Embed Size (px)
Citation preview
INTRA-ABDOMINAL
HYPERTENSION (IAH) AND
Abdominal Compartment
Syndrome (ACS)
Dr Punit D. Ghetia
MD,IDCCM.
Consultant Intensivist Banker’s Heart Institute.
WHAT WAS THEIR INTRA-ABDOMINAL PRESSURE?
Have you ever seen a critically ill patient
become progressively more swollen and
edematous after fluid resuscitation?
Have any of your ICU patients developed renal
failure requiring dialysis?
Have you ever seen a patient develop multiple
organ failure and die?
CASE: SEPTIC CHILD5 year / female child presenting with sepsis:
Treatment: Fluids, antibiotics, vasopressors
24 hours into therapy develops worsening
hypotension, oliguria, hypoxemia,
hypercarbia. PIP rises from 20 to 40 cm
IAP = 26 mm Hg decompressive
laparotomy
Immediate resolution of renal, pulmonary and
hemodynamic compromise
7 days later abdomen closed. Alive and well
now.DeCou, J Ped Surg 2000
CASE: DYSPNEA IN ER
67 year/female presenting to ER with pleurisy, dyspnea
Hypotensive, agitated.
IVF resuscitation, intubation, sedation
Worsened over next 4-6 hours - Difficult to ventilate, hypoxic/hypercarbic, hypotension, no UOP.
IAP = 45 mm Hg, abdominal ultrasound showed tense ascites paracentesis of 4500 cc fluid (IAP = 14)
Immediate resolution of renal, pulmonary and hemodynamic compromise.
Pathology shows malignant effusion – pancreatic CA.
Etzion, Am J EM 2004
CASE: ASPIRATION PATIENT
77 year male aspirated on general medicine floor. Transferred to MICU & intubated; hypotensive.
4.5 liters IVF overnight plus noradrenalin high dose
Anuric (35 ml urine in 8 hours).
IAP = 31 mm Hg.
USG-massively distended small and large bowel AND no free ascitic fluid.
Surgeon consulted for possible decompressivesurgery
Rx: NGT, Rectal Tube, oral cathartics
1 hour later: IAP 12 mm Hg, UOP 210 ml, noradrenaline discontinued.
Cheatham, WSACS 2006
CASE POINTS
Trauma is not required for ACS to develop: Intra-abdominal hypertension and ACS occur in
many settings (PICU, MICU, SICU, OR, ER).
IAP measurements are clinically useful: Help to determine if IAH is contributing to organ dysfunction
