The districts between 900 and 1200 m (green) represent the area routinely sprayed in the pastantimalaria program. In these areas, both vector control and chemotherapy were undertaken. In other areas, the Ministry of Health relied onchemotherapy alone that was provided through the rural clinic services to prevent outbreaks of malaria. The green zone acted as a barrier toprevent the encroachment of malaria onto the high plateau, which was the most heavily populated part of the country.
288 SHIFF CLIN. MICROBIOL. REV.
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

pertise to plan and execute the operations. Such methodscould be implemented wherever there is a concern about sea-sonal encroachment into areas which are considered to be ahigh priority by local health authorities and politicians.
Structured Malaria Control
Situations occur where health authorities must attempt toprotect defined communities from epidemics or reduce theoverall intensity of malaria transmission. Under such circum-stances, the area and community affected would be identifiedthrough specific local health priorities and may expand overwide stretches of country; however, the extent of the workwould be limited by the availability of a sustained flow offinancial resources. Examples would be large agricultural orindustrial complexes, mines, and even cities or large popula-tion centers (115), as well as major areas which fall into themalaria control strategy of the country where the infection isendemic. In such instances it is feasible to design and planinterventions based on sustained vector control operations.These would commence just before the start of the main trans-mission seasons and would have to be maintained in a highstate of coverage for the duration of the transmission period.
Such interventions require coordination and planning aswell as the cooperation of the local communities involved.Because the programs involve and protect the overall commu-nity and even other population groups living in adjacent areas,it is important that all sectors of the community are keptinformed and participate wherever possible. It is quite feasiblefor communities to select the type of vector control interven-tion which they feel is the most suitable, because in the longrun, sustained success will depend on local interest and effort.Here again, levels of subsidy and remuneration must be nego-tiated, because it is essential that high levels of compliance areachieved in the vector control activities.
This structured approach would incorporate both vectorcontrol and chemotherapy. It would be feasible for the com-munity to be protected with prophylaxis if the level of organi-zation can cope with the logistics. In instances where effectivevector control is in place, there should be little likelihood ofbreakthrough of resistant parasites. As mentioned above, thecombination drug Deltaprim (pyrimethamine-dapsone) hasbeen used in such circumstances in southeastern Zimbabwe forover 40 years with no discernible side effects and little evidenceof failure in a community of approximately 50,000 persons (A.Morar, personal communication).
Evaluation of Efficacy
There is no need to review past results of the use of indoorspraying to control transmission of malaria; its efficacy is wellknown and accepted (47). However, the effect of ITNs remainsa matter of debate, mainly because there has not been a majorsustained national program in operation outside China (59)and because in the areas of holoendemic infection where mosttrials have been carried out, these trials have been of shortduration, lasting at the most 5 years. However, the indicationsare good, and one can expect that sustained ITN programs willbe successful. Original trials in The Gambia (32) and Tanzania(64) showed a decline in the number of infective mosquitoes
and an improvement in indicators of both malaria infectionand morbidity in the control area. Similar reports have comefrom elsewhere in Africa (68, 82, 89, 99) and from othersources quoted in Net Gain (52). It has been noted that ITNsmay not reduce the overall population of mosquitoes; crepus-cular (twilight-loving) forms and many culicine species are notalways reduced in number (74). Even specimens of vectormosquitoes are still found in experimental traps, but since fewof these are actually infected, the effect achieved is to reducetransmission (68, 113). An ITN program which will reduce thelife expectancy of vector mosquitoes will thus achieve the effectpredicted by the vectorial capacity model.
INSECTICIDES, INSECTICIDE RESISTANCE,AND MALARIA CONTROL
A list of some commonly used insecticides, together withcost-effective ratios, is given in Table 5. Although not exhaus-tive, it does cover the various classes of insecticides in use andenables comparisons to be made. Unfortunately, mention ofDDT is contentious these days, and therefore some commentsare appropriate. The advent of DDT and other chlorinatedhydrocarbon insecticides provided the mainstay of malariacontrol after World War II. In fact, DDT was initially devel-oped as a public health insecticide prior to its widespread usein agriculture and its identification as a major environmentalpollutant (25). In spite of widespread use and exposure ofhumans across the globe, this insecticide has been relativelysafe for use in public health programs as long as it is not spreadinto the environment. When used for indoor spraying, envi-ronmental contamination is greatly restricted, thus avoidingentry of the pesticide into the global food chain (10).
Resistance is also important. Widespread use of any insec-ticide will probably lead to the selection of resistant forms ofthe target organism. This has happened in several countriesand with several vector species. However, in spite of its pro-longed use over nearly 50 years, DDT is still effective in manyparts of the world. Being a cost-effective insecticide for indoorspraying, DDT still plays an important role in some malariacontrol programs. More recently introduced (although devel-oped for agriculture) pyrethroid insecticides have been ex-tremely valuable in public health use. In spite of the wide-spread agricultural usage, Curtis (28) has reported little or noevidence of pyrethroid resistance among the important vectorsin eastern Africa. In South Africa however, workers have dem-onstrated significant resistance of A. funestus to pyrethroidsand have recommended reintroduction of DDT spraying inKwaZulu/Natal (46). In a recent symposium held under theauspices of the American Association for the Advancement ofScience, the case was made not to ban DDT as a noxiouspollutant because of its importance at a public health pesticide(94). Considerable debate has taken place about the role ofDDT in public health. The reader is referred to a detailedsummary of a recent discussion by Taverne (109). Properlyused, the insecticide is applied in small quantities to indoorwalls. As such, it is unlikely to contribute to the outdoor pol-lution problem, and it can help save many lives in the lessadvantaged, malaria-endemic regions of the world. However,indoor application of insecticides may impact the vector pop-ulation in unexpected ways. In a recent review of malaria,
VOL. 15, 2002 INTEGRATED APPROACH TO MALARIA CONTROL 289
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

Phillips (89) quotes workers from Brazil who mention changesin the behavior of A. darlingi, which, although previously en-dophilic (indoor resting), now moves outdoor soon after feed-ing and thus is less exposed to insecticide than earlier in thecontrol operations. Similarly, in Africa, indoor spraying haseliminated the endophilic A. gambiae in some areas, only tohave it replaced by the more exophilic A. arabiensis (46). How-ever, transmission by the latter species can still be controlled byindoor spraying of insecticide (47).
