Embed Size (px)
Citation preview

Int J Pharm Bio Sci 2014 April ; 5 (2) : (B) 880 - 887
This article can be downloaded from www.ijpbs.net
B - 880
Case report Pathology
International Journal of Pharma and Bio Sciences ISSN
0975-6299
ANOMALOUS ORIGIN OF LEFT CORONARY ARTERY FROM
PULMONARY ARTERY [ALCAPA] –A CASE REPORT
EPHRAIM.V.R.K* AND V.LEELA
Department of Anatomy, Deccan College of Medical Sciences, Hyderabad, India.
ABSTRACT
ALCAPA a rare congenital coronary anomaly, which usually manifests as an isolated defect, and can develop when there is an embryological failure of normal communication to the left coronary bud in the aorta, with an abnormal connection to the pulmonary bud instead. If left untreated, up to 90% of pediatric patients with this syndrome die within the 1st year of life. To survive beyond infancy, patients with ALCAPA syndrome develop significant collateral circulation from the right coronary artery(RCA) to the Left coronary artery(LCA) However, often it is not sufficient to supply the left ventricle, especially in the subendocardial region, manifesting as various degrees of the adult type of the disease. This study presents such a rare adult case, and its pathognesis, clinical spectrum, and findings are discussed. Management was successful, by placement of a Coronary artery bypass graft(CABG) with ligation of the anomalous LCA: the choice of procedures available & their implications are outlined.
KEYWORDS: adult-onset ALCAPA, coronary anomalies, vascular steal, CT coronary angiography, coronary artery bypass graft
EPHRAIM.V.R.K
Department of Anatomy, Deccan College of Medical Sciences, Hyderabad, India.
Int J Pharm Bio Sci 2014 April ; 5 (2) : (B) 880 - 887
This article can be downloaded from www.ijpbs.net
B - 881
INTRODUCTION
Anomalous origin of the left main coronary artery from the main pulmonary artery (ALCAPA) or “Bland White Garland Syndrome”1 is a rare congenital abnormality that affects 1 in 300,000 live births2 & accounts for 0.25%19–0.5% of all congenital heart defects; and survival to adulthood is further rare, accounting for 10-15% of these cases3. In 5% of cases it may be associated with other cardiac anomalies such as atrial septal defect, ventricular septal defect, & aortic coarctation.4 This anomaly may result from either abnormal septation of cono-truncus into aorta and pulmonary artery, or from persistence of pulmonary buds with involution of aortic buds, that will eventually form coronary arteries5. The male to female ratio of 1:2 in adults contrasts with that found in infants and children (2:1), suggesting that men are more susceptible to death resulting from this disorder if left untreated6. ALCAPA syndrome results in the “coronary steal” phenomenon, in which a left-to-right shunt leads to abnormal left ventricular perfusion.4 In patients who live to adulthood, ALCAPA syndrome may cause myocardial infarction, in which a left-to-right shunt, left ventricular dysfunction and mitral regurgitation, or silent myocardial ischemia, can lead to sudden