“Spot” IAP check results in delayed diagnosis SO TREND OF IAP IS ESSENTIAL and IAP monitoring will allow early detection and early intervention for IAH before ACS develops.
Waiting for clinically obvious ACS to develop before checking IAP worsen the problem.
DEFINITIONSWSACS*, ANTWERP BELGIUM 2007
*WORLD SOCIETY OF THE ABDOMINAL COMPARTMENT
SYNDROME
Intra-abdominal Pressure (IAP): Intrinsic pressure within the abdominal cavity
Intra-abdominal Hypertension (IAH): An IAP > 12 mm Hg (often causing occult ischemia) without obvious organ failure
Abdominal Compartment Syndrome (ACS): IAH with at least one overt organ failing
TYPES OF IAH /ACSWSACS, ANTWERP BELGIUM 2007
Primary – Injury/disease of abdomino-pelvic region, “surgical”
Secondary – Sepsis, capillary leak, burns, “medical”
Recurrent – ACS develops despite surgical intervention
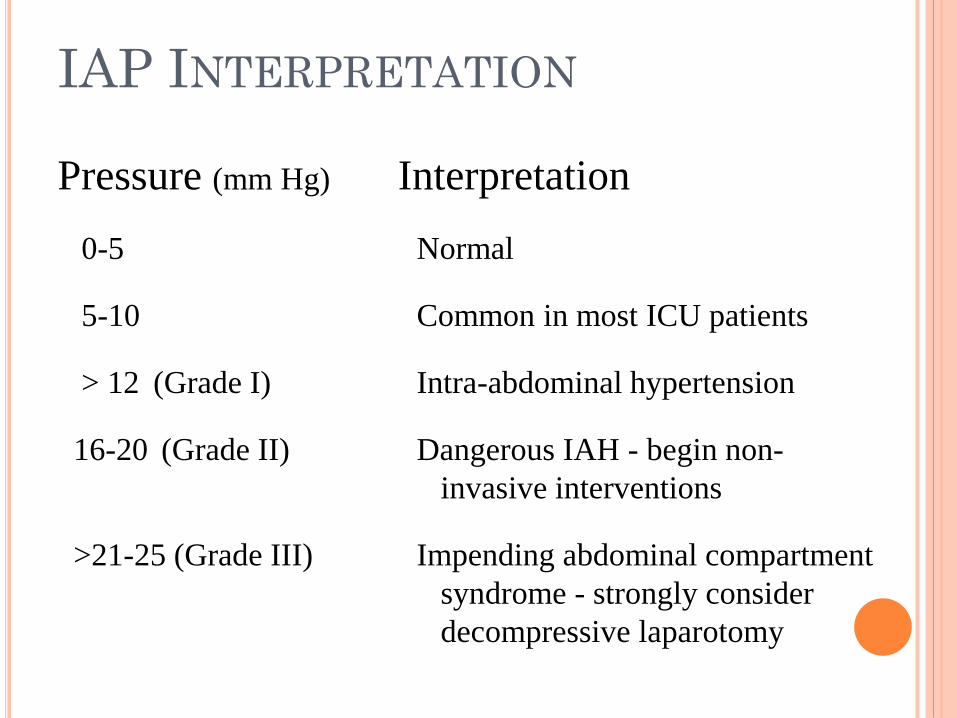
IAP INTERPRETATION
Pressure (mm Hg) Interpretation
0-5 Normal
5-10 Common in most ICU patients
> 12 (Grade I) Intra-abdominal hypertension
16-20 (Grade II) Dangerous IAH - begin non-
invasive interventions
>21-25 (Grade III) Impending abdominal compartment
syndrome - strongly consider
decompressive laparotomy
HISTORY:
Fietsam et al (1989) first to describe the
abdominal compartment syndrome (ACS) as the
collective effects of increased intra-abdominal
pressure (IAP) on the body.
Their description was in the setting of ruptured
abdominal aortic aneurysms.
Trauma literature now a major source of information.
In general, the trauma literature has recognized that
end organ dysfunction occurs in the presence of a
grossly distended and tense abdomen..So there was
“Open abdomen concept”.
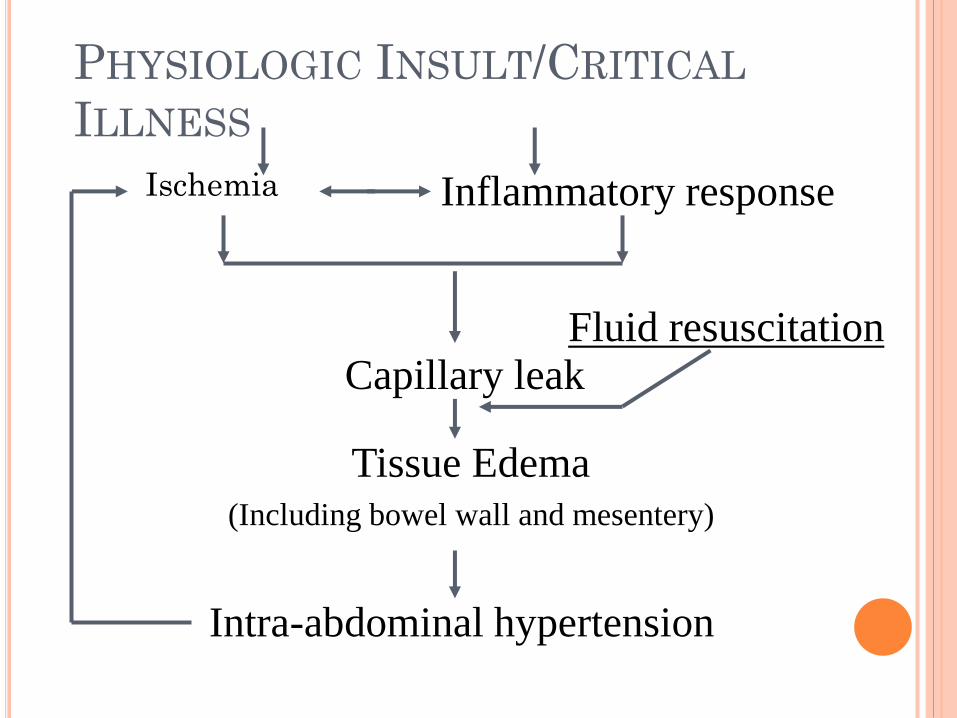
PHYSIOLOGIC INSULT/CRITICAL
ILLNESS
Ischemia Inflammatory response
Capillary leak
Tissue Edema (Including bowel wall and mesentery)
Intra-abdominal hypertension
Fluid resuscitation
CAUSES OF INTRA-ABDOMINAL
PRESSURE (IAP) ELEVATION
Major abdominal / retroperitoneal problem
Ischemic insult / SIRS requiring fluid
resuscitation with a positive fluid balance of 5
or more liters within 24 hours – (10 lb/4.5 kg
weight gain)
Cause are…..
