Embed Size (px)
Citation preview
Intervention
Interventions• Conservative observation• Dissolution agents• Relief of Obstruction• Extracorporeal Shockwave Lithotripsy (ESWL)• Ureteroscopic stone extraction• Percutaneous Nephrolithotomy• Open stone surgery• Pyelolithotomy• Anatrophic Nephrolithotomy• Radial Nephrotomy• Ureterolithotomy• others
Conservative management• Majority of stones pass out within a 6 week period after
the onset of symptoms• depends on the size of the calculi and its location
Dissolution agents• Use alkalinizing agents• Given oral, IV or intrarenal
Relief of the Obstruction• Emergent drainage in patient with signs of UTI
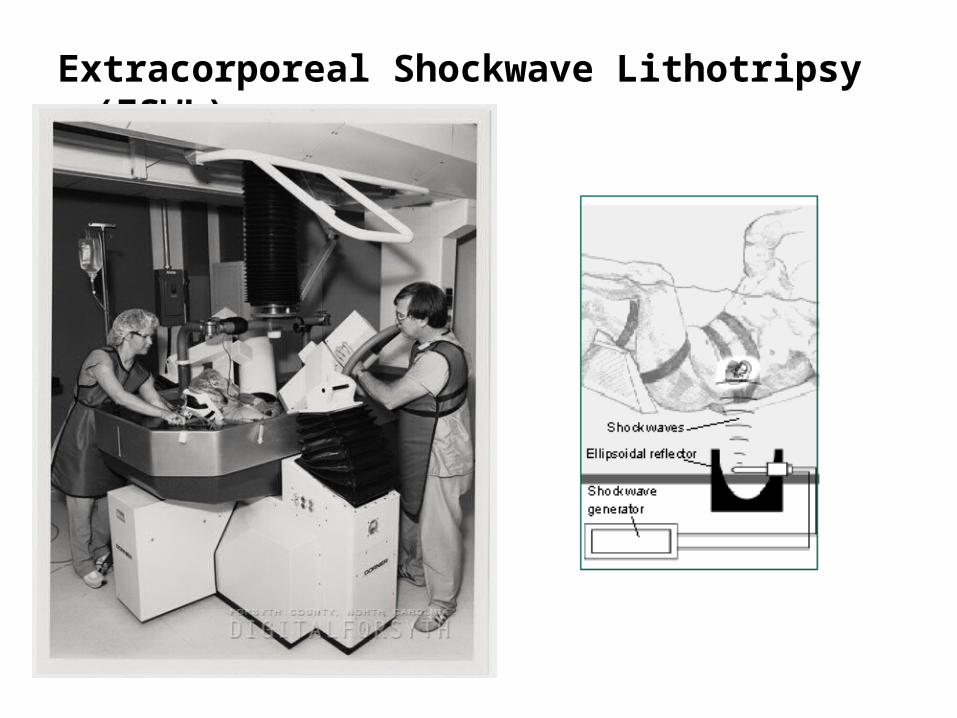
Extracorporeal Shockwave Lithotripsy (ESWL)
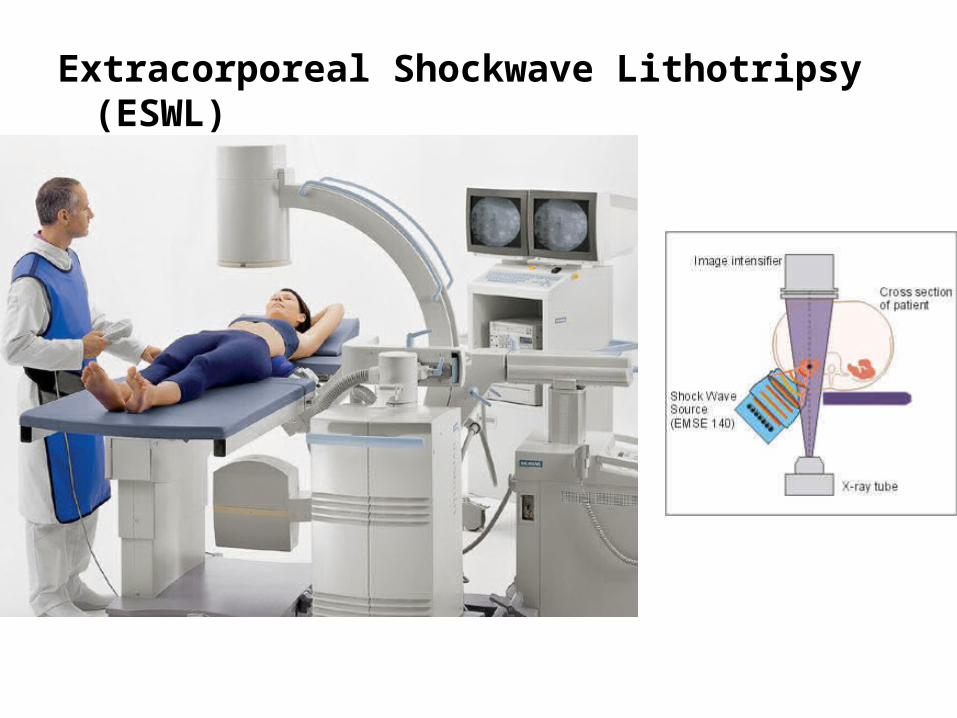
Extracorporeal Shockwave Lithotripsy (ESWL)
• excessive weight (>300 lb) may severely limit or preclude ESWL.