cardiac death. The oldest reported case is said to be that of an 85 year old Caucasian woman, in Iran7. Here, we present one such rare adult case; factors affecting, management modalities, and comparative literature are discussed. Case: A 45-year old female patient presented to the cardiac out-patient department, with complaints of dyspnoea on exertion & intermittent chest pain8 of 1 month duration. There was no history of sweating, giddiness, nausea, vomiting or pedal edema. No past history of diabetes mellitus, hypertension, bronchial asthma, tuberculosis, Chronic Obstructive Pulmonary Disease, or Coronary Artery Disease was found. Nothing significant was elicited from personal and family histories. Examination revealed a generally good condition of the patient, except for dyspnoea NYHA Class –II. Hemodynamic, haematological, bio-chemical parameters were within normal limits.9 First line Investigations done:
• ECG : Sinus Rhythm, Left Ventricular Hypertrophy, & Left Axis Deviation
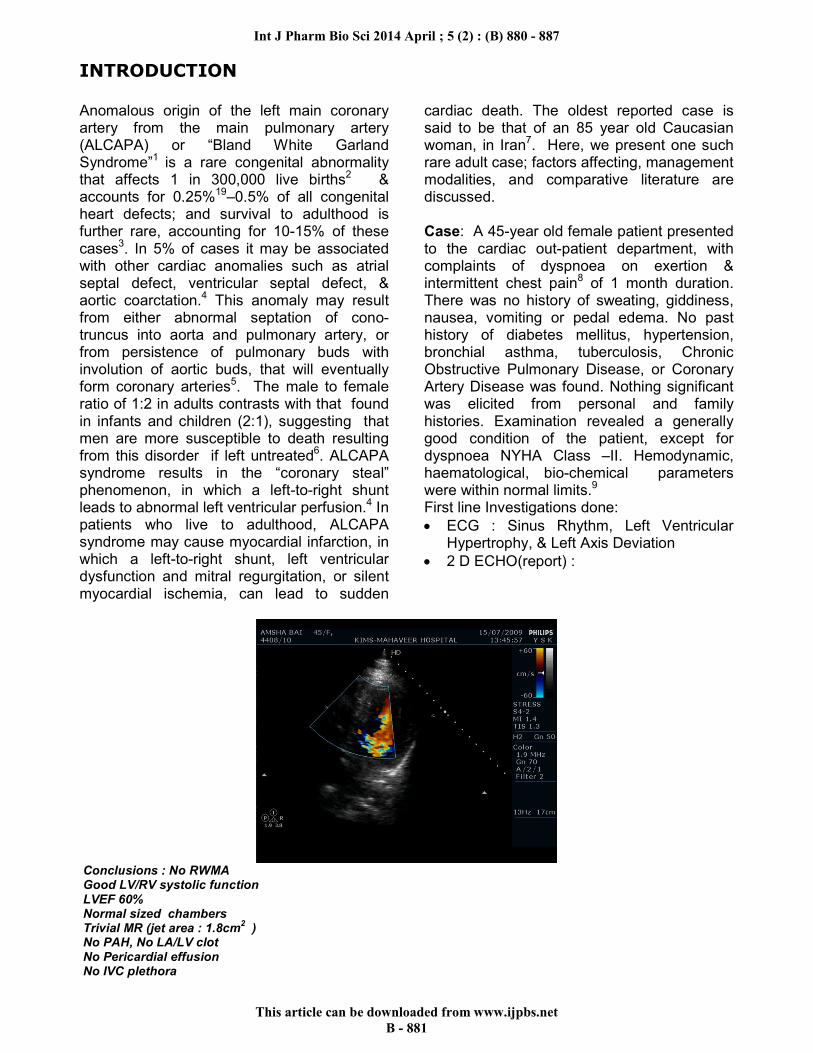
• 2 D ECHO(report) :
Conclusions : No RWMA Good LV/RV systolic function LVEF 60% Normal sized chambers Trivial MR (jet area : 1.8cm
2 )
No PAH, No LA/LV clot No Pericardial effusion No IVC plethora

Int J Pharm Bio Sci 2014 April ; 5 (2) : (B) 880 - 887
This article can be downloaded from www.ijpbs.net
B - 882
Special investigations [ cardiac work up] were ordered
• Trans Esophageal EchoCardiography (TEE) showed
Conclusions: Dilated RCA (Size: 9 mm) LCA Arising from MPA with retrograde flow Dilated Coronary Arterial System Good LV/RV Systolic function Trivial MR, No PAH
Impression : ALCAPA
• Coronary Angiogram
Coronary Angiogram Report: Diagnosis : Dyspnoea Class II and Exertional Angina Class II, Good LV function. Approach : Right radial artery. Pressures : 150 / 60 (105) Flouro time : 28.2 mins RCA : Normal origin and diffusely dilated significantly (aneurysmal), on RCA injection, left system fills retrogradely by the collaterals. Opacification of the MPA, RPA and LPA seen from the LCA. LCA : Arising from Pulmonary artery, aneurysmal and filling retrogradely through RCA. Right heart catheterisation and oximetry : PA :48/21(30),RV :70 % RPA :75.6% MPA : 77%, FA : 96.2%
Impression : ALCAPA Recommendation : Coronary Artery Reimplantation / Ligation of Left Coronary Artery(LCA) and CABG(Left Internal Mammary Artery to Left Anterior Descending Artery(LIMA �LAD) and Saphenous Venous Graft to Left Circumflex artery(SVG �LCx )

Int J Pharm Bio Sci 2014 April ; 5 (2) : (B) 880 - 887
This article can be downloaded from www.ijpbs.net
B - 883
• CT Coronary Angiogram
CT Coronary Angiogram Report Technique CT Coronary angiography has been done on multislice CT scanner using 80cc of non ionic contrast intravenously. FINDINGS There is anomalous origin of left main coronary artery from main pulmonary artery, which is short and large in caliber. The artery measuring 8.7 mm in diameter, is dividing into LAD and LCx branches. LAD is large in caliber and tortuous. Diagonal 1 is small and Diagonal 2 is normal. LCx is co-dominant, slightly large in caliber OM1 is normal and OM2 is small RCA is co-dominant arising from right coronary cusp, tortuous and hypertrophied. Circulation is co-dominant Impression : Anomalous origin of left main coronary artery from main pulmonary artery.Left main coronary artery is giving rise to LAD and LCx, which are large in caliber and tortuous. Large hypertrophied tortuous RCA arising from right coronary cusp.
