Embed Size (px)
Citation preview
INTERACT II: INTERACT II: Interventions to Reduce Acute Interventions to Reduce Acute
Care TransfersCare Transfers
Joseph G. Ouslander, M.D.Joseph G. Ouslander, M.D.
Professor of Clinical Biomedical ScienceProfessor of Clinical Biomedical ScienceAssociate Dean for Geriatric ProgramsAssociate Dean for Geriatric Programs
Charles E. Schmidt College of Biomedical ScienceCharles E. Schmidt College of Biomedical ScienceFlorida Atlantic UniversityFlorida Atlantic University
Assistant Dean for Geriatric EducationAssistant Dean for Geriatric EducationUniversity of Miami Miller School of Medicine (UMMSM) at Florida Atlantic UniversityUniversity of Miami Miller School of Medicine (UMMSM) at Florida Atlantic University
Laurie Herndon, MSN, GNP-BC, ANP-BCLaurie Herndon, MSN, GNP-BC, ANP-BC
Director of Clinical QualityDirector of Clinical QualityMassachusetts Senior Care FoundationMassachusetts Senior Care Foundation
Today we will…Today we will…
Describe the key components of the Describe the key components of the INTERACT II toolkitINTERACT II toolkit
Share “early lessons” from current Share “early lessons” from current INTERACT II collaborative projectINTERACT II collaborative project
Provide strategies for immediate Provide strategies for immediate implementation of INTERACT II tools at implementation of INTERACT II tools at your facilityyour facility
Why this matters…Why this matters…
Mr. DeMayo is an 97 year old long term Mr. DeMayo is an 97 year old long term care resident at your facility. care resident at your facility.
Pancreatic cancerPancreatic cancer
Functional declineFunctional decline
No appetiteNo appetite
““Ready to go be with Eleanor”Ready to go be with Eleanor”
DNR/DNIDNR/DNI
Saturday morning wakes up and says he Saturday morning wakes up and says he feels lousy.feels lousy.Stays in bed all day and doesn’t eatStays in bed all day and doesn’t eatSunday morning has a fever and has Sunday morning has a fever and has several episodes of vomitingseveral episodes of vomitingAppears dehydrated and weakAppears dehydrated and weakSon visits and expresses concern for his Son visits and expresses concern for his father. Wonders if “this is the beginning of father. Wonders if “this is the beginning of the end?”the end?”
Nurse calls covering physicianNurse calls covering physician
Reports that son is concernedReports that son is concerned
Physician says to send this resident to the Physician says to send this resident to the ED for evaluationED for evaluation
What just happened here?What just happened here?Did he want to go to the hospital?Did he want to go to the hospital?Did that conversation ever happen?Did that conversation ever happen?Was the ED the best place for this resident Was the ED the best place for this resident to be evaluated?to be evaluated?Could his needs have been met in the Could his needs have been met in the nursing home? nursing home? Could this transfer have been prevented?Could this transfer have been prevented?How would you know?How would you know?Where would you begin?Where would you begin?
