Embed Size (px)
DESCRIPTION
ppt
Citation preview
Interdisciplinary Approach in Periodontal
Therapy
CONTENTS
• Perio-Ortho• Perio-Prostho• Endo-Perio
Orthodontics and Periodontics
Management of periodontal conditions with
orthodontic tooth movement as an adjunct
AND
Management of periodontal problems
arising during and after orthodontic tooth
movement
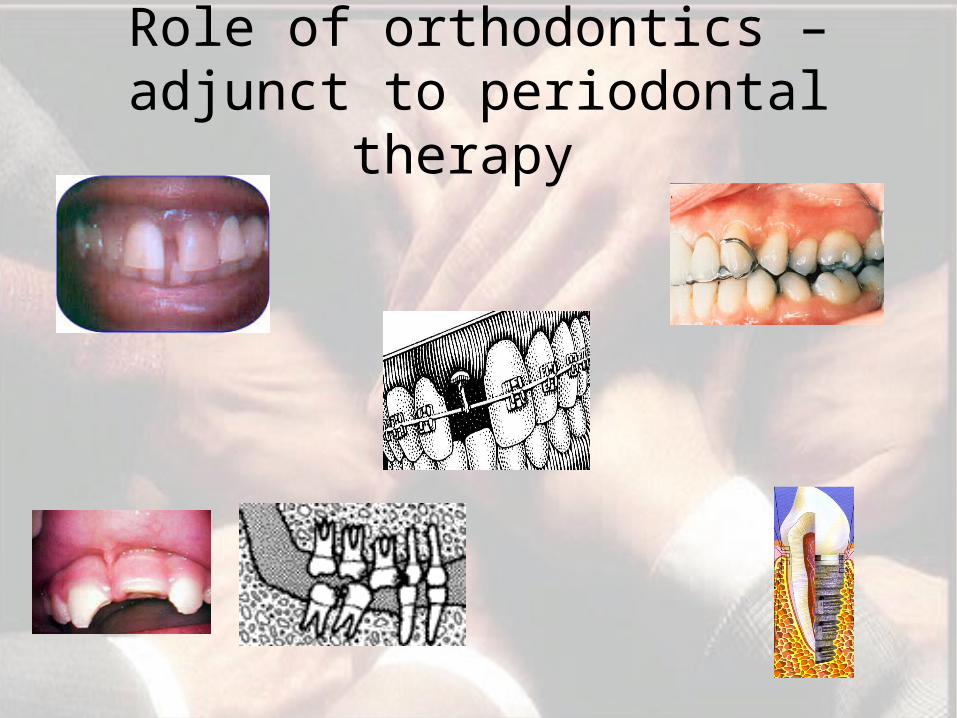
Role of orthodontics – adjunct to periodontal therapy
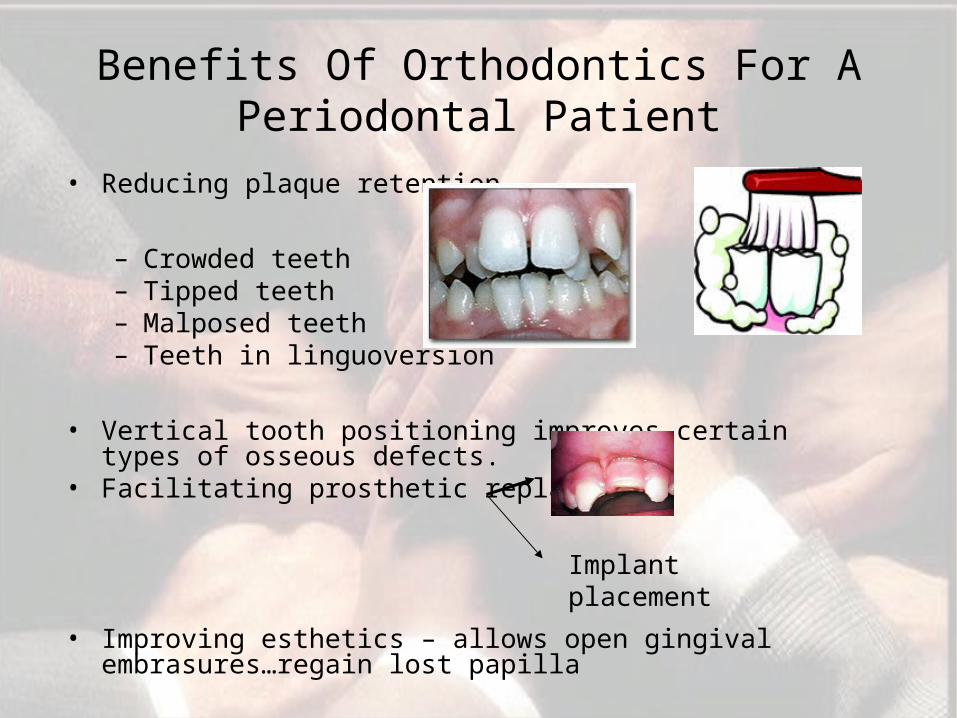
Benefits Of Orthodontics For A Periodontal Patient
• Reducing plaque retention
– Crowded teeth– Tipped teeth– Malposed teeth– Teeth in linguoversion
• Vertical tooth positioning improves certain types of osseous defects.
• Facilitating prosthetic replacements
• Improving esthetics – allows open gingival embrasures…regain lost papilla
Implant placement
•Inflammation
+
• Orthodontic forces
+
•Occlusal trauma
=
•Rapid destruction
(Kessler 1976)
Orthodontic tooth movement in adults with periodontal tissue breakdown.
Study by Artun & Urbye (1988)
Bone level measurements on radiographs indicated that the majority of sites showed little or no additional loss of bone support.
(Nelson & Arun 1997, Ree et al 2000)
• Pretreatment evidence of periodontal tissue destruction is no contraindication for orthodontics.
• Orthodontic therapy improves the possibilities of saving and restoring a deteriorated dentition.
• The risk of recurrence of an active disease process is not increased during appliance therapy.
Orthodontic Treatment Considerations
• Eliminate/reduce Plaque accumulation Gingival inflammation
• Fixed appliances
• Design of the appliance
Need to facilitate oral hygiene
• Bonded ceramic brackets
• Appliances & mechanics simple
• Avoid hooks, elastomeric rings, excess bonding resin
• Steel ligatures preferred over elastomeric rings ( Forsberg
et al 1991)
• Bonds preferable to bands
• Periodic professional tooth cleaning at 3 months interval
Possibilities and limitations
• Each individual treatment plan may depend on a variety of
factors and can be limited by biomechanical considerations
(force systems, limited anchorage), by periodontal risk factors
(tooth/alveolar bone topography, sinus recesses, activity and
prognosis of the periodontitis), and by limited patient motivation
and poor oral hygiene co-operation.
• Single case reports have documented successful periodontal-
orthodontic treatment with ( LAP) after conventional
periodontal therapy. However, until more evidence is
accumulated, it may seem wise to avoid orthodontic treatment in
patients with particularly ( GAP) forms of periodontal disease.
Orthodontic Treatment Of Osseous Defects
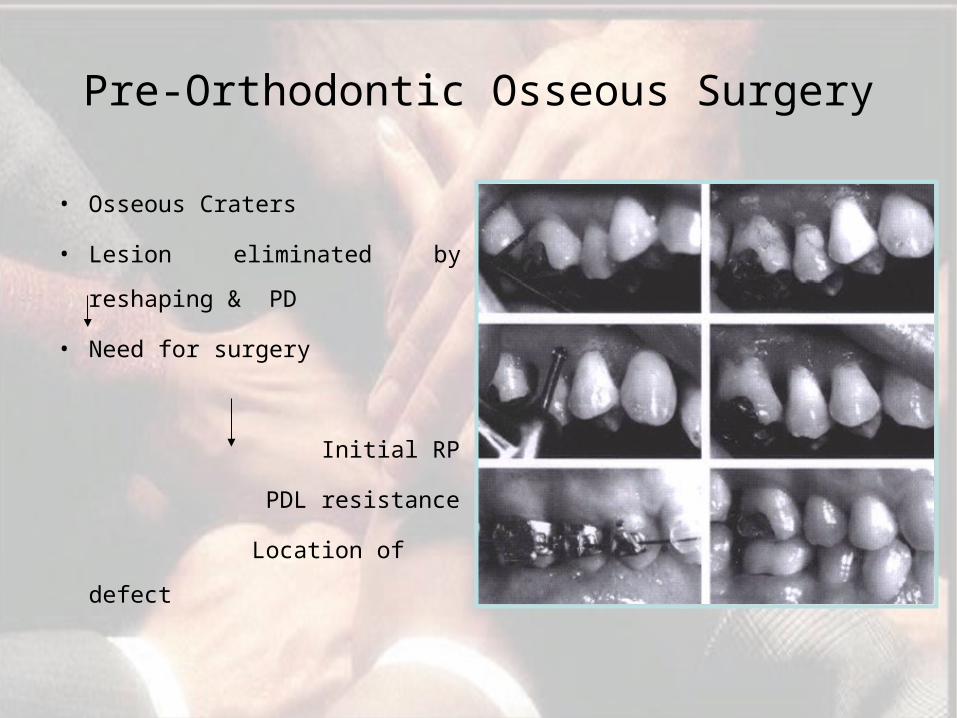
Pre-Orthodontic Osseous Surgery
• Osseous Craters
• Lesion eliminated by
reshaping & PD
• Need for surgery
Initial RP
PDL resistance
Location of defect
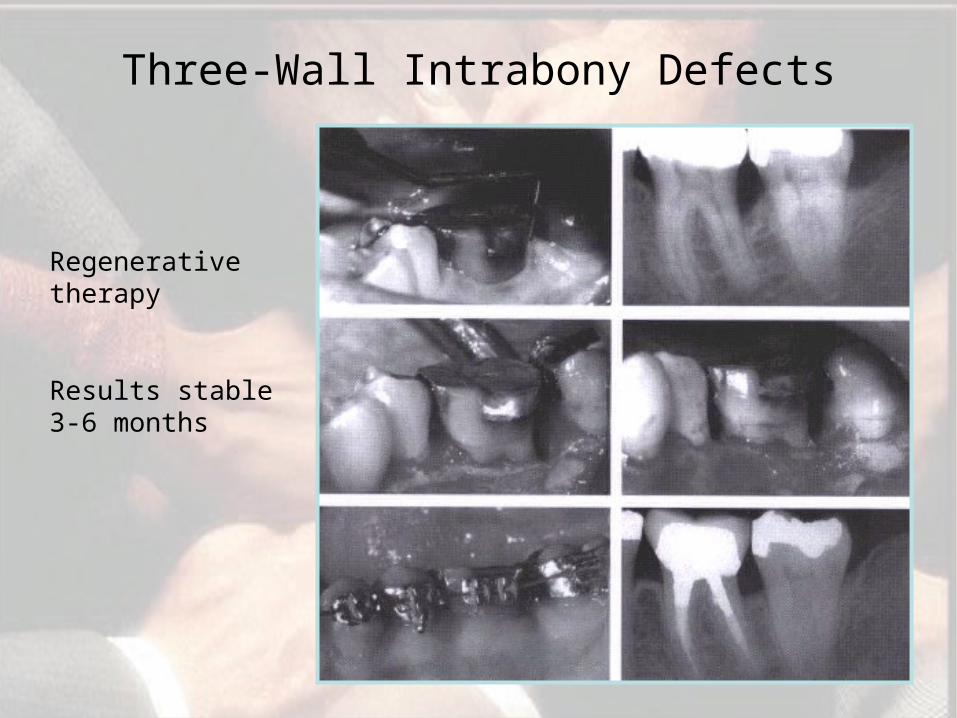
Three-Wall Intrabony Defects
Regenerative therapy
Results stable 3-6 months
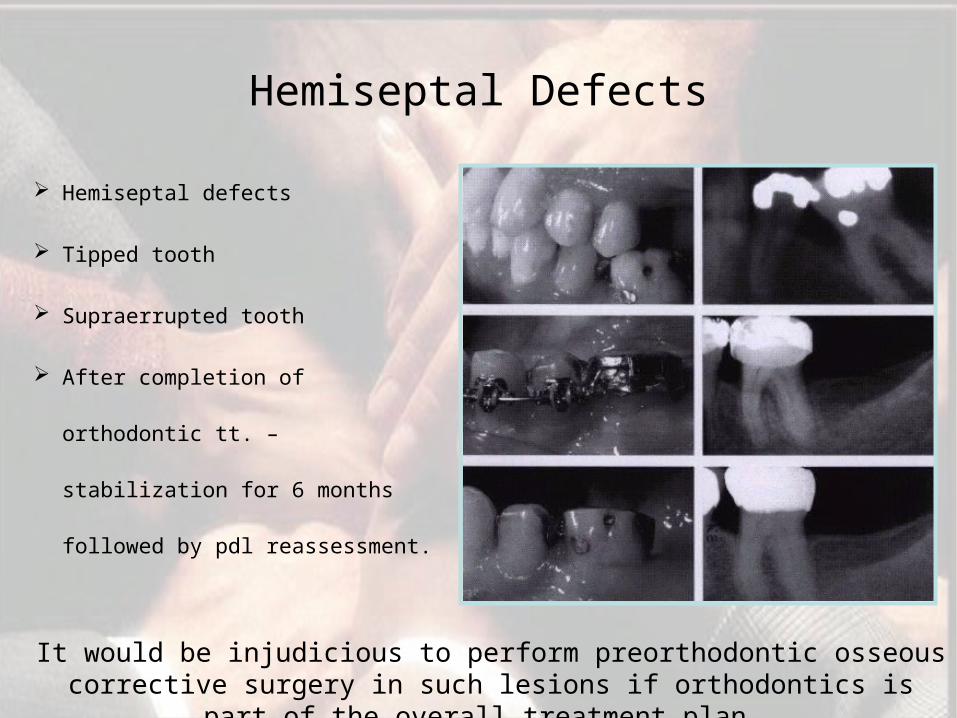
Hemiseptal defects
Tipped tooth
Supraerrupted tooth
After completion of orthodontic
tt. – stabilization for 6 months
followed by pdl reassessment.
Hemiseptal Defects
It would be injudicious to perform preorthodontic osseous corrective surgery in such lesions if orthodontics is part of the
overall treatment plan.