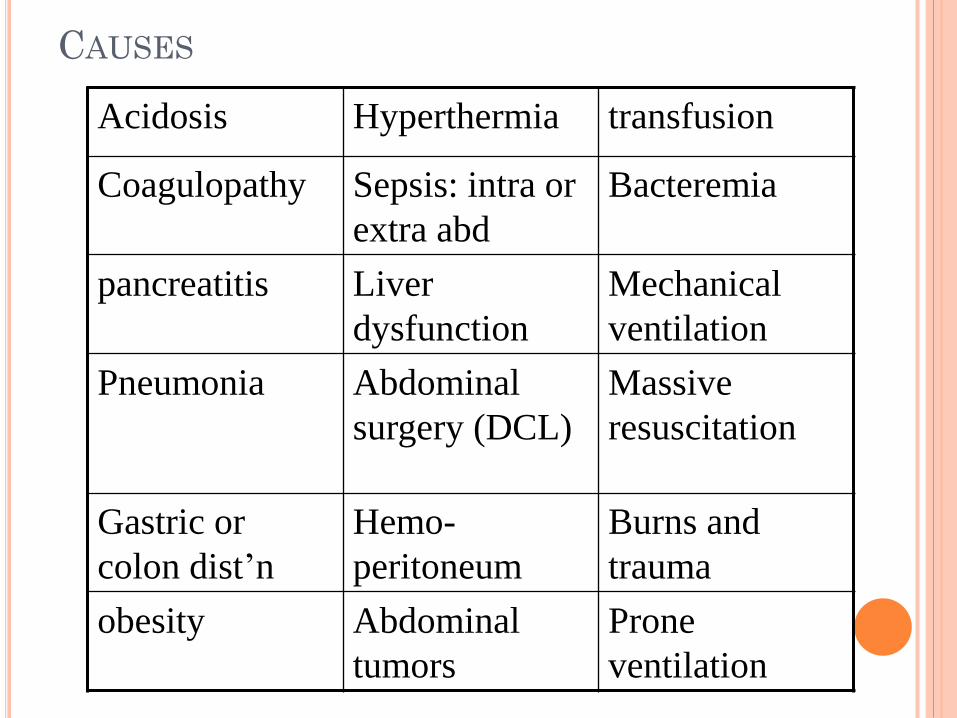
CAUSES
Acidosis Hyperthermia transfusion
Coagulopathy Sepsis: intra or
extra abd
Bacteremia
pancreatitis Liver
dysfunction
Mechanical
ventilation
Pneumonia Abdominal
surgery (DCL)
Massive
resuscitation
Gastric or
colon dist’n
Hemo-
peritoneum
Burns and
trauma
obesity Abdominal
tumors
Prone
ventilation
INTRA-ABDOMINAL
HYPERTENSION
&
ABDOMINAL
COMPARTMENT SYNDROME
Physiologic Sequelae
PHYSIOLOGIC SEQUELAE
Cardiac:
Increased intra-abdominal pressures cause: Compression of vena cava with reduced venous
return
Elevated intra-thoracic pressure with multiple negative cardiac effects
Result: Decreased cardiac output, increased SVR
Increased cardiac workload
Decreased tissue perfusion
Misleading elevations of CVP and PAWP
Cardiac insufficiency; cardiac arrest
PHYSIOLOGIC SEQUELAE
Pulmonary:
Increased intra-abdominal pressures causes: Elevated diaphragm, reduced lung volumes &
alveolar inflation, stiff thoracic cage,, increased interstitial fluid
Result: Elevated intrathoracic pressure (which further
reduces venous return to heart, exacerbating cardiac problems)
Increased peak pressures, reduced tidal volumes Barotrauma - atelectasis, hypoxia, hypercarbia ARDS (indirect - extrapulmonary)
PHYSIOLOGIC SEQUELAE
Gastrointestinal:
Increased intra-abdominal pressures causes: Compression / Congestion of mesenteric veins
and capillaries
Reduced cardiac output to the gut
The result: Decreased gut perfusion, increased gut edema
and leak