Int J Pharm Bio Sci 2014 April ; 5 (2) : (B) 880 - 887
This article can be downloaded from www.ijpbs.net
B - 884
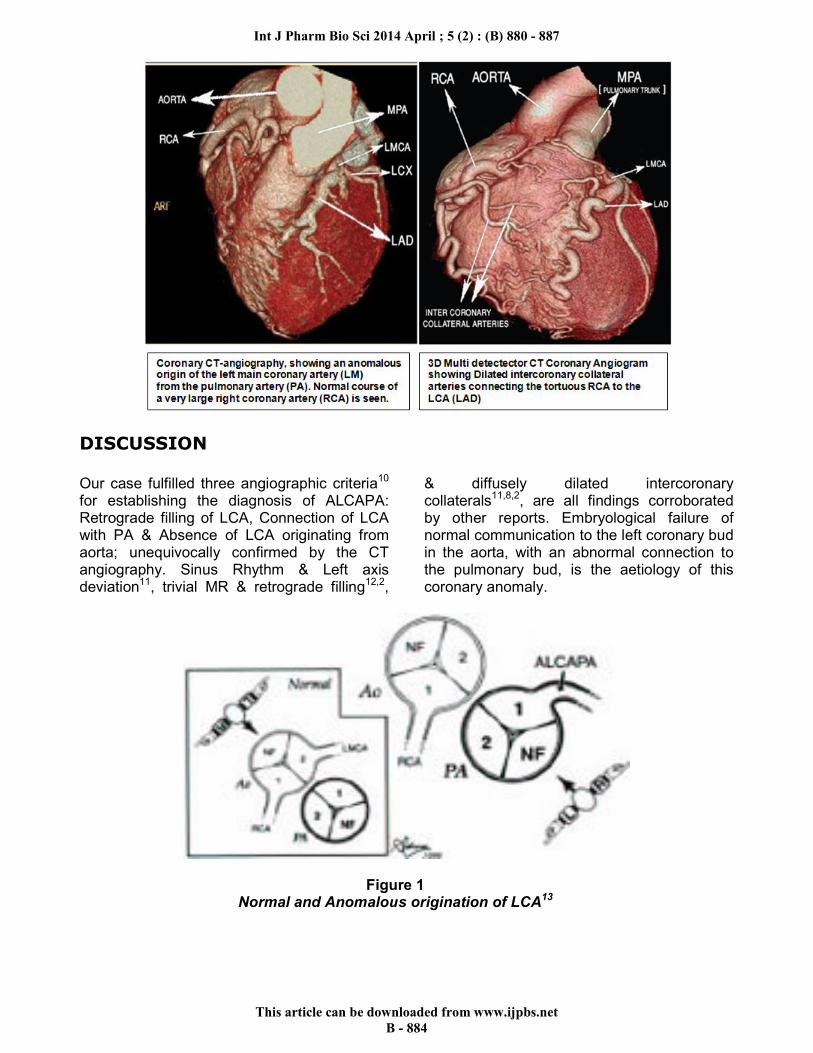
DISCUSSION
Our case fulfilled three angiographic criteria10
for establishing the diagnosis of ALCAPA: Retrograde filling of LCA, Connection of LCA with PA & Absence of LCA originating from aorta; unequivocally confirmed by the CT angiography. Sinus Rhythm & Left axis deviation11, trivial MR & retrograde filling12,2,
& diffusely dilated intercoronary collaterals11,8,2, are all findings corroborated by other reports. Embryological failure of normal communication to the left coronary bud in the aorta, with an abnormal connection to the pulmonary bud, is the aetiology of this coronary anomaly.
