Embed Size (px)
Citation preview

Laboratory investigation of platelet function disorders
Sara Israels MD, FRCPC Professor, Dept. of Pediatrics and Child Health Senior Investigator, Manitoba Institute of Cell Biology University of Manitoba Director, Hemostasis Laboratory, Health Sciences Centre Winnipeg, Canada
International Society of Laboratory Hematology, May 2015

Objectives 1. To develop an approach to
investigation of platelet disorders 2. To understand the utility and limitations
of commonly used platelet function assays
3. To consider the future of diagnostic testing for platelet disorders

(Harrison, Blood Rev 2005; 19:111)
In vivo activation

Prevalence of platelet function disorders: • There are no population-based studies. • Prevalence studies hampered by: • Access to testing • Comprehensiveness of testing: heterogeneity of
disorders • Quality of testing: standardization and interpretation
Registry Data UK registry (2012): 1575 PD
9377 VWD Canadian registry (2014): 802 PD
3963 VWD

Quiroga et al. Haematologica 2007;92:357 280 bleeders and 299 controls Clinical histories and bleeding scores Bleeding times VWD testing, clotting factor testing Platelet aggregation and secretion studies Clot lysis assays RESULTS in 280 patients VWD 17.9% PFD 23.2% Factor deficiencies 3.9% BT prolonged 18.6% No laboratory abnormality 36.4%
RESULTS in 299 controls 2.5% had decreased VWF 7% had decreased platelet aggregation or secretion
Prevalence of platelet function disorders:

Pre-pre-analytical variables: Does the patient require testing?
• Why are you testing?
• Patient and family history – Clinical associations
• Medication history – Can the patient stop their
medication? – Should the patient stop their
medication?
Healthy Individuals (n > 700)
Prevalence (%)
Epistaxis 5-11 Menorrhagia 17-44 Dental bleeding 5-11 Hematomas 12 Gum bleeding 7-37 Post-surgical bleeding 1-6 Post-partum bleeding 3-23 Joint bleeding 6
(Rydz & James, JTH 2012)

Bleeding assessment tools Does the patient require testing?
• Standardized questionnaires to: 1. Improve diagnostic accuracy 2. Predict bleeding risk 3. Describe symptom severity – Which BAT to use?
• Global bleeding symptom BATs • Focused BATs (eg, menorrhagia, pediatric)
– Can we use them as a screening tool to know who we should be testing?
• Maybe. Very good NPV. – Can they direct us to the specific diagnosis?
• No. Poor specificity. Rodeghiero et al, JTH 2010 Rydz & James, JTH 2012 Lowe et al, JTH 2013

Laboratory testing for PFD Gresele et al. J Thromb Haemost 2014;12:1562 • Global survey of 202 laboratories in 37 countries • 14,000 patients investigated yearly: PFD identified in 40%
Initial laboratory testing

Global tests of hemostasis
Bleeding Time Platelet Function Analyzer
Invasive Poorly reproducible Not specific Poor sensitivity for common PFD
Simple Reproducible Not specific Even less sensitive to common PFD

CBC and blood film
• Platelet count • MPV • Blood film

(www.youtube.com/watch?v=0pnpoEy0eYE)
In vivo activation
!!
(Rand, Israels, McNicol, 2010)

Light transmission aggregometry (LTA)
(Jackson, Blood 2007;109:5087)

Platelet aggregometry
• Lack of standardization – Surveys of existing practices: 2005-2012
Issues that required attention: 1. Patient screening
2. Collection and sample preparation
3. Agonist panel and concentrations
4. Laboratory specific reference intervals and controls 5. Interpretation of results 6. Quality assurance/EPT

• Clinical and Laboratory Standards Institute: Christie et al. Platelet function testing by aggregometry: approved guideline. www.clsi.org 2008
• NASCOLA: Hayward et al. Development of NA consensus guidelines for medical laboratories that perform and interpret platelet function testing using light transmission aggregometry. AJCP 2010
• British Committee for Standards in Haematology: Harrison et al. Guidelines for the laboratory investigation of heritable disorders of platelet function. BJH 2011
• ISTH Platelet Physiology Subcommittee: Cattaneo et al. Recommendations for the standardization of light transmission aggregometry. JTH 2013
Standardization recommendations and guidelines:

Pre-analytical variables • Instructions for patients on day of collection • Pre-collection medication questionnaire • Sample collection • Sample transport/handling • PRP/PPP preparation and quality assessment • Standardization of the platelet count
– ISTH SSC Survey 2009 results showed that 95% of clinical laboratories adjusted the platelet counts in PRP.
– Recent studies show that there is no advantage to adjusting PRP platelet counts and addition of autologous PPP may inhibit aggregation.
– Published guidelines provide contrary advice on adjustment of platelet counts.