Ischemia, necrosis
Bacterial translocation
Development and progression of SIRS
Further increases in intra-abdominal pressure
PHYSIOLOGIC SEQUELAE
Renal:
Elevated intra-abdominal pressure causes: Compression of renal veins, parenchyma
Reduced cardiac output to kidneys
The Result:
Reduced blood flow to kidney
Renal congestion and edema
Decreased glomerular filtration rate (GFR)
Renal failure, oliguria/anuria Mortality of renal failure in ICU is over 50% - DO NOT
WAIT for this to occur!
PHYSIOLOGIC SEQUELAE
Neuro:
Elevated intra-abdominal pressure causes: Increases in intrathoracic pressure
Increases in superior vena cava (SVC) pressure with reduction in drainage of SVC into the thorax
The Result:
Increased central venous pressure
Increased intracranial pressure
Decreased cerebral perfusion pressure
Cerebral edema, brain anoxia, brain injury
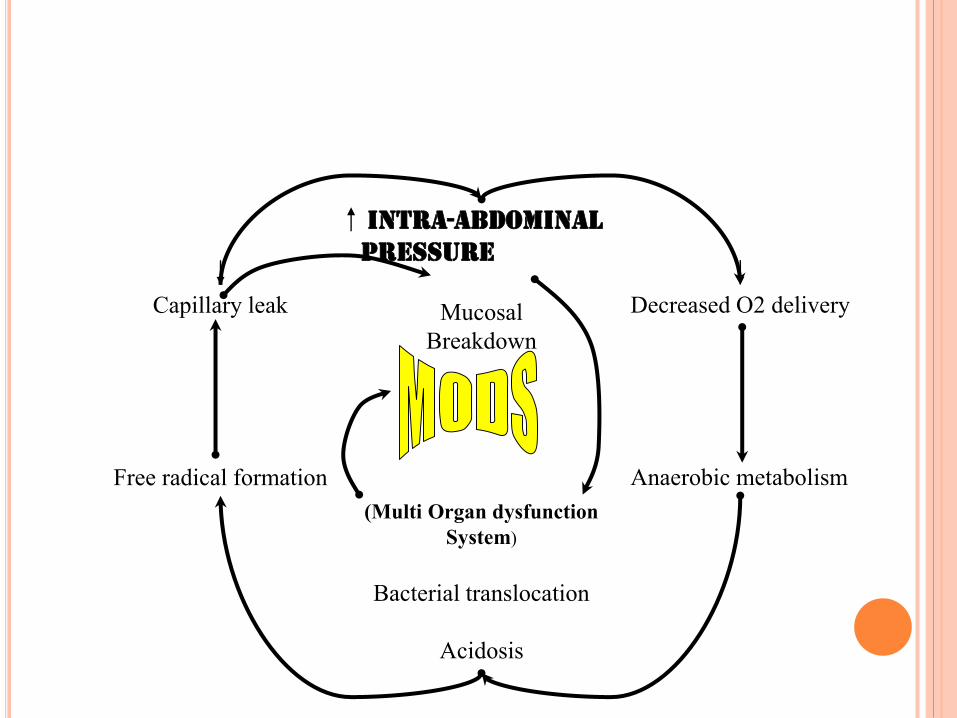
Intra-abdominal
Pressure
Mucosal
Breakdown
(Multi Organ dysfunction
System)
Bacterial translocation
Acidosis
Decreased O2 delivery
Anaerobic metabolism
Capillary leak
Free radical formation
IAH / ACS AFFECTS OUTCOMEPoints: IAH and ACS are common entities in the critical care
environment (including your own). IAH and ACS increase morbidity, mortality and ICU
length of stay…………
However: Clinical signs of IAH are unreliable and only show
up late in the clinical course …..SO
Early monitoring (TRENDS OF PRESSURE READINGS) & detection of IAH with early intervention is needed to reduce these complications.