• Pregnant women and patients with large abdominal aortic aneurysms or uncorrectable bleeding disorders should not be treated with ESWL.
• Individuals with cardiac pacemakers should be thoroughly evaluated by a cardiologist.
Consideration
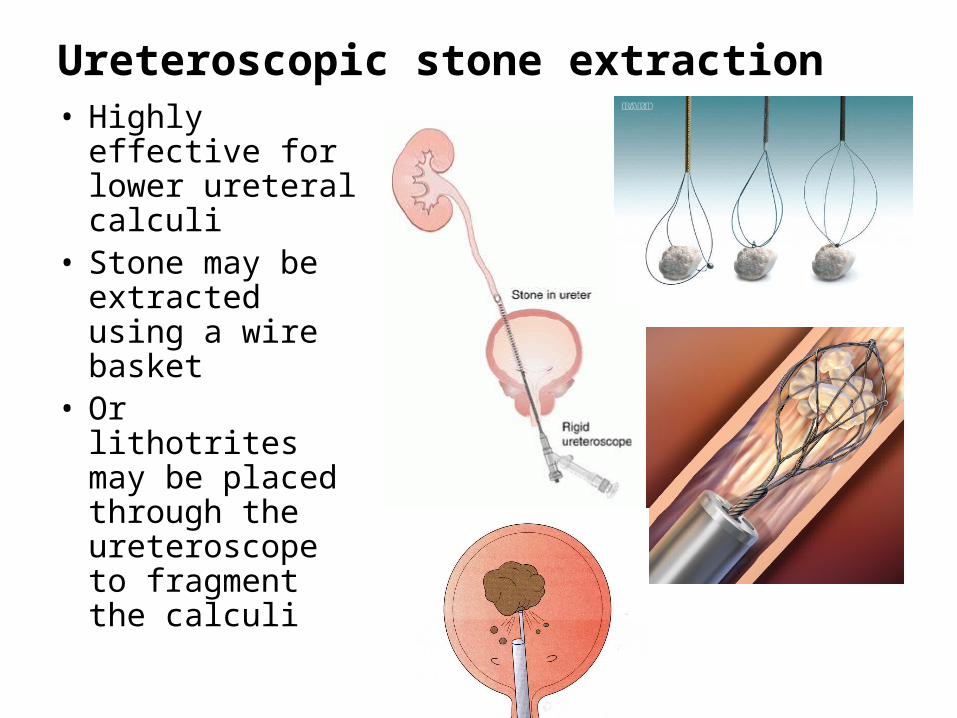
Ureteroscopic stone extraction• Highly effective
for lower ureteral calculi
• Stone may be extracted using a wire basket
• Or lithotrites may be placed through the ureteroscope to fragment the calculi
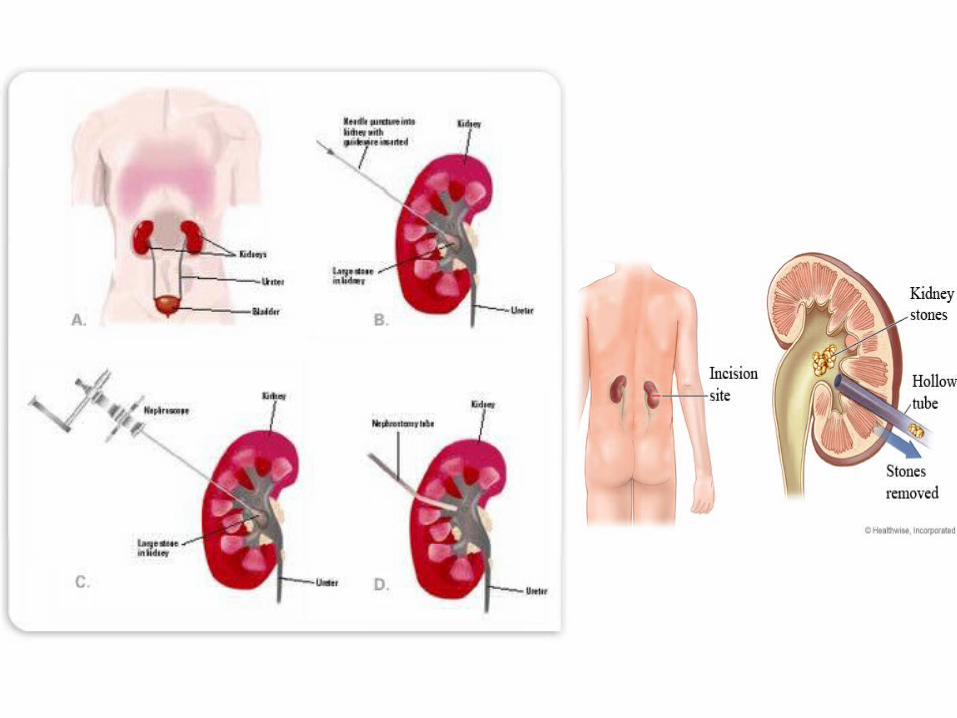
Percutaneous Nephrolithotomy
• the treatment of choice for large (>2.5 cm) calculi; renal and proximal ureteral calculi, those resistant to ESWL, select lower pole calyceal stones with a narrow, long infundibulum and an acute infundibulo- pelvic angle, and instances with evidence of obstruction