DIAGNOSIS OF INFECTION
As with all infections, rapid diagnosis must be integral to anappropriate treatment program. However, diagnosis of malar-ial infection is, for all practical purposes, the purview of villagehealth workers, trained or untrained nurses, and some medicalofficers. Ideally, it should be done in a timely manner bytrained medical laboratory technologists, but even then ma-laria parasites are difficult to see. This is often exacerbatedwhen staining conditions are not optimal, a situation whichoften happens in rural settings. Even under hospital conditionswhere staff are usually under severe pressure, it is difficult toobtain results in a timely fashion; hence, most diagnoses inregions of endemic infection are based on clinical symptoms.When the patient is nonimmune, clinical indications are usu-ally suggestive of malaria, but in areas of endemic infectionthese are extremely misleading and fraught with inaccuracies.Studies in northeastern Zimbabwe of 104,000 cases over a12-month period showed that fewer than 30% of diagnosesmade by trained nursing staff operating at rural clinics wereslide positive (P. Taylor and A. Taputaira, Zimbabwe Sci. As-soc. First Natl. Symp. Sci. Technol., 1988). A similar result wasnoted in Madagascar, where only 12% of 6,884 presumptivediagnoses carried out in hospitals between 1997 and 1998 werefound to be slide positive (2). This discrepancy is not alwaysseen. In Ghana, malaria diagnosis at a health center was shownto be 62% slide positive (35). However, this was still threetimes more accurate than in home diagnoses (35). Unskilledhome diagnosis is likely to be the most inaccurate means ofdiagnosing malaria and will result in high proportions of un-necessary and inappropriate treatments.
In response to the obvious need for rapid, easily interpreteddiagnostics, a series of rapid malaria tests have been developedbased on detecting parasite-specific circulating antigens suchas HRP-2 (86). The dipstick tests use specific monoclonalantibodies to detect these antigens and reveal positive reac-tions with a colored line as in the ParaSIGHT-F test (91, 100).Over time, new products have been developed which use sim-ilar monoclonal antibodies. The ICT-Pf/Pv test, which detectsHRP-2 of P. falciparum and also a unique antigen expressed byP. vivax (49, 92), is thus able to discriminate between these twoparasites. Both these antigen capture tests perform well withhigh sensitivity and specificity and have been extremely widelytested. Since they detect circulating antigen, these assays re-main positive for about 10 days following treatment (100).These tests may also cross-react with rheumatoid factor (43),but that does not reduce their exceptional value for rapid andeffective diagnosis of both important malaria parasites (71). Anadditional dipstick test which detects the enzyme lactate dehy-drogenase and so also recognizes both parasite species has
been tested in Central America (84) and India (104). This testhas the advantage of turning from positive to negative in about5 days after effective elimination of the parasites. Selection ofthe appropriate test is probably most dependent on cost, anissue which precludes the more widespread use of these im-portant diagnostic procedures at this time.
Because of the importance of these tests in the overallGlobal Strategy of Malaria Control, there should be somedrive to subsidise or reduce costs for the tests in countrieswhere infection is endemic in order to make them economicaland of greater value in malaria treatment programs. Perhapsthis would be a role for Roll Back Malaria or WHO.
TRAVEL MEDICINE AND PROBLEMS DUE TO GLOBALCLIMATE CHANGE
The problem of imported malaria is gaining notoriety in devel-oped countries. MMWR Reports from CDC (www.cdc.gov) haveshown gradually increasing numbers of cases detected in theUnited States, peaking at over 2,000 in 1980, but since then thecase detection rate has remained around 1,600 annually. In theUnited States this presents a hazard of initiating so-called crypticcases, which are probably mosquito borne. Several good vectorsof malaria exist in the country, A. hermsi in California and A.quadrimaculatus in the south and much of the east; these speciesare capable of picking up gametocytes and initiating foci of trans-mission (45; MMWR Reports [www.cdc.gov]). Imported malaria isof increasing concern in Europe (83). In Aberdeen, over a 5-yearperiod 110 cases of malaria were diagnosed; 60% of patients hadP. falciparum infections, and the remainder were mainly P. vivaxinfections. The majority of infections were acquired due to lapseor absence of prophylaxis (63). A similar casual attitude has beenreported from the United States, where records in San Franciscoover a 10-year period ending in 1997 show that only 23% oftravelers to areas of endemic infection had been compliant withantimalaria prophylaxis and none of these had developed infec-tion (34).
