Embed Size (px)
Citation preview

Integrating HIV Prevention and
Surveillance: Building an Effective Program and
Workforce Moderator: Romni Neiman, Assistant Branch Chief, CDPH STD Control Branch
Panelists: Matthew Millspaugh, Chief, HIV Program Section, CDPH/OA
Kristy Michie, MS, Monterey County Public Health Department
Lauren Brookshire, MPH, MSW, HIV, STD, Hepatitis Branch, Public Health Services, San Diego County
Jessica Osorio, HIV/AIDS and STD Programs, Contra Costa County Public Health Department

Learning Objectives • Identify existing workforce resources (e.g., personnel,
job roles/titles, staffing structure, outside stakeholders, etc) and possible ways to shift resources to match new priorities.
• Describe how several LHJs have successfully adjusted workforce resources in order to integrate surveillance and prevention activities.
• Identify concrete first and follow up steps towards filling gaps and aligning resources with new priorities under 18-1802 funding.

Program Expectations • Treatment as Prevention!
• Achieve viral suppression through • HIV testing of those at risk
• Young Gay/Bi/MSM of Color • Trangendered Individuals
• Linkage to PrEP and PEP • Linkage to STD Testing/Treatment
• Linkage to HIV care and treatment
• Use data to inform public health interventions • Data sharing to initiate client-level service integration for
STD, PrEP and HIV care. • Evaluate outcomes of local HIV program interventions (i.e.
number of new positives identified, proportion of new positives linked to care, people linked to PrEP, etc.)

Program Direction • Do More
• Routine opt-out HIV testing in medical settings
• Client navigation services for health insurance, PrEP & HIV care and treatment
• Client-level integration of STD & HIV services
• Partner services as a pathway to facilitate testing and linkage
• Support Syringe Services Programs (SSP)
• Data driven interventions for those at highest risk for acquiring HIV or falling out of care.
• Do Less • Risk Reduction Activities
(RRA) • Targeted HIV Testing in
sites with no positivity in past three years.

Program Implications • Is your current program well positioned to meet the new program
expectations? • Can be big challenge to re-align staffing and program emphasis • 3rd Party such as a CBA provider facilitate a capacity building effort to think
through staffing/contractual/program changes. • What opportunities will the PrEP-AP program bring regarding providing STD care
and linkage to PrEP • What policies & procedures do you have to
• Support STD/HIV surveillance informed public health program action • Implement integrated services by
• public health • medical providers
• What program organization & staffing do you have or need to develop/hire for • support client navigation (PrEP. LTC, re-engangement to care) • support partner services • Routine Testing • Intergration of STD/HIV/Hep client level

Program Implications Cont. • Syringe Exchange/SSP
• Huge Change – Previously no CDC funding has gone to SSP’s in the 20 jurisdictions being funded.
• Understand that certain LHJs directly supporting SSPs is not politically viable – however what other steps can you take to support SSP indirectly? • LTC- Many people having a romance with drugs have a
difficult time remaining in care. Funding LTC within a SSP either directly or via a CBO could be an option.
• Funding other services in support of LTC and whole person health for HIV positive persons, navigating to PrEP, etc. could be a solution
• You are not alone, OA has team of people ready to assist you with TA, consultation and strategy in support of developing SSPs and support services at SSPs

Program Implications Cont.
• SSP Certification • In 2013 CDPH/OA established the Syringe
Exchange Certification Program • Allows qualified entities to apply directly to
CDPH/OA for authorization to provide syringe exchange services.
• All qualified SEPs are eligible to participate in the CA Syringe Exchange Supply Clearinghouse, which prides a baseline level of supplies to authorized programs.

Workforce/Strategy Changes at OA • OA staff will need to change our work to reflect 18-
1802 so we can support the LHJs and move forward towards Getting to Zero
• Prevention has utilized a CBA Provider to take a look at our branch structure and is currently evaluating what steps to take to re-align staff towards activities under 18-1802 • PrEP/PEP Navigation • LTC • Routine Testing • Gay Men/Transgender Sexual Health • D2C • PS • Enhanced support of coordinating CBA providers and related
evaulation

Workforce/Strategy Changes at OA • Build and strengthen programmatic
integration between STDCB and OA • OA currently funds PS training and capacity
building efforts with STDCB – build on this to enhance capacity to support STD/HIV/PrEP/D2C program capacity at LHJ level
• Strengthen collaboration with CARE, Surveillance and ADAP • Support strategies for braiding funding and
resources under Prevention, CARE and PrEP-AP • Bring in CBA to assist with capacity building

OA, CBA Providers and your fellow LHJs are resources • Utilize OA staff for TA and guidance while you
are developing your transition plans • Utilize CBA providers to assist with capacity
building, provider training, workforce training/development, consumer engagement, etc.
• Engage with other LHJs you have heard from how they have approached challenges regarding LTC, Routine Testing, PrEP/PEP Navigation etc.

