Embed Size (px)
Citation preview
1
DRAFT Integrated Care Pathway: Amputee Care
Stream of Care: Frail Elderly/Medically Complex Patient Population/Condition: Lower Extremity Amputation
Rehabilitative Care Setting
Desired Outcome Best Practice &
Source of Evidence (where it exists)
Metric Target
Performance
Current Performance
Activities to Support Achievement of Desired Outcome/Best Practice
A. PRE-OP
I. Communication/collaboration amongst health care providers for patients at risk for/requiring amputation:
a) Surgery b) Specialized
Amputee Teams c) Diabetic care d) Wound care e) Primary Care
When medically possible pre-operative consultation with the Specialized Amputee Team (SAT) occurs allowing for:
Clinical advice from the SAT about the prognosis for future prosthetic use which may assist in decision making in terms of level of amputation.
Recommendations for preoperative intervention: ie PT exercise prescription, CCAC home assessment.
Patient education: Each new amputee given a post op information brochure.
Evidence supporting pre-operative assessment by the SAT. 1,2,3,4,5,6
# Of pre-op consultations linked to pre-op intervention to maximize fitness, level of amputation, post op time to prosthetic fitting, achievement of functional prosthetic use.
When possible patients at high risk for amputation/ scheduled for amputation receive pre-op assessment with the appropriate SAT. If not medically stable enough to attend consultation between surgeon and with the SAT team (or individual team members) can be arranged.
Pre-operative consultation between surgeons and the SAT’s is rare.
i) Dysvascular patients: when it is identified that amputation may be/is required a referral to the most appropriate Specialized Amputee Team (SAT) according to the referral process may occur: Prosthetic and Orthotic Clinic, Grand River Hospital, Amputee Clinic at St. Joseph’s Health Centre occurs.
ii) Elective amputation (may be related to a traumatic orthopedic injury, congenital impairment) patients are referred to the amputee team prior to their surgery for initial assessment, consultation and education.
Appendix A: Referral Process Appendix B: Referral forms
Evidence supporting the benefits of patients having comprehensive information regarding the course of care they can anticipate. 1,3,4,15
# of new amps seen in SAT reporting having received information.
100 % of new amputee receive post-op brochure.
Patients assessed in the SAT post amputation report frustration at the lack of information they received post
Once identified as requiring amputation patients/families are provided with consistent, written information identifying possible next steps they can anticipate.
Appendix C: Amputee Care Brochure
2
operatively. Information given is not done so in a structured or consistent way.
II. Preventative approach to patient at high risk of lower extremity skin breakdown.
Communication and consultation between the P&O Clinic /SAT’s and the Waterloo Wellington Regional Diabetes Coordination Centre (WWRDCC):
- the SAT initiates referral to the WWRDCC if this has not already been done.
- The WWRDCC refers cases where diabetic orthotics/bracing is required to the Prosthetic and Orthotic Clinic .
Communication and consultation between the SAT’s and wound care services in the region: The SAT contacts the CCAC case manager to inform them of the SAT assessment.
Evidence supporting methods to off-load difficult wounds. 9 Evidence supporting a multidisciplinary approach for the complex medical lower extremity amputee. 1,2,4,5,6,7, 13,15,20, 34
# referrals from SAT to WWRDCC
# of off-loading devices prescribed vs dispensed
monitor reasons that devices not dispensed (often is related to patient not having ability/willingness to pay).
Patients who may benefit from assessment for off-loading devices, diabetic orthotics are offered referral to certified foot care providers (certified orthotist (including via P&O clinic, chiropody, podiatry, specialized nursing).
Patients with skin breakdown are referred for best practice wound care
Patients with lower extremity ulceration are referred to the Prosthetic and Orthotic Clinic at Freeport regarding off-loading devices primarily as inpatients at the Freeport site. Community referrals occur, but data regarding the source of this referral, frequency of referral is not currently monitored. Referral to either CCAC or the Amputee
Patients identified as high risk for skin breakdown leading to ulceration and potential amputation are provided with information regarding foot care providers (available via : http://www.waterloowellingtondiabetes.ca/foot-care.htm)
Patients may be referred to the Prosthetic and Orthotic clinic for assessment regarding offloading devices. Patients may be identified by: family doctors, family health care teams, primary care clinics, diabetic clinics, orthopedic clinics, ED, renal program.
Patients with skin breakdown seen in Prosthetic and Orthotic Clinic who are not already receiving wound care are referred to CCAC for wound assessment and care.
The physician in the Prosthetic and Orthotic Clinic refers for: special testing (ie. vascular studies, bone scan ) as indicated ; specialist consultation (vascular, orthopaedics) as indicated.
