Embed Size (px)
Citation preview

ARTHRITIS & RHEUMATISM
0 1995, American College of Rheumatology 1055 Vol. 38, NO. 8 , August 1995, pp 1055-1059
INTERLEUKIN- 1 RECEPTOR ANTAGONIST IN PATIENTS WITH ACTIVE SYSTEMIC LUPUS ERYTHEMATOSUS
Enhanced Production by Monocytes and Correlation with Disease Activity
HIROSHI SUZUKI, HIROY UKI TAKEMURA, and HEIHACHIRO KASHIWAGI
Objective. To evaluate the relationship between the serum concentration of interleukin-1 receptor antag- onist (IL-1Ra) and systemic lupus erythematosus (SLE) disease activity, and to investigate the expression of IL-1Ra messenger RNA (mRNA) and its production by monocytes from patients with SLE.
Methods. Serum IL-1Ra was measured by en- zyme-linked immunosorbent assay, and expression of IL-1Ra mRNA was determined by Northern blotting.
Results. Serum IL-1Ra concentrations were sig- nificantly higher in patients with active SLE compared with normal subjects and patients with other rheumatic diseases, and showed a strong correlation with SLE disease activity. IL-1Ra mRNA expression in freshly isolated monocytes from patients with active SLE was consider- ably higher than that in normal monocytes. Moreover, monocytes from patients with active SLE produced increased amounts of IL-1Ra in response to adherent IgG, compared with monocytes from normal subjects.
Conclusion. A high serum concentration of IL- 1Ra is a pathophysiologic feature of active SLE and a good indicator of disease activity. Functional changes of monocytes, such as increased secretion of IL-1Ra in response to adherent IgG and enhanced expression of IL-1Ra mRNA in freshly isolated cells, may be involved in the enhanced IL-1Ra production in active SLE. High concentrations of IL-1Ra in the circulation and possibly in peripheral lymphoid tissues may influence immuno- logic and inflammatory features of SLE.
Supported in part by grants from the University of Tsukuba Project Research, and the Ministry of Health and Welfare, Japan.
Hiroshi Suzuki, MD, Hiroyuki Takemura, MD, Heihachiro Kashiwagi, MD: University of Tsukuba, Tsukubashi, Japan.
Address reprint requests to Hiroshi Suzuki, MD, Depart- ment of Rheumatology, Institute of Clinical Medicine, University of Tsukuba, Tsukubashi, Ibarakiken 305, Japan.
Submitted for publication August 22, 1994; accepted in revised form February 23, 1995.
Several recent studies indicate that interleu- kin- 1 (IL-I) activity in inflammatory and immunologic disorders is regulated by naturally occurring IL- 1 antagonists, such as IL-1 receptor antagonist (IL-1Ra) (1). IL-1Ra is a member of the IL-1 family and is secreted mainly by cells of monocyte/macrophage lineage. Regulation of IL-1Ra production by mono- cytes and macrophages is distinct from that of IL-1 production. Adherent IgG and adherent immune com- plexes are potent stimulators of IL- 1Ra production, but their potential to induce IL-1 is weak (2). The lymphokines of type-2 T helper (Th2) cells (IL-4, IL-10, and IL-13) enhance IL-1Ra production, but they inhibit IL-1 production (1).
Elevated immune complex levels and immune deposits are major causes of pathologic lesions in systemic lupus erythematosus (SLE). In addition, recent reports suggest an important role of Th2 cells in the development of immunologic abnormalities in mu- rine and human SLE (3,4). These pathophysiologic conditions in SLE appear to be favorable for the induction of IL-1Ra synthesis. IL-lRa, if present in high concentrations, may in turn influence immuno- logic and inflammatory responses. Therefore, we con- ducted the present study to investigate the expression and concentrations of IL-1Ra in SLE. We observed elevated concentrations of circulating IL-I Ra in pa- tients with active disease and a strong correlation between IL- 1Ra concentration and clinical activity of SLE. We also found increased IL-1Ra messenger RNA (mRNA) expression and enhanced IL-IRa pro- duction by monocytes from patients with SLE.