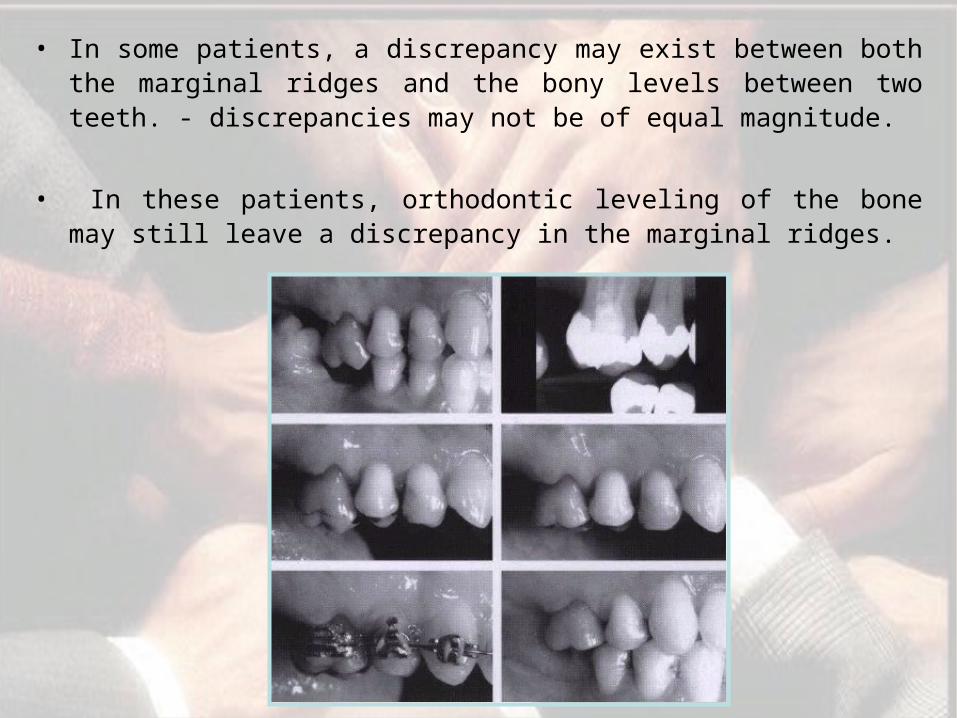
• In some patients, a discrepancy may exist between both the marginal ridges and the bony levels between two teeth. - discrepancies may not be of equal magnitude.
• In these patients, orthodontic leveling of the bone may still leave a discrepancy in the marginal ridges.
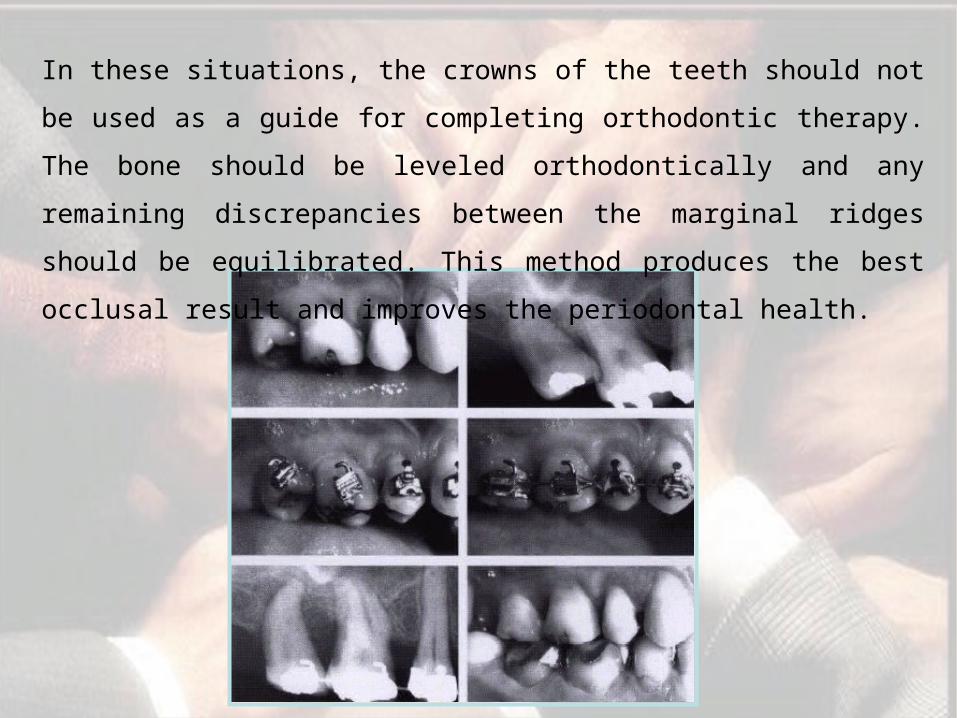
In these situations, the crowns of the teeth should not be used
as a guide for completing orthodontic therapy. The bone should
be leveled orthodontically and any remaining discrepancies
between the marginal ridges should be equilibrated. This
method produces the best occlusal result and improves the
periodontal health.
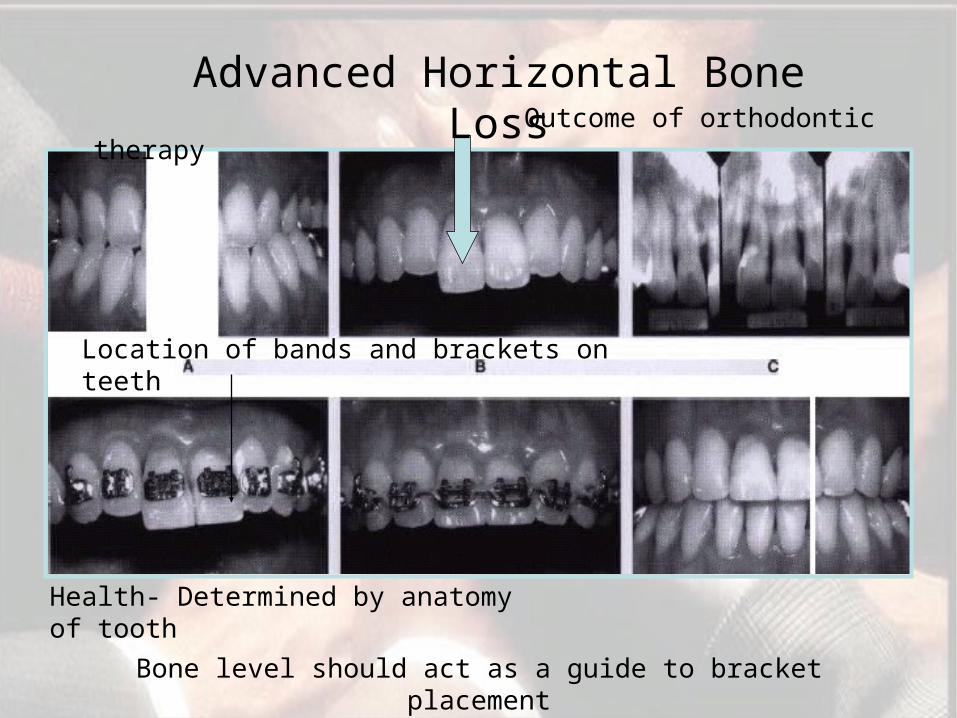
Outcome of orthodontic therapy
Location of bands and brackets on teeth
Health- Determined by anatomy of tooth
Advanced Horizontal Bone Loss
Bone level should act as a guide to bracket placement
Molar Uprighting
Tipped molars- a causative/aggravating factor future periodontal tissue breakdown
Indications-functionally disturbing interferences, paralleling or space problems associated with prosthetic rehabilitation, or traumatic occlusion.
It causes a shallowing-out of the angular defect, with new bone forming at the mesial alveolar crest
When there is a definite osseous defect caused by periodontitis on the mesial surface of the inclined molar, uprighting the tooth and tipping it distally will widen the osseous defect.
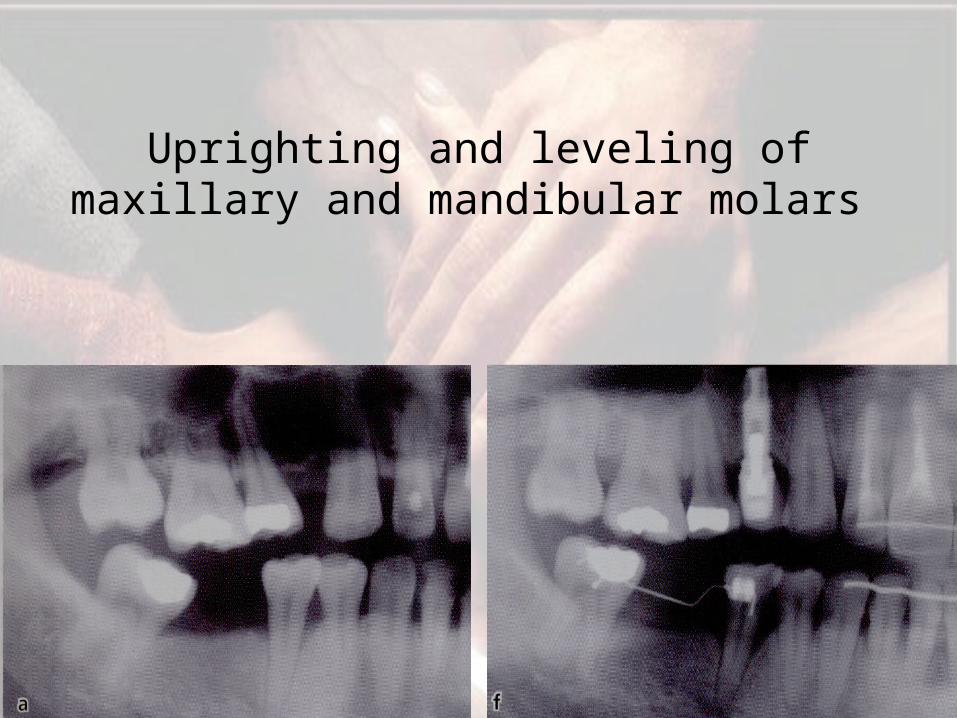
Uprighting and leveling of maxillary and mandibular molars
Furcation Defects
Require special attention..
Bands with tubes & other attachments impede patient's access to
buccal furcation for home care & instrumentation at the time of
recall.
If a patient with a Class III furcation defect will be undergoing
orthodontic treatment, a possible method for treating the furcation
is to eliminate it by hemisecting the crown and root of the tooth.
However, this procedure requires endodontic, periodontal, and
restorative treatment.
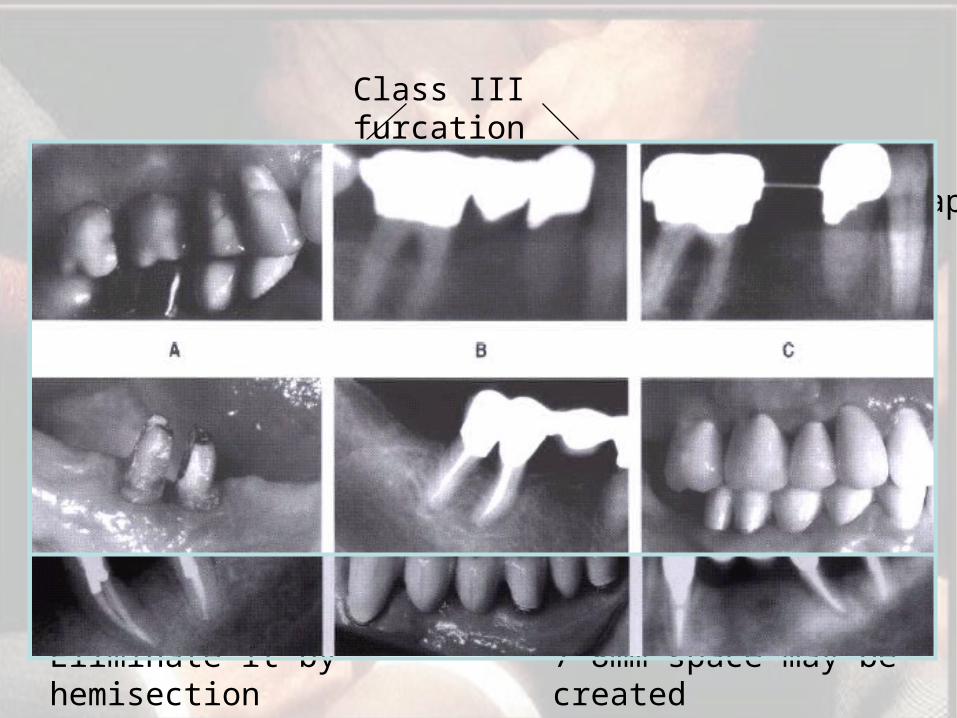
Class III furcation
Orthodontic therapy
Eliminate it by hemisection
If roots not to be moved apart
2 to 3 months recall visits
Endodontic therapy
If roots need to be moved apart
Do hemisection pre Ortho
Place brackets on roots and coil springs to seperate
Size of eden. space and occlusion
7-8mm space may be created
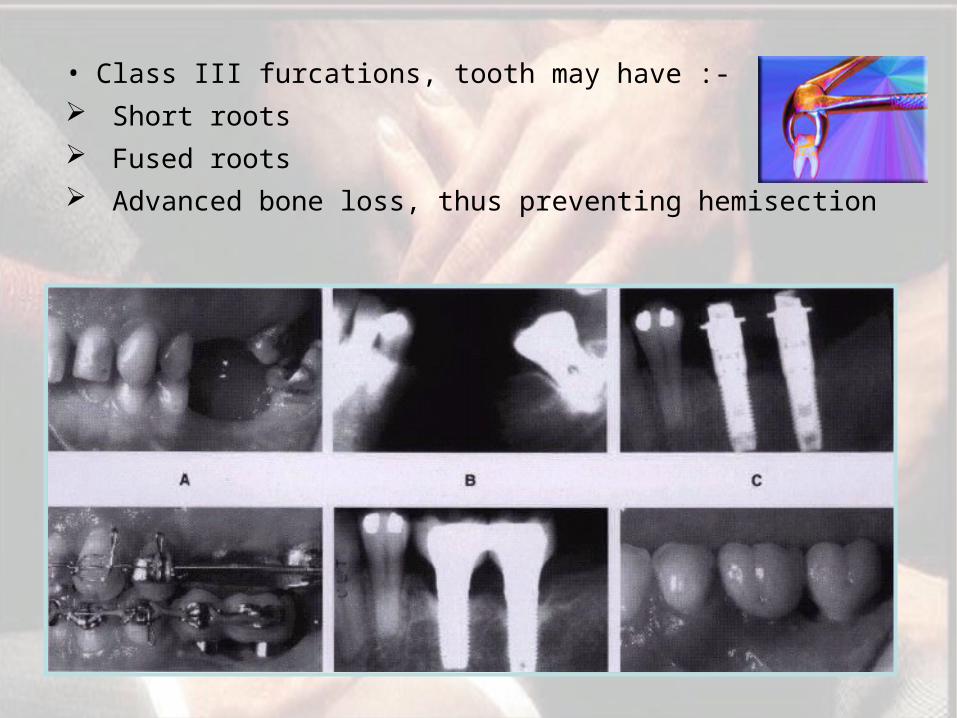
• Class III furcations, tooth may have :-
Short roots
Fused roots
Advanced bone loss, thus preventing hemisection
• Extract the root and place implant
• Implant can act as anchor to facilitate prerestorative
orthodontic therapy.