3
via CCAC. clinics pre-amputation is rare.
a)
# referrals to P&O clinic via WWRDCC
# interventions that occur as a result,
incidence of wound healing/ prevention with treatment
time to healing of established wounds
incidence of conversion to amputation.
Evidence of increased communication between the SAT’s, diabetic and wound care services in the region.
The SAT’s and diabetic services have not had substantially robust relationship and knowledge of each other’s services.
Patients identified at high risk for LE ulceration requiring diabetic orthotics or off-loading devices referred to the P&O clinic via the WWRDCC referral form.
Longstanding amputees identified in the diabetic clinics as having skin breakdown, comfort or gait issues with their prosthesis, or breakdown risk in their remaining limb are referred to the SAT with which they have been previously affiliated (Prosthetic and Orthotic Clinic at Grand River Hospital, the Amputee Clinic at St. Joseph’s Health Centre).
III. Maximization of the fitness level of patients at risk for amputation. Evidence indicates that pre-operative condition is a significant predictor of post-amputation potential for successful prosthetic use. a) Prevention of contracture
formation; in the transfemoral amputee avoiding hip flexion and abduction contractures. In the transtibial amputee avoiding hip flexion and
Evidence of predictors of successful prosthetic use: 2,3,6,8,10,11,12,13,14,33
Referral frequency and sources.
Lower extremity ROM and strength (pre and post op if able)
Timed arm ergometry
PT referral to the outpatient program closest to patient for assessment: identification of ROM/strength/endurance impairments. Referral to CCAC if patient is not able to access outpatients.
Referral to either CCAC or the Amputee clinics pre-amputation is rare.
Patients identified as high risk or requiring amputation receive PT assessment, intervention and recommendations regarding exercise activities to maximize fitness in preparation for potential amputation.
PT referral via CCAC, Geriatric Rehab services or the SAT (to assist with recommendations)
Referral to additional services as required (OT, SW, Registered Dietician).
In cases where patient does not demonstrate strong ability to complete program appropriately and
4
especially, knee flexion contractures.
b) Activity tolerance/endurance
independently short course intervention can occur. This may be group format, with therapy assistant support. Discharge planning includes provision of home program, referral to community programs and plan for monitoring.
Out patient teams , CCAC to have access to consistent assessment, education materials and exercise instructions for distribution to patients.
Evidence of predictors of successful prosthetic use : contractures at the hip (particularly for AKA) and knee (BKA) negatively impact successful prosthetic fitting and use. Severe contracture is a contraindication to fitting. 3,17
-Lower extremity ROM, strength
Hip extension ROM to 0-10 degrees on a modified Thomas test. Hip abduction ROM to neutral. Knee extension ROM 0-5 degrees.
This kind of preventative care has not typically occurred.
PT Intervention related to ROM/strength;
Patients are educated about the importance of their ROM and the impact on their potential prosthetic use.
Patient are educated to stretch daily to avoid the formation of contracture:
o Prone lying if tolerated o Active hip extension in prone. o Hip extension in standing o Knee extension stretching o Hip, knee and ankle
strengthening o Core strengthening. o UE strengthening o Home exercise prescription.
Appendix D: Above-Knee Amputation Post-op Information
Appendix E: Below-Knee Amputation Post-op Information
Evidence for the impact of pre-operative fitness and
Timed tests: i.e. walking tests, bicycle
PT intervention: endurance;
Patients are educated about the

5
activity level on the potential for successful prosthetic fitting. 2,3,8
ergometry, as appropriate.
importance of their endurance. o In clinic access to
endurance training on treadmill, upright or recumbent bicycle/elliptical, arm ergometry as appropriate.
Recommendations re home appropriate home activity.
The self-management plan should include components of the following:
An understanding of the link between fitness level and the potential for prosthetic candidacy and functional prosthetic outcome.
Demonstrated ability to properly perform basic ROM, strengthening and cardiovascular activity.
Demonstrate the ability to perform a daily lower extremity skin inspection.
Demonstrate and understanding of principles of hygiene and skin care.
Throughout the continuum of care.
Smoking cessation counseling (as taken from CHF pathway)
ECS Guidelines CCS Position Paper
% Of patients identified as smokers on admission who are offered NRT/counseling
Counselling during admission and follow up after discharge—“At all times, health care providers should strongly enforce stringent measures against active cigarette smoking” “Minimal interventions, lasting less than 3 minutes, should systematically be offered to every smoker with the understanding that more intensive counselling with pharmacotherapy results in the highest quit rates and should be used whenever possible”
6
NRT provided Referral to smokers help line (Appendix F: Smokers Help Line) Communicate NRT to primary care provider for continuation post discharge
C. ACUTE
I. Best practice surgical and post surgical management;
Where possible effort taken to perform transtibial or through joint amputation.