Diagnosis of these imported cases is critical because of thelife-threatening condition which may develop from a P. falci-parum infection. A recent study in Italy comparing genus-specific PCR and Southern blot species-specific hybridizationwith rapid diagnostics and microscopy showed the advantageof both good-quality microscopy and the rapid diagnostic testsin securing a rapid and accurate diagnosis. PCR and micros-copy had 100% agreement, while the rapid ParaSIGHT-F testshowed a specificity and sensitivity of 94% (88).
With the impending changes in global climates, the problemof imported malaria will become more widespread because ofthe spread of malaria into new areas of endemicity and thecavalier attitude regarding prophylaxis among overseas travel-ers (63). In areas of endemicity, encroaching transmission hasbeen reported in areas previously free of transmission. This islikely to be a response to warming conditions or else to periodsof prolonged summer rains which occur as a result of extremeclimatic episodes, which are becoming more frequent. Exam-ples of this can be seen with the advent of malaria epidemics inthe highlands of Madagascar (2); Kenya, where transmissionmay encroach on Nairobi and the Kenya highlands; andUganda, where similar encroachment is happening (55) as wellas in Lusaka, where malaria transmission occurs occasionally
290 SHIFF CLIN. MICROBIOL. REV.
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

although the city was previously free of transmission (14).When conditions favor the extension of transmission into thesepreviously malaria-free zones, increasing numbers of travelersare likely to return home with prepatent infections.
MALARIA VACCINES
Attempts to develop a malaria vaccine began early in the 20thcentury, and in spite of advances in biomedical technology andperiodic bouts of unsubstantiated optimism in the field, no effec-tive vaccine is available for use (95). It is not the purpose of thisreview to cover the current status of malaria vaccine develop-ment. However, mention of the various strategies pursued byresearch workers is in order so that we can develop a perspectiveof how vaccines may be utilized in controlling malaria.
The development of malaria vaccines has become the focus ofconsiderable research. On the basis of research with rodents,scientists in the early 1970s demonstrated that irradiated sporo-zoites of P. falciparum and P. vivax inoculated into naive volun-teers would provide protection against challenge from fully infec-tive mosquitoes (7, 23). The main opportunity for this work toflourish occurred following the decisions to reduce emphasis oneradication programmes in the early 1970s (120). This was aperiod when discoveries in molecular techniques were incorpo-rated into the studies of the malaria parasite. The fact that P.falciparum was amenable to in vitro cultivation prompted thisspecies to become the main focus of study, an emphasis which haslasted until the present. The situation with P. vivax is more diffi-cult because this species cannot yet be cultured in vitro. With P.falciparum the research effort has followed three main routes. Thefirst has been to try and destroy circulating sporozoites before orduring early stages of infection of hepatocytes to produce a sterileimmunity. The second has been directed against the blood stageantigens of the parasite trophozoites in an attempt to reduce thevirulence of infection and, by preventing further development ofschizonts, to interrupt reproduction. Finally, there is an approachto prevent the development of sexual forms, and if they do de-velop, to attack the maturing forms when ingested by the vectormosquito. This last strategy is called transmission-blocking immu-nity. Cocktails of these vaccines are being contemplated (95).
Research has brought several candidate vaccines throughphase 1 and in some cases phase 2 of vaccine development.The only vaccine to reach phase 3 was a multicomponentsynthetic peptide, SPf66, which was claimed to have protectiveeffects in trials in Columbia (87). The vaccine was tested in aseries of trials in holoendemic situations in Africa (4, 31) andshowed marginal, if any, protection. Finally, no protection wasobserved in a trial when it was incorporated in an ExtendedProgram of Immunization program and administered to chil-dren as part of the initial immunization program (1).
FINALE: ROLL BACK MALARIA
Malaria control is an increasingly important focus for theinternational body concerned with public health and diseasecontrol. The need for reactivation and revitalization of pastcontrol programs, finance to support interventions, and theneed to rationalise the concepts of malaria control has beenseen by senior administrators such as Gro Brundtland, Direc-tor General of WHO. In response, the Roll Back Malaria
initiative has arisen with backing from the United NationsDevelopment Program, World Bank, United Nations Chi-dren’s Fund, and WHO (80). Philanthropic organizations suchas the Gates Foundation, the National Institutes of Health,and others have added resources to this body, so that theenterprise has considerable opportunity to make an impact.The initiative is examining various strategies to do this. How-ever, to any observing malariologist, the main weakness glo-bally is the dearth of trained, properly remunerated technicalpersonnel prepared to work in the field (13).
Without local expertise to develop local strategies for the im-plementation of control programs, ministries of health will floun-der in the process of implementation and their efforts will dissi-pate. The underlying necessity required to develop and sustainnational programmes is to rebuild local infrastructure and exper-tise. This will require selection and training of local personnelfrom countries with endemic infection who have a commitment tolearning about malaria and who will remain and develop theircareers locally. There is a need for the local governments and alsouniversities to offer such personnel the basic elements for careerdevelopment (101, 103). This is the challenge for Roll Back Ma-laria, to help reestablish scientific civil services in areas of endemicinfection since such organizations are the root of internal stabilityand drive. There is no easy solution, but one is essential otherwisewe will have no real program for malaria control, neither this yearnor in 10 years.