• 4-6 months after placement
• If not acting as an anchor – can be placed after orthodontic
therapy

Fractured Teeth/ Forced Eruption
Root length –crown-root ratio – 1:1
Root form – broad & non tapering , root canal should not be
more than one third.
Level of fracture
Relative importance of tooth
Esthetics – high lip line
Endo-perio prognosis
Orthodontic considerations:-
Mechanics can vary from elastic traction to banding and
bracketing.
Root may be erupted – slowly or rapidly
Criteria
Orthodontic Treatment Of Gingival Discrepancies
Gingival margin discrepancies
Abrasion of incisal edges
Delayed migration of gingival margins
Can be corrected
Orthodontically Surgically
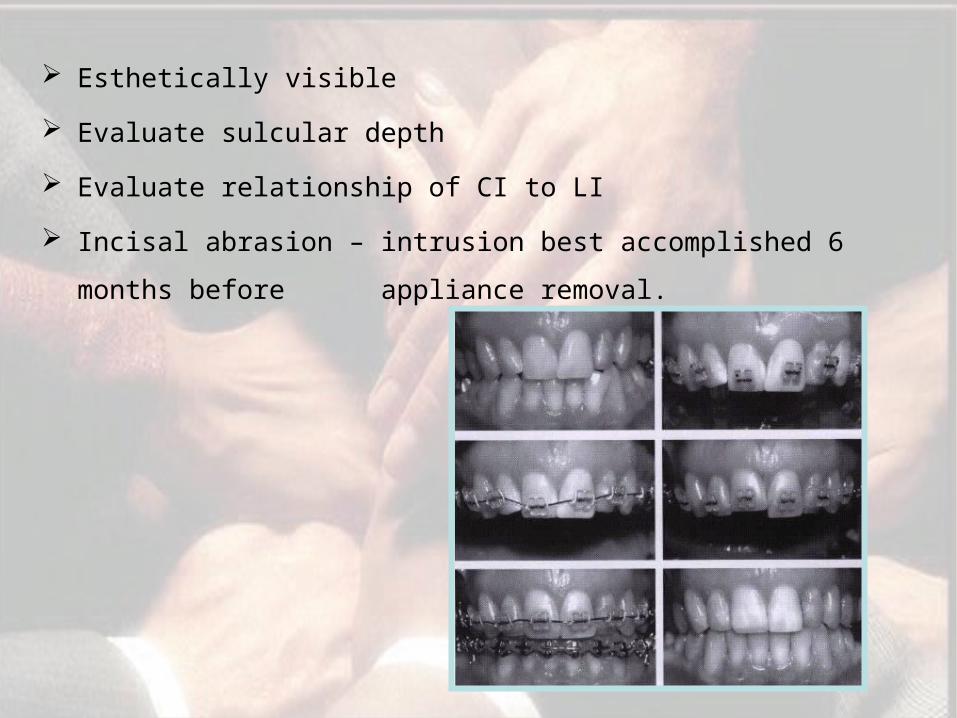
Esthetically visible
Evaluate sulcular depth
Evaluate relationship of CI to LI
Incisal abrasion – intrusion best accomplished 6 months
before appliance removal.
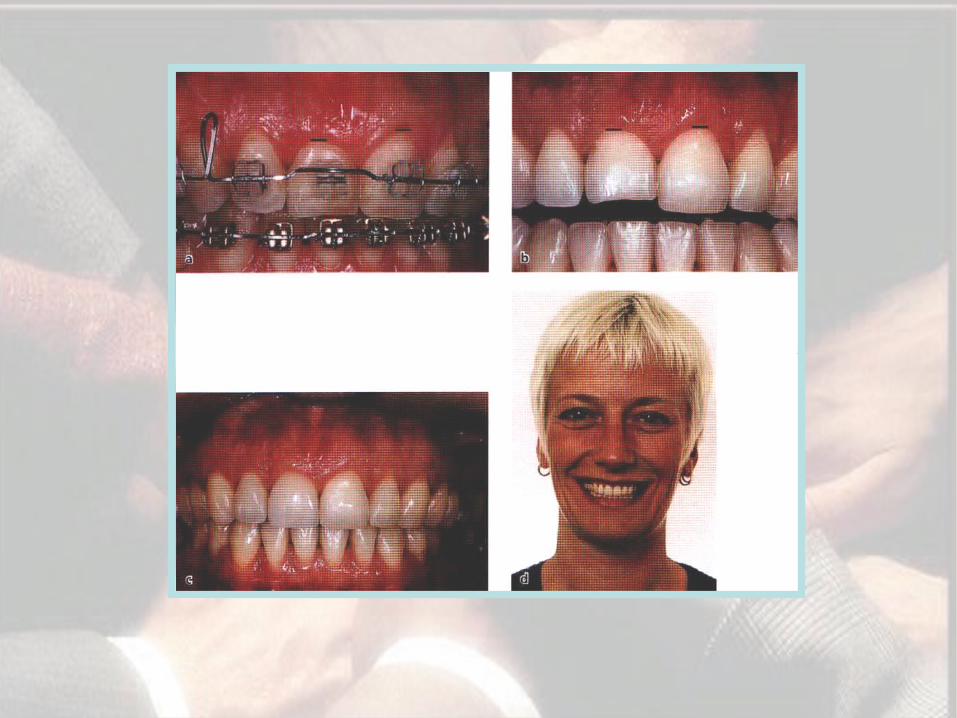
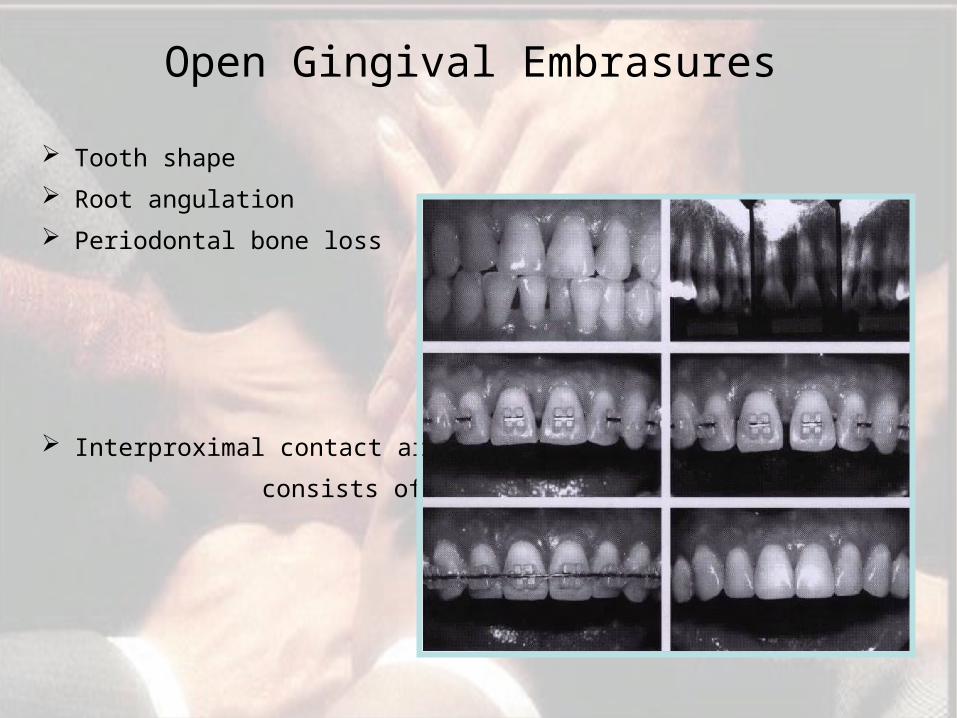
Open Gingival Embrasures
Tooth shape
Root angulation
Periodontal bone loss
Interproximal contact area
consists of two parts..
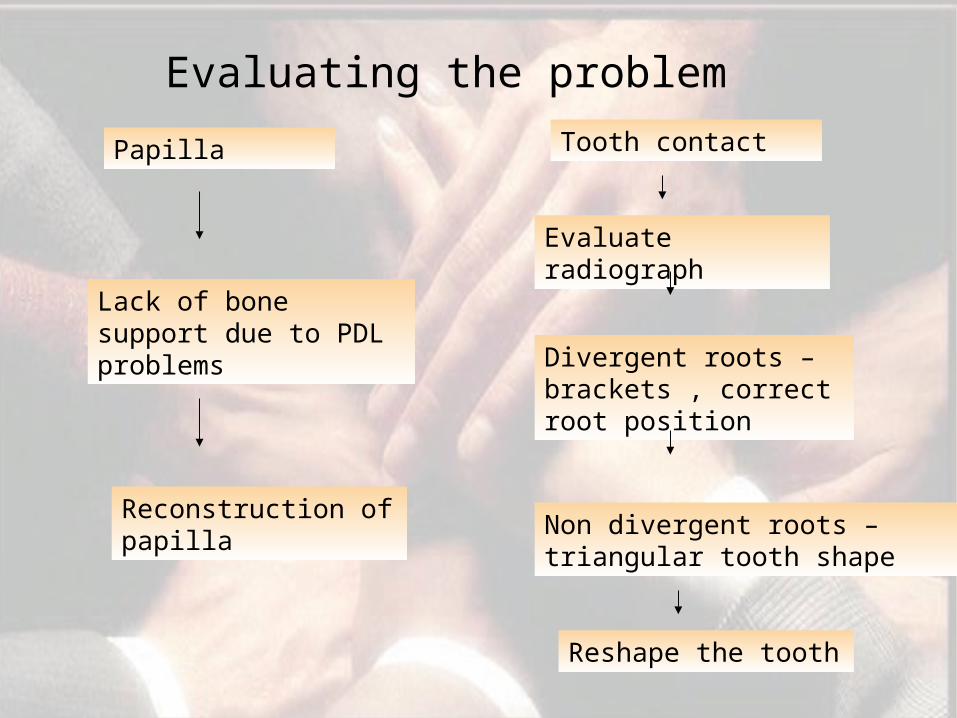
Evaluating the problem
Papilla
Lack of bone support due to PDL problems
Reconstruction of papilla
Tooth contact
Evaluate radiograph
Divergent roots – brackets , correct root position
Non divergent roots – triangular tooth shape
Reshape the tooth

Elimination of unesthetic soft tissue gaps
The problems that may arise during or after orthodontic therapy are
grouped as follows :-
Associated with orthodontic bands.
Associated with excessive orthodontic force.
Orthodontic relapse.
Difficulty in tooth movement.
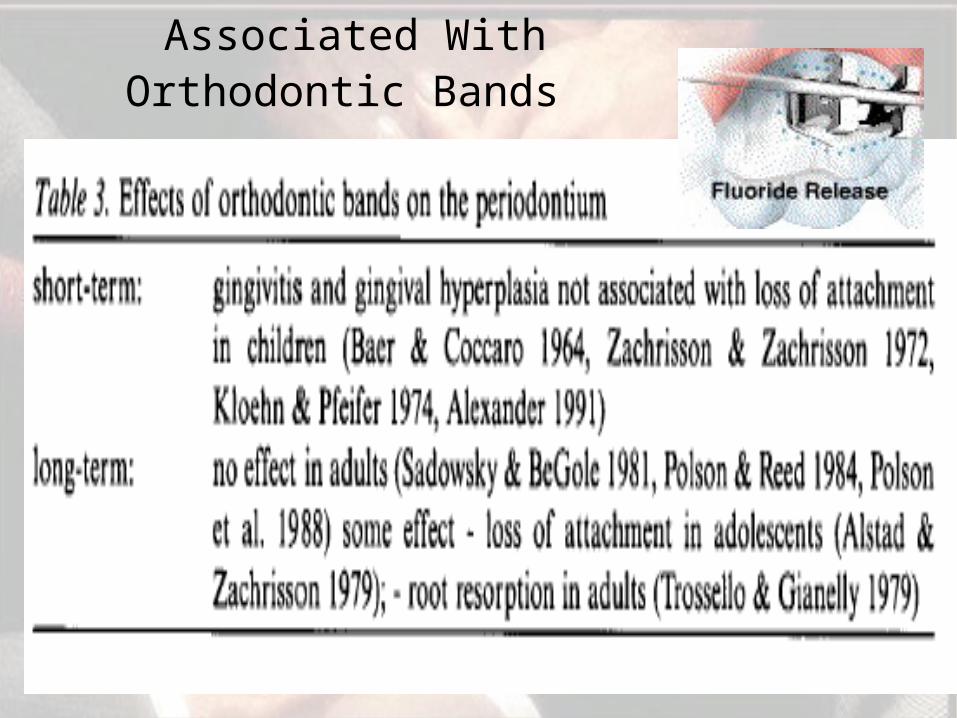
Associated With Orthodontic Bands
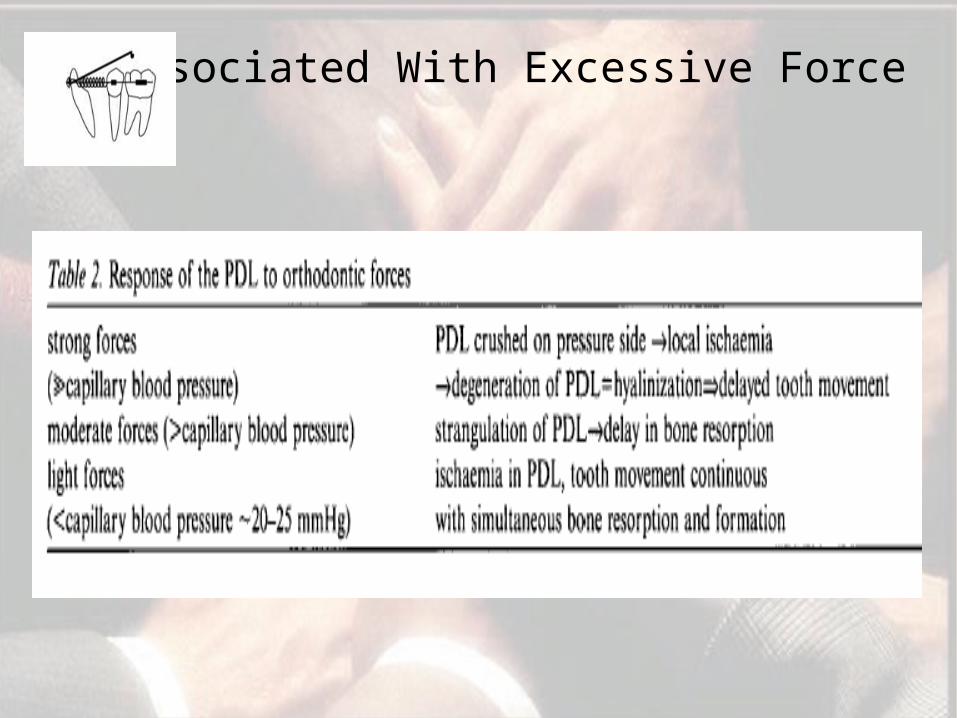
Associated With Excessive Force
ORTHODONTIC RELAPSE
• When teeth are moved to a new position these fibers stretch and they remodel very slowly.