Optimal length of amputation (either transtibial or transfemoral)
Limit the potential for hip and/or knee flexion contracture
Best practice wound care: prolonged wound healing is often the primary cause of delayed prosthetic trial and increased the likelihood of secondary impairments
Evidence of the impact of level of amputation on successful prosthetic use. 1,2,3,5,6,16,17,
Incidence amputations performed in WW
Frequency of revision amputations.
Post-op infection rates.
Incidence of levels of amputation
That the desired practice/outcome in terms of the contribution level, length and minimization of contracture is considered at the operative stage.
Currently the amputee teams have limited to no involvement pre-op and are not generally consulted regarding the factors that may contribute to a better prosthetic outcome.
Determination of amputation procedure balancing potential to heal from surgery with optimal potential for achieving functional prosthetic use.
When possible, pre-op consultation with the SAT.
Ability for surgeons to consult remotely with Amputee team member: physiatrist, prosthetist, rehab assessor (physiotherapist).
Evidence for best practice post-op management of transtibial amputees. 15,21,22,23,24,25,26,27,32
That early post surgical management includes efforts to minimize the formation of knee flexion contractures in the transtibial amputee. That post surgical management is consistent.
The current post surgical management of amputees varies significantly depending on the surgeon. This report is consistent to all 3 acute care sites.
Transtibial amputation: when
resources, time and expertise allow, the use of rigid dressing post-operatively is
beneficial. Dressing applied with the knee in full extension.
7
Evidence for best practice post-op management of transtibial amputees. 15,21,22,23,24,25,26,27,32
For transtibial amputees rigid or semi rigid dressings with the knee held in full extension is identified in the literature as best practice. Transfemoral amputation: standard wound care with hip extension ROM as soon as tolerated by the patient.
As noted above immediate post op dressings varies significantly depending on the surgeon.
Wound management and shaping:
Other amputation levels (ie foot/forefoot, transfemoral) and transtibial amputation once rigid dressing removed: wound care as directed by physician/nurse/wound care expert.
Once rigid/semi-rigid dressings are removed a method of edema management, residual limb shaping and protection is introduced.
The selection of edema/shaping management must result in the safest, most consistent method and may change as patient moves from acute care to rehab and assessment in the SAT. (Transtibial amputees must use a stump board in their wheelchair and be educated about the importance of its use.
Transfemoral amputees must be educated to stretch hip flexors.
Appendix G: Transtibial Residual Limb Edema/Shaping Documents
II. Prompt referral to the appropriate ADP registered SAT.
Evidence for the early involvement of the SAT in the course of care for the lower extremity amputee. Core members with specialize skills and knowledge in amputee care: physician (surgeon, physiatrist or other
# or referrals of new amputees to the SAT’s
Wait time from referral to first visit with SAT.
Referral to the Prosthetic Clinics occurs in the acute care setting unless a pre-operative consultation has already occurred and follow-up is booked. Referral to the Amputee team that is going
How referral to the SAT occurs is variable. Patients who are discharged home rather than to inpatient rehabilitation are at risk of having
II.i Early involvement with the appropriate amputee clinic (SAT):
Unless it is clear that a patient is not a prosthetic candidate, the patient is refusing referral, or the patient was already see pre-operatively referral to the appropriate SAT team occurs as a standing referral.
The SAT sees patient as soon possible once they are medically able to attend the clinic. New amputee are identified
8
medical doctor with interest and skill in the area of amputee care), prosthetist, physiotherapist, nursing (with wound care/diabetic care specialization). Additionally access to occupational therapy and social work. 1,2,4,5,6,7, 13,15,20, 34
to meet patient needs based on their home location occurs.
delayed referral to the SAT. Referral to the SAT that is going to best meet the patient’s ongoing, life long needs generally occurs. However, with the first rehab bed policy patient’s are occasionally referred to the less appropriate SAT.
as a priority booking. (Appendix A: Referral Process)
III. Focus of physiotherapy /occupational therapy to include PROM and AROM to avoid contracture formation, to maximize activity tolerance, to support the patient’s knowledge of the process and requirements for prosthetic fitting.
Early mobilization: OT/PT to initiate transfer training to appropriate seating. This includes OT assessment for wheelchair and surface selection. All transtibial amputees are prescribed an
Evidence identifying the key rehab focus in the acute care setting to maximize safety for discharge as well as preparedness for prosthetic trial. 3,4, 7,15,17,
# Patients who receive education materials, measure the incidence of communication between care providers, d/c to community vs. inpatients.
Exercise prescription is consistent with pre-operative education and focuses on the identified ROM, strength and endurance as well as basic mobility and ADL functions for safe discharge home. Wheelchairs provided with appropriate
Current practice does include such exercise prescription. However there is not consistent written material provided to patients.