Analytical variables • Standard settings for temp, rpm, etc • Baseline tracings should be observed
for oscillations and stability before the addition of agonists
• LTA should be completed within 4 hours of collection of the sample.
• Comparison with normal controls • A basic testing panel with single
concentrations of standard agonists – Published guidelines give a range of
recommended agonist concentrations
• Laboratory-determined reference intervals for % maximal aggregation for each agonist and concentration
178 Am J Clin Pathol 2005;123:172-183178 DOI: 10.1309/Y9EC63RW3XG1V313
© American Society for Clinical Pathology
Zhou and Schmaier / PLATELET FUNCTION TESTING
Normal values for collagen and arachidonic acid in our labo-ratory are shown in Table 1.
Thrombin-Induced Platelet AggregationThrombin activates 2 receptors on platelets, PAR1 and
PAR4. However, the activation of these receptors is not seenspecifically in an aggregometer tracing. There is little pub-lished clinical experience of the use of !-thrombin to assessplatelet activation in patient samples. !-Thrombin activatesplatelets in PRP by proteolyzing PAR4 and PAR1. The amountof !-thrombin necessary to induce threshold platelet activationvaries by the preparation of !-thrombin and the individual’splatelets. Platelet aggregation in response to low and high con-centrations of !-thrombin is shown in !Image 4!. In Image 4(left), a 57 nmol/L concentration of human !-thrombin wasinsufficient to induce platelet aggregation, although it inducedshape change on binding. Alternatively, in Image 4 (right), theinstillation of a 114 nmol/L concentration of !-thrombin (indi-cated by “2”) induced a shape change (indicated by “3”), fol-lowed by a single wave aggregation curve (indicated by “4”).
Ristocetin-Induced Platelet AggregationTwo concentrations of ristocetin were used to determine the
presence and integrity of GPIb"-V-IX complex on platelets andvWF in the PRP !Image 5!. All normal platelets should respond
to 1.2 mg/mL of ristocetin (Image 5, left) but not to 0.6 mg/mL(Image 5, right). The tracing seen with the addition of the high-er concentration of ristocetin actually is initially platelet-plateletagglutination, which on close contact induces intracellularplatelet activation and subsequent platelet aggregation.
Normal Platelet Function StudiesThe mean values and range for aggregation and secretion
for each of the platelet agonists is shown in Table 1. The meanagonist concentration that initiates primary and secondarywave aggregation (ie, threshold concentration) is given forADP and epinephrine (Table 1). The threshold concentrationfor primary and secondary wave aggregation with ADP isquite narrow in a healthy population, usually from concentra-tions of 1 to 7.5 µmol/L (Table 1). The range of concentrationsof epinephrine to induce both primary and secondary waveaggregation was wide, from 0.5 to 10 µmol/L (Table 1).
The range of 14C-serotonin secretion for ADP and epi-nephrine at threshold second wave aggregation is given. Theselatter values are clinically useful because not infrequently, onecannot see the inflection of secondary wave aggregation withADP. Knowing that the level of secretion is within the normalrange at an agonist concentration between 1 and 7.5 µmol/Lindicates that secondary wave aggregation must have occurredbecause ADP induces aggregation-dependent secretion.7
Ligh
t Tr
ansm
issi
on
12
3
4
2 min
12
3
4
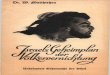
!Image 3! Collagen-induced (left) and arachidonic acid–induced (right) platelet activation. Platelet aggregation in response tocollagen (5 µg/mL) is characterized by a prolonged lag phase between the addition of the collagen, a spike to the left of “2,” andshape change, to the left of “3.” A single wave response is shown below “4.” “1” represents the stabilization of the baseline.Platelet aggregation in response to arachidonic acid (500 µg/mL) is shown after stabilization of the baseline, indicated by “1.” Theinstillation of the agonist arachidonic acid is indicated by the spike to the right of “2.” The induction of shape change is to the leftof “3,” and the single wave aggregation response is shown by the curve labeled “4.” These images are representative ofcollagen- and arachidonic acid–induced platelet aggregation, respectively.
Agonist Conc. Epinephrine 5 µM ADP 2.5 µM Collagen 1.5 µg/mL Arach. Acid 1 mM U46619 1 µM Ristocetin 1.2 mg/mL
0.5 mg/mL
(Zhou & Shmaier, AJCP 2005)

Agonist panels
(Rand, Trans Apher Sci 2003; 28:307) (from Yee, Blood 2005;106:2723)
ADP aggregation in normal controls
• Extended agonist panels are not clearly better than streamlined panels of LTA agonists
• Testing algorithms • Interpretation
Hayward et al, JTH 2009 Dawood et al, Blood 2012