• Rapid cure
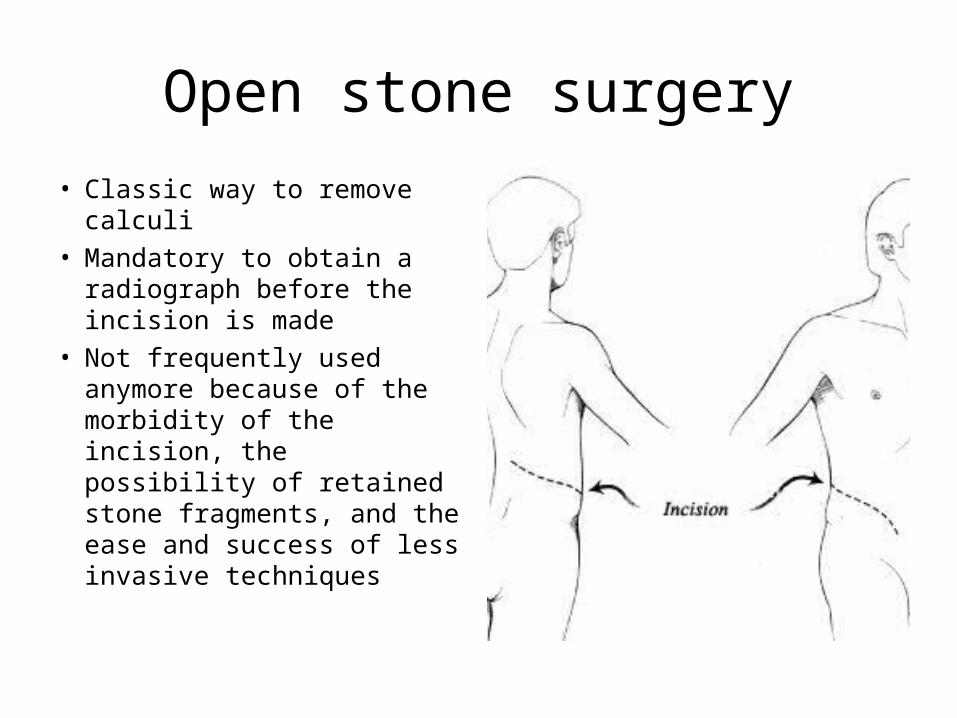
Open stone surgery• Classic way to remove
calculi• Mandatory to obtain a
radiograph before the incision is made
• Not frequently used anymore because of the morbidity of the incision, the possibility of retained stone fragments, and the ease and success of less invasive techniques
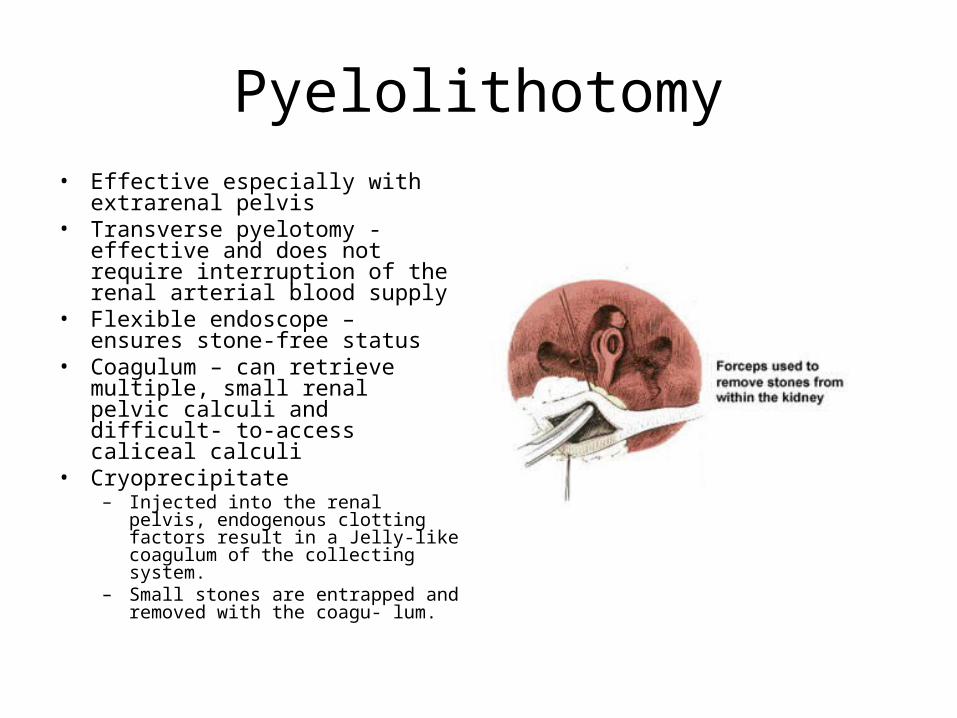
Pyelolithotomy• Effective especially with extrarenal
pelvis• Transverse pyelotomy - effective
and does not require interruption of the renal arterial blood supply
• Flexible endoscope – ensures stone-free status