ACKNOWLEDGMENTS
Many of the thoughts expressed here are based on nearly 30 years ofexperience in malaria control in the country now called Zimbabwe. Forthe camaraderie and collaboration over these years, I must express thanksto members of all the malaria teams with whom I worked.. Particularly, Ithank Vic Clarke, Director of the Blair Research Laboratory, who pro-vided the inspiration and leadership which made the programs the successthey were. Thanks are due also to Don Roberts of the Uniformed Uni-versity of the Health Sciences for his suggestions regarding control pro-grams in Central and South America and to Doug Norris of Johns Hop-kins for his revisions and suggestions. Finally, my deep thanks go to DavidClyde, a lifelong friend and colleague who has dedicated so much of hislife to malaria control in Africa.
Financial support from the Johns Hopkins Malaria Research Insti-tute is acknowledged.
REFERENCES
1. Acosta, C., C. Galindo, D. Schellenberg, J. Aponte, E. Kahigwa, H. Urassa,J. Armstrong-Schellenberg, H. Massanja, R. Hayes, A. Kitua, F. Lwilla, M.Tannr, and P. Alonso. 1999. Evaluation of the SPf66 vaccine for malariacontrol when delivered through the EPI scheme in Tanzania. Trop. Med.Int. Health 4:368–376.
2. Albonico, M., F. De Giorgi, J. Razanakolana, A. Raveloson, G. Sabatinelli,V. Pietra, and D. Modiano. 1999. Control of epidemic malaria on thehighlands of Madagascar. Parassitologia 41:373–376.
3. Alonso, P., S. Limdsay, J. Armstrong-Schellenberg, K. Keita, F. Gomez, A.Hill, G. Fegan, K. Cham, and B. M. Greenwood. 1993. A malaria controltrial using insecticide treated bednets and targeted chemoprophylaxis in arural area of the Gambia, West Africa. 6. Impact of the interventions onmortality and morbidity from malaria. Trans. R. Soc. Trop. Med. Hyg.87:37–44.
4. Alonso, P., T. Smith, and J. Armstrong-Schellenberg. 1994. Randomisedtrial of efficacy of SPf66 vaccine against Plasmodium falciparum malaria inchildren in southern Tanzania. Lancet 344:1175–1181.
5. Alves, W., and D. W. Blair. 1955. Malaria control in Southern Rhodesia. Jo.Trop. Med. Hyg. 58:273–280.
6. Alves, W. 1958. Malaria parasite rates in Southern Rhodesia: May–Septem-ber 1956. Bull. W. H. O. 19:69–74.
7. Anders, R., and A. Saul. 2000. Malaria vaccines. Parasitol. Today 16:444–447.
8. Anonymous. 2001. Zimbabwe National Health Profile 1998. Ministry ofHealth and Child Welfare, Harare, Zimbabwe.
VOL. 15, 2002 INTEGRATED APPROACH TO MALARIA CONTROL 291
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

9. Armstrong Schellenberg, J., S. Abdulla, H. Minja, R. Nathan, O. Mukasa,T. Marchant, S. Maponda, and C. Lengeler. 1999. KINET: a social mar-keting programme of treated nets and net treatment for malaria control inTanzania, with evaluation of childhealth and long term survival. Trans. R.Soc. Trop. Med. Hyg. 93:225–231.
10. Attaran, A., D. Roberts, C. Curtis, and W. Kilama. 2000. Balancing risks onthe backs of the poor. Nat. Med. 6:729–731.
11. Babiker, H., J. Lines, and D. Walliker. 1997. Population structure of Plas-modium falciparum in villages with different malaria endemicity in eastAfrica. Am. J. Trop. Med. Hyg. 56:141–147.
12. Baird, J. K. 2000. Resurgent malaria at the millennium. Drugs 59:719–741.13. Balter, M. 2000. Can WHO roll back malaria. Science 290:430–431.14. Barat, L., B. Himonga, M. Ettling, T. Ruebush, W. Kapela, and P. B.
Bloland. 1998. A systematic approach to the development of a rationaltreatment policy in Zambia. Trop. Med. Int. Health 3:535–542.
15. Barber, M. A. 1929. The history of malaria in the United States. USA PublicHealth Rep. 44:2575–2587.
16. Bijl, H., J. Kager, D. Koetsier, and T. S. van der Werf. 2000. Chloroquineand sulfadoxine-pyrimethamine-resistant falciparum malaria in vivo—a pi-lot study in rural Zambia. Trop. Med. Int. Health 5:692–695.
17. Binka, F., A. Kubaji, M. Adjuik, L. Williams, C. Lengeler, G. Maude, G.Armah, B. Kajihara, J. Aiamah, and P. G. Smith. 1996. Impact of per-methrin treated bednets on child mortality in Kasena-Nankana district,Ghana: a randomized controlled trial. Trop. Med. Int. Health 1:147–154.
18. Birkholtz, L., L. Visser, A. Brink, and A. Louw. 1998. Drug-resistant andmixed species malaria infections in Mpumalunga, South Africa. S. Af. J. Sci.94:39–43.
19. Briercliffe, R. 1935. The Ceylon Malaria Epidemic 1934–35. GovernmentPress, Colombo, Sri Lanka.
20. Bruce-Chwatt, L. J. 1988. The history of malaria from prehistory to erad-ication, p. 1–60. In W. Wernsdorfer and I. McGregor (ed.), Malaria.Churchill Livingstone, Edinburgh, United Kingdom.
