Embed Size (px)
Citation preview
Interventional Treatment VTE: Radiologic Approach
Hae Giu Lee, MDProfessor, Dept of Radiology
Seoul St. Mary’s HospitalThe Catholic University of Korea
Introduction
• Incidence– High incidence: 250,000-1,000,000/year in US– In Korea: increased in incidence
• Aging society• Malignancy• High detection rate
DVT of lower extremities
• High detection rate
• Risk Factors•Old age, Debilitating state, Malignancy, Major surgery•Hypercoagulability, Pregnancy, Contraceptive, Hormonal therapy•Antiphospholipid antibody syndrome, Inflammatory bowel disease, SLE, •Varicose vein, Previous DVT, Central venous catheter
Introduction
• Post-thrombosis syndrome– Pain, swelling, skin discoloration, heaviness, venous
claudication & ulceration– Iliofemoral DVT
• High incidence & worse prognosis• Rarely recanalize via endogenous processes
Complications of DVT
• Rarely recanalize via endogenous processes• Persistent outflow obstruction-High venous pressure• Higher incidence of recurrent DVT than infrainguinal
thrombosis– Damaged venous valve & obstruction
• Rapid progression in recurrent thrombosis– Incidence: 1 yr - 17.3%, 8 yr – 29%
• Severity of DVT & Occ. of PTS: low correlation– Worse life quality
Br J Radiol 2009;82:198, Arch Intern Med 2002;62:1144, Arch Intern Med 2004;164:17, J Vasc Surg 2009;49:704
Introduction
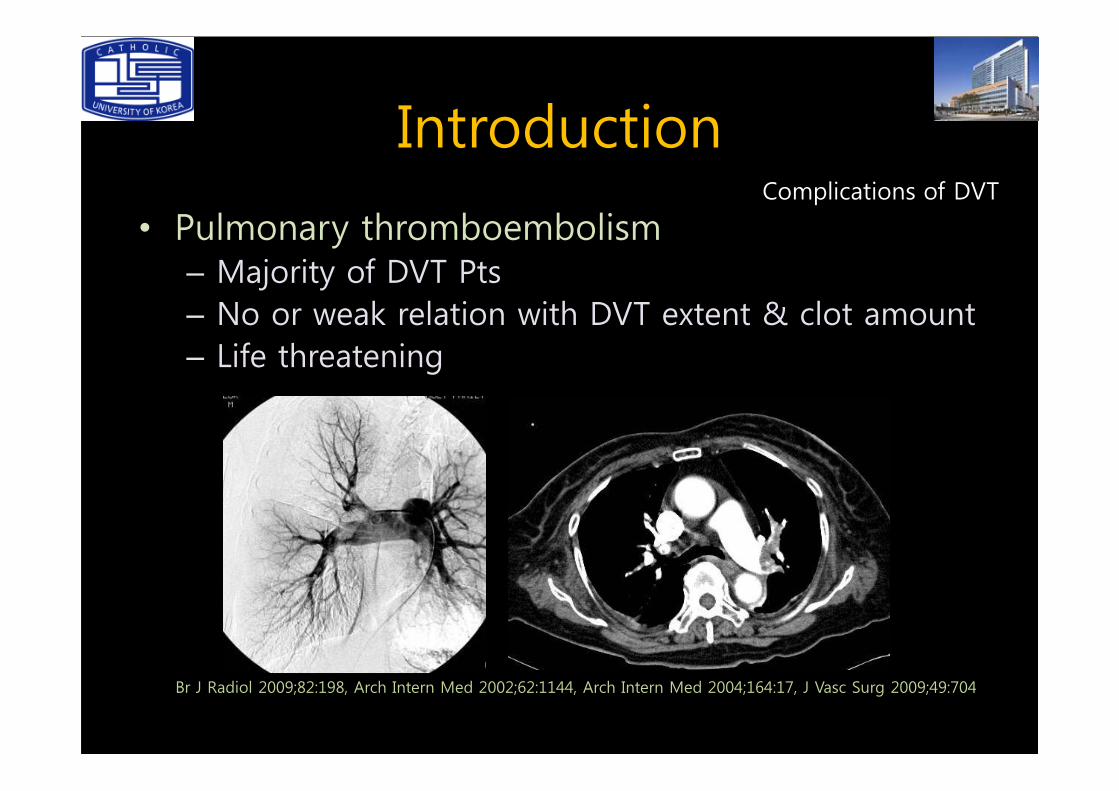
• Pulmonary thromboembolism– Majority of DVT Pts– No or weak relation with DVT extent & clot amount– Life threatening
Complications of DVT
Br J Radiol 2009;82:198, Arch Intern Med 2002;62:1144, Arch Intern Med 2004;164:17, J Vasc Surg 2009;49:704
Introduction
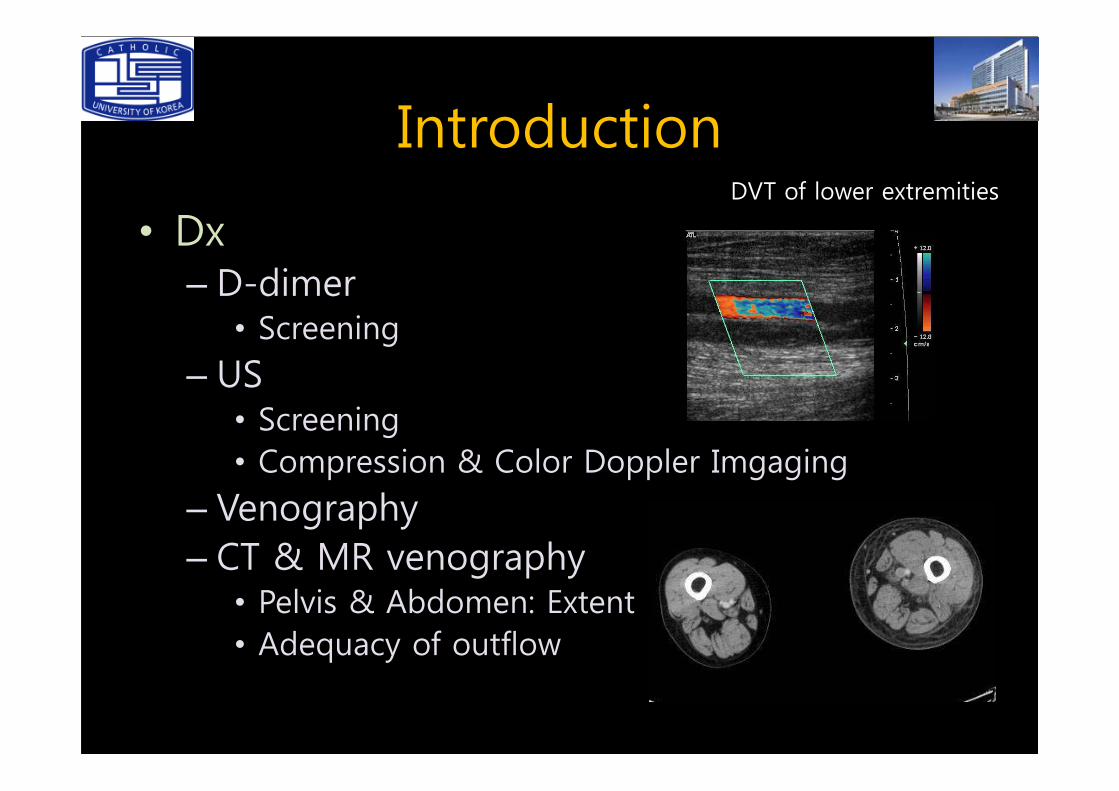
• Dx– D-dimer• Screening
– US
DVT of lower extremities
US• Screening• Compression & Color Doppler Imgaging
– Venography– CT & MR venography• Pelvis & Abdomen: Extent• Adequacy of outflow
Introduction