• The pull of these fibers tend to revert the teeth to their old positions.
• If the supracrestal fibers are sectioned (i.e. by circumferential supracrestal fibrotomy CSF) and allowed to heal while the teeth are held in the proper position, relapse caused by gingival elasticity is reduced.
Reorganization of collagen & elastic supracrestal gingival fibers
Reiten (1969) reported that most relapse following
orthodontic tooth movement occurred during the first five
hours after the appliance was removed hence it is advisable
to do the fiberotomy procedure few weeks before the
removal of appliance.
Several clinical and histologic investigations indicate that the
major relapse pull on a rotated tooth appears to be in the
supracrestal fibers.
Difficulties In Orthodontics Tooth Movement
• Age is not a contraindication to orthodontic treatment.
• With increasing age cellular activity decreases and the tissue
becomes richer in collagens.
• In the elderly, the tissue response to orthodontic forces
including both cell mobilization and conversion of collagen
fibers is much slower than in children and teenagers.
• In adults, hyalinized zones are formed more easily on the
pressure side of an orthodontically moved tooth and these
zones may temporarily prevent the tooth from moving in the
intended direction.
• Since the growth in adults is completed, it is not possible by
orthodontic measures to influence zone of growth and
therefore treatment in adult individuals is restricted to different
types of tooth alignment.
• It is far more difficult for an adult individual to adopt to an
orthodontic appliance than for a child.
• Phonetic adjustment to a removable appliance for instance,
generally require more time in an adult.
• A fixed appliance is usually better tolerated by adult patient.
Frenum Considerations
• Many- frenum prevents mesial migration of maxillary CI.
• Others- removal of frenum allows space to be closed
orthodontically
• Generally , removal of frenum should be delayed until after
orthodontic therapy, unless tissue becomes painful or
prevents space closure, to change irreversible hyperplastic
tissue to normal gingival form & to enhance post
treatment stability.
The Role Of Implants In Orthodontics
• Implants as a source of absolute anchorage
• Implants used for anchorage and as abutments for
restorations
• Implant site preparation improved by orthodontics
• Implants in osteogenic distraction.
Time Relationship between Orthodontic
& Periodontal Therapy
• It is generally recommended that orthodontics be preceded by PDL therapy based on the belief that orthodontics in the presence of inflammation can lead to rapid and irreversible breakdown of the periodontium (Lindhe et al. 1974).
• SRP (if necessary, by open flap debridement procedures for access) & gingival augmentation should be performed as appropriate before any tooth movement (Glickman 1964, Prichard 1965, Profflt 1993d).
• The corrective phase of periodontal therapy, i.e., osseous or pocket reduction/ elimination surgery ought to be delayed until the end of orthodontic therapy, because tooth movement may modify gingival and osseous morphology (Goldman & Cohen 1968).
Periodontal Restorative Interrelationship
• Active pdl disease …………
• Restorative dentistry performed on ….
• Implant dentistry ………….
Prep of periodontium for restorative dentistry
• Shrinkage of tissue – helps in locating ideal gingival margin …..
• Position of teeth altered in PDL disease- injurious tension &
pressure
• Impairment of functional demands
• Impressions made from inflamed gingiva – improper fit
• Mobility & pain – interferes with
masticaton & function
• Aim is not only to eliminate periodontal pockets and restore gingival
health.
• Treatment should also create the gingivomucosal environment &
osseous topography necessary for the proper function of prosthesis.
• Control of active dental disease
• Higher quality
• Pocket. – Ulceration , edema, vascularity
• Return of healthy state in 2 weeks
• Thus plaque control, calculus removal and the removal or
correction of any inadequate dental restorations in the
gingival environment should be initial procedures.
Phase I Therapy
Management of Mucogingival Problems
It often is necessary to carry out a free soft tissue autograft in the patient who has a mucogingival defect and requires a dental restoration in the immediate environment of the gingiva.
Should be carried out at least 2 months before placement of the dental restorations - allows time for mature tissue to form
Augmentation of keratinized gingiva provides stability of the free gingival margin and surrounding gingival tissues so that the dental restoration can be placed in an environment in which gingival health can be maintained.
Techniques to increase the width of attached gingiva
1.Free gingival autografts
2.Apically positioned flap
3.Free connective tissue autograft
4.Pedicle grafts:
laterally displaced
coronally displaced
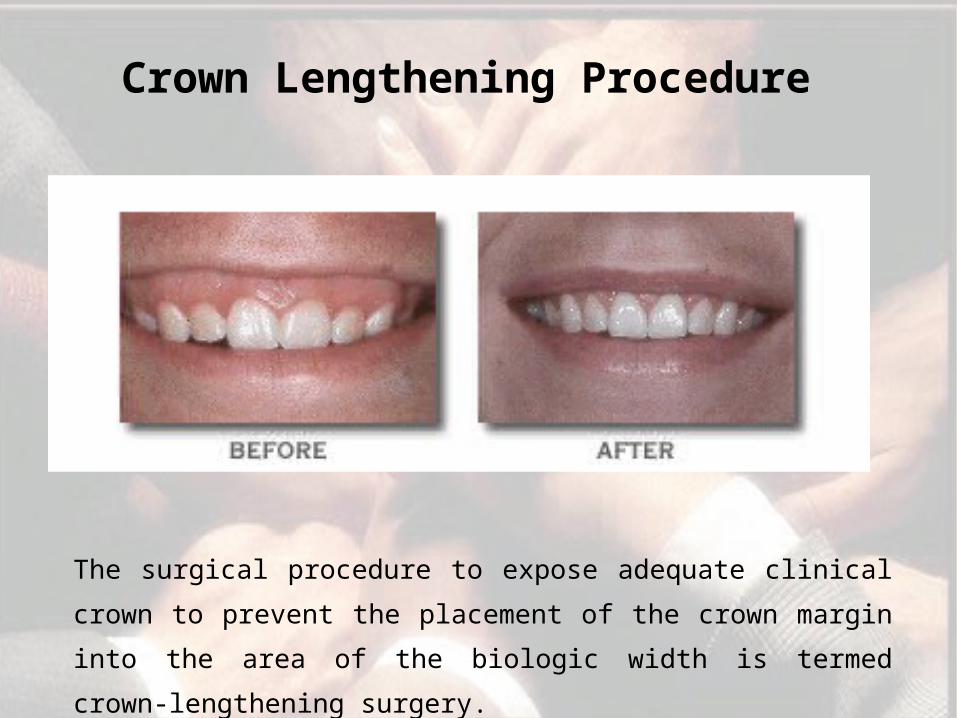
Crown Lengthening Procedure
The surgical procedure to expose adequate clinical crown
to prevent the placement of the crown margin into the area
of the biologic width is termed crown-lengthening surgery.
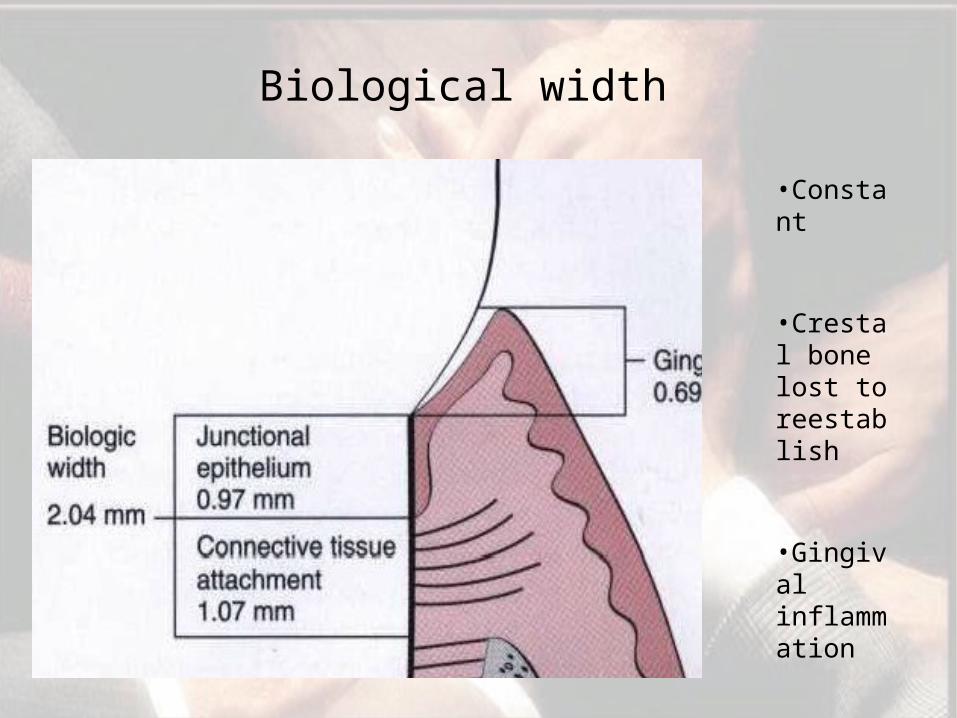
Biological width
•Constant
•Crestal bone lost to reestablish
•Gingival inflammation
•Pocket formation

Gingivectomy
Crown lenthening procedure
• It is essential that there be at least 3 mm between the most apical extension of the restoration margin and the alveolar bone crest.
• This space allows sufficient room for the supracrestal collagen fibers that are part of the periodontal support mechanism, as well as providing a gingival crevice of 2 to 3 mm.
• If this guideline is used, the margin of the crown is finally positioned at its correct level, approximately halfway down the gingival crevice.
• Failure to allow sufficient space between the crown margin and the alveolar crest height means that the finished restoration is positioned deep in the periodontal tissues and results in increased inflammation and pocket formation.
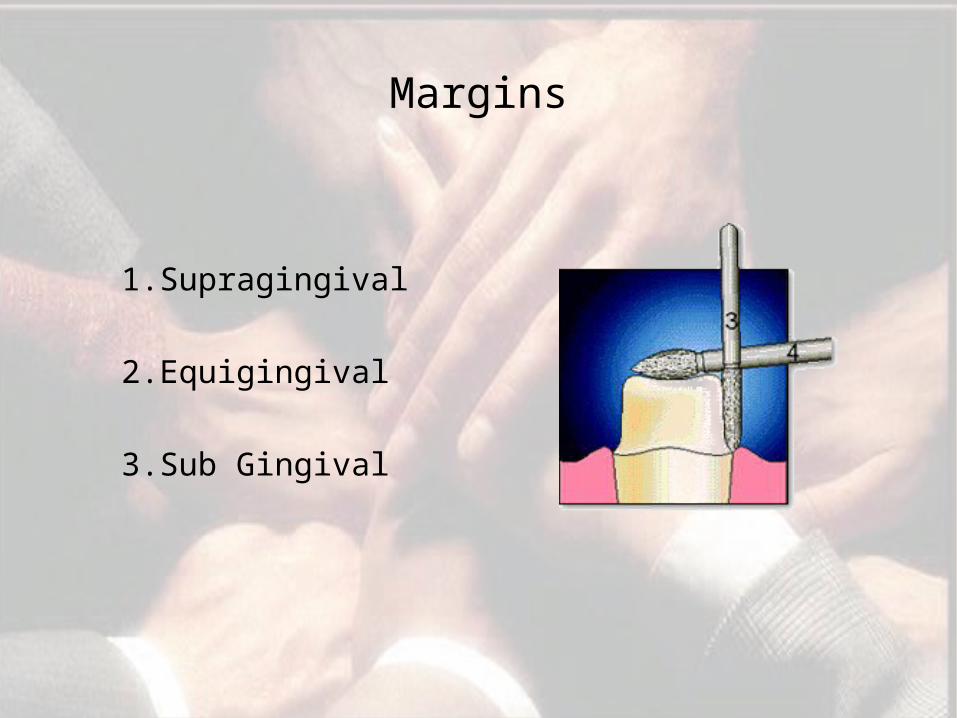
Margins
1.Supragingival
2.Equigingival
3.Sub Gingival

• Least Impact On Periodontium• Applied In Non Esthetic Areas
Supra Gingival
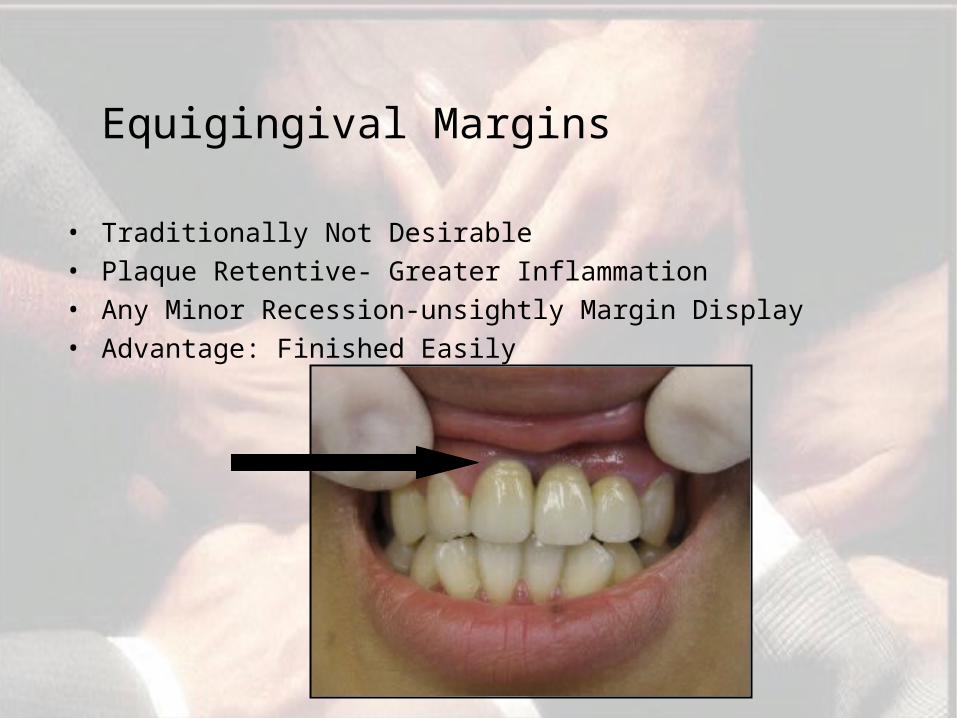
Equigingival Margins
• Traditionally Not Desirable• Plaque Retentive- Greater Inflammation• Any Minor Recession-unsightly Margin Display• Advantage: Finished Easily
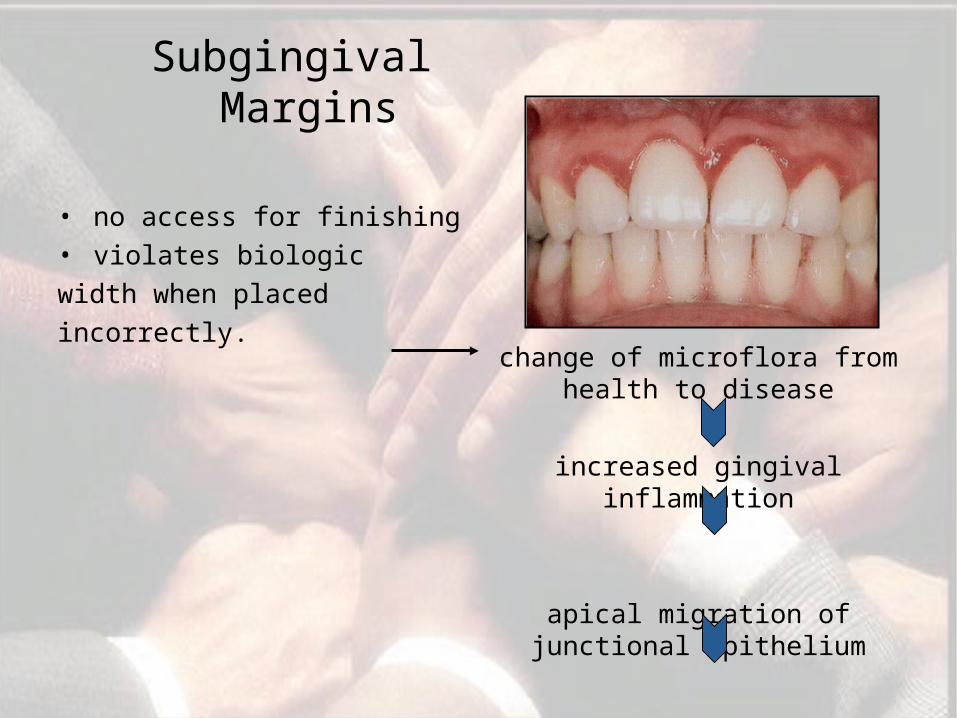
Subgingival Margins
• no access for finishing• violates biologicwidth when placedincorrectly.
