Embed Size (px)
Citation preview

Integrated Dual Diagnosis Integrated Dual Diagnosis TreatmentTreatment
Implementation and Program Implementation and Program MaintenanceMaintenance
in Mental Health and in Mental Health and Substance Abuse SettingsSubstance Abuse Settings
Randi Tolliver, PhD, CADCRandi Tolliver, PhD, CADC
Illinois Co-Occurring Illinois Co-Occurring Center for ExcellenceCenter for Excellence

Training ObjectivesTraining Objectives
Review Key Components of the Integrated Dual Diagnosis Treatment Model
Program ImplementationOrganizational IssuesProgrammatic IssuesAgency Infrastructure

Training ObjectivesTraining Objectives
Program Evaluation
Agencies in Transition
Other Management & Staffing Considerations

“Co-occurring disorders may include any combination of two or more substance abuse disorders and mental disorders identified in the Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV). There are nospecific combinations of….disorders that are defined uniquely as co-occurring disorders.”
In “A Report to Congress on the Prevention and Treatment of Co-Occurring Substance Abuse Disorders and Mental Disorders”
SAMHSA DefinitionSAMHSA Definition

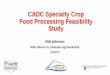
Comorbidity of Substance Use and Comorbidity of Substance Use and Specific AXIS I Psychiatric DisordersSpecific AXIS I Psychiatric Disorders
AnySubstance
AlcoholDiagnosis
Other Drug Diagnosis
Schizophrenia 47%
33.7% 27.5%
ASPD 83.6% 73.6% 42%
Anxiety disorders 23.7%
17.9% 11.9%
Phobia 22.9% 17.3% 11.2%
Panic disorder 35.8% 28.7% 16.7%
OCD32.8%
24% 18.4%
Bipolar Disorder
60.7% 46.2% 40.7%
Major depression 27.2%
16.5%* 18%
Regier DA et al. JAMA. 1990(Nov Regier DA et al. JAMA. 1990(Nov 21);264(19):2511-251821);264(19):2511-2518

Evidence-Based PracticeEvidence-Based Practice
Two Directions in EBP
Evidence-Based Interventions: • EB Guidelines, EB Practices, Empirically-
supported (validated) Treatments
Evidence-Based Process for decision-making:• EB Process, EB Individual Practice

Evidence-Based GuidelinesEvidence-Based Guidelines (EBG)(EBG)
Different methods for designing guidelines: global subjective judgment or consensus-based, outcomes based, preference based, expert opinion, evidence based
Importance of explicit, evidence-based process in developing guidelines

Evidence-Based ProcessEvidence-Based Process
EB Process is a way of doing practice which involves an individualizing process whereby evidence is used to make collaborative decisions with clients and caregivers. (Mullen, 2004)
EB Process is the integration of best research evidence with clinical expertise and patient values (Sackett et al., 2000).

Quadrants of CareQuadrants of Care

Integrated Dual Diagnosis Integrated Dual Diagnosis ServicesServices
Improve quality of life Utilize biopsychosocial treatments Promote consumer and family
involvement in service delivery Promote stable housing Promote employment as an expectation Promote hopeful interactions

Promote a recovery concept Increase continuity of care Increase consumer quality of life
outcomes Increase stable housing Increase employment Increase independent living
Integrated Dual Diagnosis Integrated Dual Diagnosis ServicesServices

Integrated Dual Diagnosis Integrated Dual Diagnosis TreatmentTreatment
Multidisciplinary TeamMultidisciplinary Team Views all activities of life as part of the
recovery process.
The Team provides each consumer with a variety of service professionals that can help in all aspects of life.
Members meet individually and as a group with each consumer and their support network (family, friends etc.) to discuss consumer’s progress and goals.

Stage-Wise InterventionsStage-Wise Interventions Individuals with dual disorders gain the
most confidence with their ability to recover or develop independent living skills and to meet daily living needs when they experience incremental successes through stages of treatment and change.
Caregivers and professional service providers should utilize the four stages of treatment to guide every interaction with individuals who have dual disorders.

Access to Comprehensive Access to Comprehensive ServicesServices
Programs offer comprehensive services because the recovery process occurs in the context of daily living.
Comprehensive Services Include:
Case Management
Integrated Substance Abuse and Mental Health Counseling
Medical Services
Housing/Residential Services
Supported Employment
Family Services
Assertive Community Treatment or Intensive Case Management

Time-Unlimited ServicesTime-Unlimited Services
Consumers with dual disorders may experience cycles of relapse and recovery throughout their lives.
Consumers will achieve the highest quality of life when they have access to services all the time.