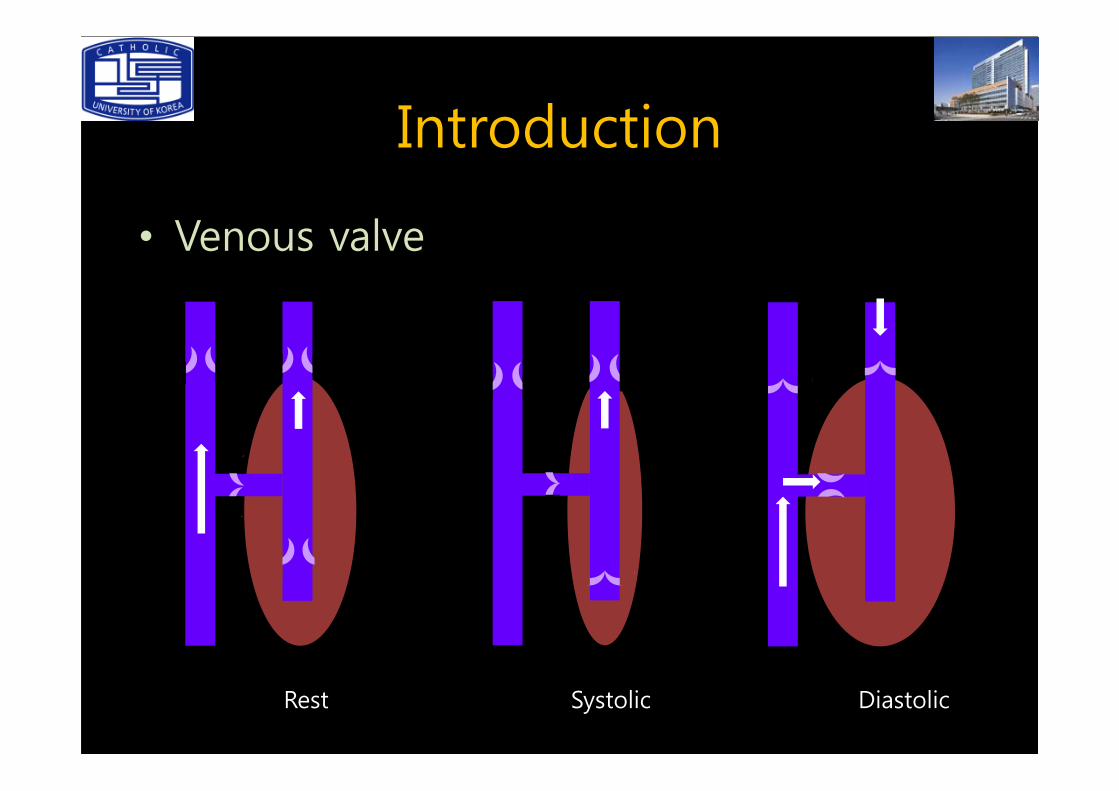
• Venous valve
Rest Systolic Diastolic
Introduction
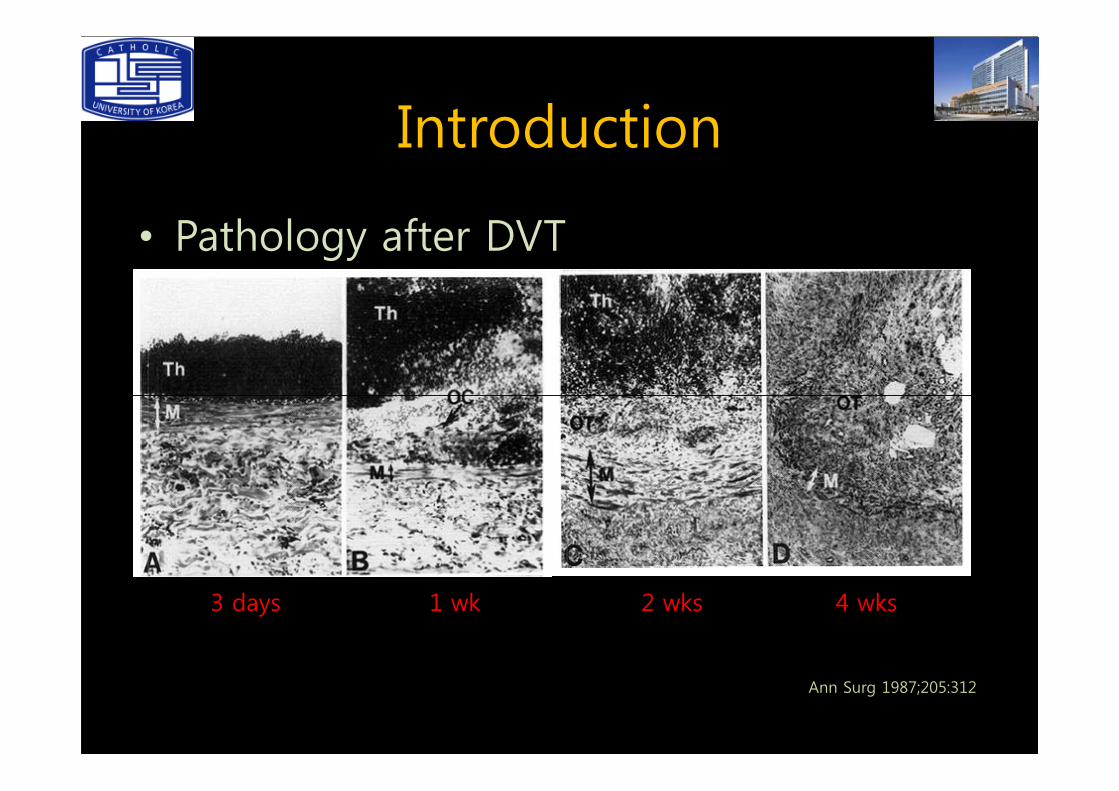
• Pathology after DVT
Ann Surg 1987;205:312
3 days 2 wks1 wk 4 wks
Introduction
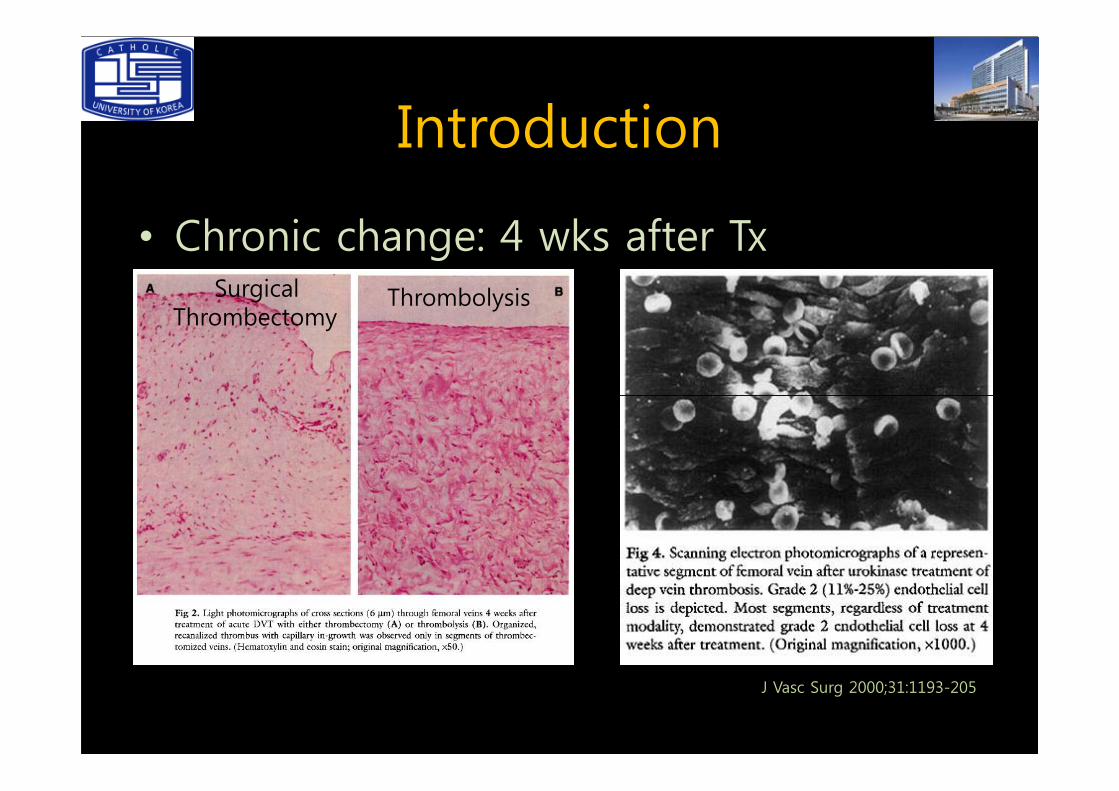
• Chronic change: 4 wks after TxSurgical
ThrombectomyThrombolysis
J Vasc Surg 2000;31:1193-205
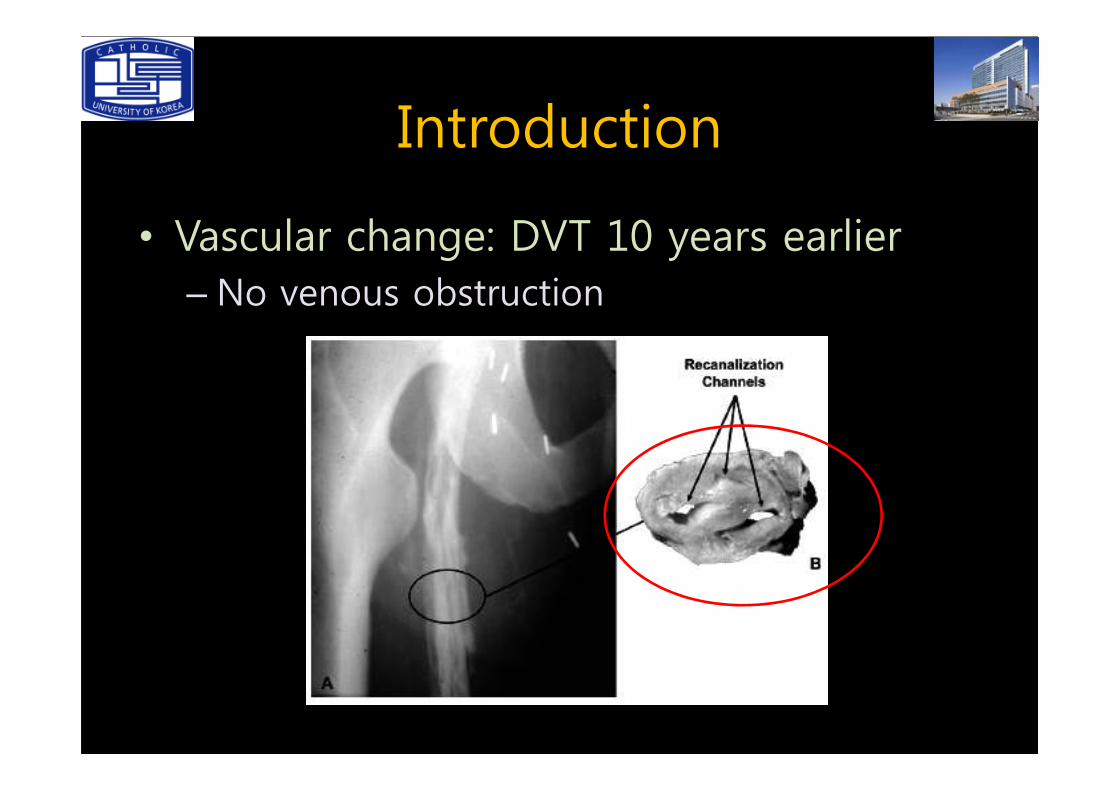
Introduction
• Vascular change: DVT 10 years earlier– No venous obstruction
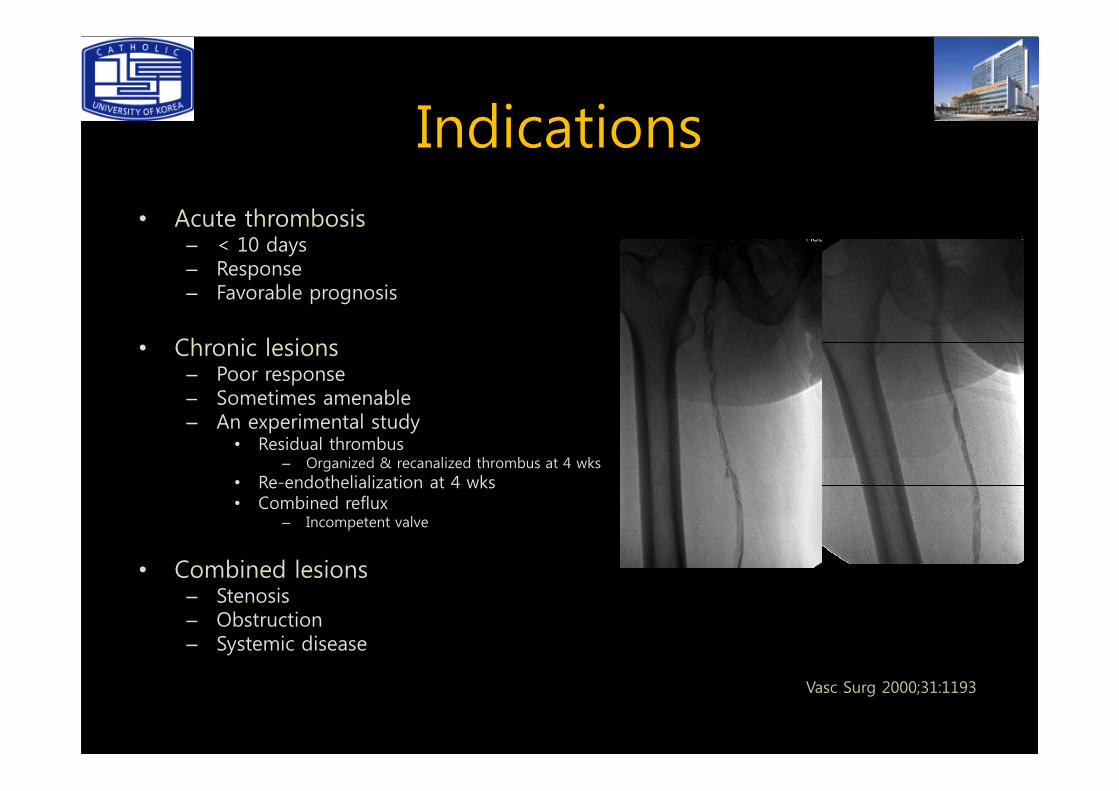
Indications• Acute thrombosis
– < 10 days– Response– Favorable prognosis
• Chronic lesions– Poor response– Sometimes amenable– Sometimes amenable– An experimental study
• Residual thrombus– Organized & recanalized thrombus at 4 wks
• Re-endothelialization at 4 wks • Combined reflux
– Incompetent valve
• Combined lesions– Stenosis– Obstruction– Systemic disease
Vasc Surg 2000;31:1193
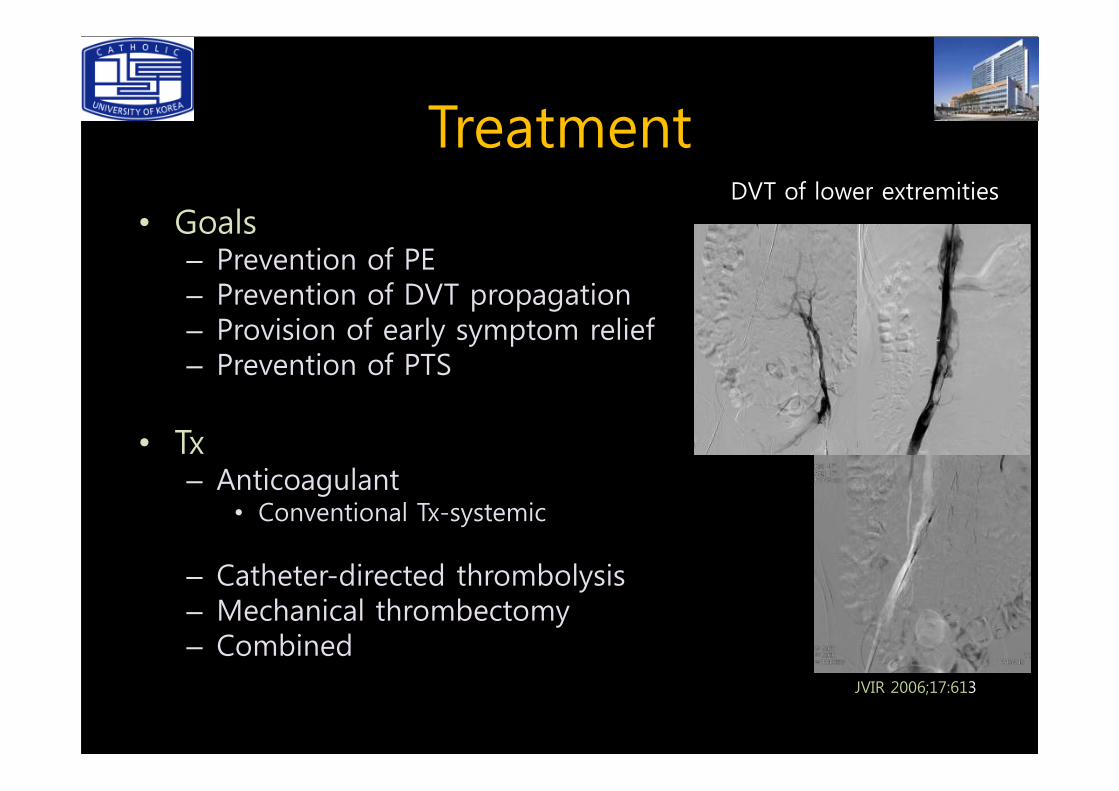
Treatment