Hospitalizations of NH residents Hospitalizations of NH residents are commonare common
In any six month period, more than 15% of long stay In any six month period, more than 15% of long stay residents are hospitalizedresidents are hospitalized
– O Intrator, J. Zinn, and V. Mor, “Nursing Home Characteristics and Potentially Preventable Hospitalizations” O Intrator, J. Zinn, and V. Mor, “Nursing Home Characteristics and Potentially Preventable Hospitalizations” Journal of the American Geriatrics Society 52, no. 10(2004): 1730-1736Journal of the American Geriatrics Society 52, no. 10(2004): 1730-1736
Previous research suggests many such hospitalizations are Previous research suggests many such hospitalizations are inappropriate and are related to ambulatory care sensitive inappropriate and are related to ambulatory care sensitive diagnoses diagnoses
45% of admissions of 100 residents from 7 Los Angeles 45% of admissions of 100 residents from 7 Los Angeles nursing homes to acute hospitals were rated as nursing homes to acute hospitals were rated as inappropriateinappropriate Saliba et al, J Amer Geriatr Soc 48:154-163, 2000Saliba et al, J Amer Geriatr Soc 48:154-163, 2000
Why this matters…Why this matters…
Hospitalizations Hospitalizations cause cause morbid morbid complications complications for for NH residentsNH residents– DeconditioningDeconditioning– Pressure UlcersPressure Ulcers– DeliriumDelirium– Injurious FallsInjurious Falls– PolypharmacyPolypharmacy
Why this matters…Why this matters…
Unnecessary hospitalizations are expensiveUnnecessary hospitalizations are expensive