Figure 1 Normal and Anomalous origination of LCA13

Int J Pharm Bio Sci 2014 April ; 5 (2) : (B) 880 - 887
This article can be downloaded from www.ijpbs.net
B - 885
The differences between the infant and adult types of ALCAPA syndrome, the importance of developing inter-coronary collateral vessels, and the different clinical manifestations are summarized in the figure below.4
Dilated inter-coronary collateral arteries are seen along the epicardial surface of the heart or within the IVS representing the collateral pathways between the RCA & LCA. LVH & dilation result from chronic myocardial ischemia is seen. ADULT TYPE: As pressure decreases in the pulmonary circulation & as flow reverses in the LCA, the LCA fails to supply the myocardium &“drains” fully oxygenated blood into the main pulmonary artery. There is preferential blood flow into the low-pressure pulmonary circulation rather than into
Int J Pharm Bio Sci 2014 April ; 5 (2) : (B) 880 - 887
This article can be downloaded from www.ijpbs.net
B - 886
the high-resistance myocardial circulation. This left to-right shunt is known as the steal phenomenon. Despite significant collateral circulation from the RCA to the LCA developed to support life upto adulthood, chronic left ventricular sub-endocardial ischemia ensues, & patients may develop malignant ventricular dysrhythmias. These patients are at risk for sudden cardiac death, which occurs in 80%–90% of cases.
INTERVENTION : Types Of Surgical Repair in ALCAPA4
TYPE OF REPAIR DESCRIPTION INDICATIONS
One –coronary system Ligation of the anomalous LCA at the pulmonary origin
Not used anymore
Two –coronary system Coronary button transfer Takeuchi procedure(trans-pulmonary baffling) Placement of a CABG combined with ligation of anomalous LCA.
Direct re-implantation of anomalous artery into the aorta by transferring it with a button of the main pulmonary artery. A baffle made from the pulmonary artery wall is used to tunnel the coronary artery through main pulmonary artery into the left coronary ostium. A venous or arterial bypass graft is placed from aorta to proximal LAD artery, and the anomalous LCA is ligated at its pulmonary origin
Used in infants; the most anatomic correction and yields excellent long-term results. Used in infants when coronary button transfer is not feasible due to unfavourable coronary anatomy. Preferred technique in adults.
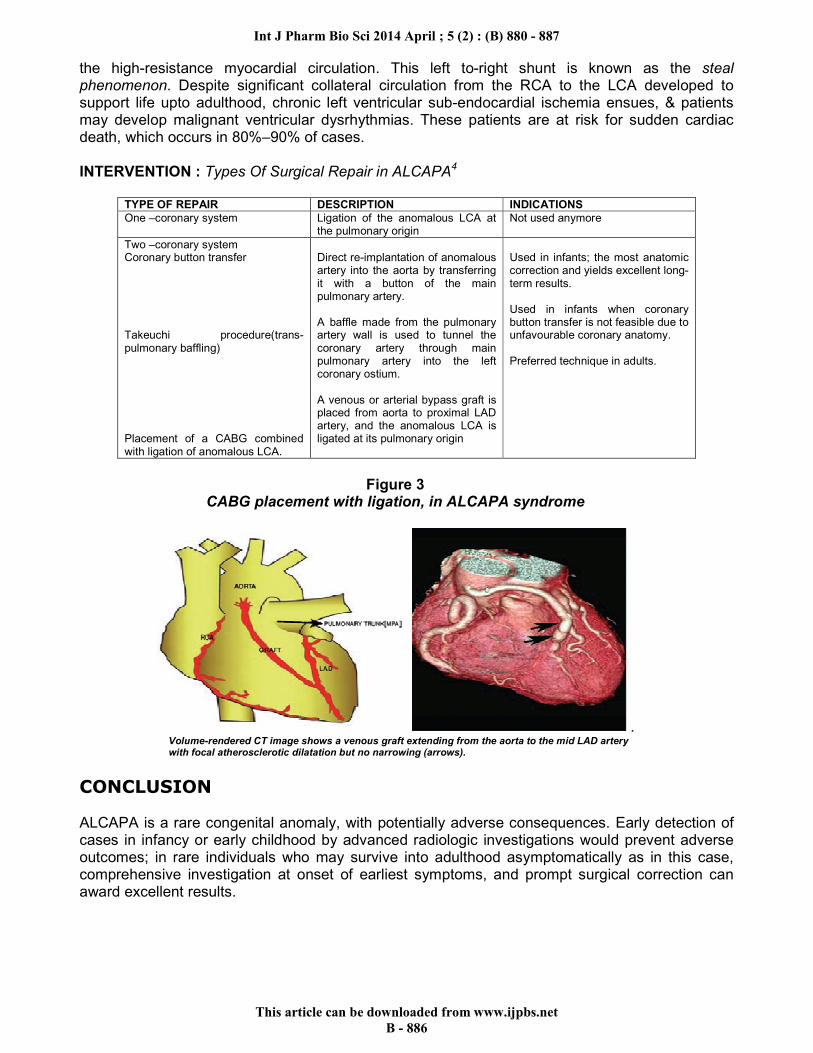
Figure 3
CABG placement with ligation, in ALCAPA syndrome
. Volume-rendered CT image shows a venous graft extending from the aorta to the mid LAD artery with focal atherosclerotic dilatation but no narrowing (arrows).