INDEX OF SUSPICION: In following Settings,
Ascites
Bowel distention: mechanical obstruction/ileus
Bowel edema: resuscitation or ischaemia
Retroperitoneal hematoma
Hemoperitoneum
Coagulopathy
Trauma
Abdominal packing after damage control
surgery
DIAGNOSIS: Index of suspicion
When any signs of intra-abdominal hypertension are present:
Abdominal distention
Refractory oliguria
Hypercarbia
Refractory hypoxemia
Increasing PIPs
Refractory hypotension
INTRA-ABDOMINAL PRESSURE
MONITORING
Bladder pressure monitoring through the Foley catheter is:
The current standard for monitoring abdominal
pressures (Consensus, World Congress ACS Dec 2004)
Comparable to direct intraperitoneal pressure
measurements, but is non-invasive (Fusco 2001, Davis 2005, Risin 2006, Schachtrupp 2006)
More reliable and reproducible than clinical judgment(Kirkpatrick, CJS 2000; Sugrue World J Surg 2002)
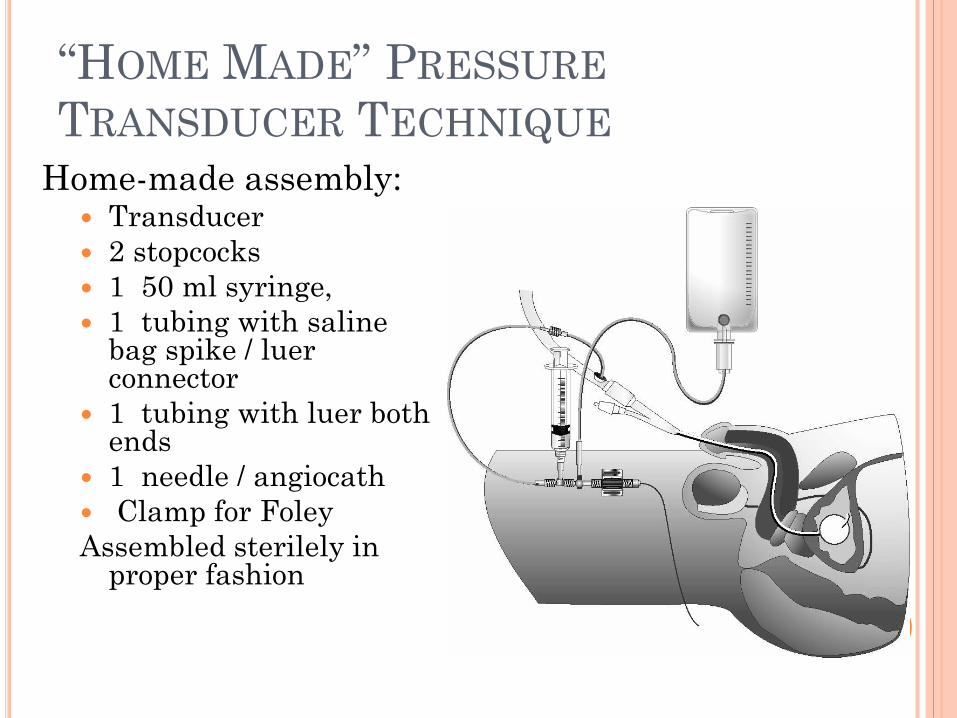
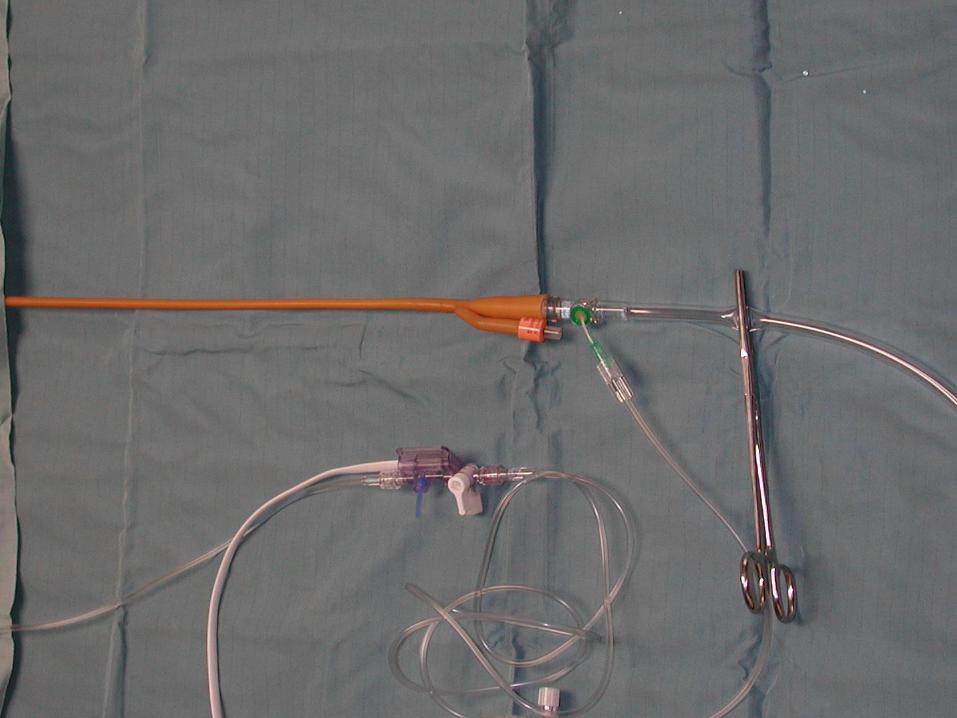
“HOME MADE” PRESSURE
TRANSDUCER TECHNIQUE
Home-made assembly: Transducer
2 stopcocks
1 50 ml syringe,
1 tubing with saline bag spike / luerconnector
1 tubing with luer both ends
1 needle / angiocath
Clamp for Foley
Assembled sterilely in proper fashion
27
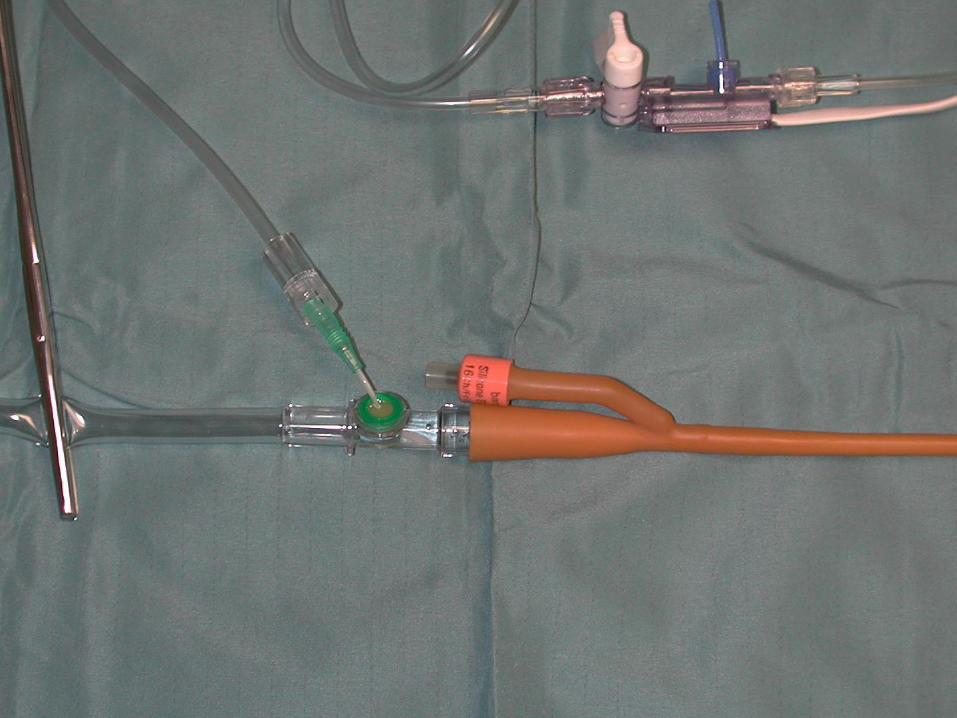
Method for Measuring the pressure
Insert a Foley catheter and clamp the tube distal
to the sample port
Instill 10-20 ml of saline into the bladder so as to
leave a continuous column of fluid from the
bladder to the sample port on the Foley
Insert a 18g catheter into the sample port and