change of microflora from health to disease
increased gingival inflammation
apical migration of junctional epithelium
bone loss
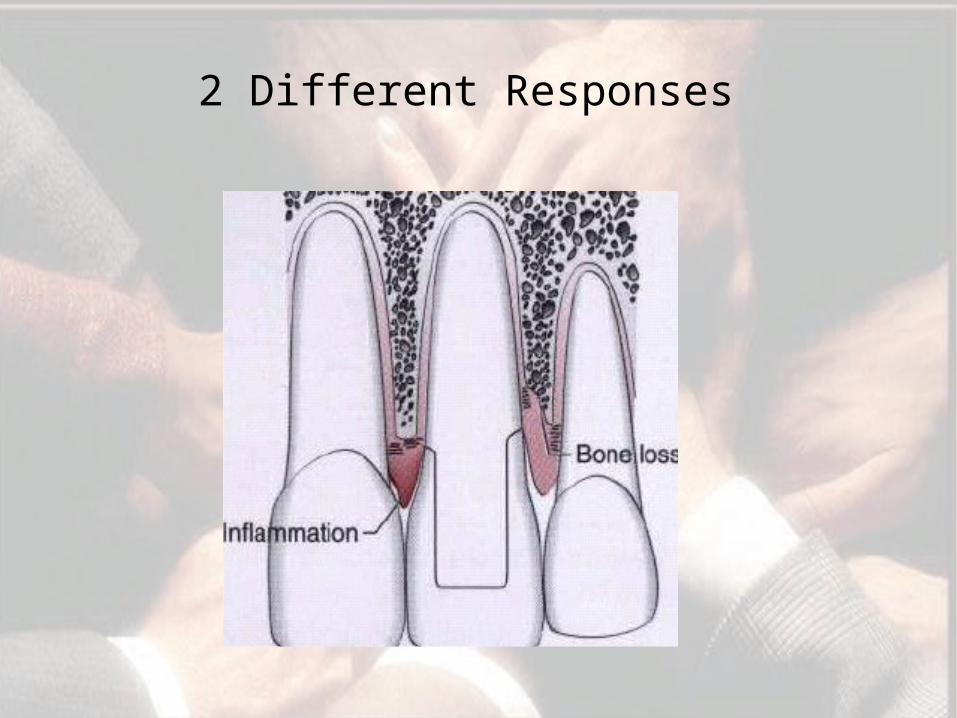
2 Different Responses
Supragingival/Subgingival Margins
• Guy.M.Newcomb (1974 )“The relationship between the location of subgingival crown margins and gingival inflammation” and concluded that the nearer a subgingival crown margin approaches the base of the gingival crevice, the more likely its that severe inflammation will occur.
• D.A.Orkin and D. Bradshaw (1987) conducted a study on the “Relationship of the positions of crown margins to gingival health” and showed that gingival tissues tend to bleed 2.42 times more frequently with subgingival margins and have 2.65 times higher chance of gingival recession
• D.A.Felton (1991) “Effects of in vivo crown margin discrepancies on the periodontal health” in his study he strongly supported the placement of supragingival margins for artificial crowns and FPD’s.
• William.G.Reeves in his review article concluded that more supragingivally a restorative margin is placed, the less chance that the margin will contribute to gingival inflammation.
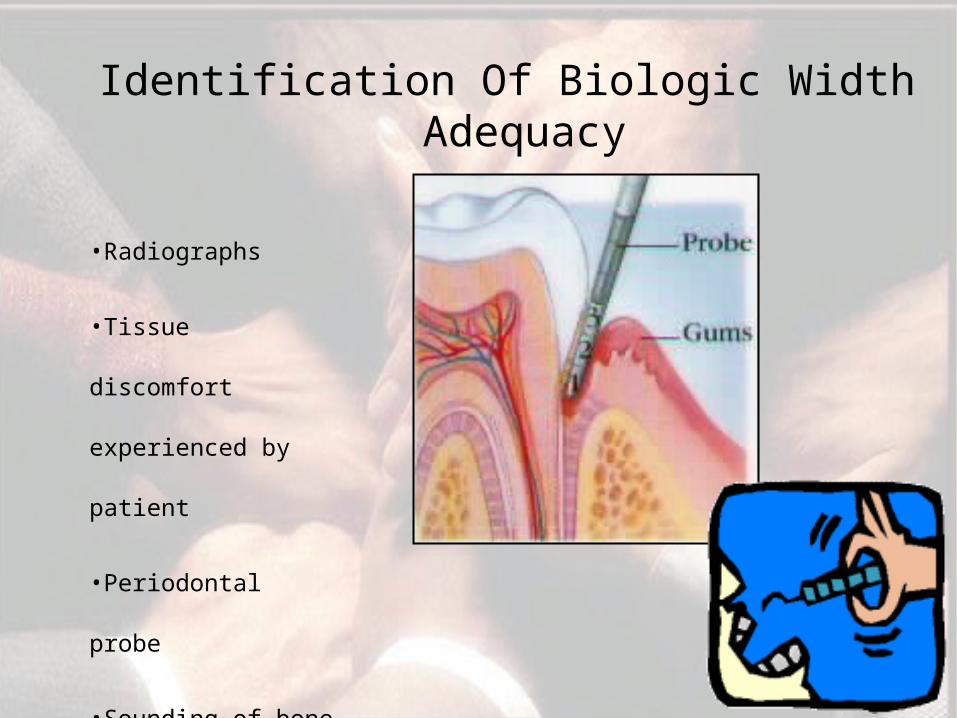
Identification Of Biologic Width Adequacy
•Radiographs
•Tissue discomfort
experienced by patient
•Periodontal probe
•Sounding of bone
In 1994, Vacek et al investigated the biologic width phenomenon. Although their average width finding of 2 mm was the same as that previously presented by Gargiulo et al, they also reported a range of different, patient-specific biologic widths.
They reported biologic widths as narrow as 0.75 mm in some individuals, whereas others had biologic widths as tall as 4.3 mm.
• Dictates that specific biologic width assessment should be performed for each patient for restorations to be in harmony with their gingival tissues.

Biological Width Violations
Gingival Inflammation
Gingival Inflammation
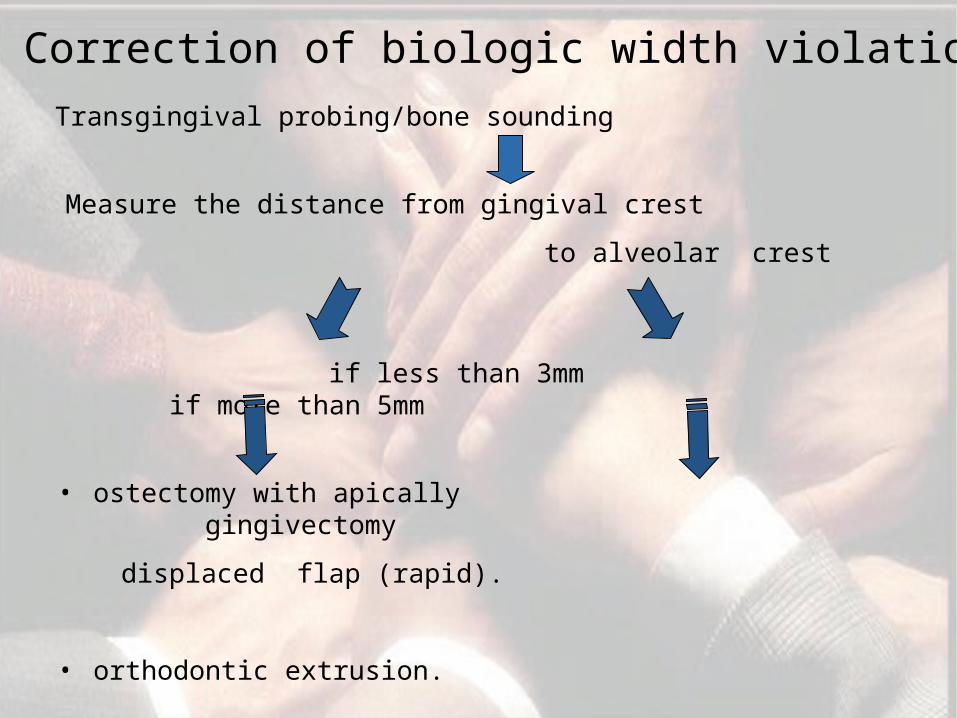
Correction of biologic width violation
Transgingival probing/bone sounding
Measure the distance from gingival crest
to alveolar crest
if less than 3mm if more than 5mm
• ostectomy with apically gingivectomy
displaced flap (rapid).
• orthodontic extrusion.
Tissue Retraction
In this process, the tissue must be protected from abrasion,
which will cause hemorrhage and can adversely affect the
stability of the tissue level around the tooth.
During final impression making , a clean, fluid controlled
environment is desired. Tissue management is achieved
with gingival retraction cords, using the appropriate size to
achieve the displacement required.
Thin, fragile gingival tissues and shallow sulcus - smaller
diameter cords be chosen to achieve the desired tissue
displacement.
• Journal of Prosthodontics, Vol 15, No 2 ( March-April), 2006: pp 108-112
Gingival retraction causes an acute injury that heals clinically in 2 weeks as is indicated by the GI.
It also provides the first evidence that gingival retraction results in an elevation of the proinflammatory cytokine, TNF-α, in GCF.
Marginal fit
• Marginal fit - producing an inflammatory response in the periodontium.
• It has been shown that the level of gingival inflammation can increase, corresponding with the level of marginal opening.
• Open margins are capable of harboring large numbers of bacteria and may be responsible for the inflammatory response seen.
• However, the quality of marginal finish and the margin location relative to the attachment are far more critical to the periodontium.
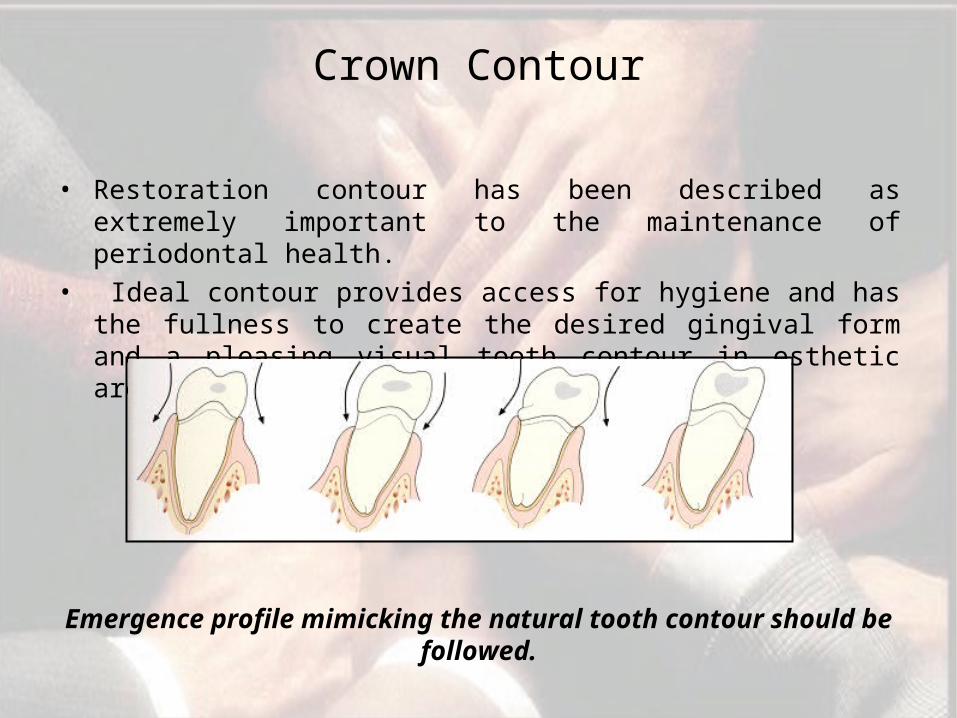
Crown Contour
• Restoration contour has been described as extremely important to the maintenance of periodontal health.
• Ideal contour provides access for hygiene and has the fullness to create the desired gingival form and a pleasing visual tooth contour in esthetic areas.
Emergence profile mimicking the natural tooth contour should be followed.
