Embed Size (px)
Citation preview
Internal mammary artery pseudoaneurysms complicating chest wall
infection in children
Diagnosis and endovascular therapy
Hemant Deshmukha, Srinivasa R. Prasadb,*, Tufail Patankara, Madhavi Zankara
aDepartment of Radiology, King Edward Memorial Hospital, Bombay, IndiabDepartment of Abdominal Imaging, 9th Floor, Mallinckrodt Institute of Radiology, St. Louis, MO 63110, USA
Received 3 April 2001; accepted 2 June 2001
Abstract
Mycotic internal mammary artery (IMA) pseudoaneurysms are sparsely reported in medical literature. We report imaging findings of IMA
pseudoaneurysms secondary to chest wall abscesses (staphylococcal and tuberculous) in two children. Both children were successfully
treated by endovascular method thus obviating the need for surgery. D 2001 Elsevier Science Inc. All rights reserved.
Keywords: Abscess; Internal mammary artery; Pseudoaneurysm; Embolization
1. Introduction
Internal mammary artery (IMA) aneurysms are extremely
rare. Postoperative [1], posttraumatic, mycotic [2], and
atherosclerotic aneurysms of the IMA are described in the
literature. IMA may be a source of significant mediastinal
hemorrhage with possible catastrophic consequences espe-
cially in patients with blunt or penetrating trauma [3].
Angiographic demonstration of an aneurysm is critical in
establishing specific diagnosis and detects the source of
hemorrhage to enable timely institution of endovascular
treatment. We report two cases of bleeding IMA pseudoa-
neurysms in children (staphylococcal and tuberculous pseu-
doaneurysms) that were successfully embolized using coils.
2. Case reports
2.1. Case 1
A 5-year-old boy developed fever and a large, left-sided
anterior chest wall abscess 1 week following an accidental
fall from a treetop. Incision and drainage of this abscess in a
peripheral hospital had yielded blood admixed with pus and
had resulted in considerable hemorrhage. The pus had
grown Staphylococcus aureus and the patient was put on
antistaphylococcal antibiotics. The patient was referred to
our hospital following two episodes of massive hemoptysis.
Clinical examination revealed a large, anterior chest wall
abscess. Contrast-enhanced CT scan of the chest demon-
strated a large, partially thrombosed pseudoaneurysm; how-
ever, its precise arterial origin could not be ascertained
(Fig 1). In addition, there was a lenticular-shaped hemo-
thorax. Arch aortogram, bronchial, and intercostal angio-
grams were normal. Selective left subclavian angiogram
showed a large pseudoaneurysm arising from the IMA just
distal to its origin (Fig. 2a). Complete occlusion of the IMA
at its origin with obliteration of the pseudoaneurysm was
achieved using 4-mm diameter, 3-cm-long steel coil (Cook,
Bloomington, US) placed through a 4F head hunter (Cook)
(Fig. 2b). A follow-up CT scan at 2 weeks showed marked
diminution in the size of the pseudoaneurysm. The patient
was discharged after 2 weeks following an uneventful
course in the hospital.
2.2. Case 2
An 11-year-old girl presented with low-grade fever and a
right-sided anterior chest wall cold abscess. An incision and
drainage was attempted in a peripheral hospital resulting in
0899-7071/01/$ – see front matter D 2001 Elsevier Science Inc. All rights reserved.
PII: S0899 -7071 (01 )00325 -4
* Corresponding author.
E-mail address: [email protected] (S.R. Prasad).
Journal of Clinical Imaging 25 (2001) 396–399

significant bleeding. Hemostasis was achieved by surgical
packing of the wound. The patient was then referred to our
hospital. Doppler sonography of the chest demonstrated a
large pseudoaneurysm in the bed of the chest wall abscess
(Fig. 3). Acid-fast bacilli were identified in the pus by Ziehl–
Nielsen staining (the cultures were positive for Mycobacte-
Fig. 1. (Case 1) Contrast-enhanced CT scan of the chest shows a large,
partially thrombosed aneurysm (arrow).
Fig. 2. (Case 1) (a) Delayed phase of left subclavian angiogram demonstrates the lumen of the pseudoaneurysm (curved arrow). Note opacification of the left
upper and mid zones and the marked deviation of the esophageal Ryle’s tube to the right (arrow). (b) Postembolization left subclavian angiogram shows
complete occlusion of the IMA and the pseudoaneurysm. Arrow shows the coil at the origin of the IMA.
Fig. 3. (Case 2) Chest ultrasound showing the pseudoaneurysm (straight
arrows) in the bed of tuberculous cold abscess (curved arrows). AO: Aorta.
H. Deshmukh et al. / Journal of Clinical Imaging 25 (2001) 396–399 397
rium tuberculosis 4 weeks later). Arch aortogram, bronchial,
and intercostal angiograms did not show any abnormality.