Assertive OutreachAssertive Outreach
Programs utilize assertive outreach to keep consumers engaged in relationships (service professional, family, friends)
Service professionals who use assertive outreach:
Meet with their clients in the community Meet regularly with clients Offer practical assistance with daily needs
and living skills.

Motivational InterviewingMotivational Interviewing
The role of Motivational Interviewing in IDDT:
Help consumers examine their ambivalence about their goals and strategies
Help consumers identify their goals for daily living
Help consumers develop strategies for achieving those goals

Substance Abuse CounselingSubstance Abuse Counseling
Consumers are provided counseling that promotes recovery skills during the Active Treatment or Relapse Prevention Stage of Treatment
In group treatment• Consumers can develop peer support• Consumers learn from each other

Group TreatmentGroup Treatment
Agencies that offer group treatment:
Offer a menu of group treatment options
Offer group treatment options to all consumers who experience dual disorders

Family PsychoeducationFamily Psychoeducation
Social support plays a critical role in improving assessments and reducing relapse and hospitalization in persons with severe mental illness.
Family psychoeducational programs can be a powerful approach for improving substance abuse outcomes in clients with severe mental illness.

Participation in Alcohol & Participation in Alcohol & Drug Self-Help GroupsDrug Self-Help Groups
Social support plays an important role in reducing relapse for persons with dual disorders
Self-Help Groups provide consumers with opportunities to share and learn from others who experience dual disorders

Pharmacological TreatmentPharmacological Treatment
Medications are effective in the treatment of persons with severe mental illness and dual disorders
Medications are often most effective when accompanied by comprehensive integrated services and treatments.

Interventions to Promote Interventions to Promote HealthHealth
Individuals with dual disorders are at risk for poor health including:
Hospitalization and emergency room visits
Suicide and violence
Infectious diseases Complications resulting from
chronic illnesses

Secondary Interventions Secondary Interventions for Non-Responders for Non-Responders
to Substance Abuse Treatmentto Substance Abuse Treatment Have a specific plan to identify individuals
who are not responding to IDDT treatment
Questions to consider: What are the criteria to identify non -
responders? What is the process for the secondary
intervention? How does this get followed up?

Delivery of Services Delivery of Services
Guiding Principles for Effective Guiding Principles for Effective TreatmentTreatment
1 Employ a wellness & recovery perspective
2 Adopt a multi-problem viewpoint
3 Develop a phased approach
4 Address real-life problems early
5 Plan for cognitive and functional impairments
6 Use support systems to maintain and extend treatment effectiveness
Adapted from SAMHSA Tip 42

Organizational EnvironmentOrganizational Environment
Differences: Treatment
philosophy Treatment
practice Relationships
Common ground: Values and principles Guidelines Outcome measures
Vocabulary Basic competencies

Organizational ChangeOrganizational Change
Understanding the organization’s model
Multi-level organizations• Mutual and conflicting needs• Traditional versus innovative ways of
communicating• Systems tend to resist substantial
changeAdapted from Hendrickson, E. L (2006)

Program DevelopmentProgram Development
Utilize evidence-based or best practices
Utilize a competency-based perspective
Employ recovery support specialists
Develop a plan to address housing needs
Employ employment specialists

Program DevelopmentProgram Development
Develop policy & procedures for program operations
Develop a clear understanding of target population
Develop a marketing strategy that will ensure adequate numbers of consumers are engaged

Program DevelopmentProgram Development
Develop a realistic time frame for hiring and training staff
Establish a functional and clear admission and referral process
Allow easy accessibility to program services across the continuum of care

Necessary InfrastructureNecessary Infrastructure
Supervisor support for models or changes
Specific assessment instruments
Training protocol for providers
Implementation of treatment model Utilization of outcome evaluation Considerations of staff qualifications and training
needs Recognition of additional/other needs

Questions to Consider Questions to Consider for Development and for Development and
ImplementationImplementation Currently, which co-occurring treatment
services are being offered to which consumers?
Where in the continuum of care are the services being offered?
Do current services demonstrate the qualities of “effective” services?
Do the services meet the needs of the community?
SAMHSA Tip 42

Questions to ConsiderQuestions to Consider
What is the capacity of the agency to implement comprehensive, integrated services?
What are the core competencies needed for staff to provide effective services?