PATIENTS AND METHODS
Patients and controls. Sera were obtained from 31 patients (28 women and 3 men) who fulfilled the American
1056 SUZUKI ET AL
College of Rheumatology criteria for the classification of SLE (5 ) . Their mean % SD age was 38.6 2 15.2 years. Disease activity was assessed according to the SLE Disease Activity Index (SLEDAI) (6). Patients with SLEDAI scores of 2 3 were considered to have active SLE (n = 21), and those with scores of <3 to have inactive SLE (n = 10). Patients classified as having inactive disease had no clinical symptoms and no or only 1 abnormal laboratory result (low serum complement level or increased DNA binding activity or leukocytopenia). Laboratory data (anti-DNA, C3, C4, and IgG levels, and white blood cell [WBC] count) and SLEDAI scores were determined at the time of serum sampling.
Sera were also obtained from patients with rheuma- toid arthritis (RA) (25 women and 7 men, mean ? SD age 48.4 * 13.2 years), systemic sclerosis (20 women and 2 men, mean * SD age 52.2 2 17.3 years), and polymyositis/ dermatomyositis (9 women and 1 man, mean -t SD age 47.6 2 14.6 years). Sera were obtained from normal subjects (20 women and 15 men, mean ? SD age 34.7 * 18.5 years) to use as controls. All patients with RA had active synovitis at the time serum samples were obtained. None of the patients was receiving immunosuppressive drugs or >30 mg/day of pred- nisolone at the time of serum sampling.
Serum samples. Blood obtained by venipuncture was allowed to clot at room temperature for 1 hour. After centrifugation, the serum was divided into aliquots and stored at -70°C until used.
Reagents. Recombinant human IL- la (rHuIL-la; 2 X lo7 unitslmg protein) was kindly provided by Dainippon Pharmaceutical (Osaka, Japan), and rHuIL-4 ( lo6 unitslmg protein) was kindly provided by Ono Pharmaceutical (Osaka, Japan). Purified IgG for clinical use was obtained from Sandoz Japan. These reagents contained <0.2 ng endotoxidmg protein or mg IgG, as determined by the Limulus amebocyte lysate assay; the detection limit of the assay kit (Pyrodick; Seikagaku Kogyo, Tokyo, Japan) was 0.2 ng/ml. Lipopolysaccharide (LPS) (Escherichia coli 026: B6) was purchased from Difco (Detroit, MI).
Separation and culture of monocytes. Monocytes were separated from peripheral blood mononuclear cells (PBMC) by Ficoll-Paque density-gradient centrifugation. PBMC were suspended in culture medium (RPMI 1640 containing 10% fetal calf serum [FCS]; Hyclone Laborato- ries, Logan, UT) and incubated on a plastic plate precoated with FCS for 30 minutes at 37°C. After removal of nonad- herent cells, adherent cells were treated with phosphate buffered saline (PBS) containing 0.25% EDTA, at 4°C for 30 minutes. Adherent cells (monocytes) were detached by flushing with chilled PBS and suspended in culture medium after centrifugation. The purity of monocytes obtained by this procedure was consistently >85%, as determined by nonspecific esterase staining and labeling with the anti-CD14 monoclonal antibody Leu-M3 (Becton Dickinson, Mountain View, CA), and their viability was >95% as assessed by trypan blue dye exclusion.
For studies of IL-1Ra production, monocytes (1 x lo5), suspended in 3 ml of culture medium, were cultured for 24 hours on 35-mm wells of a 6-well culture plate (no. 3506; Costar, Cambridge, MA) precoated with clinical-grade IgG (adherent IgG stimulation). For studies of LPS stimulation, monocytes were cultured on untreated plates in the presence
of 1 ng/ml of LPS. In some experiments, the cell lysates were obtained after removal of supernatants, addition of 3 ml of medium, and freeze-thawing for 3 cycles.