21. Butler, W., and D. Roberts. 2001. Malaria in the Americas: a model ofreemergence. Mil. Med. 165:897–901.
22. Reference deleted.23. Clyde, D. F., V. McCarthy, R. M. Miller, and W. E. Woodward. 1975.
Immunization of man against falciparum and vivax malaria by use of at-tenuated sporozoites. Am. J. Trop. Med. Hyg. 24:397–401.
24. Coleman, P., C. Goodman, and A. Mills. 1999. Rebound mortality and thecost-effectiveness of malaria control: potential impact of increased mortal-ity in late childhood following the introduction of insecticide treated nets.Trop. Med. Int. Health 4:175–186.
25. Curtis, C. F., and J. Lines. 2000. Should DDT be banned by Internationaltreaty? Parasitol. Today 16:119–121.
26. Curtis, C. F. 1996. Impregnated bednets, malaria control and child mor-tality in Africa. Trop. Med. Int. Health 1:137–138.
27. Curtis, C. F. 1999. Malaria control: bednets or spraying? Trans. R. Soc.Trop. Med. Hyg. 93:453–454.
28. Reference deleted.29. Curtis, C. F., J. Miller, M. Hodjati, J. Kolazhinski, and I. Kasumba. 1998.
Can anything be done to maintain the effectveness of pyrethroid-impreg-nated bednets against malaria vectors? Philos. Trans. R. Soc. Lond. Ser. B353:1769–1775.
30. Curtis, C. F. and A. E. Mnzava. 2000. Comparison of house spraying andinsecticide-treated nets for malaria control. Bull. W. H. O. 78:1389–1400.
31. D’Alessandro, U., A. Leacj, C. Drakely, S. Bennett, B. Olaleye, and D.Fagan. 1995. Efficacy trial of malaria vaccine SPf66 in Gambian infants.Lancet 146:462–467.
32. D’Alessandro, U., B. Olaleye, W. McGuire, P. Langerock, S. Bennett, M.Atkins, M. Thompson, M. K. Cham, and B. M. Greenwood. 1995. Mortalityand morbidity from malaria in Gambian children after introduction of animpregnated programme. Lancet 345:497–483.
33. Desowitz, R. S. 1999. Milestones in the history of malaria, p. 3–56. In M.Wahlgren and P. Perlmann (ed.), Malaria. Harwood Academic, Amster-dam, The Netherlands.
34. Dorsey G, M. Gandhi, J. Oyugi, and P. Rosenthal. 2000. Difficulties in theprevention, diagnosis, and treatment of imported malaria. Arch. Intern.Med. 160:2505–2510.
35. Dunyo, S., E. K. Afari, K. Koram, C. K. Ahorlu, I. Abubaker, and F. K.Nkrumah. 2000. Health centre versus home presumptive diagnosis of ma-laria in southern Ghana: implications for home-based care policy. Trans. R.Soc. Trop. Med. Hyg. 94:285–288.
36. Feighner, B., S. Pak, W. Novakoski, L. Kelsey, and D. Strickman. 1998.Re-emergence of Plasmodium vivax malaria in the Republic of Korea.Emerg. Infect. Dis. 4:295–297.
37. Fidock, D., X.-Z. Su, K. Deitsch, and T. E. Wellems. 1999. Genetic ap-proaches to the determinants of drug response, pathogenesis and infectivityin Plasmodium falciparum malaria, p. 217–248. In M. Wahlgren and P.Perlmann (ed.), Malaria. Harwood Academic Publishers, Amsterdam, TheNetherlands.
38. Garrett-Jones, C., and B. Grab. 1964. The assessment of insecticidal impact
on the malaria mosquito’s vectorial capacity from data on the proportion ofparous females. Bull. W. H. O. 31:165–185.
39. Garrett-Jones, C. 1964. The human blood index of malaria vectors inrelation to epidemiological assessment. Bull. W. H. O. 31:71–86.
40. Gillies, M. T. 1972. Some aspects of mosquito behaviour in relation to thetransmission of parasites. Zoo. J. Linnean Soc. 51:61–81.
41. Gillies, M. T. 2001. Vector behaviour and bionomics, p. 453–485. In W.Wernsdorfer and I. McGregor (ed.), Malaria. Churchill Livingstone, Edin-burgh, United Kingdom.
42. Gramaccia, G., and P. Beales. 1988. The recent history of malaria eradi-cation and control, p. 1335–1378. In W. Wernsdorfer and I. McGregor(ed.), Malaria. Churchill Livingstone, Edinburgh, United Kingdom.
43. Grobusch, M., T. Jelinek, and T. Hanscheid. 1999. False positivity of rapidantigen detection tests for diagnosis of Plasmodium falciparum malaria: theissue appears to be more complicated than presented. J. Clin. Microbiol.37:3781–3782.
44. Guarda, J., R. Asayag, and R. Witzig. 1999. Malaria re-emergence in thePeruvian Amazon region. Emerg. Infect. Dis. 5:209–215.
45. Gusmao, R. D. 1999. Overview of Malaria Control in the Americas. Paras-sitologia 41:355–360.
46. Hargreaves, K., L. Koekemoer, B. Brooke, R. H. Hunt, J. Mthembu, and M.Coetzee. 2000. Anopheles funestus resistant to pyrethroid insecticides inSouth Africa. Med. Vet. Entomol. 14:181–189.
47. Haworth, J. 1988. The global distribution of malaria and the present controlefforts, p. 1379–1420. In M. Wernsdorfer and I. McGregor (ed.), Malaria.Churchill Livingstone, Edinburgh, United Kingdom.