Diagnostic Value of LTA • Goal: to distinguish PFD from no PFD • Studies evaluating diagnostic utility of LTA
– Consensus on definition of patients vs. controls – Additional laboratory information in defining the patients vs
controls – Agonist panels and definition of abnormal results
• LTA alone will not identify all patients with PFD • The most useful additional test is a measure of granule
secretion
Hayward et al, JTH 2009 Quiroga et al, Br J Haematol 2009 Pai et al, Am J Clin Pathol 2011 Dawood et al, Blood 2012
NOT for the evaluation of antiplatelet therapy

Investigating platelet secretion defects
ADP epinephrine collagen
Frequently, but not always demonstrate abnormal LTA
The frequency of release abnormalities in the setting of normal LTA results varies across studies from 14.3% to 56%.
ADP
Agonist
ATP release assay measures DG secretion
Agg
rega
tion
Lum
ines
cenc
e
ATP + D-luciferin + O2 AMP + PPi + oxyluciferin + CO2 + light

• Not all guidelines address secretion assays • Evidence for improved sensitivity for diagnosis PFD
when LTA and secretion assays are combined. • How to best use secretion assays:
– Should all patients have secretion assays done in conjunction with LTA?
– Should patients with LTA results suggestive of a secretion defect have secretion assays done?
– Should patients with normal LTA but a high pre-test probability of PFD have secretion assays done?
Investigating platelet secretion defects

Investigating platelet secretion defects
DG quantification by EM whole mount, mepacrine labeling, biochemical measures of ATP/ADP, or 14C-serotonin uptake.
ADP
Agonist
Release defect or DG deficiency?

2012-1 NASCOLA Platelet Dense Granule Proficiency Challenge!! "#$%!&!!
!
! !"#$%&'%%
! "#$!%&'!(#))#*+,-!.!')'/%$#,!0+/$#1/#23!+04-'15!2)'41'!+,6+/4%'!7()*+!3#8!*#8)6!4-$''!+%!+1!4!6',1'!-$4,8)'!#$!7,-+!3#8!*#8)6!,#%!4-$''!+%!+1!4!6',1'!-$4,8)'!(#$!%&'!,809'$'6!1%$8/%8$'1:!
;)'41'!',%'$!3#8$!$'12#,1'1!81+,-!%&'!(#))#*+,-!<8$='3>#,?'3 !)+,?@!!!
&%%2@AA***:18$='30#,?'3:/#0A1ABCD"EFG!
!
! H04-'!I@!
!
!
!
!
!
JK<GLMK!N)'/%$#,!>+/$#1/#23!B',1'!O$4,8)'!G&4))',-'!
PQIPRI!
!
I!
P!S!
.!
T!
U!
V!IQ!
W!
C!
II!
IS!
I.!
IP!
IV!
External proficiency testing • An additional challenge
– College of American Pathologists (CAP) o Platelet Function Analyzer o LTA
– NASCOLA o Interpretation of aggregation tracings
– Case-based
o Dense granule enumeration – Electron micrographs
Hayward et al, Sem Thromb Hemost 2012

Flow cytometric analysis RESTING ACTIVATED
CD62P αIIbβ3
GPIb-IX-V
Fibrinogen ö CD63
α-granules
CD62P αIIbβ3
GPIb-IX-V δ-granules
CD63
• Membrane receptors • Dense granule enumeration
• Platelet activation • Granule exocytosis • Fibrinogen binding • Procoagulant surface development • Microparticle release
PS

Other platelet function tests
PlaCor, Inc
Roche Diagnostics
Accumetrics
Haemonetics

The role of genetic testing
• THE BAD NEWS: The combination of clinical assessment, and laboratory evaluation still leaves approximately 50% of patients with evidence of a platelet disorder without a specific diagnosis.
• THE GOOD NEWS: Characterization of molecular defects in recognized disorders and in previously unrecognized disorders is advancing, aided by powerful and efficient genomic analysis.

Clinical utility of genetic testing? It depends on what you have:
1. Well characterized syndromic conditions with known genetic cause
2. Well characterized pedigree with definitive phenotype
3. Everybody else
Genetic variation and platelet phenotype • SNP associations with platelet count, volume or
reactivity • Multiple SNPs associated with one trait • Identified loci not previously known to be associated
with platelet traits

Summary 1. Platelet disorders are common; diagnostic evaluation is
a challenge. 2. Screening assays are neither sensitive nor specific;
BAT may more helpful in determining who requires further investigation.
3. Aggregometry and secretion assays are the most useful functional assays for the clinical laboratory but will still leave a portion of patients without a definitive diagnosis.
4. Improved understanding phenotype-genotype relationships will move us towards clinically useful genetic diagnostics.