Medicare spent close to $200 million on hospitalizations Medicare spent close to $200 million on hospitalizations related to Ambulatory Care Sensitive Diagnoses among related to Ambulatory Care Sensitive Diagnoses among long-stay NH residents in New York state in 2004long-stay NH residents in New York state in 2004
This figure This figure does not includedoes not include residents on the Part A residents on the Part A skilled benefit, who get hospitalized frequentlyskilled benefit, who get hospitalized frequently
Grabowski et al, Health Affairs 26: 1753-1761, 2007Grabowski et al, Health Affairs 26: 1753-1761, 2007
The OpportunityThe Opportunity
Reducing potentially avoidable Reducing potentially avoidable hospitalizations of NH residents hospitalizations of NH residents represents an opportunity to:represents an opportunity to:– Decrease emotional trauma to the Decrease emotional trauma to the
resident and familyresident and family
– Decrease complications of Decrease complications of hospitalizationhospitalization
– Reduce overall health care costsReduce overall health care costs
BackgroundBackground
CMS Special Study awarded to Georgia CMS Special Study awarded to Georgia Medical Foundation July 2006-Jan 2008Medical Foundation July 2006-Jan 2008– Looked at characteristics of NHs in Georgia Looked at characteristics of NHs in Georgia
with high and low hospitalization rateswith high and low hospitalization rates– Implemented toolkit in 3 NHs with high Implemented toolkit in 3 NHs with high
hospitalization rateshospitalization rates– 50% reduction in hospitalizations50% reduction in hospitalizations– 36% reduction in hospitalizations rated as 36% reduction in hospitalizations rated as