• Coagulum – can retrieve multiple, small renal pelvic calculi and difficult- to-access caliceal calculi
• Cryoprecipitate – Injected into the renal pelvis,
endogenous clotting factors result in a Jelly-like coagulum of the collecting system.
– Small stones are entrapped and removed with the coagu- lum.
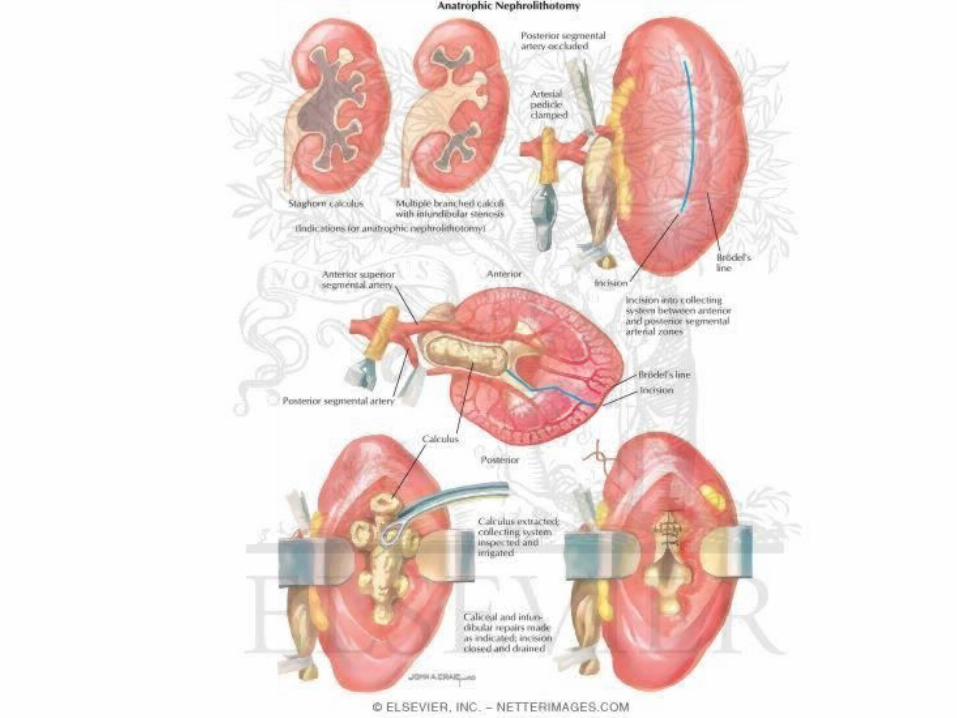
Anatrophic nephrolithotomy• Used with complex staghorn calculi
– Complete staghorn calculus– Partial staghorn calculus
1.Incision made on the convex surface of the kidney posterior to the line of Brodel
2.Occlusion of the renal artery followed by renal cooling with slushed ice
3.Nerve hook is helpful to tease out calculi4.Repair of narrowed infundibula helps reduce
stone recurrence rates.