connect to a CVP transducer
Level the transducer at the symphysis pubis Fusco et al J Trauma 2001
Guidelines for measurement by WSACS
Completely supine
Relaxed abdominal wall
mid-axillary line
25 mL saline into the bladder
“HOME MADE !” PRESSURE
TRANSDUCER TECHNIQUE
PROBLEMS:
Home-made !: No standardization
Sterility issues
Time consuming – therefore it is used infrequently due to the hassle factor (i.e. not monitoring - waiting for ACS !!!!)
Data reproducibility errors - what are the costs / morbidity of inaccurate or delayed information?
Other: Needle stick, recurrent penetration of sterile system, leaks, re-zeroing problems, failure to trend
BLADDER PRESSURE MONITORING:
HOW TO DO IT
Commercially available devices :
Foley Manometer – (Bladder manometer)
CiMon (Gastric)
Spiegelberg (Gastric)
AbViser – (Bladder transduction)
Advantages – Simple, standardized, reproducible,
time-efficient, sterile
ABVISER INTRA-ABDOMINAL PRESSURE
MONITORING KIT
Closed system in-line with the Foley
catheter
Once attached it is left in place during
entire time IAP is measured.
30 seconds to measure IAP
Standardized measurement
No reproducibility errors
INTRA-ABDOMINAL PRESSURE
MONITORING
How much fluid should be infused into the bladder?
The minimal amount of fluid required to obtain a reliable IAP measurement.
Too much fluid leads to bladder over distention and bladder wall compliance issues
Currently it appears that one never needs more than 25 ml in an adult, less (10-20 ml) is probably adequate
DIAGNOSIS;
Most papers suggest several measurements