avoidableavoidable
Principal Investigator: Principal Investigator: Dr. Joseph G OuslanderDr. Joseph G Ouslander
Co-Principal Investigator: Co-Principal Investigator: Dr. Gerri Lamb Dr. Gerri Lamb
Independence Foundation and Independence Foundation and Wesley Woods ChairWesley Woods Chair
Associate Professor of NursingAssociate Professor of NursingEmory UniversityEmory University
Collaborators:Collaborators: Laurie Herndon, MSN, GNP-BCLaurie Herndon, MSN, GNP-BC Senior Project CoordinatorSenior Project Coordinator
Alice Bonner, PhD, RNAlice Bonner, PhD, RNCo-InvestigatorCo-InvestigatorMassachusetts Department of Public Massachusetts Department of Public
HealthHealth
Multidisciplinary teams from MA, NY, and FLMultidisciplinary teams from MA, NY, and FL
INTERACT IIINTERACT IIFunded by the Commonwealth FundFunded by the Commonwealth Fund
MethodsMethods
Obtain inputObtain input– National expertsNational experts– Frontline staffFrontline staffRefine toolkitRefine toolkitImplement and evaluate refined toolkitImplement and evaluate refined toolkit– Quality Improvement projectQuality Improvement project– Principals of Institute for Healthcare Principals of Institute for Healthcare
Improvement (IHI) CollaborativeImprovement (IHI) CollaborativeChampionChampionCollaborative CallsCollaborative Calls
MethodsMethods
– Collect data during the Collaborative that will be used Collect data during the Collaborative that will be used to:to:
Understand factors and strategies that are Understand factors and strategies that are important for successful implementation and important for successful implementation and sustained use of the toolkit sustained use of the toolkit