• Goals– Prevention of PE– Prevention of DVT propagation– Provision of early symptom relief– Prevention of PTS
DVT of lower extremities
• Tx– Anticoagulant
• Conventional Tx-systemic
– Catheter-directed thrombolysis– Mechanical thrombectomy– Combined
JVIR 2006;17:613
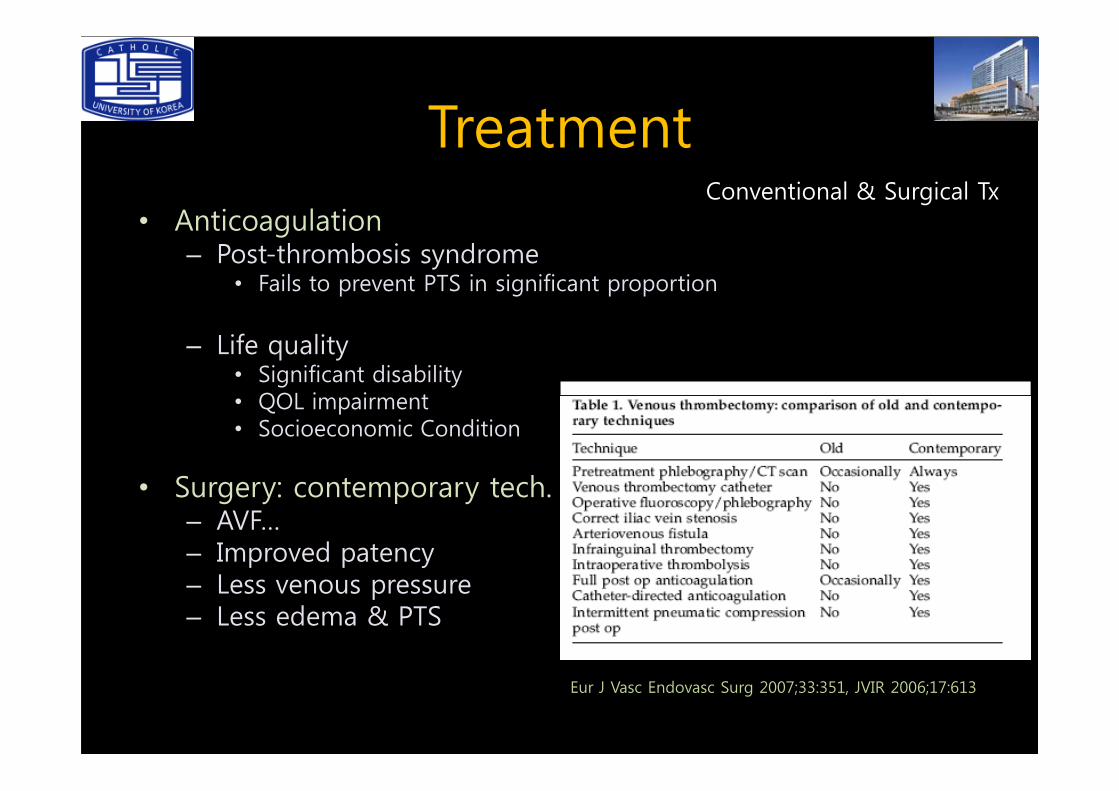
Treatment• Anticoagulation
– Post-thrombosis syndrome• Fails to prevent PTS in significant proportion
– Life quality• Significant disability• QOL impairment
Conventional & Surgical Tx
• QOL impairment• Socioeconomic Condition
• Surgery: contemporary tech.– AVF…– Improved patency– Less venous pressure– Less edema & PTS
Eur J Vasc Endovasc Surg 2007;33:351, JVIR 2006;17:613
Treatment
• Catheter-directed thrombolysis– Decreases incidence of PTS
• Early thrombosis removal• Normal valvular function
– 72% vs 12%(anticoagulation)
Interventional Tx
– 72% vs 12%(anticoagulation)
– Improved QOL– Faster Sx relief than anticoagulation
• Hours to days