Northern blot analysis. Total cytoplasmic RNA was prepared from monocytes (1 x lo6 cells) by the RNAzol B method (Biotecx Laboratories, Houston, TX), according to the manufacturer’s instructions. Ten micrograms of RNA was denatured at 37°C for 3 minutes and then applied to a 1% agarose gel prepared in 7% formaldehyde/MOPS buffer. After electrophoresis, RNA was transferred to a nitrocellu- lose membrane (Schleicher & Schuell, Keene, NH). Hybrid- ization was performed in 50% formamide, 10% dextran sulfate, 5x SSC (salinesodium citrate), 0.1% sodium dode- cyl sulfate, 10 pg salmon sperm DNA, with 32P-labeled DNA probes (1 x lo6 counts per minutelml) for 16 hours at 42°C. After washing, the membrane was exposed to x-ray film at -70°C. Amounts of IL-1Ra mRNA were estimated by den- sitometric scanning of the specific bands on the x-ray film, obtained by autoradiography. Human IL-1Ra complemen- tary DNA (cDNA; kindly supplied by Dr. D. E. Tracey, The Upjohn Company, Kalamazoo, MI) (71, human IL- lp cDNA (supplied by Dr. S. Nakai, Ohtsuka Pharmaceutical, Toku- shima, Japan) (8), and mouse p-actin cDNA (as a probe for pactin mRNA; provided by Dr. K. Tokunaga, Chiba Cancer Research Institute, Chiba, Japan) were used for Northern blot analyses.
Enzyme-linked immunosorbent assay for cytokines. IL-lRa, IL-lp, and interferon-a (IFNa) concentrations were determined by enzyme-linked immunosorbent assay, ac- cording to the manufacturers’ instructions. The detection limits of the assays were 100 pg/ml for IL-1Ra (R & D Systems, Minneapolis, MN), 30 pg/ml for IL-1p (Ohtsuka), and 40 pg/ml for IFNa (BioSource International, Westlake Village, CA) .
RESULTS
In normal subjects (n = 3 3 , the mean 2 SD serum IL-1Ra concentration was 0.43 2 0.22 ng/ml. More than 95% of the sera from patients with active SLE (20 of 21) exhibited abnormally high concentra- tions of IL-1Ra (designated as >0.87 ng/ml, the level 2 SD above the mean value in normal subjects). The mean serum IL-1Ra concentration in patients with active SLE was significantly higher than that in pa- tients with other rheumatic diseases (Table l). In patients with inactive SLE, the mean serum IL-1Ra concentration did not differ from that in normal sub- jects (Table 1). The serum IL-lP concentration was lower than the detection limit (i.e., <30 pg/ml) in all patients with active SLE (Table 1).
We next examined the relationship between serum IL-1Ra concentration and clinical and labora- tory features of SLE. Clinical and laboratory data at the time sera were obtained for IL-1Ra determination were available for 23 SLE patients. We observed a

INTERLEUKIN-1Ra IN SLE 1057
Table 1. Serum interleukin-I receptor antagonist (IL-1Ra) concen- trations and detection of serum IL-Ip in normal subjects and in patients with systemic lupus erythematosus (SLE) and other rheu- matic diseases
Group (n)*
Active (21) Inactive (10)
SLE
Normal (35) RA (32) ssc (22) PM/DM ( I 0)
IL-1Ra
Mean 2 SD ndml Pt
2.90 2 1.80 0.54 2 0.43 <O.ool 0.43 2 0.22 <O.ooI 1.24 * 1.01 <O.ool 0.94 * 0.87 ( 0 .oo 1 0.64 5 0.57 <0.001
IL-lp, no. of subjectst
0/2 1 1/10 1/35
22/32 ND ND
* RA = rheumatoid arthritis; SSc = systemic sclerosis; PM/DM = polymyositis/dermatomyositis. t Versus the active SLE group, by Student’s t-test. $ Number with detectable IL-lp (detection limit 30 pdml). ND = not determined.
strong correlation between serum IL-1Ra concentra- tion and SLEDAI score (r = 0.73, P < 0.01). We also found an inverse correlation between serum IL-1Ra level and C3 (r = -0.58, P < 0.01) or C4 (r = -0.44, P < 0.05) concentrations. A weak inverse correlation was observed between serum IL- 1Ra concentration and WBC count (r = -0.34, P not significant). Al- though we observed elevated serum IFNa concentra- tions in most patients with active SLE (data not shown), as reported previously (9), we did not find a correlation between IL-1Ra and IFNa levels (r = -0.03). In addition, no correlation between serum IL-1Ra and IgG levels was observed (r = 0.01).