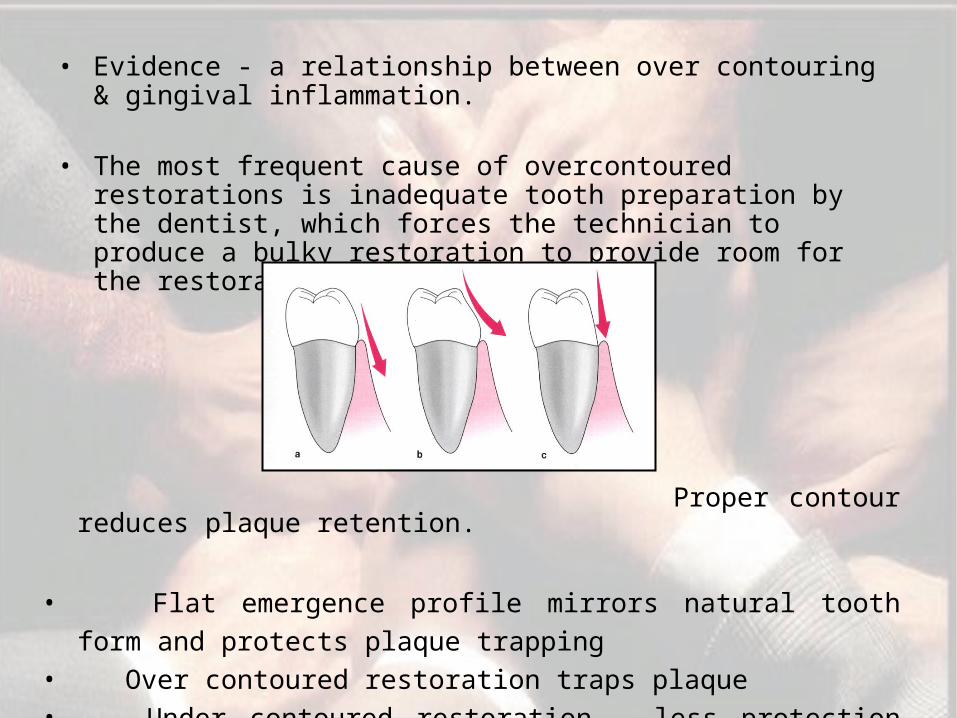
• Evidence - a relationship between over contouring & gingival inflammation.
• The most frequent cause of overcontoured restorations is inadequate tooth preparation by the dentist, which forces the technician to produce a bulky restoration to provide room for the restorative material.
Proper contour reduces plaque retention.
• Flat emergence profile mirrors natural tooth form and protects plaque trapping
• Over contoured restoration traps plaque• Under contoured restoration - less protection from
physical trauma
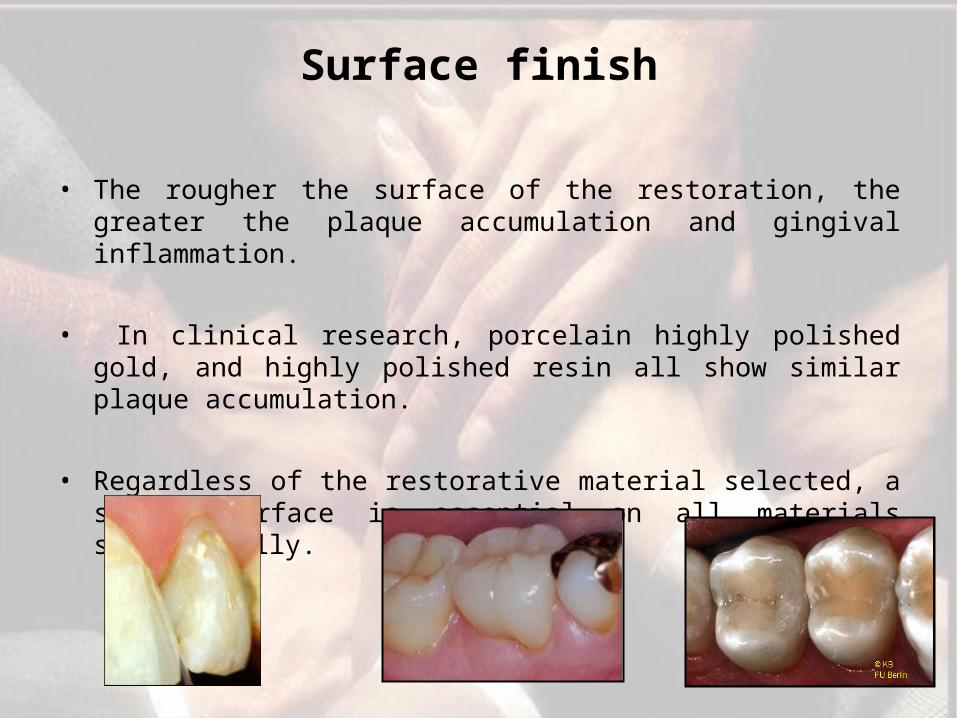
Surface finish
• The rougher the surface of the restoration, the greater the plaque accumulation and gingival inflammation.
• In clinical research, porcelain highly polished gold, and highly polished resin all show similar plaque accumulation.
• Regardless of the restorative material selected, a smooth surface is essential on all materials subgingivally.
Restorative Correction of Open Gingival Embrasures
• 2 causes of open gingival embrasures.
• Either the papilla is inadequate in height due to bone loss. OR• The interproximal contact is located too high coronally.
• If a high contact has been diagnosed as the cause of the problem, there are two potential reasons.
• If the root angulations of the teeth diverge, the interproximal contact is moved coronally, resulting in the open embrasure.
• However if the roots are parallel, the papilla form is normal, and an open embrasure exists, then the problem is probably related to tooth shape, specifically, an excessively tapered form. Restorative
dentistry
Orthodontic therapy
Periodontral therapy
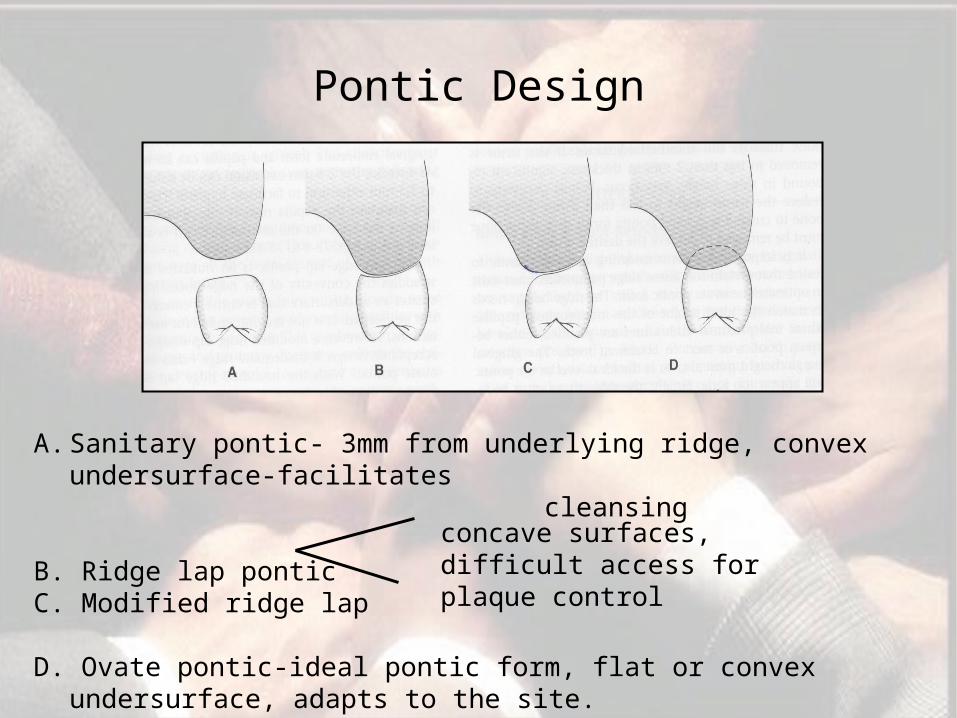
Pontic Design
A. Sanitary pontic- 3mm from underlying ridge, convex undersurface-facilitates
cleansing
B. Ridge lap pontic C. Modified ridge lap
D. Ovate pontic-ideal pontic form, flat or convex undersurface, adapts to the site.
easily maintainable
concave surfaces, difficult access for plaque control

Overhanging Restorations
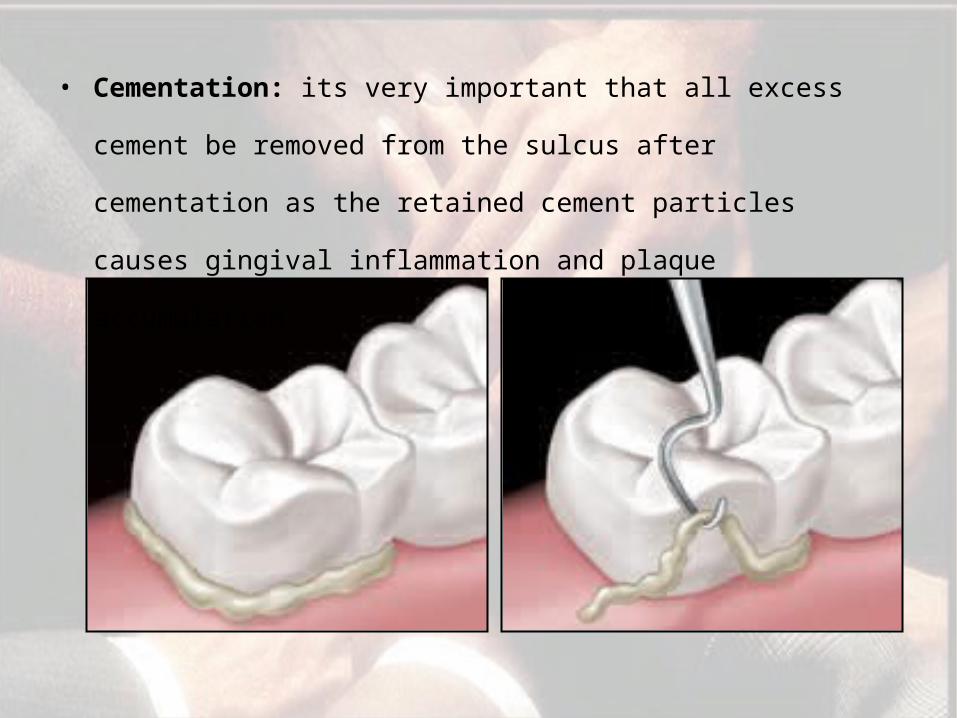
• Cementation: its very important that all excess cement be
removed from the sulcus after cementation as the retained
cement particles causes gingival inflammation and plaque
accumulation.
Splinting
• Mobility of teeth - impairs patient comfort, migration of teeth, or prosthetics where multiple abutments are necessary.
• Before considering splinting, the etiology of the instability must be identified.' Excessive occlusal forces from parafunction or deflective tooth contacts …..
• Whenever the occlusion is the cause, occlusal therapy is always performed first.
• The mobility is then evaluated over time to determine whether it resolves before splinting is considered.
• In addition, any inflammation of the periodontal supporting apparatus must be controlled before making a decision on splinting because inflammation can produce mobility in the presence of normal occlusal forces and normal periodontal support.
• The rigidity of the splint and the number of teeth used determines how the forces are distributed.
• It is critical that adequate crown length on the teeth is being splinted Also, adequate space is needed between the connector and the papilla for access with - interproximal brush ..
Periodontics and Endodontics
Interrelationship
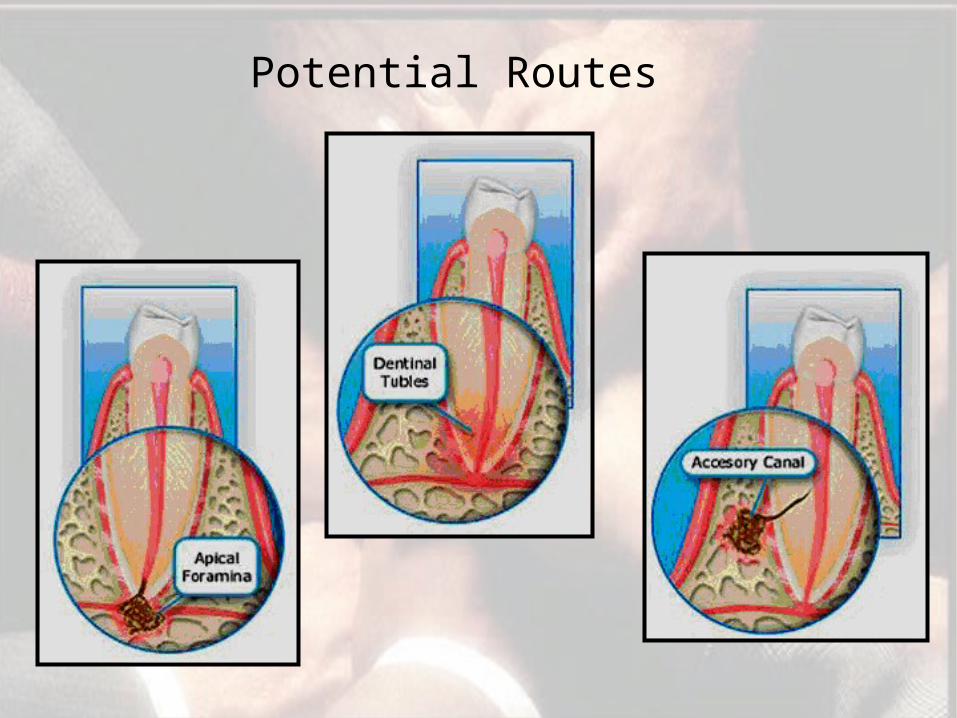
Potential Routes
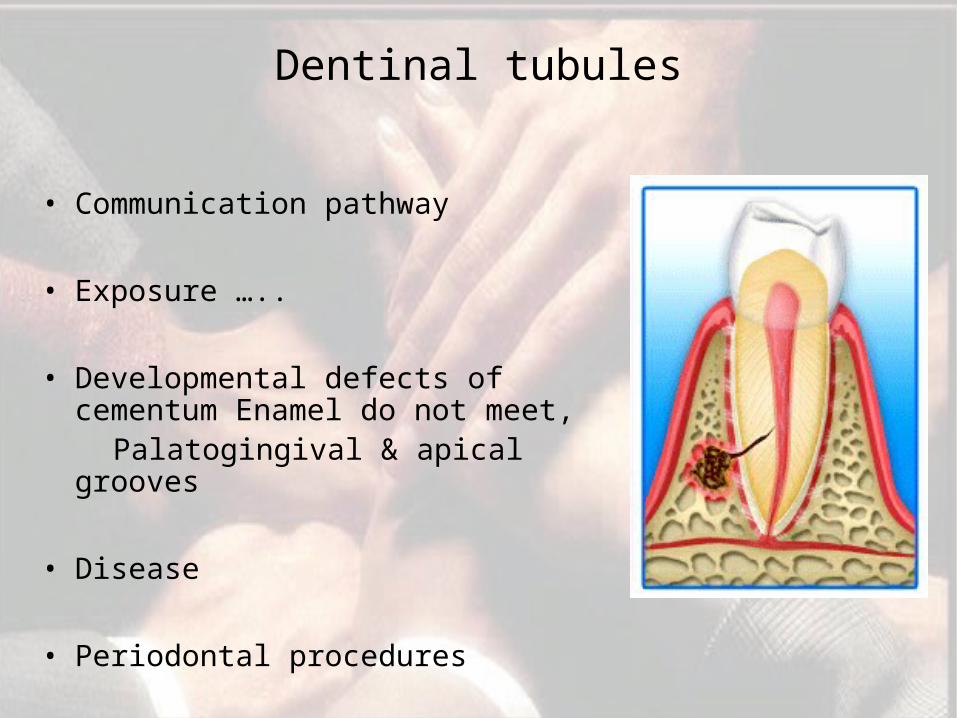
Dentinal tubules
• Communication pathway
• Exposure …..