• PE & PE related death: 0.9% & 0.1%Radiology 1999:211:39, JVIR 2005;16:815, J Vasc Surg 2000;32:130, JVIR 2006;17:613
Treatment
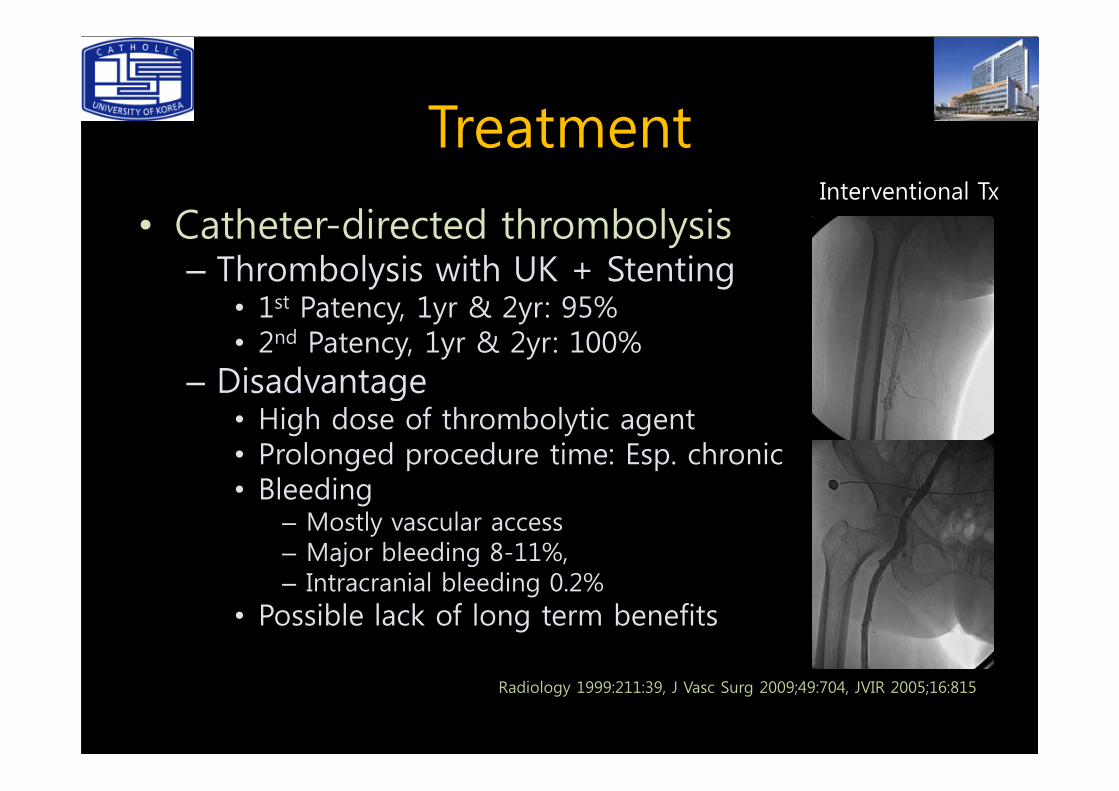
• Catheter-directed thrombolysis– Thrombolysis with UK + Stenting
• 1st Patency, 1yr & 2yr: 95% • 2nd Patency, 1yr & 2yr: 100%
– Disadvantage
Interventional Tx
– Disadvantage• High dose of thrombolytic agent• Prolonged procedure time: Esp. chronic• Bleeding
– Mostly vascular access– Major bleeding 8-11%, – Intracranial bleeding 0.2%
• Possible lack of long term benefits
Radiology 1999:211:39, J Vasc Surg 2009;49:704, JVIR 2005;16:815
TreatmentInterventional Tx
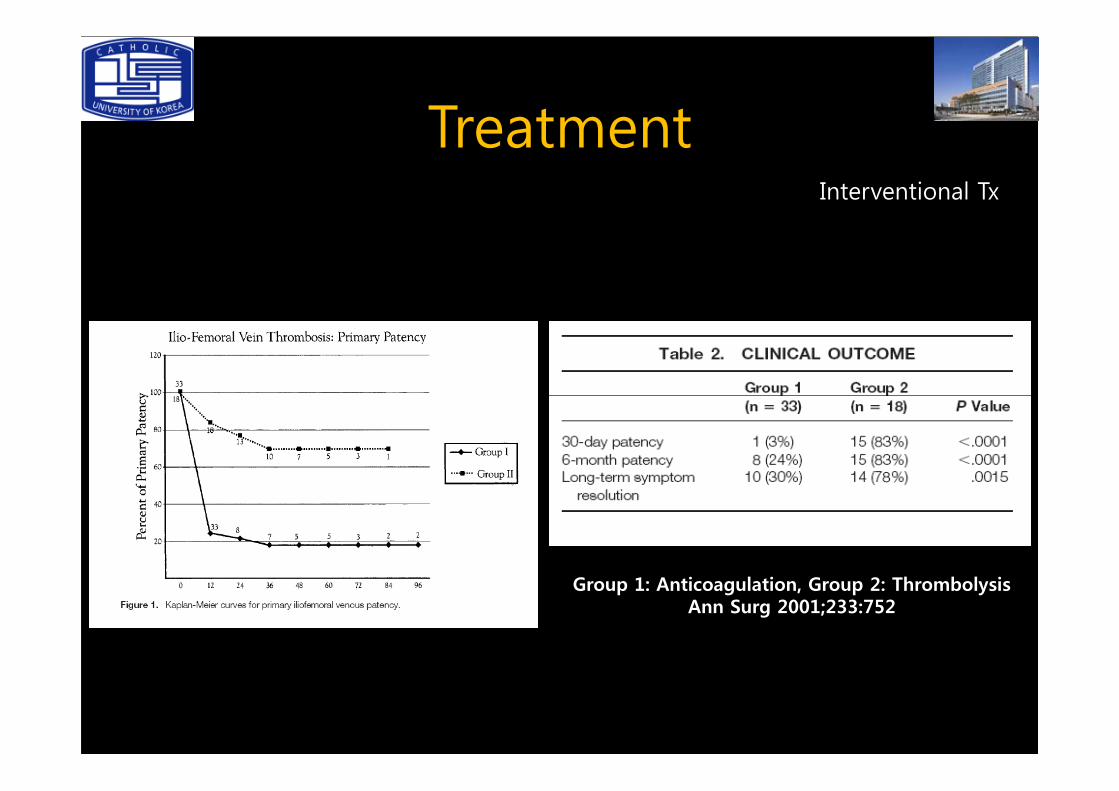
Group 1: Anticoagulation, Group 2: ThrombolysisAnn Surg 2001;233:752
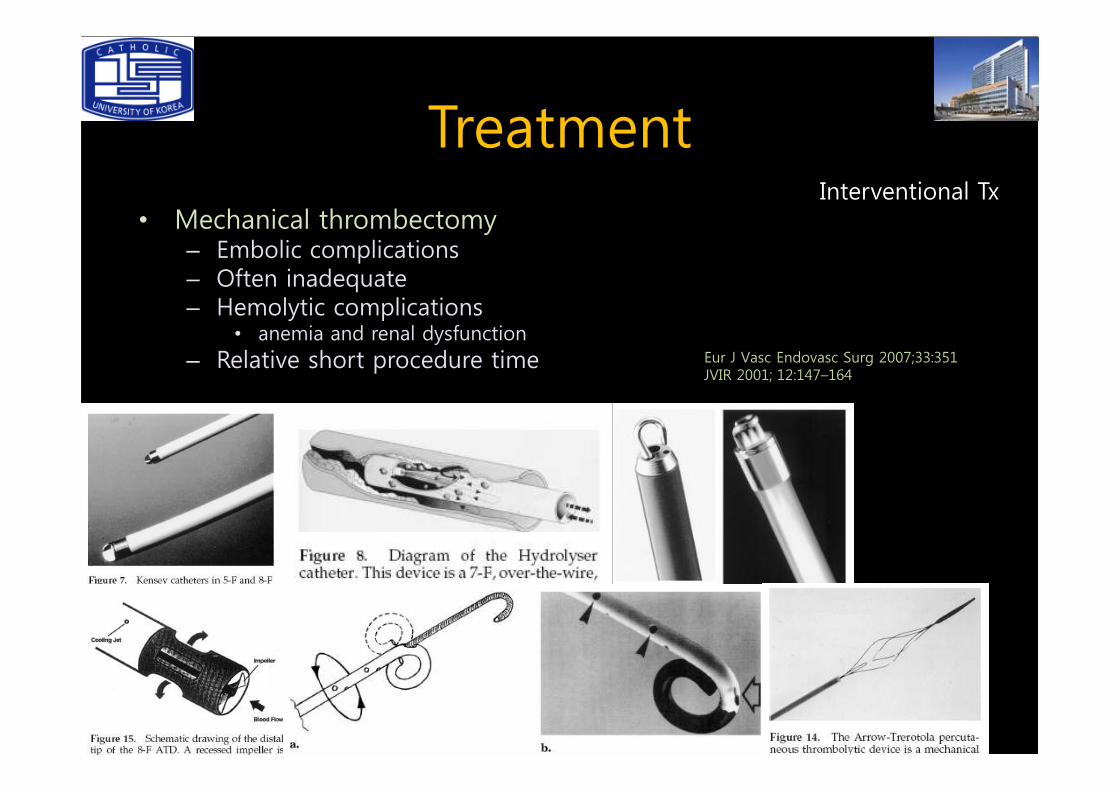
Treatment• Mechanical thrombectomy
– Embolic complications– Often inadequate– Hemolytic complications
• anemia and renal dysfunction– Relative short procedure time
