Embed Size (px)
Citation preview

Interventional Pain Management:
Not All Injections are Created Equal
Craig W. Davis, MDGranger Pain & Spine
President UTSIPP
Vice-President UAPM

Disclosures
Conultant/Faculty with Stryker
Interventional Spine
Consultant/Faculty with St. Jude/Abbott
Neuromodulation

Objectives
1) Identify and evaluate the options for interventional
treatment as they pertain to the low back
2) Identify and evaluate the options for interventional
treatment as they pertain to the neck
3) Identify the basic tenets of advanced interventional pain
procedures
4) Identify when a referral is warranted

Common Types of Low Back Pathology
1)Myofascial Pain
2)Facet mediated pain
3)Disc Mediated pain: herniations, annular tears, discogenic
4)Sacroiliac Dysfunction

Myofascial pain
Pain localized to paraspinal
musculature & PSIS
Spasm probable
Limited flex. & ext. (pain)
No radiating pain
May not correlate to specific
mechanism
--Treatment options, PT, NSAIDs,
muscle relaxants, TPIs, CBT

Facet Mediated Low Back Pain
~40% of all LBP
Vague symptoms that mimic
other pathologies
Localized pain
Often improves with activity
Nerve entrapment may result
from compensatory posturing
Worsened by:
Repeated spine-loading activities (ext,
side bending, rotation)
Poor LE flexibility
Poor Trunk strength
Tenderness over facet joint

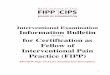
Facet Mediated Referral Patterns

Facet Mediated Pain Treatment
1) Exhaust Conservative care: NSAIDs, MRs, SNRI/SSRI,
PT, acupuncture, CBT, etc
2) Interventional treatment:
1) Facet Injection
2) MBB/RFA
1) Potential for longer duration of relief

Lumbar Disc Lesion
Crack in annulus fibrosus herniation of
nucleus pulposus
Pressure on nerve rootpain/burning
sensation
“Bulge” pathology
Radiating pain into buttocks and down leg
MRI for best diagnosis
Altered standing posture
Symptoms with activity
Bilateral or unilateral symptoms
Usually acute onset

Lumbar Disc Lesion, cont.
herniated disc
radiating leg pain > back pain
pain ↑ sitting & leaning forward, coughing,
sneezing, & straining
neurologic deficits are usually present
+ ipsilateral straight leg raising test
annular tears
back pain > leg pain
pain ↑ sitting & leaning forward, coughing, sneezing, & straining
may have muscle spasm and loss of lordosis
+ ipsilateral straight leg raising test

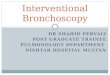
Dermatome Map

Epidural Steroid Injection
Injection of the corticosteroids as close to the nerve as
possible – TO REDUCE SYPTOMS DUE TO
INFLAMMATION / OR SENSITIVITY
Multiple studies – suggest that surgery can be avoided in
upto 75% cases
Compression of the disc may continue in spite of resolution
of symptoms following ESI

Steroid – How it helps???
• Anti inflammatory
• Reverses effect of inflammatory mediators, Stops
inflammation cascade, Helps in healing annular
tear
• Reduces edema – improves micro circulation
• Reduce ischemia – reduce hypersensitivity of
dorsal horn cells

Steroid – How it helps???
• Direct inhibition of C-fibers neuromembrane excitation
• Stabilizes cell membrane
• Interact with 5HT & NE at Substantia Gelatinosa in dorsal horn – modulate
the pain inputs from peripheral nociceptors
• Delays pain impulse conduction
• Gives pain/ inflammation free time for disc herniation to settle down by natural
process (Natural history of disc disease)

Sacroiliac Dysfunction
unilateral, dull pain that extends into buttock & posterior thigh
ASIS or PSIS may appear asymmetric bilaterally
leg-length discrepancy
↑ pain w/ standing on one leg & stair climbing
↑ pain w/ lateral flexion toward injured side
↑ pain w/ straight leg raises beyond 45º
--common after MVAs, pregnancy, fusion
Treatment: PT, Brace, NSAIDs, yoga, etc…interventional options: inject, ablate, fuse

Common Types of Neck Pathology
1)Myofascial Pain
2)Facet mediated pain
3)Disc Mediated pain: herniations, annular tears

Neck Myofascial Pain
Definition: regional muscle pain disorder accompanied by
trigger points(discrete point of tenderness, palpable in a
taut band of muscle)
Treatment: PT, NSAIDs, MRs, behavioral tx, TPIs, Botox,
dry needling, etc

Cervical Facet Mediated Pain
1) Similar to lumbar facetogenic pathology
2) Common after whiplash injury
3) Often includes radiating occipital headache
4) 50% of population over 50y/o and 75% over 65 y/o have
radiologic evidence of cervical spondylosis
1) Treatment: similar to lumbar
1) NSAIDs, TCAs, PT, TENS
2) Interventional options: facet joint steroid injections vs MBB/RFA

Cervical Disc Pathology
Similar to Lumbar; ie radicular component, however,
radiculopathy does not always mean radiation to the hand
MRI with spinal cord edema, would recommend surgical
consult
Treatments include: PT, NSAIDs, MRs, rest, ice, heat; anti-
convulsents, etc;
Interventional options: epidural steroid injection

Piriformis syndrome
Radiating pain in the buttock,
posterior thigh and lower leg)
and the physical exam finding of
tenderness in the area of the
sciatic notch.
The pain is exacerbated with
activity, prolonged sitting, or
walking.
The diagnosis is largely clinical
and is one of exclusion.
In physical examination, attempts

Advanced Interventional Pain Procedures
1) Sympathetic Nerve Blocks
2) Head and Facial Blocks
3) Spinal Cord Stimulation
4) Intrathecal Drug Delivery
5) Vertebral Augmentation

Sympathetic Nerve Blocks
1)Helpful for a multitude of sympathetically mediated pain
syndromes including(but not limited to) CRPS I and II;
abdominal pain; pelvic pain; perineal pain;
1)Stellate Ganglion
2)Celaic/Splanchnic
3)Superior Hypogastric Plexus
4)Ganglion Impar

Head and Facial Blocks
1)Helpful for a multitude of headache and or facial pain
syndromes; including migraine, Trigeminal neuralgia, etc
1)GONB, SONB, ATNBs, etc
2)Trigeminal nerve block
3)Botulinum toxin

Spinal Cord Stimulation
Indications: CRPS I and II; Radiculopathy; Failed Back
Surgery Syndrome; Arachnoiditis; PHN; Phantom Limb;
Ischemia secondary to PVD; Intractable Angina
**Patients able to “try before buy” with temporary implant
Evolving therapy: Improved technologies over past 5 years
including wave-form technologies; Battery technology;
MRI compatibility; and specific DRG therapy

Intrathecal Drug Delivery
Indications:
1)Severe pain from: Failed back surgery syndrome;
Cancer pain, CRPS I and II; Arachnoiditis; Chronic
pancreatitis
2)Severe Spasticity from: stroke, brain injury, cerebral
palsy, MS, spinal cord injury

Vertebral Augmentation
1)Diagnosis: Often under diagnosed; ultimately need MRI to
eval STIR image; or bone scan if MR contraindicated
2) Pain worse with standing, sitting; rolling out of bed
excruciating; LE symptoms may indicate another etiology
or concurrent one, ie spinal stenosis, radiculopathy
3) High success rate; complications minimal; ONLY “FIX”
for IPM Physicians
4)NEJM- Kalmes/Buchbinder studies both downgraded in
2013 after meta-anlaysis