Implementation ChallengesImplementation Challenges
Physician or psychiatrist staffing
Physical resources
Billing and reimbursement issues
McGovern, Xie, et. al. (2006).

Implementation ChallengesImplementation Challenges
Identifying and responding to gaps in workforce competencies, certifications, and licensure
Addressing increases in staff concern related to changes in roles and responsibilities
Addressing discrepancies in record keeping

Implementation ChallengesImplementation Challenges
Addressing organizational structure and policies
Resolving differences in treatment philosophies
Establishing a cohesive multidisciplinary team

Program EvaluationProgram Evaluation
General Organization Index (GOI)
Integrated Dual Diagnosis Treatment (IDDT) Fidelity Scale
Dual Diagnosis Capability in Addiction Treatment (DDCAT) Index

General Organizational General Organizational IndexIndex
1. Program Philosophy2. Eligibility/ Consumer Information3. Penetration4. Assessment5. Individualized Treatment Plan6. Individualized Treatment7. Training

General Organizational General Organizational IndexIndex
8. Supervision9. Process Monitoring10. Outcome Monitoring11. Quality Assurance12. Consumer Choice Regarding Service
Provision

IDDT Fidelity ScaleIDDT Fidelity Scale
1. Multidisciplinary Team2. Stage-Wise Interventions3. Access to Comprehensive DD
Services4. Time-Unlimited Services5. Outreach6. Motivational

IDDT Fidelity ScaleIDDT Fidelity Scale
7. Substance Abuse Counseling8. Group DD Treatment9. Family Psychoeducation on DD10. Participation in Alcohol & Drug Self-Help
Groups11. Pharmacological Treatment12. Interventions to Promote Health13. Secondary Interventions to Substance
Abuse Treatment Non-Responders

Dual Diagnosis Capability Dual Diagnosis Capability in Addiction Treatmentin Addiction Treatment
(DDCAT) Index(DDCAT) Index
1. Program Structure2. Program Milieu3. Clinical Process:
Assessment4. Clinical Process: Treatment5. Continuity of Care6. Staffing7. Training

DDCAT (3.2): 7 DIMENSIONS DDCAT (3.2): 7 DIMENSIONS
Dimension Content of items
I Program Structure
Program mission, structure and financing, format for delivery of mental health services.
II Program Milieu
Physical, social and cultural environment for persons with psychiatric problems.
III Clinical Process: Assessment
Processes for access and entry into services, screening, assessment & diagnosis.
IV Clinical Process: Treatment
Processes for treatment including pharmacological and psychosocial evidence-based formats.
V Continuity of Care
Discharge and continuity for both substance use and psychiatric services, peer recovery supports.
VI Staffing Presence, role and integration of staff with mental health expertise, supervision process
VII Training Proportion of staff trained and program’s training strategy for co-occurring disorder issues.
McGovern, Giard, et al. (2006).

Measuring Changes Measuring Changes
Client Readiness for Change (Prochaska, DiClemente, and Norcoss, 1992)
Substance Abuse Treatment Scale (Mueser, Drake, Clark, Mchugo, Mercer-
McFadden, Ackerson, 1995)
Stages of Change Readiness and Treatment Eagerness Scale
(Miller & Tonigan, 1996)

Program Commitment PlanProgram Commitment Plan Specific statements of services to be
implemented
Identification of individual(s) to monitor implementation
Identification of ways to measure effectiveness of services
Method for implementing services
Adapted from Hendrickson, E. L (2006)

Program Commitment PlanProgram Commitment Plan
Development of timeline for implementation
Process to determine effectiveness of plan implementation
Method for ongoing review and modification of the plan
Adapted from Hendrickson, E. L (2006)

Agencies in TransitionAgencies in Transition
Currently numerous agencies within Illinois are providing a level of dual diagnosis services
• Organizational level• Program level• Provider level

Program ManagementProgram Management
Ensure compliance with all licensure requirements
Develop policies and procedures for all program activities
Maintain effective working relations with other community agencies / Collaborate
Build consensus Adapted from Hendrickson, E. L (2006)

Program ManagementProgram Management
Maintain systems that ensure consumers move through treatment services in the easiest manner
Manage data systems
Ensure all information needed by funding sources is provided accurately and on time
Adapted from Hendrickson, E. L (2006)