Interventional Tx
Eur J Vasc Endovasc Surg 2007;33:351JVIR 2001; 12:147–164
Treatment
• Amplatz device– Rotational blender-like impeller• 100,000 to 150,000 rpm• Aspirate & re-circulate macerated thrombus
Mechanical thrombectomy
• Aspirate & re-circulate macerated thrombus
– Results• Removal of thrombus: 75-83%• 6 month patency: 77%
– Procedural related desaturation– No clinically significant PE
Eur J Vasc Endovasc Surg 2007;33:351
Treatment
• Arrow-Trerotola device– Rotational design
• 4 helically arranged nitinol wires• 3000 rpm
Re-circulates macerates thrombus
Mechanical thrombectomy
• Re-circulates macerates thrombus
– Thrombolytic therapy & angioplasty with stents• Technical & clinical success: 100%• 16-month: 92%
– Valve & intimal damage• No reports
Eur J Vasc Endovasc Surg 2007;33:351
Treatment
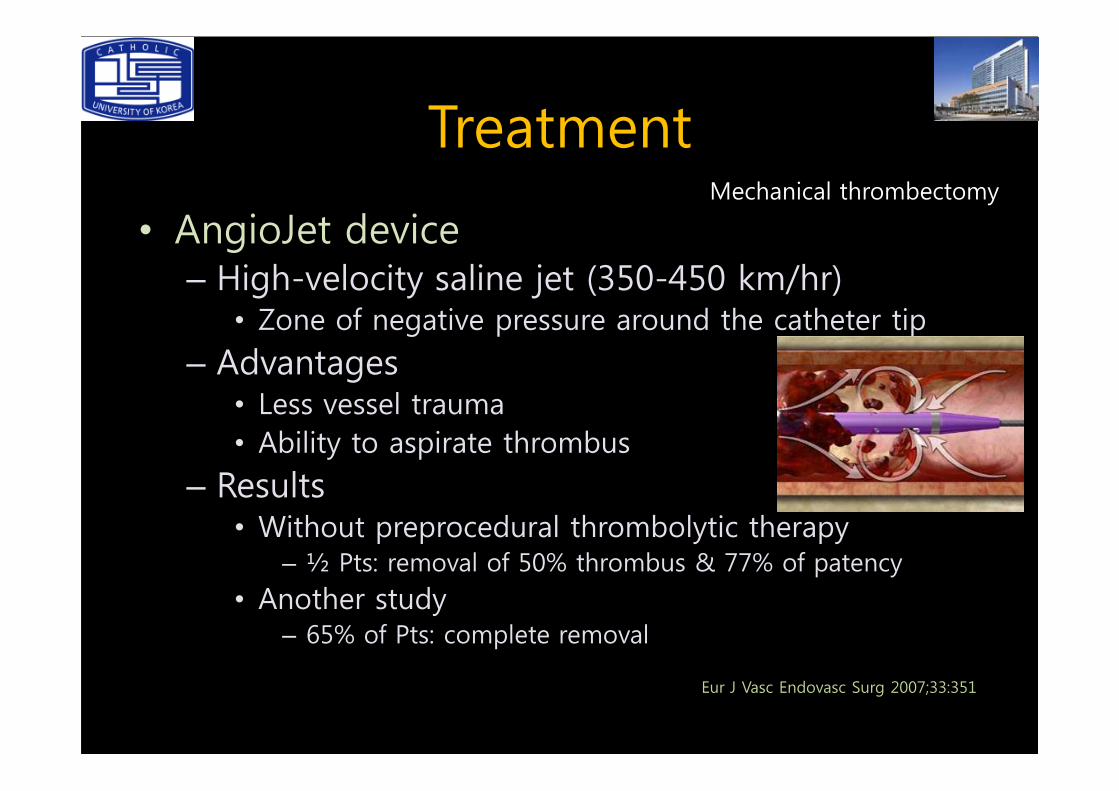
• AngioJet device– High-velocity saline jet (350-450 km/hr)
• Zone of negative pressure around the catheter tip