Physiotherapy and Occupational intervention including common educational materials across sites.
Early mobilization; When medically stable patients should begin mobilization. Post –op day 1-2.
Transfer training; slider board, low pivot, standing pivot.
Practice single leg stance.
ROM and stretching program as soon as tolerated.
UE ROM/strengthening exercise prescription.
Increasing activity tolerance:
Wheelchair mobility may be used as
9
appropriate amputee board.
PT and OT also support early discharge from the acute care site to the appropriate setting.
surface to prevent skin breakdown and appropriate alignment, including a amputee board for all transtibial amputees. Transfemoral amputees do not require an amputee board.
endurance activity if tolerated.
Hopping should be carefully assessed, likely performed with supervision or assistance.
Hopping independently should only occur in cases where balance and hopping skills demonstrated by the patient are highly proficient due to the risk of falling.
Seating and positioning (assessment and prescription occurs as soon as patient is medically stable enough to begin mobilizing): Transtibial residual limb is kept from dangling/hanging. When sitting in a wheelchair an amputee board is used to support the knee in extension, thereby reducing the risk of knee flexion contracture, assisting with edema management, pain control , alignment and skin integrity. Seating and positioning is complimented by patient education regarding the importance of elevation of the transtibial residual limb, as well as AROM exercises, in particular for hip and knee extension strength and ROM for all LE amputees.
Education materials are developed that are consistent.
Currently the education materials provided to a patient are not consistent or collaborative across the continuum.
Patients educated and provided with instructional guide. Materials provided support and empower the patient in their self management;
10
Better communication between acute care, rehab and the SAT is required.
The decision to refer to rehab or discharge home is based on the functional assessment and the needs for safe return to the home environment. If the patient is not likely to achieve these goal in a timely manner referral to rehab occurs.
Discharge planning begins on admission with a goal of discharge to inpatient rehabilitation or home with supports in 5-7 days.
Discharge planning; transition to inpatient rehab/restoration.
A decision to refer to inpatient rehab/restorative care is made based on the multidisciplinary team assessment. Referral occurs in a timely manner.
Acknowledging the first bed policy attempt is made to admit patients to the facility in which the SAT to which they are referred.
The patient and family are educated about the focus of an inpatient stay: to maximize their safe mobility and function in the home environment prior to prosthetic fitting or in the absence of prosthetic fitting.
Referral to the appropriate SAT is completed.
Discharge planning: transition to care in the community should include the following arrangements.
Confirmation of an appointment with
11
the appropriate SAT team.
CCAC OT assessment for home safety unless the patient has demonstrated high-level mobility and independence in the acute care setting (likely younger, non-dysvascular patients).
B. IN-PATIENT
I. Goals focus on safe discharge to the community and preparation for prosthetic fitting.
Ongoing mobilization: OT/PT to continue transfer training, strength, ROM, endurance activities.
Re-assessment: OT assessment for wheelchair and surface selection. All transtibial amputees are prescribed an appropriate amputee board.
LOS for amputees
Frequency of OP pre-gait follow-up on discharge
ROM and strength.
Discharge location.
The focus remains on function and activities required for safe discharge to the home environment There is an opportunity to increase the expectations of patients in taking responsibility for their role in recovery and the impact this has on their potential to achieve prosthetic use. Consistent messaging from all care providers is required
The core aspects of intervention occur. A focus on transfer of responsibility to the patient is less consistent.
Physiotherapy and Occupational intervention including common educational materials across sites. The inpatient stay continues with the goals established in acute care.
Appendix D: Above-Knee Amputation Post-op Information
Appendix E: Below-Knee Amputation Post-op Information
Mobilization;
Transfer training; slider board, low pivot, standing pivot.
Practice single leg stance.
ROM and stretching program as soon as tolerated.
UE ROM/strengthening exercise prescription.
Increasing activity tolerance:
Wheelchair mobility may be used as endurance activity if tolerated.
Hopping should be carefully assessed, likely performed with supervision or assistance.
Hopping independently should only occur in cases where balance and hopping skills demonstrated by the patient are highly proficient due to the risk of falling.
12
Seating and positioning (assessment and prescription occurs as soon as patient is medically stable enough to begin mobilizing): Transtibial residual limb is kept from dangling/hanging. When sitting in a wheelchair an amputee board is used to support the knee in extension, thereby reducing the risk of knee flexion contracture, assisting with edema management, pain control , alignment and skin integrity. Seating and positioning is complimented by patient education regarding the importance of elevation of the transtibial residual limb, as well as AROM exercises, in particular for hip and knee extension strength and ROM for all LE amputees. Improved patient self management; patient to be educated about the importance that they take responsibility for their recovery process should they wish to pursue prosthetic trial;
In preparation for discharge the patient is encouraged to complete aspects of their exercise program independently either in their room or with access to therapy area when distant supervision is possible.