48. Institute of Medicine. 1991. Malaria: obstacles and opportunities, p. 37–55.National Academy Press, Washington, D.C.
49. Jelinek, T., M. Grobusch, and H. D. Northdurft. 2000. Use of dipstick testsfor the rapid diagnosis of malaria in nonimmune travelers. J. Travel Med.7:175–179.
50. Kouznetsov, R. L. 1977. Malaria control by application of indoor sprayingof residual insecticides in Tropical Africa and its impact on populationhealth. Trop. Doct. 7:81–91.
51. Leeson, H. S. 1931. Anopheline mosquitoes in Southern Rhodesia, 1926–1928. Mem. Lond. School Hyg. Trop. Med. 4:1–55.
52. Lengeler, C., J. Cattani, and D. de Savigny. 1996. Net Gain, p. 17–53. WorldHealth Organization, Geneva, Switzerland.
53. Le Sueur, D., B. Sharp, and C. C. Appleton. 1993. A historical perspectiveof the malaria problem in Natal with emphasis on the period 1928–1932. S.Afri. J. Sci. 89:232–239.
54. Li, Z., M. Zhang, B. Zhoug, G. Lin, and H. Huang. 1989. Trial of delta-methrin impregnated bednets for the control of malaria transmitted by An.sinensis and An. anthropophagus. Am. J. Trop. Med. Hyg. 40:356–359.
55. Lindblade, K., E. Walker, A. Onapa, J. Katungu, and M. L. Wilson. 1999.Highland malaria in Uganda: prospective analysis of an epidemic associatedwith E1 Niño. Trans. R. Soc. Trop. Med. Hyg. 93:480–487.
56. Lines, J., J. Myamba, and C. F. Curtis. 1987. Experimental hut trials ofpermethrin impregnated mosquito nets and eave curtains against malariavectors in Tanzania. Med. Vet. Entomol. 1:37–51.
57. Litsios, S. 1997. The tomorrow of malaria, p. 92–105. Pacific Press, Well-ington, New Zealand.
58. Logan, J. A. 1953. The Sardinian Project: an experiment in the eradicationof an indigenous malaria vector. Johns Hopkins Press, Baltimore, Md.
59. Luo, D.-P., D. La, R. Yao, X. Huo, L. Wen, S. Zhang, H. Huo, and L. Shang.1994. Alphamethrin-impregnated bed nets for malaria and mosquito con-trol in China. Trans. R. Soc. Trop. Med. Hyg. 88:625–628.
60. Macdonald, G. 1951. Analysis of malaria epidemics. Trop. Dis. Bull. 50:871–879.
61. Macdonald, G. 1957. The epidemiology and control of malaria. OxfordUniversity Press, Oxford, United Kingdom.
62. MacDonald, M., and J. D. McGuire. 1999. Commercial sector partnershipsfor malaria control. Trop. Med. Int. Health 4:319–321.
63. Mackenzie, A., R. Liang, J. G. Douglas, N. Scott, and C. C. Smith. 2000.Impact of the oil industry on malaria diagnosis and management in north-east Scotland. Scott. Med. J. 45:72–74.
64. Magesa, S., T. Wilkes, A. Mnzava, K. Njunwa, J. Myamba, M. Kivuyo, N.Hill, J. Lines, and C. Curtis. 1991. Trial of pyrethroid impregnated bednetsin an area of Tanzania holoendemic for malaria. 2 effects on the malariavector population. Acta Trop. 49:97–108.
65. Makemba A., P. Winch, S. Kamazima, V. Makame, F. Sengo, P. Lubega, J.Minjas, and C. J. Shiff. 1995. Community-based sale, distribution andinsecticide impregnation of mosquito nets in Bagamoyo District, Tanzania.Health Policy Planning 10:50–59.
66. Marsh, K. 1992. Malaria—a neglected disease. Parasitology 104:S53–S59.67. Martens, W., R. Kovats, S. Nijhof, P. deVries, M. Livermore, A. Mc-
Michael, D. Bradley, and J. S. H. Cox. 1999. Climate change and futurepopulations at risk of malaria. Global Environ. Change 9:S89–S107.
68. Maxwell, C., J. Myamba, K. Njumwa, B. Greenwood, and C. F. Curtis. 1999.Comparison of bednets impregnated with different pyrethroids for theirimpact on mosquitoes and on re-infection with malaria after clearance of
292 SHIFF CLIN. MICROBIOL. REV.
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from

pre-existing infections with chlorproguanil-dapsone. Trans. R. Soc. Trop.Med. Hyg. 93:4–11.
69. Mharakurwa, S. 1998. Status of chloroquine efficacy on falciparum malariain Mola area of Kariba district, Zimbabwe. Ann. Trop. Med. Parasitol.91:655–661.
70. Reference deleted.71. Mharakurwa, S., B. Manyame, and C. J. Shiff. 1997. Trial of the Para-
Sight-F test for malaria diagnosis in the primary health care system, Zim-babwe. Trop. Med. Int. Health 2:544–550.
72. Miller, J., A. Buriyo, A. Karigila, and J. Lines. 1999. A new strategy fortreating nets. Part I: formulation and dosage. Trop. Med. Int. Health4:160–166.