during a 24 hr period: every 4 hrs
Repeat measurements are indicated by the
clinical appearance of the abdomen and on the
clinical situation (index of suspicion)
INTERPRETATION:
NORMAL IAP
3-15 mmHg
Obesity: higher (8 vs. 5 mmHg)
Age: no definite trend
Surgery: no definite trend
Comorbidities: trend to higher IAP with more
concurrent illnesses
Sanchez et al Am Surg Mar 2001
INTERPRETATION: As the pressure rises over 15 mmHg there
will be some evidence of hypoperfusion
Most will accept surgical decompression if the intra-abdominal pressure is over 20-25 mmHg.
More recent authors are advocating surgical decompression for IAP of 20-25 mmHg (Cheatham et al)
WSACS: suggests need for treatments above 12 mmHg
INTERPRETATION:….evidence
Decreased ACS with earlier decompression
Decreased mortality with earlier
decompression: ??? Need further study ..
More pronounced benefit with increasing age
MANAGEMENT OF IAH
AND ACS
Management:
Medical:
Maintain APP (Abdominal Perfusion Pressure) >60mmHg
Sedation / Analgesia
NMB
Supine positioning
NG / Colonic decompression
diuretics
ABDOMINAL PERFUSION PRESSURE
(APP)APP = MAP – IAP
APP :Abdominal Perfusion Pressure
MAP :MEAN ARTERIAL PRESSURE
IAP : INTRA ABDOMINAL PRESSURE
Abdominal perfusion pressure reflects actual gut
perfusion better than IAP alone
Optimizing APP to > 60 mm Hg should probably be
primary endpoint
Surgical:
Percutaneous tube drainage
Abdominal decompression
DECOMPRESSIVE LAPAROTOMY
• Delay in abdominal decompression
may lead to intestinal ischemia
• Decompress early!