Radial nephrotomy
• Allows access to limited calyces of the collecting system
• Frequently used in blown-out calyces with thin overlying parenchyma
• Intraoperative ultrasound to localize the calyx and the calculi
• A shallow incision of the renal capsule can be followed by puncture into the collecting system.
• Stones may be cut with heavy Mayo scissors, and remaining fragments can be retrieved.
Other renal procedures
• Partial nephrectomy – for large stones in a renal pole with marked parenchymal thinning– Caution should be taken even with a normal
contralateral kidney as stones are frequently associated with a systemic metabolic defect that may recur in the contralateral kidney
• Ileal ureter substitution – to decrease pain with frequent stone passage
• Autotransplantation with pyelocystostomy – for patients with rare malignant stone disease
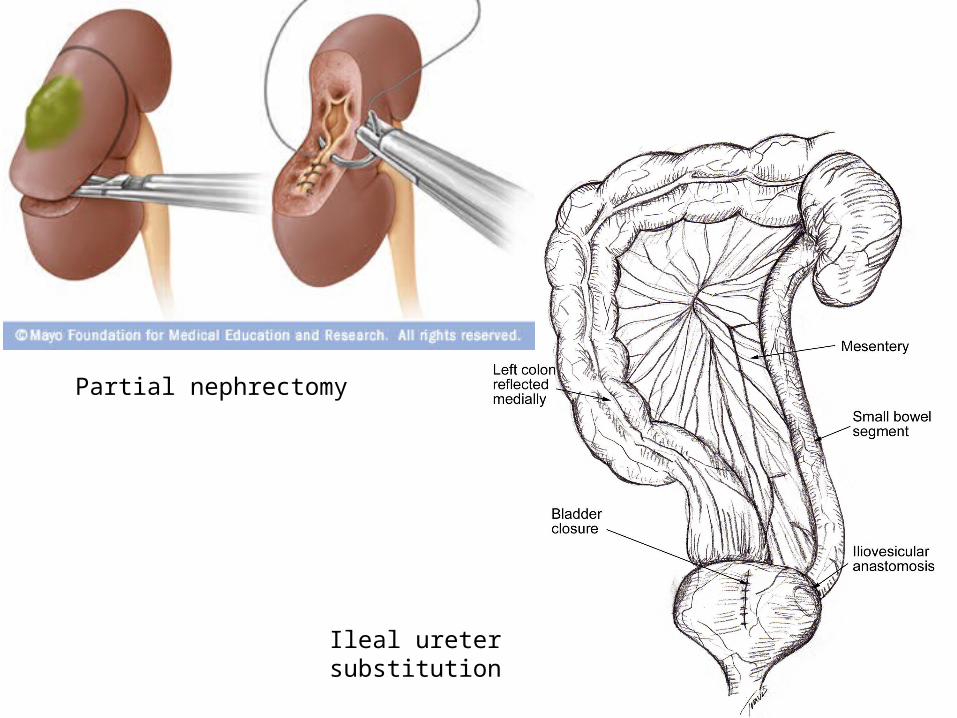
Partial nephrectomy
Ileal ureter substitution
Ureterolithotomy
• Long standing ureteral calculi1. Preoperative radiograph to document stone location
2. Incision lateral to the sacrospinalis muscles to allow medial retraction of the quadratus lumborum; anterior fascicle of the dorsal lumbar fascia must be incised to gain proper exposure
3. Vessel loop or Babcock clamp placed proximal to the stone to prevent frustrating stone migration
4. Longitudinal incision over the stone with a hooked blade to expose the calculus
5. Nerve hook to tease out the stone





























