Embed Size (px)
DESCRIPTION
Integrating Primary Eye Care and Primary Health Care 17 th Sept 2012. Dr Padmaja Kumari Rani,M.S,FNB (Retina) Head, Village Vision Complex International Centre for Advancement of Rural Eye Care (ICARE) L V Prasad Eye Institute Hyderabad. - PowerPoint PPT Presentation
Citation preview

Integrating Primary Eye Care and
Primary Health Care17th Sept 2012
Dr Padmaja Kumari Rani,M.S,FNB (Retina)Head, Village Vision ComplexInternational Centre for Advancement of Rural Eye Care (ICARE)L V Prasad Eye InstituteHyderabad

Acknowledgement:Puwat Charukamnoetkanok, MD, Thailand

IntegratingPrimary Eye Care
and Primary Health Care
• Why • What• How • Global Scenario – Thailand Case Study• Indian Scenario (OEU & LVPEI Case studies)• Challenges• Way forward

Why?
• Holistic care
• Treating causes of causes
• Wide reach
• Sustainability

What?
WHO

What?
• Horizontal approach
• Team work
• Networking

What?
WHO

How?
• Location
• Areas of Integration
• Stake holders

How?
Khan et al

Global scenario-Thailand

Global scenario-Thailand

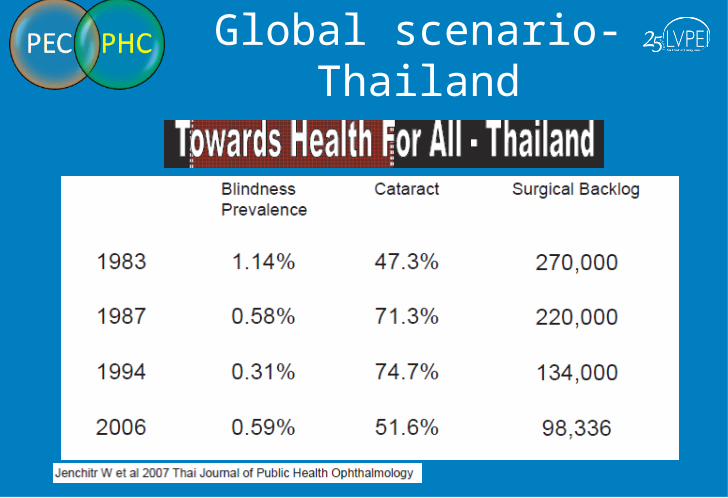
Global scenario-Thailand

• Launched in 1963
• 15 Projects
• 11 Partners
• 9 States & UT
• 3.4 million - people
covered
• 0.75 million – persons
directly benefited
HBCEHP –
USEHP –
OE India -
Indian scenario – OEU Operation Eye Sight Universal – India
•Immunization coverage •ANC/ PNC coverage has reached 100%•Increased Awareness levels

Indian scenario – LVPEI
To eliminate avoidable blindness through
integration of Primary eye care with Primary health
care by community Development Initiatives.

Who is a Vision health guardian
•Local village person
•Literate
•Healing touch
•Health worker background

LVPEI (2010-2012)
• One tiny Village (5 months) – n-746
• Mandal ( District Subunit) – 54 villages with (2011-14) n-39,000
• Present Coverage – 70 villages -n-100,000

Methodology
i. Identification and Training of Village Vision Health Guardians
i. Awareness creation
ii. Service delivery
iii. Community Development Initiatives

Methodology I . Identification and Training of Village Vision Health
Guardians and village vision committee formation

Methodology
II. Awareness creation
Teacher conducting Eye screeningTeachers Training Program

Methodology
III. Service delivery

MethodologyIV: Community Development Initiatives
JSS trade training program inauguration JSS trade training program in house wiring and electrical maintenance for village youth
Vision Garden Inauguration