73. Miller, J., C. Jones, S. Ndunguru, C. Curtis, and J. Lines. 1999. A newstrategy for treating nets. 2. Users perception of efficacy and washing prac-tices and their implications for insecticide dosage. Trop. Med. Int. Health4:167–174.
74. Misra, S., R. Webber, J. Lines, S. Jaffar, and D. J. Bradley. 1999. Malariacontrol:bednets or spraying? Spray versus treated nets using delta-methrin—a community randomised trial in India. Trans. R. Soc. Trop.Med. Hyg. 93:456–457.
75. Mnzava, A., S. Dhlamini, B. Sharp, K. Mthembu, I. Gumede, I. Klein-schmidt, and E. Gouws. 1999. Malaria control: bednets or spraying? Trial inKwazulu-Natal, South Africa. Trans. R. Soc. Trop. Med. Hyg. 93:455–456.
76. Molyneux, D., K. Floyd, G. Barnish, and E. M. Fevre. 1999. Transmissioncontrol and drug resistance in malaria: a crucial interaction. Parasitol.Today 15:238–240.
77. Reference deleted.78. Mouchet, J., and P. Carnavale. 1998. Entomological biodiversity of malaria
in the World. Res. Rev. Parasitol. 58:189–195.79. Mutambu, S., and C. Shiff. 1997. Implementing and sustaining community-
based mosquito net interventions in Africa. Parasitol. Today 13:204–205.80. Nabarro, D. 1999. Roll Back Malaria. Parassitologia 41:501–504.81. Nardin, E. 1999. Synthetic peptides as malaria vaccines, p. 495–540. In M.
Wahlgren and P. Perlmann (ed.), Malaria. Harwood Academic Publishers,Amsterdam, The Netherlands.
82. Nevill, C., E. Some, V. Mung’’ala, W. Mutemi, L. New, K. Marsh, C.Lengeler, and R. W. Snow. 1996. Insecticide treated bednets reduce mor-tality and severe morbidity from malaria from children on the Kenyan coast.Trop. Med. Int. Health 1:139–146.
83. Nuesch, R., M. Scheller, and N. Gyr. 2000. Hospital admissions for malariain Basel, Switzerland: an epidemiological review of 150 cases. J. TravelMed. 7:95–97.
84. Palmer, C., L. L. J. Validum, A. Camap, M. Makler, R. Cuadrado, and A.Ager. 1999. Field evaluation of the OptiMAL rapid malaria diagnostic testduring antimalarial therapy in Guyana. Trans. R. Soc. Trop. Med. Hyg.93:517–518.
85. Pampana, E. J. 1937. Malaria in Italy and “bonifications.” Malayan Med. J.12:1–8.
86. Para, M., C. Evans, and D. W. Taylor. 1991. Identification of Plasmodiumfalciparum histidine-rich protein-2 in the plasma of humans with malaria.J. Clin. Microbiol. 29:1629–1634.
87. Patarroyo, M. E., and R. Armador. 1999. SPf66: The first and towards thesecond generation of malaria vaccines, p. 541–554. In M. Wahlgren and P.Perlmann (ed.), Malaria. Harwood Academic Publishers, Amsterdam, TheNetherlands
88. Perandin, F., N. Manca, G. Galati, G. Piccolo, A. Calderaro, L. Viani, L.Ricci, G. Dettori, and A. Turano. 2001. Usefulness of genus-specific PCRand Southern blot species-specific hybridization for the detection of im-ported malaria cases in Italy. New Microbiol. 24:69–76.
89. Phillips, R. S. 2001. Current status of malaria and potential for control.Clin. Microbiol. Rev. 14:208–226.
90. Premji, Z., P. Lubega, Y. Hamisi, F. Mchopa, J. Minjas, W. Checkley, andC. J. Shiff. 1995. Changes in malaria associated morbidity in children usinginsecticide treated mosquito nets in the Bagamoyo District of CoastalTanzania. Trop. Med. Parasitol. 40:147–153.
91. Premji, Z., J. Minjas, and C. J. Shiff. 1994. Laboratory diagnosis of malariaby village health workers using the rapid manual ParaSight-F test. Trans. R.Soc. Trop. Med. Hyg. 88:418.
92. Proux, S., F. Nosten, L. Hkirijareon, C. Ngamngonkiri, S. McConnell, andF. Nosten. 2001. Paracheck-Pf(R): a new, inexpensive and reliable rapid testfor P. falciparum malaria. Trop. Med. Int. Health 6:99–101.
93. Rafatjah, H. A. 1988. Malaria control: environmental management, p.1135–1172. In W. Wernsdorfer and I. McGregor (ed.), Malaria. ChurchillLivingstone, Edinburgh, United Kingdom.
94. Roberts, D., S. Manguin, and J. Mouchet. 2000. DDT house spraying andre-emerging malaria. Lancet 356:330–332.
95. Rogers, W., and S. Hoffman. 1999. Malaria vaccines, p. 430–494. In M.Wahlgren and P. Perlmann (ed.), Malaria. Harwood Academic Publishers,Amsterdam, The Netherlands.
96. Rozendaal, J. A. 1997. Vector control: methods for use by individuals andcommunities. World Health Organization, Geneva, Switzerland.
97. Sharma, V. P. 1987. Community-based malaria control in India. Parasitol.Today 3:222–226.
98. Shiff, C., W. Checkley, P. Winch, Z. Premji, J. Minjas, and P. Lubega. 1996.Changes in weight gain and anaemia attributable to malaria in Tanzanianchildren living under holoendemic conditions. Trans. R. Soc. Trop. Med.Hyg. 90:262–265.