– Advantages• Less vessel trauma
Mechanical thrombectomy
• Less vessel trauma• Ability to aspirate thrombus
– Results• Without preprocedural thrombolytic therapy
– ½ Pts: removal of 50% thrombus & 77% of patency
• Another study– 65% of Pts: complete removal
Eur J Vasc Endovasc Surg 2007;33:351
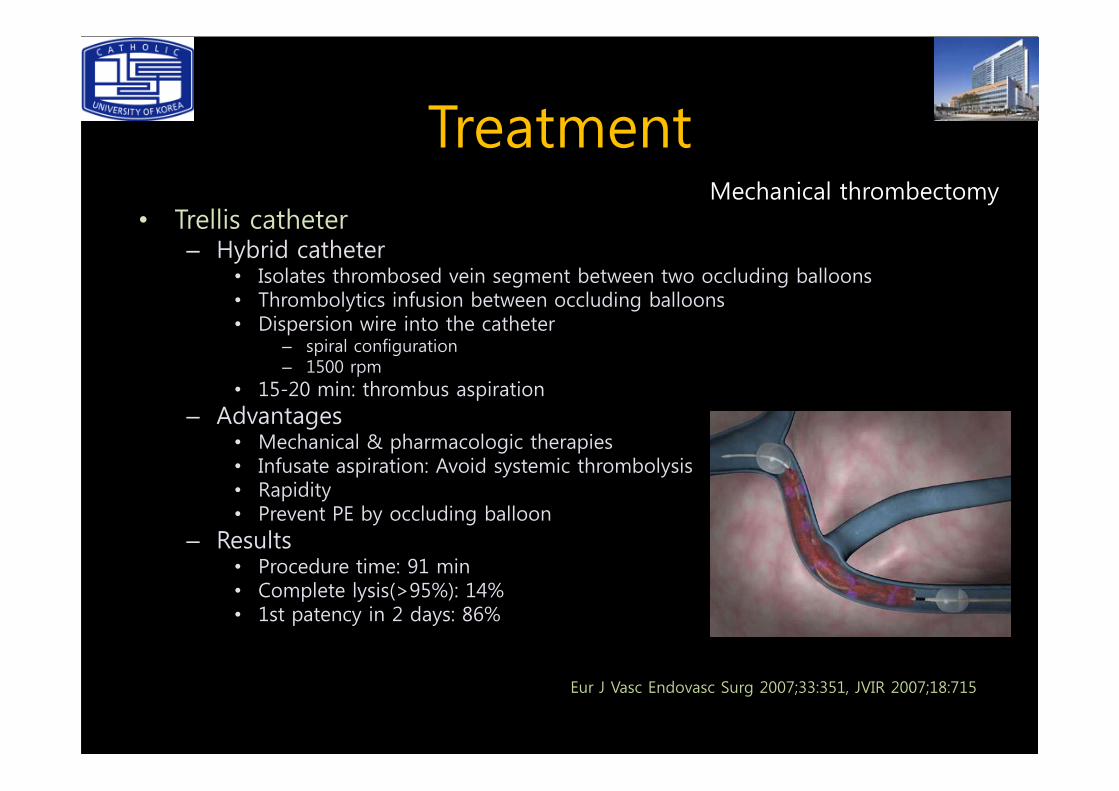
Treatment• Trellis catheter
– Hybrid catheter • Isolates thrombosed vein segment between two occluding balloons• Thrombolytics infusion between occluding balloons• Dispersion wire into the catheter
– spiral configuration– 1500 rpm
• 15-20 min: thrombus aspiration
Mechanical thrombectomy
• 15-20 min: thrombus aspiration– Advantages
• Mechanical & pharmacologic therapies• Infusate aspiration: Avoid systemic thrombolysis• Rapidity• Prevent PE by occluding balloon
– Results• Procedure time: 91 min• Complete lysis(>95%): 14%• 1st patency in 2 days: 86%
Eur J Vasc Endovasc Surg 2007;33:351, JVIR 2007;18:715