Discharge planning begins on admission with a goal of discharge to home with supports in 1-3 weeks.
Goals for d/c focus on safe ability to transfer for ADL’s and IADL’s , education, independence and
13
adherence with exercise and edema/shaping management recommendations.
If patient has already been assessed in SAT follow-up outpatient PT appointment is provided.
If not yet assessed in the SAT patient is provided with this appointment (1-2 weeks post discharge).
CCAC OT assessment for home safety unless the patient has demonstrated high-level mobility and independence in the acute care setting (likely younger, non-dysvascular patients).
Inpatient rehab for prosthetic gait training: Most often by the time patients are ready to proceed with prosthetic gait training they no longer have the nursing needs that require an inpatient stay. In the case of transfemoral amputees the skills that are predictive of successful, functional prosthetic use of prosthesis include higher level, independently mobility. However there may be times where an inpatient stay is required.
Unilateral transtibial amputee: occasionally a patient may be struggling with some of the core skills (i.e. single leg stance) but the consensus of the SAT is that introduction of a prosthesis will allow the patient to improve their strength, ROM and ability to achieve the mobility required to be discharged to the community. In such cases prosthetic casting and fabrication should occur as soon as possible.
Bilateral transtibial amputees: again
14
consensus of the SAT may include prosthetic prescription to facilitate independent transfers and mobility required for safe discharge to the community.
Rurally located patients may have difficulty accessing the specialized outpatient amputee gait training programs. Alternative arrangements may need to be considered. This may involve CCAC to coordinate a respite, restorative or inpatient rehab stay to allow initial gait training with the support of the SAT. The prosthesis must be ready at the time of admission. On discharge PT care is transitioned to outpatients or CCAC in the patient’s community. Providers in the community must have access to consultation with the SAT. Arrangements for follow up in the SAT are established as part of discharge to the community.
II. Proper residual limb care resulting in the best quality limb for prosthetic fitting.
Evidence for best practice residual limb care. 15,21,22,23,24,25,26,27,32
Patients are assessed to determine the most appropriate and feasible residual limb shaping and edema control technique.
Tensor bandaging technique is inconsistent whether performed by the patient or nursing staff. The result is that tensoring is often done by therapy staff resulting in inadequate frequency of
See the wound management and shaping approach identified in acute care.
Where proper tensoring technique is not or cannot occur alternative methods must be implemented. This may include a elastic stockinette provided by the PT involved in care, or a manufactured shrinker or silicone liner provided by the certified prosthetist. Appendix G: Transtibial Residual Limb Edema/Shaping Documents
15
re-wrapping.
III. Ongoing best practice wound care.
There is an opportunity to increase collaboration regarding residual limb wound management between the inpatient unit and the SAT’s
There is not a strategy in place to facilitate specific collaboration.
BPG’s as overseen by in hospital wound care providers.
Develop a strategy for Communication and collaboration with the SAT’s.
C. OUT-PATIENT
I. Specialized Amputee Teams (Grand River Hospital: Prosthetic and Orthotic Clinic, St. Joseph’s Heatlh Care Amputee Clinic): Referral to the appropriate team occurs in a timely manner (see acute care).
Regular follow-up with the SAT occurs. For new amputees visits are more frequent. As the amputee gains functional independence with their prosthesis frequency of follow up is reduce and may become on an as needed basis only. Patients identified as high risk seen more frequently in order to prevent serious complications that may result in a decline in function, inability to use their prosthesis, higher level of care requirements, or hospitalization.
Evidence supporting the role of the SAT Evidences for benefits of preventative care. 1,2,4,5,6,7, 13,15,20, 34
Time from surgical intervention to initial assessment in SAT.
# New amputees assessed
# of new amputee that proceed to prosthetic trial
# longstanding prosthetic users /year
Level of new amputations.
Amputee Patients have prompt and ongoing access to the SAT. Assessment by a multi disciplinary , specialized team occurs promptly. The team include wound care expertise. There is a standing order for physiotherapy within the SAT.
Currently there are the two identified clinics. The clinic Guelph clinic has lacked adequate physician support as per ADP requirements.
Neither amputee team currently includes nursing support. Amputee teams have the ability to refer to social work, registered dietician, via
Grand River Hospital: Prosthetic and Orthotic Clinic, St. Joseph’s Health Care Amputee Clinic are both ADP registered clinics. ADP requires the prescriber (physiatrist); authorizer /vendor (Certified Prosthetist) and Rehabilitation Assessor (PT/OT) in the clinic delivery model for initial preparatory and definitive prostheses.