• Developmental defects of cementum Enamel do not meet,
Palatogingival & apical grooves
• Disease
• Periodontal procedures
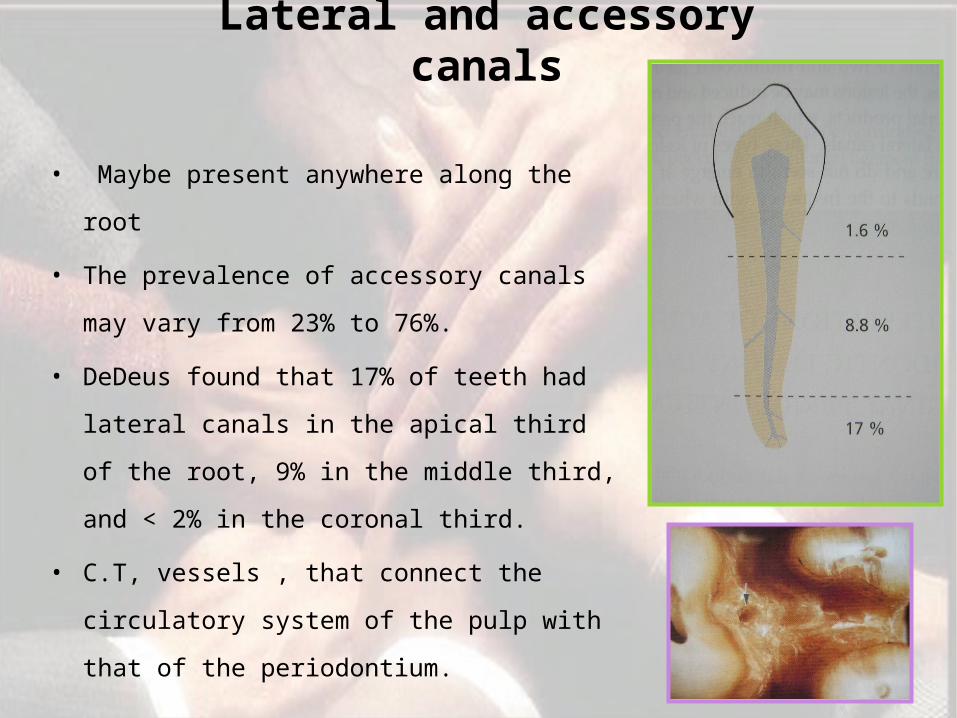
Lateral and accessory canals
• Maybe present anywhere along the root
• The prevalence of accessory canals may
vary from 23% to 76%.
• DeDeus found that 17% of teeth had
lateral canals in the apical third of the
root, 9% in the middle third, and < 2% in
the coronal third.
• C.T, vessels , that connect the
circulatory system of the pulp with that
of the periodontium.
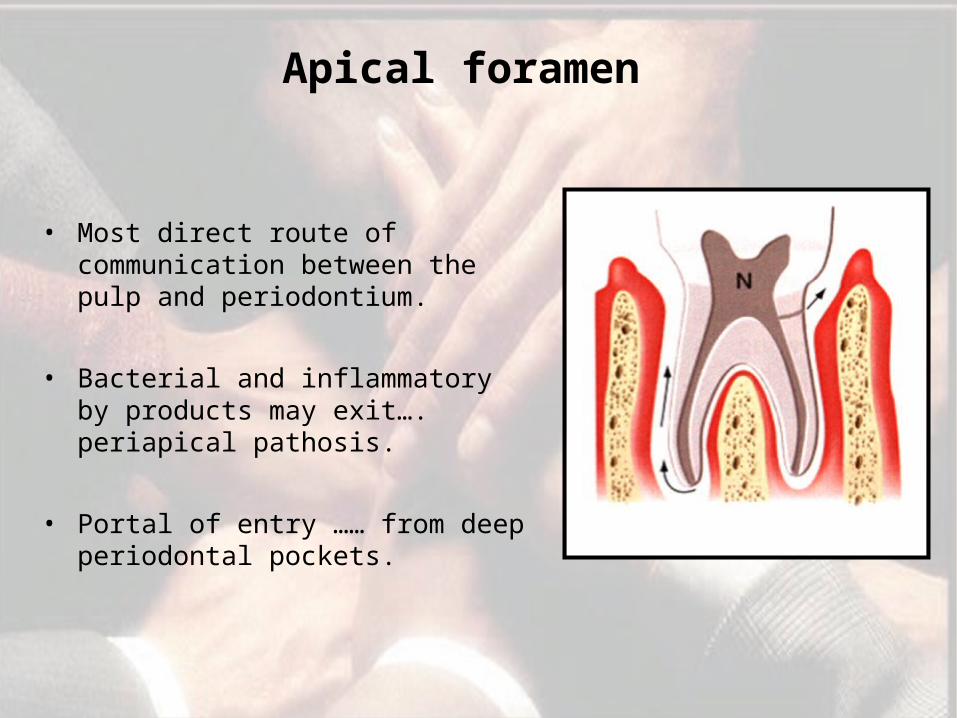
Apical foramen
• Most direct route of communication between the pulp and periodontium.
• Bacterial and inflammatory by products may exit…. periapical pathosis.
• Portal of entry …… from deep periodontal pockets.
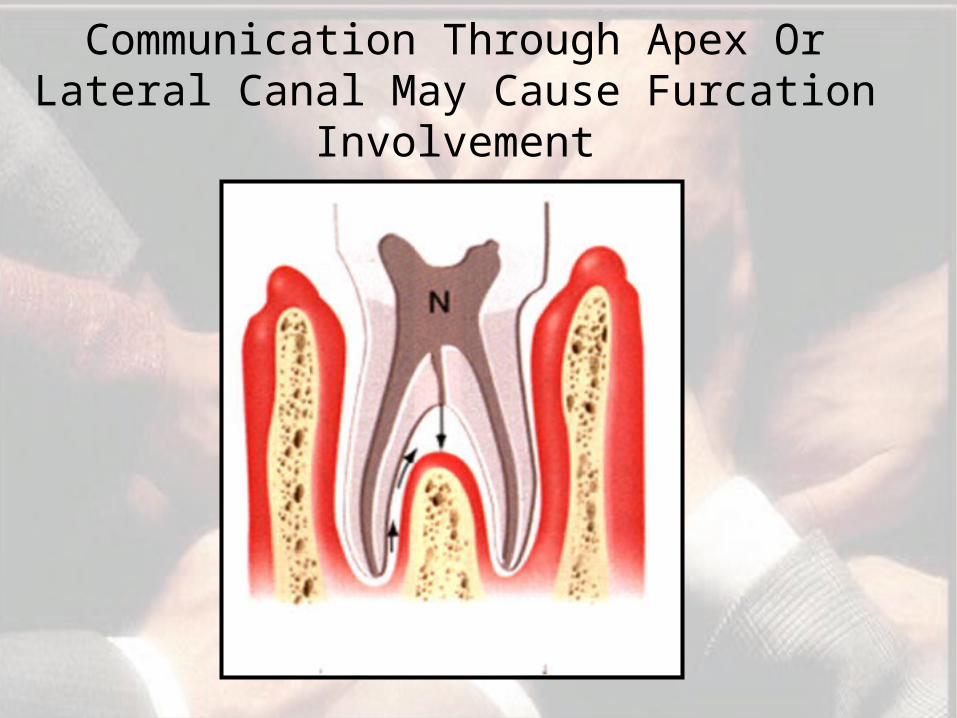
Communication Through Apex Or Lateral Canal May Cause Furcation
Involvement
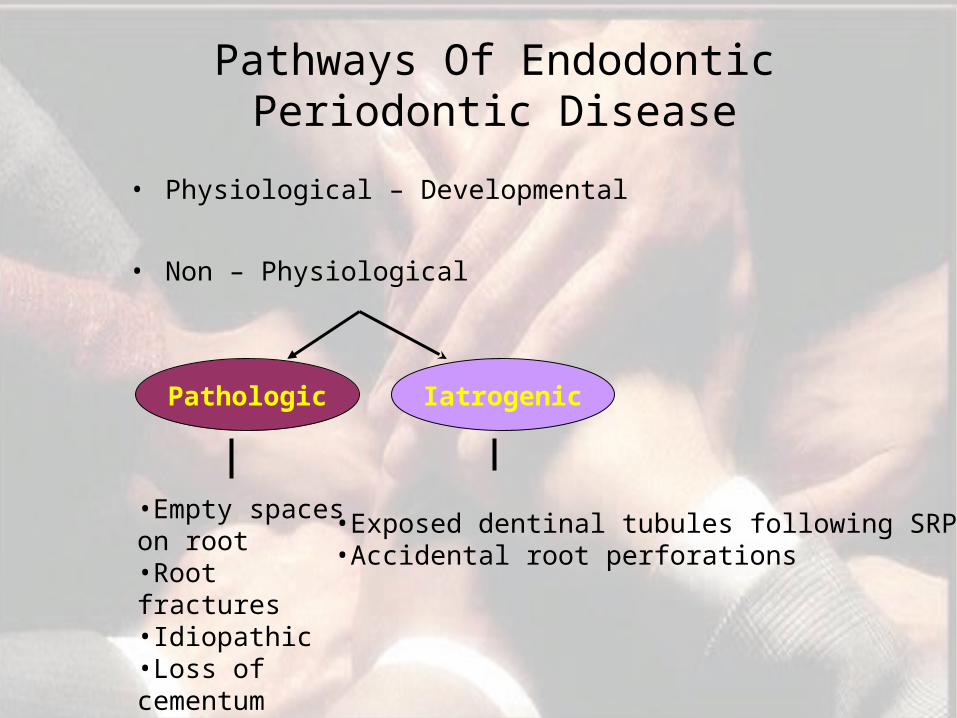
Pathways Of Endodontic Periodontic Disease
• Physiological – Developmental
• Non – Physiological
Pathologic Iatrogenic
•Empty spaces on root•Root fractures•Idiopathic•Loss of cementum
•Exposed dentinal tubules following SRP•Accidental root perforations
• CLASSIFICATION OF CLASSIFICATION OF ENDODONTIC PERIODONTIC ENDODONTIC PERIODONTIC
LESIONSLESIONS
• Based on etiology - by Simon, (1972)
• Type1 - Primary endodontic lesions• Type2 - Primary endodontic lesions with secondary
periodontal • involvement• Type 3 - Primary periodontal lesions• Type 4 - Primary periodontal lesions with secondary
endodontic • involvement• Type 5 - True combined lesions
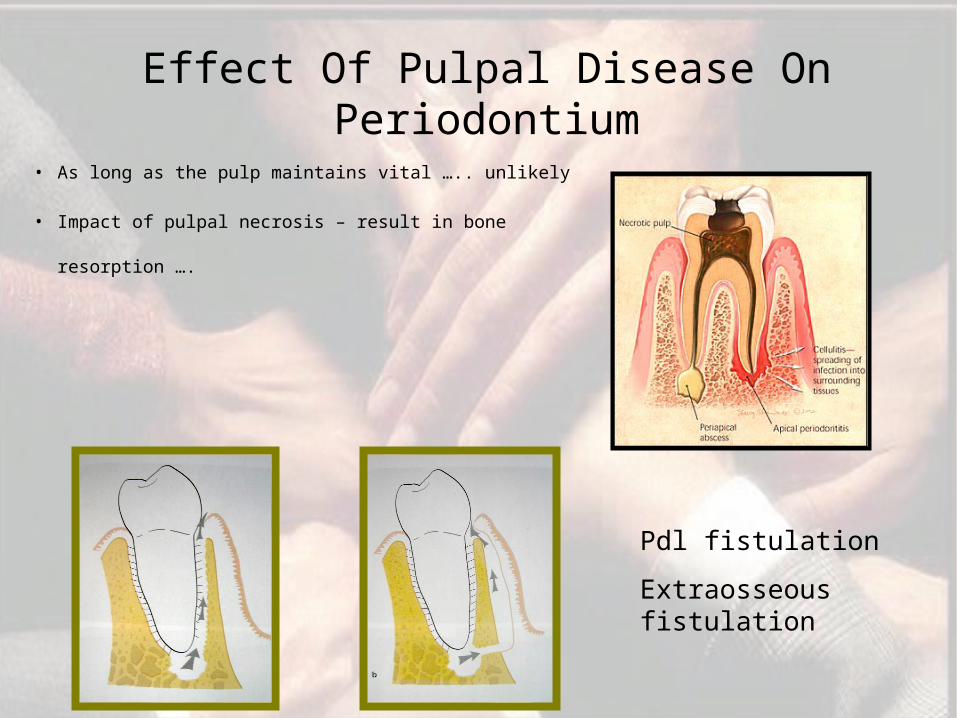
Effect Of Pulpal Disease On Periodontium
• As long as the pulp maintains vital ….. unlikely
• Impact of pulpal necrosis – result in bone
resorption ….
Pdl fistulation
Extraosseous fistulation
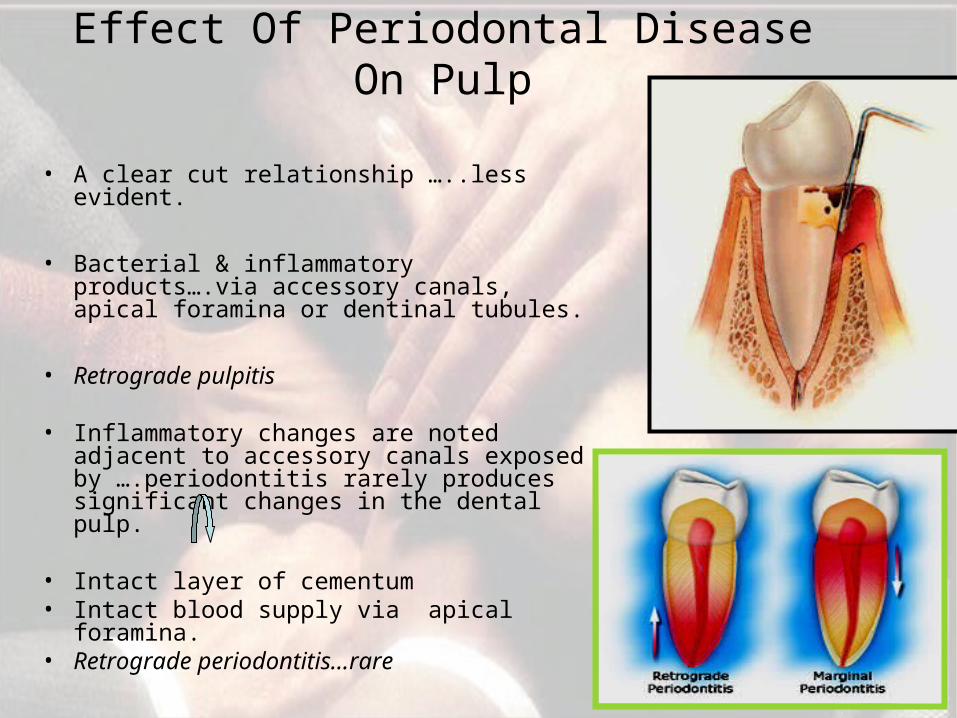
Effect Of Periodontal Disease On Pulp
• A clear cut relationship …..less evident.