Estimate the costs of implementing the toolkit to Estimate the costs of implementing the toolkit to inform P4P initiativesinform P4P initiatives
– Explore incorporating key elements of the toolkit into Explore incorporating key elements of the toolkit into health information technology (HIT) using web-based health information technology (HIT) using web-based formats and/or an electronic health recordformats and/or an electronic health record

Working Together to Improve Care, Communication, and Continuity for
our Residents
Organization of Tools in ToolkitOrganization of Tools in Toolkit
Communication ToolsCommunication Tools
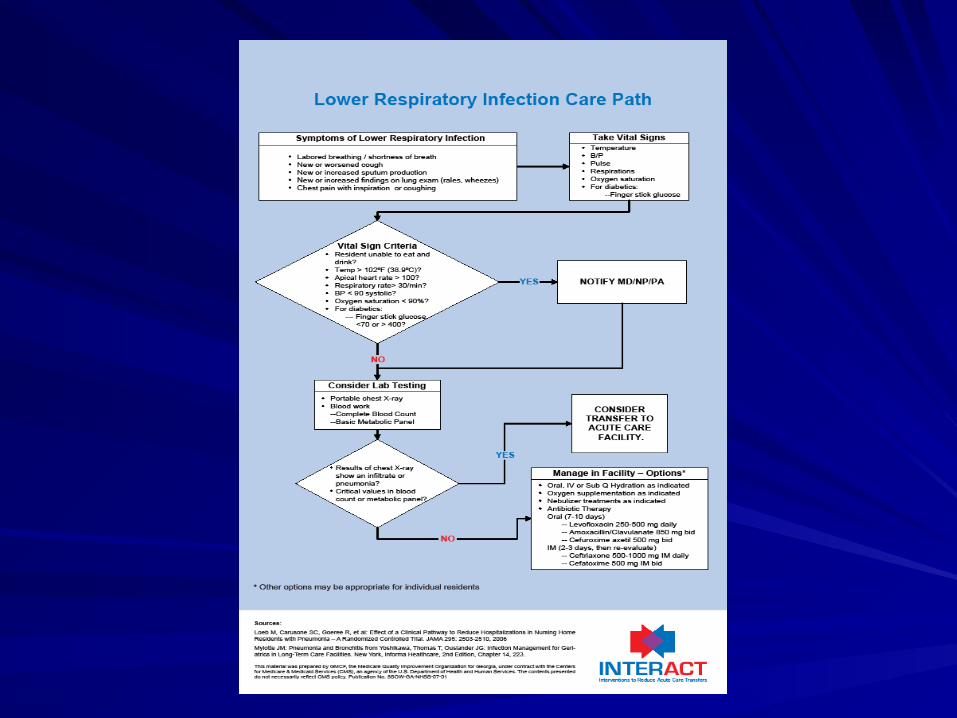
Clinical Care PathsClinical Care Paths
Advance Care Planning ToolsAdvance Care Planning Tools
Purpose Of ToolkitPurpose Of Toolkit
Aid in the early identification of a resident Aid in the early identification of a resident change of status change of status
Guide staff through a comprehensive resident Guide staff through a comprehensive resident assessment when a change has been identified assessment when a change has been identified
Improve documentation around resident change Improve documentation around resident change in condition in condition
Enhance communication with other health care Enhance communication with other health care providers about a resident change of status providers about a resident change of status
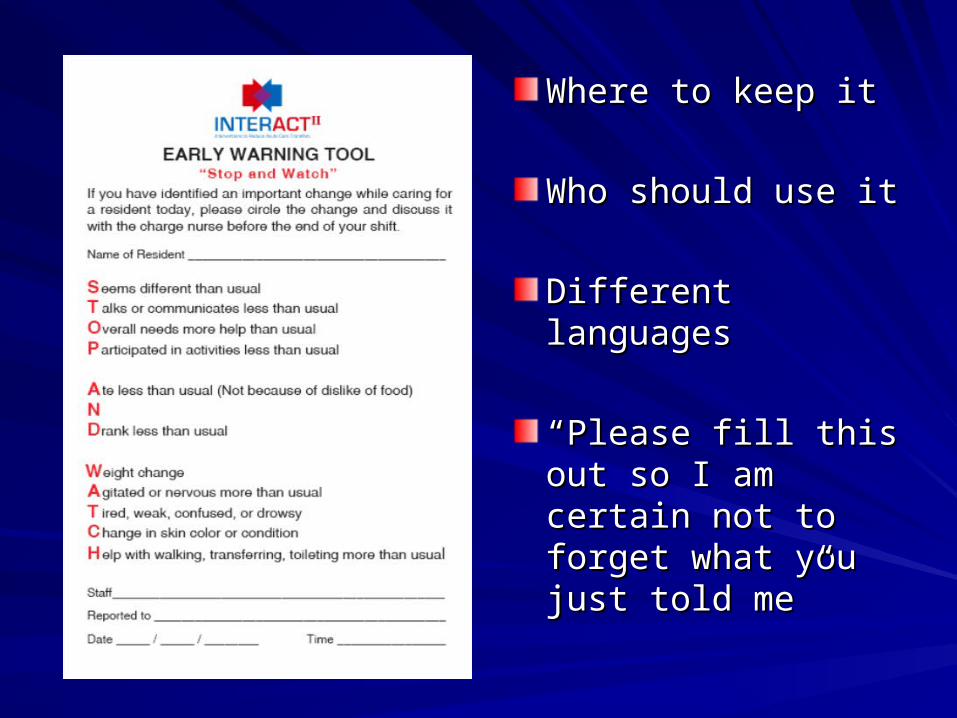
Where to keep itWhere to keep it
Who should use itWho should use it
Different languagesDifferent languages
““Please fill this out Please fill this out so I am certain not to so I am certain not to forget what you just forget what you just told me”told me”