Amputee Teams have access to wound care expertise/nursing, social work, dietician, and occupational therapy (and recreation therapy). Referrals to the services are generated if the patient requires).
Initial visit to the SAT team includes a comprehensive, multi disciplinary assessment by the specialized team (Appendix H: Assessment Form)
Referral to PT for pre-gait involvement and for gait training is established as a standing order from the Amputee teams.
16
supporting outpatient programs.
# of patients on PRN status vs regular call back
age of amputees.
Follow up occurs regularly with the SAT Team. In high risk patients are placed on a call back schedule for check ups with the SAT in order to prevent complications (ie poor prosthetic fit management, skin breakdown issues both in the residual limb and remaining limb)
This currently occurs, but in less than consistent manner.
Regular follow –up through pre-gait, gait training, post gait, transition from the initial preparatory device to definitive prosthesis, regular follow post dispensation of the definitive particularly in higher risk case to prevent and/or manage complications.
SAT visits:
Initial consultation
Follow-up pre-gait if candidacy for prosthetic trial could not be determined at initial consult
Follow up review once gait training has begun (opportunity to team problem solving, alignment adjustment, planning)
Follow-up at 6 months post dispensation of temporary device to determine readiness to proceed to definitive prosthesis.
Follow-up post dispensation of definitive device.
If high risk patient may placed on call back schedule .
High functioning patients seek re-referral to SAT (ie for prosthetic wear, new medical changes) on a PRN basis.
Pre-gait training provided in cases where additional support and monitoring recommended by the SAT.
Evidence of key predictors of successful transition to functional prosthetic use. 2,3,6,8,10,11,12,13,1
# of pre-gait patients that proceed to fitting.
Length of time to fitting
An individualized pre-gait plan is established by the SAT to meet patient needs. Community
The SAT’s currently provide pre-gait consultation.
Physiotherapy: Pre-gait training, focused on ROM, strengthening, single leg stance tolerance, and activity tolerance, edema control/residuum shaping, monitoring of wound healing:
17
4,33 Cause of delay in fitting (wound healing, remaining limb status)
partners are engaged as needed to support the plan. Regular monitoring and plan adjustment occurs in the SAT.
A) Patient deemed an appropriate prosthetic candidate, but has not yet healed. The patient is identified by the SAT as high risk for the development of secondary impairments while waiting wound healing. Supervision of exercise activity is therefore recommended. Treatment can occur in a group format and be supervised by a therapy assistant with regular PT re-assessment, particularly for wound healing and readiness for fitting.
B) Patient deemed an appropriate prosthetic candidate but has not yet healed. Healing is expected to be fairly quick and the patient is assessed to be capable of independently completing a home program. Treatment is more consultative with instruction regarding home exercise program with periodic check up with the PT to monitor wound healing and readiness for fitting.
Once deemed appropriate for prosthetic trial the patient in provided with the appropriate information package. Appendix I: BKA prosthetic training information Appendix J: AKA prosthetic training information C) Patient is deemed borderline
appropriate for prosthetic trial. Time bound period of intervention (4 weeks) to determine if the patient demonstrates progression towards the skills required to be considered for prosthetic trial. At the end of the PT trial follow-up with the SAT occurs to
18
discuss next steps.
Individualized therapy plan is established and modified to address patient impairments and goals.
Occurs Physiotherapy intervention:
ROM: stretching for hip flexors, knee flexors and other ROM’s noted as limited.
Strengthening: UE progressive weight program, LE AROM and progressive weights as tolerated for hip extension, ab/adduction, knee extension, remaining ankle and core.
Activity tolerance activity: arm ergometry, recumbent elliptical, parallel bar hopping, wheelchair skills.
Single stance with progressive reduction in UE support.
If the patient or family is able to demonstrate the skills to properly tensor (technique and frequency) than education and training is provided.
In cases where tensoring cannot be safely implemented, alternative shaping/edema control must be implemented.
Appendix G: Transtibial Residual Limb Edema/Shaping Documents
Discharge planning:
A) Patient achieves wound healing and is able to proceed to the gait training process.
B) Patient demonstrates improved ability to follow through on independent home program but still does not have adequate wound closure. Visits
19
reduced to periodic wound checks and assessment with PT until ready for prosthetic fitting.
C) The patient who is borderline for prosthetic trial is re-assessed in the SAT following 4 weeks of intervention
Patient is now deemed a prosthetic candidate: either continues with pre-gait training or proceeds to prosthetic fitting.
Patient deemed unlikely to become a prosthetic candidate are educated why they are not a candidate, the specific skills required are re-iterated, referrals as required are generated (i.e. CCAC for wheelchair, other mobility devices, if not already done, community programs, social work, recreation therapy)
III. Outpatient PT provided by physiotherapist with specialized skills, abilities and knowledge of amputee care. The rehab assessor takes the lead.