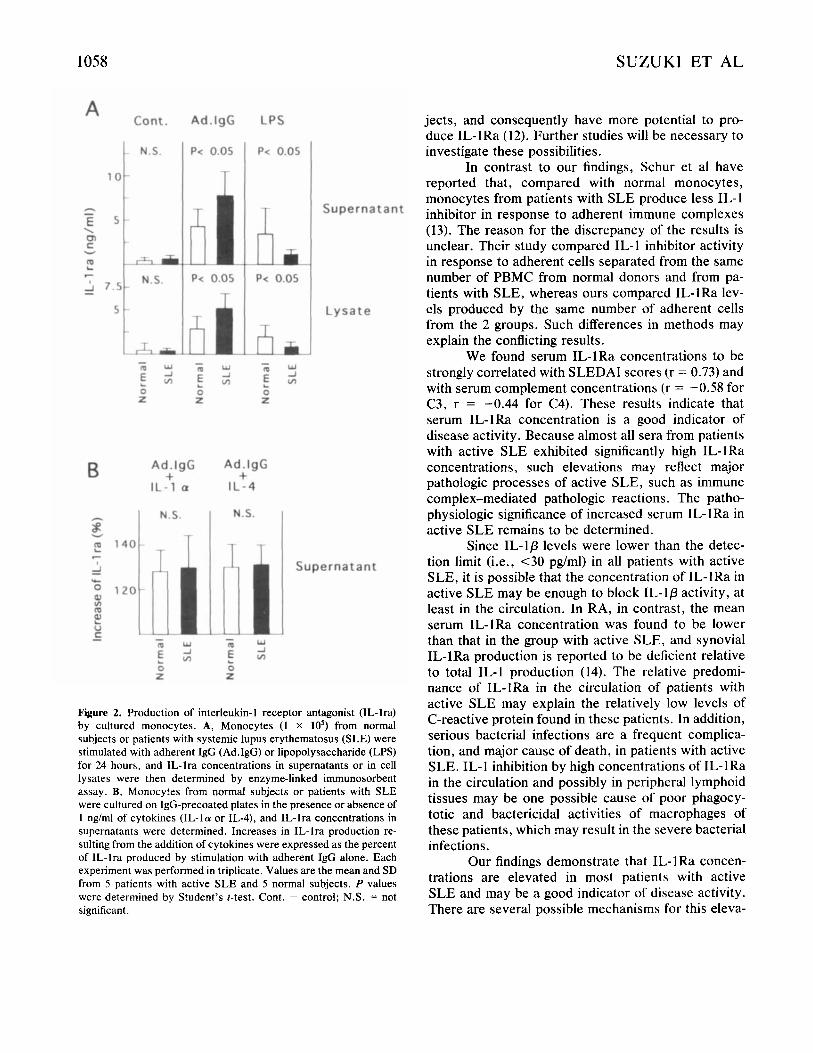
To elucidate the source of elevated serum IL- 1Ra concentrations in active SLE, we examined IL- 1Ra mRNA expression in freshly isolated monocytes. As shown in Figure 1, IL-1Ra mRNA levels in mono- cytes from patients with active SLE were significantly higher than those in monocytes from normal subjects. IL-lp mRNA could not be detected in the same blots (results not shown). Moreover, IL-1Ra production by monocytes in response to adherent IgG, both in super- natants and in cell lysates, was significantly elevated in patients with active SLE compared with normal sub- jects (Figure 2A). IL-1Ra production in response to LPS was, however, significantly depressed in patients with active SLE compared with normal subjects (Fig- ure 2A). Enhancement of IL-1Ra production in re- sponse to IL-1 or IL-4 was not significantly different between monocytes from patients with active SLE and monocytes from normal subjects (Figure 2B). IL-1Ra production by monocytes cultured in medium alone
1 2 3 4 5 6 7
I? -Actin-
L ~ o r m a t J L-..- SLE J Figure 1. Northern blot analysis of interleukin-1 receptor antago- nist (IL-lra) and pactin messenger RNA (mRNA) in freshly isolated monocytes (1 x lo6) from 3 normal subjects (lanes 1-3) and 4 patients with active systemic lupus erythematosus (SLE) (lanes 47) . The blot was hybridized to the IL-Ira probe, stripped of the probe by boiling in water for 5 minutes, and then rehybridized to the mouse pactin probe. IL-lra mRNA levels were determined by densitometry and expressed relative to pactin mRNA values.
was very low both in patients with active SLE and in normal subjects (Figure 2A).