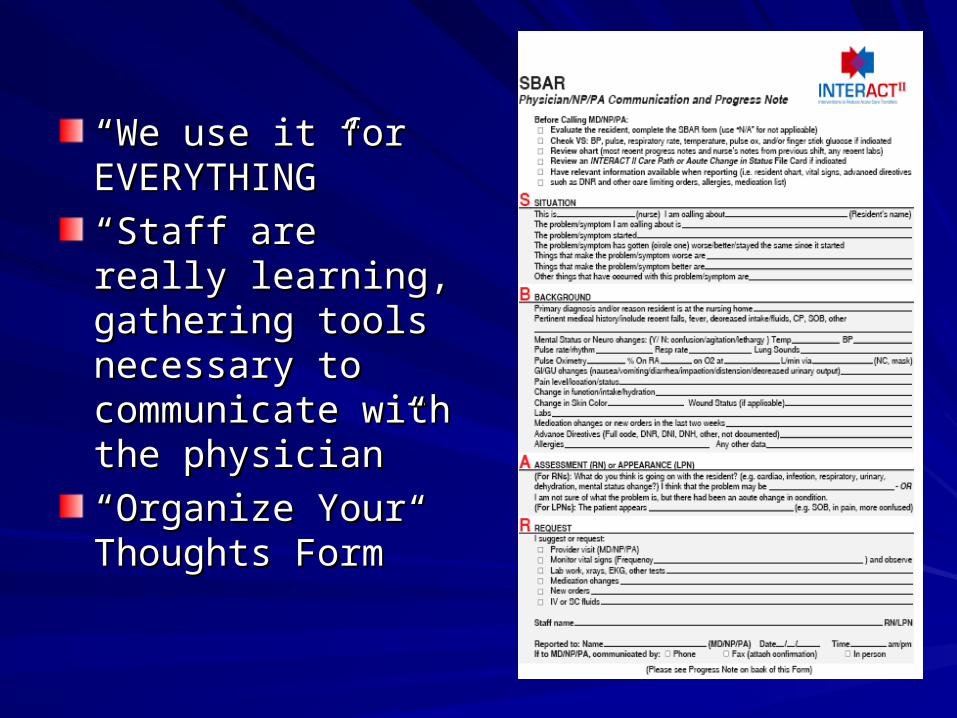
““We use it for We use it for EVERYTHING”EVERYTHING”
““Staff are really Staff are really learning, gathering learning, gathering tools necessary to tools necessary to communicate with the communicate with the physician”physician”
““Organize Your Organize Your Thoughts Form”Thoughts Form”
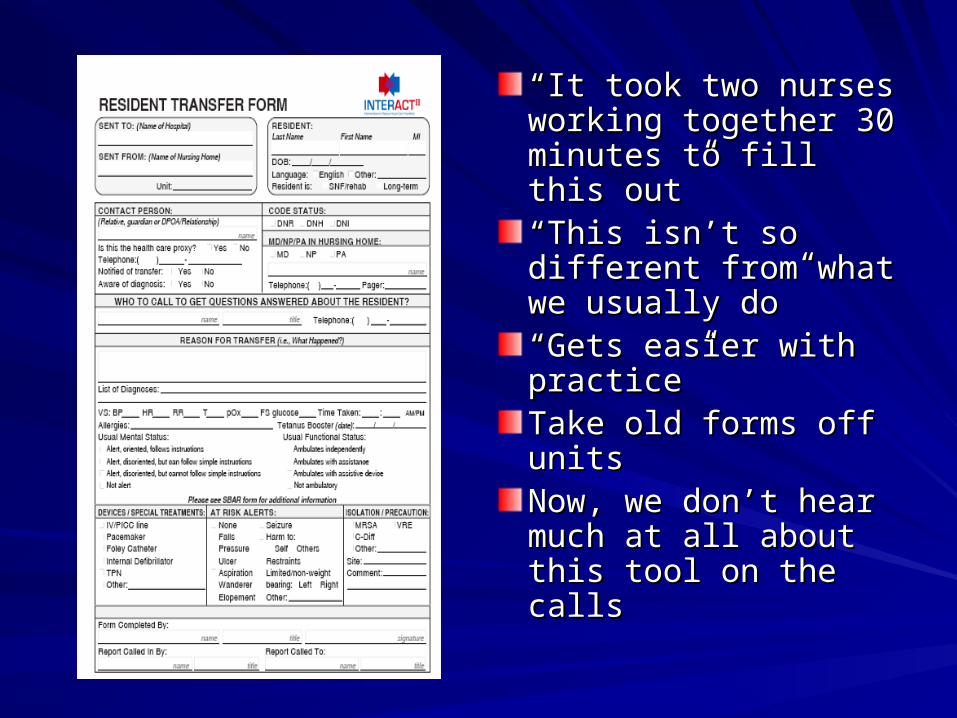
““It took two nurses It took two nurses working together 30 working together 30 minutes to fill this out”minutes to fill this out”““This isn’t so different This isn’t so different from what we usually from what we usually do”do”““Gets easier with Gets easier with practice”practice”Take old forms off Take old forms off unitsunitsNow, we don’t hear Now, we don’t hear much at all about this much at all about this tool on the callstool on the calls
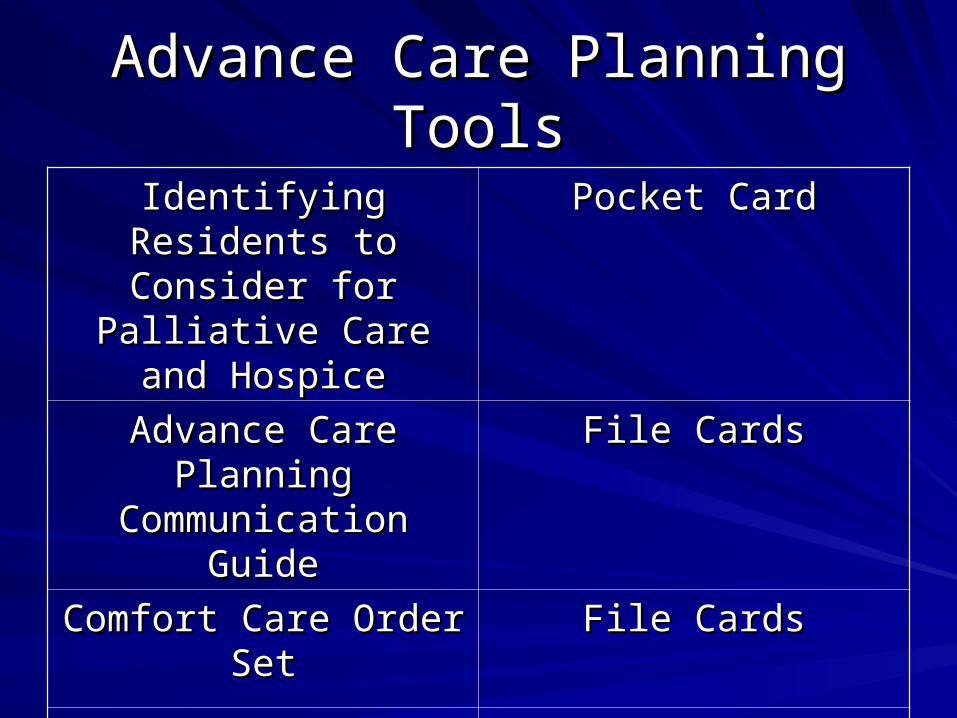
Advance Care Planning ToolsAdvance Care Planning Tools
Identifying Residents to Identifying Residents to Consider for Palliative Consider for Palliative
Care and HospiceCare and Hospice
Pocket CardPocket Card
Advance Care Planning Advance Care Planning Communication GuideCommunication Guide
File CardsFile Cards
Comfort Care Order SetComfort Care Order Set File CardsFile Cards
Educational Information Educational Information for Familiesfor Families
ReprintsReprints
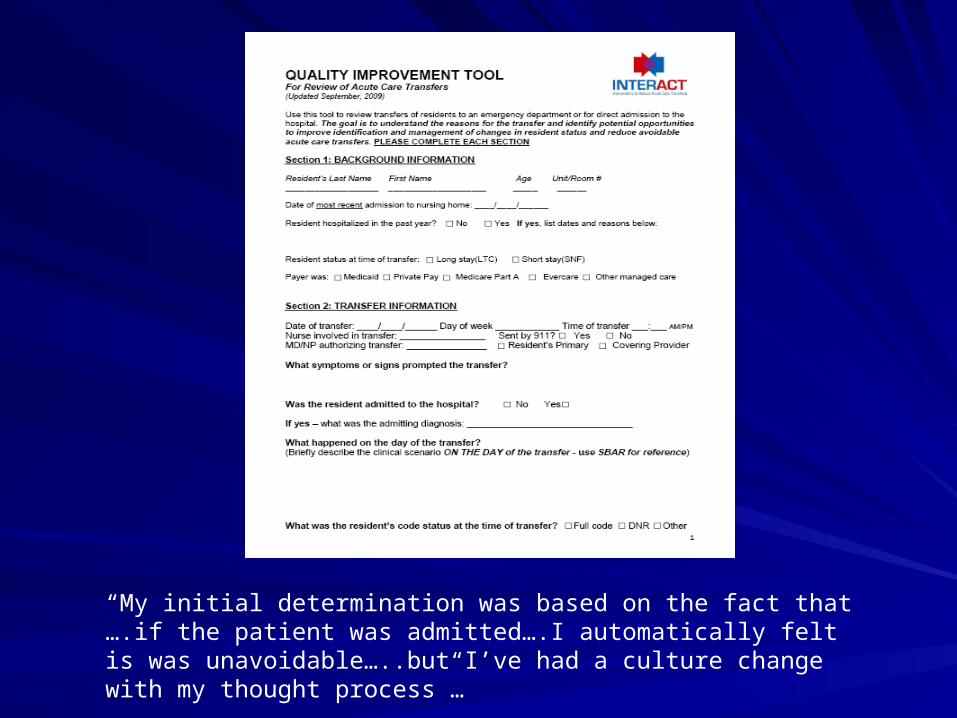
“My initial determination was based on the fact that ….if the patient was admitted….I automatically felt is was unavoidable…..but I’ve had a culture change with my thought process”…
Lessons so far….Lessons so far….