Evidence of the benefits of the specialized team and care providers with expertise and experience in amputee care. Evidence supporting outcome measures for lower extremity amputees: timed walking test, LCI, SIGHAM
Timed walking tests when appropriate. (2MWT, L-Test, TUG, 6 MWT)
SIGAM
Monitoring progression of gait aid
Incidence of skin break down
LOS (AKA vs. BKA)
Degree of
The majority of patients deemed appropriate for prosthetic trial achieve some functional use. This should be documented in the ongoing monitoring and care through the SAT. Record keeping using standardized outcome measure: timed walking tests (2MWT, L-test)
This target occurs based on monitoring by the SAT of patients, however quantification of this could be more robust.
Physiotherapy: GAIT TRAINING: Once the patient has been casted and fitted they are ready to proceed with gait training. Prosthetist attends first PT visit with patient.
Frequency of visits are maximized in the first month of prosthetic use .
Visits may be group format, individual or a combination of depending on patient needs. Transtibial amputee typically is more easily managed in a group setting. Transfemoral amputee may require more individual sessions.
Progressive gait training; as patient skin integrity and tolerance allows the patient is progressed through a variety of gait aids, balance activities,
20
functional ambulation achieved (from limited indoor to community)
functional/ activity measures (LCI, SIGHAM). Data collection represents opportunity to participate and collaborate with larger teaching centres in research.
functional gait activity. o Ambulation in parallel bars o 2WW or rollator o single point canes, quad canes. o Balance activities; weight
shifting on level ground, on soft surfaces, stepping task, step up tasks, reaching
o Stair climbing, uneven ground, inclines, curbs
Activity tolerance.
Sock ply management.
Skin care and monitoring: residuum and remaining limb.
Falls education, floor to chair transfers.
Home use is gradually introduced when the patient is safely able to do so. Specific instructions are sent home with the patient.
As patient independence increases and home use is initiated PT visits are reduced. and then to periodic follow-up visits.
Discharge planning: individualize goals are set with each patient. There is significant variability amongst the amputee population depending on the patient’s age, level of amputation, etiology of amputation, number of co-morbidities. The level of anticipated functional prosthetic use is therefore also variable from limited indoor prosthetic use with a gait aid, to full community ambulation and re-integration without a device.
As a patient reaches their individualized goals Active PT intervention is reduced.
A follow-up plan with the Amputee
21
Team is established (see section re Prosthetic teams above.)
Links to community programs as appropriate are established.