Program ManagementProgram Management
Ensure compliance with all licensure requirements
Develop policies and procedures for all program activities
Maintain effective working relations with other community agencies
Adapted from Hendrickson, E. L (2006)

Effective ManagementEffective Management
The ability to communicate to all staff in a clear and timely manner the decisions made and the rationale for them
The ability to successfully develop relationships with other community agencies
The ability to operate both as an ally and loyal opposition when dealing with organizations the that have authority over the program.
Adapted from Hendrickson, E. L (2006)

Effective ManagementEffective Management
Understanding traditions, values, and ethics that clinicians and administrative staff follow
Leadership
Ensuring program survival
Being able to listen and consider all staff input while being decisive when necessary
Adapted from Hendrickson, E. L (2006)

TIP 42, Figure 3-7TIP 42, Figure 3-7
Essential Attitudes and Values Essential Attitudes and Values for Providers of Co-Occurring for Providers of Co-Occurring
Disorder ServicesDisorder Services• Awareness of personal reactions and
feelings
• Recognition of limitations of one’s own personal knowledge and expertise
• Recognition of the value of consumer input into treatment goals and receptivity to client feedback

TIP 42, Figure 3-7TIP 42, Figure 3-7
Essential Attitudes and Values Essential Attitudes and Values
• Desire and willingness to work with individuals diagnosed with a co-occurring disorder
• Appreciation of the complexity of co-occurring disorders
• Cultural competence
• Openness to new information• Ability to employ diverse theories, concepts,
models, and methods

TIP 42, Figure 3-7TIP 42, Figure 3-7
Essential Attitudes and Values Essential Attitudes and Values
• Belief that all individuals have strengths and are capable of growth and development
• Patience, perseverance, and therapeutic optimism
• Recognition of the rights of consumers diagnosed with co-occurring disorders, including the right and need to understand assessment results and the treatment plan

Additional AttributesAdditional Attributes
• Flexibility • Optimism • Creativity• Respectfulness• Cooperativeness

ReferencesReferences
• Evans, K. & Sullivan, J. M. (2001). Dual Diagnosis: Counseling the Mentally Ill Substance Abuser (2nd Ed.). New York: Guilford.
• Gibbs, L.E. (2003). Evidence-based practice for the helping professions: A practical guide with integrated multimedia. Pacific Grove, CA: Brooks/Cole-Thompson Learning.
• Hendrickson, E. L (2006). Designing, Implementing, and Managing Treatment Services for Individuals with Co-Occurring Mental Health and Substance Use Disorders: Blueprints for Action. Binghampton, NY: Haworth Press.

ReferencesReferences• Hendrickson, E. L. & Schmal, M. (1993). Dual
Disorders Page, TIE Lines, 10 (3), 11.
• McGovern, M. P., Giard, J., Brown, J., Comaty, J., & Riise, K. (2006). The Dual Diagnosis Capability in Addiction Treatment (DDCAT): A Toolkit for Enhancing Addiction Only Service (AOS) Programs and Dual Diagnosis Capable (DDC) Programs. Unpublished manuscript, Dartmouth Medical School.
• McGovern, M.P., Xie, H., Segal, S. R., Siembab, L., & Drake, R. E. (2006). Addiction treatment services and co-occurring disorders: Prevalence estimates, treatment practices, and barriers. Journal of Substance Abuse Treatment (31), 276-275.

ReferencesReferences• Mullen, E. J. (2004). Facilitating practitioner
use of evidence-based practice. In A. R. Roberts & K. Yeager (Eds.), Evidence-Based Practice Manual: Research and Outcome Measures in Health and Human Services. New York: Oxford University Press.
• Regier, D. A., Farmer, M. E., Rae, D. S., et al. Regier, D. A., Farmer, M. E., Rae, D. S., et al. (1990). (1990). Comorbidity of mental disorders with Comorbidity of mental disorders with alcohol and other drug abuse: Results from alcohol and other drug abuse: Results from the Epidemiologic Catchment Area (ECA) the Epidemiologic Catchment Area (ECA) StudyStudy. Journal of American Medical . Journal of American Medical Association, 264, 2511-2518. Association, 264, 2511-2518.

ReferencesReferences
• Sackett, D.L., Richardson, W.S., Rosenberg, W. M. C., & Haynes, R. B. (2000). Evidence-Based Medicine: How to Practice and Teach Evidence Based Medicine (2nd ed.). London: Churchill-Livingstone.