CONCLUSION
ALCAPA is a rare congenital anomaly, with potentially adverse consequences. Early detection of cases in infancy or early childhood by advanced radiologic investigations would prevent adverse outcomes; in rare individuals who may survive into adulthood asymptomatically as in this case, comprehensive investigation at onset of earliest symptoms, and prompt surgical correction can award excellent results.

Int J Pharm Bio Sci 2014 April ; 5 (2) : (B) 880 - 887
This article can be downloaded from www.ijpbs.net
B - 887
ACKNOWLEDGEMENT
Our sincere thanks to Dr.Y.Shiva Kumar MD,DM (Consultant Cardiologist, ,Dr.Sarat Surapaneni MS,Mch(Cardio Thoracic & Vascular Surgeon),KIMS-Mahaveer Hospital,Hyderabad,for their valuable suggestions and providing clinical material and Mr.Nithin Shakamuri, Odessa High School, Odessa, Texas, for his assistance in acquiring the references for this study.
REFERENCES
1. Cowles RA, Berdon WE. Bland-White-Garland syndrome of anomalous left coronary artery arising from the pulmonary artery (ALCAPA): a historical review. Pediatric Radiology, 37(9): 890-895, (2007).
2. Thomas K, Klaus KF, Steffen H, Morten H, Sondergaard L. Anomalous origin of left coronary artery from pulmonary artery (ALCAPA) presenting with ventricular fibrillation in an adult : a case report. Journal of Cardiothoracic Surgery, 3:33 doi:10.1186/1749-8090-3-33,( 2008).
3. Wesselhoft H , Fawcet JS, Johnson AL. Anomalous origin of left coronary artery from pulmonary trunk: its clinical spectrum, its pathology and pathophysiology based on review of 140 cases with seven further cases. Circulation, 38: 403-25, (1968).
4. Peña E, Nguyen ET, Merchant N, Dennie C. ALCAPA Syndrome : Not Just a Pediatric Disease. RadioGraphics, 29:553–565 (2009)
5. Satpathy M. In: Clinical Diagnosis of Congenital Heart Disease . Jaypee Brothers Medical Publishers(P)Ltd, New Delhi,187(2008).
6. Frank M, Darren RI , Graver LM .128(4_Meeting Abstracts):271 S.doi:10.1378/chest.128.4_Meeting Abstracts.271 S-a. Chest (2005)
7. Separham A, Aliakbarzadeh P. Anomalous left coronary artery from the pulmonary artery presenting with aborted sudden death in an octogenarian : a case
report. Journal of Medical Case Reports, 6 :12,1-3(2012).
8. Selej M. ALCAPA : A rare cause of cardiac arrest. 142(4_Meeting Abstracts):123.A doi:10.1378/chest.1390340, Indiana University, Indianapolis, IN. Chest. (2012)
9. Gaurab M, Saibal R, Somnath G, Bhattacharya S, Kaul A. Management of anomalous left coronary artery from pulmonary artery in an adult patient- A case report. Annals of cardiac anaesthesia,10: 142-144 ( 2007)
10. Culham JAG. Abnormalities of coronary arteries. In: Freedom RM,Mawson JB, Yoo SJ, Benson LN (eds). Congenital Heart disease Text book of angiocardio Graphy. Armonk, NY: Futura Publishing company Inc.,862-66 (1997)
11. Cem B, Oben BS, Baris B, Kutsi K, Hurkan K. Late presentation of anomalous origin of left coronary artery from the pulmonary artery (ALCAPA) : How can clinicians diagnose?.Gulhane Tip Derg, 52:280-282. (2010)
12. Esmaeilzadeh M, Hadizadeh N, Noohi F. Anomalous origin of the left coronary artery from the pulmonary artery(ALCAPA) in an old adult. J Teh Univ Heart Ctr, 6(3):148 – 151 (2011)
13. Mancini MC. In: Anomalous Left Coronary Artery From the Pulmonary Artery , Chief Ed: Neish SR, http://emedicine.medscape.com/article / 893290 - overview
14. Childrens Hospital Boston, http://www.childrenshospital.org/





