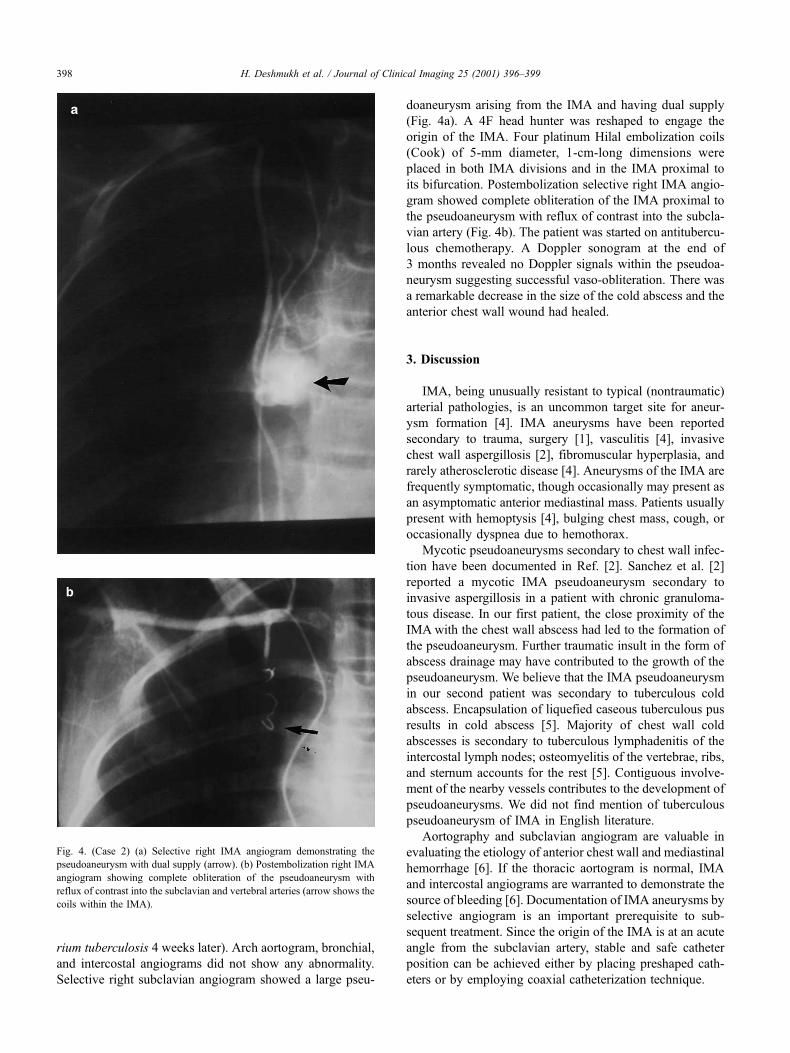
Selective right subclavian angiogram showed a large pseu-
doaneurysm arising from the IMA and having dual supply
(Fig. 4a). A 4F head hunter was reshaped to engage the
origin of the IMA. Four platinum Hilal embolization coils
(Cook) of 5-mm diameter, 1-cm-long dimensions were
placed in both IMA divisions and in the IMA proximal to
its bifurcation. Postembolization selective right IMA angio-
gram showed complete obliteration of the IMA proximal to
the pseudoaneurysm with reflux of contrast into the subcla-
vian artery (Fig. 4b). The patient was started on antitubercu-
lous chemotherapy. A Doppler sonogram at the end of
3 months revealed no Doppler signals within the pseudoa-
neurysm suggesting successful vaso-obliteration. There was
a remarkable decrease in the size of the cold abscess and the
anterior chest wall wound had healed.
3. Discussion
IMA, being unusually resistant to typical (nontraumatic)
arterial pathologies, is an uncommon target site for aneur-
ysm formation [4]. IMA aneurysms have been reported
secondary to trauma, surgery [1], vasculitis [4], invasive
chest wall aspergillosis [2], fibromuscular hyperplasia, and
rarely atherosclerotic disease [4]. Aneurysms of the IMA are
frequently symptomatic, though occasionally may present as
an asymptomatic anterior mediastinal mass. Patients usually
present with hemoptysis [4], bulging chest mass, cough, or
occasionally dyspnea due to hemothorax.