Leadership “buy in” is Leadership “buy in” is importantimportant
““This is great…we This is great…we would love to do this would love to do this at our facility”at our facility”
But…But…
The frontlines are where it happensThe frontlines are where it happens
The Champion is keyThe Champion is key
““I still think there is incredible I still think there is incredible value to this project and am value to this project and am going to keep working very going to keep working very hard on it”hard on it”
““I tell the staff to go out onto I tell the staff to go out onto the units and look for transfers the units and look for transfers waiting to happen”waiting to happen”
““I am going to elicit an alliance”I am going to elicit an alliance”
““I’m seeing it happen…walking I’m seeing it happen…walking on the units and seeing the on the units and seeing the nurses using the SBAR…it’s nurses using the SBAR…it’s great.” great.”
““Oh No! It’s Oh No! It’s Kryptonite!”Kryptonite!”
Relationships matterRelationships matter
““Our NP told me she couldn’t believe how much Our NP told me she couldn’t believe how much the nursing assessments have improved since the nursing assessments have improved since we started this”we started this”
““Does the ED staff know about this project? Does the ED staff know about this project? They keep calling to ask about the forms.”They keep calling to ask about the forms.”
““The EMT’s wouldn’t sign the envelope”The EMT’s wouldn’t sign the envelope”
““Does this mean they will be checking up on Does this mean they will be checking up on me?”me?”
““It’s all about teamwork”It’s all about teamwork”
Customizing the programCustomizing the program
NewsletterNewsletterGrand RoundsGrand RoundsMorbidity and Mortality RoundsMorbidity and Mortality RoundsNCR paper for Transfer FormsNCR paper for Transfer FormsTools part of new hire orientationTools part of new hire orientationScratch cards, free lunchScratch cards, free lunch““Its about more than just the tools. It’s Its about more than just the tools. It’s about culture and how you do business”about culture and how you do business”
For tomorrow:For tomorrow:www.interact.geriu.orgwww.interact.geriu.org
Getting StartedGetting Started– About INTERACT IIAbout INTERACT II– How to use the websiteHow to use the website– What is a champion and why do I need one?What is a champion and why do I need one?– All of the tools with instructions for eachAll of the tools with instructions for each
www.interact.geriu.orgwww.interact.geriu.org
ImplementationImplementation
– Deciding when and where to startDeciding when and where to start– Tips for training staffTips for training staff– Informing family members about INTERACT IIInforming family members about INTERACT II– Improving communication with the hospitalImproving communication with the hospital– Quality Improvement Review and feedbackQuality Improvement Review and feedback– Case StudiesCase Studies– How to download the whole toolkitHow to download the whole toolkit
FeedbackFeedback
Feedback on the trainingFeedback on the training
Team approach from the beginningTeam approach from the beginning
Frequent repeatsFrequent repeats
Small groupsSmall groups
1:11:1
Couple it with other initiativesCouple it with other initiatives– MOLST/POLSTMOLST/POLST– Consistent assignmentsConsistent assignments
Think aboutThink about
Processes/systems already in placeProcesses/systems already in place
Strengths/gapsStrengths/gaps
Other things going on in the buildingOther things going on in the building
How will you enlist front line supportHow will you enlist front line support
How you are going to track your dataHow you are going to track your data
THANK YOU!!!THANK YOU!!!