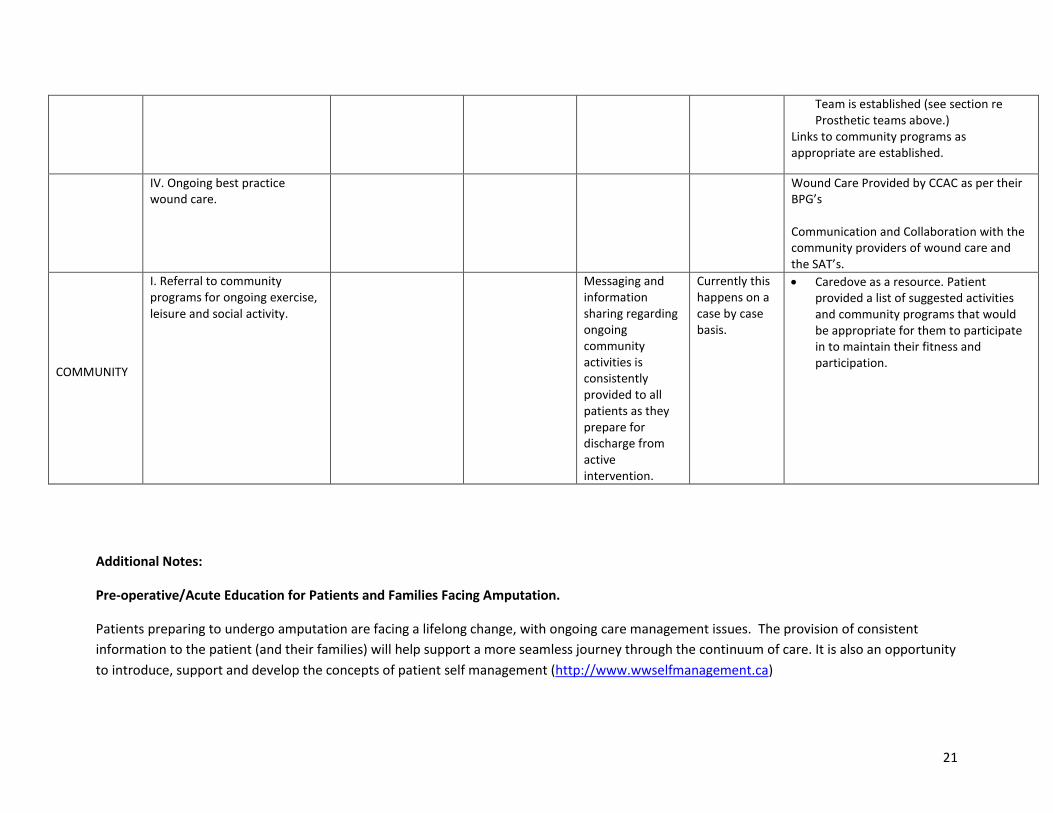
IV. Ongoing best practice wound care.
Wound Care Provided by CCAC as per their BPG’s Communication and Collaboration with the community providers of wound care and the SAT’s.
COMMUNITY
I. Referral to community programs for ongoing exercise, leisure and social activity.
Messaging and information sharing regarding ongoing community activities is consistently provided to all patients as they prepare for discharge from active intervention.
Currently this happens on a case by case basis.
Caredove as a resource. Patient provided a list of suggested activities and community programs that would be appropriate for them to participate in to maintain their fitness and participation.
Additional Notes:
Pre-operative/Acute Education for Patients and Families Facing Amputation.
Patients preparing to undergo amputation are facing a lifelong change, with ongoing care management issues. The provision of consistent
information to the patient (and their families) will help support a more seamless journey through the continuum of care. It is also an opportunity
to introduce, support and develop the concepts of patient self management (http://www.wwselfmanagement.ca)
22
There may be a risk of overwhelming the patient with information so whenever possible the documents should be delivered and explained to
family as well. The document should include:
Early post-op course; early mobilization procedure, dressings, post-op bed exercises.
d/c planning; when patient will be referred to rehab/restoration vs. when patient will be discharged home.
Referral to speacialized amputee clinic; which clinic they will be referred to (and if time and medical stability allows pre-op visit with the
amputee team)
o This includes information about the role of the clinic in determining a patient’s suitability for prosthetic trial, process if deemed
appropriate and long term follow up.
o ADP program information.
o Peer support services.
o Web based resources.
CCAC services that may be required.
Post-op follow-up with surgeon
Residual Limb Management in the transtibial amputation (for additional information see the Transtibial (Below Knee) Residual Limb Edema
and Shape Management Recommendation documents.
The impact of hip and knee flexion contractures on fitness for prosthetic trial:
The presence of hip and knee flexion contractures complicates the ability to comfortably and successfully fit an amputee with prosthesis.
In the transfemoral amputee hip flexion contractures of greater than 10-20 degrees negatively impact the amputee’s ability to achieve mid-stance alignment and to control the prosthetic knee joint. The patient is more likely to have difficulty locking the prosthetic knee in stance and is therefore at greater fall risk. Patients will compensate for the contracture by using hip retraction in stance and or increasing lumbar extension. This results in altered gait mechanics and poorer comfort.
In the transtibial amputee the presence of hip flexion contractures has similar impacts in increasing hip retraction and lumbar extension in stance. Knee flexion contractures result in increased pressure to the distal residuum, increased potential for skin breakdown, decreased comfort. The presence of significant contracture to both joints negatively impacts a patient’s ability to achieve safe standing balance, thereby limiting the potential to progress away from gait aids for safe ambulation, limiting the scope of standing tasks they can safely perform.
23
Contracture, once present in an amputee are difficulty to resolve due to the reduce lever arm for stretching that results post amputation. Pre-operative maximization of ROM, surgical procedures to avoid contracture formation and early post-surgical intervention to prevent contracture formation are key.
Multi-disciplinary Amputee Team Assessment: Initial assessment document in Appendices
- Current History as it relates to the amputation or potential amputation. - Past medical history; previous referrals and related health care supports (i.e. diabetic services), renal care, - Social history - Observation: circulatory assessment, LE and UE sensation, wound description and measurement (document with photo), strength and
ROM assessment, identification of contractures, particularly at hip and knee, stump shape, length, - Analysis; multidisciplinary analysis to establish recommendations regarding;
o Orthotic prescription to minimize risk of skin breakdown, support alignment (i.e. in case of a Charcot joint), off-load and promote healing In a LE with open areas
o Pre-amputation, pre- prosthetic need for PT assessment and intervention to maximize fitness and preparedness for potential gait training.
o Fitness for prosthetic trial. o For longstanding amputees; need to adjustments, repair, and replacement of prosthesis.
- Plan; multidisciplinary team provides: o Referral to other supports: diabetic clinic (via central referral), wound care services (CCAC) o Completion of ADP documentation for devices. o Referral to PT as required for pre-amputation, pre-gait and gait training.