• Bacterial & inflammatory products….via accessory canals, apical foramina or dentinal tubules.
• Retrograde pulpitis
• Inflammatory changes are noted adjacent to accessory canals exposed by ….periodontitis rarely produces significant changes in the dental pulp.
• Intact layer of cementum• Intact blood supply via apical
foramina.• Retrograde periodontitis…rare
Influence Of PeriodontalTreatment Measures On The Pulp
• SRP …Cementum & dentin may also be removed …
• Microbial colonization of the exposed root dentin may result in bacterial invasion of the dentinal tubules.
• (Adriaens et al 1988)
• Vitality of the pulp is not normally put at risk ( Bergenholtz , lindhe 1978)
• Rare occasions, deep scaling……………expose lateral canals…symptoms of pulpitis.
Impact Of Endodontic Treatment Measures On The Periodontium
• a) Root filled teeth of poor quality:• Unfilled spaces in root canal
Spread of infectious products into the periodontium
Contribute to increased probing depth. Retarded or impaired periodontal tissue healing subsequent to periodontal therapyJansson, Ehnevid, Lindskog & Blomlof (1993)
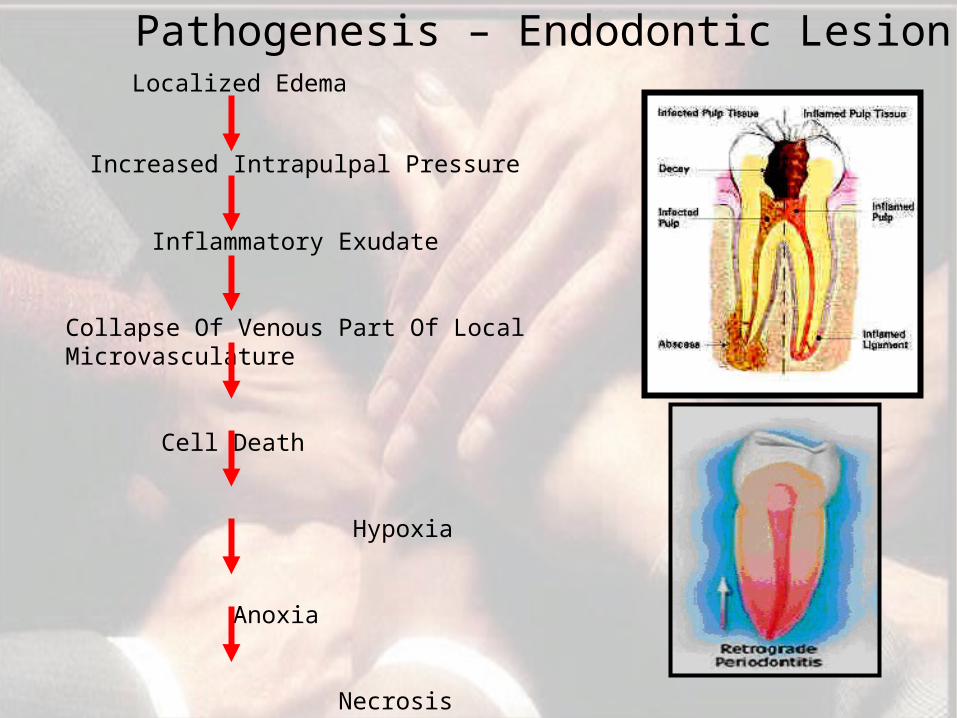
Localized Edema
Increased Intrapulpal Pressure
Inflammatory Exudate
Collapse Of Venous Part Of Local Microvasculature
Cell Death
Hypoxia
Anoxia
Necrosis
Pathogenesis – Endodontic Lesion
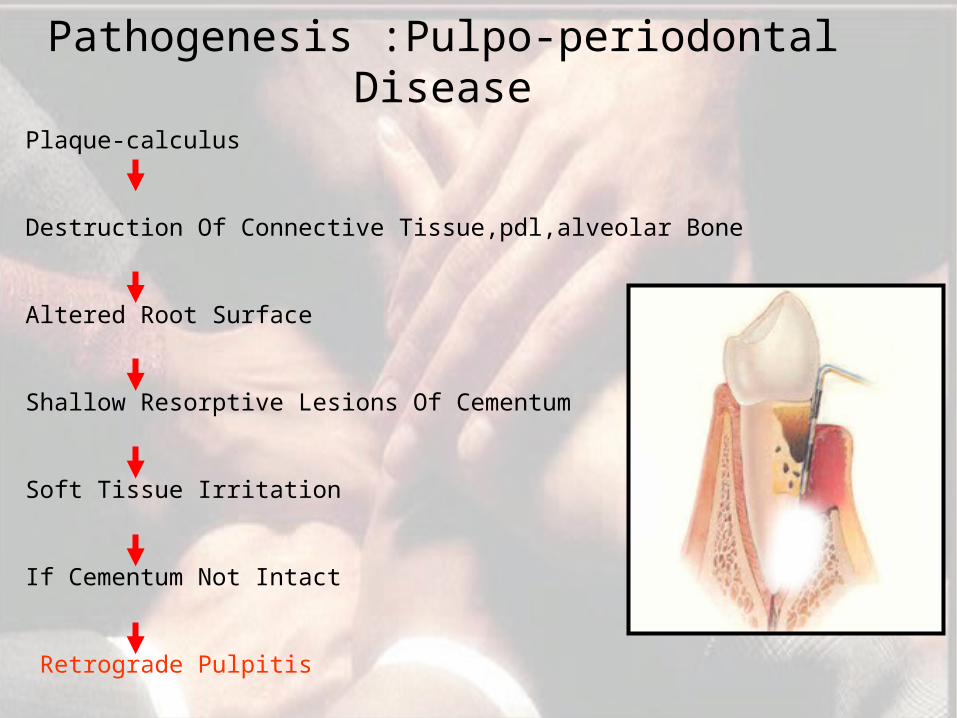
Pathogenesis :Pulpo-periodontal Disease
Plaque-calculus
Destruction Of Connective Tissue,pdl,alveolar Bone
Altered Root Surface
Shallow Resorptive Lesions Of Cementum
Soft Tissue Irritation
If Cementum Not Intact
Retrograde Pulpitis
•History •Clinical examination– Intra oral visual – Swelling
•Probing•Mobility•Tests•Percussion & palpation•Cold test•Electric pulp test•Radiographs
DiagnosisDiagnosis
LDF
PO
MRI
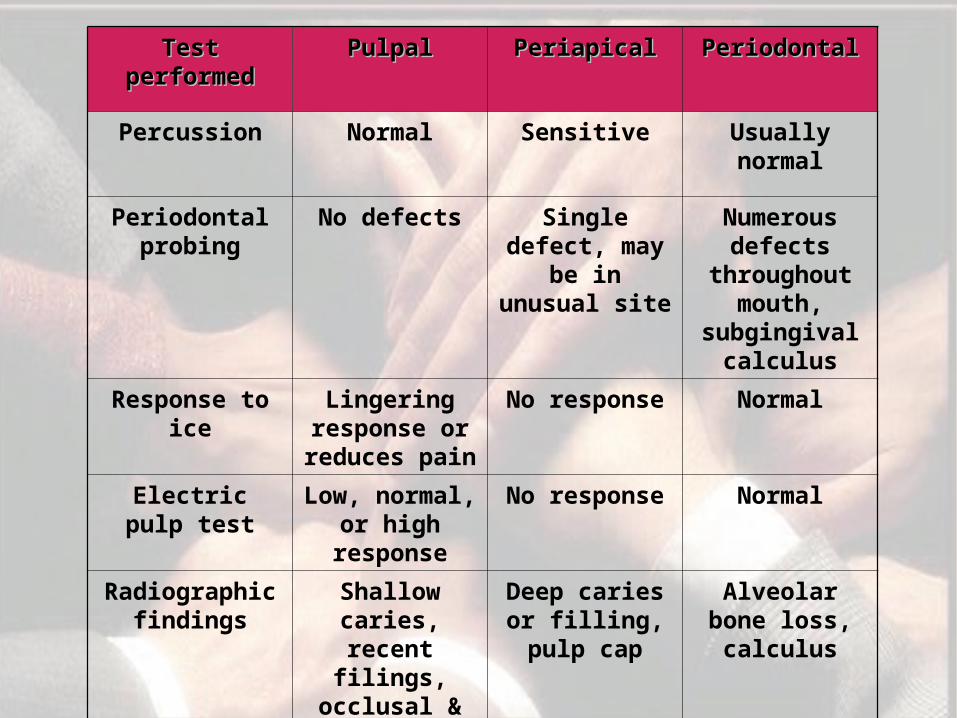
Test Test performedperformed
PulpalPulpal PeriapicalPeriapical PeriodontalPeriodontal
Percussion Normal Sensitive Usually normal
Periodontal probing
No defects Single defect, may
be in unusual site
Numerous defects
throughout mouth,
subgingival calculus
Response to ice
Lingering response or reduces pain
No response Normal
Electric pulp test
Low, normal, or high
response
No response Normal
Radiographic findings
Shallow caries, recent filings,
occlusal & physical trauma
Deep caries or filling, pulp cap
Alveolar bone loss, calculus
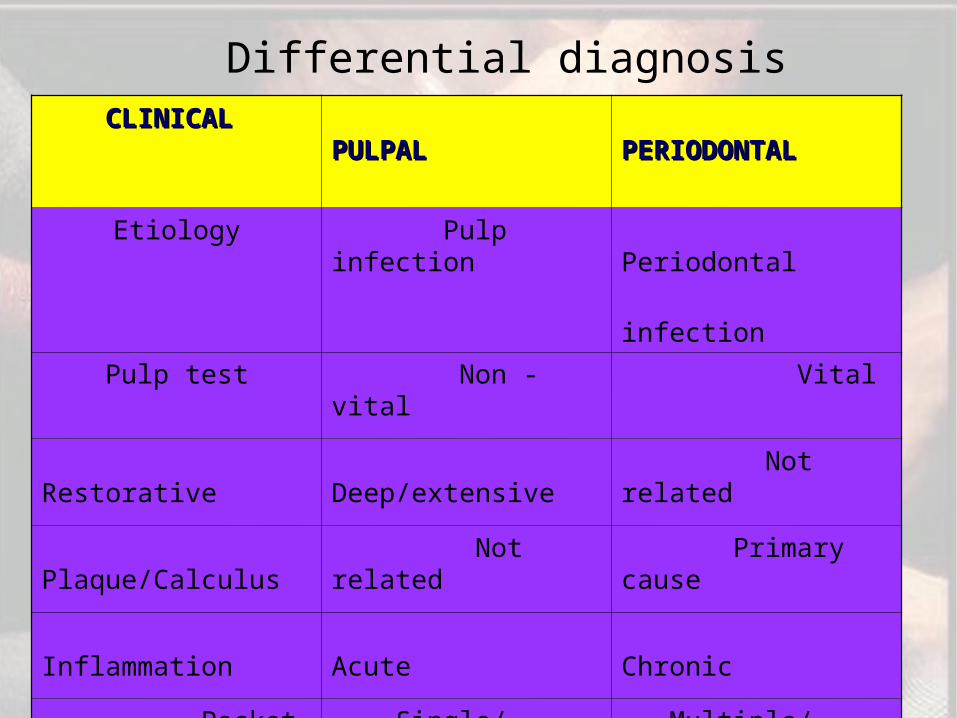
CLINICALCLINICAL PULPALPULPAL PERIODONTALPERIODONTAL
Etiology Pulp infection Periodontal
infection
Pulp test Non - vital Vital
Restorative Deep/extensive Not related
Plaque/Calculus Not related Primary cause
Inflammation Acute Chronic
Pocket Single/ Narrow Multiple/ wide
Differential diagnosis
Treatment decision-making
• The main factors to consider are:– Pulp vitality and – Type and extent of the periodontal defect.
• Primary endodontic lesions should only be treated by endodontic therapy and has a good prognosis.
• Primary periodontic lesions should only be treated by periodontal therapy. Prognosis depends on severity of the periodontal disease and patient response.
• Primary endodontic disease with secondary periodontal involvement should first be treated with endodontic therapy.
• Treatment results should be evaluated in 2 to 3 months and
only then should periodontal treatment be considered.
• Prognosis depends primarily on the severity of periodontal
involvement, periodontal treatment and patient response.
• Primary periodontal disease with secondary endodontic
involvement and true combined endodontic periodontal
diseases require both endodontic and periodontal therapies.

Coming together is the beginning
Keeping together is progress
But working together is success.”
THANK YOU
References
Clinical Periodontology – Carranza – 9th edition
Clinical Periodontology and Implant Dentistry – 4th edition - Jan Lindhe
Interrelationships between Periodontics and adult OrthodonticsJ Clin
Periodontol 1998; 25: 271-277
The role of implants in orthodontics – Net ref
The endo-perio lesion: a critical appraisal of the disease condition. Endodontic
Topics 2006, 13, 34–56
Tylman’s “Theory and practice of fixed prosthodontics” 8th edition.
Paul A. Fugazzotto “ Preparation of the periodontium for the restorative
dentistry”1st edition.
Thomas G. Wilson “Fundamentals of periodontics”
M.Martignoni “Precision fixed prosthodontics:Clinical and
labobatory aspects.
Rosenstiel “Contemporary fixed prosthodontics” 3rd edition
Shillingberg H.T – Fundamentals of FPD 3rd edition
Reconstruction of the maxillary midline papilla following a
combined orthodontic–periodontic treatment in adult
periodontal patients. J Clin Periodontol 2004; 31: 79–84.
References












![Wound healing [including healing after periodontal therapy]](https://img.pdfslide.net/doc/110x75/55c476d8bb61ebc2228b4694/wound-healing-including-healing-after-periodontal-therapy.jpg)