Embed Size (px)
Citation preview

VIVA 2008 ( Las Vegas, NV)September 22nd 2008
1 AP2928021 Rev A
Carotid stenting is not currently approved by the FDA for asymptomatic patients who are at standard risk for surgery.CAUTION: Investigational device. Limited by Federal (or United States) law to investigational use.Confidential: This information is confidential and is intended for distribution to ACT I Study Site participants ONLY. This document contains Abbott Laboratories and Abbott Vascular proprietary information and shall not be duplicated, disclosed to others, or used for purposes other than to carry out the intent for which this material is delivered.©2008
Asymptomatic Carotid stenosis, stenting versus endarterectomy Trial
Update on ACT IAlex Abou-Chebl, MD

SymptomaticHigh-risk
Symptomatic
Standard-risk
Asymptomatic
Standard-risk
Asymptomatic
High-risk
Asymptomatic Carotid Artery Disease RCT’s: CAS vs. CEA
CRESTACT 1, SPACE 2
ongoing

VIVA 2007 ( Las Vegas, NV)September 25th 2007
ACT I: Study Design
•Prospective, randomized, 2-arm, multicenter trial
•3:1 randomization CAS to CEA
•Lead-in enrollment of up to 400 subjects
•Maximum of 1658 pivotal subjects
•Followed at 1, 6, 12 months & annually for 5 yrs
•Contemporary medical therapy for all patients

4
ACT I: Primary Endpoint
• Composite of Death, Stroke, MI at 30 days post procedure
PLUS
• Ipsilateral Stroke from 31 to 365
days post procedure

5
ACT I: Secondary Endpoints• Death (years 2-5)
• Ipsilateral stroke (years 2-5)
• Composite Morbidity Measure: Cranial nerve injury, bleeding, vascular and/or wound complications requiring treatment, complications of general anesthesia, access artery, renal and airway complications
• Freedom from clinically-indicated target lesion revascularization (TLR) at 6 and 12 months
• Acute stent success: Residual stenosis < 50% by QCA covering an area no longer than original lesion
• Acute filter success: Successful deployment and retrieval of filter in absence of angiographic distal embolization.
• Procedure success: Residual stenosis < 50% by QCA and freedom from Major Adverse Event at 30 days

VIVA 2007 ( Las Vegas, NV)September 25th 2007
ACT 1 (vs. CREST)Patients
• Asymptomatic only– powered to look at them independently
• Lesion criteria– Stenosis > 70%
– DUS velocities higher
• NO Octogenarians
• Emphasis on case selection…avoidance of patients not
good for both therapies
• Encouragement to cross over if CAS/CEA not appropriate
(more about the patient than proving the therapy)

VIVA 2007 ( Las Vegas, NV)September 25th 2007
ACT 1 (vs. CREST)Investigators
• SMC and IMC highly “selective”– Actual case angio reviews (IMC)
• Later in experience curve of stenting– Optimal case selection
– Operator experience more comparable to surgeons doing CEA
• Ongoing review of outcomes: Trigger for MAE that are
well beyond expected event rates• Enrollment expectations…Probation and termination of
non-enrolling sites/investigators• Fewer # study sites, all high-quality

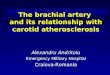
The influence of experience
* Hierarchical Events – Includes only the most serious event for each patient and includes only each patient’s first occurrence of each event.
All stroke/death*
Level I CAPTURE: n= 210
EXACT: n= 267 CAPTURE 2: n=83
Level 2 CAPTURE: n= 1879 EXACT: n=776 CAPTURE 2: n=1026
Level 3 CAPTURE: n=735
EXACT: n=482 CAPTURE 2: n=318
Asymptomatic patients <80 years
2.5%
3.4%3.8%
0%
1%
2%
3%
4%
5%
6%
7%
8%
Str
oke
Dea
th r
ates
Avoiding the Eva3S debacle!

VIVA 2007 ( Las Vegas, NV)September 25th 2007
ACT 1 (vs. CREST)Devices
•Devices: – Xact stent (closed cell) with Emboshield/Embo-pro
Vs
– Acculink (open cell) with Accunet

Carotid Stents - open vs closed cell?Stent cell area
Houdart E, CIRSE 2006
closed closed open open open closed openStentDesign:
Cell area (mm2)

Tortuous ICA: • 90 degree take-off• 120 degree prox.
turn
Excessive TortuosityHeavy concentric Ca++
Excluded from ACT I

VIVA 2007 ( Las Vegas, NV)September 25th 2007
ACT 1 vs. CRESTConduct of trial- adjuvant therapy
•Emphasis on Optimal Medical Therapy– Mandatory monitoring of Hgb-A1C, cholesterol, etc.