DISCUSSION
In this study, we observed elevated concentra- tions of circulating IL-1Ra in patients with active SLE. Moreover, increased IL- 1Ra mRNA expression was found in freshly isolated monocytes from these pa- tients. These findings suggest that augmented IL-1Ra production is a pathophysiologic feature of active SLE. One possible explanation would be that depos- ited immune complexes induce augmented IL-IRa production in this disease. Formation and deposition of immune complexes are major pathologic processes in active SLE (10). IL-1Ra mRNA expression may then result from the in vivo exposure of monocytes to deposited immune complexes in this disease. More- over, Fcy receptors on the monocytes of SLE patients are increased despite impaired Fc y receptor-mediated phagocytosis (1 1). Enhanced IL-1Ra production by SLE monocytes in response to adherent IgG may arise as a result of increased ligand-binding activity via Fcy receptors and may explain the elevated concentrations of circulating IL-1Ra in patients with active disease. Another possible explanation for the augmented IL- 1Ra production would be that SLE monocytes are more differentiated than are those from normal sub-
1058 SUZUKI ET AL
Cont. A
2 7.5 - t N-S.
L - m E 0 z
A d . l g G
P< 0.05
d P< 0.05
ni W J
v,
A d . I g G + IL -1 a
N.S.
'i - m u J
5 - 0 Z
LPS
P< 0.05
L P< 0.05
iL - a Y E m h
0 z
A d . l g G + IL-4
N.S.
111 - m Y
E m 0 Z
Supernatant
Lysate
Supernatant
Figure 2. Production of interleukin-1 receptor antagonist (IL-lra) by cultured monocytes. A, Monocytes (1 X lo5) from normal subjects or patients with systemic lupus erythematosus (SLE) were stimulated with adherent IgG (Ad.IgG) or lipopolysaccharide (LPS) for 24 hours, and IL-lra concentrations in supematants or in cell lysates were then determined by enzyme-linked immunosorbent assay. B, Monocytes from normal subjects or patients with SLE were cultured on IgG-precoated plates in the presence or absence of 1 n g h l of cytokines (IL-la or IL-4), and IL-lra concentrations in supernatants were determined. Increases in IL-lra production re- sulting from the addition of cytokines were expressed as the percent of 1L-lra produced by stimulation with adherent IgG alone. Each experiment was performed in triplicate. Values are the mean and SD from 5 patients with active SLE and 5 normal subjects. P values were determined by Student's t-test. Cont. = control; N.S. = not significant.
jects, and consequently have more potential to pro- duce IL-1Ra (12). Further studies will be necessary to investigate these possibilities.
In contrast to our findings, Schur et a1 have reported that, compared with normal monocytes, monocytes from patients with SLE produce less IL-1 inhibitor in response to adherent immune complexes (13). The reason for the discrepancy of the results is unclear. Their study compared IL-1 inhibitor activity in response to adherent cells separated from the same number of PBMC from normal donors and from pa- tients with SLE, whereas ours compared IL-1Ra lev- els produced by the same number of adherent cells from the 2 groups. Such differences in methods may explain the conflicting results.
We found serum IL-1Ra concentrations to be strongly correlated with SLEDAI scores (r = 0.73) and with serum complement concentrations (r = -0.58 for C3, r = -0.44 for C4). These results indicate that serum IL-IRa concentration is a good indicator of disease activity. Because almost all sera from patients with active SLE exhibited significantly high IL-1Ra concentrations, such elevations may reflect major pathologic processes of active SLE, such as immune complex-mediated pathologic reactions. The patho- physiologic significance of increased serum IL- 1Ra in active SLE remains to be determined.