Mycotic pseudoaneurysms secondary to chest wall infec-
tion have been documented in Ref. [2]. Sanchez et al. [2]
reported a mycotic IMA pseudoaneurysm secondary to
invasive aspergillosis in a patient with chronic granuloma-
tous disease. In our first patient, the close proximity of the
IMA with the chest wall abscess had led to the formation of
the pseudoaneurysm. Further traumatic insult in the form of
abscess drainage may have contributed to the growth of the
pseudoaneurysm. We believe that the IMA pseudoaneurysm
in our second patient was secondary to tuberculous cold
abscess. Encapsulation of liquefied caseous tuberculous pus
results in cold abscess [5]. Majority of chest wall cold
abscesses is secondary to tuberculous lymphadenitis of the
intercostal lymph nodes; osteomyelitis of the vertebrae, ribs,
and sternum accounts for the rest [5]. Contiguous involve-
ment of the nearby vessels contributes to the development of
pseudoaneurysms. We did not find mention of tuberculous
pseudoaneurysm of IMA in English literature.
Aortography and subclavian angiogram are valuable in
evaluating the etiology of anterior chest wall and mediastinal
hemorrhage [6]. If the thoracic aortogram is normal, IMA
and intercostal angiograms are warranted to demonstrate the
source of bleeding [6]. Documentation of IMA aneurysms by
selective angiogram is an important prerequisite to sub-
sequent treatment. Since the origin of the IMA is at an acute
angle from the subclavian artery, stable and safe catheter
position can be achieved either by placing preshaped cath-
eters or by employing coaxial catheterization technique.
Fig. 4. (Case 2) (a) Selective right IMA angiogram demonstrating the
pseudoaneurysm with dual supply (arrow). (b) Postembolization right IMA
angiogram showing complete obliteration of the pseudoaneurysm with
reflux of contrast into the subclavian and vertebral arteries (arrow shows the
coils within the IMA).
H. Deshmukh et al. / Journal of Clinical Imaging 25 (2001) 396–399398

Embolization of the IMA has been reported for the
control of traumatic and tumoral hemorrhage. Embolo-
therapeutic occlusion of the IMA has been performed using
various embolic materials such as gelfoam [6], autologous
clots [7], Gianturco coils [3], and absolute alcohol [8].
Potential complications of the procedure include inadvertent
embolization of the vertebral or subclavian arteries that can
be avoided by stable and selective catheter placement and
cautious embolization [6]. Rich collateral vascular supply
excludes the possibility of chest wall infarction after select-
ive embolization. Retrograde collateral flow to the bleeding
site can be prevented by injecting particulate embolic
material into the IMA distal to the arterial pathology [6].
In our two patients with staphylococcal and tuberculous
pseudoaneurysms complicated by trauma, coil embolization
of the IMA resulted in total obliteration of the pseudoaneur-
ysms. Complete control of hemoptysis was achieved, thus
obviating the need for emergency thoracotomy and its
attendant complications. Endovascular treatment of the pseu-
doaneurysms combined with antibiotics ensured cure of the
pseudoaneurysms and healing of the chest wall abscesses.
In conclusion, IMA pseudoaneurysms, though distinctly
rare, may contribute to life-threatening hemorrhage. Anterior
chest wall abscesses should be treated aggressively to
prevent transthoracic spread of infection leading to vascular
complications. Percutaneous transcatheter vaso-occlusion of
the IMA pseudoaneurysm is a safe, effective, and minimally
invasive nonsurgical means of achieving cure.
References
[1] Millner RW, Guvendik L, Blauth C, Treasure T, Pepper JR. False
aneurysm of the right internal mammary artery. Ann Thorac Surg
1991;51(5):831–2.
[2] Sanchez FW, Freland PN, Bailey GT, Vujic I. Embolotherapy of a
mycotic pseudoaneurysm of the internal mammary artery in chronic
granulomatous disease. Cardiovasc Intervent Radiol 1985;8:43–5.
[3] Smith DC, Senac MO, Bailey LL. Embolotherapy of a ruptured internal
mammary artery secondary to blunt chest trauma. J Trauma 1982;
22:333–5.
[4] Giles JA, Sechtin AG, Waybill MM, Moser RP. Bilateral internal mam-
mary artery aneurysms: a previously unreported cause for anterior me-
diastinal mass. Am J Roentgenol 1990;154:1189–90.
[5] Hurt RL. The thorax. In: Mann CV, Russell RCG, editors. Love and
Bailey’s short practice of surgery. 21st ed. London: ELBS with Chap-
man & Hall, 1994. p. 831.
[6] Husted JW, Stock JR, Manella WJ. Traumatic anterior mediastinal
hemorrhage: control by internal mammary artery embolization. Cardi-
ovasc Intervent Radiol 1982;5:268–70.
[7] Harrington DP, Barth KH, Baker RR, Truax DT, Abeloff MD, White
RI. Therapeutic embolization for hemorrhage from locally recurrent
cancer of the breast. Radiology 1978;129:307–10.
[8] McLean GK, Mackie JA, Hartz WH, Freidman DB. Percutaneous al-
cohol injection for control of internal mammary artery bleeding. Am J
Roentgenol 1983;141:181–2.
H. Deshmukh et al. / Journal of Clinical Imaging 25 (2001) 396–399 399