Treatment
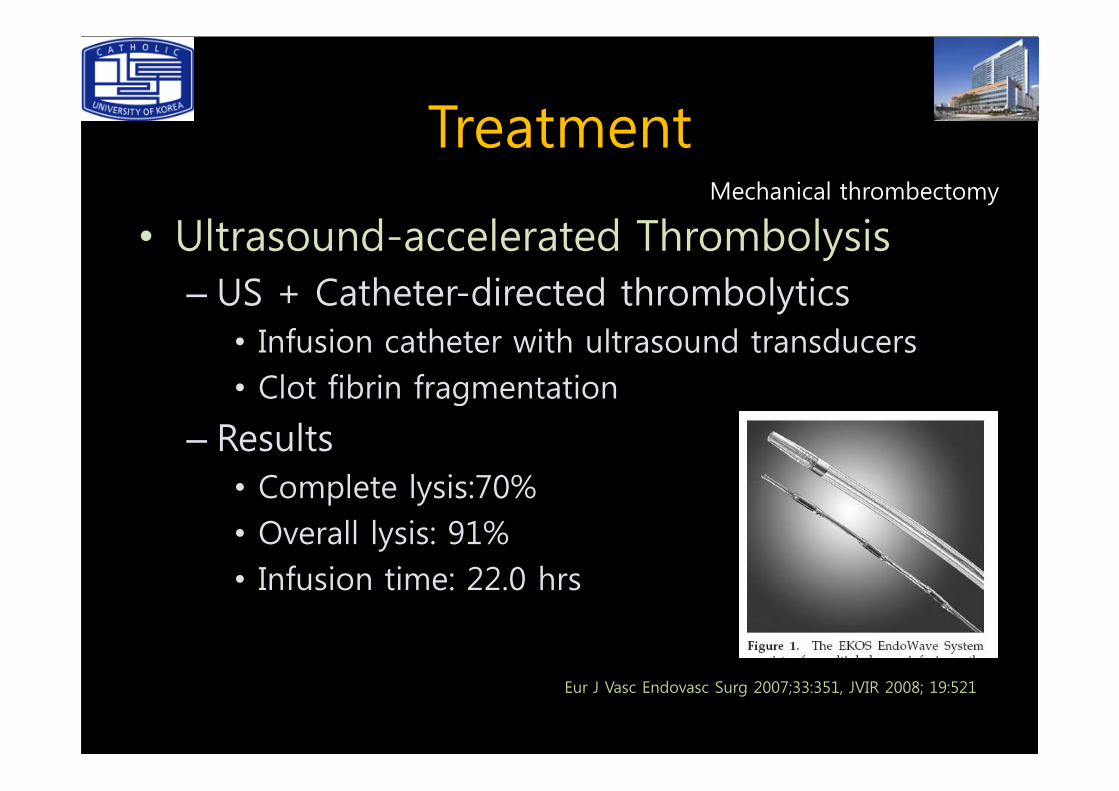
• Ultrasound-accelerated Thrombolysis– US + Catheter-directed thrombolytics• Infusion catheter with ultrasound transducers• Clot fibrin fragmentation
Mechanical thrombectomy
• Clot fibrin fragmentation
– Results• Complete lysis:70%• Overall lysis: 91%• Infusion time: 22.0 hrs
Eur J Vasc Endovasc Surg 2007;33:351, JVIR 2008; 19:521
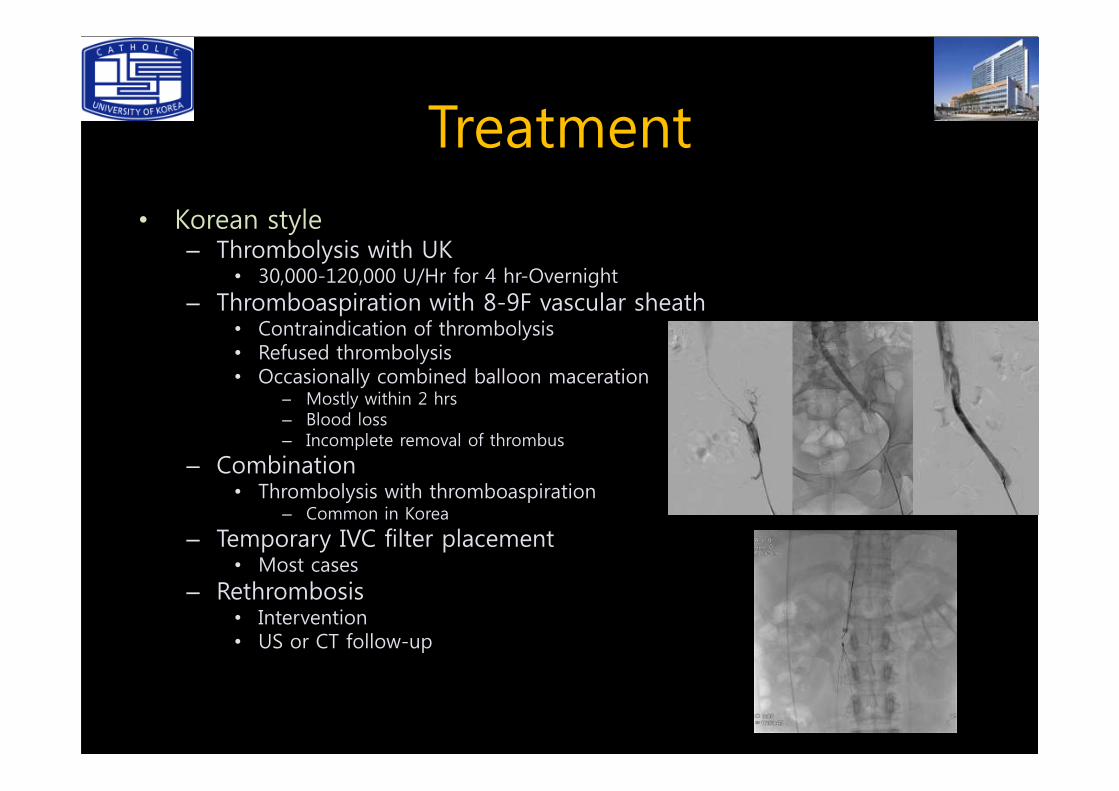
Treatment• Korean style
– Thrombolysis with UK• 30,000-120,000 U/Hr for 4 hr-Overnight
– Thromboaspiration with 8-9F vascular sheath• Contraindication of thrombolysis• Refused thrombolysis• Occasionally combined balloon maceration
– Mostly within 2 hrs– Mostly within 2 hrs– Blood loss– Incomplete removal of thrombus
– Combination• Thrombolysis with thromboaspiration
– Common in Korea
– Temporary IVC filter placement • Most cases
– Rethrombosis• Intervention• US or CT follow-up





