Monterey County Health Department: Testing Strategy • Discontinued OA funded community-based HIV
testing in early 2015 • Low yield of new positives for effort
• 2013: cost ≈ $15,000 for 1 new + (1 + / 490 tests) • 2014: cost ≈ $15,000 for 1 new + (1 + / 125 tests, 2x $)
• Identified priority providers and facility types • Reported >1 case in 2014 (low hanging fruit) • Potential high volume testers • Did not include HIV care clinics
• Initiated routine, opt-out testing outreach • Provider outreach (not detailing) for prioritized facilities • Added to other individual provider-level interactions
(convenience outreach) • Health Updates and articles in other routine provider
communications

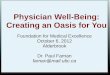
Monterey County Health Department: Testing Strategy
0
2
4
6
8
10
12
Num
ber o
f New
Pos
itive
s
New Positives by Diagnosing Facility Type
2014 2017*
*Through October 2017

San Diego Data to Care
Lauren Brookshire County of San Diego November 29, 2017

San Diego – Data to Care
• Organizational structure • Work teams • Training • Roll-out • Working with providers • Lessons learned

Contra Costa County Workforce Implications of Data-to-Care & RAPID
Interventions
Jessica Osorio Interim Director
HIV/AIDS & STD Program

Contra Costa Snapshot • Mid-sized LHJ – Part of Bay Area counties • Approximately 100 new infections a year • Roughly 2300 PLWHA • Integrated HIV/STD program • 4 county Positive Health Clinics
• Staffed by our program’s medical case managers
• Staff: • 9 MSWs • 6 DITs/Senior DITs (2 housed with STD, 2 HIV Outreach
Workers, all provide HIV counseling & testing) • 2 Health Educators

Intervention One: Line List Program • Uses State STD Surveillance data to identify
individuals at increased risk of HIV and link them to services
• Line List Priority Individuals: • Coinfected (HIV & STD) • MSM • Transgender • Women of Color
• Disease Intervention Technicians (DITs) are assigned lists of priority individuals: Spanish language calls also made.

Line List Calls Process & Outcomes • Use separate scripts & conversation flow charts for HIV+ and
HIV- • HIV+: provide risk reduction education, link / re-link to HIV & STD
care, offer partner services • HIV-: provide risk reduction education, link to HIV testing, link / re-
link to STD care, connect with PrEP Navigator • “Sub lists” forming for additional follow up and support: Already on
PrEP, Linked to PrEP, Repeat STDs (same individual on multiple lists for new STD infections)
• Workforce Outcomes: • DITs with expertise with high-risk negative • Sr DIT developed as PrEP Navigator developing PrEP campaign • Further integration of HIV & STD teams
• Outcomes tracked by Planner/Evaluator & Education & Prevention Manager

Intervention Two: RAPID Linkage to Care • In Spring 2016, set goal
to decrease linkage time (prescribing meds at first visit as opposed to waiting for lab work)
• Utilized existing staff & policies from HIV/AIDS & STD Program
• Protocol for linking new positives was shared with clinicians more widely
Funding • Nothing new – a little bit
of many peoples’ time • Part A: Medical Case
Management (linkage) / Ambulatory Care (some provider time, labs, etc.)
• Part B: Outreach Services (DITS), MAI
• Part C: Outreach Services (Community-based)

Linkage to Care Overview
• HIV/AIDS Program outreach workers (DITs) get new positives from testing site to first positive health appointment (warm handoffs)
• Clinicians: Call our program right away with any new positives • Notice in EPIC put in place with instruction to call our program
• All new positives are called within 24 hours by MCM • If no response, assigned to an outreach worker: additional calls, home visits
• Counseling and overview of MCM program, services, and care • Assistance making appointments to get lab work and begin treatment
ASAP • MCMs and outreach workers staff positive health clinics; meet clients
there for first appointment • Enroll in MCM • Provide with urgent referrals and information: food, housing, nurse case
management

Linkage to Care Workforce Outcomes • All existing staff – no new hires • Increased coordination between clinical & PH
department staff • Clinicians • Outreach Workers • DITs / Sr DITs (PrEP navigation / “prevention with
positives” • Health Educators (New positives class; risk reduction
education) • PH Management • Epidemiologist (Partner Services)