Coverage of One Mandal -54 Villages

Situational Analysis of Study area
Illiteracy in Jainad Mandal 39.45 % - very low in females
% of population below poverty line >26%
Pattern of agricultureDry crops / irrigated dry crops cultivation due to lack of perennial source of irrigation
InfrastructurePoor Drainage / Sanitation / Power supply, roads etc.,
Employment opportunitiesMeager, due to lack of industries or arable lands and low scope for self employment
Type of houses 50% Semi pucca
Gas connection 30%
Individual toilets attached to houses 26%
Average percapita annual income
Rs 29,187/-
GDP : 8,786 crores [2007-2008]
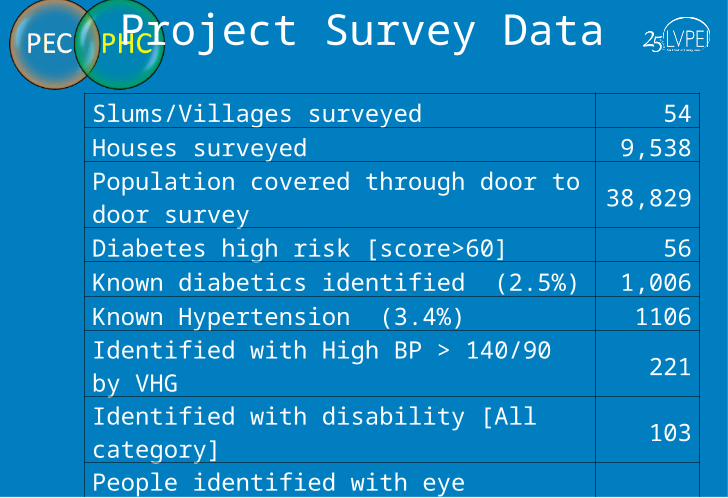
Project Survey Data
Slums/Villages surveyed 54Houses surveyed 9,538
Population covered through door to door survey 38,829
Diabetes high risk [score>60] 56Known diabetics identified (2.5%) 1,006Known Hypertension (3.4%) 1106Identified with High BP > 140/90 by VHG 221Identified with disability [All category] 103People identified with eye ailments and referred for eye examination
2,740
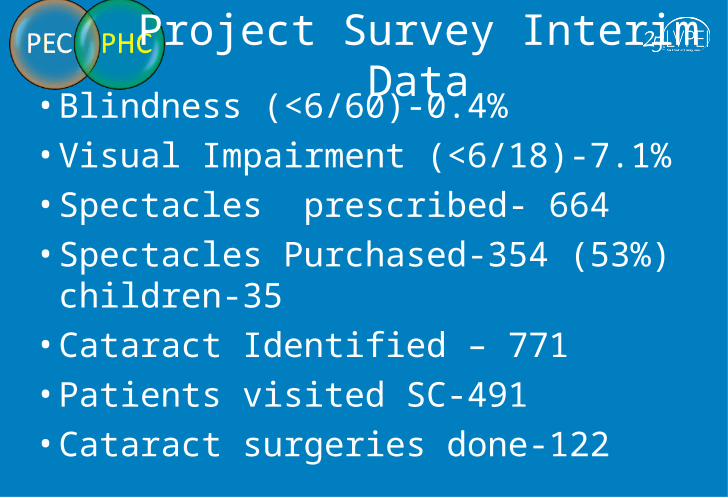
Project Survey Interim Data
• Blindness (<6/60)-0.4%• Visual Impairment (<6/18)-7.1%• Spectacles prescribed- 664• Spectacles Purchased-354 (53%) children-35• Cataract Identified – 771• Patients visited SC-491• Cataract surgeries done-122

Project Survey Interim Data
• Eye health and Primary health education events conducted -363
• n-2,877 • Number of pregnant women in the covered
villages - 408• Antenatal care-408 , Postnatal care-140

Qualitative Impact
Master SaiKumar
Three VHGs – enrolled as Vision technicians

Challenges
• Slow Process• Linkage with health care providers• Understanding Motivators/Barriers for
performance of VHGs • Measuring the Impact

Way forward
• Cost effective Technology Innovations
• Care of the Community, by the Community and for the Community

“Thousands of candles can be lit from a single candle, and the life of the candle will not be shorter. Happiness never decreases by being shared.”
The Buddha

L V Prasad Eye Institutewww.lvpei.org
Thank you!
Excellence
Equity
Efficiency





