VIVA 2007 ( Las Vegas, NV)September 25th 2007
ACT 1 vs. CREST
• Industry sponsored and monitored
vs.
•NIH Trial

VIVA 2007 ( Las Vegas, NV)September 25th 2007
ACT 1 Reasons to pursue and complete
• Need for accrual of as much “clean” data as possible– To achieve scientific goals– To validate or invalidate the therapy as viable option for
patients for the future• CREST not comparable• No similar trial is likely to happen in the future• ACT I is unmatched in its scientific rigor and sets the
standard for CAS trials• Determine merits of CAS vs. CEA on scientific, evidence-
based grounds (not political or economic)

15
Enrollment Update
As of 13 Jan 2010:– Total Randomized Subjects: 980– Total number of lead-ins to date: 176– Total number of sites initiated: 53

VIVA 2007 ( Las Vegas, NV)September 25th 2007
William Beaumont Hospital
St. John’s Hospital / Prairie Medical Millard Fillmore Hospital
Lenox Hill Hospital
Riverside Methodist Hospital
St. Mary’s Hospital/ VA Cardiovascular Specialists
Duke University
El Camino Hospital Washington Hospital Center Northwestern University Memorial Hospital
Berks Cardiology
Harrisburg Hospital / Pinnacle Health
Cleveland Clinic Foundation
Hoag Memorial Hospital Presbyterian
Presbyterian Heart Institute-Dallas
Oregon Health & Science University
Parkview Hospital
North Central Heart Institute Detroit Medical Center
Baptist Hospital of East Tennessee
BCVI
Forsyth Medical Center
Ochsner Clinic Foundation
Massachusetts General Hospital
Deaconess Medical Center
St. Joseph Hospital Wellness Center
Albany Medical Center
St. Luke’s Episcopal Hospital, Houston
Columbia Presbyterian
Rush University Medical Center
Cardiovascular Inst. of the South
Austin Heart P.A.
Wake Medical Center
Kaiser Foundation Hospital – San Diego
NYU Medical Center
St. Luke’s Hospital, Phoenix
Westlake Medical Center
Dartmouth Enrolling Sites as of September 2009
Kaiser Permanente Hawaii
University of Rochester
St. Francis, NY
Providence Medical Center
Our Lady of Lourdes
Allegheny General Hospital
Chesapeake General Hospital
Hospital of Univ. of Pennsylvania
St. Luke’s Milwaukee
Stern Cardiovascular Center
Wellmont Holston Valley
St. John’s Mercy
Heritage Valley

VIVA 2007 ( Las Vegas, NV)September 25th 2007
ACT I: Primary Endpoint
•Composite of Death, Stroke, MI at 30 days post procedure
PLUS
• Ipsilateral Stroke from 31 to 365 days post procedure

VIVA 2007 ( Las Vegas, NV)September 25th 2007
Independent Clinical Events Committee (CEC)
•Reviews and adjudicates the following events:– Cause of Death through 30 days (Attempt to determine if neurological,
cardiac, other)– Suspected Stroke (All through 30 days, Ipsilateral between 31 days and 365
days (post-procedure)– Suspected MI (All suspected Q wave and non-Q wave through 30 days of
procedure)

VIVA 2007 ( Las Vegas, NV)September 25th 2007
Analysis Cohort
•Patient cohort analyzed:
ACT I Lead In, n=160 as of June 30, 2009
•Analysis cohort includes:– patients with 30 day follow-up visits or
event(s) within 30 days (n=160).– Patients with 1 year follow-up visits or
event(s) within 1 year (n=146).

VIVA 2007 ( Las Vegas, NV)September 25th 2007
Procedural and Device Success
• Procedural Success- 98.1% (157/160)
• Acute Xact Success- 97.5% (159/163)
• Emboshield Success- 99.4% (160/161)

VIVA 2007 ( Las Vegas, NV)September 25th 2007
ACT I: Outcomes Lead In Patients
Event 30 days, N=160
Death, Stroke and MI 1.3% (2/160)
All Stroke and Death 1.3%
Major Stroke and Death 0.0%
Death 0.0%
All Stroke 1.3%
Major Stroke 0.0%
Minor Stroke 1.3%
MI 0.0%
31-365 days, N=146
Ipsilateral Stroke 0.0%

CREST Lead-In Phase
•Up to 20 patients per interventionist•Non-randomized N =1246
– Low and High-CEA risk– 65% Asymptomatic
•30-Day Stroke/Death – Asymptomatic 3.1%– Symptomatic 4.3%– Combined 3.9%– Age>80 12.1%

VIVA 2007 ( Las Vegas, NV)September 25th 2007
Summary
•ACT I is a randomized trial comparing patients at standard risk for CEA and CAS
•Lead-in data suggests CAS event rates comparable to CEA
•Results from ACT I will, more than any trial to date, determine the role of CAS
•Patients, physicians, CMS, other payers will make therapeutic decisions based on results of ACT I

Poor Stent Candidates