TREATMENT: SURGICAL DECOMPRESSION /
DAMAGE CONTROL LAPAROTOMY
Surgical decompression involves opening
the abdominal wound and packing the
wound open or closing it with a plastic
dressing
Delayed closure can be done once the edema /
bleeding has resolved
Ascites can be drained percutaneously
DAMAGE CONTOL LAPAROTOMY:
Stone et al (1982)
Useful in Penetrating injuries to the abdomen
Try to Avoid hypothermia / acidosis / coagulopathy
Damage control surgery Involves:Rapid control of bleeding and contamination.Skin closure only or plastic tent closure.

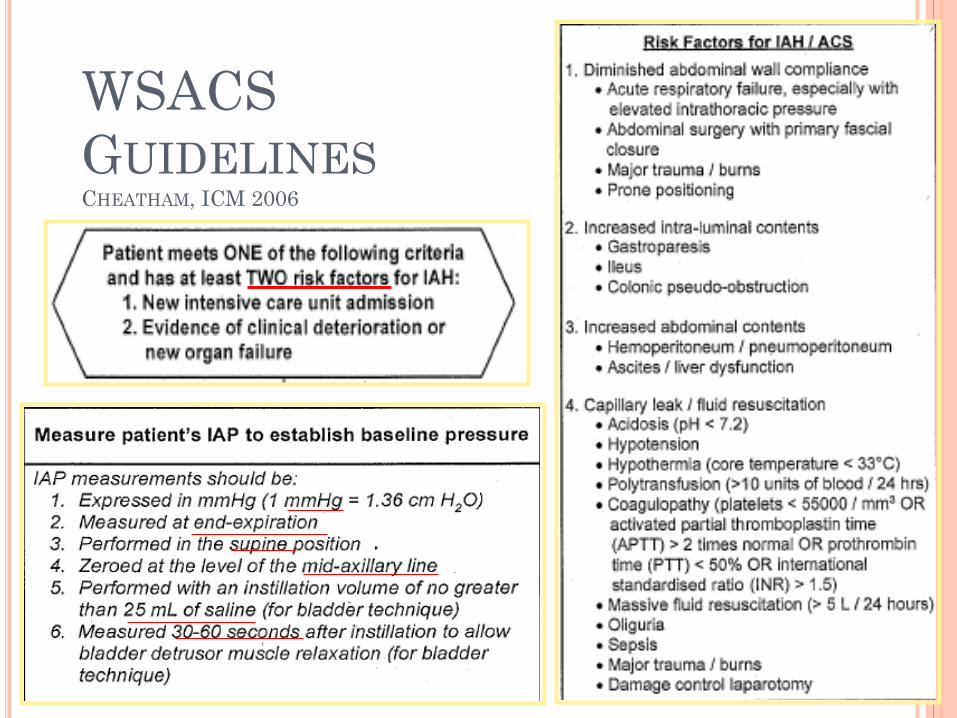
WSACS
GUIDELINESCHEATHAM, ICM 2006
SUMMARY:
IAP – measureable / preventable / treatable
ACS – end organ dysfunction from untreated or undertreated elevated IAP
Measurement: simple technique with an 18 g needle through the Foley port and a CVP transducer
Damage control – the standard for avoiding or treating elevated IAP or ACS
Deompressive laparotomy:
Most studies show a significant decrease in the IAP
Overall benefit for oxygenation (PaO2/FiO2) and increased urine output
Still Mortality Rate remained high at 35%
Do NOT wait for signs of ACS to check IAP
By then the patient has one foot in the grave!
You have lost your opportunity for medical therapy
Monitor all high risk patients early and often:
TREND IAP like a vital sign
30-50% of all ICU patients have some IAH and they are at risk for ACS and
in such high risk group ,1 in 11 suffer full blown abdominal compartment syndrome
FOR MORE INFORMATION
IAH and ACS Educational Web sites:
www.abdominal-compartment-syndrome.org





