99. Shiff, C., J. Minjas, T. Hall, R. Hunt, S. Lyimo, and J. R. Davis. 1995.Malaria infection potential of anopheline mosquitoes sampled by lighttrapping indoors in coastal Tanzania. Med. Vet. Entomol. 9:256–262.
100. Shiff, C., Z. Premji, and J. N. Minjas. 1993. The rapid manual ParaSight-Ftest. A new diagnostic tool for Plasmodium falciparum infection. Trans. R.Soc. Trop. Med. Hyg. 87:646–648.
101. Shiff, C. J. 2001. The Internet: a valuable tool for Roll Back Malaria: aresponse. Trends Parasitol. 17:161.C. J.
102. Shiff, C. J. 1998. Vector control, community participation and malariamorbidity in the Bagamoyo district of Rural Tanzania. Res. Rev. Parasitol.58:209–215.
103. Shiff, C. J. 2001. Can Roll Back Malaria achieve its goal? Parasitol. Today16:271–272.
104. Singh, N., A. Saxena, and N. Valecha. 2000. Field evaluation of the ICTmalaria P.f/P.v immunochromatographic test for the diagnosis of Plasmo-dium falciparum and P. vivax infection in forest villages of Chhindwara,central India. Trop. Med. Int. Health 5:765–770.
105. Stallworthy, G. 1997. Social marketing of impregnated mosquito nets inMashonaland Central, Zimbabwe, p. 1–20. PSI Washington, Washington,D.C.
106. Stamps, T. J. 1993. Remarks by the head of the Zimbabwe Delegation atthe Ministerial Conference on Malaria, Amsterdam, 1992. Med. Res. Coun-cil Zimbabwe Newsl. 1:5–6.
107. Sternberg, G. W. 1884. Malaria and malarial diseases, p. 121–122. WilliamWood & Co., New York, N.Y.
108. Subbarao, S., and V. P. Sharma. 1997. Anopheline species complexes andmalaria control. Indian J. Med. Res. 106:164–173.
109. Taverne, J. 1999. DDT—to ban or not to ban. Parasitol. Today 15:180–181.110. Taylor, P., J. Govere, and M. Crees. 1986. A field trial of microencapsulated
deltamethrin, a synthetic pyrethroid for malaria control. Trans. R. Soc.Trop. Med. Hygi. 80:537–545.
111. Taylor, P., and S. Mutambu. 1986. A review of the malaria situation inZimbabwe with special reference to the period 1972–1981. Trans. R. Soc.Trop. Med. Hyg. 80:12–19.
112. Reference deleted.113. Temu, E., J. Minjas, Z. Premji, R. Hunt, and C. J. Shiff. 1999. The use of
permethrin impregnated bed nets for malaria control in coastal Tanzania:preliminary entomological impact on vectors. Afri. Entomol. 7:1–10.
114. Temu, E., J. Minjas, C. Shiff, and A. Majala. 1999. Bedbug control bypermethrin-impreganted bednets in Tanzania. Med. Vet. Entomol. 13:457–459.
115. Trape, J., and A. Zoulani. 1987. Malaria and urbanisation in Central Africa,the example of Brazzaville. Trans. R. Soc. Trop. Med. Hyg. 81:10–18.
116. Wernsdorfer, W. M. 1991. The development and spread of drug resistancein Plasmodium falciparum malaria. Parasitol. Today 7:297–303.
117. White, G. B. 1974. Anopheles gambiae complex and disease transmission inAfrica. Trans. R. Soc. Trop. Med. Hyg. 68:278–301.
118. White, G. B. 1999. Malaria prevention by vector control: effectiveness ofinsecticidal methods. Parassitologia 41:385–387.
119. World Health Organization. 1957. Expert Committee on Malaria: sixthreport. World Health Organization, Geneva, Switzerland.
120. World Health Organization. 1974. WHO Expert Committee on Malaria:16th report. World Health Organization, Geneva, Switzerland.
121. World Health Organization. 1979. Expert Committee on Malaria: 17threport. World Health Organization, Geneva, Switzerland.
122. World Health Organization. 1983. Integrated vector control, p. 1–72. WorldHealth Organization, Geneva, Switzerland.
123. World Health Organization. 1993. A global strategy for malaria control, p.1–26. World Health Organization, Geneva, Switzerland.
124. World Health Organization. 1993. Implementation of the global malariacontrol strategy, p. 1–56. World Health Organization, Geneva, Switzerland.
125. World Health Organization. 2000. Expert Committee on Malaria. WHOTech. Rep. Ser. 892:1–40.
126. World Health Organization. 1997. World malaria situation in 1994. III.Wkly. Epidemiol. Rec. 72:277–284.
127. World Health Organization. 1970. Insecticide resistance and vector control.17th report of WHO Expert Committee on Insecticides. World HealthOrganization, Geneva, Switzerland.
128. World Health Organization. 1995. Vector control for malaria and othermosquito-borne diseases. WHO Tech. Rep. Ser. 857:8–65.
129. World Health Organization. 1966. Malaria eradication in 1965. WHOChron. 20:283–300.
VOL. 15, 2002 INTEGRATED APPROACH TO MALARIA CONTROL 293
on July 24, 2020 by guesthttp://cm
r.asm.org/
Dow
nloaded from