Since IL-Ip levels were lower than the detec- tion limit (i.e., <30 pg/ml) in all patients with active SLE, it is possible that the concentration of IL-IRa in active SLE may be enough to block IL-lp activity, at least in the circulation. In RA, in contrast, the mean serum IL-1Ra concentration was found to be lower than that in the group with active SLE, and synovial IL-1Ra production is reported to be deficient relative to total IL-1 production (14). The relative predomi- nance of IL-IRa in the circulation of patients with active SLE may explain the relatively low levels of C-reactive protein found in these patients. In addition, serious bacterial infections are a frequent complica- tion, and major cause of death, in patients with active SLE. IL-I inhibition by high concentrations of IL-1Ra in the circulation and possibly in peripheral lymphoid tissues may be one possible cause of poor phagocy- totic and bactericidal activities of macrophages of these patients, which may result in the severe bacterial infections.
Our findings demonstrate that IL- 1Ra concen- trations are elevated in most patients with active SLE and may be a good indicator of disease activity. There are several possible mechanisms for this eleva-

INTERLEUKIN-1Ra IN SLE 1059
tion. The cause of this abnormality and determination its specific clinical effects remain to be elucidated.
regulation of the interleukin- 1 receptor antagonist protein in U937 cells. Eur J Immunol 23:3945, 1993
8. Okada M, Yoshimura N, Ichimori Y. Kishimoto S, Nakai S,
REFERENCES 1. Dinarello CA: Modalities for reducing interleukin 1 activity in
disease. Immunol Today 14:260-264, 1993 2. Arend WP, Smith MF Jr, Janson RW, Joslin G: IL-1 receptor
antagonist and IL-1p production in human monocytes are regulated differently. J Immunol 147: 1530-1536, 1991
3. Ishida H, Muchamuel T, Sakaguchi S, Andrade S, Menon S, Howard M: Continuous administration of anti-interleukin 10 antibodies delays onset of autoimmunity in NZB/W F, mice. J Exp Med 179:305-310, 1994
4. Takeno M, Hirayama K, Sakane T: The pathogenic role of Th2 cells in systemic lupus erythematosus (abstract). Arthritis Rheum 35 (suppl9):S159, 1992
5. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield NF, Schaller JG, Tala1 N, Winchester RJ: The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 25:1272-1277, 1982
6. Bombardier C, Gladman DD, Urowitz MB, Caron D, Chang CH, and the Committee on Prognosis Studies in SLE: Deriva- tion of the SLEDAI: a disease activity index for lupus patients. Arthritis Rheum 3k630-640, 1992
7. Berger AE, Carter DB, Hankey SO, McEwan RN: Cytokine
Nishio N, Kishimoto T: Immunologic and molecular character- ization of T-cell-derived T cell activating factor. J Immunol 136:1288-1294, 1986
9. Kim T, Kanayama Y, Negoro N, Okamura M, Takeda T, Inoue T: Serum levels of interferons in patients with systemic lupus erythematosus. Clin Exp Immunol 70562-569, 1987
10. Emlen W: Immune complexes in systemic lupus erythematosus. In, Dubois’s Lupus Erythematosus, Fourth edition. Edited by DJ Wallace, BH Hahn. Philadelphia, Lea & Febiger, 1992
11. Fries LF, Mullin WW, Cho KR, Plotz PH, Frank MM: Mono- cyte receptors for the Fc portion of IgG are increased in systemic lupus erythematosus. J Immunol 132:695-700, 1984
12. Janson RW, Hance KR, Arend WP: Production of IL-1 receptor antagonist by human in vitro derived macrophages: effects of lipopolysaccharide and granulocyte-macrophage colony- stimulating factor. J Immunol 147:4218-4223, 1991
13. Schur PH, Chang D-M, Baptiste P, Uhteg LC, Hanson DC: Human monocytes produce IL-I and an inhibitor of IL-1 in response to two different signals. Clin Immunol Immunopathol 57:45-63, 1990
14. Firestein GS, Boyle DL, Yu C, Paine MM, Whisenand TD, Zvaifler NJ, Arend WP: Synovial interleukin- 1 receptor antag- onist and interleukin-1 balance in rheumatoid arthritis. Arthritis Rheum 37:644-652, 1994